SCIENTIFIC 9PROGRAMME... 9 INVITED SPEAKERS ABSTRACTS...
|
|
|
- Katherine Holland
- 6 years ago
- Views:
Transcription

1
2 Contents SCIENTIFIC 9PROGRAMME... 9 INVITED SPEAKERS ABSTRACTS... 2 Immunotherapy in HCC and the hepatologist what does the future multidisciplinary team look like? Genomic diversity in HCC: the TCGA experience Mutational signatures in HCC resulting from exogenous and endogenous exposure From tumour diversity to individualised management: What is different about NAFLD-HCC? Debate: DAA treatment of cirrhotic HCV infected patients with HCC con Liver polyploidy: a good guy or a bad guy Diagnostic and prognostic role of circulating microparticles in hepatobiliary cancers Extent of intratumoral genomic diversity Telomerase activation WNT/ß-catenin activation Epigenetic targets in hepatocarcinogenesis The Hippo/YAP signalling pathway in liver tumor initiation and progression Is there a role for Contrast Enhanced Ultra Sound (CEUS) for improving the diagnostic accuracy of imaging techniques? The hepatologist view How to best diagnose HCC? Do we need hepatobiliary MR contrast agents? The radiologist view 38 Is biopsy adding clinically relevant information? The pathologist view What is the role of biomarkers in diagnosis, prognosis and surveillance? Development of tumor markers for diagnosis, prognosis and tumor response prediction Clinical scores - What is their added value? Locoregional therapies in HCC: Ablation, transarterial therapies or combination of boths Liver transplantation for HCC: How to optimize patient selection? Update of the EASL Clinical Practice Guideline on management of hepatocellular carcinoma Advanced HCC: A multidisciplinary approach - Tumour board #3: Clinical case presentation... 5 Approved systemic treatments for HCC: Which is the best treatment approach? Assessment of systemic treatment activity by imaging Inflammation in liver tumorigenesis: Potential targets for immunotherapy Role of immunology in HCC development and progression Patient-derived models for drug discovery in liver cancer eposter ABSTRACT PRESENTATIONS P0-0RANDOMIZED TRIAL OF PREOPERATIVE ADMINISTRATION OF ORAL PREGABALIN FOR POSTOPERAIVE ANALGESIA IN PATIENTS SCHEDULED FOR RADIOFREQUENCY ABLATION OF FOCAL LESIONS IN THE LIVER P0-02 MIRNA PROFILE AS A PROGNOSTIC BIOMARKER FOR HEPATOCELLULAR CARCINOMA DEVELOPMENT P0-03 IMPACT OF BCLC TREATMENT STAGE MIGRATION IN THE SURVIVAL OF PATIENTS WITH HEPATOCELLULAR CARCINOMA
3 P0-04YI RIP3-DEPENDENT SIGNALLING CONTRIBUTES TO NON-ALCOHOLIC FATTY LIVER DISEASE-RELATED CARCIONOGENESIS P0-05 THE BIOMARKER POTENTIAL OF KI67 AND PH2AXIMMUNOHISTOCHEMISTRY IN GUIDING USE OF THE LIVER-TARGETING NUCLEOTIDE MIV-88 INPATIENTS WITH HEPATOCELLULAR CARCINOMA P0-06YI SARCOPENIA PREDICTSSURVIVAL IN PATIENTS WITH ADVANCED HEPATOCELLULAR CARCINOMA TREATED WITHSORAFENIB P0-07YI RAPAMYCIN AND ZOLEDRONIC ACID STRONGLY INHIBIT GROWTH OF ADVANCED MURINE HEPATOCELLULAR CARCINOMA VIA ACTIVATION OF INNATE AND ADOPTIVE IMMUNITY P0-08YI ZOLEDRONIC ACID SUPPRESSES TUMOUR ASSOCIATED MACROPHAGES AND MYELOID DERIVED SUPPRESSOR CELLS IN MURINE HCC P0-0 DISTINCT FUNCTIONS OF AP- (FOS/JUN) DIMERS IN LIVER CANCER P0-YI LIVER CANCER, NOT ETIOLOGY OR STEATOSIS OR FIBROSIS, IS THE ONLY INDEPENDENT PREDICTOROF ELEVATED PERIOSTIN CONCENTRATION AMONG CAUCASIAN PATIENTS WITH LIVER DISEASE P02-0YI HEPATOCELLULAR CARCINOMA INAUGURATING CIRRHOSIS: A DESCRIPTIVE STUDY P02-02YI PRESENCE OF HCC DOES NOT AFFECT THE COURSE AND RESPONSE TO ANTICOAGULATION OF BLAND NON MALIGNANT PORTAL VEIN THROMBOSIS IN CIRRHOTIC PATIENTS... 7 P02-03 SEROLOGICAL DIAGNOSIS OF EARLY HCC IN NASH: A GERMAN MULTICENTER STUDY P02-04 LIVER TARGETING AND ANTI-TUMOUR EFFICACY OF THE NUCLEOTIDE PRODRUG MIV-88 IN NONCLINICAL MODELS OF HEPATOCELLULAR CARCINOMA P02-05YI ASSOCIATION OF ANG, ANG2 AND FGF GENETIC POLYMORPHISM AND THEIR EXPRESSION ANALYSIS IN HEPATOCELLULAR CARCINOMA P02-06YI LIQUID CRYSTALLINE NANOPARTICLES (LCNPS) BASED DELIVERY OF AN ANTICANCER BIOACTIVE, METHOTREXATE P02-08YI EVALUATION OF PROGNOSTIC FACTORS OF OVERALL SURVIVAL AND PROGRESSION-FREE SURVIVAL IN PATIENTS WITH HEPATOCELLULAR CARCINOMA P02-09YI ANTI-INFLAMMATORY POLARIZATION OF TUMOR ASSOCIATED MACROPHAGES PROMOTING TUMOR GROWTH AND ANGIOGENESIS IN HCC OF CHEMOKINE RECEPTOR CXCR3 DEFICIENT MICE P02-0 HAND FOOT SKIN REACTION AND OVERALL SURVIVAL IN THE PHASE 3 RESORCE TRIAL OF REGORAFENIB FOR TREATMENT OF HEPATOCELLULAR CARCINOMA PROGRESSING ON SORAFENIB P02- INTRA-TUMORAL TERTIARY LYMPHOID STRUCTURES ARE ASSOCIATED WITH A LOW RISK OF EARLY TUMOR RECURRENCE IN PATIENTS WITH HEPATOCELLULAR CARCINOMA... 8 P02-2 HEPAVAC-0 FIRST-IN-MAN THERAPEUTIC CANCER VACCINE PHASE I/II CLINICAL TRIAL FOR HEPATOCELLULAR CARCINOMA PATIENTS P03-0YI GENOMIC EXPRESSION ANALYSIS OF INFILTRATING NATURAL KILLER CELLS SUGGESTS A MIGRATION DEFECT INTO THE TUMOR MICROENVIRONMENT P03-02 GLYCOLYTIC ENZYMES PKM2 AND PGK ARE INSTRUMENTAL TO DNA DAMAGE PROTEIN CHK2 IN SUSTAINING GENOMIC INSTABILITY IN HEPATOCELLUAR CARCINOMA P03-03YI IMMUNE INFLAMMATION INDICATORS AND ALBI SCORE TO PREDICT OCCURRENCE AND RECURRENCE OF HEPATOCELLULAR CARCINOMA IN HCV-RELATED CIRRHOSIS TREATED WITH DIRECT-ACTING ANTIVIRALS
4 P03-04YI EPIGENETIC CONTROL OF HEPATIC HOMEOSTASIS P03-05YI PATIENT-DERIVED LIVER CANCER CELL LINES IN PERSONALIZED TREATMENT APPROACH: FROM PHENOTYPIC AND MOLECULAR CHARACTERIZATION TO THERAPEUTIC TARGET IDENTIFICATION P03-06YI DEVELOPMENT OF SLN AS CARRIERS FOR DELIVERY OF HEPATITIS B FOR VACCINATION USING SUBCUTANEOUS ROUTE P03-07 PONCIRUS FRUCTUS INHIBITED THE PROLIFERATION AND INDUCEDTHE APOPTOSIS IN HEPATOCELLULAR CARCINOMA BY THE DOWN-REGULATION OF NF-ΚB.. 90 P03-08 A LARGE SET OF MIRNAS IS DEREGULATED SINCE THE EARLIEST STEPS OF HUMAN HCC DEVELOPMENT... 9 P03-09YI CYTOTOXIC T LYMPHOCYTES (TC) AND REGULATORY T CELLS (TREG) PREDICT THE DEVELOPMENT OF DERMATOLOGIC ADVERSE EFFECTS IN PATIENTS WITH HEPATOCELLULAR CARCINOMA TREATED WITH SORAFENIB P03-0 A HIGH ALPHA-FETOPROTEIN SLOPE PRIOR TO THERAPY CORRELATES WITH POOR SURVIVAL OF PATIENTS WITH HEPATOCELLULAR CARCINOMAS P03- MACROTRABECULAR-MASSIVE HEPATOCELLULAR CARCINOMA: A DISTINCTIVE HISTOLOGICAL SUBTYPE WITH CLINICAL RELEVANCE P03-2YI MACROPHAGE MIGRATION INHIBITORY FACTOR IS UPREGULATED IN MURINE HEPATOCELLULAR TUMOR TISSUE AND EXERTS PRO-PROLIFERATIVE AND ANTI- APOPTOTIC EFFECTS ON HEPATOMA CELLS IN VITRO P04-0 INCIDENCE AND PREDICTORS OF DE-NOVO HEPATOCELLULAR CARCINOMA IN HCV CIRRHOTIC PATIENTS TREATED WITH DIRECT-ACTING ANTIVIRALS: A SINGLE- CENTER PROSPECTIVE 3 YEAR STUDY P04-02YI METRONOMIC CAPECITABINE VS. BEST SUPPORTIVE CARE IN CHILD-PUGH B HEPATOCELLULAR CARCINOMA: A PROOF OF CONCEPT P04-03YI EFFICACY OF RADIOFREQUENCY IN PATIENTS WITH HEPATOCELLULAR CARCINOMA: META-ANALYSIS P04-04 PHENOTYPICAL AND MOLECULAR CHANGES IN NODULE IN NODULE HEPATOCELLULAR CARCINOMA WITH PATHOGENETIC IMPLICATIONS P04-05YI SYSTEMATIC REVIEW AND METANALYSIS ESTABLISH DERMATOLOGY ADVERSE EVENTS AS A POSITIVE PREDICTOR OF SURVIVAL IN HEPATOCELLULAR CARCINOMA PATIENTS TREATED WITH SORAFENIB... 0 P04-06YI DOXORUBICIN AND HYPOXIA TREATMENT OF HCC CELL LINES: CELL VIABILITY AND ONCOLOGIC PROTEIN PROFILE P04-07 PRESENCE OF HCC AND BCLC STAGE SIGNIFICANTLY INFLUENCE SOLUBLE FIBRINOGEN-LIKE PROTEIN 2 (SFGL-2) IN CIRRHOTIC PATIENTS P04-08YI RETROSPECTIVE OBSERVATIONAL STUDY OF CHARACTERISTICS OF HCC PATIENTS FROM EGYPT AND IMPACT OF SURVEILLANCE ON IMPROVING THEIR OUTCOMES P04-09YI MODIFICATION OF THE ALBI-T SCORE: NEW PROGNOSTIC MODEL FOR PATIENTS WITH HEPATOCELLULAR CARCINOMA P04-0YI DYNAMIC SURVIVAL ANALYSIS OF THE DATA FROM THE NATIONAL SURVEY OF HCC AND LIVER TRANSPLANT IN BRAZIL P04-YI ASSESSMENT OF HYPOTHYROIDISM AS A MARKER OF RESPONSE TO SORAFENIB IN PATIENTS WITH HEPATOCELLULAR CARCINOMA. SYMPTOMS MAKE THE DIFFERENCE P04-2YI EFFICACY AND SAFETY OF REGORAFENIB IN CLINICAL PRACTICE IN THE TREATMENT OF HEPATOCELLULAR CARCINOMA. MULTICENTRE EXPERIENCE
5 P05-0 TLL POLYMORPHISM DO NOT PREDICT THE DEVELOPMENT OF DE-NOVO HEPATOCELLULAR CARCINOMA IN HCV CIRRHOTICS TREATED WITH IFN-FREE DAA- BASED REGIMENS P05-02YI DYSREGULATION OF THE LYSOSOMAL COMPARTMENT WITH VERTEPORFIN POTENTIATES THE ANTI-TUMOR EFFECT OF SORAFENIB IN HEPATOCELLULAR CARCINOMA... 0 P05-03YI NON ADHERENCE TO AASLD-EASL GUIDELINES FOR THE MANAGEMENT OF HEPATOCELLULAR CARCINOMA DOES NOT TRANSLATE INTO WORSE OUTCOMES... P05-04YI MALDI IMAGING OF HEPATOCHOLANGIOCARCINOMAS: A CLUE TO TACKLE TUMOR HETEROGENEITY. PRELIMINARY RESULTS P05-05YI HYPERBILIRUBINEMIA IS A FALLACIOUS PARAMETER TO DETECT LIVER TOXICITY IN PATIENTS WITH HEPATOCELLULAR CARCINOMA TREATED WITH SORAFENIB AND MAY LEAD TO INADEQUATE TREATMENT INTERRUPTION... 3 P05-06YI HCC RECURRENCE AFTER DAA TREATMENT IN HCV PATIENTS P05-07YI SHORT-TERM RECURRENCE OF HEPATOCELLULAR CARCINOMA IN HCV INFECTED PATIENTS IS UNAFFECTED BY DIRECT ANTIVIRAL AGENTS THERAPY. A CASE- CONTROL, SINGLE CENTER STUDY P05-08YI ENDOPLASMIC RETICULUM STRESS IN HEPATIC STELLATE CELLS CONTRIBUTES TO THE PROGRESSION OF HEPATOCELLULAR CARCINOMA P05-09 COMPREHENSIVE EVALUATION OF THE ROLE OF RECEPTOR TYROSINE KINASE FAMILY IN HEPATOCELLULAR CARCINOGENESIS... 7 P05-0 PREDICTORS OF HEPATOCELLULAR RECURRENCE AFTER LIVER TRANSPLANT IN HEPATITIS C PATIENTS: A TEN-YEARS SINGLE CENTER COHORT... 9 P05- EARLY TREATMENT WITH SORAFENIB AND MTOR INHIBITOR IN RECURRENT HEPATOCELLULAR CARCINOMA AFTER LIVER TRANSPLANTATION: SAFETY AND SURVIVAL P05-2YI CHANGING CLINICAL PROFILE AND EPIDEMIOLOGY OF HEPATOCELLULAR CARCINOMA IN INDIA... 2 P06-0 GLOBAL PROTEIN ABERRATION SCORE (GLOPAS), A COMPREHENSIVE RISK SCORE TO PREDICT HEPATOCELLULAR CARCINOMA BIOLOGY AND ESTIMATE PATIENTS' SURVIVAL P06-02YI A NEW PROGNOSTIC SCORING SYSTEM FOR CIRRHOSIS AND HEPATOCELLULAR CARCINOMA UTILIZING CD44 RS875 GENE POLYMORPHISM P06-04 PRESENCE OF NON-HYPERVASCULAR HYPOINTENSE NODULE ON HEPATOBILIARY PHASE OF GADOXETIC-ACID ENHANCED MR: RISK OF TUMOR RECURRENCE AFTER CURATIVE TREATMENT FOR SMALL SINGLE NODULAR HCC AND GUIDANCE FOR SELECTION OF TREATMENT METHODS P06-05YI UP-REGULATION OF MIR-324 SUPPORTS PROLIFERATION OF HEPATOCELLULAR CARCINOMA CANCER CELLS AND CORRELATES WITH POOR PROGNOSIS OF HCC PATIENTS P06-06 RECURRENCE AND "DE NOVO" DIAGNOSIS OF HEPATOCELLULAR CARCINOMA AND OTHER NEOPLASMS IN PATIENTS WITH HEPATITIS C TREATED WITH DIRECT-ACTING ANTIVIRALS P06-07 CLINICAL AND GENETIC PREDICTORS OF HCC OCCURING IN CAUCASIAN COMPESATED HBV CIRRHOTICS TREATED BY ENTECAVIR OR TENOFOVIR FOR 8 YEARS P06-08YI ELEVATED CIRCULATING IMMATURE NEUTROPHILS PREDICTS POOR RESPONSE TO THERAPY, SHORTER TIME TO PROGRESSION AND POORER SURVIVAL IN PATIENTS WITH HEPATOCELLULAR CARCINOMA P06-09YI ANGPT2 POLYMORPHISMS AND CLINICAL OUTCOME IN ADVANCED HEPATOCELLULAR CARCINOMA PATIENTS RECEIVING SORAFENIB
6 P06-0 EXCELLENT 5 YEARS SURVIVAL FOR CIRRHOTIC PATIENTS DEVELOPING AN HEPATOCELLULAR CARCINOMA DURING LONG-TERM ORAL THERAPY FOR HBV... 3 P06-YI HCC PROGRESSION AND SURVIVAL FOLLOWING HCV ANTI-VIRAL THERAPY P06-2YI CONTRAST ENHANCED VERSUS CONVENTIONAL ULTRASOUND GUIDED LIVER BIOPSY IN THE DIAGNOSIS OF HEPATOCELLULAR CARCINOMA : A PROSPECTIVE STUDY P07-0YI DEPLETION OF ACTIVATED STROMAL FIBROBLASTS IN LIVER FIBROSIS - A PROMISING APPROACH TO PREVENT LIVER CANCER? P07-02YI SPHINGOLIPIDS: A FURTHER STEP INTO THE DETECTION OF EARLY AND ADVANCED HEPATOCELLULAR CARCINOMA P07-03YI THE ROLE OF INTERLEUKIN 6 SIGNALING PATHWAY IN CHOLANGIOCARCINOMA P07-04YI LIVER CANCER CELL LINES DISTINCTLY REFLECT THE METABOLIC GENE EXPRESSION PATTERN OBSERVED IN CLINICAL MICROARRAYS P07-05YI GENETIC INACTIVATION OF NRF2 PREVENTS CLONAL EXPANSION OF CARCINOGEN-INITIATED CELLS IN A NUTRITIONAL MODEL OF RAT HEPATOCARCINOGENESIS P07-06YI ACTIVATED PLATELETS CONTRIBUTE TO THE PROGRESSION OF HEPATOCELLULAR CARCINOMA BY ALTERING THE IMMUNE CELL ENVIRONMENT P07-07 THE COMBINATION OF PIVKA-II AND AFP LEVELS IMPROVES THE DIAGNOSTIC ACCURACY FOR THE DIAGNOSIS OF HCC DEVELOPING IN LONG-TERM NUC SUPPRESSED HBV CAUCASIAN CIRRHOTICS... 4 P07-08YI NEW INSIGHTS IN TRANSFORMING GROWTH FACTOR BETA SIGNALING PATHWAY ON TUMOR SUPPRESSION AND METASTATIC PROPERTIES IN PRIMARY LIVER CANCER P07-09 IN VIVO REACTIVATION OF THYROID HORMONE NUCLEAR RECEPTORS BY 3,5,3' TRIIODOTHYRONINE HAS A THERAPEUTIC POTENTIAL IN HEPATOCELLULAR CARCINOMA P07-0 COST-EFFECTIVE TARGETED SEQUENCING FOR HEPATOCELLULAR CARCINOMA MUTATIONAL SCREENING P07-YI INCREASED INTESTINAL PERMEABILITY AND INFLAMMATION ARE ASSOCIATED WITH HEPATOCELLULAR CARCINOMA IN PATIENTS WITH NAFLD-RELATED LIVER CIRRHOSIS P07-2 LINC0052 MAY FUNCTION AS A CERNA CORE COMPONENT IN HUMAN HEPATOCELLULAR CARCINOMA P08-0YI HEPATOCELLULAR CARCINOMA - HOW DOES BCLC SCORE INFLUENCE THERAPEUTIC DECISION? P08-02 CLINICAL SIGNIFICANCE OF TIME RELATED FLUCTUATIONS OF AFP AND PIVKA-II SERUM LEVELS IN PATIENTS WITH CIRRHOSIS UNDERGOING SURVEILLANCE FOR HEPATOCELLULAR CARCINOMA P08-03YI MIR-2 ABLATION PREVENTS NASH-ASSOCIATED HEPATOCELLULAR CARCINOMA P08-04 ROLE OF THE HES5/NOTCH SIGNALING PATHWAY IN LIVER CARCINOGENESIS.. 5 P08-05YI LONG NON-CODING RNA H9: A BIOMARKER OF HEPATOCELLULAR CARCINOMA P08-06YI INHIBITING THE P2Y2 RECEPTOR DECREASES TUMOUR CELL VIABILITY AND AFFECTS DIFFERENT CELL TYPES IN THE STROMA P08-07YI OVERCOMING HEAT-SINK IN PORTAL VEIN RELATED HEPATOCELLULAR CARCINOMAS WITH COMBINED RADIOFREQUENCY ABLATION AND PERCUTANEOUS ETHANOL INJECTION
7 P08-08 LONG-TERM SORAFENIB TREATMENT IN A LARGE COHORT OF HCC PATIENTS: A MULTI CENTER STUDY P08-09YI FACTORS ASSOCIATED WITH OCCURRENCE/RECURRENCE OFHEPATOCELLULAR CARCINOMA EARLY AFTER TREATMENT OF HEPATITIS C WITH DIRECTANTIVIRAL AGENTS P08-0YI SERUM ENDOGLIN (CD05) AS A POTENTIAL MARKER FOR HEPATOCELLULAR CARCINOMA IN CIRRHOTIC HEPATITIS C VIRUS AND HEPATITIS B VIRUS PATIENTS P08-YI IMPACT OF REGORAFENIB IN THE CLINICAL PRACTICE AND IDENTIFICATION OF SECOND-LINE TREATMENT ORPHAN PATIENTS P09-0YI CONTRAST-ENHANCED ULTRASOUND FOR NON-INVASIVE DIAGNOSIS OF HEPATOCELLULAR CARCINOMA: A COMPARISON BETWEEN CEUS LI-RADS AND ESCULAP CRITERIA IN A LARGE HIGH-RISK COHORT OF PATIENTS P09-02YI REGORAFENIB AFTER PROGRESSION ON SORAFENIB FOR ADVANCED HCC.. 6 P09-03YI PREDICTORS OF RECURRENCE AND SURVIVAL OF HEPATOCELLULAR CARCINOMA: PROSPECTIVE STUDY INCLUDING TRANSIENT ELASTOGRAPHY AND CANCER STEM CELL MARKERS P09-04YI EPITHELIAL-TO-MESENCHYMAL TRANSITION INDUCED DRUG RESISTANCE IN HEPATOCELLULAR CARCINOMA DERIVED CANCER STEM CELLS P09-05YI S00A IS PART OF A WHOLE NETWORK OF TUMOR SUPPRESSORS AND ONCOGENES DEREGULATED EARLY WITH HEPATIC STEATOSIS AND CONTRIBUTING TO HEPATOCELLULAR CARCINOMA DEVELOPMENT P09-06YI EVALUATION OF THE SINGLE AND MULTIPLE NATURAL RASS PREVALENCE IN THE MAIN HCV GENOTYPES IN ITALIAN COURT P09-07 PROGNOSTIC EFFECT OF YTTRIUM-90 RADIOEMBOLIZATION FOR HEPATOCELLULAR CARCINOMA WITH PORTAL VEIN INVASION P09-08YI EARLY DETECTION OF HEPATOCELLULAR CARCINOMA IN CIRRHOTIC LIVER MODEL IN MRI USING IRON DOPED NANO-CALCIUM PHOSPHATE CONTRAST AGENT P09-0YI DISSECTING THE SPATIAL HETEROGENEITY OF CIRCULATING TUMOR CELLS REVEALS CCL5-TREG MEDIATED IMMUNE EVASION IN HEPATOCELLULAR CARCINOMA 70 P09-YI IMPACT OF REGORAFENIB IN THE CLINICAL PRACTICE AND IDENTIFICATION OF THE SECOND-LINE TREATMENT ORPHAN PATIENTS... 7 P09-2 IFN-FREE DAA TREATMENT OF CIRRHOTIC HCV PATIENTS WITH OR WITHOUT HISTORY OF HCC: A MULTICENTER PROSPECTIVE TRIAL IN ITALY P0-0 SUPERIORITY OF MULTIPLE RANDOM GENE SETS IN PREDICTING SURVIVAL OF PATIENTS WITH HEPATOCELLULAR CARCINOMA P0-02 CLINICALFEATURES OF HEPATOCELLULAR CARCINOMA IN THE ELDERLY IN A HEPATITIS B ENDEMICCOUNTRY - A COMPARATIVE STUDY OF 430 CASES P0-03YI PREDICTION OF HEPATOCELLULAR CARCINOMA USING NON INVASIVE BIOMARKERS OF LIVER FIBROSIS: A RETROSPECTIVE STUDY OF 2363 PATIENTS P0-04 PERCUTANEOUS ELECTROCHEMOTHERAPY OF HEPATOCELLULAR CARCINOMA AT HEPATICHILUM P0-05YI GP38+ HEPATIC PROGENITOR CELL-DERIVED EXTRACELLULAR VESICLES IN HCC AND BILIARY CANCER - A NOVEL LIQUID BIOPSY MARKER? P0-06YI UBIQUITIN CARBOXY-TERMINAL HYDROLASE L INHIBITION AS A POTENTIAL STRATEGY TO MODULATE THE SORAFENIB RESPONSE OF HEPATOCELLULAR CARCINOMA P0-07YI LARGE UNRESECTABLE HEPATOCELLULAR CARCINOMA: EFFICACY OF PERCUTANEOUS THERMAL ABLATION AFTER OCCLUSION OF TUMOR BLOOD SUPPLY BY GELFOAM
8 P0-08 THE MELD SCORE IS POSITIVELY CORRELATED WITH NEUTROPHIL TO LYMPHOCYTE RATIO AND RED BLOOD CELL DISTRIBUTION IN ASSESSMENT OF MORTALITY NAS RECURRENCE IN PATIENTS WITH HEPATOCELLULAR CARCINOMA AFTER LIVING DONOR LIVER TRANSPLANTATION P0-09 YAP DRIVES CHROMOSOMAL INSTABILITY IN HCC PATIENTS,WHICH CORRELATES WITH CLINICAL AND MOLECULAR PATIENT FEATURES P0-0 PORTAL VEIN TUMOR THROMBOSIS HAS A DIRECT IMPACT ON LIVER FUNCTION P0-YI REGISTRATION OF COMPLETE RESPONSE TO CHEMOEMBOLIZATION AT 2 AND 6 MONTHS AVOIDS >0% OF FOLLOW-UP ANGIOGRAPHIES AND PERMITS AN EFFECTIVE TRANSITION INTO SYSTEMIC THERAPY UPON PROGRESSION, THUS ENSURING OPTIMAL SURVIVAL P0-2 CHANGES OF AFP AND PIVKA-II LEVELS DURING DAA TREATMENT AND THEIR PREDICTIVE VALUE FOR EARLY DIAGNOSIS OF HCC IN HCV CIRRHOTIC PATIENTS WITH SVR TO DAA TREATMENT P-0 HEPAMINE - A LIVER DISEASE MICROARRAY DATABASE, VISUALIZATION PLATFORM AND DATA-MINING RESOURCE P-02YI CHARACTERIZATION OF HBV INTEGRATION LANDSCAPE IN TUMOR AND NON- TUMOR LIVER TISSUES BY A HIGH-THROUGHPUT VIRAL INTEGRATION DETECTION APPROACH P-03YI ROLE OF SERUM AMYLOID A AND LONG NON-CODING RNA AF AS DIAGNOSTIC BIOMARKERS FOR HEPATITIS B AND C RELATED HEPATOCELLULAR CARCINOMA P-04YI EXOSOME-TRANSMITTED CIRCRNA_04797 SUSTAINS SORAFENIB RESISTANCE IN HEPATOCELLULAR CARCINOMA P-05 CHEMO-PREVENTIVE AND ANTI-TUMOR EFFECTS OF BENZYL ISOTHIOCYNATE ON HCC MODELS: A POSSIBLE CROSSTALK BETWEEN HGF/PAKT/STAT3 PATHWAY AND VEGF P-06YI PROGNOSTIC SCORES FOR SORAFENIB-TREATED HEPATOCELLULAR CARCINOMA PATIENTS: A VALIDATION STUDY OF THE HAP AND SAP SCORES P-07YI COMBINED TARGETING OF THE PPMD/WIP AND MDM2 NEGATIVE FEEDBACK SUPPRESSORS OF P53 IN TP53 WILD-TYPE HUMAN LIVER CANCER CELLS P-08YI CLINICAL CORRELATES OF THE GENETIC VARIABILITY OF THE CD274 GENE (PROGRAMMEDCELL DEATH-LIGAND ) AMONG PATIENTS WITH HEPATOCELLULAR CARCINOMA P-09 A SPECIFIC ECM COMPOSITION REGULATES SMAD - DEPENDENT - TGFBETA- INDUCED EMT RESPONSE IN HEPG2 CELLS ENGINEERED IN CIRRHOTIC AND HEALTHY HUMAN LIVER 3D SCAFFOLDS P-0YI HEPATOCELLULAR CARCINOMA AS A COMPLICATION OF VASCULAR DISEASE OF THE LIVER AFTER FONTAN PROCEDURE P-YI OUTCOMES OF SINGLE OR SEQUENTIAL DUAL MODALITY LOCO-REGIONAL THERAPIES IN HEPATOCELLULAR CARCINOMA P-2 MULTIMODAL AND SEQUENTIAL TREATMENTE FOR HEPATOCELLULAR CARCINOMA: HOW "REAL-LIFE" COMPLIES WITH INTERNATIONAL RECOMMENDATIONS 206 ACKNOWLEDGEMENTS INDUSTRY INDUSTRY SATELLITE SYMPOSIA COMPANY PROFILES
9 SCIENTIFIC PROGRAMME 9
10 SCIENTIFIC ORGANISING COMMITTEE Alejandro Forner, Spain Peter Galle, Germany Jessica Zucman-Rossi, France Thursday March 208 Welcome and Introduction Alejandro FORNER, Spain Peter GALLE, Germany HCC in 208: Which are the pressing issues? Chairs: Alejandro FORNER, Spain Peter GALLE, Germany 5:5-5:45 The changing epidemiology of HCC how do we identify and screen patients at risk? Jean-François DUFOUR, Switzerland 5:45-6:5 Tumour biology stroma immune cells where are the best targets? Jessica ZUCMAN-ROSSI, France 6:5-6:45 Immunotherapy in HCC and the hepatologist what does the future multidisciplinary team look like? Jordi BRUIX, Spain From tumour diversity to individualised management Chairs: Matías AVILA, Spain Massimo COLOMBO, Italy 7:5-7:45 Genomic diversity in HCC: the TCGA experience Lewis ROBERTS, United States 7:45-8:5 Mutational signatures in HCC resulting from exogenous and endogenous exposure Eric LETOUZÉ, France 8:5-8:45 What is unique about fatty-liver-associated HCC? Helen Louise REEVES, United Kingdom 8:45-8:55 Debate: DAA treatment of cirrhotic HCV infected patients with HCC: Pro Antonio CRAXI, Italy 8:55-9:05 Debate: DAA treatment of cirrhotic HCV infected patients with HCC: Cons Sabela LENS, Spain 9:05-9:5 Debate: DAA treatment of cirrhotic HCV infected patients with HCC: Discussion Friday 2 March 208 Intratumoural heterogeneity and mechanisms of therapy resistance Chairs: Helen Louise REEVES, United Kingdom Jessica ZUCMAN-ROSSI, France 08:00-08:30 Polyploide and prognostic role of circulating microparticles in hepatobiliary cancers Chantal DESDOUETS, France 08:30-09:00 Diagnostic and prognostic role of circulating microparticles in hepatobiliary cancers Miroslaw KORNEK, Germany 09:00-09:30 Liquid biopsy for patient management: lesson from colon cancer Pierre LAURENT-PUIG, France 0
11 09:30-0:00 Extent of intratumoural genomic diversity Augusto VILLANUEVA, United States From molecular defects to new targeted therapies in HCC Chairs: Josep M. LLOVET, United States Tom LÜDDE, Germany 0:30-0:50 Telomerase activation Jean Charles NAULT, France 0:50 - :0 WNT/ß-catenin activation Sabine COLNOT, France :0 - :0 Epigenetic targets in hepatocarcinogenesis Matías AVILA, Spain :0 - :30 The Hippo/YAP signalling pathway in liver tumour initiation and progression Kai BREUHAHN, Germany :30 - :50 FGF axis and FGFR inhibitors :50-2:0 ROUNDTABLE Translatability of results from animal models Early diagnostis of HCC: Which is the best strategy? Chairs: Fabio PISCAGLIA, Italy Maxime RONOT, France 3:30-3:40 Tumour board #: Clinical case presentation Maxime RONOT, France 3:40-4:00 Is there a role for Contrast Enhanced Ultra Sound (CEUS) for improving the diagnostic accuracy of imaging techniques? The hepatologist view Fabio PISCAGLIA, Italy 4:00-4:20 How to best diagnose HCC? Do we need hepatobiliary MR contrast agents? The radiologist view Christophe AUBÉ, France 4:20-4:40 Is biopsy adding clinically relevant information? The pathologist view Valérie PARADIS, France 4:40-5:00 Tumuor board #: Clinical case discussion Scores and biomarkers Chairs: Philip JOHNSON, United Kingdom Franco TREVISANI, Italy 5:00-5:20 What is the role of biomarkers in diagnosis, prognosis and surveillance? Franco TREVISANI, Italy 5:20-5:50 Development of tumour makers for diagnosis, prognosis and tumour response prediction Josep M. LLOVET, United States 5:50-6:0 What is the added value of clinical scoring systems? Philip JOHNSON, United Kingdom 6:0-6:30 Roundtable discussion: How we can improve the current staging systems? Curative treatment of HCC: A multidicsciplinary management Chairs: Pietro MAJNO, Switzerland Vincenzo MAZZAFERRO, Italy 7:00-7:0 Tumour board #2: Clinical case presentation Pietro MAJNO, Switzerland 7:0-7:40 Expanding boundaries of surgical resection in HCC Pietro MAJNO, Switzerland 7:40-8:0 Locoregional therapies in HCC: Ablation, transarterial therapies or combination of boths
12 Rita GOLFIERI, Italy 8:0-8:40 Liver transplantation how to optimize patient selection? Vincenzo MAZZAFERRO, Italy 8:40-9:00 Tumour board #2: Clinical case discussion Saturday 3 March 208 Introduction Current Status of the EASL Clinical Practice Guidelines on HCC 08:00-08:20 Peter GALLE, Germany Advanced HCC: A multidisciplinary approach Chairs: Jens RICKE, Germany Bruno SANGRO, Spain 08:20-08:30 Tumour board #3: Clinical case presentation Marcus-Alexander WÖRNS, Germany 08:30-09:00 Approved systemic treatments for HCC: Which is the best treatment approach? Maria REIG, Spain 09:00-09:30 Transarterial radioembolization: Role in the treatment of HCC Jens RICKE, Germany 09:30-09:50 Assessment of systemic treatment activity by imaging Maxime RONOT, France 09:50-0:00 Tumour board #3: Clinical case discussion Immune system and HCC: Potential role of immunotherapy Chairs: Massimo COLOMBO, Italy Marcus-Alexander WÖRNS, Germany 0:30-0:50 Inflammation in liver tumorigenesis: Potential targets for immunotherapy Eli PIKARSKY, Israel 0:50 - :0 Role of immunology in HCC development and progression Pablo SAROBE, Spain :0 - :40 Immunotherapy in HCC: Current evidence and future perspective Bruno SANGRO, Spain :40-2:30 Roundtable: Novel approaches in immunotherapy Future perspectives in HCC Chairs: Jordi BRUIX, Spain Sandrine FAIVRE, France 3:30-3:50 Screening for new drugs Lars ZENDER, Germany 3:50-4:0 Patient-derived models for drug discovery in liver cancer Jens MARQUARDT, Germany 4:0-4:30 What have we learned from failed trials and how do we design future trials? Sandrine FAIVRE, France 4:30-5:00 Future perspectives in HCC: The industry perspective Gerold MEINHARD, United States 2
13 Thursday March 208 eposter Session 6:45-7:5 Randomized trial of preoperative administration of oral pregabalin for postoperaive analgesia in patients scheduled for radiofrequency ablation of focal lesions in the liver. Sherief ABD-ELSALAM, Egypt 6:45-7:5 MiRNA profile as a prognostic biomarker for hepatocellular carcinoma development Alexandr ABRAMOV, Russian Federation 6:45-7:5 Impact of BCLC treatment stage migration in the survival of patients with hepatocellular carcinoma Silvia ACOSTA-LÓPEZ, Spain 6:45-7:5 RIP3-dependent signalling contributes to non-alcoholic fatty liver diseaserelated carcionogenesis Marta B. AFONSO, Portugal 6:45-7:5 The biomarker potential of Ki67 and ph2aximmunohistochemistry in guiding use of the liver-targeting nucleotide MIV-88 in patients with hepatocellular carcinoma Mark ALBERTELLA, Sweden 6:45-7:5 Sarcopenia PredictsSurvival in Patients with Advanced Hepatocellular Carcinoma treated with Sorafenib. Giulio ANTONELLI, Italy 6:45-7:5 Rapamycin and Zoledronic Acid strongly inhibit growth of advanced murine hepatocellular carcinoma via activation of innate and adoptive immunity Muhammad ASHFAQ-KHAN, Germany 6:45-7:5 Zoledronic Acid suppresses tumour associated macrophages and myeloid derived suppressor cells in murine HCC Misbah ASLAM, Germany 6:45-7:5 Distinct functions of AP- (FOS/JUN) dimers in liver cancer Latifa BAKIRI, Spain 6:45-7:5 Liver cancer, not etiology or steatosis or fibrosis, is the only independent predictor of elevated periostin concentration among caucasian patients with liver disease Matteo Nazzareno BARBAGLIA, Italy eposter session 2 9:5-9:45 Hepatocellular carcinoma inaugurating cirrhosis: a descriptive study soumaya BEN AMOR, Tunisia 9:5-9:45 Presence of HCC does not affect the course and response to anticoagulation of bland non malignant portal vein thrombosis in cirrhotic patients Francesca BENEVENTO, Italy 9:5-9:45 Serological diagnosis of early HCC in NASH: A German multicenter Study Jan BEST, Germany 9:5-9:45 Liver targeting and anti-tumour efficacy of the nucleotide prodrug MIV-88 in nonclinical models of hepatocellular carcinoma Richard BETHELL, Sweden 9:5-9:45 Association of Ang, Ang2 and FGF Genetic Polymorphism and their expression analysis in Hepatocellular Carcinoma DIPU BHARALI, India 9:5-9:45 Liquid Crystalline Nanoparticles (LCNPS) based delivery of an anticancer bioactive, Methotrexate Mani BHARGAVA, India 9:5-9:45 Evaluation of prognostic factors of overall survival and progression-free survival in patients with hepatocellular carcinoma Cristiana BIANCO, Italy 3
14 9:5-9:45 Anti-inflammatory polarization of tumor associated macrophages promoting tumor growth and angiogenesis in HCC of chemokine receptor Cxcr3 deficient mice Elisa Fabiana BRANDT, Germany 9:5-9:45 Hand foot skin reaction and overall survival in the phase 3 RESORCE trial of regorafenib for treatment of hepatocellular carcinoma progressing on sorafenib Jordi BRUIX, Spain 9:5-9:45 Intra-tumoral tertiary lymphoid structures are associated with a low risk of early tumor recurrence in patients with hepatocellular carcinoma Julien CALDERARO, France 9:5-9:45 HepaVac-0 first-in-man therapeutic cancer vaccine Phase I/II clinical trial for hepatocellular carcinoma patients Luigi BUONAGURO, Italy eposter session 3 9:45-20:5 Genomic expression analysis of infiltrating Natural Killer cells suggests a migration defect into the tumor microenvironment Diana CANETTI, Italy 9:45-20:5 Glycolytic enzymes PKM2 and PGK are instrumental to DNA damage protein CHK2 in sustaining genomic instability in hepatocelluar carcinoma Vinicio CARLONI, Italy 9:45-20:5 Immune inflammation indicators and ALBI score to predict occurrence and recurrence of hepatocellular carcinoma in HCV-related cirrhosis treated with direct-acting antivirals Andrea CASADEI GARDINI, Italy 9:45-20:5 Epigenetic control of hepatic homeostasis Marco CASSANO, Switzerland 9:45-20:5 Patient-Derived Liver Cancer Cell Lines in Personalized Treatment Approach: From Phenotypic and Molecular Characterization to Therapeutic Target Identification Darko CASTVEN, Germany 9:45-20:5 Development of SLN as carriers for delivery of Hepatitis B for vaccination using subcutaneous route Mani BHARGAVA, India 9:45-20:5 Poncirus Fructus inhibited the proliferation and induced the apoptosis in hepatocellular carcinoma by the down-regulation of NF-κB Lokendra CHAND, Korea, Rep. of South 9:45-20:5 A large set of mirnas is deregulated since the earliest steps of human HCC development Amedeo COLUMBANO, Italy 9:45-20:5 Cytotoxic T lymphocytes (TC) and regulatory T cells (TREG) predict the development of dermatologic adverse effects in patients with hepatocellular carcinoma treated with sorafenib Josep COROMINAS, Spain 9:45-20:5 A high alpha-fetoprotein slope prior to therapy correlates with poor survival of patients with hepatocellular carcinomas. Carolin CZAUDERNA, Germany 9:45-20:5 Macrotrabecular-massive hepatocellular carcinoma: a distinctive histological subtype with clinical relevance Julien CALDERARO, France 9:45-20:5 Macrophage migration inhibitory factor is upregulated in murine hepatocellular tumor tissue and exerts pro-proliferative and anti-apoptotic effects on hepatoma cells in vitro Theresa WIRTZ, Germany 4
15 Friday 2 March 208 eposter session 4 0:00-0:30 Incidence and predictors of de-novo hepatocellular carcinoma in HCV cirrhotic patients treated with direct-acting antivirals: a single-center prospective 3 year study Roberta D'AMBROSIO, Italy 0:00-0:30 Metronomic capecitabine vs. best supportive care in Child-Pugh B hepatocellular carcinoma: a proof of concept Stefania DE LORENZO, Italy 0:00-0:30 Efficacy of radiofrequency in patients with hepatocellular carcinoma: meta-analysis Andrea CASADEI GARDINI, Italy 0:00-0:30 Phenotypical and molecular changes in nodule in nodule hepatocellular carcinoma with pathogenetic implications Luca DI TOMMASO, Italy 0:00-0:30 Systematic review and metanalysis establish dermatology adverse events as a positive predictor of survival in hepatocellular carcinoma patients treated with sorafenib Alvaro DIAZ-GONZALEZ, Spain 0:00-0:30 Doxorubicin and hypoxia treatment of HCC cell lines: cell viability and oncologic protein profile Ilse DUBBELBOER, Sweden 0:00-0:30 Presence of HCC and BCLC stage significantly influence soluble fibrinogen-like protein 2 (sfgl-2) in cirrhotic patients Ioannis ELEFSINIOTIS, Greece 0:00-0:30 Retrospective observational study of characteristics of HCC patients from Egypt and impact of surveillance on improving their outcomes Medhat ELHOSARY, Egypt 0:00-0:30 Modification of the ALBI-T score: new prognostic model for patients with Hepatocellular Carcinoma Omar ELSHAARAWY, Germany 0:00-0:30 Dynamic survival analysis of the data from the National Survey of HCC and Liver Transplant in Brazil Guilherme FELGA, Brazil 0:00-0:30 Assessment of hypothyroidism as a marker of response to sorafenib in patients with hepatocellular carcinoma. Symptoms make the difference. Pablo FLOREZ DÍEZ, Spain 0:00-0:30 Efficacy and safety of regorafenib in clinical practice in the treatment of hepatocellular carcinoma. Multicentre experience. Miguel FRAILE, Spain eposter session 5 2:30-3:00 TLL polymorphism do not predict the development of de-novo hepatocellular carcinoma in HCV cirrhotics treated with IFN-free DAAbased regimens Enrico GALMOZZI, Italy 2:30-3:00 Dysregulation of the lysosomal compartment with verteporfin potentiates the anti-tumor effect of sorafenib in hepatocellular carcinoma Jacopo GAVINI, Switzerland 2:30-3:00 Non adherence to AASLD-EASL guidelines for the management of hepatocellular carcinoma does not translate into worse outcomes Alessio GERUSSI, Italy 2:30-3:00 MALDI IMAGING OF HEPATOCHOLANGIOCARCINOMAS: A CLUE TO TACKLE TUMOR HETEROGENEITY. PRELIMINARY RESULTS. Elia GIGANTE, France 2:30-3:00 Hyperbilirubinemia is a fallacious parameter to detect liver toxicity in patients with hepatocellular carcinoma treated with sorafenib and may lead to inadequate treatment interruption 5
16 Alvaro DIAZ-GONZALEZ, Spain 2:30-3:00 HCC recurrence after DAA treatment in HCV patients. maria GUARINO, Italy 2:30-3:00 Short-term recurrence of hepatocellular carcinoma in HCV infected patients is unaffected by direct antiviral agents therapy. A case-control, single center study. Marco GUARRACINO, Italy 2:30-3:00 Endoplasmic reticulum stress in hepatic stellate cells contributes to the progression of hepatocellular carcinoma. Femke HEINDRYCKX, Sweden 2:30-3:00 Comprehensive Evaluation of the Role of Receptor Tyrosine Kinase Family in Hepatocellular Carcinogenesis Sen-Yung HSIEH, Taiwan 2:30-3:00 Predictors of hepatocellular recurrence after liver transplant in Hepatitis C patients: a ten-years single Center cohort Massimo IAVARONE, Italy 2:30-3:00 Early treatment with Sorafenib and mtor inhibitor in recurrent hepatocellular carcinoma after liver transplantation: safety and survival. Federica INVERNIZZI, Italy 2:30-3:00 Changing clinical profile and epidemiology of Hepatocellular carcinoma in India Vaneet JEARTH, India eposter session 6 3:00-3:30 Global Protein Aberration Score (GloPAS), a comprehensive risk score to predict Hepatocellular Carcinoma biology and estimate patients' survival Ahmed KASEB, United States 3:00-3:30 A new prognostic scoring system for cirrhosis and hepatocellular carcinoma utilizing CD44 rs875 gene polymorphism A Ali KHALIFA, Egypt 3:00-3:30 Presence of non-hypervascular hypointense nodule on hepatobiliary phase of gadoxetic-acid enhanced MR: risk of tumor recurrence after curative treatment for small single nodular HCC and guidance for selection of treatment methods Dong Ho LEE, Korea, Rep. of South 3:00-3:30 Up-regulation of MIR-324 supports proliferation of Hepatocellular Carcinoma cancer cells and correlates with poor prognosis of HCC patients Pengyu LIU, Netherlands 3:00-3:30 Recurrence and "de novo" diagnosis of hepatocellular carcinoma and other neoplasms in patients with hepatitis C treated with direct-acting antivirals Monica LLORENTE BARRIO, Spain 3:00-3:30 Clinical and genetic predictors of HCC occuring in caucasian compesated HBV cirrhotics treated by Entecavir or Tenofovir for 8 years Alessandro LOGLIO, Italy 3:00-3:30 Elevated circulating immature neutrophils predicts poor response to therapy, shorter time to progression and poorer survival in patients with hepatocellular carcinoma Sheba MACHEKA, United Kingdom 3:00-3:30 ANGPT2 polymorphisms and clinical outcome in advanced hepatocellular carcinoma patients receiving Sorafenib Giorgia MARISI, Italy 3:00-3:30 Excellent 5 years survival for cirrhotic patients developing an hepatocellular carcinoma during long-term oral therapy for HBV Massimo IAVARONE, Italy 3:00-3:30 HCC progression and survival following HCV anti-viral therapy Jibran MECCI, United Kingdom 6
17 3:00-3:30 Contrast enhanced versus conventional ultrasound guided liver biopsy in the diagnosis of hepatocellular carcinoma : A prospective study Tudor MOCAN, Romania eposter session 7 6:30-7:00 Depletion of activated stromal fibroblasts in liver fibrosis - a promising approach to prevent liver cancer? Anja MONCSEK, Switzerland 6:30-7:00 Sphingolipids: a further step into the detection of early and advanced hepatocellular carcinoma Iuliana NENU, Romania 6:30-7:00 The role of Interleukin 6 signaling pathway in Cholangiocarcinoma Thi Mai Ly NGUYEN, Germany 6:30-7:00 Liver cancer cell lines distinctly reflect the metabolic gene expression pattern observed in clinical microarrays Zeribe NWOSU, Germany 6:30-7:00 Genetic inactivation of Nrf2 prevents clonal expansion of carcinogeninitiated cells in a nutritional model of rat hepatocarcinogenesis Claudia ORRÚ, Italy 6:30-7:00 Activated platelets contribute to the progression of hepatocellular carcinoma by altering the immune cell environment Natasa PAVLOVIC, Sweden 6:30-7:00 The combination of Pivka-II and afp levels improves the diagnostic accuracy for the diagnosis of HCC developing in long-term nuc suppressed HBV caucasian cirrhotics Alessandro LOGLIO, Italy 6:30-7:00 New insights in Transforming Growth Factor Beta signaling pathway on tumor suppression and metastatic properties in primary liver cancer Sharon PEREIRA, Germany 6:30-7:00 In vivo reactivation of thyroid hormone nuclear receptors by 3,5,3' triiodothyronine has a therapeutic potential in hepatocellular carcinoma Andrea PERRA, Italy 6:30-7:00 Cost-effective targeted sequencing for hepatocellular carcinoma mutational screening Salvatore PISCUOGLIO, Switzerland 6:30-7:00 Increased intestinal permeability and inflammation are associated with hepatocellular carcinoma in patients with NAFLD-related liver cirrhosis Francesca PONZIANI, Italy 6:30-7:00 LINC0052 may function as a cerna core component in human hepatocellular carcinoma Rosella PELLEGRINO, Germany eposter session 8 9:00-9:30 Hepatocellular carcinoma - how does BCLC score influence therapeutic decision? Daniela REIS, Portugal 9:00-9:30 Clinical significance of time related fluctuations of AFP and PIVKA-II serum levels in patients with cirrhosis undergoing surveillance for hepatocellular carcinoma Gabriele RICCO, Italy 9:00-9:30 mir-2 ablation prevents NASH-associated hepatocellular carcinoma Pedro M. RODRIGUES, Portugal 9:00-9:30 Role of the HES5/NOTCH signaling pathway in liver carcinogenesis Stephanie ROESSLER, Germany 9:00-9:30 Long non-coding RNA H9: a biomarker of hepatocellular carcinoma Ángela ROJAS, Spain 7
18 9:00-9:30 Inhibiting the P2Y2 receptor decreases tumour cell viability and affects different cell types in the stroma Natasa PAVLOVIC, Sweden 9:00-9:30 Overcoming heat-sink in portal vein related hepatocellular carcinomas with combined radiofrequency ablation and percutaneous ethanol injection Hisham SAAD MOHAMED ELSAYED ABDELAAL, Egypt 9:00-9:30 Long-term Sorafenib treatment in a large cohort of HCC patients: a multi center study Rodolfo SACCO, Italy 9:00-9:30 Factors associated with occurrence/recurrence of hepatocellular carcinoma early after treatment of hepatitis C with direct antiviral agents Livia SALMI, Italy 9:00-9:30 Serum endoglin (CD05) as a potential marker for hepatocellular carcinoma in cirrhotic hepatitis C virus and hepatitis B virus patients Mohamed SAMY, Egypt 9:00-9:30 Impact of regorafenib in the clinical practice and identification of secondline treatment orphan patients Marco SANDUZZI ZAMPARELLI, Spain Saturday 3 March 208 eposter session 9 0:00-0:30 Contrast-enhanced ultrasound for non-invasive diagnosis of hepatocellular carcinoma: a comparison between CEUS LI-RADS and ESCULAP criteria in a large high-risk cohort of patients Antonio SAVIANO, France 0:00-0:30 Regorafenib after progression on Sorafenib for advanced HCC Kornelius SCHULZE, Germany 0:00-0:30 predictors of recurrence and survival of hepatocellular carcinoma: prospective study including transient elastography and cancer stem cell markers Hend SHOUSHA, Egypt 0:00-0:30 Epithelial-to-mesenchymal transition induced drug resistance in hepatocellular carcinoma derived cancer stem cells Ritu SHRESTHA, Australia 0:00-0:30 S00a is part of a whole network of tumor suppressors and oncogenes deregulated early with hepatic steatosis and contributing to hepatocellular carcinoma development Cyril SOBOLEWSKI, Switzerland 0:00-0:30 Evaluation of the single and multiple natural RASs prevalence in the main HCV genotypes in Italian court Maria Chiara SORBO, Italy 0:00-0:30 Prognostic effect of Yttrium-90 radioembolization for hepatocellular carcinoma with portal vein invasion Carlo SPOSITO, Italy 0:00-0:30 Early detection of hepatocellular carcinoma in cirrhotic liver model in MRI using iron doped nano-calcium phosphate contrast agent Badrinathan SRIDHARAN, India 0:00-0:30 Dissecting the spatial heterogeneity of circulating tumor cells reveals CCL5-treg mediated immune evasion in hepatocellular carcinoma Yunfan SUN, China 0:00-0:30 Impact of regorafenib in the clinical practice and identification of the second-line treatment orphan patients Marco SANDUZZI ZAMPARELLI, Spain 0:00-0:30 IFN-free DAA treatment of cirrhotic HCV patients with or without history of HCC: a multicenter prospective trial in Italy Angelo SANGIOVANNI, Italy 8
19 eposter session 0 2:30-3:00 Superiority of multiple random gene sets in predicting survival of patients with hepatocellular carcinoma Andreas TEUFEL, Germany 2:30-3:00 Clinicalfeatures of hepatocellular carcinoma in the elderly in a hepatitis B endemic country - a comparative study of 430 cases Chee-Kiat TAN, Singapore 2:30-3:00 prediction of hepatocellular carcinoma using non invasive biomarkers of liver fibrosis: a retrospective study of 2363 patients Hend SHOUSHA, Egypt 2:30-3:00 Percutaneous electrochemotherapy of hepatocellular carcinoma at hepatichilum Luciano TARANTINO, Italy 2:30-3:00 gp38+ hepatic progenitor cell-derived extracellular vesicles in HCC and biliary cancer - a novel liquid biopsy marker? Sabine URBAN, Germany 2:30-3:00 Ubiquitin carboxy-terminal hydrolase L inhibition as a potential strategy to modulate the sorafenib response of hepatocellular carcinoma. Astrid VANDIERENDONCK, Belgium 2:30-3:00 Large unresectable hepatocellular carcinoma: efficacy of percutaneous thermal ablation after occlusion of tumor blood supply by gelfoam. Letizia VERONESE, Italy 2:30-3:00 The MELD score is positively correlated with neutrophil to lymphocyte ratio and red blood cell distribution in assessment of mortality nas recurrence in patients with hepatocellular carcinoma after living donor liver transplantation Chih-Chi WANG, Taiwan 2:30-3:00 YAP drives chromosomal instability in HCC patients, which correlates with clinical and molecular patient features Sofia WEILER 2:30-3:00 Portal vein tumor thrombosis has a direct impact on liver function Arndt WEINMANN, Germany 2:30-3:00 Registration of complete response to chemoembolization at 2 and 6 months avoids >0% of follow-up angiographies and permits an effective transition into systemic therapy upon progression, thus ensuring optimal survival Marco SANDUZZI ZAMPARELLI, Spain 2:30-3:00 Changes of AFP and PIVKA-II levels during DAA treatment and their predictive value for early diagnosis of HCC in HCV cirrhotic patients with SVR to DAA treatment Angelo SANGIOVANNI, Italy eposter session 3:00-3:30 Hepamine - A liver disease microarray database, visualization platform and data-mining resource Andreas TEUFEL, Germany 3:00-3:30 Characterization of HBV integration landscape in tumor and non-tumor liver tissues by a high-throughput viral integration detection approach Deborah D'ALIBERTI, Italy 3:00-3:30 role of serum amyloid A and long non-coding RNA AF as diagnostic biomarkers for hepatitis B and C related hepatocellular carcinoma Hend SHOUSHA, Egypt 3:00-3:30 Exosome-Transmitted circrna_04797 Sustains Sorafenib Resistance in Hepatocellular Carcinoma Junjie XU, China 3:00-3:30 chemo-preventive and anti-tumor effects of benzyl isothiocynate on HCC models: a possible crosstalk between HGF/pAkt/STAT3 pathway and VEGF 9
20 sherin ZAKARIA, Egypt 3:00-3:30 Prognostic scores for sorafenib-treated hepatocellular carcinoma patients: a validation study of the HAP and SAP scores Francesco TOVOLI, Italy 3:00-3:30 Combined targeting of the PPMD/WIP and MDM2 negative feedback suppressors of p53 in TP53 wild-type human liver cancer cells Ahmed MAHDI, United Kingdom 3:00-3:30 Clinical correlates of the genetic variability of the CD274 gene (Programmed Cell Death-Ligand ) among patients with hepatocellular carcinoma Federico DAFFARA, Italy 3:00-3:30 A specific ECM composition regulates Smad - dependent - TGFbeta- induced EMT response in HepG2 cells engineered in cirrhotic and healthy human liver 3D scaffolds Krista ROMBOUTS, United Kingdom 3:00-3:30 Hepatocellular carcinoma as a complication of vascular disease of the liver after Fontan procedure. Chiara MAZZARELLI, Italy 3:00-3:30 Outcomes of single or sequential dual modality loco-regional therapies in Hepatocellular carcinoma Vinay Kumar BALACHANDRAKUMAR, United Kingdom 3:00-3:30 Multimodal and sequential treatmente for hepatocellular carcinoma: how "real-life" complies with international recommendations Angelo SANGIOVANNI, Italy 20
21 INVITED SPEAKERS ABSTRACTS 2
22 Immunotherapy in HCC and the hepatologist what does the future multidisciplinary team look like? Jordi Bruix Hospital clinic, Barcelona, Spain The term multidisciplinary team or board is usually understood as a group of experts from different fields of knowledge who work together. In this case, the area of work is liver cancer. The main issue in such group is not to simply meet all together at the same time, but rather share a common strategy about how to approach the diagnosis and treatment of patients with such condition. This common approach has to be based in scientific evidence so that decisions taken about a clinical case are not the result of a random debate around personal opinions, but rather the result of the blend of scientific data with personal experience and individualised assessment of the specific patient. According to this philosophy the multidisciplinary teams have to incorporate expert clinicians in the field of hepatic oncology, diagnostic and interventional radiologists, pathologists, surgeons and experts in radiation. Understanding of molecular mechanisms and proper interpretation of biomarkers and pathology profiling should prime the incorporation of experts in such topics, but always respecting the need to differentiate between wishful thinking and robust data for clinical decision making. Indeed, one key player in such teams is a statistician whose expert assessment of data should allow to distinguish between scientific strength and biased approach to results. Currently, immune therapies are part of an intense research activity that has elicited major optimist about its efficacy. When proven in phase 3 trials, it will be key to understand the data that allow to identify who benefits from therapy and who does not. This may come from the analysis of tumour biopsy or from specific hematology assessment. Tumour biopsy data may be always hampered by the well known tumour heterogeneity. This has been the case for the already proposed molecular signatures that up to now have no impact in prognosis prediction or treatment allocation. As a consequence, experts in the specific assessment to be in place in due time will need to be incorporated. In summary, teams devoted to liver cancer should be able to coordinate the knowledge of different areas of expertise, but always using the scientific strength of the data to take clinical decisions. 22
23 Genomic diversity in HCC: the TCGA experience Lewis Roberts Mayo Clinic, Rochester, United States The Cancer Genome Atlas (TCGA) project was initiated by the US National Cancer Institute (NCI) and National Human Genome Research Institute (NHGRI) in 2006 to perform comprehensive multimodality characterization of cancer through the application of genome analysis technologies, especially largescale genome sequencing. By the end of the project in 207, comprehensive characterization had been performed on 33 different tumor types, including 0 rare cancer types, based on paired tumor and normal samples from,000 patients, using 7 different genome and protein analysis technologies. For each major cancer type, the goal was to profile 500 cancers, of which 0% or 50 were characterized for mutations and genetic aberrations by whole genome sequencing, while the remainder were characterized by whole exome sequencing. All tumors were further characterized by whole genome genotyping array for copy number variations, RNA sequencing, microrna sequencing, whole genome methylation array analysis, and reverse phase protein array analysis. For each cancer type, an analysis working group was assembled that developed a list of key clinical variables to be abstracted by the tissue source sites. A worldwide call for tissue source sites resulted in a fairly broad geographic representation of tumors for many of the tumor types, although most tumors were obtained from sites in North America. There were strict criteria for tissue qualification, which included tumor purity, DNA quality and RNA quality. For the TCGA HCC project, 377 HCCs were qualified for analysis, Strengths of TCGA HCC project include the relatively large number of tumors profiled from patients with a wide range of etiologies, including alcoholic liver disease, hepatitis B, hepatitis C, and non alcoholic fatty liver disease. Histopathologically, the tumors exhibited a variety of pathologic phenotypes. Bioinformatic analyses subclassified the TCGA HCCs into different numbers of subgroups based on the analysis technology. Further integrated analysis using the icluster algorithm resulted in classification of HCCs into 3 distinct subgroups, which were shown to be associated with different clinical outcomes. The TCGA approach had a number of limitations. Because frozen resected tissue was used, there was a bias towards early stage disease. The requirement for high tumor purity meant that tumors with high stromal content did not qualify for analysis. Due to limitations in funding and tissue availability it did not address the issue of intratumoral heterogeneity. Finally, because prior chemotherapy was not allowed and there was almost no information on receipt of systemic therapy after resection, analyses could not be performed based on response to therapy. Future goals for integrative genomic analyses of HCCs include the identification of prognostic and predictive biomarkers, detailed characterization of regulatory pathway networks, analyses of the complex effects of mrna splice variation, and additional whole genome and HBV integration analyses. TCGA HCC data is available from the Genomic Data Commons (GDC) Data Portal ( Reference: The Cancer Genome Atlas Research Network, Wheeler DA*, Roberts LR* (* Co-Corresponding Authors), Comprehensive and Integrative Genomic Characterization of Hepatocellular Carcinoma. Cell 207; 69: PMID:
24 Mutational signatures in HCC resulting from exogenous and endogenous exposure Eric Letouzé INSERM, Paris, France Liver cancers mostly develop in a context of liver disease related to various etiologies including viral infection, alcohol abuse or metabolic syndrome. In the last 5 years, our team has used genomic profiling to understand how the interplay of risk factors and endogenous cellular processes reshape the genomes of liver cancer cells. Whole exome and whole genome sequencing by us and others revealed 0 mutational signatures characterized by distinct substitution types occurring preferentially in specific trinucleotide contexts. These signatures reflect the wide diversity of mutational processes operative in liver cells. By quantifying the activity of these processes in a meta-series of 300 HCC genomes, we analyzed in-depth their relationships with environmental exposures, replication, transcription, and driver genes. Five signatures correspond to ubiquitous mutational processes operative in every liver cell and increase with age, but their intensity is modulated by risk factors like gender, tobacco and alcohol. Other signatures are restricted to specific cases and associated with particular exposures (aflatoxin B, aristolochic acid) that may be highly prevalent in specific geographic areas. Different mutational processes have different propensities to affect specific driver genes depending on the local nucleotide context. For instance, the liver cancer-specific signature 6, associated with alcohol consumption, was a preferential source of CTNNB mutations, which may explain the higher prevalence of CTNNB mutations in alcohol-related cases. Every signature is differently modulated by replication and transcription. Signatures of bulky DNA adducts like aflatoxin B are less active in highly expressed genes where they are corrected by transcription-coupled repair. By contrast, very highly expressed hepato-specific genes like ALB or APOB acquire flood of indels, likely resulting from replicationtranscription collisions. We extended mutational signature analysis to structural rearrangements, showing that specific signatures of duplications, translocations and deletions occur in liver cancers and define particular subgroups with striking rearrangement phenotypes. These studies shed new light on the diversity of risk factors and their effect on liver cancer genomes. 24
25 From tumour diversity to individualised management: What is different about NAFLD-HCC? Helen Louise Reeves Northern Institute for Cancer Research, Newcastle University, Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle upon Tyne, United Kingdom In an era where the incidence and mortality attributed to HBV and HVC related HCC is falling in geographical locations with effective immunization, prevention, surveillance and treatment programmes, the incidence and mortality attributed to NAFLD-HCC is rising - reflecting the global prevalence of obesity, type 2 diabetes and NAFLD. Cohort studies indicate that NAFLD-HCC patients tend to be older. NAFLD-HCC more frequently presents in the absence of cirrhosis, typically in patients that are older still. NAFLD-HCC patients more often present at advanced stages having not been in surveillance programmes. NAFLD-HCC patients also tend to have a poorer prognosis after presentation, but rather than being disease specific, this is likely a consequence primarily of the stage of disease at presentation, as well as age/metabolic syndrome related comorbidities which have a significant impact on treatment options and survival. Because NAFLD-HCC more often arises in the absence of established cirrhosis, patients are more likely to have a biopsy to confirm their diagnosis. Histopathology studies indicate similar subtypes of HCC, but with a higher prevalence of steatohepatitic (SH) HCC. SH-HCC are cancers enriched with fat accumulation, ballooned hepatocytes and an inflammatory infiltrate. These characteristics of NAFLD-HCC are ones that we need to try and understand at a biological level, if we want to develop individualized management plans for earlier detection, prevention and treatment. For clues about the risk of HCC in NAFLD, we have to look deeper than simply the presence of obesity, type 2 diabetes and NAFLD. These conditions are so common that a cancer surveillance programme would involve half the population and be prohibitively expensive. It would also be futile - principally because within the large NAFLD population, the individual risk of developing HCC is small - much smaller than the cancer risk in an individual with cirrhosis or HBV infection. What we need to identify are those factors that elevate individual risk in patients with NAFLD. The presence of cirrhosis remains the most well established risk for NAFLD-HCC, but there are others both endogenous and exogenous. There is evidence for a heritable component, with single nucleotide polymorphisms affecting risk identified in a number of candidate genes that influence metabolic regulation in the liver (PNPLA3, KLF6). Advances in molecular technologies are identifying less common genetic variations also associated with risk (TERT). Drugs which influence hepatic metabolism, such as metformin, can also delay the age of onset of HCC more so than other antidiabetic treatments. Liver biopsy studies often reveal periodic acid-schiff (PAS) positive globules or iron overload in non-tumour liver in NAFLD-HCC patients, suggesting co-existent conditions which elevate exposure to DNA or cellular damage. Human studies have been complimented in the last decade by a wealth of data from animal models - highlighting amongst other things, roles for the immune response in the progression of NAFLD-HCC. This lecture will give an overview as above, providing the background for the subsequent focus and interpretation of data generated from our own animal model of NAFLD-HCC and human tissues biobank. We hypothesize that the NAFLD environment is a hyperproliferative one. While the impact of this is not as great as the proliferative state observed within the regenerative nodules of a cirrhotic liver, with the passage of time it is sufficient, in patients with additional risks, to create a selection pressure for cells that acquire mutations conferring a growth or survival advantage. 25
26 Debate: DAA treatment of cirrhotic HCV infected patients with HCC con Sabela Lens Hospital Clinic Barcelona, Barcelona, Spain Direct antiviral agents mark a major progress for the treatment of chronic hepatitis C virus infection. Due to a more favorable efficacy and safety profile, special populations such as patients with advanced liver disease (decompensated cirrhotics) or patients with hepatocellular carcinoma (HCC), which were excluded in the major studies assessing the antiviral effectiveness of DAAs, have since been treated. Several studies have recently described a potential unexpected recurrence of HCC in successfully treated patients who were disease-free for different periods of time. These reports have generated a great and controversial debate and have been followed by a series of other publications not confirming such increased risk. The possibility that treatment with DAAs may favor tumor growth and spread in individual patients with active HCC foci is suggested by some observations. Indeed, other reports have indicated that antiviral therapy may be associated with the reactivation of hepatitis B virus or the emergence of herpes virus in a time-related manner. The most likely explanation to these clinical findings is an inflammatory distortion in the setting of a rapid decrease in viral load, which suddenly produces an immune homeostasis misbalance. Major epidemiological, clinical and translational research is very relevant in order to determine and personalize the risks and benefits of DAA antiviral therapy in patients with previous HCC. 26
27 Liver polyploidy: a good guy or a bad guy Chantal Desdouets 2 3 INSERM, U06, Institut Cochin, Paris, France, 2 CNRS, UMR804, Paris, France, 3 Université Paris Descartes, Sorbonne Paris Cité, Paris, France chantal.desdouets@inserm.fr Polyploidization (multiple complete sets of chromosomes) is one of the most dramatic changes that occurs in the genome. The diploid state (2n) is the norm for mammalian cells, but various studies have demonstrated a major role, in specific tissues, of diploid-polyploid conversion during physiological processes (e.g. embryogenesis, terminal differentiation) but also during pathological conditions (e.g. genotoxic, metabolic and oncogenic process). Polyploid cells arrive through a variety of division errors (e.g. defects in cytokinesis, chromosome endoreplication, telomere erosion). Alarmingly, proliferating polyploid cells were shown to be genetically unstable. Accumulating evidence point to a significant contribution of polyploid intermediates in shaping the composition of cancer genomes: 20% of all solid tumors exhibit polyploid karyotypes. Polyploidy is a physiological characteristic feature of mammalian hepatocytes. Up to 50% of human hepatocytes are polyploid; the majority being tetraploid with two nuclei (binuclear 2x2n, chromosomally stable). Importantly, throughout life, the liver is exposed to various lesions. Beyond these injuries, hepatocytes retain the unique property to self-renew and to restore the liver ad integrum while preserving its ploidy/dna integrity. How polyploid profile is modified in damaged livers and its consequences to genomic instability is an open question. 27
28 Diagnostic and prognostic role of circulating microparticles in hepatobiliary cancers Miroslaw Kornek Universität des Saarlandes, Homburg, Germany Hepatic cancers were the sixth most common-incident cancer worldwide and accordingly to the Global Burden of Disease Study 205, and the fourth most common cause of cancer death. On the other hand, the Italian Liver Cancer Group showed that the 5-year overall survival rate in hepatocellular carcinoma (HCC) was 32.7% in semiannually surveilled patients, 25.2% in annually surveilled patients, and 2.2% in symptomatic patients. These results strongly arguing that a semiannually HCC screening might prolong lifespan depending on the progression of HCC at the time point of recognition []. Nowadays, extracellular vesicles (EVs) such as submicron microparticles (MPs) [2] and microvesicles (MVs) [3] as well as nano-sized exosomes [4], are raising more and more attention as a novel and unique approach as a liquid biomarker for diseases diagnosis, including liver diseases and liver tumours [5-5]. Larger EVs were first time described as an unwanted contamination of an experimental preparation of platelets and eventually called platelets dust by Wolf et al. 967 [6]. However, during the last decade, advanced methodologies such as fluorescence activated cell scanning (FACS) enabled their detailed characterization. MPs/MVs are nm in diameter, sometimes referred to ectosomes, and represent a novel route of horizontal communication between cells within the living organism through various body fluids. In contrast, exosomes are smaller in size, <00 nm, and in contrast to MPs they are formed and stored within the source-cell before their release [2, 4, 7, 8]. Many recent reviews summarize and provide in depth discussions of their differences, how to use them as putative biomarkers, as novel non-cell based therapy option and their impact on cell-cell communication [6, 9-22]. However, only few research articles are available. In 2008, a hepatocellular carcinoma (HCC) pilot study was published, showing that the levels of endothelial (CD3 + /CD42 - ) and hepatocyte (HepPar) derived MPs in HCC liver transplant patients were altered after surgery and correlated with the clinical outcome [23]. 206, Lu L et al. correlated the content of HCC derived microvesicles with the HCC presence [24]. Additionally, parallel to our latest publication in 207 on liver cancer associated tamps [8], HepPar + MPs were associated with HCC. [0]. In case of biliary cancers, a group from Geneva linked elevated numbers of plain exosomes in bile and serum with the presence of malignant (M) vs. nonmalignant (NM) CBD stenosis [25] and the group from Spain could correlated distinguished proteomic signatures found in serum EV with CCA, PSC, and HCC patients [9]. As discussed by us recently [5] and being part of the presentation, we believe that the large EVs, so called MPs/MVs have certain advantages over small EVs, as exosomes, in regard of diagnosis, whereas exosomes could be very well superior over MPs/MVs in therapy monitoring. Learning Objectives Bibliographic References To understand the major differences between large (MPs/MVs) and small EVs (exosomes). To be enable to acknowledge the limitation of both EVs populations regarding cancer diagnosis. To address the question if EVs are suitable for early cancer screening?. Cucchetti, A., et al., Estimation of lead-time bias and its impact on the outcome of surveillance for the early diagnosis of hepatocellular carcinoma. J Hepatol, (2): p Boilard, E., et al., Platelets amplify inflammation in arthritis via collagen-dependent microparticle production. Science, (5965): p Fourcade, O., et al., Secretory phospholipase A2 generates the novel lipid mediator lysophosphatidic acid in membrane microvesicles shed from activated cells. Cell, (6): p
29 4. Thery, C., L. Zitvogel, and S. Amigorena, Exosomes: composition, biogenesis and function. Nat Rev Immunol, (8): p Urban, S.K., et al., Reply to: "Diagnostic and prognostic role of circulating microparticles in hepatocellular carcinoma". J Hepatol, Szabo, G. and F. Momen-Heravi, Extracellular vesicles in liver disease and potential as biomarkers and therapeutic targets. Nat Rev Gastroenterol Hepatol, (8): p Maji, S., et al., Extracellular vesicles in liver diseases. Am J Physiol Gastrointest Liver Physiol, (3): p. G94-G Julich-Haertel, H., et al., Cancer-associated circulating large extracellular vesicles in cholangiocarcinoma and hepatocellular carcinoma. J Hepatol, Arbelaiz, A., et al., Serum extracellular vesicles contain protein biomarkers for primary sclerosing cholangitis and cholangiocarcinoma. Hepatology, Abbate, V., et al., HepPar-Positive Circulating Microparticles Are Increased in Subjects with Hepatocellular Carcinoma and Predict Early Recurrence after Liver Resection. Int J Mol Sci, (5).. Sato, K., et al., Exosomes in liver pathology. J Hepatol, (): p Ban, L.A., N.A. Shackel, and S.V. McLennan, Extracellular Vesicles: A New Frontier in Biomarker Discovery for Non-Alcoholic Fatty Liver Disease. Int J Mol Sci, (3): p Lemoinne, S., et al., The emerging roles of microvesicles in liver diseases. Nat Rev Gastroenterol Hepatol, 204. (6): p Kornek, M. and D. Schuppan, Microparticles: Modulators and biomarkers of liver disease. J Hepatol, (5): p Kornek, M., et al., Circulating microparticles as disease-specific biomarkers of severity of inflammation in patients with hepatitis C or nonalcoholic steatohepatitis. Gastroenterology, (2): p Wolf, P., The nature and significance of platelet products in human plasma. Br J Haematol, (3): p Thery, C., M. Ostrowski, and E. Segura, Membrane vesicles as conveyors of immune responses. Nat Rev Immunol, (8): p Beyer, C. and D.S. Pisetsky, The role of microparticles in the pathogenesis of rheumatic diseases. Nat Rev Rheumatol, (): p Reiner, A.T., et al., Concise Review: Developing Best-Practice Models for the Therapeutic Use of Extracellular Vesicles. Stem Cells Transl Med, (8): p Borger, V., et al., Mesenchymal Stem/Stromal Cell-Derived Extracellular Vesicles and Their Potential as Novel Immunomodulatory Therapeutic Agents. Int J Mol Sci, (7). 2. Becker, A., et al., Extracellular Vesicles in Cancer: Cell-to-Cell Mediators of Metastasis. Cancer Cell, (6): p Hirsova, P., et al., Extracellular vesicles in liver pathobiology: Small particles with big impact. Hepatology, (6): p Brodsky, S.V., et al., Dynamics of circulating microparticles in liver transplant patients. J Gastrointestin Liver Dis, (3): p Lu, L., et al., Abnormal mirnas Targeting Chromosome Open Reading Frame Genes were Enriched in Microvesicles Derived from the Circulation of HCC. Biochem Genet, (2): p Severino, V., et al., Extracellular Vesicles in Bile as Markers of Malignant Biliary Stenoses. Gastroenterology, (2): p e8. 29
30 Extent of intratumoral genomic diversity Augusto Villanueva Icahn School of Medicine, Mont Sinai, New York, United States Despite the clinical efficacy of targeted therapies in HCC, the almost inevitable emergence of acquired drug resistance stands in the way of a definitive cancer cure. The ability of cancer cells to adapt to pharmacological pressures can be described in terms of tumor evolution, and stems from the intrinsic diversity, or heterogeneity of cancer. Cancer heterogeneity refers to the presence of distinct genetic alterations and phenotypes between cancer cells within the same tumor nodule (i.e., intra-tumor heterogeneity (ITH)) or different nodules of the same patient 2. Cells with the same mutation or DNA chromosomal aberration that are not shared by other cells can be grouped into sub-clones. Some mutations provide a fitness advantage and are considered drivers. Multiregional tissue biopsies have been pivotal to reconstruct tumor dynamics and demonstrate clonal evolution. A recent application of this approach in lung cancer found sub-clonal driver mutations in 75% of the 00 tumors analyzed 3 which emphasizes their role in acquired resistance. It also underscores the limitations of single-biopsies to accurately recapitulate the complex mutational landscape of cancer. Even though tumors are complex ecosystems incorporating non-tumoral cells, most ITH studies have disregarded the critical facet of immune selection pressure in cancer progression. Recent exceptions aimed at dissecting the mechanisms underlying immune escape during breast and ovarian cancer progression 4,5. The relevance of delineating tumor-immune interactions is highlighted in light of the current pan-cancer revolution in immunotherapy. Indeed, a phase 2 trial testing the checkpoint inhibitor nivolumab in HCC resulted in a remarkable 20% objective response rate 6, which prompted its recent approval by the FDA in HCC. The landmark study by Gerlinger et al. mapped shared and private mutations in multiple regions of two patients with renal carcinoma 7. This spearheaded a series of investigations to reconstruct phylogenetic relationships of spatially distinct tumor regions. In HCC, many studies describe patterns of ITH that support a clonal evolution model 8. Xue et al. analyzed 43 lesions collected from 0 HCC patients, including primary tumors and intrahepatic metastasis 9. Variable amount of heterogeneity was found among patients, with clonal mutations displaying a wide range from 8-90%. Evidence of both linear and branched evolution was similarly demonstrated in a recent study using sequencing data from multiple regions of 9 HCC patients 0. There is also evidence of neutral evolution driving ITH in HCC. A study utilizing deep sequencing of a densely sampled 3.5 cm HCC (i.e., 309 core biopsies) reported 20 sub-clones, with a distribution of mutations consistent with neutral evolution. Few studies have evaluated the interactions between immune and cancer cells in human samples. A recent study performed an integrated analysis of whole-exome sequencing (WES), gene expression, neo-antigen burden, and T-cell clonality from multiple tumor sites of a heavily treated ovarian cancer patient 4. It demonstrates heterogeneous cancer-immune interactions within the same patient, further questioning the ability of single biopsies to fully recapitulate the tumoral genomic landscape 2. Another paper aimed at dissecting the mechanisms underlying immune escape during breast cancer progression 5. Authors reported a switch to a less active immune environment during the in situ to invasive cancer transition. More intriguing, they found evidence of co-evolution of cancer and immune cells. Single-cell sequencing technologies have emerged as powerful tools to discriminate cell lineages, study differentiation dynamics and discover rare cell types 3. Its application to study cancer heterogeneity uncovered distinct tumor microenvironment patterns in melanoma including cell-to-cell interactions 4, and helped decipher developmental hierarchies in gliomas 5. Interactions of immune and cancer cells have also been evaluated with scrnaseq, as shown in breast 6 and lung cancer 7. In HCC, a recent study 8 confirmed intra-tumor T-cell clonal expansion at the single-cell level, and revealed a highly complex T-cell ecosystem. REFERENCES. McGranahan N, Swanton C. Cancer Evolution Constrained by the Immune Microenvironment. Cell 207;70(5): Alizadeh AA, Aranda V, Bardelli A, et al. Toward understanding and exploiting tumor heterogeneity. Nat Med 205;2(8): Jamal-Hanjani M, Wilson GA, McGranahan N, et al. Tracking the Evolution of Non-Small-Cell Lung Cancer. N Engl J Med [Internet] 207;Available from: 4. Jiménez-Sánchez A, Memon D, Pourpe S, et al. Heterogeneous Tumor-Immune Microenvironments among Differentially Growing Metastases in an Ovarian Cancer Patient. Cell 207;70(5): e20. 30
31 5. Gil Del Alcazar CR, Huh SJ, Ekram MB, et al. Immune Escape in Breast Cancer During In Situ to Invasive Carcinoma Transition. Cancer Discov [Internet] 207;Available from: 6. El-Khoueiry AB, Sangro B, Yau T, et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): an open-label, non-comparative, phase /2 dose escalation and expansion trial. Lancet [Internet] 207;Available from: 7. Gerlinger M, Rowan AJ, Horswell S, et al. Intratumor heterogeneity and branched evolution revealed by multiregion sequencing. N Engl J Med 202;366(0): Craig AJ, von Felden J, Villanueva A. Molecular profiling of liver cancer heterogeneity. Discov Med 207;24(3): Xue R, Li R, Guo H, et al. Variable Intra-Tumor Genomic Heterogeneity of Multiple Lesions in Patients With Hepatocellular Carcinoma. Gastroenterology 206;50(4): Zhai W, Lim TK-H, Zhang T, et al. The spatial organization of intra-tumour heterogeneity and evolutionary trajectories of metastases in hepatocellular carcinoma. Nat Commun 207;8: Ling S, Hu Z, Yang Z, et al. Extremely high genetic diversity in a single tumor points to prevalence of non-darwinian cell evolution. Proc Natl Acad Sci U S A 205; McGranahan N, Swanton C. Clonal Heterogeneity and Tumor Evolution: Past, Present, and the Future. Cell 207;68(4): Grün D, van Oudenaarden A. Design and Analysis of Single-Cell Sequencing Experiments. Cell 205;63(4): Tirosh I, Izar B, Prakadan SM, et al. Dissecting the multicellular ecosystem of metastatic melanoma by single-cell RNA-seq. Science 206;352(6282): Tirosh I, Venteicher AS, Hebert C, et al. Single-cell RNA-seq supports a developmental hierarchy in human oligodendroglioma. Nature 206;539(7628): Chung W, Eum HH, Lee H-O, et al. Single-cell RNA-seq enables comprehensive tumour and immune cell profiling in primary breast cancer. Nat Commun 207;8: Lavin Y, Kobayashi S, Leader A, et al. Innate Immune Landscape in Early Lung Adenocarcinoma by Paired Single-Cell Analyses. Cell 207;69(4): e7. 8. Zheng C, Zheng L, Yoo J-K, et al. Landscape of Infiltrating T Cells in Liver Cancer Revealed by Single-Cell Sequencing. Cell 207;69(7): e6. 3
32 Telomerase activation Jean Charles Nault INSERM, Paris, France Hepatocarcinogenesis is a multistep process starting with the exposure to different risk factors, followed by the development of a chronic liver disease and cirrhosis precede in the vast majority of the cases the development of HCC. Several lines of evidence have underlined the pivotal role of telomere maintenance in both cirrhosis and HCC pathogenesis. TERT promoter mutations were identified as the most frequent genetic alterations in hepatocellular carcinoma with an overall frequency around 60%. Other mechanisms of telomerase reactivation were viral insertional mutagenesis in TERT and amplification or translocation of the TERT gene. Moreover, in cirrhosis, TERT promoter mutations are observed at the early steps of hepatocarcinogenesis since they are recurrently identified in low grade and high grade dysplastic nodules. In contrast, acquisition of genomic diversity through mutations of classical oncogenes and tumor suppressor genes (TP53, CTNNB, ARIDA ) occurred only in progressed HCC. In normal liver, a subset of HCC can be derived from the malignant transformation of hepatocellular adenoma (HCA). In HCA, CTNNB mutations predispose to transformation of HCA in HCC and TERT promoter mutations are required in most of the cases as a second hit for a full malignant transformation. All these findings have refined our knowledge of HCC pathogenesis and have pointed telomerase as a target for tailored therapy in the future. 32
33 WNT/ß-catenin activation Sabine Colnot INSERM, Paris, France One third of HCCs have activating mutations of the CTNNB gene encoding β-catenin. These tumors have unique transcriptomic, histological and metabolic features. β-catenin activation in hepatocytes also leads to a unique epigenetic landscape, correlated with metabolic changes. Recent work of the lab has focused on the impact of mutational activation of the β-catenin pathway in the liver on choline metabolism, and as a consequence on DNA methylation status of the tumors. This study demonstrates that a simple non-invasive routine FCH-PET imaging can be used to genotype β- catenin-mutated HCCs. Increases in the uptake and use of dietary choline have specific consequences in tumoural hepatocytes displaying β-catenin activation, and can therefore be seen as a treatment target for this category of HCCs. 33
34 Epigenetic targets in hepatocarcinogenesis Matías Avila Hepatology Program, CIBERehd, IdiSNA, CIMA, University of Navarra, Spain Hepatocellular carcinoma (HCC) usually develops on a background of inflammation and fibrosis. Environmental factors trigger adaptative epigenetics mechanisms, including alterations in DNA methylation or post-translational modification of histones, which control gene expression and cellular behaviour. Many of the enzymes carrying out these epigenetic events, such as DNA and histone methyltransferases, present altered expression and activity in chronic liver disease and HCC. Histones and DNA methylation are dynamic enzymatic processes amenable to pharmacological intervention. Euchromatic histone-lysine N-methyltransferase 2 (EHMT2/G9a) is a histone methyltransferase specific for histone H3K9 mono- and di-methylation. G9a is also important for the establishment of DNA methylation patterns. However, information on the functional roles of G9a in hepatocarcinogeneis is limited. We characterized the expression and clinical significance of G9a in human HCC and its association with other epigenetic effectors, such as DNMT and UHRF. We have developed new firstin-class small molecule dual inhibitors of G9a and DNMT with novel mechanism of action, and evaluated their therapeutic activity in HCC models. G9a, DNMT and UHRF expression was examined in non-tumoral and tumoral human livers and in murine models. The effects of G9a and DNMT expression/activity inhibition was studied in HCC cell lines and human hepatic stellate cells (HSCs). Antitumoral effects of G9a/DNMT inhibitors were evaluated in vitro and in xenograft models. G9a expression is increased in human HCC correlating with DNMT and UHRF and with poor patients prognosis. G9a expression is higher in human HCC cell lines than in normal human hepatocytes, increases during mouse HSCs activation in culture and in mouse models of fibrosis-associated HCC. sirna-mediated G9a and DNMT knockdown markedly inhibited HCC cells growth and HSCs fibrogenic activation. CM272, our lead G9a/DNMT specific inhibitor, showed GI50 values in the nm range towards HCC cell lines. CM272 presented a good safety profile in vivo, and potent antifibrotic properties both in vitro and in an in vivo. CM-272 displayed a remarkable antitumoral effect over several HCC cell lines, and in clinically relevant xenograft models of HCC. Mechanistically, CM272 inhibited HSC activation and pro-fibrogenic transdifferentiation, reversed the pro-tumorigenic metabolic reprogramming of HCC cells and their adaptation to hypoxia We have shown that G9a plays an important role in both liver fibrogenesis and HCC growth. Our stduy suggests that the pharmacologic interference with G9a/DNMT may be a novel strategy for the development of effective therapies in fibrosis-associated HCC. 34
35 The Hippo/YAP signalling pathway in liver tumor initiation and progression Kai Breuhahn Institute of Pathology, University Hospital Heidelberg, Heidelberg, Germany The Hippo pathway and its negatively regulated downstream effector yes-associated protein (YAP) are key regulators of tissue homeostasis and their dysregulation has been implicated in liver cancer development. This talk is focusing on two key aspects of Hippo/YAP biology in the process of hepatocarcinogenesis. First, we describe the cell autonomous mechanisms how YAP induces tumor formation. For this, YAP together with TEAD4 stimulates the transcription of FOXM to drive chromosomal instability (CIN) gene expression by the formation of a YAP/TEAD4/FOXM complex. Overexpression of YAP is sufficient to induce CIN signature gene expression, nuclear polymorphisms, aneuploidy and pathological mitosis in hepatocytes and tumor cells of YAP 27A transgenic mice. The perturbation of FOXM activity using the inhibitor Thiostrepton attenuated the YAP-induced hepatomegaly and reduced CIN gene expression highlighting its therapeutic potential to block YAP-dependent oncogenic properties. Moreover, HCC patients with nuclear enrichment of YAP show a positive correlation with CIN gene expression and higher frequency of chromosomal alterations. Second, YAP activation in tumor cells regulates the microenvironment through the secretion paracrineacting factors. Time-resolved expression profiling of primary endothelial cell subpopulations (liver sinusoidal endothelial cells; LSECs vs. capillary endothelial cells (CECs) revealed dynamic transcriptome changes in the process of YAP 27A -induced hepatomegaly and tumorigenesis. The communication between LSECs and CECs is partly mediated by the HGF/c-MET signaling axis and regulated by YAP-induced expression of Osteopontin (OPN). Indeed, perturbation of c-met activity on CECs by Cabozantinib blocked the observed morphological changes detected in YAP 27A mice. 35
36 Is there a role for Contrast Enhanced Ultra Sound (CEUS) for improving the diagnostic accuracy of imaging techniques? The hepatologist view Fabio Piscaglia, Francesca Benevento, Francesco Tovoli Unit of Internal Medicine, Bologna Liver Oncology Group (BLOG), Department of Medical and Surgical Science, Italy fabio.piscaglia@unibo.it CT and MRI are the reference imaging techniques for the characterization of focal liver lesions in cirrhosis, thanks to their diagnostic capacity and for providing a panoramic overview of the liver and of the upper abdomen able to stage HCC before treatment allocation, with MRI being more multiparametric and slightly more sensitive for HCC in case of small lesions. The hallmark diagnostic pattern for the characterization as HCC is considered to be arterial phase hyperenhancement followed by washout appearance (Piscaglia F, et al. Ultraschall Med. 207 ;38:9 ). Contrast enhanced ultrasound (CEUS) had been initially included among the dagnostic imaging technique for HCC in 2005, but later removed for the reported risk of misdiagnosis with cholangiocarcinoma, when the hallmark pattern is adopted with no dedicated refinement (Vilana et al, Hepatology 200; Galassi M et al, Liver International 203). Such misdiagnosis can be estimated however to occur in no more thanl % of focal liver lesions arisen in cirrhosis and in no more than 2% of liver malignancies, but even such small numbers are held of relevance, expecially in the setting of transplantation and systemic therapy. A recent refinement of the typical hallmark patterns of HCC at CEUS has been proposed by the American College of Radiology within the Liver Imaing Reporting And Data System (LI RADS) project. The refinement was designed to aim to minimize the risk of misdiagnosis and consist in helding as typical for HCC only a washout appearance with onset after 60 seconds post-injectiong and of mild degree at around 2 minutes. Only when arterial hyperenhancement is followed by this specific washout pattern a lesion can be considered HCC, otherwise, in case of early or marked washout it has to be called malignant of uncertain cellular origin. A large retrospective study in more than 000 nodules validated this proposal (Terzi et al, 208 e-pub), showing an almost nullified risk of misdiagnosis with a limited decrease in sensitivity (from 67% to 62% of all nodules). Nonetheless, CEUS cannot be considered as a stand alone technique in first imaging line, because it lacks panoramicity and does not always well explore the liver dome or other parts of the liver in a number of patients (overweight / obese, fatty liver, wide chest, etc). Despite its limitations CEUS has several advantages: it works in real time, recognizing also transient and short lasting enhancement abormalities, it hardly suffer from poor patient cooperation in the arterial phase, it hardly suffers from false positive findings of non lesional arterial hyperenhancement, since the study starts from prevoiusly detected nodules, the contrast agent is excreted though the lungs and has no contraindication even for repeat exams in the very short time, it can be utilized at the bedside or immediately after lesion detection during surveillance even by non radiologists, it can identify specific enhancing lesions by using the same expected approach to be utilized for subsequent interventional procedures (diagnostic or therapeutical) thus judging their feasibility and the diagnostic capacity to characterize liver nodules well explorable at ultrasound is very high adopting the LI RADS criteria. In particular, in connection to the last point, it does not suffer the risk of misdiagnosis of benign versus malignant lesions in case of cholangiocarcinoma (differently from MRI and CT, in which cholangiocarcinoma tipically does not show washout at all). Worth to mention that the LI RADS system and the guidelines of EFSUMB (European Federation of Societies for Ultrasound in Medicine and Biology) also include the characterization of tumor venous invasion. Indeed, the characterization of portal thrombosis is extremely accurate with ultrasound plus CEUS, even more accurate than with CT and MRI in the instance of intrahepatic involvement (Claudon et al, Ultraschall Med. 203;34:-29). To this end, tumor venous invasion nearly invariable occurs at an intrahepatic level and is therefore accurately diagnosed by ultrasound. To summarize, CEUS can be of high value for the hepatologist in the following diagnostic settings in cirrhotic patients either to improve the diagnostic accuracy of CT/MRI or replace them when contraindicated: ) characterization of liver nodules which have received non diagnostic or technically suboptimal CT or MRI (expecially in case of breath motion artifacts in the arterial phase, which is reported to occur at higher incidence with Gadoxeate disodium) (Well L, Rofo. 208;90:20-30) or in case of inadequate contrast injection with CT/MRI. 2) Characterization of benign vs malignat nodules with inconclusive CT/MRI and suspected cholangiocarcinoma (hyperenhancement in the venous phase not without other characteristics of hemangioma) in regions unsuitable for biopsy 36
37 3) Characterization of focal liver lesions in patients with compromized renal function contraindicating CT/MRI contrast injection 4) Characterization of focal liver lesions in patients with personal conditions contraindicating MRI (claustrophobia, metallic foreign bodies, allergy to contrast agents) or CT (hyperthiroidism, allergy to iodinated contrast agents, etc). 5) Characterization of intrahepatic portal thrombosis in combination with CT/MRI according to accepted accurate diagnostic criteria 6) Choice of the correct target lesion for ultrasound guided biopsy in case of non diagnostic CT/MRI but with a greater cancer suspicion in specific nodules among several ones. 7) For pre-ablation assessment in order to allow precise comparison with the post-treatment appearance to guide the need of immediate retreatment and maximize the rate of complete ablation, improving the outcome at the -mont post-ablation CT/MRI REFERENCES Bruix J, Sherman M; Practice Guidelines Committee, American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma. Hepatology Nov;42(5): Claudon M, Dietrich CF, Choi BI, Cosgrove DO, Kudo M, Nolsøe CP, Piscaglia F, Wilson SR, Barr RG, Chammas MC, Chaubal NG, Chen MH, Clevert DA, Correas JM, Ding H, Forsberg F, Fowlkes JB, Gibson RN, Goldberg BB, Lassau N, Leen EL, Mattrey RF, Moriyasu F, Solbiati L, Weskott HP, Xu HX. Guidelines and good clinical practice recommendations for contrast enhanced ultrasound (CEUS) in the liver update 202: a WFUMB-EFSUMB initiative in cooperation with representatives of AFSUMB AIUM, ASUM, FLAUS and ICUS. Ultraschall Med. 203 Feb;34():-29 Galassi M, Iavarone M, Rossi S, Bota S, Vavassori S, Rosa L, Leoni S, Venerandi L, Marinelli S, Sangiovanni A, Veronese L, Fraquelli M, Granito A, Golfieri R, Colombo M, Bolondi L, Piscaglia F. Patterns of appearance and risk of misdiagnosis of intrahepatic cholangiocarcinoma in cirrhosis at contrast enhanced ultrasound. Liver Int. 203 May;33(5):77-9 Kim TK, Noh SY, Wilson SR, Kono Y, Piscaglia F, Jang HJ, Lyshchik A, Dietrich CF, Willmann JK, Vezeridis A, Sirlin CB. Contrast-enhanced ultrasound (CEUS) liver imaging reporting and data system (LI-RADS) a review of important differences compared to the CT/MRI system. Clin Mol Hepatol. 207 Dec;23(4): Piscaglia F, Gianstefani A, Ravaioli M, Golfieri R, Cappelli A, Giampalma E, Sagrini E, Imbriaco G, Pinna AD, Bolondi L; Bologna Liver Transplant Group. Criteria for diagnosing benign portal vein thrombosis in the assessment of patients with cirrhosis and hepatocellular carcinoma for liver transplantation. Liver Transpl. 200 May;6(5): Piscaglia F, Wilson SR, Lyshchik A, Cosgrove D, Dietrich CF, Jang HJ, Kim TK, Salvatore V, Willmann JK, Sirlin CB, Kono Y. American College of Radiology Contrast Enhanced Ultrasound Liver Imaging Reporting and Data System (CEUS LI-RADS) for the diagnosis of Hepatocellular Carcinoma: a pictorial essay. Ultraschall Med. 207 Jun;38(3): Rossi S, Ghittoni G, Ravetta V, Torello Viera F, Rosa L, Serassi M, Scabini M, Vercelli A, Tinelli C, Dal Bello B, Burns PN, Calliada F. Contrast-enhanced ultrasonography and spiral computed tomography in the detection and characterization of portal vein thrombosis complicating hepatocellular carcinoma. Eur Radiol Aug;8(8): Tarantino L, Francica G, Sordelli I, Esposito F, Giorgio A, Sorrentino P, de Stefano G, Di Sarno A, Ferraioli G, Sperlongano P. Diagnosis of benign and malignant portal vein thrombosis in cirrhotic patients with hepatocellular carcinoma: color Doppler US, contrast-enhanced US, and fine-needle biopsy. Abdom Imaging Sep-Oct;3(5): PubMed PMID: Terzi E, Iavarone M, Pompili M, Veronese L, Cabibbo G, Fraquelli M, Riccardi L, De Bonis L, Sangiovanni A, Leoni S, Zocco MA, Rossi S, Alessi N, Wilson SR, Piscaglia F; CEUS LI-RADS Italy study group collaborators:. Contrast ultrasound LI-RADS LR-5 identifies hepatocellular carcinoma in cirrhosis in a multicenter restropective study of,006 nodules. J Hepatol. 207 Nov. pii: S (7) doi: 0.06/j.jhep [Epub ahead of print] Vilana R, Forner A, Bianchi L, García-Criado A, Rimola J, de Lope CR, Reig M, Ayuso C, Brú C, Bruix J. Intrahepatic peripheral cholangiocarcinoma in cirrhosis patients may display a vascular pattern similar to hepatocellular carcinoma on contrast-enhanced ultrasound. Hepatology. 200 Jun;5(6):
38 How to best diagnose HCC? Do we need hepatobiliary MR contrast agents? The radiologist view Christophe Aubé Department of Radiology, University hospital of Angers, Angers, France A diagnosis of HCC by non-invasive imaging modalities is accepted when a nodule on cirrhosis shows the typical hallmark i.e. a combination of arterial phase hyper enhancement and wash-out on portal venous and/or delayed phases, This non-invasive diagnosis is possible because of the peculiar vascular derangement occurring during multi-step hepatic carcinogenesis and by the high probability of HCC in cirrhosis. In studies comparing ultrasound, contrast enhanced ultrasound (CEUS), computed tomography (CT) and magnetic resonance imaging (MRI) the sensitivity of MRI was higher than that of other techniques. Specificity was higher using MR and CEUS but often not significantly. An important point is that results vary according to HCC size (sensitivity of 48% and 62% for CT and MRI in tumours smaller than 20 mm vs. 92% and 95% for CT and MRI in tumours larger than 20 mm) (Lee radiology 203). In a recent prospective multicentric study in a series of 544 nodules MRI using extracellular contrast agents shows a sensitivity and specificity of 72.3% and 89.4% in lesions between mm and 70.6% and 83.2% in the 0-20 mm lesions (Aube liver inter 207). These results confirm the higher performance of MRI for the diagnosis of HCC but highlight the quite low sensitivity of the technique and the limited performance for the diagnosis of small nodules. In the way to improve diagnosis, combination or substitution of the typical feature by complementary or alternative MR feature (T, T2 or DWI hypersignal, capsula, fat content) have been tested. But none of these combinations provide better diagnosis performance than typical features. Hepatospecific contrast agent especially Gd-EOB-DTPA (gadoxetic acid) in addition to its distribution in the extracellular space (as any Gadolinium), has approximately 50% of the administered dose actively taken up by hepatocytes via the organic anion transporting polypeptide 8 (OATP8) and excreted into the bile duct via the multidrug resistance protein 2 (MRP2). The other 50% are eliminated by renal excretion. Maximum hepatocytes uptake (hepatobiliary biliary phase - HBP) is reach in about 20 minutes after intravenous injection. Therefore, Hepatospecific contrast agent provide information about the vascular phases, and additional information regarding the HBP. At this phase normal hepatic parenchyma is enhanced, but most HCCs (88 to 95%) appear as hypointense nodules. The hepatocyte uptake of Gd-EOB-DTPA is quite quick, indeed at the classical delayed phase (3 minutes) the normal parenchyma is already enhanced via this uptake. Consequently, it is not possible to attribute the hyposignal of a nodule to a real WO or to a default of hepatospecific agent uptake. Therefore, on a MRI performed with Gd-EOB-DTPA this 3 min phase is named transitional phase instead of delayed phase and is no more taken in consideration to define the typical WO. On another hand, taking in account not only typical hallmark but also hypointensity on the transitional phase and/or the hepatobiliary phase as an alternative to classical WO, the sensitivity for the diagnosis of HCC is increased (85-90%) but consequently the specificity decreased. The increase of sensitivity is particularly significant for small nodules. It is important to notice that all hypointense nodules in HBP are not HCC. Kwon et al. (abdominal imaging 204) have reported that 67% of benign nodules showed hypointensity in the HBP. Non-hypervascular and HBP hypointense nodules have specific interest since they seem able to progress to HCC. In recent studies, it has been show that approximately 30% of non-hypervascular and HBP hypointense nodules become hypervascular HCCs during a follow-up period of one year. In addition, associated risk factors to change of this non-hypervascular HBP hypointense nodules to hypervascular HCCs have been defined. They include nodule size larger than 0mm, rapid doubling time of the tumour volume, hyperintensity on T2 or T or diffusion weighted imaging and intratumoural fat components. Therefore Gd-EOB-DTPA could become a prognostic biomarker of HCC and be used to determine more appropriate strategies for follow-up. Specific contrast agents are heterogeneously introduced in the international guide lines. In the present EASL and AASLD recommendations they are not cited. In the Liver Reporting and Data System (LIRADS) HBP hypointensity is an ancillary feature favouring malignancy. It allows to upgrade by category the nodule but not to class it LR5 (the class that define the certain diagnosis of HCC). 38
39 Therefore, its rule remains limited. In Korean (KLCSG-NCC), Japanese (JSH) and Asiatic (APASL) guidelines Gd-EOB-DTPA enhanced MRI as well as dynamic CT or MRI with extracellular contrast media as primary diagnostic tests for the noninvasive diagnosis of HCC. Therefore Gd-EOB-DTPA could contribute to increased sensitivity, this could be at a cost of losing specificity. This difference in the western and Eastern guidelines may have been caused by the wishes to promote either higher sensitivities or specificities of the imaging modalities for HCC. 39
40 Is biopsy adding clinically relevant information? The pathologist view Valérie Paradis Pathology Dpt, Beaujon hospital & INSERM UMR 49, Paris, France Clinically information provided by biopsy may be relevant in several aspects:. Diagnostic issue: Indications of biopsy in cirrhotic patients with hepatocellular carcinoma (HCC) are restricted to atypical nodules on imaging. This mostly concerns diagnosis of small size nodules (<2 cm) for which imaging may fail to differentiate preneoplastic (dysplastic nodules) which should be followed from malignant nodules (very early HCC) which should be treated []. Biopsy of small nodules arising on cirrhosis is still challenging on biopsy, and although the use of immunophenotypical markers has been shown helpful [2,3], more sensitive molecular markers are needed. The development of liquid biopsy will potentially provide non invasive biomarkers for improving diagnosis, such as the detection of circulating tumour DNA methylation marker [4]. Primary liver malignancies define a large spectrum of tumors from HCC to cholangiocarcinoma. In between, the diagnosis of mixed hepatobiliary carcinoma seems to be more and more recognized [5]. While its diagnosis may impact on clinical management, histology remains the gold standard as imaging is not enough performant. With the significant advances provided by molecular approaches, allowing identification of different subtypes [6], diagnosis of hepatocholangiocarcinoma may be suggested on biopsy. 2. Prognostic issue: Genetic complexity of HCC represents a significant drawback for translating into clinical practice the different available molecular classifications that identify distinct phenotypes. Nevertheless, some morphological features have been shown their prognostic relevance, such as the macrotrabecular pattern or presence of vascular invasion [7,8]. While the macrotrabecular pattern may be assessed on biopsy, surrogate markers of vascular invasion are needed. 3. Theranostic issue: Therapeutic options for cirrhotic patients with HCC are various, ranging from surgery to targeted therapies. Given the policy not to biopsy HCC and despite the wellcharacterized molecular picture of HCC, very few biomarkers able to predict response to therapy have been identified or validated when characterized [9]. References [] International Consensus Group for Hepatocellular NeoplasiaThe International Consensus Group for Hepatocellular Neoplasia. Pathologic diagnosis of early hepatocellular carcinoma: a report of the international consensus group for hepatocellular neoplasia. Hepatol Baltim Md 2009;49: doi:0.002/hep [2] Di Tommaso L, Destro A, Seok JY, Balladore E, Terracciano L, Sangiovanni A, et al. The application of markers (HSP70 GPC3 and GS) in liver biopsies is useful for detection of hepatocellular carcinoma. J Hepatol 2009;50: doi:0.06/j.jhep [3] Tremosini S, Forner A, Boix L, Vilana R, Bianchi L, Reig M, et al. Prospective validation of an immunohistochemical panel (glypican 3, heat shock protein 70 and glutamine synthetase) in liver biopsies for diagnosis of very early hepatocellular carcinoma. Gut 202;6:48 7. doi:0.36/gutjnl [4] Xu R-H, Wei W, Krawczyk M, Wang W, Luo H, Flagg K, et al. Circulating tumour DNA methylation markers for diagnosis and prognosis of hepatocellular carcinoma. Nat Mater 207;6:55 6. doi:0.038/nmat4997. [5] Brunt E, Aishima S, Clavien P-A, Fowler K, Goodman Z, Gores G, et al. chcc-cca: Consensus terminology for primary liver carcinomas with both hepatocytic and cholangiocytic differentation. Hepatol Baltim Md 208. doi:0.002/hep [6] Moeini A, Sia D, Zhang Z, Camprecios G, Stueck A, Dong H, et al. Mixed hepatocellular cholangiocarcinoma tumors: Cholangiolocellular carcinoma is a distinct molecular entity. J Hepatol 207;66: doi:0.06/j.jhep [7] Ziol M, Poté N, Amaddeo G, Laurent A, Nault J-C, Oberti F, et al. Macrotrabecular-massive hepatocellular carcinoma: A distinctive histological subtype with clinical relevance. Hepatol Baltim Md 207. doi:0.002/hep [8] Poté N, Cauchy F, Albuquerque M, Cros J, Soubrane O, Bedossa P, et al. Contribution of virtual biopsy to the screening of microvascular invasion in hepatocellular carcinoma: A pilot study. Liver Int Off J Int Assoc Study Liver 207. doi:0./liv
41 [9] Sciarra A, Ronot M, Di Tommaso L, Raschioni C, Castera L, Belghiti J, et al. TRIP: a pathological score for transarterial chemoembolization resistance individualized prediction in hepatocellular carcinoma. Liver Int Off J Int Assoc Study Liver 205;35: doi:0./liv
42 What is the role of biomarkers in diagnosis, prognosis and surveillance? Franco Trevisani University of Bologna, Bologna, Italy Biomarkers are molecules measurable in body fluids, tissues or cells that can predict the risk of cancer development, and/or reveal the presence of a subclinical (asymptomatic) disease, and/or confirm/exclude tumor presence when it is clinically suspected. The biomarkers utilized in oncology are called oncomarkers. They can be used as a surveillance test or as a complementary diagnostic tool when imaging techniques detect lesions to be characterized. Blood/urine marker measurement, since it is non-invasive, economic and objective, may have great diagnostic value, provided that a suitable diagnostic accuracy is achieved. Some oncomarkers also provide information about tumor response to treatment, and have a prognostic meaning, as they are highly overexpressed in aggressive tumors. A great number of oncomarkers have been proposed and tested in the setting of hepatocellular carcinoma (HCC) (, 2). The most studied are alpha-fetoprotein (AFP), its isoform AFP-L3, and Desgamma-Carboxy Prothrombin (DCP), but many other molecules can be taken into account, including Glypican 3, Glutamine synthase, HSP70 (tissue), Cytokeratin 9, Golgi protein 73, Midkine, Osteopontin, Squamous Cell Carcinoma Antigen (SCCA), Annexin A2, Fibroblast Growth Factor 3/4 (FGF3/4, )micro-rnas, cell-free DNA and biomarkers obtained by proteomic-based approaches. In addition, genetic signatures can be also included among oncomarkers with prognostic meaning. Only AFP has reached the phase 5 of biomarker development (prospective randomized studies) aimed at defining the utility of biomarkers, but its use in clinical practice is mainly limited by an unsatisfactory sensitivity (around 65%) at cut-off values maintaining a sufficiently high specificity (3,4). Moreover, most studies on HCC biomarkers have a two-gate design (comparison with control group(s) without HCC) instead of the more appropriate one-gate design (all comers with suspected HCC are consecutively enrolled to ensure a prevalence similar to that of clinical practice). Finally, these studies usually suffer from the verification bias since the reference standard (CT scan or MRI) to exclude the tumor presence in non-hcc cases was not performed in all subjects. Based on the available evidence, the current scenario regarding oncomarkers for HCC can be summarized as follow: The measurement every 3-6 months of serum AFP or the combination of AFP+ALP-P3+DCP is included in the diagnostic algorhythm of hepatic nodules by Oriental guidelines for HCC management, but not by Western guidelines. Immunohistochemical measurement of Glypican 3, Glutamine synthase and HSP70 is recommended by European guidelines as a useful tool to distinguish well differentiated HCC from dysplastic nodules. AFP and SCCA may predict the risk of HCC in patients with chronic liver disease (5, 6). AFP level has been incorporated in a number of staging systems for HCC patients, such as CLIP, CUPI, GRETCH, and MESIAH. AFP has been incorporated in nomograms or calculators to predict the outcome of hepatic resection (7) and transplantation (8). FGF3/4 amplification has shown to predict response to sorafenib (9). Changes in AFP levels predict the outcome of patients treated with transarterial therapies (0) or Sorafenib (, 2), and a decrement of circulating SCCA-IgM after locoregional or systemic treatments marks a positive radiological response (3). The monitoring of cell-free DNA in the urine has been recently reported to be a promising tool to predict HCC recurrence (4). A good prognostic ability has been also reported for some genetic signatures obtained from tumoral specimens (5, 6). None of the new oncomarkers outperform the conventional ones in such a way that it has been widely adopted in clinical practice. The diagnostic accuracy, particularly for early stage HCC, can be improved combining two or more oncomarkers. This can allow to reach an acceptable (>80%) sensitivity with a modest decrement in specificity (7, 8). For this purpose, the accuracy can be also improved measuring the over time variability of the oncomarker (9, 4). However, all these proposals are waiting for prospective and external validations, and there are no recommended recall policies based on biomarker 42
43 combinations or variability for the surveillance of patients at risk of developing HCC. Moreover, no biomarker combination is considered to be reliable enough to diagnose a lesion as HCC without confirmatory histological or radiological features. References. Lou J, Zhang L, Lv S, Zhang C, Jiang S. Biomarkers for hepatocellular carcinoma. Biomark Cancer. 207;9:-9. doi: 0.77/79299X eCollection Chaiteerakij R, Addissie BD, Roberts LR. Update on biomarkers of hepatocellular carcinoma. Clin Gastroenterol Hepatol. 205;3(2): doi:0.06/j.cgh Marrero JA, Feng Z, Wang Y, Nguyen MH, Befeler AS, Roberts LR, et al. Alpha-fetoprotein, des-gamma carboxyprothrombin, and lectin-bound alpha-fetoprotein in early hepatocellular carcinoma. Gastroenterology. 2009;37(): Biselli M, Conti F, Gramenzi A, Frigerio M, Cucchetti A, Fatti G, et al. A new approach to the use of α-fetoprotein as surveillance test for hepatocellular carcinoma in patients with cirrhosis. Br J Cancer. 205;2(): Sangiovanni A, Del Ninno E, Fasani P, De Fazio C, Ronchi G, Romeo R, Morabito A, et al. Increased survival of cirrhotic patients with a hepatocellular carcinoma detected during surveillance. Gastroenterology. 2004;26(4): Pontisso P, Quarta S, Caberlotto C, Beneduce L, Marino M, Bernardinello E, et al. Progressive increase of SCCA-IgM immune complexes in cirrhotic patients is associated with development of hepatocellular carcinoma. Int J Cancer. 2006;9(4): Li C, Shen JY, Zhang XY, Peng W, Wen TF, Yang JY, Yan LN. Predictors of Futile Liver Resection for Patients with Barcelona Clinic Liver Cancer Stage B/C Hepatocellular Carcinoma. J Gastrointest Surg. 207 Nov 8. doi: 0.007/s Mazzaferro V, Sposito C, Zhou J, Pinna AD, De Carlis L, Fan J, et al. Metroticket 2.0 Model for Analysis of Competing Risks of Death After Liver Transplantation for Hepatocellular Carcinoma.Gastroenterology. 208;54(): Arao T, Ueshima K, Matsumoto K, Nagai T, Kimura H, Hagiwara S, et al. FGF3/FGF4 amplification and multiple lung metastases in responders to sorafenib in hepatocellular carcinoma. Hepatology. 203 Apr;57(4): Memon K, Kulik L, Lewandowski RJ, Wang E, Ryu RK, Riaz A, et al. Alpha-fetoprotein response correlates with EASL response and survival in solitary hepatocellular carcinoma treated with transarterial therapies: a subgroup analysis. J Hepatol. 202;56(5): Personeni N, Bozzarelli S, Pressiani T, Rimassa L, Tronconi MC, Sclafani F, et al. Usefulness of alpha-fetoprotein response in patients treated with sorafenib for advanced hepatocellular carcinoma. J Hepatol. 202;57(): Nakazawa T, Hidaka H, Takada J, Okuwaki Y, Tanaka Y, Watanabe M, et al. Early increase in α-fetoprotein for predicting unfavorable clinical outcomes in patients with advanced hepatocellular carcinoma treated with sorafenib. Eur J Gastroenterol Hepatol. 203 Jun;25(6): Guarino M, Di Costanzo GG, Gallotta A, Tortora R, Paneghetti L, Auriemma F, et al. Circulating SCCA-IgM complex is a useful biomarker to predict the outcome of therapy in hepatocellular carcinoma patients. Scand J Clin Lab Invest. 207 Oct;77(6): Hann HW, Jain S, Park G, Steffen JD, Song W, Su YH. Detection of urine DNA markers for monitoring recurrent hepatocellular carcinoma. Hepatoma Res. 207;3:05 5. Nault JC, De Reyniès A, Villanueva A, Calderaro J, Rebouissou S, Couchy G, et al. A hepatocellular carcinoma 5-gene score associated with survival of patients after liver resection. Gastroenterology. 203;45(): Villa E, Critelli R, Lei B, Marzocchi G, Cammà C, Giannelli G, et al. Neoangiogenesis-related genes are hallmarks of fast-growing hepatocellular carcinomas and worst survival. Results from a prospective study. Gut. 206;65(5): Lok AS, Sterling RK, Everhart JE, Wright EC, Hoefs JC, Di Bisceglie AM, Morgan TR, Kim HY, Lee WM, Bonkovsky HL, Dienstag JL; HALT-C Trial Group.Des-gamma-carboxy prothrombin and alpha-fetoprotein as biomarkers for the early detection of hepatocellular carcinoma. Gastroenterology. 200;38(2): Chen H, Chen S, Li S, Chen Z, Zhu X, Dai M, Kong L, Lv X, Huang Z, Qin X. Combining desgamma-carboxyprothrombin and alpha-fetoprotein for hepatocellular carcinoma diagnosing: an update meta-analysis and validation study. Oncotarget. 207;8(52): Lee E, Edward S, Singal AG, Lavieri MS, Volk M. Improving screening for hepatocellular carcinoma by incorporating data on levels of α-fetoprotein, over time. Clin Gastroenterol Hepatol. 203 Apr;(4):
44 Development of tumor markers for diagnosis, prognosis and tumor response prediction Josep M. Llovet 2 3 Liver Cancer Translational Research Laboratory, Barcelona Clinic Liver Cancer Group (BCLC), Liver Unit, IDIBAPS, Hospital Clínic, University of Barcelona, Barcelona, Spain, 2 Mount Sinai Liver Cancer Program, Icahn School of Medicine at Mount Sinai, Mount Sinai School of Medicine, New York, NY, United States, 3 Institució Catalana de Recerca i Estudis Avançats (ICREA), Barcelona, Spain jmllovet@clinic.ub.es Advances in genomics have improved our understanding of the biology of HCC. Translational research efforts are focused on specific clinical situations that would benefit from a comprehensive molecular analysis Biomarkers defining HCC risk assessment HCC usually arises on a previously damaged liver. The annual incidence of HCC in cirrhotic patients is 3-5% and one third of them will develop a tumor over their lifespan, representing also the leading cause of death among them. Aside of the classical clinic-pathological markers for defining high risk in cirrhotic patients, such as platelet count and bilirubin, two biomarkers have been proposed: a) a single nucleotide polymorphisms (SNPs) in germ-line EGF associated with HCC on HCV-related cirrhosis. Also, specific 86 gene signature defining high risk of HCC development in cirrhotic patients has been developed. Biomarkers for HCC diagnosis Non-invasive diagnosis using EASL/AASLD criteria allows a confidential diagnosis of most HCCs above 2cm. However, imaging is less reliable in one third of small nodules and a liver biopsy is often indicated. In this scenario, EASL guidelines recommend testing the combination of 3 immunohistochemical markers (GPC3, HSP70 and glutamine synthase). In addition, a 3-gene signature including GPC3, LYVE and survivin has also been proposed as an accurate molecular tool (sensitivity of 95% and specificity of 94%) to discriminate dysplastic nodules and HCC smaller than 2cm in the setting of HCV etiology. A step forward in the diagnosis of HCC could be provided by the development of a liquid biopsy, i.e., the identification in the peripheral circulation of circulating tumor cells (CTCs) or circulating tumor DNA (ctdna) that have detached from a primary tumor. A recent paper reported preliminary data in 8 tumor types, including HCC. Prognostic biomarkers. Plasma AFP level have been used for the assessment of HCC prognosis in different clinical stages, and has been adopted for prognostic stratification at a cut-off of 200 or 400 ng/dl as predictor of drop-out in the list of transplantation, and as stratification factor in phase III trials testing systemic therapies. In terms of prognostic signatures, from the tumor, a 5-gene score based on the expression of TAF9, RAN, RAMP3, KRT9 and HN genes, represents the strongest predictor of survival after liver resection identified so far in multiple cohorts (8). Also, a 86 gene from adjacent tumoral tissue was shown to have independent prognostic significance to predict overall survival in HCC patients. Predictors of response to therapeutic targets Sorafenib has been the standard of care for patients with advanced HCC for the last decade. High levels of c- Kit and low levels of HGF showed a non-significant trend towards better sorafenib efficacy. Similarly patients with HCV-related HCC showed a higher benefit from sorafenib (HR: 0.47) compared to non-hcv patients (HR: 0.8). Recently, lenvaitinb in front line and regorafenib and cabozantinib in second-line have shown survival benefits as well. No biomarker studies have been reported so far. A recent phase I-II clinical trial assessing nivolumab in 260 patients with advanced HCC has shown up to 6% of objective responses, some of them of long duration, obtaining a median overall survival of 6 months. PD- and PD-L immunostaining status did not predict response to nivolumab. A recent gene signature capturing the immune class of HCC (~30% of patients) is currently tested to explore if it can predict treatment response. 44
45 References. Llovet JM, Zucman-Rossi J, Pikarsky E, et al. Hepatocellular carcinoma. Nat Rev Dis Prim 206;2: EASL-EORTC Guidelines of clinical management of HCC. J Hepatol 202;56: Zucman-Rossi J, Villanueva A, Nault JC, Llovet JM. Genetic Landscape and Biomarkers of Hepatocellular Carcinoma. Gastroenterology 205;49: Hoshida Y, Villanueva A, Kobayashi M, et al. Gene expression in fixed tissues and outcome in hepatocellular carcinoma. N Engl J Med 2008;359: Llovet JM, Pena CE a., Lathia CD, Shan M, Meinhardt G, Bruix J. Plasma Biomarkers as Predictors of Outcome in Patients with Advanced Hepatocellular Carcinoma. Clin Cancer Res 202;8: Sia D, Jiao Y, Martinez-Quetglas I, Kuchuk O,et al. Identification of an Immune-specific Class of Hepatocellular Carcinoma, Based on Molecular Features. Gastroenterology 207;53:
46 Clinical scores - What is their added value? Philip Johnson University of Liverpool, Liverpool, United Kingdom philip.johnson@liverpool.ac.uk Clinicians aim to take into account several factors (or variables ) in arriving at a diagnosis, identifying appropriate treatment or assessing prognosis. Experts are identified as those who have sufficient clinical experience and judgment to successfully and consistently fulfil these aims. However, it has been recognised for more than 60 years that it may be possible to make explicit use of mathematical manipulation of data rather than relying on subjective interpretation of data through skilled clinical judgment. The implicit request in the title of this talk is to show that clinical scores, probably better called models or algorithms, can enhance or improve upon conventional clinical judgment and expertise. Clinical scores such as the Child-Pugh (C-P) score (for assessing liver function) have already been widely and successfully used in HCC. More recently more rigorously evidence-based scores such as MELD have been introduced into routine clinical practice. The modern clinical approach requires application of rigorous statistical methodology to identify variables that influence a particular outcome followed by modeling to build a score or algorithm. The models are first developed in a training set and then validated in an independent, internal, dataset and finally in external datasets, usually from different countries and healthcare systems. Our approach has been to use only clinical features that are widely available for our models. Locally developed laboratory and radiological tests are generally unhelpful because their performance has seldom been appropriately validated and the methods are not widely or simply available. Secondly, when using continuous variables such age, tumour size or biomarker levels, it is now recognised that categorising this data, for example by using cut-off points such as < or > 60 years, or AFP as < or > than 400 ng/ml wastes a considerable amount of information. Our models therefore, wherever possible, use available data in its continuous form. Finally, whereas points based scores for prognosis or function assessment (such as the C-P score) are simple and easy to apply at the bedside, mathematical functions are often seen as too complicated for routine clinical use. However, such modeling approaches have been widely used in other professions and there is no reason why this should not be the case in medicine. Therefore, for each model we develop a simple online calculator, applicable to smartphones, that can generate useful output, such as individual patient prognosis, within minutes. Whilst conventional multivariable modeling has been most widely used to date we are now entering the era of machine learning with artificial intelligence soon to appear. Examples of each of these approaches will be presented together with evidence that they may indeed offer added value over and above what can be achieved by expert clinical judgment. Reference. Meehl PE, Clinical vs. Statistical Prediction. University of Minnesota press
47 Locoregional therapies in HCC: Ablation, transarterial therapies or combination of boths Rita Golfieri Università di Bologna, Bologna, Italy Locoregional treatments are extensively performed in HCC at various stages. The current staging and treatment strategy in Europe is the algorithm from the Barcelona Clinic Liver Cancer group (BCLC), distinguishing different stages depending on the liver function, tumour extent and performance status of the patient and suggesting different therapeutic approach for each stage. In early stage HCC, percutaneous ethanol injection (PEI), Radiofrequency (RFA) or Microwave ablations (MWI) are proposed. For intermediate HCC, the reference treatment is transarterial chemoembolization (TACE) and combination of percutaneous tumor ablation with TACE can be advocated in large HCC. Transarterial radioembolization (TARE) has been evaluated in advanced HCC and in large and hypovascular tumors unresponsive to TACE. Ablation. Percutaneous ablation is a safe and effective treatment for small HCC, who unsuitable for surgery or as a bridging therapy to liver transplant. PEI and RFA can be equally efficacious for lesions up to 2 cm, but the necrotising effect of RFA is more predictable and significantly better than with PEI for larger lesions. Therefore, for HCC 2 cm, RFA is considered the first-line treatment when performed in expert centres. For HCC of 2. 3 cm, the choice between surgery and RFA should be made on a case-by-case after a multi-disciplinary evaluation. As compared to surgical resection, percutaneous ablation is associated with lower morbidity and mortality, shorter length of hospitalisation, and lower sanitary costs. Percutaneous MWI is increasingly being used in clinical practice for the treatment of HCC. The safety profile appears good, although specific confirmation in larger series of cirrhotic patients is still awaited. In the only comparative study with RFA, MWI showed equivalent efficacy but required more therapeutic sessions. Transarterial therapies. TACE, both in the conventional lipiodol-based modality (c-tace)and with drug-eluting beads (DEB-TACE) is the most frequently used treatment for HCC worldwide. TACE is indicated in BCLC intermediate stage patients, not eligible for surgery or ablation. The best candidates for TACE are asymptomatic Child-Pugh class A patients, although those with a Child-Pugh score of B7 or ECOG PS can also be considered. TACE is not indicated in patients with jaundice, untreatable ascites, main or branch portal vein thrombosis, hepatofugal portal blood flow, HCC nodules >0 cm. TACE can be also utilised in patients with early stage HCC, if surgical or ablative techniques are not applicable due to technical conditions and/or comorbidities. TACE treatment aims both to achieve selective delivery of chemotherapy using any type of carrier and to obtain complete obstruction of the tumor vasculature. Therefore, to be effective, TACE should be carried out with a selective or superselective (segmental or sub-segmental) technique in order to optimise the risk/benefit ratio and increase the likelihood of complete response of the target lesion(s). Current evidence suggests that one cycle of c-tace may not be sufficient for effective treatment of intermediate-stage HCC. There is evidence which suggests that repeating TACE prolongs survival. TACE can be repeated continuously in the case of a suspicious viable tumor in follow-up imaging. However, there is no real consensus regarding the frequency of TACE and the interval between two TACE treatments. DEB-TACE may be preferred to conventional TACE in Child-Pugh B or ECOG PS patients, although additional prospective comparisons are needed before this approach can be definitely recommended in the clinical practice. Even though TACE is the most frequently used intrarterial treatment for HCC, yet there is not convincing evidence in favour of TACE over bland embolization (TAE) -without drug- in terms of patients survival. TARE may be indicated in patients with large masses and/or portal thrombosis/invasion, but it should be utilised in the context of prospective studies aimed at ascertaining its cost-effectiveness profile. Two non-randomised studies demonstrated that TACE and TARE are not different in terms of both overall survival and toxicity, while toxic effects were lower with TARE in another large series of patients. In patients with tumour portal vein thrombosis, when TACE is contra-indicated, TARE was reported to be effective and well tolerated. Combination of ablation and TACE. In non-surgical cases, a combined/sequential approach (TACE plus PEI, RFA, or MWI) should be considered for multinodular HCCs and for each nodule >3 cm, after a multidisciplinary assessment. In a number of prospective randomised trials, TACE combined with thermal ablation has demonstrated its superiority in local control and survival compared with thermal ablation or TACE alone, and this has been mentioned in the NCCN and in the German guidelines, but 47
48 not in the BCLC. The combination of locoregional therapies offers the maximal flexibility which allows an approach tailored to the characteristics of each nodule in each patient with multifocal disease. 48
49 Liver transplantation for HCC: How to optimize patient selection? Vincenzo Mazzaferro Fondazione IRCCS Istituto Nazionale dei Tumori, Milano, Italy Liver transplantation (LT) is a potentially curative option for hepatocellular carcinoma (HCC). However, LT is a resource-demanding option to be offered only when sufficient benefit is achievable, as HCC in patients with well-compensated cirrhosis has alternative options competing with transplantation. In addition, organ availability, list dynamics, non-cancer indications and waiting time are limitations to deal with in case of transplantation. In order to optimize indications to LT for HCC, various levels of intervention could be envisaged:. Optimization of transplant eligibility criteria Milan criteria are still the most favoured indication for HCC patients but a consensus on those tumors beyond Milan eligible to LT is lacking. A crucial step in indicating transplantation is a modern diagnostic approach to HCC when LT is discussed. LI-RADS categorization can contribute to HCC staging when LT discussion is in place, as UNOS T-stages used in liver transplant listing correlates with the LI-RAD observation categories. Some important and somehow hidden points emerging from comparison of these systems will be discussed. 2. Optimization of heterogeneity of pre-transplant HCC management Nowadays, bridging and downstaging are considered for almost any patient with HCC and response to loco-regional treatments (LRT) used in downstaging protocols has become a leading factor for indicating LT at different levels of priority. Treatment response varies the risk of drop-out as well as post-lt outcome. If treatment response is a priority driver for HCC beyond Milan (Intermediate stage) innovative strategies may be designed, considering that not all the HCC have the same pattern of presentation, progression and response to therapy. Priority is in fact a decision based on the risk of drop-out and the amount of benefit offered by LT. 3. Optimization of composite criteria considering also tumor biology surrogates such as alphafetoprotein (AFP). A mathematic interaction between morphology of the tumor (size + number) and AFP level can be calculated and so the post-transplant survival according to the response to LRT (using a calculator freely accessible at: 4. Optimization of the endpoints of LT for HCC in the DAA era Cancer vs. non-cancer conditions are known to affect post-transplant outcome, and since non-cancer conditions of mortality are decreasing in the DAA era, cancer-specific survival can become a very actionable endpoint. Safety thresholds for post-transplant HCC-specific survival have been identified and may influence future decision on eligibility to LT in the near future. 49
50 Update of the EASL Clinical Practice Guideline on management of hepatocellular carcinoma Peter Galle University Medical Center Mainz, I. Medical Department, Mainz, Germany In 202, the previous guideline for the management of hepatocellular carcinoma (HCC) was published as a result of a joint effort by the European Association for the Study of the Liver (EASL) and the European Organisation for Research and Treatment of Cancer (EORTC). Since then several clinical and scientific advances have been achieved. Thus, an updated version of the document is needed. For this purpose EASL established a guideline development group composed of international experts in the field of HCC, comprising the areas of hepatology (Peter R. Galle, Alejandro Forner, Josep Llovet, Fabio Piscaglia), surgery (Vincenzo Mazzaferro), radiology (Valerie Vilgrain), oncology (Jean-Luc Raoul) and pathology (Peter Schirmacher). The process was moderated by a methodologist (Markus Follmann). In a first step the panel identified, prioritised and selected relevant topics and agreed on key questions to be answered. These questions were clustered and distributed according to the defined working groups, which are reflected in the different chapters. According to the key questions, a literature search was performed. The studies identified and included were assessed and assigned to categories related to study design and strength of evidence according to endpoints. Based on this evidence, the drafts for recommendation and chapters were created. Consent was provided for all recommendations during the consensus conference. Formal consensus methodology (nominal group technique) was used to agree upon the recommendations. All expert panel members were entitled to vote on the recommendations. The consensus conference was performed as a personal meeting over two days (in June and September 207). When evaluating the evidence, the balance of benefits and harms, and the quality of the evidence were taken into consideration. Expert opinion and experience was included, particularly, if the body of evidence was insufficient and if further aspects such as time and costs, additional side effects, quality of life, resource use, etc. had to be considered. The presentation will give an overview and focus on changes compared to the previous version. 50
51 Advanced HCC: A multidisciplinary approach - Tumour board #3: Clinical case presentation Marcus-Alexander Wörns First Department of Medicine / Cirrhosis Centre Mainz (CCM), University Medical Centre of the Johannes Gutenberg-University Mainz, Mainz, Germany marcus-alexander.woerns@unimedizin-mainz.de Preserved liver function (Child-Pugh A) and performance status (ECOG PS 0/) are basic requirements for the implementation and success of a multidisciplinary approach in HCC. Real-life observations in the past revealed an exaggerated usage of locoregional treatment overall delaying or even preventing (by deterioration of liver function) timely administration of systemic therapy. However, in consequence of the positive results from recent trials that demonstrated clinically meaningful objective response rates and overall survival benefit for systemic therapies in first- and second line setting, it is likely that an increased percentage of patients with HCC will receive systemic treatment in the near future []. We here present a clinical case of a female patient with HCC due to chronic HCV infection and advanced liver fibrosis. This case underlines that a timely discontinuation of locoregional treatment may be important to guarantee continuum of care in HCC and, furthermore, how particularly sequential application of systemic therapies can be effective in both intermediate as well as advanced stages. We will highlight which patients may experience most benefit from sorafenib in clinical practice (e.g. patients with early skin toxicity, HCV, and without EHS, respectively), challenge radiological response assessment and show the high clinical value of a sequential assessment of alpha-fetoprotein (AFP). We will also discuss available recommendations for discontinuing sorafenib or other targeted therapies in clinical practice, and will again delineate the critical prognostic implications of portal vein thrombosis/macroscopic vascular invasion (MVI) in the natural course of the disease. As routine practice in other GI tumour entities, sequential systemic treatment is now possible in intermediate to advanced HCC. In addition, on the basis of good tolerance, checkpoint inhibitors will probably stimulate combined approaches with different immunotherapeutics or complementary to targeted therapy [2]. References [] Wörns MA, Galle PR. Hepatocellular carcinoma in 207: Two large steps forward, one small step back. Nat Rev Gastroenterol Hepatol. 208 Feb;5(2): [2] Wörns MA, Galle PR. Immune oncology in hepatocellular carcinoma-hype and hope. Lancet. 207 Jun 24;389(0088):
52 Approved systemic treatments for HCC: Which is the best treatment approach? Marco Sanduzzi-Zampareli, Álvaro Díaz-Gonzalez, Maria Reig Barcelona Clinic Liver Cancer (BCLC) Group, Liver Unit, Hospital Clinic Barcelona, IDIBAPS, University of Barcelona, Barcelona, Spain The systemic treatment and management of patients with hepatocellular carcinoma has evolved in the last 0 years[]. Sorafenib[2,3] and regorafenib[4] have been approved to treat HCC patients in first and second line due to their benefits on overall survival and the adequate safety profile[]. Nivolumab received a FDA accelerated approval for the HCC in patients who have been previously treated with sorafenib based on the overall response rate results[5]. In addition, lenvatinib[6] and cabozantinib[7] demonstrated a positive impact on the overall survival but are still waiting for their approval in HCC. Thus, when more than drug is approved in an specific line, our proposal is to decide the agent based on OS benefit as a first step and then, consider safety profile and indirect markers if both drugs have demonstrated the same OS benefits. Sorafenib and lenvatinb offer the same OS in first-line[6], but the rate of patients who will benefit from lenvatinib will be less than with sorafenib due to the restrictive inclusion criteria of the phase III trial (main portal vein thrombosis, more than 50% of liver involved or biliary invasion were excluded). Regarding safety, it is not possible to do a direct comparison between both drugs because safety was not an end-point in that trial but patients with lenvatinib presented more severe-related adverse events. Regarding second line, the situation is more complex due to the different inclusion criteria between the trials and the impact of the evolutionary events which appeared during sorafenib treatment such as BCLCp stage[8], and early dermatologic events[9] which were not considered on the available OS analysis of nivolumab. Thus, from the data available in February 208, we consider sorafenibregorafenib treatment as the best approach for those patients who meet the same criteria of the phase III trials. However, if this is not the case and the country concerned has the nivolumab approval, this agent could be considered for sorafenib-intolerant patients. For sure this strategy will change when lenvatinib and cabozantinib receive their approval and the results of the phase III trial for nivolumab/sorafenib will be reported. References:. Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 208; In press. 2. Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, de Oliveira AC, Santoro A, Raoul JL, Forner A, Schwartz M, Porta C, Zeuzem S, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med [Internet]. 2008/07/ ; 359: doi: 359/4/378 [pii]0.056/nejmoa Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S, Kim JS, Luo R, Feng J, Ye S, Yang TS, Xu J, Sun Y, Liang H, et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: a phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol [Internet]. 2008/2/ ; 0: doi: S (08) [pii]0.06/s (08) Bruix J, Qin S, Merle P, Granito A, Huang Y-H, Bodoky G, Pracht M, Yokosuka O, Rosmorduc O, Breder V, Gerolami R, Masi G, Ross PJ, et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): a randomised, doubleblind, placebo-controlled, phase 3 trial. Lancet [Internet]. 207 [cited 207 Jun 5]; 389: doi: 0.06/S (6) FDA grants accelerated approval to nivolumab for HCC previously treated with sorafenib. 52
53 6. Kudo M, Finn RS, Qin S, Han K-H, Ikeda K, Piscaglia F, Baron A, Park J-W, Han G, Jassem J, Blanc JF, Vogel A, Komov D, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet (London, England) [Internet]. 208 [cited 208 Feb 9];. doi: 0.06/S (8) Abou-Alfa, Ghassan K. Meyer T, Cheng A-L, El-Khoueiry AB, Rimassa L, Baek-Yeol Ryoo, Irfan Cicin, Philippe Merle, Joong-Won Park, Jean-Frédéric Blanc, Luigi Bolondi, Heinz Josef Klümpen, Stephen Lam Chan, Vincenzo Dadduzio, Colin Hessel, Anne E. Borgman-Hagey, Gisela Schwab RKK. Cabozantinib (C) versus placebo (P) in patients (pts) with advanced hepatocellular carcinoma (HCC) who have received prior sorafenib: Results from the randomized phase III CELESTIAL trial. J Clin Oncol. 208; 36: abstr Reig M, Rimola J, Torres F, Darnell A, Rodriguez-Lope C, Forner A, Llarch N, Rios J, Ayuso C, Bruix J. Postprogression survival of patients with advanced hepatocellular carcinoma: Rationale for second-line trial design. Hepatology [Internet]. 203/06/ ; 58: doi: 0.002/hep Reig M, Torres F, Rodriguez-Lope C, Forner A, LLarch N, Rimola J, Darnell A, Ríos J, Ayuso C, Bruix J, N LL, Rios J. Early dermatologic adverse events predict better outcome in HCC patients treated with sorafenib. J Hepatol [Internet]. 204/04/ [cited 204 Dec 9]; 6: doi: S (4)002-6 [pii]0.06/j.jhep
54 Assessment of systemic treatment activity by imaging Maxime Ronot Medical Imaging, Beaujon University Hospital, Clichy, France Response Evaluation Criteria In Solid Tumors. (RECIST.) is currently approved as a standard method for the evaluation of tumor response in patients in clinical trials and is considered to be a surrogate endpoint to predict survival outcome in patients with solid tumors. Yet, The overall survival benefit of sorafenib in HCC is in contrast with the low objective response rate of <5% by RECIST., raising concerns as to the appropriateness of these criteria as a surrogate endpoint for survival in HCC. Similar observations have been reported with sunitinib (Sutent ; Pfizer Inc., New York, NY), another antiangiogenic multikinase inhibitor, when used to treat patients with advanced HCC. Investigation of alternative radiological methods to assess advanced HCC is thus warranted. Several other criteria have been proposed such as the European Association for the Study of the Liver (EASL) criteria, the modified RECIST (mrecist) criteria, or the Choi criteria. These alternative criteria are designed to evaluate the effects of treatment on tumor vascularization based on modifications observed in tumor dimension and/or attenuation on contrast-enhanced phase scans. Recent retrospective studies showed promising results with these criteria, suggesting that they might be a potential prognostic factor for survival in advanced HCC patients treated by sorafenib. Indeed, alternative enhancement-based criteria identified more responders than RECIST. and patients with objective response had better survival outcomes compared to patients without. Yet, these criteria also suffer from limitations (inter-reader variability, context of use, definitions and applicability) that need to be addressed. Other approaches, including functional or quantitative imaging have also been proposed. Perfusion parameters (using either CT or MR) have been shown to decrease early and significantly in responders when compared to non-responders. Higher baseline perfusion values are also observed in patients in whom the disease is further controlled. French teams also reported that standardized quantitative CEUS could predict tumor progression. These results are promising but remain limited to the field of clinical research. 54
55 Inflammation in liver tumorigenesis: Potential targets for immunotherapy Eli Pikarsky The Hebrew University of Jerusalem, School of Medicine-IMRIC-Immunology and Cancer Research, Jerusalem, Israel The different roles of the adaptive immune system in cancer are beginning to unfold. The dramatic responses to immune check point drugs in some tumors generated an accelerated need for understanding the complex set of interactions between tumor and immune cells. In view of the major pathophysiological role of immune cells in hepatocellular carcinoma is not surprising that malignant hepatocytes interact extensively with adaptive immune cells, resulting in both pro-tumor immunopathology and anti-tumor protective immunity. Identifying potential responders to drugs that target the adaptive immune system, monitoring their immune response to the tumor and devising the best treatment combinations depends on understanding the complex set of interactions taking place within the tumor and in the adjacent hepatic parenchyma. Cellular infiltration usually entails a diffuse influx of immune cells, scattered throughout the inflamed tissue. However, infiltrating leukocytes often form ectopic lymphoid aggregates or even more complex structures that histologically resemble lymphoid organs. These structures direct various B and T cell responses and are referred to as ectopic lymphoid-like structures (ELSs). ELSs often develop at sites of chronic inflammation where they can influence the course disease. In many cancers, the presence of ELSs correlates with a better prognosis and they may coordinate endogenous antitumor immune responses. Surprisingly, in the liver the presence of ELSs is positively correlated with HCC. The potential role of immunosuppression in ELS protumorigenic function will also be discussed. 55
56 Role of immunology in HCC development and progression Pablo Sarobe University of Navarra, Pamplona, Spain The liver behaves as an important line of defence against blood-borne pathogens, simultaneously avoiding responses against non-pathogenic antigens, maintaining thus a balance between immunity and tolerance. In this regard, in addition to the role of chronic liver inflammation as a tumour-inducing factor, the immune response is involved in the surveillance of tumour growth, through recognition of tumour cell-associated molecules and antigens by innate and adaptive immunity. Therefore, infiltration of effector cell subsets, such as T cells, into liver tumours has been associated with better survival in animal models and clinical studies. However, as the tumour progresses in advanced stages, some of the natural tolerance mechanisms operating in the liver are upregulated, subverting the nature of the immune response and leading to a pro-tumorigenic effect, which facilitates tumour growth. Tumour intrinsic features as well as environmental factors like the production of anti-inflammatory cytokines and expression of inhibitory ligands by different subsets of tumour and myeloid cells lead to exhausted effector T cells and expansion of regulatory T cells, allowing tumour evasion. Identification of the relevant cellular and molecular targets implicated in immune response activation and in tumour escape will allow the design of proper immunotherapeutic strategies for HCC patients. 56
57 Patient-derived models for drug discovery in liver cancer Jens Marquardt Department of Medicine I, Lichtenberg Research Group, Johannes Gutenberg University, Mainz, Germany Precision medicine approaches explore next-generation technologies to obtain molecular information and assign patients to most effective treatment. While matching of genome-based diagnostics with therapeutic strategies is convincing, the approach is limited by our insufficient biological understanding as well as underappreciated intratumoral heterogeneity that contribute to the observed rapid induction of chemoresistance in primary liver cancer (PLC). Further, results from recent clinical trials and large consortial efforts clearly delineate that not all of the putative actionable alterations will result in a meaningful therapeutic efficacy. However, several of these limitations can be addressed by integration of functional genomics into the (pre-)clinical pipeline. Herein, patient-derived models followed by direct target evaluation can be highly valuable tools for translational studies on PLC. To date, several of these patient-derived models, including patient-derived cancer lines (PDCL), organoid cultures as well as patient-derived xenografts, are available and have been explored in HCC. While the overall impact and representation of these models for authentic human HCC is currently difficult to estimate, these models not only enable individual evaluation of drug response, but also direct exploration of putative actionable targets. Therefore, development of primary culture models that closely recapitulate phenotypic and molecular diversities of PLC is particularly promising. We have recently established long-term culture of liver cancer cells of hepatocellular, cholangiocellular and metastatic origin using defined culture conditions and performed detailed morphological as well as dynamic molecular characterization. Our results demonstrated that PDCL fully resemble morphological features of the primary cancers in vitro and in vivo. Genomic alterations as well as transcriptome profiles further confirmed a high similarity with primary tumors during long-term culturing. Direct target evaluation revealed key oncogenic mutations of PLC such as TP53, KRAS, CTNNB and identified actionable mutations (e.g. MET, ckit, KDR) amenable for individualized therapeutic approaches. Integrative genomic and transcriptomic characterization further demonstrated that PDCL more closely resemble molecular and prognostic features of PLC than established cell lines. Together, our integrative analysis provides evidence that the use of PDCL represents a refined model for discovery of relevant molecular subgroups and exploration of precision medicine approaches for the treatment PLC. The PDCL might, therefore, significantly advance translational research efforts into liver cancer. 57
58 eposter ABSTRACT PRESENTATIONS 58
59 P0-0RANDOMIZED TRIAL OF PREOPERATIVE ADMINISTRATION OF ORAL PREGABALIN FOR POSTOPERAIVE ANALGESIA IN PATIENTS SCHEDULED FOR RADIOFREQUENCY ABLATION OF FOCAL LESIONS IN THE LIVER. Sherief Abd-Elsalam, Nehad Hawash, Amr Magdy Abdelfattah 2, Amr Hanafy 3 Tanta University, Tropical Medicine Department, Tanta, Egypt, 2 Tanta University, Anasthesia and Pain management, 3 Zagazig University, Internal Medicine Department, zagazig, Background and Aims: The aim of this study was to evaluate the effect of preoperative pregabalin on postoperative analgesia in patients presented for radiofrequency ablation of hepatic focal lesions. Method: This randomized controlled study was carried out on 70 adult patients with hepatocellular carcinoma presented to Tanta University Hospital for radiofrequency ablation of hepatic focal lesions. They were randomized into two groups, 35 patients in each group: Group I: Patients in this group received placebo and Group II: patients in this group received 50 mg of oral pregabalin one hour before the procedure. The primary outcome was the analgesic effect in the form of the severity of postoperative pain and the need of opioid analgesics. Our secondary outcome was the safety of the drug in the form of incidence of side effects. Results: Regarding pain assessed by visual analogue pain scale (VAS Pain) post operatively, there were no significant differences between both groups immediately postoperative (P=0.84), then a highly significant difference in pain (P= 0.00) between two groups had been noticed as pregabalin showed high efficacy in decreasing pain in group II compared to group I, also patients received pregabalin had decreased requirements for the use of post operative analgesics. Regarding side effects, there was no significant difference regarding blood pressure (P=0.74) nor oxygen saturation (P=0.53) between the two studied groups, on the other hand patients in pregabalin group showed fewer side effects as nausea, vomiting (P=0.0) and bradycardia (P=0.02) and were discharged earlier when compared with the other group (P=0.0). Conclusion: Oral pregabalin is safe and effective for postoperative analgesia in patients scheduled for radiofrequency ablation of focal lesions in liver. [ClinicalTrials.gov Identifier: NCT03523] 59
60 P0-02 MIRNA PROFILE AS A PROGNOSTIC BIOMARKER FOR HEPATOCELLULAR CARCINOMA DEVELOPMENT Alisa Petkevich, Alexandr Abramov, Elena Kuhareva, Pavel Ogurtsov Российский университет дружбы народов, Москва, Russian Federation Background and Aims: We have entered a new era in liver diseases treatment when chronic hepatitis C virus infection (HCV) is no longer an incurable disease and this became possible due to direct-acting antivirals. However, there are still unsolved problems concerning consequences of this disease, and one of them is hepatocellular carcinoma (HCC). In cirrhotic patients with sustained virologic response (SVR) the annual incidence of HCC is -7% per year [Goossens N. et al., 205]. Clinical criteria such as age, obesity, diabetes and others are not enough for precise prediction of HCC. In order to find biomarkers reflecting precancerous processes in liver cells we referred to microrna. MiRNA are small molecules (8-25nucleotides) involved in epigenetic regulations of gene expression and associated with different pathologic processes [Egger G. et all, 2004]. Method: Blood samples and cheek swabs from 28 patients with SVR and different fibrosis stage, 6 liver biopsy and 2 saliva samples from the same patients; blood samples from 9 healthy volunteers as control group. Blood sampling and keeping was performed under different conditions (tubes Streck, Vacuette and others; different time and storage temperature before centrifugation and mirna extraction). Levels of 7 mirnas were assessed (mirna 6, mirna2, mirna34, mirna 22, mirna25, mirna26, mirna45). Electrophoresis in polyacrylamide gel was performed to estimate specificity of qrt-pcr. Concentration of extracted mirna was determined by nanodrop. qrt-pcr was performed according to standard protocol. In order to assess specificity of changes in mirna profile, supernatant from two liver cancer cell lines (Huh7 and HepG2) cultured for 7 days after defrosting was studied for the same 7 mirnas. Results: All mirnas were determined in biopsy and blood samples, some of mirnas were undected in saliva, cheek swab samples and supernatant from Huh7 and HepG2. Some mirna (mirna6, mirna25, mirna45) are highly expressed in all kind of samples. MiRNA 26 is not detected in saliva. Conclusion: An attempt to study mirna profile in different biological samples faces with many problems such as normalization of detected mirnas, standardization of biological sampling and difficulties of preanalytical step. Another great obstacle is specificity of detected correlations. However, further research is needed to find new promising mirna molecules as diagnostic and prognostic biomarker for HCC transformation. 60

61 P0-03 IMPACT OF BCLC TREATMENT STAGE MIGRATION IN THE SURVIVAL OF PATIENTS WITH HEPATOCELLULAR CARCINOMA Silvia Acosta-López, Dácil Díaz Bethencourt, Julio Plata-Bello 2, Antonio González Rodríguez, Estefanía Berge Garrido, Francisco Andrés Pérez Hernández Hospital Universitario Nuestra Señora de la Candelaria, Liver Unit, Santa Cruz de Tenerife, Spain, 2 Hospital Universitario de Canarias, Santa Cruz de Tenerife, Spain Background and Aims: The Barcelona-Clinic Liver Center (BCLC) classification determines the best therapeutic option in each liver cancer stage. However, some clinical conditions may lead to a migration in the first-line treatment to other therapeutic option. This situation seems to be usual, but the impact of this treatment-migration has not been entirely studied. The aim of the present work is to analyze the causes and impact of treatment migration in each BCLC stages in terms of overall survival. Method: A prospective registry of patients with a diagnosis of hepatocellular carcinoma have been performed since January 20. One-hundred and thirty-eight patients were included in the study. The BCLC classification system was used to identify the first-line-treatment that corresponded for each stage. Treatment stage migrations were also identified and analyzed. Non-parametric tests were used to identify differences between first-line vs. migration treatment groups in each BCLC stage. Survival analysis in each BCLC stage was performed. Statistical significance was considered when p-value was below Results: Thirty-three percent of patients had a treatment stage migration (43.5% of patients in BCLC A; 8.9% in BCLC B; and 50% in BCLC C). Regarding BCLC A patients, migration-treatment patients were significantly older than the patients who receive the first-line-treatment (p<0.00). OS was significantly higher in the last group (median survival of 90.0 months vs months) (p<0.00). Hazard ratio (HR) for migration-treatment group (adjusted by age) in BCLC A patients was 3. (95% C.I. of.2 7.7) (p=0.05). Bearing in mind BCLC B patients, migration-treatment group presented a higher number of lesions than first-line-treatment group (p=0.0). The OS was also significantly higher in the first-line-treatment patients (median survival of 3.8 vs. 7.9 months) (p=0.003). HR for migration-treatment was 4.9 (95% C.I. of.3 7.8). Finally, BCLC C patients showed a different distribution of CHILD categories between the treatment groups. All patients in the first-line treatment group of BCLC C patients were classified as CHILD A, while only 33% of migration-treatment presented such categorization. No differences in OS were identified between both treatment groups (p=0.225). Conclusion: BCLC A and BCLC B hepatocellular carcinoma patients with a treatment stage migration present a significant worse prognosis than patients with first-line-treatment options. Figure: Figure. Kaplan-Meier survival analysis for both treatment groups in each BCLC stages where migration stage treatment was present. 6
62 P0-04YI RIP3-DEPENDENT SIGNALLING CONTRIBUTES TO NON-ALCOHOLIC FATTY LIVER DISEASE-RELATED CARCIONOGENESIS Marta B. Afonso, Pedro M. Rodrigues, André Simão, André A. Santos, Maria Manuela Gaspar, Rui E. Castro, Cecília M. P Rodrigues Research Institute for Medicines (imed.ulisboa), Faculty of Pharmacy, Universidade de Lisboa, Lisbon, Portugal Background and Aims: Hepatocellular death, inflammation and fibrosis are implicated in the pathogenesis of non-alcoholic steatohepatitis (NASH), including development and progression to hepatocellular carcinoma (HCC). Necroptosis is a highly immunogenic regulated cell death routine that depends on receptor-interacting protein 3 (RIP3) kinase activity. We aimed to evaluate the role of necroptosis in the pathogenesis of non-alcoholic fatty liver disease (NAFLD)-driven carcinogenesis. Method: C57BL/6 wild-type (WT) or RIP3-deficient (RIP3 -/-) mice were fed a choline-deficient L-amino acid-defined diet (CDAA; n=4) or a control choline-sufficient L-amino acid-defined (CSAA; n=4) diet for 66 weeks, with subsequent histological and biochemical analysis of hepatic damage and carcinogenesis. Insulin resistance and oxidative stress were also investigated. Results: CDAA-fed WT mice exhibited all the main histological features of liver injury associated with NASH, namely steatosis, hepatocellular ballooning, immune cell infiltration, and fibrosis. RIP3 deficiency ameliorated CDAA-induced inflammation and fibrosis, and decreased the NAFLD activity score. In agreement, hepatic gene expression of pro-inflammatory mediators was also significantly decreased in CDAA-fed RIP3 -/- mice, compared with WT. Intriguingly, RIP3 -/- mice displayed increased body weight gain with time, as well as insulin resistance at 66 weeks as assessed by homeostasis model assessment-estimated insulin resistance and decreased insulin receptor substrate phosphorylation, compared with WT mice on CSAA or CDAA diet. RIP3 -/- mice tended to show reduced incidence of macroscopic preneoplasic nodules, accompanied by significantly reduced Ki67 positive hepatocytes and increased proapoptotic Bax and cell cycle regulator cyclin-dependent kinase 2-associated protein (CDK2AP). Absence of RIP3 further hampered signaling pathways controlling tumor microenvironment and protected against oxidative stress and mitochondrial dynamic dysfunction. Conclusion: Overall, RIP3 ablation halts long-term inflammation, fibrosis, hepatocyte proliferation, and genetic resistance of dysplastic hepatocytes to cell death, oxidative stress and tissue microenvironment changes associated with NASH-driven hepatocarcinogenesis. Targeting RIP3-dependent signalling might be a promising approach to arrest NAFLD progression to HCC, although complementary approaches may be required to control insulin resistance in obese patients. (Funding: PTDC/BIM- MEC/0895/204; SAICTPAC/009/205). 62
63 P0-05 THE BIOMARKER POTENTIAL OF KI67 AND PH2AXIMMUNOHISTOCHEMISTRY IN GUIDING USE OF THE LIVER- TARGETING NUCLEOTIDE MIV-88 INPATIENTS WITH HEPATOCELLULAR CARCINOMA Mark Albertella, Biljana Rizoska, Misti Mccain 2, Calum Kirk 2, Fredrik Öberg, Richard Bethell, Helen Reeves 2 3 Medivir AB, Biology, Huddinge, Sweden, 2 Northern Institute For Cancer Research, United Kingdom, 3 Newcastle upon Tyne Hospitals NHS Foundation Trust, The Liver Unit, United Kingdom Background and Aims: MIV-88, a nucleotide prodrug of troxacitabine-monophosphate has been designed to deliver high levels of the chain-terminating nucleotide troxacitabine-triphosphate (TRX-TP) to the liver after oral dosing while minimizing systemic exposure. TRX-TP is expected to be delivered to normal and tumor liver tissue, but only to be toxic to replicating cells. We have demonstrated marked anti-proliferative effects in cancer cells in vitro. Our aim was to evaluate effects in vivo, but also to consider the possible impact of MIV-88 in patients with chronic liver disease, where baseline levels of proliferation and DNA damage in non-tumor (NT) vs tumor tissues are unclear and might have relevance to toxicity. Method: In vivo efficacy was evaluated in nude mice with subcutaneous HepG2 xenografts. MIV-88 (00 mg/kg PO) was given twice daily for 5 days. Quantitative immuno-fluorescence histology assessed xenograft DNA damage (ph2ax) and proliferation (BrdU). Matched tumor and NT biopsy (n=30) or resection tissues (n=0) from 40 patients with HCC were assessed with Ki67 (proliferation) and ph2ax IHC, quantified using Aperio digital analysis. Results: MIV-88 treatment had no adverse effects on mice and resulted in significant tumor growth inhibition and growth delay of 26 days. Dose dependent inhibition of proliferation (94%) and dramatic (>20-fold) induction of DNA damage was evident in tumors post treatment. In patient tissues, % of Ki67 positive hepatocytes (%Ki67) was significantly higher in tumor compared to NT tissues (mean 8.7 [SD.0] vs to.3 [SD0.89], p<0.00). The range of %Ki67 was 0.6 to 4.02 in NT tissues, with no significant difference in presence of cirrhosis. In tumor tissues %Ki67 (range %) correlated with tumor size, PVT & TNM. %Ki67 above 6% (median) was associated with poorer survival (7.6 vs months, p=0.00). %Ki67 was independently associated with survival in multivariate cox regression including tissue type (biopsy/resection), tumor number, size, age and PVT. Baseline %ph2ax was low in tumor ( ) and NT ( ) tissues. Conclusion: MIV-88 is highly toxic to proliferating cells in vivo without adverse effects in mice. Using the surrogate marker Ki67, HCC showed marked elevations in proliferation relative to NT tissues. %Ki67 may have value as a patient selection biomarker, predicting response. Low baseline DNA damage in patient tissues supports the development of elevated ph2ax as a pharmacodynamic marker of MIV- 88, to demonstrate delivery and target engagement. 63
64 P0-06YI SARCOPENIA PREDICTSSURVIVAL IN PATIENTS WITH ADVANCED HEPATOCELLULAR CARCINOMA TREATED WITHSORAFENIB. Giulio Antonelli, Elia Gigante, Massimo Iavarone 2, Paola Begini, Piero Biondetti 2, Adriano Maria Pellicelli 3, Angelo Sangiovanni 2, Pietro Lampertico 4, Massimo Marignani Digestive and Liver Disease Unit, Sant'Andrea University Hospital, Sapienza University of Rome, Rome, Italy, 2 A. M. and A. Migliavacca Center for Liver Disease, Division of Gastroenterology and Hepatology,, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Università degli Studi di Milano, Milan, Italy, 3 Liver Unit, San Camillo - Forlanini Hospital, Rome, Italy, 4 Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Università degli Studi di Milano, Milano, Italy Background and Aims: Sarcopenia, a condition characterized by muscle wasting and considered a parameter of malnutrition, has been associated with poor outcomes in patients with cirrhosis and solid tumors. We analyzed the influence of sarcopenia on the survival of patients with advanced hepatocellular carcinoma (HCC) treated with sorafenib, the standard of care for this stage. Method: We conducted a multicenter, retrospective study on 96 patients with advanced HCC treated with sorafenib. Patients with an abdominal computed tomography (CT) scan within 30 days from treatment start were enrolled. Data on pre-treatment anthropometric features, baseline laboratory findings, toxicity, treatment duration and overall survival (OS) were collected. Transverse CT images corresponding to third lumbar vertebrae (L3) were collected to calculate the skeletal muscle index, defining the presence of sarcopenia. Results: In our cohort, patients were mainly males (78%) and sarcopenia was present in 49% of patients, with a significant major prevalence in women (M 37,3% vs F 90,5% p=0,0000). Patients were divided into two groups according to sarcopenia and compared: age was significantly higher in the sarcopenic group [66 years (3-87) vs 72 years (30-84)], while all other baseline features were similar, without significant difference in albumin levels, INR, body max index, serum sodium, creatinine, bilirubin and MELD score. Patients with sarcopenia showed a significantly shorter OS [39 (95% CI 26-50) vs 6 (95% CI 47-77) weeks (p= 0,02)], as well as time on treatment of sarcopenic patients [2,3 (95% CI 8-9) vs 25,9 (95% CI 5-33) weeks], while no significant differences in the cause of drug interruption were detected. At multivariate analysis, sarcopenia was found to be an independent predictor of reduced OS (p = 0.028), and of a reduced time on treatment (p = ). Conclusion: Sarcopenia measured with CT-scan is present in nearly half of patients with advanced HCC, and it can be used as a predictor of mortality and worse response to sorafenib. 64
65 Figure: 65
66 P0-07YI RAPAMYCIN AND ZOLEDRONIC ACID STRONGLY INHIBIT GROWTH OF ADVANCED MURINE HEPATOCELLULAR CARCINOMA VIA ACTIVATION OF INNATE AND ADOPTIVE IMMUNITY Muhammad Ashfaq-Khan, Misbah Aslam, Asif Qureshi 2, Detlef Schuppan Institute of Translational Immunology and Research Center for Immunotherapy, Mainz, Germany, 2 Dow university of medical sciences, Karachi, Pakistan Background and Aims: Treatment options for hepatocellular carcinoma (HCC) remain limited. Activation of the cancer immune microenvironment opens novel therapeutic opportunities to control tumor progression and block metastatic spread. We assessed single and combined treatment of experimental HCC with Zoledronic Acid (ZA) and Rapamycin (RA), two drugs that display myeloid cell regulating potential. Method: Mdr2(Abcb4)-/- mice were injected intraperitoneally with diethyl-nitrosamine DEN (0μg/g of bw) at the age of 5 days, followed by 0.05% phenobarbital in drinking water starting at the age of 3 weeks. This syngenic mouse model replicates key features of human HCC, with a genetic defect found in man and an external carcinogen. Mice were treated with vehicle, (ZA thrice a week as IP injection 00µg/kg ), RA (trice a week as oral gavage 5mg/body weight), or a combination of ZA and RA from age 5-6 months. After 6 months tumor volume and number of nodules were counted. 50% of livers were digested and CD45+ immune cells subjected to multicolour fluorescence assisted cell sorting using antibodies to CDb, CDc, Ly6C, Ly6G, CD86, CD4, CD8, CD25, CD3, CD90.2, CD206, F4/80, MHC-II, NK., Foxp3 and CD9. qpcr and IHC were performed for target molecules of interest. Results:Treatment with RA>ZA significantly reduced tumor growth. The combination of ZA and RA synergistically reduced the volume and number of HCC foci by 90 and 85 % respectively (p<0.000). The combination significantly reduced the population of M0- (CD45 + CDb + LY6G - F4/80 + ) and M2 macrophages (CD45 + CDb + LY6G - F4/80 + CD206 + ), and of myeloid derived suppresser cells (CD45 + CDc + LY6C high), representing central tumor promoting myeloid cell populations, while Myeloid derived dendric cells (CD45 + CDc high CDb + CD86 + ) that promote anti-cancer immunity were significantly upregulated. In parallel, total CD4+ T cells and especially CD4+CD25 regulatory T cells were significantly suppressed, while CD8+T cells were significantly increased in the combination treatment vs the untreated group. Changes in immune cell populations were confirmed by transcript patterns and IHC. Ki-67-positive cancer cells were nearly undetectable, and IHC for CD68 and YM- confirmed a dramatic shift from tumour associated M2 to M macrophages. The combination of ZA and RAPA significantly downregulated TAMs and MDSC markers like CSF-, VEGF, TGFβ, Cox2, HIFα, CCL2, CCL3, CCL5 and CCL7 that attract circulating monocytes into the tumour stroma. Conclusion:. Combination therapy of RAPA and ZA polarize myeloid (and T cells) towards a robust anti-hcc response; 2. Their combination is synergistic in an optimized syngenic model of murine HCC; 3. Both drugs have proven safety for other indications, and clinical studies in patients with HCC are warranted. 66
67 P0-08YI ZOLEDRONIC ACID SUPPRESSES TUMOUR ASSOCIATED MACROPHAGES AND MYELOID DERIVED SUPPRESSOR CELLS IN MURINE HCC Misbah Aslam, Muhammad Ashfaq-Khan, Asif Qureshi 2, Mirko Nick, Marcel Senkowski, Leonard Kaps, Kim Yong Ook, Detlef Schuppan Institute of Translational Immunology and Research Center for Immunotherapy, Mainz, Germany, 2 Dow university of medical sciences, Karachi, Pakistan Background and Objectives: HCC is associated with chronic inflammation leading to recruitment of bone marrow derived cells, mainly tumour associated macrophages (TAM, M2) and myeloid-cell derived suppressor cells (MDSC). Both cell types markedly suppress anti-hcc immune responses and are present in all stages of HCC. Zoledronic acid (ZA) is used in patients with osteoporosis to inhibit osteoclasts, i.e., bone macrophages with TAM-like properties. We hypothesized that ZA can polarize tumour promoting TAM and MDSC towards M macrophages with anti-tumour activity. Methods: Mouse bone marrow derived in vitro M or M2 polarized macrophages () were exposed to increasing concentrations of ZA. Transcript levels of M markers (TNFα, IL-β, inos, TIMP) and M2 markers (Fizz, ARG, VEGF, YM, MRC, MMP-9) were determined by qpcr. IL-2 and SOCS3 (M), IL-0 and VEGF (M2) secretion were measured by ELISA. Mice bearing a syngenic HCC (DEN/Mdr2KO model) received 3 doses of 00µg ZA/kg BW or vehicle control intraperitoneally weekly for a period of one month from age month 5-6. After four weeks of treatment mice were sacrificed to measure hepatic tumor number and volume and livers were assessed by H&E histology, IHC and qpcr. Results: ZA dose-dependently decreased M2 (Fizz, ARG, STAT6, YM, MRC, MMP-9) and increased M macrophage (inos, TNF-alpha, IL-beta, SOCS3) specific transcript levels without affecting cell viability in vitro. This was paralleled by a significant upregulation of IL-2 and dowregulation of IL-0 protein secretion into the cell supernatant. Compared to vehicle controls, treatment of DEN/Mdr2KO mice with ZA reduced tumour number and volume by 33.3% and 68%, respectively (p<0.004). Tumour cell proliferation as evaluated via Ki-67-positive cells was significantly blunted by ZA. Staining of YM- and glypican positive M2 and CD68 positive total macrophages of ZA treated HCC liver sections showed a significant upregulation of M>M2 macrophages and reduced numbers of TAM. ZA significantly downregulated hepatic transcript levels the TAM/MDSC markers CSF-, VEGF, TGFβ, Cox2, Hifα, CCL2, CCL3, CCL5 and CCL7. Conclusions:. ZA exhibits potent macrophage (and MDSC) repolarizing activity (M2 towards M) invitro and in-vivo, thereby increasing anti-hcc immune responses and limiting angiogenesis. 2. Since ZA has a well-known clinical safety profile, it should be assessed alone or in combination with other anticancer agents in patients with HCC. 67
68 P0-0 DISTINCT FUNCTIONS OF AP- (FOS/JUN) DIMERS IN LIVER CANCER Latifa Bakiri, Sebastian C. Hasenfuss 2, Rainer Hamacher 3, Martin K. Thomsen 4, Ana Guío- Carrión, Peter Hasselblatt 5, Erwin F. Wagner CNIO, Spanish National Cancer Centre, CANCER CELL BIOLOGY, MADRID, Spain, 2 LEK Consulting, Boston, United States, 3 University Hospital Essen, Department of Medical Oncology, Essen, Germany, 4 University of Aarhus, Department of Biomedicine, Aarhus, Denmark, 5 University Hospital Freiburg, Department of Medicine II, Freiburg, Germany Background and Aims: Genetically engineered mice are potent tools to discover disease-relevant molecular pathways (). The AP- transcription factor, formed by dimers between Jun and Fos/Fra proteins, is a key regulator of liver homeostasis and disease. c-jun and c-fos are essential for mouse liver tumorigenesis (2-5), while the two closely related Fra- and Fra-2 proteins have both distinct and overlapping functions in liver fibrosis (7) and hepatosteatosis (7). Here we investigated the hepatic functions of specific Jun/Fos and Jun/Fra AP- dimers in adult mice. Method: Tetracycline-switchable alleles of Fra-, Fra-2 as well as forced c-jun~fra-/2 and Jun~Fos dimers were generated by recombinase-mediated transgene integration in embryonic stem cells. Transgene expression was directed to hepatocytes and temporally controlled using the Lap-tTA allele and ad libitum dietary Doxycycline supplementation. The resulting mice allow temporal, dose-dependent and reversible hepatocyte-specific expression of AP- monomers and forced dimers in vivo. Transgene expression was induced by removing Doxycycline and animals followed up for several months. Results: While expression of Fra-, Fra-2, c-jun~fra- or JunB~c-Fos did not cause an overt phenotype, expression of c-jun~fra-2, c-jun~c-fos or JunD~c-Fos dimers resulted in premature mortality, liver dysfunction as indicated by serum biochemistry and spontaneous liver tumours. Histological analyses revealed dysplastic nodules with hepatocyte proliferation, alpha fetoprotein positivity and immune cell infiltration, with lung metastases and cachexia in the Fos-dimer mutants. Interestingly, sustained c-jun~fra-2 and Fos-dimer expression appeared necessary to maintain the cancer phenotype. Subsequent in depth analyses revealed distinct dimer-specific alterations in hepatocyte morphology, proliferation and dedifferentiation as well as altered expression of pathways connected to human hepatocellular carcinoma (HCC), such as Wnt/ -catenin, nuclear receptors and c- Myc, some of which appear directly regulated by AP-. Conclusion: These results highlight the power of genetically engineered mouse models to exploit and mechanistically dissect the involvement of specific AP- dimers in liver cancer, with the ultimate aim of identifying new prognostic biomarkers and therapeutic targets.. Bakiri L, Wagner EF, Mol Oncol Eferl R, et al., Cell Min L, et al., Nat Cell Biol Trierweiler et al., Cell Death Differ Bakiri L, Hamacher R, et al., J Exp Med Hasenfuss SC et al., Hepatology Hasenfuss SC et al., Cell Metabolism
69 P0-YI LIVER CANCER, NOT ETIOLOGY OR STEATOSIS OR FIBROSIS, IS THE ONLY INDEPENDENT PREDICTOROF ELEVATED PERIOSTIN CONCENTRATION AMONG CAUCASIAN PATIENTS WITH LIVER DISEASE Matteo Nazzareno Barbaglia, Giulia Maria Ghirardi, Violante Mulas, Margherita Tran Minh, Livia Salmi, Deborah Camatta, Michela Emma Burlone, Rosalba Minisini, Mario Pirisi Università del Piemonte orientale, Translational Medicine, NOVARA, Italy Background and Aims: It has been claimed that serum periostin may represent a biomarker of nonalcoholic fatty liver disease (NAFLD). Here, we aimed to verify the association of periostin both with histological steatosis and/or fibrosis, and with etiology of liver disease. Moreover, the possible relationship between genetics of periostin and liver/serum periostin expression was studied. Method: N.=55 patients with either NAFLD (Group A, N.=74) or hepatitis C virus (HCV) infection (Group B, N.=8), as well as N.=27 healthy controls (Group C, N.=27 with normal transient elastography and controlled attenuation parameter), were studied. Serum periostin was measured by the Human Periostin/OSF-2 DuoSet ELISA (R&D Systems, Inc., Minneapolis). POSTN haplotype analysis was based on rs , rs , and rs In N.=45 cases, periostin mrna was quantified on liver biopsy specimens. Results: The median (interquartile range, IQR) serum periostin concentration was.6 ng/ml ( ); it was 0.9 ng/ml ( ) in Group A, 2.0 ng/ml ( ) in Group B, and 2.0 ng/ml ( ) in Group C, respectively (p=0.06). The Table presents serum periostin in relationship to the severity of liver disease. Serum (ng/ml) Total Group A Group B Group C periostin Fibrosis Minimal/absent (N-=79) 0.5 (8.-5.0) 9.9 (6.8-3.) 0.4 ( ) 2.0 (9.-6.3) Fibrosis Moderate (N.=38) 2.0 ( ) 0.9 (7.-.3) 3. ( ) - Fibrosis Advanced (N.=48). ( ) 0.2 ( ).5 ( ) - Hepatocellular carcinoma (N.=7) 6.8 ( ) 5.4 (2.-8.3) 8.2 ( ) - p NA Serum periostin was not associated with steatosis, neither in Group A (p=0.409) nor in Group B (p=0.899) and had a trend to be inversely related to body mass index (Spearman Rho= 0.34, p=0.086). Moreover, there was no association between liver periostin mrna, histological grade or stage, or serum periostin concentration However, possession of the haplotype 2 (rs = G, rs = C, rs = A; N.=6) was associated with lower serum periostin in comparison to all other haplotypes (haplotypes 3-6, N.=65, none had a haplotype ) (.3 pg/ml, IQR vs. 2.3, IQR , p=0.039). At multivariate analysis, HCC was the only independent predictor of high serum periostin concentration (OR=7.3, 95%CI , p=0.005). Conclusion: In Caucasians, serum periostin concentrations are not influenced by etiology of liver disease, fibrosis progression or degree of steatosis. 69
70 P02-0YI HEPATOCELLULAR CARCINOMA INAUGURATING CIRRHOSIS: A DESCRIPTIVE STUDY Soumaya Ben Amor, Arwa Guediche, Olfa Ghannei, Wafa Ben Mansour, Leila Safer faculty of medecine of monastir, gastro-enterology, Tunisia Background and Aims: Hepatocellular carcinoma (HCC) is a redoubtable complication of cirrhosis. If it can be screened in known cirrhotic patients, HCC is still a revealing circumstance of cirrhosis in our country. Our work aims to make a descriptive study of HCC inaugurating cirrhosis. Method: This is a retrospective descriptive study of patients hospitalized for the management of HCC between 2000 and 206. Patients with non-cirrhotic HCC or already known cirrhotic were excluded from the study. For each patient, we have calculated the CLIP score as a prognostic classification system. Results: Of the 83 HCC reported cases, 48 patients (58%) had a HCC inaugurating cirrhosis, divided into 40 men (83.3%) and 8 women of 62 years of age (40-86 years). 63% of the patients were smokers, 29% ethylic and 20% diabetic. The most common complaint was pain in the right hypochondrium (88%). Hepatic dysfunction was noted in the majority of patients (96%). Alpha-fetoprotein was high in 43 patients (90%) with a rate greater than 400 ng / l in 46% of cases. The majority of patients had a CHLID score > = B7, only 3 patients (27%) had CHILD A. Cirrhosis was decompensated in 48% of cases and complicated with gastrointestinal bleeding in 23% cases. The etiology of cirrhosis was dominated by viral infection (B in 79% of cases and C in 0% of cases). All patients underwent abdominal CTA and / or liver MRI. Only 2 patients had a liver biopsy puncture because of atypical vascular kinetics. A single nodule was found in 4 patients (29%). The median diameter of the nodules was 00 mm (50 mm-80 mm). HCC was associated with portal thrombosis in 8 patients (37%). Curative treatment was indicated for 4 patients and palliative arterial chemo-embolization for 6 patients. The treatment was symptomatic for the others. The CLIP score was> = 3 in the majority of patients (63%). Median survival was 9 months (0-50 months). Conclusion: According to our study, HCC complicating and inaugurating viral cirrhosis is a frequent situation with a reserved prognosis. Hence, mass screening programs for viral infections are needed. 70
71 P02-02YI PRESENCE OF HCC DOES NOT AFFECT THE COURSE AND RESPONSE TO ANTICOAGULATION OF BLAND NON MALIGNANT PORTAL VEIN THROMBOSIS IN CIRRHOTIC PATIENTS Francesca Benevento, Anna Pecorelli 2, Horia Stefanescu 3, Zeno Sparchez 3, Irene Pettinari 4, Ranka Vukotic, Crina Grigoras 5, Pietro Andreone, Luigi Bolondi, Fabio Piscaglia, Department of Medical and Surgical Sciences, Bologna, Italy, 2 Unit of Radiology, Monza, Italy, 3 Regional Institute of Gastroenterology and Hepatology "O Fodor",, Gastroenterology Department, Cluj Napoca, Romania, 4 Unit of Radiology, Bologna, Italy, 5 Regional Institue of Gastroenterology and Hepatology, Cluj Napoca, Romania Background and Aims: Malignancies are considered in general a risk factor for thrombosis and may hamper recanalization. HCC often occurs in cirrhosis a condition suffering an incidence of 5-20%/year of Portal Vein Thrombosis (PVT). To investigate whether the natural course and response to anticoagulant treatment of bland PVT in patients with cirrhosis complicated by HCC differs from those without HCC. Method: Retrospective study in two hepatology referral centers, in Italy and Rumenia. Inclusion criteria: diagnosis of bland PVT on cirrhosis between January 2008 and March 206 (based on strict imaging criteria and biopsy when needed). At least 3 months of follow up with repeated imaging. Exclusion criteria: previously treated HCC with no current active tumor; active extrahepatic neoplasm. Recanalization was defined as complete clearance of main portal vein trunk if involved or reduction by 50% in thrombus size. Results: A total of 62 patients with PVT were identified, 30 with HCC that were compared to 32 without HCC. Etiologies, Child-Pugh (7 vs 7) and MELD scores ( vs 2, p=0.3679) did not differ. Anticoagulation was administered to 43% HCC vs 42% nonhcc. The extension of PVT in the main portal trunk was similar: partial/total involvement was 73.3/6.7% in HCC vs 67.4/6.% in nonhcc, p= The remainder had intrahepatic PVT. Overall PVT recanalization was achieved in 30% of HCC vs 37.9% of nonhcc, p= Major bleeding incidence was almost identical (3.3% vs 3.8%, p=). The recanalization rate was 6.5% and 60.7% in HCC / nonhcc in anticoagulated patients (p=). Progression of PVT after stopping therapy did not differ (0% vs 5.9% respectively,p=0.09). Conclusion: The course of bland non-malignant PVT in cirrhosis is not affected by the presence of active HCC. Thus HCC complicated by bland non-malignant PVT could be treated with anticoagulation, possibly enabling otherwise contraindicated therapies (e.g. TACE). 7
72 P02-03 SEROLOGICAL DIAGNOSIS OF EARLY HCC IN NASH: A GERMAN MULTICENTER STUDY Jan Best, Lars Bechmann 2, Alexander Dechêne, Kristina Pflanz, Sotiria Bedreli, Clemens Schotten, Thomas Berg 3, Janett Fischer 3, Arndt Vogel 4, Heike Bantel 4, Arndt Weinmann 5, Jörn Schattenberg 5, Yvonne Huber 5, Henning Wege 6, Kornelius Schulze 6, Johann von Felden 6, Bettinger Dominik 7 8, Robert Thimme 7, Friedrich Sinner 2, Kerstin Schuette 2, Karl Heinz Weiss 9, Sarah Berhane 0, Philip Johnson 0, Guido Gerken, Ali Canbay 2 University Hospital Essen, Germany, 2 Otto-von-Guericke University Magdeburg, 3 University Leipzig, 4 Hannover Medical School, 5 University Medical Center Mainz, 6 University Medical Center Hamburg- Eppendorf, 7 Medical Center University of Freiburg, 8 Faculty of Medicine, University of Freiburg, 9 University Hospital Heidelberg, 0 University of Liverpool, University Hospital Essen Background and Aims: Hepatocellular carcinoma (HCC) is one of the leading causes of death in cirrhotic patients worldwide. There is increasing incidence of HCC in non-alcoholic steatohepatitis (NASH), even in the absence of cirrhosis. NASH is frequently associated with obesity resulting in poor performance of ultrasound surveillance in these patients. This creates an urgent need for serological approaches to ameliorate the current situation with HCC detection predominantly at advanced stages. Therefore, this study aims to explore whether the biomarkers AFP, AFP-L3 and DCP have the potential to be used in the screening setting in NASH patients in a German multicenter cohort. Method: From 8 German centers, 2 NASH patients with newly diagnosed HCC and 224 NASH control patients were enrolled. AFP, AFP-L3 and DCP were measured using the µtaswako i30 automated immunoanalyzer. The diagnostic performance of biomarkers was measured as single parameters, in a logistic regression model and by ROC analysis. A diagnostic algorithm (GALAD) that combined gender, age and the three biomarkers mentioned above was tested in this NASH cohort. Results: AFP, AFP-L3 and DCP showed comparable sensitivities and specificities for HCC detection. The GALAD score achieved an AUROC of 0.98 compared to individual application of AFP (0.88), AFP- L3 (0.92) and DCP (0.88) (p<0.0005) (Fig.). In early stage HCC (BCLC A) the GALAD algorithm again provided the highest overall AUROC (0.93) which was significantly superior to any of the individual markers. Conclusion:This German multicenter NASH-HCC cohort demonstrates a high sensitivity and specificity of the GALAD score for HCC early cases and warrants future prospective study in the surveillance setting. 72

73 Figure: Figure : This figure exhibits the ROC curves, sensitivities and specificities of the individual biomarkers and their combined utilization in the GALAD Score for HCC detection. * This is the optimal GALAD cutoff for specificity and sensitivity for this dataset. **This is the published optimal GALAD cut-off for specificity and sensitivity according to the original GALAD publication (Johnson PJ et al.; Cancer Epidemiol Biomarkers Prev; 204; 23; 44-53) 73
74 P02-04 LIVER TARGETING AND ANTI-TUMOUR EFFICACY OF THE NUCLEOTIDE PRODRUG MIV-88 IN NONCLINICAL MODELS OF HEPATOCELLULAR CARCINOMA Biljana Rizoska, Johan Bylund, Karin Tunblad, Rodrigo Palma Villar, Alastair Kyle 2, Andrew Minchinton 2, Richard Bethell, Karin Göhlin, Mark Albertella Medivir AB, Huddinge, Sweden, 2 BC Cancer, Vancouver, Canada Background and Aims: Troxacitabine (TRX) is a chain terminating nucleoside analogue with preclinical anticancer activity against hepatocellular carcinoma (HCC). Clinical development of TRX (given IV) was halted due to systemic toxicity. MIV-88, a nucleotide prodrug of troxacitabine-monophosphate (TRX- MP), has been designed as a novel approach to deliver high levels of the chain-terminating nucleotide troxacitabine-triphosphate (TRX-TP) to the liver after oral dosing while minimizing systemic exposure. Liver targeting was investigated in rats after oral dosing and anti-tumour efficacy of MIV-88 was evaluated in vivo in HCC mouse xenograft models. Method: MIV-88 (80 µmol/kg, PO) and TRX (80 µmol/kg, PO and IV) were administered to rats. TRX plasma levels and TRX-TP liver levels were analysed by LC-MS/MS. Nude mice with subcutaneous Hep3B or HepG2 xenografts were treated with MIV-88 (30, 50 or 00 mg/kg PO) twice daily for 5 days. Quantitative immuno-fluorescence histology was used to assess DNA damage (ph2ax), proliferation (BrdU), and hypoxia (pimonidazole) in the tumours. Results: MIV-88 administered PO to rats resulted in a liver TRX-TP Cmax of.0 nmol/g and a liver TRX-TP AUC(0-24) of 0 nmol*h/g. The same dose of TRX administered IV and PO resulted in liver TRX-TP concentrations below the limit of quantification (0.05 nmol/g) at all time points. The AUC(0-24) liver TRX-TP vs plasma TRX ratio for MIV-88 after PO dosing was >9 times higher than for TRX after IV dosing. In the Hep3B xenograft model, treatment with MIV-88 resulted in dose-dependent effects on tumour growth inhibition (TGI), reaching a maximal TGI of 40% at 00 mg/kg. Larger antitumour effects were observed in the HepG2 xenograft model, with a maximal TGI of 96% at 00 mg/kg and a tumour growth delay of 23 days, suggesting that the HepG2 model is more sensitive to MIV-88. In both models, the anti-tumour effect correlated with significant changes in the plasma alpha-fetoprotein levels. MIV-88 treatment resulted in dose-dependent inhibition of proliferation (by 94%) and induction of DNA damage (20-fold) in the HepG2 model. Conclusion: MIV-88 is a nucleotide prodrug of TRX with improved liver targeting in rat and anti-tumour effects in mouse xenograft models of HCC. MIV-88 is currently in nonclinical development in preparation for the initiation of clinical trials in patients with advanced HCC and other liver cancers. 74
75 P02-05YI ASSOCIATION OF ANG, ANG2 AND FGF GENETIC POLYMORPHISM AND THEIR EXPRESSION ANALYSIS IN HEPATOCELLULAR CARCINOMA Dipu Bharali, Suresh Kumar 2, Premashis Kar 3 Maulana Azad Medical College, Medicine, New Delhi, India, Maulana Azad Medical College, Medicine, New Delhi, India, 3 Max Superspeciality Hospital, Gastroenterology, New Delhi, India Background and Aims: Hepatocellular carcinoma (HCC) is one of the most malignant tumors and common cause of cancer death in India. HCC is a hypervascular carcinoma due to angiogenesis which is closely regulated by angiogenic factors such as Ang, Ang2 and FGF. This study is designed with an aim to find out the genetic polymorphism and differential expression of these factors in HCC compared to controls without HCC in chronic liver diseases in Indian population. Method: A total of 75 confirm diagnosed HBV related HCC cases and 50 individuals of controls without HCC were included in this study. Ang, Ang2 and FGF DNA polymorphism were analyzed by direct sequencing of the PCR products and their differential expression were done using real time PCR. Results: The Ang CC genotype (p.05; O.R=.8) and Ang AC genotype (p.05; O.R=.2) was found to be a risk in chronic liver diseases patient developing to HCC. C, T allele (Ang) individually was also found to be high risk in chronic liver disease patients for further progress to HCC. Ang2 AA genotype (p<.05; OR=.89) is a risk for chronic hepatitis patients. Allele A is an individual risk of HCC in CLD patients. FGF TT genotype (p<.05; OR=.3) is a risk for chronic liver disease patients. Allele T is an individual risk of HCC in CLD patients. FGF2 CC genotype (p<.05; OR=.06) is a risk for chronic liver disease patients. Allele C is an individual risk of HCC in CLD patients. The expression level of Ang lower in HCC compared to controls without HCC. The difference is significant (p=.002) and also Ang2 and FGF mrna expression level is higher in HCC compared to controls without HCC. The difference is significant (p=.002; p=.00). Conclusion: The abnormal vasculature of HCC might be due to Ang, Ang2 and FGF genetic polymorphism and their differential expression that serves as an important diagnostic element in HCC or cancer diagnosis. Angiogenesis is a very complicated network which is closely regulated by many angiogenic factors. The association of polymorphism of angiogenic factors such as Ang, Ang2 and FGF gene and their expression level might play an important role in the angiogenic and differentiation processes in HCC in CLD and also in initiation and progression of angiogenesis in tumors. Therefore genetic polymorphism of angiogenic factors might be a risk to develop HCC from chronic liver diseases in Indian population. The data on genotype polymorphism and differential expression of angiogenic factors in carcinogenesis found in this study may be worthy for diagnostic and career counselling purpose in Indian popultaion and may also worthy of further study. Key words: HCC, CLD, Ang, Ang2, fibroblast growth factor, single nucleotide polymorphism, PCR. 75

76 P02-06YI LIQUID CRYSTALLINE NANOPARTICLES (LCNPS) BASED DELIVERY OF AN ANTICANCER BIOACTIVE, METHOTREXATE Mani Bhargava, Saurabh Bhargava 2 ICFAI University, India, 2 United Institute Of Pharmacy, India Background and Aims: Liver cancer is a disease of uncontrolled cell growth, which may invade adjacent tissue and cause infiltration beyond the liver. Most of the potent and effective anticancer drugs used in liver cancer therapy shows poor bioavailability at desired site as well as toxic in nature.the aim of the study was to investigate mannose modified Liquid Crystalline Nanoparticle(LCNPs) carrier for efficient and site specific delivery of potent anticancer drug (Methotrexate) used in hepatic carcinoma therapy. Method: MTX loaded LCNPs were prepared by lipid cast film method and sonication method. The nanoparticles were characterized in-vitro for their shape, size, percent drug entrapment and stability by Optical Microscopy, Cross Polarized Light Microscpy (CPLM), Transmission Electron Microscopy (TEM), X-ray diffraction (XRD) and Atomic Force Microscopy (AFM). Results: In-vitro stability studies reveal that LCNPs formulations are stable for 20 days at room temperature. Ex-vivo cell cytotoxicity was performed on Human hepatoma cell line. In-vivo studies included fluorescence microscopy and organ distribution studies which show the Mannose modified LCNPs exhibit better accumulation in liver as compared to unmodified system. The results of the present study indicate, this system is more stable as compared to other system. Conclusion: Eventually it may be concluded that incorporation of MTX in mannose modified LCNPs increases the residing time of drug in the body by altering of pharmacokinetics and biodistribution pattern, and the drug primarily concentrates in the liver. This system showed excellent cytotoxicity towards cancer cells. From the present investigation it is evident that this system may be used for liver cancer and other liver disease. Figure: 76
77 P02-08YI EVALUATION OF PROGNOSTIC FACTORS OF OVERALL SURVIVAL AND PROGRESSION-FREE SURVIVAL IN PATIENTS WITH HEPATOCELLULAR CARCINOMA Igor Bramuzzo, Alessio Gerussi, Silvia Maier, Cristiana Bianco, Valerio Barghini, Laura Scatà, Cristiana Laghi Pasini, Arianna Romanin, Debora Donnini, Alessandro Vit 2, Alessandro Uzzau 3, Leonardo Alberto Sechi, Giorgio Soardo University of Udine, Liver unit, Internal Medicine, Department of Experimental and Clinical Medical Sciences, Udine, Italy, 2 Azienda Sanitaria Univeristaria Integrata Udine, Division of Vascular and Interventional Radiology, Udine,, 3 University of Udine, Program of oncological surgery, Department of Experimental and Clinical Medical Sciences, Udine, Italy Background and Aims: HCC is a common malignancy worldwide, characterized by an heterogenous presentation, ranging from an asymptomatic nodule detected on surveillance imaging to advanced and symptomatic cancer. To identify prognostic factors at diagnosis is of paramount importance to better stratify patients and guide appropriate and tailored treatment strategies. Method: 57 patients managed at a single tertiary center for a first diagnosis of HCC between January 20 and December 206 were retrospectively included. Transplanted patients (9) were excluded from the analysis. Demographics features and laboratory values at diagnosis were collected and Child-Pugh score, model for end stage liver disease (MELD), aspartate aminotransferase platelet ratio index (APRI score) were calculated. The extension of the tumor burden was classified according to Milan criteria and patients were stratified according to Barcelona Clinic Liver Cancer (BCLC) classification. Cases were censored at the occurrence of death. A multivariate Cox regression analysis was performed to assess factors independently associated with overall survival and relapse at any time. Results: Median age of the cohort was 69 years (IQR 2). Cirrhotic patients were 20 (87%) and the most frequent etiologies were alcoholic (65, 47.%) and HCV (45, 32.6%). The majority of patients were in BCLC stage A or B (72.4 %), and 70 patients (50.7%) did not meet Milan criteria. On multivariate Coxregression analysis higher Child-Pugh values (HR.88, p <0.00), not fulfilling Milan criteria (HR 2.07, p 0.05), higher values of alkaline phosphatase (ALP) (HR 2.6, p <0.004) and higher values of alphafetoprotein (afp) (HR.6, p <0.003) were independently associated with worse outcome. Stratifying according to BCLC stage, higher values of ALP increased the hazard of death only in stage 0 and A. Higher APRI score (HR.34, p < 0.002) and not fulfilling Milan criteria (HR.97, p < 0.027) were found to be independent predictors of relapse at any time. Conclusion: Our data underline the established role of numbers and size of HCC nodules, according to Milan criteria, and degree of hepatic failure in predicting prognosis of patients with HCC. The study also adds a piece of evidence that afp and ALP, for overall survival, and APRI score, for relapse at any time, are cheap and simple prognostic biomarkers and scores that should be taken into account. 77
78 P02-09YI ANTI-INFLAMMATORY POLARIZATION OF TUMOR ASSOCIATED MACROPHAGES PROMOTING TUMOR GROWTH AND ANGIOGENESIS IN HCC OF CHEMOKINE RECEPTOR CXCR3 DEFICIENT MICE Elisa Fabiana Brandt, Petra Fischer, Theresa Wirtz, Christian Trautwein, Hacer Sahin, Marie- Luise Berres Aachen, Uniklinik, Medical Department III, Aachen, Germany Background and Aims: The tumor microenvironment can be classified in two parts - cellular and noncellular components-. The cellular component includes peritumoral parenchymal cells as well as nonparenchymal cells e.g. infiltrating immune cells. These cells produce the non-cellular components, including growth factors and inflammatory cytokines. HCC progression is linked to the dynamic crosstalk between tumor cells and the tumor microenvironment. Chemokine receptor CXCR3 is implicated in these processes and plays a key role during acute and chronic liver injury in mice and human. Here we aimed to investigate the role of CXCR3 in HCC progression. Method: HCC was induced in Cxcr3 -/- and wild-type (WT) mice via a single i.p. injection of N- Diethylnitrosamin (DEN, 4 d after birth) and weekly i.p. injections of low dose carbon tetrachloride (CCl4, week 4-26). Mice were sacrificed after 26 weeks and tumor burden was assessed. Liver tissue was characterized by histologically staining for proliferation, apoptosis and vascularization markers (Ki67, cleaved caspase 3 and CD3). The HCC-related immune response was analyzed by multicolor flow cytometry (leukocyte subpopulations) and immunofluorescence staining (e.g. CD68, F4/80) with specific focus on tumor associated macrophage (TAM)-related immune response. In vitro, Cxcr3 -/- and WT bone marrow culture-derived macrophages (BMM) and TAMs were stimulated with conditioned medium of Hepa-6 cells. The mrna expression of HCC and inflammation related genes were determined by quantitative RT-PCR. Furthermore, macrophage phenotype was assessed by flow cytometry and immunofluorescence staining. Results: Liver of DEN/CCl4 treated Cxcr3 -/- mice displayed a significantly increased tumor burden compared to WT mice, which was strongly associated with a higher number of proliferative tumor cells (Ki67) and enhanced CD3+ microvessel density. Moreover, deteriorated HCC phenotype in Cxcr3 -/- mice was linked to an accumulation of CD68+ macrophages associated with reduced number of apoptotic macrophages (cl.caspase 3) in tumor and surrounding tissue. Cxcr3 -/- macrophages could be further subcategorized to an anti-inflammatory Ly6C low /MHCII low phenotype by flow cytometric analysis. In vitro, control and conditioned medium fosters survival and expression of anti-inflammatory, proangiogenetic cytokines and hepatic growth factor (qpcr) in Cxcr3 -/- macrophages, which was also reflected by expression analysis in the mouse model. Conclusion: Our results indicate a functional link between Cxcr3 and angiogenesis as well as tumor cell proliferation mediated by TAM polarization and survival in a murine liver cancer model. These data suggests that CXCR3 could be a new therapeutic target for HCC treatment modulating macrophage polarization and neovascularization. 78
79 P02-0 HAND FOOT SKIN REACTION AND OVERALL SURVIVAL IN THE PHASE 3 RESORCE TRIAL OF REGORAFENIB FOR TREATMENT OF HEPATOCELLULAR CARCINOMA PROGRESSING ON SORAFENIB Jordi Bruix, Philippe Merle 2, Alessandro Granito 3, Yi-Hsiang Huang 4, György Bodoky 5, Osamu Yokosuka 6, Olivier Rosmorduc 7, Valeriy Breder 8, René Gerolami 9, Gianluca Masi 0, Paul J. Ross, Shukui Qin 2, Tianqiang Song 3, Jean-Pierre Bronowicki 4, Isabelle Ollivier-Hourmand 5, Masatoshi Kudo 6, Lei Xu 7, Annette Baumhauer 8, Gerold Meinhardt 7, Guohong Han 9, on behalf of the RESORCE Investigators BCLC Group, Liver Unit, Hospital Clinic, University of Barcelona, IDIBAPS, CIBEREHD, Barcelona, Spain, 2 Groupement Hospitalier Lyon Nord, Hepatology Unit, Lyon, France, 3 Department of Medical and Surgical Sciences, University of Bologna, S. Orsola-Malpighi Hospital, Bologna, Italy, 4 Division of Gastroenterology and Hepatology, Taipei Veterans General Hospital; Institute of Clinical Medicine, National Yang-Ming University, Taipei, Taiwan, 5 St. Laszlo Teaching Hospital, Budapest, Hungary, 6 Department of Gastroenterology and Nephrology, Chiba University, Chiba, Japan, 7 Department of Gastroenterology and Hepatology, Hôpital de la Pitié-Salpêtrière, Assistance Publique-Hôpitaux de Paris and Université Pierre et Marie Curie, Sorbonne Universités, Paris, France, 8 National Medical Research Center of Oncology n.a.n.blokhin, Moscow, Russian Federation, 9 CHU Timone, Université de la Méditerranée, Marseille, France, 0 Azienda Ospedaliero-Universitaria Pisana, Pisa, Italy, King s College Hospital NHS Foundation Trust, London, United Kingdom, 2 Chinese People s Liberation Army Cancer Center of Nanjing Bayi Hospital, Nanjing, China, 3 Tianjin Medical University Cancer Hospital, Tianjin, China, 4 INSERM 954, CHU de Nancy, Université de Lorraine, Nancy, France, 5 Service d Hépatogastroentérologie, CHU, Caen, France, 6 Kindai University Faculty of Medicine, Osaka, Japan, 7 Bayer HealthCare Pharmaceuticals, Whippany, NJ, United States, 8 Bayer AG, Leverkusen, Germany, 9 Department of Liver Disease and Digestive Interventional Radiology, National Clinical Research Center for Digestive Disease, Xijing Hospital of Digestive Diseases, Xijing Hospital, Fourth Military Medical University, Xi an, China Background and Aims: Skin toxicity is a known adverse effect of multikinase inhibitors, and was shown to be a predictor of overall survival (OS) in patients (pts) with hepatocellular carcinoma (HCC) treated with sorafenib (Reig M, 204). In the RESORCE trial, regorafenib improved OS versus placebo in pts with HCC progressing on sorafenib (hazard ratio [HR] 0.62, 95% confidence interval [CI] ; Bruix J, 207). This retrospective analysis explored whether hand foot skin reaction (HFSR) with regorafenib was associated with OS in RESORCE. Method: Pts in RESORCE who were randomised to regorafenib 60 mg/day during the first 3 weeks of each 4-week cycle were divided into subgroups based on whether or not they had HFSR. Estimates of OS (95% CI) were calculated using the Kaplan Meier method. Pts who were randomised, but not treated, were included in the no HFSR group for the analysis of survival. Results: Of 379 pts randomised, 374 received at least dose of regorafenib. Of the treated pts, 53% (n=99) had HFSR of any grade and 3% (n=47) had grade 3 HFSR. Among pts with HFSR at any time during the study, 77% (n=53) had the first HFSR event (any grade) during Cycle. Subgroups of pts with and without HFSR at any time had some imbalances in baseline characteristics (Table). OS was improved in pts who had HFSR at any time versus those who did not (Table). Pts who had a HFSR event during Cycle also had improved OS versus those who did not (median OS 3.2 vs 8.5 months; HR 0.66, 95% CI ). Conclusion: In this post-hoc exploratory analysis, HFSR with regorafenib was associated with a longer OS, as was previously shown for sorafenib. Development of HFSR during regorafenib treatment should lead to dose adjustment according to established recommendations. 79
80 Table: HFSR (any grade; n=99) Median age, years (range) 6 (2 84) Geographic region Asia/Rest of World, % 50/50 ECOG performance status 0/, % 75/25 BCLC stage A/B/C, %* /7/83 Alpha-fetoprotein 400 ng/ml, % 40 Macrovascular invasion (MVI), % 24 Extrahepatic disease (EHD), % 68 MVI and/or EHD, % 77 No HFSR (n=80) 65 (9 85) 24/76 54/46 0// Child Pugh score 5/6/7, % 76/22/2 Median OS, months (95% CI) 4. (.7 6.5) HR (95% CI) 0.52 ( ) 5/47/ 6.6 ( ) *Numbers may not sum to 00 due to rounding; Child Pugh score missing in pt. BCLC, Barcelona Clinic Liver Cancer; ECOG, Eastern Cooperative Oncology Group. 80
81 P02- INTRA-TUMORAL TERTIARY LYMPHOID STRUCTURES ARE ASSOCIATED WITH A LOW RISK OF EARLY TUMOR RECURRENCE IN PATIENTS WITH HEPATOCELLULAR CARCINOMA Julien Calderaro, Florent Petitprez 2, Etienne Becht 2, Théo Hirsch 3, Benoit Rousseau 4, Giuliana Amaddeo 5, Jessica Zucman-Rossi 3, Hervé Fridman 2, Catherine Sautès-Fridman 2 Henri Mondor University Hospital, Pathology, Créteil, France, 2 Centre de Recherche des Cordeliers, Inserm U38, Paris, France, 3 Inserm U62, Functional genomics of solid tumors, Paris,, 4 Henri Mondor University Hospital, Hepatology, Créteil,, 5 Henri Mondor University Hospital, Surgery, Créteil, Background and Aims: Tertiary lymphoid structures (TLS) provide a local and critical microenvironment for the induction of anti-tumoral cellular and humoral immune responses, and are associated with improved clinical outcome in most solid tumors investigated so far. Their role in hepatocellular carcinoma (HCC) is however debated, as they have recently been shown to promote, in the non-tumoral liver, the growth of malignant hepatocyte progenitors. We thus aimed to determine the significance of intra-tumoral TLS in HCC. Method: We investigated the prognostic impact of intra-tumoral TLS in 2 independent retrospective cohorts of patients with HCC treated by surgical resection (Henri Mondor University (HMN) Hospital Cohort n=273, analyzed by pathological reviewing, and LCI (Liver Cancer Institute) Cohort n=225, analysed by gene expression profiling). Clinical endpoint was early recurrence, which is considered to reflect metastasis of the resected primary tumor rather than de novo carcinogenesis. Results: Pathological reviewing identified TLS in 47% of the tumors of the HMN series, with lymphoid aggregates, primary and secondary follicles in 26%, 6% and 5% of the cases, respectively. Univariate and Multivariate analyses showed that intra-tumoral TLS were significantly associated to a lower risk of early relapse (<2 years after surgery, hazard ratio 0.47, p=0.004). Interestingly, the risk of recurrence was also related to the degree of TLS maturation (primary or secondary follicles vs lymphoid aggregates, p=0.0). A gene-expression signature associated with the presence of intra-tumoral TLS was also independently associated with a lower risk of early relapse in the LCI cohort (hazard ratio 0.45, p=0.0). No correlation with any clinical, biological or pathological feature was identified. Conclusion: We have shown in two independent series of patients with HCC treated by surgical resection that intra-tumoral TLS are associated with a lower risk of early relapse. Depending on their location, TLS are thus likely to play a dual role in human hepatocarcinogenesis Figure: A HMN Cohort Early recurrence B LCI Cohort Early recurrence TLS TLS TLS - p= TLS - p=0.006 Numbers at risk Time (months) Numbers at risk Time (months) TLS TLS TLS TLS Legend: In both series investigated (HMN A, LCI B), intra-tumoral TLS were significantly associated to a lower risk of early relapse (<2 years after surgery). 8
82 P02-2 HEPAVAC-0 FIRST-IN-MAN THERAPEUTIC CANCER VACCINE PHASE I/II CLINICAL TRIAL FOR HEPATOCELLULAR CARCINOMA PATIENTS Andrea Mayer-Mokler, Yuk T. MA 2, Roberto Accolla 3, Regina Heidenreich 4, Antonio Avallone 5, Alfred Koenigsrainer 6, Markus Loeffler 6 7, Cecile Gouttefangeas 7, Christian Flohr, Jorg Ludwig, Sarah Kutscher, Hans-Georg Rammensee 7, Bruno Sangro 8, Sven Francque 9, Danila Valmori 0, Tanguy Chaumette 0, Toni Weinschenk, Carsten Reinhardt, Ulrike Gnad-Vogt 4, Hapreet Singh- Jasuja, Luigi Buonaguro 5 Immatics Biotechnologies GmbH, Tübingen, Germany, 2 Univ. of Birmingham, NIHR Biomedical Research Unit in Liver Disease, School of Immunity and Infection, Birmingham, United Kingdom, 3 Univ. of Insubria, Surgical and Morphological Sciences, Varese, Italy, 4 CureVac AG, Tübingen, Germany, 5 National Cancer Institute "Pascale", Medical Oncology, Naples, Italy, 6 Univ. Hospital of Tuebingen, General, Visceral and Transplant Surgery, Tübingen, Germany, 7 Univ. of Tuebingen, Immunology, Tübingen, Germany, 8 Clinica Universidad de Navarra and CIBEREHD, Liver Unit, Pamplona, Spain, 9 Antwerp Univ. Hospital, Gastroenterology and Hepatology, Edegem, Belgium, 0 Univ. of Nantes, EA Thérapeutiques cliniques et expérimentales des infections, Nantes, France Background and Aims: HepaVac-0 is a phase I/II, first-in-man, single-arm clinical trial assessing the safety, tolerability and immunogenicity of a therapeutic cancer vaccine IMA970A adjuvanted with CV802 in hepatocellular carcinoma (HCC) patients. IMA970A is an off-the-shelf, multi-peptide-based HCC vaccine composed of 6 newly discovered and overexpressed tumor-associated peptides (TUMAPs) directly identified from resected HCC tissues. Of these TUMAPs, 7 are restricted to HLA- A*02, 5 to HLA-A*24 and 4 to HLA class II. CV802 is a novel ribonucleic acid (RNA) based immunostimulatory agent consisting of a single-stranded, non-coding, long-chain RNA. CV802 has the ability to increases the immunogenicity of peptide based antigens and induces balanced immune responses, comprising humoral and cellular, Th and Th2, as well as effector and memory responses. Method: Patients with very early, early and intermediate stage of HCC are enrolled to be treated with a single pre-vaccination infusion of low-dose cyclophosphamide, followed by 9 intradermal vaccinations consisting of IMA970A plus CV802. The study drugs are applied without concomitant anti-tumor therapy, in order to reduce risk of tumor recurrence/progression in patients having received all indicated standard treatments. The primary endpoints are safety, tolerability, and immunogenicity. Secondary/exploratory endpoints are additional immunological parameters in circulation (e.g. regulatory T-cells, myeloid-derived suppressor cells, impact of the standard therapy on the natural immune response), infiltrating T-lymphocytes in tumor tissue, biomarkers in blood and tissue, disease-free survival/progression-free survival and overall survival. Once safety of this vaccination approach has been established in the first 0-20 patients the addition of a checkpoint inhibitor is considered. Overall, it is planned to enroll 40 patients. Suitable patients enrolled at Tuebingen are invited to participate in a trial extension investigating an actively personalized vaccine (APVAC). Results: The HepaVac-0 trial is conducted in 6 centers located in 5 European countries, i.e. Italy (Naples and Negrar), Germany (Tübingen), UK (Birmingham), Spain (Pamplona) and Belgium (Antwerpen). The clinical trial protocol has been approved by all 5 involved Regulatory Agencies and 4 ethical review committees. Three clinical sites are actively recruiting patients and one additional site will start enrollment in Dec 207. As of the time of abstract submission, 3 HCC patients have been screened for HLA haplotype and is eligible for vaccination. Conclusion: The HepaVac project started in September 203 and is supported by the EU 7 th FP under the Grant Agreement Nr ( The HepaVac-0 trial identification numbers are NCT (Clinical trials.gov) as well as (EudraCT). 82
83 P03-0YI GENOMIC EXPRESSION ANALYSIS OF INFILTRATING NATURAL KILLER CELLS SUGGESTS A MIGRATION DEFECT INTO THE TUMOR MICROENVIRONMENT Gabriele Missale, Diana Canetti, Chiara Carone 2, Valeria Regina, Valentina Capizzuto, Andrea Olivani, Raffaele Dalla Valle 3, Carlo Ferrari, Elisabetta Cariani 2 Infectious Diseases and Hepatology, 2 Toxicology and Advanced Diagnostics, 3 Department of Surgery Background and Aims: Natural Killer (NK) cells represent one of the most important arms of anti-tumor immune activity. Reduced intra-tumor NK cell infiltrate and dysfunction have been observed in several human solid tumors, including hepatocarcinoma (HCC), and associated with poor clinical outcome. Our aim was to investigate the molecular mechanisms associated with NK cell functional deficiency in HCC. Method: Tumor and non-tumorous tissues obtained from patients undergoing liver resection for early HCC in HCV-related cirrhosis were processed in order to derive viable lymphomononuclear cell infiltrate. CD56+CD3- NK cells were derived by fluorescence flow-cytometry cell sorting. Genomic expression on tissue infiltrating NK cells was studied by RNA extraction, PCR amplification followed by hybridization with Sure Print G3 Human GE v3 60K (Agilent). Microarrays data were analyzed by Ingenuity Pathway Analysis 8.5 (IPA) software. Results: Comparison of non-tumor liver infiltrating NK-cells (L-NK) and tumor infiltrating NK-cells (T- NK) showed 22 differentially expressed (DE) genes (0 up and 2 downregulated). Functional analysis showed activation of a single pathway, Phospholipase C Signaling, in L-NK. Analysis based on function and networking of DE genes showed activation of functions: cell movement of leukocytes and transmigration of mononuclear leukocytes, both upregulated in L-NK vs T-NK. Next we analyzed networks in order to identify biologically relevant (hub) genes. The hub gene of the L-NK/T-NK network was CCR2, involved in NK cell recruitment during inflammation, that was downregulated in T-NK cells. Conclusion: Our results suggest impaired activation of NK cells in HCC and identify cell movement, adhesion and migration as possible mechanisms involved in NK-cell dysfunction. 83
84 P03-02 GLYCOLYTIC ENZYMES PKM2 AND PGK ARE INSTRUMENTAL TO DNA DAMAGE PROTEIN CHK2 IN SUSTAINING GENOMIC INSTABILITY IN HEPATOCELLUAR CARCINOMA Vinicio Carloni, Matteo Lulli 2, Stefania Madiai, Caecilia Sukowati 3, Andrea Galli 4, Antonio Mazzocca 5, Hiromi Imamura 6 University of Florence, Department of Experimental and Clinical Medicine, 2 University of Florence, Department of Experimental and Clinical Biomedical Science, General Pathology Unit, 3 Italian Liver Foundation, Centro Studi Fegato, Trieste, 4 University of Florence, Department of Experimental and Clinical Biomedical Science, Gastroenterology Unit, Italy, 5 University of Bari, Interdisciplinary Department of Medicine, Italy, 6 Kyoto University, Department of Functional Biology, Graduate School of Biostudies, Japan Background and Aims: 8 F-FDG PET-CT has been indicated superior to Gd-EOB-DTPA-enhanced MRI to predict microvascular invasion and recurrence within 2 years after curative hepatic resection for hepatocellular carcinoma (HCC). The uptake of 8 F-FDG (fludeoxyglucose) by dysplastic/neoplastic tissue is a marker for the uptake of glucose on PET-CT, and glucose is a major source of cellular energy (ATP) and new cell mass for proliferating cells. However, this vision represents a partial view on glucose requirements by neoplastic cells. Recently, we identified that inappropriate activation of mitotic DNA damage protein CHK2 induces chromosome segregation errors promoting DNA damage and chromosomal instability (Gut 207; doi:0.36/gutjnl ). The aim of the study was to investigate the contribute of mitotic DNA damage/chromosomal instability (CIN) and the role of CHK2 in fuelling aerobic glycolysis. Method: The transgenic mouse expressing PreS, S and X proteins of HBV was employed. To assess the functional role of glycolytic enzymes hexokinase I, PKM2, phosphoglycerate kinase (PGK) gain on-and loss-of-function, immunofluorescence and live imaging were performed. Results: Displastic/neoplastic lesions of transgenic mice showed nuclear upregulation of Chk2 and phospho-histone H2AX (y-h2ax) known to be expressed in the presence of DNA damage. This coincided with the cytoplasmic expression of PKM2 a pyruvate kinase isoform which is upregulated in several human cancers. In vitro, Chk2 and y-h2ax negative Huh7 cells expressed low levels of hexokinase I, PKM2, and PGK. Conversely, Chk2 and y- H2AX positive HuS cells overexpressed hexokinase I, PKM2, and PGK. Furthermore, transaldolase a rate-limiting enzyme of pentose phosphate pathway not showed difference between Huh7 and HuS. Interesting PKM2, and PGK two ATP-generating enzymes co-localized with centromeric protein CENP-A and Chk2 in mitotic HuS cells but not in Huh7. Co-localization of PKM2 and PGK with mitotic structures suggests the need to maintain high levels of ATP due to mitotic DNA damage/cin as revealed by time-lapse microscopy in HuS cells transfected with the FRET-based biosensor for ATP. Conclusion: The data obtained reveal an unprecedented mechanistic linkage between aerobic glycolysis and mitotic DNA damage response/cin. The results derived from this study may have several immediate consequences. First, HCC evaluation with 8 F-FDG PET-CT could provide information such as the presence of mitotic DNA damage/cin. Second, mitotic DNA damage response requires robust glucose availability that can be diverted e.g. from T cell and macrophages and this may limit anti-tumor immune responses. Third, a better understanding of the connection between mitotic DNA damage/cin and aerobic glycolysis will contribute to a better use of therapeutic strategies in the management of HCC. 84
85 P03-03YI IMMUNE INFLAMMATION INDICATORS AND ALBI SCORE TO PREDICT OCCURRENCE AND RECURRENCE OF HEPATOCELLULAR CARCINOMA IN HCV-RELATED CIRRHOSIS TREATED WITH DIRECT-ACTING ANTIVIRALS Andrea Casadei Gardini, Francesco Foschi 2, Fabio Conti 3, Giorgia Marisi, Stefano Brillanti 4, Pietro Andreone 4 IRST-IRCCS, 2 ASL Romagna, 3 Unibo, 4 UNIBO Background and Aims: Recent studies have shown unexpected high HCC recurrence rate of 27%- 29% among patients treated with resection or ablation, who received DAA therapy, but this results were not reproduced in others analyses.the aim of this study was to evaluate the prognostic value for occurrence and recurrence of hepatocellualr carcinoma of ALBI grade and immunoinflamation indicators[systemic immune- inflammation index(sii);platelet to lymphocyte ratio(plr);ast to lymphocyte ratio index(alri)]in patients treated with DAA for chronic hepatitis C. Method: In this retrospective cohort study, we analysed data from all the consecutive patients with cirrhosis who were prospectively enrolled for treatment with DAAs. We analysed the basal level of NLR, SII, PLR, ALRI and ALBI at baseline. Results: For patients without history of previous HCC we analysed the clinical characteristics and the risk of HCC development. Based on univariate analysis, increase of AST (p = 0.036, HR:.0, 95% CI:.00.0), increase of bilirubin (p = 0.035, HR:.46, 95% CI: ), decrease of albumin (p = 0.004, HR: 0.34, 95% CI: ),increase ALRI score (p =v0.002, HR:.0, 95% CI:.0.0) decrease of platelets (p = 0.007, HR: 0.99, 95% CI: ) and increase of ALBI grade (p = 0.00, HR: 2.99, 95% CI: ) were significantly associated with HCC development. At multivariate analysis, two variables resulted independently associated with HCC development: increase of ALBI grade (p = 0.038, HR: 2.35, 95% CI: ) and decrease of platelets (p =0.048, HR: 0.99, 95% CI: ). For patients with history of previous HCC we analysed the clinical characteristics and the risk of HCC recurrence. Based on univariate analysis, increase of ALRI (p = HR:.00, 95% CI:.0.20;) were significantly associated with HCC recurrence. We evaluate clinical parameters between basal and end of treatment. We show that the treatment determines a statistically significant increase of neutrophils (patients without previous HCC: 3.7 ±.47; patients with previous HCC 2.72 ±.2) and decrease in lymphocytes (patients without previous HCC:.47 ± 0.79; patients with previous HCC.25 ± 0.67), the different was statistically significant. Conclusion: Low cost, easy determination, and reproducibility of a full blood count make ALBI grade, platelets and ALRI a promising tool for evaluate patients with high risk of hepatocellular carcinoma after treatment with direct-acting antiviral. 85
 represents the fifth most common form of cancer worldwide and carries a high mortality rate due to lack of")
86 P03-04YI EPIGENETIC CONTROL OF HEPATIC HOMEOSTASIS Marco Cassano, Andrew Macpherson 2, Didier Trono 3 EPFL, Lausanne, Switzerland, 2 Mucosal Immunology Lab, Department of Clinical Research, Switzerland, 3 EPFL, Switzerland Background and Aims: Hepatocellular carcinoma (HCC) represents the fifth most common form of cancer worldwide and carries a high mortality rate due to lack of effective treatment (Fattovich et al, 2004). Males are eight times more likely to develop HCC that females, an effect largely driven by sex hormones, albeit through still poorly understood mechanisms (Bosch et al. 2004). Method: We previously identified TRIM28 (tripartite protein 28), a scaffold protein capable of recruiting a number of chromatin modifiers, as a crucial mediator of sexual dimorphism in the liver. Trim28 hep-/- mice display sex-specific transcriptional deregulation of a wide range of bile and steroid metabolism genes and development of liver adenomas in males. Results: We now demonstrate that obesity and aging precipitate alterations of TRIM28-dependent transcriptional dynamics, leading to a metabolic infection state responsible for highly penetrant malerestricted hepatic carcinogenesis. Molecular analyses implicate aberrant androgen receptor stimulation, biliary acid disturbances, and altered responses to gut microbiota in the pathogenesis of Trim28 hep-/- - associated HCC. Correspondingly, androgen deprivation markedly attenuates the frequency and severity of tumors, and raising animals under axenic conditions completely abrogates their abnormal phenotype, even upon high-fat diet challenge. Conclusion: This work underpins how discrete polyphenic traits in epigenetically metastable conditions can contribute to a cancer-prone state and more broadly provides new evidence linking hormonal imbalances, metabolic disturbances, gut microbiota, and cancer. Given the close similarity with the human hepatocarcinogenesis, our model provides a powerful tool to investigate new therapeutic approaches targeting the microbiota modulation. Humanized gnotobiotic cancer-prone mice could represent the ideal milieu for conducting proof-of-principle clinical trials aimed to tests the environmental impact of corrupted microbiota in the host physiology. Figure: 86
87 P03-05YI PATIENT-DERIVED LIVER CANCER CELL LINES IN PERSONALIZED TREATMENT APPROACH: FROM PHENOTYPIC AND MOLECULAR CHARACTERIZATION TO THERAPEUTIC TARGET IDENTIFICATION Darko Castven, Diana Becker, Carolin Czauderna, Diana Wilhelm, Jesper Andersen 2, Susanne Strand, Stefanie Heilmann-Heimbach 3, Wilfried Roth 4, Nils Hartmann 4, Beate Straub 4, Friederike Mahn, Sophia Franck, Sharon Pereira, Monika Hartmann, Anna Haupts 4, Arndt Vogel 5, Marcus-Alexander Wörns, Arndt Weinmann, Stefan Heinrich 6, Hauke Lang 6, Snorri Thorgeirsson 7, Peter Galle, Jens Marquardt Johannes Gutenberg University, Department of Medicine I, Lichtenberg Research Group, Mainz, Germany, 2 University of Copenhagen, Biotech Research and Innovation Centre (BRIC), Department of Health and Medical Science, Copenhagen, Denmark, 3 University of Bonn, Department of Genomics, Life & Brain Center, Bonn, Germany, 4 Johannes Gutenberg University, Institute of Pathology, Mainz, Germany, 5 Hannover Medical School, Department of Gastroenterology, Hepatology and Endocrinology, Hannover, Germany, 6 Johannes Gutenberg University, Department of Surgery, Mainz, Germany, 7 National Cancer Institute, Laboratory of Human Carcinogenesis (LHC), Center for Cancer Research, Bethesda, United States Background and Aims: Primary liver cancers (PLCs) rank among the most lethal solid cancers worldwide due to lack of effective biomarkers for early detection and limited treatment options in advanced stages. While cell lines have been of significant impact for cancer research over the last decades, development of in vitro models that closely recapitulate phenotypic and molecular diversity of the primary cancers is urgently needed to improve the outcome of patients. Method: Long-term culture of 0 liver cancer cell lines of hepatocellular, cholangiocellular and metastatic origin were established using defined culture conditions. Morphological and histological characteristics of obtained cell lines and xenograft tumors were analyzed and compared to original tumors. Further, time course analyses of transcriptomic and genomic changes were performed using next-generation sequencing (NGS). Key oncogenic alterations were further identified by targeted NGS and cell lines carrying potentially actionable mutations were treated with corresponding specific inhibitors. Response to the treatments was further evaluated. Results: The newly patient-derived cell lines (PDCL) fully resembled morphological features of the primary cancers in vitro and in vivo. Genomic alterations as well as transcriptome profiles of the PDCL showed high concordance with the primaries and remained stable for at least 30 passages. Nextgeneration sequencing approaches confirmed that key oncogenic mutations such as TP53, KRAS, CTNNB as well as potentially actionable mutations (e.g. MET, ckit, KDR) were highly conserved in the PDCL. Integrative genomic and transcriptomic approaches demonstrate the utility of PDCL as representative model for distinct prognostic subpopulations of liver cancer patients. Moreover, the PDCL could be effectively used for therapeutic testing. Specific targeting of detected actionable mutations, such as MET and ckit, confirmed a superior response and sustained sensitivity to specific inhibition in comparison to non-mutated control cells. Conclusion: Together, our integrative analysis demonstrates that the use of newly established cell lines represents a sophisticated model to discover relevant molecular subgroups and to test drug sensitivity by exploring precision medicine approaches. 87
88 P03-06YI DEVELOPMENT OF SLN AS CARRIERS FOR DELIVERY OF HEPATITIS B FOR VACCINATION USING SUBCUTANEOUS ROUTE Mani Bhargava, Saurabh Bhargava 2, Vishal Bhargava 3 ICFAI University, India, 2 United Institute Of Pharmacy, India, 3 KRV Hospitals, India Background and Aims: The search for innovative ways of vaccination has intensified recently with declining vaccine coverage and growing public concern about new virulent disease outbreaks. Immunization is a prophylactic approach through which the body is shielded from any incoming pathogenic invasion. The work envisaged here concerns exploring potential of Solid Lipid Nanoparticles(SLN) in efficient protein delivery through surface modifications, which will in turn; enhance loading efficiency and cellular uptake of SLN using subcutaneous route. Method: The SLN were prepared by Solvent Injection Method. SLN were optimized for various parameters as lipid, surfactant concentration, stirring time and speed. By considering particle size, polydispersity index (PI) and entrapment efficiency. The characterization parameters included Transmission & Scanning Electron Microscopy, X-Ray Diffraction Analysis, In-vitro release, Kinetics of uptake by flow cytometer, Evaluation of cell apoptosis, T-cell proliferative response assay, TH/TH2 cytokine profile and Internalization studies by spectral bioimaging. The in-vivo study comprised of fluorescence studies and estimation of IgG response in serum and siga in various body secretions using specific ELISA. Results: The particulate system is better carrier system for immunization because of less diffusivity and restricted movement. SLNs themselves act as signal for the phagocytic cells.surface modified SLNs can entrap greater amount of antigen, provide its sustained release and rapidly internalized by the antigen presenting cells.in-vitro T cell proliferation and induction of TH type of immune response clearly marks the potential of this novel carrier system.fluorescence uptake studies showed better uptake of surface modified SLNs.Higher and more sustained antibody titer obtained with surface modified SLNs suggests their better immunological potential. Thus, subcutaneous immunization could be an efficient alternative approach for vaccination against hepatitis. Conclusion: The formulations developed in this study can be further explored for the incorporation and delivery of other proteins and peptides and should subsequently be subjected to pilot plant scale-up as well as clinical trial to establish their potential for subcutaneous immunization against hepatitis B. 88

89 Figure: 89
90 P03-07 PONCIRUS FRUCTUS INHIBITED THE PROLIFERATION AND INDUCEDTHE APOPTOSIS IN HEPATOCELLULAR CARCINOMA BY THE DOWN-REGULATION OF NF-ΚB Lokendra Chand, Yeon Jun Jeong 2, Suvesh Munakarmi Chonbuk National University, Biomedical research Institute, Jeonju,, 2 Chonbuk National University Hospital, Biomedical research Institute, Jeonju, Korea, Rep. of South Background and Aims: Many epidemiological studies has demonstrated that Hepatocellular Carcinoma (HCC) is one of the most common carcinoma and third leading cause of cancer related death globally. The emerging challenges of HCC are arising increasingly in pre-cirrhotic stages. There are number of drugs that are already discovered and are in developmental pipeline, none of them are as yet, approved by drug regulating agencies. Poncirus Fructus (PF), a phytochemical found in dry immature fruits of poncirus trifoliata, has been traditionally used for the treatment of various disease including gastrointestinal disorders in East Asia, can be potential candidate of the treatment of HCC. In this study we presented the evidence that PF inhibited the proliferation and migration of HCC by the down-regulation of NF-κB. The transcription factor NF-κB is responsible for the regulation of more than 200 genes and involved in many cellular processes such as inflammatory and immune responses, cellular growth, developmental process and apoptosis. The role of NF-κB has been implicated in number of diseases including cancer. In this study we aims to find out the role of PF in the treatment of HCC with Hep3B cell line via expression of NF-κB. Method: Hep3B and ALM-2 cells were cultured in DMEM medium with FBS and antibiotics. Cell viability and migration assays were performed by MTT and wound healing assay. Expression of NF-κB and apoptosis were evaluated by western blotting. Results: The number of viable cells was decreased significantly while treated with PF in a dose dependent manner but the normal mouse hepatocytes were remaining unaffected. Furthermore PF inhibited the proliferation of Hep3B cells by down-regulating the cell cycle, inflammation and expression of NF-κB. This result suggests that PF inhibits the proliferation and induce the apoptosis. Conclusion: PF can inhibit the proliferation and induce the apoptosis of Hep3B cells by the down regulation of NF-κB pathway. 90
91 P03-08 A LARGE SET OF MIRNAS IS DEREGULATED SINCE THE EARLIEST STEPS OF HUMAN HCC DEVELOPMENT Pia Sulas, Luca DI Tommaso 2, Chiara Novello 2, Francesca Rizzo 3, Antonio Rinaldi 3, Alessandro Weisz 3, Massimo Roncalli 2, Amedeo Columbano university of cagliari, Biomedical Sciences, Cagliari, Italy, 2 Humanitas University, Rozzano, Biomedical Sciences, Rozzano, Italy, 3 University of Salerno, Department of Medicine, Surgery and Dentistry, Salerno, Italy Background and Aims: Hepatocellular carcinoma (HCC) mostly results from a stepwise process characterized by the development of premalignant lesions, such as low- (LGDN) or high-grade (HGDN) dysplastic nodules in a cirrhotic setting. MicroRNAs (mirnas) are small noncoding RNAs involved in post-transcriptional regulation of gene expression that can act as oncogenes or tumor suppressors. Whether and which mirnas are involved in the early stages of HCC development remains elusive Method: Here, small RNA sequencing was applied to profile mirna expression in 55 samples (cirrhotic nodules, CNs), LGDNs, HGDNs, early HCCs (ehccs) and small progressed HCCs (phccs), obtained from 7 patients bearing HCCs of different etiology Results: A mirna expression signature of 62 mirnas distinguishing phccs from matched CNs was identified. Interestingly, 52 of these mirnas discriminated CNs from LGDNs/HGDNs, regardless of the etiology, and remained modified along the tumorigenic process. Functional analysis of the predicted mrna targets of deregulated mirnas identified common modifications between early and late stages of HCC development likely involved in the stepwise process of HCC development. Conclusion: Our results demonstrate that mirnas deregulation takes place very early in human liver carcinogenesis, implying their critical role in the tumorigenic process. The identification of mirnas discriminating cirrhotic from neoplastic nodules may have relevant translational implications for early diagnosis. 9
92 P03-09YI CYTOTOXIC T LYMPHOCYTES (TC) AND REGULATORY T CELLS (TREG) PREDICT THE DEVELOPMENT OF DERMATOLOGIC ADVERSE EFFECTS IN PATIENTS WITH HEPATOCELLULAR CARCINOMA TREATED WITH SORAFENIB Josep Corominas, Víctor Sapena, Álvaro Díaz-Gonzázlez, Marco Sanduzzi Zamparelli, Esther Samper, Cristina Millan, Jordi Bruix, María Reig, Loreto Boix Hospital Clinic de Barcelona. IDIBAPS. CIBERehd, BCLC Group. Hepatology Unit., Barcelona, Spain Background and Aims: Sorafenib is the standard treatment for patients with advanced hepatocellular carcinoma (HCC). However, more than 90% of patients develop adverse events (AE) during treatment, being the dermatologic adverse effects (DAE) the most common ones. Among these, 37% show up along the first 60 days (DAE60) and are associated with an increase in survival, but yet there are no markers that can predict which patients are at risk. Thus, our goal is to assess the association of the lymphoid populations profile in sorafenib-treated HCC patients at the start of their treatment with the appearance of AE at 60 days (AE60). Method: Thirty patients started treatment with sorafenib (800mg/day). The follow-up was carried out monthly and at all points of treatment modification. Lymphoid populations were identified by flow cytometry using signature markers: T lymphocyte (CD3+CD56-), TH (CD3+CD56-CD4+), TC (CD3+CD56-CD8+), TREG (CD3+CD56-CD4+CD25+), B lymphocyte (CD9+), Natural Killer (NK, CD56+CD3-) and NK T (CD56+CD3+); plus several non-characterized subpopulations. The ratio between TREG and TC (T-Ratio) was also calculated. Survival Cox models using baseline data were conducted to analyse Performance Status (PS) and DAE60. Further analyses were conducted using binary longitudinal marginal models to account for intrasubject correlations; sensitivity analyses were done using extended time-dependent Cox models. Results: 66.7% of patients were BCLC-C, 93.3% showed a PS of 0 and 93.3% had preserved hepatic function (Child-Pugh A). Twenty-one patients presented, at least, one dose modification due to AE60, 8 of which were DAE. Stratifying the patients by Child-Pugh and BCLC classifications, high numbers of TC or low numbers of TREG at basal samples were associated with the development of DAE60 (Hazard Ratio for tercil tendency tests: 2.66, p=0.09 and HR: 0.44, p=0.046, respectively). For all samples, independently of their time point, an increase of TREG was associated with lower risk of DAE60 (OR: 0.85, p=0.004) but with worsening of the PS (OR:.9, p=0.006). On the other hand, an increase of T cells at any point increased the risk of DAE60 (OR:.09, p=0.025). TREG, TC, CD9, CD56+CD3+CD4+ subpopulation and T-Ratio increase during follow-up were also associated with PS worsening; with highly significant association for the T-Ratio (OR: 2.57, p<0.000). Conclusion: A high count of TC lymphocytes or a low count of TREG at the beginning of sorafenib treatment predicts the risk of developing DAE along the first 60 days of treatment, and the ratio between these two populations is strongly associated with the worsening of the patients PS. Our results reinforce immune mediated inflammation as a key mechanism in the development of DAE. Moreover, we characterize a new cellular population (CD56+CD3+CD4+) which increase along the first 60 days of treatment is associated with a worsening of the PS. 92
93 P03-0 A HIGH ALPHA-FETOPROTEIN SLOPE PRIOR TO THERAPY CORRELATES WITH POOR SURVIVAL OF PATIENTS WITH HEPATOCELLULAR CARCINOMAS. Carolin Czauderna, Sandra Koch, Lukas Pilz, Sophia Franck, Wörns Marcus, Hauke Lang 2, Roman Klöckner 2, Peter Galle, Jens Marquardt, Arndt Weinmann University Mainz, I. Departement of Medicine, Mainz, Germany, 2 University Mainz Background and Aims: Hepatocellular Carcinoma (HCC) is a leading cause of death in cirrhotic patients and ranks among the most lethal cancers worldwide. Novel biomarkers for accurate prediction of prognosis and optimal treatment selection are urgently needed to improve patient management. Alpha-fetoprotein (AFP) is a well-established and widely used biomarker for HCC. However, diagnostic accuracy of static AFP-values is limited and clinical potential as a prognostic and/or predictive marker needs to be more precisely defined. Therefore, we evaluated the prognostic impact of pre-treatment serum AFP-changes on the overall survival (OS) of HCC-patients in a German cohort. Method: We retrospectively analyzed patients with confirmed HCC (n=859) treated at the University Medical Center of the Johannes Gutenberg-University Mainz between 998 and 204. Baseline parameters as well as pre-treatment static and dynamic AFP were investigated. AFP-slope was defined as the delta of two pre-treatment measurements normalized to daily increment/decline. Prognostic impact was assessed by Kaplan-Meier analyses and cox regression models. Optimal-cut-off values were defined using receiver operating characteristic curves. Results: Single AFP-values failed to show a prognostic impact in cox regression analyses. Conversely, pre-treatment AFP-slope was a faithfully and independent predictor for OS of HCC-patients (p<0.00) besides several known clinical parameters such as Child Pugh B (p=0.027) and C (p<0.00), portal vein thrombosis (PVT) (p<0.00), extrahepatic spread (p<0.00) and tumor size (p<0.00). The best discriminant cut-off value was a pre-treatment AFP-slope greater than 0,0752ng/ml/day with a sensitivity of 53,4% and specificity of 75,4%. Patients with an AFP-slope greater than 0,0752ng/ml/day prior to liver transplantation, HCC resection, local ablation and Sorafenib therapy had a markedly reduced overall survival than those with an AFP-slope under the threshold. Conclusion: AFP changes prior to therapy are predictive for the overall survival of HCC-patients. The addition of an AFP-slope to established prognostic parameters might improve prognostic classification of HCC. Figure: 93
94 P03- MACROTRABECULAR-MASSIVE HEPATOCELLULAR CARCINOMA: A DISTINCTIVE HISTOLOGICAL SUBTYPE WITH CLINICAL RELEVANCE Marianne Ziol, Nicolas Poté 2, Giuliana Amaddeo 3 4, Alexis Laurent 5, Jean Charles Nault 6 7, Frédéric Oberti 8, Charlotte Costentin 3, Sophie Michalak 9, Bouattour Mohamed 0, Claire Francoz 0, Georges-Philippe Pageaux, Jeanne Ramos 2, Decaens Thomas 3, Alain Luciani 4, Boris Guiu 5, Valerie Vilgrain 6, Christophe Aubé 7, Jonathan Derman 8, Cécile Charpy 8, Jessica Zucman- Rossi 9 20, Nathalie Barget 2, Olivier Seror 22, Nathalie Ganne-Carrié 6, Valérie Paradis 2, Julien Calderaro 4 8 Hôpital Jean Verdier, Pathology, 2 Hôpital Beaujon, Pathology, 3 Hôpital Henri Mondor, Hepatology, 4 Inserm U955, Team 8, 5 Henri Mondor University Hospital, 6 Hôpital Jean Verdier, Hepatology, 7 Inserm U62, 8 CHU Angers, Hepatology, 9 CHU Angers, Pathology, 0 Hôpital Beaujon, Hepatology, CHU Montpellier, Hepatology, 2 CHU Montpellier, Pathology, 3 CHU Grenoble, Hepatology, 4 Hôpital Henri Mondor, Medical Imaging, 5 CHU Montpellier, Medical Imaging, 6 Hôpital Beaujon, Medical Imaging, 7 CHU Angers, Medical Imaging, 8 Hôpital Henri Mondor, Pathology, 9 Inserm U62, Functionnal Genomics of Solid Tumors, 20 INSERM, Université Paris Diderot, 2 Hôpital Jean Verdier, 22 Hôpital Jean Verdier, Medical Imaging Background and Aims: We recently identified a novel histological subtype of hepatocellular carcinoma, designated as "macrotrabecular-massive" (MTM-HCC) and associated with specific molecular features. In order to assess the clinical relevance of this novel variant, we aimed to investigate its prognostic value in two large series of patients treated either by surgical resection or radiofrequency ablation (RFA). Method: We retrospectively included 389 HCC surgical samples and 284 HCC liver biopsies from patients treated by surgical resection and RFA, respectively. Histological slides were reviewed by pathologists specialized in liver disease, and the MTM-HCC subtype was defined by the presence of a predominant (>50%) macrotrabecular architecture (more than 6 cells thick). The main clinical and biological features were recorded at baseline. Clinical endpoints were early and overall recurrence. Results: The MTM-HCC subtype was identified in 4% of the whole cohort (9% of surgically resected samples, 8.5% of liver biopsy samples). Interobserver agreement for the diagnosis of MTM-HCC was good (k=0.72) and excellent (k=0.82) in the surgical and RFA series, respectively. This subtype was associated at baseline with known poor prognostic factors (tumor size, AFP level, satellite nodules and vascular invasion). Multivariate analysis showed that MTM-HCC subtype was an independent predictor of early and overall recurrence (surgical series: OR 2.90 ( ), p=0.0 and 2.83 ( ), p<0.00); RFA series: 2.37 ( ), p=0.002 and 2.9 ( ), p=0.00, respectively). Its prognostic value was retained even after patients stratification according to common clinical, biological and pathological features of aggressiveness. The relative risk of relapse associated with MTM-HCC was also higher than those associated with classical HCC outcome predictors, such as AFP serum levels, vascular invasion or satellite nodules. No other baseline parameter was independently associated to recurrence in the RFA series. Conclusion: The MTM-HCC histological subtype, reliably observed in 4% of patients eligible for a curative treatment, represents an aggressive form of HCC that may require more specific therapeutic strategies. 94
95 P03-2YI MACROPHAGE MIGRATION INHIBITORY FACTOR IS UPREGULATED IN MURINE HEPATOCELLULAR TUMOR TISSUE AND EXERTS PRO- PROLIFERATIVE AND ANTI-APOPTOTIC EFFECTS ON HEPATOMA CELLS IN VITRO Theresa Wirtz, Saal Alena, Bergmann Irina, Petra Fischer, Daniel Heinrichs, Janine Koehncke, Elisa Fabiana Brandt, Lacy Michael 2, Jürgen Bernhagen 2, Christian Trautwein, Marie-Luise Berres RWTH Aachen University Hospital, Medical Department III, 2 Ludwig-Maximilian University of Munich, Institute for Stroke and Dementia Research Background and Aims: Macrophage Migration Inhibitory Factor (MIF) is a proinflammatory chemokinelike function chemokine and has been characterized in different chronic diseases as well as solid tumors. Here, MIF exerts a carcinogenic role as it drives neo-angiogenesis and metastasis but inhibits apoptosis. Referring to the MIF receptors, CD74 was identified as an important target of MIF in malignant diseases, e.g. colon cancer. In this study we first analyze the role of MIF in murine hepatoma cells in vitro. Next we apply a toxic model of murine hepatocellular carcinoma (HCC) to study the role of MIF and CD74 in HCC in vivo. Method: In vitro Hepa -6 cells were stimulated with recombinant MIF in the presence or absence of CD74 neutralizing antibodies. Effects of MIF on proliferation and migration were assessed by BrdU incorporation or scratch assay respectively. To further study the role of MIF in apoptosis of Hepa -6 cells an Annexin assay as well as a TUNEL-staining was conducted where sorafenib was used as a cytotoxic agent. To examine the role of MIF/CD74 signaling in hepatocarcinogenesis in vivo, WT C57/B6J mice as well as CD74 deficient mice were subjected to the DEN/CCl4 model to induce multilocular HCC. Tumor number and size were determined after 24 weeks and qpcr of dissected liver tissue as well as immunohistochemical staining was performed to investigate MIF expression. Results: MIF promoted the proliferation of Hepa -6 cells in a dose-dependent manner. This effect could be reversed using a CD74 neutralizing antibody. Moreover, MIF exerted an anti-migratory effect on Hepa -6 cells in physiologic concentrations. During induction of cell death using sorafenib MIF showed an anti-apoptotic effect in Annexin- as well as TUNEL-staining. In WT mice, qpcr of dissected liver tissue showed a significantly increased expression of MIF in tumor as well as surrounding tissue compared to fibrotic liver tissue. The same was true for the MIF receptors CXCR2, CXCR4, CXCR7 and CD74. Moreover immunohistochemical staining of MIF proved an induction of MIF expression in tumor tissue. Most interesting, in CD74 deficient mice DEN/CCl4 treatment resulted in a decreased number and size of tumors compared to WT mice. Conclusion: In this study we present first data on MIF s impact on hepatoma cells where MIF exerts a pro-proliferative and anti-apoptotic function. Moreover we identify CD74 as a possible partner of MIF in murine HCC in vivo. As a conclusion, the MIF/CD74 axis could present a promising target in further HCC studies as well as therapeutic approaches. 95
96 P04-0 INCIDENCE AND PREDICTORS OF DE-NOVO HEPATOCELLULAR CARCINOMA IN HCV CIRRHOTIC PATIENTS TREATED WITH DIRECT-ACTING ANTIVIRALS: A SINGLE-CENTER PROSPECTIVE 3 YEAR STUDY Roberta D'ambrosio, Elisabetta Degasperi, Massimo Iavarone, Angelo Sangiovanni, Alessio Aghemo 2, Roberta Soffredini, Marta Borghi, Riccardo Perbellini, Giovanna Lunghi 3, Pietro Lampertico Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Università degli Studi di Milano, CRC A.M. and A. Migliavacca for Liver Disease, Division of Gastroenterology and Hepatology, Milano, Italy, 2 Humanitas University, Department of Biomedical Sciences, Rozzano, Italy, 3 Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Università degli Studi di Milano, Microbiology and Virology Unit, Milano, Italy Background and Aims: Incidence of hepatocellular carcinoma (HCC) in cirrhotic patients treated with direct-acting antivirals (DAAs) for hepatitis C (HCV) virus infection is still controversial. Aim of the study was to evaluate incidence and predictors of de novo HCC in HCV cirrhotics treated with DAAs Method: Consecutive HCV cirrhotics starting DAAs between November 204 and December 206 at a single Center were enrolled. Exclusion criteria were HIV infection, previous HCC history, active HCC or undefined liver nodules at baseline and Child-Pugh-Turcotte (CPT) score C. Cirrhosis was defined clinically, histologically or by liver stiffness measurement (LSM >.9 kpa). HCC was diagnosed and staged according to EASL recommendations. Baseline clinical features, biochemistry and non-invasive markers of liver fibrosis (LSM, APRI, Fib-4, LSPS) were assessed Results: 50 HCV cirrhotics were enrolled: age was 63 (28-87) years, 60% males, 47% HCV-b, 82% CPT A, 3% with baseline esophageal varices (EV). Median LSM was 7.3 ( ) kpa, APRI 2.0 ( ), Fib ( ), LSPS.7 ( ). A sustained virological response was achieved by 49 (96%). After 22 (-36) months, de novo HCC occurred in 24 (4.9%) patients, with a 3-year cumulative probability of 6% (95% CI 4%-9%). At diagnosis, median HCC size was 8 (0-00) mm, monofocal in 7%, BCLC 0-A in 83% ; CPT was A in 79% patients and median alpha-fetoprotein (AFP) was 6 (-57) ng/ml. At univariate analysis, de novo HCC was associated with male gender (p=0.03), diabetes (p=0.00), baseline LSM (<0.000) and LSPS (<0.000). At multivariate analysis, in patients without available LSM (n=489), male gender [HR 4.42 (95% CI ), p=0.02], diabetes [HR 3.59 (95% CI ), p=0.002] and baseline Fib-4 [HR.08 (95% CI.0-.5), p=0.08] were independently associated with HCC development. In those with available LSM (n=404), male gender [HR 0.0 (95% CI ), p=0.025], diabetes [HR 2.7 (95% CI ), p=0.037] and LSM [HR.03 (95% CI.0-.06), p=0.004] predicted the occurrence of HCC. The 3-year cumulative probability of HCC was 8.7% in males vs..6% in females (p=0.005), 8.0% in diabetics vs. 3.2% non-diabetics (p=0.0003), and 3.4% vs. 23% in patients with LSM < or 30 kpa (p<0.000). Conclusion: In a large, single-center prospective study of DAA-treated HCV cirrhotics, male gender, diabetes and noninvasive markers of fibrosis independently predicted the development of HCC. 96
97 P04-02YI METRONOMIC CAPECITABINE VS. BEST SUPPORTIVE CARE IN CHILD-PUGH B HEPATOCELLULAR CARCINOMA: A PROOF OF CONCEPT Stefania De Lorenzo, Francesco Tovoli 2, Maria Aurelia Barbera, Andrea Palloni, Giorgio Frega, Ingrid Garajova, Francesca Garuti 2, Franco Trevisani 2, Giovanni Brandi Sant Orsola-Malpighi Hospital, University of Bologna, Department of Experimental, Diagnostic and Specialty Medicine, Bologna, Italy, 2 Sant Orsola-Malpighi Hospital, University of Bologna, Department of Medical and Surgical Sciences, Bologna, Italy Background and Aims: Child-Pugh B hepatocellular carcinoma (HCC) needing systemic treatment has a poor prognosis. Due to the confounding factor of possibly non-cancer related death, these patients are usually excluded from clinical trials. As such, they are an orphan category with no available systemic treatment. Preliminary studies suggest that capecitabine may be safe and effective in HCC patients. We retrospectively evaluated the safety and efficacy of metronomic capecitabine (MC) in patients with moderate liver dysfunction. Method: This multicentre study retrospectively analyzed data of Child-Pugh B-HCC patients naïve to systemic therapies, treated with MC or best supportive care (BSC). Exclusion criteria for both groups: a) performance status (PST)>2; b) severe ascites; c) moderate-to-severe encephalopathy; d) bilirubin 3 mg/dl; c) creatinine.5 mg/dl; d) platelets<30000/mmc; e) neutrophils <000/mmc. The patients were matched for the following factors: a) BCLC stage; b) extrahepatic spread; c) macrovascular invasion; d) PST [0 vs -2]; e) AFP 400ng/ml; f) Child-Pugh score [B7 vs. B8-9]. Results: According to the aforementioned criteria, we identified 35 patients treated with MC and 70 controls (matched in a :2 fashion). Median overall survival was 7.8 months in patients receiving MC and 5. months in patients receiving BSC (p=0.002). The result of univariate unweighted Cox regression model showed a 49% reduction in death risk for patients on MC (95%CI: ; p =0.003). After weighting for potential confounders, death risk remained essentially unaltered (52%; 95%CI: ; p = 0.00). In the MC group, ten (28.6%) patients experienced at least one adverse event, the most common of which were: hand-foot syndrome (8.5%), fatigue (8.5%), anaemia (5.7%), neutropenia (5.7%), bilirubin elevation (2.9%), thrombocytopenia (2.9%), nausea/vomiting (2.9%), mucositis (2.9%). Conclusion: MC seems a safe option in selected Child-Pugh B-HCC patients, showing a potential antitumor activity which needs prospective evaluation. 97

98 Figure: 98
99 P04-03YI EFFICACY OF RADIOFREQUENCY IN PATIENTS WITH HEPATOCELLULAR CARCINOMA: META-ANALYSIS Andrea Casadei Gardini IRST-IRCCS Background and Aims: The purpose of this meta-analysis is to evaluate predictive prognostic factors of survival and recurrence free survival in patients treated with radiofrequency, with the aim of identifying parameters that can help clinicians in the therapeutic choice and to identify stratification factors for future studies in this subset of patients. Method: Clinical trials that values prognostic factors of radiofrequency ablation were considered. We excluded randomized controlled trials between radiofrequency and surgery. We excluded radiofrequency with microwave and with ethanol. Results: 35 studies published from 2003 to 207 were analyzed. They included.26 HCC patients treated with radiofrequency. For overall survival the analysis of the liver functionality show that child pugh B versus Child pugh A (HR = 2.32, 95% CI = ; P < 0.000) (Fig A), increase of bilirubin (HR =.03, 95% CI =.0.04; P < 0.000) (Fig B), precense of Portosystemic collaterals (HR =.54, 95% CI =.3.82; P < 0.000)(Fig C) and ALBI score vs 0 (HR=2.69, 95% CI = ; p < 0.000) (Fig D) was predicted of poor OS. Decrease of Prothrombin activity (HR = 0.97, 95% CI = ; P < 0.000) (Fig E) and increase of albumin (HR = 0.90, 95% CI = ; P < 0.000) (Fig F) was predicted of good OS. The analysis of tumor size show that if we consider the size of the nodule as a continuous variable, it is not predictive of OS (HR =.0, 95% CI = ; P 0.269) (Fig 2A), but if considered the cut off the data show that > 2cm versus < 2 (HR =.4, 95% CI =.23.6; P < 0.000)(Fig 2B) and >3cm versus <3 cm (HR =.43, 95% CI =.7.74; P < 0.000) (Fig 2C) was predictive of poor OS. If considered the number of nodules the data show that the precense of > nodules (HR =.59, 95% CI =.46.74; P < 0.000) (Fig 2D) was predictive of poor OS. For alfafetoprotein the data show that the cutoff of 20 ng/ml ( > 20 ng/ml vs < 20 ng/ml HR =.46, 95% CI =.25.70; P < 0.000) (Fig 3 A) was predictive of poor prognosis, conversely cutoff of 200 ( > 200 ng/ml vs < 200 ng/ml HR =.2, 95% CI = ; P 0.448) (Fig 3B) and 400 ( > 400 ng/ml vs < 400 ng/ml HR =.30, 95% CI = ; P 0.448) (Fig 3C) was not predictive of poor prognosis. Conclusion: In conclusion, our meta-analysis shows that the maximum benefit of RFA is in children pugh A, ALBI score, tumor size <2 cm with single nodule and with alpha-fetoprotein less than 20 ng / ml, 99
100 P04-04 PHENOTYPICAL AND MOLECULAR CHANGES IN NODULE IN NODULE HEPATOCELLULAR CARCINOMA WITH PATHOGENETIC IMPLICATIONS Arianna Cappuccetti, Noemi Rudini, Chiara Novello, Annarita Destro, Elena Riboldi 2, Matteo Donadon 3, Luca Viganò 3, Emanuela Morenghi 4, Massimo Roncalli 3, Luca DI Tommaso 3 Humanitas Clinical and Research Hospital, Pathology, 2 Novara University, 3 Humanitas University, Biomedical Sciences, 4 Humanitas Clinical and Research Hospital, Biostatistical Unit Background & Aims: Nodule in nodule hepatocellular carcinoma (N/N HCC) is a convincing proof of multistep hepatocarcinogenesis. In this lesion an inner expansile HCC develops within an outer more differentiated tumor, which can be rapidly taken over by the former so that N/N HCC is rarely detected and studied. Methods: We have collected 0 resected N/N HCC in cirrhosis characterized, as outer lesions, by early (n.3) and G (n.7) HCC and, as inner lesions, by G (n.3) and G2 (n.7) HCC. The largest/smallest diameters of outer and inner nodules were, respectively, 20/6 and 6/4 mm. We investigated vascular (CD34, endocan), hepatocellular (VEGF, GS, GPC3, HSP70, CHC) and molecular (TERT promoter, β- catenin) changes taking place from outer to inner neoplastic compartments (ONC to INC). Results: A diffuse pattern of CD34+ capillarized vessels and focal endocan immunoreactivity were major distinctive features acquired in INC; by contrast VEGF immunoreactivity resulted inversely related to CD34 staining. A variable gain in the number of GPC3, HSP70 and CHC but not GS immunoreactive cells also occurred in INC. TERT promoter mutations were seen in half of the cases in both compartments, while β-catenin mutations were more rarely detectable. Conclusions: These results document major vascular changes and, to a lesser extent, in the phenotype of malignant cells in N/N HCC. Molecular markers such as TERT promoter mutations take place frequently and very early and, at variance with β-catenin mutations, do not appear acquired in the N/N growth. Overall either N/N compartments are phenotypically and molecularly more heterogeneous than predicted by morphology and size. The study of tumor neovascularization can be informative on the biology and clinical progression of early stage HCC. 00
101 P04-05YI SYSTEMATIC REVIEW AND METANALYSIS ESTABLISH DERMATOLOGY ADVERSE EVENTS AS A POSITIVE PREDICTOR OF SURVIVAL IN HEPATOCELLULAR CARCINOMA PATIENTS TREATED WITH SORAFENIB Alvaro Diaz-Gonzalez, Marco Sanduzzi-Zamparelli, Víctor Sapena, Ferran Torres 2, Neus Llarch, Gemma Iserte, Alejandro Forner, Leonardo Gomes Da Fonseca, José Ríos 3, Jordi Bruix, Maria Reig BCLC group. Liver Unit. Hospital Clínic de Barcelona. IDIBAPS. CIBERehd, Hospital Clínic i Provincial de Barcelona, Barcelona, Spain, 2 Medical Statistics core facility, IDIBAPS, Hospital Clinic Barcelona, Biostatistics Unit, Faculty of Medicine, Universitat Autònoma de Barcelona, Barcelona, Spain, Spain, 3 Medical Statistics Core Facility, Institut d Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS) and Hospital Clinic, Barcelona, Spain., Biostatistics Unit, Faculty of Medicine, Universitat Autònoma de Barcelona, Spain Background and Aims: Sorafenib is the established st -line systemic therapy for hepatocellular carcinoma (HCC) but, in an era of new options for st and 2 nd line, it is key to fully understand the treatment related events that may drive a better outcome and thus, should prime a careful decision to interrupt therapy and move to other options because of perceived impairment of quality of life and/or irrelevant disease progression. In this regard, dermatologic adverse events (DAEs) have been suggested to be a marker of better outcome in sorafenib treated patients. The aim of this systematic review and metanalysis is to explore the impact of DAEs in HCC patients treated with sorafenib in order to unequivocally define if DAEs, as an early evolutionary event, are associated to an improved outcome. Method: The study was done according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. Two authors retrieved all data and a 3 rd one solved discrepancies. DAEs were defined as the presence of any kind of skin symptoms that are congruent with sorafenib side effects and maintain a reasonable temporary relationship. Results: 33 studies were identified until July/ studies were full-text manuscripts and met the inclusion criteria. They included 926 patients (82.5% Child-Pugh A, 84% BCLC-C, and 30% ECOG-0), 2 were prospective, 7 retrospective and not disclosed. Only 2 studies were focused on early DAEs. 45% of the patients developed hand foot skin reaction and 24% other dermatologic adverse events. The presence of DAE was associated with a higher probability of overall survival when compared with those patients without DAEs. The pooled Hazard Ratio was 0.49 (CI-95%; ) and there was no heterogeneity for the analysis (p=0.307; I 2 =4.8%). Conclusion: This metanalysis demonstrates the positive association between the development of DAEs and better prognosis in patients with HCC treated with sorafenib. This association indicates the need to investigate the mechanism underlying the pathophysiology of DAEs and how this may help to define the mechanism for a less malignant tumor progression. At the same time, development of DAEs should not be seen as a disadvantage as compared with drugs with lower rate of DAEs, but rather become part of the decision process to sense the risk/benefit balance of HCC therapy across different options. 0
102 F o ld - c h a n g e in c e l l v ia b i l it y ( h y p o x ia /n o r m o x ia ) P04-06YI DOXORUBICIN AND HYPOXIA TREATMENT OF HCC CELL LINES: CELL VIABILITY AND ONCOLOGIC PROTEIN PROFILE Ilse Dubbelboer, Femke Heindryckx 2, Hans Lennernäs Uppsala universitet, Department of Pharmacy, Uppsala, Sweden, 2 Uppsala universitet, Department of Medical Cell Biology, Uppsala, Sweden Background and Aims: Doxorubicin (DOX) is one of the most widely used cytostatic agent in the locoregional treatment of hepatocellular carcinoma (HCC). The infusion of DOX together with different drug delivery systems is often combined with an embolization of the tumor feeding vessel. The tumor is thus exposed to high DOX concentrations and hypoxia. It is difficult to separate the possible synergistic effect of the drug exposure and the embolization in vivo. The aim of this study was to evaluate the effect of DOX exposure and hypoxia in different HCC cell lines over time. Method: Three HCC cell lines (HepG2, Huh7, SNU449) were seeded in a 96-wells plate at a concentration of cells/well. Cell lines were exposed to DOX (0-000 µm) during 6, 24, 48, and 72 h. Conditions were repeated in chemically induced hypoxia. Hypoxia was induced with 00 µm Cobalt (iii) chloride hexahydrate. Cell viability was evaluated with resazurin and drug-response as concentration which gives 50% cell viability reduction (IC50). For the biomarker assay, 8 conditions were tested per cell line: exposure to 0 or 0. µm DOX during 6 or 72 h, under norm- or hypoxia. These corresponded to the conditions of the cell viability studies. Oncologic biomarkers were determined in cell lysates with the Olink Oncology II panel. This is a highthroughput, multiplex immunoassay, analyzing normalized protein expression of 92 proteins. Results: The three cell lines showed a relevant difference in response to DOX, as shown in table. While cytotoxicity of DOX was reciprocal with time in HepG2 and Huh7 cell lines, the drug-response of SNU449 cells showed more variations over-time. From 6 to 72 h, IC50 decreased from 260 to 0.2 µm in HepG2 cells and from 70 to 0.3 µm in Huh7 cells. Hypoxia affected cell viability, as shown in the Figure. As expected, hypoxia also affected the cell s response to DOX. Drug-response to DOX increased in HepG2 and decreased in Huh7; HepG2 IC50 decreased 6-fold and Huh7 IC50 increased from 4.5-fold at 48h. Number of proteins detected in over 75% of the samples was 4 of 92 (45%). Large differences were seen between cell lines. For example, vascular endothelial growth factor A and toll-like receptor 3 had lower, while protein S00-A4 had higher normalized expression in HepG2 compared to Huh7 and SNU449 cells. Interestingly, fewer oncogenic proteins could be detected in HepG2 compared to Huh7 and SNU449 cells. Conclusion: Three commonly used HCC-cell lines (HepG2, Huh7 and SNU-449) have critically different responses to chemotherapy and hypoxia. This was also reflected in their different protein expression profile. These different responses to hypoxia and chemotherapy emphasize the need for validating in vitro findings in multiple cell lines. It further suggests that tumors can respond differently to the combination of local chemotherapy and embolization, which is important for future treatment optimization. Figure: R e s p o n s e to h y p o x ia H e p G 2 H u h 7 S N U h 2 4 h 4 8 h 7 2 h 02
103 P04-07 PRESENCE OF HCC AND BCLC STAGE SIGNIFICANTLY INFLUENCE SOLUBLE FIBRINOGEN-LIKE PROTEIN 2 (SFGL-2) IN CIRRHOTIC PATIENTS Ioannis Elefsiniotis, Georgia Barla, Athanasia Tasovasili, Christos Mavrogiannis ACADEMIC DEPARTMENT OF HEPATOGASTROENTEROLOGY, GENERAL AND ONCOLOGY HOSPITAL OF KIFISIA, ATHENS, GREECE, Greece Background and Aims: Soluble fibrinogen-like protein 2 (sfgl2) is the soluble form of fibrinogen-like protein 2, that is mainly secreted by regulatory T cell (Treg) populations, and exerts potently immunosuppressive microenvironment so sfgl2 might play a role in inhibiting anti-tumor immune responses. The aim of our study was to evaluate plasma sfgl2 levels in cirrhotic patients with compensated or decompensated liver disease with or without HCC Method: 07 consecutive cirrhotic patients (39 decompensated, 66 CPT-A, median CPT=6, median MELD=9) were evaluated for sfgl2 levels during routine upper GI endoscopy. 28 of them had documented concurrent HCC (6 BCLC-A, 4 BCLC-B, 2 BCLC-C and 6 BCLC-D) with (n=4) or without (n=4) portal vein thrombosis (PVT). Results: Mean sfgl2 levels were 4.04±3.80 pg/ml and were significantly higher in patients with decompensated liver disease (6.07±4.80 pg/ml vs 2.82±2.27 pg/ml, p<0.000) and in those with HCC (6.4±4.20 pg/ml vs 3.24±3.29 pg/ml, p=0.00). Patients with BCLC C/D HCC stages had remarkable higher levels compared to those of BCLC A/B stages (8.7±4.3 pg/ml vs 3.53±2.20 pg/ml, p=0.008). Patients with decompensated cirrhosis and HCC exhibit significantly higher levels compared to those with decompensated liver disease without HCC (7.48±4.24 pg/ml vs 4.87±5.20 pg/ml, p=0.024). Conclusion: sfgl2 levels is significantly higher in cirrhotic patients with decompensated liver disease compared to those with compensated cirrhosis. Presence of HCC and stage of the disease according to BCLC system seem to significantly influence sfgl2 levels in cirrhotic patients. Figure: FGL-2 mean (pg/ml) COMP DECOMP DECOMP-HCC ADVANCE HCC C- D DECOMP-NO HCC FGL-2 mean 03
104 P04-08YI RETROSPECTIVE OBSERVATIONAL STUDY OF CHARACTERISTICS OF HCC PATIENTS FROM EGYPT AND IMPACT OF SURVEILLANCE ON IMPROVING THEIR OUTCOMES Medhat Elhosary, Hisham Saad Mohamed Elsayed Abdelaal 2 Kafr El Sheikh Liver Research Center, Hepatology, Kafr elsheikh,, 2 Kafr El Sheikh Liver Research Center, Hepatology, Kafr elsheikh, Egypt Background and Aims: HCC is the sixth most common cancer worldwide and the third most common cause of cancer death. In Egypt, liver cancer forms.68% of the total malignancies. HCC constitutes 70.48% of all liver tumors among Egyptians. HCC represents the main complication of cirrhosis. A major impact on its incidence should be achieved through current vaccinations for HBV infection, screening and treatment for HCV, and from the reduction of alcoholic liver disease. We studied the characteristics of HCC patients from Delta region in Egypt and the impact of a surveilla nce program on improving their outcomes. Method:W e studied 425 HCC patients out of 730 chronic liver disease patients visited our clinic in K afr Elsheikh from 2005 to 200. Analysis of their characteristics has been done to show the pattern of HCC in this area. This included gender, age, residence, AFP, and gross morphology of lesions. Based on the outcome of each HCC patient and his adherence to surveillance visits, we could study the impact of implementing a surveillance program on improving the outcome of HCC. Results:HCC was more common in men (77.4%) than women (22.6%). Age of HCC patients ranged f rom 29 to 7 years. 76.7% of HCC patients were living in rural areas while 2.3% in urban. The lowest value of AFP was.75 ng/ml, highest was 58, When we used 400 as a cut-off point to diagnose HCC, it showed no difference as only 5.3% were > 400 ng/ml. Studying the morphology of lesions showed that 80.9% (344/425) were single, among those 54.7% (88/344) were multifocal. Patients who were regular in their visits showed a higher chance for radiofrequency ablation (RFA) an d therefore their outcomes were much better. Conclusion:HCC could occur in a young age down to twenties. AFP could be used for screening of H CC but negative results do not exclude HCC. Surveillance programs have a positive impact on improving the outcome of HCC patients. 04

105 P04-09YI MODIFICATION OF THE ALBI-T SCORE: NEW PROGNOSTIC MODEL FOR PATIENTS WITH HEPATOCELLULAR CARCINOMA Omar Elshaarawy, Asmaa Ibrahim, Naglaa Allam, Zahraa Alkhatieb, Mostafa Elhelbawy, Eman Rewisha, Imam Waked National Liver Institute, Hepatology department, Shebiene Elkom, Egypt Background and Aims: ALBI score eliminates the need for the subjective variables required in the C- P grade and to offer more precise selection of patients. The tumor stage is a very important factor in that affect survival of patients HCC this was represented in the TNM stage which was put in a formula that resulted in ALBI-T score. In this study we propose a modification to the ALBI-T by adding Ogasawara sub classification of ALBI score in order to get better prognostic model. Method: We accrued data from the HCC clinic at National Liver Institute, Menoufia University. We had access to a data set of a cohort of 90 patients diagnosed with HCC and fulfilled the inclusion criteria. CTP, BCLC, ALBI, ALBI-T and modified ALBI-T scores were estimated. Patients were followed up from the time of diagnosis to the date of death or date of data collection if they remained alive. Overall survival and the received treatment were determined. Survival data were analyzed using Kaplan Meir Survival curves using log rank test and multivariate analysis. Results: For 90 patients, the mean age was 57 years, 575 were males. At presentation, 50.6% were CTP A, 36.% were CTP B and 3.4 % were CTP C. Most of patients were ALBI grade 2 (63.2%), 7.8 % were ALBI grade 2A while 45.5% were ALBI grade 2B. ALBI grade & 3 were 2% & 24.7% respectively. The overall median survival was 3 months; the median survival was better in patients with ALBI grade than ALBI 2 & 3 (28.6, 4 and 5.8 months respectively, P< 0.00). Moreover, the median survival for ALBI grade 2A patients was better than ALBI 2B (8.6 vs. 3 months respectively, P< 0.00). ALBI-T grades 0 & patients had better median survival than those of ALBI-T grades 2, 3, 4 & 5(42, 24.4, 7, 8.9, 5 and 3 months respectively (P < 0.00)). On adding the ALBI sub classification proposed by Ogasawara, the modified ALBI-T showed significant improvement in the median survival. Modified ALBI-T grades 2, 3, 4, 5 and 6 to be 28.6, 20.9, 3.9,8 and 4 months respectively. Conclusion: ALBI-T score is a superior total prognostic tool that selects patients with HCC and better liver reservoir than ALBI and CTP scores. This ability increases by adding Ogasawara sub classification of ALBI score to ALBI-T score. Modified ALBI-T is the ideal overall prognostic model in patients with HCC. Figure: Showing survival curves for ALBI grade II patients according to original and modified scores 05
106 P04-0YI DYNAMIC SURVIVAL ANALYSIS OF THE DATA FROM THE NATIONAL SURVEY OF HCC AND LIVER TRANSPLANT IN BRAZIL Guilherme Felga 2, Aline Chagas 2, Marcio Dias Almeida, Venâncio Avancini Ferreira Alves 3, Flair José Carrilho 2, And The Brazilian Hcc Study Group 4 Hospital Municipal da Vila Santa Catarina, Serviço de Transplante de Fígado, São Paulo, Brazil, 2 Faculdade de Medicina da Universidade de São Paulo, Gastroenterologia, São Paulo, Brazil, 3 Faculdade de Medicina da Universidade de São Paulo, Patologia, São Paulo, Brazil, 4 The Brazilian HCC Study Group, Brazil Background and Aims: Traditional survival analysis provides inadequate estimates of the future prognosis for patients with accrued survival. Conditional survival (CS) adjusts future survival by the already accrued survival. It provides insights into the temporal distribution of the effect of predictors. We aimed to estimate and to analyse overall (OS) and disease free survival (DFS) and its independent predictors; to estimate and to analyse 5 years overall (OCS) and disease free conditional survival (DFCS) until the 5th year and the behaviour of the previously identified predictors. Method: Retrospective cohort from 3 Brazilian transplantation centers. Clinical, radiological, and anatomopathological data were considered. The Kaplan-Meier method with the long-rank test and the Cox proportional hazards model were adopted. CS was calculated through life tables. The standardized difference reassessed differences between variables. Results: 57 patients were included. OS in, 3, 5, 7 and 0 years was 78,6%, 72,3%, 66,0%, 6,3%, and 59,4%, respectively. OS was predicted by age [HR,04 (95% CI,02-,06), p 0.000], female sex [HR,35 (95% CI,02-,79), p 0.038], post-operative HCC recurrence [HR,35 (95% CI,08-,79), p 0.003], diameter of the largest viable nodule on the explant [HR,0 (95% CI,0-,02), p 0.006], nondiscriminated vascular invasion [HR 3,8 (95% CI,48-6,85), p 0.004], micro [HR,65 (95% CI,27-2,5), p 0.00] and macrovascular invasion [HR 2,25 (95% CI,30-3,89), p 0.000]. 5-year OCS at the end of the st, 3rd and 5th year was 79,5%, 82,2%, and 90,0%, respectively. Predictors of OS presented with an erratic behaviour over time. DFS in, 3, 5, 7 and 0 years was 94,2%, 90,%, 89,8%, 87,5%, and 87,5%, respectively. DFS was predicted by serum AFP upon diagnosis [HR,0 (95% CI,0-,02), p 0.000], HCC within the Milan criteria upon diagnosis [HR 0,42 (95% CI 0,22-0,80), p 0.008], explant within the Milan criteria [HR 0,34 (95% CI 0,7-0,68), p 0.002], undifferentiated tumor or hepatocholangiocarcinoma on the explant [HR 3,04 (95% CI,75-5,30), p 0.000], non-discriminated vascular invasion [HR 5,72 (95% CI 3,44-7,83), p 0.000], micro [HR 3,40 (95% CI,83-6,28), p 0.000], and macrovascular invasion [HR,96 (95% CI 5,20-27,47), p 0.000]. 5-year DFCS at the end of the st, 3rd and 5th year was 94,%, 97,%, and 97,4%, respectively. Predictors of recurrence usually presented with greater impact during the st or 2 nd post-operative year. Conclusion: Outcomes of liver transplantation in Brazil were comparable to those from the US and Europe. Survival estimates were pessimistic due to greater early losses. Conditional survival offers a different perspective for the same data. The behaviour of predictive values varies over time. 06
107 P04-YI ASSESSMENT OF HYPOTHYROIDISM AS A MARKER OF RESPONSE TO SORAFENIB IN PATIENTS WITH HEPATOCELLULAR CARCINOMA. SYMPTOMS MAKE THE DIFFERENCE. Pablo Florez Díez, Noelia Rodríguez Ferreiro, Victor J Beltrán, Andrés Castano-Garcia, Maria Luisa Gonzalez Dieguez, Carmen Álvarez-Navascués, Valle Cadahía-Rodrigo, Manuel Rodríguez, Maria Varela Hospital Universitario Central de Asturias, Spain Background and Aims: Vascular invasion, alpha-fetoprotein (AFP) and high neutrophil to lymphocyte ratio (NLR) have been described as predictors of poor prognosis in advanced hepatocellular carcinoma (HCC) (Bruix et al, J Hepatol 207). In addition, absence of extrahepatic spread, HCV etiology and low NLR predict good response to sorafenib (SOR). On the other hand, appearance of hypothyroidism (hypot) is associated with greater treatment efficacy and lower tumor growth in clinical studies with other multikinase inhibitors. AIM: Analysis of hypot as an adverse event of SOR. Assessment of prognostic & predictive factors described above in the HCC cohort treated at our site. Method: Prospective unicentric cohort of patients consecutively treated with sorafenib. Only those with compensated cirrhosis Child < =B 7 and ECOG PS <= were included. Patients were evaluated at baseline, 2, 4, 8 and 2 weeks from the start of SOR, every 8 weeks thereafter, including TSH measure. We analyzed vascular invasion, AFP (>= 200 ng/ml), NLR (>=2.74, median value), HCV etiology, extrahepatic spread, symptoms (ECOG PS 0 vs ) and the appearance of significant hypot, defined as TSH>0 miu/l throughout treatment as possible prognostic variables. Results: A total of 42 patients were included with follow-up until Oct 25 th 7. The majority were compensated cirrhotic Child A-5 (n = 94), ECOG PS-0 (n = 0), BCLC-C (n = 02). Those with prior cervical radiotherapy (n=3), TSH out of range ( miu/l) (n=4), amiodarone (n=6) or levothyroxine (n = 4) were excluded, leaving a population of 28 patients. The appearance of hypot during follow-up was low, n=2 (9.4%). Only 0 started levothyroxine. Median duration of SOR was 8 months (IQR ). Median survival censored at the start of the 2nd line was 5 months (IQR ). At univariate analysis, vascular invasion (p = 0.033), high AFP (p = 0.030), high NLR (p = 0.0) and ECOG PS (p <0.00) were significant. At multivariate analysis, the only independent predictor of survival was the presence of symptoms (ECOG PS 0 vs ) (p = 0.009, HR 0.537, 95% CI ). Conclusion: Appearance of hypothyroidism was an uncommon adverse event in HCC treated with sorafenib and it didn t impact in survival of patients. In our cohort, the other factors evaluated were not associated with survival except for the presence of symptoms at the beginning of treatment. 07
108 P04-2YI EFFICACY AND SAFETY OF REGORAFENIB IN CLINICAL PRACTICE IN THE TREATMENT OF HEPATOCELLULAR CARCINOMA. MULTICENTRE EXPERIENCE. Miguel Fraile, Maria Teresa Ferrer 2, Ana M Matilla 3, José Luis Lledó 4, Beatriz Minguez 5, Alicia Hernandez 6, Christie Perelló 7, Javier Fernández-Castroagudín 8, Carlos Rodríguez de Lope 9, María Dolores Espinosa Aguilar 0, Silvia Montoliu, Margarita Sala 2, Marta Romero-Gutiérrez 3, Sonia Pascual 4, Juan José Urquijo 5, Dalia Elena Morales Arraez 6, Maria Jose Blanco Rodriguez 7, Maria Varela 8 Hospital Universitario Central de Asturias, 2 Hospital Universitario Virgen del Rocío. Sevilla, 3 Hospital General Universitario Gregorio Marañón. Madrid, 4 Hospital Universitario Ramón y Cajal. Madrid, 5 Hospital Vall de Hebron. Barcelona, 6 Hospital General Universitario de Ciudad Real, 7 Hospital Universitario Puerta de Hierro. Majadahonda, 8 Complexo Hospitalario Universitario de Santiago, 9 Hospital Universitario Marqués de Valdecilla. Santander, 0 Hospital Virgen de las Nieves. GRANADA, Hospital Universitari de Tarragona Joan XXIII. Tarragona, 2 Hospital Universitari Germans Trias i Pujol. Badalona, 3 Complejo Hospitalario Universitario de Toledo., Toledo,, 4 Hospital General Universitario de Alicante., 5 Hospital General Universitario de Valencia., 6 Hospital Universitario de Canarias, 7 Hospital de Jerez, Jerez de la Frontera. Cádiz,, 8 Hospital Universitario Central de Asturias. Oviedo Background and Aims: Regorafenib (REGO) improves survival of hepatocellular carcinoma (HCC) in 2nd line after sorafenib (SOR). Patients with dermatological adverse effects> grades 2 in the first 60 days with SOR (DAE60) have greater survival (Reig et al., J Hepatol 204). Finally, appearance of handfoot syndrome (HFS) with REGO has a positive impact on survival (Merle et al., ILCA Congress 207). AIMS: ) to describe applicability, adverse effects (AE) and radiological response at 3 months of REGO in real life; 2) to assess if DAE60 with SOR is predictor of HFS with REGO. Method: 65 patients (7 centres) were prospectively recruited: 58 with REGO indicated after SOR (group A); 3 after SOR and nivolumab (3rd line) (group B); 4 in post-transplant setting (group C). Results: GROUP A: applicability 83%: 7 hasn t received REGO for symptomatic progression, 3 for lack of authorization. In the remaining 48: median age 64 yr, 79%men, etiology(%): 27 alcohol, 46 HCV, 0 HBV, 8 NAFLD. At diagnosis all were asymptomatic, Child A 89%, BCLC 0/A 39.6%, BCLC-B 39.6%, BCLC-C 20.8%. Tolerance to SOR estimated by final dose: full dose 70.8%, 600mg 4.2%, 400mg 25%. Median duration of REGO 3 months (P25P75-6). 45.8% had DAE60, associated with non-significant greater survival from the start of SOR: mean 42.9 (95% CI ) vs 28 months (95% CI ), p = The sensitivity, specificity, positive predictive value and negative predictive value of DAE60 to predict HFS with REGO were 89%, 80%, 73% and 92% respectively. Initial radiological evaluation was available in 28 cases: 35.7% (n=0) presented absence of progression. Median survival from the start of SOR (SOR+REGO) was 5 months (P25-P ) and from diagnosis of HCC 28.4 months (P25-P ). Absence of symptoms at the beginning of SOR was the only predictor of higher survival: ECOG PS 0(n=54) median 2 months, mean 4.9 (IC95% ) vs ECOG PS (n=4), mean 6.7 months (IC95% ), p= GROUP B: applicability 33%, scarce number of patients and short follow-up to draw conclusions. GROUP C: the most frequent AEs were asthenia, anorexia and diarrhoea. No HFS in the post-transplant setting. Conclusion: In real life, REGO delays initial radiological progression of HCC in more than a third of patients. Absence of DAE60 with SOR predicts absence of HFS with REGO in 92% of cases, which can be useful when we have alternative 2nd line treatments. 08
109 P05-0 TLL POLYMORPHISM DO NOT PREDICT THE DEVELOPMENT OF DE- NOVO HEPATOCELLULAR CARCINOMA IN HCV CIRRHOTICS TREATED WITH IFN-FREE DAA-BASED REGIMENS Enrico Galmozzi, Floriana Facchetti, Roberta D'ambrosio, Elisabetta Degasperi, Alessio Aghemo 2, Roberta Soffredini, Marta Borghi, Riccardo Perbellini, Massimo Iavarone, Angelo Sangiovanni, Pietro Lampertico Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Università degli Studi di Milano, CRC A.M. and A. Migliavacca for Liver Disease, Division of Gastroenterology and Hepatology, Milano, Italy, 2 Humanitas University, Department of Biomedical Sciences, Rozzano, Italy Background and Aims: A genome wide association study (GWAS) has recently demonstrated an association between the Tolloid Like (TLL) rs polymorphism and the development of hepatocellular carcinoma (HCC) among hepatitis C virus (HCV) patients with a sustained virological response (SVR) to Interferon, but whether this holds true for direct-acting antivirals (DAAs)-treated patients remains unknown. Aim of our study was to assess the association of TLL rs with HCC development in a cohort of HCC-free HCV cirrhotics who were treated with DAA-based regimens. Method: 453 consecutive HCC-free HCV cirrhotics [aged 63 (28-87), 58% males, 60% HCV-b, 87% CPT-A, liver stiffness measurement (LSM) 7.4 (2.-75) kpa, alpha fetoprotein (αfp) 9.4 ( ) ng/ml, 9% with diabetes] treated with DAA between January 205 and December 206 were enrolled in a single Center real-life study. Cirrhosis was defined clinically, histologically (METAVIR F4) or by LSM (>.9 kpa). HCC was diagnosed according to International recommendations. TLL rs A/T polymorphism was analyzed using Taq-Man SNP genotyping assay Results: Genotype distribution of TLL variant was AA in 330 (73%), AT in 6 (25.5%) and TT in 7 (.5%) patients. Patients carrying the AA or the AT/TT genotypes were similar according to the most important demographic features such as male gender (56% vs. 62%), age (63 vs. 63) and body mass index (25 vs. 25). They were also similar in terms of HCV genotype distribution (HCV-: 6% vs. 60%), baseline LSM (8 vs. 6 kpa), diabetes prevalence (20% vs. 8%) and platelets count (2 vs. 26 x 0 3 /mm3). De-novo HCC occurred in 25 (5.5%) patients after 3-28 (median 0) months from DAA start, with a 3-year cumulative probability of 6.9%. The 3-year cumulative incidence of HCC was 6.5% in patients with TLL AA and 7.7% in those carrying the AT/TT genotypes (p=0.98). No significant differences were found between AA and AT/TT carriers according to HCC characteristics. They were similar in terms of time to HCC development (0 vs.2 months, p=0.35), nodules number (single node in 80% vs. 50%, p=0.2), αfp values (6 vs. 2 ng/ml, p=0.50), BCLC stage (0-A: 89% vs. 66%, p=0.4), Milan-in criteria (89% vs. 67%, p=0.23) and severity of liver disease (CPT-A in 90% vs.00%, p=0.6). Conclusion: In a large cohort of HCC-free HCV cirrhotics treated with DAA, TLL polymorphism failed to predict the development of de-novo HCC. 09
110 P05-02YI DYSREGULATION OF THE LYSOSOMAL COMPARTMENT WITH VERTEPORFIN POTENTIATES THE ANTI-TUMOR EFFECT OF SORAFENIB IN HEPATOCELLULAR CARCINOMA Jacopo Gavini, Noëlle Dommann, Manuel Jakob, Adrian Keogh, Daniel Candinas 2, Laure Bouchez 3, Deborah Stroka, Vanessa Banz 2 Department for BioMedical Research, University of Bern, Department for Visceral Surgery and Medicine, Bern University Hospital, University of Bern, Bern, Switzerland, Bern, Switzerland, 2 Inselspital of Bern, Department for Visceral Surgery and Medicine, Bern University Hospital, University of Bern, Bern, Switzerland, Bern, Switzerland, 3 Novartis Institutes for Biomedical Research, Basel - Switzerland, Basel, Switzerland Background and Aims: Hepatocellular carcinoma (HCC) is one of the most common malignant cancers worldwide and Sorafenib (SF) is still the first-line treatment for patients with advanced HCC. Alteration in the autophagic flux and in lysosomal compartment are often linked to carcinogenesis and chemoresistance development. Here we study the effect of the photosensitizer Verteporfin (VP) on HCC growth in a preclinical model without prior light activation, focusing particularly on its mechanism of action alone or in combination with SF. Results: Combining in vitro VP with SF led to a synergistic (HuH7) and additive (HepG2) reduction of tumor proliferation. It also decreased SF-induced autophagic flux, which was distinctly and differently activated between the two cell lines. Immunoblot analysis showed that VP inhibits the formation of newly forming autophagosomes (LC3-I) and induces an accumulation of high-molecular weight complexes of proteins (HMW-p62). Furthermore, VP targets lysosomes, increasing their number, altering their shape, size and inducing a strong alkalinization of lysosomal ph (assessed by FACS), which finally leads to lysosomal membrane permeabilization (LMP). VP-induced lysosomal compartment instability synergistically contrasts the passive lysosomotropism of SF, which gives rise to its drug-resistance development. Similar results were obtained in a subcutaneous HCC-cell line and patient-derived xenograft (PDX) mouse model. Here VP potentiated the antitumor effect of SF, by synergistically decreasing tumor cell proliferation (Ki67), tumor angiogenesis (CD3) and the SF-induce autophagic flux, followed by a decreased accumulation of lysosomes. Conclusion: Taken together, these findings suggest that VP, without prior light activation, can significantly potentiate the anti-tumor effect of SF in a HCC preclinical model. Verteporfin inhibits the formation of newly forming autophagososmes and - by specifically targeting the lysosomal compartment stability - concurrently induces their dysregulation and permeabilization. Targeting these pathways with Verteporfin, might constitute a novel strategy to overcome chemoresistance development and to improve cancer therapy in the setting of advanced HCC. 0
111 P05-03YI NON ADHERENCE TO AASLD-EASL GUIDELINES FOR THE MANAGEMENT OF HEPATOCELLULAR CARCINOMA DOES NOT TRANSLATE INTO WORSE OUTCOMES Igor Bramuzzo, Alessio Gerussi, Silvia Maier, Cristiana Bianco, Valerio Barghini, Rosario Francesco Brizzi, Anna Gonta, Alessandro Uzzau 2, Alessandro Vit 3, Debora Donnini, Leonardo Alberto Sechi, Giorgio Soardo University of Udine, Liver unit, Internal Medicine, Department of Experimental and Clinical Medical Sciences, Udine, Italy, 2 University of Udine, Program of oncological surgery, Department of Experimental and Clinical Medical Sciences, Udine, Italy, 3 Azienda Sanitaria Univeristaria Integrata Udine, Division of Vascular and Interventional Radiology, Udine, Italy Background and Aims: Real-life data about adherence to established guidelines for the management of HCC and whether it has an impact on outcome are still lacking. In addition, it is also debated if treatment with TACE is appropriate for all patients with Barcelona Clinic Liver Cancer (BCLC) stage B. Our aim was to assess adherence to AASLD (20) and EASL (202) guidelines in our center, evaluating any difference between adherent and non-adherent patients, including transplant-free survival. Method: 57 patients managed at a single tertiary center for a first diagnosis of HCC between January 20 and December 206 were retrospectively included. Detection of a lesion more than 24 months after a previous hepatic resection for HCC has been considered a new event. Demographics features and laboratory values at diagnosis were collected and Child-Pugh score, model for end stage liver disease (MELD), aspartate aminotransferase platelet ratio index (APRI score) were calculated. The extension of the tumor burden was classified into 4 patterns, monofocal, oligofocal (2-3 lesions), multifocal, and infiltrative pattern, and also according to Milan criteria. Patients were stratified according to BCLC classification. Adherence was assessed on first treatment after diagnosis. To assess baseline factors associated with non-adherence to guidelines a univariate binary logistic regression analysis was performed. Cases were censored at the occurrence of death or liver transplant. A Kaplan-Meier survival analysis was performed to assess transplant free survival (TFS) in adherent patients compared to nonadherent ones. Results: Median age was 68 years (IQR 4). The prevalence of cirrhosis was 88.5% and the main etiologies were alcoholic and HCV (47% and 35% respectively). Overall adherence to guidelines was 73.9%. Non-adherent patients (n = 4) were mostly in BCLC A (34%) or B (39%) stages, and they did not have a different transplant-free survival than those treated according to the standard of care. Only oligofocal cases were associated with less adherence to guidelines (OR 0.34, p < 0.0). However, patients with oligofocal tumor not being treated according to standards did not show a worse TFS than those with oligofocal onset treated according to guidelines. After stratifying patients for BCLC stage there was still no difference in TFS between adherent and non-adherent ones. Conclusion: Our data suggest that non-adherence to guidelines for the management of HCC does not necessarily translate into worse outcomes. Non-adherence is more prevalent in oligofocal cases since these ones are more likely to be discussed in a multidisciplinary context, where strategies different from the established guidelines may be agreed to reach a more tailored management.

112 P05-04YI MALDI IMAGING OF HEPATOCHOLANGIOCARCINOMAS: A CLUE TO TACKLE TUMOR HETEROGENEITY. PRELIMINARY RESULTS. Elia Gigante, Rita Casadonte 2, Julie Le Faouder, Miguel Albuquerque, Nicolas Poté 3, Olivier Soubrane 4, Valérie Paradis 3 INSERM 49, Université Paris Diderot, Clichy, France, 2 Proteopath GmbH, Proteopath GmbH, Trier, Germany, 3 Beaujon Hospital, Pathology Department, Clichy, France, 4 Beaujon Hospital, Department of HPB surgery, Clichy, France Background and Aims: Hepatocholangiocarcinomas (H-ChCs), are mixed primary tumors of the liver, defined by the presence of hepatocellular carcinoma (HCC) and cholangiocarcinoma (CC) components that may display stem cell features. Accordingly, H-ChC represents the most illustrative heterogeneous liver malignancies. Its tumoral heterogeneity hampers molecular analysis that may provide various signatures according to the area analyzed. The aim of this study was to assess the peptidic profiles of the different morphological patterns constitutive of H-ChC by MALDI imaging, an in situ approach able to connect molecular profiles with specific histological features, without preliminary step of molecular extraction or labeling. Method: MALDI imaging (RapifleX and Autoflex III MALDI, Bruker Daltonik GmbH) was applied on paraffin tumor sections of tissues microarrays (TMAs) built from 60 surgical cases of H-ChC. Entire tissue sections of selected cases were also analyzed (0 cases). Peptidic spectra were obtained from the different tumor patterns constitutive of H-ChC as well as from CC (n=29) and HCC (n=23) and the most discriminant peaks were identified. Results: Rich peptides spectra were obtained from all tumor cases tested, with more than 90 peptides peaks identified. The comparison of the relative intensities of each m/z value (peptidic peak) between the three tumor types (H-ChC, HCC, CC) revealed 9 discriminant peaks exhibiting a statistical significance. They showed a receiver operating curve (ROC) curve superior to 0.7 in the identification of H-ChCs when applied on cases and controls (Example, peak 466 in figure ). Comparative analysis of H-ChC cases showed great heterogeneity () from case to case (Fig. lanes and 2 compared to lanes 3 to 5), (2) within case from different areas of the tumor (Fig. lanes 2 and 3), and (3) within case from a single tumor area (Fig. lane ). Conclusion: This preliminary study demonstrates that MALDI imaging is a powerful tool for providing peptidic signatures from formalin fixed paraffin-embedded tumor samples. In addition, it confirms that H-ChCs are highly heterogeneous at the molecular level both at the inter and intratumoral scale. The identification of the proteins specifically associated with the different tumor components is currently ongoing. Figure: Fig. Expression of m/z 466 peak on a TMA. Each lane corresponds to a H-ChC case. A) Optical image, B) ion density map of peak 466, C) magnification of core 5, showing an enhanced intensity of m/z 466 in specific tumoral zones D) optical image, core 5, tumoral zones are highlighted in red discontinuous line. 2
113 P05-05YI HYPERBILIRUBINEMIA IS A FALLACIOUS PARAMETER TO DETECT LIVER TOXICITY IN PATIENTS WITH HEPATOCELLULAR CARCINOMA TREATED WITH SORAFENIB AND MAY LEAD TO INADEQUATE TREATMENT INTERRUPTION Alvaro Diaz-Gonzalez, Víctor Sapena, Marco Sanduzzi-Zamparelli, Ferran Torres 2, Neus Llarch, Gemma Iserte, Alejandro Forner, Leonardo Gomes Da Fonseca, José Ríos 3, Jordi Bruix, Maria Reig BCLC group. Liver Unit. Hospital Clínic de Barcelona. IDIBAPS. CIBERehd, Hospital Clínic i Provincial de Barcelona, Barcelona, Spain, 2 Medical Statistics core facility, IDIBAPS, Hospital Clinic Barcelona, Biostatistics Unit, Faculty of Medicine, Universitat Autònoma de Barcelona, Barcelona, Spain, 3 Medical Statistics Core Facility, Institut d Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Hospital Clinic, Barcelona, Spain. Biostatistics Unit, Faculty of Medicine, Universitat Autònoma de Barcelona Background and Aims: The elevation of 2 points on Child-Pugh (CP) or jaundice in hepatocellular carcinoma (HCC) patients without tumor progression may drive to an early discontinuation of sorafenib in some centers. Nevertheless, 96% of the drug is metabolized through CYP3A4 /UGTA9. Thus, increasing bilirubin (TB) may not reflect only liver dysfunction. The objective is to identify and characterize the profile of sorafenib-treated patients that have an early (within the first 60 days) discontinuation because of CP or TB increase and to compare their outcomes with those patients that do not present such event or those who have a BT increase because of indirect bilirubin (IB). Method: We analyzed a prospective database of patients with HCC (CP A/B7 and PS 0/) treated with sorafenib. We defined as increase of TB the change of at least grade of TB (as per CTCAE classification). We considered the increase secondary to IB if ratio the DB/IB was <. Results: Between , 299 patients were treated with sorafenib (54,2% BCLC-C, 88,6% ECOG- PS0 y 83,6% CPA). Median treatment and overall survival (OS) of the cohort was 6.5 and 3.3 months, respectively. Thirty patients out of 87 who started sorafenib with normal TB presented an early increase of TB (6%) and 34/2 with increased baseline TB presented an early elevation of TB (2.42%). 2 patients had an early modification of CP, 3 of them due to IB elevation but 2 presented also encephalopathy and ascites. The median treatment duration of the 0 patients who presented an early increase (>= 2 grades) was 5.4 months (IQR ). However, the median treatment duration and OS of the 4 patients who had an early TB increase because of IB was 9. months (IQR ) and 0. months (IC95; ), respectively. The other 289 patients that did not have TB increase, the time on treatment and OS was 6.5 months (IQR ) and 3.5 months (IC ). Although only 4 patients had TB increase because of IB, median treatment duration and OS in those patients was not statistically different to those that did not have an early increase of TB. Conclusion: About 20% of patients treated with sorafenib present an early increase of total bilirubin. However, that increase is mainly because of indirect bilirubin (40%) and does not have an impact on survival. Attending to this, isolated increase of total bilirubin must not be seen as liver failure in patients treated with sorafenib. 3
114 P05-06YI HCC RECURRENCE AFTER DAA TREATMENT IN HCV PATIENTS. Maria Guarino, Dario Bruzzese 2, Giovan Giuseppe DI Costanzo 3, Marco Guarracino 3, Federica Morando 4, Luca Rinaldi 5, Marcello Persico 6, Angelo Salomone Megna 7, Nicola Coppola 8, Nicola Caporaso 9, Filomena Morisco 0 University of Naples Federico II, Gastroenterology Unit, Department of Clinical Medicine and Surgery, Naples, Italy, 2 University of Naples Federico II, Department of Public Health, Naples, Italy, 3 Cardarelli Hospital, Hepatology Unit, Naples, Italy, 4 University of Naples Federico II, Gastroenterology Unit, Department of Clinical Medicine and Surgery, Naples, Italy, 5 University of Campania "Luigi Vanvitelli", Department of Medical, Surgical, Neurological, Geriatric and Metabolic Sciences, Naples, Italy, 6 University of Salerno, Department of Medicine and Surgery, Salerno, Italy, 7 Rummo Hospital, Division of Infectious Diseases, Benevento, Italy, 8 University of Campania Luigi Vanvitelli, Department of Mental Health and Public Medicine, Section of Infectious Diseases, Naples, Italy, 9 University of Naples Federico II, Gastroenterology Unit, Department of Clinical Medicine and Surgery, Naples,, University of Naples Federico II, Gastroenterology Unit, Department of Clinical Medicine and Surgery, Naples, Italy Background and Aims: Recently several studies reported conflicting and unexpected data about the possible increased risk of HCC recurrence after DAAs therapy. The present real-life multicenter, prospective study aims to investigate the impact of new DAAs IFN-free therapies in HCV patients with a previous successfully treated HCC, in terms of neoplastic recurrence. Method: From March 205 to March 207, all consecutive HCV patients with a previous successfully treated HCC underwent DAAs therapy were enrolled. The baseline clinical, biochemical and radiological data were registered. The assessment of neoplastic recurrence was used as primary outcome, while a secondary outcome was the evaluation of patients characteristics predicting HCC recurrence. Results: Eighty patients (mean age 66.8±8.9 yrs, 63.8% male, BMI 25.8±3.0) were consecutively enrolled. Eighty-two percent of them were in Child-Pugh class A, and 86% had a history of HCC BCLC stage 0/A, while 36.3% of patients had a prior HCC recurrence. Eighty-eight percent of the patients achieved sustained virological response (SVR). The median time between the last HCC treatment and DAAs-starting was 0.2 months (range ), while the median time from the radiological confirmation of HCC complete response was 4.8 (range ) Twenty-two HCC recurrences were observed from DAAs-starting in a median observational follow-up of 5.9 months (range: ), showing a nodular or infiltrative pattern in 9% and 9%, respectively. The cumulative rate of recurrence was 9.6/00 person-year (95% C.I ). The 6-, 2- and 24-months HCC recurrence rates were.2%, 9.% and 30.%, respectively. Higher BMI (HR.25, 95% C.I ) and DAAs treatment failure (5.43, 95% C.I ) were significantly associated with higher risk of HCC recurrence, both at univariate and at Cox multivariate analysis. Conclusion: Patients without HCC recurrence are characterized by lower BMI and higher SVR rate. These data suggest that the absence of well-known HCC risk factors reduces the recurrence rate of HCC also in patients treated with DAAs. 4
115 P05-07YI SHORT-TERM RECURRENCE OF HEPATOCELLULAR CARCINOMA IN HCV INFECTED PATIENTS IS UNAFFECTED BY DIRECT ANTIVIRAL AGENTS THERAPY. A CASE-CONTROL, SINGLE CENTER STUDY. Raffaella Tortora, Marco Guarracino, Massimo De Luca, Giuseppe Arenga 2, Luca Campanella 2, Walter Santaniello 2, Giovan Giuseppe DI Costanzo "Cardarelli" Hospital, Transplantation, Liver Unit., Napoli, Italy, 2 "Cardarelli" Hospital, Transplantation, Surgery Unit., Napoli, Italy Background and Aims: The implementation of direct antiviral agents (DAA) represented a major advance in hepatology. However, it is still largely debated if the rapid removal of HCV infection may affect the immune surveillance favoring the growth and spread of cancer cells. This study aimed to prospectively evaluate the rate of HCC recurrence following DAA therapy. Method: From April 205 to August 207,004 HCV infected patients received DAAs at Liver Unit of Cardarelli Hospital. Among these, 70 patients previously treated for HCC were enrolled. Before starting DAA, CT or MRI were done to evaluate complete cancer necrosis. Five patients were excluded because the review of pre-treatment imaging showed active HCC. Genotype distribution was: 54 patients Gb, 3 Ga, 5 G2, and 3 G3. Only a Gb and a G3 patient relapsed after treatment (SVR = 97%). BCLC HCC stage was A in the majority (83%) of cases. Ultrasound and AFP were performed monthly during treatment, bimonthly in the next 6 months, and every three months thereafter. CT or MRI were done every six months and when recurrence was suspected. One hundred eighty-six HCV cirrhotics with successfully treated HCC, never treated with DAA, represented the control group. Results: Median interval between last HCC treatment and DAA starting was 9 (-37) months. Median follow-up was 8 (-30) months. Four patients died and 2 received liver transplantation. Crude recurrence rate was 27.7%.Median time-to-recurrence was 23.2 (95%CI, ) months among DAA-treated and 23.0 (95%CI, ) months in the control group. Pattern of recurrence in DAAtreated patients was monofocal in 76%, multifocal in 2%, and advanced in 2%. Conclusion: DAA treatment was highly effective in HCV patients with successfully treated HCC. Shortterm HCC recurrence rate was comparable to that of untreated controls. Longer follow-up is needed to evaluate if SVR may reduce HCC recurrence rate. 5
116 P05-08YI ENDOPLASMIC RETICULUM STRESS IN HEPATIC STELLATE CELLS CONTRIBUTES TO THE PROGRESSION OF HEPATOCELLULAR CARCINOMA. Femke Heindryckx, Natasa Pavlovic, Pär Gerwins 2 Uppsala University, Medical Cell Biology, Uppsala, Sweden, 2 Akademiska sjukhuset, Radiology, Uppsala, Sweden Background and Aims: One of the key players in the progression of cirrhosis to hepatocellular carcinoma (HCC) is the hepatic stellate cell, which is activated during liver damage. Activated stellate cells create a favourable tumour environment and produce growth factors and cytokines that enhance tumour cell proliferation and migration. We have recently shown that inhibiting the endoplasmic reticulum (ER) stress-induced IREa signalling pathway blocks stellate cell activation in vitro and reduces liver fibrosis in vivo. We now wanted to identify the role of ER-stress in the cross-talk between stellate cells and cancer cells in HCC. Method: HCC was induced in mice by weekly injections with diethylnitrosamine. Mice were treated with an IREa inhibitor 4u8C or control, samples were taken after 25 weeks. Tumour burden and collagen deposition was quantified on H&E and Sirius red staining, respectively. The HCC-cell lines (HepG2 and Huh7) and stellate cell line (LX2) were co-cultured using transwell assays and RNA was isolated after 48 hours. Tumour spheroids were formed by culturing HepG2 and LX2 cells on ultra-low-attachment plates on which viability was measured by resazurin. Non-directional and directional migration (chemotaxis) was assessed on fluorescently labelled cells using scratch wound assays and 2D CellDirectors, respectively. ER-stress was inhibited in vitro with 4u8C or sirna against IREa. Results: Treatment with 4u8C significantly decreased the number of tumours in vivo, compared to controls. Sirius red staining showed a significant decrease in collagen after treatment with 4u8C, compared to controls. Co-culturing experiments confirmed that tumour cells (HepG2 and Huh7) secrete factors that significantly increase mrna expression of ER-stress markers (CHOP, spliced XBP and BiP) in LX2 cells. Co-culturing also led to significantly increased mrna expression of stellate cell activation markers (asma and collagen) compared to monocultures. This was significantly decreased by 4u8C. Inhibition of ER-stress by 4u8C or by siirea transfection of LX2-cells significantly decreased proliferation in spheroids and 2D cocultures. Co-culturing HepG2 and LX2 cells significantly increased migration on a scratch wound compared to mono-cultures. Treatment with 4u8C significantly decreased nondirectional and directional migration towards a gradient of chemoattractant in LX2-HepG2 cocultures in 2D CellDirectors. Conclusion: Our results suggest that ER-stress is an important mediator in the communication between stellate cells and cancer cells. Tumour cells secrete factors that induce ER-stress in stellate cells, which contributes to their activation. Blocking the IREa ER-stress pathway reduces stellate cell activation, tumour cell proliferation and migration. Components of the ER stress pathway may therefore be therapeutically relevant for HCC-patients. 6
117 P05-09 COMPREHENSIVE EVALUATION OF THE ROLE OF RECEPTOR TYROSINE KINASE FAMILY IN HEPATOCELLULAR CARCINOGENESIS Sen-Yung Hsieh Chang Gung Memorial Hospital, Linkou, Gastroenterology and Hepatology, Taoyuan, Taiwan Background and Aims: Receptor tyrosine kinases (RTKs) are of great clinical interest because of their fundamental roles in physiology and as treatment targets in many types of human cancer. The human RTK family comprises 59 members and many of them have been reported to be required for the oncogenesis of many human cancers, thereby serving as treatment targets. However, primary and acquired resistance to anti-rtk therapies remains as the primary challenges in anti-cancer therapies. Method: We systematically evaluated their expression of all the RTK family members in human HCCs and conducted an RNA interference screen on the entire RTK family to evaluate their roles in the tumorigenicity of hepatocellular carcinoma (HCC). Results: We found that more than half of RTKs were expressed in each HCC (26.2 ± 7.34) and normal liver sample (30.38 ± 4.3; N vs. T, P = 0.022), and that advanced HCCs (24.00 ± 7.52) expressed fewer RTKs than early HCCs (30.38 ± 5.2; N vs. T, P = ). Loss-of-function screen through xenograft-tumor growth in nude mice and tumor-sphere formation in soft agars revealed that 3 and 7 RTKs presented with promoting or suppressing effects on the tumorigenicity of human Huh7 cells. Interestingly, the counteracting roles oncogenic and tumor-suppressive activities exerted by different members of the same RTK subfamilies were frequently found. Gene ontology revealed that coexpression of multi-rtks in HCC might be involved in regulation of cell proliferation, differentiation, death evasion, angiogenesis, immune reaction, and cell-matrix interaction to counteract with an everchanging microenvironment. Conclusion: Our findings suggest a complex intra- or/and inter-subfamily interplays of RTKs in human HCC and a high potential of HCC cells to respond to and counteract diverse microenvironmental stimuli, which reveals a new insight about how cancer cells survive and evade anti-cancer treatment. Our findings will assist in developing new strategies to improve current anti-hcc strategies. 7

118 Figure: Figure. Multiple RTKs play diverse roles in hepatocellular carcinogenesis. Expression of multiple RTKs in hepatocytes and hepatoma cells endows cells with diverse capacity to counteract different microenvironmental stimuli during the different stages of hepatocellular carcinogenesis. (A) Chronic inflammation of the liver (chronic hepatitis) persistently activates certain RTKs (such as TYRO3, ALX, MER, NTRK) to facilitate cell proliferation. (B) Cirrhosis provides a unique microenvironment that fosters tumor transformation. (C) Multiple RTKs provide growth stimuli, angiogenic induction, and deathevasion for tumor both progression and resistance to anti-cancer therapies. Notably, the neuregulin/erbb3 autocrine loop represents an autonomous growth signaling for HCC development. 8
119 P05-0 PREDICTORS OF HEPATOCELLULAR RECURRENCE AFTER LIVER TRANSPLANT IN HEPATITIS C PATIENTS: A TEN-YEARS SINGLE CENTER COHORT Massimo Iavarone, Maria Francesca Donato, Federica Invernizzi, Matteo Angelo Manini, Sara Monico, Angelo Sangiovanni, Marco Maggioni 2, Paolo Reggiani 3, Giorgio Rossi 3, Pietro Lampertico Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Università degli Studi di Milano, CRC A.M. and A. Migliavacca for Liver Disease, Division of Gastroenterology and Hepatology, Milano, Italy, 2 Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Department of Pathology, Milano, Italy, 3 Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, University of Milan, HBP Surgery and Liver Transplantation Unit, Milano, Italy Background and Aims: Liver transplantation (LT) is a well-established treatment for HCV-related cirrhosis and HCC within Milan criteria (MC) with a reported recurrence rate of 6%. Recently contradictory results on HCC recurrence in HCV patients treated with DAA emerged. The study aims to identify biological and clinical predictors of HCC recurrence and to report overall survival (OS) post-lt in HCV-cirrhotic patients with HCC. Method: Between November 2004 and August 206, 08 HCV consecutive cirrhotic patients underwent LT for HCC (8% males, age 57 years, 80% genotype, 22% HCV-RNA negative at LT, 33% nonresponder to previous IFN-therapy, 22% treated by DAA). At LT median AFP was 0 ng/ml ( 5,655). At explant pathology: 78% were within MC, median viable neoplastic nodules were 2 (0 9), 22% showed microvascular invasion, 47% with Edmonson score 3 and 3 cases showed mixed HCC/cholangiocarcinoma (icc). Results: During 46 months of post-lt follow-up (.5-58), HCC recurred in 4 patients (extra-hepatic 86%) after 6 (4 90) months, with a 3-year cumulative probability of 9%. Among them: 5 were beyond MC, 7 with vascular invasion, had Edmonson score 3 or mixed HCC/iCC; 9 patients were HCV RNA negative at the time of recurrence (4 after IFN, 5 after DAA pre-lt). At univariate analysis vascular invasion (HR 4.3, 95%CI , p<0.00) and Edmonson score 3 or mixed HCC/iCC (HR 7.4, 95%CI , p=0.009) predicted HCC recurrence. These predictors were confirmed by multivariate analysis (HR 2.7, 95%CI.-6., p=0.09 and HR 9.2, 95%CI.-76, p=0.04, respectively). Twenty-four patients died after of 3 months (.5-94): 5 for HCC progression, 5 due to HCV recurrence, 7 for sepsis, 5 for non-liver tumors and 2 for surgical complications. Five-years OS was 77%. Conclusion: In our series of HCV-HCC transplanted patients, only tumor-related histological features at explant pathology predicted HCC recurrence. 9
120 P05- EARLY TREATMENT WITH SORAFENIB AND MTOR INHIBITOR IN RECURRENT HEPATOCELLULAR CARCINOMA AFTER LIVER TRANSPLANTATION: SAFETY AND SURVIVAL. Federica Invernizzi, Massimo Iavarone, Maria Francesca Donato, Angelo Sangiovanni, Sara Monico, Matteo Angelo Manini, Umberto Maggi 2, Barbara Antonelli 2, Daniele Dondossola 2, Giorgio Rossi 2, Pietro Lampertico Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Università degli Studi di Milano, CRC A.M. and A. Migliavacca for Liver Disease, Division of Gastroenterology and Hepatology, Milan, Italy, 2 Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, University of Milan, HBP Surgery and Liver Transplantation Unit, Milano, Italy Background and Aims: Sorafenib is currently used in hepatocellular carcinoma (HCC) recurring after liver transplantation (LT), generally when other approaches are unsuitable, while the association of sorafenib and mtor inhibitors (mtori) has been poorly studied. Aim of the study was to assess the safety and effectiveness of early introduction of sorafenib+mtori for HCC recurring after LT. Method: Patients with HCC recurring after LT started sorafenib+mtori in a longitudinal cohort study. Surgical/locoregional treatments were performed before and during sorafenib+mtori. Modifications and interruptions of sorafenib and mtori were based on adverse events (AE), liver graft dysfunction and/or symptomatic cancer progression. Endpoints were safety, effectiveness and overall survival (OS). Results: Twenty non-cirrhotic patients received sorafenib+mtori as soon as HCC recurred (age 58, male 80%, HCV-RNA positive 20%, surgery/locoregional treatments 75%). During 2 (-70) months of sorafenib treatment all patients had at least one sorafenib-associated AE, generally graded 2. Sorafenib was reduced in 5 patients and discontinued in 9 (symptomatic progression in 6, AE in one, liver graft dysfunction in 2). mtori-associated AEs occurred in 9 patients, dose was reduced in 6 and discontinued in 4. No significant drug-drug interactions were registered. Time-to-first radiological progression was 7.5 months (95%CI 3.9-). Eight patients died, all for HCC progression: the - and 5- year cumulative OS were 82% (95%CI 53-94%) and 33% (95%CI 9-6%), respectively, with a median OS of 29 months (95%CI 26-3). Conclusion: Early treatment with sorafenib+mtori combined with locoregional treatments extended patients survival with a favourable safety profile in HCC recurring after LT. 20
121 P05-2YI CHANGING CLINICAL PROFILE AND EPIDEMIOLOGY OF HEPATOCELLULAR CARCINOMA IN INDIA Vaneet Jearth, Sridhar Sundaram, Prachi Patil, Shaesta Mehta TATA Memorial Hospital, GASTROENTEROLOGY, Mumbai, India Background and Aims: Hepatocellular carcinoma (HCC) is one of the common cancers worldwide. The number of patients of HCC with non-viral etiology is increasing as the prevalence of lifestyle-related factors like chronic alcoholism, obesity, diabetes and metabolic syndrome change globally. Unlike Hepatitis B Virus (HBV)/ Hepatitis C Virus (HCV) related HCC (HBHC HCC), in which the high-risk populations and surveillance programs are well established, little is known about the characteristics of HCC negative for markers of chronic viral hepatitis labeled as Non-B Non-C HCC. We analyzed etiological and clinical profile of consecutive HCC patients registered at our tertiary care cancer center. Our aim was to study the change in epidemiology and compare clinical characteristics of patients with non-b non-c HCC (NBNC HCC) with those having viral etiology for HCC.Method: Consecutive patients diagnosed with HCC with age >8 years between June 207 and November 207 were prospectively enrolled. Patients with history of any prior surgical or interventional treatment were excluded. 64 consecutive patients of HCC were screened and 55 patients were enrolled for the study. All patients of HCC with negative HbsAg and Anti HCV were evaluated for IgG Anti Hbc.Those patients who detected positive for core antibody were analyzed for HBV DNA in serum. Patients who detected negative for viral markers were labeled as Non B Non C HCC (NBNC HCC). Patients with presence of only core antibody with non detectable HBVDNA in serum were also grouped under NBNC HCC category in view of doubtful oncological significance. Results: Most of patients were males (n=39, 89.7%) with mean (± SD) age of 56. ± 3.6. Total number of patients with NBNC HCC were 66 (42.6 %). Overall HCC was found to be most commonly associated with HBV (n= 6). Abdominal pain was the most common symptom on presentation in both groups. Cirrhosis was detected in 65.5 % (n= 43) of patients with NBNC and 86.5% (n= 77) of patients with HBHC HCC (p value = 0.002). Out of patients with cirrhosis CTP A, B and C were 34.2 %, 34.2 % and 2.3 % respectively with no significant difference in both the groups. Percentage of patients in BCLC A,B,C and D were 3.2 % ( n=5), 30.3 %(n=47), 5.6%( n=80) and 4.8% (n=23) respectively with no significant difference with both groups. Major vascular invasion was found to be more common in HBHC (56.% vs 5.5 %, p value = 0.55). Conclusion: Incidence of HCC is increasing rapidly in India. Although hepatitis B still remains the leading cause of HCC in India, NBNC HCC are on the rise accounting for approximately 40% patients (past estimate was 5-5 %). Follow up is needed to assess the differential response to treatment between viral and non viral HCC. Table. HCC AFP ng/ml < >400 Bilirubin mg/dl Mean (± SD) Size of largest lesion (cm) Mean (± SD) Albumin g/dl Mean (± SD) Ascites HBHC ± ± ± NBNC ± ± ±
122 P06-0 GLOBAL PROTEIN ABERRATION SCORE (GLOPAS), A COMPREHENSIVE RISK SCORE TO PREDICT HEPATOCELLULAR CARCINOMA BIOLOGY AND ESTIMATE PATIENTS' SURVIVAL Ahmed Kaseb, Emma Zohner, Lianchun Xiao, Zeya Wang, Manal Hassan, Reham Ali, Karri Ballard 2, Wenyi Wang, Hesham Amin, Jeffrey Morris The University of Texas MD Anderson Cancer Center, 2 Myriad Rules Based Medicine (RBM), Austin, Texas Background and Aims: Existing hepatocellular carcinoma (HCC) staging systems use a small number of empirically selected clinical/biological variables. We hypothesize that GloPAS (global protein aberration score) will capture a more global measurement of disease biology that can partition HCC into three subsets: () essentially normal profiles, (2) extremely aberrant profiles, and (3) slightly aberrant profiles. Method: We collected plasma samples and clinical data prospectively from 767 HCC patients and 200 healthy controls, and quantified 37 proteins using a CLIA-certified panel by Myriad RBM, Austin, TX. We applied a deconvolution algorithm, originally developed for determining percent normal contamination for tumor, to quantify the degree of global protein aberration, for each patient, relative to normal controls. We defined three distinct groups of patients with low (<0.3), medium ( ), and high (>0.8) GloPAS and assessed GloPAS association with overall survival (OS) and other prognostic factors using log-rank tests and compared the prognostic abilities of GloPAS vs. existing systems using concordance index(c-index). We developed a single-sample GloPAS (ssglopas) using an algorithm that can be applied to the single sample setting. Results: Although determined without using information about OS or any patient-level clinical or demographic factors (i.e. unsupervised), GloPAS showed remarkable prognostic separability (low/med/high GloPAS, with median OS 38.2mo/8.3mo/7.mo, p<0.000). GloPAS prognostic ability was far above any existing HCC staging system (C-index=0.75 vs p<0.000), demonstrating even more prognostic information than key factors such as metastatic status and vascular invasion, and providing substantial refinements to existing staging systems. The ssglopas was able to recapitulate the global signal captured by the GloPAS score with a much smaller subset of 4 proteins. Conclusion: GloPAS significantly improved prediction of OS and prognostic stratification of conventional HCC staging systems. After further validation, ssglopas could be used to guide therapy decisions and stratify HCC patients for clinical trials. The novel concept underlying GloPAS methodology can be applied to other cancer settings to build disease-specific prognostic blood scores. 22
123 P06-02YI A NEW PROGNOSTIC SCORING SYSTEM FOR CIRRHOSIS AND HEPATOCELLULAR CARCINOMA UTILIZING CD44 RS875 GENE POLYMORPHISM Ayman El-Shayeb, Nermeen Abdeen, Neveen Lewis 2, A Ali Khalifa Faculty of Medicine, Alexandria University, Tropical Medicine Department, Alexandria, Egypt, 2 Faculty of Medicine, Alexandria University, Clinical Pathology Department, Alexandria, Egypt Background and Aims: Hepatocellular carcinoma (HCC) is the third leading cause of cancer death worldwide. HCC occurs in approximately % of non-cirrhotic HCV patients and in 7% in those with cirrhosis. Irreversible accumulation of genetic alterations is an integral driving force in the development of HCC. Despite all current diagnostic and therapeutic modalities, HCC still has a poor long-term prognosis. This has been attributed to the general state of the patient, poor liver profile and the tumour behaviour per sae. Hence, a scoring system that encompasses the prior points could provide a better understanding of the liability of cirrhotic patients to develop HCC and the aggressiveness of the tumour. We established a new prognostic scoring system for the assessment of the potentiality of developing HCC among cirrhotic patients as well as the aggressiveness of HCC. What s new about this study is the incorporation of CD44 gene polymorphism, a liver-specific cancer stem cell that has been proven to play a pivotal role in tumour behaviour. CD44 is closely associated with aggressive behaviour and correlates with poor prognosis in a variety of human malignancies by inducing cellular proliferation, adhesion, and migration. Method: 20 Egyptian patients were enrolled in our study; they were classified into four groups: Group I 20 patients having metastatic HCC Group II 20 patients having non metastatic HCC Group III 40 patients with HCV related cirrhosis Group IV 40 healthy subjects as a control. Using a multivariate logistic regression analysis, 6 parameters were found to be independent risk factors for the predication of HCC development; these were CRP, ESR, AFP, cahexia, Child-Pugh (CPT) score, and CD44 rs875 gene polymorphism. Moreover, we established another score for prediction of metastatic HCC among HCC patients, this score incorporated CRP, ESR, AFP, cahexia, and portal vein thrombosis (PVT). Results: We developed a score of 0 points for prediction of the probability of developing HCC among cirrhotic patients. This score is composed of AFP >200 (score 4), cahexia (), CPT B/C (2), CD44 (), ESR >35 (), CRP >5 (). Score of >3 had sensitivity of 87.5% and specificity of 72.5%. In addition, we established a score of 8 points for prediction of the probability of developing metastatic HCC among patients with early stage HCC. This score is composed of AFP >200 (score ), cahexia (2), PVT (), CD44 (2), ESR >35 (), CRP >5 (). Score of >5 had sensitivity of 90.4% and specificity of 68.4%. Conclusion: All the currently available HCC scoring systems arise as a compromise between easy applicability and discriminatory capability. We designed a scoring system that takes in consideration both patients clinical statuses, and genetic induced malignant tumour behaviour. Our scoring system has shown to be useful in assessing the risk of developing HCC and the risk of developing the highly aggressive metastatic HCC. 23
124 P06-04 PRESENCE OF NON-HYPERVASCULAR HYPOINTENSE NODULE ON HEPATOBILIARY PHASE OF GADOXETIC-ACID ENHANCED MR: RISK OF TUMOR RECURRENCE AFTER CURATIVE TREATMENT FOR SMALL SINGLE NODULAR HCC AND GUIDANCE FOR SELECTION OF TREATMENT METHODS Dong Ho Lee Seoul National University Hospital, Radiology, Seoul, Korea, Rep. of South Background and Aims: To evaluate whether presence of non-hypervascular hypointense nodue (NHHN) on hepatobiliary phase of gadoxetic acid enhanced liver MR could predict tumor recurrence after curative treatment for small single nodular HCC using either surgical resection or radiofrequency ablation (RFA) and could guide the selection of treatment option. Method: A total of 396 patients with single nodular HCC 3 cm treated by either surgical resection (n=57) or RFA (n=239) were included in this study. All patients underwent gadoxetic acid enhanced liver MR before treatment for HCC. After treatment, overall and recurrence-free survival (RFS) was estimated using Kaplan-Meier method. The presence of NHHN on hepatobiliary phase was assessed, and its prognostic implication was evaluated by using Cox-proportional hazard regression model. Results: The 5-year estimated overall survival was not significantly different between surgical resection and RFA (P=0.46). The estimated 5-year RFS was 57.7% in surgical resection group and 38.5% in RFA group, respectively: this difference was statistically significant (P=0.002). Presence of NHHN was significant predictive factor for RFS in both surgical resection group (62.% 5-year RFS in 38 patients without NHHN vs. 30.3% in 9 patients with NHHN; P=0.002, Hazard ratio [HR]=2.74) and RFA group (42.2% 5-year RFS in 87 patients without NHHN vs. 24.3% in 52 patients with NHHN; P=0.00, HR=.97). In 7 patients with NHHN, there was no significant difference in RFS between surgical resection and RFA (30.3% 5-year RFS in surgical resection vs. 24.3% in RFA, P=0.504). However, when NHHN was absent, 5-year RFS was 62.% in 38 patients treated by surgical resection whereas 42.2% in 87 patients treated by RFA: this difference was statistically significant (P=0.009, HR=.67). Conclusion: Presence of NHHN was significant predictive factor for tumor recurrence after both surgical resection and RFA for single nodular HCC 3 cm, and surgical resection could be a preferred treatment option for patients without NHHN as surgical resection would provide significantly better RFS than RFA for these patients. 24


125 Figure: Recurrence-free survival after surgical resection was compared to that after RFA for single nodular HCC equal to or less than 3cm in patients with non-hypervascular hypointense nodule on hepatobiliary phase gadoxetic acid enhanced MR. Recurrence-free survival after surgical resection was compared to that after RFA for single nodular HCC equal to or less than 3cm in patients without non-hypervascular hypointense nodule on hepatobiliary phase gadoxetic acid enhanced MR. 25
126 P06-05YI UP-REGULATION OF MIR-324 SUPPORTS PROLIFERATION OF HEPATOCELLULAR CARCINOMA CANCER CELLS AND CORRELATES WITH POOR PROGNOSIS OF HCC PATIENTS Pengyu Liu, Menggang Liu, Wenhui Wang, Shan LI, Maikel Peppelenbosch, Ron Smits Erasmus MC, Department of Gastroenterology and Hepatology, Erasmus MC-University Medical Center, Rotterdam, Netherlands Background and Aims: Previous studies have identified several micrornas that exert critical roles in modulating hepatocellular carcinoma (HCC) growth. However, the function of a large number of micrornas remains unclear. Therefore, we aimed to identify potential novel micrornas that associate with HCC patient survival. Method: Using the significance analysis of microarrays (SAM) tool, the TCGA LIHC mirna-seq database (n=372 samples) was explored for mirnas associating with patient survival. Selected mirnas were knocked-down in 4 HCC cell lines using anti-mirnas and knocked-out in two cell lines using CRISPR/Cas9 mediated gene-editing. Treated cell lines were investigated for cell proliferation, colony formation capabilities and RNA-seq analysis. Results: mir-324/3p expression was significantly up-regulated in patient HCC tissues (P<0.000). In addition, higher expression of mir-324/3p (P<0.000) and mir-324/5p (P<0.05) associated with adverse prognosis. Knock-down of mir-324/3p in 4 HCC cell lines resulted in around 30-60% reduced cell viability. To further investigate the function of mirna-324, gene-editing was applied to completely knock-out its expression in the SNU398 and Hep3B cell lines. For SNU398, three independent knockout clones invariably showed reduced proliferation and colony formation ability, whereas this was less obvious in a single-obtained Hep3B clone. RNA-seq analysis of these clones and controls thereof is currently in progress. Conclusion: We demonstrated that mirna-324/3p and 5p correlate with adverse outcome and exerts tumor-supportive effects in cell line models. Uncovering its mode of action is currently in progress. 26
127 P06-06 RECURRENCE AND "DE NOVO" DIAGNOSIS OF HEPATOCELLULAR CARCINOMA AND OTHER NEOPLASMS IN PATIENTS WITH HEPATITIS C TREATED WITH DIRECT-ACTING ANTIVIRALS Javier Fuentes Olmo, Mónica Llorente, Ana Martínez Sapiña 2, Herminia Navarro Aznárez 3, Silvia Espina Cadena, Paula García Cámara, Jesús Gotor Delso, Rosario María Monzón Báez, Patricia Sanz Segura Hospital Universitario Miguel Servet. Zaragoza, Gastroenterology Department, Zaragoza, Spain, 2 Hospital Universitario Miguel ServetZaragoza, Microbiology Department, Zaragoza, Spain, 3 Hospital Universitario Miguel Servet.Zaragoza, Pharmacy Department, Zaragoza, Spain Background and Aims: Direct-acting antivirals (DAAs) have revolutionized HCV patients treatment thanks to their efficacy on eradicating the virus. Recent studies have pointed out some concerns about DAAs increasing the risk of HCC relapse after starting the therapy. Even though discrepancy in the resuts of different investigations exists, the possibility that DAAs may have a role in HCC and other tumors genesis due to a quick alteration in inmune response, can not be refused yet. Method: Retrospective study about a cohort of patients with HCV chronic infecton who underwent treatment with DAAs between By electronic clinical history review, data about basal state, genotype and viral copies, treatment and duration, and evoution after therapy was collected. Results: 25 patients were studied, of which 75,2% were cirrhotics. Mean follow-up time was 8 months. 94,4% got SVR. 7 patients (5,6%) had HCC de novo and 2 had HCC relapse (50%). Statistical association linking fibrosis grade, bilirrubin, albumin, AST, platelets, INR to HCC appearance was observed. 30% of genotype 3 patients developed HCC. We did not find out differences between both therapies except for the use of ribavirin (p=0,067). 2 of 4 patients with previous tumor different from HCC developed relapse (4%). 2 patients were diagnosed of de novo colorectal carcinoma during the follow-up. Conclusion: We did not observe a greater number of de novo or relapse of HCC after the start of DAAs therapy. Grade of liver fibrosis and function seems to be the mean risk factor for HCC. Besides, genotype 3 and ribavirin use may be linked to a major HCC risk, although more specific studies are needed. There does not seem to be a clear conection between DAAs therapy and the appearance or relapse of tumors different from HCC, but it would be neccesary a greater sample to analyse this association. 27
128 P06-07 CLINICAL AND GENETIC PREDICTORS OF HCC OCCURING IN CAUCASIAN COMPESATED HBV CIRRHOTICS TREATED BY ENTECAVIR OR TENOFOVIR FOR 8 YEARS Alessandro Loglio, Enrico Galmozzi, Massimo Iavarone, Glenda Grossi, Mauro Viganò 2, Floriana Facchetti, Maria Grazia Rumi 2, Riccardo Perbellini, Angelo Sangiovanni, Pietro Lampertico Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Università degli Studi di Milano, CRC A.M. and A. Migliavacca for Liver Disease, Division of Gastroenterology and Hepatology, Milano, Italy, 2 Ospedale San Giuseppe, Università degli Studi di Milano, Division of Hepatology, Milano, Italy Background and Aims: HCC development remains the leading complication in HBV-related compensated cirrhotics long-term treated by TDF or ETV but the clinical and genetic predictors are poorly known. We therefore looked for baseline predictors of HCC, including the tolloid like gene (TLL) rs polymorphism which has been recently shown to predict HCC in HCV patients cured by IFN therapy. Method: 258 Caucasian HBV-monoinfected HCC-free CPT-A cirrhotics were consecutively enrolled in a longitudinal cohort study when starting TDF or ETV. Age was 6 (2-83) yr, 82% males, 88% HBeAg negative, 69% with normal ALT, BMI 25 (7-40) kg/m 2, 2% diabetics, 60% NUCs-experienced, 5% with previously treated HCCs, PLT 53 (48-304) x0 9 /L, spleen diameter (7-20) cm, liver stiffness 9 (3-60) kpa, 4% with esophageal varices (EV). Liver stiffness based model (LSPS) 0.62 ( ), 4% PAGE-B score >8. Patients were regularly followed with blood tests and 6-month abdominal imaging until HCC development or Nov 207. Results: Over 02 (8-26) months of study period, 36 (4%) patients developed an HCC after 52 (8-00) months. The 8-year cumulative HCC incidence was 5% (yearly rate.9%). HCC developed in 0 (5%) out of 66 AT/TT (26%) patients compared to 26 (3.5%) among 92 AA (74%) subjects, with a 5- year cumulative HCC incidence of 3.5% vs 8.8%, respectively (p=0.642). At univariate analysis, among several baseline genetic, clinical, demographic and virological features, the presence of EV, HCC history, spleen diameter, baseline Fibroscan, PLT count, age, LSPS and PAGE-B score predicted HCC. At multivariate analysis, previous HCC (HR 7.5, 95%CI 3.4-6, p<0.00), EV (HR 3.3, 95%CI.5-7, p=0.002), diabetes (HR 2.4, 95%CI.-5.5, p=0.03), age (HR., 95%CI.0-., p<0.00) and PLT (HR 0.99, 95%CI ,99, p=0.0) independently predicted de-novo HCC. Among the 244 patients without previous HCC, baseline EV (HR 3.6, 95%CI.4-9., p=0.008), spleen diameter (HR.6, 95%CI.-.5, p=0.005) and age (HR.3, 95%CI.0-., p=0.00) were independent predictors of HCC. The 8-year incidence of HCC was 43% and 7% among patients with and without baseline EV (p<0.00), 20% and 9% among those with spleen diameter >2 or <2 cm (p=0.02), and 7% and 6% among those >60 or <60 years (p=0.007). Conclusion: In HBV compensated cirrhotics NUC-treated for 8 years, older age and severity of portal hypertension at baseline strongly predict HCC, independently from TLL variants. 28
129 P06-08YI ELEVATED CIRCULATING IMMATURE NEUTROPHILS PREDICTS POOR RESPONSE TO THERAPY, SHORTER TIME TO PROGRESSION AND POORER SURVIVAL IN PATIENTS WITH HEPATOCELLULAR CARCINOMA Sheba Macheka, Misti Mccain, Joao Mauricio, Laura Ogle, Claire Hutton, Steven Masson 2, Stuart Mcpherson 2, Peter Littler 3, Ruchi Shukla, Derek A Mann 4, Caroline Wilson 4, David Jamieson, Helen Louise Reeves 2 Newcastle University, Northern Institute for Cancer Research, Newcastle-upon-Tyne, United Kingdom, 2 Newcastle upon Tyne Hospitals NHS Foundation Trust, The Liver Unit, Newcastle-upon-Tyne, United Kingdom, 3 Newcastle upon Tyne Hospitals NHS Foundation Trust, Radiology, Newcastle-upon-Tyne, United Kingdom, 4 Newcastle University, Institute for Cellular Medicine, Newcastle-upon-Tyne, United Kingdom Background and Aims: Neutrophils are first line defenders against pathogens. We have recently shown that () circulating neutrophil number (not lymphocytes or platelets) is associated with poor survival in HCC and (2) neutrophil depletion in a murine HCC model has profound anti-tumour effects 2. A key role promoting HCC progression, metastasis and cachexia is suspected. Our aim was to explore Imagestream Fluorescent microscopy as a means of defining circulating neutrophil maturity in HCC patients, to identify the subtype(s) associated with poorer outcome. Method: The morphology of the nucleus of circulating neutrophils was assessed using the lobe count feature in Ideas software in 69 patients with HCC previously recruited to a pilot study exploring circulating tumour cells (CTCs) 3. Analysis was on images of residual white blood cells stained with DAPI and CD45, interpreted alongside tumour data, radiological response (Complete response CR; partial response/stable disease PR; progressive disease PD), time to radiological progression (TTRP) and survival. Results: The distribution of % neutrophils within each lobe category in a small number healthy volunteers (n=8; % lobe 23%; 2 lobes 25%; 3 lobes 35%; 4 lobes 7%) was similar to that of our HCC series (28%;25%; 33%;4%), although HCC patient heterogeneity was evident - % immature lobe: range 4-59; % mature 4 lobe (5% to 25%). % lobe neutrophils correlated +vely with total circulating neutrophils (0.258, p=0.032, Spearman), while 4 lobe neutrophils correlated negatively (-0.355, p=0.003). % lobe neutrophils correlated significantly with tumour size, the presence of extrahepatic disease, type 2 diabetes and poor performance status (PST). A cut off of 30% in treated patients (<30% n=35; >30% n=9) identified patients with poorer response (CR/PR /PD: <30% 6/4/5 vs >30% 3/4/2, Chi 2 p<0.00) and a shorter TTRP (4. vs 7.5 months; Kaplan Meier p=0.04). Considering the whole series (<30% n= 4; >30% n=28), >30% lobe neutrophils was significantly associated with poorer survival (9.8 vs 22.3 months; p =0.005). Conclusion: These data indicate that elevations in circulating neutrophils in patients with HCC are attributed to an excess of immature lobe cells in the circulation. It is these cells in particular that are associated with deteriorating PST, resistance to treatment, cancer progression and poor survival. Whether these immature cells are mechanistically involved in these processes, or a biomarker of sequestration of more mature multi-lobed neutrophils elsewhere remains to be determined. While the neutrophil count or NLR have a limited role in the management of individual patients, these data suggest that determining the lobe count and phenotype of neutrophils may be much more useful clinically.. Margetts J. et al. BJC Wilson CL. et al. Nat Comms Ogle LF. et al. J Hep
130 P06-09YI ANGPT2 POLYMORPHISMS AND CLINICAL OUTCOME IN ADVANCED HEPATOCELLULAR CARCINOMA PATIENTS RECEIVING SORAFENIB Giorgia Marisi, Luca Faloppi 2, Mario Scartozzi 2, Francesco Giuseppe Foschi 3, Gianfranco Lauletta 4, Martina Valgiusti 5, Stefano Cascinu 6, Paola Ulivi 7, Giovanni Luca Frassineti 5, Andrea Casadei Gardini 5 Biosciences Laboratory, Istituto Scientifico Romagnolo per lo Studio e la Cura dei Tumori (IRST) IRCCS, Meldola, Italy, 2 Medical Oncology, Department of Medical Sciences M.Aresu, University of Cagliari, 3 DPT Internal Medicine, Faenza Hospital, AUSL Romagna, Faenza, Italy, 4 Department of Biomedical Sciences and Human Oncology, Internal Medicine G. Baccelli, University of Bari A. Moro, Bari, Italy, 5 Department of Medical Oncology, Istituto Scientifico Romagnolo per Lo Studio e Cura Dei Tumori (IRST) IRCCS, Meldola, Italy, 6 Modena Cancer Center, Policlinico di Modena, Università di Modena e Reggio Emilia, 7 Biosciences Laboratory, Istituto Scientifico Romagnolo per lo Studio e la Cura dei Tumori (IRST) IRCCS, Meldola, Italy Background and Aims: Sorafenib (S), an oral multi-kinase inhibitor, represents the standard of care for advanced hepatocellular carcinoma (HCC), even if a large number of patients reports limited efficacy with respect to toxic effects. Biomarkers of S efficacy or resistance have yet to be identified. Angiopoietin-2 (Ang-2) is an angiogenic factor that binds Tie2 receptor and cooperates with the vascular endothelial growth factor (VEGF) pathway to maintain physiological functions. Genetic variants in Ang- 2 gene (ANGPT2) may lead to altered activities of the gene. We analyzed the role of ANGPT2 polymorphisms in relation to clinical outcome in advanced HCC patients receiving S. Method: Our retrospective study included 30 advanced HCC patients all undergoing S treatment from June 2009 to April 205. These preliminary data were carried out on one hundred patients and ANGPT2 polymorphisms (rs , rs373939, rs373939, rs96222, rs302022, rs655967, rs296747, rs ) were analyzed by direct sequencing in relation to progression-free survival (PFS) and overall survival (OS). Results: All genotype frequencies followed the Hardy-Weinberg equilibrium. Patients homozygous for ANGPT2 rs GG genotype showed significantly longer PFS (8.3 vs 2.4 month, p= ) and OS (6.7 vs 6.4 months, p= ) than those with the other genotypes (GT+TT), respectively. Median PFS was 3.9 (95% CI ), while median OS was.8 months (95% CI ). No statistically significant differences were observed for the other polymorphisms. Conclusion: Our preliminary results suggest that ANGPT2 gene may be capable of identifying a subset of HCC patients who are more responsive to S. 30
131 P06-0 EXCELLENT 5 YEARS SURVIVAL FOR CIRRHOTIC PATIENTS DEVELOPING AN HEPATOCELLULAR CARCINOMA DURING LONG-TERM ORAL THERAPY FOR HBV Massimo Iavarone, Alessandro Loglio, Glenda Grossi, Mauro Viganò 2, Floriana Facchetti, Maria Grazia Rumi 2, Riccardo Perbellini, Angelo Sangiovanni, Pietro Lampertico Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Università degli Studi di Milano, CRC A.M. and A. Migliavacca for Liver Disease, Division of Gastroenterology and Hepatology, Milano, Italy, 2 Ospedale San Giuseppe, Università degli Studi di Milano, Division of Hepatology, Milano, Italy Background and Aims: Long-term oral nucleos(t)ide analog (NUC) therapy in patients with hepatitis B virus (HBV)-related chronic hepatitis or cirrhosis reduces the development of hepatocellular carcinoma (HCC) but the clinical features of HCC and patients survival in this specific population are still poorly characterized. Method: All HCCs developing between 2005 and 206 in NUC treated HBV patients were studied in our two Liver Centers. HCC surveillance and diagnosis were performed according to international guidelines. HCC occurring within the first six months of NUC therapy were excluded. Endpoints of the study were clinical features of HCC and patients outcome. Results: 76 patients developed a HCC after 7 years (-6) of NUC therapy. Age was 67 years (40-83), 84% male, 96% Caucasian, 95% HBeAg negative, 96% with undetectable HBV DNA, 89% genotype D, 80% with normal ALT levels, 87% cirrhotics (9% CPT score A). At HCC diagnosis median AFP levels were 4 ng/ml (-3,65), with 36% of the patients with AFP >7 ng/ml. HCC was monofocal in 78%, with median diameter of 20 mm (range: 6-57), 92% BCLC 0 or A, 93% within Milan criteria, neoplastic portal vein thrombosis was present in 3%. As first-line treatment, 78% patients received radical therapies (39% RFA, 28% surgical resection, % liver transplantation - LT). Overall, a complete response was obtained in 6 (80%) patients: in 40 after a first-line treatment, in 3 after the second-line treatment, in 2 after a third-line treatment, while 6 were transplanted. During 45 (range 7-44) months of follow-up after HCC diagnosis, 9 (25%) patients died, 84% for HCC progression. The median time to recurrence of 20.2 (3-53) months and the overall 5-year survival was 69% (LT=alive) or 50% (LT=dead). Conclusion: Most HCCs developing in patients long-term treated with NUC are small, single tumors, within Milan criteria, BCLC 0/A and therefore amenable to curative therapies which led to excellent 5- year survival rates. 3
132 P06-YI HCC PROGRESSION AND SURVIVAL FOLLOWING HCV ANTI-VIRAL THERAPY Jibran Mecci, Polychronis Kemos, Jennifer Benselin 2, Sarah Mcdonald 3, Philip Johnson 4, Graham Foster, William Irving 2 Blizard Institute, United Kingdom, 2 Queen's Medical Centre, United Kingdom, 3 HCV Research UK Biobank, MRC-University of Glasgow Centre for Virus Research, Glasgow, United Kingdom, 4 University of Liverpool, United Kingdom Background and Aims: Hepatitis C virus (HCV) in cirrhotic patients is now readily treatable but controversy remains over hepatocellular carcinoma (HCC) occurrence and cancer progression following this. We studied patients who achieved viraemic control with those with ongoing viraemia, to evaluate the effects on HCC progression and survival. Method: All cases of HCC in patients with advanced cirrhosis within the UK early access program were reviewed. We compared patients who had cleared virus with DAA treatment to patients who remained viraemic, composed of DAA failures, interferon (IFN) failures and untreated patients. Cross-sectional imaging and multidisciplinary team reports were reviewed to ascertain date of HCC diagnosis and date of first progression by RECIST criteria. Patients were censored after liver transplant, initiation of palliative care including sorafenib or death. Kaplan-Meier analysis and log rank test for comparison were performed. Results: 2 cases of HCC were reviewed with 55 achieving SVR. There were 57 viraemics (28 DAA exposed, 5 untreated, 4 IFN exposed), characteristics shown in Table. All had a history of active or past decompensation and no previous HCC. Median follow up was 0.8 (5.2-8.) months following HCC diagnosis and maximum 32 months. There was no difference in mortality or time to death = 4/55 non-viraemic and 28/57 viraemic deaths respectively with an average of 5.44 and 5.2 months from diagnosis to death. For progression, reports on 78 patients were available, 35 non-viraemic and 43 viraemics. Baseline tumour burden (cm) was <2=2, <3=0 and multifocal=3 in non-viraemics and <2=6, <3= and multifocal=26 in viraemics. Of these, 26 (74%) and 39 (90%) showed tumour progression respectively. There was no difference in time to first HCC progression ( ) months in non-viraemic cases and 4.07 ( ) months in viraemics. Conclusion: From our national retrospective case control study, we find no supporting evidence that achieving viraemic control affects HCC progression. However, we found indications of possible effect on survival but were unable to verify possibly because a higher power study is required. 32
133 Non-Viraemic (%) Viraemic (%) Total (2) 55 (49) 57 (5) Age (average) Males 42 (76) 44 (77) Died 4 (25) 28 (49) Transplant 8 (33) 6 (28) Childs-Pugh A 4 (25) 23 (40) Childs-Pugh B 35 (64) 28 (49) Genotype 3 (56) 6 (28) Genotype 3 22 (40) 36 (63) Age at death (avg.) Duration from DAA treatment to cancer (months) Duration from cancer to death (months) 9.67 ( ) N/A 5.44 (2.-8.4) 5.2 (2.7-.7) Figure: P =

134 P06-2YI CONTRAST ENHANCED VERSUS CONVENTIONAL ULTRASOUND GUIDED LIVER BIOPSY IN THE DIAGNOSIS OF HEPATOCELLULAR CARCINOMA : A PROSPECTIVE STUDY Tudor Mocan, Pompilia Radu, Teodor Zaharia, Cristina Cebotaru 2, Gabriel Kacso 3, Nadim Al Hajjar 4, Zeno Sparchez 5 Institute for Gastroenterology and Hepatology, 2, Oncological Department, 3 Oncological Department, 4 University of Medicine and Pharmacy, Cluj Napoca, Romania, 5 Institute for Gastroenterology and Hepatology, University of Medicine and Pharmacy, Cluj Napoca, Romania Background and Aims: Hepatocellular carcinoma (HCC) is the only major cancer in which diagnosis is not regularly established by histology. However, there are several circumstances were liver biopsy is recommended. Unfortunately, the sensitivity of ultrasound guided liver biopsy (USLB) is less than 80% and a negative biopsy does not rule out malignancy. Contrast enhanced ultrasound (CEUS) is an excellent method for both diagnostic and intervention procedures. The aim of this study was to evaluate the diagnostic accuracy of CEUS guided liver biopsy (CEUSLB) versus USLB in cirrhotic patients with focal liver lesions (FLL). Method: A total number of 52 cirrhotic patients with either inconclusive FLL on CT or candidates for Sorafenib therapy were evaluated for inclusion in the study. Eight patients refused to sign the informed consent. The remaining 44 patients were randomly divided into two groups: a group who underwent CEUSLB (79 patients, 49 lesions) and another who underwent USLB (65 patients, 22 lesions). The pathologic diagnosis was considered definitive if the biopsy result was malignant. If the initial biopsy result was benign or negative for malignancy, then the result was either confirmed or denied on the basis of CT, MRI, or clinical follow-up over a period of 6-2 months. Results: In the CEUSLB group 96.2% of the lesions were malignant (55 HCC, 5 cholangiocarcinoma and 2 metastasis) compared to 96.9% (56 HCC, 5 cholangiocarcinoma, lymphoma and metastasis) in the USLB group (p > 0.05). There were no differences in tumor size between the two groups: mm in USLB compared to mm in the CEUSLB (p = 0.38). The diagnostic accuracy was significantly higher in CEUSLB group than in the USLB group (94.93% vs 73.38%, respectively; p < 0.00). On subgroup analysis the sensitivity of CEUSLB compared to USLB was higher for both poorly visible tumors (92% vs 64%; respectively; p = 0.006) and tumors larger than 5 cm (95% vs 74%; respectively; p = 0.0). No major complications occurred in our study except one case of hemoperitoneum in the USLB group. Conclusion: The use of contrast agents in guiding liver biopsy improved the diagnostic accuracy of the procedure especially in poorly visible tumors and large tumors by providing important intralesional information for differentiating viable, denaturalized, or necrotic tissue Figure: 34
135 P07-0YI DEPLETION OF ACTIVATED STROMAL FIBROBLASTS IN LIVER FIBROSIS - A PROMISING APPROACH TO PREVENT LIVER CANCER? Anja Moncsek, Weber Achim 2, Beat Müllhaupt 3, Joachim C. Mertens 3 University Zürich c/o University Hospital Zürich, Gastroenterology and Hepatology, Zürich, Switzerland, 2 University Hospital, Pathology and Molecular Pathology, Zürich, Switzerland, 3 University Hospital, Gastroenterology and Hepatology, Zürich, Switzerland Background and Aims: Activated stromal fibroblasts (ASF) are the main stromal cell population in liver fibrosis and desmoplastic liver cancers and have been implicated in the development of these liver diseases. Persistent activation of fibroblasts is a key feature in chronic fibrotic diseases such as primary sclerosing cholangitis (PSC). Advanced liver fibrosis is a known risk factor for tumor development. The activated fibroblast phenotype is linked to an increased apoptotic sensitivity. The mechanism behind this apoptotic priming seems to be an alteration of apoptosis regulating Bcl-2 proteins. We have demonstrated in vitro that activated fibroblasts derived from CCA are sensitive to navitoclax, a proapoptotic inhibitor of anti-apoptotic Bcl-2 proteins. Moreover, navitoclax treatment leads to the depletion of ASF, and a reduction of tumor size and metastasis in a syngeneic rat model of CCA (Mertens et al., Cancer Res 203). We hypothesize that activated fibroblasts in chronic liver fibrosis share key features with cancer-derived fibroblasts, are similarly primed for apoptosis and can also be targeted with proapoptotic BH3 mimetics. Method: For in vitro studies, human and mouse fibroblasts were treated with platelet derived growth factor (PDGF) to induce fibroblast activation. Alterations of the Bcl-2 family were assessed with qpcr and Western blot. PDGF-activated fibroblasts were treated with BH3 mimetics specific for Mcl-, Bcl-2 and Bcl-xL. Induction of apoptosis was examined biochemically by caspase-3/7 activity and morphologically using DAPI staining for apoptotic nuclei. To investigate the anti-fibrotic potential in vivo, we treated Mdr2 -/- mice with the selective Bcl-xL inhibitor A for two weeks by daily oral gavage. Liver fibrosis was assessed by morphometric analysis of Sirius red staining and quantification of hydroxyproline. Results: Our data indicate that a) the survival of activated fibroblasts is Bcl-xL-dependent, and b) specific inhibition of Bcl-xL by the BH3 mimetic A ameliorates biliary fibrosis in Mdr2 -/- mice. In vitro activated fibroblasts demonstrated a reduction of anti-apoptotic Bcl-2. Therefore, the survival of activated fibroblasts became more dependent on another pro-survival factor such as Bcl-xL. Treatment of Mdr2 -/- mice, a mouse model for PSC, with the BH3 mimetic A resulted in a significant reduction of liver fibrosis. Conclusion: Inhibition of Bcl-xL induces apoptosis in activated fibroblasts in vitro and reduces fibrosis in vivo. This indicates that activated fibroblasts from PSC and CCA can be similarly targeted. We therefore propose that targeting ASF at the level of fibrosis with Bcl-xL inhibitors may prevent liver cancer development. 35

136 P07-02YI SPHINGOLIPIDS: A FURTHER STEP INTO THE DETECTION OF EARLY AND ADVANCED HEPATOCELLULAR CARCINOMA Iuliana Nenu, Andreea-Bianca Ardelean, Cristina-Nelida Bora, Andrei Otto Mitre, Sorana Pascalau, Horia Stefanescu, Bogdan Procopet 2, Carmen Socaciu 3, Zeno Sparchez 2, Marcel Tantau 2, Mircea Grigorescu 2 Regional Institute of Gastroenterology and Hepatology Octavian Fodor, Cluj-Napoca, Romania, 2 "Iuliu Hatieganu" University of Medicine and Pharmacy, Cluj-Napoca, Romania, 3 Center for Applied Biotechnology BIODIATECH, SC Proplanta, Cluj-Napoca, Romania Background and Aims: Throughout the last years metabolomics has played an important role in providing new insights into the detection and progression of hepatocellular carcinoma (HCC). Sphingolipids, a family of membrane lipids, are involved in numerous cell functions, including cell death pathways and have an altered expression in many types of cancer. The aim of the study was to identify a metabolomic biomarker for HCC diagnosis and to compare its diagnostic accuracy with alpha fetoprotein (AFP). Method: 04 patients (54 HCC BCLC stages 0, A and B developed on compensated cirrhosis and 50 compensated cirrhotic controls) were included. Common workup for the assessment of liver disease and AFP was carried out in each patient. High pressure liquid chromatography (HPLC) coupled with quadruple time of flight electrospray in a positive ionization mode mass spectrometry (QTOF-ESI+-MS) was performed from serum samples of each patient. MetaboAnalysis, performing univariate and multivariate statistical analysis was used to identify candidate biomarkers. Their performance for detection of early/intermediate HCC was evaluated using semi-quantitative assessment and through a leave-one-out cross-validation based on area under the receiver operating characteristics (ROC) curve. Results: 5 metabolites were identified. Sphingolipids are the most upregulated in HCC patients, particularly C6 sphinganine (C6-SPH) (p <0.00 vs. compensated cirrhosis). The expression of C6- SPH was times higher in HCC than in cirrhotic controls (p<0.005). The area under the curve (AUC) of C6-SPH for the diagnosis of HCC was significantly higher compared to AFP [0.969 (95%CI, ) vs (95%CI, ), p (delong test) <0.00]. For a cutoff value of 0.737, C6-SPH correctly classified 97/04 (93.26%) of patients. Conclusion: Sphingolipids show a significant upregulation in patients with HCC compared to patients with cirrhosis. Of them, C6-SPH might stand as a novel diagnostic marker for the identification of early and intermediate HCC in patients with chronic liver diseases. Figure: 36
137 P07-03YI THE ROLE OF INTERLEUKIN 6 SIGNALING PATHWAY IN CHOLANGIOCARCINOMA Thi Mai Ly Nguyen, Khac Cuong Bui, Tim Scholta, Jun Xing, Vikas Bhuria, Thirumalaisamy P. Velavan 2, Linh Toan Nguyen 3, Huu Song Le 4, Przemyslaw Bozko, Ruben Plentz 5 Medical University Hospital, Department of Internal Medicine I, Tuebingen, Germany, 2 Medical University Hospital, Institut für Tropenmedizin Tübingen, Tuebingen, Germany, 3 Vietnam Military Medical University, Department of Pathophysiology, Hanoi, Viet Nam, 4 08 Military Central Hospital, Faculty of Infectious and Tropical Diseases, Hanoi, Viet Nam, 5 Klinikum Bremen Nord, Innere Medizin II (Gastroenterologie, Onkologie und Diabetologie), Bremen, Germany Background and Aims: Cholangiocarcinoma (CC) is the second common hepatic malignancy. Combination of Gemcitabine and Cisplastin is currently the first line treatment for inoperable patients. However, new molecular therapies are needed. Interleukin 6 (IL-6) is an anti-inflammation cytokine that operates survival in various non-solid cancers: lymphoma, myeloma, leukemia... but the anti-cancer effect of IL-6 inhibitor on CC is not totally known yet. The aims of this project are to analyze the role of IL-6 during cholangiocarcinogenesis and the effect of Siltuximab, an IL-6 antibody in vitro, in vivo. Method: Extra- (TFK) and intra-hepatic CC (SZ) cell lines were treated with different concentrations of Siltuximab, followed by observation on invasion (2D and 3D culture models), senescence and signalling transformation. Western Blot targeting p.stat3, EMT markers, p.akt, Wnt/β-Catenin was performed. RT-qPCR was applied to compare IL-6 mrna expression in CC tumours and normal livers of CC engineered mice (Alb-Cre/LSL- KRAS G2D /p53 L/L, n=7). Xenograft mice were used to investigate anti-cancer effect of Siltuximab in vivo. Results: Siltuximab treatment resulted in deceleration of 2D and 3D cell invasion, IL-6 mrna and acceleration senescence. Siltuximab led to down-regulation of p.stat3, Wnt/β-Catenin, EMT markers and up-regulation of p.akt. On engineered mice, the expression of IL-6 mrna in tumour tissues was significantly higher than that in adjacent normal livers. The level of mrna IL-6 in tumours was correlated with tumour volume. On the xenograft model, Siltuximab-treated mice showed smaller tumours than control animals. Conclusion: IL-6 plays important role in cholangiocarcinogenesis and Siltuximab might become a promising therapy for CC. 37
138 P07-04YI LIVER CANCER CELL LINES DISTINCTLY REFLECT THE METABOLIC GENE EXPRESSION PATTERN OBSERVED IN CLINICAL MICROARRAYS Zeribe Nwosu, Weronika Pioronska, Christoph Meyer, Dominik Megger 2 3, Steven Dooley Medical Faculty Mannheim, University of Heidelberg, Dept. of Medicine II, Molecular Hepatology Section, Germany, 2 Medizinisches Proteom-Center, Ruhr-Universität Bochum, Department of Clinical Proteomics, Germany, 3 Institute of Virology, University Hospital, University Duisburg-Essen, Germany Background and Aims: Cell lines are useful models for the mechanistic study of cancer features, e.g. metabolic alterations. However, there is a knowledge gap on the extent to which hepatocellular carcinoma (HCC) cell lines reflect the molecular features of clinical tumours. Here, we examined how consistently altered metabolic genes in clinical HCC are expressed in cell lines with contrasting cancer phenotypes (e.g. proliferation and migration). Method: We compared gene expression in well-differentiated, more hepatocyte-like cells (HUH7, HEPG2) versus poorly-differentiated cell lines (SKHEP, HLF and HLE) using publicly available microarray dataset. The significantly expressed genes were used for pathway annotation analysis. We further compared how 634 metabolic genes we reported to be consistently deregulated in clinical HCC are expressed in HUH7 versus HLE cell lines. We validated selected genes by qpcr, and also analysed protein level expression by mass spectrometry. Results: Functional annotation showed that poorly differentiated HCC cell lines substantially reflect pathway alterations observed in clinical microarrays, e.g. upregulation of MAPK and Ras signaling, and the downregulation of amino acid metabolic pathways. Similarly, several metabolic targets downregulated in clinical HCC (e.g. ARG, ASL in urea cycle and GLUD, PHGDH, PSAT, SHMT2, GLDC in amino acid metabolism) emerged as lowly expressed in HLE cells at gene and protein level. However, the expression of some metabolic targets did not correlate with oncogenic features in the cell lines. Specifically, despite having less aggressive features, HUH7 cells displayed a higher expression of notable metabolic targets that are upregulated in clinical HCC (e.g. HK2, PSPH, ASNS, FASN, ACLY). Conclusion: Our findings could assist in further identification of metabolic targets that are core drivers of hepatocellular carcinogenesis or instead are likely more relevant as biomarkers for tumour grading. 38
139 P07-05YI GENETIC INACTIVATION OF NRF2 PREVENTS CLONAL EXPANSION OF CARCINOGEN-INITIATED CELLS IN A NUTRITIONAL MODEL OF RAT HEPATOCARCINOGENESIS Claudia Orrú, Marta Szydlowska, Keiko Taguchi 2, Patrizia Zavattari, Andrea Perra, Masayuki Yamamoto 2, Amedeo Columbano University of Cagliari, Biomedical Sciences, Cagliari, Italy, 2 Tohoku University, Medical Biochemistry, Sendai, Japan Background and Aims: Dysregulation of the Keap-Nrf2 pathway has been observed in experimental and human tumors, suggesting possible roles of the pathway in cancer development. Here we examined whether Nrf2 activation occurs at early steps of rat hepatocarcinogenesis, to assess critical contributions of Nrf2 to the onset of hepatocellular carcinoma (HCC). Method: We used wild type (WT) and Nrf2 knockout (Nrf2 KO) rats treated with a single injection of diethylnitrosamine (DENA) followed by choline-devoid methionine-deficient (CMD) diet. This experimental model causes massive fatty liver and steatohepatitis with fibrosis and allows to identify early stages of hepatocarcinogenesis. Results: We found that Nrf2 activation takes place already in early preneoplastic lesions identified by the marker glutathione S-transferase placental form (GSTP). Nrf2 missense mutations, known to disrupt the Keap-Nrf2 binding, were present in 44% of GSTP-positive foci. Nrf2 KO rats were used to directly investigate whether Nrf2 is critical for initiation and/or clonal expansion of DENA-damaged hepatocytes. While Nrf2 genetic inactivation did not alter DENA-induced initiation, it led to increased liver injury and chronic compensatory hepatocyte regeneration when rats were fed CMD diet. However, in spite of such a permissive environment, the livers of Nrf2 KO rats did not display any preneoplastic lesion unlike those of WT rats. Conclusion: These results demonstrate that, in a model of hepatocarcinogenesis resembling human non-alcoholic fatty liver disease: i) Nrf2 is activated at early steps of the tumorigenic process and ii) Nrf2 is mandatory for the clonal expansion of initiated cells, indicating that Nrf2 is critical for the onset of HCC. 39
140 P07-06YI ACTIVATED PLATELETS CONTRIBUTE TO THE PROGRESSION OF HEPATOCELLULAR CARCINOMA BY ALTERING THE IMMUNE CELL ENVIRONMENT Natasa Pavlovic, Femke Heindryckx, Linus Edlund, Pär Gerwins 2 Uppsala University, Medical Cell Biology, Uppsala, Sweden, 2 Akademiska sjukhuset, Surgical Sciences, Radiology, Uppsala, Sweden Background and Aims: The inflammatory process plays a critical role in the complex molecular pathogenesis of hepatocellular carcinoma (HCC). Macrophages are a key part of the inflammatory environment, and their role in tumour progression is determined by their state of activation, which can be classified as anti-tumoural (M) and pro-tumoural (M2). Platelets have been reported to interact with different cell types in the tumour microenvironment, including macrophages and Kupffer cells. This study aimed to identify the effect of platelets on the inflammatory cell population and HCC development, as well as to determine whether anti-platelet therapy can decrease the progression of HCC. Method: Mice were injected weekly with diethylnitrosamine to induce HCC. From week 0, mice were treated with anti-platelet drug Clopidogrel or control, samples were taken for RNA-analysis and histology after 25 weeks. Tumour burden and collagen deposition was quantified on H&E and Sirius red staining, respectively. Platelets and macrophages were quantified by immunohistochemical stainings with CD4 and F4/80 antibodies, respectively. For in vitro experiments, fluorescently labelled HCC-cells (HepG2) and differentiated macrophages (PMA-treated THP-cells) were co-cultured with platelets isolated from healthy donors. Results: Blocking platelet activation with Clopidogrel significantly decreased tumour burden in vivo, compared to untreated controls. mrna analysis confirmed a decreased expression of PCNA in Clopidogrel-treated mice with HCC, suggesting a decrease in proliferation. CD4 immunohistochemistry revealed that treatment with Clopidogrel significantly decreased the number of infiltrated platelets in the liver of mice with HCC. Anti-platelet therapy also significantly decreased collagen deposition in mice. Clopidogrel treatment led to a significant decrease in the total number of F4/80-positive macrophages, while it increased mrna expression of several anti-tumoral M macrophage activation markers (TNFa, IL-, CD40, Fpr2) and decreased M2-marker Arginase- expression. In vitro experiments showed THP- differentiated macrophages phagocytose HepG2-cells and that adding platelets to a co-culture of macrophages and tumor cells significantly decreased the macrophage s capacity to phagocytose tumour cells. Immunocytochemical analysis showed that co-culturing platelets with THP- differentiated macrophages significantly decreased the M marker HLA-DR protein expression in macrophages. Conclusion: These findings suggest that platelets play an important role in creating a pro-tumoural inflammatory environment and thereby facilitate HCC progression. The use of anti-platelet drugs may therefore be therapeutically relevant for patients with HCC. 40
141 P07-07 THE COMBINATION OF PIVKA-II AND AFP LEVELS IMPROVES THE DIAGNOSTIC ACCURACY FOR THE DIAGNOSIS OF HCC DEVELOPING IN LONG-TERM NUC SUPPRESSED HBV CAUCASIAN CIRRHOTICS Alessandro Loglio, Massimo Iavarone, Floriana Facchetti, Glenda Grossi, Enrico Galmozzi, Riccardo Perbellini, Giovanna Lunghi 2, Claudio Galli 3, Maria Teresa Sandri 4, Angelo Sangiovanni, Pietro Lampertico Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Università degli Studi di Milano, CRC A.M. and A. Migliavacca for Liver Disease, Division of Gastroenterology and Hepatology, Milano, Italy, 2 Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, University of Milan, Microbiology and Virology Unit, Milano, Italy, 3 Abbott Diagnostics, Medical Scientific Liaison Europe, Roma, Italy, 4 European Institute of Oncology, Laboratory Medicine Division, Milano, Italy Background and Aims: Protein Induced by Vitamin K Absence or Antagonist-II (PIVKA-II) has been suggested as a possible serum biomarker for HCC, but its diagnostic accuracy and ability to predict survival in long-term nucleos(t)ide analogs (NUCs) treated Caucasian cirrhotics have not been explored yet. Method: This cross-sectional single center cohort study was conducted in two groups: 59 consecutive NUC suppressed cirrhotic patients with HCC (HCC group) and 07 HBV NUC suppressed cirrhotic patients (control group) who remained HCC-free for 75 (60-9) additional months after serum collection. Patients in anticoagulant therapy were excluded. Alpha-fetoprotein (AFP) levels were tested by standard techniques while PIVKA-II levels were determined by a CMIA Immunoassay (Abbott; limit of quantification: 8.2 mau/ml). Results: The HCC and control groups had similar clinical and virological features. Most were male (78%), older than 60 years (66%), HBeAg negative (98%), with normal ALT levels (95%), undetectable HBV DNA (00%), and treated with ETV or TDF (86%). Both PIVKA-II and AFP levels significantly differed (p<0.00) between HCC and control group: 09 (7-2.57) vs 30 (3-82) mau/ml and 5 (-.63) vs 2 (-4) ng/ml, respectively. As none of control group patients had PIVKA >82 mau/ml, this level was used as the upper limit of normal for the analysis. While AFP >7 ng/ml had 42% sensitivity and 00% specificity (AUROC 0.7, ) in detecting HCC, PIVKA-II >82 mau/ml had 54% and 00% (AUROC 0.77, ), respectively, with 00% positive (PPV) and 80% negative (NPV) predictive values. Among HCC, AFP was the only positive marker in 4%, PIVKA in 25%, both were positive in 29%, both were negative in 32% and at least one positive in 68%. PIVKA-II >82 mau/ml could identify 25% of AFP-negative HCC, and was associated with lesions >20 mm diameter (OR 4.6, p=0.007) but not with neoplastic thrombosis nor multifocal HCC. During 40 (2-44) months of follow-up, 2 (20%) patients died of HCC progression. AFP >7 ng/ml (HR 3.7, 95% Confidence Interval -3, p=0.045) and neoplastic thrombosis (HR 2., 95% CI.9-76, p=0.008) but not PIVKA-II >82 mau/ml (HR.5, 95% CI 0.5-5, p=0.489) were associated with HCC-related mortality. Conclusion: The combination of PIVKA-II and AFP levels increases the diagnostic accuracy of HCCs developing in NUC suppressed compensated Caucasian cirrhotics with HBV. 4
142 P07-08YI NEW INSIGHTS IN TRANSFORMING GROWTH FACTOR BETA SIGNALING PATHWAY ON TUMOR SUPPRESSION AND METASTATIC PROPERTIES IN PRIMARY LIVER CANCER Sharon Pereira, Luis Rodrigues, Darko Castven, Nadja M.Meindl-Beinker 2, Dennis Strand 3, Hauke Lang 4, Steven Dooley 2, Peter Grimminger, Peter Galle, Jens Marquardt, Frederike L Mahn University of Mainz, Department of Medicine I, Lichtenberg Research Group, Mainz, Germany, 2 Molecular Hepatology- Alcohol-Associated Diseases,, Department of Medicine II. Medizinische Klinik Gastroenterologie, Hepatologie, Infektiologie, Mannheim, Germany, 3 University of Mainz, Department of Medicine I, Mainz, Germany, 4 University of Mainz, Department of Surgery, Mainz, Germany Background and Aims: Transforming Growth Factor Beta (TGF-beta) belongs to a superfamily of cytokines that induces pleiotropic effects on different processes and cell types in the liver. During cancer progression while TGF-beta signaling exerts tumor suppressor effects at pre-neoplastic and early tumor stages, cytostatic effects of TGF-beta are often lost in progressed stages due to (epi-) genetic disruption of several members of the signaling pathway. This progressed stage is characterized by activation of a late TGF-beta signature which promotes the phenotypic switch from tumor suppressor to promoter of cancer. Consequently, cancer cells display an epithelial-mesenchymal-transition (EMT) phenotype by acquiring pro-metastatic properties. Method: Newly generated primary (HCC & CCA) and established cell lines (PLC & HuCCT-) were exposed to TGF-β and TGF-β2 (ng/ml) for 72 hr. NGS Analysis was performed to identify significant differences in gene expression patterns. Appropriate statistical and bioinformatics tools (IPA) was used to study pathways and networks to understand how they these genes interact biologically. The effect of TGF-β on tumor-initiating potential was determined by colony and sphere formation assays. Invasive and migratory properties were determined using the wound healing assay and the Boyden chamber assay. Results: Treatment with TGF-β and TGF-β2 led to a significant reduction in colony and spheroid forming ability in all investigated cell lines. Consistent with the reduced in vitro tumorigenicity and spherogenicity, a drastic effect of TGF- β on the putative tumor-initiating cell population was observed, reflected by the downregulation of stemness markers CD33 and EpCAM. Interestingly, treatment with TGF-β led to a significant increase in the expression of CD44 accompanied by the activation of established epithelial-mesenchymal-transition (EMT) transition markers. Accordingly, a significant downregulation of E-Cadherin paralleled by upregulation in SNAIL transcription factor was seen. Consequently, enhanced migratory and invasive properties of HCC and CCA were observed evidenced by increased wound healing and invasion. In addition, pathways enriched with differentially expressed genes known to be involved in EMT (P3K, WNT/β-Catenin pathway) were identified by NGS analysis. Conclusion: In conclusion, we here confirm the cytostatic effect of TGF- β and TGF- β2 by reducing the frequency of cancer cells in both HCC and icca. Further, TFG-β seems to be an important regulator in progressed PLCs. These context-dependent dichotomic effects should be considered in TGF-β based therapeutic approaches. We would further validate the obtained findings in vivo using a battery of different xenotransplantation models representing the observed in vitro findings. 42
 is one of the")
")
143 P07-09 IN VIVO REACTIVATION OF THYROID HORMONE NUCLEAR RECEPTORS BY 3,5,3' TRIIODOTHYRONINE HAS A THERAPEUTIC POTENTIAL IN HEPATOCELLULAR CARCINOMA Andrea Perra, Marta Anna Kowalik, Elisabetta Puliga, Pia Sulas, Giovanna Maria Ledda- Columbano, Amedeo Columbano Università degli Studi di Cagliari, Biosciences, Cagliari, Italy Background and Aims: Hepatocellular carcinoma (HCC) is one of the leading cause of cancer-related deaths worldwide. The reasons for this lethality are the absence of a reliable marker for early diagnosis and the lack of an effective therapeutic strategy. Our previous studies demonstrated that while hepatic preneoplastic lesions and advanced HCCs, induced in rats, display an intracellular hypothyroidism, administration of 3,5,3 -triiodothyronine (T3) was able to induce regression of hepatic preneoplastic nodules and inhibit the carcinogenic process. The potential utility of this therapeutic approach has been reinforced by some evidence of a permissive role of hypothyroidism in HCC progression in humans and by the finding that human HCCs display a reduced expression of the thyroid hormone receptor beta (THRβ). Based on these observations, we investigated the molecular mechanism underlying the inhibitory effect of T3 on carcinogenic process, and whether also fully developed HCCs could respond to the anti-tumorigenic and pro-differentiating effects of T3 Method: F-344 rats were subjected to a model of hepatocarcinogenesis, consisting of a single dose of the carcinogen diethylnitrosamine (DENA) and a 2-week exposure to a promoting regime. Ten weeks after initiation, animals were divided into 2 groups. The first was maintained in basal diet, while the second group was fed a T3-supplemented diet (T3-diet) and the rats were killed 2 4 or 7 days after. Gene expression analysis was done on the Laser-microdissected preneoplastic lesions. At 0 months, other 2 groups of rats exposed to the R-H protocol was either fed normal diet or the T3-diet (one/every 3 weeks). Rats were sacrificed after or 5 cycles of treatment Results: Transcriptomic analysis showed that a short treatment with T3 caused a shift of the global expression profile of aggressive preneoplastic nodules, towards that of normal liver. This reprogramming preceded the disappearance of the nodules and involved genes responsible for hepatocyte differentiation (Klf-9, Hnf4a, Hnfa and Bmp4), antioxidant response (Nrf2) and PPP activation (G6PDH). Moreover, the expression of these transcription factors was found to be up-regulated also in early HCCs after T3 treatment, reinforcing the hypothesis re-activation of the THR-T3 axis may induce differentiation of neoplastic cells towards a more benign phenotype. Finally, T3 treatment for 5 cycles induced the regression of fully developed HCC Conclusion: Collectively, these findings suggest that T3 may act as a potent anti-tumoral agent and that thyroid hormones or its analogues, particularly agonists of the TRβ isoform, can represent useful tools in HCC therapy Figure: A) Gene expression profile in control livers and preneoplastic lesions from rats treated for 2 and 4 days with T3. B) Treatment of HCC bearing rats with the T3-diet for 5 cycles resulted in the regression of most neoplastic lesions 43

144 P07-0 COST-EFFECTIVE TARGETED SEQUENCING FOR HEPATOCELLULAR CARCINOMA MUTATIONAL SCREENING Viola Paradiso, Andrea Garofoli, Nadia Tosti, Manuela Lanzafame, Valeria Perrina, Luca Quagliata, Matthias Matter, Stefan Wieland 2, Markus Heim 2, Salvatore Piscuoglio, Charlotte Ng, Luigi Maria Terracciano University Hospital Basel, Institute of Pathology, Basel / Basel, Switzerland, 2 University of Basel, Department of Biomedicine, Basel, Switzerland Background and Aims: Commercially available targeted or exome panels miss some genes and regions frequently mutated in hepatocellular carcinoma (HCC). We aim to design and benchmark a targeted sequencing panel specific for mutational profiling for HCC. Method: We designed a custom Ion AmpliSeq panel targeting all exons of 33 protein-coding and 2 long non-coding RNA genes frequently mutated in HCC, TERT promoter. We profiled DNA from fresh frozen tumor (FFT, n=0, median depth 495x) and/or formalin-fixed paraffin-embedded (FFPE) tumor with low input DNA (n=36, median depth 530x), and their non-tumoral counterparts from 39 HCCs using the custom panel. We benchmarked the somatic mutations identified against those from Illumina wholeexome sequencing (WES) of the equivalent FFT samples (median depth 2x). Results: At least one somatic mutation was identified in 35/39 cases using the custom panel. Median of 2.5 (0-74) and 3 (0-76) mutations were identified in FFT and FFPE samples, respectively. 98% (6/62) of the mutations identified from WES of the 0 FFT samples were successfully recovered using the custom panel, with the identification of an additional 6 and 32 mutations in coding and non-coding regions, respectively. Similarly, all 04 mutations identified from WES were also found based on the analysis of our custom panel of the 36 FFPE biopsies. We identified an additional 8 and 70 somatic mutations in coding and noncoding genes, respectively, using our custom panel, including 2 CTNNB activating mutations. Conclusion: We have established a sequencing assay for the sensitive detection of somatic mutations in HCC-associated driver genes. Figure: 44
145 P07-YI INCREASED INTESTINAL PERMEABILITY AND INFLAMMATION ARE ASSOCIATED WITH HEPATOCELLULAR CARCINOMA IN PATIENTS WITH NAFLD-RELATED LIVER CIRRHOSIS Francesca Ponziani, Sherrie Bhoori 2, Valentina Petito, Francesco Paroni Sterbini 3, Daniele Morelli 4, Teresa De Michele 5, Maurizio Sanguinetti 3, Antonio Gasbarrini, Maurizio Pompili, Vincenzo Mazzaferro 2 Fondazione Policlinico Universitario Agostino Gemelli, Internal Medicine, Gastroenterology, Hepatology, Roma, Italy, 2 Istituto Nazionale dei Tumori, Hepatobiliary and Liver Transplant Surgery, Milano, Italy, 3 Fondazione Policlinico Universitario Agostino Gemelli, Microbiology, Roma, Italy, 4 Istituto Nazionale dei Tumori, Biochemistry and Microbiology, Milano, Italy, 5 Fondazione Policlinico Universitario Agostino Gemelli, Biochemistry, Roma, Italy Background and Aims: Increased intestinal permeability (IP) is common in patients with cirrhosis. Leaky gut is associated with the translocation of microbial products and fragments and this process is involved in the pathogenesis of NAFLD. The aim of this study is to investigate if intestinal permeability and inflammation are associated with HCC in NAFLD patients. Method: 2 Cirrhotic patients with NAFLD and HCC, 33 liver cirrhotic patients (20 with NAFLD and 3 with chronic hepatitis C) comparable for age, liver function and portal hypertension and 20 age-matched healthy controls were included in the study. Quantification of zonulin- (ZO) and lipopolysaccharide (LPS), as indices of IP, and fecal calprotectin as marker of intestinal inflammation were performed using ELISA and the Liaison analyzer. Subjects affected by gastrointestinal or systemic diseases potentially affecting IP and those with documented alcohol intake during the last year or who had taken antibiotics during the last 6 months were excluded from the study. Results: IP was increased in patients with liver cirrhosis who had higher serum levels of ZO and LPS compared to controls (ZO:.33 (.93) vs IQR 2.4 ng/ml p <0.000; LPS 3.7 IQR 3.0 vs 2.52 IQR 2.4 EU/mL p=0.02; Figure ). There was no significant difference between cirrhotic patients with HCC and those without HCC (ZO:.35 IQR.6 vs.23 IQR ng/ml p=0.993; LPS 2.82 IQR 2.82 IQR 2.2 p=0.974 EU/mL Figure ). Fecal calprotectin levels were increased in cirrhotic patients with and without HCC compared to controls (75.65 IQR vs 0.35 IQR 9.2 mcg/g p<0.000 Figure ). Within the cirrhosis group, patients with HCC showed higher calprotectin levels than patients without HCC (457 IQR 603 vs IQR 85 mcg/g, p<0.005 Figure ). Conclusion: IP is increased in cirrhotic patients with and without HCC, but the latter also show higher fecal calprotectin. This could be related to a higher intestinal inflammatory status, which may contribute to exacerbate the inflammatory liver injury contributing to the development of neoplastic lesions in cirrhotic NAFLD patients. 45
146 Figure : 46
147 P07-2 LINC0052 MAY FUNCTION AS A CERNA CORE COMPONENT IN HUMAN HEPATOCELLULAR CARCINOMA Rosella Pellegrino 2, Fabio Ticconi 3, Britta Skawran 4, Mirco Castoldi 5, Ariane Neumann, Federico Pinna, Peter Schirmacher, Ivan Costa 3, Thomas Longerich 2 Institute of Pathology, University Hospital Heidelberg, Germany, 2 Institute of Pathology, University Hospital RWTH Aachen, Germany, 3 Computational Biolology, IZKF Aachen and Helmholtz Institute for Biomedical Engineering, Centre of Medical Technology, Aachen, Germany, 4 Institute of Human Genetics, Hannover Medical School, Hannover, Germany, 5 Department of Gastroenterology, Hepatology and Infectious Diseases, Heinrich Heine University, Düsseldorf, Germany Background and Aims: Recent studies have shown the potential role of long non-coding RNAs (LincRNAs) in cancer by affecting different cellular processes. Using methylome analysis and integrative profiling of human hepatocellular carcinoma (HCC) we observed a significant hypomethylation of the LincRNA 52 (LINC0052) promoter in human HCCs compared to normal liver tissues, leading to LINC0052 overexpression in the tumor tissues. Recently, LINC0052 has been identified as competing endogenous RNA (cerna) in gastric cancer. Therefore we hypothesized that LINC0052 may function as sponge for mirnas, in turn modulating the expression of mirna target genes in human HCC. Method: Potential LINC0052 binding mirnas were identified using mircode ( and their expression levels were determined by array analysis of human HCC samples. Furthermore, the potential mirna target genes of a LINC0052-mediated cerna network were defined by a metaapproach ( and only those candidates predicted by at least two independent algorithms were selected ( An integrative analysis was performed by evaluating the correlation of mirna targets and LINC0052 expression in our human HCC cohort as well as the representative TGCA datasets. Additionally, Ago2-RNA IP was used to investigate whether LINC0052 interacts with mirnas in vitro. For experimental validation LINC0052 knockout HuH7 cells were established by CRISPR/Cas9 technology. Results: In silico analysis revealed that the LINC0052 splice variant 3, the most abundantly expressed in human HCC, contains binding sites for 24 mirna members, from which 22 mirnas was detectable in our human HCC cohort. The potential LINC0052-mediated cerna network contained 2664 genes in total. The integrative analysis identified mir.23a.3p, mir.25a.5p mir.25b.5p, mir.223.3p and mir.43.3p as top candidates, potentially affecting the expression of STK39, FAM60A, FUT4, PALLD, and MAP3K. Moreover, the expression of these target genes was significantly decreased in LINC0052 deficient cells when compared to the corresponding controls. Finally, LINC0052 was shown to be part of ribonucleoprotein complexes. Conclusion: Our data demonstrate that LINC0052 overexpression is induced by an epigenetic mechanism in human HCC. Upregulated LINC0052 interacts with ribonucleoprotein complexes and may thus support a protumorigenic cerna network in human HCC. 47
148 P08-0YI HEPATOCELLULAR CARCINOMA - HOW DOES BCLC SCORE INFLUENCE THERAPEUTIC DECISION? Daniela Reis, Rita Rodrigues 2, Sofia Carvalhana, Afonso Gonçalves 3, Rui Tato Marinho, José Velosa, Helena Cortez-Pinto 4 Hospital de Santa Maria, Centro Hospitalar Lisboa Norte, EPE, Gastroenterology and Hepatology, Lisbon, Portugal, 2 Instituto Português de Oncologia Francisco Gentil, Gastroenterology, Lisbon, Portugal, 3 Hospital de Santa Maria, Centro Hospitalar Lisboa Norte, EPE, Radiology, Lisbon, Portugal, 4 Faculdade de Medicina, Universidade de Lisboa, Laboratório de Nutrição, Lisbon, Portugal Background and Aims: The Barcelona Clinic Liver Cancer (BCLC) system stratifies patients with hepatocellular carcinoma (HCC), defining first-line treatment options for each stage. However, there has been controversy regarding its use, mostly in advanced forms. Our aim was to evaluate, from a single unit experience, to which extent it was used and how it predicted survival. Method: We retrospectively reviewed 98 cirrhotic patients, diagnosed with HCC between January 203 and December 206 who underwent treatment (resection, radiofrequency ablation, chemoembolization and Sorafenib) after a multidisciplinary team discussion. Patients referred for liver transplantation were excluded from this analysis. Retrospective classification of the BCLC status was done at decision time. Results: Median age was 65. years (35-87), mainly males (82.7%). The most prevalent etiology of cirrhosis was alcohol-related in 46%, followed by HCV (3.6%) and HBV infection (.2%). Seventy-two patients (73.5%) were under ultrasound screening. The majority was Child-Pugh A: 66.3%, and ECOG 0: 69.4%. Portal vein thrombosis: 68.4%. Patients BCLC distribution: 4 in stage-0, 28.6%; 28 in stage- A, 24.6%; 24 in stage-b, 22.2%; 27 in stage-c,.5%; and 5 in stage D, 3.%. Mean survival time was 26.3 months (95%CI: ). Fifty-seven patients died (58.2%). Mean survival time according to BCLC score was stage 0: 36.5 months (95%CI: ), stage A: 40.8 months (95%CI: ), stage B: 37. months (95%CI: ), stage C: 2.5 months (95%CI: ) and stage D: 3.months (95%CI: ). In univariate analysis, factors significantly correlating with HCC survival time (Person test, p<0.05) were: age (p=0.036), being under ultrasound screening (p=0.00), largest lesion size (p=0.007), PVT (p=0.000), ECOG (p=0.000), CTP score (p=0.000), BCLC (p=0.000), type of treatment (p=0.0), alpha-fetoprotein level (p=0.07), total bilirubin level (p=0.00) and albumin level (p=0.08). However, in a multivariate analysis, none of these factors were independent predictors of survival. Finally, 7 patients (72.4%) were treated according to BCLC staging. Even though there was no correlation with survival (p=0.059), there was a tendency of increased survival for patients with individualized treatment compared to those whose treatment was chosen according to recommendations (35.6 vs 22.2 months). Conclusion: BCLC is an effective system to stratify patients according to prognosis. However, there may be a benefit from an individualized decision of treatment for some patients according to experts experience. 48
149 P08-02 CLINICAL SIGNIFICANCE OF TIME RELATED FLUCTUATIONS OF AFP AND PIVKA-II SERUM LEVELS IN PATIENTS WITH CIRRHOSIS UNDERGOING SURVEILLANCE FOR HEPATOCELLULAR CARCINOMA Gabriele Ricco 2, Chiara Cosma 3, Giorgio Bedogni 4, Alessandra Biasiolo 5, Maria Guarino 6, Patrizia Pontisso 5, Filomena Morisco 6, Filippo Oliveri 7, Daniela Cavallone 7, Ferruccio Bonino 4 8 9, Mario Plebani 3, Maurizia R. Brunetto 2 7 Hepatology Unit and Laboratory of Molecular Genetics and Pathology of Hepatitis Viruses, Reference Center of the Tuscany Region for Chronic Liver Disease and Cancer, University Hospital of Pisa, Pisa,, 2 Department of Clinical and Experimental Medicine, University of Pisa, Pisa, Italy, 3 Department of Laboratory Medicine, University-Hospital of Padua, Padua, Italy, 4 Italian Liver Foundation (FIF), Trieste,, 5 Department of Internal Medicine, University of Padua, Padua, Italy, 6 Department of Clinical Medicine and Surgery Gastroenterology Unit, University of Naples "Federico II", 7 Hepatology Unit and Laboratory of Molecular Genetics and Pathology of Hepatitis Viruses, Reference Center of the Tuscany Region for Chronic Liver Disease and Cancer, University Hospital of Pisa, 8 UPMC Institute for Health, Chianciano Terme, Siena,, 9 Department of Biostructure and Bioimaging, National Research Council, Naples, Background and Aims: The clinically meaningful variations of circulating HCC biomarkers in the single patient are uncertain. We studied the dynamics of AFP and PIVKA-II in 2-3 consecutive sera obtained at random time points in cirrhotic patients with and without HCC. Method: AFP and PIVKA-II were measured in 63 sera of 48 cirrhotics (3.%HBV, 58.6%HCV, 0.3%Non-viral) undergoing ultrasound HCC surveillance at 3 centres: 24 developed HCC (29 with and 95 with 2 sera before the serum at diagnosis), 294 remained HCC free for at least 2 months after the last specimen (2 sera in 62 and 3 sera in 232). Tests were performed in a single laboratory using automated chemiluminescent-enzyme-immunoassays (Fujirebio, Tokyo, Japan). Time between timepoints (t, t2, t3) was expressed in months. AFP/PIVKA-II time-related changes were analysed by calculating the month-related variation coefficients (MVC={[(xtlast xtfirst)/xtfirst]x00}/(xtlast xtfirst)) and using a random-effect generalized least squares (RE-GLS) regression model. Results: In figure we report the MVC between groups. Multiple time-related ROC curve analysis of MVC shows 6 months (±.5) as best time frame for both biomarkers. Using 0% MVC as cut-off the Sensitivity/Specificity for HCC diagnosis were 7.8/96.3% and 27.7/93.8% for AFP and PIVKA-II, respectively. Log0AFP time-related (-6 months) changes estimated by RE-GLS ranged between (95%CI ) and (95%CI ) for HCC+ and HCC-, whereas the values of log0pivka-ii were (95%CI ) and (95%CI ), respectively. In HCC- patients AFP was influenced by disease activity and showed more variability than PIVKA-II. The gap of median MVC between HCC+ and HCC- was up to six-fold higher for PIVKA-II than AFP. Conclusion: The month-related variation coefficient (MVC) of AFP and PIVKA-II appears a reliable measure for individualized HCC surveillance with an optimal time frame [6 (±.5) months] coincident with the suggested timing of ultrasound surveillance. A 0% MVC cut-off for both biomarkers qualifies as a candidate diagnostic tool worth to be tested in prospective studies. Figure: 49
150 P08-03YI MIR-2 ABLATION PREVENTS NASH-ASSOCIATED HEPATOCELLULAR CARCINOMA Pedro M. Rodrigues, Marta B. Afonso, André Simão, André A. Santos, Tawhidul Islam, Maria Manuela Gaspar, Cecília M. P Rodrigues, Rui E. Castro Research Institute for Medicines (imed.ulisboa), Faculty of Pharmacy, Universidade de Lisboa, Lisbon, Portugal Background and Aims: The molecular mechanisms regulating the transition from non-alcoholic steatohepatitis (NASH) to hepatocellular carcinoma (HCC) are not entirely known. We have recently shown that concomitant mir-2 ablation and FXR activation prevents NASH development in mice. Here, we aimed to evaluate the role of the mir-2/pparα pathway in NASH-associated carcinogenesis. Method: Wild-type (WT) and mir-2 KO C57BL/6N mice were fed either a choline-sufficient, amino acid-defined control diet (CSAA; n=28) or a choline-deficient, amino acid-defined diet (CDAA; n=28) for 32 and 66 weeks. After sacrifice, serum was collected and the number of pre-neoplastic nodules counted. Liver samples were processed for histological analysis and measurement of mir-2, PPARα and metabolic relevant genes, and pro-inflammatory/pro-fibrogenic cytokines by qpcr and immunoblotting. Results: WT mice fed the CDAA diet for 32 weeks developed macrovesicular steatosis, hepatocyte ballooning, NASH and fibrosis, concomitantly with accumulation of perivascular lymphoid cells and macrophage agglomerates. After 66 weeks, all mice on the CDAA diet developed at least one preneoplastic nodule - average of 5.2 nodules/animal - with one animal developing trabecular HCC. In addition, livers presented hyperplastic foci and anisokaryosis, as well as phenotypically altered hepatocytes. Further, hepatocytes from CDAA-fed mice were highly proliferative, as evidenced by Ki- 67 staining, and expressed significantly increased levels of pro-inflammatory/fibrogenic markers, particularlly in pre-neoplastic liver tissue. mir-2 expression was significantly increased in CDAA-fed mice and further increased in HCC, concomitantly with decreased expression of PPAR and its direct transcriptional genes. Of note, mir-2 KO mice fed the CDAA diet for 32 weeks displayed markedly decreased fatty acid serum levels, compared with WT mice, and PPAR target genes were markedly increased. After 66 weeks, serum transaminase levels were similar to control animals, liver nodules greatly decreased - average of 2.3 nodules/animal, hepatocyte profliferation was reduced and the pro-inflammatory/fibrogenic milleau reversed to almost baseline. Conclusion: Overall, the mir-2/pparα pathway appears to contribute to NASH-associated carcinogenesis, with its inhibiton halting HCC development. Targeting mir-2 and/or PPARα may constitute an appealing therapeutic approach to prevent NASH and its complications. (PTDC/BIM- MEC/0895/204, SFRH/BD/8822/202, SAICTPAC/009/205 FCT, PT). 50
151 P08-04 ROLE OF THE HES5/NOTCH SIGNALING PATHWAY IN LIVER CARCINOGENESIS Sarah Luiken, Matthias Bieg 2, Benjamin Goeppert, Stefan Pusch 3, Thomas Longerich, Peter Schirmacher, Stephanie Roessler Institute of Pathology, Heidelberg, Germany, 2 German Cancer Research Center, Division of Applied Bioinformatics, Heidelberg, Germany, 3 German Cancer Research Center, Clinical Cooperation Unit Neuropathology, Heidelberg, Germany Background and Aims: Notch signaling is an evolutionary conserved pathway which is crucial in liver development and regeneration. Deregulated Notch signaling is a potential driver of liver inflammation and liver tumorigenesis. Interestingly, altered Notch signaling has been reported to induce both hepatocellular (HCC) and cholangiocellular carcinoma (CCA). Previous studies mainly focused on the expression level of the Notch receptors; however, downstream pathway components and their relevance in liver cancer are poorly understood. Method: Whole exome sequencing of 57 human HCC samples was performed and identified mutations were analyzed in silico for their potential effect on protein function. HES5 and mutant HES5-Arg3Gly were further characterized in cell culture and mouse experiments. Results: We discovered 9 nonsynonymous mutations in 5 different Notch pathway genes which were confirmed to be somatic by Sanger sequencing. In total, 4 of 57 (25%) patients presented at least one mutation in one Notch pathway components. Using multiple online tools to predict the effect of the mutations on protein function and tumor relevance, we observed that HES5-Arg3Gly mutation ranked highest. In order to test, whether HES5 is activated by Notch in HCC cells, we generated cell lines with inducible expression of NOTCH or NOTCH3 intracellular domain and found that HES5 but not HES is strongly activated in several HCC cell lines. Furthermore, induction of HES5 in an inducible cell line resulted in decreased cell migration and colony formation. In preliminary mouse experiments using hydrodynamic transduction of transposons expressing MYC and HES5, we found that HES5 increased tumor formation compared to MYC alone. Interestingly, HES5-Arg3Gly had no influence on cell migration and colony formation and also did not altered expression of HES5 target genes. We also observed that HES5 negatively regulated HES and NOTCH expression suggesting a negative feedback loop, whereas, HES5-Arg3Gly had no effect. Conclusion: Thus, we identified somatic mutations in Notch pathway genes in 25% of HCC patients and functional analyses showed that HES5 has oncogenic properties. 5
152 P08-05YI LONG NON-CODING RNA H9: A BIOMARKER OF HEPATOCELLULAR CARCINOMA Ángela Rojas, Antonio Gil-Gomez, Raúl González 2, Rocío Gallego-Durán, Rocio Munoz Hernandez, Marta Garcia Valdecasas 2, M. Carmen Rico, Yolanda Sánchez, Maria Teresa Ferrer, Javier Padillo 3, Javier Ampuero, Jordi Muntané 3, Manuel Romero Gomez Instituto de Biomedicina de Sevilla (IBiS), Hospital Universitario Virgen del Rocío/CSIC/Universidad de Sevilla, España., UGC Enfermedades de enfermedades Digestivas y CIBERehd, Sevilla, Spain, 2 Instituto de Biomedicina de Sevilla (IBiS), Hospital Universitario Virgen del Rocío/CSIC/Universidad de Sevilla, España., Sevilla, Spain, 3 Departamento de Cirugía General, Hospital Universitario Virgen del Rocío/IBiS/CSIC/Universidad de Sevilla, Sevilla, España. Instituto de Biomedicina de Sevilla (IBiS), Sevilla, España. CIBEREHD., Departamento de Cirugía General, Hospital Universitario Virgen del Rocío/IBiS/CSIC/Universidad de Sevilla, Sevilla, España. Instituto de Biomedicina de Sevilla (IBiS), Sevilla, España. CIBEREHD., Sevilla, Spain Background and Aims: Non-coding RNAs are involved in carcinogenesis pathways. However, their actual roles in the molecular mechanisms underlying hepatocellular carcinoma (HCC) development still remain unknown. (i)to study the epigenetic profile of long non-coding RNAs (lncrnas) in liver tissue from cirrhotic patients vs HCC (ii)to determine circulating lncrnah9 levels in a cohort of cirrhotic vs HCC patients, with or without curative treatments (iii)to isolate and characterize liver cancer stem cells (LCSC) in vitro and to analyse their epigenetic profile. Method: (i) Fourteen cirrhotic patients were included in this study. Of them, 7/4(50%) suffered from HCC (7.4%(5/7) underwent ablation therapy). 85.7%(2/4) were men; mean age yo. Total RNA from liver tissue (the furthest from the tumour area) was isolated by mirvana kit. lncrnas expression levels were determined by RT2 IncRNA PCR Array Cancer (Qiagen) by pooling samples into 2 groups (cirrhotic vs HCC patients) and individually validated by qpcr. (ii)circulating levels of lncrna H9 were evaluated in eighteen patients (89%(6/8) men, mean age 59.±5.3 yo). 44%(8/8) were cirrhotic, 27.8%(5/8) had HCC BCLC-A stage and 27.8% (5/8) underwent ablation therapy. Plasma RNA was isolated by using Trizol and H9 expression levels were determined by qpcr. (iii) In vitro, EpCAM and CD33 positive cells were isolated from Huh7.5 cell line by FACS (Facs Aria Fusion BD). Total RNA was isolated by Trizol and the expression levels of NANOG, SOX2, OCT4 and H9 were measured by qpcr. Results: H9 was found significantly increased in liver tissue from HCC patients compared to cirrhotic patients (p=0.020) showing a positive correlation with AFP serum levels (r=0.6; n=4, p=0.02). Regarding circulating levels, H9 was upregulated in HCC patients compared with cirrhotics (foldchange.79±0.57;p=0.09). On the other hand, plasma levels of H9 were significantly lower in patients that underwent ablation compared with HCC (fold-change 0.28±0.3;p=0.007). EpCAM + CD33 + showed a higher expression of NANOG (fold-change 2.66±0.38;p<0.000), SOX2 (fold-change 3.52±0.62;p=0.063), OCT4 (fold-change.94±0.7;p<0.0) and H9 levels (fold-change 2.8±0.32;p=0.003). Conclusion: lncrna H9 was found increased in liver tissue and plasma from HCC patients as well as in a liver cancer stem cell line. The curative treatment of HCC normalized plasma H9 expression levels, so H9 is an interesting biomarker in the context of HCC. 52
153 P08-06YI INHIBITING THE P2Y2 RECEPTOR DECREASES TUMOUR CELL VIABILITY AND AFFECTS DIFFERENT CELL TYPES IN THE STROMA Natasa Pavlovic, Linus Edlund, Pär Gerwins 2, Femke Heindryckx Uppsala University, Medical Cell Biology, Uppsala, Sweden, 2 Akademiska sjukhuset, Radiology, Uppsala, Sweden Background and Aims: P2Y2 belongs to the G-protein coupled purinergic receptors and is a chemoreceptor for ADP. While the function of P2Y2 on platelets has been described extensively, we investigated the role of these receptors on different cell types involved in hepatocellular carcinoma. Hypoxia or inflammation, activates the release of extracellular nucleotides such as ATP and UTP which interact with cell surface P2Y-receptors to induce a broad range of physiological responses, which could be relevant in the pathogenesis of hepatocellular carcinoma. Method: P2Y2 expression was inhibited in vitro by ticagrelor. HepG2 and Huh7 (hepatocellular carcinoma), LX2 (hepatic stellate cells), THP (monocytes/macrophages) and RAW cells (kupffer cells) were exposed for 6 hours to different concentrations (0uM-0 um) of ticagrelor and cell viability was assessed using resazurin. IC50 values were determined on log-transformed viability curves. Western blot was used to identify the protein expression of P2Y2 in the different cell types. mrna expression for markers of stellate cell activation (asma, CTGF and collagen) was measured using qpcr. THP- cells were differentiated to macrophages with 5 ng/ml PMA for 48 hours. Macrophage polarization was checked using arginase- and HLA-DR on immunocytochemistry. Results: Inhibition of the P2Y2 receptor with ticagrelor led to a decreased viability of Hepg2-cells, Huh7-cells, LX2-cells, THP-differentiated macrophages and RAW cells. The IC50 values were 2.4 um for HepG2, 3.2 um for Huh7, 2.9 um for LX2,.7 um for THP-differentiated macrophages and 4.4 um for RAW cells, meaning 50% of the cells died in all cell types when exposed to concentrations between um ticagrelor. All of the tested cell types expressed the P2Y2 receptor, although expression differed considerably between cell types. A low 0.5 um dose of ticagrelor was used to stimulate LX2 stellate cells and THP-macrophages. Interestingly, low dosage of ticagrelor significantly blocked stellate cell activation and significantly decreased expression of the M2-marker (arginase ) in THP-macrophages, while significantly increasing the expression of the M-marker HLA- DR. Conclusion: P2Y2 is expressed in several hepatic cell types that are involved in the hepatocarcinogenesis, including tumor cells, hepatic stellate cells, kupffer cells and macrophages. Inhibiting P2Y2 not only decreases tumor cell viability, it could also affect several actors in the surrounding stroma. We found that P2Y2-inhibition decreases stellate cell activation and possibly induces an anti-tumoural M-phenotype in macrophages. 53
154 P08-07YI OVERCOMING HEAT-SINK IN PORTAL VEIN RELATED HEPATOCELLULAR CARCINOMAS WITH COMBINED RADIOFREQUENCY ABLATION AND PERCUTANEOUS ETHANOL INJECTION Hisham Saad Mohamed Elsayed Abdelaal, Medhat El Hosary Kafr El Sheikh Liver Research Center, Egypt Background and Aims: Heat sink Phenomenon commonly explains incomplete ablation in hepatocellular carcinomas (HCCs) directly in contact with the portal vein (PV). The purpose of this study was to investigate whether combining percutaneous ethanol injection (PEI) with radiofrequency ablation (RFA) improves treatment outcomes in these cases. Method: Our study was conducted from May 204 to December 206 on 40 patients having single lesion of HCC (3. 5 cm in diameter). Patients were randomized into 2 groups (20 patients each); RFA group: Patients treated with RFA alone. RFA+PEI group: Patients treated with combined RFA & PEI. All lesions were in close contact to the PV. PEI was performed into the part of the tumor closest to PV before RFA. Follow up of the patients of the two groups was done for about 6 months with special emphasis on recurrence of HCC, any remote complication related to the procedure, development of liver decompansation hematemsis, or death. Results: Regarding primary success In our study, the total success rate was (90%) in the two groups. Success rate in RFA group was 85%. Success rate RFA+PEI group was 95%. CT findings after 6 months: 37 patients showed maintained ablation while 3 patients showed reenhancement (local recurrence). Complications of the procedures: abdominal pain, fever, hematemsis and biliary injury were the most common early complications encountered in our study. While ascites and portal vein thrombosis were the most common late complications. Conclusion: Combined PEI and RFA treatment has a tendency to be more effective than RFA alone for managing medium sized HCCs in contact with PV. PEI & RFA are generally accepted as safe procedures, but it may cause major biliary complications and PVT in lesions adjacent to the portal vein. Figure: Table: Success rate of the two procedures after month. Results According to spiral CT & biopsy Partial ablation Complete ablation Partial ablation Failure with reablation Failure with no further treatment RFA group (n = 20) RFA + PEI group (n = 20) No (%) No (%) 7 (85%) 9 (95%) 3 (5%) (5%) 2 (0%) 0 (0%) (5%) (5%) P value P= P2=0.633 P=.0 P2=
155 P08-08 LONG-TERM SORAFENIB TREATMENT IN A LARGE COHORT OF HCC PATIENTS: A MULTI CENTER STUDY Rodolfo Sacco, Alessandro Granito 2, Teresa Zolfino 3, Carlo Saitta 4, Luca Marzi 5, Gherardo Tapete, Giampaolo Bresci, Sara Marinelli 6, Francesco Tovoli 2, Simona Attardo 7, M. Rossi 7, Giuseppe Cabibbo 7 Pisa University Hospital, Gastroenterology and Metabolic Diseases, Pisa, Italy, 2 Bologna University, Department of Medical and Surgical Sciences, Bologna, Italy, 3 Brotzu Hospital, Gastroenterology, Cagliari, Italy, 4 Messina University, Internal Medicine, Messina, Italy, 5 Modena University, Gastroenterology, Modena, Italy, 6 Bologna University, Medical and Surgical Sciences, Bologna, Italy, 7 Palermo University, Gastroenterology, DIBIMIS, Palermo, Italy Background and Aims: Given the introduction of regorafenib as a second-line therapy for hepatocellular carcinoma (HCC), the therapeutic algorithm for this disease will be further developed. Therefore, it is important to have information on factors predictive of the duration of and response to systemic therapy with sorafenib. In this multicenter, field-practice study, we evaluated outcomes of longterm sorafenib in a cohort of patients with HCC. Method: HCC patients consecutively enrolled and treated with Sorafenib were identified from 6 Italian referral centers. We considered to analyze those subjects who had received sorafenib treatment for 2 months. Results: Out of a total of 800 patients treated with Sorafenib, 8 (0%) received long-term treatment with this systemic therapy. Sorafenib was administered in the first-line setting in 9 patients (23.5%). Median duration of sorafenib treatment was 22.7 months (range ). Adverse events (AEs) of any grade were reported in 74 patients (9%); however, only 2 (26%) reported grade 3/4 AEs. Only four patients (6%) permanently discontinued sorafenib due to AEs. Best response to sorafenib was CR in patients (4%) and PR in 5 (6%). Median duration of objective response was 8. months (4 83.5). Median OS was 34.8 months (95%CI ), with 2-, 3- and 5-years survival rates of 76.3%, 46.4% and 25.4%, respectively. The only parameter associated with survival was baseline Child-Pugh class, with median survival of 36.5 months in Child A (95%CI ) and 23.3 months (95%CI ) in Child B patients (P=0.02). Conclusion: This large field-practice study highlights that sorafenib treatment could result in long-term control of HCC in a relevant proportion of patients. Given also the availability of regorafenib in the second-line setting, an earlier introduction of systemic therapy may be considered for those patients who may be ineligible or non-responders to TACE or to other treatments, when they have preserved liver function. 55
156 P08-09YI FACTORS ASSOCIATED WITH OCCURRENCE/RECURRENCE OFHEPATOCELLULAR CARCINOMA EARLY AFTER TREATMENT OF HEPATITIS C WITH DIRECTANTIVIRAL AGENTS Livia Salmi, Deborah Camatta, Matteo Nazzareno Barbaglia, Margherita Tran Minh, Giuseppe Mancuso, Federico Daffara, Rosalba Minisini, Monica Leutner 2, Renzo Boldorini, Mario Pirisi Università del Piemonte orientale, Translational Medicine, NOVARA, Italy, 2 AOU Maggiore della Carità, NOVARA, Italy Background and Aims: Recently, several groups have reported a surprisingly high rate of either de novo or recurrent hepatocellular carcinoma (HCC) early after treatment of chronic hepatitis C with direct antiviral agents (DAA). Both the very existence of this phenomenon and its putative explanation (sudden loss of host immune control in the liver) have been questioned. In the present study, our aims were a) to provide further data on the rates of early HCC occurrence/recurrence in this unprecedented setting, in which far more advanced patients than in the past qualify for treatment; b) to identify possibly associated factors. Method: N.=286 consecutive patients (N.=66 males; median age 64 years; 66% cirrhotics; N.=3 with a previous HCC diagnosis) who received a DAA regimen were studied. All were free of suspicious nodules and were followed up for at least 6 months after concluded treatment. Circulating microrna (mir) -22, -373 and -55 were quantified on serum samples at baseline, at the end of treatment and at week 2 post-treatment (timing of definition of sustained viral response, SVR2) from patients who developed HCC (group A) and a selection of control patients (n.=30; group B). Results: Along the first 24 weeks of follow up de novo HCC was detected in 9/273 patients (incidence rate 7.% per year) and recurrent HCC in 2/3 patients (incidence rate 33.4% per year). These /286 patients did not differ regarding age, gender, baseline viral load and liver biochemistry parameters from the remaining 275/286 patients. However, as compared to the latter, they did have a significantly higher liver stiffness at transient elastography (median 2.5 kpa, IQR vs. 4.3, IQR ; p=0.029), as well as lower hemoglobin (3 g/l, IQR vs. 40, IQR 30-5; p=0.040). They displayed a trend towards having higher body mass index (29.7 kg/m 2, IQR vs. 25.6, IQR ). Importantly, the intention-to-treat SVR2 rates were lower among patients with de novo/recurrent HCC than among their counterparts HCC-free at the end of follow up (7/, 64% vs. 26/275, 95%; p<0.00). Circulating mir concentrations at baseline were not different between group A and group B patients; however, serum mir-22 concentrations declined between baseline, end-oftreatment and post-treatment week 2 among group B (p=0.003) but not among group A patients (p=0.290). Conclusion: Advanced disease and failure to clear the virus (accompanied by a flat kinetic of mir-22) identify patients who develop early HCC occurrence/recurrence following DAA treatment, suggesting that treatment per se does not favour the emergence of HCC. A practical implication of these findings is that patients with the above high risk features should have counselling and surveillance optimized before and after DAA treatment of hepatitis C. 56
157 P08-0YI SERUM ENDOGLIN (CD05) AS A POTENTIAL MARKER FOR HEPATOCELLULAR CARCINOMA IN CIRRHOTIC HEPATITIS C VIRUS AND HEPATITIS B VIRUS PATIENTS Mohamed Samy, Khaled Mohieden 2, Ali Elkady 2, Akram Deghedy 2, Rania Abou Youssef 2 Faculty of Medicine Alexandria University, tropical medicine, Alexandria, Egypt, 2 Faculty of Medicine Alexandria University, Alexandria, Egypt Background and Aims: HCC has a rising incidence in Egypt mostly due to high prevalence of viral hepatitis B&C and their complications. AFP is an early serum marker of HCC but with low sensitivity. Therefore, there is a need for new serum markers of HCC. Endoglin (CD05) is a promising serum marker for HCC which may be more sensitive and specific than AFP. The aim was to assess the value of serum Endoglin level, as a potential marker for HCC. And to correlate serum Endoglin level with serum AFP and GGT as well Method: The study was conducted on eighty patients classified into two groups: group I consisted of 30 patients of HCV and HBV induced liver cirrhosis without HCC; group II included 50 patients with HCC on top of HCV and HBV induced liver cirrhosis. Serum Endoglin was measured by ELISA. Patients with pulmonary disease, alcoholics, those suffering from fever, patients with autoimmune hepatitis or other malignancies were excluded from the study. Results: Serum Endoglin, GGT AND AFP were significantly higher in HCC (group II) than in cirrhotic patients (group I) (p<0.00 * ), (P value * ) and P value <0.00 * ) respectively. Moreover, significant positive correlation was found between serum Endoglin and Child Pugh score in HCC and cirrhosis (P<0.00 * ) and (p<0.009 * ) respectively. There was also significant positive correlation between serum Endoglin and BCLC in HCC group (P<0.00 * ), moreover there was a positive correlation between serum Endoglin and portal vein thrombosis (P<0.040 * ), and tumor number in cases of HCC (P<0.00 * ) respectively. On the other hand, there were no significant correlations between Serum Endoglin and tumor size in which (P value equal <0.879), PCR for HBV (x0 3 ) and HCV (x0 3 ) in which (P value equal 0.923) and (P value equal 0.660) respectively. Diagnosis of HCC among patients with HCV and HBV cirrhosis could be suggested when serum Endoglin is detected at a cutoff value of 5. ng/ml with sensitivity of 88.0%, specificity of 73.33%, positive predictive value of 84.6 % and negative predictive value of 78.6%. As for AFP at a cutoff value of 48 ng/ml with sensitivity of 80.0%, specificity of 70.0 %, positive predictive value of 8.6 % and negative predictive value of 76.7%. Regarding GGT at a cutoff value of 69 ng/ml with sensitivity of 64.0%, specificity of 53.3 %, positive predictive value of 69.6 % and negative predictive value of 47.%. Conclusion: Serum Endoglin might be used as a valuable serum marker for HCC development in cirrhotic HCV and HBV patients particularly in those with normal AFP level. The significant correlation between Serum Endoglin and BCLC in patients with HCC could suggest its use as a prognostic factor in patients with HCC. Combined use of Serum Endoglin, AFP and GGT could represent a better diagnostic tool for HCC. 57
158 Figure: ROC curve for different parameters to predict HCC cases vs cirrhosis 58
159 P08-YI IMPACT OF REGORAFENIB IN THE CLINICAL PRACTICE AND IDENTIFICATION OF SECOND-LINE TREATMENT ORPHAN PATIENTS Marco Sanduzzi Zamparelli, Víctor Sapena, Álvaro Díaz-Gonzázlez, Anna Darnell 2, Neus Llarch, Ernest Belmonte 3, Loreto Boix, Gemma Iserte, Alejandro Forner, Josep Corominas, Leonardo Gomes Da Fonseca, Carmen Ayuso 2, María Reig, Jordi Bruix Hospital Clínic de Barcelona. IDIBAPS. CIBERehd., BCLC group. Liver Unit., Barcelona, Spain, 2 Hospital Clínic de Barcelona. CIBERehd. Universitat de Barcelona., BCLC group. Radiology department., Barcelona, Spain, 3 Hospital Clínic de Barcelona. IDIBAPS. CIBERehd., BCLC group. Radiology department., Barcelona, Spain Background and Aims: The RESORCE study showed that regorafenib provides a significant benefit in terms of overall survival (OS) to patients with hepatocellular carcinoma (HCC) who tolerated sorafenib (400 mg/day) and presented radiologic progression. Data on regorafenib treatment in clinical practice are scarce and the percentage of patient candidates or orphans of effective second-line treatment is unknown. The purpose of this study was to investigate the feasibility and tolerance of regorafenib in clinical practice and to evaluate the proportion of patients who can benefit from it. Method: we analysed a prospective database of patients with HCC treated with sorafenib to investigate the regorafenib applicability and assessed the outcome of patients that have received this novel option. This includes 9 patients [5 within the research trials and 4 under compassionate use]. All patients started at 60 mg/day. Treatment was continued until symptomatic progression, unacceptable adverse events or patient decision. Results: Eighty of the 299 patients treated with sorafenib were alive at the time of regorafenib availability, 2/80 continued on sorafenib and 59 definitively discontinued (4 due to toxicity, 7 for tumor progression and because of patient decision). 23% (4/59) of the patient who discontinued sorafenib started regorafenib and 4/7 (82.35%) with tumor progression started regorfenib. Among all the patients treated with regorafenib 85% were BCLC-C with the tumor progression pattern of: 5% BCLCp- B (n=3), 35% BCLCp-C (n=7) and 50% BCLCp-C2 (n=0). The median follow-up was 9.9 and 5.6 months for the research and clinical practice patients respectively. /20 patients have died (range 3-32 months). The median time to st dose modification was 3.8 days and modifications were due to: fatigue (n=4), skin reaction (n=4) and diarrhoea (n=3). Seven of the 8 patients who discontinued regorafenib did so because of symptomatic progression. Conclusion: Since regorafenib approval for HCC, the number of patients treated with regorafenib is low but data on the tolerability and survival reproduce the RESORCE results even if presenting the poor prognosis pattern (50% BCLCp-C2). More than half of the patients treated with sorafenib are a potential candidate for regorafenib, although a relevant number of patients remains orphan for effective secondline treatment. 59
160 P09-0YI CONTRAST-ENHANCED ULTRASOUND FOR NON-INVASIVE DIAGNOSIS OF HEPATOCELLULAR CARCINOMA: A COMPARISON BETWEEN CEUS LI-RADS AND ESCULAP CRITERIA IN A LARGE HIGH-RISK COHORT OF PATIENTS Antonio Saviano 2, Laura Riccardi 2, Maria Assunta Zocco 2, Thomas Baumert 3, Gian Ludovico Rapaccini 2, Maurizio Pompili 2, Antonio Gasbarrini 2 Inserm Unit 0; Institut de Recherche Sur Les Maladies Virales et Hépatiques, Strasbourg, France; Université de Strasbourg, Strasbourg, France, 2 Internal Medicine, Gastroenterology and Liver Disease Unit, Policlinico "A. Gemelli", Catholic University, Rome, Italy, 3 Institut Hospitalo-Universitaire, Pôle Hépato-Digestif, Nouvel Hôpital Civil, Rome, Italy Background and Aims: Contrast-enhanced ultrasound (CEUS) for the non-invasive diagnosis of hepatocellular carcinoma (HCC) in patients with liver cirrhosis raised concerns for the risk of misdiagnosis with intrahepatic cholangiocarcinoma (ICC) and was removed as diagnostic technique from international guidelines. To address this issue, the American College of Radiology recently released the CEUS LI-RADS criteria for HCC diagnosis in liver cirrhosis. Other criteria, named ESCULAP (Erlanger Synopsis of Contrast-enhanced Ultrasound for Liver lesion Assessment in Patients at Risk) were also recently published and reported to have a better accuracy compared to CEUS LI- RADS. Aim of this study was to assess and compare, for the first time, the diagnostic accuracy of these criteria in a large independent cohort. Method: Between 2005 and 205, 8 nodules in 56 patients with chronic liver disease at high HCC risk were retrospectively collected in the Center of Liver Diseases at the Catholic University of Rome and were enrolled in this study. The diagnostic accuracy of the CEUS LI-RADS LR-5 and ESCULAP-4 categories for the diagnosis of HCC was assessed and compared. The 200 AASLD criteria applied to HCC>cm were also evaluated. A comparison of the diagnostic performance of the categories CEUS LI-RADS LR-M (non-hcc malignancies) and ESCULAP-C (ICC diagnosis) was made. The diagnostic reference was histology or CT/MRI. Results: The 58.6% of patients had HCV cirrhosis and the median nodule size was.8 cm (range cm). HCC represented the 78.5% of diagnosis while ICC the 2.2%. LR-5 category (52% of nodules) had a positive predictive value (PPV) for HCC of 00% and a sensitivity of 58% with no risk of misdiagnosis with ICC. ESCULAP-4 (76% of nodules) had a PPV of 92% and a sensitivity of 77% for HCC. In this cohort, the 200 AASLD criteria showed a PPV and a sensitivity for HCC diagnosis of 93% and 64%, respectively. No nodules could be classified as ICC using the ESCULAP-C category whereas all the non-hcc malignancies (included all the ICCs) were classified as LR-M according to CEUS LI- RADS. Conclusion: CEUS LI-RADS LR-5 category has a high specificity and PPV for HCC diagnosis eliminating the risk of failure to diagnose ICC. ESCULAP criteria have higher sensitivity but lower specificity for HCC diagnosis and do not avoid the risk of ICC misdiagnosis. A marked and/or early wash-out in CEUS (LR-M feature) is the most important feature for CEUS diagnosis of ICC arising in liver cirrhosis. 60
161 P09-02YI REGORAFENIB AFTER PROGRESSION ON SORAFENIB FOR ADVANCED HCC Kornelius Schulze, Johann von Felden, Harald Ittrich 2, Ines Gil-Ibanez, Thorben Fruendt, Jenny Krause, Kathrin Karkmann, Ansgar Lohse, Henning Wege University Medical Center Hamburg-Eppendorf, Department of Internal Medicine, 2 University Medical Center Hamburg-Eppendorf, Diagnostic and Interventional Radiology Regorafenib after progression on Sorafenib for advanced HCC Kornelius Schulze, Johann von Felden, Harald Ittrich 2, Ines Gil-Ibanez, Thorben Fründt, Jenny Krause, Kathrin Karkmann, Ansgar W. Lohse, Henning Wege. Department of Internal Medicine, University Medical Center Hamburg-Eppendorf, Hamburg, Germany 2. Department for Diagnostic and Interventional Radiology, University Medical Center Hamburg- Eppendorf, Hamburg, Germany Background and Aims: Advanced hepatocellular carcinoma (HCC) with distant metastasis or macrovascular invasion (BCLC stage C) has a dismal prognosis. Especially treatment after progression on first-line Sorafenib (SOR) remains challenging. Recently, the RESORCE trial tested Regorafenib (REG) superior to placebo as second-line treatment in terms of overall survival (OS, 0.6 vs. 7.8 months) and progression free survival (PFS, 3. vs..5 months), despite a high prevalence of treatmentemergent adverse events (AE) (Bruix et al, Lancet 207). The aim of our single center study was to investigate the real-life outcomes of REG treatment after progression on SOR in patients with advanced HCC. Method: Ten patients with advanced HCC (BCLC stage C) who started REG after progression on SOR at the University Medical Center Hamburg-Eppendorf between September 206 and November 207 were prospectively followed. Primary endpoint was efficacy assessed with OS and PFS according to mrecist. The secondary endpoint was safety. Results: The cohort contained 70% male patients. 60% of patients had liver cirrhosis. All patients progressed on SOR with a median PFS of 7.0 months. Three patients received subsequent treatment prior to REG; two patients received intravenous Doxorubicin-Transdrug within a clinical trial (NCT ) and one patient received capecitabine and doxorubicin outside a clinical trial. At start of REG, all patients had compensated liver function and were ECOG 0-2, median AFP was 48 kiu/l (range 2-57,659). Median OS was not reached (median follow-up 9 months, range -4). Median PFS on REG was 5.7 months, with four patients still on treatment (duration to date, 2, 6 and 3 months, respectively). 80% of patients had AE, predominantly hand-foot skin reaction (38%), hypertension (25%), diarrhea (25%), stomatitis (25%) and fatigue (3%), ranging from CTCAE grade -3. One death on treatment occurred. Dose-adjustments of REG due to AE were necessary in five patients (50%). Conclusion: In this single center real-life cohort, REG showed good efficacy (median OS not reached, PFS 5.7 months vs. 3. months in the RESORCE trial) and acceptable safety with highly frequent (80%), but mostly low-grade AE. Despite one death, no cessation of treatment due to AE was necessary. Figure: 6
162 P09-03YI PREDICTORS OF RECURRENCE AND SURVIVAL OF HEPATOCELLULAR CARCINOMA: PROSPECTIVE STUDY INCLUDING TRANSIENT ELASTOGRAPHY AND CANCER STEM CELL MARKERS Ashraf Omar, Mohamed Nabil, Tamer Elbaz, Ahmed Abdelmaksoud 2, Hend Shousha, Zeinab Abdellatif, Ghada Habib, Rabab Omar Faculty of medicine, Cairo university, endemic medicine and hepatogastroenterology department, Cairo, Egypt, 2 Faculty of medicine, Cairo university, diagnostic and interventional radiology department, Cairo, Egypt Background and Aim: Hepatocellular carcinoma is associated with high recurrence rates, even after radical treatment. Transient elastography is reliable in assessing liver stiffness (LS). Cancer Stem Cells (CSC) such as Ep-CAM and cytokeratin-9 are indicators of tumor aggressiveness. Aim: to investigate whether LS and CSCs could predict HCC recurrence post-ablation (complete response; following the modified Response Evaluation Criteria in Solid Tumor) and their impact on clinical outcome and overall survival. Method: A prospective study that included 79 HCV-related HCC patients. HCCs were ablated according to BCLC guidelines. All patients performed transient elastography and serum CSCs before and 6 months post treatment. We compared patients with complete and partial ablation. Follow up of patients with complete ablation and their sub-analysis as recurrent and non-recurrent groups were done. We looked for predictors of recurrence and Kaplan-Meier survival analysis. Results: Studied patients (n=79) were predominantly males aged 59.7±6.3 years. The majority were Child Pugh A (74.9%). Tumors were mostly single (54.7%) located in right lobe (60.9%) and median size of tumor was 4cm. TACE was the commonest line of management (79.8%). Complete ablation was achieved in 97 patients; 55 of them developed HCC recurrence. Post treatment, LS increased significantly while significant reduction of CSCs levels occurred in both complete and partial ablation groups. Median time to recurrence: 4 months. LS increased significantly post ablation in patients with recurrence versus no recurrence. Although CSCs markers declined in both recurrence and nonrecurrence groups, higher levels were recorded at baseline and post ablation in patients with recurrence but without statistical significance. Cox regression analysis for prediction of recurrence determined low platelet count and baseline CK-9 levels. Univariate analysis for prediction of overall survival mentioned many significant factors including LS and EpCAM (baseline and posttreatment) while multivariate analysis limited factors to Child score B and partial ablation. Conclusion: Dynamic changes occurred in LS and CSCs in response to complete ablation and tumor recurrence. Low platelet count and baseline CK-9 significantly correlated with recurrence while Child score and partial ablation significantly affected survival. 62
163 Figure: LIVER STIFFNESS Baseline 3-months LS P value Recurrence 25.5 ( ) ( ) No recurrence 22.8 (4.8-32) 20.5 ( ) Baseline 6-months LS Recurrence 25 ( ) 28 ( ) No recurrence 22.8 ( ) 20.9 ( ) 0.7 Recurrence Baseline After treatment EPCAM 366 ( ) 250 (5-324) CK-9 62 (48-84.) 44. ( ) <0.00 <0.00 No recurrence EPCAM (94-533) CK ( ) 98.5 (7-35) ( ) <0.00 <

164 P09-04YI EPITHELIAL-TO-MESENCHYMAL TRANSITION INDUCED DRUG RESISTANCE IN HEPATOCELLULAR CARCINOMA DERIVED CANCER STEM CELLS Ritu Shrestha 2 3, Haolu Wang 3, Prashanth Prithviraj 4, Xiawoen Liang 3, Kim Bridle 2, Darrell Crawford 2, Haotian Yang 3, Aparna Jayachandran 2 3 University of Queensland, Faculty of Medicine, Australia, 2 Greenslopes Private Hospital, Gallipoli Medical Research Foundation, Australia, 3 University of Queensland Diamantina Institute, TRI, Australia, 4 Fiona Elsey Cancer Research Institute, Australia Background and Aims: The global burden of Hepatocellular carcinoma (HCC) is increasing partly due to the limited treatment options available for this disease and recurrence due to therapy resistance. Epithelial-to-mesenchymal transition (EMT) responsible for emergence of cancer stem cells (CSCs) is implicated as the mechanism of therapy resistance in cancers including HCC. The aim of this study is to enrich and purify CSCs from human and murine HCC cell lines and to examine the relationship between therapy resistance and EMT properties of CSCs. Method: A modified sphere forming serum-free culture system was used to enrich stem-like cells from a panel of human and mouse derived HCC cell lines which were assessed by stemness and CSC markers and high resolution multiphoton fluorescence lifetime imaging (MPM-FLIM). The effect of anticancer drugs Cisplatin, Doxorubicn, 5-Flurouracil and Sorafenib were assessed by MTS assay. EMT traits were assessed via immunofluorescence localization of putative EMT markers including E- cadherin, Vimentin, Fibronectin, ZO- and Snail. Colony forming and motility assays were used to examine the relationship between drug resistant CSCs and EMT. Using bioinformatics platform SurvExpress, HCC patient datasets were probed to examine the clinical relevance of our findings. Results: Three-dimensional spheres that expressed enhanced stemness markers CD33 and CD44 compared to parental cells grown as adherent cultures were enriched. Subsequently, using MPM-FLIM we assessed the levels of metabolic coenzymes that are informative in comparing the cellular metabolic rates between CSCs and parental cell populations. CSCs showed significantly higher cell viability to cytotoxic drugs. The downregulation of E-Cadherin and ZO- along with upregulation of Vimentin, Fibronectin and Snail in CSCs supports the role of EMT in emergence of drug resistant CSCs. The CSCs were more motile and aggressive as per motility assay indicating the association of EMT with drug resistant CSCs in HCC. The HCC patient datasets showed that expression of EMT markers resulted in worse overall survival and recurrence free survival further supporting the link of EMT to therapy resistance in HCC. Conclusion: Our study highlights the role of EMT as a key driver for drug resistance in HCC. CSCs that exhibit distinctive EMT markers can be potentially utilized as biomarkers to stratify HCC patients and also may serve as druggable targets of HCC. Figure: 64
165 P09-05YI S00A IS PART OF A WHOLE NETWORK OF TUMOR SUPPRESSORS AND ONCOGENES DEREGULATED EARLY WITH HEPATIC STEATOSIS AND CONTRIBUTING TO HEPATOCELLULAR CARCINOMA DEVELOPMENT Cyril Sobolewski, Abegg Daniel 2, Flavien Berthou, Nicolas Calo, Christine Sempoux 3, Anne- Sophie Ay, Pierre Clavien 4, Humar Bostjan 4, Dufour Jean-Francois 5, Adibekian Alexander 6, Michelangelo Foti Faculty of Medicine, University of Geneva, Dept of Cell Physiology and Metabolism, Geneva,, 2 Faculty of Sciences, University of Geneva, Dept of Organic Chemistry, Geneva,, 3 Lausanne University Hospital, Pathology, Lausanne, Switzerland, 4 University Hospital Zurich, Department of Surgery, Zurich, Switzerland, 5 University of Berne, Hepatology, Department of Clinical Research, Berne, Switzerland, 6 Faculty of Sciences, University of Geneva, Dept of Organic Chemistry, Geneva, Switzerland Background and Aims: Hepatocellular carcinoma (HCC) develops frequently in the context of fatty liver disease (FLD) with distinct etiologies. Genetic mutations of tumor suppressor (TS) and oncogenes (ONC) have been widely characterized in HCC. However, increasing evidence indicate that deregulations of the activity/expression of TS/ONCs may also occur with FLD independently of specific mutations. This study aimed at uncovering and characterizing major TS and ONC deregulated at early stages of FLD and potentially fostering hepatocarcinogenesis Method: Hepatic tissues from a mouse model of FLD spontaneously progressing towards the development of HCC (hepatocyte-specific PTEN knockout, LPTENKO mice) were used to identify through unbiased LC-MS/MS spectrometry, deregulations of TS and ONC occurring with steatosis. Expression of TS/ONC identified by mass spectrometry were then investigated in hepatic tissues of various mouse models of FLD, in mouse/human cancer cells and in HCC Human Tissue Microarrays. S00A functions in carcinogenesis were examined in vitro using human HepG2 cells. Results: Proteomic analyses of steatotic hepatic tissues from LPTENKO mice identified a network of more than 30 TS/ONC respectively down- or up- regulated in early stages of FLD. Alterations of these TS/ONC expression were further confirmed in various diet-induced and genetic mouse models of hepatic steatosis and were found to be present also in genetically- and carcinogen-induced HCC in mice. Among these TS/ONC, S00A was upregulated with hepatic steatosis and further increased in mouse HCC. The relevance of S00A overexpression was further confirmed in human hepatic cancer cells, as well as in human HCC tissues, where it correlates in particular with HCC grade II-III. Finally, in vitro analyses showed that inhibition of S00A expression in hepatic cancer cells leads to decreased cell proliferation, upregulation of cell cycle inhibitors, induction of cell death, as well as inhibition of cell migration and invasion. Conclusion: Our findings indicate that deregulation of a whole network of TS/ONCs, which may foster hepatocarcinogenesis, occurs early with steatosis. Among this deregulated network of cancer-related factors, S00a has relevant oncogenic functions in HCC and might represent both a target and a risk factor biomarker for high grade HCC development. 65
166 P09-06YI EVALUATION OF THE SINGLE AND MULTIPLE NATURAL RASS PREVALENCE IN THE MAIN HCV GENOTYPES IN ITALIAN COURT Maria Chiara Sorbo, Valeria Cento 2, Ada Bertoli 2, Francesca Ceccherini-Silberstein 2, Carlo Federico Perno 2 Università degli Studi di Roma Tor Vergata, Rome, Italy, 2 Università degli Studi di Roma Tor Vergata Aim: Natural resistance-associated substitutions (RASs) show highly variable prevalence across different HCV genotypes (GTs)/subtypes. This work investigate the natural RASs frequency, and NS5A- RASs role on treatment efficacy, in a large real-life database including the 4 main HCV-GTs circulating in Italy. Methods: RASs in NS3 (N=032), NS5A (N=833) and NS5B (N=496) were analysed in 93 HCVinfected DAAs-naïve patients (pts). Sanger-sequencing was performed by home-made protocols on 74 GTa, 989 GTb, 35 GT2c, 333 GT3a, 24 GT4a and 66 GT4d samples. RASs with fold-change >00 were defined as major. Results: Overall, 45/93 (35%) pts showed natural RASs, independently by cirrhosis, but with differences for GT/subtypes. GTa-b-4a frequently showed NS3 RASs ( %, respectively), with high prevalence of 80K in GTa (7%). Major RASs 68A/E/T/V had 3% prevalence in GT2c and 4% in GT4d. Also in NS5A, GTa-b-4a showed the highest prevalence of RASs (0-3-38%, respectively) with major RASs detected in 0% GTa (28V, 30H/R, 3M, 93C/H), 9% GTb (30R, 93H), 5% GT2c (3M, 93H), 4% GT3a (93H) and 2% GT4d (30S).The most common major NS5A RAS was 93H. In NS5B, the major sofosbuvir 282T RAS was never found, while the putative RASs 59F and 36N were exclusively detected in GTb (3% and 9%) often in association (phy=0.67, p<0.00 by covariation analysis). Notably, this pattern was more present in interferon+ribavirin-experienced (7-%, respectively), than in naïve pts (3-4%; p=0.07 and p=0.02, respectively). 0% of 372 pts with resistance test in all 3 genes showed multiple RASs, with NS3+NS5A RASs as the most prevalent association (3%, mainly GT and 4). Only 2 GTb pts showed RASs on all 3 drug targets. In 38 pts treated with a NS5Ainhibitor, the potential role of natural NS5A-RASs was evaluated. Among 26 non-cirrhotic pts, 4 with baseline minor NS5A RASs reached a sustained viral response (SVR2). 4/2 cirrhotic pts, showed major NS5A RASs;two of them, (GTb:93H; GT4d:30S) treated with not-recommended regimens, without ribavirin, failed; the other 2 (GTb:93H; GTa:30R) receiving a recommended-regimen with ribavirin reached SVR. Conclusions: Natural RASs are common across all HCV-GTs, and up to 0% of pts show multipleclass resistance, though only the major mutations with a probable clinical relevance. Therefore, the qualitative identification mainly of major natural RASs and their correct evaluation is required to properly guide DAA-based therapy. 66
167 P09-07 PROGNOSTIC EFFECT OF YTTRIUM-90 RADIOEMBOLIZATION FOR HEPATOCELLULAR CARCINOMA WITH PORTAL VEIN INVASION Carlo Sposito, Carlo Spreafico 2, Marta Vaiani 2, Tommaso Cascella 2, Sherrie Bhoori 3, Carlo Morosi 2, Rodolfo Lanocita 2, Raffaele Romito 4, Carlo Chiesa 5, Marco Maccauro 5, Marta Mira 5, Alfonso Marchiano 2, Vincenzo Mazzaferro 3 Fondazione IRCCS Istituto Nazionale Tumori, GI Surgery and Liver Transplantation, Milan, Italy, 2 Fondazione IRCCS Istituto Nazionale Tumori, Radiology, Milan,, 3 Fondazione IRCCS Istituto Nazionale Tumori, GI Surgery and Liver Transplantation, Milan,, 4 Ospedale Maggiore di Novara, Chirurgia Generale 2, Novara, Italy, 5 Fondazione IRCCS Istituto Nazionale Tumori, Nuclear Medicine, Milan, Background and Aims: Yttrium-90 trans-arterial radioembolization (TARE) has shown promising efficacy in the treatment of patients with hepatocellular carcinoma (HCC) associated with tumoral portal vein thrombosis (PVTT). Aim of this study is to identify prognostic factors for survival in patients with HCC and PVTT undergoing TARE, and build a prognostic classification for these patients. Method: This is a single Center retrospective study conducted over 6 years ( ), on consecutive patients undergoing TARE. Patients were included if they met the following criteria: presence of at least one measurable HCC, presence of PVTT not occluding the main portal trunk, absence of extra-hepatic metastases, Child-Pugh score within B7, ECOG performance status 0-. Uni- and multivariable analysis was used to explore the variables that showed an independent relationship with survival. A prognostic score was then derived, and three prognostic categories were identified. Results: A total of 20 patients were included in the study. Median OS was 4. months (95%CI: ) and median PFS was 6.5 months (95%CI: ). The only variables independently correlated with OS were bilirubin, extension of PVTT and tumor burden. Three prognostic categories were identified: favourable prognosis (0 points), intermediate prognosis (2-3 points) and dismal prognosis (> 3 points). Median OS in the three categories was 32.2 months, 4.9 months and 7.8 months respectively (p<.000). Also PFS (p=.045) and risk of liver decompensation (p<.000) significantly differed along the same prognostic categories. Conclusion: Radioembolization with Yttrium-90 is an effective therapy for patients with HCC and PVTT. The proposed prognostic stratification may help to better identify good candidates for the treatment, and those for whom TARE may be futile. 67
168 Figure: Proposed point system according to β regression coefficients of the final Cox model built on the three variables independently related to post-tare patients survival. Overall survival according to prognostic stratification. 68
169 P09-08YI EARLY DETECTION OF HEPATOCELLULAR CARCINOMA IN CIRRHOTIC LIVER MODEL IN MRI USING IRON DOPED NANO-CALCIUM PHOSPHATE CONTRAST AGENT Anusha Ashokan, Badrinathan Sridharan, Rupal Jobanputra, Siddaramana Gowd Genekehal, Ida M Anna, Vijay Harish Somasundaram, Sivanarayanan T B 2, Unni A.K.K. 2, Shantikumar Nair, Manzoor Koyakutty Amrita Institute of Medical Sciences and Research Centre, Amrita Vishwa Vidhayapeetham University, Amrita Centre for Nanosciences and Molecular Medicine, Kochi, India, 2 Amrita Institute of Medical Sciences and Research Centre, Amrita Vishwa Vidhayapeetham University, Central Animal Facility, Kochi, India Background and Aims: Management of Hepatocellular Carcinoma (HCC) primarily depend on image based diagnosis which has to be specific and timely. Ambiguity with certain other liver lesions makes non-invasive Magnetic Resonance Imaging (MRI) based diagnosis of HCC, a challenging affair for the medical experts. A contrast agent with better biocompatibility has become an absolute requirement, since Super Paramagnetic Iron Oxide Nanoparticles (SPIONs), an excellent T2 contrast agent, has been withheld from the global market due to toxicity concerns. Here we report a novel T2 contrast agent based on biomineral calcium phosphate nanoparticles (ncp) for Reticulo-Endothelial system (RES) based T2 contrast enhancement. Method: Doped ncp was synthesized and characterized to study the size and structural properties using DLS, SEM and EDAX mapping. To study the contrast properties of doped ncp, Cirrhotic model was indued with Thioacetamide (300 mg/l mixed in drinking water) and orthotopic HCC model was developed in Sprague-Dawley rats using NS rat hepatoma cell lines. The characterized nano-contrast agent was administered through intravenous injection at a concentration of 20 mg/kg of body weight and the tumor was visualized in 7T animal MRI station. Results: Doped ncp showed a particle size of around 6 nm and a substantial colloid stability for a period of 48 hrs. SEM analyses showed spherical shape of particles while elemental analyses showed 0% Fe doping in ncp. Significant reduction in T2 contrast of normal liver surrounding the tumor resulted in contrast enhancement of HCC nodule (< cm) in rat NS HCC model and in cirrhotic model with NS HCC nodules. Histological observations showed cirrhosis and HCC were progressed significantly and were in concordance with the MR observations. Clearance studies revealed that ncp showed a complete biological elimination by the end of 96 hours from normal animals, whereas SPIONs showed prolonged retention up to one month in liver. This findings were supported by histological sections of the liver stained with H & E and Prussian blue dyes. Liver function test or ROS generation studies showed no significant toxicity issues with ncp. Conclusion: Based on the results, we propose that doped calcium phosphate nanoparticle can be considered as a prospective nano-contrast agent for detection of small HCC nodules in the background of cirrhosis. Acknowledgements Authors thank Nanobiotechnology-task force, DBT Govt. of India for funding the project entitled Translational Development of Protein nanomedicine and calcium phosphate nanocontrast agent, Project No: BT/PK 7665/NNT/28/658/203 Authors are grateful to Amrita University for the infrastructure support. 69
170 P09-0YI DISSECTING THE SPATIAL HETEROGENEITY OF CIRCULATING TUMOR CELLS REVEALS CCL5-TREG MEDIATED IMMUNE EVASION IN HEPATOCELLULAR CARCINOMA Yunfan Sun, Xin-Rong Yang, Jia Fan Liver Cancer Institute, Department of Liver Surgery, Zhongshan Hospital, Fudan University, Shanghai, China Background and Aims: The prognosis of hepatocellular carcinoma (HCC) is closely linked to the occurrence of recurrent, metastatic disease, which has been proposed to be initiated by circulating tumor cells (CTCs); however, the transcriptomic plasticity and adaptive mechanisms of CTCs in systemic circulation are not well defined. Method: Blood was drawn from four key vascular sites along the dissemination route in ten HCC patients, including hepatic vein (HV), peripheral artery (PA), peripheral vein (PV) and portal vein (PoV). Single CTCs were isolated by negative enrichment and robotic micromanipulator, followed by single-cell full-length RNA sequencing. The results of single-cell RNA sequencing were validated in three independent HCC cohorts. In vitro and in vivo assays were performed to investigate the CCL5 mediated immune evasion mechanism of CTCs via recruitment of regulatory T cells. Results: We established single-cell RNA-sequencing profiles of 3 CTCs isolated from four key vascular sites along the dissemination route in ten HCC patients. In our study, we found that single CTCs displayed profound spatial transcriptional heterogeneity within the circulatory system, which is associated with increased transcriptional activity, cell cycle progression, and chemokine-induced immune escape programs. In particular, CTCs dynamically drove chemokine (C-C motif) ligand 5 (CCL5) expression over the course of circulation. We demonstrated that increased CCL5 expression in turn recruited regulatory T cells to facilitate immune evasion and metastatic progression, as rigorously validated by our in vitro and in vivo models. Finally, we identified an inherently dormant CTC subset with an epithelial-mesenchymal transition and immune-evasive phenotype, and demonstrated its potential prognostic implications. Conclusion: Collectively, our results reveal the previously unappreciated spatial heterogeneity of CTCs, and define its role in immune-regulatory programs and cellular states. Our study offers new insight into metastatic mechanisms, highlighting the potential utility of anti-ctc therapeutic strategies. 70
171 P09-YI IMPACT OF REGORAFENIB IN THE CLINICAL PRACTICE AND IDENTIFICATION OF THE SECOND-LINE TREATMENT ORPHAN PATIENTS Marco Sanduzzi Zamparelli, Víctor Sapena, Álvaro Díaz-Gonzázlez, Anna Darnell 2, Neus Llarch, Ernest Belmonte 3, Loreto Boix, Gemma Iserte, Alejandro Forner, Josep Corominas, Leonardo Gomes Da Fonseca, Carmen Ayuso 2, María Reig, Jordi Bruix Hospital Clínic de Barcelona. IDIBAPS. CIBERehd., BCLC group. Liver Unit., Barcelona, Spain, 2 Hospital Clínic de Barcelona. CIBERehd. Universitat de Barcelona., BCLC group. Radiology department., Barcelona, Spain, 3 Hospital Clínic de Barcelona. IDIBAPS. CIBERehd., BCLC group. Radiology department., Barcelona, Spain Background and Aims: The RESORCE study showed that regorafenib provides a significant benefit in terms of overall survival (OS) to patients with hepatocellular carcinoma (HCC) who tolerated sorafenib (400 mg/day) and presented radiologic progression. Data on regorafenib treatment in clinical practice are scarce and the percentage of patient candidates or orphans of effective second-line treatment is unknown. The purpose of this study was to investigate the feasibility and tolerance of regorafenib in clinical practice and to evaluate the proportion of patients who can benefit from it. Method: we analysed a prospective database of patients with HCC treated with sorafenib to investigate the regorafenib applicability and assessed the outcome of patients that have received this novel option. This includes 9 patients [5 within the research trials and 4 under compassionate use]. All patients started at 60 mg/day. Treatment was continued until symptomatic progression, unacceptable adverse events or patient decision. Results: Eighty of the 299 patients treated with sorafenib were alive at the time of regorafenib availability, 2/80 continued on sorafenib and 59 definitively discontinued (4 due to toxicity, 7 for tumor progression and because of patient decision). 23% (4/59) of the patient who discontinued sorafenib started regorafenib and 4/7 (82.35%) with tumor progression started regorfenib. Among all the patients treated with regorafenib 85% were BCLC-C with the tumor progression pattern of: 5% BCLCp- B (n=3), 35% BCLCp-C (n=7) and 50% BCLCp-C2 (n=0). The median follow-up was 9.9 and 5.6 months for the research and clinical practice patients respectively. /20 patients have died (range 3-32 months). The median time to st dose modification was 3.8 days and modifications were due to: fatigue (n=4), skin reaction (n=4) and diarrhoea (n=3). Seven of the 8 patients who discontinued regorafenib did so because of symptomatic progression. Conclusion: Since regorafenib approval for HCC, the number of patients treated with regorafenib is low but data on the tolerability and survival reproduce the RESORCE results even if presenting the poor prognosis pattern (50% BCLCp-C2). More than half of the patients treated with sorafenib are a potential candidate for regorafenib, although a relevant number of patients remains orphan for effective secondline treatment. 7
172 P09-2 IFN-FREE DAA TREATMENT OF CIRRHOTIC HCV PATIENTS WITH OR WITHOUT HISTORY OF HCC: A MULTICENTER PROSPECTIVE TRIAL IN ITALY Angelo Sangiovanni, Eleonora Alimenti, Michele Barone 2, Luca Saverio Belli 3, Elia Biganzoli 4, Guglielmo Borgia 5, Matteo Brunacci 6, Maurizia Brunetto 7, Roberta D'ambrosio, Silvia Fargion 8, Roberto Filomia 9, Martina Gambato 0, Roberto Gattai 7, Edoardo Giovanni Giannini 6, Sergio Maimone 9, Luca Marzi, Filippo Oliveri 7, Elisabetta Parente 2, Gaia Pellegatta 6, Giovanni Raimondo 9, Maria Grazia Rumi 2, Francesco Paolo Russo 0, Ilaria Serio 3, Natalia Terreni 4, Luca Valenti 8, Erica Villa, Pietro Lampertico Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Università degli Studi di Milano, CRC A.M. and A. Migliavacca for Liver Disease, Division of Gastroenterology and Hepatology, Milano, Italy, 2 University of Bari, Gastroenterology Unit, Department of Emergency and Organ Transplantation (D.E.T.O.), Bari, Italy, 3 Ospedale Niguarda, UOC Epatologia e Gastroenterologia, Milan, Italy, 4 IRCCS Istituto Nazionale Tumori, Unit of Medical Statistics, biometry and bioinformatics, Milan, Italy, 5 University of Naples 'Federico II', Department of Clinical Medicine and Surgery, Section of Infectious Diseases, Naples, Italy, 6 University of Genoa, Gastroenterology Unit, Department of Internal Medicine, Genoa, Italy, 7 University Hospital of Pisa, Hepatology Unit and Laboratory of Molecular Genetics and Pathology of Hepatitis Viruses, Pisa, Italy, 8 Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico, Università degli Studi di Milano, Internal Medicine and Metabolic Diseases, Milan, Italy, 9 University Hospital of Messina, Division of Clinical and Molecular Hepatology, Messina, Italy, 0 Padua University Hospital, Multivisceral Transplant Unit, Department of Surgery, Oncology, and Gastroenterology, Padua, Italy, Azienda Ospedaliero-Universitaria Policlinico di Modena, Gastroenterology Unit, Modena, Italy, 2 Ospedale San Giuseppe, Università degli Studi di Milano, Division of Hepatology, Milan, Italy, 3 University of Bologna, Department of Medical and Surgical Sciences, Bologna, Italy, 4 Valduce Hospital, Division of Gastroenterology, Como, Italy Background and Aims: Whether sustained virologic response (SVR) to Interferon (IFN) free direct antiviral agents (DAAs) therapy is associated with an increased risk of developing HCC is a matter of debate. Aim of this study was to evaluate whether the incidence of de novo or recurrent HCC increases after starting DAA treatment and which variables are associated with HCC development. Method: In a multicenter prospective cohort enrolled between Jun. 204 and Sep. 207, 028 consecutive HCV cirrhotic patients with no history of HCC, and 20 consecutive patients with radiological complete response to HCC treatment were treated with IFN-free DAA. SVR was obtained in 957 (97%) cirrhotic patients (Group ): 559 (58%) males, median age 66 years (22-85), pending SVR in 36 cases and in (96%) patients with HCC (Group 2): 75 (68%) males, median age 74 yrs (46-86), pending SVR in 5 cases. Time from last imaging and last HCC treatment, age, gender, Child, AFP, HCV GT, presence of undefined/non-malignant liver nodules, duration of DAA therapy, were considered. Hazard rate analysis on time was performed to assess instant HCC incidence and recurrence, comparing values across the entire follow-up with flexible non-parametric smoothing techniques and parametric survival. Multivariable Cox regression analysis was performed to assess the association of variables with HCC development and recurrence. Results: In SVR patients, during a median follow-up of 65 wks (range -74) 33 de novo HCC occurred in Group (9/93 in cirrhotic patients with undefined/non-malignant nodules before starting DAA), corresponding to a mean annual incidence of 3.% (2.5% in patients without undefined/non-malignant liver nodules and 7.8% in patients with such nodules, p=0.002), and during a median follow up of 50 wks (range 4-28) 3 HCC recurred in Group 2, corresponding to a mean annual incidence of 29%. Looking to smoothed estimation, an underlying non monotonic trend was observed in both groups with an increase of HCC instant incidence at 43 wks in Group (at 50 weeks in patients without undefined/non-malignant liver nodules and at 8 weeks in patients with such nodules) and at 35 weeks in Group 2. By multivariable Cox regression models, the presence of undefined/non-malignant hepatic nodules (HR= 3. CI.5-6.9, p=0.003, with a time dependent relation, and Child-Pugh (HR=.6, 95% CI.2-2., p=0.00) were associated with de novo HCC incidence in Group, while no variables showed evidence of association with HCC recurrence. 72
173 Conclusion: In HCV cirrhotic patients SVR to IFN-free DAA treatment, a progressive decrease of de novo HCC incidence was observed after an increased number of HCC at 43 weeks after starting DAA in patients without history of HCC, associated to the presence of undefined/non malignant liver nodules. A transient increased incidence of recurrent HCC was observed at 35 weeks after stating DAA in patients with history of HCC. 73
174 P0-0 SUPERIORITY OF MULTIPLE RANDOM GENE SETS IN PREDICTING SURVIVAL OF PATIENTS WITH HEPATOCELLULAR CARCINOMA Timo Itzel 2, Rainer Spang 3, Thorsten Maass 4, Stefan Munker 5, Hans Jürgen Schlitt 6, Wolfgang Herr 7, Matthias Evert 8, Andreas Teufel 2 Department of Medicine II, Division of Clinical Bioinformatics, Heidelberg University, Medical Faculty Mannheim, Mannheim, Germany, 2 Department of Medicine II, Division of Hepatology, Heidelberg University, Medical Faculty Mannheim, Mannheim, Germany, 3 Department of Functional Genomics, Statistical Bioinformatics, University Medical Center, Regensburg, Germany, 4 Hepacult GmbH, 5 Department of Medicine II, Großhadern University Medical Center, Ludwig Maximilians University, München, Germany, 6 Department of Surgery, University Medical Center, Regensburg, Germany, 7 Department of Medicine III, University Medical Center, Regensburg, Germany, 8 Department of Pathology, University of Regensburg, Regensburg, Germany Background and Aims: Despite multiple publications, molecular signatures predicting the course of hepatocellular carcinoma (HCC) have not yet been integrated into clinical routine decision making. Given the diversity of signatures published throughout the past decade, optimal number, best combinations, and benefit of functional associations of genes in prognostic signatures still remain to be defined. Method: We investigated a vast number of randomly chosen gene sets (varying between and genes) in order to encompass the full range of prognostic gene sets on 242 transcriptomic profiles of patients with HCC. Results: Depending on the selected size, 4.7 to 23.5% of all random gene sets exhibit prognostic potential by separating patient subgroups with significantly diverse survival. This was further substantiated by investigating gene sets and signaling pathways also resulting in a comparable high number of significantly prognostic gene sets. However, combining multiple random gene sets using swarm intelligence resulted in a significantly improved predictability for approximately 63% of all patients. In these patients, approx. 70% of all random 50-gene containing gene sets resulted in equal and stable prediction of survival. For all other patients a reliable prediction seems highly unlikely for any selected gene set. Using a machine learning and independent validation approach, we demonstrated a high reliability of random gene sets and swarm intelligence in HCC prognosis. Conclusion: In conclusion, we demonstrate that using swarm intelligence of multiple gene sets for prognosis prediction may not only be superior but also more robust for predictive purposes. 74
175 P0-02 CLINICALFEATURES OF HEPATOCELLULAR CARCINOMA IN THE ELDERLY IN A HEPATITIS B ENDEMICCOUNTRY - A COMPARATIVE STUDY OF 430 CASES Chang-Chuen Mark Cheah, Boon-Bee George Goh, Pik-Eu Jason Chang, Chee-Kiat Tan Singapore General Hospital, Department of Gastroenterology and Hepatology, Singapore Background and Aims: Patients with hepatitis B and C related hepatocellular carcinoma (HCC) commonly present between years old. Although hepatitis B is endemic in Singapore and is the main aetiology of HCC, we hypothesize that prevalence of hepatitis B related HCC is lower in our elderly (ELD) HCC patients as cryptogenic (commonly attributed to non-alcoholic steatohepatitis (NASH)) HCC becomes increasingly important. We also compared other clinical features and survival outcomes between ELD and non-eld patients. Method: The study cohort comprised 430 patients seen in the Department of Gastroenterology and Hepatology, Singapore General Hospital, prospectively enrolled in a HCC database since 988. The ELD group consisted of patients with HCC diagnosed at age 70 years or more. Demography, clinical characteristics and mortality data were compared between ELD and non-eld groups. Survival census was performed with the National Registry of Deaths on 3 October 205. Statistical and survival analyses were performed using SPSS. Study was approved by IRB. Results: There were 378 (26.4%) and 052 (73.6%) patients in ELD and non-eld groups respectively. Median age was 75 and 59 years respectively (p<0.00). There were significantly more female patients in ELD group (30.4% vs 3.8%, p<0.0). Hepatitis B was significantly less prevalent in ELD group (35.9% vs 68.5%, p<0.000). Conversely, cryptogenic (presumably NASH) HCC was significantly more prevalent in ELD group (27.3% vs %, p<0.000). There were significantly less Child Pugh A (CP-A) patients in ELD group (CP-A/B/C in ELD vs non-eld: 42%/44.3%/3.7% vs 53.6%/32.6%/3.8%, p<0.00). Single lesion HCC at presentation was more common in ELD group (55.8% vs 49.0%, p<0.05). There was no significant difference in BCLC staging between ELD and non-eld. Portal vein invasion was less common in ELD group (25.4% vs 35.6%, p <0.00). Mean±SEM survival of ELD was significantly lower than non-eld (23.8±2.67 vs 53.7±4.45 months, p<0.0). Conclusion: There were more female elderly patients with HCC compared with non-elderly patients. Cryptogenic (presumably NASH) HCC becomes more important in elderly patients. Elderly patients tended to have less aggressive disease with less multifocal disease and less portal vein invasion but still had poorer survival. Thus, the outcome of HCC is poorer and risk indicators associated with HCC in the elderly differ from our younger patients. This has implications in the surveillance for HCC in the elderly. 75
176 P0-03YI PREDICTION OF HEPATOCELLULAR CARCINOMA USING NON INVASIVE BIOMARKERS OF LIVER FIBROSIS: A RETROSPECTIVE STUDY OF 2363 PATIENTS Ashraf Omar, Dalia Omran, Mohamed Nabil, Ahmed Abdelmaksoud 2, Tamer Elbaz, Eman Medhat, Rania Leithy, Hend Shousha Faculty of medicine, Cairo university, endemic medicine and hepatogastroenterology department, Cairo, Egypt, 2 Faculty of medicine, Cairo university, diagnostic and interventional radiology department, Cairo, Egypt Background and Aims: Hepatocellular carcinoma (HCC) is the third leading cause of cancer deaths worldwide with poor prognosis. The risk of hepatocarcinogenesis depends on background liver factors, of which fibrosis is a major determinant. Serum markers and developed scores are of increasing importance in non-invasive diagnosis of hepatic fibrosis. Aim: to predict the occurrence of hepatocellular carcinoma in patients with advanced liver fibrosis using noninvasive fibrosis scores calculated using routine patients data. Method: A retrospective study included 29 HCC Egyptian patients (group ) recruited from multidisciplinary HCC clinic, Kasr Al-Aini hospital, Faculty of medicine, Cairo University in the period between February 2009 and June 206 and 072 patients (group 2) with chronic hepatitis C naïve patients with advanced fibrosis ( F3) and cirrhosis (F4). King, Fibro Q, Aspartate aminotransferase-toplatelet ratio index (APRI), AST to ALT ratio (AAR), LOK, Göteborg University Cirrhosis Index (GUCI), Fibro alpha and BRC scores were calculated for all patients. Regression analysis and receiver operator curves were plotted to assess the sensitivity, specificity and predictive values for the significant scores with the best cut-off for predicting HCC. Results: HCC group had significantly older patients 57.83±7.5 years than group 48.24±8.27 years (p= <0.00). There was highly significant difference between the 2 groups in all calculated scores (P=0.000). Our own score was calculated; an MHC-Egy Score (Logit probability of HCC = *age -0.2*Hb *INR.059*Alb+0.022*AFP *Sex. Male=, Female=0) with cut off of was superior to other scores for predicting HCC with a sensitivity of 90%, specificity of 80.6%. Conclusion: The HCC MHC Egy-Score is a promising, easily calculated, accurate, cost-effective score in the prediction of HCC on top of advanced liver fibrosis in chronic HCV patients. 76

177 Figure: Score Cut off Sensitivity Specificity AUC 95% confidence interval P-value Lower Bound Upper Bound King score Firo Q APRI AAR LOK score GUCI score Fibro-alpha BRC MHC-egy score <
178 P0-04 PERCUTANEOUS ELECTROCHEMOTHERAPY OF HEPATOCELLULAR CARCINOMA AT HEPATICHILUM Luciano Tarantino, Aurelio Nasto, Giuseppina Busto 2, Sara Bortone 3, Raffaele Fristachi 4, Luigi Cacace 2, Paolo Tarantino, Riccardo Aurelio Nasto 5, Maria Rosaria Romano 5 A.Tortora Cancer Hospital, Surgery, Pagani(SA), Italy, 2 A.Tortora Cancer Hospital, oncology, Pagani(SA), Italy, 3 A.Tortora Cancer Hospital, Radiology, Pagani(SA), Italy, 4 A.Tortora Cancer Hospital, AnatomoPathology, Pagani(SA), Italy, 5 A.Tortora Cancer Hospital, Anesthesiology, Pagani(SA), Italy Background and Aims: Thermal Ablation of Hepatocellular Carcinoma infiltrating the hepatic hilum (hh-hcc) is contraindicated because of possible severe thermal injury of main bile ducts, hepatic hilum vessels or duodenum. We evaluated the feasibility, efficacy and safety of Electrochemotherapy (ECT), a non-thermal ablation technique, in a series of patients with hh-hcc. Method: 5 patients (3M,2F; year, mean: 6 year), in Child-Pugh-A, 4 in Child-Pugh- B-class, with biopsy proven hh-hcc (diameter range: cm; mean: 3.6 cm) underwent ECT. Four to six electrode-needles connected to Cliniporator Vitae (IGEA SpA, Carpi, Modena, Italy), a pulse generator with 6 independently controlled and electrically isolated outputs, each providing up to 3000 Volts, were inserted percutaneously under US guidance along the external margin of hh-hcc. Eight minutes after intravenous bolus injection (5000 IU/m 2 ) of Bleomycine sulfate (Bleoprim, Sanofi Aventis, Paris, France), electric pulses were delivered. 9 patients had complete or partial portal vein tumor thrombosis (PVTT), 6 patients had a hh-hcc next to main portal vein bifurcation.. All patients underwent control of the efficacy by contrast-enhanced-mdct 4 weeks after treatment and follow-up CT controls every 6 months thereafter. Results: No perioperative major complication occurred. 2/5 (3%) patients died because of hemorrhage from GEV at 4 and 5 weeks after treatment. Post-treatment CT showed complete absence of enhancement of the treated nodule and/or PVTT in /3(85%) and partial necrosis in 2/3(5%) cases. The follow-up ranged from 5 to 36 months (median: 4 months). Follow-up-CT showed local progression of the tumor in the 2 cases of partial response. 4 patients dropped-out the follow-up at 6, 9, 0 and 2 months because of death from liver failure in 3 and hemorrhage from gastroaesophageal varices in case, respectively. In these 4 patients, 6-months-CT confirmed complete necrosis and absence of local recurrence. In the other 7 patients, no local recurrence was detected at CT during follow-up. During follow-up, intrahepatic recurrences in other segments were detected in 4/3 (3%)patients. Conclusion: ECT seems to be a feasible, safe and effective treatment for local control of hh-hcc. Because of a relative high risk (3%) of late post-operative hemorrage from GEV, patients with at-risk for bleeding varices should be excluded. 78
179 P0-05YI GP38+ HEPATIC PROGENITOR CELL-DERIVED EXTRACELLULAR VESICLES IN HCC AND BILIARY CANCER - A NOVEL LIQUID BIOPSY MARKER? Sabine Urban, Marcin Krawczyk 2, Arnulf Willms 3, Joanna Ligocka 4, Hanna Sänger, Krzysztof Jankowski 5, Marek Krawczyk 4, Krzysztof Zieniewicz 4, Waldemar Patkowski 5, Robert Schwab 3, Aliona Wöhler 3, Sebastian Gehlert 6, Jesus M. Banales 7, Piotr Milkiewicz 8 9, Frank Lammert, Miroslaw Kornek 3, Veronika Lukacs-Kornek Saarland University Medical Center, Saarland University, Department of Medicine II, Homburg, Germany, 2 Medical University of Warsaw, Laboratory of Metabolic Liver Diseases, Department of General, Transplant and Liver Surgery, Warsaw, Poland, 3 German Armed Forces Central Hospital, Department of General, Visceral and Thoracic Surgery, Koblenz, Germany, 4 Medical University of Warsaw, Department of General, Transplant and Liver Surgery, Warsaw, Poland, 5 Medical University of Warsaw, Department Internal Medicine and Cardiology, Warsaw, Poland, 6 Institute of Cardiovascular Research and Sport Medicine, German Sport University Cologne, Department of Molecular and Cellular Sport Medicine, Cologne, Germany, 7 Biodonostia Health Research Institute Donostia University Hospital, University of the Basque Country (UPV/EHU), CIBERehd, Ikerbasque, Department of Liver and Gastrointestinal Diseases, San Sebastian, Spain, 8 Medical University of Warsaw, Liver and Internal Medicine Unit, Department of General, Transplant and Liver Surgery, Warsaw, Poland, 9 Pomeranian Medical University, Translational Medicine Group, Szczecin, Poland Background and Aims: Large extracellular vesicles (EVs), so-called microparticles (MPs), are cellderived membrane vesicles that harbor the same surface antigens as their parental cells. Recently, we showed that tumor-associated MPs (tamps) could be useful for discriminating hepatic cancers from cirrhosis. To further distinguish between hepatocellular carcinoma (HCC) and biliary cancer (cholangiocarcinoma (CCA) and gallbladder carcinoma (GbC)), we employed this minimal-invasive MP approach with surface marker compositions based on gp38/podoplanin, a recently described novel marker for liver progenitor cell subpopulations (Eckert. C. et al. 206 AJP, Lukacs-Kornek et al. 207 JHEP). Method: The presence of gp38+ progenitor cells was confirmed in various organs in wild type C57Bl/6J mice by FACS. TaMPs from patients sera were isolated by sequential ultracentrifugation at 2,000 and 20,000xg. To identify tamp populations, FACS was applied. In total, 43 HCC and 9 biliary cancer patients were enrolled in the study accompanied by 47 cirrhosis patients and 46 healthy individuals that served as controls. Results: i) Recently described liver progenitor marker gp38 was evaluated in additional organs in order to assess its potential use as a biomarker for discriminating HCC from biliary cancer. Indeed, gp38+epcam+ and gp38+epcam+cd33+ cells were found in murine liver and lung but were absent in gallbladder. ii) AnnexinV+EpCAM+ASGPR+ tamps pinpointed liver cancers (HCC and CCA) and distinguished these from cirrhosis. Of note, gp38 in the combinations AnnexinV+gp38+EpCAM+ and AnnexinV+gp38+EpCAM+CD33+ identified tamps that allowed the distinction of HCC from biliary cancer. In detail, AnnexinV+gp38+EpCAM+ tamps were increased in biliary cancer patients by 6.5-fold as compared to HCC patients. AUROC value (0.798), sensitivity (80%), specificity (65%) as well as positive predictive value (83%) indicated their diagnostic value as a novel biomarker for discriminating HCC from biliary cancer. AnnexinV+gp38+EpCAM+CD33+ tamps confirmed our differentiation between HCC and biliary cancer patients, albeit with slightly lower diagnostic accuracy. Conclusion: Our results provide evidence that the novel progenitor marker gp38/podoplanin in the combination AnnexinV+gp38+EpCAM+ identifies tamps that serve as a novel, minimal invasive biomarker for discriminating HCC from biliary cancer. Acknowledgement: Communities and patients, Ministries of health and partner of different sites. Funding: Unitaid 79
180 P0-06YI UBIQUITIN CARBOXY-TERMINAL HYDROLASE L INHIBITION AS A POTENTIAL STRATEGY TO MODULATE THE SORAFENIB RESPONSE OF HEPATOCELLULAR CARCINOMA. Astrid Vandierendonck, Lindsey Devisscher, Helena Degroote, Sanne Van Campenhout, Francesca Fornari 2, Marleen Van Troys 3, Christophe Ampe 3, Xavier Verhelst 4, Anja Geerts 4, Yves- Paul Vandewynckel 4, Hans Van Vlierberghe 4 Ghent University, Department of Gastroenterology and Hepatology, Ghent, Belgium, 2 S.Orsola- Malpighi, Pad. 20, Lab. CRBA, Universitá di Bologna, Department of Medical and Surgical Sciences, Bologna, Italy, 3 Ghent University, Department of Biochemistry, Ghent, Belgium, 4 Ghent University, Department of Gastroenterology and Hepatology, Ghent, Belgium Background and Aims: Hepatocellular carcinoma (HCC) is the second leading cause of cancer-related mortality worldwide. Merely 30-40% of patients are eligible for curative treatments 2. For advanced HCC, systemic therapy with the oral multi-tyrosine kinase inhibitor sorafenib (SFN) remains the golden standard 3. However, efficacy is limited with a mean overall survival benefit of 3 months and adverse events occur frequently 4. Consequently, alternative treatment options or treatment strategies combining SFN with targeted compounds are an unmet medical need 5,6. Here, we investigated the potential of Ubiquitin carboxy-terminal hydrolase L (UCHL) inhibition to modulate the SFN response of HCC. Method: For the expression study of UCHL, 2 micro-array datasets (GSE59259, GSE46408) of human HCC and corresponding non-neoplastic liver tissue were analysed and RT-qPCR was performed on livers of rats and mice with diethylnitrosamine (DEN)-induced HCC. The effect of the UCHL inhibitor LDN57444 (LDN) on tumour cell viability upon SFN treatment was analysed in Hep3B cells by MTT and LDH assays. The capacity of solitary tumour cells to produce progeny (i.e. reproductive viability), a proposed cancer stem cell (CSC) feature, was assessed via a colony formation assay 7. Upon multifocal HCC induction with DEN for 25 weeks 8, mice were treated with SFN (0 mg/kg/day, n=7), LDN (0.4 mg/kg biweekly, n=7), combined therapy (n=7) or vehicle (n=6) for 5 weeks. Results: Micro-array analysis showed that UCHL expression is significantly increased in human HCC A. This was confirmed by RT-qPCR in a DEN-induced HCC rat and mouse model B,C. In vitro combinational treatment of SFN with UCHL inhibition significantly enhances loss of viability, induced apoptosis and subsequent loss of cell integrity compared to both monotherapies D,E. Furthermore, SFN-enabled reproductive viability can be suppressed by LDN F. In vivo, SFN treatment improves the survival of mice with HCC and similar survival benefits can be reached with combinational therapy G. Conclusion: UCHL expression is upregulated in both human and experimental HCC and its inhibition enhances the in vitro anti-tumour efficacy of SFN. Furthermore, UCHL inhibition reverses SFN-induced reproductive viability, which suggests UCHL inhibition abolishes the induction of CSC features by SFN. Further studies will have to reveal if this strategy reduces other SFN-induced resistance and stemness features and its efficacy on tumorigenicity in vivo. 80
181 Figure: 8
182 P0-07YI LARGE UNRESECTABLE HEPATOCELLULAR CARCINOMA: EFFICACY OF PERCUTANEOUS THERMAL ABLATION AFTER OCCLUSION OF TUMOR BLOOD SUPPLY BY GELFOAM. Letizia Veronese, Francesca Torello Viera, Laura Rosa, Luisa Siciliani, Lorenzo Moramarco 2, Nicola Cionfoli 2, Pietro Quaretti 2, Valentina Ravetta Fondazione IRCCS Policlinico San Matteo, III Department of Internal Medicine- Interventional Ultrasound, Pavia, Italy, 2 Fondazione IRCCS Policlinico San Matteo, Radiodiagnostic- Interventional Radiology, Pavia, Italy Background and Aims: To evaluate the usefulness of percutaneous thermal ablation (TA) after occlusion of the tumor arterial supply for treatment of large unresectable hepatocellular carcinoma (HCC). Method: One hundred forty-four cirrhotic patients (33 F, M) with a median age of 7±9 years (range, years) with biopsy-proven HCC larger than 3.0 cm (mean diameter, 4.7 cm; range, cm) underwent the TA procedure(s) after interruption of the tumor arterial supply by occluding the feeding arteries with gelfoam (TAE). The results of TAE plus TA were classified as complete responses (CRs), defined as a non-enhancing area corresponding in shape to the treated HCC at computed tomography or magnetic resonance imaging, or treatment failures. Results: Ninety-four (65.3%) patients had a single nodule while 26 (8.%) had double and 24 (6.6%) had three nodules in the same hepatic lobe. Therefore, two hundred eighteen nodules underwent treatment. CRs were obtained in 56 nodules (7.5%). No procedure-related deaths occurred in 44 TAE plus TA sessions. Major complications were observed in 20 patients (3.9%). During a median follow-up of 37.5 months (range, 8-42 months), local recurrence was observed in 4 nodules (8.8%), while non-local recurrences were detected in 73 patients (50.6%). Estimated 3-and 5-year overall survival rates were 55.0% and 25.%, respectively. Conclusion: TA after occlusion of the HCC arterial supply resulted in a large volume of thermal necrosis selectively involving tumor tissue and sparing surrounding non-tumoral tissue. Therefore this technique is useful for treatment of large unresectable HCC nodule in cirrhosis. 82
183 P0-08 THE MELD SCORE IS POSITIVELY CORRELATED WITH NEUTROPHIL TO LYMPHOCYTE RATIO AND RED BLOOD CELL DISTRIBUTION IN ASSESSMENT OF MORTALITY NAS RECURRENCE IN PATIENTS WITH HEPATOCELLULAR CARCINOMA AFTER LIVING DONOR LIVER TRANSPLANTATION Chih-Chi Wang, Chih-Che Lin, Kuang-Den Chen 2, Kuang-Tzu Huang 2, Chun-Hsien Wu 2, Tsan- Shiun Lin 2, Shih-Ho Wang 3, Chee-Chien Yong 3, Ting-Lung Lin 2, Yu-Hung Lin 3, Chao-Long Chen 2 Kaohsiung Chang Gung Memorial Hospital, Surgery, Kaohsiung, Taiwan, 2 Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan, 2 Kaohsiung Chang Gung Memorial Hospital, Kaohsiung, Taiwan Background and Aims: The host inflammatory response is well-known in playing an important role in carcinogenesis and disease progression. One of the famous examples called neutrophil to lymphocyte ratio (NLR) has been investigated for the prognostic role in cancer patients. However, few studies have examined the relationship between NLR and hepatocellular carcinoma (HCC) prognosis after liver transplantation (LT), and the detailed molecular mechanism of NLR in the LT process still unclear. The aim of this study is to investigate the clinical significance and related biochemical features of RDW, its relations to NLR, and the potential underlying mechanism which may impact survival of HCC patients after LT. Method: Patients with HCC were divided into high NLR and low NLR to compare the cumulative survival rates, recurrence, the blood biochemical datasets and the model for end-stage liver disease (MELD) scores. Next gene sequencing (NGS) analysis was performed for finding the NLR-related mrna or mirna, and real-time PCR for validation. HCC cell line, Hep3B, and immortalized human T lymphocyte cells, Jurkat, were applied to investigate the effect of NLR-related factor on cancer and immune cell in variety of mechanism. Results: High post-lt NLR is associated with significantly higher MELD scores/decompensated cirrhosis, elevated RDW, poor survival and HCC recurrence. In NGS results, the expressions of mrna and mirna e.g. SLC3A, IL7D, PLAC4, SLAMF9, mir-35a-5p, and mir-490-3p etc., which are concerning cancer or immune system but undetermined in HCC, was found to have obvious variation between different NLR s condition. After validation by real-time PCR, PLAC4 and mir-35a were selected, and the effect in proliferation, migration, apoptosis and autophagy of cancer or immune cell will be further analyzed. Conclusion: This study demonstrated a potent linkage of NLR to cancer and immune cell through pathological gene regulation which could be initiated during HCC progression. Further examine NLRrelated factors in cell model to explore potential mechanism is needed. 83
184 P0-09 YAP DRIVES CHROMOSOMAL INSTABILITY IN HCC PATIENTS,WHICH CORRELATES WITH CLINICAL AND MOLECULAR PATIENT FEATURES Sofia Weiler, Federico Pinna, Thomas Wolf, Aman Geldiyev 2, Vladimir Ustiyan 3, Peter Schirmacher 4, Vladimir Kalinichenko 3, Kai Breuhahn 4 Institute of Pathology, Heidelberg,, 2 International Educational-Scientific Center, Ashgabat City, Turkmenistan, 3 Cincinnati Children's Hospital Medical Center, Division of Pulmonary Biology, Cincinnati, United States, 4 Institute of Pathology, Heidelberg, Germany Background and Aims: Chromosomal instability (CIN) is a hallmark of cancer but little is known about the factors leading to its development. The Hippo pathway effector Yes-associated protein (YAP) has been described as an oncogene in liver cancer, promoting hepatomegaly and HCC formation when overexpressed in transgenic mice. However, the downstream effector mechanisms of YAP are not well understood and therefore the role of YAP in the development of chromosomal instability was analysed. Method: Transcriptomic data from HCC patients (n=370) were analysed for expression of a CIN signature (CIN25) and correlated with clinical patient data. Using liver cancer cells lines, YAPdependency of CIN signature genes was investigated using sirna inhibitions. YAP-transgenic mice were used to assess markers of CIN. Tissue-microarrays of human HCC patients (n=05) were analysed for correlations between YAP and CIN signature genes. Results: HCC patients are characterized by the expression of a CIN signature which correlates with poor patient prognosis. YAP together with the transcription factors TEAD4 and FOXM induces CIN gene expression in liver cancer cells and the overexpression of constitutively active YAP in transgenic mice leads to CIN development. The inhibition of the downstream effector FOXM blocks YAPdependent hepatomegaly and CIN development in YAP-transgenic mice. Moreover, human HCC patients show a positive correlation between YAP enrichment and CIN gene expression. Analysis of clinical data further revealed that YAP-induced CIN signature expression is higher in patients with poor tumor grading, high serum α-fetoprotein levels and Asian origin. Mutations in TP53 are also positively correlated with CIN signature expression whereas CTNNB mutations show an inverse correlation. Conclusion: YAP-dependent expression of CIN signature genes characterizes HCC patients with poor prognosis. Based on clinical and molecular parameters patients could be identified that may benefit from YAP/FOXM-targeted therapies. 84
185 P0-0 PORTAL VEIN TUMOR THROMBOSIS HAS A DIRECT IMPACT ON LIVER FUNCTION Arndt Weinmann, Verena Steinle 2, Sandra Koch 3, Roman Klöckner 2, Sebastian Schotten 2, Aline Maehringer-Kunz 2, Christoph Düber 2, Hauke Lang 4, Dirk Graafen 2, Franziska Meyer 2, Jens Marquardt, Marcus-Alexander Wörns, Peter Galle University Medical Center of the Johannes Gutenberg University, Department of Medicine I, Mainz, Germany, 2 University Medical Center of the Johannes Gutenberg University, Department of Diagnostic and Interventional Radiology, Mainz, Germany, 3 University Medical Center of the Johannes Gutenberg University, Clinical Registry Unit, Mainz, Germany, 4 University Medical Center of the Johannes Gutenberg University, Allgemein-, Viszeral- und Transplantationschirurgie, Mainz, Germany Background and Aims: Portal vein tumor thrombosis (PVTT) has a significant impact on the prognosis of patients with hepatocellular carcinoma (HCC). However, the mechanisms leading to shorter survival of such patients are still unknown. According to our clinical experience, the liver function deteriorates in such patients, considerably limiting treatment options. Aim of this study was to quantify liver function impairment due to newly diagnosed PVTT. Method: A total of 478 patients with proven HCC were treated in our tertiary referral center between 0/2005 0/207. As we aimed for an intraindividual comparison to minimize confounding factors, we only included patients with a newly diagnosed PVTT during the observation period. Inclusion criteria were: proven HCC; PVTT-negative CT or MRI followed by at least one PVTT-positive CT or MRI; availability of all laboratory values needed to calculate Model for End-Stage Liver Disease (MELD)-, and Albumin-Bilirubin (ALBI)- score. Albumin, AST, bilirubin, MELD-, and ALBI-score were calculated before and after the diagnosis of PVTT. PVTT was diagnosed in consensus by re-evaluation of all available CT- or MRI-studies by two board certified radiologists experienced in abdominal oncologic imaging. Results: In total, 34 patients developed a new PVTT during the observation period. Between the last PVTT-negative imaging and the first PVTT-positive imaging, AST increased from 74.8 to 95.4U/l (p=0.005), bilirubin from.53 to 2.04mg/dl (p=0.004), MELD from 0.4 to.3 points (p=0.006), and ALBI from 2.0 to 2.2 points (p=0.026). Albumin decreased from 32.8 to 30.4g/l (p=0.002). Conclusion: New PVTT is associated with a significant impairment of liver function, considerably limiting treatment options. Therefore, meticulous evaluation of cross-sectional imaging is crucial for the clinical management of patients with HCC. 85
186 P0-YI REGISTRATION OF COMPLETE RESPONSE TO CHEMOEMBOLIZATION AT 2 AND 6 MONTHS AVOIDS >0% OF FOLLOW-UP ANGIOGRAPHIES AND PERMITS AN EFFECTIVE TRANSITION INTO SYSTEMIC THERAPY UPON PROGRESSION, THUS ENSURING OPTIMAL SURVIVAL Marco Sanduzzi Zamparelli, Marta Burrel 2, Anna Darnell 3, Víctor Sapena, Marta Barrufet 2, Alejandro Sotomayor 2, Neus Llarch, Gemma Iserte, Álvaro Díaz-Gonzázlez, Ernest Belmonte 4, Alejandro Forner, Jordi Rimola 3, Carmen Ayuso 3, María Reig, Jordi Bruix Hospital Clínic de Barcelona. IDIBAPS. CIBERehd., BCLC group. Liver Unit., Barcelona, Spain, 2 Hospital Clínic de Barcelona., BCLC group. Radiology department., Barcelona, Spain, 3 Hospital Clínic de Barcelona. CIBERehd. Universitat de Barcelona., BCLC group. Radiology department., Barcelona, Spain, 4 Hospital Clínic de Barcelona. IDIBAPS. CIBERehd., BCLC group. Radiology department., Barcelona, Spain Background and Aims: Chemoembolization (TACE) is the recommended treatment for patients with hepatocellular carcinoma (HCC) at BCLC-B stage or BCLC-0/A without other options. After initial response, TACE can be performed on-demand based on the tumor evolution or at regular intervals. Usually, TACE is performed at 0, 2 months and then at 6 months, but solid data on the benefit/needs/applicability of TACE at month 2 or on the possibility to avoid the second TACE after registering radiologic complete response (CR) after the st session are still lacking. Furthermore, it is controversial if a 6 month interval is appropriate or what proportion of patients cannot be treated because of exceeding the criteria for the treatment. The aim of this study was to evaluate -if CR after the st TACE predicts the tumor de-vascularization and the futility of the 2nd TACE at month 2, -the percentage of patients who develop untreatable-progression revealed by the regular interval schedule and - validation of the currently expected overall survival (OS) Method: Between 0/204-3/207, 06 patients (HCV 5.89%, Child-Pugh-A 92.45% y BCLC-A/B 43.4/56.6%) were included. Three DCBeads-TACE (0/2/6 months) were scheduled and performed according to the radiologic and angiographic findings during the follow-up Results: Ninety-six patients (90.6%) had at least TACE, but this was not pursued in 0. The 2nd TACE was not performed in 3 patients due to no active tumor recognition (all but also registered at pre-angiography CT), while this was also the case for 4 patients at 3rd TACE. Seven patients were transplanted and 39 had untreatable-progression [20.8 % BCLC-B stage (n=22), 0.3% en BCLC-C stage (n=) and 5.6% BCLC-D stage (n=6)]. Thirty-five of 44 patients (80%) who suspended TACE started systemic treatment with sorafenib. Twenty-one patients have died after a median follow-up of 9.3 months. Median OS censoring at application of other treatment or liver transplantation was 44 months (42.6 months without censoring). Conclusion: Registration of CR at CT post st TACE may avoid the need of a 2nd or 3rd TACE during follow-up. The 0/2/6 month schedule with CT assessment at these time points allows that 80% of the patients with untreatable progression may effectively transition to systemic treatment and this strategy translates into a median OS 40 months. 86
187 P0-2 CHANGES OF AFP AND PIVKA-II LEVELS DURING DAA TREATMENT AND THEIR PREDICTIVE VALUE FOR EARLY DIAGNOSIS OF HCC IN HCV CIRRHOTIC PATIENTS WITH SVR TO DAA TREATMENT Angelo Sangiovanni, Roberta D'ambrosio, Giovanna Lunghi 2, Mariangela Bruccoleri, Eleonora Alimenti, Marta Borghi, Riccardo Perbellini, Alessio Aghemo 3, Massimo Iavarone, Massimo Colombo 3, Pietro Lampertico Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico - University of Milan, CRC A.M. and A. Migliavacca for Liver Disease, Division of Gastroenterology and Hepatology, Milan, Italy, 2 Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico - University of Milan, Virology Unit, Milan, Italy, 3 Humanitas Research Hospital, Center for Translational Hepatology Research, Rozzano, Italy Background and Aims: Serum markers for the diagnosis of hepatocellular carcinoma (HCC) were withdrawn as diagnostic tool from Western Scientific Society recommendations because of scanty performance,. However, there is no data on sensitivity and specificity of tumor markers in HCV patients with sustained virological response (SVR) to direct antiviral agents (DAA) treatment. Aim of this study was to evaluate whether serum values of AFP and PIVKA-II change after treatment with DAA and the diagnostic performance of these markers for the diagnosis of HCC in HCV cirrhotic patients with SVR. Method: In a single centre case-control study we selected :3 30 cirrhotic HCV patients with HCC developed after starting DAA treatment (Group ) and 90 cirrhotic patients (Group 2) with no history of HCC, who did not developed HCC after starting DAA during a follow up of 6 months (range 5-27). Patients were matched for age (median 65 yrs, range 43-86), gender (76% males), BMI (median 24.9, range ) and Child-Pugh (89% Child A, % Child B). HCCs were 26 (88%) BCLC 0-A, 2 (6%) BCLC B, 2 (6%) BCLC C. HCC developed after a median time of 0 months (range 2) after starting DAA. AFP and PIVKA-II were tested at DAA starting and at SVR in group 2 and at HCC diagnosis in group. AFP 20 ng/ml and PIVKA-II 80 mau/ml were used ad a cutoff for calculating sensitivity, specificity, PPV, NPV and diagnostic accuracy of tumor markers, alone or combined, for the diagnosis of HCC after DAA treatment. Results: In cirrhotic patients with no HCC AFP median values significantly fell from 4 ng/ml at DAA starting to 6 ng/ml at SVR (p <0.000), while PIVKA-II remained unchanged (35 vs. 35 mau/ml, p=0.84). At SVR, AFP and PIVKA-II were significantly lower in cirrhotic patients with no HCC than in HCC patients (AFP 6 vs. 0 ng/ml, p=0.002 and PIVKA-II 35 vs 64.5 mau/ml, p<0.000, respectively). AFP 20 ng/ml and PIVKA-II 80 mau/ml were in (%) and 8 (9%) cirrhotics and 7 (23%) and 4 (47%) HCCs, respectively. Sensitivity of AFP and PIVKA-II at SVR were 25%, 47%, specificity 98%, 9%, PPV 80% and 64%, NPV 80% and 84%, diagnostic accuracy 80%, 80%, respectively. Using combined tumor markers, specificity and PPV improved to 00% with a sensitivity, NPV and diagnostic accuracy of 7%, 78% and 79% respectively. Conclusion: AFP but not PIVKA-II serum value significantly decreased after DAA treatment in cirrhotic patients at SVR. The combination of different tumor markers achieves absolute specificity for the diagnosis of HCC. Implementation of tumor markers should be considered in International Scientific Society recommendations for the diagnosis of HCC in HCV patients with SVR to DAA. 87
188 P-0 HEPAMINE - A LIVER DISEASE MICROARRAY DATABASE, VISUALIZATION PLATFORM AND DATA-MINING RESOURCE Timo Itzel 2, Matthias Evert 3, Andreas Teufel 2 Department of Medicine II, Division of Hepatology, Heidelberg University, Medical Faculty Mannheim, Mannheim, Germany, 2 Department of Medicine II, Division of Clinical Bioinformatics, Heidelberg University, Medical Faculty Mannheim, Mannheim, Germany, 3 Department of Pathology, University of Regensburg, Regensburg, Germany Background and Aims: Throughout the past two decades, numerous gene expression profiling data on literally all liver diseases were generated and stored in public databases. These data are thought to contain deep insights into the molecular development of liver diseases, support the development of molecular diagnostics and ultimately promote precision medicine in hepatology. However, once published the majority of these data remain idle. Only very few data were used for additional analyses or comparative projects by the hepatology research community. This may mostly be due to the limited bioinformatics knowledge on how to obtain and analyze the stored raw data by most biomedical research personnel. In order to overcome this barrier and to support an easy translation of bioinformatics data into translational hepatology research, we created Hepamine, a liver disease microarray database, visualization platform and data-mining resource. Method: Microarray data were obtained from the ArrayExpress Archive of Functional Genomics Data ( Pre-analysis of expression data was performed using R statistical software and microarray analysis packages from the Bioconductor repository ( Expression data were stored locally in a postgresql database. Results: We have generated Hepamine, a web-based repository of pre-analyzed microarray data for various liver diseases. Among these are HCC, CCC, liver fibrosis/cirrhosis, chronic hepatitis, autoimmune liver disease, fatty liver disease and many more. At its initial release Hepamine contains 4 gene expression datasets, 2 microarray experiments and roughly half a million gene expression measurements. A self-explanatory website offers open and easy access to the respective gene expression profiles and support to compare samples, experiments and various liver diseases. Genes may be searched on the basis of specific expression patterns across diverse samples. Results are furthermore visualized in simple three color tables indicating up-, down-, or no differential expression in multiple experiments. To enlarge the scope of the Hepamine, all data were linked to common functional and genetic databases, in particular offering information on the respective gene, signaling pathway analysis and evaluation of biological functions by means of gene ontologies. Conclusion: Hepamine provides comprehensive data and easy access to various hepatologic gene expression data. It will open this widely unused resource particularly to hepatologists without bioinformatics or microarray profiling experience and substantially facilitate the translation of these data to molecular hepatology research. Hepamine is accessible at: 88
189 P-02YI CHARACTERIZATION OF HBV INTEGRATION LANDSCAPE IN TUMOR AND NON-TUMOR LIVER TISSUES BY A HIGH-THROUGHPUT VIRAL INTEGRATION DETECTION APPROACH Deborah D'aliberti, Domenico Giosa, Giuseppina Raffa, Cristina Musolino, Gianluca Tripodi, Daniele Lombardo, Francesca Casuscelli DI Tocco, Carlo Saitta 2, Orazio Romeo 3, Giuseppe Navarra 4, Giovanni Raimondo 5, Teresa Pollicino 4 University Hospital of Messina, Clinical and Experimental Medicine, Messina, Italy, 2 University Hospital of Messina, Internal Medicine, Messina, Italy, 3 University of Messina, Dipartimento di Scienze Chimiche, Biologiche, Farmaceutiche ed Ambientali, Messina, Italy, 4 University Hospital of Messina, Human Pathology, Messina, Italy, 5 University Hospital of Messina, Clinical and Experimental Medicine Background and Aims: Most data on HBV integration were generated by methods that favor preferential amplification and bias identification of unique integration sites (UISs). The recent nextgeneration sequencing (NGS) approaches showed a low-coverage of HBV reads. Aims of this study were (a) to conduct a high-throughput viral integration analysis on tumor (T) and non-tumor (NT) liver tissues, and on PLC/PRF/5 cells, using NGS of enriched HBV integrants, (b) to characterize the HBV DNA integration events, (c) to identify host/hbv junctures at the whole-transcriptome level. Method: DNA was fragmented by sonication, blunted, adenosine-tailed and ligated to linkers. Virus integrations were recovered by PCR using 24 different HBV-primers covering the whole viral genome. Amplicons were subjected to paired-end sequencing on Illumina-MiSeq. RNA-Seq was performed on Illumina-HiSeq High-quality reads were mapped against hybrid reference including the human genome reference GRCh38.p0 and HBV genome (NC_003977). Results: We detected 4,984 HBV integration breakpoints [4,09 in T and 862 in NT tissues (P=0.0), 3 in PLC/PRF/5 cells]. Among them, 2,04 were mapped to UISs [,684 in T and 350 in NT tissues (P=0.0), 7 in cells), 697 to intragenic region (575 in T and 20 in NT tissues (P=0.0), 2 in cells), 252 to exons [222 in T and 30 in NT (P=0.00), 0 in cells], and 2,943 to repetitive DNA sequences (2,425 in T and 52 in NT tissues (P=0.0), 6 in cells) [SINE (35,7%), simple repeats (25,7%), LINE (7,8%) and LTR (2,6%)]. An enrichment of microhomology (MH) sequences between host DNA and HBV integrants was found in most of the chimeras. Clonal expansion of HBV-integrated hepatocytes was more frequent in T tissues. Most of the HBV integrants contained pres-s and ENHI/X promoter region sequences. RNA-Seq confirmed the production of viral/human fusion transcripts (HBs-CCDC57 in PLC/PRF/5 cells, HBx-LINE/L and HBs-PTPRD in 2 different T tissue samples) Conclusion: We developed a high-throughput HBV-integration detection method that allows to characterize thoroughly the HBV integration landscape and to identify viral-human chimeric fusion genes that may be involved in HCC development. MH seems to be a major mechanism implicated in HBV integration that preferentially occurs into repetitive DNA sequences. HBV integration in exons is significantly higher in tumors as compared with non-tumor tissues. 89
190 P-03YI ROLE OF SERUM AMYLOID A AND LONG NON-CODING RNA AF AS DIAGNOSTIC BIOMARKERS FOR HEPATITIS B AND C RELATED HEPATOCELLULAR CARCINOMA Ashraf Omar, Dina Sabry 2, Hend Shousha, Moataz Maher Kamel 2, Mohamed Nabil, Tamer Elbaz, Ahmed Abdelmaksoud 3, Abeer Abdelkader 2 Faculty of medicine, Cairo university, endemic medicine department, Cairo, Egypt, 2 Faculty of medicine, Cairo university, Medical Biochemistry and Molecular Biology, Cairo, Egypt, 3 Faculty of medicine, Cairo university, diagnostic and interventional radiology department, Cairo, Egypt Background and Aims: Hepatocellular carcinoma (HCC) is the second most common neoplasm in Egypt. Chronic infection by hepatitis viruses especially HBV and HCV leads to a complicated microenvironment and consequently hepatocarcinogenesis. Long non-coding (Lnc) RNAs and serum Amyloid A (SAA) have been suggested to have role in tumorigenesis and progression. Aim: to study the role of Lnc RNA AF and SAA as a diagnostic biomarkers in sera of HBV, HCV, HCC patients. Method: Serum level of SAA was assessed by ELISA and Lnc RNA AF expression by Quantitative RT-PCR of 49 patients (all patients were naïve to antiviral and HCC treatment). They were divided into; 35 HCV-related HCC patients and 24 HBV-related HCC patients, 35 HBV-related cirrhosis and 35 HCV-related cirrhosis and 20 healthy controls. Results: The level of LncRNA-AF and SAA were significantly higher in HCC patients, cirrhotic HCV and HBV compared to controls (p-value <0.00). Higher expressions of Lnc RNA-AF and SAA were observed in HCC patients than in cirrhotic HCV and HBV. To determine the best cut-off for HCC detection, ROC curves was designed, and revealed 4.5 as the best cut-off for Lnc RNA AF with AUC= 0.999, CI = , sensitivity 00% and specificity 95%). ROC curve for SAA revealed 2.9ng/ml as the best cut-off for HCC detection with AUC= 0.927, CI = , sensitivity 87.8% and specificity 87.8%. ROC curve for SAA in HBV patients revealed 3.85 ng/ml as the best cut-off for HCC detection with AUC 0.740, CI = , sensitivity 69.6% and specificity 78.9%. ROC curve also revealed 20.5 as the best cut-off for Lnc RNA AF in HBV patients with AUC= 0.93, CI = 0.862, sensitivity 78.3% and specificity 00%. There was a negative correlation between AST and LNC RNA AF in HCV related HCC patients, r =0.493, p-value Conclusion: Lnc RNA-AF and SAA are promising potential biomarkers for HCV and HBV related HCC. Figure: control group HCV related cirrhosis HCV related HCC P value Long non coding RNA 2.52± ± ±4.8 <0.00 SAA (ng/ml).38± ± ±.76 <0.00 control group HCV related cirrhosis HCV related HCC Long non coding RNA 2.52± ±.26.74±2.77 <0.00 SAA (ng/ml).38± ± ±.06 <0.00 Data are presented as mean ±standard deviation 90

191 Figure: ROC curve for detection of cancer from hepatitis B using serum amyloid A Figure: ROC curve for detection of cancer from hepatitis B using long non coding RNA AF
192 P-04YI EXOSOME-TRANSMITTED CIRCRNA_04797 SUSTAINS SORAFENIB RESISTANCE IN HEPATOCELLULAR CARCINOMA Junjie Xu, Xiao Liang 2, Yuelong Liang 2, Xiujun Cai 2 Key Laboratory of Endoscopic Technique Research of Zhejiang Province, Department of General Surgery, Sir Run-Run Shaw Hospital, Zhejiang University,, Hangzhou, China, 2 Key Laboratory of Endoscopic Technique Research of Zhejiang Province, Department of General Surgery, Sir Run-Run Shaw Hospital, Zhejiang University, Hangzhou, China Background and Aims: Accumulating studies have suggested the primary and acquired resistance of Sorafenib in HCC with multiple molecular, cellular and microenvironmental mechanisms, which demands further improvement of Sorafenib therapy. Method: In vitro and in vivo experiments were performed and clinical samples and online databases were acquired for clinical investigation. Results: Sorafenib resistance up-regulated circrna_04797 could be transmitted by exosomes and responsible for the spread of Sorafenib resistance among HCC cells. CircRNA_04797 was critical for Sorafenib resistance maintenance and silencing circrna_04797 could substantially increase the efficacy of Sorafenib by inducing apoptosis. In vivo experiments portrayed a promising clinical application by locally injection of in vivo-grade sirna for circrna_04797 by TACE or other manners, which could intensively enhance Sorafenib efficacy in HCC patients. Conclusion: The clinical application of in vivo-grade sirna for circrna_04797 in Sorafenib treated HCC patients might shed bright future for the management of advanced HCC. 92

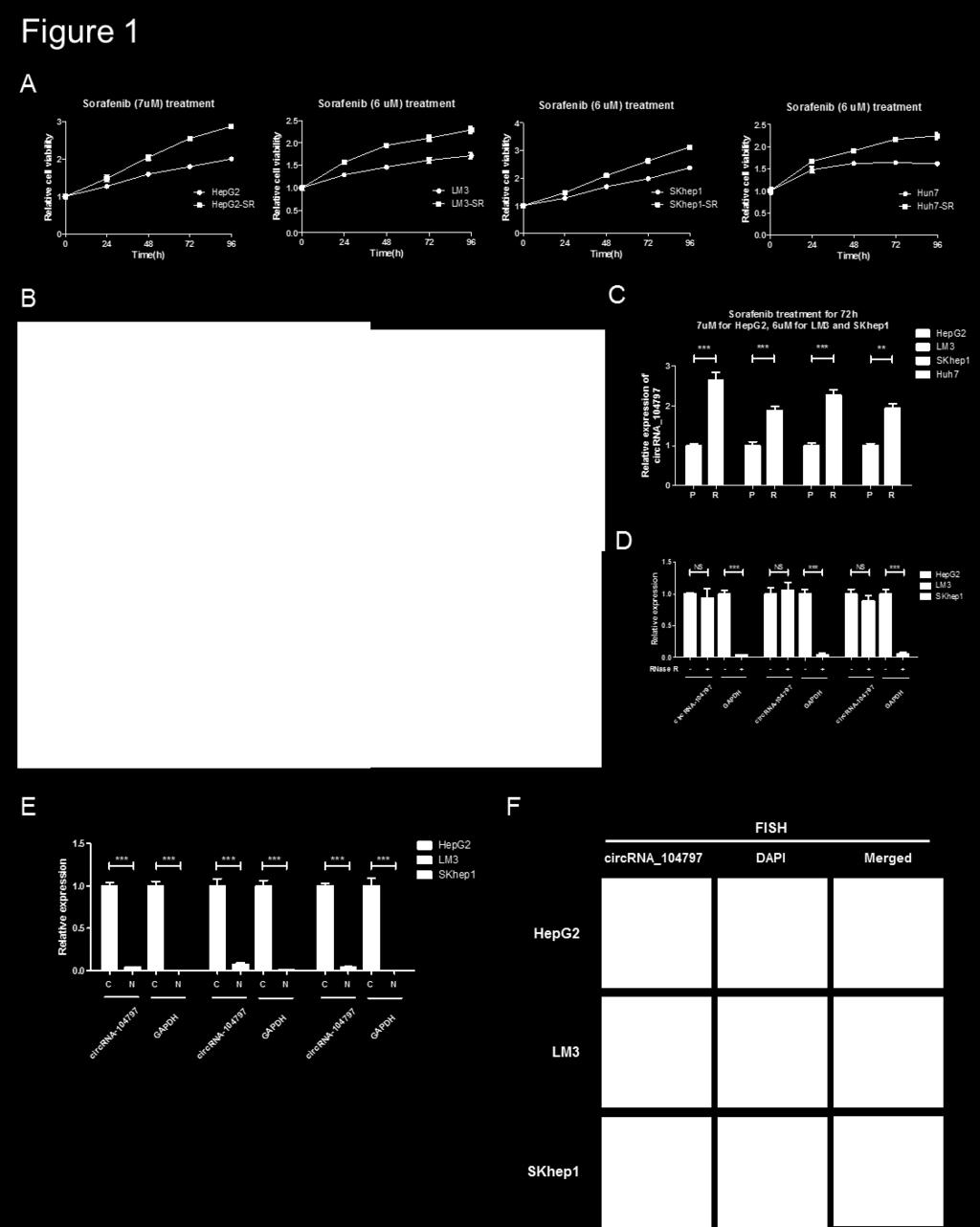
193 Figure: 93
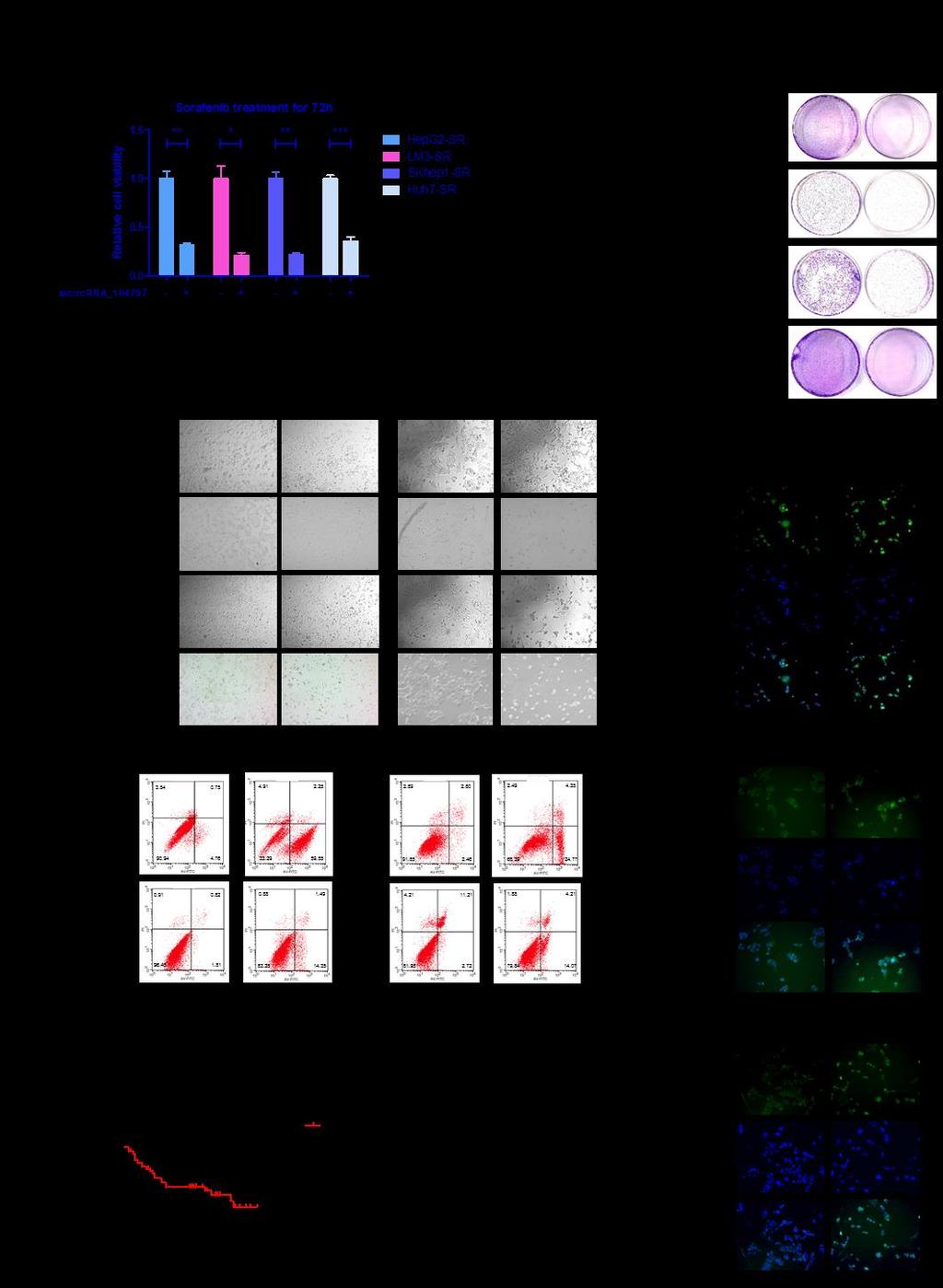
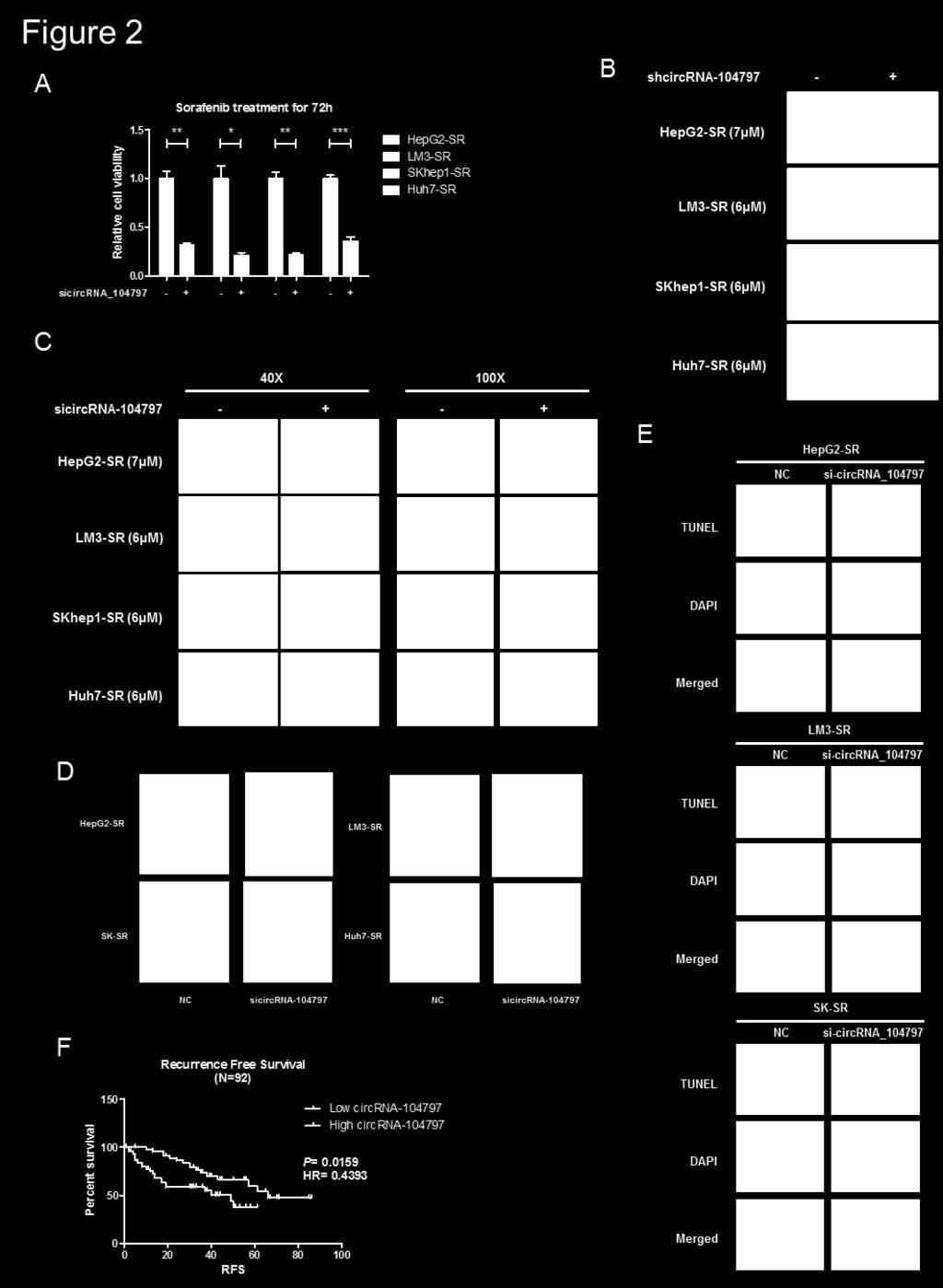
194 94
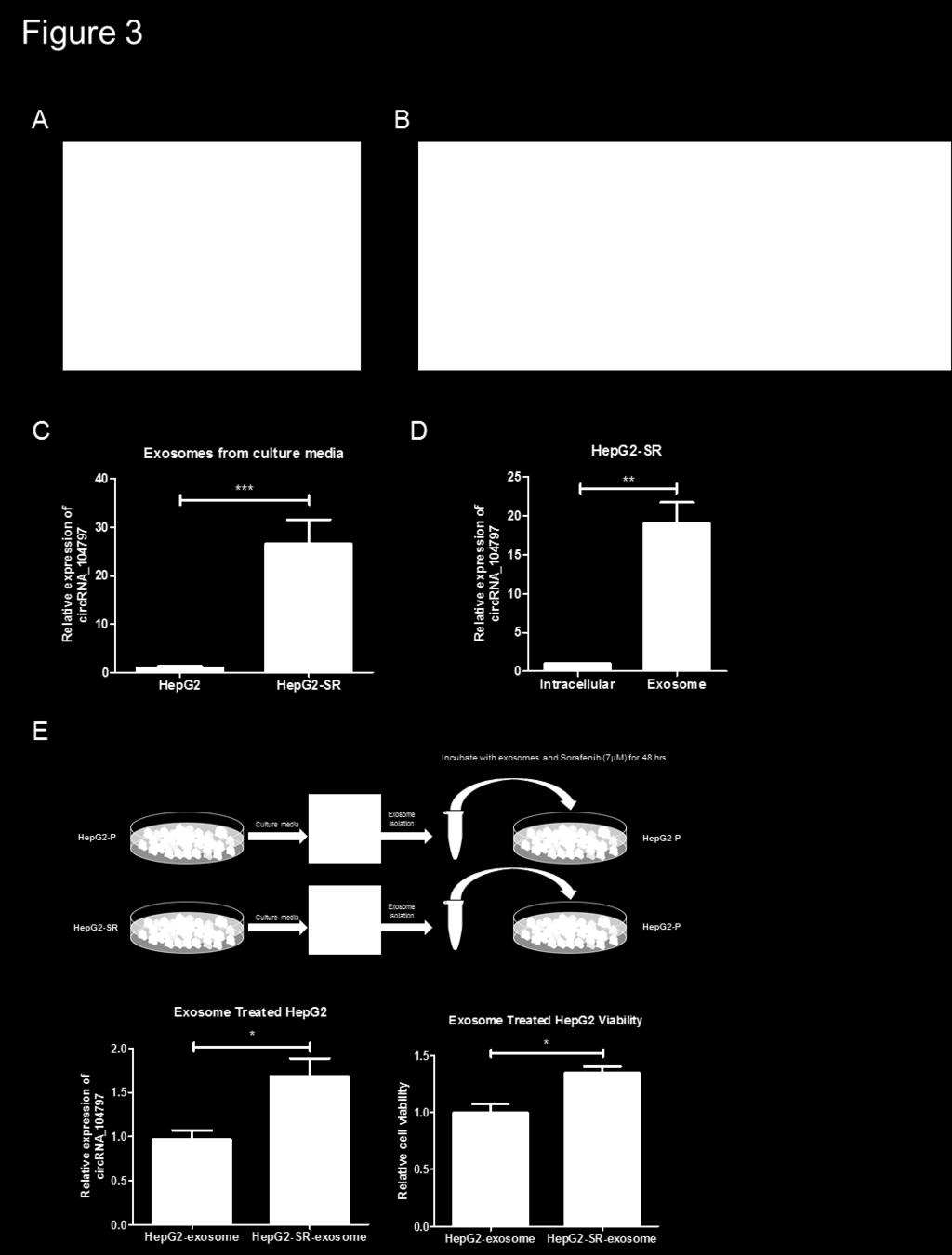
195 95
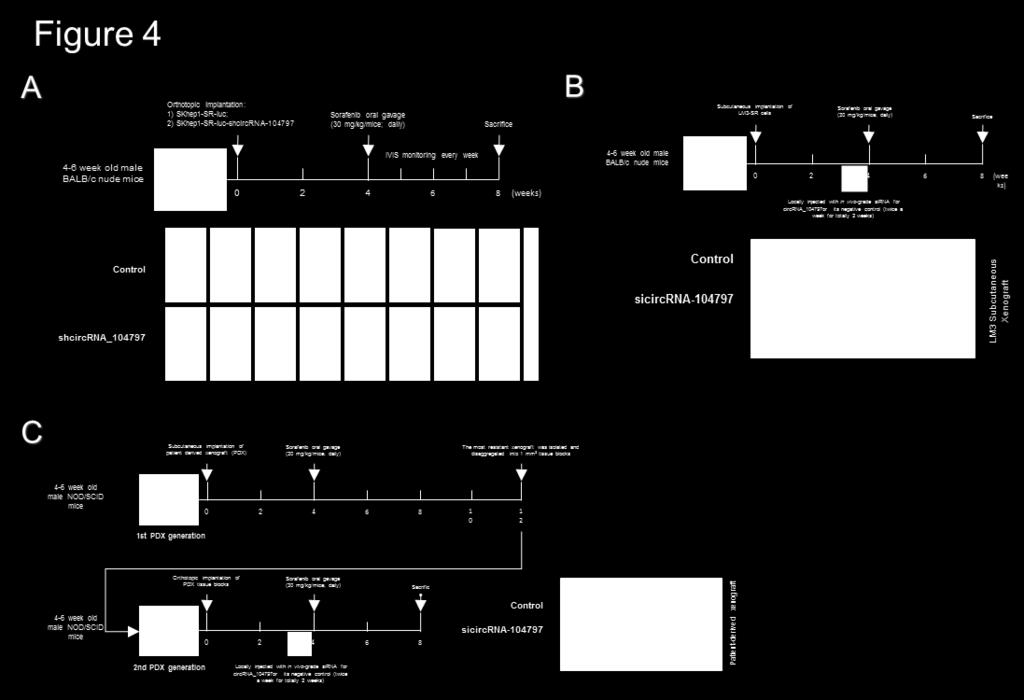
196 96


197 P-05 CHEMO-PREVENTIVE AND ANTI-TUMOR EFFECTS OF BENZYL ISOTHIOCYNATE ON HCC MODELS: A POSSIBLE CROSSTALK BETWEEN HGF/PAKT/STAT3 PATHWAY AND VEGF Sherin Zakaria, Maged Helmy 2, Ahmed Salahuddin 3, Gamal Omran 3 faculty of pharmacy, Kaferelsheikh universty, pharmacology and toxicology, Kafer el-sheikh, Egypt, 2 Faculty of Pharmacy, Damanhour University,, Department of Pharmacology and Toxicology, damanhour, Egypt, 3 Faculty of Pharmacy, Damanhour University, Department of Biochemistry, damanhour, Egypt Background and Aims: Benzyl isothiocyanate (BITC) is a member of the isothiocyanate compounds that found in cruciferous vegetables. BITC has a potential anticancer effect in different type of tumors. Few studies refer to antineoplastic effect of BITC against HCC. The mechanism of BITC whereby it retards the progress of HCC is incompletely understood. AIM: This study evaluated the role of HGF, pakt and STAT3 in BITC induced HCC growth retardation. Method: HCC was induced in mice using diethylnitrosamine (DEN) 75 mg/kg once a weak for 4 weeks. BITC 0 and 20 mg/kg was given to mice orally each day for 0 weeks. The HCC cell line hepg2 was also used to evaluate the effect of BITC on tumor cell behavior. Immunoassay was used to detect expression of caspase-3 activity, VEGF, MMP-2, TNF-α, HGF and pakt. STAT3 expression was detected in liver tissues using immunohistochemical staining Results: The results of this study showed a potential role of BITC in suppressing hepatic precancerous lesion progression of mice. The drug increased caspase-3 activity in tumor cells and inhibited angiogenesis marker VEGF. It also decrease metastases marker MMP-2. This anticancer effect of BITC was observed in DEN treated mice as well as in hepg2 cells. The reported antineoplastic activity was correlated with downregulation of HGF and its downstream molecules pakt and STAT3. Conclusion: The effect of BITC on HGF /pakt/ STAT3 axis has a potential role in both chemopreventive and chemotherapeutic effects of BITC on HCC models Figure: 97
198 P-06YI PROGNOSTIC SCORES FOR SORAFENIB-TREATED HEPATOCELLULAR CARCINOMA PATIENTS: A VALIDATION STUDY OF THE HAP AND SAP SCORES Francesco Tovoli, Giovan Giuseppe DI Costanzo 2, Giulia Magini 3, Rodolfo Sacco 4, Tiziana Pressiani 5, Franco Trevisani 6, Sara Marinelli, Raffaella Tortora 2, Laura Bucci 6, Maria Grazia Lucà 3, Luigi Bolondi, Alessandro Granito University of Bologna, Department of Medical and Surgical Sciences - Internal Medicine Unit, Bologna, Italy, 2 Cardarelli Hospital, Department of Transplantation - Liver Unit, Naples, Italy, 3 Papa Giovanni XXIII Hospital, Gastroenterology and Transplant Hepatology,, Bergamo, Italy, 4 Azienda Ospedaliero- Universitaria Pisana, Gastroenterology Unit, Pisa, Italy, 5 Humanitas Clinical and Research Center, Medical Oncology and Hematology Unit, Rozzano (Milan), Italy, 6 University of Bologna, Department of Medical and Surgical Sciences, Medical Semiotics Unit, Bologna, Background and Aims: Prognostic classifications for patients treated with sorafenib for hepatocellular carcinoma (HCC) are lacking. Very recently, Edeline and collaborators reported that both the hepatoma arterial embolisation prognostic score (HAP, previously used as a prognositic indicator for patients undergoing trans-arterial chemoembolizatio) and the authors proposed Sorafenib Advanced HCC Prognosis (SAP) score were able to provide discriminant prognostic information. Aim of our study was to validate these findings in a large cohort of sorafenib-treated patients in Italy. Method: We analyzed a large retrospective-prospective database gathering the clinical data of 432 patients from 6 Italian centres, who were prescribed with sorafenib between 2008 (date of licence in Italy) and 206. The HAP score was calculated according to the following criteria: largest tumor nodule > 7 cm ( point); bilirubin > mg/dl ( point); albumin <36 g/l ( point); alfa-fetoprotein> 400 mg/dl ( point). It was subsequently categorized as follows: HAP A (0 points); HAP B ( point); HAP C (2 points); HAP D (>2 points). The SAP score calculation was very similar, but included a further criterion (PS>0 = point). This score was categorized as proposed by Edeline et al : SAP A (0- points); SAP B(2-3 points); SAP C (>3 points). Results: The SAP score was significantly associated with the overall survival (OS), with a median OS of 4.6 months for SAP A, 9.8 months for SAP B and 5.7 months for SAP C (P < 0.00, log-rank test). Also the HAP score provided prognostic information, however HAP B and HAP C patients showed similar OS (median OS: HAP A 6.7 months, HAP B 0.9 months, HAP C 0.5 months, HAP D 5.9 months). Conclusion: Our results validate both the SAP and the HAP score as prognostic indicators for HCC patients undergoing treatement with sorafenib. Differently from the previously published paper on this topic, however, our results suggest that the SAP may be a better prognosticator compared with the HAP score. The use of these simple scores may facilitate stratification in trials and inform clinical decision making. 98

199 Figure: 99

200 P-07YI COMBINED TARGETING OF THE PPMD/WIP AND MDM2 NEGATIVE FEEDBACK SUPPRESSORS OF P53 IN TP53 WILD-TYPE HUMAN LIVER CANCER CELLS Ahmed Mahdi 2, Helen L. Reeves 3, John Lunec Northern Institute For Cancer Research, Newcastle University, Newcastle Upon Tyne, Tyne and Wear,, United Kingdom, 2 Department of pathology and forensic medicine, College of Medicine, Al-Nahrain University, Baghdad, Iraq, 3 Liver Unit, Freeman Hospital, Newcastle upon Tyne Hospitals NHS Foundation Trust, Newcastle Upon Tyne, Tyne and Wear,, United Kingdom Background and Aims: HCC is the second leading cause of cancer death worldwide with the tumour suppressor TP53 mutated in approximately a third of the cases. Small molecule inhibitors of MDM2 that stabilise and release TP53 from the inhibitory effect of MDM2 have exciting therapeutic potential for TP53 WT cancers. HDM20 is an MDM2 inhibitor already in phase II clinical trials for other cancers. GSK is a small molecule inhibitor of wild type-p53 induced phosphatase (WIPi), which is one of the downstream targets of p53 encoded by the PPMD gene and part of the auto-regulatory negative feedback loop regulating p53 function. We explored the effect of combining GSK with HDM20 as a potential therapeutic strategy for patients with TP53 WT liver cancer. Method: Using liver cancer cell lines - HepG2, SKHep (TP53 WT), Huh7 (TP53 mutated) and Hep3B (TP53 null), the effects of GSK alone and in combination with HDM20 on the expression of TP53 and its downstream transcriptional targets was assessed by qrt-pcr and western blot. Impact on growth, cell cycle and survival was assessed by SRB, FACS and clonogenic assays. Results: In both TP53 WT cell lines, GSK potentiated the effect of HDM20 on the stabilisation of p53, resulting in marked upregulation of downstream transcriptional targets (including MDM2 & CDKNA (p2)) resulting in significant potentiation of growth inhibition, with reduction in 50% growth inhibition (GI50) doses from 29.2±.6 to 6.3±0.8 nm in HepG2 (p=0.0) & from 60.±.5 to 26.±.8 nm in SK-Hep- (p=0.0002). Additionally, there was a significant reduction in 50% clonogenic survival (LC50) doses from 73.9±20.2 to 27.2±6.3 nm in SK-Hep- (p=0.04), and.±.3 to 7.9±0.4 nm for HepG2 (p=0.07). FACS and Senescence Associated beta Galactosidase (SA-beta-GAL) analyses revealed potentiation of G2 growth arrest, associated with potentiation of senescence at higher doses. Conclusion: GSK significantly increased p53 activation by HDM20 and potentiated both its growth inhibitory effect and the induction of senescence in WT liver cancer cell lines. Figure: 200
201 P-08YI CLINICAL CORRELATES OF THE GENETIC VARIABILITY OF THE CD274 GENE (PROGRAMMEDCELL DEATH-LIGAND ) AMONG PATIENTS WITH HEPATOCELLULAR CARCINOMA Federico Daffara, Livia Salmi, Matteo Nazzareno Barbaglia, Violante Mulas, Deborah Camatta, Margherita Tran Minh, Michela Emma Burlone, Rosalba Minisini, Mario Pirisi Università del Piemonte orientale, Translational Medicine, NOVARA, Italy Background and Aims: A deranged Programmed Death-Ligand (PD-L, a protein encoded by the CD274 gene) pathway is an important mechanism of immunological escape exploited by different cancers. Specifically, PD-L germline mutations modulate outcome and response to therapy in nonsmall cell lung cancer. Our aim was to verify the clinical correlates of three single nucleotide polymorphisms (SNPs) on the CD274 gene among patients with hepatocellular carcinoma (HCC). Method: The study population included N.=387 patients: N.=24 with HCC (Group A: 62 males, median age 7 years, cirrhosis in 97% and hepatitis C in 56%) and N.=64 with cirrhosis, similar for age and sex distribution (Group B: 8 males, median age 72 years, and hepatitis C in 63%) to Group A. All were genotyped for the following SNPs: rs227936, rs44385 and 8923A/C. The status of all these patients was known and documented up to (and including) the censor date of 3 Jul 207. Results: The study population did not depart from what expected based on the Hardy-Weinberg equilibrium for any of the three SNPs. For rs227936, the allelic frequencies in Group A vs. Group B were 0.39 and 0.6 vs. 0.4 and 0.59, respectively for the ancestral and variant gene (p=0.94); for rs443856, they were 0.70 and 0.30 vs. 0.7 and 0.29 (p=0.935); for 8923A/C, they were 0.57 and 0.73 vs and 0.48 (p=0.37). Patients in group A did not show differences based on the rs and 8923A/C genotypes with regard to age at diagnosis, gender distribution, hepatitis C etiology, major tumor node size, number of tumor nodes, Milan-in criteria, serum alpha-fetoprotein concentration and neutrophil-to-lymphocyte ratio. However, carriage of the variant gene for the rs44385 was associated with younger age at diagnosis, obtained at a median of 73 years (interquartile range, 65-79) for G/G homozygotes, 70 years (62-76) for G/C heterozygotes, and 68 years (59-73) for C/C homozygotes (p=0.032). Moreover, there was a trend for higher number of nodules at diagnosis in the same direction (p=0.070). Finally, median survival in Group A was 24 months; at logrank test, survival probabilities in Group A were not statistically different based on carriage of any of the germline mutations, either analyzed genotypically or using a dominant or a recessive model. Conclusion: Carriage of the rs44385 germline mutation may affect the natural history of HCC superimposed on cirrhosis by predisposing to its earlier and multinodular occurrence. 20
202 P-09 A SPECIFIC ECM COMPOSITION REGULATES SMAD - DEPENDENT - TGFBETA-INDUCED EMT RESPONSE IN HEPG2 CELLS ENGINEERED IN CIRRHOTIC AND HEALTHY HUMAN LIVER 3D SCAFFOLDS Martina Marrali, Andrea Telese, Katrin Bottcher, Luca Frenguelli, Walid Al-Akkad, Giuseppe Mazza, Massimo Pinzani, Krista Rombouts University College London, Department of Medicine, Institute for Liver and Digestive Health, LONDON, United Kingdom Background and Aims: Hepatocellular carcinoma (HCC) is the second cause of cancer deaths motivating the investigation of new therapeutic targets to provide alternative treatments. Recent studies highlight the role of the ECM microenvironment in modulating cancer development. A new 3D model was developed by using decellularized human liver which maintains the original tissue-specific 3D architecture and properties. TGFbeta plays a dual role in liver tumorigenesis. This study investigates the effect of cirrhotic and healthy ECM on ) TGFbeta-SMAD2/3 signalling in EMT-related HCC cell behaviour, and 2) drug sensitivity. Method: Human liver 3D scaffolds were obtained decellularizing healthy and cirrhotic human livers. Scaffolds were repopulated with HepG2 cells (2x0*6) for 7 days followed by TGFbeta (5-0ng/ml) treatment (n=4 for each condtion). Protein expression was assessed for P-SMAD2/3, SMAD2/3 and albumin. Changes in TGFbeta response were investigated by pre-treatment/treatment with TGFbetaR kinase inhibitor Galunisertib (0µM) for 48hrs. To investigate the involvement of the non-canonical TGFbeta pathway in HCC, Erk, Akt and JNK protein expression was assessed in cells cultured on cirrhotic and healthy scaffolds. Results: P-SMAD3 had a low expression in HepG2 cells cultured on healthy scaffolds while being highly expressed on cirrhotic scaffolds. In contrast, P-SMAD2 had a low expression in HepG2 cells cultured on cirrhotic scaffolds, while being upregulated in healthy scaffolds. SMAD2/3 proteins were expressed in HepG2 cells cultured on both cirrhotic and healthy scaffolds. Each protein was differently affected by exogenous TGFbeta treatment depending on ECM scaffold. Pre/simultaneous treatment of TGFbeta with Galunisertib affected protein expression depending on the ECM-scaffold investigated. TGFbeta-Galunisertib treatment reduced albumin protein expression in cells cultured on cirrhotic scaffolds. Erk protein expression was similar on both types of scaffolds, while Akt showed a higher expression on healthy scaffolds. Uptake/release of TGFbeta showed marked differences between healthy and cirrhotic scaffolds. Conclusion: This study suggests that the ECM composition of the 3D liver scaffold itself can affect protein expression which can be further modified by exogenous TGFbeta treatment. Although inhibiting the TGFbeta signaling pathway alone may not be sufficient, as the tumor ECM microenvironment indicates to play a major role, this study suggests that TGFbeta represent a potential target for the treatment of HCC. 202
203 P-0YI HEPATOCELLULAR CARCINOMA AS A COMPLICATION OF VASCULAR DISEASE OF THE LIVER AFTER FONTAN PROCEDURE. Chiara Mazzarelli 2, Mary D Cannon, Nigel Heaton, Debashis Sarker, Pauline Kane, Alberto Quaglia, Abid Suddle King's College Hospital NHS Foundation Trust, United Kingdom, 2 Ospedale Niguarda, Hepatology and Gastroenterology, Milano, Italy Hepatocellular Carcinoma as a complication of vascular disease of the liver after Fontan procedure. Background and Aims: Liver disease is a recognized long-term complication of the Fontan procedure, a complex corrective cardio-surgical operation, for cyanotic congenital heart disease. These patients also have a reported increased risk of developing hepatocellular cancer many years post procedure, believed to be related to abnormal vascular flow within the liver. Method: We report three patients who underwent Fontan procedure for congenital heart disease in childhood, and subsequently presented with hepatocellular cancer in adulthood. Results: Patient, a 28 year old woman with known congestive hepatopathy, developed a 9-cm infiltrative hepatocellular carcinoma with portal thrombosis, confirmed by liver biopsy. Sorafenib was commenced, but discontinued due to adverse effects. Patient 2, a 20 year old man, was diagnosed with trifocal HCC within the right lobe (70 mm, 25 mm and 20 mm) during workup for heart transplant. He had findings on imaging that were characteristic of hepatocellular carcinoma with an AFP of 2,000 ng/ml. He underwent 2 cycles of transarterial chemoembolisation. Patient 3, a 2 year old male developed a 70 mm liver nodule, confirmed as HCC by biopsy. He was placed on the waiting list for combined heart and liver transplantation and underwent chemoembolization as a downstaging treatment. All patients in our cohort developed HCC more than ten years after their original Fontan procedure. Two of the three patients underwent annual liver US screening. In addition, the radiological features of the liver were consistent with congestive hepatopathy rather than cirrhosis, and these features were also histologically confirmed in 2 of 3 patients (see figure ). Conclusion: Although cirrhosis is almost always a prerequisite for the development of HCC in patients with chronic liver disease, this is not an absolute requirement in patients with previous Fontan or other vascular liver disorders. In fact, additional unrecognized factors beyond the simple hyperplastic hepatocellular response to abnormal liver flow are probably involved. Further studies and an international registry are warranted to improve our knowledge about tumorigenesis and fibrogenesis in patients with vascular disorders of the liver, and to understand if early detection of liver disease in Fontan patients might alter the clinical management, improving their prognosis and long-term outcomes. 203

204 Figure: 204
205 P-YI OUTCOMES OF SINGLE OR SEQUENTIAL DUAL MODALITY LOCO- REGIONAL THERAPIES IN HEPATOCELLULAR CARCINOMA Vinay Kumar Balachandrakumar, Mira Swaminathan 2, Jonathan Evans 3, Nabil Kibriya 3, Daniel Palmer, Timothy Cross 2 University of Liverpool, Institute of Translational Medicine, Liverpool, United Kingdom, 2 The Royal Liverpool Hospital, Hepatology, Liverpool, United Kingdom, 3 The Royal Liverpool Hospital, Interventional Radiology, Liverpool, United Kingdom Background and Aims: Hepatocellular carcinoma (HCC) in western populations commonly occurs in the context of cirrhosis. Staging of disease has been based primarily on the Barcelona Clinic Liver Cancer (BCLC) classification in the UK. Patients not fit for Orthotopic Liver Transplantation(OLT) or liver resection in stage A disease have been offered ablations whilst patients with intermediate stage B disease have been offered trans-arterial chemoembolization (TACE). The aim was to assess outcomes from patients offered single modality or dual modality therapy for HCC, and to identify prognostic factors. Method: A single centre study of patients from the Royal Liverpool Hospital from 2003 to 206 was analysed. Patients receiving loco-regional therapy were identified from the departmental HCC database. Patient characteristics collected included age, gender, etiology, standard biochemistry, BCLC stage, performance status, tumour size and number, and treatments offered: Radiofrequency ablation(rfa) alone, RFA-TACE, TACE alone and TACE -RFA. The primary outcome measure was survival, calculated using the log-rank method. Results: Out of 295 patients in our cohort, 96 patients were identified who had ablation (RFA (pre- 200) or microwave ablation (from 200)), TACE, or a combination of the 2. The median age was 67 (57-74), the BCLC grade was 0=9 (9%), A =42 (44%), B=35 (36%), C=9 (9%), D= (%). Disease etiology was Alcoholic Liver Disease(ALD)=27, Hepatitis B=4, Hepatitis C=2, Non-Alcoholic Steatohepatitis=27, Haemochromatosis=5, ALD + viral=5, others =7. Hepatoma arterial-embolization prognostic(hap) score was available in 85 patients; HAP A=38, B=24, C=2, D=2. A total of 43 TACE and 54 ablation procedures were performed. The median survival for ablation alone was 37 months (26-48), RFA-TACE was 38 months (33-43), TACE alone was 6 months (5-7) and TACE-RFA was 34 months (22-46), log rank 3.3, p= Survival using HAP score was; HAP A =8 months (24-52), HAP B =35 months (20-50), HAP C =2 months (7-7), HAP D= 2 months (-3), log rank 68., p< Conclusion: Our data suggests that patients who cannot be down-staged with TACE to receive ablation do worse than patients with earlier stage disease who progress after ablation alone or who receive TACE following an ablation. This supports the use of dual sequential therapy where indicated. The HAP score is a useful tool to identify patients most likely to benefit from loco-regional treatments. 205
206 P-2 MULTIMODAL AND SEQUENTIAL TREATMENTE FOR HEPATOCELLULAR CARCINOMA: HOW "REAL-LIFE" COMPLIES WITH INTERNATIONAL RECOMMENDATIONS Michela Triolo 2, Angelo Sangiovanni, Massimo Iavarone, Laura Virginia Forzenigo 3, Antonio Nicolini 4, Giorgio Rossi 5, Vincenzo La Mura 2, Massimo Colombo 6, Pietro Lampertico Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Università degli Studi di Milano, CRC A.M. and A. Migliavacca for Liver Disease, Division of Gastroenterology and Hepatology, Milano, Italy, 2 Policlinico S. Donato, University of Milan, Division of Internal Medicine, San Donato Milanese, Italy, 3 Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Division of Radiology, Milano, Italy, 4 Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Division of Interventional Radiology, Milano, Italy, 5 Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, University of Milan, Division of Surgery and Liver Transplant, Milan, Italy, 6 Humanitas Clinical and Research Center, Rozzano, Italy Background and Aims: Management of hepatocellular carcinoma (HCC) is framed within standardized protocols released by Scientific Societies, whose applicability and efficacy in field practice need refining. We evaluated the applicability and effectiveness of guidelines for the treatment of HCC of the American Association for the Study of the Liver (AASLD). Method: Between January 2007 and December 20, 370 consecutive cirrhotic patients, 250 viral hepatitis/4 ethanol/79 other etiologies, median age 68 yrs, 272 (74%) males, 250 (68%) Child-Pugh A, with de-novo HCC in different stages, 253 (68%) BCLC A, 66 (8%) BCLC B, 5 (4%) BCLC C, received treatment through a multidisciplinary team (MDT) decision. Patients were followed until death or last follow-up up to December 206. Patients with a previous diagnosis of liver cancer and those with poor liver function (Child Pugh C) were excluded. Results: HCC treatment was adherent to AASLD recommendations in 205 (8%) BCLC A patients, 36 (54%) BCLC B, and 27 (53%) BCLC C. Overall, a radiological complete response was obtained in 85 (50%) patients, 65/370 (45%) after a first-line treatment, 25/7 (2%) after a second-line treatment, and 6/39 (5%) after a third-line treatment. Eleven patients (3%) achieved a complete response more than once. During 58 (range -08) months, 05 (28%) patients died, 4 (6%) BCLC A, 25 (38%) BCLC B and 39 (74%) BCLC C. In BCLC A the mean mortality rate was lower in patients treated according to AASLD recommendations than in patients otherwise treated (5.0% vs 0.4%, p=0.004), corresponding to a, 3, 5 year survival of 00%, 86%, 77% vs 93%, 75%, 47%, respectively; whereas the upward treatment stage migration was associated to a lower mortality rate as compared to standard of treatment in BCLC B (8.6% vs 20.7%, p=0.029) corresponding to a, 3, 5 year survival of 00%, 74%, 67% vs 00%, 43%, 23%, respectively, as well as in BCLC C (42.6% vs 59%, p = 0.04) corresponding to, 3, 5 yr survival 79%, 39%, 0% vs 42%, %, 0%, respectively. Conclusion: HCC multimodality treatment including other than first-line therapy is common in clinical practice and impacts on the achievement of complete response. Personalized treatment provided survival benefits to patients whose profile is not accounted for by international recommendations. 206
207 ACKNOWLEDGEMENTS 207







208 EASL thanks its Premium Sponsors AbbVie and MSD for their generous contribution and support of the association s activities with unrestricted educational grants. Gold sponsors Bronze sponsor Exhibitors The HCC Summit 208 has been supported by 208
209 INDUSTRY 209
210 INDUSTRY SATELLITE SYMPOSIA BAYER HEALTHCARE PHARMACEUTICALS, INC. Friday 02 March 208- Room: Plenary Future of HCC Care Management: Evaluation and Application of the Sorafenib to Regorafenib Sequence Chair: Jordi Bruix, Spain 9:30-9:35 Opening remarks by the Chair Jordan Bruix, Spain 9:35-9:50 Sequential therapy in HCC: Patient considerations and other decision factors Amit Singal, United States 9:50-9:55 Q&A Amit Singal, United States 9:55-20:05 Treatment of HCC: Optimizing window of opportunity to prolong OS Arndt Vogel, Germany 20:05-20:0 Q&A Arndt Vogel, Germany 20:0-20:20 Critical analysis of recent clinical evidence in HCC Pierre Gholam, United States 20:20-20:25 Q&A Pierre Gholam, United States 20:25-20:30 Closing remarks by the Chair Jordi Bruix, Spain G.COM.SM.ON L.CH.MKT.ONC EN 20
211 COMPANY PROFILES ABBVIE North Waukegan Road North Chicago United States AbbVie is a global, research-driven biopharmaceutical company committed to developing innovative advanced therapies for some of the world s most complex and critical conditions. The company s mission is to use its expertise, dedicated people and unique approach to innovation to markedly improve treatments across four primary therapeutic areas: immunology, oncology, virology and neuroscience. In more than 75 countries, AbbVie employees are working every day to advance health solutions for people around the world. For more information about AbbVie, please visit us at on Twitter, Facebook or LinkedIn. BAYER HEALTHCARE PHARMACEUTICALS, INC. 00 Bayer Boulevard P.O. Box 95 Whippany, NJ 0798 United States Bayer is committed to delivering SCIENCE FOR A BETTER LIFE by advancing a portfolio of innovative treatments. The oncology franchise at Bayer currently includes four oncology products in eight indications. Several other compounds are in various stages of clinical development, with the focus on potential first-in-class approaches across the areas of novel oncogenic signaling in combination with an effective biomarker strategy, antibody drug conjugates including a thorium platform and immuno-oncology. An Oncology Strategic Business Unit within the Pharmaceuticals Division of Bayer was established in 207 to support the accelerated development of new treatment options. BRISTOL-MYERS SQUIBB 340 Princeton Pike Lawrenceville, NJ United States Bristol-Myers Squibb is a global biopharmaceutical company whose mission is to discover, develop and deliver innovative medicines that help patients prevail over serious diseases. For more information about Bristol-Myers Squibb, visit us at BMS.com 2
212 BTG Lakeview, Riverside Way, Watchmoor Park Camberley, Surrey, GU5 3YL United Kingdom At BTG we are focused on bringing to market innovative products in specialist areas of medicine to better serve doctors and patients. Our growing portfolio of Interventional Medicine products is designed to advance the treatment of cancer, severe emphysema, severe blood clots and varicose veins, while our Specialty Pharmaceuticals portfolio offers antidotes that alleviate toxicity and treat rare conditions. Healthcare is constantly evolving so BTG never stands still. Inspired by a deep understanding of our customers needs, we re working to meaningfully improve the lives of patients and their healthcare experience. DOVE MEDICAL PRESS LTD Beechfield House Winterton Way Macclesfield Cheshire SK OLP United Kingdom Dove Medical Press ( is an open access Publisher of peer-reviewed biomedical and scientific journals, which focus on medicine, drug treatment and adherence across a breadth of disease states and technologies. Visit our booth to discuss your publishing needs. The benefits of publishing with us include wider dissemination, increased visibility and greater impact of your work. MSD 200 Galloping Hill Road Kenilworth United States For more than a century, MSD has been inventing for life, bringing forward medicines and vaccines for many of the world's most challenging diseases. Today, MSD continues be at the forefront of research to deliver innovative health solutions and advance the prevention and treatment of diseases that threaten people and animals around the world. 22
213 SIRTEX MEDICAL EUROPE GMBH Joseph-Schumpeter-Allee 33 Bonn Germany Sirtex Medical is actively engaged in the field of liver-directed therapies for cancer patients. Our innovative technology, SIR-Spheres Y-90 resin microspheres (microscopic Yttrium-90 resin beads), was approved in 2002 for use in the treatment of unresectable liver tumours within the European Union under a CE Mark. SIR-Spheres Y-90 resin microspheres are presently used to treat a variety of unresectable liver metastases as well as in hepatocellular carcinoma in more than,090 centres worldwide. SIR-Spheres Y-90 resin microspheres are the most extensively investigated SIRT. To date, more than 80,000 treatments have been delivered worldwide. TERUMO DEUTSCHLAND GMBH Bodenäckerstraße 3 Spreitenbach 8957 Switzerland Rising to the challenge of creating innovative treatments for patients, Terumo brings you a complete range of interventional oncology products that focus on access, loco-regional treatments and endovascular embolization. As a pioneer in interventional oncology, Terumo is committed to bringing you cutting-edge technology that is more effective and easier to use. 23
214 24
EASL HCC SUMMIT 2018 FROM BASIC TO CLINICAL RESEARCH: HOW TO IMPROVE HCC CLINICAL CARE? 01 03, MARCH 2018 GENEVA, SWITZERLAND
 EASL HCC SUMMIT 2018 FROM BASIC TO CLINICAL RESEARCH: HOW TO IMPROVE HCC CLINICAL CARE? 01 03, MARCH 2018 GENEVA, SWITZERLAND SCIENTIFIC ORGANISING COMMITTEE Alejandro Forner, Spain Peter Galle, Germany
EASL HCC SUMMIT 2018 FROM BASIC TO CLINICAL RESEARCH: HOW TO IMPROVE HCC CLINICAL CARE? 01 03, MARCH 2018 GENEVA, SWITZERLAND SCIENTIFIC ORGANISING COMMITTEE Alejandro Forner, Spain Peter Galle, Germany
HCC and the Hallmarks of Cancer: steps towards novel therapeutic strategies
 EASL HCC SUMMIT 2017 2-5 February 2017, Geneva, Switzerland Scientific Committee: Basic Programme: Tom Luedde, Germany Helen Reeves, United Kingdom Clinical Programme: Alejandro Forner, Spain Franco Trevisani,
EASL HCC SUMMIT 2017 2-5 February 2017, Geneva, Switzerland Scientific Committee: Basic Programme: Tom Luedde, Germany Helen Reeves, United Kingdom Clinical Programme: Alejandro Forner, Spain Franco Trevisani,
Hepatocellular Carcinoma. Markus Heim Basel
 Hepatocellular Carcinoma Markus Heim Basel Outline 1. Epidemiology 2. Surveillance 3. (Diagnosis) 4. Staging 5. Treatment Epidemiology of HCC Worldwide, liver cancer is the sixth most common cancer (749
Hepatocellular Carcinoma Markus Heim Basel Outline 1. Epidemiology 2. Surveillance 3. (Diagnosis) 4. Staging 5. Treatment Epidemiology of HCC Worldwide, liver cancer is the sixth most common cancer (749
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary)
") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Surveillance for Hepatocellular Carcinoma
 Surveillance for Hepatocellular Carcinoma Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded on April
Surveillance for Hepatocellular Carcinoma Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded on April
A) PUBLIC HEALTH B) PRESENTATION & DIAGNOSIS
 PUBLIC HEALTH B) PRESENTATION & DIAGNOSIS") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary), April 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Centre, BC Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary), April 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Centre, BC Cancer
Hepatocellular Carcinoma: Diagnosis and Management
 Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
21/02/2014. Disclosures. HCC: predicting recurrence. Outline. Liver transplant: Beyond Milan?
 Disclosures HCC: predicting recurrence Peter Ghali, MD, FRCPC, MSc (epid) None relevant to this talk other than off-label use of sirolimus Toronto, February 2014 Outline Recurrence after what? Locoregional
Disclosures HCC: predicting recurrence Peter Ghali, MD, FRCPC, MSc (epid) None relevant to this talk other than off-label use of sirolimus Toronto, February 2014 Outline Recurrence after what? Locoregional
EASL-EORTC Guidelines
 Pamplona, junio de 2008 CLINICAL PRACTICE GUIDELINES: PARADIGMS IN MANAGEMENT OF HCC EASL-EORTC Guidelines Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Levels of Evidence according
Pamplona, junio de 2008 CLINICAL PRACTICE GUIDELINES: PARADIGMS IN MANAGEMENT OF HCC EASL-EORTC Guidelines Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain Levels of Evidence according
Tumor incidence varies significantly, depending on geographical location.
 Hepatocellular carcinoma is the 5 th most common malignancy worldwide with male-to-female ratio 5:1 in Asia 2:1 in the United States Tumor incidence varies significantly, depending on geographical location.
Hepatocellular carcinoma is the 5 th most common malignancy worldwide with male-to-female ratio 5:1 in Asia 2:1 in the United States Tumor incidence varies significantly, depending on geographical location.
Hepatocellular carcinoma in Sri Lanka - where do we stand?
 SCIENTIFIC ARTICLE Hepatocellular carcinoma in Sri Lanka - where do we stand? R.C. Siriwardana 1, C.A.H. Liyanage 1, M.B. Gunethileke 2 1. Specialist Gastrointestinal and Hepatobilliary Surgeon, Senior
SCIENTIFIC ARTICLE Hepatocellular carcinoma in Sri Lanka - where do we stand? R.C. Siriwardana 1, C.A.H. Liyanage 1, M.B. Gunethileke 2 1. Specialist Gastrointestinal and Hepatobilliary Surgeon, Senior
SEQUENCING OF HCC TREATMENT. Dr. Amit G. Singal Medical Director, UT Southwestern Medical Center, USA
 SEQUENCING OF HCC TREATMENT Dr. Amit G. Singal Medical Director, UT Southwestern Medical Center, USA February 2018 DISCLAIMER Please note: The views expressed within this presentation are the personal
SEQUENCING OF HCC TREATMENT Dr. Amit G. Singal Medical Director, UT Southwestern Medical Center, USA February 2018 DISCLAIMER Please note: The views expressed within this presentation are the personal
Liver Cancer. Su Jong Yu, M.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine
 Liver Cancer Su Jong Yu, M.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine Primary Liver Cancer Hepatocellular carcinoma (HCC) : > 80% Derived
Liver Cancer Su Jong Yu, M.D. Department of Internal Medicine, Liver Research Institute, Seoul National University College of Medicine Primary Liver Cancer Hepatocellular carcinoma (HCC) : > 80% Derived
The impact of the treatment of HCV in developing Hepatocellular Carcinoma
 The impact of the treatment of HCV in developing Hepatocellular Carcinoma Paul Y Kwo, MD Professor of Medicine Medical Director, Liver Transplantation Gastroenterology/Hepatology Division Indiana University
The impact of the treatment of HCV in developing Hepatocellular Carcinoma Paul Y Kwo, MD Professor of Medicine Medical Director, Liver Transplantation Gastroenterology/Hepatology Division Indiana University
IS THERE A DIFFERENCE IN LIVER CANCER RATES IN PATIENTS WHO RECEIVE TREATMENT FOR HEPATITIS?
 IS THERE A DIFFERENCE IN LIVER CANCER RATES IN PATIENTS WHO RECEIVE TREATMENT FOR HEPATITIS? Dr. Sammy Saab David Geffen School of Medicine, Los Angeles, USA April 2018 DISCLAIMER Please note: The views
IS THERE A DIFFERENCE IN LIVER CANCER RATES IN PATIENTS WHO RECEIVE TREATMENT FOR HEPATITIS? Dr. Sammy Saab David Geffen School of Medicine, Los Angeles, USA April 2018 DISCLAIMER Please note: The views
Screening for HCCwho,
 Screening for HCCwho, how and how often? Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital HCC Global Epidemiology
Screening for HCCwho, how and how often? Catherine Stedman Associate Professor of Medicine, University of Otago, Christchurch Gastroenterology Department, Christchurch Hospital HCC Global Epidemiology
Hepatobiliary Malignancies Retrospective Study at Truman Medical Center
 Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
Hepatocellular Carcinoma Surveillance
 Amit G. Singal, MD, MS Hepatocellular Carcinoma Surveillance Postgraduate Course: Challenges in Management of Common Liver Diseases 308 1 Patient Case 69 year-old otherwise healthy male with compensated
Amit G. Singal, MD, MS Hepatocellular Carcinoma Surveillance Postgraduate Course: Challenges in Management of Common Liver Diseases 308 1 Patient Case 69 year-old otherwise healthy male with compensated
Molecular signature for management of hepatocellular carcinoma
 Molecular signature for management of hepatocellular carcinoma Yujin Hoshida, MD, PhD Liver Cancer Program, Tisch Cancer Institute Division of Liver Diseases, Department of Medicine Icahn School of Medicine
Molecular signature for management of hepatocellular carcinoma Yujin Hoshida, MD, PhD Liver Cancer Program, Tisch Cancer Institute Division of Liver Diseases, Department of Medicine Icahn School of Medicine
HCC: Is it an oncological disease? - No
 June 13-15, 2013 Berlin, Germany Prof. Oren Shibolet Head of the Liver Unit, Department of Gastroenterology Tel-Aviv Sourasky Medical Center and Tel-Aviv University HCC: Is it an oncological disease? -
June 13-15, 2013 Berlin, Germany Prof. Oren Shibolet Head of the Liver Unit, Department of Gastroenterology Tel-Aviv Sourasky Medical Center and Tel-Aviv University HCC: Is it an oncological disease? -
Friday, May 18 SESSION Opening remarks L. Bolondi - Bologna (Italy)
") Friday, May 18 09.00 Opening remarks L. Bolondi - Bologna (Italy) SESSION 1 THE ROLE OF CIRCULATING AND TISSUE BIOMARKERS Chair: J.C. Nault - Paris (France) 09.10 Predicting the development of HCC in liver
Friday, May 18 09.00 Opening remarks L. Bolondi - Bologna (Italy) SESSION 1 THE ROLE OF CIRCULATING AND TISSUE BIOMARKERS Chair: J.C. Nault - Paris (France) 09.10 Predicting the development of HCC in liver
Hepatocellular Carcinoma: A major global health problem. David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center
 Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
Update EASL Clinical Practice Guidelines: Management of Hepatocellular Carcinoma
 Update EASL Clinical Practice Guidelines: Management of Hepatocellular Carcinoma Peter R. Galle PHC 2018 - www.aphc.info Disclosure of Conflict of Interest Peter R. Galle I have the following financial
Update EASL Clinical Practice Guidelines: Management of Hepatocellular Carcinoma Peter R. Galle PHC 2018 - www.aphc.info Disclosure of Conflict of Interest Peter R. Galle I have the following financial
 MEETING PROSPECTUS www.virology-education.com CONTENT Introduction... 3 Workshop description... 4 Background...4 Meeting Objectives...4 Learning Objectives...4 Format...4 Unique Meeting Features...4 Target
MEETING PROSPECTUS www.virology-education.com CONTENT Introduction... 3 Workshop description... 4 Background...4 Meeting Objectives...4 Learning Objectives...4 Format...4 Unique Meeting Features...4 Target
3/22/2017. I will be discussing off label/investigational use of tivantinib for hepatocellular carcinoma.
 Grant/Research Support - AbbVie, Conatus, Hologic, Intercept, Genfit, Gilead, Mallinckrodt, Merck, Salix, Shire, Vital Therapies Consultant AbbVie, Gilead, Merck Member, Scientific Advisory Board Vital
Grant/Research Support - AbbVie, Conatus, Hologic, Intercept, Genfit, Gilead, Mallinckrodt, Merck, Salix, Shire, Vital Therapies Consultant AbbVie, Gilead, Merck Member, Scientific Advisory Board Vital
Hepatocellular Carcinoma in HIV-infected Patients A Growing Complication of Coinfection with HCV or HBV Mon, 31 May 2010
 Bronx VA Medical Center Mount Sinai School of Medicine Hepatocellular Carcinoma in HIV-infected Patients A Growing Complication of Coinfection with HCV or HBV Mon, 31 May 2010 Norbert Bräu, MD, MBA Associate
Bronx VA Medical Center Mount Sinai School of Medicine Hepatocellular Carcinoma in HIV-infected Patients A Growing Complication of Coinfection with HCV or HBV Mon, 31 May 2010 Norbert Bräu, MD, MBA Associate
Liver and Biliary Tract Cancers Critical Review
 Liver and Biliary Tract Cancers Critical Review Lorenza Rimassa Oncologia Medica e Ematologia Humanitas Cancer Center Humanitas Research Hospital Rozzano (Milano) Critical review Oral presentations Melero
Liver and Biliary Tract Cancers Critical Review Lorenza Rimassa Oncologia Medica e Ematologia Humanitas Cancer Center Humanitas Research Hospital Rozzano (Milano) Critical review Oral presentations Melero
Liver Pathology and the Clinician in 2015: At the Crossroads. Thomas D. Schiano, M.D. Mount Sinai Medical Center New York, New York
 Liver Pathology and the Clinician in 2015: At the Crossroads Thomas D. Schiano, M.D. Mount Sinai Medical Center New York, New York DISCLOSURES Consultant for: Salix Merck Gilead BMS Synageva Research funding:
Liver Pathology and the Clinician in 2015: At the Crossroads Thomas D. Schiano, M.D. Mount Sinai Medical Center New York, New York DISCLOSURES Consultant for: Salix Merck Gilead BMS Synageva Research funding:
LIVER IMAGING TIPS IN VARIOUS MODALITIES. M.Vlychou, MD, PhD Assoc. Professor of Radiology University of Thessaly
 LIVER IMAGING TIPS IN VARIOUS MODALITIES M.Vlychou, MD, PhD Assoc. Professor of Radiology University of Thessaly Hepatocellular carcinoma is a common malignancy for which prevention, screening, diagnosis,
LIVER IMAGING TIPS IN VARIOUS MODALITIES M.Vlychou, MD, PhD Assoc. Professor of Radiology University of Thessaly Hepatocellular carcinoma is a common malignancy for which prevention, screening, diagnosis,
Pathological Analysis of Small Hepatocellular Carcinoma with Poor Prognosis
 Pathological Analysis of Small Hepatocellular Carcinoma with Poor Prognosis Haeryoung Kim, M.D., Ph.D. Department of Pathology Seoul National University Bundang Hospital Small HCC Definition: HCC < 2cm
Pathological Analysis of Small Hepatocellular Carcinoma with Poor Prognosis Haeryoung Kim, M.D., Ph.D. Department of Pathology Seoul National University Bundang Hospital Small HCC Definition: HCC < 2cm
HEPATOCELLULAR CARCINOMA: SCREENING, DIAGNOSIS, AND TREATMENT
 HEPATOCELLULAR CARCINOMA: SCREENING, DIAGNOSIS, AND TREATMENT INTRODUCTION: Hepatocellular carcinoma (HCC): Fifth most common cancer worldwide Third most common cause of cancer mortality In Egypt: 2.3%
HEPATOCELLULAR CARCINOMA: SCREENING, DIAGNOSIS, AND TREATMENT INTRODUCTION: Hepatocellular carcinoma (HCC): Fifth most common cancer worldwide Third most common cause of cancer mortality In Egypt: 2.3%
September 20, Submitted electronically to: Cc: To Whom It May Concern:
 History Study (NOT-HL-12-147), p. 1 September 20, 2012 Re: Request for Information (RFI): Building a National Resource to Study Myelodysplastic Syndromes (MDS) The MDS Cohort Natural History Study (NOT-HL-12-147).
History Study (NOT-HL-12-147), p. 1 September 20, 2012 Re: Request for Information (RFI): Building a National Resource to Study Myelodysplastic Syndromes (MDS) The MDS Cohort Natural History Study (NOT-HL-12-147).
Learning Objectives. After attending this presentation, participants will be able to:
 Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
9th Paris Hepatitis Conference
 9th Paris Hepatitis Conference Paris, 12 January 2016 Treatment of hepatocellular carcinoma: beyond international guidelines Massimo Colombo Chairman Department of Liver, Kidney, Lung and Bone Marrow Units
9th Paris Hepatitis Conference Paris, 12 January 2016 Treatment of hepatocellular carcinoma: beyond international guidelines Massimo Colombo Chairman Department of Liver, Kidney, Lung and Bone Marrow Units
White Nights of Hepatology 2016
 White Nights of Hepatology 2016 Saint Petersburg, 3 June 2016 Long-term treatment of Chronic hepatitis B - a key to HCC prevention Massimo Colombo Chairman Department of Liver, Kidney, Lung and Bone Marrow
White Nights of Hepatology 2016 Saint Petersburg, 3 June 2016 Long-term treatment of Chronic hepatitis B - a key to HCC prevention Massimo Colombo Chairman Department of Liver, Kidney, Lung and Bone Marrow
Nexavar in advanced HCC: a paradigm shift in clinical practice
 Nexavar in advanced HCC: a paradigm shift in clinical practice Tim Greten Hanover Medical School, Germany Histopathological progression and molecular features of HCC Chronic liver disease Liver cirrhosis
Nexavar in advanced HCC: a paradigm shift in clinical practice Tim Greten Hanover Medical School, Germany Histopathological progression and molecular features of HCC Chronic liver disease Liver cirrhosis
Hepatocellular Carcinoma (HCC): Who Should be Screened and How Do We Treat? Tom Vorpahl MSN, RN, ACNP-BC
: Who Should be Screened and How Do We Treat? Tom Vorpahl MSN, RN, ACNP-BC") Hepatocellular Carcinoma (HCC): Who Should be Screened and How Do We Treat? Tom Vorpahl MSN, RN, ACNP-BC Objectives Identify patient risk factors for hepatocellular carcinoma (HCC) Describe strategies
Hepatocellular Carcinoma (HCC): Who Should be Screened and How Do We Treat? Tom Vorpahl MSN, RN, ACNP-BC Objectives Identify patient risk factors for hepatocellular carcinoma (HCC) Describe strategies
Transformation of Normal HMECs (Human Mammary Epithelial Cells) into Metastatic Breast Cancer Cells: Introduction - The Broad Picture:
 into Metastatic Breast Cancer Cells: Introduction - The Broad Picture:") Transformation of Normal HMECs (Human Mammary Epithelial Cells) into Metastatic Breast Cancer Cells: Introduction - The Broad Picture: Spandana Baruah December, 2016 Cancer is defined as: «A disease caused
Transformation of Normal HMECs (Human Mammary Epithelial Cells) into Metastatic Breast Cancer Cells: Introduction - The Broad Picture: Spandana Baruah December, 2016 Cancer is defined as: «A disease caused
Professor Norbert Bräu
 Sixth Annual BHIVA Conference for the Management of HIV/Hepatitis Co-Infection in collaboration with BASL and BVHG Professor Norbert Bräu James J Peters VA Medical Center, New York, USA COMPETING INTEREST
Sixth Annual BHIVA Conference for the Management of HIV/Hepatitis Co-Infection in collaboration with BASL and BVHG Professor Norbert Bräu James J Peters VA Medical Center, New York, USA COMPETING INTEREST
Hepatocellular carcinoma
 Hepatocellular carcinoma Mary Ann Y. Huang, M.D., M.S., FAASLD Transplant hepatologist Peak Gastroenterology Associates Porter Adventist Hospital Denver, Colorado Background - Worldwide Hepatocellular
Hepatocellular carcinoma Mary Ann Y. Huang, M.D., M.S., FAASLD Transplant hepatologist Peak Gastroenterology Associates Porter Adventist Hospital Denver, Colorado Background - Worldwide Hepatocellular
UPDATE OF EASL CLINICAL PRACTICE GUIDELINES: MANAGEMENT OF HEPATOCELLULAR CARCINOMA*
 UPDATE OF EASL CLINICAL PRACTICE GUIDELINES: MANAGEMENT OF HEPATOCELLULAR CARCINOMA* Dr. Catherine Frenette Medical Director of Liver Transplantation, Scripps Green Hospital, La Jolla, CA, USA May 2018
UPDATE OF EASL CLINICAL PRACTICE GUIDELINES: MANAGEMENT OF HEPATOCELLULAR CARCINOMA* Dr. Catherine Frenette Medical Director of Liver Transplantation, Scripps Green Hospital, La Jolla, CA, USA May 2018
Surveillance for HCC Who, how Diagnosis of HCC Surveillance for HCC in Practice
 Surveillance for Hepatocellular Carcinoma Hashem B. El-Serag, MD, MPH Dan L. Duncan Professor of Medicine Chief, Gastroenterology and Hepatology Houston VA & Baylor College of Medicine Houston, TX Outline
Surveillance for Hepatocellular Carcinoma Hashem B. El-Serag, MD, MPH Dan L. Duncan Professor of Medicine Chief, Gastroenterology and Hepatology Houston VA & Baylor College of Medicine Houston, TX Outline
Treatment of HCC in real life-chinese perspective
 Treatment of HCC in real life-chinese perspective George Lau MBBS (HK), MRCP(UK), FHKCP, FHKAM (GI), MD(HK), FRCP (Edin, Lond), FAASLD (US) Chairman Humanity and Health Medical Group, Hong Kong SAR, CHINA
Treatment of HCC in real life-chinese perspective George Lau MBBS (HK), MRCP(UK), FHKCP, FHKAM (GI), MD(HK), FRCP (Edin, Lond), FAASLD (US) Chairman Humanity and Health Medical Group, Hong Kong SAR, CHINA
Liver transplantation: Hepatocellular carcinoma
 Liver transplantation: Hepatocellular carcinoma Alejandro Forner BCLC Group. Liver Unit. Hospital Clínic. University of Barcelona 18 de marzo 2015 3r Curso Práctico de Transplante de Órganos Sólidos Barcelona
Liver transplantation: Hepatocellular carcinoma Alejandro Forner BCLC Group. Liver Unit. Hospital Clínic. University of Barcelona 18 de marzo 2015 3r Curso Práctico de Transplante de Órganos Sólidos Barcelona
Introduction. Cancer Biology. Tumor-suppressor genes. Proto-oncogenes. DNA stability genes. Mechanisms of carcinogenesis.
 Cancer Biology Chapter 18 Eric J. Hall., Amato Giaccia, Radiobiology for the Radiologist Introduction Tissue homeostasis depends on the regulated cell division and self-elimination (programmed cell death)
Cancer Biology Chapter 18 Eric J. Hall., Amato Giaccia, Radiobiology for the Radiologist Introduction Tissue homeostasis depends on the regulated cell division and self-elimination (programmed cell death)
SOMATOSTATIN RECEPTORS IN HEPATOCELLULAR CARCINOMA. Marie LEQUOY Saint-Antoine Hospital, Department of Hepatology, Paris, France
 SOMATOSTATIN RECEPTORS IN HEPATOCELLULAR CARCINOMA Marie LEQUOY Saint-Antoine Hospital, Department of Hepatology, Paris, France Somatostatin : SST Somatostatin (SST) protein : 2 active forms (alternative
SOMATOSTATIN RECEPTORS IN HEPATOCELLULAR CARCINOMA Marie LEQUOY Saint-Antoine Hospital, Department of Hepatology, Paris, France Somatostatin : SST Somatostatin (SST) protein : 2 active forms (alternative
Staging & Current treatment of HCC
 Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
HCC Imaging and Advances in Locoregional Therapy. David S. Kirsch MD Ochsner Clinic Foundation
 HCC Imaging and Advances in Locoregional Therapy David S. Kirsch MD Ochsner Clinic Foundation -Nothing to disclose Hepatic Imaging Primary imaging modalities include: US CT MR Angiography Nuclear medicine
HCC Imaging and Advances in Locoregional Therapy David S. Kirsch MD Ochsner Clinic Foundation -Nothing to disclose Hepatic Imaging Primary imaging modalities include: US CT MR Angiography Nuclear medicine
Accepted Manuscript. S (16)30397-X Reference: JHEPAT To appear in: Journal of Hepatology
30397-X Reference: JHEPAT To appear in: Journal of Hepatology") Accepted Manuscript High incidence of hepatocellular carcinoma following successful interferon-free antiviral therapy for hepatitis C associated cirrhosis Helder Cardoso, Ana Maria Vale, Susana Rodrigues,
Accepted Manuscript High incidence of hepatocellular carcinoma following successful interferon-free antiviral therapy for hepatitis C associated cirrhosis Helder Cardoso, Ana Maria Vale, Susana Rodrigues,
3 Workshop on HCV THERAPY ADVANCES New Antivirals in Clinical Practice
 3 Workshop on HCV THERAPY ADVANCES New Antivirals in Clinical Practice Rome, 13 December 2013 Management and monitoring of HCC in the future era of DAA s Prof. Massimo Colombo Chairman Department of Liver,
3 Workshop on HCV THERAPY ADVANCES New Antivirals in Clinical Practice Rome, 13 December 2013 Management and monitoring of HCC in the future era of DAA s Prof. Massimo Colombo Chairman Department of Liver,
AASLD Washington DC, USA Dr. Alexander Kim Chief Vascular and Interventional Radiology, Medstar Georgetown University Hospital
 AASLD 2017 - Washington DC, USA Dr. Alexander Kim Chief Vascular and Interventional Radiology, Medstar Georgetown University Hospital THE CHANGING LANDSCAPE IN THE TREATMENT OF HCC DISCLAIMER Please note:
AASLD 2017 - Washington DC, USA Dr. Alexander Kim Chief Vascular and Interventional Radiology, Medstar Georgetown University Hospital THE CHANGING LANDSCAPE IN THE TREATMENT OF HCC DISCLAIMER Please note:
 10 5 TH TH WORKSHOP INTERNATIONAL WORKSHOP ON CO-INFECTION NEW ANTIVIRALS IN CLINICAL PRACTICE HIV & HEPATITIS AMSTERDAM, PARIS, FRANCE THE NETHERLANDS 12-13 JUNE 2014 4-5 DECEMBER 2015 MEETING PROSPECTUS
10 5 TH TH WORKSHOP INTERNATIONAL WORKSHOP ON CO-INFECTION NEW ANTIVIRALS IN CLINICAL PRACTICE HIV & HEPATITIS AMSTERDAM, PARIS, FRANCE THE NETHERLANDS 12-13 JUNE 2014 4-5 DECEMBER 2015 MEETING PROSPECTUS
Paul Martin MD FACG. University of Miami
 Paul Martin MD FACG University of Miami 1 Liver cirrhosis of any cause Chronic C o c hepatitis epat t s B Risk increases with Male gender Age Diabetes Smoking ~5% increase in HCV-related HCC between 1991-28
Paul Martin MD FACG University of Miami 1 Liver cirrhosis of any cause Chronic C o c hepatitis epat t s B Risk increases with Male gender Age Diabetes Smoking ~5% increase in HCV-related HCC between 1991-28
Jesse Civan, M.D. Medical Director, Jefferson Liver Tumor Center
 Liver Tumors Jesse Civan, M.D. Medical Director, Jefferson Liver Tumor Center Differential Diagnosis Malignant Metastatic from non-hepatic primary Hepatocellular carcinoma Cholangiocarcinoma Biliary cystcarcinoma
Liver Tumors Jesse Civan, M.D. Medical Director, Jefferson Liver Tumor Center Differential Diagnosis Malignant Metastatic from non-hepatic primary Hepatocellular carcinoma Cholangiocarcinoma Biliary cystcarcinoma
RESEARCH ARTICLE. Validation of The Hong Kong Liver Cancer Staging System in Patients with Hepatocellular Carcinoma after Curative Intent Treatment
 DOI:10.22034/APJCP.2017.18.6.1697 RESEARCH ARTICLE Validation of The Hong Kong Liver Cancer Staging System in Patients with Hepatocellular Carcinoma after Curative Intent Treatment Alan Chuncharunee 1,
DOI:10.22034/APJCP.2017.18.6.1697 RESEARCH ARTICLE Validation of The Hong Kong Liver Cancer Staging System in Patients with Hepatocellular Carcinoma after Curative Intent Treatment Alan Chuncharunee 1,
The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page
 Vol.69(1), Page") The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page 1674-1679 Radioembolization in Treatment of Hepatocellular Carcinoma with Portal Vein Invasion Elsahhar Ahmed Hetta, Osama Mohamed
The Egyptian Journal of Hospital Medicine (October 2017) Vol.69(1), Page 1674-1679 Radioembolization in Treatment of Hepatocellular Carcinoma with Portal Vein Invasion Elsahhar Ahmed Hetta, Osama Mohamed
Locoregional Treatments for HCC Applications in Transplant Candidates. Locoregional Treatments for HCC Applications in Transplant Candidates
 Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
Impatto della clearance virale e rischio di carcinoma epatocellulare
 EPATITE CRONICA DA HCV: Impatto della clearance virale e rischio di carcinoma epatocellulare Rodolfo Sacco, M.D., PhD Direttore U.O.C. Gastroenterologia ed Endoscopia Digestiva A.O.U. Ospedali Riuniti"
EPATITE CRONICA DA HCV: Impatto della clearance virale e rischio di carcinoma epatocellulare Rodolfo Sacco, M.D., PhD Direttore U.O.C. Gastroenterologia ed Endoscopia Digestiva A.O.U. Ospedali Riuniti"
Evaluation of Liver Mass Lesions. American College of Gastroenterology 2013 Regional Postgraduate Course
 Evaluation of Liver Mass Lesions American College of Gastroenterology 2013 Regional Postgraduate Course Lewis R. Roberts, MB ChB, PhD Division of Gastroenterology and Hepatology Mayo Clinic College of
Evaluation of Liver Mass Lesions American College of Gastroenterology 2013 Regional Postgraduate Course Lewis R. Roberts, MB ChB, PhD Division of Gastroenterology and Hepatology Mayo Clinic College of
Obesity, Inflammation and Liver Cancer
 Obesity, Inflammation and Liver Cancer Richard Moreau, M.D., 1 INSERM U773, Centre de Recherche Biomédicale Bichat-Beaujon CRB3, 2 Université Denis Diderot Paris 7, 3 Service d Hépatologie, Hôpital Beaujon,
Obesity, Inflammation and Liver Cancer Richard Moreau, M.D., 1 INSERM U773, Centre de Recherche Biomédicale Bichat-Beaujon CRB3, 2 Université Denis Diderot Paris 7, 3 Service d Hépatologie, Hôpital Beaujon,
Advances in Systemic Therapy Hepatocellular Carcinoma (HCC) Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016
 Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016") Advances in Systemic Therapy for Hepatocellular Carcinoma (HCC) Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016 Scope Background Staging and treatment strategies Current systemic therapy
Advances in Systemic Therapy for Hepatocellular Carcinoma (HCC) Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016 Scope Background Staging and treatment strategies Current systemic therapy
Liver Cancer: Diagnosis and Treatment Options
 Liver Cancer: Diagnosis and Treatment Options Fred Poordad, MD Chief, Hepatology University Transplant Center Professor of Medicine UT Health, San Antonio VP, Academic and Clinical Affairs, Texas Liver
Liver Cancer: Diagnosis and Treatment Options Fred Poordad, MD Chief, Hepatology University Transplant Center Professor of Medicine UT Health, San Antonio VP, Academic and Clinical Affairs, Texas Liver
UPDATE TO THE MANAGEMENT OF PATIENTS WITH HCC HCA
 UPDATE TO THE MANAGEMENT OF PATIENTS WITH HCC HUSSEIN K. MOHAMED MD, FACS. Transplant and Hepato-biliary Surgery Largo Medical Center HCA DISCLOSURE I have no financial relationship(s) relevant to the
UPDATE TO THE MANAGEMENT OF PATIENTS WITH HCC HUSSEIN K. MOHAMED MD, FACS. Transplant and Hepato-biliary Surgery Largo Medical Center HCA DISCLOSURE I have no financial relationship(s) relevant to the
Locoregional Therapy for Hepatoma
 Locoregional Therapy for Hepatoma Robert D. Crane, MD Interventional Radiology Virginia Mason How do we know a liver mass is HCC? HCC : Bx Of pts getting liver transplant only ~ 5% had Bx to establish
Locoregional Therapy for Hepatoma Robert D. Crane, MD Interventional Radiology Virginia Mason How do we know a liver mass is HCC? HCC : Bx Of pts getting liver transplant only ~ 5% had Bx to establish
Are we adequately screening at-risk patients for hepatocellular carcinoma in the outpatient setting?
 Rajani Sharma, PGY1 Geriatrics CRC Project, 12/19/13 Are we adequately screening at-risk patients for hepatocellular carcinoma in the outpatient setting? A. Study Purpose and Rationale Hepatocellular carcinoma
Rajani Sharma, PGY1 Geriatrics CRC Project, 12/19/13 Are we adequately screening at-risk patients for hepatocellular carcinoma in the outpatient setting? A. Study Purpose and Rationale Hepatocellular carcinoma
Liver Cancer And Tumours
 Liver Cancer And Tumours What causes liver cancer? Many factors may play a role in the development of cancer. Because the liver filters blood from all parts of the body, cancer cells from elsewhere can
Liver Cancer And Tumours What causes liver cancer? Many factors may play a role in the development of cancer. Because the liver filters blood from all parts of the body, cancer cells from elsewhere can
Interventional Radiology in Liver Cancer. Nakarin Inmutto MD
 Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
Interventional Radiology in Liver Cancer Nakarin Inmutto MD Liver cancer Primary liver cancer Hepatocellular carcinoma Cholangiocarcinoma Metastasis Interventional Radiologist Diagnosis Imaging US / CT
Liver resection for HCC
 8 th LIVER INTEREST GROUP Annual Meeting Cape Town 2017 Liver resection for HCC Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre The liver is almost unique in that treatment of the
8 th LIVER INTEREST GROUP Annual Meeting Cape Town 2017 Liver resection for HCC Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre The liver is almost unique in that treatment of the
Diagnosis, Staging and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases
 Diagnosis, Staging and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases Jorge A. Marrero, MD, MS, MSHM; Laura M. Kulik, MD; Claude
Diagnosis, Staging and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases Jorge A. Marrero, MD, MS, MSHM; Laura M. Kulik, MD; Claude
PEER-REVIEW REPORT CLASSIFICATION LANGUAGE EVALUATION SCIENTIFIC MISCONDUCT CONCLUSION. [ Y] Accept [ ] Grade B: Very good
![PEER-REVIEW REPORT CLASSIFICATION LANGUAGE EVALUATION SCIENTIFIC MISCONDUCT CONCLUSION. [ Y] Accept [ ] Grade B: Very good](/thumbs/96/127805416.jpg "PEER-REVIEW REPORT CLASSIFICATION LANGUAGE EVALUATION SCIENTIFIC MISCONDUCT CONCLUSION. [ Y] Accept [ ] Grade B: Very good") Reviewer s code: 03656588 Reviewer s country: China Date reviewed: 2017-06-08 [ ] Grade A: Excellent [ Y] Accept [ ] Grade B: Very good [ ] High priority for [ Y] Grade C: Good language [ ] Major revision
Reviewer s code: 03656588 Reviewer s country: China Date reviewed: 2017-06-08 [ ] Grade A: Excellent [ Y] Accept [ ] Grade B: Very good [ ] High priority for [ Y] Grade C: Good language [ ] Major revision
Aggressive Treatment of Performance Status 1 and 2 HCC Patients Significantly Improves Survival - an Egyptian Retrospective Cohort Study of 524 Cases
 RESEARCH ARTICLE Aggressive Treatment of Performance Status 1 and 2 HCC Patients Significantly Improves Survival - an Egyptian Retrospective Cohort Study of 524 Cases Ashraf Omar Abdel Aziz 1, Dalia Omran
RESEARCH ARTICLE Aggressive Treatment of Performance Status 1 and 2 HCC Patients Significantly Improves Survival - an Egyptian Retrospective Cohort Study of 524 Cases Ashraf Omar Abdel Aziz 1, Dalia Omran
Innovations in HCC Imaging: MDCT/MRI
 Innovations in HCC Imaging: MDCT/MRI Anthony E. Cheng, M.D. Cardinal MRI Center Cardinal Santos Medical Center, Wilson Street, San Juan Innovations in HCC Imaging: Goals/Objectives MDCT/MRI Learn the diagnostic
Innovations in HCC Imaging: MDCT/MRI Anthony E. Cheng, M.D. Cardinal MRI Center Cardinal Santos Medical Center, Wilson Street, San Juan Innovations in HCC Imaging: Goals/Objectives MDCT/MRI Learn the diagnostic
Consensus AASLD-EASL HBV Treatment Endpoint and HBV Cure Definition
 Consensus AASLD-EASL HBV Treatment Endpoint and HBV Cure Definition Anna S. Lok, MD, DSc Alice Lohrman Andrews Professor in Hepatology Director of Clinical Hepatology Assistant Dean for Clinical Research
Consensus AASLD-EASL HBV Treatment Endpoint and HBV Cure Definition Anna S. Lok, MD, DSc Alice Lohrman Andrews Professor in Hepatology Director of Clinical Hepatology Assistant Dean for Clinical Research
Hepatocellular Carcinoma in Qatar
 Hepatocellular Carcinoma in Qatar K. I. Rasul 1, S. H. Al-Azawi 1, P. Chandra 2 1 NCCCR, 2 Medical Research Centre, Hamad Medical Corporation, Doha, Qatar Abstract Objective The main aim of this study
Hepatocellular Carcinoma in Qatar K. I. Rasul 1, S. H. Al-Azawi 1, P. Chandra 2 1 NCCCR, 2 Medical Research Centre, Hamad Medical Corporation, Doha, Qatar Abstract Objective The main aim of this study
National Surgical Adjuvant Breast and Bowel Project (NSABP) Foundation Annual Progress Report: 2009 Formula Grant
 Foundation Annual Progress Report: 2009 Formula Grant") National Surgical Adjuvant Breast and Bowel Project (NSABP) Foundation Annual Progress Report: 2009 Formula Grant Reporting Period July 1, 2012 June 30, 2013 Formula Grant Overview The National Surgical
National Surgical Adjuvant Breast and Bowel Project (NSABP) Foundation Annual Progress Report: 2009 Formula Grant Reporting Period July 1, 2012 June 30, 2013 Formula Grant Overview The National Surgical
Microarray Analysis and Liver Diseases
 Microarray Analysis and Liver Diseases Snorri S. Thorgeirsson M.D., Ph.D. Laboratory of Experimental Carcinogenesis Center for Cancer Research, NCI, NIH Application of Microarrays to Cancer Research Identifying
Microarray Analysis and Liver Diseases Snorri S. Thorgeirsson M.D., Ph.D. Laboratory of Experimental Carcinogenesis Center for Cancer Research, NCI, NIH Application of Microarrays to Cancer Research Identifying
Il treatment plan nella terapia sistemica dell epatocarcinoma
 Il treatment plan nella terapia sistemica dell epatocarcinoma M. Iavarone, MD PhD CRC A.M. e A. Migliavacca Center for the Study of Liver Disease Division of Gastroenterology and Hepatology Fondazione
Il treatment plan nella terapia sistemica dell epatocarcinoma M. Iavarone, MD PhD CRC A.M. e A. Migliavacca Center for the Study of Liver Disease Division of Gastroenterology and Hepatology Fondazione
HCC RADIOLOGIC DIAGNOSIS
 UCSF Transplant 2010 THE BEFORE AND AFTER HEPATOCELLULAR CARCINOMA MANAGEMENT Francis Yao, M.D. Professor of Clinical Medicine and Surgery Medical Director, Liver Transplantation University of California,
UCSF Transplant 2010 THE BEFORE AND AFTER HEPATOCELLULAR CARCINOMA MANAGEMENT Francis Yao, M.D. Professor of Clinical Medicine and Surgery Medical Director, Liver Transplantation University of California,
6/16/2016. Treating Hepatocellular Carcinoma: Deciphering the Clinical Data. Liver Regeneration. Liver Regeneration
 Treating : Deciphering the Clinical Data Derek DuBay, MD Associate Professor of Surgery Director of Liver Transplant Liver Transplant and Hepatobiliary Surgery UAB Department of Surgery Liver Regeneration
Treating : Deciphering the Clinical Data Derek DuBay, MD Associate Professor of Surgery Director of Liver Transplant Liver Transplant and Hepatobiliary Surgery UAB Department of Surgery Liver Regeneration
1. Basic principles 2. 6 hallmark features 3. Abnormal cell proliferation: mechanisms 4. Carcinogens: examples. Major Principles:
 Carcinogenesis 1. Basic principles 2. 6 hallmark features 3. Abnormal cell proliferation: mechanisms 4. Carcinogens: examples Carcinogenesis Major Principles: 1. Nonlethal genetic damage is central to
Carcinogenesis 1. Basic principles 2. 6 hallmark features 3. Abnormal cell proliferation: mechanisms 4. Carcinogens: examples Carcinogenesis Major Principles: 1. Nonlethal genetic damage is central to
Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging
 Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Hepatobiliary and Pancreatic Surgery Chief of Hepatobiliary and Pancreatic Surgery
Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Hepatobiliary and Pancreatic Surgery Chief of Hepatobiliary and Pancreatic Surgery
Synergistic combinations of targeted immunotherapy to combat cancer
 Synergistic combinations of targeted immunotherapy to combat cancer Myung Ah Lee, M.D., Ph. D Division of Medical Oncology, Hepato-biliary pancreatic cancer center Seoul St. Mary s hospital, The Catholic
Synergistic combinations of targeted immunotherapy to combat cancer Myung Ah Lee, M.D., Ph. D Division of Medical Oncology, Hepato-biliary pancreatic cancer center Seoul St. Mary s hospital, The Catholic
HIV and Hepatocellular Carcinoma. Dr Kosh Agarwal Institute of Liver Studies King s College Hospital Rome May 2013
 HIV and Hepatocellular Carcinoma Dr Kosh Agarwal Institute of Liver Studies King s College Hospital Rome May 2013 1 In theory, there is no difference between theory and practice In practice there is Chuck
HIV and Hepatocellular Carcinoma Dr Kosh Agarwal Institute of Liver Studies King s College Hospital Rome May 2013 1 In theory, there is no difference between theory and practice In practice there is Chuck
LIVER CANCER: NOVEL ADVANCEMENTS IN 2018
 MOUNT SINAI LIVER CANCER PROGRAM 13 TH ANNIVERSARY NOVEL ADVANCEMENTS IN 2018 FRIDAY, DECEMBER 14, 2018 Hatch Auditorium 1468 Madison Avenue, 2 nd floor New York, NY Program Director JOSEP M. LLOVET, MD,
MOUNT SINAI LIVER CANCER PROGRAM 13 TH ANNIVERSARY NOVEL ADVANCEMENTS IN 2018 FRIDAY, DECEMBER 14, 2018 Hatch Auditorium 1468 Madison Avenue, 2 nd floor New York, NY Program Director JOSEP M. LLOVET, MD,
The Chronic Liver Disease Foundation (CLDF) and the International Coalition of Hepatology Education Providers (IC-HEP) present:
 and the International Coalition of Hepatology Education Providers (IC-HEP) present:") The Chronic Liver Disease Foundation (CLDF) and the International Coalition of Hepatology Education Providers (IC-HEP) present: Certified by: Provided by: Endorsed by: Hepatocellular Carcinoma HCC: Age
The Chronic Liver Disease Foundation (CLDF) and the International Coalition of Hepatology Education Providers (IC-HEP) present: Certified by: Provided by: Endorsed by: Hepatocellular Carcinoma HCC: Age
Management of HepatoCellular Carcinoma
 9th Symposium GIC St Louis - 2010 Management of HepatoCellular Carcinoma Overview Pierre A. Clavien, MD, PhD Department of Surgery University Hospital Zurich Zurich, Switzerland Hepatocellular carcinoma
9th Symposium GIC St Louis - 2010 Management of HepatoCellular Carcinoma Overview Pierre A. Clavien, MD, PhD Department of Surgery University Hospital Zurich Zurich, Switzerland Hepatocellular carcinoma
Posters and Presentations
 Posters and Presentations June 2017: American Society of Clinical Oncology (ASCO) Annual - Preliminary Correlative Analysis of PD-L1 expression from the SUNRISE Study. View April 2017: American Association
Posters and Presentations June 2017: American Society of Clinical Oncology (ASCO) Annual - Preliminary Correlative Analysis of PD-L1 expression from the SUNRISE Study. View April 2017: American Association
Alastair Burt Newcastle University
 Alastair Burt Newcastle University Benign Hepatocellular adenoma 8170/0 Focal nodular hyperplasia Malignancy-associated and premalignant lesions Large cell change (formerly dysplasia ) Small cell change
Alastair Burt Newcastle University Benign Hepatocellular adenoma 8170/0 Focal nodular hyperplasia Malignancy-associated and premalignant lesions Large cell change (formerly dysplasia ) Small cell change
Effective Health Care Program
 Comparative Effectiveness Review Number 143 Effective Health Care Program Techniques for the Diagnosis and Staging of Hepatocellular Carcinoma Executive Background and Objectives Hepatocellular carcinoma
Comparative Effectiveness Review Number 143 Effective Health Care Program Techniques for the Diagnosis and Staging of Hepatocellular Carcinoma Executive Background and Objectives Hepatocellular carcinoma
Translating Research into Clinical Practice: Strategies Against Hepatocellular Cancer
 Translating Research into Clinical Practice: Strategies Against Hepatocellular Cancer Kevin Staveley-O Carroll, PhD, MD, FACS Professor and Chair, Department of Surgery Director of the Ellis Fischel Cancer
Translating Research into Clinical Practice: Strategies Against Hepatocellular Cancer Kevin Staveley-O Carroll, PhD, MD, FACS Professor and Chair, Department of Surgery Director of the Ellis Fischel Cancer
Pamplona, junio de Futuro de la Hepatología: Cáncer Hepático. Bruno Sangro Clínica Universidad de Navarra. IDISNA. CIBERehd.
 Pamplona, junio de 2008 Futuro de la Hepatología: Cáncer Hepático Bruno Sangro Clínica Universidad de Navarra. IDISNA. CIBERehd. Pamplona, Spain Etiología del Cáncer Hepático HBV HCV Alcohol NAFLD Iron
Pamplona, junio de 2008 Futuro de la Hepatología: Cáncer Hepático Bruno Sangro Clínica Universidad de Navarra. IDISNA. CIBERehd. Pamplona, Spain Etiología del Cáncer Hepático HBV HCV Alcohol NAFLD Iron
RESEARCH ARTICLE. Real Life Treatment of Hepatocellular Carcinoma: Impact of Deviation from Guidelines for Recommended Therapy
 DOI:http://dx.doi.org/10.7314/APJCP.2015.16.16.6929 Real-Life HCC Treatment - Influence on Outcome of Deviation from Therapy Guidelines RESEARCH ARTICLE Real Life Treatment of Hepatocellular Carcinoma:
DOI:http://dx.doi.org/10.7314/APJCP.2015.16.16.6929 Real-Life HCC Treatment - Influence on Outcome of Deviation from Therapy Guidelines RESEARCH ARTICLE Real Life Treatment of Hepatocellular Carcinoma:
Hepatocellular carcinoma: from guidelines to individualized treatment
 AISF 2012 Rome, 22-24 February 2012 Hepatocellular carcinoma: from guidelines to individualized treatment A.D. 1088 Luigi Bolondi Professor of Medicine, Chairman Department of Digestive Diseases and Internal
AISF 2012 Rome, 22-24 February 2012 Hepatocellular carcinoma: from guidelines to individualized treatment A.D. 1088 Luigi Bolondi Professor of Medicine, Chairman Department of Digestive Diseases and Internal
«Εκτίμηση κινδφνου ανάπτυξης ΗΚΚ σε ασθενείς με HCV λοίμωξη» Evaluation of HCC risk in HCV patients
 «Εκτίμηση κινδφνου ανάπτυξης ΗΚΚ σε ασθενείς με HCV λοίμωξη» Evaluation of HCC risk in HCV patients Δημήτρησ Ν. αμωνάκησ Γαςτρεντερολογική κλινική Πανεπιςτημίου Κρήτησ Outline Epidemiology Risk factors
«Εκτίμηση κινδφνου ανάπτυξης ΗΚΚ σε ασθενείς με HCV λοίμωξη» Evaluation of HCC risk in HCV patients Δημήτρησ Ν. αμωνάκησ Γαςτρεντερολογική κλινική Πανεπιςτημίου Κρήτησ Outline Epidemiology Risk factors
Guidelines for SIRT in HCC An Evolution
 Guidelines for SIRT in HCC An Evolution 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore The challenge of HCC Surgery is potentially curative in early
Guidelines for SIRT in HCC An Evolution 2 nd Asia Pacific Symposium on Liver- Directed Y-90 Microspheres Therapy 1st November 2014, Singapore The challenge of HCC Surgery is potentially curative in early
Advances in percutaneous ablation and systemic therapies for hepatocellular carcinoma
 Advances in percutaneous ablation and systemic therapies for hepatocellular carcinoma Paris Hepatology Congress 2019 Pierre Nahon Service d Hépatologie Hôpital Jean Verdier Bondy Université Paris 13 INSERM
Advances in percutaneous ablation and systemic therapies for hepatocellular carcinoma Paris Hepatology Congress 2019 Pierre Nahon Service d Hépatologie Hôpital Jean Verdier Bondy Université Paris 13 INSERM
BIT 120. Copy of Cancer/HIV Lecture
 BIT 120 Copy of Cancer/HIV Lecture Cancer DEFINITION Any abnormal growth of cells that has malignant potential i.e.. Leukemia Uncontrolled mitosis in WBC Genetic disease caused by an accumulation of mutations
BIT 120 Copy of Cancer/HIV Lecture Cancer DEFINITION Any abnormal growth of cells that has malignant potential i.e.. Leukemia Uncontrolled mitosis in WBC Genetic disease caused by an accumulation of mutations
Carcinogenesis. Carcinogenesis. 1. Basic principles 2. 6 hallmark features 3. Abnormal cell proliferation: mechanisms 4. Carcinogens: examples
 Carcinogenesis 1. Basic principles 2. 6 hallmark features 3. Abnormal cell proliferation: mechanisms 4. Carcinogens: examples Major Principles (cont d) 4. Principle targets of genetic damage: 4 classes
Carcinogenesis 1. Basic principles 2. 6 hallmark features 3. Abnormal cell proliferation: mechanisms 4. Carcinogens: examples Major Principles (cont d) 4. Principle targets of genetic damage: 4 classes
Liver Tumors. Prof. Dr. Ahmed El - Samongy
 Liver Tumors Prof. Dr. Ahmed El - Samongy Objective 1. Identify the most important features of common benign liver tumors 2. Know the risk factors, diagnosis, and management of hepatocellular carcinoma
Liver Tumors Prof. Dr. Ahmed El - Samongy Objective 1. Identify the most important features of common benign liver tumors 2. Know the risk factors, diagnosis, and management of hepatocellular carcinoma
Conducting Successful Oncology Clinical Trials in Asia Pacific: PharmaNet experience using Case Studies
 Conducting Successful Oncology Clinical Trials in Asia Pacific: PharmaNet experience using Case Studies Emily Tan Executive Director Asia Pacific PharmaNet Conducting Successful Oncology Clinical Trials
Conducting Successful Oncology Clinical Trials in Asia Pacific: PharmaNet experience using Case Studies Emily Tan Executive Director Asia Pacific PharmaNet Conducting Successful Oncology Clinical Trials