HCV treatment options in clinical practice. Current treatment options for HCV-G4
|
|
|
- Lucas Simpson
- 5 years ago
- Views:
Transcription

1 HCV treatment options in clinical practice Current treatment options for HCV-G4 C. Triantos Gastroenterology Department University Hospital of Patras
2 Conflicts of interest Speaker and research/travel grants from MSD, Roche, Abbvie, Bristol-Myers Squibb, Bayer and Gilead Sciences.
3 Treatment of Chronic HCV Genotype 4 Background Initial Treatment Retreatment of Prior Non-responders Future Therapies Real Clinical Practice Data Recommendations Not included data on the management of CHC in patients with decompensated cirrhosis, HBV/HIV co-infections and patients with hemoglobinopathies

4 Global Distribution and Prevalence of Hepatitis C Virus Genotypes Genotype 4 Globally, approximately 20% of all hepatitis C infections, 34 million people are chronically infected with HCV-4 Dominant HCV genotype in Egypt, North Africa, and sub-saharan Africa. Its prevalence has increased in several European countries, which is considered to be largely a consequence of immigration and intravenous drug use Messina J, Hepatology 2015

5 Epidemiological changes in chronic hepatitis C infection in Greece Savvas, S, Journal of Viral Hepatitis, 2005 Raptopoulou M, Hippoktatia 2011


6 Prospective studies evaluating a fixed 48-wk treatment using a standard dose of pegylated interferon and ribavirin in patients with hepatitis C genotype 4 Predictors of response to antiviral treatment in patients with hepatitis C virus genotype 4 infection Papastergiou V, World J Clin Cases 2015
7 Genotype 4 HCV infection is difficult to cure with pegylated interferon and ribavirin. Results from a Greek Nationwide Cohort Study Anagnostou O, Hippokratia 2014
8 Genotype 4 HCV: Initial Treatment Ledipasvir-Sofosbuvir - NIAID Synergy Ombitasvir-Paritaprevir-Ritonavir - PEARL-I Sofosbuvir + Ribavirin - Egyptian Ancestry Sofosbuvir + Ribavirin + Peginterferon - NEUTRINO
9 Genotype 4 HCV: Initial Treatment IFN-based Regimens


10 Sofosbuvir + PEG + RBV: Treatment-Naive HCV GT 1,4,5,6 NEUTRINO Trial Drug Dosing Sofosbuvir: 400 mg once daily Peginterferon alfa-2a: 180 µg once weekly Ribavirin (weight-based and in 2 divided doses): 1000 mg/day if < 75 kg or 1200 mg/day if 75 kg Lawitz E, N Engl J Med. 2013



11 Sofosbuvir + PEG + RBV: Treatment-Naive HCV GT 1,4,5,6 NEUTRINO Trial: Results Lawitz E, N Engl J Med. 2013
 or TE relapsers (n =")

12 Patients (%) with SVR12 Simeprevir + Peginterferon + Ribavirin in Genotype 4 RESTORE trial, Moreno C, J Hepatology 2015 Open-label, phase 3, n = 107, 8 centres in France and Belgium TN (n = 35) or TE relapsers (n = 22) Experienced (Nonresponder): partial (n = 10), null (n = 40) METAVIR Fibrosis Stage: F4 = 29%; F3 = 14% lack of a control arm serious AEs were infrequent (4.7%) All Treatment-Naïve Relapsers Partial Null
13 High efficacy of a 12-week simeprevir plus peginterferon alfa 2a/ribavirin regimen in treatment-naïve patients with chronic HCV genotype 4 infection and mild-to-moderate fibrosis Phase-3, open-label study Europe and Saudi Arabia G4 patients who achieved HCV-RNA <25 IU/mL (detectable/undetectable in IL28B CC, undetectable in CT/TT) at Week 2, and undetectable at Weeks 4 and 8 (Roche COBAS Taqman ), stopped all treatments at Week 12 (12-week group). Otherwise, PR was continued to Week 24 (24-week group). The 24-week group also included patients discontinuing treatment early for any reason. 67, G4 patients were enrolled (male: 69%, white: 80%, G4a/d/other: 40/37/23%, METAVIR F0 1/F2: 81/18%) SVR12 rates were 97% (33/34) and 84% (21/25) for the 12-week and 24-week groups, respectively Asselah T, AASLD 2015



14 Daclatasvir + Peg/RBV in Treatment-Naïve Genotype 4, COMMAND-4 Study, Phase 3 randomized, placebo-controlled trial, United States and Europe HezodeC, ID Week. 2014
15 Genotype 4 HCV: Initial Treatment All-oral Regimens



16 Ledipasvir-Sofosbuvir in Genotype 4 F4, 33% single-site trial nonrandomised enrolment without ribavirin Kohli A, Lancet Infect Dis. 2015
17 LDV/SOF in GT 4 Patients Multicenter study in TN/TE GT 4 or 5 patients in France Open-label, single-arm study: 12 wks LDV/SOF 90/400 mg QD LDV/SOF for 12 weeks was highly effective and well tolerated, without the need for RBV Naïve n=22 Experienced n= SVR Mean age, years (range) 52 (21 69) 50 (30 62) Male, n (%) 11 (50) 17 (77) White, n (%) 19 (86) 17 (77) Cirrhosis, n (%) 1 (5) 9 (41) IL28B non-cc, n (%) 15 (68) 21 (95) Mean HCV RNA, log 10 IU/mL (range) 6.0 ( ) 6.3 ( ) GT 4a, n (%) 13 (59) 12 (55) GT 4d, n (%) 5 (23) 5 (23) GT 4b, 4f, 4m, 4o, 4r, n (%) 4 (18) 5 (23) /22 20/22 31/34 10/10 TN TE No Yes Treatment Status Cirrhosis Abergel EASL, 2015

, Paritaprevir (150 mg once daily), Ritonavir (100 mg once")
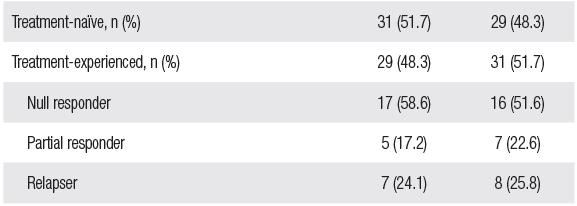
18 Ombitasvir + Paritaprevir + Ritonavir +/- RBV in HCV GT4 PEARL-I: Baseline demographics and disease characteristics France, Hungary, Italy, Poland, Romania, Spain,Turkey, and USA large study lack of examination of a ribavirin-free regimen in treatment experienced patients. only non-cirrhotic patients Drug Dosing Ombitasvir (25 mg once daily), Paritaprevir (150 mg once daily), Ritonavir (100 mg once daily) Ribavirin (RBV): weight-based and divided bid (1000 mg/day if < 75kg or 1200 mg/day if 75kg) Hézode C, Lancet. 2015


19 Ombitasvir + Paritaprevir + Ritonavir +/- RBV in HCV GT4 PEARL-I: Results Hézode C, Lancet. 2015
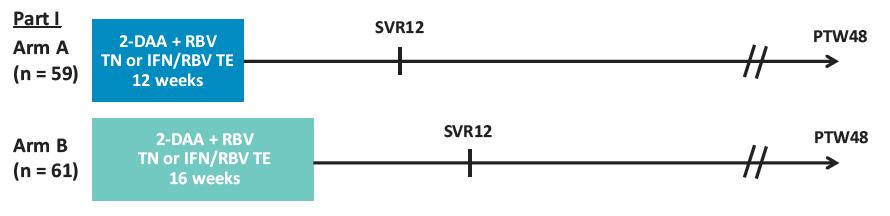
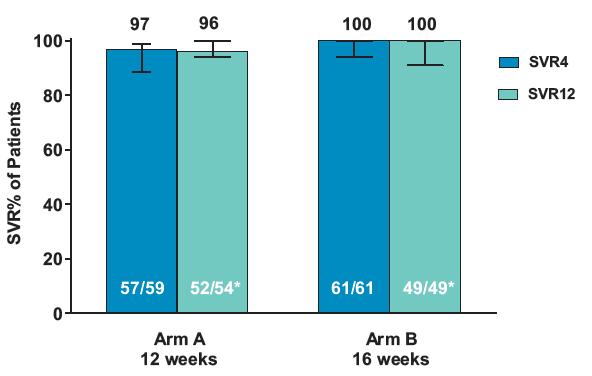
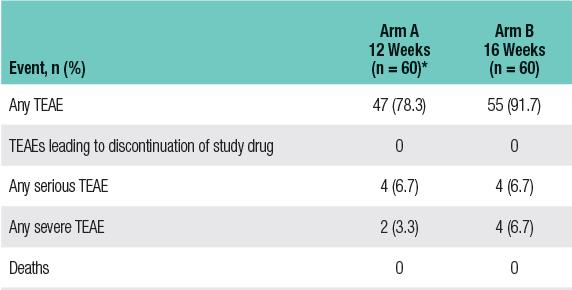
20 Efficacy and Safety of Ombitasvir/Paritaprevir/Ritonavir Co-Administered with Ribavirin in Adults with Genotype 4 Chronic Hepatitis C Infection and Cirrhosis (AGATE-I) Canada, Europe and US Asselah T, AASLD 2015

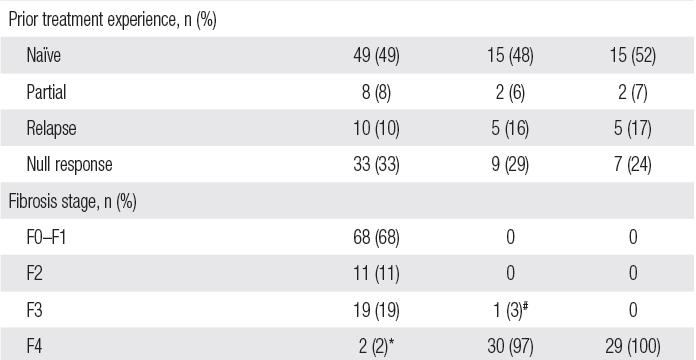
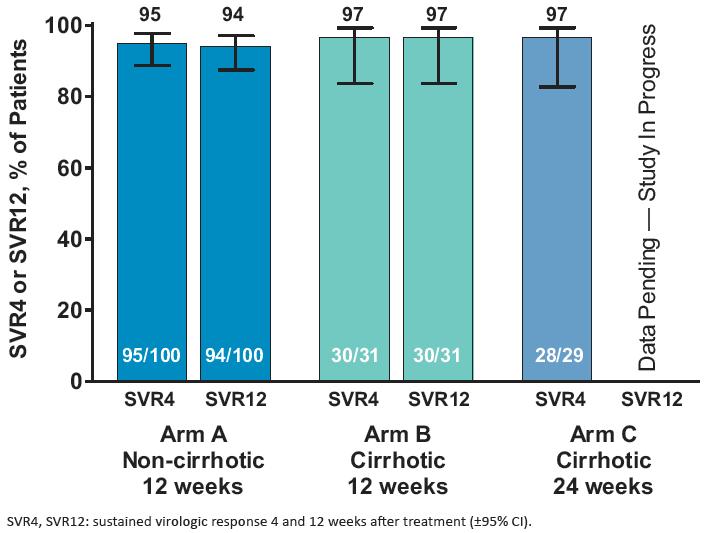
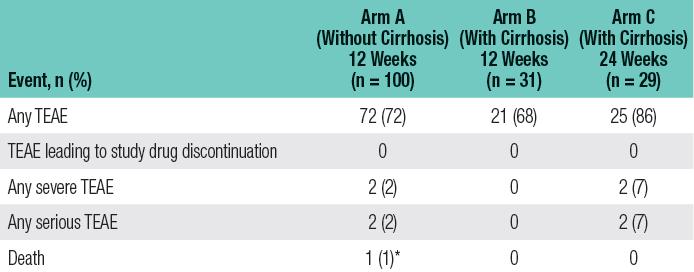
21 Efficacy and Safety of Co-Formulated Ombitasvir/Paritaprevir/ Ritonavir with Ribavirin in Adults with Chronic HCV Genotype 4 Infection in Egypt (AGATE-II) Esmat G, ASLD 2015
: 1000 mg/day if < 75 kg or 1200 mg/day if 75 kg Ruane PJ, J")
22 Sofosbuvir and Ribavirin in HCV Genotype 4 Egyptian Ancestry Trial Drug Dosing Sofosbuvir: 400 mg once dailyweight-based Ribavirin (in 2 divided doses): 1000 mg/day if < 75 kg or 1200 mg/day if 75 kg Ruane PJ, J Hepatol. 2015
23 Sofosbuvir and Ribavirin in HCV Genotype 4 Egyptian Ancestry Trial: Results absence of complete prior treatment histories in all patients small number of patients infected with non-4a HCV. Ruane PJ, J Hepatol. 2015

 and GS-US-334-0138 in Egypt (n=103).")
24 Sofosbuvir plus Ribavirin in the Treatment of Egyptian Patients with Chronic Genotype 4 HCV Infection An integrated analysis was conducted of data from treatment-naïve and treatmentexperienced patients enrolled in Study GS-US in the USA (n=60) and GS-US in Egypt (n=103). Doss W, AASLD 2015
25 Retreatment of GT4 Chronic HCV Ledipasvir-Sofosbuvir - NIAID Synergy (Genotype 4) Ombitasvir-Paritaprevir-Ritonavir - PEARL-I Sofosbuvir + Ribavirin - Egyptian Ancestry
 100 80 60 65 83 86 60 40 40 20 0 All Treatment-Naïve Relapsers Partial Null Moreno C, J Hepatology")
26 Patients (%) with SVR12 Retreatment of GT4 Chronic HCV - IFN-based Regimens Simeprevir + Peginterferon + Ribavirin in Genotype 4 (RESTORE) All Treatment-Naïve Relapsers Partial Null Moreno C, J Hepatology 2015




27 Retreatment of GT4 Chronic HCV All-oral Regimens Kohli A, Lancet Infect Dis Abergel, EASL, 2015 Hézode C, Lancet Ruane PJ, J Hepatol. 2015



 SVR 12, 100 %")

28 Treatment of Hepatitis C Genotype 4 patients with Simeprevir and Sofosbuvir: Preliminary Results from a Phase IIa, Partially Randomised, Open-label Trial conducted in Egypt (OSIRIS) SVR 12, 100 % independently of prior PR response or cirrhosis G. Van Dooren, AASLD 2015

29 Figure 1. Study Designs Advanced cirrhosis ALLY-1 c Post-liver transplant Treatment-naive ALLY-2 Treatment-experienced Sofosbuvir + Daclatasvir +RBV DCV 60 mg + SOF 400 mg + RBV DCV 60 mg + SOF 400 mg + RBV DCV 30/60/90 mg + SOF 400 mg SVR12 b Regimen Study SVR 12 DCV 30/60/90 mg + SOF 400 mg DCV 30/60/90 mg + SOF 400 mg DCV + SOF + RBV ALLY (4) (advanced cirrhosis) Treatment-naive ALLY-3 Treatment-experienced AI d GT 1 Treatment-naive GT 2/3 Treatment-naive DCV 60 mg +SOF 400 mg DCV 60 mg +SOF 400 mg A: SOF 7 d, then DCV 60 mg + SOF 400 mg C: DCV 60mg + SOF 400 mg E: DCV 60 mg + SOF 400 mg + RBV G: DCV 60 mg + SOF 400 mg H: DCV 60 mg + SOF 400 mg + RBV B: SOF 7 d, then DCV 60 mg + SOF 400 mg D: DCV 60 mg + SOF 400 mg F: DCV 60 mg + SOF 400 mg + RBV SVR12 b GT 1 PI failures I: DCV 60 mg + SOF 400 mg J: DCV 60 mg + SOF 400 mg + RBV Week 0 Week 8 Week 12 Week 24 Week 36
 (with or without IFN).")
30 HCV genotype 4: SVR with different direct-acting antivirals (DAAs) (with or without IFN). Asselah T, Journal of Hepatology 2015
31 Future Regimens for GT-4
32 Future Regimens for GT-4 Daclatasvir and Asunaprevir Plus Peginterferon Alfa-2a and Ribavirin Daclatasvir, asunaprevir, and beclabuvir Sofosbuvir-Velpatasvir Grazoprevir-Elbasvir Ravidasvir (PPI-668) and Sofosbuvir




33 Daclatasvir and Asunaprevir Plus Peginterferon Alfa-2a and Ribavirin in Patients With HCV Genotype 1 or 4 Infection: Phase 3 HALLMARK-QUAD, Jensen IDWeek 2014
34 A randomized trial of daclatasvir in combination with asunaprevir and beclabuvir in patients with chronic hepatitis C virus genotype 4 infection RCT, 1:1 to receive a twice-daily oral regimen comprising of 75 mg or 150 mg of beclabuvir, each with daclatasvir (30 mg) and asunaprevir (200 mg), for 12 weeks with 48 weeks of post-treatment follow up. Patients with compensated cirrhosis were permitted although none were enrolled. Hassanein T, Journal of Hepatology 2015
35 ASTRAL-1, -2, -3, -4 Trials Sofosbuvir/ Velpatasvir FDC ± RBV in GT1-6 HCV Multicenter, randomized phase III trials in Tx-naive and Tx-experienced pts 12 wks 24 wks ASTRAL-1 [1] : GT 1, 2, 4, 5, or 6 HCV (N = 740) ASTRAL-2 [2] : GT2 HCV (N = 266) Sofosbuvir/Velpatasvir (n = 624) Placebo QD (n = 116) Sofosbuvir/Velpatasvir (n = 134) Sofosbuvir + RBV (n = 132) Gen 4, SVR % (116/116) ASTRAL-3 [3] : GT3 HCV (N = 552) ASTRAL-4 [4] : GT1-6 HCV and CTP B cirrhosis (N = 267) Sofosbuvir/Velpatasvir (n = 277) Sofosbuvir + RBV (n = 275) Sofosbuvir/Velpatasvir (n = 90) Sofosbuvir/Velpatasvir + RBV (n = 87) Sofosbuvir/Velpatasvir (n = 90) Sofosbuvir/velpatasvir 400/100 mg QD 1. Feld JJ, et al. NEJM Sulkowski MS, et al. AASLD Abstract Mangia A, et al. AASLD Abstract Charlton MR, et al. AASLD Abstract LB-13.
36 Grazoprevir/Elbasvir Studies: Overview C-EDGE TN C-EDGE TE C-EDGE Coinfection C-SALVAGE C-SCAPE C-WORTHY C C-SWIFT C-SURFER 12 wks of grazoprevir/elbasvir in treatment-naive pts with GT1, 4, or 6 HCV infection 12 or 16 wks of grazoprevir/elbasvir ± RBV in pts with GT1, 4, or 6 HCV and previous failure of pegifn/rbv 12 wks of grazoprevir/elbasvir in HCV treatment-naive pts coinfected with HIV and GT1, 4, or 6 HCV 12 wks of grazoprevir/elbasvir + RBV in pts with GT1 HCV and previous failure of HCV PI + pegifn/rbv 12 wks of grazoprevir ± elbasvir ± RBV in treatment-naive, noncirrhotic pts with GT2, 4, 5, or 6 HCV 8 wks of grazoprevir/elbasvir ± RBV in treatment-naive, noncirrhotic pts with GT1b HCV Short-duration therapy with grazoprevir/elbasvir + sofosbuvir in treatment-naive, GT1 or 3 HCV infected pts ± cirrhosis 12 wks of grazoprevir/elbasvir in pts with GT1 HCV infection and stage 4 or 5 CKD
37 Grazoprevir/Elbasvir Studies: Overview C-EDGE TN C-EDGE TE C-SCAPE 12 wks of grazoprevir/elbasvir in treatment-naive pts with GT1, 4, or 6 HCV infection 22% cirrhotics, SVR12, 100% (18/18) 12 or 16 wks of grazoprevir/elbasvir ± RBV in pts with GT1, 4, or 6 HCV and previous failure of pegifn/rbv 34 % cirrhotics SVR 4, GZR/EBR - 78 % (7/9) - GZR/EBR+RBV 100 % (15/15) 12 wks of grazoprevir ± elbasvir ± RBV in treatment-naive, noncirrhotic pts with GT2, 4, 5, or 6 HCV N=20, SVR12 GZR/EBR 100 % - GZR/EBR+RBV 90 % C-EDGE CO-STAR (PWID) (+- cirrhosis), SVR12 92 % (11/12)
38 Grazoprevir/Elbasvir Studies: Overview C-EDGE TN C-EDGE TE C-SCAPE 12 wks of grazoprevir/elbasvir in treatment-naive pts with GT1, 4, or 6 HCV infection 22% cirrhotics, SVR12, 100% (18/18) 12 or 16 wks of grazoprevir/elbasvir ± RBV in pts with GT1, 4, or 6 HCV and previous failure of pegifn/rbv 34 % cirrhotics SVR 4, GZR/EBR - 78 % (7/9) - GZR/EBR+RBV 100 % (15/15) 12 wks of grazoprevir ± elbasvir ± RBV in treatment-naive, noncirrhotic pts with GT2, 4, 5, or 6 HCV N=20, SVR12 GZR/EBR 100 % - GZR/EBR+RBV 90 % C-EDGE CO-STAR (PWID) (+- cirrhosis), SVR12 92 % (11/12)
39 GT4 infected patients enrolled in the GZR/EBR phase 2/3 clinical program Asselah T, AASLD 2015 Child-Pugh A cirrhosis. SVR 12 (TE) - 76, 4% (13/17) (includes 13 pts treated for 12 wks and 4 pts treated for 16/18 wks). Jacobson IM, et al. AASLD 2015

 and Sofosbuvir:")

40 High Virologic Response Rate in Egyptian HCV-Genotype 4 Patients Treated with Ravidasvir (PPI-668) and Sofosbuvir: Results of a Large Multicenter Phase 3 Registrational Trial Esmat G, AASLD 2015
41 Genotype 4 - Real Clinical Practice Data - 1 SOF/PEG/RBV IFN/RBV/SOF N=24 M.H.Wehmeyer GERMA NY Dig Liver Dis 2015 Cirrhosis, 23.1% TE, 50 % SVR % SOF/PEG/RBV SOF/PEG/RBV N=16 N=4 S. Alqahtani Cirrhosis, USA % EASL 2015 TE, Cirrhosis % % SVR12, TE, % -88 % SVR 4, 88% SOF/PEG/RBV N=11 K. Bichoupan USA EASL % had a FIB-4 score 3.25 NA SVR12, 82% SOF/PEG/RBV D.Ouzan FRANCE EASL 2015 Cirrhosis 77% TE 100 % SVR 12, 67 % SOF/RBV SOF/RBV N=2 K. Bichoupan USA EASL % had a FIB-4 NA SOF/RBV N=2 Cirrhosis, % TE, 59 score % 3.25 SVR12, % SVR12, 50% SOF/RBV M=45 Moutaz F. Derbala QATAR AASLD 2015 Cirrhosis, 34.3% TE 58.8% SVR4, 96%
42 Genotype 4 - Real Clinical Practice Data - 2 SOF/DCV SOF/DCV N=33 ANRS CO22 HEPATHER FRANCE EASL 2015 Cirrhosis 78,8 % TE 70,7 % SVR 12, 12 W 90 % SOF/DCV N=1 Cirrhosis, 78 % TE, 71 % SVR 12, 24 W 100 % SOF/DCV/RBV N=15 12 W 90 % ANRS CO22 FRANCE EASL Cirrhosis 86,7 % 24 TE W 66-% 100 % SVR 12, HEPATHER W 100 % SOF/DCV/RBV N= 2 Cirrhosis, % TE, % SVR 12, 24 W 100 % 12 W 100 % SOF/DCV/RBV D.OUZAN FRANCE EASL W 100 % Cirrhosis 77% TE 100 % SVR 12, 100 % SMV/DCV SMV/DCV N=47 SMV/DCV Mohamed Alzaabi N=2 UNITED ARAB Cirrhosis, AASLD % Cirrhosis, 72.3 TE, 56 % TE, 56.1% SVR12, 85 % SVR 4, 85% EMIRATES SMV/DCV N=47 E. Taleb UNITED ARAB EMIRATES AASLD 2015 Cirrhosis, 68,4 % TE 56.1% SVR12, 85 %
43 Genotype 4 - Real Clinical Practice Data - 3 SOF/SMV+/- RBV SOF/SMV+/- ribavirin SOF/SMV+/- RBV (G 1/4) SOF/SMV+/- RBV (G 1/4) N=73 C. Moreno BELGIUM AASLD 2015 Cirrhosis 56.2 % Te 78.8 % W12, 74 % N=108 Z. Kayali USA AASLD 2015 Cirrhosis 100 % TE 46% SVR12, 77% N=130 E. Nguyen-Khac FRANCE AASLD 2015 Cirrhosis 66.9%. TE 70 % SVR % SMV/SOF N=19 E. Taleb UAE AASLD 2015 Cirrhosis 68.4 TE 56.1% SVR12, 94% SOF/SIM N=6 Cirrhosis, % TE, % SVR 12, % SOF/SMV N=40 F. Derbala Qatar AASLD 2015 Cirrhosis 34.3% TE 58.8% SVR4 96% SOF/SIM/RBV N= 7 Cirrhosis, % TE, % SVR 12, % SOF/SIM N=6 S. Alqahtani USA EASL 2015 Cirrhosis 38% TE 50 % 100% SOF/SIM + RBV N=6 S. Alqahtani USA EASL 2015 Cirrhosis 33% TE 83 % 100% SOF/SIM N=32 A.M. Hefner USA EASL 2015 Cirrhosis 100 % TE 71% SVR 12, naive 80%, TE 81% SOF/SMV N=27 K. Bichoupan USA EASL % had a FIB-4 score 3.25, NA SVR12 81% SOF/SMV/RBV N=70 K. Bichoupan USA EASL % had a FIB-4 score 3.25, NA SVR12 86% SOF/SIM N=22, 12 w N=32 24 w ANRS CO22 HEPATHER FRANCE AASLD 2015 Cirrhosis 53 %, 12 w Cirrhosis 61 %, 24 w TE 73 % SVR 12, 12 W 84 % 24 W 100 % SOF/SIM/RBV N=24, 12 w N=32 24 w ANRS CO22 HEPATHER FRANCE AASLD 2015 Cirrhosis 67 %, 12 w Cirrhosis 89 %, 24 w TE 71 % SVR 12, 12 W 100 % 24 W 100 % SOF/SIM/RBV D.OUZAN FRANCE EASL 2015 Cirrhosis 77% TE 100 % SVR 12, 100 %

44 Real Clinical Practice Data in Greece, n=52 SVR12, % Pts 1/ 4 /0 4/ 20/ 4 4/ 0/ 0 6/ 0/ 3 1/ 5/ 0 Papatheodoridis G, ΠΓΣ 2015
45
46 Recommendations on Treatment of Hepatitis C Genotype 4 AASLD Treatment naïve ledipasvir (90 mg)/sofosbuvir (400 mg) for 12 weeks paritaprevir (150 mg)/ritonavir (100 mg)/ombitasvir (25 mg) and weight-based RBV for 12 weeks sofosbuvir (400 mg) and weight-based RBV for 24 weeks Alternative regimen for patients eligible to receive interferon sofosbuvir (400 mg) and weight-based RBV plus weekly PEG-IFN for 12 week Prior treatment with PEG-IFN and RBV has failed ledipasvir (90 mg)/sofosbuvir (400 mg) for 12 weeks paritaprevir (150 mg)/ritonavir (100 mg)/ombitasvir (25 mg) (PrO) and weight based RBV for 12 weeks sofosbuvir (400 mg) for 12 weeks and daily weight based RBV plus weekly PEG-IFN for 12 weeks sofosbuvir (400 mg) and weight-based RBV for 24 weeks.
47 Recommendations on Treatment of Hepatitis C Genotype 4 European Association for the Study of the Liver cirrhosis ΚΕ.ΕΛ.Π.ΝΟ 12 w SMV+PR / PR x12/12 ή 36 w 24 w SOF/LDV SOF/LDV + RBV x 12 w + PR x 24 ή 48 w x 12 w x 12 w Sof +DCV SOF+DCV +RBV x12 ή 24 w

48 Recommendations on Treatment of Hepatitis C Genotype 4 European Association for the Study of the Liver 96 % 83 % 96 % 100 % cirrhosis 100 % RWD 100 % RWD % 100 % 97 % 100 % RWD 100 % ΚΕ.ΕΛ.Π.ΝΟ 12 w SMV+PR / PR x12/12 ή 36 w 24 w SOF/LDV SOF/LDV + RBV x 12 w + PR x 24 ή 48 w x 12 w x 12 w Sof +DCV SOF+DCV +RBV x12 ή 24 w
49 Treatment recommendations for retreatment of HCV-monoinfected or HCV/HIV coinfected patients with chronic hepatitis C who failed to achieve an SVR on prior antiviral therapy containing one or several DAA(s) EASL - Genotype 4 Patients that failed SOF alone, in combination with RBV or in combination with PegIFN-α and RBV GT4 LDV/SOF + RBV 12 wk or 24 wk (if F3) OBV/PTV/R TV + RBV 12 wk or 24 wk (if F3) SOF + SMV + RBV 12 wk or 24 wk (if F3) SOF + DCV + RBV 12 wk or 24 wk (if F3) Patients that failed PegIFN-α, RBV and SMV or SOF and SMV GT1 or 4 LDV/SOF + RBV 12 wk SOF + DCV + RBV 12 wk or 24 wk (if F3) Patients that failed PegIFN-α, RBV and DCV GT4 SOF + SMV + RBV 12 wk or 24 wk (if F3) Patients that failed SOF and DCV or LDV/SOF GT4 SOF + SMV + RBV 12 wk or 24 wk (if F3) Patients that failed OBV/PTV/RTV and DSV (GT1) or OBV/PTV/RTV (GT4) GT4 LDV/SOF + RBV 12 wk or 24 wk (if F3) SOF + SMV + RBV 12 wk or 24 wk (if F3) SOF + DCV + RBV 12 wk or 24 wk (if F3)
50 Summary Genotype 4 hepatitis C virus infection is not common in the United States, but it is highly prevalent in the Middle East, Africa, and Southern Europe. HCV-G4 has been considered difficult to treat with pegylated interferon (PegIFN) and ribavirin (RBV) treatment, with sustained virological response (SVR) rates around 50% The main limitations on HCV-G4 are their small sample size and the relatively mild stage of liver diseases included in patients There are effective regimens There is optimism for patients with genotype 4 HCV infection, with several promising ongoing trials. With these excellent data, the next steps will be to improve screening and access to therapy
51
TREATMENT OF GENOTYPE 2
 Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Treatment of Genotype 2, 3,and 4 David E. Bernstein, MD, FACG Advisory Committee/Board Member: AbbVie Pharmaceuticals, Gilead, Merck, Janssen Consultant: AbbVie Pharmaceuticals, Bristol-Myers Squibb, Gilead,
Treatments of Genotype 2, 3,and 4: Now and in the future
 Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Treatments of Genotype 2, 3,and 4: Now and in the future THERAPY FOR THE TREATMENT OF GENOTYPE 2 1 GT 2 and GT 3 Treatment-Naïve: SOF+RBV vs PEG-IFN+RBV FISSION Study Design HCV GT 2 and GT 3 Treatment-naïve
Genotype 4, finally cured? Imam Waked Professor of Medicine National Liver Institute
 Genotype 4, finally cured? Imam Waked Professor of Medicine National Liver Institute Paris, January 12, 215 Disclosures Investigator, speaker, and advisory board member for: Roche, MSD, BMS, Gilead, Janssen,
Genotype 4, finally cured? Imam Waked Professor of Medicine National Liver Institute Paris, January 12, 215 Disclosures Investigator, speaker, and advisory board member for: Roche, MSD, BMS, Gilead, Janssen,
5/12/2016. Learning Objectives. Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients
 5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
5/12/216 Management of Hepatitis C Virus Genotype 2 or 3 Infected Treatment-Naive or Experienced Patients Alexander Monto, MD Professor of Clinical Medicine University of California San Francisco San Francisco,
HCV Treatment of Genotype 1: Now and in the Future
 HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
HCV Treatment of Genotype 1: Now and in the Future Bruce R. Bacon, MD, FACG James F. King, MD Endowed Chair in Gastroenterology Professor of Internal Medicine Co-Director of the Abdominal Transplant Program
Treatment of HCV infection in daily clinical practice. Which are the optimal options for Genotypes 2 and 3? Jiannis Vlachogiannakos
 Treatment of HCV infection in daily clinical practice. Which are the optimal options for Genotypes 2 and 3? Jiannis Vlachogiannakos Associate Professor of Gastroenterology Academic Department of Gastroenterology
Treatment of HCV infection in daily clinical practice. Which are the optimal options for Genotypes 2 and 3? Jiannis Vlachogiannakos Associate Professor of Gastroenterology Academic Department of Gastroenterology
HCV Infection: EASL Clinical Practice Guidelines Francesco Negro University Hospital Geneva Switzerland
 HCV Infection: EASL Clinical Practice Guidelines 2016 Francesco Negro University Hospital Geneva Switzerland Panel Codinat: Jean-Michel Pawlotsky Panel: Alessio Aghemo David Back Geoffrey Dusheiko Xavier
HCV Infection: EASL Clinical Practice Guidelines 2016 Francesco Negro University Hospital Geneva Switzerland Panel Codinat: Jean-Michel Pawlotsky Panel: Alessio Aghemo David Back Geoffrey Dusheiko Xavier
Update in the Management of Hepatitis C: What Does the Future Hold
 Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
Update in the Management of Hepatitis C: What Does the Future Hold Paul Y Kwo, MD, FACG Professor of Medicine Mdi Medical ldirector, Liver Transplantation tti Gastroenterology/Hepatology Division Indiana
What is the Optimized Treatment Duration? To Overtreat versus Undertreat. Nancy Reau, MD Associate Professor of Medicine University of Chicago
 What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
What is the Optimized Treatment Duration? To Overtreat versus Undertreat Nancy Reau, MD Associate Professor of Medicine University of Chicago Learning Objectives: 1. Discuss patient populations appropriate
Hepatitis C in Special Populations
 Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
Hepatitis C in Special Populations David E. Bernstein, MD, FACG Vice Chairman of Medicine for Clinical Trials Chief, Division of Hepatology and Sandra Atlas Bass Center for Liver Diseases Northwell Health
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London
 HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
HCV Treatment Failure: What Next? Dr Ashley Brown, Imperial College Healthcare NHS Trust, London European HIV Hepatitis Co-infection Conference QEII Conference Centre 10 th December 2015 Dr Ashley Brown
Initial Treatment of HCV G Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona
 Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Initial Treatment of HCV G1 2016 Hugo E. Vargas, MD Professor of Medicine Medical, Director Office of Clinical Research Mayo Clinic Arizona Disclosure Information Disclosure Information Dr. Vargas receives
Expert Perspectives: Best of HCV from EASL 2015
 Best of HCV from EASL 2015 Expert Perspectives: Best of HCV from EASL 2015 Saeed Hamid, MD Alex Thompson, MD, PhD This activity is supported by educational grants from AbbVie, Bristol-Myers Squibb, and
Best of HCV from EASL 2015 Expert Perspectives: Best of HCV from EASL 2015 Saeed Hamid, MD Alex Thompson, MD, PhD This activity is supported by educational grants from AbbVie, Bristol-Myers Squibb, and
IFN-free therapy in naïve HCV GT1 patients
 IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
IFN-free therapy in naïve HCV GT1 patients Paris Hepatitis Conference Paris, 12th January, 2015 Pr Tarik Asselah MD, PhD; Service d Hépatologie & INSERM U773 University Paris Diderot, Hôpital Beaujon,
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France
 How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
How to optimize treatment in G3 patients? Jérôme GOURNAY, MD Hépatologie Centre Hospitalier Universitaire de Nantes France Paris Hepatitis Conference, January 12, 2016 Disclosures I have received funding
Saeed Hamid, MD Alex Thompson, MD, PhD
 Saeed Hamid, MD Alex Thompson, MD, PhD 1 We will review some top line data from EASL Majority of the time discussing how the data affects daily practice 2 Grazoprevir (GZR; MK-5172) + Elbasvir (EBR; MK-
Saeed Hamid, MD Alex Thompson, MD, PhD 1 We will review some top line data from EASL Majority of the time discussing how the data affects daily practice 2 Grazoprevir (GZR; MK-5172) + Elbasvir (EBR; MK-
HCV-G3: Sofosbuvir with ledipasvir or daclatasvir?
 HCV-G3: Sofosbuvir with ledipasvir or daclatasvir? Ioannis Goulis, MD Aristotelian University of Thessaloniki XXIII International Hepatitis B & C Meeting of Athens Hadziyannis HCV genotype 3 therapy Chronic
HCV-G3: Sofosbuvir with ledipasvir or daclatasvir? Ioannis Goulis, MD Aristotelian University of Thessaloniki XXIII International Hepatitis B & C Meeting of Athens Hadziyannis HCV genotype 3 therapy Chronic
A One-day Scientific Conference: Updates on Hepatitis C Treatments along with Consensus on Management of Hepatitis C in Iran
 A One-day Scientific Conference: Updates on Hepatitis C Treatments along with Consensus on Management of Hepatitis C in Iran Teheran, 22 July 2016 Massimo Colombo Treatment of HCV genotype 1 & 4 with DAAs
A One-day Scientific Conference: Updates on Hepatitis C Treatments along with Consensus on Management of Hepatitis C in Iran Teheran, 22 July 2016 Massimo Colombo Treatment of HCV genotype 1 & 4 with DAAs
Treatement Experienced patients without cirrhosis. Rafael Esteban Hospital Universitario Valle Hebron Barcelona
 Treatement Experienced patients without cirrhosis Rafael Esteban Hospital Universitario Valle Hebron Barcelona Agenda With IFN PegIFN+ Ribavirin + Simeprevir PegIFN+ Ribavirin+ Sofosbuvir Without IFN Sofosbuvir
Treatement Experienced patients without cirrhosis Rafael Esteban Hospital Universitario Valle Hebron Barcelona Agenda With IFN PegIFN+ Ribavirin + Simeprevir PegIFN+ Ribavirin+ Sofosbuvir Without IFN Sofosbuvir
Hepatitis C Treatment 2014
 Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
Hepatitis C Treatment 214 Brendan M. McGuire, MD UAB Liver Center Outline Epidemiology/National History Terminology for Treatment Treatment Considerations Current Treatment Options Genotype 1 (GT 1) Genotype
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients
 2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
2017 Bruce Lucas Hepatology and Liver Transplant Symposium October 13th 2017 Management of Hepatitis C in Pre- and Post-Transplant Patients Jens Rosenau, MD Associate Professor of Medicine Acting Director
Genotype 1 HCV in 2016: Clinical Decision Making in a Time of Plenty
 Genotype 1 HCV in 216: Clinical Decision Making in a Time of Plenty Ira M. Jacobson, MD Chair, Department of Medicine Mount Sinai Beth Israel Senior Faculty and Vice-Chair, Department of Medicine Icahn
Genotype 1 HCV in 216: Clinical Decision Making in a Time of Plenty Ira M. Jacobson, MD Chair, Department of Medicine Mount Sinai Beth Israel Senior Faculty and Vice-Chair, Department of Medicine Icahn
VIRAL LIVER DISEASE. OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015
 VIRAL LIVER DISEASE OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015 Financial Interest Disclosure (over the past 24 months) Dr. Paul Marotta Relationships related to this presentation! Research
VIRAL LIVER DISEASE OAG Post DDW Course Westin Prince, Toronto, June 13-14, 2015 Financial Interest Disclosure (over the past 24 months) Dr. Paul Marotta Relationships related to this presentation! Research
HCV In 2015: Maximizing SVR
 HCV In 2015: Maximizing SVR Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia ramji_a@hotmail.com Disclosures (within Last
HCV In 2015: Maximizing SVR Alnoor Ramji Gastroenterology & Hepatology Clinical Associate Professor Division of Gastroenterology University Of British Columbia ramji_a@hotmail.com Disclosures (within Last
Tough Cases in HIV/HCV Coinfection
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Tough Cases in HIV/HCV Coinfection John Scott, MD, MSc Assistant Professor University of Washington Presentation prepared by: J Scott Last Updated: Jun 5, 2014
Rome, February nd Riunione Annuale AISF th AISF ANNUAL MEETING
 Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
Rome, February 20-21 nd 2014 Riunione Annuale AISF 2014 14 th AISF ANNUAL MEETING Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations IFN
Future strategies with new DAAs
 Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
Future strategies with new DAAs Ola Weiland professor New direct antiviral drugs Case no 1 male with genotype 2b Male with gt 2b chronic HCV Male with gt 2b relapse afer peg-ifn + RBV during 24 weeks
SVR Updates from the 2013 EASL
 Updates from the 2013 EASL By Tracy Swan, Treatment Action Group Streamlining HCV Treatment Treatment for hepatitis C virus (HCV) is becoming simpler, shorter, and more effective. All-oral combinations
Updates from the 2013 EASL By Tracy Swan, Treatment Action Group Streamlining HCV Treatment Treatment for hepatitis C virus (HCV) is becoming simpler, shorter, and more effective. All-oral combinations
Hepatitis C Emerging Treatment Paradigms
 Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
Hepatitis C Emerging Treatment Paradigms David R Nelson MD Assistant Vice President for Research Professor of Medicine Director, Clinical and Translational Science Institute University of Florida Gainesville,
HCV Management in Decompensated Cirrhosis: Current Therapies
 Treatment of Patients with Decompensated Cirrhosis and Liver Transplant Recipients Paul Y. Kwo, MD, FACG Professor of Medicine Gastroenterology/Hepatology Division Stanford University email pkwo@stanford.edu
Treatment of Patients with Decompensated Cirrhosis and Liver Transplant Recipients Paul Y. Kwo, MD, FACG Professor of Medicine Gastroenterology/Hepatology Division Stanford University email pkwo@stanford.edu
4/30/2015. Interactive Case-Based Presentations and Audience Discussion. Debika Bhattacharya, MD, MSc. Learning Objectives
 4/3/215 Interactive Case-Based Presentations and Audience Discussion Debika Bhattacharya, MD, MSc Assistant Clinical Professor University of California Los Angeles Los Angeles, California Formatted:4-27-215
4/3/215 Interactive Case-Based Presentations and Audience Discussion Debika Bhattacharya, MD, MSc Assistant Clinical Professor University of California Los Angeles Los Angeles, California Formatted:4-27-215
Update on chronic hepatitis C treatment: current trends, new challenges, what next?
 Update on chronic hepatitis C treatment: current trends, new challenges, what next? Matti Maimets 12.06.2015 MMaimets15 Disclosure this presentation is sponsored by Gilead Sciences MMaimets15 MMaimets15
Update on chronic hepatitis C treatment: current trends, new challenges, what next? Matti Maimets 12.06.2015 MMaimets15 Disclosure this presentation is sponsored by Gilead Sciences MMaimets15 MMaimets15
Why make this statement?
 HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
HCV Council 2014 10 clinical practice statements were evaluated by the Council A review of the available literature was conducted The level of support and level of evidence for the statements were discussed
Need to Assess HCV Resistance to DAAs: Is it Useful and When?
 Need to Assess HCV Resistance to DAAs: Is it Useful and When? Stéphane Chevaliez French National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
Need to Assess HCV Resistance to DAAs: Is it Useful and When? Stéphane Chevaliez French National Reference Center for Viral Hepatitis B, C and delta Department of Virology & INSERM U955 Henri Mondor Hospital
Current Treatment Options for HCV Patients. Michael Manns Dept. of Gastroenterology, Hepatology and Endocrinology Hannover Germany
 Current Treatment Options for HCV Patients Michael Manns Dept. of Gastroenterology, Hepatology and Endocrinology Hannover Germany 7th International Congress of Internal Medicine of Central Greece, Larissa,
Current Treatment Options for HCV Patients Michael Manns Dept. of Gastroenterology, Hepatology and Endocrinology Hannover Germany 7th International Congress of Internal Medicine of Central Greece, Larissa,
Current trends in CHC 1st genotype treatment
 Current trends in CHC 1st genotype treatment Tarik Asselah MD, PhD Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France Disclosures Employee of Paris Public University
Current trends in CHC 1st genotype treatment Tarik Asselah MD, PhD Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France Disclosures Employee of Paris Public University
The Egyptian Plan to Cure HCV
 The Egyptian Plan to Cure HCV Gamal Esmat Professor of Endemic Medicine & Hepatology Vice President of Cairo University for Graduate Studies and Research Disclosure Advisory Committee Board Member : MSD,
The Egyptian Plan to Cure HCV Gamal Esmat Professor of Endemic Medicine & Hepatology Vice President of Cairo University for Graduate Studies and Research Disclosure Advisory Committee Board Member : MSD,
Associate Professor of Medicine University of Chicago
 Nancy Reau, MD Associate Professor of Medicine University of Chicago Management of Hepatitis C: New Drugs and New Paradigms HCV is More Lethal than HIV Infection HCV superseded HIV as a cause of death
Nancy Reau, MD Associate Professor of Medicine University of Chicago Management of Hepatitis C: New Drugs and New Paradigms HCV is More Lethal than HIV Infection HCV superseded HIV as a cause of death
Latest Treatment Updates for GT 2 and GT 3 Patients
 Latest Treatment Updates for GT 2 and GT 3 Patients Eric Lawitz, MD, AGAF, CPI Vice President, Scientific and Research Development The Texas Liver Institute Clinical Professor of Medicine University of
Latest Treatment Updates for GT 2 and GT 3 Patients Eric Lawitz, MD, AGAF, CPI Vice President, Scientific and Research Development The Texas Liver Institute Clinical Professor of Medicine University of
HCV therapy : Clinical case
 HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
HCV therapy : Clinical case PHC 2018 Paris January 14th, 2018 Tarik Asselah (MD, PhD) Professor of Medicine Hepatology, Chief INSERM UMR 1149, Hôpital Beaujon, Clichy, France. Disclosures Professor Asselah
Shorter Durations and Pan-genotypic Regimens The Final Frontier. Professor Greg Dore
 Shorter Durations and Pan-genotypic Regimens The Final Frontier Professor Greg Dore Disclosures Funding and speaker fees from AbbVie, Bristol-Myers Squibb, Gilead Sciences and Merck Efficacy Evolution
Shorter Durations and Pan-genotypic Regimens The Final Frontier Professor Greg Dore Disclosures Funding and speaker fees from AbbVie, Bristol-Myers Squibb, Gilead Sciences and Merck Efficacy Evolution
CCO Official Conference Coverage: Clinical Impact of New Data From AASLD 2015
 CCO Official Conference Coverage: Clinical Impact of New Data From AASLD 2015 CCO Official Conference Coverage of the 2015 Annual Meeting of the American Association for the Study of Liver Diseases, November
CCO Official Conference Coverage: Clinical Impact of New Data From AASLD 2015 CCO Official Conference Coverage of the 2015 Annual Meeting of the American Association for the Study of Liver Diseases, November
Treatment of HCV in 2016
 5/1/16 Treatment of HCV in 16 Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novartis, Springbank,
5/1/16 Treatment of HCV in 16 Graham R Foster Professor of Hepatology QMUL Conflicts of Interest Speaker and consultancy fees received from AbbVie, BI, BMS, Gilead, Janssen, Roche, Merck, Novartis, Springbank,
A treatment revolution: current management for chronic HCV
 A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
A treatment revolution: current management for chronic HCV Ray Chung, M.D. Director of Hepatology and Liver Center Kevin and Polly Maroni Research Scholar Massachusetts General Hospital Disclosures Research
HCV Resistance Clinical Aspects. Sanjay Bhagani Royal Free Hospital/UCL London
 HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
HCV Resistance Clinical Aspects Sanjay Bhagani Royal Free Hospital/UCL London DAAs in 2018, and beyond % patients % patients Changing characteristics of patients treated with DAA over time Prospective,
Treatment of Hepatitis C and Renal Disease
 Treatment of Hepatitis C and Renal Disease David E. Bernstein, MD, FACG Vice Chair of Medicine for Clinical Trials Chief, Division of Hepatology and Director, Sandra Atlas Bass Center for Liver Diseases
Treatment of Hepatitis C and Renal Disease David E. Bernstein, MD, FACG Vice Chair of Medicine for Clinical Trials Chief, Division of Hepatology and Director, Sandra Atlas Bass Center for Liver Diseases
Dr. Siddharth Srivastava
 Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
Dr. Siddharth Srivastava MD, DM (Gastroenterology) Associate Professor GIPMER, New Delhi Rashtriya Gaurav Award 2013 for work on hepatitis B and C Set up Liver clinic at GIPMER and in charge EUS laboratory.
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis. Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA
 Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
Case 4: A 61-year-old man with HCV genotype 3 with cirrhosis Ira M. Jacobson, M.D. Weill Cornell Medical College New York, New York USA 1 Genotype 3 case 61-year-old man with HCV genotype 3 Cirrhosis on
STATE OF THE ART Update: Treatment Options 2016 Mark Sulkowski, MD
 Housekeeping Please turn off or silence cell phones. Restrooms are located on this floor. Make a left out of the ballroom foyer and the men s room is on your left. The ladies room is across from the elevators
Housekeeping Please turn off or silence cell phones. Restrooms are located on this floor. Make a left out of the ballroom foyer and the men s room is on your left. The ladies room is across from the elevators
Management of HCV Tawesak Tanwandee
 Management of HCV 2016 Tawesak Tanwandee Topics Burden of HCV in our countries Natural history and unmet need for HCV treatment Current treatment as for 2016 Conclusion Evolution from HCV infection to
Management of HCV 2016 Tawesak Tanwandee Topics Burden of HCV in our countries Natural history and unmet need for HCV treatment Current treatment as for 2016 Conclusion Evolution from HCV infection to
VII CURSO AVANCES EN INFECCIÓN VIH Y HEPATITIS VIRALES
 VII CURSO AVANCES EN INFECCIÓN VIH Y HEPATITIS VIRALES REGIMENES TERAPÊUTICOS DE LA HEPATITIS C, INTERFERÓN FREE A Coruña 2 Febrero 2013 Rui Sarmento e Castro Centro Hospitalar do Porto HJU ECS Universidade
VII CURSO AVANCES EN INFECCIÓN VIH Y HEPATITIS VIRALES REGIMENES TERAPÊUTICOS DE LA HEPATITIS C, INTERFERÓN FREE A Coruña 2 Febrero 2013 Rui Sarmento e Castro Centro Hospitalar do Porto HJU ECS Universidade
Treating HCV After Liver Transplantation: What are the Treatment Options?
 4 th OPTIMIZE WORKSHOP USING DAAs IN PATIENTS WITH CIRRHOSIS AND LIVER RECIPIENTS Treating HCV After Liver Transplantation: What are the Treatment Options? Maria Carlota Londoño, MD Liver Unit, Hospital
4 th OPTIMIZE WORKSHOP USING DAAs IN PATIENTS WITH CIRRHOSIS AND LIVER RECIPIENTS Treating HCV After Liver Transplantation: What are the Treatment Options? Maria Carlota Londoño, MD Liver Unit, Hospital
The HCV Pipeline Ira M. Jacobson, MD, FACP, FACG, AGAF. Slide Presentation. IFN-free DAA combinations (G1)
") Slide Presentation The HCV Pipeline Vincent Astor Distinguished Professor of Medicine Chief, Division of Gastroenterology and Hepatology Medical Director, Center for the Study of Hepatitis C Weill Cornell
Slide Presentation The HCV Pipeline Vincent Astor Distinguished Professor of Medicine Chief, Division of Gastroenterology and Hepatology Medical Director, Center for the Study of Hepatitis C Weill Cornell
TREATING HEPATITIS C TODAY
 TREATING HEPATITIS C TODAY Nikolaos K. Gatselis Department of Medicine& Research Laboratory of Internal Medicine, Larissa Medical School, Thessaly University Disclosure Research Support: Gilead, Janssen,
TREATING HEPATITIS C TODAY Nikolaos K. Gatselis Department of Medicine& Research Laboratory of Internal Medicine, Larissa Medical School, Thessaly University Disclosure Research Support: Gilead, Janssen,
THE LIVER MEETING 2014:
 THE LIVER MEETING 2014: Summary of presentations from the 65 th Annual Liver Meeting of the American Association for the of Liver Diseases (AASLD), held in Boston, Massachusetts, USA, on 7 th -11 th November
THE LIVER MEETING 2014: Summary of presentations from the 65 th Annual Liver Meeting of the American Association for the of Liver Diseases (AASLD), held in Boston, Massachusetts, USA, on 7 th -11 th November
Transformation of Chronic Hepatitis C Treatment
 Transformation of Chronic Hepatitis C Treatment UVHS, Adana, 22 May 2015 Christoph Sarrazin Goethe-University Hospital Frankfurt am Main Germany Epidemiology of HCV Infection Global Global HCV Prevalence
Transformation of Chronic Hepatitis C Treatment UVHS, Adana, 22 May 2015 Christoph Sarrazin Goethe-University Hospital Frankfurt am Main Germany Epidemiology of HCV Infection Global Global HCV Prevalence
Pivotal New England Journal of Medicine papers 2014 Phase 3 Trial data
 4 th HCV Therapy Advances Meeting Paris, December 12-13, 14 Pivotal New England Journal of Medicine papers 14 Phase 3 Trial data Stefan Zeuzem, MD University of Frankfurt Germany Disclosures Consultancies:
4 th HCV Therapy Advances Meeting Paris, December 12-13, 14 Pivotal New England Journal of Medicine papers 14 Phase 3 Trial data Stefan Zeuzem, MD University of Frankfurt Germany Disclosures Consultancies:
Ledipasvir-Sofosbuvir (Harvoni)
") HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
HEPATITIS WEB STUDY HEPATITIS C ONLINE Ledipasvir-Sofosbuvir (Harvoni) Robert G. Gish MD Professor, Consultant, Stanford University Medical Center Senior Medical Director, St Josephs Hospital and Medical
Wonder pills, breakthroughs and continuing challenges HIV and Hepatitis C antiviral treatments revisited
 Wonder pills, breakthroughs and continuing challenges HIV and Hepatitis C antiviral treatments revisited Harald Hofer Department of Internal Medicine III Division of Gastroenterology and Hepatology Medical
Wonder pills, breakthroughs and continuing challenges HIV and Hepatitis C antiviral treatments revisited Harald Hofer Department of Internal Medicine III Division of Gastroenterology and Hepatology Medical
O. Giouleme Assistant Professor of Gastroenterology Ippokration General Hospital of Thessaloniki
 O. Giouleme Assistant Professor of Gastroenterology Ippokration General Hospital of Thessaloniki Disclosures Advisory Board: Abbvie Pharmaceuticals Speaker: Gilead Sciences, Bristol-Myers Squibb Research
O. Giouleme Assistant Professor of Gastroenterology Ippokration General Hospital of Thessaloniki Disclosures Advisory Board: Abbvie Pharmaceuticals Speaker: Gilead Sciences, Bristol-Myers Squibb Research
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV?
 Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Can we afford to Cure all HIV-HCV Co-infected Patients of HCV? Michael S. Saag, MD Professor of Medicine University of Alabama at Birmingham Birmingham, Alabama FINAL AU EDITED: 09-17-14 Disclosure Dr
Treatment of Hepatitis C Recurrence after Liver Transplantation. Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona
 Treatment of Hepatitis C Recurrence after Liver Transplantation Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Agenda 1. Introduction 2. Treatment options for hepatitis C recurrence after transplantation
Treatment of Hepatitis C Recurrence after Liver Transplantation Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Agenda 1. Introduction 2. Treatment options for hepatitis C recurrence after transplantation
Clinical Сase A previously relapse to PEG IFN + RBV in HCV G3a patient. Konstantin Zhdanov
 Clinical Сase A previously relapse to PEG IFN + RBV in HCV G3a patient Konstantin Zhdanov Genotype 3 in Europe Canada Norway Germany Sweden Czech Republic Poland Approximately 1/3 of HCV-infected patients
Clinical Сase A previously relapse to PEG IFN + RBV in HCV G3a patient Konstantin Zhdanov Genotype 3 in Europe Canada Norway Germany Sweden Czech Republic Poland Approximately 1/3 of HCV-infected patients
6/2/2015. Interactive Case-Based Presentations and Audience Discussion
 6/2/215 Interactive Case-Based Presentations and Audience Discussion Andrew Aronsohn, MD Assistant Professor of Medicine University of Chicago Medical Center Chicago, Illinois Formatted:5-6-215 Washington,
6/2/215 Interactive Case-Based Presentations and Audience Discussion Andrew Aronsohn, MD Assistant Professor of Medicine University of Chicago Medical Center Chicago, Illinois Formatted:5-6-215 Washington,
HIV/Hepatitis C in France: data from real life cohorts LIONEL PIROTH CHU DIJON UNIVERSITY OF BURGUNDY DECEMBER LONDON
 HIV/Hepatitis C in France: data from real life cohorts LIONEL PIROTH CHU DIJON UNIVERSITY OF BURGUNDY DECEMBER 2015 - LONDON The need Decreasing prevalence of chronic hepatitis C in French people living
HIV/Hepatitis C in France: data from real life cohorts LIONEL PIROTH CHU DIJON UNIVERSITY OF BURGUNDY DECEMBER 2015 - LONDON The need Decreasing prevalence of chronic hepatitis C in French people living
Update on Real-World Experience With HARVONI
 Update on Real-World Experience With A RESOURCE FOR PAYERS This information is intended for payers only. The HCV-TARGET and TRIO studies were supported by Gilead Sciences, Inc. Real-world experience data
Update on Real-World Experience With A RESOURCE FOR PAYERS This information is intended for payers only. The HCV-TARGET and TRIO studies were supported by Gilead Sciences, Inc. Real-world experience data
Update on the Treatment of HCV
 Update on the Treatment of HCV K. Rajender Reddy, MD Professor of Medicine Director of Hepatology Director, Viral Hepatitis Center University of Pennsylvania Philadelphia, USA 1 K. Rajender Reddy, MD Disclosure
Update on the Treatment of HCV K. Rajender Reddy, MD Professor of Medicine Director of Hepatology Director, Viral Hepatitis Center University of Pennsylvania Philadelphia, USA 1 K. Rajender Reddy, MD Disclosure
Current HCV Treatment by Genotype
 Current HCV Treatment by Genotype Ari Bunim, MD Assistant Professor Clinical Medicine Weill Cornell Medical College Clinical Director of Hepatology New York-Presbyterian/Queens Objectives To understand
Current HCV Treatment by Genotype Ari Bunim, MD Assistant Professor Clinical Medicine Weill Cornell Medical College Clinical Director of Hepatology New York-Presbyterian/Queens Objectives To understand
Massimo Puoti SC Malattie Infettive AO Ospedale Niguarda Cà Granda, Milano. Eradicazione da HCV e nuove prospettive: Prospetive Terapeutiche future
 Massimo Puoti SC Malattie Infettive AO Ospedale Niguarda Cà Granda, Milano Eradicazione da HCV e nuove prospettive: Prospetive Terapeutiche future DAA classes and subclasses Drug Class Subclass Potency
Massimo Puoti SC Malattie Infettive AO Ospedale Niguarda Cà Granda, Milano Eradicazione da HCV e nuove prospettive: Prospetive Terapeutiche future DAA classes and subclasses Drug Class Subclass Potency
10/21/2016. Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina. Learning Objectives
 A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
A Crash Course on the AASLD/IDSA Hepatitis C Virus Infection Treatment Guidelines: What s New Susanna Naggie, MD, MHS Associate Professor of Medicine Duke University Durham, North Carolina FORMATTED: 1/3/16
THE ROLE OF SOFOSBUVIR/VELPATASVIR IN HCV CURE MARIA SCHINA INTERNIST-HEPATOLOGIST ATHENS EUROCLINIC
 THE ROLE OF SOFOSBUVIR/VELPATASVIR IN HCV CURE MARIA SCHINA INTERNIST-HEPATOLOGIST ATHENS EUROCLINIC ATHENS, MARCH 10 th 2017 DISCLOSURES Research grants from Roche, Bristol-Myers Squibb Lectures for Bristol-Myers
THE ROLE OF SOFOSBUVIR/VELPATASVIR IN HCV CURE MARIA SCHINA INTERNIST-HEPATOLOGIST ATHENS EUROCLINIC ATHENS, MARCH 10 th 2017 DISCLOSURES Research grants from Roche, Bristol-Myers Squibb Lectures for Bristol-Myers
Viva La Revolución: Options to Combat Hepatitis C
 Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
Viva La Revolución: Options to Combat Hepatitis C David L. Wyles, MD Professor of Medicine University of Colorado Chief, Division of Infectious Disease Denver Health Learning Objectives After attending
Will difficult-to-treat patients remain difficultto-treat. generation of treatments?
 Will difficult-to-treat patients remain difficultto-treat with the new generation of treatments? Jordan J Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University
Will difficult-to-treat patients remain difficultto-treat with the new generation of treatments? Jordan J Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University
Direct Acting Antivirals for the Treatment of Hepatitis C Infection
 Hepatitis C Core Curriculum, Module 2 Direct Acting Antivirals for the Treatment of Hepatitis C Infection Jason J. Schafer, PharmD, MPH, BCPS, AAHIVP Objectives Discuss the evolution of hepatitis C treatment
Hepatitis C Core Curriculum, Module 2 Direct Acting Antivirals for the Treatment of Hepatitis C Infection Jason J. Schafer, PharmD, MPH, BCPS, AAHIVP Objectives Discuss the evolution of hepatitis C treatment
Feeling right at home
 Feeling right at home Getting to Cure From Cure to Eradication Jordan J. Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University of Toronto SVR Dramatic Improvements
Feeling right at home Getting to Cure From Cure to Eradication Jordan J. Feld MD MPH Toronto Centre for Liver Disease Sandra Rotman Centre for Global Health University of Toronto SVR Dramatic Improvements
What Should We Do With Difficult to Treat HCV Populations?
 What Should We Do With Difficult to Treat HCV Populations? Norah Terrault, MD Professor of Medicine and Surgery Director, Viral Hepatitis Center University of California San Francisco Disclosures Norah
What Should We Do With Difficult to Treat HCV Populations? Norah Terrault, MD Professor of Medicine and Surgery Director, Viral Hepatitis Center University of California San Francisco Disclosures Norah
PEARL-I. Ombitasvir + Paritaprevir + Ritonavir +/- Ribavirin in HCV GT4. Treatment Naïve and Treatment Experienced
 Phase 2b Treatment Naïve and Treatment Experienced Ombitasvir + Paritaprevir + Ritonavir +/- Ribavirin in HCV GT4 PEARL-I Hézode C, et al. Lancet. 2015 March 30. [Epub ahead of print] PEARL-I: Study Design
Phase 2b Treatment Naïve and Treatment Experienced Ombitasvir + Paritaprevir + Ritonavir +/- Ribavirin in HCV GT4 PEARL-I Hézode C, et al. Lancet. 2015 March 30. [Epub ahead of print] PEARL-I: Study Design
Hepatitis C Virus Management
 Hepatitis C Virus Management FDA-Approved Medications Hepatitis C is caused by a virus and results in liver inflammation, which can lead to advanced liver disease and/or liver cancer. An estimated 3 to
Hepatitis C Virus Management FDA-Approved Medications Hepatitis C is caused by a virus and results in liver inflammation, which can lead to advanced liver disease and/or liver cancer. An estimated 3 to
IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE?
 IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE? Francesco Paolo Russo Department of Surgery, Oncology and Gastroenterology Multivisceral/ Gastroenterology Section University
IL TRAPIANTO DI FEGATO: QUALE FUTURO CON LE NUOVE TERAPIE PER LE MALATTIE EPATICHE? Francesco Paolo Russo Department of Surgery, Oncology and Gastroenterology Multivisceral/ Gastroenterology Section University
Dr Janice Main Imperial College Healthcare NHS Trust, London
 BHIVA AUTUMN CONFERENCE 2014 Including CHIA Parallel Sessions Dr Janice Main Imperial College Healthcare NHS Trust, London 9-10 October 2014, Queen Elizabeth II Conference Centre, London BHIVA AUTUMN CONFERENCE
BHIVA AUTUMN CONFERENCE 2014 Including CHIA Parallel Sessions Dr Janice Main Imperial College Healthcare NHS Trust, London 9-10 October 2014, Queen Elizabeth II Conference Centre, London BHIVA AUTUMN CONFERENCE
Treatment of HCV Genotype 4
 Hepatitis C Online PDF created August 26, 2018, 11:55 pm Treatment of HCV Genotype 4 This is a PDF version of the following document: Module 5: Treatment of Chronic Hepatitis C Infection Lesson 4: Treatment
Hepatitis C Online PDF created August 26, 2018, 11:55 pm Treatment of HCV Genotype 4 This is a PDF version of the following document: Module 5: Treatment of Chronic Hepatitis C Infection Lesson 4: Treatment
Addressing Unmet Medical Needs in HCV Genotype 3
 Addressing Unmet Medical Needs in HCV Genotype 3 Karen Doucette, MD, MSc (Epi), FRCPC Associate Professor, Division of Infectious Diseases, Department of Medicine University of Alberta Objectives Identify
Addressing Unmet Medical Needs in HCV Genotype 3 Karen Doucette, MD, MSc (Epi), FRCPC Associate Professor, Division of Infectious Diseases, Department of Medicine University of Alberta Objectives Identify
Next generation DAAs: Combining efficacy and safety profile. Jiannis Vlachogiannakos
 Next generation DAAs: Combining efficacy and safety profile. Jiannis Vlachogiannakos Associate Professor of Gastroenterology, Academic Department of Gastroenterology, National and Kapodistrian University
Next generation DAAs: Combining efficacy and safety profile. Jiannis Vlachogiannakos Associate Professor of Gastroenterology, Academic Department of Gastroenterology, National and Kapodistrian University
Treating now vs. post transplant
 Resistance with treatment failure Treating now vs. post transplant Pros (for treating pre transplant) If SVR efficacy means Better quality of life Removal from waiting list No post transplant recurrence
Resistance with treatment failure Treating now vs. post transplant Pros (for treating pre transplant) If SVR efficacy means Better quality of life Removal from waiting list No post transplant recurrence
Highlights of AASLD 2012 CCO Official Conference Coverage of the 2012 Annual Meeting of the American Association for the Study of Liver Diseases
 Highlights of AASLD 12 CCO Official Conference Coverage of the 12 Annual Meeting of the American Association for the Study of Liver Diseases November 9-13, 12 Boston, Massachusetts In partnership with
Highlights of AASLD 12 CCO Official Conference Coverage of the 12 Annual Meeting of the American Association for the Study of Liver Diseases November 9-13, 12 Boston, Massachusetts In partnership with
5/10/2016. Management of Hepatitis C Virus Genotype 1 and 4 Treatment-Naive and Treatment-Experienced Patients. HCV life-cycle and antiviral targets
 5/1/216 Management of Hepatitis C Virus Genotype 1 and 4 Treatment-Naive and Treatment-Experienced Patients David L. Wyles, MD Associate Professor of Medicine University of California San Diego La Jolla,
5/1/216 Management of Hepatitis C Virus Genotype 1 and 4 Treatment-Naive and Treatment-Experienced Patients David L. Wyles, MD Associate Professor of Medicine University of California San Diego La Jolla,
New developments in HCV research and their implications for front-line practice
 New developments in HCV research and their implications for front-line practice Dr. Curtis Cooper Associate Professor, University of Ottawa Director, Ottawa Hospital Viral Hepatitis Program June 17, 2013
New developments in HCV research and their implications for front-line practice Dr. Curtis Cooper Associate Professor, University of Ottawa Director, Ottawa Hospital Viral Hepatitis Program June 17, 2013
Introduction. The ELECTRON Trial
 63rd AASLD November 9-13, 12 Boston, Massachusetts Faculty Douglas T. Dieterich, MD Professor of Medicine and Director of CME Department of Medicine Director of Outpatient Hepatology Division of Liver
63rd AASLD November 9-13, 12 Boston, Massachusetts Faculty Douglas T. Dieterich, MD Professor of Medicine and Director of CME Department of Medicine Director of Outpatient Hepatology Division of Liver
Treatment of genotype 4 patient. with cirrhosis. Vincent LEROY Clinique Universitaire d Hépato-Gastroentérologie INSERM U823 CHU de Grenoble
 Treatment of genotype 4 patient with cirrhosis Vincent LEROY Clinique Universitaire d Hépato-Gastroentérologie INSERM U823 CHU de Grenoble Clinical case 52 year-old patient Intra-venous drug user 1987-1989
Treatment of genotype 4 patient with cirrhosis Vincent LEROY Clinique Universitaire d Hépato-Gastroentérologie INSERM U823 CHU de Grenoble Clinical case 52 year-old patient Intra-venous drug user 1987-1989
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD
 Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD") Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
Direct-acting Antiviral (DAA) Regimens in Late-stage Development: Which Patients Should Wait? Fred Poordad, MD The HCV Lifecycle: Multiple Targets Polymerase Inhibitors Protease Inhibitors NS5A Inhibitors
Program Disclosure. Provider is approved by the California Board of Registered Nursing, Provider #13664, for 1.5 contact hours.
 Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
Program Disclosure This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint-sponsorship
Hepatitis C Virus: HIV/Hepatitis C Coinfection Wednesday, August 24, 2016
 Hepatitis C Virus: HIV/Hepatitis C Coinfection Debika Bhattacharya, MD, MSc Associate Clinical Professor University of California Los Angeles Los Angeles, California Washington, DC: August 24, 2016 Slide
Hepatitis C Virus: HIV/Hepatitis C Coinfection Debika Bhattacharya, MD, MSc Associate Clinical Professor University of California Los Angeles Los Angeles, California Washington, DC: August 24, 2016 Slide
Treating HCV Genotype 2 & 3
 Treating HCV Genotype 2 & 3 3rd Workshop on HCV Therapy Advances, Rome 14.12.2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Frankfurt am Main, Germany HCV Genotypes 2 & 3 Laurel and Hardy
Treating HCV Genotype 2 & 3 3rd Workshop on HCV Therapy Advances, Rome 14.12.2013 Christoph Sarrazin Klinikum der J. W. Goethe-Universität Frankfurt am Main, Germany HCV Genotypes 2 & 3 Laurel and Hardy
Clinical Management: Treatment of HCV Mono-infection
 Clinical Management: Treatment of HCV Mono-infection Curtis Cooper, MD, FRCPC Associate Professor-University of Ottawa The Ottawa Hospital- Infections Diseases Viral Hepatitis Program- Director Industry
Clinical Management: Treatment of HCV Mono-infection Curtis Cooper, MD, FRCPC Associate Professor-University of Ottawa The Ottawa Hospital- Infections Diseases Viral Hepatitis Program- Director Industry
Update on Real-World Experience With HARVONI
 Update on Real-World Experience With A RESOURCE FOR PAYERS MAY 217 This information is intended for payers only. The HCV-TARGET study was supported by Gilead Sciences, Inc. Real-world experience data were
Update on Real-World Experience With A RESOURCE FOR PAYERS MAY 217 This information is intended for payers only. The HCV-TARGET study was supported by Gilead Sciences, Inc. Real-world experience data were
HCV Update from AASLD 2016
 HCV Update from AASLD 2016 Ahmed Elsharkawy Consultant Hepatologist QE Birmingham Secretary and Chair-Elect of BVHG BHIVA/BVHG Feedback Meeting November 2016 Speaker Name Ahmed Elsharkawy Statement Speaking
HCV Update from AASLD 2016 Ahmed Elsharkawy Consultant Hepatologist QE Birmingham Secretary and Chair-Elect of BVHG BHIVA/BVHG Feedback Meeting November 2016 Speaker Name Ahmed Elsharkawy Statement Speaking
Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2)
") Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2) PegIFN and RBV remain vital components of HCV therapy-- selected presentations from: Program Disclosure This activity has been planned and
Emerging Therapies for HCV: Highlights from AASLD 2012 (Part 2) PegIFN and RBV remain vital components of HCV therapy-- selected presentations from: Program Disclosure This activity has been planned and
Baseline and acquired viral resistance to DAAs: how to test and manage
 Baseline and acquired viral resistance to DAAs: how to test and manage Round table discussion by Marc Bourliere, Robert Flisiak, Vasily Isakov, Mark Sulkowsky & Konstantin Zhdanov Prevalence of baseline
Baseline and acquired viral resistance to DAAs: how to test and manage Round table discussion by Marc Bourliere, Robert Flisiak, Vasily Isakov, Mark Sulkowsky & Konstantin Zhdanov Prevalence of baseline
47 th Annual Meeting AISF
 47 th Annual Meeting AISF Rome, 21 February 2014 Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations (HCV/HIV coinfection, advanced cirrhosis,
47 th Annual Meeting AISF Rome, 21 February 2014 Present and future treatment strategies for patients with HCV infection: chronic hepatitis and special populations (HCV/HIV coinfection, advanced cirrhosis,
HCV Treatment in 2016
 HCV Treatment in 2016 Hugo E. Vargas, MD Professor of Medicine Mayo College of Medicine Medical Director, Clinical Trials Office Vice Chair, Department of Research Educational Goals Caveats: Cannot cover
HCV Treatment in 2016 Hugo E. Vargas, MD Professor of Medicine Mayo College of Medicine Medical Director, Clinical Trials Office Vice Chair, Department of Research Educational Goals Caveats: Cannot cover