Treatment of Addictive Disorders Alcohol and Opiates October 22, 2017
|
|
|
- Malcolm Harrington
- 5 years ago
- Views:
Transcription
1 Treatment of Addictive Disorders Alcohol and Opiates October 22, 2017 John A. Renner, Jr., MD Consultant, Department of Psychiatry Massachusetts General Hospital Professor of Psychiatry Boston University School of Medicine
2 Disclosures I have the following relevant financial relationship with a commercial interest to disclose: Johnson & Johnson: stockholder General Electric: stockholder
3 Agenda Alcohol Use Disorder Drinking Trends SBIRT & Screening for Alcohol Related Problems DSM-5 Alcohol Biomarkers Alcohol Withdrawal Medications Anticraving Medications Opiate Use Disorder Changes in Abuse Patterns Treating Opioid Overdose Opioid Withdrawal Protocols Opioid Agonist Therapy Opioid Antagonist Therapy Appendix Managing Dual Diagnosis Patients
4 Alcohol Use; Monitoring The Future,
5 Alcohol Use Disorders Epidemiology: Alcohol use accounts for 1 in 10 deaths in US adults age 20 to 64, approximately 88,000 deaths per year Drinkers lives are shortened by about 30 years Drinking costs US $224 billion a year due to lost productivity, including reduced wages and health care costs CDC
6 SBIRT & SCREENING FOR PROBLEM DRINKING Screening, Brief Intervention, Referral to Treatment (SBIRT): Single Alcohol Screening Question (SASQ) How many times in the past year have you had 5 or more drinks in one day? (4 drinks for women) Any positive response within the past year warrants assessment for problem drinking. Review drinking during the last 28 days. Review DSM-5 criteria. (Canagasby & Vinson, Alcohol Alcohol, May-June 2005) A large British study has questioned the effectiveness of screening and brief interventions in primary care settings E Kaner, et al. BMJ 2013;346:e8501
7 RECOMMENDATIONS FOR SCREENING The SBIRT approach is effective for individuals with heavy/at risk drinking There is little evidence of efficacy for individuals with an alcohol use disorder or a drug use disorder More intensive counseling or interventions are required for individuals with more serious problems None the less all patients should be screened to identify risky or problem drinking R.Saitz JAMA 2014;312(5):
8 DSM-5 CHANGES CRITERIA FOR SUBSTANCE USE DISORDERS 1. USE IN LARGER AMOUNTS / LONGER PERIODS THAN INTENDED 2. UNSUCCESSFUL EFFORTS TO CUT DOWN 3. EXCESSIVE TIME SPENT TAKING DRUG 4. FAILURE TO FULFILL MAJOR OBLIGATIONS 5. CONTINUED USE DESPITE KNOWLEDGE OF PROBLEMS 6. IMPORTANT ACTIVITIES GIVEN UP 7. RECURRENT USE IN PHYSICALLY HAZARDOUS SITUATIONS 8. CONTINUED USE DESPITE SOCIAL OR INTERPERSONAL PROBLEMS 9. TOLERANCE 10. WITHDRAWAL 11. CRAVING SEVERITY: 0 TO 1 CRITERIA: NO DIAGNOSIS 2 TO 3 CRITERIA: MILD 4 TO 5 CRITERIA: MODERATE 6 OR MORE CRITERIA: SEVERE
9 ALCOHOL BIOMAKERS INDIRECT TESTS all measure long-term drinking only 1. Carbohydrate-Deficient Transferrin (CDT): most sensitive indicator of relapse (serum) > 20 units/l in men > 26 units/l in women 2. GGT: > 65 units/l in men > 50 units/l in women 3. MCV> 95 microns/cubic ml. in males > 100 microns/cubic ml. in females 4. LFT s: AST, ALT, & Alk. Phos. 5. CAMP in WBC are 3 x normal
10 ALCOHOL BIOMARKERS DIRECT TESTS can detect recent relapse / drinking 1. Blood Alcohol Concentration (BAC) 2. Ethyl Glucuronide (EtG) is present for 5 days in urine, very sensitive and may have a high incidence of false positives. Use can be problematic in monitoring situations. 3. Phosphatidyl Ethanol (Peth): 2 drinks/day for 2 weeks (in RBCs) will track moderate drinking; is positive for 2-4 weeks
11 ALCOHOL SUBTYPES NESARC study, adapted from Moss H, Drug Alc Depend, 2007 YOUNG ADULTS 32% LATE ONSET 38% EARLY ONSET 30% EPISODIC HEAVY BINGE DRINKING MODERATE DRINKING SEVERE CHRONIC DRINKING LITTLE PSYCHO-PATHOLOGY MINIMAL PSYCHO-PATHOLOGY SEVERE PSYCHO-PATHOLOGY MINIMAL GENETIC RISK MODERATE GENETIC RISK SEVERE GENETIC RISK
12 NEUROBIOLOGY OF ALCOHOL: CHRONIC ALCOHOL USE UP-REGULATION OF NMDA RECEPTORS: EXCITATORY NEUROTRANSMISSION, PRIMARY CAUSE OF WITHDRAWAL SYMTPOMS DOWN-REGULATION OF INHIBITORY GABA RECEPTORS DOWN-REGULATION OF EXCITATORY DOPAMINE D-2 RECEPTORS INCREASED NOREPINEPHRINE ACTIVITY
13 NEUROBIOLOGY OF ALCOHOL EFFECTS OF ALCOHOL WITHDRAWAL: CNS HYPERACTIVITY- NO OPPOSITION TO ALCOHOL INDUCED EXCITATORY STATE (NMDA HYPERACTIVITY) RELEASE OF CRF PREDICTORS OF RELAPSE: DELAYED RECOVERY OF D-2 RECEPTOR SENSITIVITY AFTER DETOX ELEVATED ACTIVITY IN THE VENTROMEDIAL PREFRONTAL CORTEX (vmpfc) R. Sinha, JAMA Psychiatry 2013
14 MEDICATIONS FOR ALCOHOL WITHDRAWAL Benzodiazepines remain the standard of care Anticonvulsants (carbamazine & valproic acid) are effective but have significant side effects (Myrick, 2003) Gabapentin may offer an alternative option for ambulatory withdrawal treatment: 400 mg TID for 8-10 days Effective control of withdrawal As compared to lorazepam, less craving, anxiety & sedation Reduced probability of relapse in postwithdrawal week (Myrick, Alcohol Clin Exp Res, : ) Can present abuse problems in some patients
15 RELAPSE PREVENTION PHARMACOTHERAPY ANTICRAVING MEDICATIONS AS THE NEW STANDARD OF CARE Consider, immediately post-detoxification for ALL alcoholics Efficacy requires counseling and/or frequent physician monitoring; med compliance is critical for success
16 ADDICTION PHARMACOTHERAPY: MEDICATIONS IN THE LONG-TERM MANAGEMENT OF ALCOHOLISM DISULFIRAM * NALTREXONE (PO* & IM* formulations) ACAMPROSATE * TOPIRAMATE ONDANSETRON SSRIs CLOZAPINE QUETIAPINE * FDA APPROVED
17 NALTREXONE (ReVia) Opioid antagonist / oral formulation Modulates the mesolimbic dopamine system in the VTA & projections to the nucleus accumbens Reduces alcohol craving and euphoric effects of alcohol Dose: 50 to 100 MG QDaily with meals Side effects GI: abdominal pain, decreased appetite, nausea Sedation: daytime sleepiness, fatigue, insomnia, headache Works best with compliant patients(zweben, 2008); requires counseling (CBT) or frequent MD monitoring visits (Project Combine, 2006) Efficacy questioned in women (O Malley, 2007)
18 Naltrexone Outcome associated with variants of opioid receptor gene OPRM 1 Asp 40 Allel Asn 40 Allel NALTREXONE 87% GOOD OUTCOME 55% GOOD OUTCOME PLACEBO 49% GOOD OUTCOME 54% GOOD OUTCOME Project Combine; Anton R. Arch Gen Psychiatry In meta-analysis of 6 studies, patients carrying the G allele of A118G polymorphism of OPRM1 had lower relapse rates, but no difference in abstinence rates (Chamorro et al, 2012)
19 ER-NALTREXONE (Vivitrol) Long-acting injectible formulation: 80 mg IM q 28 days Screen LFTs More stable plasma concentrations compared to the oral formulation Side effects: NAUSEA & HEADACHE; more sedation than with the oral formulation Injection site reactions possible Best results in patients sober 1 week prior to starting the medication Efficacy shown in more severe alcoholics Reduction in heavy-drinking days (48.9% vs 30.9% on placebo) Pettinati HM, Alcohol Clin Exp Res, May 2011
20 RECOMMENDATIONS FOR USE OF NALTREXONE Screening tests for hepatic function Begin 50 mg ORAL Naltrexone after 4-5 days sobriety (post detox) If no response after 2 weeks, go to 100 mg If no response or minimal responses, add Gabapentin 12OO mg/day Anton R. Am J Psychiatry, July 2011 If no response, switch to ER-Naltrexone Pettinati HM. Alcohol Clin Exp Res, May 2011 If no response consider Acamprosate or Disulfiram
21 DISULFIRAM (Antabuse) DOSE: 500 mg po qd x 10 days; then 250 mg po qd SIDE EFFECTS: drowsiness, headache, metallic taste, decreased libido/potency SUPPORTIVE COUNSELING NECESSARY SUPERVISED DOSING recommended Follow serial LIVER FUNCTION TESTS Monitor for ALCOHOL-INDUCED HEPATITIS Rx for Antabuse reaction: BENADRYL 50 mg IM or IV Jergensen CH, Alcohol Clin Exp Res, Oct 2011
22 ACAMPROSATE (Campral) Glutamate antagonist Alters GABA & NMDA systems Restores balance between inhibitory & excitatory neurotransmission Attenuates acute & prolonged withdrawal Reduces rewarding effects of alcohol No tolerance, withdrawal or sedation Minimal side effects (mild diarrhea) Excreted through the kidneys No drug-drug interactions Dose: 666 mg PO TID
23 ACAMPROSATE (Campral) COCHRANE REVIEW, Rosner S, RCT s with 6915 subjects Reduced risk of relapse to 86% of the risk in the placebo group Increased by 3 the number of abstinent days per month NNTB = 9 Authors anticipate better results in fully compliant patients Post-treatment benefit (10 RCT s) effect sustained 3 to 12 mos. after end of treatment ACA vs. NTX (6 trials; inconclusive data) ACA plus NTX results promising but inconclusive 41% higher dropout rate than ACA alone
24 PROJECT COMBINE 1383 patients randomized to varying combinations of oral Naltrexone, Acamprosate, combined behavioral intervention (CBI) and medical management (MM) ALL groups improved Naltrexone + MM had the best outcome Adding CBI did not improve results Adding Acamprosate did not improve results One-year outcome: no significant differences among the groups JAMA. 2006;295:
25 TOPIRAMATE (Topamax) Facilitates GABA Inhibits Glutamate Reduced drinking and craving: DBPC trial (Johnson. Lancet. 2003) 150 subjects Dose: 25 mg PO QD, then increase dose up to 100 mg TID over an 8 week period Side effects: fatigue & cognitive dulling Replicated in 371 subjects DBPC randomized trial (Johnson. JAMA. 2007) Changed to pregnancy CATEGORY D in 2011
26 ONDANSETRON (Zofran) Anti-nausea drug approved 1991 Selective 5-HT 3 blocker Reduced drinking in EARLY-ONSET Alcoholism (Type B) Dose: 4 microgm/kg po bid equivalent dose not currently marketed DBPC 11-week trial; 321 patients Johnson BA. JAMA. Aug 23, 2000 Less expensive generic version available since 2008 Higher efficacy in individuals with the LL GENOTYPE of the 5-HTT gene Johnson BA. AM J PSYCHIATRY, Jan 2011
27 SSRIs May Reduce Drinking in Some Alcohol Subtypes CITALOPRAM: Reduced drinking in nondepressed male alcoholics; no efficacy in non-depressed female alcoholics (Naranjo, 2000) SERTRALINE: Reduced drinking in Late Onset men; no efficacy, or made drinking worse in Late Onset women or Early Onset men or women (Pettinati, 2004)
28 QUETIAPINE (Seroquel) Atypicals target both DA & 5-HT Systems Reduced substance use on clozapine 12-week DBPC trial in 61 subjects 11 of 61 achieved total abstinence: 9 were on quetiapine 2 were on placebo TYPE B/Early Onset marked quetiapine benefit TYPE A/Late Onset no difference from placebo Kampman & Pettinati. J Clin Psychopharmacology A large meta-analysis of 13 DB studies of antipsychotics failed to demonstrate efficacy for relapse prevention. Subjects were not categorized by subtypes. T. Kishi, J Clin Psych 2013
29 ALCOHOLISM PHARMACOTHERAPY SUGGESTIONS ALCOHOLISM SUBTYPE Binge Drinking Young Adults Early Onset; Severe Psychiatric Co-morbidity Late Onset; Moderate Late Onset; Severe Psychiatric Co-morbidity Elderly Onset INTERVENTION Education Motivational Enhancement Therapy Naltrexone - oral Ondansetron Topiramate; Atypical Antipsychotics? Naltrexone ER formulation Topiramate SSRIs in males Naltrexone ER formulation Topiramate Naltrexone ER formulation
30 Marijuana as a Medication for Alcoholism? Among other purported benefits of marijuana, it has been recommended as a substitute for alcohol in some alcohol-dependence individuals A review of the literature concluded that there is no clear pattern of outcomes related to marijuana substitution. Any clinical recommendations were thought to be premature. Subbaraman MS, Alcohol Alcohol 2014, 49(3): People using both marijuana and alcohol reported increased alcohol consumption and greater prescription drug misuse (Osilla et al, 2014)

31 Treatment Costs Alcohol Dependent Patients
32 Patient Management Techniques SOBRIETY is the primary goal Supportive care - BUILD DEFENSES MEDICATIONS for relapse; monitor compliance Treat co-morbid psychiatric disorders Learn to work with A.A. CBT & relapse prevention counseling Anticipate lapses & relapses Active therapeutic stance For persistent insomnia: TRAZODONE Avoid prescription tranquilizers

33 Substances for Which Most Recent Treatment Was Received in the Past Year among Persons Aged 12 or Older:
34 Heroin Use; Monitoring The Future,
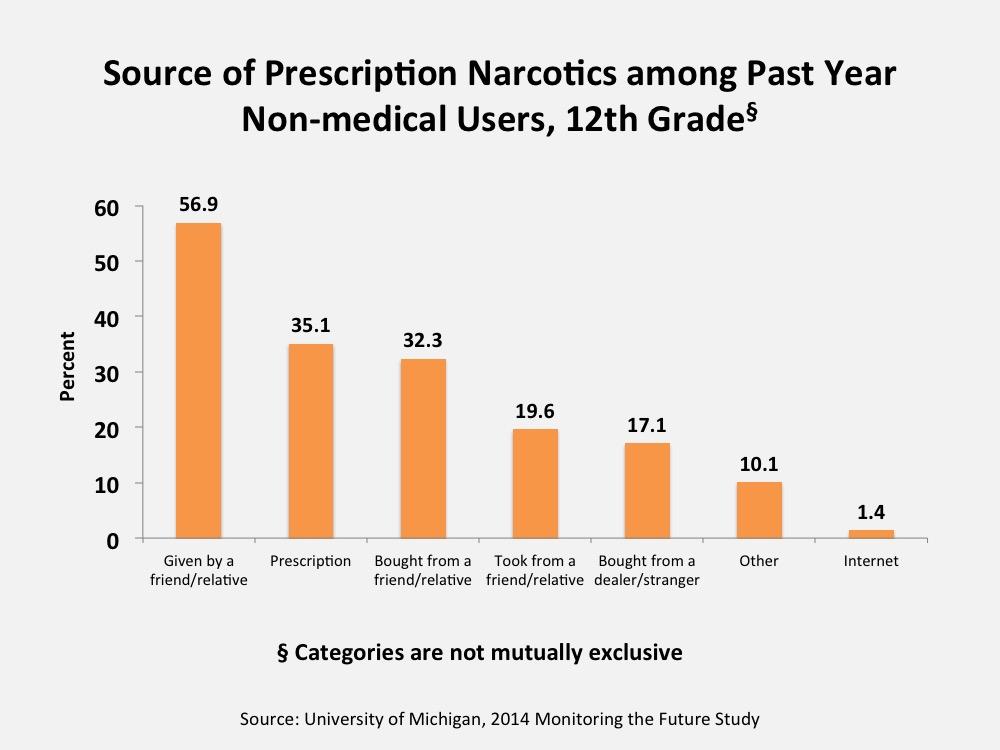
35 Narcotics use other than heroin, Monitoring the Future
36
37 National Survey of Drug Use and Health 2014, SAMHSA
38

39 CDC 3/18/17
40 National Survey of Drug Use and Health 2014, SAMHSA
41
42
43
44
45
46 The Treatment of Opioid Overdose Signs: Coma, pinpoint pupils, depressed pulse and respirations, hypothermia Treatment Naloxone (Narcan) 0.4 mg (1ml) iv, q.4 min., prn If no response, treat for sedative/hypnotic OD Monitor methadone overdose patients for hrs. Single naloxone dose lasts 1-4 hours Fentanyl may require multiple doses of naloxone to reverse Major public health initiative with Naloxone Rescue formulations; new standard of care
47 Heroin-related Deaths, San Francisco: begins, 2003 Introduction of intranasal naloxone *Data compiled from San Francisco Medical Examiner s Reports, **no data available for FY
48 Neurobiology of Opioid Withdrawal Hyperactivity of nor-adrenergic neurons in the locus coeruleus causes: Increased BP, HR, respirations Increased sweating, diarrhea Clonidine & opiates reverse these effects Increased GABA effects; reduced dopamine in the nucleus accumbens cause: Dysphoria, depression, craving Only opiates (methadone & buprenorphine) reverse these effects
49 Withdrawal Treatment - Methadone Initiate treatment only after documenting withdrawal Do not exceed initial dose of 20 mg methadone (10 mg in younger addicts) May repeat dose in 2 hrs., if withdrawal increases Inpatients rarely require over 40 mg / 24 hours Titrate dose to avoid intoxication or withdrawal Detox taper: cut by 10 mg / day down to 20 mg then cut by 5 mg / day down to zero Adding Very Low Dose Naltrexone (0.125 or mg q daily) may improve outcome and ease transition to postdetox care (Mannelli, Am J Addict 2009)
50 Inpatient Buprenorphine Withdrawal Rx Document withdrawal before giving 1 ST dose DAY 1: BUP/NALOXONE 4/1 mg SL, may redose in 2 to 4 hrs, up to 8/2 mg SL DAY 2: 8/2 to 12/3 mg SL DAY 3: 6/1.5 mg SL, final dose; may also taper 2-3 days 7 day protocol may be more effective Addicts prefer buprenorphine over methadone or clonidine Umbricht, 2003
51 Withdrawal Rx - Outcome Data Percent patients drug-free at 13 weeks, MEDICATION BUPRENORPHINE / NALOXONE INPATIENT DETOXIFICATION 77 % 29 % CLONIDINE 22 % 5 % OUTPATIENT DETOXIFICATION W. Ling, 2005
52 Opioid Agonist Therapy BUPRENORPHINE: High affinity partial MU-opioid agonist / ceiling effect for respiratory depression Low overdose risk Kappa receptor antagonist Sublingual buprenorphine/naloxone tablet New film strip formulation in 2010 Generic sublingual formulations 2013 Extended release subdermal rods 2016 Over 400,000 patients currently in active treatment Prescribing requires training & CSAT / DEA WAIVER waiver limit can be increased from 30 to 100 to 275
53 Opioid Agonist Therapy BUPRENORPHINE: DSM-5 criteria for addiction (Opioid Use Disorder Moderate) Can treat patients age 16 and older Rapid stabilization in 1-2 days Maintenance range: mg Long half-life: 24 to 72 hr dosing No evidence of hepatoxicity (Bogneschutz, 2010) Best option for younger, motivated patients with shorter addiction histories and less sociopathy Not recommended in severe chronic pain syndromes
54 Opioid Agonist Therapy BUPRENORPHINE OUTPATIENT INDUCTION RECOMMENDATIONS: Abstinence prior to first BUP/NX dose: 16 hrs for short-acting opioids (heroin) 24 hrs for sustained-release opioid medications 36 hrs for methadone (30mg x 2 weeks; 15mg x 1 day; no methadone x 1 day; then induce on BUP/NX) COWS score 8-10 before 1 st dose (2 or 4 mg) Rapid escalation to 16mg, if needed, by end of day 1 Gunderson EW, et al. Am J Addiction Sept, 2011
55 The Role of Counseling Standard recommendations since 1965 have stressed the importance of ancillary counseling for success in opioid agonist therapy Benefits are well documented by research Ball & Ross, 1991; McLellan,1993 Four recent buprenorphine trials suggest that brief, frequent physician medication monitoring visits are equal to, if not more effective than more intensive drug counseling Fiellin, 2006; Weiss, 2011
56 BUPRENORPHINE IN PREGNANCY The MOTHER Study: 175 pregnant opioid dependent women 8 international sites DB, double-dummy, flexible-dosing, randomized, controlled trial (methadone PO vs. buprenorphine SQ) Both drugs safe and effective Retention: 72% methadone vs. 67% buprenorphine* * Most BUP dropouts in first few days, or with first dose Comparison of 131 neonates (BUP vs. Methadone) Morphine dose required for NAS: 1.1 vs mg morphine Duration NAS: 4.1 vs. 9.9 days Duration hospital stay: 10.0 vs days Jones HE, et al. N Eng J Med, Dec 2010
57 Neonatal Abstinence Syndrome Jones et al, N Engl J Med,
58 Buprenorphine Recommendations for minimizing diversion & abuse: Use BUP/NX for all patients except pregnant women Whenever possible keep dose to 16/4 mgs or below After initial stabilization, wait at least 5-7 days to assess benefit of any dose increase Over 16/4 mg, emphasize psychosocial techniques to manage ongoing craving or use Weekly physician visits until stable Regular urine toxicology screens Regular check of state Prescription Drug Monitoring Program Call-backs for pill counts and tox screens, as needed Dose reductions to 8/2 mg for long-term patients Encourage AA / NA
59 Opiate Agonist Therapy Pain Management Opioid agonist maintained patients do experience pain and will have high tolerance to opioids Manage with non-opioids meds if possible For Methadone patients a full opioid agonist can be added as needed, or dispense methadone in divided doses For Buprenorphine patients add supplemental BUP dose or dispense in divided doses or add full agonists to daily buprenorphine dose switch to methadone or morphine For patients with chronic pain and addiction Buprenorphine/Naloxone in divided doses may be ideal for long term management
60 COMPARING METHADONE & BUPRENORPHINE / NX BUP/NX METHADONE Setting Office-based Clinic-based Diagnosis DSM-5 1 year proven history Age > 16 > 18 Target dose 12 to 16 mg 80 to 120 mg Safety (risk of OD) Ceiling effect No ceiling effect Cardiac risks None Over 100 mg, QTc risk Pregnancy Safe; less NAS Safe Efficacy Comparable in multiple studies Pain treatment Off-label FDA approved Diversion risk Higher Low from clinics
61 NEW PHARMACOTHERAPIES Lofexidine for opioid withdrawal treatment comparable to clonidine but fewer side effects and better efficacy. Has not yet been approved by FDA Probuphine - extended release subdermal buprenorphine implant rods. (R. Rosenthal, W. Ling, et al. Addiction 8/2013) FDA approved Patients must be stabilized 1 st on BUP/NX SL, 8mg/2mg or a lower dose Patients may require supplemental SL BUP/NX Improved medication compliance Option for stable long term patients; not appropriate for patients new to treatment or unstable patients Monthly injectable buprenorphine / NDA submitted
62 Opioid Antagonist Therapy ER-NALTREXONE (Vivitrol) Long-acting injectable formulation 380 mg IM every 28 days FDA approved for opioid use disorder in 2010 Questions: 24 week placebo controlled trial in Russia 250 patients in randomized control design FDA approval prior to publication Krupitsky E, Lancet, April, 2011 Many positive clinical reports, but no well designed studies comparing ER-NX to Methadone or to BUP/NX. NIDA trial of BUP/NX vs ER-NX is in final stages.
63 Opioid Antagonist Therapy ER-NALTREXONE (Vivitrol) Clinical Concerns Identification of appropriate patients Difficulty initiating treatment risk of precipitated opioid withdrawal; patients must be opioid free for 3 days from shortacting opiates; 7 days from long-acting opioids Risk for accidental overdoses and death: Opioid use at end of 1 month dosing interval Opioid use after missing monthly injection Attempts to overcome opioid blockade Contraindicated in acute hepatitis / liver failure Lack of long-term studies Managing need for acute analgesia has not been a problem; Naltrexone blockade can be over-ridden in inpatient settings

64 Treatment Costs Opiate Dependent Patients
65 Cost Containment Issues State efforts to limit funding for treatment of opioid use disorder Illinois has limited BUP/NX Medicare coverage to 1 year Ohio and other states have proposed dose limit of 16/4 mg BUP/NX Pending budget tsunami for new Hep C drugs: sofosbuvir (Solvaldi) from Gilead Sciences $1000 per pill or $84,000 to $100,000 for 12 week course of treatment ($ 2.27 Billion sales 1 st quarter 2014) 90% efficacy 3 million US infected; 50% in public sector (Veterans Administration, Medicare, prison population) primarily IV drug users States fear out of control costs Buprenorphine plus counseling reduced total health care costs compared to untreated individuals (Lynch FL, Addiction Science & Clinical Practice 2014, 9:16)
66 Questions?
67 Alcoholism: Rank of Co-morbid Conditions 1. Abuse of a second substance 2. Antisocial personality disorder 3. Phobias (& other anxiety disorders) 4. Major depressive disorder: 13% of women alcoholics 3% of male alcoholics 5. Dysthymic disorder NOTE: Co-Morbidity is the norm for most alcoholics seen in any clinical setting
68 Depression in Alcoholics 20% of SUD patients have a co-occurring mood or anxiety disorder (NESARC, 2004) Prolonged dysphoria & depression - rule out substance-induced depression For alcoholics with an independent major depressive disorder or dysthymic disorder. Review of randomized, DBPC trials, 1980 to 2009: Efficacy shown for tricyclics and nefazodone SSRI s data currently inadequate Iovieno N, et al. J Clin Psychiatry, August 2011
69 Failure to Respond to Antidepressant Meds Medication NON-COMPLIANCE Check for RELAPSE: CDT GGT Check plasma levels of TCAs Consider enforced therapy Consider adding NALTREXONE or ACAMPROSATE
70 Bipolar Disorder and Co-Occurring Alcoholism Drinking typically follows onset of mania Patients rarely relapse when depressed or euthymic Alcoholism often remits after moods are stabilized Medication SUGGESTIONS (no adequate DBPC trials): BIPOLAR I LITHIUM BIPOLAR II VALPROIC ACID ATYPICAL ANTISPYCHOTICS
71 Anxiety Disorders in Alcoholics DIAGNOSIS: Wait 4 to 6 weeks for withdrawal symptoms to clear Positive family history +/- Symptoms antedate alcohol use TREATMENT RECOMMENDATIONS: Generalized anxiety dis.: BUSPIRONE Panic disorder: ANTIDEPRESSANTS BEHAVIORAL THERAPY Agoraphobia: ANTIDEPRESSANTS BEHAVIORAL THERAPY Social phobia: PROPRANOLOL or CLONIDINE
72 Treating ADHD in at Risk Patients 20% to 25% incidence of ADHD with any psychoactive substance use disorder TREATMENT PROTOCOL Adults with SUD & co-occurring ADHD: CBT X 2 weeks without medication Then start meds if symptoms persist medication choices ranked by risk potential Atomoxetine (Stratera) has no abuse potential Bupropion Desipramine Extended Release Stimulants: Methylphenidate ER generic (Concerta) or Adderal XR (amphetamine/dextroamphetamine mixed salts) T. Wilens, 2012
73 Anxiety Disorders in Addicts The Role of Benzodiazepines: Comprehensive literature review Efficacy demonstrated for: GAD, panic disorder and agoraphobia Probable efficacy for: Social phobia, alcohol induced anxiety disorders Little evidence of added risk for medication abuse or increased relapse Posternak & Mueller. Am J Addict. 2001;10:48-68.




74 Naloxone Rescue Formulations
Treatment of Addictive Disorders Alcohol and Opiates October 23, 2016
 Treatment of Addictive Disorders Alcohol and Opiates October 23, 2016 John A. Renner, Jr., MD Consultant, Department of Psychiatry Massachusetts General Hospital Professor of Psychiatry Boston University
Treatment of Addictive Disorders Alcohol and Opiates October 23, 2016 John A. Renner, Jr., MD Consultant, Department of Psychiatry Massachusetts General Hospital Professor of Psychiatry Boston University
Dr. Renner receives honoraria from Reed Medical Education
 Substance Use Disorders Symposium on Men s Health Massachusetts Medical Society June 17, 2010 John A. Renner, Jr., M.D. John A. Renner Jr., MD DISCLOSURES Johnson & Johnson Stock Holder Dr. Renner receives
Substance Use Disorders Symposium on Men s Health Massachusetts Medical Society June 17, 2010 John A. Renner, Jr., M.D. John A. Renner Jr., MD DISCLOSURES Johnson & Johnson Stock Holder Dr. Renner receives
Treatment Alternatives for Substance Use Disorders
 Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
Treatment Alternatives for Substance Use Disorders Dean Drosnes, MD, FASAM Associate Medical Director Director, Chronic Pain and SUD Program Caron Treatment Centers 1 Disclosure The speaker has no conflict
6/6/2018. Objectives. Outline. Rethinking Medication Treatment for Opioid Use Disorder
 Rethinking Medication Treatment for Opioid Use Disorder International Conference on Opioids June 10, 2018 Dustin Patil, MD Fellow, Addiction Psychiatry Boston Medical Center John Renner, MD Professor of
Rethinking Medication Treatment for Opioid Use Disorder International Conference on Opioids June 10, 2018 Dustin Patil, MD Fellow, Addiction Psychiatry Boston Medical Center John Renner, MD Professor of
Buprenorphine as a Treatment Option for Opioid Use Disorder
 Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Buprenorphine as a Treatment Option for Opioid Use Disorder Joji Suzuki, MD Assistant Professor of Psychiatry Harvard Medical School Director, Division of Addiction Psychiatry Brigham and Women s Hospital
Medication Assisted Treatment. Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs
 Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
Medication Assisted Treatment Karen Drexler, MD National Mental Health Program Director-Substance Use Disorders Department of Veterans Affairs Disclosures Employed by the Department of Veterans Affairs
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2009 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
8/5/2013. MOSBIRT Annual Training The Big change in addiction medicine? Before we dive into pharmacotherapy
 Medication Assisted Treatment for Substance Abuse in Primary Care Dan Vinson August 1, 2013 1 The Big change in addiction medicine? These diseases are rapidly becoming medical diseases. Done are the days
Medication Assisted Treatment for Substance Abuse in Primary Care Dan Vinson August 1, 2013 1 The Big change in addiction medicine? These diseases are rapidly becoming medical diseases. Done are the days
Arwen Podesta, MD. ABIHM, ABAM, Forensic Psychiatry
 The State of Medicine in Addiction Recovery Arwen Podesta, MD ABIHM, ABAM, Forensic Psychiatry www.podestawellness.com 504-252-0026 http://www.addictionpolicy.org/ Overview Addiction is a serious, chronic
The State of Medicine in Addiction Recovery Arwen Podesta, MD ABIHM, ABAM, Forensic Psychiatry www.podestawellness.com 504-252-0026 http://www.addictionpolicy.org/ Overview Addiction is a serious, chronic
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center
 Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Kurt Haspert, MS, CRNP University of Maryland Baltimore Washington Medical Center Data from the National Vital Statistics System Mortality The age-adjusted rate of drug overdose deaths in the United States
Opioids. October 29, Addiction Medicine Review Course CSAM, Newport Beach, CA
 Opioids October 29, 2010 Addiction Medicine Review Course CSAM, Newport Beach, CA Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Boston University School of Medicine Boston Medical
Opioids October 29, 2010 Addiction Medicine Review Course CSAM, Newport Beach, CA Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Boston University School of Medicine Boston Medical
Medical Assisted Treatment. Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center
 Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Medical Assisted Treatment Dr. Michael Baldinger Medical Director Haymarket Center Harborview Recovery Center Current Trends Prescription Drug Abuse/Addiction Non-medical use of prescription pain killers
Addiction Medicine: What s new for primary care
 Addiction Medicine: What s new for primary care Dan Vinson, MD Family and Community Medicine How to talk so our patients listen, and listen so our patients talk. 1 2 Comfortably engaging your patient in
Addiction Medicine: What s new for primary care Dan Vinson, MD Family and Community Medicine How to talk so our patients listen, and listen so our patients talk. 1 2 Comfortably engaging your patient in
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2008 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2008 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice
 Opioids Research to Practice May 2013 Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Assistant Dean, Continuing Medical Education Case 32 yo female brought in after heroin overdose
Opioids Research to Practice May 2013 Daniel P. Alford, MD, MPH, FACP, FASAM Associate Professor of Medicine Assistant Dean, Continuing Medical Education Case 32 yo female brought in after heroin overdose
THE STATE OF MEDICINE IN ADDICTION RECOVERY
 OVERVIEW: Review addiction stats and trends Define addiction Explain neurobiology of addiction Review treatments of addiction Addiction Definition: A Primary, chronic, relapsing disease of brain reward,
OVERVIEW: Review addiction stats and trends Define addiction Explain neurobiology of addiction Review treatments of addiction Addiction Definition: A Primary, chronic, relapsing disease of brain reward,
Opioids Research to Practice
 Opioids Research to Practice CRIT/FIT 2016 April 2016 Daniel P. Alford, MD, MPH Associate Professor of Medicine Assistant Dean, Continuing Medical Education Director, Clinical Addiction Research and Education
Opioids Research to Practice CRIT/FIT 2016 April 2016 Daniel P. Alford, MD, MPH Associate Professor of Medicine Assistant Dean, Continuing Medical Education Director, Clinical Addiction Research and Education
Medication-Assisted Treatment. What Is It and Why Do We Use It?
 Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Medication-Assisted Treatment What Is It and Why Do We Use It? What is addiction, really? o The four C s of addiction: Craving. Loss of Control of amount or frequency of use. Compulsion to use. Use despite
Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents
 Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents Myth or Reality? Complete Recovery means a medication-free state True or False? Treatment of Alcoholism Assessment Motivation Alcohol
Long term pharmacotherapy for Alcohol Dependence: Anti Craving agents Myth or Reality? Complete Recovery means a medication-free state True or False? Treatment of Alcoholism Assessment Motivation Alcohol
Substitution Therapy for Opioid Use Disorder The Role of Suboxone
 Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Substitution Therapy for Opioid Use Disorder The Role of Suboxone Methadone/Buprenorphine 101 Workshop, December 10, 2016 Leslie Lappalainen, MD, CCFP, dip ABAM Prepared by Mandy Manak, MD, ABAM, CCSAM
Opioid Use in Youth. Amy Yule M.D. March 2,
 Opioid Use in Youth Amy Yule M.D. March 2, 2018 An opioid is a substance that acts on opioid receptors Beta-endorphin Endogenous opioids Dynorphin Opiates Natural products of the poppy plant Morphine Heroin
Opioid Use in Youth Amy Yule M.D. March 2, 2018 An opioid is a substance that acts on opioid receptors Beta-endorphin Endogenous opioids Dynorphin Opiates Natural products of the poppy plant Morphine Heroin
Pharmacotherapy of Alcohol Use Disorders
 Pharmacotherapy of Alcohol Use Disorders Roger D. Weiss, MD Professor of Psychiatry, Harvard Medical School Chief, Division of Alcohol and Drug Abuse McLean Hospital rweiss@mclean.harvard.edu Consultant
Pharmacotherapy of Alcohol Use Disorders Roger D. Weiss, MD Professor of Psychiatry, Harvard Medical School Chief, Division of Alcohol and Drug Abuse McLean Hospital rweiss@mclean.harvard.edu Consultant
Overview of Medication Assisted Treatment Methadone, Buprenorphine and Naltrexone
 Overview of Medication Assisted Treatment Methadone, Buprenorphine and Naltrexone Alexander Y. Walley, MD, MSc Associate Professor of Medicine Director, Addiction Medicine Fellowship Boston University
Overview of Medication Assisted Treatment Methadone, Buprenorphine and Naltrexone Alexander Y. Walley, MD, MSc Associate Professor of Medicine Director, Addiction Medicine Fellowship Boston University
Main Questions. Why study addiction? Substance Use Disorders, Part 1 Alecia Schweinsburg, MA Abnromal Psychology, Fall Substance Use Disorders
 Substance Use Disorders Main Questions Why study addiction? What is addiction? Why do people become addicted? What do alcohol and drugs do? How do we treat substance use disorders? Why study addiction?
Substance Use Disorders Main Questions Why study addiction? What is addiction? Why do people become addicted? What do alcohol and drugs do? How do we treat substance use disorders? Why study addiction?
Identification and Treatment of Opioid Use Disorders in Primary Care Settings
 Identification and Treatment of Opioid Use Disorders in Primary Care Settings 17th Annual Primary Care Symposium February 24, 2018 Kelly S. Barth, DO Associate Professor, Psychiatry & Internal Medicine
Identification and Treatment of Opioid Use Disorders in Primary Care Settings 17th Annual Primary Care Symposium February 24, 2018 Kelly S. Barth, DO Associate Professor, Psychiatry & Internal Medicine
Medication-Assisted Treatment (MAT) Overview
 Overview") Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
Medication-Assisted Treatment (MAT) Overview 2014 Opiate Conference: Don t Get Me Started Hyatt Regency, Columbus, Ohio June 30-July 1, 2014 Christina M. Delos Reyes, MD Medical Consultant, Center for
LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE
 LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE DR. SHILPA ADARKAR ASSOCIATE PROFESSOR DEPARTMENT OF PSYCHIATRY & DRUG DEADDICTION CENTRE OF EXCELLENCE SETH GSMC & KEMH LONG TERM OPTIONS FULL AGONIST PARTIAL
LONG TERM PHARMACOTHERAPY OF OPIOID DEPENDENCE DR. SHILPA ADARKAR ASSOCIATE PROFESSOR DEPARTMENT OF PSYCHIATRY & DRUG DEADDICTION CENTRE OF EXCELLENCE SETH GSMC & KEMH LONG TERM OPTIONS FULL AGONIST PARTIAL
Prescription Opioid Addiction
 CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
CSAM-SCAM Fundamentals Prescription Opioid Addiction Presentation provided by Meldon Kahan, MD Family & Community Medicine University of Toronto Conflict of interest statement I received funds from Rickett
Serious Mental Illness and Opioid Use Disorder
 Serious Mental Illness and Opioid Use Disorder Serious Mental Illness and Opioid Use Disorders Arthur Robin Williams, MD MBE Columbia University, Department of Psychiatry Nick Szubiak, MSW, LCSW Director,
Serious Mental Illness and Opioid Use Disorder Serious Mental Illness and Opioid Use Disorders Arthur Robin Williams, MD MBE Columbia University, Department of Psychiatry Nick Szubiak, MSW, LCSW Director,
Pharmacotherapy for Substance Use Disorders
 Pharmacotherapy for Substance Use Disorders Vanessa de la Cruz, MD Chief of Psychiatry Mental Health and Substance Abuse Services Santa Cruz County Health Services Agency 1400 Emeline Avenue Santa Cruz,
Pharmacotherapy for Substance Use Disorders Vanessa de la Cruz, MD Chief of Psychiatry Mental Health and Substance Abuse Services Santa Cruz County Health Services Agency 1400 Emeline Avenue Santa Cruz,
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Opiate Use Disorder and Opiate Overdose
 Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Opiate Use Disorder and Opiate Overdose Irene Ortiz, MD Medical Director Molina Healthcare of New Mexico and South Carolina Clinical Professor University of New Mexico School of Medicine Objectives DSM-5
Understanding and Combating the Heroin Epidemic
 Understanding and Combating the Heroin Epidemic Kelly Dunn, Ph.D. Assistant Professor; Johns Hopkins School of Medicine Department of Psychiatry and Behavioral Sciences 1 Talk Outline What is causing the
Understanding and Combating the Heroin Epidemic Kelly Dunn, Ph.D. Assistant Professor; Johns Hopkins School of Medicine Department of Psychiatry and Behavioral Sciences 1 Talk Outline What is causing the
ALCOHOL USE DISORDER WITHDRAWAL MANAGEMENT AND LONG TERM TREATMENT ANA HOLTEY, MD ADDICTION MEDICINE FELLOW UNIVERSITY OF UTAH HEALTH
 ALCOHOL USE DISORDER WITHDRAWAL MANAGEMENT AND LONG TERM TREATMENT ANA HOLTEY, MD ADDICTION MEDICINE FELLOW UNIVERSITY OF UTAH HEALTH Prevalence of 12-Month Alcohol Use, High-Risk Drinking, and DSM-IV
ALCOHOL USE DISORDER WITHDRAWAL MANAGEMENT AND LONG TERM TREATMENT ANA HOLTEY, MD ADDICTION MEDICINE FELLOW UNIVERSITY OF UTAH HEALTH Prevalence of 12-Month Alcohol Use, High-Risk Drinking, and DSM-IV
Opioids Research to Practice
 Opioids Research to Practice CRIT Program May 2010 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
Opioids Research to Practice CRIT Program May 2010 Daniel P. Alford, MD, MPH Associate Professor of Medicine Boston University School of Medicine Boston Medical Center 32 yo female brought in after heroin
DRUGS USED IN THE TREATMENT OF ADDICTION JOSEPH A. TRONCALE, MD FASAM RETREAT PREMIERE ADDICTION TREATMENT CENTERS
 DRUGS USED IN THE TREATMENT OF ADDICTION JOSEPH A. TRONCALE, MD FASAM RETREAT PREMIERE ADDICTION TREATMENT CENTERS MAJOR CATEGORIES OF TREATMENTS Detoxification and Post-Acute Withdrawal Maintenance Co-Occurring
DRUGS USED IN THE TREATMENT OF ADDICTION JOSEPH A. TRONCALE, MD FASAM RETREAT PREMIERE ADDICTION TREATMENT CENTERS MAJOR CATEGORIES OF TREATMENTS Detoxification and Post-Acute Withdrawal Maintenance Co-Occurring
Health Systems and Addiction: Provider Issues
 Health Systems and Addiction: Provider Issues The Emerging Roles of Primary Care Patrick G. O Connor MD, MPH Dan and Amanda Adams Professor of General Medicine Chief, General Internal Medicine Yale University
Health Systems and Addiction: Provider Issues The Emerging Roles of Primary Care Patrick G. O Connor MD, MPH Dan and Amanda Adams Professor of General Medicine Chief, General Internal Medicine Yale University
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT
 and acute pain management on MAT") An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
An overview of Medication Assisted Treatment (MAT) and acute pain management on MAT Goals of Discussion Recognize opioid use disorder (OUD) Discuss the pharmacology of medication assisted treatments (MAT)
Pharmacotherapy for Alcohol Use Disorder
 Pharmacotherapy for Alcohol Use Disorder Laura G. Kehoe, MD, MPH Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither my
Pharmacotherapy for Alcohol Use Disorder Laura G. Kehoe, MD, MPH Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither my
Screening, Diagnosis, and Medication Assisted Treatment for Alcohol Use Disorders
 Psychiatry and Addictions Case Conference Screening, Diagnosis, and Medication Assisted Treatment for Alcohol Use Disorders MARK DUNCAN, MD Acting Assistant Professor, Co-lead University of Washington
Psychiatry and Addictions Case Conference Screening, Diagnosis, and Medication Assisted Treatment for Alcohol Use Disorders MARK DUNCAN, MD Acting Assistant Professor, Co-lead University of Washington
Dr. Oslin receives grant support from the NIH, VA, and the Pennsylvania Department of Aging.
 David W. Oslin, MD University of Pennsylvania Philadelphia VAMC Dr. Oslin receives grant support from the NIH, VA, and the Pennsylvania Department of Aging. Dr. Oslin is a consultant to the Hazelden Betty
David W. Oslin, MD University of Pennsylvania Philadelphia VAMC Dr. Oslin receives grant support from the NIH, VA, and the Pennsylvania Department of Aging. Dr. Oslin is a consultant to the Hazelden Betty
Extended-Release Naltrexone for Opioid Relapse Prevention
 Extended-Release Naltrexone for Opioid Relapse Prevention 1.NYU SOM; Bellevue Hospital Center 2.Brown Univ. 3. Friends Research Institute 4. Columbia Univ. 5. Univ. Pennsylvania 6. Univ. Virginia Funding:
Extended-Release Naltrexone for Opioid Relapse Prevention 1.NYU SOM; Bellevue Hospital Center 2.Brown Univ. 3. Friends Research Institute 4. Columbia Univ. 5. Univ. Pennsylvania 6. Univ. Virginia Funding:
Restoration of Parenting Ability Through Treatment for Substance Use Disorders
 Restoration of Parenting Ability Through Treatment for Substance Use Disorders DEBRA M. BARNETT, MD Board Certified in General Psychiatry, Addiction Psychiatry, Geriatric Psychiatry, and Forensic Psychiatry
Restoration of Parenting Ability Through Treatment for Substance Use Disorders DEBRA M. BARNETT, MD Board Certified in General Psychiatry, Addiction Psychiatry, Geriatric Psychiatry, and Forensic Psychiatry
(Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines)
") Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Buprenorphine Initiation and Maintenance in Pregnancy (Adapted with permission from the D-H Knowledge Map Primary Care Buprenorphine Guidelines) Assessment The diagnosis of OUD should be confirmed by DSM-5
Opioid dependence and buprenorphine treatment
 Opioid dependence and buprenorphine treatment David Roll, MD Revere Family Health, Cambridge Health Alliance Instructor in Medicine, Harvard Medical School Joji Suzuki MD Medical Director of Addictions
Opioid dependence and buprenorphine treatment David Roll, MD Revere Family Health, Cambridge Health Alliance Instructor in Medicine, Harvard Medical School Joji Suzuki MD Medical Director of Addictions
Medical Assisted Treatment of Opioid
 Medical Assisted Treatment of Opioid Dependence with XR-NTX(Vivitrol) Michael McNamara DO, FACN Medical Director Mental Health Center of Greater Manchester Manchester NH Outline Overview of Opioid Dependence
Medical Assisted Treatment of Opioid Dependence with XR-NTX(Vivitrol) Michael McNamara DO, FACN Medical Director Mental Health Center of Greater Manchester Manchester NH Outline Overview of Opioid Dependence
Medical Management of Substance Use Disorders: Does research translate to clinical practice
 Medical Management of Substance Use Disorders: Does research translate to clinical practice Ashwin A Patkar, MD Professor of Psychiatry & Community & Family Medicine Duke University Medical Center Durham,
Medical Management of Substance Use Disorders: Does research translate to clinical practice Ashwin A Patkar, MD Professor of Psychiatry & Community & Family Medicine Duke University Medical Center Durham,
2/19/18. Today s talk. Today s talk. The Role of Behavioral Interventions in Buprenorphine Treatment of Opioid Use Disorders
 The Role of Behavioral Interventions in Buprenorphine Treatment of Opioid Use Disorders Roger D. Weiss, MD Chief, Division of Alcohol and Drug Abuse, McLean Hospital, Belmont, MA Professor of Psychiatry,
The Role of Behavioral Interventions in Buprenorphine Treatment of Opioid Use Disorders Roger D. Weiss, MD Chief, Division of Alcohol and Drug Abuse, McLean Hospital, Belmont, MA Professor of Psychiatry,
SW OREGON OPIOID SUMMIT. Medication Assisted Recovery for Opioid Use Disorder. Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass
 SW OREGON OPIOID SUMMIT Medication Assisted Recovery for Opioid Use Disorder Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass Opioid Agonists Mu (μ) receptors stimulated by opioids causing full
SW OREGON OPIOID SUMMIT Medication Assisted Recovery for Opioid Use Disorder Gregory S. Brigham, Ph.D. Adapt / SouthRiver CHC / Compass Opioid Agonists Mu (μ) receptors stimulated by opioids causing full
GUIDELINES FOR THE USE OF PSYCHOACTIVE MEDICATIONS IN INDIVIDUALS WITH CO-OCCURRING SUBSTANCE USE DISORDERS
 City and County of San Francisco Mayor Gavin Newsom Department of Public Health Community Behavioral Health Services 1380 Howard Street 5 th Floor San Francisco, CA 94103 GUIDELINES FOR THE USE OF PSYCHOACTIVE
City and County of San Francisco Mayor Gavin Newsom Department of Public Health Community Behavioral Health Services 1380 Howard Street 5 th Floor San Francisco, CA 94103 GUIDELINES FOR THE USE OF PSYCHOACTIVE
Buprenorphine for Family Medicine. Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17
 + Buprenorphine for Family Medicine Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17 + Disclosures No conflicts of interest Off-label use of medications + Who here: Has taken care of a patient
+ Buprenorphine for Family Medicine Hannah Snyder, MD Addiction Medicine Fellow, UCSF 12/7/17 + Disclosures No conflicts of interest Off-label use of medications + Who here: Has taken care of a patient
The future of pharmacological treatment.
 The future of pharmacological treatment. Anne Lingford-Hughes Professor of Addiction Biology, Imperial College. Hon Consultant CNWL NHS Foundation Trust. What substances and when? What Nicotine Alcohol
The future of pharmacological treatment. Anne Lingford-Hughes Professor of Addiction Biology, Imperial College. Hon Consultant CNWL NHS Foundation Trust. What substances and when? What Nicotine Alcohol
Medication for Addiction Treatment (MAT)
") SBIRT Training Screening, Brief Intervention & Referral to Treatment Medication for Addiction Treatment (MAT) The Faith & Spirituality Integrated SBIRT Network Navigating the Training Welcome! These health
SBIRT Training Screening, Brief Intervention & Referral to Treatment Medication for Addiction Treatment (MAT) The Faith & Spirituality Integrated SBIRT Network Navigating the Training Welcome! These health
Methadone and Naltrexone ER
 Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither I nor my
Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither I nor my
Prepared by: Dr. Elizabeth Woodward, University of Toronto Resident in Psychiatry
 Prepared by: Dr. Elizabeth Woodward, University of Toronto Resident in Psychiatry In broad terms, substance use disorders occur when a substance is used in a compulsive manner with a lack of control over
Prepared by: Dr. Elizabeth Woodward, University of Toronto Resident in Psychiatry In broad terms, substance use disorders occur when a substance is used in a compulsive manner with a lack of control over
Management of high risk MMT patients. Meldon Kahan MD Methadone Prescribers Conference Toronto, Nov 15, 2013
 Management of high risk MMT patients Meldon Kahan MD Methadone Prescribers Conference Toronto, Nov 15, 2013 CFPC CoI Templates: Slide 1 Faculty Disclosure Faculty: Meldon Kahan Relationships with commercial
Management of high risk MMT patients Meldon Kahan MD Methadone Prescribers Conference Toronto, Nov 15, 2013 CFPC CoI Templates: Slide 1 Faculty Disclosure Faculty: Meldon Kahan Relationships with commercial
Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates
 and Medication Assisted Treatment (MAT) for Opiates") Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates What is MAT? Medication Assisted Treatment (MAT) is the use of medications, in addition to counseling, cognitive behavioral
Substance Use Disorders (SUDs) and Medication Assisted Treatment (MAT) for Opiates What is MAT? Medication Assisted Treatment (MAT) is the use of medications, in addition to counseling, cognitive behavioral
MAT in the Corrections Setting
 MEDICATION ASSISTED TREATMENT AND CORRECTIONS Frank Filippelli, DO, PhD September 2017 MAT in the Corrections Setting Who Does This Affect? What is MAT and What is the Evidence of Efficacy? Emphasis on
MEDICATION ASSISTED TREATMENT AND CORRECTIONS Frank Filippelli, DO, PhD September 2017 MAT in the Corrections Setting Who Does This Affect? What is MAT and What is the Evidence of Efficacy? Emphasis on
Overview of Opioid Use Disorder
 Overview of Opioid Use Disorder Doug Burgess, MD Medical Director of Outpatient Services, Truman Medical Centers Assistant Professor of Psychiatry, University of Missouri- Kansas City Objectives History
Overview of Opioid Use Disorder Doug Burgess, MD Medical Director of Outpatient Services, Truman Medical Centers Assistant Professor of Psychiatry, University of Missouri- Kansas City Objectives History
The role of behavioral interventions in buprenorphine treatment of opioid use disorders
 The role of behavioral interventions in buprenorphine treatment of opioid use disorders Roger D. Weiss, MD Harvard Medical School, Boston, MA, McLean Hospital, Belmont, MA, USA Today s talk Review of studies
The role of behavioral interventions in buprenorphine treatment of opioid use disorders Roger D. Weiss, MD Harvard Medical School, Boston, MA, McLean Hospital, Belmont, MA, USA Today s talk Review of studies
Medications For Alcohol Use Disorder. DATE: October 10, 2017 PRESENTED BY: Alann Weissman-Ward, MD, Addiction Medicine fellow
 Medications For Alcohol Use Disorder DATE: October 10, 2017 PRESENTED BY: Alann Weissman-Ward, MD, Addiction Medicine fellow None DISCLOSURES OBJECTIVES Be able to name 4 medications to treat AUD Describe
Medications For Alcohol Use Disorder DATE: October 10, 2017 PRESENTED BY: Alann Weissman-Ward, MD, Addiction Medicine fellow None DISCLOSURES OBJECTIVES Be able to name 4 medications to treat AUD Describe
Medication Assisted Treatment:
 Medication Assisted Treatment: A Training For Multidisciplinary Addiction Professionals Module III Medications 101 Goals for Module III This module reviews the following: Overview of three medications
Medication Assisted Treatment: A Training For Multidisciplinary Addiction Professionals Module III Medications 101 Goals for Module III This module reviews the following: Overview of three medications
Thaddeus Ulzen MD FRCP(C)FAPA FCGP Professor & Chair, Department of Psychiatry and Behavioral Medicine, Associate Dean for Academic Affairs
FAPA FCGP Professor & Chair, Department of Psychiatry and Behavioral Medicine, Associate Dean for Academic Affairs") Thaddeus Ulzen MD FRCP(C)FAPA FCGP Professor & Chair, Department of Psychiatry and Behavioral Medicine, Associate Dean for Academic Affairs CCHS/University of Alabama School of Medicine Assessment History
Thaddeus Ulzen MD FRCP(C)FAPA FCGP Professor & Chair, Department of Psychiatry and Behavioral Medicine, Associate Dean for Academic Affairs CCHS/University of Alabama School of Medicine Assessment History
NALTREXONE DAVID CRABTREE, MD, MPH UNIVERSITY OF UTAH HEALTH, 2018
 NALTREXONE DAVID CRABTREE, MD, MPH TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications
NALTREXONE DAVID CRABTREE, MD, MPH TREATMENT OF OPIOID USE DISORDER (OUD) Majority of people who develop OUD are not receiving treatment Only a small fraction of patients are offered treatment with medications
The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines
 The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines Background, Objectives and Methods Systematic reviews (SRs) published by Cochrane Drugs
The available evidence in the field of treatment of opiate: The experience of developing the WHO clinical guidelines Background, Objectives and Methods Systematic reviews (SRs) published by Cochrane Drugs
MEDICATION ASSISTED TREATMENTS (MAT) FOR SUBSTANCE USE DISORDERS
 FOR SUBSTANCE USE DISORDERS") MEDICATION ASSISTED TREATMENTS (MAT) FOR SUBSTANCE USE DISORDERS PHYLLIS RAYNOR, PHD, PMHNP-BC, APRN CLINICAL ASSISTANT PROFESSOR, USC COLLEGE OF NURSING LEARNING OBJECTIVES: Define types of SUD and purposes
MEDICATION ASSISTED TREATMENTS (MAT) FOR SUBSTANCE USE DISORDERS PHYLLIS RAYNOR, PHD, PMHNP-BC, APRN CLINICAL ASSISTANT PROFESSOR, USC COLLEGE OF NURSING LEARNING OBJECTIVES: Define types of SUD and purposes
GOALS AND OBJECTIVES
 SUBOXONE AND VIVITROL: ARE THERE DISPARITIES SURFACING IN MEDICATION ASSISTED TREATMENTS? P R E S E N T E D B Y D R. K I AM E M AH A N I A H & D R. M Y E C H I A M I N T E R - J O R D AN GOALS AND OBJECTIVES
SUBOXONE AND VIVITROL: ARE THERE DISPARITIES SURFACING IN MEDICATION ASSISTED TREATMENTS? P R E S E N T E D B Y D R. K I AM E M AH A N I A H & D R. M Y E C H I A M I N T E R - J O R D AN GOALS AND OBJECTIVES
9/13/2017. Buprenorphine Treatment (Suboxone) Disclosures. We ve Got a Big Opioid Problem. Selahattin Kurter, MD Spectrum Healthcare
 Disclosures. We ve Got a Big Opioid Problem. Selahattin Kurter, MD Spectrum Healthcare") Buprenorphine Treatment (Suboxone) Selahattin Kurter, MD Spectrum Healthcare Board Certified in Psychiatry and Addiction Medicine Disclosures No financial reimbursement for this lecture Consultant for
Buprenorphine Treatment (Suboxone) Selahattin Kurter, MD Spectrum Healthcare Board Certified in Psychiatry and Addiction Medicine Disclosures No financial reimbursement for this lecture Consultant for
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction
 Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction Multiple Choice Identify the choice that best completes the statement or answers the question. 1. Executive Summary
Management of Opioid Use Disorder in Primary Care
 1 Northwest ATTC presents Management of Opioid Use Disorder in Primary Care Joseph O. Merrill, MD, MPH University of Washington Associate Professor of Medicine 4/26/2018 Today s Presenter 2 Joseph Merrill,
1 Northwest ATTC presents Management of Opioid Use Disorder in Primary Care Joseph O. Merrill, MD, MPH University of Washington Associate Professor of Medicine 4/26/2018 Today s Presenter 2 Joseph Merrill,
Medications For Alcohol Use Disorder
 Medications For Alcohol Use Disorder PRESENTED BY: Alann Weissman-Ward, MD, Addiction Medicine fellow June 19, 2018 DISCLOSURES Speaker: Alann Weissman-Ward, MD, has nothing to disclose. Planning Committee:
Medications For Alcohol Use Disorder PRESENTED BY: Alann Weissman-Ward, MD, Addiction Medicine fellow June 19, 2018 DISCLOSURES Speaker: Alann Weissman-Ward, MD, has nothing to disclose. Planning Committee:
Treatment Approaches for Drug Addiction
 Treatment Approaches for Drug Addiction NOTE: This fact sheet discusses research findings on effective treatment approaches for drug abuse and addiction. If you re seeking treatment, you can call the Substance
Treatment Approaches for Drug Addiction NOTE: This fact sheet discusses research findings on effective treatment approaches for drug abuse and addiction. If you re seeking treatment, you can call the Substance
Class Update: Substance Use Disorders
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Hot Topics in Addiction Medicine. Timothy Fong MD 44 th Annual Family Medicine Refresher March 2017
 Hot Topics in Addiction Medicine Timothy Fong MD 44 th Annual Family Medicine Refresher March 2017 Financial Disclosures Speaker Bureau Indivior Research Support Constellation Health Onward Hot Topics
Hot Topics in Addiction Medicine Timothy Fong MD 44 th Annual Family Medicine Refresher March 2017 Financial Disclosures Speaker Bureau Indivior Research Support Constellation Health Onward Hot Topics
Medication Assisted Treatment. MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment
 Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
Medication Assisted Treatment MAT Opioid dependence/addiction Opioid treatment programs OTP Regulation of OTP Office Based Treatment Opioid Drugs Opium Morphine Heroin Codeine Oxycodone Roxycodone Oxycontin
Pharmacotherapy of Substance Use Disorders in Children and Adolescents: Special Considerations
 Pharmacotherapy of Substance Use Disorders in Children and Adolescents: Special Considerations Dr. Ajeet Sidana Department of Psychiatry Government Medical College & Hospital Chandigarh Scope of Presentation
Pharmacotherapy of Substance Use Disorders in Children and Adolescents: Special Considerations Dr. Ajeet Sidana Department of Psychiatry Government Medical College & Hospital Chandigarh Scope of Presentation
Class Update: Substance Use Disorders
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Pharmacotherapy for opioid addiction. Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco
 Pharmacotherapy for opioid addiction Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco Disclosure slide No commercial conflicts to disclose. Gaps in current treatment of opioid
Pharmacotherapy for opioid addiction Judith Martin, MD Medical Director BAART Turk Street Clinic San Francisco Disclosure slide No commercial conflicts to disclose. Gaps in current treatment of opioid
Wasted AN INTRODUCTION TO SUBSTANCE ABUSE
 Wasted AN INTRODUCTION TO SUBSTANCE ABUSE Dr. Brian L. Bethel Child and Family Therapist Independent Trainer and Consultant LPCC-S, LCDC III, RPT-S www.brianlbethel.com INTERPLAY COUNSELING & CONSULTING
Wasted AN INTRODUCTION TO SUBSTANCE ABUSE Dr. Brian L. Bethel Child and Family Therapist Independent Trainer and Consultant LPCC-S, LCDC III, RPT-S www.brianlbethel.com INTERPLAY COUNSELING & CONSULTING
Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They?
 Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They? Yngvild Olsen, MD, MPH Cecil County Board of Health Workgroup Meeting Elkton, MD October 8, 2013 Objectives
Medications in the Treatment of Opioid Use Disorder: Methadone and Buprenorphine What Really Are They? Yngvild Olsen, MD, MPH Cecil County Board of Health Workgroup Meeting Elkton, MD October 8, 2013 Objectives
POLYSUBSTANCE USE IN THE TREATMENT OF OPIOID USE DISORDER WITH BUPRENORPHINE
 Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences POLYSUBSTANCE USE IN THE TREATMENT OF OPIOID USE DISORDER WITH BUPRENORPHINE MARK DUNCAN, MD November 8, 2018 SPEAKER
Psychiatry and Addictions Case Conference UW Medicine Psychiatry and Behavioral Sciences POLYSUBSTANCE USE IN THE TREATMENT OF OPIOID USE DISORDER WITH BUPRENORPHINE MARK DUNCAN, MD November 8, 2018 SPEAKER
Addictions Pharmacotherapy
 Addictions Pharmacotherapy Thomas Kosten MD Associate Vice President for Research JH Waggoner Chair & Professor of Psychiatry, Pharmacology & Neuroscience Baylor College of Medicine Disclosure Thomas Kosten,
Addictions Pharmacotherapy Thomas Kosten MD Associate Vice President for Research JH Waggoner Chair & Professor of Psychiatry, Pharmacology & Neuroscience Baylor College of Medicine Disclosure Thomas Kosten,
MAT - ICAAD 2018 Ron Jackson, MSW, LICSW
 The ATTC Network Ten Regional Centers northwest@attcnetwork.org www.attcnetwork.org/northwest phone. 206-685-4419 1107 NE 45 th St, Ste 120, Seattle, WA 98105 http://attcnetwork.org/northwest U.S. Opioid
The ATTC Network Ten Regional Centers northwest@attcnetwork.org www.attcnetwork.org/northwest phone. 206-685-4419 1107 NE 45 th St, Ste 120, Seattle, WA 98105 http://attcnetwork.org/northwest U.S. Opioid
Disclosures. Topics of today s training 4/24/2017. Evolving Treads in Medication Assisted Treatment. Christopher J Davis D.O.
 Evolving Treads in Medication Assisted Treatment Christopher J Davis D.O. CAADC, FASAM Medical Director, The Ranch of Pennsylvania Medical Director, Pyramid Healthcare Diplomate of The American Board of
Evolving Treads in Medication Assisted Treatment Christopher J Davis D.O. CAADC, FASAM Medical Director, The Ranch of Pennsylvania Medical Director, Pyramid Healthcare Diplomate of The American Board of
Addiction to Opioids. Marvin D. Seppala, MD Chief Medical Officer
 Addiction to Opioids Marvin D. Seppala, MD Chief Medical Officer Mayo Clinic Opioid Conference: Evidence, Clinical Considerations and Best Practice Friday, September 30, 2016 26 y.o. female from South
Addiction to Opioids Marvin D. Seppala, MD Chief Medical Officer Mayo Clinic Opioid Conference: Evidence, Clinical Considerations and Best Practice Friday, September 30, 2016 26 y.o. female from South
Topics of today s training
 Extended Release Naltrexone Vivitrol Christopher J Davis D.O. CAADC, FASAM Medical Director, Brightwater Landing Medical Director, Pyramid Healthcare Diplomate of The American Board of Addition Medicine
Extended Release Naltrexone Vivitrol Christopher J Davis D.O. CAADC, FASAM Medical Director, Brightwater Landing Medical Director, Pyramid Healthcare Diplomate of The American Board of Addition Medicine
Start Low, Go Slow but Treat to Target
 Start Low, Go Slow but Treat to Target Pharmacotherapy for Depression, Anxiety and At-Risk Alcohol Use in Late Life September 29, 2014 Audio and Control Panel instruction On the phone? Raise your hand
Start Low, Go Slow but Treat to Target Pharmacotherapy for Depression, Anxiety and At-Risk Alcohol Use in Late Life September 29, 2014 Audio and Control Panel instruction On the phone? Raise your hand
6B / Boswell, Grant and Slutske Day 2 August 14, 2008
 Pharmacological Treatment of Pathological Gambling Jon E. Grant, JD, MD, MPH Associate Professor University of Minnesota School of Medicine Minneapolis, MN Disclosure Information I have the following financial
Pharmacological Treatment of Pathological Gambling Jon E. Grant, JD, MD, MPH Associate Professor University of Minnesota School of Medicine Minneapolis, MN Disclosure Information I have the following financial
THE MEDICAL MODEL: ADDICTION IS A BRAIN DISEASE. Judith Martin, MD Medical Director of Substance Use Services San Francisco Dept.
 THE MEDICAL MODEL: ADDICTION IS A BRAIN DISEASE Judith Martin, MD Medical Director of Substance Use Services San Francisco Dept. Public Health disclosures Dr. Martin has no conflict of interest to disclose.
THE MEDICAL MODEL: ADDICTION IS A BRAIN DISEASE Judith Martin, MD Medical Director of Substance Use Services San Francisco Dept. Public Health disclosures Dr. Martin has no conflict of interest to disclose.
Opioids and Opioid Addiction: Practical Management Approaches
 Opioids and Opioid Addiction: Practical Management Approaches Yngvild Olsen, MD, MPH Medical Director Institutes for Behavior Resources Inc/REACH Health Services Conflict of Interest No financial or advisory
Opioids and Opioid Addiction: Practical Management Approaches Yngvild Olsen, MD, MPH Medical Director Institutes for Behavior Resources Inc/REACH Health Services Conflict of Interest No financial or advisory
Opioid Dependence and Buprenorphine Management
 Opioid Dependence and Buprenorphine Management Kevin Kapila, MD Fenway Health Medical Director of Behavioral Health Instructor in Medicine Harvard Medical School Learning Objectives Understand the rationale
Opioid Dependence and Buprenorphine Management Kevin Kapila, MD Fenway Health Medical Director of Behavioral Health Instructor in Medicine Harvard Medical School Learning Objectives Understand the rationale
OAT Transitions - focus on microdosing. Mark McLean MD MSc FRCPC CISAM DABAM
 OAT Transitions - focus on microdosing Mark McLean MD MSc FRCPC CISAM DABAM Disclosures No pharmaceutical industry or other financial conflicts of interest Study Physician for research funded by Canadian
OAT Transitions - focus on microdosing Mark McLean MD MSc FRCPC CISAM DABAM Disclosures No pharmaceutical industry or other financial conflicts of interest Study Physician for research funded by Canadian
AGENDA U.S. SURGEON GENERAL, VIVEK MURTHY MD 2/5/2019
 FORMER U.S. SURGEON GENERAL, VIVEK MURTHY MD AN ESTIMATED 20.8 MILLION PEOPLE IN OUR COUNTRY ARE LIVING WITH A SUBSTANCE USE DISORDER. THIS IS SIMILAR TO THE NUMBER OF PEOPLE WHO HAVE DIABETES, AND 1.5
FORMER U.S. SURGEON GENERAL, VIVEK MURTHY MD AN ESTIMATED 20.8 MILLION PEOPLE IN OUR COUNTRY ARE LIVING WITH A SUBSTANCE USE DISORDER. THIS IS SIMILAR TO THE NUMBER OF PEOPLE WHO HAVE DIABETES, AND 1.5
U.S. SURGEON GENERAL, VIVEK MURTHY MD
 FORMER U.S. SURGEON GENERAL, VIVEK MURTHY MD AN ESTIMATED 20.8 MILLION PEOPLE IN OUR COUNTRY ARE LIVING WITH A SUBSTANCE USE DISORDER. THIS IS SIMILAR TO THE NUMBER OF PEOPLE WHO HAVE DIABETES, AND 1.5
FORMER U.S. SURGEON GENERAL, VIVEK MURTHY MD AN ESTIMATED 20.8 MILLION PEOPLE IN OUR COUNTRY ARE LIVING WITH A SUBSTANCE USE DISORDER. THIS IS SIMILAR TO THE NUMBER OF PEOPLE WHO HAVE DIABETES, AND 1.5
Buprenorphine: An Introduction. Sharon Stancliff, MD Harm Reduction Coalition September 2008
 Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
Buprenorphine: An Introduction Sharon Stancliff, MD Harm Reduction Coalition September 2008 Objective Participants will be able to: Discuss the role of opioid maintenance in reducing morbidity and mortality
Mary Ann Ferguson,Pharmacist St Josephs Health Care Concurrent Disorders Inpatient Unit
 Mary Ann Ferguson,Pharmacist St Josephs Health Care Concurrent Disorders Inpatient Unit Fergusom@stjoes.ca Medication should be considered as part of the treatment plan for addictions/substance use disorders:
Mary Ann Ferguson,Pharmacist St Josephs Health Care Concurrent Disorders Inpatient Unit Fergusom@stjoes.ca Medication should be considered as part of the treatment plan for addictions/substance use disorders:
Methadone and Naltrexone ER
 Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Objectives Review Full Opioid
Methadone and Naltrexone ER Laura G. Kehoe, MD, MPH, FASAM Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Objectives Review Full Opioid
An Internist s Guide to Unhealthy Alcohol Use. Ryan Graddy, MD JHU SOM
 An Internist s Guide to Unhealthy Alcohol Use Ryan Graddy, MD JHU SOM Disclosures None Learning Objectives Understand the terminology used to describe unhealthy alcohol use Identify means of screening
An Internist s Guide to Unhealthy Alcohol Use Ryan Graddy, MD JHU SOM Disclosures None Learning Objectives Understand the terminology used to describe unhealthy alcohol use Identify means of screening
Pharmacotherapy for Alcohol Use Disorder
 Pharmacotherapy for Alcohol Use Disorder Laura G. Kehoe, MD, MPH Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither my
Pharmacotherapy for Alcohol Use Disorder Laura G. Kehoe, MD, MPH Medical Director MGH Substance Use Disorder Bridge Clinic Assistant Professor of Medicine Harvard Medical School Disclosures Neither my
Rates of Opioid Overdose Deaths, Sales, and Treatment Admissions: US,
 Rates of Opioid Overdose Deaths, Sales, and Treatment Admissions: US, 1999 21 8 Rates of Prescription Painkiller Sales, Deaths, and Substance Abuse Treatment Admissions (1999 21) 7 Rate 6 5 4 3 Sales per
Rates of Opioid Overdose Deaths, Sales, and Treatment Admissions: US, 1999 21 8 Rates of Prescription Painkiller Sales, Deaths, and Substance Abuse Treatment Admissions (1999 21) 7 Rate 6 5 4 3 Sales per