Alcohol Abuse a really quick review
|
|
|
- Sherman Collins
- 6 years ago
- Views:
Transcription
1 Alcohol Abuse a really quick review Anthony Albanese, M.D. Associate Clinical Professor of Medicine & Psychiatry, UC Davis Medical School Director, Chemical Dependency & Hepatology Programs Sacramento VA Medical Center
2 DISCLAIMER I have no pertinent financial relationships to disclose.
3 Objectives Review the topic of Alcohol Abuse in preparation for the ABAM Board Examination, with special attention to Epidemiological characteristics Medical and behavioral symptoms Pharmacology/acute intoxication Detoxification Pharmacologic and non-pharmacologic Tx Issues related to pregnancy
4 Since our earliest days, there has been a desire in us to experiment with alcohol Genesis 9: And Noah began to be a farmer, and he planted a vineyard. Then, he drank of the wine and was drunk, and became uncovered in his tent.
5 Since our earliest days, there has been a desire in us to experiment with alcohol Genesis 19:33,35,36 - So they made their father (Lot) drink wine that night. And the firstborn went in and lay with her father and he did not know when she lay down or when she arose.then they made their father drink wine that night also. And the younger arose and lay with him and he did not know when she lay down or when she arose. Thus both the daughters of Lot were with child by their father.

6

7 Per capita ethanol consumption by beverage type, United States, Source: Lakins, N.E.; LaVallee, R.A.; Williams, G.D.; and Yi, H. Surveillance Report #85: Apparent Per Capita Alcohol Consumption: National, State, and Regional Trends, Bethesda, MD: NIAAA, Division of Epidemiology and Prevention Research, Alcohol Epidemiologic Data System, November 2008,

8 Substances for Which Most Recent Treatment Was Received in the Past Year among Persons Aged 12 or Older: 2009 Source: NSDUH 2009, SAMHSA

9 Alcohol Dependence or Abuse in the Past Year among Adults Aged 21 or Older, by Age at First Use of Alcohol: 2009 Source: NSDUH 2009, SAMHSA

10 Current, Binge, and Heavy Alcohol Use among Persons Aged 12 or Older, by Race/Ethnicity: 2009 Source: NSDUH 2009, SAMHSA

11

12 Age-adjusted death rates of liver cirrhosis by sex and race, United States, Source: Yoon, Y.H.; and Yi, H. Surveillance Report #83: Liver Cirrhosis Mortality in the United States, Bethesda, MD: NIAAA, Division of Epidemiology and Prevention Research, Alcohol Epidemiologic Data System, August 2008,

13 Percentage of alcohol involvement among drivers in fatal traffic crashes, according to age, United States, 1998 and 2004 Source: Yi, H.; Chen, C.M.; and Williams, G.D. Surveillance Report #76: Trends in Alcohol-Related Fatal Traffic Crashes, United States, Bethesda, MD: NIAAA, Division of Epidemiology and Prevention Research, Alcohol Epidemiologic Data System, August 2006,

14

15
16 National Longitudinal Alcohol Epidemiologic Survey ,862 face to face interviews, Americans 18 or older. 66% consumed alcohol 49% had first drink before 21 3% had first drink before % alcohol abuse 3% met criteria for alcohol dependent Alcohol use before 14 triples likelihood of being injured while drinking.

17

18
19 Alcohol Dependence Type 2 (B) - Begins drinking heavily at an early age (before 12 y/o) - often uses other drugs in combination with alcohol. Experiences medical, legal,and social complications in teens and twenties. Type 1 (A)- slower, more classic pattern of progression. ~ 75% males alcoholics. Low degree of novelty seeking, fighting, etc.
20
21 DSM Criteria for Alcohol Withdrawal (2 or more) Autonomic hyperactivity (sweating or p > 100) Increased hand tremor Insomnia Nausea & Vomiting Visual, tactile, or auditory hallucinations or illusions Psychomotor agitation Anxiety Grand mal seizures
22 DSM Criteria for Alcohol Withdrawal A. Cessation of heavy alcohol use B. Two or more of preceding symptom list C. Symptoms cause clinically significant distress or impairment in social, occupational or other important areas of function D. Symptoms not due to other general medical condition or mental disorder
23 Systems Affected by Alcohol ( partial list) CNS- great mimicker of psychiatric disorders, decreased sleep latency, blackout, peripheral neuropathy Wernike s and Korsakoff s syndromes, cerebellar degeneration, dementia s GI- esophagitis, gastritis, enteritis, increased gastric acid production, lowers LES tone, promotes absorption of iron, interferes with absorption of some B vitamins, toxic to pancreas, associated with esophageal, gastric, pancreatic, hepatoma,and colon cancer. Fatty liver, cirrhosis. Hematopoietic- pancytopenia, toxic granulocytosis, elevated MCV.
24 Systems Affected by Alcohol ( partial list) Cardiovascular- increases HDL, 1-2 drinks per day may decrease the risk of cardiac death. decreases myocardial contractility, peripheral vasodilatation- decreases BP in low doseincreases BP long term in high doses, cardiomyopathy, arrhythmias, holiday heart. GU- modest doses increase sex drive- but decrease erectile capacity, testicular atrophy with shrinkage of the seminiferous tubules, amenorrhea, decreased ovarian size, infertility and spontaneous abortions. Other- Fetal alcohol syndrome, alcoholic myopathy, osteonecrosis with increased fractures and avascular necrosis of the femoral heads, modest reversible decreases in T3 & T4
25 Risk of Drinking During Pregnancy Fetal Alcohol Syndrome (FAS) First described in 1968 syndrome noted in 1:300 to 1:1000 live births in U.S. No safe use pattern in pregnancy has been established. Some degree of mental retardation noted in 85% of children with FAS Hyperactivity, Speech problems, cerebellar dysfunction common later in life.
26 Fetal Alcohol Syndrome Fetal growth retardation in weight, length, and height Facial dysmorphism characterized by: short palpebral fissures, hypoplastic maxilla, short upturned nose, flat philtrum, thin upper vermillion border, micrognathia or retrognathia, posteriorly rotated ears, occ. Cleft lip or palate, etc. Severe CNS dysfunction: irritability, tremulousness, inconsolable crying, hypertonia, seizures

27 Fetal Alcohol Syndrome Source: Warren, K.R. et al. Alcohol Research & Health
28 Women and Alcohol: Women have less alcohol dehydrogenase in their stomach lining this leads to higher blood alcohol levels in women than you would expect based on weight considerations alone
29 WHY DRINK??? Prohibition the noble experiment ended in 1933! It s our right! Solomon wrote in Ecclesiastes 9:15 So I recommend having fun, because there is nothing better for people to do in this world than to eat, drink, and enjoy life

30

31

32

33
 -- euphoria and perceived reduction in anxiety With.06-.")
 -- sedation With 0.30-0.")
34 Possible Behaviors with Alcohol Ingestion ( non dependant 70kg man) With g/dl BAC (1 to 2 drinks) -- euphoria and perceived reduction in anxiety With g/dl BAC (3 to 5 drinks) -- judgment and motor coordination impaired, sometimes increased aggression With g/dl BAC (10 to 13 drinks) -- sedation With g/dl BAC -- memory impairment and loss of consciousness With 0.40 to 0.60 g/dl BAC -- depressed respiration, coma, death

 than men (58%) of comparable size")


35 Differences in Alcohol Metabolism Between Men and Women Women are smaller than men Women have lower total body water content (49%) than men (58%) of comparable size Gastric ADH lower in women Fluctuations in gonadal hormone levels during the menstrual cycle may affect the rate of alcohol metabolism Alcohol Alerts #10 & #46 - NIAAA
36 Major Alcohol Metabolic Pathway (85%) Ethanol NAD NADH Alcohol DH NAD Acetaldehyde NADH Aldehyde DH Biosynthesis Acetic Acid CO 2 + H 2 O Release to Blood
37 Considerations Microsomal ethanol oxidizing system (MEOS CYP 2E1) also important in first step. There are 3 genes that encode hepatic ADH (1-3),with alpha, beta and gamma subunits. ADH sigma - gastric mucosa Aldehyde dehydrogenase (ALDH) has 2 types. ALDH 2*1 is most active. ALDH 2*2 is less active, and in ~50% of Chinese and Japanese groups.
38 Minor Metabolic Pathways 10% ethanol can be excreted unchanged in urine, sweat, saliva, and breath. 5% of ethanol passing through the liver may be conjugate to inactive ethyl glucuronide (EG). EG can be measured in blood, saliva, urine, and hair.


39 Metabolism Rate (zero order kinetics) Relatively fixed- independent of blood concentration 80% of adult population-.015 g/dl/hr For moderate to heavy drinkers g/dl/hr
40 Estimation of BAC BAC = # Drinks x 14g/drink x.806 x 100ml/dl -.015g/dl /hr x T(hrs) Body wt (Kg) x FW (ml/g) x 1000g/kg FW = Fractional water M=.58 ml/g W=.49 ml/g.806g/ml is the constant amount of water per blood volume ( 80.6%).015 g/dl/hr is the metabolism rate for alcohol ( may vary with heavy drinkers) Example 5 beers x 14g / 86 kg x.58 ml/g x 1000g/kg = 70g/49,000 ml = x.806 g/ml = g/ml x 100 ml/dl =.115 g/dl = BAC

41
42 Diagnosis- is there a problem? Addiction Severity Index (ASI) 200 items, 7 subscales trained interviewer ~1 hour to administer and score. Free- Alcohol Dependence Scale (ADS)- 25 items, 5 minutes to administer- copyrighted- Alcohol Use Disorders Identification Test (AUDIT)- 10 item screening questionnaire copyrighted by WHO- Free- CAGE- 4 questions asked during history.
43 AUDIT: Alcohol Use Disorders Identification Test 10 items, 4 points each Maximum score 40 Usual cutoff >8 Identifies problem (hazardous) drinking and abuse and dependence May miss past problems

44
45 AUDIT score >8 Hazardous or harmful drinking Sensitivity 57-95% Specificity 78-96% Abuse or dependence Sensitivity 61-96% Specificity 85-96% Fiellin DA, O Connor PG. Ann Intern Med 2000;133:815-27
46 CAGE Questions Have you ever felt you should Cut down on your drinking? Have people Annoyed you by criticizing your drinking? Have you ever felt bad or Guilty about your drinking? Have you ever taken a drink first thing in the morning (Eye-opener) to steady your nerves or get rid of a hangover?
47 CAGE With two questions answered positively: Sensitivity = 60% - 95% Specificity = 40% - 95% Can miss binge drinkers Beresford,et.al Lancet 336:
48 Diagnosis- is there a problem? Drinker Inventory of Consequences (DrInC)- 50 question self administered. Michigan Alcohol Screening Test (MAST) 25 item questionnaire- self administered or interview. Also Brief MAST, SMAST, MAST-G, Mm-MAST. Free- Self Administered Alcoholism Screening Test ( SAAST)-37 questions- copyrighted

49
50 Possible LAB Findings Gamma-glutamyl Transpeptidase (GGT)- most widely used, accurate marker for heavy alcohol consumption-production may be stimulated by alcohol, and cell damage may cause leakage. Also elevated in steatohepatitis and biliary tract disease Aspartate Aminotransferase (AST)- increased in liver damage associated with alcohol intake, but not very sensitive or specific. Mean Corpuscular Volume ( MCV)- increased as a direct result of the toxic effect of alcohol, but can be elevated by many other causes. More specific when used with GGT in absence of cirrhosis.
51 Possible LAB Findings Carbohydrate-deficent Transferrin ( CDT)-chronic alcohol consumption decreases the number of carbohydrate moieties (galactose, N-acetylglucosamine, sialic acid, mannose, etc.) attached to transferrin. Effect most evident at >3 drinks per day. Marker combinations are more sensitive and specific (CDT+ GGT), (GGT+MCV) Ethyl Glucuronide is not a marker, but a direct measure of an alcohol metabolite. This test is readily available. Combination of lab findings and clinic hx is best.
52 Detox- yes, no, maybe? Detoxicification implies safely separating the patient from the toxic effect of the drug. It may or may not require pharmaceutical assistance. The goal is to prevent harmful sequelae (such as withdrawal seizures, Delirium Tremens, acute psychotic episodes, and irrational dangerous behaviors.
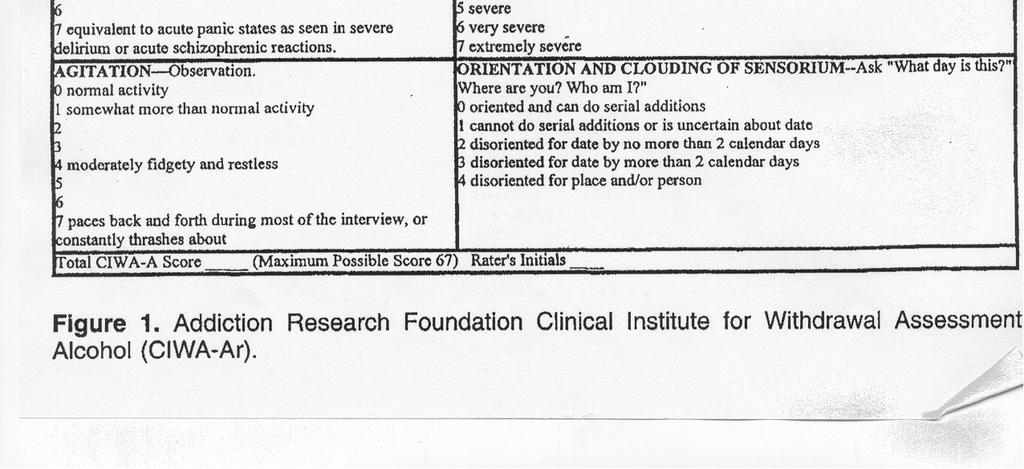
53 CIWA-Ar Clinical Institute Withdrawal Assessment - revised version (CIWA-Ar) - Structured Severity Assessment Scale -Objective Scale for use by health care personnel to evaluate patients at risk for developing alcohol withdrawal syndromes, and quantify the severity of withdrawal. Detox language - to relate severity of symptoms to clinic and non-clinical reviewers.
54 Clinical Institute Withdrawal Assessment for Alcohol Scale-revised (CIWA-Ar) 10 item rating system for alcohol withdrawal severity max of 67 points: 0- no symptoms 1- Mild 4- Moderate 7- Severe BP and HR not found to correlate with severity of withdrawal Can be given in under 2 minutes Sullivan,J.T. British Journal of Addiction, 1989; 84:
55 Clinical Institute Withdrawal Assessment for Alcohol Scale-revised (CIWA-Ar) 1. Nausea and vomiting 2. Tremor 3. Paroxysmal sweating 4. Anxiety 5. Agitation 6. Tactile disturbances 7. Visual disturbances 8. Auditory disturbances 9. Headache or fullness 10. Orientation (0-4 points) Sullivan,J.T. British Journal of Addiction, 1989; 84:
56 CIWA-Ar High scores are predictive of development of seizures and delirium. <8 = mild symptoms 9-15 = moderate symptoms > 15 = severe symptoms-high risk Scale is currently being used for medication administration at many detoxification centers. Using the CIWA-Ar was found to reduce side effects from over-sedation costs by avoiding unnecessary use of medications.


57
58 Detoxification Inpatient (levels 3 & 4) is easier because it removes Pt. from home environment and demonstrates round-the clock medical support if needed. May be pharmaceutically assisted (preferably with a symptom triggered, fixed dose, or front-loaded technique). Should be combined with some form of rehab.
59 Which Detox Method is Best? Working Group from ASAM published an evidence bases practice guideline on Pharmacological Management of Alcohol Withdrawal- JAMA July 9,1997. Meta-analysis reviewing 134 articles including 65 prospective controlled trials involving 42 medications.
60 Outcomes Reviewed 1. Severity of withdrawal syndrome 2. Alcohol Withdrawal Delirium 3. Withdrawal Seizures 4. Completion of withdrawal 5. Entry into Rehab 6. Cost
61 Benzodiazepines Reduction of alcohol withdrawal symptoms in six prospective trials with: Chlordiazepoxide Diazepam Lorazepam Overall reduction of seizures (7.7 per 100 treated) Reduction of delirium tremens (4.9 per 100 treated) All were equally efficacious* Mayo-Smith, M et al. Pharmacological Management of Alcohol Withdrawal. JAMA. 1997;278:
62 Results Treatment should be individualized. Benzodiazapines work best for moderate to severe withdrawal. Carbamazepine may also be useful. Neuroleptics may decrease delerium in combination with benzo s but are less effective as mono-therapy and may low seizure threshold. Thiamine administration on admission may prevent Wernike-Korsakoff s in high risk pt B-blockers, Clonidine, Mg generally not helpful.
63 My Personal Advise Be sure your staff is able and willing to use the CIWA-Ar in timely and correct fashion if you are going to use a purely symptom triggered protocol with short acting benzodiazapines.
64 Sample Detox Protocols Diazepam 10mg every 4 hours while awake x 24h +/- lorazepam prn (>10), then QID x 24h prn, then 5mg QIDx24h prn, then 2mg QID prn x24h then d/c. Lorazepam 2mg -repeat in 1 hr for CIWA- Ar >8, then give every 4 hours prn (>8) x 48h, then decrease to 1mg every 4h prn.
65 Sample Detox Protocols Carbamazapine- 200mg QID on day one, then 200mg TID day 2, then BID, then QD. Chlordiazepoxide 50mg QID while awake on day one, the 50mg TID prn on day 2, then 25mg prn day 3-4 ( >8).
66 TIME Sedative Detoxification (front-loading technique) Sedative level Seizure risk D.T. risk
67 Metabolism of Selected Benzodiazapines chlordiazepoxide diazepam desmethylchlordiazepoxide demoxepam desmethyldiazepam nordiazepam nordiazepam oxazepam oxazepam
68 Contraindications to long-acting sedative use for detoxification Medically unstable patients. Patients with decompensated liver disease (acute or chronic). Unexplained delirium. Respiratory compromise. Consider use of lorazepam which is conjugated to the inactive glucuronide.
69 Detoxification During Pregnancy Benzodiazapines, barbiturates, and carbamazapine all have potential fetal toxicities. Benzo s are the treatment of choice -dosed to relieve signs& symptoms. They are all significantly less teratogenic than alcohol. Detox should be performed in an inpatient setting with OB/GYN consultation.

70
71 FDA Approved Options for treatment of alcohol dependency Disulfiram Inhibits aldehyde dehydrogenase- cause nausea, vomiting, flushing, headache with alcohol intake. Black box warning- safety issues Naltrexone - oral and injectable Reduces reward from alcohol by blocking opioid receptors- Black box warning- safety issues Acamprosate Thought to inhibit action of glutamate on NMDA receptor and interact with GABA system
72 Disulfiram Effective therapy- dosed 125mg-500mg daily (avg~ 250mg/day). Doses should be dissolved in water and observed to insure compliance. LFT s must be monitored closely in the first 4 months of therapy ( weekly for 4 weeks, then biweekly for 4 weeks, then monthly). Has been associated with acute liver failure (idiosyncratic).
73 Naltrexone Has been demonstrated in multiple double blind placebo controlled studies to significantly decrease relapse drinking (23% vs 54.3%) over 12 weeks.* Dose is 50mg -100mg daily ( some start with 25mg dose and titrate up). Pt s must carry naltrexone card. Thought to block reward via opioid system from elevated endorphins and enkephalins noted with alcohol use. May work best in patients with OPRM1 Asp40 allele ** Volpicelli et al Arch Gen Psych;49;1992. pp Anton RF,et al. Arch Gen Psychiatry 2008 Feb;65(2):
74 Naltrexone VA study Dec 13, 2001 NEJM 627 veterans given 12 mo Naltrexone, or 3 mo. Naltrexone and 9 mo placebo, or 12 mo placebo No statistically significant difference in # days to relapse at 13 weeks, and no difference in % days drinking at 52 weeks Krystal, et al. NEJM Volume 345, pg , Dec 13, 2001
75 Naltrexone COMBINE STUDY 1383 pts -11 academic sites, 100mg/day dose given for 16 weeks More efficacious than placebo in increasing percentage of days of abstinence (80.6% vs 75.1%) Reduced risk of heavy drinking day (66.2% vs 73.1%) Good Clinical Outcome 73.7% vs 58.2% Women had similar response to men on re-analysis* 1)Anton RF,JAMA,2006;295: )Greenfield SF, Alcohol Clin Exp Res 2010 Jul 20
76 Naltrexone Extension of COMBINE study published in 2008 looked at efficacy of intervention 1 year post treatment. Drinking behavior and clinical status assessed at weeks 26, 52 and 68. Patients treated with medical management and either combined behavioral intervention or naltrexone or both had sustained benefit. Donovan DM, J Stud Alcohol Drugs, 2008 Jan;69(1):5-13
77 Naltrexone XR Injectable microspheres <100 microns in size injected intramuscluarly. Mu blockade effective for about 4 weeks. In a 6 month randomized double blind placebo controlled study with psychosocial intervention, 624 pts in 3 armsdemonstrated 25% decrease in heavy drinking days with 380mg dose. Garbutt JC, et.al JAMA 2005; 293:
78 Naltrexone Must be used with caution in patients with liver disease Can not be used in patients using opioids for pain management. Injectable naltrexone XR pharmacokinetics may be altered by age, creatinine clearance, smoking, alcohol and opioid use though not clinically significantly.* Compliance is a problem Dunbar JL, J Stud Alcohol Drugs Nov;68(6):862-70
79 Acamprosate Usual dose is 666 mg three times a day (1998 mg/day). Data on efficacy has been conflicting ( no efficacy in the COMBINE trial) There are multiple good studies that show efficacy for abstinence, and meta-analysis of 17 studies (4087 pts) that show improved 6 month abstinence rates (36.1% vs 23.4% for placebo). Mann K, et al Alcohol Clin Exp Res 2004;28:51-63
80 Acamprosate Pharmacodynamics Mechanism of action not completely understood. Chronic alcohol exposure is thought to alter normal balance between neuronal excitation and inhibition Acamprosate may interact with glutamate and GABA neurotransmitter systems
81 Pharmacodynamics (con t) No pharmacokinetic differences due to gender or degree of alcohol dependency. No dosage adjustment needed with mild to moderate hepatic impairment or mild renal disease. Dose adjustment is necessary in moderate renal disease (creatinine cl ml/min) Contraindicated in severe renal disease
82 DRUG INTERACTIONS No inducing potential on cytochrome CYP 1A2 and 3A4 systems. Does not inhibit metabolism mediated by CYP1A2, 2C9, 2D6, 2E1 or 3A4 No pharmacokinetic interaction with alcohol, disulfiram, or diazepam (can be taken with sedatives or non-opioid analgesics No dose adjustment needed with naltrexone
83 Acamprosate Data from pivotal trials reanalyzed again with more stringent definition of abstinence. Rates of complete abstinence significantly higher than placebo. Percent days abstinent and time to first drink also significantly greater in acamprosate group Kranzler HR, Am J Addict Jan-Feb;17(1): 70-76
84 Johnson BA, et al. JAMA 2007; 298: Topiramate (not FDA approved for alcohol dependency treatment) Antagonizes glutamate receptors, modulates cortico-mesolimbic dopamine release and enhances GABA. Usually dose is up to 300mg titrated slowly up from 25mg/day over 6-8 weeks. Study demonstrated significantly less heavy drinking days and lower GGT.* Adverse effects with paresthesia, taste perversion and anorexia are problematic Shows potential more studies needed.
85 Other non-fda approved options Baclofen GABA B agonist Ondansetron - 5-HT antagonist- may be more effective in patients with long allele on 5-HTT, chrom-17* Tricyclic antidepressants SSRIs Nalmefene Vitamin/herbal infusions Johnson BA, Am J Psychiatry 167 : , June 2010
86 Non-Pharmacologic Treatment 12 Step meetings- AA/ Celebrate Recovery Insight oriented process groups Cognitive Behavioral Therapy Motivational Enhancement Coping Skill Enhancement No group has a significantly better outcome than the others- given the same length of treatment.
87 Alcoholics Anonymous Over 2,000,000 members world wide. Ubiquitous- >97,000 groups world wide. friends of Bill W. 39% of members were referred by health care professional.
88 Celebrate Recovery 12 Step group- claiming Jesus Christ as the higher power. 15,000 groups in 48 states, 48 state prison systems, and 28 countries. Umbrella program for all chemical dependencies,co-dependency,compulsive behaviors,abuse,pre-covery (6-12) & teens
89 Questions & Discussion
Alcohol Abuse a really quick review
 Alcohol Abuse a really quick review Anthony Albanese, M.D. Associate Clinical Professor of Medicine & Psychiatry, UC Davis Medical School Director, Chemical Dependency & Hepatology Programs Sacramento
Alcohol Abuse a really quick review Anthony Albanese, M.D. Associate Clinical Professor of Medicine & Psychiatry, UC Davis Medical School Director, Chemical Dependency & Hepatology Programs Sacramento
ALCOHOL USE DISORDER WITHDRAWAL MANAGEMENT AND LONG TERM TREATMENT ANA HOLTEY, MD ADDICTION MEDICINE FELLOW UNIVERSITY OF UTAH HEALTH
 ALCOHOL USE DISORDER WITHDRAWAL MANAGEMENT AND LONG TERM TREATMENT ANA HOLTEY, MD ADDICTION MEDICINE FELLOW UNIVERSITY OF UTAH HEALTH Prevalence of 12-Month Alcohol Use, High-Risk Drinking, and DSM-IV
ALCOHOL USE DISORDER WITHDRAWAL MANAGEMENT AND LONG TERM TREATMENT ANA HOLTEY, MD ADDICTION MEDICINE FELLOW UNIVERSITY OF UTAH HEALTH Prevalence of 12-Month Alcohol Use, High-Risk Drinking, and DSM-IV
Chapter 7. Screening and Assessment
 Chapter 7 Screening and Assessment Screening And Assessment Starting the dialogue and begin relationship Each are sizing each other up Information gathering Listening to their story Asking the questions
Chapter 7 Screening and Assessment Screening And Assessment Starting the dialogue and begin relationship Each are sizing each other up Information gathering Listening to their story Asking the questions
Metabolism and Pharmacology of Ethanol Part I. Prof. David W. Craig Dept. of Chemistry Hobart and William Smith Colleges
 Metabolism and Pharmacology of Ethanol Part I Prof. David W. Craig Dept. of Chemistry Hobart and William Smith Colleges Behavioral Manifestations of Alcohol Ingestion With 1 to 2 drinks (.01-.05 g/dl BAC)
Metabolism and Pharmacology of Ethanol Part I Prof. David W. Craig Dept. of Chemistry Hobart and William Smith Colleges Behavioral Manifestations of Alcohol Ingestion With 1 to 2 drinks (.01-.05 g/dl BAC)
Sedative Hypnotics. Isopropyl Alcohol H H H H OH H. H H Ethyl Alcohol (Ethanol)
") Sedative Hypnotics Alcohol - The most commonly used Sedative- Hypnotic. Probably the oldest psychoactive drug used by humans. Alcohol use is common our society. 2/3 of people drink. 10% are problem drinkers
Sedative Hypnotics Alcohol - The most commonly used Sedative- Hypnotic. Probably the oldest psychoactive drug used by humans. Alcohol use is common our society. 2/3 of people drink. 10% are problem drinkers
Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents
 Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents Myth or Reality? Complete Recovery means a medication-free state True or False? Treatment of Alcoholism Assessment Motivation Alcohol
Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents Myth or Reality? Complete Recovery means a medication-free state True or False? Treatment of Alcoholism Assessment Motivation Alcohol
THE SCIENCE OF FEELING GOOD & FEELING BAD WITH ALCOHOL
 THE SCIENCE OF FEELING GOOD & FEELING BAD WITH ALCOHOL Professor David W. Craig Department of Chemistry Hobart and William Smith Colleges 7:30 8:30 pm Tuesday, October 17, 2006 Geneva Room Alcohol Awareness
THE SCIENCE OF FEELING GOOD & FEELING BAD WITH ALCOHOL Professor David W. Craig Department of Chemistry Hobart and William Smith Colleges 7:30 8:30 pm Tuesday, October 17, 2006 Geneva Room Alcohol Awareness
Pharmacotherapy of Alcohol Use Disorders
 Pharmacotherapy of Alcohol Use Disorders Roger D. Weiss, MD Professor of Psychiatry, Harvard Medical School Chief, Division of Alcohol and Drug Abuse McLean Hospital rweiss@mclean.harvard.edu Consultant
Pharmacotherapy of Alcohol Use Disorders Roger D. Weiss, MD Professor of Psychiatry, Harvard Medical School Chief, Division of Alcohol and Drug Abuse McLean Hospital rweiss@mclean.harvard.edu Consultant
1/10/2017. A common Alcoholics Anonymous (AA) saying is There is no problem that alcohol cannot make worse.
 saying is There is no problem that alcohol cannot make worse.") Alcohol still addicts more people than all other drugs combined Understand difference between alcohol use, abuse and dependence Learn the potential physiological and emotional affects of alcohol Distinguish
Alcohol still addicts more people than all other drugs combined Understand difference between alcohol use, abuse and dependence Learn the potential physiological and emotional affects of alcohol Distinguish
Complicated Withdrawal
 Complicated Withdrawal Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim Nejad,
Complicated Withdrawal Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim Nejad,
Withdrawal.
 Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts General
Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts General
An Internist s Guide to Unhealthy Alcohol Use. Ryan Graddy, MD JHU SOM
 An Internist s Guide to Unhealthy Alcohol Use Ryan Graddy, MD JHU SOM Disclosures None Learning Objectives Understand the terminology used to describe unhealthy alcohol use Identify means of screening
An Internist s Guide to Unhealthy Alcohol Use Ryan Graddy, MD JHU SOM Disclosures None Learning Objectives Understand the terminology used to describe unhealthy alcohol use Identify means of screening
Complicated Withdrawal
 Complicated Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts
Complicated Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts
Prepared by: Dr. Elizabeth Woodward, University of Toronto Resident in Psychiatry
 Prepared by: Dr. Elizabeth Woodward, University of Toronto Resident in Psychiatry In broad terms, substance use disorders occur when a substance is used in a compulsive manner with a lack of control over
Prepared by: Dr. Elizabeth Woodward, University of Toronto Resident in Psychiatry In broad terms, substance use disorders occur when a substance is used in a compulsive manner with a lack of control over
ANTICONVULSANTS IN ALCOHOL WITHDRAWAL TREATMENT: A BETTER WAY?
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences ANTICONVULSANTS IN ALCOHOL WITHDRAWAL TREATMENT: A BETTER WAY? RICHARD RIES MD PROFESSOR OF PSYCHIATRY AND DIRECTOR
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences ANTICONVULSANTS IN ALCOHOL WITHDRAWAL TREATMENT: A BETTER WAY? RICHARD RIES MD PROFESSOR OF PSYCHIATRY AND DIRECTOR
Patterns of Alcohol Use
 Alcohol and Tobacco Learning Objectives 1) Describe the patterns of alcohol use, and the health risks and social problems that can result from alcohol use, abuse, and dependence 2) Explain treatment approaches
Alcohol and Tobacco Learning Objectives 1) Describe the patterns of alcohol use, and the health risks and social problems that can result from alcohol use, abuse, and dependence 2) Explain treatment approaches
Main Questions. Why study addiction? Substance Use Disorders, Part 1 Alecia Schweinsburg, MA Abnromal Psychology, Fall Substance Use Disorders
 Substance Use Disorders Main Questions Why study addiction? What is addiction? Why do people become addicted? What do alcohol and drugs do? How do we treat substance use disorders? Why study addiction?
Substance Use Disorders Main Questions Why study addiction? What is addiction? Why do people become addicted? What do alcohol and drugs do? How do we treat substance use disorders? Why study addiction?
Complicated Withdrawal
 Complicated Withdrawal Shamim Nejad, MD Medical Director, Division of Psychosocial Oncology Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim
Complicated Withdrawal Shamim Nejad, MD Medical Director, Division of Psychosocial Oncology Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim
Chapter 7. Screening and Assessment
 Chapter 7 Screening and Assessment Screening And Assessment Starting the dialogue and begin relationship Each are sizing each other up Information gathering Listening to their story Asking the questions
Chapter 7 Screening and Assessment Screening And Assessment Starting the dialogue and begin relationship Each are sizing each other up Information gathering Listening to their story Asking the questions
Basics of Benzodiazepine Use Disorder. DATE: June 12, 2018 PRESENTED BY: Melissa B. Weimer, DO, MCR
 Basics of Benzodiazepine Use Disorder DATE: June 12, 2018 PRESENTED BY: Melissa B. Weimer, DO, MCR Disclosures Speaker: Melissa Weimer, DO, MCR, has nothing to disclose. Planning Committee: The members
Basics of Benzodiazepine Use Disorder DATE: June 12, 2018 PRESENTED BY: Melissa B. Weimer, DO, MCR Disclosures Speaker: Melissa Weimer, DO, MCR, has nothing to disclose. Planning Committee: The members
Screening, Diagnosis, and Medication Assisted Treatment for Alcohol Use Disorders
 Psychiatry and Addictions Case Conference Screening, Diagnosis, and Medication Assisted Treatment for Alcohol Use Disorders MARK DUNCAN, MD Acting Assistant Professor, Co-lead University of Washington
Psychiatry and Addictions Case Conference Screening, Diagnosis, and Medication Assisted Treatment for Alcohol Use Disorders MARK DUNCAN, MD Acting Assistant Professor, Co-lead University of Washington
Underwriting the Habits Risk of Alcohol Use Gregory Ferrara New York Life Underwriting January, 2013
 Underwriting the Habits Risk of Alcohol Use Gregory Ferrara New York Life Underwriting January, 2013 The Company You Keep 1 Antitrust 2 New York Life adheres to the letter and spirit of the antitrust laws.
Underwriting the Habits Risk of Alcohol Use Gregory Ferrara New York Life Underwriting January, 2013 The Company You Keep 1 Antitrust 2 New York Life adheres to the letter and spirit of the antitrust laws.
UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES Discipline of Biochemistry and Molecular Biology
 UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES Discipline of Biochemistry and Molecular Biology 1 PBL SEMINAR ACUTE & CHRONIC ETHANOL EFFECTS An Overview Sites
UNIVERSITY OF PNG SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES Discipline of Biochemistry and Molecular Biology 1 PBL SEMINAR ACUTE & CHRONIC ETHANOL EFFECTS An Overview Sites
DRUGS THAT ACT IN THE CNS
 DRUGS THAT ACT IN THE CNS Anxiolytic and Hypnotic Drugs Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 OTHER ANXIOLYTIC AGENTS/ A. Antidepressants Many antidepressants are effective in the treatment
DRUGS THAT ACT IN THE CNS Anxiolytic and Hypnotic Drugs Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 OTHER ANXIOLYTIC AGENTS/ A. Antidepressants Many antidepressants are effective in the treatment
Basics of Benzodiazepine Use Disorder. DATE: March 20, 2018 PRESENTED BY: Melissa B. Weimer, DO, MCR
 Basics of Benzodiazepine Use Disorder DATE: March 20, 2018 PRESENTED BY: Melissa B. Weimer, DO, MCR Disclosures Speaker: Melissa Weimer, DO, MCR, has nothing to disclose. Planning Committee: The members
Basics of Benzodiazepine Use Disorder DATE: March 20, 2018 PRESENTED BY: Melissa B. Weimer, DO, MCR Disclosures Speaker: Melissa Weimer, DO, MCR, has nothing to disclose. Planning Committee: The members
Medications For Alcohol Use Disorder. DATE: October 10, 2017 PRESENTED BY: Alann Weissman-Ward, MD, Addiction Medicine fellow
 Medications For Alcohol Use Disorder DATE: October 10, 2017 PRESENTED BY: Alann Weissman-Ward, MD, Addiction Medicine fellow None DISCLOSURES OBJECTIVES Be able to name 4 medications to treat AUD Describe
Medications For Alcohol Use Disorder DATE: October 10, 2017 PRESENTED BY: Alann Weissman-Ward, MD, Addiction Medicine fellow None DISCLOSURES OBJECTIVES Be able to name 4 medications to treat AUD Describe
Anxiolytic, Sedative and Hypnotic Drugs. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Anxiolytic, Sedative and Hypnotic Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Anxiolytics: reduce anxiety Sedatives: decrease activity, calming
Anxiolytic, Sedative and Hypnotic Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Anxiolytics: reduce anxiety Sedatives: decrease activity, calming
Decreasing Alcohol Use with Medications: What Works?
 Decreasing Alcohol Use with Medications: What Works? Annual Review of Family Medicine December 7 th, 2017, UCSF Mission Bay Ben Smith, MD MPH Assistant Professor of Family and Community Medicine San Francisco
Decreasing Alcohol Use with Medications: What Works? Annual Review of Family Medicine December 7 th, 2017, UCSF Mission Bay Ben Smith, MD MPH Assistant Professor of Family and Community Medicine San Francisco
Tranquilizers & Sedative-Hypnotics
 Tranquilizers & Sedative-Hypnotics 1 Tranquilizer or anxiolytic: Drugs used therapeutically to treat agitation or anxiety Sedative-Hypnotic: drugs used to sedate and aid in sleep Original sedatives (before
Tranquilizers & Sedative-Hypnotics 1 Tranquilizer or anxiolytic: Drugs used therapeutically to treat agitation or anxiety Sedative-Hypnotic: drugs used to sedate and aid in sleep Original sedatives (before
Dr. Oslin receives grant support from the NIH, VA, and the Pennsylvania Department of Aging.
 David W. Oslin, MD University of Pennsylvania Philadelphia VAMC Dr. Oslin receives grant support from the NIH, VA, and the Pennsylvania Department of Aging. Dr. Oslin is a consultant to the Hazelden Betty
David W. Oslin, MD University of Pennsylvania Philadelphia VAMC Dr. Oslin receives grant support from the NIH, VA, and the Pennsylvania Department of Aging. Dr. Oslin is a consultant to the Hazelden Betty
The Council for Disability Awareness
 Alcohol and Your Health It's a fact: alcohol is a prevalent part of our social lives. We unwind by drinking a beer or two at the game or having a glass of wine with dinner. We toast holidays and special
Alcohol and Your Health It's a fact: alcohol is a prevalent part of our social lives. We unwind by drinking a beer or two at the game or having a glass of wine with dinner. We toast holidays and special
Unit II Problem 7 Pharmacology: Substance Abuse, Dependence and Addiction
 Unit II Problem 7 Pharmacology: Substance Abuse, Dependence and Addiction Drugs are classified as being Used (medically approved) abused (medically NOT approved) - What is the difference between dependence
Unit II Problem 7 Pharmacology: Substance Abuse, Dependence and Addiction Drugs are classified as being Used (medically approved) abused (medically NOT approved) - What is the difference between dependence
BAPTIST HEALTH SCHOOL OF NURSING NSG 3036A: PSYCHIATRIC-MENTAL HEALTH
 BAPTIST HEALTH SCHOOL OF NURSING NSG 3036A: PSYCHIATRIC-MENTAL HEALTH THERAPEUTIC INTERVENTION AND RESOURCE MANAGEMENT: SUBSTANCE RELATED DISORDERS: CO-DEPENDENCY AND THE IMPAIRED NURSE LECTURE OBJECTIVES:
BAPTIST HEALTH SCHOOL OF NURSING NSG 3036A: PSYCHIATRIC-MENTAL HEALTH THERAPEUTIC INTERVENTION AND RESOURCE MANAGEMENT: SUBSTANCE RELATED DISORDERS: CO-DEPENDENCY AND THE IMPAIRED NURSE LECTURE OBJECTIVES:
Guidelines for the In-Patient Management of Alcohol Withdrawal at Frimley Park Hospital NHS Foundation Trust
 Guidelines for the In-Patient Management of Alcohol Withdrawal at Frimley Park Hospital NHS Foundation Trust Authors: Dr Aftab Ala, Consultant Gastroenterologist & Hepatologist Dr Tasneem Pirani, ST4 in
Guidelines for the In-Patient Management of Alcohol Withdrawal at Frimley Park Hospital NHS Foundation Trust Authors: Dr Aftab Ala, Consultant Gastroenterologist & Hepatologist Dr Tasneem Pirani, ST4 in
Session 2: Alcohol and Recovery 2-1
 Session 2: Alcohol and Recovery 2-1 Alcohol in the Brain Alcohol upsets a delicate balance between chemical systems that stimulate and chemical systems that inhibit functions of the brain and body. Matrix
Session 2: Alcohol and Recovery 2-1 Alcohol in the Brain Alcohol upsets a delicate balance between chemical systems that stimulate and chemical systems that inhibit functions of the brain and body. Matrix
ALCOHOL Other name(s): ethyl alcohol, ethanol, grain alcohol, hootch, liquor, booze, firewater, EtOH Class: alcohols are molecules with a hydroxyl
: ethyl alcohol, ethanol, grain alcohol, hootch, liquor, booze, firewater, EtOH Class: alcohols are molecules with a hydroxyl") Other name(s): ethyl alcohol, ethanol, grain alcohol, hootch, liquor, booze, firewater, EtOH Class: alcohols are molecules with a hydroxyl (OH) bound to carbon atoms. In EtOH, the carbon is in an ethyl
Other name(s): ethyl alcohol, ethanol, grain alcohol, hootch, liquor, booze, firewater, EtOH Class: alcohols are molecules with a hydroxyl (OH) bound to carbon atoms. In EtOH, the carbon is in an ethyl
Basics of Benzodiazepine Use Disorder. DATE: October 3, 2017 PRESENTED BY: Melissa B. Weimer, DO, MCR
 Basics of Benzodiazepine Use Disorder DATE: October 3, 2017 PRESENTED BY: Melissa B. Weimer, DO, MCR Disclosures Speaker disclosure: One time lecture sponsored by Indivior about overlap of pain and opioid
Basics of Benzodiazepine Use Disorder DATE: October 3, 2017 PRESENTED BY: Melissa B. Weimer, DO, MCR Disclosures Speaker disclosure: One time lecture sponsored by Indivior about overlap of pain and opioid
ACUTE & CHRONIC ETHANOL EFFECTS An Overview
 ACUTE & CHRONIC ETHANOL EFFECTS An Overview University of Papua New Guinea School of Medicine & Health Sciences, Division of Basic Medical Sciences Clinical Biochemistry: PBL Seminar MBBS Yr 4 VJ Temple
ACUTE & CHRONIC ETHANOL EFFECTS An Overview University of Papua New Guinea School of Medicine & Health Sciences, Division of Basic Medical Sciences Clinical Biochemistry: PBL Seminar MBBS Yr 4 VJ Temple
Treatment of Alcohol and Opiate Withdrawal
 Objectives Treatment of Alcohol and Opiate Withdrawal Renee Striker, Pharm.D., BCPS, BCPP Pharmacy Clinical Specialist Huron Hospital East Cleveland, Ohio Outline the diagnostic criteria for substance
Objectives Treatment of Alcohol and Opiate Withdrawal Renee Striker, Pharm.D., BCPS, BCPP Pharmacy Clinical Specialist Huron Hospital East Cleveland, Ohio Outline the diagnostic criteria for substance
Alcohol withdrawal. Clinical features
 Alcohol withdrawal Clinical features Severity increase with amount consumed; uncommon with < drinks per day. Predictable pattern: patients with previous withdrawal seizures are at high risk for recurrence.
Alcohol withdrawal Clinical features Severity increase with amount consumed; uncommon with < drinks per day. Predictable pattern: patients with previous withdrawal seizures are at high risk for recurrence.
ROLE OF HEALTH CARE PROVIDERS IN THE MANAGEMENT OF ALCOHOL AND DRUG USE RELATED PROBLEMS
 ROLE OF HEALTH CARE PROVIDERS IN THE MANAGEMENT OF ALCOHOL AND DRUG USE RELATED PROBLEMS Dr. Anita Rao? ASK SCREEN Refer HELP T T Ranganathan Clinical Research Foundation TTK Hospital IV Main Road, Indira
ROLE OF HEALTH CARE PROVIDERS IN THE MANAGEMENT OF ALCOHOL AND DRUG USE RELATED PROBLEMS Dr. Anita Rao? ASK SCREEN Refer HELP T T Ranganathan Clinical Research Foundation TTK Hospital IV Main Road, Indira
Treatment Alternatives for Substance Use Disorders
 Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Dr. Renner receives honoraria from Reed Medical Education
 Substance Use Disorders Symposium on Men s Health Massachusetts Medical Society June 17, 2010 John A. Renner, Jr., M.D. John A. Renner Jr., MD DISCLOSURES Johnson & Johnson Stock Holder Dr. Renner receives
Substance Use Disorders Symposium on Men s Health Massachusetts Medical Society June 17, 2010 John A. Renner, Jr., M.D. John A. Renner Jr., MD DISCLOSURES Johnson & Johnson Stock Holder Dr. Renner receives
Pharmacotherapy for Alcohol Use Disorder
 Pharmacotherapy for Alcohol Use Disorder Laura G. Kehoe, MD, MPH Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither my
Pharmacotherapy for Alcohol Use Disorder Laura G. Kehoe, MD, MPH Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither my
Medications For Alcohol Use Disorder
 Medications For Alcohol Use Disorder PRESENTED BY: Alann Weissman-Ward, MD, Addiction Medicine fellow June 19, 2018 DISCLOSURES Speaker: Alann Weissman-Ward, MD, has nothing to disclose. Planning Committee:
Medications For Alcohol Use Disorder PRESENTED BY: Alann Weissman-Ward, MD, Addiction Medicine fellow June 19, 2018 DISCLOSURES Speaker: Alann Weissman-Ward, MD, has nothing to disclose. Planning Committee:
Management of high risk MMT patients. Meldon Kahan MD Methadone Prescribers Conference Toronto, Nov 15, 2013
 Management of high risk MMT patients Meldon Kahan MD Methadone Prescribers Conference Toronto, Nov 15, 2013 CFPC CoI Templates: Slide 1 Faculty Disclosure Faculty: Meldon Kahan Relationships with commercial
Management of high risk MMT patients Meldon Kahan MD Methadone Prescribers Conference Toronto, Nov 15, 2013 CFPC CoI Templates: Slide 1 Faculty Disclosure Faculty: Meldon Kahan Relationships with commercial
ADDICTIONS. Mine Özmen, M.D. University of İstanbul Cerrahpaşa School of Medicine Department of Psychiatry
 ADDICTIONS Mine Özmen, M.D. University of İstanbul Cerrahpaşa School of Medicine Department of Psychiatry Addictions-terminology drug abuse drug dependence drug addiction intoxication withdrawal tolerance
ADDICTIONS Mine Özmen, M.D. University of İstanbul Cerrahpaşa School of Medicine Department of Psychiatry Addictions-terminology drug abuse drug dependence drug addiction intoxication withdrawal tolerance
Management of Alcohol Dependence
 STANDARD TREATMENT GUIDELINES Management of Alcohol Dependence Quick Reference Guide February 2016 Ministry of Health & Family Welfare Government of India 1 Table of Contents Objectives-... 3 Diagnosis...
STANDARD TREATMENT GUIDELINES Management of Alcohol Dependence Quick Reference Guide February 2016 Ministry of Health & Family Welfare Government of India 1 Table of Contents Objectives-... 3 Diagnosis...
Overview of Psychoactive Drug use
 Overview of Psychoactive Drug use By Dr. Oladosu Ahmed Kayode Specialist in mental health Attending physician Dept. of psychiatry, GH Ilorin & Hopeville Psychiatric Hospital, Ilorin. Learning objectives
Overview of Psychoactive Drug use By Dr. Oladosu Ahmed Kayode Specialist in mental health Attending physician Dept. of psychiatry, GH Ilorin & Hopeville Psychiatric Hospital, Ilorin. Learning objectives
ANTICONVULSANTS IN ALCOHOL WITHDRAWAL TREATMENT: A BETTER WAY?
 Psychiatry and Addictions Case Conference Medicine Psychiatry and Behavioral Sciences ANTICONVULSANTS IN ALCOHOL WITHDRAWAL TREATMENT: A BETTER WAY? RICHARD RIES MD PROFESSOR OF PSYCHIATRY AND DIRECTOR
Psychiatry and Addictions Case Conference Medicine Psychiatry and Behavioral Sciences ANTICONVULSANTS IN ALCOHOL WITHDRAWAL TREATMENT: A BETTER WAY? RICHARD RIES MD PROFESSOR OF PSYCHIATRY AND DIRECTOR
Management of substance use disorders in primary care. Meldon Kahan, MD
 Management of substance use disorders in primary care Meldon Kahan, MD i 2015 Women s College Hospital All rights reserved. Version date: November 27, 2015 ii Contents Introduction... vii Part I: Alcohol
Management of substance use disorders in primary care Meldon Kahan, MD i 2015 Women s College Hospital All rights reserved. Version date: November 27, 2015 ii Contents Introduction... vii Part I: Alcohol
Substance and Alcohol Related Disorders. Substance use Disorder Alcoholism Gambling Disorder
 Substance and Alcohol Related Disorders Substance use Disorder Alcoholism Gambling Disorder What is a Substance Use Disorder? According to the DSM-5, a substance use disorder describes a problematic pattern
Substance and Alcohol Related Disorders Substance use Disorder Alcoholism Gambling Disorder What is a Substance Use Disorder? According to the DSM-5, a substance use disorder describes a problematic pattern
Lecture 19. Alcohol Use. Lecture 19
 Lecture 19 Alcohol Use 1 Lecture 19 1. What is Alcohol? 2. History of Alcohol Consumption 3. Patterns of Alcohol Use 4. Short-Term Effects of Alcohol Use 5. Long-Term Effects of Alcohol Use 6. Alcohol
Lecture 19 Alcohol Use 1 Lecture 19 1. What is Alcohol? 2. History of Alcohol Consumption 3. Patterns of Alcohol Use 4. Short-Term Effects of Alcohol Use 5. Long-Term Effects of Alcohol Use 6. Alcohol
Alcohol abuse and dependence: diagnosis and treatment
 Alcohol abuse and dependence: diagnosis and treatment Psychiatry lecture for medical students Erika Szily Semmelweis University 2016 Burden of excessive alcohol use Risk factor for Social problems, Financial
Alcohol abuse and dependence: diagnosis and treatment Psychiatry lecture for medical students Erika Szily Semmelweis University 2016 Burden of excessive alcohol use Risk factor for Social problems, Financial
SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR ALCOHOL DEPENDENCE INDICATION
 SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR ALCOHOL DEPENDENCE INDICATION Naltrexone is used as part of a comprehensive programme of treatment against alcoholism to reduce the
SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR ALCOHOL DEPENDENCE INDICATION Naltrexone is used as part of a comprehensive programme of treatment against alcoholism to reduce the
Substitution Therapy for Opioid Use Disorder The Role of Suboxone
 Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Pharmacotherapy for Substance Use Disorders
 Pharmacotherapy for Substance Use Disorders Vanessa de la Cruz, MD Chief of Psychiatry Mental Health and Substance Abuse Services Santa Cruz County Health Services Agency 1400 Emeline Avenue Santa Cruz,
Pharmacotherapy for Substance Use Disorders Vanessa de la Cruz, MD Chief of Psychiatry Mental Health and Substance Abuse Services Santa Cruz County Health Services Agency 1400 Emeline Avenue Santa Cruz,
9/22/2015. Timothy W. Lineberry, MD Chief Medical Officer Greater Green Bay Aurora Health Care
 Timothy W. Lineberry, MD Chief Medical Officer Greater Green Bay Aurora Health Care Differentiate between hazardous drinking and alcohol use disorders Recognize issues associated with comorbidity between
Timothy W. Lineberry, MD Chief Medical Officer Greater Green Bay Aurora Health Care Differentiate between hazardous drinking and alcohol use disorders Recognize issues associated with comorbidity between
General Effects. Special Patient Populations. Alcoholism. Who is an Alcoholic
 Alcohol Use & Abuse in Acutely and Critically Ill Patients: Don t Be Fooled General Effects Christine Schulman, RN, MS, CNS, CCRN Clinical Nurse Specialist & Consultant Trauma & Critical Care Nursing Portland,
Alcohol Use & Abuse in Acutely and Critically Ill Patients: Don t Be Fooled General Effects Christine Schulman, RN, MS, CNS, CCRN Clinical Nurse Specialist & Consultant Trauma & Critical Care Nursing Portland,
Genetic Contributors to Alcohol Use and Misuse in Young People
 Genetic Contributors to Alcohol Use and Misuse in Young People Marianne BM van den Bree Professor of Psychological Medicine Institute of Psychological Medicine and Clinical Neurosciences MRC Centre for
Genetic Contributors to Alcohol Use and Misuse in Young People Marianne BM van den Bree Professor of Psychological Medicine Institute of Psychological Medicine and Clinical Neurosciences MRC Centre for
Substance Misuse Nurse service Belfast Trust
 Substance Misuse Nurse service Belfast Trust Alcohol is the most widely available socially acceptable drug in Northern Ireland It can be an addictive substance It is a depressant- slows down the central
Substance Misuse Nurse service Belfast Trust Alcohol is the most widely available socially acceptable drug in Northern Ireland It can be an addictive substance It is a depressant- slows down the central
A. Incorrect! Seizures are not typically linked to alcohol use. B. Incorrect! Epilepsy is a seizure that is commonly associated with convulsions.
 Pharmacology - Problem Drill 17: Central Nervous System Depressants Question No. 1 of 10 Instructions: (1) Read the problem statement and answer choices carefully (2) Work the problems on paper as 1. occur(s)
Pharmacology - Problem Drill 17: Central Nervous System Depressants Question No. 1 of 10 Instructions: (1) Read the problem statement and answer choices carefully (2) Work the problems on paper as 1. occur(s)
Medication for the Treatment of Alcohol Use Disorder. Pocket Guide
 Medication for the Treatment of Alcohol Use Disorder Pocket Guide Medications are underused in the treatment of alcohol use disorder. According to the National Survey on Drug Use and Health, of the estimated
Medication for the Treatment of Alcohol Use Disorder Pocket Guide Medications are underused in the treatment of alcohol use disorder. According to the National Survey on Drug Use and Health, of the estimated
Alcohol Support Services
 Alcohol Alcohol Support Services Washington Recovery Line: 1-866-789-1511 Teen Link: 866-TEENLINK (866-833-6546) Crisis Clinic: 206-461-3222/1-866-427-4747 Alcoholics Anonymous: 206-587-2838 Alanon & Alateen:
Alcohol Alcohol Support Services Washington Recovery Line: 1-866-789-1511 Teen Link: 866-TEENLINK (866-833-6546) Crisis Clinic: 206-461-3222/1-866-427-4747 Alcoholics Anonymous: 206-587-2838 Alanon & Alateen:
Update on Pharmacologic Treatments for Alcoholism
 Update on Pharmacologic Treatments for Alcoholism Michel A. Sucher, MD Presentation to California Society of Toxicologists Phoenix, AZ June 8, 2007 Disclosure Michel A. Sucher,, MD is on the Speakers Bureaus
Update on Pharmacologic Treatments for Alcoholism Michel A. Sucher, MD Presentation to California Society of Toxicologists Phoenix, AZ June 8, 2007 Disclosure Michel A. Sucher,, MD is on the Speakers Bureaus
THE MEDICAL MODEL: ADDICTION IS A BRAIN DISEASE. Judith Martin, MD Medical Director of Substance Use Services San Francisco Dept.
 THE MEDICAL MODEL: ADDICTION IS A BRAIN DISEASE Judith Martin, MD Medical Director of Substance Use Services San Francisco Dept. Public Health disclosures Dr. Martin has no conflict of interest to disclose.
THE MEDICAL MODEL: ADDICTION IS A BRAIN DISEASE Judith Martin, MD Medical Director of Substance Use Services San Francisco Dept. Public Health disclosures Dr. Martin has no conflict of interest to disclose.
The future of pharmacological treatment.
 The future of pharmacological treatment. Anne Lingford-Hughes Professor of Addiction Biology, Imperial College. Hon Consultant CNWL NHS Foundation Trust. What substances and when? What Nicotine Alcohol
The future of pharmacological treatment. Anne Lingford-Hughes Professor of Addiction Biology, Imperial College. Hon Consultant CNWL NHS Foundation Trust. What substances and when? What Nicotine Alcohol
Multiple Choice Questions
 Multiple Choice Questions 25yo M presents without psychiatric or medical history, with complaint of tremor to the ER. He denies drinking alcohol but his friend at bedside takes you to the side and reports
Multiple Choice Questions 25yo M presents without psychiatric or medical history, with complaint of tremor to the ER. He denies drinking alcohol but his friend at bedside takes you to the side and reports
Managing the Member with Substance Use: (Alcohol) November 15, Presenter: Steve Edfors, LCPC
 November 15, Presenter: Steve Edfors, LCPC") Managing the Member with Substance Use: (Alcohol) November 15, 2018 Presenter: Steve Edfors, LCPC University of Illinois at Chicago College of Nursing 1 Learning Objectives Upon completion of this learning
Managing the Member with Substance Use: (Alcohol) November 15, 2018 Presenter: Steve Edfors, LCPC University of Illinois at Chicago College of Nursing 1 Learning Objectives Upon completion of this learning
Using Benzodiazepines in Primary Care
 Using Benzodiazepines in Primary Care Spencer A. Tighe MD, FRCPC Saturday, Feb. 16, 2008 Overview Historical context Drug information Indications Side effects Abuse vs. physical dependence Clinical practice
Using Benzodiazepines in Primary Care Spencer A. Tighe MD, FRCPC Saturday, Feb. 16, 2008 Overview Historical context Drug information Indications Side effects Abuse vs. physical dependence Clinical practice
Drugs in American Society CHD 601. Legal Drugs Alcohol
 Drugs in American Society CHD 601 Legal Drugs Alcohol Unit 2 Last updated April 12, 2017 Edward Pierce, LCSW Overview From the last class Counseling videos Quiz 1 Process Other items Alcohol Biochemical
Drugs in American Society CHD 601 Legal Drugs Alcohol Unit 2 Last updated April 12, 2017 Edward Pierce, LCSW Overview From the last class Counseling videos Quiz 1 Process Other items Alcohol Biochemical
Pharmacotherapy for Alcohol Use Disorder
 Pharmacotherapy for Alcohol Use Disorder Laura G. Kehoe, MD, MPH Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither my
Pharmacotherapy for Alcohol Use Disorder Laura G. Kehoe, MD, MPH Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither my
Please review the following slides prior to class. Information from these slides will be used to answer patient cases. Come prepared!
 Please review the following slides prior to class Information from these slides will be used to answer patient cases. Come prepared! Alcohol and Opiate Dependence Reference Slides Substances of Abuse A
Please review the following slides prior to class Information from these slides will be used to answer patient cases. Come prepared! Alcohol and Opiate Dependence Reference Slides Substances of Abuse A
Alcoholism Psychiatric Perspective
 Alcoholism Psychiatric Perspective Dr. Vishwak Reddy 2 nd year PG Dept. of Psychiatry OUTLINE Introduction Types of alcohol beverages and their equivalence Physiology of effects of alcohol on CNS Etiology
Alcoholism Psychiatric Perspective Dr. Vishwak Reddy 2 nd year PG Dept. of Psychiatry OUTLINE Introduction Types of alcohol beverages and their equivalence Physiology of effects of alcohol on CNS Etiology
Varenicline and Other Pharmacotherapies for Tobacco Dependence
 Varenicline and Other Pharmacotherapies for Tobacco Dependence J. Taylor Hays, M.D. Associate Director Nicotine Dependence Center Mayo Clinic 2012 MFMER slide-1 Learning Objectives Understand the mechanism
Varenicline and Other Pharmacotherapies for Tobacco Dependence J. Taylor Hays, M.D. Associate Director Nicotine Dependence Center Mayo Clinic 2012 MFMER slide-1 Learning Objectives Understand the mechanism
Management of Unhealthy Alcohol Use: From Research to Practice
 Management of Unhealthy Alcohol Use: From Research to Practice Richard Saitz MD, MPH, FACP, DFASAM Professor of Community Health Sciences & Medicine Boston University Schools of Medicine & Public Health
Management of Unhealthy Alcohol Use: From Research to Practice Richard Saitz MD, MPH, FACP, DFASAM Professor of Community Health Sciences & Medicine Boston University Schools of Medicine & Public Health
Shhh! Let s Talk About Moderation for Mild Alcohol Use Disorders. Cyndi Turner, LCSW, LSATP, MAC Craig James, LCSW, MAC
 Shhh! Let s Talk About Moderation for Mild Alcohol Use Disorders Cyndi Turner, LCSW, LSATP, MAC Craig James, LCSW, MAC Shhh! Let s Talk About Moderation for Mild to Moderate Alcohol Use Disorders Insight
Shhh! Let s Talk About Moderation for Mild Alcohol Use Disorders Cyndi Turner, LCSW, LSATP, MAC Craig James, LCSW, MAC Shhh! Let s Talk About Moderation for Mild to Moderate Alcohol Use Disorders Insight
Behavioral Health Service Request Form Detox and Substance Abuse Rehab
 Medicaid Call for Pre-Certification of Admissions: 1-855-620-1861 Kentucky Medicaid Fax: 1-877-338-3686 Standard Request Requests for prior authorization (with supporting clinical information and documentation)
Medicaid Call for Pre-Certification of Admissions: 1-855-620-1861 Kentucky Medicaid Fax: 1-877-338-3686 Standard Request Requests for prior authorization (with supporting clinical information and documentation)
Managing presenting alcohol users an Introduction to SPECTRUM (CRI) By Dr Gideon Felton MRCPsych Consultant Psychiatrist and Clinical Lead
 By Dr Gideon Felton MRCPsych Consultant Psychiatrist and Clinical Lead") Managing presenting alcohol users an Introduction to SPECTRUM (CRI) By Dr Gideon Felton MRCPsych Consultant Psychiatrist and Clinical Lead PLAN OF PRESENTATION Assessment of alcohol dependence Psychiatric
Managing presenting alcohol users an Introduction to SPECTRUM (CRI) By Dr Gideon Felton MRCPsych Consultant Psychiatrist and Clinical Lead PLAN OF PRESENTATION Assessment of alcohol dependence Psychiatric
Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They?
 Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They? Yngvild Olsen, MD, MPH Cecil County Board of Health Workgroup Meeting Elkton, MD October 8, 2013 Objectives
Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They? Yngvild Olsen, MD, MPH Cecil County Board of Health Workgroup Meeting Elkton, MD October 8, 2013 Objectives
Depression & Alcohol
 Depression & Alcohol Black Dog Institute Mission: To advance the understanding and management of the mood disorders through Research Clinical Services Community Support Education Community Support Clinical
Depression & Alcohol Black Dog Institute Mission: To advance the understanding and management of the mood disorders through Research Clinical Services Community Support Education Community Support Clinical
WHEN AND HOW TO USE BENZODIAZEPINES IN TREATING ANXIETY: AM I WITHHOLDING TREATMENT IF I DON'T USE BENZODIAZEPINES?
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences WHEN AND HOW TO USE BENZODIAZEPINES IN TREATING ANXIETY: AM I WITHHOLDING TREATMENT IF I DON'T USE BENZODIAZEPINES?
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences WHEN AND HOW TO USE BENZODIAZEPINES IN TREATING ANXIETY: AM I WITHHOLDING TREATMENT IF I DON'T USE BENZODIAZEPINES?
Buspirone Carbamazepine Diazepam Disulfiram Ethosuximide Flumazeil Gabapentin Lamotrigine
 CNS Depressants Buspirone Carbamazepine Diazepam Disulfiram Ethosuximide Flumazeil Gabapentin Lamotrigine Lorazepam Phenobarbital Phenytoin Topiramate Valproate Zolpidem Busprione Antianxiety 5-HT1A partial
CNS Depressants Buspirone Carbamazepine Diazepam Disulfiram Ethosuximide Flumazeil Gabapentin Lamotrigine Lorazepam Phenobarbital Phenytoin Topiramate Valproate Zolpidem Busprione Antianxiety 5-HT1A partial
Anxiety Pharmacology UNIVERSITY OF HAWAI I HILO PRE -NURSING PROGRAM
 Anxiety Pharmacology UNIVERSITY OF HAWAI I HILO PRE NURSING PROGRAM NURS 203 GENERAL PHARMACOLOGY DANITA NARCISO PHARM D Learning Objectives Understand the normal processing of fear vs fear processing
Anxiety Pharmacology UNIVERSITY OF HAWAI I HILO PRE NURSING PROGRAM NURS 203 GENERAL PHARMACOLOGY DANITA NARCISO PHARM D Learning Objectives Understand the normal processing of fear vs fear processing
William H. Swiggart, MS
 William H. Swiggart, MS Co-Director, Center for Professional Health Vanderbilt University Medical Center 2015 All rights reserved. I have no financial relationships to disclose. The purpose of this session
William H. Swiggart, MS Co-Director, Center for Professional Health Vanderbilt University Medical Center 2015 All rights reserved. I have no financial relationships to disclose. The purpose of this session
SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR OPIOID DEPENDENCE
 SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR OPIOID DEPENDENCE INDICATION Naltrexone is a pure opiate antagonist licensed as an adjunctive prophylactic therapy in the maintenance
SHARED CARE GUIDELINE FOR THE MANAGEMENT OF PATIENTS ON NALTREXONE FOR OPIOID DEPENDENCE INDICATION Naltrexone is a pure opiate antagonist licensed as an adjunctive prophylactic therapy in the maintenance
Thaddeus Ulzen MD FRCP(C)FAPA FCGP Professor & Chair, Department of Psychiatry and Behavioral Medicine, Associate Dean for Academic Affairs
FAPA FCGP Professor & Chair, Department of Psychiatry and Behavioral Medicine, Associate Dean for Academic Affairs") Thaddeus Ulzen MD FRCP(C)FAPA FCGP Professor & Chair, Department of Psychiatry and Behavioral Medicine, Associate Dean for Academic Affairs CCHS/University of Alabama School of Medicine Assessment History
Thaddeus Ulzen MD FRCP(C)FAPA FCGP Professor & Chair, Department of Psychiatry and Behavioral Medicine, Associate Dean for Academic Affairs CCHS/University of Alabama School of Medicine Assessment History
Substance Use Disorders. A Major Problem. Defining Addiction 2/24/2009. Lifetime rates of alcoholism estimated at 13.4 %
 Substance Use Disorders A Major Problem Lifetime rates of alcoholism estimated at 13.4 % Rates of drug abuse estimated at 6% Marijuana is most frequent Approximately 600,000 deaths each year from substance
Substance Use Disorders A Major Problem Lifetime rates of alcoholism estimated at 13.4 % Rates of drug abuse estimated at 6% Marijuana is most frequent Approximately 600,000 deaths each year from substance
Alcoholism has been demonstrated to have a genetic component, especially among men.
 Causes and Treatment of Substance-Related Disorders (Chapter 10) Familial and Genetic Influences Alcoholism has been demonstrated to have a genetic component, especially among men. Seems to be a common
Causes and Treatment of Substance-Related Disorders (Chapter 10) Familial and Genetic Influences Alcoholism has been demonstrated to have a genetic component, especially among men. Seems to be a common
Alcohol and Other Drug Screening & Assessment
 Alcohol and Other Drug Screening & Assessment Richard Saitz, MD, MPH, FACP, FASAM Professor of Medicine & Epidemiology Boston University Schools of Medicine & Public Health Boston Medical Center Do substance
Alcohol and Other Drug Screening & Assessment Richard Saitz, MD, MPH, FACP, FASAM Professor of Medicine & Epidemiology Boston University Schools of Medicine & Public Health Boston Medical Center Do substance
Substance Use Disorders: What Can We Do to Help Break the Cycle of Addiction
 Handout for the Neuroscience Education Institute (NEI) online activity: Substance Use Disorders: What Can We Do to Help Break the Cycle of Addiction Learning Objectives Identify patients who are dependent
Handout for the Neuroscience Education Institute (NEI) online activity: Substance Use Disorders: What Can We Do to Help Break the Cycle of Addiction Learning Objectives Identify patients who are dependent
Investigation of HAZARDOUS DRINKING. 2 November 2010 best tests
 Investigation of HAZARDOUS DRINKING 2 November 2010 best tests Key concepts: Approximately 20 25% of New Zealanders consume alcohol at a harmful or hazardous level In approximately three-quarters of patients
Investigation of HAZARDOUS DRINKING 2 November 2010 best tests Key concepts: Approximately 20 25% of New Zealanders consume alcohol at a harmful or hazardous level In approximately three-quarters of patients
What is Alcohol? Produced by a fermentation process Proof is the amount of alcohol in the substance (ex. 100 proof bottle of vodka is 50% alcohol)
") ALCOHOLISM What is Alcohol? Depressant Contains intoxicating substance called ethyl alcohol or ethanol Slows down the functions of the brain and other parts of the nervous system What is Alcohol? Produced
ALCOHOLISM What is Alcohol? Depressant Contains intoxicating substance called ethyl alcohol or ethanol Slows down the functions of the brain and other parts of the nervous system What is Alcohol? Produced
Types of epilepsy. 1)Generalized type: seizure activity involve the whole brain, it is divided into:
Generalized type: seizure activity involve the whole brain, it is divided into:") Types of epilepsy We have different types of epilepsy, so it is not one type of seizures that the patient can suffer from; we can find some patients with generalized or partial seizure. So, there are two
Types of epilepsy We have different types of epilepsy, so it is not one type of seizures that the patient can suffer from; we can find some patients with generalized or partial seizure. So, there are two
1 pint beer = 2 units 1 glass sherry = 1 unit 1 glass wine = 1 unit (one 750ml bottle = 7-10 units) 1 bottle of 30 units
 1 bottle of 30 units") Alcohol Abuse: Acute vs. : An overview Dr Carolyn Fedler Of all the drugs of abuse (DOA) category, alcohol is the most commonly abused. Alcohol abuse is a serious health issue with major socio-economic
Alcohol Abuse: Acute vs. : An overview Dr Carolyn Fedler Of all the drugs of abuse (DOA) category, alcohol is the most commonly abused. Alcohol abuse is a serious health issue with major socio-economic
*IN10 BIOPSYCHOSOCIAL ASSESSMENT*
 BIOPSYCHOSOCIAL ASSESSMENT 224-008B page 1 of 5 / 06-14 Please complete this questionnaire and give it to your counselor on your first visit. This information will help your clinician gain an understanding
BIOPSYCHOSOCIAL ASSESSMENT 224-008B page 1 of 5 / 06-14 Please complete this questionnaire and give it to your counselor on your first visit. This information will help your clinician gain an understanding
DRUGS USED IN THE TREATMENT OF ADDICTION JOSEPH A. TRONCALE, MD FASAM RETREAT PREMIERE ADDICTION TREATMENT CENTERS
 DRUGS USED IN THE TREATMENT OF ADDICTION JOSEPH A. TRONCALE, MD FASAM RETREAT PREMIERE ADDICTION TREATMENT CENTERS MAJOR CATEGORIES OF TREATMENTS Detoxification and Post-Acute Withdrawal Maintenance Co-Occurring
DRUGS USED IN THE TREATMENT OF ADDICTION JOSEPH A. TRONCALE, MD FASAM RETREAT PREMIERE ADDICTION TREATMENT CENTERS MAJOR CATEGORIES OF TREATMENTS Detoxification and Post-Acute Withdrawal Maintenance Co-Occurring
Lorazepam Tablets, USP
 Lorazepam Tablets, USP DESCRIPTION: Lorazepam, an antianxiety agent, has the chemical formula, 7-chloro-5-(o-chlorophenyl)-1,3-dihydro-3-hydroxy-2H -1,4-benzodiazepin-2-one: Cl H N N O Cl OH It is a white
Lorazepam Tablets, USP DESCRIPTION: Lorazepam, an antianxiety agent, has the chemical formula, 7-chloro-5-(o-chlorophenyl)-1,3-dihydro-3-hydroxy-2H -1,4-benzodiazepin-2-one: Cl H N N O Cl OH It is a white
Riunione Monotematica AISF 2017 Roma 5 Ottobre Management of Alcohol Use Disorders in Patients with Alcoholic Liver Disease
 Riunione Monotematica AISF 2017 Roma 5 Ottobre 2017 Management of Alcohol Use Disorders in Patients with Alcoholic Liver Disease Lorenzo Leggio, M.D., Ph.D., M.Sc. Lorenzo Leggio, M.D., Ph.D., M.Sc. Il
Riunione Monotematica AISF 2017 Roma 5 Ottobre 2017 Management of Alcohol Use Disorders in Patients with Alcoholic Liver Disease Lorenzo Leggio, M.D., Ph.D., M.Sc. Lorenzo Leggio, M.D., Ph.D., M.Sc. Il
ALCOHOL. Do Now Activity. Fact or Fiction. According to the CDC Alcohol is the most used and abused drug among US youth.
 ALCOHOL Do Now Activity Fact or Fiction According to the CDC Alcohol is the most used and abused drug among US youth. According to the 2009 Monitoring the Future Survey 37% of 8 th graders have tried alcohol,
ALCOHOL Do Now Activity Fact or Fiction According to the CDC Alcohol is the most used and abused drug among US youth. According to the 2009 Monitoring the Future Survey 37% of 8 th graders have tried alcohol,