Today s workshop is sponsored by BSAS
|
|
|
- Kelley Allison
- 6 years ago
- Views:
Transcription

1
2 Today s workshop is sponsored by BSAS The Bureau of Substance Addiction Services: Provides access to addictions services for the uninsured Funds and monitors prevention, intervention, treatment and recovery support services Licenses addictions treatment programs and counselors Tracks statewide substance use trends Develops and implements policies and programs Supports the addictions workforce Helpful Websites: BSAS: Helpline: Careers of Substance:
3 Disclosure The Center for Social Innovation, Praxis and trainers do not receive any financial incentives from programs and providers that provide MAT or pharmaceutical companies.
4 Learning Goals 1. Understanding the effects of substance use disorders on the brain 2. Understanding the risks and benefits of medication-assisted treatment 3. Exploring prejudice and myths about MAT 4. Helping people with opioid use disorders make informed decisions about MAT 5. Learning how to access MAT resources
5 The Power of Language Medication assisted treatment vs. Medication assisted recovery

6 Opioid Overdose Deaths in Massachusetts

7 Opioid Overdose Deaths in Massachusetts
8 Compelling Reasons to Consider M.A.T. Most people who have overdosed on opioids have had treatment experiences that were not effective in bringing them relief from craving, relapse, and compulsive use Opioid overdoses are the leading cause of accidental death in the U.S. Research shows that MAT is effective in reducing relapse when used in combination with other psycho-social treatment and support strategies Between , fatal overdoses in Baltimore decreased by 50% as the availability of MAT increased (Schwartz et al, 2013)
9 Outcomes of MAT Medication assisted therapy is more effective than no MAT for opioid use disorder even with high-quality behavioral treatment MAT with maintenance produces substantially better outcomes than detoxification1 50% abstinent at the end of active treatment vs. 8% when medication is withdrawn Sources : 1. Weiss RD, Potter JS, Griffin ML, McHugh RK, Haller D, Jacobs P, Gardin J 2nd, Fischer D, Rosen KD. Adjunctive Counseling During Brief and Extended Buprenorphine-Naloxone Treatment for Prescription Opioid Dependence: A 2-Phase Randomized Controlled Trial Published in final edited form as: Arch Gen Psychiatry December; 68(12):
10 Opioids Opiates Opium Morphine Codeine Semi-Synthetic Heroin Hydrocodone Hydromorphone Oxycodone Oxymorphone Buprenorphine Synthetic Fentanyl Methadone Tramadol
11 The 3 Ways Opioids Are Produced 1. Your body makes its own opioids that moderate pain and produce feelings of pleasure and well being Endogenous opioids, such as beta endorphins 2. They are derived from the plant-based alkaloids related to the opium poppy Opiates: codeine, morphine, laudanum Travel the same pathways as endogenous opioids, but much more potent 3. They are partially or completely synthesized in a lab to produce the opioid response Heroin, oxycodone, fentanyl More efficiently target and alter brain chemical processes


12 Opioid Receptors in the Body
13 Czli
14 Susan s Brain
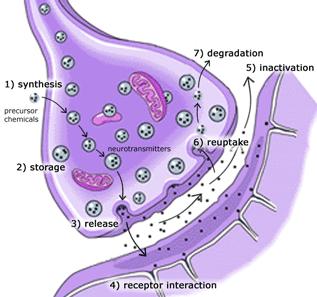
15 Synapse
16 Substance Use Disorders Are Conditions of Brain Chemistry Addictive drugs seem to match the transmitter system that is deficient Substance use disorders tend to be chronic diseases There are mild, moderate, and severe forms of the condition Detoxification is usually the first step in the total treatment process
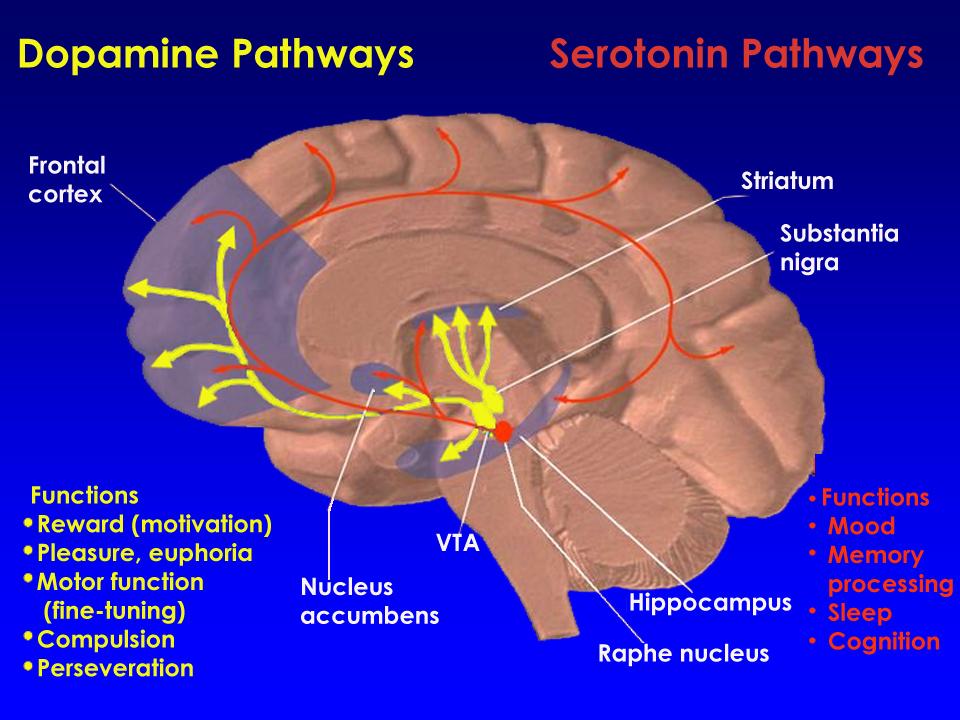
17 Drugs Associated with Neurotransmitters Why do people have drugs of choice? Dopamine Serotonin Endorphins GABA Glutamate Acetylcholine amphetamines, cocaine, alcohol LSD, alcohol opioids, alcohol benzodiazepines, alcohol alcohol nicotine, alcohol



18 Opioids: Dependence, Tolerance, and Substance Use Disorders Physical Dependence Withdrawal symptoms Tolerance Physiologic adaptations to opioid therapy Substance use disorders Compulsive use and maladaptive behaviors Savage SR, et al. J Pain Symptom Manage Jul;26(1):




19 Substance Use Disorders Involve Multiple Factors Biology/Genes Environment DRUG Brain Mechanisms Substance Use Disorders
20 Risk Factors for Substance Use Disorders Some people become physically dependent on opioid analgesics while taking them for pain but stop with minor difficulties while others experience intense cravings and compulsive use. What accounts for these different responses? o Heredity / Genetics o Willpower o Access o Education level o Mental health disorders o Strength of character o Intelligence o Environment o Modeling o Age of first use o Chronic pain o Illegal vs. legal substance o Childhood trauma o Early cigarette smoking
21 Risk Factors for Substance Use Disorders Some people become physically dependent on opioid analgesics while taking them for pain but stop with minor difficulties while others experience intense cravings and compulsive use. What accounts for these different responses? þ Heredity / Genetics o Willpower þ Access o Education level þ Mental health disorders o Strength of character o Intelligence þ Environment þ Modeling þ Age of first use þ Chronic pain o Illegal vs. legal substance þ Childhood trauma þ Early cigarette smoking




22 Opioids and Substance Use Disorders Lasting changes in the brain resulting from regular use: An endorphin deficiency that persists Tolerance Need for larger and larger amounts to get the desired effects or, after prolonged use, to feel normal. Continued use: the body relies on the drug; its own opioid production shuts down. Reacts if external supply is cut off: Withdrawal


23 Opioids and Mood: What goes up must come down Prolonged use = deficiencies in the brain s capacity to regulate mood Pre-existing depression = stronger reinforcing effects = increase risk of a substance use disorder

24 Opioids and Pain About 29%-60% of people with opioid use disorders deal with chronic pain Prolonged use = deficiencies in the body s capacity to neutralize pain Opioid use for chronic pain can lead to misuse and a substance use disorder
25 Opioids and Motivation Most people can t just walk away even when they want to Manage short periods, despite severe withdrawal Long-term recovery = dealing with continuous craving Altered brain chemistry = Long-term distress The brain s motivation mechanisms are affected Research shows better outcomes require counseling, recovery support and at least 12 month on medication.
 Partial Agonists Unable to fully activate opioid receptors even with very large doses (e.g., buprenorphine) Antagonists Occupy but do not activate receptors, hence blocking agonist effects (e.")
26 General Principles of Pharmacotherapies How each medication works PHARMACODYNAMICS Agonists Directly activate opioid receptors (e.g., morphine, methadone) Partial Agonists Unable to fully activate opioid receptors even with very large doses (e.g., buprenorphine) Antagonists Occupy but do not activate receptors, hence blocking agonist effects (e.g., naloxone)

27 The Medications: Methadone Methadone is a long-acting opioid medication that reduces cravings and withdrawal symptoms People stabilized on the right dose feel normal, can continue to work and perform daily tasks, like driving. Can be started at any time. Dispensed daily at licensed, registered clinics; long-term patients can be approved for take-home doses Recommended for people with histories of intense cravings and withdrawal; long use; those living with chronic pain or HIV/AIDS HIGH RISK of overdose at start of treatment and if combined with other substances such as alcohol and benzodiazepines RISK of serious heart problems & sudden cardiac death
28 The Ideal Candidates for Opioid Dependency Treatment with Methadone Have been objectively diagnosed with an opioid dependency. Recommended for people with higher levels of opioid dependency, intense cravings and withdrawals. A person who is pregnant. Not have a significant heart problem. Is willing to use this medication as part of a comprehensive treatment plan and understands that this medication does not take the place of therapy or counseling.

29 The Medications: Buprenorphine Buprenorphine is a long-acting opioid medication that reduces cravings and withdrawal symptoms Combined with naloxone to prevent misuse (Suboxone) A mono-drug formulation has buprenorphine alone. Clients stabilized on the right prescribed dose feel normal, can continue to work and perform tasks like driving. Available through doctors with special training and certification & at OTPs Up to a 30-day supply from pharmacies for clients making progress Can t be started until at least hours have passed since last opioid use RISK of overdose when combined with other substances such as alcohol and benzodiazepines. FDA approved for use in treatment of opioid use disorders in 2002
30 The Ideal Candidates for Opioid Dependency Treatment with Buprenorphine Have been objectively diagnosed with an opioid dependency Are willing to follow safety precautions for the treatment Have been cleared of any health conflicts with using buprenorphine Have reviewed other treatment options before agreeing to buprenorphine treatment Is willing to use this medication as part of a comprehensive treatment plan and understands that this medication does not take the place of therapy or counseling.
31 The Medications: Buprenorphine Buprenorphine s opioid effects increase with each dose until at moderate doses they level off, even with further dose increases. This ceiling effect lowers the risk of misuse, dependency, and side effects
32 Buprenorphine Safety People should use the following precautions when taking buprenorphine: Do not take other medications without first consulting your doctor. Do not use illegal drugs, drink alcohol, or take sedatives, tranquilizers, or other drugs that slow breathing. Physicians should monitors any liverrelated health issues that they may have.
33 Pregnant or Breastfeeding Women and Buprenorphine Limited information exists on the use of buprenorphine in women who are pregnant and have an opioid dependency. The the few case reports available have not demonstrated any significant problems resulting from use of buprenorphine during pregnancy. The FDA classifies buprenorphine products as Pregnancy Category C medications, indicating that the risk of adverse effects has not been ruled out.
34 Switching from Methadone to Buprenorphine Studies indicate that buprenorphine is equally as effective as moderate doses of methadone. Buprenorphine is unlikely to be as effective as more optimal-dose methadone. It may not be the treatment of choice for patients with high levels of physical dependency.
35 Switching from Methadone to Buprenorphine It is best to SLOWLY reduce the therapeutic dose of Methadone to 30 mg a day or less for at least a week, before discontinuing it completely for at least 36 hours before starting Buprenorphine.
36 Switching from Buprenorphineto Methadone Transferring from buprenorphine to methadone treatment is less complicated than the transition from methadone to buprenorphine. Methadone can be commenced 24 hours after the last dose of buprenorphine
37 Buprenorphine Misuse Potential Naloxone is added to buprenorphine to decrease the likelihood of diversion When taken as prescribed, buprenorphine s opioid effects dominate and blocks opioid withdrawals If sublingual tablets are crushed and injected the naloxone effect dominates and can bring on opioid withdrawals
38 Commencing Naltrexone Following Buprenorphine Maintenance Treatment To minimize the risk of withdrawal symptoms, naltrexone should be delayed for 5-7 days after the last buprenorphine dose. Doses of naltrexone taken earlier than this are likely to induce some withdrawal symptoms depending on the buprenorphine doses in the last few weeks of treatment.

39 The Medications: Naltrexone Naltrexone is an opioid blocker an antogonist it blocks euphoric and pain relieving effects of opioids; has a similar effect with alcohol Vivitrol: monthly long-acting injection Naltrexone: available in pill form Not a controlled substance; no potential for diversion; no need to taper. Injections through any doctor, P.A. or ARNP pills through pharmacies. Recommended for people with less intense withdrawal and cravings, highly motivated for recovery, adolescents and mandated clients. Must wait 7-10 days after last opioid use to begin without adverse affects HIGH RISK of overdose if people use large amounts override blocking effects or use after completing a period of treatment due to lowered tolerance.
40 The Ideal Candidates for Opioid Dependency Treatment with Vivitrol Have been objectively diagnosed with an opioid dependency Recommended for people with lower levels of opioid dependency. T Must be opioid-free for 5-7 days Not have a diagnosis of significant liver or kidney disease. Is willing to use this medication as part of a comprehensive treatment plan and understands that this medication does not take the place of therapy or counseling.
41 Stages of MAT Community providers use a four stage process 1 Induction: assessment, individualized starting dosages; HIGH RISK for overdose during this stage 2 3 Stabilization: adjustment to medication, withdrawal and cravings begin to be under control Maintenance: long-term phase of treatment lasting for months / years; periodic reassessment 4 Tapering: medically managed withdrawal through gradually reduced doses over a period of months
42 Regulatory Issues MAT for opioid use disorders is carefully regulated by federal agencies Research consistently shows treatments less than 90 days are not sufficient for long-term behavioral change Research outcomes for MAT for opioid use disorders are better when treatment continues for months
43 Federal Opioid Treatment Standards Required services: (42 CRF 8.12) General OTP shall provide adequate medical, counseling, vocational, educational and other assessment and treatment services. Medical Assessment Special services for pregnant clients Initial and periodic assessments Counseling-including health and harm reduction counseling
44 Essential Services in MAT Programs Initial and periodic assessment with goal setting Medical assessment and treatment Substance use counseling Vocational and educational assessment and counseling Health and prevention counseling (HIV, HCV STI) Linkage to basic supports Drug testing services and monitoring
45 Legal Issues + Driver s licenses; commercial license restrictions. + Protected by confidentiality and antidiscrimination laws + Employment protection + Government benefits + Child welfare, drug courts, probation/parole cannot legally require MAT to stop

46 Opioid Use Disorders: All Available Resources Chances of success improve we help people use all recovery supports Professional treatment services; substance abuse counseling Medications Person with Opioid Use Disorder Peer recovery support; family support; connections to community Other essential services; mental health, housing, medical care

47 A Real Life Example
48 What do people need to know to inform choices and make decisions about medication-assisted treatment? Outcome research on effectiveness of MAT Risks vs. benefits of medication options What to expect from MAT Providers that offer MAT How to talk to others about their decisions Sources of peer/community recovery support
49 Medication-Assisted Treatment: Outcomes When medications are part of a comprehensive treatment program: Decreases illicit opiate use Decreases injection drug use Decreases hepatitis and HIV infections Decreases sexually transmitted infections Decreases in overdose fatality rates Decreases criminal activity
50 Why Consider MAT? When programs incorporate MAT according to practice guidelines some of the outcomes include: Increases treatment retention Improves family stability Increases employment Cost effective treatment
51 Essential Question Can I or do I want to try MAT? Which MAT protocol is best for me? What will it take for me to use MAT?
52 Sequence of Decisions 1. Whether MAT is right for them 2. Which medication is right 3. How to get services that are supportive 4. What kinds of support are needed


53 Weighing the Risks and Benefits of MAT Benefits MAT Risks MAT Medication-assisted Treatment Benefits No MAT Risks No MAT
54 How do you help a person make decisions about MAT? 1. Conduct opioid overdose risk assessment 2. Explore treatment goals 3. Explore beliefs about MAT 4. Educate about the benefits of MAT 5. Educate about the services and supports available to people on MAT 6. Perform harm reduction interventions
55 Risks & Benefits of MAT Benefits Stabilizes brain functions Long term treatment can reverse some of the damage Allows people to function normally continue to work Relieves withdrawal symptoms and reduces craving Risks Withdrawal, if stopped abruptly Controlled substances w/abuse potential Medication side effects & interactions Risk of overdose or fatality, especially if taken with benzodiazapines
56 When do you help a person make decision about MAT? Intake Assessments Educational groups Counseling sessions Family meetings Every available opportunity
57 What do you do if a person decides not to participate in MAT? Harm reduction strategies including: Opioid overdose prevention education Opioid overdose risk assessment Train person and family members to use Narcan Provide resources for MAT in case the person changes his/her mind Offer all other services and supports available to help the person recover
58 Comparing Medication Options Benefit from structured programs Able to get an approved program Pregnant and post-partum women Have chronic pain People getting treatment for HIV/AIDS When can I start? Immediately Methadone How long do I take it? Best results when for at least 1 year Safe for long-term maintenance Periodic assessment for ongoing treatment based on individual needs What happens if I stop? Methadone withdrawal symptoms Gradual tapering doses reduces severity What if I use opioid drugs? High risk of overdose May not have euphoric effict Alcohol or other drug use increases risk Fatalities reported with benzodiazepines Buprenorphine Who does well? Are best treated in doctors offices Pregnant and post-partum women Are getting treatment for HIV/AIDS Motivated to try buprenorphine Able to adhere to medication treatment Starting/Stopping When can I start? hours after last use How long do I take it? Best results when taken 9 months or more Safe for long-term maintenance Periodic assessment for ongoing treatment based on individual needs What happens if I stop? Withdrawal, less intense, but unpleasant Gradual tapering reduces severity What if I use opioid drugs? Moderate to high risk of overdose May cancel out effects of other opioids Also moderate to high risk of overdose with alcohol or other substances Naltrexone Able to stop using for 7-10 days Mandated by court or employer Also benefit from avoiding alcohol Motivated to eliminate all opioids now Re-entering from prison or jail When can I start? After 7-10 days completely opioid-free Or risk of bringing on severe withdrawal symptoms How long do I take it? Long-acting injectable lasts 30 days Little effect with short-term treatment Most studies treat subjects for 5-6 months What happens if I stop? No withdrawal symptoms What if I use opioid drugs? Risk of overdose If taken while physicallly dependent on opioids, withdrawal can result Effects of opioids may be blocked
59 Information You ll Want from Your Provider What treatment options do you offer for opioid use disorders? What medication(s) do you use to treat opioid use disorders? How flexible is the program? Will I be able to do this with my work schedule? What are the costs? How do people pay for treatment? How soon can I begin treatment? What other kinds of help are available? Help with transportation HIV testing Help with benefits &coverage Support groups Childcare Recovery support services Counseling Other:
60 Information Your Provider Will Want from You Gather Your Information: ü List all your current health conditions and concerns. ü List the medications and supplements you use now. ü List the opioid drugs you have using, how long, and an estimate of how much. ü List any other legal or illicit drugs you use (for example: marijuana, tobacco, valium, alcohol, etc.). ü List dates and details of any past or current treatment for opioid use disorders (for example: where, when, and how it worked out).






61 MAT for Justice-Involved Clients STUDIES SHOW: Decreased recurrent drug use Increased follow up with community treatment upon release; lower recidivism Decreased criminal activity & arrests Decreased behavioral problems and parole/probati on violations Decreased in HIV risk behavior
62 Federal Government Set To Crack Down On Drug Courts That Fail Addicts WASHINGTON The federal government is cracking down on drug courts that refuse to let opioid addicts access medical treatments such as Suboxone, said Michael Botticelli, acting director of the White House s Office of National Drug Control Policy, on Thursday. Drug courts that receive federal dollars will no longer be allowed to ban the kinds of medication-assisted treatments that doctors and scientists view as the most effective care for opioid addicts, Botticelli announced in a conference call with reporters Huffington Post Feb. 6, 2015
63 SAMHSA & BJA Drug Court Grantees Under no circumstances may a drug court judge, other judicial official, correctional supervision officer, or any other staff deny the use of these medications when made available to the client under the care of a properly authorized physician prescription... Substance Abuse Mental Health Services Administration Applicants must affirm that the treatment drug court(s) for which funds are sought will not deny any eligible client for the treatment drug court access to the program because of their use of FDAapproved medications for the treatment of substance use disorders Bureau of Justice Assistance

64 Reentry and Drug Overdose In the first 2 weeks post-release, a former inmate s risk for death by drug overdose = 129 times the risk for the general population. Deaths per 100,000 Person Years Overall >9 Weeks After Release Binswanger IA, Stern MF, Deyo RA, Heagerty PJ, Cheadle A, Elmore JG, Koepsell TD. Release from prison-a high risk of death for former inmates. N Engl J Med. 2007;356(2):
65 Criminal Justice & Opioid Use Disorders in Massachusetts Opioid Task Force Recommendations: Increase availability of treatment at designated DOC facilities Increase use of injectable naltrexone (Vivitrol) for people with opioid use disorders returning to community from correctional facilities
66 MAT during Pregnancy If a pregnant woman stops opioids abruptly, withdrawal can harm the developing fetus Methadone is the oldest and best-research course of treatment; safe for the mother; no damage to fetal development Pregnant women treated with methadone are 3x times more likely to stay in treatment Promising studies show buprenorphine (the mono-drug formula only-subutex) is also safe Complete withdrawal not advised during pregnancy. Should not be attempted without medical supervision
67 MAT during Pregnancy Special challenges include: Few social supports, discrimination, harassment, even when seeking treatment Neo-natal abstinence syndrome manageable in newborns but may delay baby s discharge from hospital High risk of relapse after delivery, especially if MAT is discontinued too quickly
68 MAT for those with Mental Health Conditions Research shows that most people who are addicted to opioids have a mental health disorder (may or may not be diagnosed) Methadone-psychiatric medication interactions are a concern and monitoring and dosage adjustments are necessary Collaboration with mental health staff and community mental health centers is important People with mental health condition using MAT may need additional services and supports
69 MAT for those with Chronic Pain An estimated 29%-60% of people with opioid use disorders deal with chronic pain (CSAT, 2012a). Referral for pain management Providers with experience with pain management and MAT Chances for relapse increase with inadequate pain relief Medication doses of long-acting opioid agonists used in ORT are often not effective for pain management TIP 54: Managing chronic pain in adults with or in recovery from substance use disorder. (2012)
70 MAT for those with HIV/AIDS and Viral Hepatitis HIV and Hepatitis C risk behaviors decrease significantly among patients receiving MAT. HIV infection rates decrease and adherence to anti-retroviral medication treatment increases significantly (Springer, Chen, Altice, 2010; Ullman et al., 2010). All medications used for MAT have been used safely by persons with Hepatitis C, even while undergoing treatment. Most doctors review liver function tests prior to initiating MAT to during treatment.
71 System/Program-Level Issues Historically MAT and recovery-oriented services while sharing the same goals did not share similar methods leading to mutual distrust or suspicion Staff from MAT programs and staff from recovery programs rarely interacted Each program has its own models for service provision.
72 No wrong door Part of the Continuum of Care model, No Wrong Door allows clients to access essential services including recover/treatment services (for example housing services, DTA and other support services) from any other statesponsored agency, as seamlessly as possible.
73 No wrong door Use as many effective tools as are available One size does not fit all: as many doors as possible A full continuum of care: multiple services with flexible responses Engagement promotes progress Expectation of relapsing/remitting course Expectation of variable and shifting treatment readiness Recovery as a gradual process, not an overnight event -- expectation of incremental progress
74 Additional Resources TIP 43: Medication-Assisted Treatment for Opioid Addiction in Opioid Treatment Programs. Treatment-for-Opioid-Addiction-in-Opioid-Treatment- Programs/SMA
Medication-Assisted Treatment. What Is It and Why Do We Use It?
 Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Brief History of Methadone Maintenance Treatment
 METHADONE Brief History of Methadone Maintenance Treatment Methadone maintenance treatment was on the cusp of the social revolution in the sixties. Doctors and public health workers had concluded what
METHADONE Brief History of Methadone Maintenance Treatment Methadone maintenance treatment was on the cusp of the social revolution in the sixties. Doctors and public health workers had concluded what
FY17 SCOPE OF WORK TEMPLATE. Name of Program/Services: Medication-Assisted Treatment: Buprenorphine
 FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
FY17 SCOPE OF WORK TEMPLATE Name of Program/Services: Medication-Assisted Treatment: Buprenorphine Procedure Code: Modification of 99212, 99213 and 99214: 99212 22 99213 22 99214 22 Definitions: Buprenorphine
Medication Assisted Treatment
 Meeting the Needs of Your Clients: Building Competencies in Mental Health and Addiction Services Medication Assisted Treatment November 5, 2018 In partnership with: House Keeping Because this is a webinar,
Meeting the Needs of Your Clients: Building Competencies in Mental Health and Addiction Services Medication Assisted Treatment November 5, 2018 In partnership with: House Keeping Because this is a webinar,
Medication Assisted Treatment. MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment
 Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction
 Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
What Is Heroin? Examples of Opioids. What Science Says about Opioid Use Disorder and Its Treatment 6/27/2016
 What Science Says about Opioid Use Disorder and Its Treatment Perilou Goddard, Ph.D. Department of Psychological Science Northern Kentucky University Examples of Opioids Agonists (activate opioid receptors)
What Science Says about Opioid Use Disorder and Its Treatment Perilou Goddard, Ph.D. Department of Psychological Science Northern Kentucky University Examples of Opioids Agonists (activate opioid receptors)
Treatment Approaches for Drug Addiction
 Treatment Approaches for Drug Addiction NOTE: This fact sheet discusses research findings on effective treatment approaches for drug abuse and addiction. If you re seeking treatment, you can call the Substance
Treatment Approaches for Drug Addiction NOTE: This fact sheet discusses research findings on effective treatment approaches for drug abuse and addiction. If you re seeking treatment, you can call the Substance
2004-L SEPTEMBER
 BULLETIN INTELLIGENCE Buprenorphine: Potential for Abuse Product No. 2004-L0424-013 SEPTEMBER 2004 U. S. D E P A R T M E N T O F J U S T I C E NDIC Within the past 2 years buprenorphine a Schedule III
BULLETIN INTELLIGENCE Buprenorphine: Potential for Abuse Product No. 2004-L0424-013 SEPTEMBER 2004 U. S. D E P A R T M E N T O F J U S T I C E NDIC Within the past 2 years buprenorphine a Schedule III
GOALS AND OBJECTIVES
 SUBOXONE AND VIVITROL: ARE THERE DISPARITIES SURFACING IN MEDICATION ASSISTED TREATMENTS? P R E S E N T E D B Y D R. K I AM E M AH A N I A H & D R. M Y E C H I A M I N T E R - J O R D AN GOALS AND OBJECTIVES
SUBOXONE AND VIVITROL: ARE THERE DISPARITIES SURFACING IN MEDICATION ASSISTED TREATMENTS? P R E S E N T E D B Y D R. K I AM E M AH A N I A H & D R. M Y E C H I A M I N T E R - J O R D AN GOALS AND OBJECTIVES
MEDICATION ASSISTED TREATMENT
 MEDICATION ASSISTED TREATMENT MODULE 14 ALLIED TRADES ASSISTANCE PROGRAM PREVENTATIVE EDUCATION: SUBSTANCE USE DISORDER Medication Assisted Treatment Types of Medication Assisted Treatment: Methadone Naltrexone
MEDICATION ASSISTED TREATMENT MODULE 14 ALLIED TRADES ASSISTANCE PROGRAM PREVENTATIVE EDUCATION: SUBSTANCE USE DISORDER Medication Assisted Treatment Types of Medication Assisted Treatment: Methadone Naltrexone
Rule Governing the Prescribing of Opioids for Pain
 Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
Rule Governing the Prescribing of Opioids for Pain 1.0 Authority This rule is adopted pursuant to Sections 14(e) and 11(e) of Act 75 (2013) and Sections 2(e) and 2a of Act 173 (2016). 2.0 Purpose This
MAT in the Corrections Setting
 MEDICATION ASSISTED TREATMENT AND CORRECTIONS Frank Filippelli, DO, PhD September 2017 MAT in the Corrections Setting Who Does This Affect? What is MAT and What is the Evidence of Efficacy? Emphasis on
MEDICATION ASSISTED TREATMENT AND CORRECTIONS Frank Filippelli, DO, PhD September 2017 MAT in the Corrections Setting Who Does This Affect? What is MAT and What is the Evidence of Efficacy? Emphasis on
Opioid Treatment in North Carolina SEPTEMBER 13, 2016
 Opioid Treatment in North Carolina SEPTEMBER 13, 2016 Source Where Pain Relievers Were Obtained for Most Recent Nonmedical Use among Past Year Users Aged 12 or Older: 2007 Source Where Respondent Obtained
Opioid Treatment in North Carolina SEPTEMBER 13, 2016 Source Where Pain Relievers Were Obtained for Most Recent Nonmedical Use among Past Year Users Aged 12 or Older: 2007 Source Where Respondent Obtained
Disclosures. Topics of today s training 4/24/2017. Evolving Treads in Medication Assisted Treatment. Christopher J Davis D.O.
 Evolving Treads in Medication Assisted Treatment Christopher J Davis D.O. CAADC, FASAM Medical Director, The Ranch of Pennsylvania Medical Director, Pyramid Healthcare Diplomate of The American Board of
Evolving Treads in Medication Assisted Treatment Christopher J Davis D.O. CAADC, FASAM Medical Director, The Ranch of Pennsylvania Medical Director, Pyramid Healthcare Diplomate of The American Board of
Clinical Guidelines for the Pharmacologic Treatment of Opioid Use Disorder
 Clinical Guidelines for the Pharmacologic Treatment of Community Behavioral Health (CBH) is committed to working with our provider partners to continuously improve the quality of behavioral healthcare
Clinical Guidelines for the Pharmacologic Treatment of Community Behavioral Health (CBH) is committed to working with our provider partners to continuously improve the quality of behavioral healthcare
Opiate Use Disorder and Opiate Overdose
 Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Appendix F Federation of State Medical Boards
 Appendix F Federation of State Medical Boards Model Policy Guidelines for Opioid Addiction Treatment in the Medical Office SECTION I: PREAMBLE The (name of board) recognizes that the prevalence of addiction
Appendix F Federation of State Medical Boards Model Policy Guidelines for Opioid Addiction Treatment in the Medical Office SECTION I: PREAMBLE The (name of board) recognizes that the prevalence of addiction
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center
 Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Substance Abuse Suboxone Treatment
 Substance Abuse Suboxone Treatment Program Waterbury Hospital Infectious Disease Clinic Richard Smith, LCSW Leonard Savage, Consumer Steven I. Aronin, MD FACP, Program Director Ryan White All Grantee Meeting
Substance Abuse Suboxone Treatment Program Waterbury Hospital Infectious Disease Clinic Richard Smith, LCSW Leonard Savage, Consumer Steven I. Aronin, MD FACP, Program Director Ryan White All Grantee Meeting
Child Welfare and MOMS: Building Partnerships to Improve Care
 Child Welfare and MOMS: Building Partnerships to Improve Care Goals Develop collaborative partnerships between MOMS pilot sites and child welfare agencies: Facilitate successful outcomes for clients Jointly
Child Welfare and MOMS: Building Partnerships to Improve Care Goals Develop collaborative partnerships between MOMS pilot sites and child welfare agencies: Facilitate successful outcomes for clients Jointly
Medication Assisted Treatment. Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs
 Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
Heroin, Fentanyl and Other Opioids. Steve Hanson
 Heroin, Fentanyl and Other Opioids Steve Hanson Heroin/Opiates Neurotransmitter-receptor interactions To transmit instructions to cells, neurotransmitters interact with their receptors. receptor neurotransmitters
Heroin, Fentanyl and Other Opioids Steve Hanson Heroin/Opiates Neurotransmitter-receptor interactions To transmit instructions to cells, neurotransmitters interact with their receptors. receptor neurotransmitters
Prescription Opioids
 What are prescription opioids? Prescription Opioids Opioids are a class of drugs naturally found in the opium poppy plant. Some prescription opioids are made from the plant directly, and others are made
What are prescription opioids? Prescription Opioids Opioids are a class of drugs naturally found in the opium poppy plant. Some prescription opioids are made from the plant directly, and others are made
Division of Mental Health and Addiction Services
 Division of Mental Health and Addiction Services A DAM BUCON, LSW DMHAS Mission DMHAS, in partnership with consumers, family members, providers and other stakeholders, promotes wellness and recovery for
Division of Mental Health and Addiction Services A DAM BUCON, LSW DMHAS Mission DMHAS, in partnership with consumers, family members, providers and other stakeholders, promotes wellness and recovery for
Closing the Loop in Treating Opioid Addiction:
 Closing the Loop in Treating Opioid Addiction: Integrating MAT into Prison and Jail Health Systems May 9, 2018 Webinar Housekeeping All lines are muted This session will be recorded To ask a question:
Closing the Loop in Treating Opioid Addiction: Integrating MAT into Prison and Jail Health Systems May 9, 2018 Webinar Housekeeping All lines are muted This session will be recorded To ask a question:
Vivitrol Drug Court and Medication Assisted Treatment
 Vivitrol Drug Court and Medication Assisted Treatment Amy Black, CNP and Judge Fred Moses Court program Self-starters Mission Statement To provide court-managed, medically assisted drug intervention treatment
Vivitrol Drug Court and Medication Assisted Treatment Amy Black, CNP and Judge Fred Moses Court program Self-starters Mission Statement To provide court-managed, medically assisted drug intervention treatment
Building capacity for a CHC response to Ontario's Opioid Crisis
 Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Building capacity for a CHC response to Ontario's Opioid Crisis Rob Boyd Oasis Program Director Luc Cormier, RN, MScN Community Health Nurse Sandy Hill Community Health Centre #AOHC2016 @rboyd6 @SandyHillCHC
Prepublication Requirements
 Issued Prepublication Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
Issued Prepublication Requirements The Joint Commission has approved the following revisions for prepublication. While revised requirements are published in the semiannual updates to the print manuals
The CARA & Buprenorphine Prescribing for APNs & PAs
 The CARA & Buprenorphine Prescribing for APNs & PAs William J. Lorman, JD, PhD, MSN, PMHNP-BC, CARN-AP FIAAN Assistant Clinical Professor, Drexel University, Philadelphia, PA V. P. & Chief Clinical Officer,
The CARA & Buprenorphine Prescribing for APNs & PAs William J. Lorman, JD, PhD, MSN, PMHNP-BC, CARN-AP FIAAN Assistant Clinical Professor, Drexel University, Philadelphia, PA V. P. & Chief Clinical Officer,
Medical Assisted Treatment. Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center
 Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets. Risk Evaluation and Mitigation Strategy (REMS) Program
 Program") SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
SUBOXONE Film, SUBOXONE Tablets, and SUBUTEX Tablets Risk Evaluation and Mitigation Strategy (REMS) Program Office-Based Buprenorphine Therapy for Opioid Dependence: Important Information for Prescribers
Methadone and Naltrexone ER
 Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither I nor my
Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither I nor my
Wasted AN INTRODUCTION TO SUBSTANCE ABUSE
 Wasted AN INTRODUCTION TO SUBSTANCE ABUSE Dr. Brian L. Bethel Child and Family Therapist Independent Trainer and Consultant LPCC-S, LCDC III, RPT-S www.brianlbethel.com INTERPLAY COUNSELING & CONSULTING
Wasted AN INTRODUCTION TO SUBSTANCE ABUSE Dr. Brian L. Bethel Child and Family Therapist Independent Trainer and Consultant LPCC-S, LCDC III, RPT-S www.brianlbethel.com INTERPLAY COUNSELING & CONSULTING
2/24/2017. Pregnant Women Who Use Drugs: Stigma, Science and Society
 Pregnant Women Who Use Drugs: Stigma, Science and Society Mishka Terplan MD MPH FACOG FASAM Professor Departments Obstetrics and Gynecology and Psychiatry Associate Director Addiction Medicine Virginia
Pregnant Women Who Use Drugs: Stigma, Science and Society Mishka Terplan MD MPH FACOG FASAM Professor Departments Obstetrics and Gynecology and Psychiatry Associate Director Addiction Medicine Virginia
Treatment Alternatives for Substance Use Disorders
 Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Opioid Use and Justice Involvement: Challenges in Treatment, Engagement, and Continuity
 Opioid Use and Justice Involvement: Challenges in Treatment, Engagement, and Continuity Holly Hills, Ph.D. June 13, 2017 Department of Mental Health Law and Policy Overview: Persons who have not been in
Opioid Use and Justice Involvement: Challenges in Treatment, Engagement, and Continuity Holly Hills, Ph.D. June 13, 2017 Department of Mental Health Law and Policy Overview: Persons who have not been in
Understanding Medication in Addiction Treatment for Drug Court Participants
 Understanding Medication in Addiction Treatment for Drug Court Participants Introduction This pocket guide is for drug court participants who may be prescribed or considering medication as a part of addiction
Understanding Medication in Addiction Treatment for Drug Court Participants Introduction This pocket guide is for drug court participants who may be prescribed or considering medication as a part of addiction
Linking Opioid Treatment in Primary Care. Roxanne Lewin M.D.
 Roxanne Lewin M.D. The Facts Fewer than 10 percent of individuals with an alcohol use disorder and only about 20 percent of individuals with an opioid use disorder receive specialty treatment. Many individuals
Roxanne Lewin M.D. The Facts Fewer than 10 percent of individuals with an alcohol use disorder and only about 20 percent of individuals with an opioid use disorder receive specialty treatment. Many individuals
THA Medication Safety Summit. Wesley Geminn, PharmD, BCPP
 THA Medication Safety Summit Wesley Geminn, PharmD, BCPP Current Trends: Overdose Deaths in 2017 72,000 Or 197 per day 8 per hour National Opioid Overdose Statistics https://www.drugabuse.gov/related-topics/trendsstatistics/overdose-death-rates
THA Medication Safety Summit Wesley Geminn, PharmD, BCPP Current Trends: Overdose Deaths in 2017 72,000 Or 197 per day 8 per hour National Opioid Overdose Statistics https://www.drugabuse.gov/related-topics/trendsstatistics/overdose-death-rates
Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings
 Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings BRIAN GARVEY, MD, MPH REBECCA CANTONE, MD OREGON HEALTH & SCIENCE UNIVERSITY SCAPPOOSE RURAL HEALTH CENTER Disclosures
Interdisciplinary Management of Opioid Use Disorder in Rural Primary Care Settings BRIAN GARVEY, MD, MPH REBECCA CANTONE, MD OREGON HEALTH & SCIENCE UNIVERSITY SCAPPOOSE RURAL HEALTH CENTER Disclosures
Methadone Maintenance 101
 Methadone Maintenance 101 OTP/DAILY DOSING CLINICS - ANDREW PUTNEY MD Conflicts of Interest - Employed by Acadia HealthCare 1 Why Methadone? At adequate doses methadone decreases opioid withdrawal symptoms
Methadone Maintenance 101 OTP/DAILY DOSING CLINICS - ANDREW PUTNEY MD Conflicts of Interest - Employed by Acadia HealthCare 1 Why Methadone? At adequate doses methadone decreases opioid withdrawal symptoms
HARM REDUCTION & TREATMENT. Devin Reaves MSW
 HARM REDUCTION & TREATMENT Devin Reaves MSW The mission of PAHRC is to promote the health, dignity, and human rights of individuals who use drugs and communities impacted by drug use. Recognizing that
HARM REDUCTION & TREATMENT Devin Reaves MSW The mission of PAHRC is to promote the health, dignity, and human rights of individuals who use drugs and communities impacted by drug use. Recognizing that
Understanding and Combating the Heroin Epidemic
 Understanding and Combating the Heroin Epidemic Kelly Dunn, Ph.D. Assistant Professor; Johns Hopkins School of Medicine Department of Psychiatry and Behavioral Sciences 1 Talk Outline What is causing the
Understanding and Combating the Heroin Epidemic Kelly Dunn, Ph.D. Assistant Professor; Johns Hopkins School of Medicine Department of Psychiatry and Behavioral Sciences 1 Talk Outline What is causing the
Opioid Management of Chronic (Non- Cancer) Pain
 Pain") Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
Optima Health Opioid Management of Chronic (Non- Cancer) Pain Guideline History Original Approve Date 5/08 Review/Revise Dates 11/09, 9/11, 9/13, 09/15, 9/17 Next Review Date 9/19 These Guidelines are
Helping Recovery Residences Adapt
 to Support People with Helping Recovery Residences Adapt Medication-Assisted Recovery info@narronline.org narronline.org 855-355-NARR (6277) In this Brief Many people with opioid use disorders embrace
to Support People with Helping Recovery Residences Adapt Medication-Assisted Recovery info@narronline.org narronline.org 855-355-NARR (6277) In this Brief Many people with opioid use disorders embrace
Discover the Hope: Opiate Treatment and Recovery
 Discover the Hope: Opiate Treatment and Recovery The Continued Struggle to Find and Implement Best Practices Ted Parran JR. M.D. FACP Carter and Isabel Wang Professor of Medical Education CWRU School of
Discover the Hope: Opiate Treatment and Recovery The Continued Struggle to Find and Implement Best Practices Ted Parran JR. M.D. FACP Carter and Isabel Wang Professor of Medical Education CWRU School of
Many drugs of abuse are illegal drugs. Possessing, using, buying, or selling these drugs is illegal for people of any age.
 1 Chapter 12 Section 1 Objectives List six ways illegal drug use can be dangerous. State five reasons a person might try illegal drugs. Identify the reason drug abuse is especially dangerous to teens.
1 Chapter 12 Section 1 Objectives List six ways illegal drug use can be dangerous. State five reasons a person might try illegal drugs. Identify the reason drug abuse is especially dangerous to teens.
MAT IN PREGNANCY KAYLA LIFE STAGE 1: ADOLESCENCE LIFE STAGE 2: EARLY ADULTHOOD. family History of addiction. addiction to oral opioids
 MAT IN PREGNANCY R. COREY WALLER MD, MS PRINCIPAL, HEALTH MANAGEMENT ASSOCIATES FACULTY, INSTITUTE FOR HEALTHCARE INNOVATION (IHI) CHAIR, LEGISLATIVE ADVOCACY COMMITTEE, ASAM KAYLA LIFE STAGE 1: ADOLESCENCE
MAT IN PREGNANCY R. COREY WALLER MD, MS PRINCIPAL, HEALTH MANAGEMENT ASSOCIATES FACULTY, INSTITUTE FOR HEALTHCARE INNOVATION (IHI) CHAIR, LEGISLATIVE ADVOCACY COMMITTEE, ASAM KAYLA LIFE STAGE 1: ADOLESCENCE
201 KAR 9:270. Professional standards for prescribing or dispensing Buprenorphine-Mono-Product or Buprenorphine-Combined-with-Naloxone.
 201 KAR 9:270. Professional standards for prescribing or dispensing Buprenorphine-Mono-Product or Buprenorphine-Combined-with-Naloxone. RELATES TO: KRS 311.530-311.620, 311.990 STATUTORY AUTHORITY: KRS
201 KAR 9:270. Professional standards for prescribing or dispensing Buprenorphine-Mono-Product or Buprenorphine-Combined-with-Naloxone. RELATES TO: KRS 311.530-311.620, 311.990 STATUTORY AUTHORITY: KRS
QUARTERLY PROVIDER MEETING MARCH 9, 2017 SUZANNE BORYS, ED.D.
 2017 State Targeted Response to the Opioid Crisis Grants QUARTERLY PROVIDER MEETING MARCH 9, 2017 SUZANNE BORYS, ED.D. H.R.6-21st Century Cures Act The 21st Century Cures Act is a United States law enacted
2017 State Targeted Response to the Opioid Crisis Grants QUARTERLY PROVIDER MEETING MARCH 9, 2017 SUZANNE BORYS, ED.D. H.R.6-21st Century Cures Act The 21st Century Cures Act is a United States law enacted
Buprenorphine as a Treatment Option for Opioid Use Disorder
 Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Anyone Can Become Addicted. Anyone.
 Anyone Can Become Addicted. Anyone. PAStop.org Family Toolkit Seeking Drug Abuse Treatment: Know What to Ask Trying to identify the right treatment programs for a loved one can be a difficult process.
Anyone Can Become Addicted. Anyone. PAStop.org Family Toolkit Seeking Drug Abuse Treatment: Know What to Ask Trying to identify the right treatment programs for a loved one can be a difficult process.
ADDRESSING THE OPIOID EPIDEMIC. Joint principles of the following organizations representing front-line physicians
 ADDRESSING THE OPIOID EPIDEMIC Joint principles of the following organizations representing front-line physicians American Academy of Family Physicians American Academy of Pediatrics American College of
ADDRESSING THE OPIOID EPIDEMIC Joint principles of the following organizations representing front-line physicians American Academy of Family Physicians American Academy of Pediatrics American College of
2/21/2018. What are Opioids?
 Opioid Crisis: South Carolina Responds Carolyn Bogdon, MSN, FNP-BC Coordinator for Emergency Department Medication Assisted Treatment Program Medical University of South Carolina Opioid Crisis: A Mounting
Opioid Crisis: South Carolina Responds Carolyn Bogdon, MSN, FNP-BC Coordinator for Emergency Department Medication Assisted Treatment Program Medical University of South Carolina Opioid Crisis: A Mounting
Medication for the Treatment of Addiction (MAT)
") Medication for the Treatment of Addiction (MAT) Karol Kaltenbach, PhD Emeritus Professor of Pediatrics Sidney Kimmel Medical College at Thomas Jefferson University Terminology: Words Matter Medication
Medication for the Treatment of Addiction (MAT) Karol Kaltenbach, PhD Emeritus Professor of Pediatrics Sidney Kimmel Medical College at Thomas Jefferson University Terminology: Words Matter Medication
Talking with your doctor
 SUBOXONE (buprenorphine and naloxone) Sublingual Film (CIII) Talking with your doctor Opioid dependence can be treated. Talking with your healthcare team keeps them aware of your situation so they may
SUBOXONE (buprenorphine and naloxone) Sublingual Film (CIII) Talking with your doctor Opioid dependence can be treated. Talking with your healthcare team keeps them aware of your situation so they may
Prescription Opioid Addiction
 CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
Attitudes Toward Medication-Assisted Treatment Within a Drug Court Program. Caroline Allison. Dr. Kathleen Moore, Ph.D.
 Running Head: MEDICATION-ASSISTED TREATMENT ATTITUDES Attitudes Toward Medication-Assisted Treatment Within a Drug Court Program Caroline Allison Dr. Kathleen Moore, Ph.D. Department of Mental Health Law
Running Head: MEDICATION-ASSISTED TREATMENT ATTITUDES Attitudes Toward Medication-Assisted Treatment Within a Drug Court Program Caroline Allison Dr. Kathleen Moore, Ph.D. Department of Mental Health Law
Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention
 The Accountable Community for Health of King County Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention May 7, 2018 1 Opiate Treatment & Overdose Prevention Project Goal Immediate:
The Accountable Community for Health of King County Addressing the Opioid Crisis Workgroup: Treatment and Overdose Prevention May 7, 2018 1 Opiate Treatment & Overdose Prevention Project Goal Immediate:
7/7/2016 Journal of the American Medical Association,
 1 2 Journal of the American Medical Association, 2008 3 The Clinical Trial 152 Adolescents and Young Adults (Age 15 to 21) randomly assigned to either; 1. 2 weeks of Buprenorphine detox 2. 12 weeks of
1 2 Journal of the American Medical Association, 2008 3 The Clinical Trial 152 Adolescents and Young Adults (Age 15 to 21) randomly assigned to either; 1. 2 weeks of Buprenorphine detox 2. 12 weeks of
Methadone and Pregnancy
 Methadone and Pregnancy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Charissa Patricelli, MD, CCFP, ABAM Clinical Associate Professor, Dept. of Family Practice UBC American Board of Addiction Medicine
Methadone and Pregnancy Methadone/Buprenorphine 101 Workshop, April 1, 2017 Charissa Patricelli, MD, CCFP, ABAM Clinical Associate Professor, Dept. of Family Practice UBC American Board of Addiction Medicine
OUTPATIENT TREATMENT WESTPORT, CONNECTICUT
 OUTPATIENT TREATMENT WESTPORT, CONNECTICUT ABOUT CLEARPOINT At Clearpoint, we focus on healing the whole person: mind, body, and spirit. Our comprehensive care methods set clients up for long-term success
OUTPATIENT TREATMENT WESTPORT, CONNECTICUT ABOUT CLEARPOINT At Clearpoint, we focus on healing the whole person: mind, body, and spirit. Our comprehensive care methods set clients up for long-term success
Addiction Overview. Diane A. Rothon MD. Causes Consequences Treatments. Methadone/Buprenorphine 101 April 1, 2017
 Addiction Overview Causes Consequences Treatments Methadone/Buprenorphine 101 April 1, 2017 Diane A. Rothon MD Why? would you listen to this presentation Review the definition and neurobiology of addiction
Addiction Overview Causes Consequences Treatments Methadone/Buprenorphine 101 April 1, 2017 Diane A. Rothon MD Why? would you listen to this presentation Review the definition and neurobiology of addiction
HARM REDUCTION & THE OPIOID EPIDEMIC. CHELSEA RAINWATER Co-Founder & Executive Director No Overdose Baton Rouge
 HARM REDUCTION & THE OPIOID EPIDEMIC CHELSEA RAINWATER Co-Founder & Executive Director No Overdose Baton Rouge NO OVERDOSE BATON ROUGE Formed in late 2013 Community education Naloxone distribution Syringe
HARM REDUCTION & THE OPIOID EPIDEMIC CHELSEA RAINWATER Co-Founder & Executive Director No Overdose Baton Rouge NO OVERDOSE BATON ROUGE Formed in late 2013 Community education Naloxone distribution Syringe
OPIATES IN PRISON. Jeffrey C. Fetter, MD
 OPIATES IN PRISON Jeffrey C. Fetter, MD Agenda Opioids in the Correctional Environment MAT and Corrections Substance Abuse Treatment in NH DOC Suboxone Suboxone: Contraband Suboxone Contraband Scale of
OPIATES IN PRISON Jeffrey C. Fetter, MD Agenda Opioids in the Correctional Environment MAT and Corrections Substance Abuse Treatment in NH DOC Suboxone Suboxone: Contraband Suboxone Contraband Scale of
Buprenorphine & Controlled Substance Treatment Agreement
 Buprenorphine & Controlled Substance Treatment Agreement I agree to accept the following treatment contract for buprenorphine office-based opioid addiction treatment: 1. I will keep my medication in a
Buprenorphine & Controlled Substance Treatment Agreement I agree to accept the following treatment contract for buprenorphine office-based opioid addiction treatment: 1. I will keep my medication in a
Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates
 and Medication Assisted Treatment (MAT) for Opiates") Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates What is MAT? Medication Assisted Treatment (MAT) is the use of medications, in addition to counseling, cognitive behavioral
Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates What is MAT? Medication Assisted Treatment (MAT) is the use of medications, in addition to counseling, cognitive behavioral
Opioid Use in Youth. Amy Yule M.D. March 2,
 Opioid Use in Youth Amy Yule M.D. March 2, 2018 An opioid is a substance that acts on opioid receptors Beta-endorphin Endogenous opioids Dynorphin Opiates Natural products of the poppy plant Morphine Heroin
Opioid Use in Youth Amy Yule M.D. March 2, 2018 An opioid is a substance that acts on opioid receptors Beta-endorphin Endogenous opioids Dynorphin Opiates Natural products of the poppy plant Morphine Heroin
Treating Opioid Use Disorders: An Update for Counselors and Other Providers
 Treating Opioid Use Disorders: An Update for Counselors and Other Providers Brad Shapiro, MD Medical Director Opiate Treatment Outpatient Program Zuckerberg San Francisco General THE DOSING WINDOW HISTORICAL
Treating Opioid Use Disorders: An Update for Counselors and Other Providers Brad Shapiro, MD Medical Director Opiate Treatment Outpatient Program Zuckerberg San Francisco General THE DOSING WINDOW HISTORICAL
PATIENT INTAKE: MEDICAL HISTORY. Name. Address. Phone (W) (H) (C) DOB Age SS# Emergency Contact. Relationship to patient Phone
 (H) (C) DOB Age SS# Emergency Contact. Relationship to patient Phone") PATIENT INTAKE: MEDICAL HISTORY Name Address Phone (W) (H) (C) DOB Age SS# Emergency Contact Relationship to patient Phone Primary care physician Phone Have you ever had an EKG? Y N Date Current or past
PATIENT INTAKE: MEDICAL HISTORY Name Address Phone (W) (H) (C) DOB Age SS# Emergency Contact Relationship to patient Phone Primary care physician Phone Have you ever had an EKG? Y N Date Current or past
SANTA BARBARA COUNTY DEPARTMENT OF Behavioral Wellness A System of Care and Recovery
 Page 1 of 9 SANTA BARBARA COUNTY DEPARTMENT OF Behavioral Wellness A System of Care and Recovery Departmental Polley and Procedure Section Sub-section Alcohol and Drug Program (ADP) Effective: 7/11/2018
Page 1 of 9 SANTA BARBARA COUNTY DEPARTMENT OF Behavioral Wellness A System of Care and Recovery Departmental Polley and Procedure Section Sub-section Alcohol and Drug Program (ADP) Effective: 7/11/2018
OPIOIDS IN AMERICA. A complex crisis. A comprehensive response.
 OPIOIDS IN AMERICA A complex crisis. A comprehensive response. Prescription opioids play a critical role in helping millions of people effectively manage chronic pain. But for some, opioid use has become
OPIOIDS IN AMERICA A complex crisis. A comprehensive response. Prescription opioids play a critical role in helping millions of people effectively manage chronic pain. But for some, opioid use has become
TREATING OPIOID ADDICTION IN HOMELESS POPULATIONS
 TREATING OPIOID ADDICTION IN HOMELESS POPULATIONS Challenges and Opportunities Providing Medication Assisted Treatment (Buprenorphine) August 18, 2016 SPEAKERS TODAY Nilesh Kalyanaraman, MD, Chief Health
TREATING OPIOID ADDICTION IN HOMELESS POPULATIONS Challenges and Opportunities Providing Medication Assisted Treatment (Buprenorphine) August 18, 2016 SPEAKERS TODAY Nilesh Kalyanaraman, MD, Chief Health
Buprenorphine: An Introduction. Sharon Stancliff, MD Harm Reduction Coalition September 2008
 Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE
 LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE DR. SHILPA ADARKAR ASSOCIATE PROFESSOR DEPARTMENT OF PSYCHIATRY & DRUG DEADDICTION CENTRE OF EXCELLENCE SETH GSMC & KEMH LONG TERM OPTIONS FULL AGONIST PARTIAL
LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE DR. SHILPA ADARKAR ASSOCIATE PROFESSOR DEPARTMENT OF PSYCHIATRY & DRUG DEADDICTION CENTRE OF EXCELLENCE SETH GSMC & KEMH LONG TERM OPTIONS FULL AGONIST PARTIAL
Medications for Opioid Use Disorder. Charles Brackett, MD, MPH General Internal Medicine, DHMC
 Medications for Opioid Use Disorder Charles Brackett, MD, MPH General Internal Medicine, DHMC Opioid Related Deaths are on the Rise in the US National Vital Statistics System Mortality File Deaths are
Medications for Opioid Use Disorder Charles Brackett, MD, MPH General Internal Medicine, DHMC Opioid Related Deaths are on the Rise in the US National Vital Statistics System Mortality File Deaths are
Opioid Use Disorders as a Brain Disease Why MAT is so important. Ron Jackson, M.S.W., L.I.C.S.W.
 Opioid Use Disorders as a Brain Disease Why MAT is so important Ron Jackson, M.S.W., L.I.C.S.W. Affiliate Professor School of Social Work University of Washington Organization Name: CareOregon Course Title:
Opioid Use Disorders as a Brain Disease Why MAT is so important Ron Jackson, M.S.W., L.I.C.S.W. Affiliate Professor School of Social Work University of Washington Organization Name: CareOregon Course Title:
COMPASS RECOVERY OPIOID REHABILITATION PROGRAM QUESTIONAIRE FOR PROSPECTIVE OPIOID REHABILITATION. Name Birthdate / /
 COMPASS RECOVERY OPIOID REHABILITATION PROGRAM QUESTIONAIRE FOR PROSPECTIVE OPIOID REHABILITATION Name Birthdate / / Home phone ( ) - Cell phone ( ) - Please answer the following questions which will help
COMPASS RECOVERY OPIOID REHABILITATION PROGRAM QUESTIONAIRE FOR PROSPECTIVE OPIOID REHABILITATION Name Birthdate / / Home phone ( ) - Cell phone ( ) - Please answer the following questions which will help
Medication Assisted Treatment: Right for you, Right for your Recovery? Robert Matylewicz, DO, FASAM Medical Director, Clarity Way Inc.
 Medication Assisted Treatment: Right for you, Right for your Recovery? Robert Matylewicz, DO, FASAM Medical Director, Clarity Way Inc. Elements Behavioral Health Diplomate, American Board of Addiction
Medication Assisted Treatment: Right for you, Right for your Recovery? Robert Matylewicz, DO, FASAM Medical Director, Clarity Way Inc. Elements Behavioral Health Diplomate, American Board of Addiction
NALTREXONE DAVID CRABTREE, MD, MPH UNIVERSITY OF UTAH HEALTH, 2018
 NALTREXONE DAVID CRABTREE, MD, MPH TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications
NALTREXONE DAVID CRABTREE, MD, MPH TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications
Developed and Presented by Randall Webber, MPH, CADC JRW Behavioral Health Services
 Developed and Presented by Randall Webber, MPH, CADC JRW Behavioral Health Services www.randallwebber.com MAT clients are still addicted Truth: MAT clients will experience withdrawal symptoms if they stop
Developed and Presented by Randall Webber, MPH, CADC JRW Behavioral Health Services www.randallwebber.com MAT clients are still addicted Truth: MAT clients will experience withdrawal symptoms if they stop
gatewaycorrections.org TCU & Gateway Foundation 9/23/2014 Disclosures Topics Covered Opioid Use Disorders & the CJ System
 Mid-America ATTC Regional Conference Medication Assisted Treatment: Promoting Tools for Successful Recovery September 23, 2014 The Use of Medication-Assisted Treatment with Justice-Involved Clients Kevin
Mid-America ATTC Regional Conference Medication Assisted Treatment: Promoting Tools for Successful Recovery September 23, 2014 The Use of Medication-Assisted Treatment with Justice-Involved Clients Kevin
Addiction vs. Dependence. Introduction. Methadone: Historical Background. Addiction vs. Dependence. C.O.R.E. Medical Clinic, Inc.
 C.O.R.E. Medical Clinic, Inc. Chapter I Opioids and the Brain 2 Chapter Overview Introduction Addiction vs. Dependence Methadone: Historical Background Brain Chemistry: Before & After Opiate Use Methadone
C.O.R.E. Medical Clinic, Inc. Chapter I Opioids and the Brain 2 Chapter Overview Introduction Addiction vs. Dependence Methadone: Historical Background Brain Chemistry: Before & After Opiate Use Methadone
Evidence-Based Practices for the Treatment of Opioid Use Disorder. Zach Ludwig, LPC Corporate Director Clinical Programs Bradford Health Services
 Evidence-Based Practices for the Treatment of Opioid Use Disorder Zach Ludwig, LPC Corporate Director Clinical Programs Bradford Health Services Objectives Review the scope of the opioid epidemic Discuss
Evidence-Based Practices for the Treatment of Opioid Use Disorder Zach Ludwig, LPC Corporate Director Clinical Programs Bradford Health Services Objectives Review the scope of the opioid epidemic Discuss
The Opioid-Exposed Woman
 The Opioid-Exposed Woman Management Considerations for Labor and Delivery Jane Sublette, MS, RN, CNM, WHNP-BC Fairview Ridges Hospital Objectives Describe opioid-associated risks to the mother and fetus
The Opioid-Exposed Woman Management Considerations for Labor and Delivery Jane Sublette, MS, RN, CNM, WHNP-BC Fairview Ridges Hospital Objectives Describe opioid-associated risks to the mother and fetus
John Murphy DO, MS Lynx Healthcare
 Addiction to Pain Medication and Treatment John Murphy DO, MS Lynx Healthcare No Disclosures Objectives 1 Understand basic neurobiology and learning theory around opioid addiction 2 Identify aberrant behavior
Addiction to Pain Medication and Treatment John Murphy DO, MS Lynx Healthcare No Disclosures Objectives 1 Understand basic neurobiology and learning theory around opioid addiction 2 Identify aberrant behavior
Opioid Use Disorders &Medication Treatment
 Agency medical director comments Opioid Use Disorders &Medication Treatment Charissa Fotinos, MD, MSc Deputy Chief Medical Officer Washington State Health Care Authority Learning Objectives: 1) Review
Agency medical director comments Opioid Use Disorders &Medication Treatment Charissa Fotinos, MD, MSc Deputy Chief Medical Officer Washington State Health Care Authority Learning Objectives: 1) Review
Utah. Prescribing and Dispensing Profile. Research current through November 2015.
 Prescribing and Dispensing Profile Utah Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of view
Prescribing and Dispensing Profile Utah Research current through November 2015. This project was supported by Grant No. G1599ONDCP03A, awarded by the Office of National Drug Control Policy. Points of view
Table of Contents Interim Report of the OxyContin Task Force, Newfoundland & Labrador, January 30, 2004
 OXYCONTIN TASK FORCE INTERIM REPORT January 30, 2004 Submitted to Hon. Elizabeth Marshall, Minister of Health & Community Services, Government of Newfoundland and Labrador Table of Contents INTRODUCTION
OXYCONTIN TASK FORCE INTERIM REPORT January 30, 2004 Submitted to Hon. Elizabeth Marshall, Minister of Health & Community Services, Government of Newfoundland and Labrador Table of Contents INTRODUCTION
Topics of today s training
 Extended Release Naltrexone Vivitrol Christopher J Davis D.O. CAADC, FASAM Medical Director, Brightwater Landing Medical Director, Pyramid Healthcare Diplomate of The American Board of Addition Medicine
Extended Release Naltrexone Vivitrol Christopher J Davis D.O. CAADC, FASAM Medical Director, Brightwater Landing Medical Director, Pyramid Healthcare Diplomate of The American Board of Addition Medicine
Medication for Addiction Treatment (MAT)
") SBIRT Training Screening, Brief Intervention & Referral to Treatment Medication for Addiction Treatment (MAT) The Faith & Spirituality Integrated SBIRT Network Navigating the Training Welcome! These health
SBIRT Training Screening, Brief Intervention & Referral to Treatment Medication for Addiction Treatment (MAT) The Faith & Spirituality Integrated SBIRT Network Navigating the Training Welcome! These health
Opioid Agonists. Natural derivatives of opium poppy - Opium - Morphine - Codeine
 Natural derivatives of opium poppy - Opium - Morphine - Codeine Opioid Agonists Semi synthetics: Derived from chemicals in opium -Diacetylmorphine Heroin - Hydromorphone Synthetics - Oxycodone Propoxyphene
Natural derivatives of opium poppy - Opium - Morphine - Codeine Opioid Agonists Semi synthetics: Derived from chemicals in opium -Diacetylmorphine Heroin - Hydromorphone Synthetics - Oxycodone Propoxyphene
Noel Schenk MD. Davis Behavioral Health
 Noel Schenk MD Davis Behavioral Health Michael Botticelli Director of National Drug Control Policy What is Addiction? Addiction is defined as a chronic, relapsing brain disease that is characterized by
Noel Schenk MD Davis Behavioral Health Michael Botticelli Director of National Drug Control Policy What is Addiction? Addiction is defined as a chronic, relapsing brain disease that is characterized by
Community Response Addressing The Opioid Crisis. Leon, Wakulla, Gadsden, Franklin, Liberty, Jefferson, Madison and Taylor Counties
 Community Response Addressing The Opioid Crisis Leon, Wakulla, Gadsden, Franklin, Liberty, Jefferson, Madison and Taylor Counties Strong Partnerships = Health Communities Creating strong communities armed
Community Response Addressing The Opioid Crisis Leon, Wakulla, Gadsden, Franklin, Liberty, Jefferson, Madison and Taylor Counties Strong Partnerships = Health Communities Creating strong communities armed
Rationale & Strategy For Integrating Buprenorphine Treatment Into Community Health Centers
 Rationale & Strategy For Integrating Buprenorphine Treatment Into Community Health Centers Marwan S. Haddad, M.D. Community Health Center, Inc. Connecticut September 16, 2008 Community Health Center, Inc.
Rationale & Strategy For Integrating Buprenorphine Treatment Into Community Health Centers Marwan S. Haddad, M.D. Community Health Center, Inc. Connecticut September 16, 2008 Community Health Center, Inc.
The Social Worker s Role in Medication Assisted Treatment
 The Social Worker s Role in Medication Assisted Treatment Rocky Ephraim Lucas, LICSW Behavioral Health Consultant, Kanawha City Health Center (Cabin Creek Health Systems) What is Medication-Assisted Treatment
The Social Worker s Role in Medication Assisted Treatment Rocky Ephraim Lucas, LICSW Behavioral Health Consultant, Kanawha City Health Center (Cabin Creek Health Systems) What is Medication-Assisted Treatment
THE STATE OF MEDICINE IN ADDICTION RECOVERY
 OVERVIEW: Review addiction stats and trends Define addiction Explain neurobiology of addiction Review treatments of addiction Addiction Definition: A Primary, chronic, relapsing disease of brain reward,
OVERVIEW: Review addiction stats and trends Define addiction Explain neurobiology of addiction Review treatments of addiction Addiction Definition: A Primary, chronic, relapsing disease of brain reward,
Opioid Task Force Kick-Off Meeting. February 29, 2016
 Opioid Task Force Kick-Off Meeting February 29, 2016 Scope of the Opioid Problem and Data Review Olivia Kasirye, MD, MS County Public Health Officer OVERVIEW The Opioid Epidemic Opioid Task Force Development
Opioid Task Force Kick-Off Meeting February 29, 2016 Scope of the Opioid Problem and Data Review Olivia Kasirye, MD, MS County Public Health Officer OVERVIEW The Opioid Epidemic Opioid Task Force Development
ADAPTING YOUR COURT STRUCTURE
 ADAPTING YOUR COURT STRUCTURE Developed by: National Drug Court Institute NDCI, March 2018 The following presentation may not be copied in whole or in part without the written permission of the author
ADAPTING YOUR COURT STRUCTURE Developed by: National Drug Court Institute NDCI, March 2018 The following presentation may not be copied in whole or in part without the written permission of the author