Diagnosis and Treatment of Primary Hyperparathyroidism. Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic
|
|
|
- Diana Welch
- 5 years ago
- Views:
Transcription
1 Diagnosis and Treatment of Primary Hyperparathyroidism Geoffrey B. Thompson, MD Professor of Surgery College of Medicine, Mayo Clinic
2 Disclosure Nothing to Disclose
3 Primary HPT Autonomous secretion of excess PTH Normal inhibitory feedback lost Few patients remain asymptomatic
4 Primary HPT 100,000 new cases annually (U.S.) 1/1000-1/500 per year (U.S.) 8,500 cases recurrent / persistent HPT per year (U.S.)
5 Primary HPT Women > age 50 All ages, races Both sexes
6 Primary HPT Single adenoma: 85% MGD: 12-14% 14% Cancer: < 1 %
7 Primary HPT Familial (usually MGD) MEN 1 (95%) MEN 2A (10-35%) FIH HPT -- jaw tumor syndrome (SGD)
8 Clinical Manifestations Osteopenia / osteoporosis Fractures Hypercalciuria Renal dysfunction Nephrolithiasis, nephrocalcinosis
9 Clinical Manifestations (HPT) Fatigue Muscle weakness (aches & pains) Neuropsychiatric disturbances GI disturbances Impaired CV health
10 Symptomatic HPT (<20%) Nephrolithiasis Fractures, osteitis fibrosa cystica Hypercalcemic Crisis Pancreatitis
11 NIH Consensus Conference for Parathyroidectomy in Patients with HPT Age < 50 years Nephrolithiasis Markedly elevated serum calcium level :>1.0 mg/dl above normal Osteitis fibrosa cystica Creatinine clearance 30% less than that of age-matched normal subjects History of hypercalcemic crisis Urinary calcium > 400mg/day Bone density more than 2 std dev below controls Documented neuromuscular symptoms Medical surveillance not desirable or possible
12 Primary Hyperparathyroidism Over 90% of our operated patients meet the new NIH criteria Over 80% of patients have a myriad of non-classical, subclinical signs and symptoms at presentation Primary HPT offers something (bad) for everyone if you look for it
13 Asymptomatic Hyperparathyroidism IT DOES NOT EXIST! Or at least aproblematic hpt does not exist
14 Excess Mortality from HPT 896 pts operated between 1953 and 1982 Increased relative risk for premature death Risk ameliorated by successful surgery Return to normal risk occurred more quickly in milder cases Hedback, 1991
15 Excess Mortality Seen in mild and severe hpt Diminished by surgery (Palmer, 1987; Ronni-Sivula,1985) Mayo-Wermers 1998: Increased risk of death in more severe untreated cases
16 Bone Disease Often clinically silent until fractures occur $14 billion dollar medical expense in U.S.
17 Risk of Fracture in HPT 407 patients with HPT at Mayo Observed increase of 30% over expected in hpt group Parathyroid surgery may have protective effect Khosla,1999
18 Effect of Surgery on Bone 10-year follow-up study ALL symptomatic, non-operated, operated, patients progressed After surgery all pts had improved BMD No difference in symptomatic vs asymptomatic pts No reliable predictors for who will progress Silverberg, 1999
19 Editorial Comment-R. Utiger Asymptomatic does not necessarily mean unharmed Surgical Treatment.should now be recommended for (nearly) all hpt pts.
20 PTx vs. Antiresorptive Agents Increase in BMD less than 10% over 3 years (Liberman, 1995,1996) with ARA s PTx increases BMD 8-12% 8 in 1-31 years (Silverberg, 1999)
21 Neuropsychiatric and Musculoskeletal Symptoms Joborn (1989) Numann (1984) Chan (1985) Lundgren (1998) Burney (1996,1998,1999) Pasieka (2002)
22 Burney SF-36 Questionnaire 140 pts: Ca<10.9, Ca> domains: physical function, physical role limit, bodily pain, general health, vitality, social function, emotional role limit, mental health
23 Burney Much lower scores in preops compared to pts without hpt Great improvement over 2-62 months post op in 7 of 8 categories irrespective of calcium level pre-op Operate sooner rather than later
24 Pasieka QOL tool based on a visual analog scale Given pre- and post-op op Validated in prospective study Pts fulfilling and not fulfilling NIH criteria Thyroidectomy pts as controls
25 Pasieka Conclusions Sx s s just as severe in pts not fulfilling NIH criteria for operation These pts achieved significant improvement in symptoms with parathyroidectomy NIH guidelines need to be broadened
26 DIAGNOSIS Elevated Calcium (total or ionized) Elevated or Inappropriate PTH Elevated or Normal 24hr Urine Calcium Normal Creatinine Low Normal Phosphorus Lithium and Thiazides
27 Standard Cervical Exploration Success: >98% Complications: <1%

28 Reoperative Parathyroid Surgery Success: 88% RLN injury: 1% Hypoparathyroidism: 13%

29 Minimally Invasive Parathyroidectomy Is this a valuable procedure or a stretch of the imagination?
30 Minimally Invasive Surgery Cholecystectomy Nissen fundoplication Colectomy Adrenalectomy Splenectomy

31 Minimally Invasive Surgery Fewer Advantages Appendectomy Hernia repair Operative site easily accessible via small incisions CP
32 New Outcome Measures Patient-Focused General anesthesia after-effects effects Nausea & vomiting Clouded sensorium Incisional pain Outpatient dismissal Postoperative convalescence
33 MIP Image-guided guided MIP Radioguided MIP Endoscopic or video-assisted MIP
34 Minimally Invasive Parathyroid Surgery Sestamibi parathyroid scanning Ultrasound Intraoperative PTH monitoring

35 Sestamibi Parathyroid Scan Dual photon, Subtraction scans With Planar, Oblique and SPECT imaging

36 Parathyroid Ultrasound
37 IOPTH Rapid results Highly reliable: SGD & MGD Cost: $1,000/patient? Immulite: $ PTH
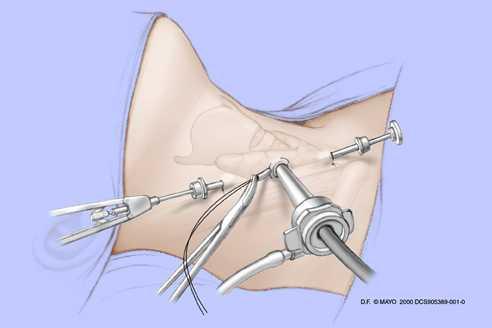
38 Endoscopic Technique
39 Endoscopic Technique

40 MIP Endoscopic Courtesy Dr. Barry Inabnet


41 Radioguided MIP Probe Gelpe retractor J. Norman, Tampa, FL 33% failure rate at Mayo Clinic
42 Image-Guided MIP Based on highly accurate preop SPS or US images IOPTH CP
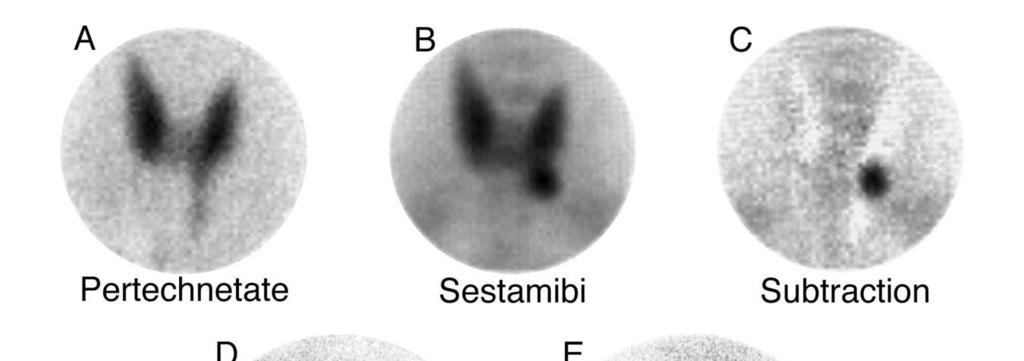
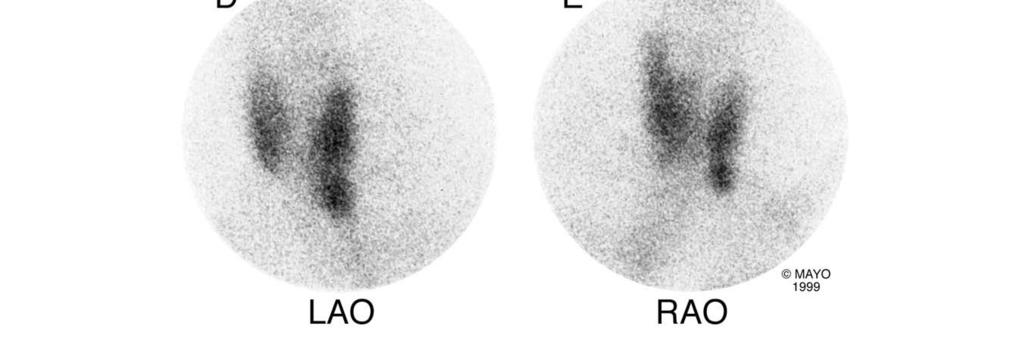
43 SPS
44 SPS
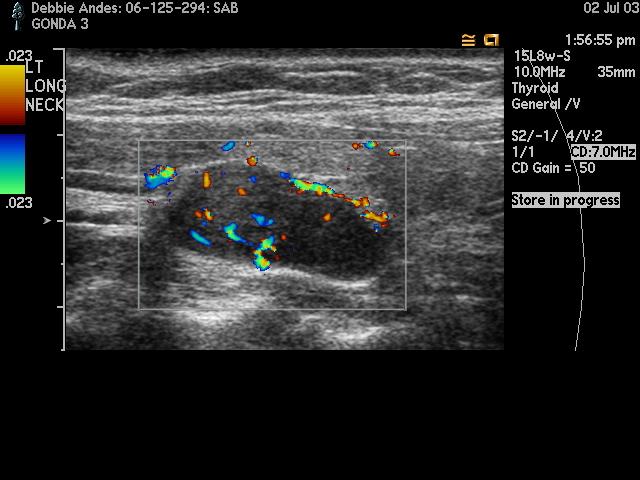
45 Parathyroid Ultrasound
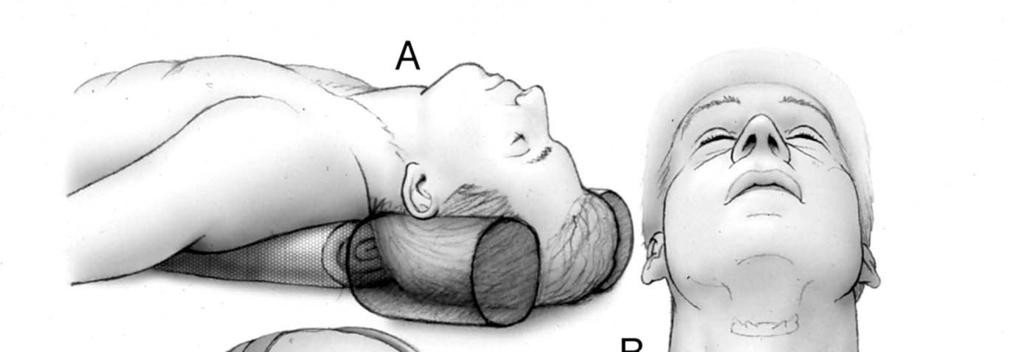
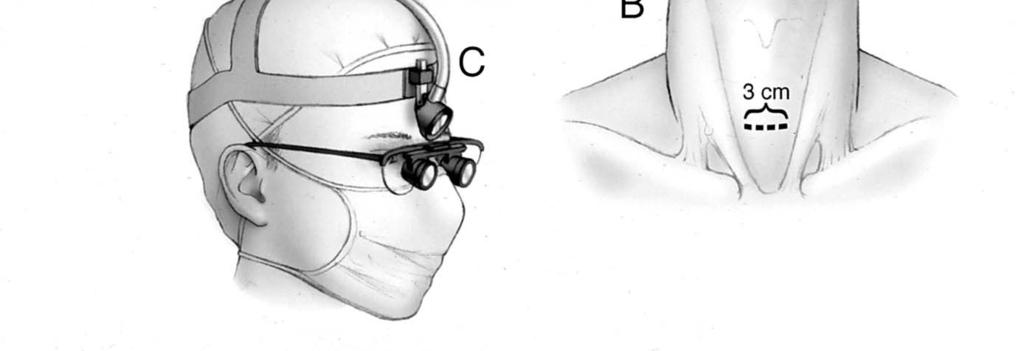
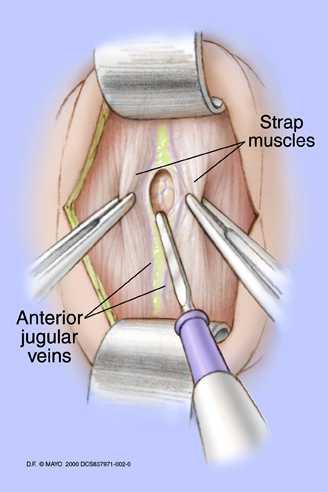
46 Image-Guided MIP 3-cm collar incision/unilateral exploration Local anesthesia/general anesthesia Outpatient setting Less nausea, pain Confirm results with IOPTH
47 MIP

48 MIP Technique
49

50 MIP Technique

51 MIP Technique

52 MIP Technique

53 MIP Technique




54 3 Months
55
56

57 MIP Technique

58 MIP Technique
59 SPS
60
61

62 MIP Technique

63 First Fifty Patients Outcomes similar Morbidity <1% Return to normal Overall satisfaction Scar satisfaction Similar Pain and nausea* less in MIP group Cosmesis better? *When performed under local anesthesia
64 HPT: Mayo 6/98-9/09 9/09 3,187 pts Age 61 (10-97) 25% 75%
65 HPT: Mayo Clinic Experience 3,187 pts (3,203 ops) MIP converted 4% Conventional 49% 47% Median gland wt: 430 mg (range, 20-56,000 mg) 88% SGD 12% MGD Mean Ca mg/dl MIP
66 HPT: Localization Overall Sestamibi (n=2,869) US (n=1,095) Sensitivity PPV False + False -
67 Reasons: Conventional Op 1,257 pts (includes reops) Reop (33%) No Reason (16%) HPT-related (4%) Pt preference: (2%) Tx-related (13%) Combined op (4%) Localization problem (28%)
68 MIP: Length of Stay/Anesthesia Outpatient General > 1 day 11% 31% 70% 58% 30% 23 MAC
69 MIP: Methodology Influences SPS: 2,869 cases (90%); Sensitivity 86%, PPV 92%, FP 7.4%, FN 13.0% IOPTH: 2,422 cases (76%); accuracy: 97% 194 (8%) true negatives most beneficial Gamma-probe inaccurate in 32% of 93 cases Thyroid resected in 439 cases (14%)
70 HPT: Success Cure Rates (3,187 patients) Conventional (exc reops) 96% MIP (exc reops) 98% Overall (inc reops) 97% MGD 95%
71 Complications RLN injury 0.1% Hematoma 0.3%
72 MIP: Assessment Advance Estimate 60-70% eligible for image- guided MIP Dependent on high-quality imaging and interpretation IOPTH truly valuable in <10%, but quite reassuring in others With the use of IOPTH, cure should be very little different from standard open procedure - probe not valuable in our hands
73 MIP: Assessment-2 Added Value Small incision Local anesthesia for majority of patients (no longer critical) minimize pain, nausea, mental fogginess outpatient General anesthesia if pt still outpatient Expense equivalent or increased Modest step forward---not a quantum leap
74 Indications for Standard Exploration Negative preoperative imaging Concomitant thyroid pathology * Family history of endocrinopathy Family history of HPT * Imaging suggesting MGD * History of neck irradiation * Certain reoperations *Relative contraindications for MIP
75 Persistent/Recurrent HPT Confirm Diagnosis: R/O FHH, Thiazides, Lithium Assess the risks of not reoperating Vocal cord examination Operative Reports-talk talk to surgeon Pathology blocks and slides (not just reports)

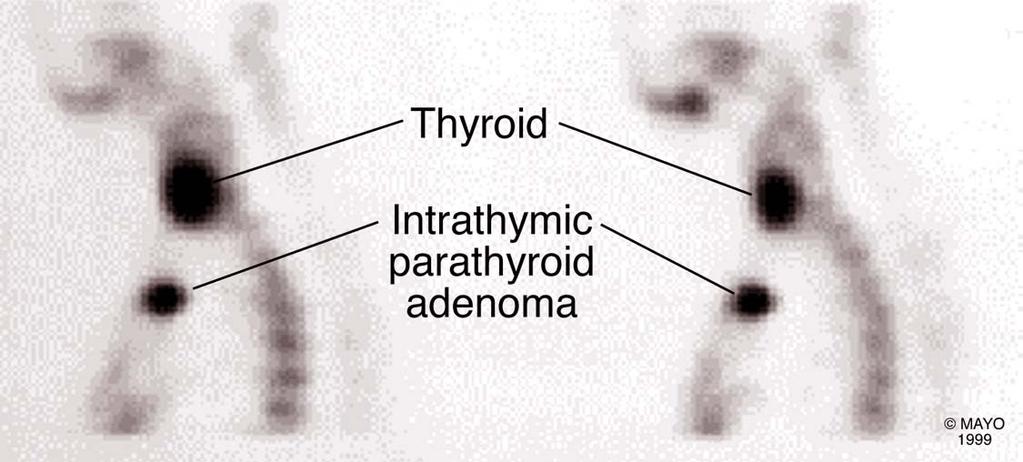
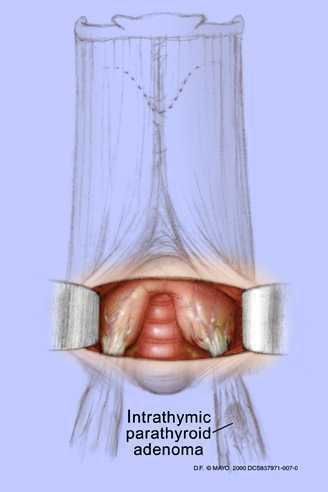
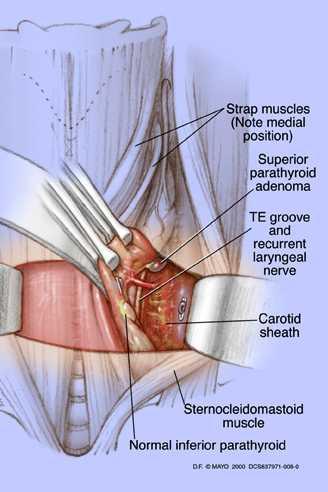
76 Reoperative Parathyroid Surgery: Location of Missed Glands in Cured Patients Normal Mediastinum 8 Intrathyroidal Carotid sheath 6 Anterior trachea 3 Retroesophageal 2
77 Persistent/Recurrent HPT(cont.)
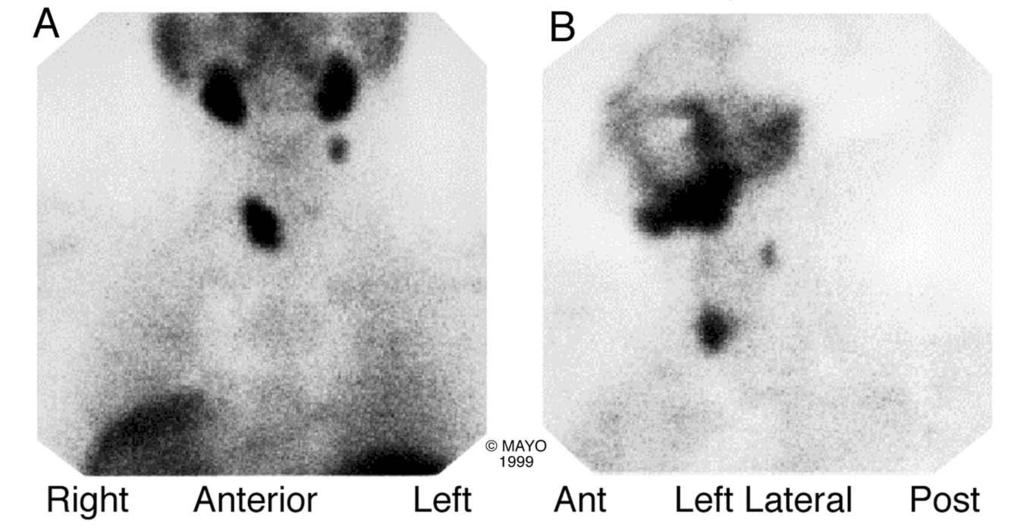
78

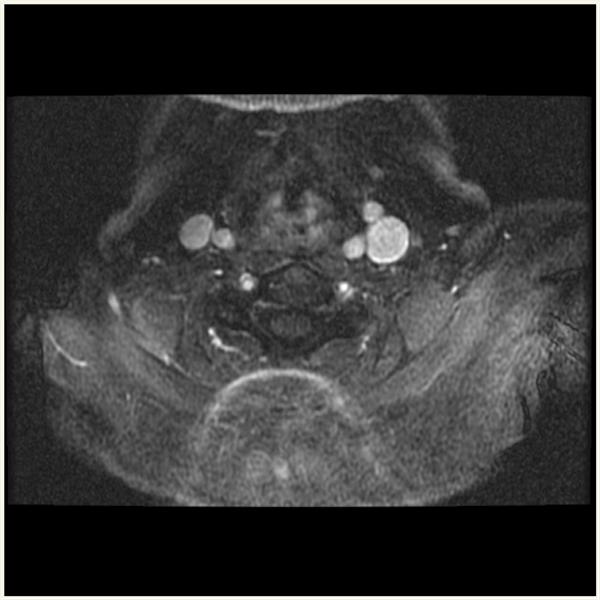
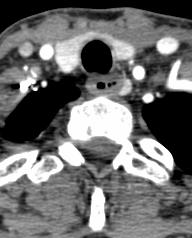
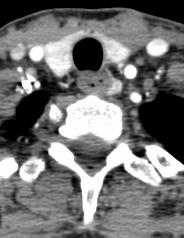
79 Left thyroid pole to left tracheoesophageal groove Nucs- US- Nothing convincing prior exploration



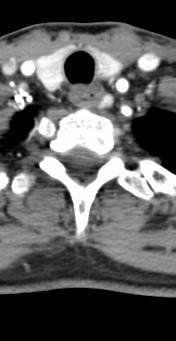
80 Arterial, 2mm slices, adenoma measured 8x4x14mm on CT


81
82


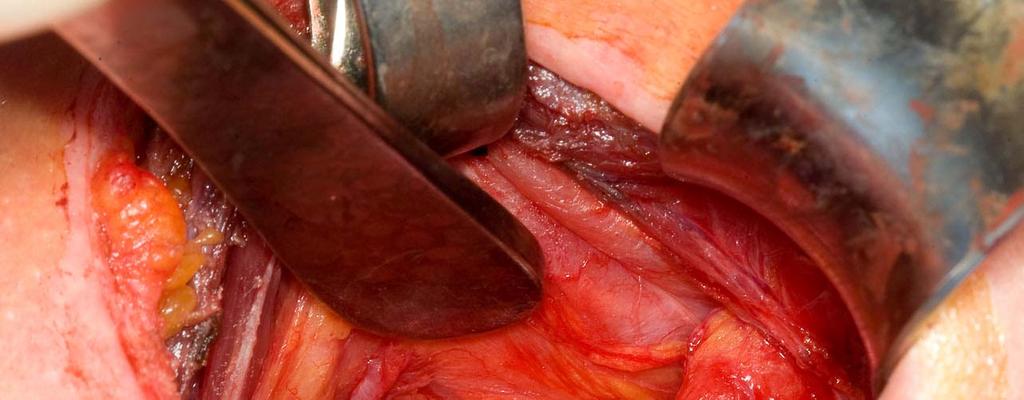

83 Courtesy Geoffrey Thompson, MD
84 Thank You
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE
 HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
HYPERPARATHYROIDIS M FAISAL GHANI SIDDIQUI MBBS; FCPS; PGDIP-BIOMEDICAL ETHICS; MCPS-HPE PROFESSOR OF SURGERY J I N N A H S I N D H M E D I C A L U N I V E R S I T Y PREAMBLE Anatomy & physiology of the
PRIMARY HYPERPARATHYROIDISM
 PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
PRIMARY HYPERPARATHYROIDISM HYPERPARATHYROIDISM Inappropriate excess secretion of Parathyroid Hormone in Primary Hyperparathyroidism Appropriate Hypersecretion in Secondary Hyperparathyroidism PTH and
Potential conflicts of interest: None
 Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene November 6, 2013 Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline
Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene November 6, 2013 Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline
Hyperparathyroidism. When to Suspect, How to Diagnose, When and How to Intervene. Johanna A. Pallotta, MD, FACP, FACE
 Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline Definition of hyperparathyroidism
Hyperparathyroidism When to Suspect, How to Diagnose, When and How to Intervene Johanna A. Pallotta, MD, FACP, FACE Potential conflicts of interest: None Johanna A. Pallotta, MD Outline Definition of hyperparathyroidism
Outline. Parathyroid Localization Studies. Mira Milas MD, FACS Associate Professor of Surgery Director, The Thyroid Center
 Parathyroid Localization Studies Mira Milas MD, FACS Associate Professor of Surgery Director, The Thyroid Center Outline Clinical Context of Primary Hyperparathyroidism Ultrasound, Sestamibi, and Other
Parathyroid Localization Studies Mira Milas MD, FACS Associate Professor of Surgery Director, The Thyroid Center Outline Clinical Context of Primary Hyperparathyroidism Ultrasound, Sestamibi, and Other
Clinical Approach to Hypercalcemia For the Primary Care Provider
 Clinical Approach to Hypercalcemia For the Primary Care Provider Christina Maser, MD FACS UCSF Fresno Department of Surgery, Endocrine Surgery 2/2/19 Objectives Recognition of pitfalls of diagnosis of
Clinical Approach to Hypercalcemia For the Primary Care Provider Christina Maser, MD FACS UCSF Fresno Department of Surgery, Endocrine Surgery 2/2/19 Objectives Recognition of pitfalls of diagnosis of
hypercalcemia of malignancy hyperparathyroidism PHPT the most common cause of hypercalcemia in the outpatient setting the second most common cause
 hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
hyperparathyroidism A 68-year-old woman with documented osteoporosis has blood tests showing elevated serum calcium and parathyroid hormone (PTH) levels: 11.2 mg/dl (8.8 10.1 mg/dl) and 88 pg/ml (10-60),
"Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy
 "Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy Rebecca S. Sippel, M.D. Assistant Professor Department of Surgery Section of Endocrine Surgery University of Wisconsin Primary Hyperparathyroidism
"Asymptomatic" Hyperparathyroidism: Reasons for Parathyroidectomy Rebecca S. Sippel, M.D. Assistant Professor Department of Surgery Section of Endocrine Surgery University of Wisconsin Primary Hyperparathyroidism
2016 Arizona AACE Meeting: Updated Guidelines for the Management of Primary Hyperparathyroidism (PHPT)
") 2016 Arizona AACE Meeting: Updated Guidelines for the Management of Primary Hyperparathyroidism (PHPT) Scott M. Wilhelm, MD, FACS Associate Professor and Section Head Endocrine Surgery University Hospitals-Cleveland
2016 Arizona AACE Meeting: Updated Guidelines for the Management of Primary Hyperparathyroidism (PHPT) Scott M. Wilhelm, MD, FACS Associate Professor and Section Head Endocrine Surgery University Hospitals-Cleveland
Minimally invasive parathyroidectomy
 Minimally invasive parathyroidectomy Jessica E. Gosnell MD Assistant Professor of Surgery March 22, 2011 1 Minimally invasive parathyroidectomy 1. What? 2. When? 3. How? 4. Convert? 5. What adjuncts? Primary
Minimally invasive parathyroidectomy Jessica E. Gosnell MD Assistant Professor of Surgery March 22, 2011 1 Minimally invasive parathyroidectomy 1. What? 2. When? 3. How? 4. Convert? 5. What adjuncts? Primary
HPI joint pain/arthritis serum calcium 11.5 PTH 147pg/ml
 HPI 45 yo female Increased calcium level during evaluation for joint pain/arthritis W/U showed serum calcium 11.5 and PTH 147pg/ml (Normal 11-67pg/ml) Otherwise asymptomatic PMH/PSH Arthritis Tonsillectomy
HPI 45 yo female Increased calcium level during evaluation for joint pain/arthritis W/U showed serum calcium 11.5 and PTH 147pg/ml (Normal 11-67pg/ml) Otherwise asymptomatic PMH/PSH Arthritis Tonsillectomy
Approach to a patient with hypercalcemia
 Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Approach to a patient with hypercalcemia Ana-Maria Chindris, MD Division of Endocrinology Mayo Clinic Florida 2013 MFMER slide-1 Background Hypercalcemia is a problem frequently encountered in clinical
Parathyroid Imaging. A Guide to Parathyroid Surgery
 Parathyroid Imaging A Guide to Parathyroid Surgery Primary Hyperparathyroidism (PHPT) 3 rd most common endocrine disorder after diabetes and hyperthyroidism Prevalence in women 2% Often discovered in asymptomatic
Parathyroid Imaging A Guide to Parathyroid Surgery Primary Hyperparathyroidism (PHPT) 3 rd most common endocrine disorder after diabetes and hyperthyroidism Prevalence in women 2% Often discovered in asymptomatic
4/20/2015. The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy. Learning Objectives
 Testing During Surgical Parathyroidectomy. Learning Objectives") The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy Nichole Korpi-Steiner, PhD, DABCC, FACB University of North Carolina Chapel Hill, NC Learning
The Neck xt Exploration: Intraoperative Parathyroid Hormone (IOPTH) Testing During Surgical Parathyroidectomy Nichole Korpi-Steiner, PhD, DABCC, FACB University of North Carolina Chapel Hill, NC Learning
PARATHYROID NUCLEAR MEDICINE IMAGING REVIEW DISCLOSURES
 PARATHYROID NUCLEAR MEDICINE IMAGING REVIEW Miguel Hernandez Pampaloni, M.D., Ph.D. Chief, Nuclear Medicine Assistant Professor of Radiology UCSF Department of Radiology and Biomedical Imaging DISCLOSURES
PARATHYROID NUCLEAR MEDICINE IMAGING REVIEW Miguel Hernandez Pampaloni, M.D., Ph.D. Chief, Nuclear Medicine Assistant Professor of Radiology UCSF Department of Radiology and Biomedical Imaging DISCLOSURES
Normal PTH Levels in Primary Hyperparathyroidism: Still the Same Disease?
 Ann Surg Oncol (2011) 18:3437 3442 DOI 10.1245/s10434-011-1744-x ORIGINAL ARTICLE ENDOCRINE TUMORS Normal PTH Levels in Primary Hyperparathyroidism: Still the Same Disease? Amanda L. Amin, MD, Tracy S.
Ann Surg Oncol (2011) 18:3437 3442 DOI 10.1245/s10434-011-1744-x ORIGINAL ARTICLE ENDOCRINE TUMORS Normal PTH Levels in Primary Hyperparathyroidism: Still the Same Disease? Amanda L. Amin, MD, Tracy S.
PARATHYROID IMAGING. James Lee, MD Chief, Endocrine Surgery Co-Director NY Thyroid-Parathyroid Center Columbia University Medical Center
 PARATHYROID IMAGING James Lee, MD Chief, Endocrine Surgery Co-Director NY Thyroid-Parathyroid Center Columbia University Medical Center NO DISCLOSURES Overview The hallmarks of the ideal test Benefits
PARATHYROID IMAGING James Lee, MD Chief, Endocrine Surgery Co-Director NY Thyroid-Parathyroid Center Columbia University Medical Center NO DISCLOSURES Overview The hallmarks of the ideal test Benefits
Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones
 Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) 30 yr-old woman with 7 yr history
Case 2: 30 yr-old woman with 7 yr history of recurrent kidney stones Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) 30 yr-old woman with 7 yr history
PRIMARY HYPERPARATHYROIDISM PRIMARY HYPERPARATHYROIDISM. Hyperparathyroidism Etiology. Common Complex Insidious Chronic Global Only cure is surgery
 ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
ENDOCRINE DISORDER PRIMARY HYPERPARATHYROIDISM Roseann P. Velez, DNP, FNP Francis J. Velez, MD, FACS Common Complex Insidious Chronic Global Only cure is surgery HYPERPARATHYROIDISM PARATHRYOID GLANDS
Parathyroids, Small but Mighty Current Pathways to Early Diagnosis and Cure of Parathyroid Disease
 Parathyroids, Small but Mighty Current Pathways to Early Diagnosis and Cure of Parathyroid Disease Mira Milas MD, FACS Professor of Surgery Director of Endocrine Surgery No conflicts of interest or financial
Parathyroids, Small but Mighty Current Pathways to Early Diagnosis and Cure of Parathyroid Disease Mira Milas MD, FACS Professor of Surgery Director of Endocrine Surgery No conflicts of interest or financial
Outline. Primary Hyperparathyriodism. SPECT/CT in Parathyroid Localisation. Ann-Marie Quigley Nuclear Medicine Royal Free Hospital London
 SPECT/CT in Parathyroid Localisation Ann-Marie Quigley Nuclear Medicine Royal Free Hospital London Outline Pathophysiology Current guidelines SPECT/CT the evidence SPECT/CT in clinical scenarios MGD, Nodular
SPECT/CT in Parathyroid Localisation Ann-Marie Quigley Nuclear Medicine Royal Free Hospital London Outline Pathophysiology Current guidelines SPECT/CT the evidence SPECT/CT in clinical scenarios MGD, Nodular
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases
 Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand
 International Endocrinology Volume 2012, Article ID 952426, 4 pages doi:10.1155/2012/952426 Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand Poramaporn
International Endocrinology Volume 2012, Article ID 952426, 4 pages doi:10.1155/2012/952426 Research Article Primary Hyperparathyroidism: 11-Year Experience in a Single Institute in Thailand Poramaporn
USEFULNESS OF INTRAOPERATIVE PARATHYROID HORMONE MONITORING DURING MINIMALLY INVASIVE VIDEO-ASSISTED PARATHYROIDECTOMY
 USEFULNESS OF INTRAOPERATIVE PARATHYROID HORMONE MONITORING DURING MINIMALLY INVASIVE VIDEO-ASSISTED PARATHYROIDECTOMY Elisabetta Stenner elisabetta.stenner@asuits.sanita.fvg.it Introduction: primary hyperparathyroidism
USEFULNESS OF INTRAOPERATIVE PARATHYROID HORMONE MONITORING DURING MINIMALLY INVASIVE VIDEO-ASSISTED PARATHYROIDECTOMY Elisabetta Stenner elisabetta.stenner@asuits.sanita.fvg.it Introduction: primary hyperparathyroidism
Outline. SPECT/CT in Parathyroid Disease. Pathophysiology. Current guidelines. SPECT/CT the evidence. SPECT/CT in clinical scenarios
 SPECT/CT in Parathyroid Disease Ann-Marie Quigley Nuclear Medicine Royal Free Hospital London Outline Pathophysiology Current guidelines SPECT/CT the evidence SPECT/CT in clinical scenarios MGD, Nodular
SPECT/CT in Parathyroid Disease Ann-Marie Quigley Nuclear Medicine Royal Free Hospital London Outline Pathophysiology Current guidelines SPECT/CT the evidence SPECT/CT in clinical scenarios MGD, Nodular
Parathyroid Disease Scenarios for the Practicing Clinician. Vijaya Chockalingam MD Faculty Endocrinologist Banner University Medical Center- Phoenix
 Parathyroid Disease Scenarios for the Practicing Clinician Vijaya Chockalingam MD Faculty Endocrinologist Banner University Medical Center- Phoenix Clinical Scenario-1 73 year man (BK) with hypercalcemia
Parathyroid Disease Scenarios for the Practicing Clinician Vijaya Chockalingam MD Faculty Endocrinologist Banner University Medical Center- Phoenix Clinical Scenario-1 73 year man (BK) with hypercalcemia
RADIOGUIDED PARATHYROIDECTOMY IS SUCCESSFUL IN 98.7% OF SELECTED PATIENTS
 Original Article RADIOGUIDED PARATHYROIDECTOMY IS SUCCESSFUL IN 98.7% OF SELECTED PATIENTS Charles D. Livingston, MD, FACS ABSTRACT Objective: To examine an individualized approach to patients with primary
Original Article RADIOGUIDED PARATHYROIDECTOMY IS SUCCESSFUL IN 98.7% OF SELECTED PATIENTS Charles D. Livingston, MD, FACS ABSTRACT Objective: To examine an individualized approach to patients with primary
Marcin Barczynski, 1 Aleksander Konturek, 2 Alicja Hubalewska-Dydejczyk, 2. Filip Gołkowski, 1 Stanislaw Cichon, 1 Piotr Richter, 1 Wojciech Nowak
 3 rd Chair and Department of General Surgery 1 and Chair and Department of Endocrinology 2 Jagiellonian University, Medical College Head: Prof. Wojciech Nowak, MD, PhD INTRAOPERATIVE BILATERAL INTERNAL
3 rd Chair and Department of General Surgery 1 and Chair and Department of Endocrinology 2 Jagiellonian University, Medical College Head: Prof. Wojciech Nowak, MD, PhD INTRAOPERATIVE BILATERAL INTERNAL
Parathyroid Imaging What is best
 Parathyroid Imaging What is best Mike Avison Bradford Why me? I m honoured to be asked to present this. There is no killer paper or text which clearly proves the best methodology. Bradford has performed
Parathyroid Imaging What is best Mike Avison Bradford Why me? I m honoured to be asked to present this. There is no killer paper or text which clearly proves the best methodology. Bradford has performed
The parathyroid glands participate in the regulation
 41 HERNAN I. VARGAS STANLEY R. KLEIN The parathyroid glands participate in the regulation of calcium metabolism. Disorders of the parathyroid gland are most commonly a result of hyperfunction and rarely
41 HERNAN I. VARGAS STANLEY R. KLEIN The parathyroid glands participate in the regulation of calcium metabolism. Disorders of the parathyroid gland are most commonly a result of hyperfunction and rarely
Hyperparathyroidism: Operative Considerations. Financial Disclosures: None. Hyperparathyroidism. Hyperparathyroidism 11/10/2012
 Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Hyperparathyroidism: Operative Considerations Financial Disclosures: None Steven J Wang, MD FACS Associate Professor Dept of Otolaryngology-Head and Neck Surgery University of California, San Francisco
Primary Hyperparathyroidism
 Primary Hyperparathyroidism Copyright Copyright 2019 2019 American American Associa7on Associa7on of Clinical of Clinical Endocrinologists Endocrinologists 1 Primary Hyperparathyroidism In primary hyperparathyroidism
Primary Hyperparathyroidism Copyright Copyright 2019 2019 American American Associa7on Associa7on of Clinical of Clinical Endocrinologists Endocrinologists 1 Primary Hyperparathyroidism In primary hyperparathyroidism
Hypercalcemia & Parathyroid Disorders. W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology
 Hypercalcemia & Parathyroid Disorders W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology Objectives Review diagnostic workup for hypercalcemia Review management of primary hyperparathyroidism Review
Hypercalcemia & Parathyroid Disorders W. Reid Litchfield, MD, FACE, ECNU Desert Endocrinology Objectives Review diagnostic workup for hypercalcemia Review management of primary hyperparathyroidism Review
Case 4: 27 yr-old woman with history of kidney stones and hyperparathyroidism.
 Case 4: 27 yr-old woman with history of kidney stones and hyperparathyroidism. Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) Hyperparathyroidism
Case 4: 27 yr-old woman with history of kidney stones and hyperparathyroidism. Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) Hyperparathyroidism
PAPER. The Effectiveness of Radioguided Parathyroidectomy in Patients With Negative Technetium Tc 99m Sestamibi Scans
 PAPER The Effectiveness of Radioguided Parathyroidectomy in Patients With Negative Technetium Tc 99m Sestamibi Scans Herbert Chen, MD; Rebecca S. Sippel, MD; Sarah Schaefer, NP Background: Many surgeons
PAPER The Effectiveness of Radioguided Parathyroidectomy in Patients With Negative Technetium Tc 99m Sestamibi Scans Herbert Chen, MD; Rebecca S. Sippel, MD; Sarah Schaefer, NP Background: Many surgeons
Bone and Renal Stone Disease in Patients Operated for Primary Hyperparathyroidism in Pakistan: Is the Pattern of Disease different from the West?
 ecommons@aku Section of Urology Department of Surgery August 1999 Bone and Renal Stone Disease in Patients Operated for Primary Hyperparathyroidism in Pakistan: Is the Pattern of Disease different from
ecommons@aku Section of Urology Department of Surgery August 1999 Bone and Renal Stone Disease in Patients Operated for Primary Hyperparathyroidism in Pakistan: Is the Pattern of Disease different from
Hyperparathyroidism (primary): diagnosis, assessment and initial management
: diagnosis, assessment and initial management") National Institute for Health and Care Excellence. Hyperparathyroidism (primary): diagnosis, assessment and initial management NICE guideline . October 2018 This guideline was developed by the
National Institute for Health and Care Excellence. Hyperparathyroidism (primary): diagnosis, assessment and initial management NICE guideline . October 2018 This guideline was developed by the
Parathyroid Imaging: Current Concepts. Maria Gule-Monroe, M.D. Nancy Perrier, M.D.
 Parathyroid Imaging: Current Concepts Maria Gule-Monroe, M.D. Nancy Perrier, M.D. Disclosures None Objectives Ultrasound characteristics of parathyroid adenomas vs. lymph nodes 4D-CT evaluation of hyperparathyroidism
Parathyroid Imaging: Current Concepts Maria Gule-Monroe, M.D. Nancy Perrier, M.D. Disclosures None Objectives Ultrasound characteristics of parathyroid adenomas vs. lymph nodes 4D-CT evaluation of hyperparathyroidism
Use of PTH at Point of Surgery for Non-Localized Cases of Hyperparathyoidism
 Use of PTH at Point of Surgery for Non-Localized Cases of Hyperparathyoidism Keck Hospital of USC Private, non-profit 400 bed hospital Teaching and research, USC Keck School of Medicine Approx. 40 parathyroid
Use of PTH at Point of Surgery for Non-Localized Cases of Hyperparathyoidism Keck Hospital of USC Private, non-profit 400 bed hospital Teaching and research, USC Keck School of Medicine Approx. 40 parathyroid
Southern Derbyshire Shared Care Pathology Guidelines. Primary Hyperparathyroidism
 Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
Southern Derbyshire Shared Care Pathology Guidelines Primary Hyperparathyroidism Please use this Guideline in Conjunction with the Hypercalcaemia Guideline Definition Driven by hyperfunction of one or
When the level of calcium in the blood falls too low, the parathyroid glands secrete just enough PTH to restore the blood calcium level.
 Hyperparathyroidism Primary hyperparathyroidism is a disorder of the parathyroid glands, also called parathyroids. Primary means this disorder originates in the parathyroids: One or more enlarged, overactive
Hyperparathyroidism Primary hyperparathyroidism is a disorder of the parathyroid glands, also called parathyroids. Primary means this disorder originates in the parathyroids: One or more enlarged, overactive
PTH > 60pg/ml PRIMARY HYPERPARATHYROIDISM. Introduction Biochemical Diagnosis. Normal Parathyroid. Parathyroid Glands
 next speaker: Declan Neeson Belfast/UK SPECT/CT scanning and parathyroid surgery in Southern Trust, N. Ireland D Neeson M Korda, G Gray, C Leonard, M Fawzy, R Lambon Parathyroid Glands PRIMARY HYPERPARATHYROIDISM
next speaker: Declan Neeson Belfast/UK SPECT/CT scanning and parathyroid surgery in Southern Trust, N. Ireland D Neeson M Korda, G Gray, C Leonard, M Fawzy, R Lambon Parathyroid Glands PRIMARY HYPERPARATHYROIDISM
O~iginalArtrc!~'" MINIMALLY INVASIVE RADIO-GUIDED PARATHYROIDECTOMY IN 152 CONSECUTIVE PATIENTS WITH PRIMARY HYPERPARATHYROIDISM
 O~iginalArtrc!~'",,_.~.~_.,_,,~_......_. ~.o:-'';:...:/-.~. ~'.:::.., MINIMALLY INVASIVE RADIO-GUIDED PARATHYROIDECTOMY IN 152 CONSECUTIVE PATIENTS WITH PRIMARY HYPERPARATHYROIDISM Douglas Politz, MD,
O~iginalArtrc!~'",,_.~.~_.,_,,~_......_. ~.o:-'';:...:/-.~. ~'.:::.., MINIMALLY INVASIVE RADIO-GUIDED PARATHYROIDECTOMY IN 152 CONSECUTIVE PATIENTS WITH PRIMARY HYPERPARATHYROIDISM Douglas Politz, MD,
ORIGINAL ARTICLE. Appearance of Ectopic Undescended Inferior Parathyroid Adenomas on Technetium Tc 99m Sestamibi Scintigraphy
 ORIGINAL ARTICLE Appearance of Ectopic Undescended Inferior Parathyroid Adenomas on Technetium Tc 99m Sestamibi Scintigraphy A Lesson From Reoperative Parathyroidectomy David Axelrod, MD; James C. Sisson,
ORIGINAL ARTICLE Appearance of Ectopic Undescended Inferior Parathyroid Adenomas on Technetium Tc 99m Sestamibi Scintigraphy A Lesson From Reoperative Parathyroidectomy David Axelrod, MD; James C. Sisson,
Endoscopic Parathyroidectomy: Why and When?
 World J Surg (2008) 32:2509 2515 DOI 10.1007/s00268-008-9709-3 Endoscopic Parathyroidectomy: Why and When? Jean-François Henry Æ Frédéric Sebag Æ Mariya Cherenko Æ Giuseppe Ippolito Æ David Taieb Æ Josiane
World J Surg (2008) 32:2509 2515 DOI 10.1007/s00268-008-9709-3 Endoscopic Parathyroidectomy: Why and When? Jean-François Henry Æ Frédéric Sebag Æ Mariya Cherenko Æ Giuseppe Ippolito Æ David Taieb Æ Josiane
301 S. Westfield Rd., Suite 250 Madison, WI See inside for information about our Endocrine Surgery Referral Program
 301 S. Westfield Rd., Suite 250 Madison, WI 53717 See inside for information about our Endocrine Surgery Referral Program December 2017 Dear Colleague, Thank you for referring your patient(s) to UW Health
301 S. Westfield Rd., Suite 250 Madison, WI 53717 See inside for information about our Endocrine Surgery Referral Program December 2017 Dear Colleague, Thank you for referring your patient(s) to UW Health
THYROID CANCER IN CHILDREN. Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine
 THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
Effect of open minimally invasive parathyroidectomy in the management of primary hyperparathyroidism
 International Surgery Journal Kumar SR et al. Int Surg J. 2017 Nov;4(11):3660-3664 http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Original Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20174881
International Surgery Journal Kumar SR et al. Int Surg J. 2017 Nov;4(11):3660-3664 http://www.ijsurgery.com pissn 2349-3305 eissn 2349-2902 Original Research Article DOI: http://dx.doi.org/10.18203/2349-2902.isj20174881
Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs
 Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs Shereen Ezzat, MD, FRCP(C), FACP Professor Of Medicine & Oncology Head, Endocrine Oncology Princess Margaret Hospital/University
Pituitary, Parathyroid Pheochromocytomas & Paragangliomas: The 4 Ps of NETs Shereen Ezzat, MD, FRCP(C), FACP Professor Of Medicine & Oncology Head, Endocrine Oncology Princess Margaret Hospital/University
New technologies in Endocrine Surgery
 New technologies in Endocrine Surgery 1. Nerve monitoring 2. New technologies in Endocrine Surgery Jessica E. Gosnell MD Post graduate course in General Surgery March 28, 2012 1 2 Recurrent laryngeal nerve
New technologies in Endocrine Surgery 1. Nerve monitoring 2. New technologies in Endocrine Surgery Jessica E. Gosnell MD Post graduate course in General Surgery March 28, 2012 1 2 Recurrent laryngeal nerve
Perioperative parathormone assessment during surgery for primary hyperparathyroidism;
 08. hoofdstuk 08 23-07-2001 09:52 Pagina 79 Perioperative parathormone assessment during surgery for primary hyperparathyroidism; Comparison of four techniques 8 Submitted for publication as Smit PC, Borel
08. hoofdstuk 08 23-07-2001 09:52 Pagina 79 Perioperative parathormone assessment during surgery for primary hyperparathyroidism; Comparison of four techniques 8 Submitted for publication as Smit PC, Borel
Supplementary Online Content
 Supplementary Online Content Wilhelm SM, Wang TS, Ruan DT, et al. The American Association of Endocrine Surgeons guidelines for definitive management of primary hyperparathyroidism. JAMA Surg. Published
Supplementary Online Content Wilhelm SM, Wang TS, Ruan DT, et al. The American Association of Endocrine Surgeons guidelines for definitive management of primary hyperparathyroidism. JAMA Surg. Published
THE PARATHYROID GLAND THEORY AND NUCLEAR MEDICINE PRACTICE
 THE PARATHYROID GLAND THEORY AND NUCLEAR MEDICINE PRACTICE George N. Sfakianakis MD Professor of Radiology and Pediatrics Director, Division of Nuclear Medicine UM/JMMC Miami FL October 2009 ENDONCRINE
THE PARATHYROID GLAND THEORY AND NUCLEAR MEDICINE PRACTICE George N. Sfakianakis MD Professor of Radiology and Pediatrics Director, Division of Nuclear Medicine UM/JMMC Miami FL October 2009 ENDONCRINE
ORIGINAL ARTICLE. An Optimal Algorithm for Intraoperative Parathyroid Hormone Monitoring
 ORIGINAL ARTICLE An Optimal Algorithm for Intraoperative Parathyroid Hormone Monitoring Melanie L. Richards, MD; Geoffrey B. Thompson, MD; David R. Farley, MD; Clive S. Grant, MD Background: A minimally
ORIGINAL ARTICLE An Optimal Algorithm for Intraoperative Parathyroid Hormone Monitoring Melanie L. Richards, MD; Geoffrey B. Thompson, MD; David R. Farley, MD; Clive S. Grant, MD Background: A minimally
Cases in Endocrinology
 Bones, Moans and Groans Diagnosing and Treating Primary Hyperparathyroidism By M. Usman Chaudhry, MD Table 1 Laboratory parameters Her bone density had osteopenic T-Scores of -2.3 at lumbar spine, and
Bones, Moans and Groans Diagnosing and Treating Primary Hyperparathyroidism By M. Usman Chaudhry, MD Table 1 Laboratory parameters Her bone density had osteopenic T-Scores of -2.3 at lumbar spine, and
Hyperparathyroidism February 2012
 TITLE: Hyperparathyroidism SOURCE: Grand Rounds Presentation, The University of Texas Medical Branch (UTMB Health) Department of Otolaryngology DATE: Feb 24, 2012 RESIDENT PHYSICIAN: Susan Edionwe, MD
TITLE: Hyperparathyroidism SOURCE: Grand Rounds Presentation, The University of Texas Medical Branch (UTMB Health) Department of Otolaryngology DATE: Feb 24, 2012 RESIDENT PHYSICIAN: Susan Edionwe, MD
Primary hyperparathyroidism
 How to Treat PULL-OUT SECTION Complete How to Treat quizzes online /cpd to earn CPD or PDP points. INSIDE Pathophysiology Clinical features Investigations Management Prognosis Special cases Case study
How to Treat PULL-OUT SECTION Complete How to Treat quizzes online /cpd to earn CPD or PDP points. INSIDE Pathophysiology Clinical features Investigations Management Prognosis Special cases Case study
CKD: Bone Mineral Metabolism. Peter Birks, Nephrology Fellow
 CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
CKD: Bone Mineral Metabolism Peter Birks, Nephrology Fellow CKD - KDIGO Definition and Classification of CKD CKD: abnormalities of kidney structure/function for > 3 months with health implications 1 marker
76 year-old female presents with muscle cramps. Jess Hwang 12/6/12
 76 year-old female presents with muscle cramps Jess Hwang 12/6/12 HPI Worked up for outpatient hypercalcemia Calcium had been 10.3-11.1, PTH ~120 No h/o osteoporosis, CKD, kidney stones Not taking calcium
76 year-old female presents with muscle cramps Jess Hwang 12/6/12 HPI Worked up for outpatient hypercalcemia Calcium had been 10.3-11.1, PTH ~120 No h/o osteoporosis, CKD, kidney stones Not taking calcium
ORIGINAL ARTICLE. Persistent Parathyroid Hormone Elevation Following Curative Parathyroidectomy for Primary Hyperparathyroidism
 Persistent Parathyroid Hormone Elevation Following Curative Parathyroidectomy for Primary Hyperparathyroidism Elizabeth A. Mittendorf, MD; Christopher R. McHenry, MD ORIGINAL ARTICLE Background: Persistent
Persistent Parathyroid Hormone Elevation Following Curative Parathyroidectomy for Primary Hyperparathyroidism Elizabeth A. Mittendorf, MD; Christopher R. McHenry, MD ORIGINAL ARTICLE Background: Persistent
Persistent post transplant hyperparathyroidism. Shiva Seyrafian IUMS-97/10/18-8/1/2019
 Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Persistent post transplant hyperparathyroidism Shiva Seyrafian IUMS-97/10/18-8/1/2019 normal weight =18-160 mg In HPT= 500-1000 mg 2 Epidemiology Mild 2 nd hyperparathyroidism (HPT) resolve after renal
Thyroid and Parathyroid Disease. RTC Conference Christina Edwards Bailey Faculty: Dr. Carmen Solorzano April 2, 2010
 Thyroid and Parathyroid Disease RTC Conference Christina Edwards Bailey Faculty: Dr. Carmen Solorzano April 2, 2010 Case Presentation # 1 CC: Neck Mass HPI: 51f found to have a neck mass on routine PE.
Thyroid and Parathyroid Disease RTC Conference Christina Edwards Bailey Faculty: Dr. Carmen Solorzano April 2, 2010 Case Presentation # 1 CC: Neck Mass HPI: 51f found to have a neck mass on routine PE.
Hypercalcemia. Hypercalcemia: When to Worry, When to Treat! Mineral Metabolism : A Short Course
 Hypercalcemia: When to Worry, When to Treat! Michael A. Levine has no financial relationships to disclose or Conflicts of Interest to resolve. Michael A. Levine, M.D. This presentation will not involve
Hypercalcemia: When to Worry, When to Treat! Michael A. Levine has no financial relationships to disclose or Conflicts of Interest to resolve. Michael A. Levine, M.D. This presentation will not involve
Primary hyperparathyroidism: review and recommendations on evaluation, diagnosis, and management. A Canadian and international consensus
 Primary hyperparathyroidism: review and recommendations on evaluation, diagnosis, and management. A Canadian and international consensus The Harvard community has made this article openly available. Please
Primary hyperparathyroidism: review and recommendations on evaluation, diagnosis, and management. A Canadian and international consensus The Harvard community has made this article openly available. Please
Role of Imaging in the Localization of Parathyroid Adenoma
 Role of Imaging in the Localization of Parathyroid Adenoma Authors S A Kabir 1, Z Khanzada 2, S I Akhtar 3, S I Kabir 4, N Wariach 1, 1. Department of Surgery, Lincoln County Hospital, Lincoln LN2 5QY,
Role of Imaging in the Localization of Parathyroid Adenoma Authors S A Kabir 1, Z Khanzada 2, S I Akhtar 3, S I Kabir 4, N Wariach 1, 1. Department of Surgery, Lincoln County Hospital, Lincoln LN2 5QY,
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life.
 B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
B. Environmental Factors. a. The major risk factor to papillary thyroid cancer is exposure to ionizing radiation, during the first 2 decades of life. b. Deficiency of dietary iodine: - Is linked with a
International Journal of Biological & Medical Research. An Uncommon Case of Persistent Hypercalcaemia following Parathyroid Surgery
 Int J Biol Med Res.2015;6(4):5336-5340 Int J Biol Med Res www.biomedscidirect.com Volume 6, Issue 2, April 2015 Contents lists available at BioMedSciDirect Publications International Journal of Biological
Int J Biol Med Res.2015;6(4):5336-5340 Int J Biol Med Res www.biomedscidirect.com Volume 6, Issue 2, April 2015 Contents lists available at BioMedSciDirect Publications International Journal of Biological
The Parathyroid Glands and Hyperparathyroidism: II
 GENERAL SURGERY BOARD REVIEW MANUAL PUBLISHING STAFF PRESIDENT, GROUP PUBLISHER Bruce M. White EXECUTIVE EDITOR Debra Dreger SENIOR EDITOR Miranda J. Hughes, PhD ASSISTANT EDITOR Melissa Frederick EDITORIAL
GENERAL SURGERY BOARD REVIEW MANUAL PUBLISHING STAFF PRESIDENT, GROUP PUBLISHER Bruce M. White EXECUTIVE EDITOR Debra Dreger SENIOR EDITOR Miranda J. Hughes, PhD ASSISTANT EDITOR Melissa Frederick EDITORIAL
SPECT/CT in Endocrine Diseases and Dosimetry
 SPECT/CT in Endocrine Diseases and Dosimetry Heather A. Jacene, MD Division of Nuclear Medicine Russell H. Morgan Dept. of Radiology and Radiological Science Johns Hopkins University Baltimore, MD Disclosures
SPECT/CT in Endocrine Diseases and Dosimetry Heather A. Jacene, MD Division of Nuclear Medicine Russell H. Morgan Dept. of Radiology and Radiological Science Johns Hopkins University Baltimore, MD Disclosures
Minimally Invasive Endocrine Surgery. How far have we come?
 Minimally Invasive Endocrine Surgery How far have we come? Introduction Minimally invasive surgery describes a field of surgery that crosses all traditional disciplines. It is not a discipline into itself
Minimally Invasive Endocrine Surgery How far have we come? Introduction Minimally invasive surgery describes a field of surgery that crosses all traditional disciplines. It is not a discipline into itself
Surgery for Primary Hyperparathyroidism
 Surgery for Primary Hyperparathyroidism Glenda G. Callender, MD; and Robert Udelsman, MD, MBA In the Western world, primary hyperparathyroidism is now a relatively common disorder that is diagnosed in
Surgery for Primary Hyperparathyroidism Glenda G. Callender, MD; and Robert Udelsman, MD, MBA In the Western world, primary hyperparathyroidism is now a relatively common disorder that is diagnosed in
Controversies in the treatment of primary hyperparathyroidism
 Controversies in the treatment of primary hyperparathyroidism Thier, Mark Published: 2016-01-01 Document Version: Publisher's PDF, also known as Version of record Link to publication Citation for published
Controversies in the treatment of primary hyperparathyroidism Thier, Mark Published: 2016-01-01 Document Version: Publisher's PDF, also known as Version of record Link to publication Citation for published
Re-explorative Parathyroid Surgery for Persistent and Recurrent Primary Hyperparathyroidism
 10.5005/jp-journals-10002-1070 ORIGINAL ARTICLE WJOES Re-explorative Parathyroid Surgery for Persistent and Recurrent Primary Hyperparathyroidism Rachel L O Connell, Karolina Afors, Martin H Thomas Ashford
10.5005/jp-journals-10002-1070 ORIGINAL ARTICLE WJOES Re-explorative Parathyroid Surgery for Persistent and Recurrent Primary Hyperparathyroidism Rachel L O Connell, Karolina Afors, Martin H Thomas Ashford
Health Sciences Centre, Team A, Dr. L. Bohacek (Endocrine Surgery) Medical Expert
 Medical Expert") Health Sciences Centre, Team A, Dr. L. Bohacek (Endocrine Surgery) Introduction Medical Expert This is a three month PGY 1-5 rotation in which residents gain exposure in the care and management of patients
Health Sciences Centre, Team A, Dr. L. Bohacek (Endocrine Surgery) Introduction Medical Expert This is a three month PGY 1-5 rotation in which residents gain exposure in the care and management of patients
Parathyroid surgery at Massachusetts General Hospital: Information for patients and families
 Parathyroid surgery at Massachusetts General Hospital: Information for patients and families We are pleased that you have chosen Massachusetts General Hospital to receive treatment for your parathyroid
Parathyroid surgery at Massachusetts General Hospital: Information for patients and families We are pleased that you have chosen Massachusetts General Hospital to receive treatment for your parathyroid
Preoperative Tc-99m-sestamibi (MIBI) scintigraphy and
 scintigraphy and") Otolaryngology Head and Neck Surgery (2006) 134, 316-320 ORIGINAL RESEARCH In Vivo Characterisation of Parathyroid Lesions by Use of Gamma Probe: Comparison With Ex Vivo Count Method and Frozen Section
Otolaryngology Head and Neck Surgery (2006) 134, 316-320 ORIGINAL RESEARCH In Vivo Characterisation of Parathyroid Lesions by Use of Gamma Probe: Comparison With Ex Vivo Count Method and Frozen Section
Case study Group 2 presentation
 Case study Group 2 presentation Patient profile HN 3095-57 Female 60 years old Hometown : Sa Kaeo province Occupation : farmer No drug and food allergy Chief complain Left neck mass 10 years PTA that gradually
Case study Group 2 presentation Patient profile HN 3095-57 Female 60 years old Hometown : Sa Kaeo province Occupation : farmer No drug and food allergy Chief complain Left neck mass 10 years PTA that gradually
A large parathyroid adenoma presenting with pathological fractures in a young male
 International Journal of Otorhinolaryngology and Head and Neck Surgery http://www.ijorl.com pissn 2454-5929 eissn 2454-5937 Case Report DOI: http://dx.doi.org/10.18203/issn.2454-5929.ijohns20150907 A large
International Journal of Otorhinolaryngology and Head and Neck Surgery http://www.ijorl.com pissn 2454-5929 eissn 2454-5937 Case Report DOI: http://dx.doi.org/10.18203/issn.2454-5929.ijohns20150907 A large
Secondary Hyperparathyroidism: Where are we now?
 Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Secondary Hyperparathyroidism: Where are we now? Dylan M. Barth, Pharm.D. PGY-1 Pharmacy Resident Mayo Clinic 2017 MFMER slide-1 Objectives Identify risk factors for the development of complications caused
Cost-analysis of minimally invasive surgery and conventional neck exploration for primary
 09. hoofdstuk 09 23-07-2001 09:51 Pagina 91 Cost-analysis of minimally invasive surgery and conventional neck exploration for primary hyperparathyroidism 9 Submitted for publication as Smit PC, Liem MSL,
09. hoofdstuk 09 23-07-2001 09:51 Pagina 91 Cost-analysis of minimally invasive surgery and conventional neck exploration for primary hyperparathyroidism 9 Submitted for publication as Smit PC, Liem MSL,
Ultrasound Evaluation of Hyperparathyroidism
 Ultrasound Evaluation of Hyperparathyroidism OBJECTIVES: 1. Why use US for localization? Advanced US course, Orlando, Florida September, 2018 2. Review the US findings and features of parathyroid adenomas
Ultrasound Evaluation of Hyperparathyroidism OBJECTIVES: 1. Why use US for localization? Advanced US course, Orlando, Florida September, 2018 2. Review the US findings and features of parathyroid adenomas
Minimally invasive parathyroid surgery
 Review Article Minimally invasive parathyroid surgery Salem I. Noureldine, Zhen Gooi, Ralph P. Tufano Division of Head and Neck Endocrine Surgery, Department of Otolaryngology, Head and Neck Surgery, Johns
Review Article Minimally invasive parathyroid surgery Salem I. Noureldine, Zhen Gooi, Ralph P. Tufano Division of Head and Neck Endocrine Surgery, Department of Otolaryngology, Head and Neck Surgery, Johns
The disease spectrum in primary hyperparathyroidism
 Original Article Symptomatic Primary Hyperparathyroidism : A Retrospective Analysis of Fifty One Cases from a Single Centre J Muthukrishnan*, Sangeeta Jha*, KD Modi*, R Jha**, J Kumar**, A Verma*, KVS
Original Article Symptomatic Primary Hyperparathyroidism : A Retrospective Analysis of Fifty One Cases from a Single Centre J Muthukrishnan*, Sangeeta Jha*, KD Modi*, R Jha**, J Kumar**, A Verma*, KVS
Challenges in the Management of Primary HPTH. Zaher Ajam, MD Ghada El-Hajj Fuleihan, MD, MPH
 Challenges in the Management of Primary HPTH Zaher Ajam, MD Ghada El-Hajj Fuleihan, MD, MPH Case Presentation 1 This a case of a 41-year-old gentleman who is referred to Endocrinology clinic for low BMD,
Challenges in the Management of Primary HPTH Zaher Ajam, MD Ghada El-Hajj Fuleihan, MD, MPH Case Presentation 1 This a case of a 41-year-old gentleman who is referred to Endocrinology clinic for low BMD,
Thyroid Ultrasound for the Endocrine Surgeon: A Valuable Clinical Tool that Enhances Diagnostic and Therapeutic Outcomes
 Thyroid Ultrasound for the Endocrine Surgeon: A Valuable Clinical Tool that Enhances Diagnostic and Therapeutic Outcomes Allan Siperstein MD The Cleveland Clinic Audience Quiz Taken ultrasound course Perform
Thyroid Ultrasound for the Endocrine Surgeon: A Valuable Clinical Tool that Enhances Diagnostic and Therapeutic Outcomes Allan Siperstein MD The Cleveland Clinic Audience Quiz Taken ultrasound course Perform
JMSCR Vol 04 Issue 04 Page April 2016
 www.jmscr.igmpublication.org Impact Factor 5.244 Index Copernicus Value: 5.88 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: http://dx.doi.org/10.18535/jmscr/v4i4.23 Persistence and Cure Rates of Primary Hyperparathyroid
www.jmscr.igmpublication.org Impact Factor 5.244 Index Copernicus Value: 5.88 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: http://dx.doi.org/10.18535/jmscr/v4i4.23 Persistence and Cure Rates of Primary Hyperparathyroid
ORIGINAL ARTICLE. Sestamibi Scans and Intraoperative Parathyroid Hormone Measurement in the Treatment of Primary Hyperparathyroidism
 ORIGINAL ARTICLE Sestamibi Scans and Intraoperative Parathyroid Hormone Measurement in the Treatment of Primary Hyperparathyroidism Eric J. Bergson, MD; Laura A. Sznyter, MD; Sanford Dubner, MD; Christopher
ORIGINAL ARTICLE Sestamibi Scans and Intraoperative Parathyroid Hormone Measurement in the Treatment of Primary Hyperparathyroidism Eric J. Bergson, MD; Laura A. Sznyter, MD; Sanford Dubner, MD; Christopher
Parathyroidectomy. Surgery for Parathyroid Problems
 Parathyroidectomy Surgery for Parathyroid Problems Why You Need Parathyroid Surgery Has your doctor just recommended that you have parathyroid surgery? If so, you likely have many questions. What are the
Parathyroidectomy Surgery for Parathyroid Problems Why You Need Parathyroid Surgery Has your doctor just recommended that you have parathyroid surgery? If so, you likely have many questions. What are the
SINGLE INCISION ENDOSCOPIC SURGERY (SIES)
") EAES CONSENSUS CONFERENCE SINGLE INCISION ENDOSCOPIC SURGERY (SIES) STATEMENTS AND RECOMMENDATIONS EAES appreciates your input! Please give your opinion on the below statements and recommendations of the
EAES CONSENSUS CONFERENCE SINGLE INCISION ENDOSCOPIC SURGERY (SIES) STATEMENTS AND RECOMMENDATIONS EAES appreciates your input! Please give your opinion on the below statements and recommendations of the
Optimizing the Minimally Invasive Approach to Mediastinal Parathyroid Adenomas
 Optimizing the Minimally Invasive Approach to Mediastinal Parathyroid Adenomas Benjamin Wei, MD, William Inabnet, MD, James A. Lee, MD, and Joshua R. Sonett, MD Division of Cardiothoracic Surgery, Duke
Optimizing the Minimally Invasive Approach to Mediastinal Parathyroid Adenomas Benjamin Wei, MD, William Inabnet, MD, James A. Lee, MD, and Joshua R. Sonett, MD Division of Cardiothoracic Surgery, Duke
Current Issues in Thyroid Cancer Surgery in 2017
 Current Issues in Thyroid Cancer Surgery in 2017 Dr. David Goldstein MD Msc FRCSC FACS Associate Professor, Department Otolaryngology Head & Neck Surgery, U of T Department of Surgical Oncology, Princess
Current Issues in Thyroid Cancer Surgery in 2017 Dr. David Goldstein MD Msc FRCSC FACS Associate Professor, Department Otolaryngology Head & Neck Surgery, U of T Department of Surgical Oncology, Princess
Endocrine University 2016 AACE-ACE-MAYO CLINIC
 Endocrine University 2016 AACE-ACE-MAYO CLINIC Dev Abraham MD, MRCP (UK), ECNU Professor of Medicine (clinical), Division of Endocrinology Adjunct Professor of Surgery and Pathology Medical Director, Utah
Endocrine University 2016 AACE-ACE-MAYO CLINIC Dev Abraham MD, MRCP (UK), ECNU Professor of Medicine (clinical), Division of Endocrinology Adjunct Professor of Surgery and Pathology Medical Director, Utah
Calcium Nephrolithiasis and Bone Health. Noah S. Schenkman, MD
 Calcium Nephrolithiasis and Bone Health Noah S. Schenkman, MD Associate Professor of Urology and Residency Program Director, University of Virginia Health System; Charlottesville, Virginia Objectives:
Calcium Nephrolithiasis and Bone Health Noah S. Schenkman, MD Associate Professor of Urology and Residency Program Director, University of Virginia Health System; Charlottesville, Virginia Objectives:
Endocrine Surgery When to Refer and What We Do
 Endocrine Surgery When to Refer and What We Do None Disclosures W. Heath Giles, M.D., F.A.C.S. Surgery Residency Program Director Assistant Professor of Surgery What is Endocrine Surgery? Who performs
Endocrine Surgery When to Refer and What We Do None Disclosures W. Heath Giles, M.D., F.A.C.S. Surgery Residency Program Director Assistant Professor of Surgery What is Endocrine Surgery? Who performs
IMPACT OF CONCOMITANT THYROID PATHOLOGY ON PREOPERATIVE WORKUP FOR PRIMARY HYPERPARATHYROIDISM
 January 28, 2009 EUROPEAN JOURNAL OF MEDICAL RESEARCH 37 Eur J Med Res (2009) 14: 37-41 I. Holzapfel Publishers 2009 IMPACT OF CONCOMITANT THYROID PATHOLOGY ON PREOPERATIVE WORKUP FOR PRIMARY HYPERPARATHYROIDISM
January 28, 2009 EUROPEAN JOURNAL OF MEDICAL RESEARCH 37 Eur J Med Res (2009) 14: 37-41 I. Holzapfel Publishers 2009 IMPACT OF CONCOMITANT THYROID PATHOLOGY ON PREOPERATIVE WORKUP FOR PRIMARY HYPERPARATHYROIDISM
Case Report A Reference Finding Rarely Seen in Primary Hyperparathyroidism: Brown Tumor
 Case Reports in Medicine Volume 2012, Article ID 432676, 4 pages doi:10.1155/2012/432676 Case Report A Reference Finding Rarely Seen in Primary Hyperparathyroidism: Brown Tumor F. Mantar, 1 S. Gunduz,
Case Reports in Medicine Volume 2012, Article ID 432676, 4 pages doi:10.1155/2012/432676 Case Report A Reference Finding Rarely Seen in Primary Hyperparathyroidism: Brown Tumor F. Mantar, 1 S. Gunduz,
Patient Information Leaflet P1
 Patient Information Leaflet P1 Parathyroid Operations in Adults What are the Parathyroid glands and what do they do? Usually, you have four parathyroid glands. These are located between the thyroid gland
Patient Information Leaflet P1 Parathyroid Operations in Adults What are the Parathyroid glands and what do they do? Usually, you have four parathyroid glands. These are located between the thyroid gland