Complicated Withdrawal
|
|
|
- Amanda Simpson
- 6 years ago
- Views:
Transcription

1 Complicated Withdrawal Shamim Nejad, MD Medical Director, Division of Psychosocial Oncology Swedish Cancer Institute Swedish Medical Center Seattle, Washington
2 Disclosures: Shamim Nejad, MD Neither I nor my spouse/partner has a relevant financial relationship with a commercial interest to disclose.
3 Complicated Withdrawal: Overview Epidemiology Complicated alcohol withdrawal syndrome (AWS) Signs and symptoms Pathophysiology Management strategies
4 Phenotypes of AWS 4 main clinical states: Autonomic hyperactivity Neuronal excitation Hallucinations (+/ paranoid state) Alcohol withdrawal delirium (delirium tremens) Stages Clinical Findings Onset (Usual * ) Early or Uncomplicated 1) Anxiety, fine tremor (anxiety), tachycardia (anxiety); headache; palpitations; anorexia; GI upset; general malaise 2) May have elements of catacholamine excess (slight coarse tremor, elevated BP, elevated HR, diaphoresis, slight fever) 6-36 hrs Uncomplicated AWS Complicated AWS Alcoholic hallucinosis Alcohol related seizures Alcohol withdrawal delirium Alcohol Withdrawal Seizure Alcoholic Hallucinosis Alcohol Withdrawal Delirium (delirium tremens) Generalized, tonic-clonic seizures, status epilepticus (rare) Visual, auditory, and/or tactile hallucinations Delirium, tachycardia, hypertension, agitation, fever, diaphoresis, coarse tremor 6-48 hrs hrs hrs
5 Neurotransmitters: GABA and Glutamate
6 GABA and Glutamate Intermittent Alcohol Use Baseline Activity GABA activity Glutamate activity
7 GABA and Glutamate Acute Alcohol Use Ethanol acting on GABA receptor Baseline Activity GABA activity Glutamate activity
8 GABA and Glutamate Chronic Alcohol Use New Baseline Activity Ethanol acting on GABA receptor Original Baseline Activity GABA activity Glutamate activity
9 GABA and Glutamate Abrupt Cessation of Alcohol Amount of GABA agonism needed to override glutamate activity Baseline Activity GABA activity Glutamate activity
10 Neurotransmitter Dysfunction in AWS Uncomplicated Withdrawal (++) GABA Activity Glutamate Activity Noradrenergic Activity + (+) (+) Dopamine Release Uncomplicated Alcohol Withdrawal Complicated Alcohol Withdrawal Clapp, P et al. How Adaptation of the Brain to Alcohol Leads to Dependence: A Pharmacological Perspective. Alcohol Research and Health Vol. 31, 2008; Pages
11 Neurotransmitter Dysfunction in AWS Alcohol Withdrawal Seizure (++) GABA Activity Glutamate Activity Noradrenergic Activity + (+) (+) Dopamine Release Uncomplicated Alcohol Withdrawal Complicated Alcohol Withdrawal Clapp, P et al. How Adaptation of the Brain to Alcohol Leads to Dependence: A Pharmacological Perspective. Alcohol Research and Health Vol. 31, 2008; Pages
12 Neurotransmitter Dysfunction in AWS Alcoholic Hallucinosis (++) GABA Activity Glutamate Activity Noradrenergic Activity + (+) (+) Dopamine Release Uncomplicated Alcohol Withdrawal Complicated Alcohol Withdrawal Clapp, P et al. How Adaptation of the Brain to Alcohol Leads to Dependence: A Pharmacological Perspective. Alcohol Research and Health Vol. 31, 2008; Pages
13 Neurotransmitter Dysfunction in AWS Alcohol Withdrawal Delirium (++) GABA Activity Glutamate Activity Noradrenergic Activity + (+) (+) Dopamine Release Uncomplicated Alcohol Withdrawal Complicated Alcohol Withdrawal Clapp, P et al. How Adaptation of the Brain to Alcohol Leads to Dependence: A Pharmacological Perspective. Alcohol Research and Health Vol. 31, 2008; Pages

14 Management of AWD Supportive Care Wernicke s Treatment/Prophylaxis Signs: thiamine 500mg IV TID Risk: thiamine 100mg IV/IM BID Pharmacologic management Benzodiazepines Antiepileptic drugs (AEDs) Ethanol Dexmedetomidine Propofol BZD Administration Strategies Prophylaxis Front loading Fixed dose Active Symptoms Symptom Triggered Fixed schedule + PRN Augmentation agents Beta Blockers Clonidine Haloperidol

 Fixed Dose BZD or Phenobarbital")
15 AWS Treatment Algorithm AWS Uncomplicated AWS Complicated AWS Normal Mental Status Delirious or high delirium risk/history of Complicated AWS CIWA (or other STP) Fixed Dose BZD or Phenobarbital Protocol
16 Rating Scales in AWS CIWA Ar (Clinical Institute Withdrawal Assessment for Alcohol Revised) AWS (Alcohol Withdrawal Symptoms rating scale) SAWS (Short Alcohol Withdrawal Scale) SAS (Severity Assessment Scale)
17 Symptom Triggered Protocols: CIWA CIWA Ar Used to guide AWS management strategies Relatively easy to use Reliable and validated assessment tool for non medically/surgically ill Scores correlate with severity of AWS for non medically/surgically ill NOT diagnostic it is an ASSESSMENT TOOL Inter rater reliability only fair to poor CIWA Ar Nausea and Vomiting Tremor Paroxysmal Sweats Anxiety Agitation Tactile Disturbances Auditory Hallucinations Visual Disturbances Headache, fullness in head Orientation, clouding of sensorium

18 CIWA Driven BZD Based 18
19 CIWA Ar: Things To Consider Patient Location Mental status Level of medical comorbidity Current severity of alcohol withdrawal History of repeated complicated alcohol withdrawal When used, remember that Epic or any protocol order set(s) are only a starting point, and you may need to adjust dose and route to be relevant to your patient Alternative protocol should be available if there are contraindications to CIWA Ar use

20 Complicated AWS: Fixed Dose
 Fixed Dose or Phenobarbital Protocol Fixed Dose or Phenobarbital Protocol Phenobarbital Protocol Dexmedetomidine BZD Symptom Triggered Protocol")
21 AWS Treatment Algorithm AWS Uncomplicated AWS Complicated AWS Normal Mental Status Delirious or high delirium risk/history of Complicated AWS Non ICU ICU CIWA (or other STP) Fixed Dose or Phenobarbital Protocol Fixed Dose or Phenobarbital Protocol Phenobarbital Protocol Dexmedetomidine BZD Symptom Triggered Protocol (RASS)
22 Non BZD Based Strategies Anti epileptic Drugs: Valproate Carbamazepine Phenobarbital Alpha agonists Dexmedetomidine
23 Phenobarbital for Treatment of AWS Reference Pts. (N) AWS Severity Control Outcome Measures Results Rosenson (2013) 102 Unknown Lorazepam +/ placebo Level of admission LOS Adverse events Decreased ICU admissions Decreased LOS None Hendey (2011) 44 Moderate Lorazepam Change in CIWA Ar Score upon ED disposition Difference not significant Young (1987) 62 Moderate None Seizures (n) Delirium (n) Discharge from ED (%) % Ives (1991) +70 Unknown None observational noncomparitive report Seizures (%) Delirium (%) No undue consequences Rosenthal (1998) 32 Mild moderate Valproate MSSA Score Phenobarbital Dose (n) Mariani (2006) 27 Moderate Gabapentin Change in CIWA Ar Score Phenobarbital Doses (n) Change not significant VPA: 20 Control: 39 p<0.05 Difference not significant Gabapentin: 8 Phenobarbital: 5 p<0.45

24 Phenobarbital: Mechanism of Action Loscher, W. Basic Pharmacology of Valproate: A Review After 35 years of Clinical Use for the Treatment of Epilepsy. CNS Drugs (10):
25 Phenobarbital Has GABA agonism AND decreases glutamate activity Research does not demonstrate decreased BZD receptor sensitivity as seen with benzodiazepines Minimal changes in mental status and no observed paradoxical disinhibition Pharmacokinetics are reliable Able to target specific serum levels (which are meaningful clinically) Does NOT have a narrow therapeutic index Longer acting Clegg A & Young JB. Which medications to avoid in people at risk of delirium: a systemic review. Age Ageing. 2011; 40(1): Sanna et al. Changes in GABAA receptor gene expression associated with selective alterations in receptor function and pharmacology after ethanol withdrawal. J of Neuroscience. 2003; 23(37): Clegg A & Young JB. Which medications to avoid in people at risk of delirium: a systemic review. Age Ageing. 2011; 40(1): Sanna et al. Changes in GABAA receptor gene expression associated with selective alterations in receptor function and pharmacology after ethanol withdrawal. J of Neuroscience. 2003; 23(37):
26 Complicated AWS: Phenobarbital Protocol Risk Factors for Alcohol Withdrawal Delirium History of past seizure or delirium tremens Seizure in the field or in ED prior to admission Acute concurrent medical illness More days since last drink (2 or more days) Elevated admission blood alcohol Heavier and longer drinking history Signs of autonomic hyperactivity with BAL of >.1g/dL AGE>40 Burn related injuries Falls, particularly with long bone fractures Elevated MCV, AST (? CDT) On one study MVA had negative predictive value Ferguson J, et al. Risk Factors for Delirium Tremens Development. J Gen Int Med, 1996; 11: Kraemer et al. Impact of Age on Severity, Course and Complications of Alcohol Withdrawal. Arch Int Med, 1997; 157: Lukan et al. Risk Factors for Delirium Tremens in Trauma Patients. J Trauma, 2002; 53(5): Palmstierna T. A model for predicting alcohol withdrawal delirium. Psychiatr Serv 2001;52:820 3.
27 Complicated AWS: Phenobarbital Protocol High Risk: Past DTs +/ Past seizures AND + Recent alcohol use (>2 weeks) or Active symptoms of AWS or + Recent alcohol use, + BAL, elevated MCV, elevated AST:ALT ratio Medium Risk (active alcohol use disorder plus 2 of the following): More days since last drink (2 or more days) Elevated BAL on admit Autonomic dysfunction with BAL >.1 g/dl Elevated MCV and/or AST:ALT ratio Heavier and longer drinking history AGE>35 Burn related injuries Falls, particularly with long bone fractures Risk of Sedation: Age >65 years old Hepatic dysfunction Opiate administration Head injury neuro checks Recent administration of BZDs Current administration of sedatives Respiratory Compromise: PNA Rib fractures Chest tube(s) Pulmonary contusion(s) C collar/brace Minimal or No Risk of Respiratory Compromise 12-15mg/kg High Risk of AWD + Risk of Sedation or Respiratory Compromise 10-12mg/kg Low Risk of AWD: Use PRN BZDs cautiously + Severe Risk of Sedation or Respiratory Compromise 6-10mg/kg Risk of Alcohol Withdrawal Delirium Minimal or No Risk of Respiratory Compromise 10-12mg/kg Medium Risk of AWD + Risk of Sedation or Respiratory Compromise 8-10mg/kg + Severe Risk of Sedation or Respiratory Compromise 6-8mg/kg Nejad et al., J of Trauma, in preparation
28 Complicated AWS: Phenobarbital Protocol Calculate target loading dose with phenobarbital depending on alcohol use severity and comorbid medical illness IBW x (6 to 15mg/kg) = total mg (of loading dose) Where: IBW for men is: kg/inch over 5 feet. IBW for women is: kg/inch over 5 feet. Give loading dose intramuscularly: 40% of loading dose given immediately 30% of loading dose given 3 hours after 1 st IM administration 30% of loading dose given 3 hours after 2 nd IM administration Serum phenobarbital level should be checked 5 hours after the 3 rd IM administration Nejad et al., J of Trauma, in preparation
29 Complicated AWS: Phenobarbital Protocol On day 2, start maintenance dose: MD = (Cl) x (CPss) x (T) (S) x (F) Where: MD: maintenance dose Cl: rate of clearance (0.096 L/day/kg) CPss: desired steady state serum level (10 20 ug/ml) If initial target level 15, then use 20ug/mL If initial level 12, then use 15ug/mL If initial level 10, then use 12ug/mL If initial level 8, then use 10ug/mL If initial level 6, then use 10ug/mL S: Fraction of the total molecular weight of active drug in salt form F: Bioavailability Therefore: (0.096L/day/kg) x IBW (in Kg) x (10 20ug/mL)(1 day) (1.0) x (1.0) = Total maintenance dose Maintenance dose is given ORALLY (or IM) and split in ½, given BID. Nejad et al., J of Trauma, in preparation
30 Complicated AWS: Phenobarbital Protocol Day 3 is the same as day 2 Day 4 the oral dose is decreased by 50% Day 5 it stays the same Day 6 decrease 50% Day 7 decrease 50% Then discontinue No benzodiazepines allowed and an order is placed that none can be given to the patient Contraindications: acute intermittent prophyria, active/previous history of SJS/TEN or rash with AEDs Nejad et al., J of Trauma, in preparation
31 Complicated AWS: Dexmedetomidine Clonidine Selectivity: 2 : 1 200:1 t 1/2 8 hrs PO, patch, epidural Antihypertensive Analgesic adjunct IV formulation not available in US Dexmedetomidine Selectivity: 2 : :1 t 1/2 2 hrs Intravenous Sedative analgesic Primary sedative Only IV 2 available for use in the US
32 Complicated AWS: Dexmedetomidine Administer as a continuous IV infusion in the range of 0.2 to 1.4 µg/kg/h Start at 0.2mcg/kg for one hour and ensure no bradycardia or hypotension, then titrate to need Almost no patient requires more than 0.6mcg/kg/hr for AWS If hypotension develops give IVF bolus and rechallenge Avoid loading dose Normal response to vasoactive drugs Decreases oxygen consumption No effect on ICP Attenuates stress response Decreases metabolism Endocrine NE release insulin release cortisol release GH release
33 Complicated AWS: Dexmedetomidine Patient Selection ICU patient with: High sympathetic activity Agitated With discomfort/pain symptoms Cirrhosis with active alcohol withdrawal symptoms Caution Low blood pressure Hypovolemic/shock/significant SIRS Conduction defects/bradyarrhythmias/poor ventricular function
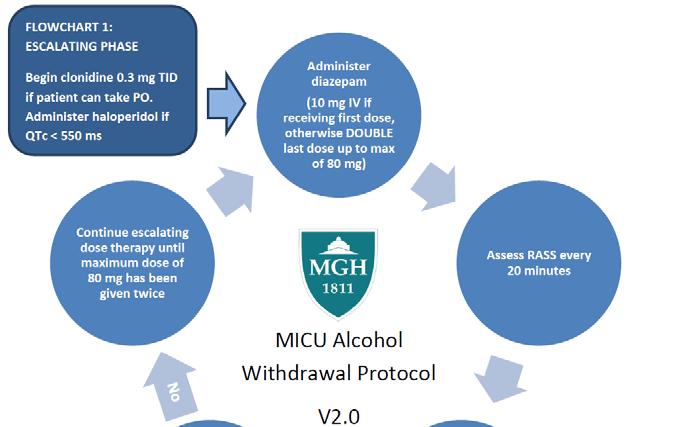
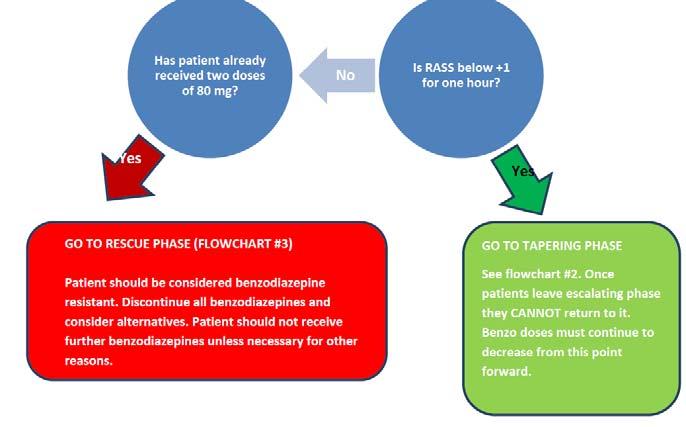
34 Complicated AWS: BZD STP ICU
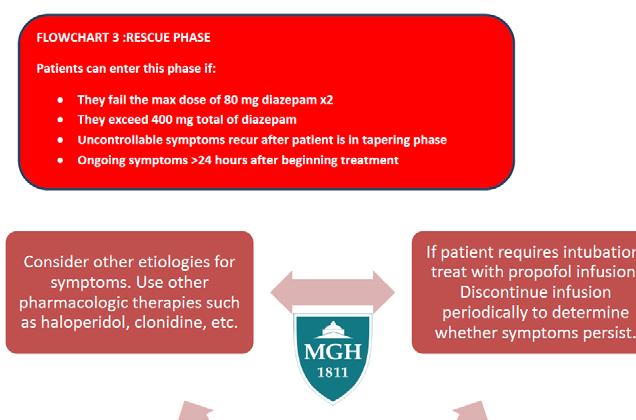
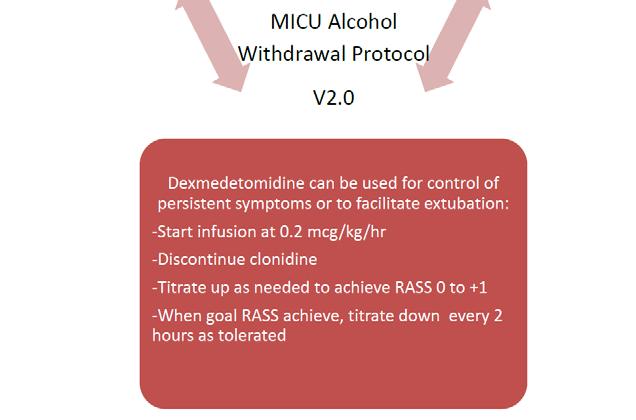
35 Complicated AWS: BZD STP ICU
36 Summary Early in hospital course, utilize epidemiologic data to help guide risk assessment for development of complicated and uncomplicated alcohol withdrawal Active medical illness and PMH, along with current AWS and past detoxification history can help guide you to management strategy: CIWA vs fixed dose vs non BZD protocols Use understanding of pathophysiology of AWS and current symptoms being observed to help guide augmentation strategies for more complicated alcohol withdrawal cases, particularly in those patient with concomitant active medical and surgical illness
Complicated Withdrawal
 Complicated Withdrawal Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim Nejad,
Complicated Withdrawal Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@Swedish.org Disclosures: Shamim Nejad,
Complicated Withdrawal
 Complicated Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts
Complicated Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts
Withdrawal.
 Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts General
Withdrawal Shamim Nejad, MD Director, Adult Burns & Trauma Psychiatry Division of Psychiatry and Medicine Medical Director, Addiction Consultation Team MGH Center for Addiction Medicine Massachusetts General
Goals for sedation during mechanical ventilation
 New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
New Uses of Old Medications Gina Riggi, PharmD, BCCCP, BCPS Clinical Pharmacist Trauma ICU Jackson Memorial Hospital Disclosure I do not have anything to disclose Objectives Describe the use of ketamine
Alcohol withdrawal. Clinical features
 Alcohol withdrawal Clinical features Severity increase with amount consumed; uncommon with < drinks per day. Predictable pattern: patients with previous withdrawal seizures are at high risk for recurrence.
Alcohol withdrawal Clinical features Severity increase with amount consumed; uncommon with < drinks per day. Predictable pattern: patients with previous withdrawal seizures are at high risk for recurrence.
Dexmedetomidine: the various roles and utilization strategies. Julie Belfer, PharmD September 2014
 Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Dexmedetomidine: the various roles and utilization strategies Julie Belfer, PharmD September 2014 Disclosure No disclosures concerning possible financial or personal relationships with commercial entities
Current Clinical Patterns in the Management of Alcohol Withdrawal Syndrome (AWS)
") 1 Current Clinical Patterns in the Management of Alcohol Withdrawal Syndrome (AWS) The goal of the survey is to evaluate current practices for the inpatient management of AWS in adult hospitals located
1 Current Clinical Patterns in the Management of Alcohol Withdrawal Syndrome (AWS) The goal of the survey is to evaluate current practices for the inpatient management of AWS in adult hospitals located
Provider Update: Alcohol Withdrawal Order Set Edits
 Provider Update: Alcohol Withdrawal Order Set Edits Situation: A revised Alcohol Withdrawal Order Set and new CIWA-Ar scoring tool will go LIVE February 12, 2018. Background: The latest guidelines for
Provider Update: Alcohol Withdrawal Order Set Edits Situation: A revised Alcohol Withdrawal Order Set and new CIWA-Ar scoring tool will go LIVE February 12, 2018. Background: The latest guidelines for
Methodist Hospital Alcohol Withdrawal Suggested Guidelines
 Methodist Hospital Alcohol Withdrawal Suggested Guidelines S. Prizada Sattar, MD Teri L Gabel, Pharm.D.,BCPP Sidney Kauzlarich, MD Subhash Bhatia, MD Mitzi Bollinger, RN S. Prizada Sattar, MD 6-20-3 Rationale
Methodist Hospital Alcohol Withdrawal Suggested Guidelines S. Prizada Sattar, MD Teri L Gabel, Pharm.D.,BCPP Sidney Kauzlarich, MD Subhash Bhatia, MD Mitzi Bollinger, RN S. Prizada Sattar, MD 6-20-3 Rationale
Multiple Choice Questions
 Multiple Choice Questions 25yo M presents without psychiatric or medical history, with complaint of tremor to the ER. He denies drinking alcohol but his friend at bedside takes you to the side and reports
Multiple Choice Questions 25yo M presents without psychiatric or medical history, with complaint of tremor to the ER. He denies drinking alcohol but his friend at bedside takes you to the side and reports
PATHOPHYSIOLOGY AND TREATMENT OF ALCOHOL WITHDRAWAL SYNDROME: A REVIEW
 PATHOPHYSIOLOGY AND TREATMENT OF ALCOHOL WITHDRAWAL SYNDROME: A REVIEW Dana Bartlett, BSN, MSN, MA, CSPI Dana Bartlett is a professional nurse and author. His clinical experience includes 16 years of ICU
PATHOPHYSIOLOGY AND TREATMENT OF ALCOHOL WITHDRAWAL SYNDROME: A REVIEW Dana Bartlett, BSN, MSN, MA, CSPI Dana Bartlett is a professional nurse and author. His clinical experience includes 16 years of ICU
Please review the following slides prior to class. Information from these slides will be used to answer patient cases. Come prepared!
 Please review the following slides prior to class Information from these slides will be used to answer patient cases. Come prepared! Alcohol and Opiate Dependence Reference Slides Substances of Abuse A
Please review the following slides prior to class Information from these slides will be used to answer patient cases. Come prepared! Alcohol and Opiate Dependence Reference Slides Substances of Abuse A
Addressing Emergency Neuro- Pharmacologic Controversies Head-On. What dose of IV benzodiazepine makes you uncomfortable?
 Addressing Emergency Neuro- Pharmacologic Controversies Head-On 38 y/o 136 bpm Bryan D. Hayes @PharmERToxGuy Sz, tremor, hallucinations Which benzodiazepine would you administer first? Why? Diazepam Lorazepam
Addressing Emergency Neuro- Pharmacologic Controversies Head-On 38 y/o 136 bpm Bryan D. Hayes @PharmERToxGuy Sz, tremor, hallucinations Which benzodiazepine would you administer first? Why? Diazepam Lorazepam
Alcohol Withdrawal: Assessment and Symptom-Triggered Treatment
 Alcohol Withdrawal: Assessment and Symptom-Triggered Treatment 2016 Alcohol, or ethanol, is produced by the fermentation of yeast, sugars and starches. Yeast breaks sugar down into ethanol and carbon dioxide.
Alcohol Withdrawal: Assessment and Symptom-Triggered Treatment 2016 Alcohol, or ethanol, is produced by the fermentation of yeast, sugars and starches. Yeast breaks sugar down into ethanol and carbon dioxide.
Risk assessment of moderate to severe alcohol withdrawal Predictors for seizures and delirium tremens
 Risk assessment of moderate to severe alcohol withdrawal Predictors for seizures and delirium tremens Results of a retrospective Cohort Study Florian Eyer, MD Toxicological Department Klinikum rechts der
Risk assessment of moderate to severe alcohol withdrawal Predictors for seizures and delirium tremens Results of a retrospective Cohort Study Florian Eyer, MD Toxicological Department Klinikum rechts der
DRAFT FOR CONSULTATION
 1) What is the accuracy of a tool and/or clinical judgement for the a) assessment b) monitoring of patients at risk of acute alcohol withdrawal? 2) Does the assessment and monitoring of patients with acute
1) What is the accuracy of a tool and/or clinical judgement for the a) assessment b) monitoring of patients at risk of acute alcohol withdrawal? 2) Does the assessment and monitoring of patients with acute
ALCOHOL WITHDRAWAL GUIDELINES
 ALCOHOL WITHDRAWAL GUIDELINES Policy author Accountable Executive Lead Approving body Policy reference Dr M Lewis, Gastroenterologist; Professor J A Vale, Clinical Toxicologist; Dr D A Robertson, Alcohol
ALCOHOL WITHDRAWAL GUIDELINES Policy author Accountable Executive Lead Approving body Policy reference Dr M Lewis, Gastroenterologist; Professor J A Vale, Clinical Toxicologist; Dr D A Robertson, Alcohol
Guidelines for the In-Patient Management of Alcohol Withdrawal at Frimley Park Hospital NHS Foundation Trust
 Guidelines for the In-Patient Management of Alcohol Withdrawal at Frimley Park Hospital NHS Foundation Trust Authors: Dr Aftab Ala, Consultant Gastroenterologist & Hepatologist Dr Tasneem Pirani, ST4 in
Guidelines for the In-Patient Management of Alcohol Withdrawal at Frimley Park Hospital NHS Foundation Trust Authors: Dr Aftab Ala, Consultant Gastroenterologist & Hepatologist Dr Tasneem Pirani, ST4 in
Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe )
") PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
Types of epilepsy. 1)Generalized type: seizure activity involve the whole brain, it is divided into:
Generalized type: seizure activity involve the whole brain, it is divided into:") Types of epilepsy We have different types of epilepsy, so it is not one type of seizures that the patient can suffer from; we can find some patients with generalized or partial seizure. So, there are two
Types of epilepsy We have different types of epilepsy, so it is not one type of seizures that the patient can suffer from; we can find some patients with generalized or partial seizure. So, there are two
Alcohol withdrawal including the Symptom triggered CIWA score Management
 Alcohol withdrawal including the Symptom triggered CIWA score Management Classification: Policy Lead Author: Ruth Brown Alcohol specialist Nurse Additional author(s): Hailey Pennington Authors Division:
Alcohol withdrawal including the Symptom triggered CIWA score Management Classification: Policy Lead Author: Ruth Brown Alcohol specialist Nurse Additional author(s): Hailey Pennington Authors Division:
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium
 Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Fighting the Fog A Collaborative Approach to Decreasing ICU Delirium Kimberly Scherr NP Jennifer Barker RN Misericordia Hospital ICU Edmonton, AB CACCN Dynamics Sept 21, 2014 Delirium Delirium is an acute
Introduction. 1 person in 20 will have an epileptic seizure at some time in their life
 Introduction 1 person in 20 will have an epileptic seizure at some time in their life Epilepsy is diagnosed on the basis of two or more epileptic seizures. Around 450,000 people in the UK have epilepsy
Introduction 1 person in 20 will have an epileptic seizure at some time in their life Epilepsy is diagnosed on the basis of two or more epileptic seizures. Around 450,000 people in the UK have epilepsy
AACN PCCN Review. Behavioral
 AACN PCCN Review Behavioral Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com 0 Behavioral I. INTRODUCTION PCCN
AACN PCCN Review Behavioral Presenter: Carol A. Rauen, RN, MS, CCNS, CCRN, PCCN, CEN Independent Clinical Nurse Specialist & Education Consultant rauen.carol104@gmail.com 0 Behavioral I. INTRODUCTION PCCN
Management of Delirium in the ICU. Yahya Shehabi
 Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
Management of Delirium in the ICU Yahya Shehabi Hello! Doctor, your patient is CAM + ve Good morning Dr, Am one of the RC, Just examined Mr XXX he is CAM +ve Positive what? Sir replied RC: I meant he is
ALCOHOL USE DISORDER WITHDRAWAL MANAGEMENT AND LONG TERM TREATMENT ANA HOLTEY, MD ADDICTION MEDICINE FELLOW UNIVERSITY OF UTAH HEALTH
 ALCOHOL USE DISORDER WITHDRAWAL MANAGEMENT AND LONG TERM TREATMENT ANA HOLTEY, MD ADDICTION MEDICINE FELLOW UNIVERSITY OF UTAH HEALTH Prevalence of 12-Month Alcohol Use, High-Risk Drinking, and DSM-IV
ALCOHOL USE DISORDER WITHDRAWAL MANAGEMENT AND LONG TERM TREATMENT ANA HOLTEY, MD ADDICTION MEDICINE FELLOW UNIVERSITY OF UTAH HEALTH Prevalence of 12-Month Alcohol Use, High-Risk Drinking, and DSM-IV
Buspirone Carbamazepine Diazepam Disulfiram Ethosuximide Flumazeil Gabapentin Lamotrigine
 CNS Depressants Buspirone Carbamazepine Diazepam Disulfiram Ethosuximide Flumazeil Gabapentin Lamotrigine Lorazepam Phenobarbital Phenytoin Topiramate Valproate Zolpidem Busprione Antianxiety 5-HT1A partial
CNS Depressants Buspirone Carbamazepine Diazepam Disulfiram Ethosuximide Flumazeil Gabapentin Lamotrigine Lorazepam Phenobarbital Phenytoin Topiramate Valproate Zolpidem Busprione Antianxiety 5-HT1A partial
Interprofessional Trauma Conference September 28th 2018 Montreal
 Interprofessional Trauma Conference September 28th 2018 Montreal Marc Perreault & Marc Alexandre Duceppe ICU Pharmacists MGH & RVH-CUSM Faculté de Pharmacie Université de Montréal I have no potential conflict
Interprofessional Trauma Conference September 28th 2018 Montreal Marc Perreault & Marc Alexandre Duceppe ICU Pharmacists MGH & RVH-CUSM Faculté de Pharmacie Université de Montréal I have no potential conflict
Lumbar Fusion. Reference Guide for PACU CLINICAL PATHWAY. All patient variances to the pathway are to be circled and addressed in the progress notes.
 Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
Reference Guide for PACU Lumbar Fusion CLINICAL PATHWAY All patient variances to the pathway are to be circled and addressed in the progress notes. This Clinical Pathway is intended to assist in clinical
CIWA-AR CLINICAL INSTITUTE WITHDRAWAL ASSESSMENT FOR ALCOHOL SCALE
 CIWA-AR CLINICAL INSTITUTE WITHDRAWAL ASSESSMENT FOR ALCOHOL SCALE SAM G CAMPBELL MB BCH, FCFP(EM), DIP PEC(SA), FCCHL, FRCP(EDIN) PROFESSOR OF EMERGENCY MEDICINE DALHOUSIE UNIVERSITY, HALIFAX, NOVA SCOTIA.
CIWA-AR CLINICAL INSTITUTE WITHDRAWAL ASSESSMENT FOR ALCOHOL SCALE SAM G CAMPBELL MB BCH, FCFP(EM), DIP PEC(SA), FCCHL, FRCP(EDIN) PROFESSOR OF EMERGENCY MEDICINE DALHOUSIE UNIVERSITY, HALIFAX, NOVA SCOTIA.
Anxiolytic, Sedative and Hypnotic Drugs. Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia
 Anxiolytic, Sedative and Hypnotic Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Anxiolytics: reduce anxiety Sedatives: decrease activity, calming
Anxiolytic, Sedative and Hypnotic Drugs Assistant Prof. Dr. Najlaa Saadi PhD Pharmacology Faculty of Pharmacy University of Philadelphia Anxiolytics: reduce anxiety Sedatives: decrease activity, calming
North Wales Critical Care Network
 North Wales Critical Care Network SEDATION GUIDELINES FOR ADULTS IN CRITICAL CARE Approved 6.9.12 1 Sedation guidelines for intensive care Betsi Cadwaladr University Health Board (Adapted from guidelines
North Wales Critical Care Network SEDATION GUIDELINES FOR ADULTS IN CRITICAL CARE Approved 6.9.12 1 Sedation guidelines for intensive care Betsi Cadwaladr University Health Board (Adapted from guidelines
Treatment of Alcohol and Opiate Withdrawal
 Objectives Treatment of Alcohol and Opiate Withdrawal Renee Striker, Pharm.D., BCPS, BCPP Pharmacy Clinical Specialist Huron Hospital East Cleveland, Ohio Outline the diagnostic criteria for substance
Objectives Treatment of Alcohol and Opiate Withdrawal Renee Striker, Pharm.D., BCPS, BCPP Pharmacy Clinical Specialist Huron Hospital East Cleveland, Ohio Outline the diagnostic criteria for substance
POST-INTUBATION ANALGESIA AND SEDATION. August 2012 J Pelletier
 POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
POST-INTUBATION ANALGESIA AND SEDATION August 2012 J Pelletier Intubated patients experience pain and anxiety Mechanical ventilation, endotracheal tube Blood draws, positioning, suctioning Surgical procedures,
DRUGS THAT ACT IN THE CNS
 DRUGS THAT ACT IN THE CNS Anxiolytic and Hypnotic Drugs Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 OTHER ANXIOLYTIC AGENTS/ A. Antidepressants Many antidepressants are effective in the treatment
DRUGS THAT ACT IN THE CNS Anxiolytic and Hypnotic Drugs Dr Karamallah S. Mahmood PhD Clinical Pharmacology 1 OTHER ANXIOLYTIC AGENTS/ A. Antidepressants Many antidepressants are effective in the treatment
Alcohol Detoxification (Inpatient) Prescribing Guidelines
 Prescribing Guidelines") Alcohol Detoxification (Inpatient) Prescribing Guidelines Author: Sponsor/Executive: Responsible committee: Consultation & Approval: (Committee/Groups which signed off the procedure, including date) This
Alcohol Detoxification (Inpatient) Prescribing Guidelines Author: Sponsor/Executive: Responsible committee: Consultation & Approval: (Committee/Groups which signed off the procedure, including date) This
Status Epilepticus: Implications Outside the Neuro-ICU
 Status Epilepticus: Implications Outside the Neuro-ICU Jeffrey M Singh MD Critical Care and Neurocritical Care Toronto Western Hospital October 31 st, 2014 Disclosures I (unfortunately) have no disclosures
Status Epilepticus: Implications Outside the Neuro-ICU Jeffrey M Singh MD Critical Care and Neurocritical Care Toronto Western Hospital October 31 st, 2014 Disclosures I (unfortunately) have no disclosures
Disclosures. Learning Objective 4/26/2017
 Management of acute alcohol withdrawal at a community hospital in an area with a high prevalence of alcoholism { Melissa Cirillo, Pharm.D. 4/29/2017 Financial: None Nonfinancial: None Disclosures List
Management of acute alcohol withdrawal at a community hospital in an area with a high prevalence of alcoholism { Melissa Cirillo, Pharm.D. 4/29/2017 Financial: None Nonfinancial: None Disclosures List
Drug. Alcohol is one of the most frequently abused drugs in American society. Update
 AACN Advanced Critical Care Volume 28, Number 3, pp. 233-238 2017 AACN Drug Update Earnest Alexander, PharmD, and Gregory M. Susla, PharmD Department Editors Pharmacologic Management of Alcohol Withdrawal
AACN Advanced Critical Care Volume 28, Number 3, pp. 233-238 2017 AACN Drug Update Earnest Alexander, PharmD, and Gregory M. Susla, PharmD Department Editors Pharmacologic Management of Alcohol Withdrawal
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University
 Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
Jennifer Mando-Vandrick, PharmD, BCPS Clinical Pharmacist, Emergency Department Director, PGY2 Critical Care Pharmacy Residency Duke University Hospital Objectives Review pertinent pharmacotherapy common
STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION
 STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION Patients receiving analgesia and/or sedation for longer than 5-7 days may suffer withdrawal if these drugs are suddenly stopped. To prevent this happening
STARSHIP WITHDRAWAL OF ANALGESIA AND SEDATION Patients receiving analgesia and/or sedation for longer than 5-7 days may suffer withdrawal if these drugs are suddenly stopped. To prevent this happening
Stabilization Algorithm
 VA/DoD Clinical Practice Guideline for the Management of Substance Use Disorders Stabilization Algorithm Stabilization Pocket Card 1 Patient and Time Information Clinical Institute Withdrawal Assessment
VA/DoD Clinical Practice Guideline for the Management of Substance Use Disorders Stabilization Algorithm Stabilization Pocket Card 1 Patient and Time Information Clinical Institute Withdrawal Assessment
Drug Treatment of ADHD. by Dr Christine Sutherland
 Drug Treatment of ADHD by Dr Christine Sutherland Psychostimulant Actions Who put the Benzedrine, in Mrs. Murphy's Ovaltine? Where did she get that stuff Now she just can't get enough She stays up nights
Drug Treatment of ADHD by Dr Christine Sutherland Psychostimulant Actions Who put the Benzedrine, in Mrs. Murphy's Ovaltine? Where did she get that stuff Now she just can't get enough She stays up nights
Epilepsy CASE 1 Localization Differential Diagnosis
 2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
2 Epilepsy CASE 1 A 32-year-old man was observed to suddenly become unresponsive followed by four episodes of generalized tonic-clonic convulsions of the upper and lower extremities while at work. Each
Title Alcohol Withdrawal Management Guidelines
 Document Control Title Alcohol Withdrawal Management Guidelines Author Directorate Date Version Issued 0.1 Dec 2009 0.2 Mar 2010 0.3 Nov 2010 Status Draft 0.4 Sep 2015 1.0 Jan 2016 2.0 Nov Final 2018 Main
Document Control Title Alcohol Withdrawal Management Guidelines Author Directorate Date Version Issued 0.1 Dec 2009 0.2 Mar 2010 0.3 Nov 2010 Status Draft 0.4 Sep 2015 1.0 Jan 2016 2.0 Nov Final 2018 Main
General Effects. Special Patient Populations. Alcoholism. Who is an Alcoholic
 Alcohol Use & Abuse in Acutely and Critically Ill Patients: Don t Be Fooled General Effects Christine Schulman, RN, MS, CNS, CCRN Clinical Nurse Specialist & Consultant Trauma & Critical Care Nursing Portland,
Alcohol Use & Abuse in Acutely and Critically Ill Patients: Don t Be Fooled General Effects Christine Schulman, RN, MS, CNS, CCRN Clinical Nurse Specialist & Consultant Trauma & Critical Care Nursing Portland,
ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments
 ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
ADENOSINE Paroxysmal SVT 1 st Dose 6 mg rapid IV 2 nd & 3 rd Doses 12 mg rapid IV push Follow each dose with rapid bolus of 20 ml NS May cause transient heart block or asystole. Side effects include chest
NonConvulsive Seizure
 Sample Protocol #5: Management of status epilepticus and seizures in hospitalized patients nconvulsive Seizure Patient presents with alteration of consciousness unexplained by other etiologies AND suspicious
Sample Protocol #5: Management of status epilepticus and seizures in hospitalized patients nconvulsive Seizure Patient presents with alteration of consciousness unexplained by other etiologies AND suspicious
Pediatric Procedural Sedation
 Pediatric Procedural Sedation Case 1: 2 year old complex facial laceration Judith R. Klein, MD, FACEP Assistant Professor of Emergency Medicine UCSF-SFGH Department of Emergency Medicine Objectives: The
Pediatric Procedural Sedation Case 1: 2 year old complex facial laceration Judith R. Klein, MD, FACEP Assistant Professor of Emergency Medicine UCSF-SFGH Department of Emergency Medicine Objectives: The
Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents
 Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents Myth or Reality? Complete Recovery means a medication-free state True or False? Treatment of Alcoholism Assessment Motivation Alcohol
Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents Myth or Reality? Complete Recovery means a medication-free state True or False? Treatment of Alcoholism Assessment Motivation Alcohol
11/1/ LLSA ARTICLES 1-4 ANGIOEDEMA ANGIOEDEMA BRADYKININ-MEDIATED HEREDITARY ANGIOEDEMA ACE INHIBITOR ANGIOEDEMA
 2017 LLSA ARTICLES 1-4 BRIAN FELICE, MD NOVEMBER 5, 2018 ANGIOEDEMA Moellman JJ, Bernstein JA, Lindsell C., et al.; American College of Allergy, Asthma & Immunology (ACAAI); Society for Academic Emergency
2017 LLSA ARTICLES 1-4 BRIAN FELICE, MD NOVEMBER 5, 2018 ANGIOEDEMA Moellman JJ, Bernstein JA, Lindsell C., et al.; American College of Allergy, Asthma & Immunology (ACAAI); Society for Academic Emergency
Analgesic-Sedatives Drug Dose Onset
 Table 4. Commonly used medications in procedural sedation and analgesia Analgesic-Sedatives Fentanyl Morphine IV: 1-2 mcg/kg Titrate 1 mcg/kg q3-5 minutes prn IN: 2 mcg/kg Nebulized: 3 mcg/kg IV: 0.05-0.15
Table 4. Commonly used medications in procedural sedation and analgesia Analgesic-Sedatives Fentanyl Morphine IV: 1-2 mcg/kg Titrate 1 mcg/kg q3-5 minutes prn IN: 2 mcg/kg Nebulized: 3 mcg/kg IV: 0.05-0.15
Substitution Therapy for Opioid Use Disorder The Role of Suboxone
 Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
I. Introduction Epilepsy is the tendency to have recurrent seizures unprovoked by systemic or acute neurologic insults. Antiepileptic drugs (AEDs)
") 1 2 I. Introduction Epilepsy is the tendency to have recurrent seizures unprovoked by systemic or acute neurologic insults. Antiepileptic drugs (AEDs) are those which decrease the frequency and/or severity
1 2 I. Introduction Epilepsy is the tendency to have recurrent seizures unprovoked by systemic or acute neurologic insults. Antiepileptic drugs (AEDs) are those which decrease the frequency and/or severity
Top 5 things you need to know about pediatric procedural sedation
 Top 5 things you need to know about pediatric procedural sedation Dr. Marc N. Francis MD, FRCPC ACH/FMC Emergency Physician Clinical Lecturer University of Calgary Assistant Program Director FRCPC-EM STARS
Top 5 things you need to know about pediatric procedural sedation Dr. Marc N. Francis MD, FRCPC ACH/FMC Emergency Physician Clinical Lecturer University of Calgary Assistant Program Director FRCPC-EM STARS
From Where? Rochester, NY
 From Where? Rochester, NY 3 Days of Sunshine Annually Invented SAD Lights Disclosures I have no financial disclosures The feds want their money back The only bad question... Objectives Review endocrine
From Where? Rochester, NY 3 Days of Sunshine Annually Invented SAD Lights Disclosures I have no financial disclosures The feds want their money back The only bad question... Objectives Review endocrine
Lead for Gastroenterology Lee Dodge Alcohol Liaison 03/03/2015. Clive Gibson Safeguarding Adults Lead Nurse 03/03/2015
 Acute Alcohol Withdrawal Management for Adult Inpatients Type: Clinical Guideline Register No: 1409 Status: Public on ratification Developed in response to: Best Practice Contributes to CQC Outcome number:
Acute Alcohol Withdrawal Management for Adult Inpatients Type: Clinical Guideline Register No: 1409 Status: Public on ratification Developed in response to: Best Practice Contributes to CQC Outcome number:
PRESCRIBING PRACTICE IN DELIRIUM. John Warburton Critical Care Pharmacist
 PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
Blame it on the Alcohol: Comparison of Propofol vs Dexmedetomidine for Refractory Alcohol Withdrawal
 Blame it on the Alcohol: Comparison of Propofol vs Dexmedetomidine for Refractory Alcohol Withdrawal Kristi Hargrove, PharmD PGY1 Pharmacy Resident Department of Pharmacotherapy and Pharmacy Services,
Blame it on the Alcohol: Comparison of Propofol vs Dexmedetomidine for Refractory Alcohol Withdrawal Kristi Hargrove, PharmD PGY1 Pharmacy Resident Department of Pharmacotherapy and Pharmacy Services,
Alcohol and Trauma. Judy Mikhail 1:45
 Alcohol and Trauma Judy Mikhail 1:45 Alcohol and Trauma: It s A Conundrum June 5, 2018 Judy Mikhail MTQIP Program Manager Alcohol and Trauma What is the relationship? MTQIP and Alcohol Data Collection
Alcohol and Trauma Judy Mikhail 1:45 Alcohol and Trauma: It s A Conundrum June 5, 2018 Judy Mikhail MTQIP Program Manager Alcohol and Trauma What is the relationship? MTQIP and Alcohol Data Collection
Management of Alcohol Dependence
 STANDARD TREATMENT GUIDELINES Management of Alcohol Dependence Quick Reference Guide February 2016 Ministry of Health & Family Welfare Government of India 1 Table of Contents Objectives-... 3 Diagnosis...
STANDARD TREATMENT GUIDELINES Management of Alcohol Dependence Quick Reference Guide February 2016 Ministry of Health & Family Welfare Government of India 1 Table of Contents Objectives-... 3 Diagnosis...
Sedation and Delirium Questions
 Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Sedation and Delirium Questions TLC Curriculum William J. Ehlenbach, MD MSc Assistant Professor of Medicine Pulmonary & Critical Care Medicine Question 1 Deep sedation in ventilated critically patients
Neurostorm: Modern understanding and nomenclature. Mitch Stanek RN, CBIS Charge Nurse/Infection Preventionist On With Life
 Neurostorm: Modern understanding and nomenclature Mitch Stanek RN, CBIS Charge Nurse/Infection Preventionist On With Life Despite its significant clinical impact, the scientific literature on this syndrome
Neurostorm: Modern understanding and nomenclature Mitch Stanek RN, CBIS Charge Nurse/Infection Preventionist On With Life Despite its significant clinical impact, the scientific literature on this syndrome
Predictors of Severity of Alcohol Withdrawal in Hospitalized Patients
 Elmer Original Article ress Predictors of Severity of Alcohol Withdrawal in Hospitalized Patients Radhames Ramos a, Thierry Mallet b, Anthony DiVittis c b, d, e, Ronny Cohen Abstract Background: Alcohol
Elmer Original Article ress Predictors of Severity of Alcohol Withdrawal in Hospitalized Patients Radhames Ramos a, Thierry Mallet b, Anthony DiVittis c b, d, e, Ronny Cohen Abstract Background: Alcohol
Pharmacological Therapy Policy Practice Guidance Note Management of Acute Alcohol Withdrawal in Adults (Over 18) - V01. Planned review: December 2017
 - V01. Planned review: December 2017") Pharmacological Therapy Policy Practice Guidance Note Management of Acute Alcohol Withdrawal in Adults (Over 18) - V01 V01 issued: Issue 1- Dec 14 Issue 2 April 17 Planned review: December 2017 PPT-PGN
Pharmacological Therapy Policy Practice Guidance Note Management of Acute Alcohol Withdrawal in Adults (Over 18) - V01 V01 issued: Issue 1- Dec 14 Issue 2 April 17 Planned review: December 2017 PPT-PGN
Tranquilizers & Sedative-Hypnotics
 Tranquilizers & Sedative-Hypnotics 1 Tranquilizer or anxiolytic: Drugs used therapeutically to treat agitation or anxiety Sedative-Hypnotic: drugs used to sedate and aid in sleep Original sedatives (before
Tranquilizers & Sedative-Hypnotics 1 Tranquilizer or anxiolytic: Drugs used therapeutically to treat agitation or anxiety Sedative-Hypnotic: drugs used to sedate and aid in sleep Original sedatives (before
9/28/2016. Sedation Strategies in the ICU. Outline. ICU sedation. Recent clinical practice guidelines Top 10 myths A practical approach
 Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Sedation Strategies in the ICU UW Medicine EMS and Trauma Conference Seattle, Washington September 26 th, 2016 C. Terri Hough, MD MSc Associate Professor of Medicine Division of Pulmonary and Critical
Sedative-Hypnotics. Sedative Agents (General Considerations)
") Sedative Agents (General Considerations) No best sedative agent Any agent given in sufficient dosage can produce any level of sedation Intravenous dosing is more predictable then intramuscular or oral
Sedative Agents (General Considerations) No best sedative agent Any agent given in sufficient dosage can produce any level of sedation Intravenous dosing is more predictable then intramuscular or oral
Mood Disorders.
 Mood Disorders Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Disclosures Neither I nor my spouse/partner
Mood Disorders Shamim Nejad, MD Medical Director, Psycho-Oncology Services Swedish Cancer Institute Swedish Medical Center Seattle, Washington Shamim.Nejad@swedish.org Disclosures Neither I nor my spouse/partner
Behavioral Health Service Request Form Detox and Substance Abuse Rehab
 Medicaid Call for Pre-Certification of Admissions: 1-855-620-1861 Kentucky Medicaid Fax: 1-877-338-3686 Standard Request Requests for prior authorization (with supporting clinical information and documentation)
Medicaid Call for Pre-Certification of Admissions: 1-855-620-1861 Kentucky Medicaid Fax: 1-877-338-3686 Standard Request Requests for prior authorization (with supporting clinical information and documentation)
Anti-epileptic Drugs
 Anti-epileptic Drugs We will continue talking about epilepsy which is a chronic disease that has to be managed, so the treatment will be a management treatment, not a single day or week treatment we will
Anti-epileptic Drugs We will continue talking about epilepsy which is a chronic disease that has to be managed, so the treatment will be a management treatment, not a single day or week treatment we will
Results of a one-year, retrospective medication use evaluation. Joseph Ladd, PharmD PGY-1 Pharmacy Resident BHSF Homestead Hospital
 Results of a one-year, retrospective medication use evaluation Joseph Ladd, PharmD PGY-1 Pharmacy Resident BHSF Homestead Hospital Briefly review ketamine s history, mechanism of action, and unique properties
Results of a one-year, retrospective medication use evaluation Joseph Ladd, PharmD PGY-1 Pharmacy Resident BHSF Homestead Hospital Briefly review ketamine s history, mechanism of action, and unique properties
Unit VIII Problem 7 Pharmacology: Principles of Management of Seizure Disorders
 Unit VIII Problem 7 Pharmacology: Principles of Management of Seizure Disorders - Terminologies: Anti-convulsants: they are used to control convulsions seen in certain types of epilepsy. Convulsions may
Unit VIII Problem 7 Pharmacology: Principles of Management of Seizure Disorders - Terminologies: Anti-convulsants: they are used to control convulsions seen in certain types of epilepsy. Convulsions may
Refractory Seizures. Dr James Edwards EMCORE May 30th 2014
 Refractory Seizures Dr James Edwards EMCORE May 30th 2014 Refractory Seizures Seizures are a common presentation to the ED and some patients will have multiple seizures or have a reduced level of consciousness
Refractory Seizures Dr James Edwards EMCORE May 30th 2014 Refractory Seizures Seizures are a common presentation to the ED and some patients will have multiple seizures or have a reduced level of consciousness
Lorraine Wilson, 74 years of age, is admitted. Alcohol Withdrawal. During Hospitalization. Early recognition and consistent intervention are critical.
 1.9 h o u r s Continuing Education Withdrawal During Hospitalization Early recognition and consistent intervention are critical. Overview: For a chronic drinker, sudden alcohol withdrawal because of an
1.9 h o u r s Continuing Education Withdrawal During Hospitalization Early recognition and consistent intervention are critical. Overview: For a chronic drinker, sudden alcohol withdrawal because of an
PHARMACOTHERAPY OF SMOKING CESSATION
 PHARMACOTHERAPY OF SMOKING CESSATION Domenic A. Ciraulo, MD Director of Alcohol Pharmacotherapy Research Center for Addiction Medicine Department of Psychiatry Massachusetts General Hospital Disclosure
PHARMACOTHERAPY OF SMOKING CESSATION Domenic A. Ciraulo, MD Director of Alcohol Pharmacotherapy Research Center for Addiction Medicine Department of Psychiatry Massachusetts General Hospital Disclosure
Anticonvulsants Antiseizure
 Anticonvulsants Antiseizure Seizure disorders Head trauma Stroke Drugs (overdose, withdrawal) Brain tumor Encephalitis/ Meningitis High fever Hypoglycemia Hypocalcemia Hypoxia genetic factors Epileptic
Anticonvulsants Antiseizure Seizure disorders Head trauma Stroke Drugs (overdose, withdrawal) Brain tumor Encephalitis/ Meningitis High fever Hypoglycemia Hypocalcemia Hypoxia genetic factors Epileptic
In our patients the cause of seizures can be broadly divided into structural and systemic causes.
 Guidelines for the management of Seizures Amalgamation and update of previous policies 7 (Seizure guidelines, ND, 2015) and 9 (Status epilepticus, KJ, 2011) Seizures can occur in up to 15% of the Palliative
Guidelines for the management of Seizures Amalgamation and update of previous policies 7 (Seizure guidelines, ND, 2015) and 9 (Status epilepticus, KJ, 2011) Seizures can occur in up to 15% of the Palliative
PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER
 Nursing Daily awakenings PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER Do not perform daily awakenings: Rationale: Daily
Nursing Daily awakenings PHYSICIAN'S ORDERS Mark in for desired orders. If is blank, order is inactive. VENTILATOR SEDATION / ANALGESIC / DELIRIUM ORDER Do not perform daily awakenings: Rationale: Daily
New antiepileptic drugs
 Chapter 29 New antiepileptic drugs J.W. SANDER UCL Institute of Neurology, University College London, National Hospital for Neurology and Neurosurgery, Queen Square, London, and Epilepsy Society, Chalfont
Chapter 29 New antiepileptic drugs J.W. SANDER UCL Institute of Neurology, University College London, National Hospital for Neurology and Neurosurgery, Queen Square, London, and Epilepsy Society, Chalfont
A NEW RATING SCALE FOR THE ASSESSMENT OF THE ALCOHOL-WITHDRAWAL SYNDROME (AWS SCALE)
") Alcohol & Alcoholism Vol. 32, No. 6, pp. 753-760, 1997 A NEW RATING SCALE FOR THE ASSESSMENT OF THE ALCOHOL-WITHDRAWAL SYNDROME (AWS SCALE) TILMAN WETTERLING*, ROLF-DETER KANTTZ, BETTINA BESTERS, DOROTHEA
Alcohol & Alcoholism Vol. 32, No. 6, pp. 753-760, 1997 A NEW RATING SCALE FOR THE ASSESSMENT OF THE ALCOHOL-WITHDRAWAL SYNDROME (AWS SCALE) TILMAN WETTERLING*, ROLF-DETER KANTTZ, BETTINA BESTERS, DOROTHEA
Delirium. Assessment and Management
 Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Delirium Assessment and Management Goals and Objectives Participants will: 1. be able to recognize and diagnose the syndrome of delirium. 2. understand the causes of delirium. 3. become knowledgeable about
Neuroprotective Effects for TBI. Craig Williamson, MD
 Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Neuroprotective Effects for TBI Craig Williamson, MD Neuroprotection in Traumatic Brain Injury Craig Williamson Clinical Assistant Professor Neurocritical Care Fellowship Director Disclosures I will discuss
Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS)
") Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS) Georgios Dadoudis Anesthesiologist ICU DIRECTOR INTERBALKAN MEDICAL CENTER Optimal performance requires:
Optimal sedation and management of anxiety in patients undergoing endobronchial ultrasound (EBUS) Georgios Dadoudis Anesthesiologist ICU DIRECTOR INTERBALKAN MEDICAL CENTER Optimal performance requires:
Disclosure. Learning Objectives
 Linda D. Leary, M.D. Associate Clinical Professor of Pediatrics & Neurology South Texas Comprehensive Epilepsy Center UT Health Science Center San Antonio Disclosure Linda D. Leary, M.D. discloses the
Linda D. Leary, M.D. Associate Clinical Professor of Pediatrics & Neurology South Texas Comprehensive Epilepsy Center UT Health Science Center San Antonio Disclosure Linda D. Leary, M.D. discloses the
improving the patient s quality of life.
 Epilepsy is the tendency to have recurrent seizures unprovoked by systemic or acute neurologic insults. Antiepileptic drugs (AEDs) are those which decrease the frequency and/or severity of seizures in
Epilepsy is the tendency to have recurrent seizures unprovoked by systemic or acute neurologic insults. Antiepileptic drugs (AEDs) are those which decrease the frequency and/or severity of seizures in
Sedation and delirium- drugs and clinical management
 Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
Sedation and delirium- drugs and clinical management Shannon S. Carson, MD Associate Professor and Chief Division of Pulmonary and Critical Care Medicine University of North Carolina Probability of transitioning
TIAGABINE. THERAPEUTICS Brands Gabitril see index for additional brand names. Generic? Yes
 TIAGABINE THERAPEUTICS Brands Gabitril see index for additional brand names Generic? Yes Class Anticonvulsant; selective GABA reuptake inhibitor (SGRI) Commonly Prescribed for (bold for FDA approved) Partial
TIAGABINE THERAPEUTICS Brands Gabitril see index for additional brand names Generic? Yes Class Anticonvulsant; selective GABA reuptake inhibitor (SGRI) Commonly Prescribed for (bold for FDA approved) Partial
Adult Drug Reference. Dopamine Drip Chart. Pediatric Drug Reference. Pediatric Drug Dosage Charts DRUG REFERENCES
 Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
Adult Drug Reference Dopamine Drip Chart Pediatric Drug Reference Pediatric Drug Dosage Charts DRUG REFERENCES ADULT DRUG REFERENCE Drug Indication Adult Dosage Precautions / Comments ADENOSINE Paroxysmal
KICU Spontaneous Awakening Trial (SAT) Questionnaire
 Questionnaire") KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
KICU Spontaneous Awakening Trial (SAT) Questionnaire Please select your best answer(s): 1. What is your professional role? 1 Staff Nurse 2 Nurse Manager 3 Nurse Educator 4 Physician 5 Medical Director
COMPARISON OF SEDATION FOR ALCOHOL WITHDRAWAL Crispo et al 911
 Comparison of Clinical Outcomes in Nonintubated Patients with Severe Alcohol Withdrawal Syndrome Treated with Continuous-Infusion Sedatives: Dexmedetomidine versus Benzodiazepines Angela L. Crispo, 1 Mitchell
Comparison of Clinical Outcomes in Nonintubated Patients with Severe Alcohol Withdrawal Syndrome Treated with Continuous-Infusion Sedatives: Dexmedetomidine versus Benzodiazepines Angela L. Crispo, 1 Mitchell
Carbamazepine has a clearance of L/h/kg for monotherapy. For immediate release carbamazepine, the oral bioavailbility is 0.8
 PHA 5128 Dose Optimization II, Spring 2013, Case Study IV Solution If you have any questions regarding this case study, do not hesitate to contact Benjamin Weber (benjaminweber@ufl.edu). Please remember
PHA 5128 Dose Optimization II, Spring 2013, Case Study IV Solution If you have any questions regarding this case study, do not hesitate to contact Benjamin Weber (benjaminweber@ufl.edu). Please remember
Delirium Monograph - Update, Spring 2014
 Delirium Monograph - Update, Spring 2014 Since publication of the APM monograph on Delirium in January 2012, three structured reviews have been published adding data relevant to the practice of identification,
Delirium Monograph - Update, Spring 2014 Since publication of the APM monograph on Delirium in January 2012, three structured reviews have been published adding data relevant to the practice of identification,
Assessment Main title and management of alcohol dependence and withdrawal in the acute hospital: concise guidance
 CONCISE GUIDANCE Clinical Medicine 01, Vol 1, No : 71 Assessment Main title and management of alcohol dependence and withdrawal in the acute hospital: concise guidance Author head name Stephen Stewart
CONCISE GUIDANCE Clinical Medicine 01, Vol 1, No : 71 Assessment Main title and management of alcohol dependence and withdrawal in the acute hospital: concise guidance Author head name Stephen Stewart
Psychopharmacology in the Emergency Room. Michael D. Jibson, M.D., Ph.D. Professor of Psychiatry University of Michigan
 Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Professor of Psychiatry University of Michigan Pretest 1. Which of the following conditions is LEAST likely to benefit from emergency
Psychopharmacology in the Emergency Room Michael D. Jibson, M.D., Ph.D. Professor of Psychiatry University of Michigan Pretest 1. Which of the following conditions is LEAST likely to benefit from emergency
Role of Quetiapine in an Adult Critical Care Practice
 American Journal of Pharmacology and Pharmacotherapeutics Short Communication Role of Quetiapine in an Adult Critical Care Practice Vikram Anumakonda* Dudley Group of Hospitals NHS Foundation Trust Birmingham,
American Journal of Pharmacology and Pharmacotherapeutics Short Communication Role of Quetiapine in an Adult Critical Care Practice Vikram Anumakonda* Dudley Group of Hospitals NHS Foundation Trust Birmingham,
Epilepsy and Epileptic Seizures
 Epilepsy and Epileptic Seizures Petr Marusič Dpt. of Neurology Charles University, Second Faculty of Medicine Motol University Hospital Diagnosis Steps Differentiation of nonepileptic events Seizure classification
Epilepsy and Epileptic Seizures Petr Marusič Dpt. of Neurology Charles University, Second Faculty of Medicine Motol University Hospital Diagnosis Steps Differentiation of nonepileptic events Seizure classification
Behavioral Health Service Request Form Detox and Substance Abuse Rehab
 Arkansas 855-538-0454 Connecticut 855-538-0454 Florida 855-538-0454 Georgia 800-424-5412 Illinois 800-504-2766 Kentucky 855-620-1861 Louisiana 855-538-0454 Arkansas 855-710-0159 Connecticut 888-365-3233
Arkansas 855-538-0454 Connecticut 855-538-0454 Florida 855-538-0454 Georgia 800-424-5412 Illinois 800-504-2766 Kentucky 855-620-1861 Louisiana 855-538-0454 Arkansas 855-710-0159 Connecticut 888-365-3233
Refractory Status Epilepticus in Children: What are the Options?
 Refractory Status Epilepticus in Children: What are the Options? Weng Man Lam, PharmD, BCPS, BCPPS PICU Clinical Pharmacy Specialist Memorial Hermann Texas Medical Center November 11, 2017 Objectives 1.
Refractory Status Epilepticus in Children: What are the Options? Weng Man Lam, PharmD, BCPS, BCPPS PICU Clinical Pharmacy Specialist Memorial Hermann Texas Medical Center November 11, 2017 Objectives 1.
11/3/2017 A CONSENSUS PARAMETER FOR THE EVALUATION AND MANAGEMENT OF ANGIOEDEMA IN THE EMERGENCY DEPARTMENT ANGIOEDEMA ANGIOEDEMA TYPES OF ANGIOEDEMA
 A CONSENSUS PARAMETER FOR THE EVALUATION AND MANAGEMENT OF IN THE EMERGENCY DEPARTMENT PHILIP PAZDERKA, MD, FACEP is a physical sign secondary to swelling of the subcutaneous or submucosal tissues and
A CONSENSUS PARAMETER FOR THE EVALUATION AND MANAGEMENT OF IN THE EMERGENCY DEPARTMENT PHILIP PAZDERKA, MD, FACEP is a physical sign secondary to swelling of the subcutaneous or submucosal tissues and