Presentation of Cases /Audience Voting/Panel/Discussion
|
|
|
- Allison Day
- 5 years ago
- Views:
Transcription

1


2 Presentation of Cases /Audience Voting/Panel/Discussion JJ Patard Tim O Brien Ninth European International Kidney Cancer Symposium Dublin April 2014
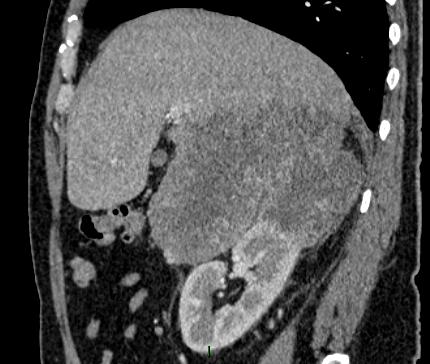
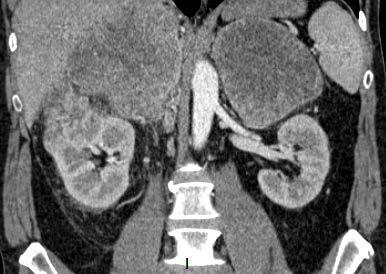
3 Clinical case 1 63 years old women Medical past history: TVT for stress urinary incontinence Incidental discovery of synchronous bilateral renal tumors Right upper pole T: 13mm Left upper pole T: 37mm Baseline Creatinine: 0.8 mg/dl Baseline MDRD GFR: 93 ml/mins








4
5 Voting questions for the audience 1. No biopsy, Partial nephrectomy on both sides? 2. Bilateral Biopsies, Partial nephrectomy on both sides? 3. No biopsy, Right partial nephrectomy and left radical nephrectomy? 4. Bilateral Biopsies, Right partial nephrectomy and left radical nephrectomy? 5. No biopsies, RFA or CA on both sides? 6. Bilateral biopsies, RFA or CA on both sides?
6 Questions for the panel 1. CT or US guided biopsies? (R?, L?, both?) 2. Upfront partial nephrectomy (R first?, L first?, both in a unique procedure?) 3. Would you consider a radical NX on the left side? 4. What approach for PN: open/lap/robot? 5. In case of ablation TT what would be your first choice: RFA or Cryo (R, L)?
7 Decision: right PN first (without Bx) Robotic PN WIT: 16 min Estimated blood loss <50cc Uneventful post operative course LHS: 3 D Post op creatinine 0.7 mg/dl Post op GFR 83 ml/min Histology: Angiomyolipoma
8 Left Side: Questions for the panel 1. CT or US guided biopsies? 2. Left partial nephrectomy without BX? 3. Left Radical Nx? 4. What approach for PN: open/lap/robot? 5. In case of ablation TT what would be your first choice: RFA or Cryo?
9 Decision: left PN(without Bx) Based on different radiologic features for the left T we decided Robotic left PN (2 months after right side) WIT: 20 min Blood loss <50cc Uneventful post operative course LHS: 3 D Post op creatinine 0.78 mg/dl Post op GFR 74 ml/min Histology: clear cell carcinoma, Fuhrman grade 2, T1a, NxM0, R0.
10 Clinical case 2 62 years old women Right partial nephrectomy in 2000 (CCRCC) Right radical nephrectomy in 2011 for local recurrence (CCRCC) May 2013, tumor 23mm on the left side Baseline Creatinine: 0.97 mg/dl Baseline MDRD GFR: 58 ml/min




11
12 Voting questions for the audience 1. Biopsy and Partial nephrectomy 2. No Biopsy and Partial nephrectomy 3. Biopsy and RFA or CA 4. No Biopsy and RFA or CA 5. Upfront radical Nx and dialysis
13 Questions for the panel 1. CT or US guided biopsies before any kind of TT? 2. Partial nephrectomy 1. OPN, LPN, RPN? 2. trans vs RP approach? 3. Main artery clamping vs hyperselective art. clamp? 3. RFA or CA? 4. What would you do for a new unique recurrence 1 year later? 1. PN again? 2. RFA or cryo? 3. Radical nephrectomy?
14 Decision: left RPN without Bx Retropéritoneal approch Main Renal artery clamping time: 8 min Uneventful post operative course LHS: 3 d 3 months post op creatinine 1.1 mg/dl Post op GFR 50 ml/min Histology: clear cell carcinoma, Fuhrman grade 1, T1a, NxM0, R0.
15 Clinical case 3 45 yrs old man No medical past history Incidental diagnosis of bilateral adrenal masses and right renal tumor No distant metastases ECOG 0

16
17 Voting questions for the audience 1. Clinical trial (Bx, neoadjuvant TT followed by surgery) 2. Systemic treatment with no upfront surgery (Bx, treat and see what happens) 3. No bx, Right radical nephrectomy and adrenalectomy (open) and left adrenalectomy 1 month later (lap) 4. No Bx, Right radical nephrectomy and bilateral adrenalectomy (open)
18 Questions for the panel 1. Clinical trial (Bx, neoadjuvant TT followed by surgery) 2. Systemic treatment with no upfront surgery (Bx, treat and see what happens) 3. Right radical nephrectomy and adrenalectomy (open) and left adrenalectomy 1 month later (lap) 4. Right radical nephrectomy and bilateral adrenalectomy (open)
19 The patient was included in the Neorad trial (everolimus 2 months followed by surgery) No effect on tumor masses Complete resection of abdominal tumors Bx and final pathology: pt4, type II pap carc, R0 Local recurrence and distant mets 3 months later Progressed (CNS, liver, lung), refractory to TKI Died 5 months following surgery
20 Clinical case 4 52 yrs old Male patient No medical past history Left flank pain Left renal mass with major nodal invasion No distant metastases
21 Voting questions for the audience 1. Bx, Systemic treatment without nephrectomy? 2. No Bx, Left nephrectomy without LND followed by systemic treatment? 3. No Bx, Left nephrectomy and extensive LND 4. Bx, Neoadjuvant treatment before Left nephrectomy and extensive LND
22 Questions for the panel 1. CT or US guided biopsies before any kind of TT? 2. Systemic treatment without nephrectomy? 3. Left nephrectomy without LND followed by systemic treatment? 4. Left nephrectomy and extensive LND 5. Neoadjuvant treatment before Left nephrectomy and extensive LND





23 Combining surgery and targeted therapy The patient recurred locally 18 months later Remained stable or slowly progressive during 2 yrs with sunitinib He died 4 years later from multi visceral metastases
24
Complex case Presentations
 Complex case Presentations Case Presentations April 2016 Lisa M Pickering Case presentations: chromophobe renal carcinoma 60 year old man. ECOG PS 0 No significant comorbodities August 2009: L radical
Complex case Presentations Case Presentations April 2016 Lisa M Pickering Case presentations: chromophobe renal carcinoma 60 year old man. ECOG PS 0 No significant comorbodities August 2009: L radical
Challenges in RCC surgery. Treatment Goals. Surgical challenges. Management options in VHL associated RCCs
 Management options in VHL associated RCCs Challenges in RCC surgery JJ PATARD, MD, PhD Paris XI University Observation, Radical nephrectomy, Renal parenchymal sparing surgery, Open, laparoscopic, robotic
Management options in VHL associated RCCs Challenges in RCC surgery JJ PATARD, MD, PhD Paris XI University Observation, Radical nephrectomy, Renal parenchymal sparing surgery, Open, laparoscopic, robotic
Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute
 Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 23 March 2012, Sao Paulo, Brazil Surgery of RCC Locally confined (small) renal tumours Locally advanced disease Metastatic
Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 23 March 2012, Sao Paulo, Brazil Surgery of RCC Locally confined (small) renal tumours Locally advanced disease Metastatic
Indications For Partial
 Indications For Partial Nephrectomy Christopher G. Wood, M. D., FACS Professor and Deputy Chairman Douglas E. Johnson, M. D. Endowed Professorship in Urology Department of Urology The University of Texas
Indications For Partial Nephrectomy Christopher G. Wood, M. D., FACS Professor and Deputy Chairman Douglas E. Johnson, M. D. Endowed Professorship in Urology Department of Urology The University of Texas
Who are Candidates for Laparoscopic or Open Radical Nephrectomy. Arieh Shalhav
 Who are Candidates for Laparoscopic or Open Radical Nephrectomy Arieh Shalhav Fritz Duda Chair of Urologic Surgery Professor of Surgery and the Comprehensive Cancer Research Center Who are Candidates for
Who are Candidates for Laparoscopic or Open Radical Nephrectomy Arieh Shalhav Fritz Duda Chair of Urologic Surgery Professor of Surgery and the Comprehensive Cancer Research Center Who are Candidates for
Management of Locally Reccurent Renal Cell Carcinoma. Jose A. Karam, MD, FACS Assistant Professor Department of Urology
 Management of Locally Reccurent Renal Cell Carcinoma Jose A. Karam, MD, FACS Assistant Professor Department of Urology DefiniAons Defini&ve treatment Aiming for cure Abla&on therapy Radiofrequency abla&on
Management of Locally Reccurent Renal Cell Carcinoma Jose A. Karam, MD, FACS Assistant Professor Department of Urology DefiniAons Defini&ve treatment Aiming for cure Abla&on therapy Radiofrequency abla&on
John Fitzpatrick Memorial Lecture. John Fitzpatrick Memorial lecture
 John Fitzpatrick Memorial Lecture John Fitzpatrick Memorial Lecture John M Fitzpatrick, 1948 2014 Head of Research at the Irish Cancer Society Professor of Surgery and Consultant Urologist at the Mater
John Fitzpatrick Memorial Lecture John Fitzpatrick Memorial Lecture John M Fitzpatrick, 1948 2014 Head of Research at the Irish Cancer Society Professor of Surgery and Consultant Urologist at the Mater
Vincenzo Ficarra 1,2,3. Associate Editor BJU International
 Partial Nephrectomy for RCC Vincenzo Ficarra 1,2,3 1 Director Department of Urology University of Udine, Italy 2 Associate Editor BJU International 3 Scientific Director OLV Robotic Surgery Institute,
Partial Nephrectomy for RCC Vincenzo Ficarra 1,2,3 1 Director Department of Urology University of Udine, Italy 2 Associate Editor BJU International 3 Scientific Director OLV Robotic Surgery Institute,
WHAT IS THE ROLE OF ACTIVE SURVEILLANCE
 WHAT IS THE ROLE OF ACTIVE SURVEILLANCE IN THE CONTEXT OF RENAL ABLATION AND PARTIAL NEPHRECTOMY? Alessandro Volpe University of Eastern Piedmont Novara, Italy RCC INCIDENCE SEER DATABASE (1975-2006) RCC
WHAT IS THE ROLE OF ACTIVE SURVEILLANCE IN THE CONTEXT OF RENAL ABLATION AND PARTIAL NEPHRECTOMY? Alessandro Volpe University of Eastern Piedmont Novara, Italy RCC INCIDENCE SEER DATABASE (1975-2006) RCC
Is renal cryoablation becoming an effective alternative to partial nephrectomy?
 Is renal cryoablation becoming an effective alternative to partial nephrectomy? J GARNON 1, G TSOUMAKIDOU 1, H LANG 2, A GANGI 1 1 department of interventional radiology 2 department of urology University
Is renal cryoablation becoming an effective alternative to partial nephrectomy? J GARNON 1, G TSOUMAKIDOU 1, H LANG 2, A GANGI 1 1 department of interventional radiology 2 department of urology University
Surgical Management of Renal Cancer. David Nicol Consultant Urologist
 Surgical Management of Renal Cancer David Nicol Consultant Urologist Roles of Surgery 1. Curative intervention localised disease 2. Symptomatic control advanced disease 3. Augmentation of efficacy of systemic
Surgical Management of Renal Cancer David Nicol Consultant Urologist Roles of Surgery 1. Curative intervention localised disease 2. Symptomatic control advanced disease 3. Augmentation of efficacy of systemic
GUIDELINES ON RENAL CELL CARCINOMA
 GUIDELINES ON RENAL CELL CARCINOMA B. Ljungberg (chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction This EAU guideline was prepared to help urologists
GUIDELINES ON RENAL CELL CARCINOMA B. Ljungberg (chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction This EAU guideline was prepared to help urologists
Guidelines on Renal Cell
 Guidelines on Renal Cell Carcinoma (Text update March 2009) B. Ljungberg (Chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction Renal cell carcinoma
Guidelines on Renal Cell Carcinoma (Text update March 2009) B. Ljungberg (Chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction Renal cell carcinoma
Clinical/Surgical trials that will change my practice
 Clinical/Surgical trials that will change my practice Mr Jim M Adshead Herts and Beds Urological Cancer Centre, Lister Hospital What s changed and where do I feel we are clutching at straws? Regional Specialist
Clinical/Surgical trials that will change my practice Mr Jim M Adshead Herts and Beds Urological Cancer Centre, Lister Hospital What s changed and where do I feel we are clutching at straws? Regional Specialist
RCC in ADPKD / CKD / ESRD
 RCC in ADPKD / CKD / ESRD FOIU 2018 David A. Goldfarb, MD,FACS Professor of Surgery, Cleveland Clinic Lerner College of Medicine Glickman Urological and Kidney Institute Cleveland Clinic, Cleveland, Ohio
RCC in ADPKD / CKD / ESRD FOIU 2018 David A. Goldfarb, MD,FACS Professor of Surgery, Cleveland Clinic Lerner College of Medicine Glickman Urological and Kidney Institute Cleveland Clinic, Cleveland, Ohio
Recent Developments in Research on Kidney Cancer: Highlights from Urological and Oncological Congresses in 2007
 european urology supplements 7 (2008) 494 507 available at www.sciencedirect.com journal homepage: www.europeanurology.com Recent Developments in Research on Kidney Cancer: Highlights from Urological and
european urology supplements 7 (2008) 494 507 available at www.sciencedirect.com journal homepage: www.europeanurology.com Recent Developments in Research on Kidney Cancer: Highlights from Urological and
RCC in Adolescents and Young Adults (AYAs): Diagnosis and Management
: Diagnosis and Management") RCC in Adolescents and Young Adults (AYAs): Diagnosis and Management Nicholas G. Cost, M.D. Assistant Professor, Department of Surgery, Division of Urology University of Colorado Cancer Center Fifteenth
RCC in Adolescents and Young Adults (AYAs): Diagnosis and Management Nicholas G. Cost, M.D. Assistant Professor, Department of Surgery, Division of Urology University of Colorado Cancer Center Fifteenth
Debate: Lymphadenectomy is Important in mrcc, CON P. Mulder, M.D., Ph.D. JJ. Patard, MD, Ph.D.
 Debate: Lymphadenectomy is Important in mrcc, CON P. Mulder, M.D., Ph.D. JJ. Patard, MD, Ph.D.. Eighth European International Kidney Cancer Symposium Budapest 03-04 May 2013 The role of LND In organ confined
Debate: Lymphadenectomy is Important in mrcc, CON P. Mulder, M.D., Ph.D. JJ. Patard, MD, Ph.D.. Eighth European International Kidney Cancer Symposium Budapest 03-04 May 2013 The role of LND In organ confined
Partial Nephrectomy Planning: Everybody s s doing it, you can to
 Partial Nephrectomy Planning: Everybody s s doing it, you can to Brian R. Herts, MD Associate Professor of Radiology Head, Abdominal Imaging, Imaging Institute & Staff, The Glickman Urological and Kidney
Partial Nephrectomy Planning: Everybody s s doing it, you can to Brian R. Herts, MD Associate Professor of Radiology Head, Abdominal Imaging, Imaging Institute & Staff, The Glickman Urological and Kidney
Guidelines for the Management of Renal Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Renal Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Renal Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Prostate Case Scenario 1
 Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
EAU GUIDELINES ON RENAL CELL CARCINOMA
 EAU GUIDELINES ON RENAL ELL ARINOMA (Limited text update March 2016) B. Ljungberg (hair), K. Bensalah, A. Bex (Vice-chair), S. anfield, R.H. Giles (Patient Organisation Representative), M. Hora, M.A. Kuczyk,
EAU GUIDELINES ON RENAL ELL ARINOMA (Limited text update March 2016) B. Ljungberg (hair), K. Bensalah, A. Bex (Vice-chair), S. anfield, R.H. Giles (Patient Organisation Representative), M. Hora, M.A. Kuczyk,
1/25/13 Right partial nephrectomy followed by completion right radical nephrectomy.
 History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
Should the primary be treated in patients with metastatic disease? Upper Tract Urothelial Cancer
 Should the primary be treated in patients with metastatic disease? Upper Tract Urothelial Cancer Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology
Should the primary be treated in patients with metastatic disease? Upper Tract Urothelial Cancer Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology
Section Activity Activity Description Details Reference(s)
") Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with Renal Cell Carcinoma AA Cancer Centre Referrals Not routine pre-op referral indicated
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with Renal Cell Carcinoma AA Cancer Centre Referrals Not routine pre-op referral indicated
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
Supplementary Table 2. Surgical prophylaxis: Summary of selected series which included prophylactic management against the risk of bleeding.
 Supplementary Tables of the article The Risks of Renal Angiomyolipoma: Reviewing the Evidence. Supplementary Table 2. Surgical prophylaxis: Summary of selected series which included prophylactic management
Supplementary Tables of the article The Risks of Renal Angiomyolipoma: Reviewing the Evidence. Supplementary Table 2. Surgical prophylaxis: Summary of selected series which included prophylactic management
Killing Tumors with Scans Not Scalpels: Kidney Cancer Ablation. Basics. What is Percutaneous Ablation? Where are your kidneys?
 Killing Tumors with Scans Not Scalpels: Kidney Cancer Ablation Ronald J. Zagoria, M.D. UCSF Professor and Vice Chair Abdominal Imaging Section Chief Basics Where are your kidneys? What is ablation? Facts
Killing Tumors with Scans Not Scalpels: Kidney Cancer Ablation Ronald J. Zagoria, M.D. UCSF Professor and Vice Chair Abdominal Imaging Section Chief Basics Where are your kidneys? What is ablation? Facts
What is the role of partial nephrectomy in the context of active surveillance and renal ablation?
 What is the role of partial nephrectomy in the context of active surveillance and renal ablation? Dogu Teber Department of Urology University Hospital Heidelberg Coming from Heidelberg obligates to speak
What is the role of partial nephrectomy in the context of active surveillance and renal ablation? Dogu Teber Department of Urology University Hospital Heidelberg Coming from Heidelberg obligates to speak
Surgical Management of VHL-related Renal Cancers. Disclosures. Glossary. Overview. none
 Surgical Management of VHL-related Renal Cancers Disclosures Presentation to the VHL Family Alliance Annual Meeting, Denver, CO October 20, 2018 none Adam R. Metwalli, M.D. Professor & Chief, Division
Surgical Management of VHL-related Renal Cancers Disclosures Presentation to the VHL Family Alliance Annual Meeting, Denver, CO October 20, 2018 none Adam R. Metwalli, M.D. Professor & Chief, Division
The Incidental Renal Mass in the Primary Care Setting
 The Incidental Renal Mass in the Primary Care Setting Adele M. Caruso, MSN, CRNP Adult Nurse Practitioner The Perelman School of Medicine at the University of Pennsylvania Abstract There are approximately
The Incidental Renal Mass in the Primary Care Setting Adele M. Caruso, MSN, CRNP Adult Nurse Practitioner The Perelman School of Medicine at the University of Pennsylvania Abstract There are approximately
Surgeons Perspective: LN as a Draining Pattern. Jose A. Karam, MD, FACS Associate Professor Department of Urology
 Surgeons Perspective: LN as a Draining Pattern Jose A. Karam, MD, FACS Associate Professor Department of Urology Disclosures EMD Serono, Pfizer, Novartis: Advisory board/consultant Disclosures I perform
Surgeons Perspective: LN as a Draining Pattern Jose A. Karam, MD, FACS Associate Professor Department of Urology Disclosures EMD Serono, Pfizer, Novartis: Advisory board/consultant Disclosures I perform
Renal Cell Cancer. Clinical case study 1 & 2. Petri Bono MD PhD Helsinki University Hospital Helsinki, Finland
 Renal Cell Cancer Clinical case study 1 & 2 Petri Bono MD PhD Helsinki University Hospital Helsinki, Finland 1 Case study 1 - RCC and Lung Metastases Case study 1: Patient History Male, 63 years old Mild
Renal Cell Cancer Clinical case study 1 & 2 Petri Bono MD PhD Helsinki University Hospital Helsinki, Finland 1 Case study 1 - RCC and Lung Metastases Case study 1: Patient History Male, 63 years old Mild
Lymphadenectomy in RCC: Yes, No, Clinical Trial?
 Lymphadenectomy in RCC: Yes, No, Clinical Trial? Viraj Master MD PhD FACS Professor Associate Chair for Clinical Affairs and Quality Director of Clinical Research Unit Department of Urology Emory University
Lymphadenectomy in RCC: Yes, No, Clinical Trial? Viraj Master MD PhD FACS Professor Associate Chair for Clinical Affairs and Quality Director of Clinical Research Unit Department of Urology Emory University
Arieh L. Shalhav Is There a Risk in Robotic Nephroureterectomy?
 Arieh L. Shalhav Is There a Risk in Robotic Nephroureterectomy? 80 patients LNU (n = 40) or ONU (n = 40) CSS (p = 0.2), BRFS (p = 0.86), MFS (p = 0.12) similar for the entire cohort Subgroups of pt3 UTUC
Arieh L. Shalhav Is There a Risk in Robotic Nephroureterectomy? 80 patients LNU (n = 40) or ONU (n = 40) CSS (p = 0.2), BRFS (p = 0.86), MFS (p = 0.12) similar for the entire cohort Subgroups of pt3 UTUC
Manchester Cancer. Guidelines for the management of renal cancer
 Guidelines for the management of renal cancer Approved by the urology pathway board September 2014 To be reviewed September 2016 Renal Cancer Guidelines 1. Introduction 1.1 Kidney cancer accounts for 3%
Guidelines for the management of renal cancer Approved by the urology pathway board September 2014 To be reviewed September 2016 Renal Cancer Guidelines 1. Introduction 1.1 Kidney cancer accounts for 3%
Renal Mass Biopsy: Needed Now More than Ever
 Renal Mass Biopsy: Needed Now More than Ever Stuart G. Silverman, MD, FACR Professor of Radiology Harvard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Boston,
Renal Mass Biopsy: Needed Now More than Ever Stuart G. Silverman, MD, FACR Professor of Radiology Harvard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Boston,
Management of High Risk Renal Cell Carcinoma
 Management of High Risk Renal Cell Carcinoma Peter E. Clark, MD Professor and Chair, Department of Urology Carolinas HealthCare System Chair, Urologic Oncology Levine Cancer Institute October 14, 2017
Management of High Risk Renal Cell Carcinoma Peter E. Clark, MD Professor and Chair, Department of Urology Carolinas HealthCare System Chair, Urologic Oncology Levine Cancer Institute October 14, 2017
Patient Selection for Surgery in RCC with Thrombus. E. Jason Abel, M.D.
 Patient Selection for Surgery in RCC with Thrombus E. Jason Abel, M.D. RCC with venous invasion Venous invasion occurs in ~10% of RCC Surgery more complex Increased risk for morbidity Thrombus may be confined
Patient Selection for Surgery in RCC with Thrombus E. Jason Abel, M.D. RCC with venous invasion Venous invasion occurs in ~10% of RCC Surgery more complex Increased risk for morbidity Thrombus may be confined
RENAL CANCER GUIDELINES
 Greater Manchester and Cheshire Cancer Network RENAL CANCER GUIDELINES Agreed by Urology CSG: July 2010 Review Date: July 2012 Renal Cancer Guidelines 1. Introduction 1.1 Kidney cancer accounts for 3%
Greater Manchester and Cheshire Cancer Network RENAL CANCER GUIDELINES Agreed by Urology CSG: July 2010 Review Date: July 2012 Renal Cancer Guidelines 1. Introduction 1.1 Kidney cancer accounts for 3%
GUIDELINES ON RENAL CELL CANCER
 20 G. Mickisch (chairman), J. Carballido, S. Hellsten, H. Schulze, H. Mensink Eur Urol 2001;40(3):252-255 Introduction is characterised by a constant rise in incidence over the last 50 years, with a predominance
20 G. Mickisch (chairman), J. Carballido, S. Hellsten, H. Schulze, H. Mensink Eur Urol 2001;40(3):252-255 Introduction is characterised by a constant rise in incidence over the last 50 years, with a predominance
SBRT for lung metastases: Case report
 SBRT for lung metastases: Case report Guillermo de Velasco MD, PhD University Hospital 12 de Octubre @H12O_GUCancer @g_develasco Case report 71 years old man Smoker DM 2005 Right radical nephrectomy Histology:
SBRT for lung metastases: Case report Guillermo de Velasco MD, PhD University Hospital 12 de Octubre @H12O_GUCancer @g_develasco Case report 71 years old man Smoker DM 2005 Right radical nephrectomy Histology:
The Surgical Management of RCC
 The Surgical Management of RCC From Robson to Radiofrequency Ablation Tony Finelli, MD, MSc, FRCSC University Health Network University of Toronto Background Renal cell carcinoma (RCC) is 9 th most common
The Surgical Management of RCC From Robson to Radiofrequency Ablation Tony Finelli, MD, MSc, FRCSC University Health Network University of Toronto Background Renal cell carcinoma (RCC) is 9 th most common
Multidisciplinary approach for renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute
 Multidisciplinary approach for renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 20 April, Antalya, Turkey RCC European Union 60.000 new diagnoses/year 26.000 Cancer related deaths
Multidisciplinary approach for renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 20 April, Antalya, Turkey RCC European Union 60.000 new diagnoses/year 26.000 Cancer related deaths
Tumor necrosis is a strong predictor for recurrence in patients with pathological T1a renal cell carcinoma
 ONCOLOGY LETTERS 9: 125-130, 2015 Tumor necrosis is a strong predictor for recurrence in patients with pathological T1a renal cell carcinoma KEIICHI ITO 1, KENJI SEGUCHI 1, HIDEYUKI SHIMAZAKI 2, EIJI TAKAHASHI
ONCOLOGY LETTERS 9: 125-130, 2015 Tumor necrosis is a strong predictor for recurrence in patients with pathological T1a renal cell carcinoma KEIICHI ITO 1, KENJI SEGUCHI 1, HIDEYUKI SHIMAZAKI 2, EIJI TAKAHASHI
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches
 Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches Cary N Robertson MD FACS Associate Professor Division of Urology Associate Director Urologic Oncology Duke Cancer
Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches Cary N Robertson MD FACS Associate Professor Division of Urology Associate Director Urologic Oncology Duke Cancer
Renal and ureteral involvement in Erdheim-Chester disease: analysis of a single centre cohort
 Renal and ureteral involvement in Erdheim-Chester disease: analysis of a single centre cohort Gaia Manari, Davide Gianfreda, Andrea Posteraro, Alessandro A. Palumbo and Augusto Vaglio Nephrology Unit and
Renal and ureteral involvement in Erdheim-Chester disease: analysis of a single centre cohort Gaia Manari, Davide Gianfreda, Andrea Posteraro, Alessandro A. Palumbo and Augusto Vaglio Nephrology Unit and
Laparoscopic Surgery. The Da Vinci Robot. Limits of Laparoscopy. What Robotics Offers. Robotic Urologic Surgery: A New Era in Patient Care
 Laparoscopic Surgery Robotic Urologic Surgery: A New Era in Patient Care Laparoscopic technique was introduced in urologic surgery in the 1990s Benefits: Improved recovery time, decreased morbidity Matthew
Laparoscopic Surgery Robotic Urologic Surgery: A New Era in Patient Care Laparoscopic technique was introduced in urologic surgery in the 1990s Benefits: Improved recovery time, decreased morbidity Matthew
Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22
 Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22 Chief complaint Unknown fever for one month Hand tremor and left huge renal tumor was noted Present illness Suffered from fever for one month, hand
Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22 Chief complaint Unknown fever for one month Hand tremor and left huge renal tumor was noted Present illness Suffered from fever for one month, hand
Carcinoma renale (I): Posters Review. Elena Verzoni Oncologia Medica 1 SS.Oncologia Genitourinaria Fondazione IRCCS Istituto Nazionale Tumori Milano
: Posters Review. Elena Verzoni Oncologia Medica 1 SS.Oncologia Genitourinaria Fondazione IRCCS Istituto Nazionale Tumori Milano") Carcinoma renale (I): Posters Review Elena Verzoni Oncologia Medica 1 SS.Oncologia Genitourinaria Fondazione IRCCS Istituto Nazionale Tumori Milano Agenda: Best Posters in Localized RCC Surgery: CN (#
Carcinoma renale (I): Posters Review Elena Verzoni Oncologia Medica 1 SS.Oncologia Genitourinaria Fondazione IRCCS Istituto Nazionale Tumori Milano Agenda: Best Posters in Localized RCC Surgery: CN (#
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
Small Renal Mass Guidelines. Clif Vestal, MD USMD Arlington, Texas
 Small Renal Mass Guidelines Clif Vestal, MD USMD Arlington, Texas Evaluation/Diagnosis 1. Obtain high quality, multiphase, cross-sectional abdominal imaging to optimally characterize/stage the renal mass.
Small Renal Mass Guidelines Clif Vestal, MD USMD Arlington, Texas Evaluation/Diagnosis 1. Obtain high quality, multiphase, cross-sectional abdominal imaging to optimally characterize/stage the renal mass.
Role and extension of lymph node dissection in kidney, bladder and prostate cancer. Omar Ghanem (PGY3 ) Moderator: Dr A. Noujem 30 th March 2017
 Moderator: Dr A. Noujem 30 th March 2017") Role and extension of lymph node dissection in kidney, bladder and prostate cancer Omar Ghanem (PGY3 ) Moderator: Dr A. Noujem 30 th March 2017 Bladder Cancer LN dissection in Bladder cancer 25% of patients
Role and extension of lymph node dissection in kidney, bladder and prostate cancer Omar Ghanem (PGY3 ) Moderator: Dr A. Noujem 30 th March 2017 Bladder Cancer LN dissection in Bladder cancer 25% of patients
Canadian Urological Association guidelines for followup of patients after treatment of nonmetastatic
 Canadian Urological Association guidelines for followup of patients after treatment of nonmetastatic renal cell carcinoma Wassim Kassouf, Leonardo L. Monteiro, Darrel E. Drachenberg, Adrian S. Fairey,
Canadian Urological Association guidelines for followup of patients after treatment of nonmetastatic renal cell carcinoma Wassim Kassouf, Leonardo L. Monteiro, Darrel E. Drachenberg, Adrian S. Fairey,
NET und NEC. Endoscopic and oncologic therapy
 NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
Urinary tract embolization
 Beograd, 14.10.2012 Urinary tract embolization asist. Peter Popovič, MD, MSc Head of abdominal radiology department, Institute of Radiology, UMC Ljubljana Embolization Who and when procedure: local/general
Beograd, 14.10.2012 Urinary tract embolization asist. Peter Popovič, MD, MSc Head of abdominal radiology department, Institute of Radiology, UMC Ljubljana Embolization Who and when procedure: local/general
Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation
 Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 61-70, Abr.-Jun., 2006 Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Acta Radiológica Portuguesa, Vol.XVIII, nº 70, pág. 61-70, Abr.-Jun., 2006 Pediatric Retroperitoneal Masses Radiologic-Pathologic Correlation Marilyn J. Siegel Mallinckrodt Institute of Radiology, Washington
Cytoreductive Radical Prostatectomy for de Novo Metastatic Prostate Cancer
 Cytoreductive Radical Prostatectomy for de Novo Metastatic Prostate Cancer Timothy G. Wilson, MD Professor and Chair of Urology John Wayne Cancer Institute Santa Monica, California Disclosures I am on
Cytoreductive Radical Prostatectomy for de Novo Metastatic Prostate Cancer Timothy G. Wilson, MD Professor and Chair of Urology John Wayne Cancer Institute Santa Monica, California Disclosures I am on
Definition Prostate cancer
 Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Chemotherapy and Bladder Cancer. Blayne Welk UBC Urology Grand Rounds June 4, 2008
 Chemotherapy and Bladder Cancer Blayne Welk UBC Urology Grand Rounds June 4, 2008 Outline Review of Incidence and Impact of bladder cancer Neoadjuvant chemotherapy Adjuvant chemotherapy Bladder preservation
Chemotherapy and Bladder Cancer Blayne Welk UBC Urology Grand Rounds June 4, 2008 Outline Review of Incidence and Impact of bladder cancer Neoadjuvant chemotherapy Adjuvant chemotherapy Bladder preservation
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Comparison of Partial and Radical Nephrectomy for pt1b Renal Cell Carcinoma
 www.kjurology.org DOI:10.4111/kju.2010.51.9.596 Urological Oncology Comparison of Partial and Radical Nephrectomy for pt1b Renal Cell Carcinoma Jong Min Kim, Phil Hyun Song, Hyun Tae Kim, Tong Choon Park
www.kjurology.org DOI:10.4111/kju.2010.51.9.596 Urological Oncology Comparison of Partial and Radical Nephrectomy for pt1b Renal Cell Carcinoma Jong Min Kim, Phil Hyun Song, Hyun Tae Kim, Tong Choon Park
Sergio Bracarda MD. Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy
 San Donato Hospital Arezzo, Italy") Sergio Bracarda MD Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy Ninth European International Kidney Cancer Symposium Dublin 25-26
Sergio Bracarda MD Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy Ninth European International Kidney Cancer Symposium Dublin 25-26
Stereotactic ablative body radiotherapy for renal cancer
 1 EVIDENCE SUMMARY REPORT Stereotactic ablative body radiotherapy for renal cancer Questions to be addressed 1. What is the clinical effectiveness of stereotactic ablative body radiotherapy for inoperable
1 EVIDENCE SUMMARY REPORT Stereotactic ablative body radiotherapy for renal cancer Questions to be addressed 1. What is the clinical effectiveness of stereotactic ablative body radiotherapy for inoperable
Surgical Management of Metastatic and Locally Recurrent Kidney Cancer: Does it Make Sense?
 Surgical Management of Metastatic and Locally Recurrent Kidney Cancer: Does it Make Sense? Philippe E. Spiess, MD, FACS Associate Member Department of GU Oncology Department of Tumor Biology Moffitt Cancer
Surgical Management of Metastatic and Locally Recurrent Kidney Cancer: Does it Make Sense? Philippe E. Spiess, MD, FACS Associate Member Department of GU Oncology Department of Tumor Biology Moffitt Cancer
Completing the Puzzle AJCC TNM Staging Breast. Nicole Catlett, CTR 2017 Kentucky Cancer Registry Fall Conference, September 21 & 22, 2017
 Completing the Puzzle AJCC TNM Staging Breast Nicole Catlett, CTR 2017 Kentucky Cancer Registry Fall Conference, September 21 & 22, 2017 OBJECTIVES Understanding of Breast TNM staging Identify clinical
Completing the Puzzle AJCC TNM Staging Breast Nicole Catlett, CTR 2017 Kentucky Cancer Registry Fall Conference, September 21 & 22, 2017 OBJECTIVES Understanding of Breast TNM staging Identify clinical
ROBOTIC SURGERY FOR RENAL CELL CANCER CLAYTON LAU, MD CHIEF OF UROLOGY AND UROLOGIC ONCOLOGY SEPT 2018
 ROBOTIC SURGERY FOR RENAL CELL CANCER CLAYTON LAU, MD CHIEF OF UROLOGY AND UROLOGIC ONCOLOGY SEPT 2018 Disclosures Consultant and Speaker for Intuitive Surgical and Covidien 2. Epidemiology 62K Estimated
ROBOTIC SURGERY FOR RENAL CELL CANCER CLAYTON LAU, MD CHIEF OF UROLOGY AND UROLOGIC ONCOLOGY SEPT 2018 Disclosures Consultant and Speaker for Intuitive Surgical and Covidien 2. Epidemiology 62K Estimated
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
Emerging Biomarkers of VEGF and mtor Inhibitors in 2015
 Emerging Biomarkers of VEGF and mtor Inhibitors in 2015 Laurence Albiges Institut Gustave Roussy, France Fourteenth International Kidney Cancer Symposium Miami, Florida, USA November 6-7, 2015 www.kidneycancersymposium.com
Emerging Biomarkers of VEGF and mtor Inhibitors in 2015 Laurence Albiges Institut Gustave Roussy, France Fourteenth International Kidney Cancer Symposium Miami, Florida, USA November 6-7, 2015 www.kidneycancersymposium.com
Complications in robotic surgery!! Review of the literature! RALP, RAPN and RARC!
 Complications in robotic surgery Review of the literature RALP, RAPN and RARC Anna Wallerstedt, MD Karolinska University Hospital Stockholm, Sweden Agenda The importance of reporting surgical complications
Complications in robotic surgery Review of the literature RALP, RAPN and RARC Anna Wallerstedt, MD Karolinska University Hospital Stockholm, Sweden Agenda The importance of reporting surgical complications
Actualités néphrologiques. Arnaud Méjean
 Actualités néphrologiques Arnaud Méjean Disclosures Pfizer, Novartis, GSK, BMS, Roche, Ipsen, Pierre Fabre, Astellas, Janssen, Ferring Epidemiology 7 th rank of cancer Incidence 2012 : 11573 news cases
Actualités néphrologiques Arnaud Méjean Disclosures Pfizer, Novartis, GSK, BMS, Roche, Ipsen, Pierre Fabre, Astellas, Janssen, Ferring Epidemiology 7 th rank of cancer Incidence 2012 : 11573 news cases
A schematic of the rectal probe in contact with the prostate is show in this diagram.
 Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Patient Reported Weight Loss Predicts Recurrence Rate in Renal Cell Cancer Cases after Nephrectomy
 DOI:10.22034/APJCP.2018.19.4.891 RESEARCH ARTICLE Editorial Process: Submission:01/04/2017 Acceptance:09/11/2017 Patient Reported Weight Loss Predicts Recurrence Rate in Renal Cell Cancer Cases after Nephrectomy
DOI:10.22034/APJCP.2018.19.4.891 RESEARCH ARTICLE Editorial Process: Submission:01/04/2017 Acceptance:09/11/2017 Patient Reported Weight Loss Predicts Recurrence Rate in Renal Cell Cancer Cases after Nephrectomy
Case(s): How to Deal with Mixed Response Giuseppe Procopio
: How to Deal with Mixed Response Giuseppe Procopio") Case(s): How to Deal with Mixed Response Giuseppe Procopio Fondazione IRCCS Istituto Nazionale dei Tumori, Milano Disclosures Advisory: Astellas, Bayer, GSK Consultant: Pfizer, Novartis Background Mixed
Case(s): How to Deal with Mixed Response Giuseppe Procopio Fondazione IRCCS Istituto Nazionale dei Tumori, Milano Disclosures Advisory: Astellas, Bayer, GSK Consultant: Pfizer, Novartis Background Mixed
Renal Mass Biopsy Should be Used for Most SRM - PRO
 Renal Mass Biopsy Should be Used for Most SRM - PRO Tony Finelli, MD, MSc, FRCSC Head, Division of Urology GU Site Lead, Princess Margaret Cancer Center GU Cancer Lead, Cancer Care Ontario Associate Professor,
Renal Mass Biopsy Should be Used for Most SRM - PRO Tony Finelli, MD, MSc, FRCSC Head, Division of Urology GU Site Lead, Princess Margaret Cancer Center GU Cancer Lead, Cancer Care Ontario Associate Professor,
Multidisciplinary management of retroperitoneal sarcomas
 Multidisciplinary management of retroperitoneal sarcomas Eric K. Nakakura, MD UCSF Department of Surgery UCSF Comprehensive Cancer Center San Francisco, CA 7 th Annual Clinical Cancer Update North Lake
Multidisciplinary management of retroperitoneal sarcomas Eric K. Nakakura, MD UCSF Department of Surgery UCSF Comprehensive Cancer Center San Francisco, CA 7 th Annual Clinical Cancer Update North Lake
Directness Consistency Precision Reporting Bias
 responsible for the accuracy and presentation of the material. Supplemental Table. Strength of evidence for primary. Key Outcomes* Studies (N) Study limitations Directness Consistency Precision Reporting
responsible for the accuracy and presentation of the material. Supplemental Table. Strength of evidence for primary. Key Outcomes* Studies (N) Study limitations Directness Consistency Precision Reporting
Diagnosis and management of retroperitoneal sarcoma
 SON Update 2017 Diagnosis and management of retroperitoneal sarcoma Andrea J MacNeill, MD MSc FRCSC Surgical Oncologist, BC Cancer Agency Vancouver 2 Histologic Subtypes of STS 3 RP Subtypes (n=684) Extremity
SON Update 2017 Diagnosis and management of retroperitoneal sarcoma Andrea J MacNeill, MD MSc FRCSC Surgical Oncologist, BC Cancer Agency Vancouver 2 Histologic Subtypes of STS 3 RP Subtypes (n=684) Extremity
GUIDELINES FOR THE MANAGEMENT OF
 GUIDELINES FOR THE MANAGEMENT OF RENAL CANCER Date of endorsement: July 2011 Authors: Mr. RD Mills & Mr. WH Turner Ref: AngCN-SSG-U3 Page 1 of 14 Approved and Published: Aug 2011 Title: Guidelines for
GUIDELINES FOR THE MANAGEMENT OF RENAL CANCER Date of endorsement: July 2011 Authors: Mr. RD Mills & Mr. WH Turner Ref: AngCN-SSG-U3 Page 1 of 14 Approved and Published: Aug 2011 Title: Guidelines for
Oncourology COMPLICATIONS OF PARTIAL NEPHRECTOMY AT OPERATIVE TREATMENT OF RENAL CELL CARCINOMA
 1 Oncourology COMPLICATIONS OF PARTIAL NEPHRECTOMY AT OPERATIVE TREATMENT OF RENAL CELL CARCINOMA Address: Eduard Oleksandrovych Stakhovsky, 03022, Kyiv, Lomonosova Str., 33/43, National Cancer Institute
1 Oncourology COMPLICATIONS OF PARTIAL NEPHRECTOMY AT OPERATIVE TREATMENT OF RENAL CELL CARCINOMA Address: Eduard Oleksandrovych Stakhovsky, 03022, Kyiv, Lomonosova Str., 33/43, National Cancer Institute
AUA Guidelines Renal Mass and Localized Kidney Cancer
 AUA Guidelines Renal Mass and Localized Kidney Cancer Steven C. Campbell, MD, PhD Chair AUA Guidelines Panel Professor Surgery, Vice Chair, Program Director Department of Urology Glickman Urological and
AUA Guidelines Renal Mass and Localized Kidney Cancer Steven C. Campbell, MD, PhD Chair AUA Guidelines Panel Professor Surgery, Vice Chair, Program Director Department of Urology Glickman Urological and
Percutaneous ablation of renal cell carcinoma. Where do we stand now? Sanja Stojanović, Spasić Aleksandar
 Percutaneous ablation of renal cell carcinoma Where do we stand now? Sanja Stojanović, Spasić Aleksandar Clinical Center of Vojvodina / Center for Radiology Novi Sad Serbia Renal cell carcinoma approximately
Percutaneous ablation of renal cell carcinoma Where do we stand now? Sanja Stojanović, Spasić Aleksandar Clinical Center of Vojvodina / Center for Radiology Novi Sad Serbia Renal cell carcinoma approximately
Freeze, Fry or Cut. Jennifer A. Linehan, MD Associate Professor Urologic Oncology John Wayne Cancer Institute 2/9/2018
 Freeze, Fry or Cut Jennifer A. Linehan, MD Associate Professor Urologic Oncology John Wayne Cancer Institute 2/9/2018 Disclosures Consultant for UroGen Pharma. REDEFINING WHAT SURGEONS SEE Bay Area-based
Freeze, Fry or Cut Jennifer A. Linehan, MD Associate Professor Urologic Oncology John Wayne Cancer Institute 2/9/2018 Disclosures Consultant for UroGen Pharma. REDEFINING WHAT SURGEONS SEE Bay Area-based
Solitary Contralateral Adrenal Metastases after Nephrectomy for Renal Cell Carcinoma
 Original Report ISSN 1537-744X; DOI 10.1100/tsw.2004.39 Solitary Contralateral Adrenal after Nephrectomy for Renal Cell Carcinoma Nikolaos Antoniou, M.D. and Demetrios Karanastasis, M.D. General Hospital
Original Report ISSN 1537-744X; DOI 10.1100/tsw.2004.39 Solitary Contralateral Adrenal after Nephrectomy for Renal Cell Carcinoma Nikolaos Antoniou, M.D. and Demetrios Karanastasis, M.D. General Hospital
Renal Parenchymal Neoplasms
 Renal Parenchymal Neoplasms د. BENIGN TUMORS : Benign renal tumors include adenoma, oncocytoma, angiomyolipoma, leiomyoma, lipoma, hemangioma, and juxtaglomerular tumors. Renal Adenomas : The adenoma is
Renal Parenchymal Neoplasms د. BENIGN TUMORS : Benign renal tumors include adenoma, oncocytoma, angiomyolipoma, leiomyoma, lipoma, hemangioma, and juxtaglomerular tumors. Renal Adenomas : The adenoma is
Cytoreductive Nephrectomy
 Cytoreductive Nephrectomy Stephen H. Culp, M.D., Ph.D. Assistant Professor, Department of Urology Outline The Historics of CN The current status of CN The importance of patient selection Cytoreductive
Cytoreductive Nephrectomy Stephen H. Culp, M.D., Ph.D. Assistant Professor, Department of Urology Outline The Historics of CN The current status of CN The importance of patient selection Cytoreductive
Upper Tract Urothelial Carcinomas (UTUCs)
") Upper Tract Urothelial Carcinomas (UTUCs) Part II: UTUC Treatment Options November 14, 2017 Moderated by: Presented by: Gary D. Steinberg, MD University of Chicago Medical Center Ahmad Shabsigh, MD Ohio
Upper Tract Urothelial Carcinomas (UTUCs) Part II: UTUC Treatment Options November 14, 2017 Moderated by: Presented by: Gary D. Steinberg, MD University of Chicago Medical Center Ahmad Shabsigh, MD Ohio
Focal Ablative Therapies for Kidney Cancer
 Focal Ablative Therapies for Kidney Cancer Robert J. Hamilton, MD, MPH, FRCSC Staff Urologist, Princess Margaret Cancer Centre Assistant Prof., Dept. of Surgery (Urology), University of Toronto ICUC January
Focal Ablative Therapies for Kidney Cancer Robert J. Hamilton, MD, MPH, FRCSC Staff Urologist, Princess Margaret Cancer Centre Assistant Prof., Dept. of Surgery (Urology), University of Toronto ICUC January
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
EUROPEAN UROLOGY 61 (2012)
") EUROPEAN UROLOGY 61 (2012) 1156 1161 available at www.sciencedirect.com journal homepage: www.europeanurology.com Platinum Priority Kidney Cancer Editorial by Alvin C. Goh and Inderbir S. Gill on pp. 1162
EUROPEAN UROLOGY 61 (2012) 1156 1161 available at www.sciencedirect.com journal homepage: www.europeanurology.com Platinum Priority Kidney Cancer Editorial by Alvin C. Goh and Inderbir S. Gill on pp. 1162
SAMPLING OF POST NEPHRECTOMY CANCER CARE (5)
") SAMPLING OF POST NEPHRECTOMY CANCER CARE (5) Universally recognized post-nephrectomy cancer treatment. Sampling: National Comprehensive Cancer Network (NCCN) NCCN Clinical Practice Guidelines in Oncology
SAMPLING OF POST NEPHRECTOMY CANCER CARE (5) Universally recognized post-nephrectomy cancer treatment. Sampling: National Comprehensive Cancer Network (NCCN) NCCN Clinical Practice Guidelines in Oncology
Gerard M. Doherty, MD
 Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Surgical Management of Differentiated Thyroid Cancer: Update on 2015 ATA Guidelines Gerard M. Doherty, MD Chair of Surgery Utley Professor of Surgery and Medicine Boston University Surgeon-in-Chief Boston
Kidney Q&A 5/5/16 Q1: Can we please get that clarification sent with the presentation and Q&A? Also a start date for that clarification
 Kidney Q&A 5/5/16 Q1: Can we please get that clarification sent with the presentation and Q&A? Also a start date for that clarification A1: Yes. See below. I don't think it will have a start date. Clarification
Kidney Q&A 5/5/16 Q1: Can we please get that clarification sent with the presentation and Q&A? Also a start date for that clarification A1: Yes. See below. I don't think it will have a start date. Clarification
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
6. Cervical Lymph Nodes and Unknown Primary Tumors of the Head and Neck
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
RAPN. in T1b Renal Masses? A. Mottrie. G. Denaeyer, P. Schatteman, G. Novara
 RAPN in T1b Renal Masses? A. Mottrie G. Denaeyer, P. Schatteman, G. Novara Department of Urology O.L.V. Clinic Aalst OLV Vattikuti Robotic Surgery Institute Aalst Belgium Guidelines on Renal Cell Carcinoma
RAPN in T1b Renal Masses? A. Mottrie G. Denaeyer, P. Schatteman, G. Novara Department of Urology O.L.V. Clinic Aalst OLV Vattikuti Robotic Surgery Institute Aalst Belgium Guidelines on Renal Cell Carcinoma