Canadian Urological Association guidelines for followup of patients after treatment of nonmetastatic
|
|
|
- Philippa Harper
- 5 years ago
- Views:
Transcription
1 Canadian Urological Association guidelines for followup of patients after treatment of nonmetastatic renal cell carcinoma Wassim Kassouf, Leonardo L. Monteiro, Darrel E. Drachenberg, Adrian S. Fairey, Antonio Finelli, Anil Kapoor, Jean-Baptiste Lattouf, Michael J. Leveridge, Nicholas E. Power, Frederic Pouliot, Ricardo A. Rendon, Robert Sabbagh, Alan I. So, Simon Tanguay, Rodney H. Breau Originally published in Can Urol Assoc J 2018;12(8):
2 Disclosures Dr. Kassouf: Received grants/honoraria from Astellas, AstraZeneca, Janssen, Merck, and Roche Dr. Fairey: Speaker for J&J and Roche Dr. Finelli: Advisor for AbbVie, Amgen, Astellas, Bayer, Janssen, Roche, and Sanofi Dr. Kapoor: Advisor for and participant in clinical trials supported by Amgen, Astellas, GSK, Janssen, Novartis, Pfizer, and Sanofi. Dr. Lattouf: Advisor for AbbVie, Amgen, Astellas, Novartis, and Pfizer; received an educational grant from Janssen Dr. Leveridge: Advisor for Astellas Dr. Power: Participant in clinical trial supported by Argos Therapeutics Dr. Pouliot: Advisor for, Amgen, Astellas, and Pfizer; speaker for Sanofi; received payment/grants/honoraria from Amgen, Astellas, Astra Zeneca, Janssen, Pfizer, and Sanofi Dr. So: Speaker for Amgen, Astellas, and Janssen. Dr. Tanguay: Advisor for Pfizer; received travel grants from Sanofi
3 Renal cell carcinoma 3% of all malignancies Risk factors Smoking, obesity, hypertension ACKD, occupational exposure Hereditary (VHL, HPRC, HLRCC, BHD, SHD-RCC, TSC) Surgical resection (radical or partial nx) remains most common treatment Ablation increasingly used
4 Methods Publications on surveillance after surgery are based on retrospective analysis, including some larger, multicentre studies and well-designed controlled studies Randomized prospective studies are sparse, rendering it difficult to obtain qualified evidence-based data No clear consensus on surveillance after surgical extirpation for patients with RCC Followup approach based on assessment of timing and location of RCC recurrence in a risk-stratified manner
5 Rationale for surveillance Surveillance after surgery monitors for Postoperative complications Renal function Local recurrence Recurrence in the contralateral kidney Development of metastasis
6 Rationale for surveillance cont d Renal function and postoperative complications are commonly assessed by: Hx & PE; egfr and Hgb at 4 6 weeks Long-term monitoring of renal function Long-term monitoring of serum egfr, and proteinuria is recommended in patients with compromised renal function prior to surgery or significant decrease in egfr after surgery Referral to a nephrologist if egfr <45 ml/min/1.73m 2 or progressive CKD develops after surgery, especially if associated with proteinuria (Grade B)
7 Rationale for surveillance cont d Recurrence in the ipsilateral kidney is associated with positive surgical margins, multifocality, higher stage and grade Tumours may develop in the contralateral kidney (incidence <2%) Early diagnosis of local and contralateral kidney recurrence is useful since majority can be cured with treatment (LOE 3)
8 Rationale for surveillance cont d Extensive tumour recurrence reduces the possibility of complete surgical resection Patients who underwent surgery when local recurrences became symptomatic have a higher rate of incomplete resection, positive surgical margins, and worse survival Early diagnosis of disease relapse may enhance efficacy of systemic therapy or allow for metastatectomy if the tumour burden is low (LOE 4; Grade C) Kapoor, CUAJ 2017; Psutka, BJUI 2017; Levy, J Urol 1998 Hence, support rationale for surveillance to detect recurrences and metastases early (LOE 4; Grade C)
9 Prognostic factors Anatomical Local extent of the primary tumor (LOE 3) Presence of nodal metastasis (LOE 3) Histological RCC subtypes (LOE 3) Carcomatoid dedifferentiation Tumour grade (LOE 4) Other tumour characteristics (size, histological coagulative necrosis, DNA ploidy) (LOE 4) Clinical ECOG status (LOE 3) Presence of symptoms (local and systemic) Serum blood parameters (LOE 4) Molecular Carbonic anhydrase IX, VEGF, HIF Ki67, p53, PTEN, E-cadherins, PD-L1, others Not recommended in clinical setting (Grade C)
10 Predictive models

11 Predictive models cont d
12 Predictive models cont d Kattan, J Urol 2001
13 Predictive models cont d
14 Predictive models cont d Several prognostic models have been published and externally validated Have not been proven superior over the stage-adapted followup Integrated prognostic system or nomograms not routinely recommended for followup
15 CUA guidelines Canadian guidelines will be based on pathological stage Other prognostic factors have not been integrated to more or less stringent f/u protocol (Grade C)
16 CUA guidelines cont d In absence of randomized studies, conclusions based on large nonrandomized cohorts with long-term followup Pulmonary recurrences Routine chest x-ray is recommended. In higher risk patients, CT chest may be performed due to the higher sensitivity (LOE 5; Grade D) Abdominal recurrences CT abdomen/pelvis is recommended, particularly in cases of tumor-associated symptoms; an abdominal ultrasound may be performed for lower risk patients (pt1-2) (LOE 4; Grade C)
17 CUA guidelines cont d CT head or bone scan is not routinely recommended unless clinically indicated (LOE 4; Grade C) PET-CT is not recommended for surveillance in RCC
18 pt1 Levy, J Urol 1998 Recurrence rate: 7% (median followup 39 months) Median time to recurrence: 38 months (range 18 67) Majority of recurrences were in lung; no recurrences in abdomen None of the pulmonary recurrences were symptomatic. Stephenson, J Urol 2004 (Canadian group) Recurrence rate: 5.3% (median followup 44 months) Median time to recurrence: 35 months (range 2 93) Only 0.9% of patients recurred at 13, 66, and 93 months in the renal fossa and were asymptomatic
19 T1 Local recurrences 2% Local recurrences more common for larger tumours following PN and ablated tumours
20 pt1 Overall 7% develop recurrences; median time to recurrence months Half will occur after 5 years 5% for T1a and 15% for T1b Late recurrence rates: T1a: 2.6% T1b: 5% T2a: 9% T2b: 10% T3a: 11% T3b: 22%
21 pt1 cont d Most common location of 1st recurrence: Lung (54%), lymph nodes (22%) Bone (20%), and liver (15%) Independent predictors of late recurrence: Lymphovascular invasion Furhman grade 3 or 4 Pathological tumour stage >pt1
22 Recommended surveillance for T1 Clinical assessment, blood biochemistry, and chest x-ray every year (LOE 4; Grade C) Abdominal CT, MRI or US is recommended at 24 and 60 months (LOC 4; Grade C) Routine imaging beyond 5 years is optional and can be risk-adapted (Grade D) Followup is the same for partial nephrectomy for <4 cm lesions (LOE 2; Grade B) Since local recurrence rates in this population is similar to radical nephrectomy CT abdomen at 3 12 months postop for patients treated with partial nephrectomy is optional (LOE 4; Grade C)
23 Recommended surveillance: Ablated T1a tumours Similar to surgically treated tumours except for Abdominal imaging (CT or MRI) at 3, 6, and 12 months, then annually thereafter for up to 5 years (LOE 4; Grade C) If pre-treatment biopsy demonstrated benign tumor and imaging post ablation shows treatment success, routine imaging beyond one year is not recommended (LOE 5; Grade D)
24 pt2 Several series have reported recurrences rates 25 35% after a median followup of 5 years Levy, J Urol 1998 Recurrence rate: 27% at a median followup of 53 months Median time to recurrence: 32 months (range 3 115) Only 2 patients developed metastasis within 6 months postop Stephenson, J Urol 2004 (Canadian group) Recurrence rate: 17% at a median followup of 38 months (asymptomatic 50%) Median time to recurrence: 25 months (range 3 95)
25 Recommended surveillance for T2 Clinical assessment, blood biochemistry, and CXR (or chest CT) every 6 months for 3 years then yearly (LOE 4; Grade C) Abdominal CT/MRI/US recommended at 12, 24, 36, 60 months (LOE 4; Grade C) Routine imaging beyond 5 years is at the discretion of the treating physician
26 pt3-4 MDACC, J Urol 1998 Recurrence rate: 39% at a median followup of 31 months Median time to recurrence: 17 months (range 2 88) Stephenson, J Urol 2004 (Canadian group) Recurrence rate: 34%; asymptomatic: 40% Median time to relapse: 14 months for pt3a; 9 months for pt3b Dabestani, World J Urol, 2016 Recurrence rate at 5-year followup: 42 47% Median time to recurrence: 21 months
27 Recommended surveillance for T3-4 Clinical assessment, blood biochemistry, and CXR (or chest CT) every 6 months for 3 years then yearly (LOE 4; Grade C) Abdominal CT or MRI recommended at 6, 12, 18, 24, 36 months, then every 2 years (LOE 4; Grade C) In pn+ disease, CXR (or chest CT) and abdominal CT/MRI are recommended at 3 and 6 months, then every 6 months for 3 years then yearly (LOE 4; Grade C)
28 EAU 2017 Risk profile Surveillance 6 mo 1 y 2 y 3 y 4 y 5 y > 5 y Low US CT US CT US CT Discharge Intermediate CT CT CT US CT CT CT once every 2 years High CT CT CT CT CT CT CT once every 2 years
29 ESMO 2016
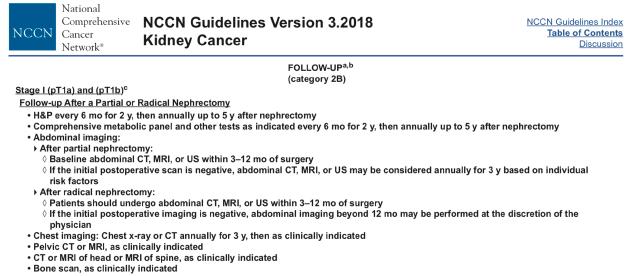
30 NCCN 2018

31 NCCN 2018 cont d

32 AUA 2013 T1 T2-4 or N+
33 CUA 2018
34 Followup post-ablation for T1a Months after surgery ct1a H&P x x x x x Blds x x x x x CXR x x x x x CT/MR x x x x x x x
SAMPLING OF POST NEPHRECTOMY CANCER CARE (5)
") SAMPLING OF POST NEPHRECTOMY CANCER CARE (5) Universally recognized post-nephrectomy cancer treatment. Sampling: National Comprehensive Cancer Network (NCCN) NCCN Clinical Practice Guidelines in Oncology
SAMPLING OF POST NEPHRECTOMY CANCER CARE (5) Universally recognized post-nephrectomy cancer treatment. Sampling: National Comprehensive Cancer Network (NCCN) NCCN Clinical Practice Guidelines in Oncology
Management of Locally Reccurent Renal Cell Carcinoma. Jose A. Karam, MD, FACS Assistant Professor Department of Urology
 Management of Locally Reccurent Renal Cell Carcinoma Jose A. Karam, MD, FACS Assistant Professor Department of Urology DefiniAons Defini&ve treatment Aiming for cure Abla&on therapy Radiofrequency abla&on
Management of Locally Reccurent Renal Cell Carcinoma Jose A. Karam, MD, FACS Assistant Professor Department of Urology DefiniAons Defini&ve treatment Aiming for cure Abla&on therapy Radiofrequency abla&on
Canadian Guidelines for Management of the Small Renal Mass (SRM)
") Canadian Guidelines for Management of the Small Renal Mass (SRM) Michael A.S. Jewett*, Ricardo Rendon, Louis Lacombe, Pierre I. Karakiewicz, Simon Tanguay, Wes Kassouf, Mike Leveridge, Ilias Cagiannos,
Canadian Guidelines for Management of the Small Renal Mass (SRM) Michael A.S. Jewett*, Ricardo Rendon, Louis Lacombe, Pierre I. Karakiewicz, Simon Tanguay, Wes Kassouf, Mike Leveridge, Ilias Cagiannos,
GUIDELINES ON RENAL CELL CARCINOMA
 GUIDELINES ON RENAL CELL CARCINOMA B. Ljungberg (chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction This EAU guideline was prepared to help urologists
GUIDELINES ON RENAL CELL CARCINOMA B. Ljungberg (chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction This EAU guideline was prepared to help urologists
Follow-up imaging after nephrectomy for cancer in Canada: urologists compliance with guidelines. An observational study
 Follow-up imaging after nephrectomy for cancer in Canada: urologists compliance with guidelines. An observational study Alice Dragomir PhD, Armen Aprikian MD, Anil Kapoor MD, Antonio Finelli MD, Frédéric
Follow-up imaging after nephrectomy for cancer in Canada: urologists compliance with guidelines. An observational study Alice Dragomir PhD, Armen Aprikian MD, Anil Kapoor MD, Antonio Finelli MD, Frédéric
Surveillance Strategies in Kidney Cancer: When is Enough? Role of Survivorship Clinic in Long-Term Follow-Up of Kidney Cancer
 Surveillance Strategies in Kidney Cancer: When is Enough? Role of Survivorship Clinic in Long-Term Follow-Up of Kidney Cancer Brandon Manley, MD Assistant Member, Genitourinary Oncology Department of Genitourinary
Surveillance Strategies in Kidney Cancer: When is Enough? Role of Survivorship Clinic in Long-Term Follow-Up of Kidney Cancer Brandon Manley, MD Assistant Member, Genitourinary Oncology Department of Genitourinary
Guidelines on Renal Cell
 Guidelines on Renal Cell Carcinoma (Text update March 2009) B. Ljungberg (Chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction Renal cell carcinoma
Guidelines on Renal Cell Carcinoma (Text update March 2009) B. Ljungberg (Chairman), D.C. Hanbury, M.A. Kuczyk, A.S. Merseburger, P.F.A. Mulders, J-J. Patard, I.C. Sinescu Introduction Renal cell carcinoma
WHAT IS THE ROLE OF ACTIVE SURVEILLANCE
 WHAT IS THE ROLE OF ACTIVE SURVEILLANCE IN THE CONTEXT OF RENAL ABLATION AND PARTIAL NEPHRECTOMY? Alessandro Volpe University of Eastern Piedmont Novara, Italy RCC INCIDENCE SEER DATABASE (1975-2006) RCC
WHAT IS THE ROLE OF ACTIVE SURVEILLANCE IN THE CONTEXT OF RENAL ABLATION AND PARTIAL NEPHRECTOMY? Alessandro Volpe University of Eastern Piedmont Novara, Italy RCC INCIDENCE SEER DATABASE (1975-2006) RCC
Is renal cryoablation becoming an effective alternative to partial nephrectomy?
 Is renal cryoablation becoming an effective alternative to partial nephrectomy? J GARNON 1, G TSOUMAKIDOU 1, H LANG 2, A GANGI 1 1 department of interventional radiology 2 department of urology University
Is renal cryoablation becoming an effective alternative to partial nephrectomy? J GARNON 1, G TSOUMAKIDOU 1, H LANG 2, A GANGI 1 1 department of interventional radiology 2 department of urology University
NCCN AND AUA GUIDELINES FOR RCC:
 NCCN AND AUA GUIDELINES FOR RCC: DO THEY EFFECTIVELY CAPTURE RECURRENCES FOLLOWING NEPHRECTOMY? Suzanne B. Stewart, MD 1, R. Houston Thompson, MD 1, Sarah P. Psutka, MD 1, John C. Cheville, MD 2, Christine
NCCN AND AUA GUIDELINES FOR RCC: DO THEY EFFECTIVELY CAPTURE RECURRENCES FOLLOWING NEPHRECTOMY? Suzanne B. Stewart, MD 1, R. Houston Thompson, MD 1, Sarah P. Psutka, MD 1, John C. Cheville, MD 2, Christine
GUIDELINES ON RENAL CELL CANCER
 20 G. Mickisch (chairman), J. Carballido, S. Hellsten, H. Schulze, H. Mensink Eur Urol 2001;40(3):252-255 Introduction is characterised by a constant rise in incidence over the last 50 years, with a predominance
20 G. Mickisch (chairman), J. Carballido, S. Hellsten, H. Schulze, H. Mensink Eur Urol 2001;40(3):252-255 Introduction is characterised by a constant rise in incidence over the last 50 years, with a predominance
Lymphadenectomy in RCC: Yes, No, Clinical Trial?
 Lymphadenectomy in RCC: Yes, No, Clinical Trial? Viraj Master MD PhD FACS Professor Associate Chair for Clinical Affairs and Quality Director of Clinical Research Unit Department of Urology Emory University
Lymphadenectomy in RCC: Yes, No, Clinical Trial? Viraj Master MD PhD FACS Professor Associate Chair for Clinical Affairs and Quality Director of Clinical Research Unit Department of Urology Emory University
Indications For Partial
 Indications For Partial Nephrectomy Christopher G. Wood, M. D., FACS Professor and Deputy Chairman Douglas E. Johnson, M. D. Endowed Professorship in Urology Department of Urology The University of Texas
Indications For Partial Nephrectomy Christopher G. Wood, M. D., FACS Professor and Deputy Chairman Douglas E. Johnson, M. D. Endowed Professorship in Urology Department of Urology The University of Texas
Small Renal Mass Guidelines. Clif Vestal, MD USMD Arlington, Texas
 Small Renal Mass Guidelines Clif Vestal, MD USMD Arlington, Texas Evaluation/Diagnosis 1. Obtain high quality, multiphase, cross-sectional abdominal imaging to optimally characterize/stage the renal mass.
Small Renal Mass Guidelines Clif Vestal, MD USMD Arlington, Texas Evaluation/Diagnosis 1. Obtain high quality, multiphase, cross-sectional abdominal imaging to optimally characterize/stage the renal mass.
Tumor necrosis is a strong predictor for recurrence in patients with pathological T1a renal cell carcinoma
 ONCOLOGY LETTERS 9: 125-130, 2015 Tumor necrosis is a strong predictor for recurrence in patients with pathological T1a renal cell carcinoma KEIICHI ITO 1, KENJI SEGUCHI 1, HIDEYUKI SHIMAZAKI 2, EIJI TAKAHASHI
ONCOLOGY LETTERS 9: 125-130, 2015 Tumor necrosis is a strong predictor for recurrence in patients with pathological T1a renal cell carcinoma KEIICHI ITO 1, KENJI SEGUCHI 1, HIDEYUKI SHIMAZAKI 2, EIJI TAKAHASHI
Renal Mass Biopsy: Needed Now More than Ever
 Renal Mass Biopsy: Needed Now More than Ever Stuart G. Silverman, MD, FACR Professor of Radiology Harvard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Boston,
Renal Mass Biopsy: Needed Now More than Ever Stuart G. Silverman, MD, FACR Professor of Radiology Harvard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Boston,
Section Activity Activity Description Details Reference(s)
") Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with Renal Cell Carcinoma AA Cancer Centre Referrals Not routine pre-op referral indicated
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with Renal Cell Carcinoma AA Cancer Centre Referrals Not routine pre-op referral indicated
RAPN. in T1b Renal Masses? A. Mottrie. G. Denaeyer, P. Schatteman, G. Novara
 RAPN in T1b Renal Masses? A. Mottrie G. Denaeyer, P. Schatteman, G. Novara Department of Urology O.L.V. Clinic Aalst OLV Vattikuti Robotic Surgery Institute Aalst Belgium Guidelines on Renal Cell Carcinoma
RAPN in T1b Renal Masses? A. Mottrie G. Denaeyer, P. Schatteman, G. Novara Department of Urology O.L.V. Clinic Aalst OLV Vattikuti Robotic Surgery Institute Aalst Belgium Guidelines on Renal Cell Carcinoma
Canadian Urological Association guideline for followup of patients after treatment of non-metastatic renal cell carcinoma
 CUA Guideline Canadian Urological Association guideline for followup of patients after treatment of non-metastatic renal cell carcinoma Wassim Kassouf, MD 1 ; Leonardo L. Monteiro, MD 1 ; Darrel E. Drachenberg,
CUA Guideline Canadian Urological Association guideline for followup of patients after treatment of non-metastatic renal cell carcinoma Wassim Kassouf, MD 1 ; Leonardo L. Monteiro, MD 1 ; Darrel E. Drachenberg,
Surgical management of renal cell carcinoma: Canadian Kidney Cancer Forum Consensus
 CONSENSUS STATEMENT Surgical management of renal cell carcinoma: Canadian Kidney Cancer Forum Consensus Ricardo A. Rendon, MD, FRCSC; * Anil Kapoor, MD, FRCSC; Rodney Breau, MD, FRCSC; Michael Leveridge,
CONSENSUS STATEMENT Surgical management of renal cell carcinoma: Canadian Kidney Cancer Forum Consensus Ricardo A. Rendon, MD, FRCSC; * Anil Kapoor, MD, FRCSC; Rodney Breau, MD, FRCSC; Michael Leveridge,
ACTIVE SURVEILLANCE FOR RENAL MASSES: Where are we in 2016?
 ACTIVE SURVEILLANCE FOR RENAL MASSES: Where are we in 2016? Phillip M. Pierorazio, MD Assistant Professor of Urology and Oncology Brady Urological Institute Sidney Kimmel Cancer Center Johns Hopkins Hospital
ACTIVE SURVEILLANCE FOR RENAL MASSES: Where are we in 2016? Phillip M. Pierorazio, MD Assistant Professor of Urology and Oncology Brady Urological Institute Sidney Kimmel Cancer Center Johns Hopkins Hospital
Patient Selection for Surgery in RCC with Thrombus. E. Jason Abel, M.D.
 Patient Selection for Surgery in RCC with Thrombus E. Jason Abel, M.D. RCC with venous invasion Venous invasion occurs in ~10% of RCC Surgery more complex Increased risk for morbidity Thrombus may be confined
Patient Selection for Surgery in RCC with Thrombus E. Jason Abel, M.D. RCC with venous invasion Venous invasion occurs in ~10% of RCC Surgery more complex Increased risk for morbidity Thrombus may be confined
St. Dominic s Annual Cancer Report Outcomes
 St. Dominic s 2017 Annual Cancer Report Outcomes Cancer Program Practice Profile Reports (CP3R) St. Dominic s Cancer Committee monitors and ensures that patients treated at St. Dominic Hospital receive
St. Dominic s 2017 Annual Cancer Report Outcomes Cancer Program Practice Profile Reports (CP3R) St. Dominic s Cancer Committee monitors and ensures that patients treated at St. Dominic Hospital receive
Should the primary be treated in patients with metastatic disease? Upper Tract Urothelial Cancer
 Should the primary be treated in patients with metastatic disease? Upper Tract Urothelial Cancer Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology
Should the primary be treated in patients with metastatic disease? Upper Tract Urothelial Cancer Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology
AUA Guidelines Renal Mass and Localized Kidney Cancer
 AUA Guidelines Renal Mass and Localized Kidney Cancer Steven C. Campbell, MD, PhD Chair AUA Guidelines Panel Professor Surgery, Vice Chair, Program Director Department of Urology Glickman Urological and
AUA Guidelines Renal Mass and Localized Kidney Cancer Steven C. Campbell, MD, PhD Chair AUA Guidelines Panel Professor Surgery, Vice Chair, Program Director Department of Urology Glickman Urological and
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
Complex case Presentations
 Complex case Presentations Case Presentations April 2016 Lisa M Pickering Case presentations: chromophobe renal carcinoma 60 year old man. ECOG PS 0 No significant comorbodities August 2009: L radical
Complex case Presentations Case Presentations April 2016 Lisa M Pickering Case presentations: chromophobe renal carcinoma 60 year old man. ECOG PS 0 No significant comorbodities August 2009: L radical
ORIGINAL RESEARCH. Abstract. Introduction
 ORIGINAL RESEARCH Positive surgical margins during partial nephrectomy for renal cell carcinoma: Results from Canadian Kidney Cancer information system (CKCis) collaborative Rahul K. Bansal, MD, MS, MCh
ORIGINAL RESEARCH Positive surgical margins during partial nephrectomy for renal cell carcinoma: Results from Canadian Kidney Cancer information system (CKCis) collaborative Rahul K. Bansal, MD, MS, MCh
REAL WORLD PRACTICE: ADJUVANT THERAPY READY FOR PRIME TIME? PRO
 REAL WORLD PRACTICE: ADJUVANT THERAPY READY FOR PRIME TIME? PRO Alain Ravaud, MD.PhD Bordeaux. France DISCLOSURES Consultant for: Pfizer, Novartis, GlaxoSmithKline, Roche, Bristol-Myers Squibb Institutional
REAL WORLD PRACTICE: ADJUVANT THERAPY READY FOR PRIME TIME? PRO Alain Ravaud, MD.PhD Bordeaux. France DISCLOSURES Consultant for: Pfizer, Novartis, GlaxoSmithKline, Roche, Bristol-Myers Squibb Institutional
Understanding the risk of recurrence after primary treatment for prostate cancer. Aditya Bagrodia, MD
 Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Surgical Management of Renal Cancer. David Nicol Consultant Urologist
 Surgical Management of Renal Cancer David Nicol Consultant Urologist Roles of Surgery 1. Curative intervention localised disease 2. Symptomatic control advanced disease 3. Augmentation of efficacy of systemic
Surgical Management of Renal Cancer David Nicol Consultant Urologist Roles of Surgery 1. Curative intervention localised disease 2. Symptomatic control advanced disease 3. Augmentation of efficacy of systemic
Surgeons Perspective: LN as a Draining Pattern. Jose A. Karam, MD, FACS Associate Professor Department of Urology
 Surgeons Perspective: LN as a Draining Pattern Jose A. Karam, MD, FACS Associate Professor Department of Urology Disclosures EMD Serono, Pfizer, Novartis: Advisory board/consultant Disclosures I perform
Surgeons Perspective: LN as a Draining Pattern Jose A. Karam, MD, FACS Associate Professor Department of Urology Disclosures EMD Serono, Pfizer, Novartis: Advisory board/consultant Disclosures I perform
Renal biopsy is mandatory for every small renal mass
 Renal biopsy is mandatory for every small renal mass Ben Challacombe Consultant Urologist The Urology Centre Guy s and St. Thomas Hospital NHS Foundation Trust Oncocytoma High Risk Partial converted to
Renal biopsy is mandatory for every small renal mass Ben Challacombe Consultant Urologist The Urology Centre Guy s and St. Thomas Hospital NHS Foundation Trust Oncocytoma High Risk Partial converted to
What is the role of partial nephrectomy in the context of active surveillance and renal ablation?
 What is the role of partial nephrectomy in the context of active surveillance and renal ablation? Dogu Teber Department of Urology University Hospital Heidelberg Coming from Heidelberg obligates to speak
What is the role of partial nephrectomy in the context of active surveillance and renal ablation? Dogu Teber Department of Urology University Hospital Heidelberg Coming from Heidelberg obligates to speak
Guidelines for the Management of Renal Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Renal Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Renal Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
January 10-12, Westin Harbour Castle Toronto, ON #CUOS19. cuos2019.org
 January 10-12, 2019 Westin Harbour Castle Toronto, ON #CUOS19 cuos2019.org Scientific Program Committee Co-Chairs: Neil Fleshner, CUOG Aly-Khan Lalani, GUMOC Himu Lukka, GUROC Andy Evans, CNUP Tony Finelli,
January 10-12, 2019 Westin Harbour Castle Toronto, ON #CUOS19 cuos2019.org Scientific Program Committee Co-Chairs: Neil Fleshner, CUOG Aly-Khan Lalani, GUMOC Himu Lukka, GUROC Andy Evans, CNUP Tony Finelli,
Role and extension of lymph node dissection in kidney, bladder and prostate cancer. Omar Ghanem (PGY3 ) Moderator: Dr A. Noujem 30 th March 2017
 Moderator: Dr A. Noujem 30 th March 2017") Role and extension of lymph node dissection in kidney, bladder and prostate cancer Omar Ghanem (PGY3 ) Moderator: Dr A. Noujem 30 th March 2017 Bladder Cancer LN dissection in Bladder cancer 25% of patients
Role and extension of lymph node dissection in kidney, bladder and prostate cancer Omar Ghanem (PGY3 ) Moderator: Dr A. Noujem 30 th March 2017 Bladder Cancer LN dissection in Bladder cancer 25% of patients
Vincenzo Ficarra 1,2,3. Associate Editor BJU International
 Partial Nephrectomy for RCC Vincenzo Ficarra 1,2,3 1 Director Department of Urology University of Udine, Italy 2 Associate Editor BJU International 3 Scientific Director OLV Robotic Surgery Institute,
Partial Nephrectomy for RCC Vincenzo Ficarra 1,2,3 1 Director Department of Urology University of Udine, Italy 2 Associate Editor BJU International 3 Scientific Director OLV Robotic Surgery Institute,
Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute
 Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 23 March 2012, Sao Paulo, Brazil Surgery of RCC Locally confined (small) renal tumours Locally advanced disease Metastatic
Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 23 March 2012, Sao Paulo, Brazil Surgery of RCC Locally confined (small) renal tumours Locally advanced disease Metastatic
Who are Candidates for Laparoscopic or Open Radical Nephrectomy. Arieh Shalhav
 Who are Candidates for Laparoscopic or Open Radical Nephrectomy Arieh Shalhav Fritz Duda Chair of Urologic Surgery Professor of Surgery and the Comprehensive Cancer Research Center Who are Candidates for
Who are Candidates for Laparoscopic or Open Radical Nephrectomy Arieh Shalhav Fritz Duda Chair of Urologic Surgery Professor of Surgery and the Comprehensive Cancer Research Center Who are Candidates for
John Fitzpatrick Memorial Lecture. John Fitzpatrick Memorial lecture
 John Fitzpatrick Memorial Lecture John Fitzpatrick Memorial Lecture John M Fitzpatrick, 1948 2014 Head of Research at the Irish Cancer Society Professor of Surgery and Consultant Urologist at the Mater
John Fitzpatrick Memorial Lecture John Fitzpatrick Memorial Lecture John M Fitzpatrick, 1948 2014 Head of Research at the Irish Cancer Society Professor of Surgery and Consultant Urologist at the Mater
Attachment #2 Overview of Follow-up
 Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Debate: Lymphadenectomy is Important in mrcc, CON P. Mulder, M.D., Ph.D. JJ. Patard, MD, Ph.D.
 Debate: Lymphadenectomy is Important in mrcc, CON P. Mulder, M.D., Ph.D. JJ. Patard, MD, Ph.D.. Eighth European International Kidney Cancer Symposium Budapest 03-04 May 2013 The role of LND In organ confined
Debate: Lymphadenectomy is Important in mrcc, CON P. Mulder, M.D., Ph.D. JJ. Patard, MD, Ph.D.. Eighth European International Kidney Cancer Symposium Budapest 03-04 May 2013 The role of LND In organ confined
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
1/25/13 Right partial nephrectomy followed by completion right radical nephrectomy.
 History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
Renal cancer in adults
 Renal cancer in adults Diagnosis, treatment and follow-up NADIA BENAHMED, JO ROBAYS, SABINE STORDEUR, THIERRY GIL, STEVEN JONIAU, NICOLAAS LUMEN, LAURETTE RENARD, SANDRINE RORIVE, DIRK SCHRIJVERS, BERTRAND
Renal cancer in adults Diagnosis, treatment and follow-up NADIA BENAHMED, JO ROBAYS, SABINE STORDEUR, THIERRY GIL, STEVEN JONIAU, NICOLAAS LUMEN, LAURETTE RENARD, SANDRINE RORIVE, DIRK SCHRIJVERS, BERTRAND
RCC in ADPKD / CKD / ESRD
 RCC in ADPKD / CKD / ESRD FOIU 2018 David A. Goldfarb, MD,FACS Professor of Surgery, Cleveland Clinic Lerner College of Medicine Glickman Urological and Kidney Institute Cleveland Clinic, Cleveland, Ohio
RCC in ADPKD / CKD / ESRD FOIU 2018 David A. Goldfarb, MD,FACS Professor of Surgery, Cleveland Clinic Lerner College of Medicine Glickman Urological and Kidney Institute Cleveland Clinic, Cleveland, Ohio
Surveillance following treatment of primary ocular melanoma
 Surveillance following treatment of primary ocular melanoma Introduction 50% of UM patients relapse with predominantly liver metastases Risk of metastatic disease can be predicted relatively accurately
Surveillance following treatment of primary ocular melanoma Introduction 50% of UM patients relapse with predominantly liver metastases Risk of metastatic disease can be predicted relatively accurately
ROBOTIC VS OPEN RADICAL CYSTECTOMY
 ROBOTIC VS OPEN RADICAL CYSTECTOMY A REVIEW Colin Lundeen December 14, 2016 Objectives Review the history of radical cystectomy Critically analyze recent RCTs comparing open radical cystectomy (ORC) to
ROBOTIC VS OPEN RADICAL CYSTECTOMY A REVIEW Colin Lundeen December 14, 2016 Objectives Review the history of radical cystectomy Critically analyze recent RCTs comparing open radical cystectomy (ORC) to
Revisione Oral Abstracts
 Revisione Oral Abstracts Francesco Massari Oncologia Medica Azienda Ospedaliero Universitaria di Bologna Policlinico S. Orsola-Malpighi UPDATES and NEWS from the Genitourinary Cancers Symposium - Milano,
Revisione Oral Abstracts Francesco Massari Oncologia Medica Azienda Ospedaliero Universitaria di Bologna Policlinico S. Orsola-Malpighi UPDATES and NEWS from the Genitourinary Cancers Symposium - Milano,
Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches
 Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches Cary N Robertson MD FACS Associate Professor Division of Urology Associate Director Urologic Oncology Duke Cancer
Partial Nephrectomy Techniques for Renal Preservation: Historical and Modern Approaches Cary N Robertson MD FACS Associate Professor Division of Urology Associate Director Urologic Oncology Duke Cancer
Appendix 4 Urology Care Pathways
 Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
GUIDELINES ON PROSTATE CANCER
 10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
Focal Ablative Therapies for Kidney Cancer
 Focal Ablative Therapies for Kidney Cancer Robert J. Hamilton, MD, MPH, FRCSC Staff Urologist, Princess Margaret Cancer Centre Assistant Prof., Dept. of Surgery (Urology), University of Toronto ICUC January
Focal Ablative Therapies for Kidney Cancer Robert J. Hamilton, MD, MPH, FRCSC Staff Urologist, Princess Margaret Cancer Centre Assistant Prof., Dept. of Surgery (Urology), University of Toronto ICUC January
Work-up/Follow-up: Baseline and Surveillance Studies for Cutaneous Melanoma Patients
 2018 AAD Annual Meeting, San Diego, CA Work-up/Follow-up: Baseline and Surveillance Studies for Cutaneous Melanoma Patients Susan M. Swetter, MD, FAAD Professor of Dermatology Director, Pigmented Lesion
2018 AAD Annual Meeting, San Diego, CA Work-up/Follow-up: Baseline and Surveillance Studies for Cutaneous Melanoma Patients Susan M. Swetter, MD, FAAD Professor of Dermatology Director, Pigmented Lesion
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better?
 Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Follow-up Care of Breast Cancer Patients
 Follow-up Care of Breast Cancer Patients Dr. Simon D. Baxter, MD, FRCPC Medical Oncologist BC Cancer Kelowna Clinical Instructor, Dept of Medicine University of British Columbia 19 April 2018 Disclosures
Follow-up Care of Breast Cancer Patients Dr. Simon D. Baxter, MD, FRCPC Medical Oncologist BC Cancer Kelowna Clinical Instructor, Dept of Medicine University of British Columbia 19 April 2018 Disclosures
RENAL CANCER GUIDELINES
 Greater Manchester and Cheshire Cancer Network RENAL CANCER GUIDELINES Agreed by Urology CSG: July 2010 Review Date: July 2012 Renal Cancer Guidelines 1. Introduction 1.1 Kidney cancer accounts for 3%
Greater Manchester and Cheshire Cancer Network RENAL CANCER GUIDELINES Agreed by Urology CSG: July 2010 Review Date: July 2012 Renal Cancer Guidelines 1. Introduction 1.1 Kidney cancer accounts for 3%
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Best Papers. F. Fusco
 Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Solitary Contralateral Adrenal Metastases after Nephrectomy for Renal Cell Carcinoma
 Original Report ISSN 1537-744X; DOI 10.1100/tsw.2004.39 Solitary Contralateral Adrenal after Nephrectomy for Renal Cell Carcinoma Nikolaos Antoniou, M.D. and Demetrios Karanastasis, M.D. General Hospital
Original Report ISSN 1537-744X; DOI 10.1100/tsw.2004.39 Solitary Contralateral Adrenal after Nephrectomy for Renal Cell Carcinoma Nikolaos Antoniou, M.D. and Demetrios Karanastasis, M.D. General Hospital
STAGING AND FOLLOW-UP STRATEGIES
 ATHENS 4-6 October 2018 European Society of Urogenital Radiology STAGING AND FOLLOW-UP STRATEGIES Ahmet Tuncay Turgut, MD Professor of Radiology Hacettepe University, Faculty of Medicine Ankara 2nd ESUR
ATHENS 4-6 October 2018 European Society of Urogenital Radiology STAGING AND FOLLOW-UP STRATEGIES Ahmet Tuncay Turgut, MD Professor of Radiology Hacettepe University, Faculty of Medicine Ankara 2nd ESUR
CONSENSUS STATEMENT. Abstract. Introduction
 CONSENSUS STATEMENT Kidney Cancer Research Network of Canada consensus statement on the role of adjuvant therapy after nephrectomy for high-risk, non-metastatic renal cell carcinoma: A comprehensive analysis
CONSENSUS STATEMENT Kidney Cancer Research Network of Canada consensus statement on the role of adjuvant therapy after nephrectomy for high-risk, non-metastatic renal cell carcinoma: A comprehensive analysis
Proton or Photon RT for Retroperitoneal Sarcomas
 Principle Investigator Thomas F. DeLaney, M.D. Contact Additional Info Institution Thomas DeLaney, MD 617-726-6876 tdelaney@partners.org www.clinicaltrials.gov NCT01659203 Massachusetts General Hospital
Principle Investigator Thomas F. DeLaney, M.D. Contact Additional Info Institution Thomas DeLaney, MD 617-726-6876 tdelaney@partners.org www.clinicaltrials.gov NCT01659203 Massachusetts General Hospital
Patient Reported Weight Loss Predicts Recurrence Rate in Renal Cell Cancer Cases after Nephrectomy
 DOI:10.22034/APJCP.2018.19.4.891 RESEARCH ARTICLE Editorial Process: Submission:01/04/2017 Acceptance:09/11/2017 Patient Reported Weight Loss Predicts Recurrence Rate in Renal Cell Cancer Cases after Nephrectomy
DOI:10.22034/APJCP.2018.19.4.891 RESEARCH ARTICLE Editorial Process: Submission:01/04/2017 Acceptance:09/11/2017 Patient Reported Weight Loss Predicts Recurrence Rate in Renal Cell Cancer Cases after Nephrectomy
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Follow-up investigations. Omgo E. Nieweg
 Follow-up investigations Omgo E. Nieweg Systematic literature review follow-up investigations identify few patients with recurrence frequent false positive findings impact on survival unclear Nieweg, Surg
Follow-up investigations Omgo E. Nieweg Systematic literature review follow-up investigations identify few patients with recurrence frequent false positive findings impact on survival unclear Nieweg, Surg
Targeted Therapies in the Management of Non-Small Cell Lung Cancer. A Multi-Disciplinary Approach
 Targeted Therapies in the Management of Non-Small Cell Lung Cancer A Multi-Disciplinary Approach Course Faculty Medical Oncologists: Dr. Barb Melosky British Columbia Cancer Agency, Vancouver, BC Dr. Jeff
Targeted Therapies in the Management of Non-Small Cell Lung Cancer A Multi-Disciplinary Approach Course Faculty Medical Oncologists: Dr. Barb Melosky British Columbia Cancer Agency, Vancouver, BC Dr. Jeff
Presentation of Cases /Audience Voting/Panel/Discussion
 Presentation of Cases /Audience Voting/Panel/Discussion JJ Patard Tim O Brien Ninth European International Kidney Cancer Symposium Dublin 25-26 April 2014 Clinical case 1 63 years old women Medical past
Presentation of Cases /Audience Voting/Panel/Discussion JJ Patard Tim O Brien Ninth European International Kidney Cancer Symposium Dublin 25-26 April 2014 Clinical case 1 63 years old women Medical past
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Adam J. Hansen, MD UHC Thoracic Surgery
 Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer. Dr. Simon Yu Nov 18, 2017
 GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer Dr. Simon Yu Nov 18, 2017 Faculty/Presenter Disclosure Faculty: Dr. Simon Yu Relationships with commercial interests: Grants/Research
GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer Dr. Simon Yu Nov 18, 2017 Faculty/Presenter Disclosure Faculty: Dr. Simon Yu Relationships with commercial interests: Grants/Research
North of Scotland Cancer Network Clinical Management Guideline for Carcinoma of the Uterine Cervix
 THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
Bone Metastases in Muscle-Invasive Bladder Cancer
 Journal of the Egyptian Nat. Cancer Inst., Vol. 18, No. 3, September: 03-08, 006 AZZA N. TAHER, M.D.* and MAGDY H. KOTB, M.D.** The Departments of Radiation Oncology* and Nuclear Medicine**, National Cancer
Journal of the Egyptian Nat. Cancer Inst., Vol. 18, No. 3, September: 03-08, 006 AZZA N. TAHER, M.D.* and MAGDY H. KOTB, M.D.** The Departments of Radiation Oncology* and Nuclear Medicine**, National Cancer
GUIDELINES ON PENILE CANCER
 GUIDELINES ON PENILE CANCER (Text updated March 2005) G. Pizzocaro (chairman), F. Algaba, S. Horenblas, H. van der Poel, E. Solsona, S. Tana, N. Watkin 58 Penile Cancer Eur Urol 2004;46(1);1-8 Introduction
GUIDELINES ON PENILE CANCER (Text updated March 2005) G. Pizzocaro (chairman), F. Algaba, S. Horenblas, H. van der Poel, E. Solsona, S. Tana, N. Watkin 58 Penile Cancer Eur Urol 2004;46(1);1-8 Introduction
Management of High Risk Renal Cell Carcinoma
 Management of High Risk Renal Cell Carcinoma Peter E. Clark, MD Professor and Chair, Department of Urology Carolinas HealthCare System Chair, Urologic Oncology Levine Cancer Institute October 14, 2017
Management of High Risk Renal Cell Carcinoma Peter E. Clark, MD Professor and Chair, Department of Urology Carolinas HealthCare System Chair, Urologic Oncology Levine Cancer Institute October 14, 2017
Attachment #2 Overview of Follow-up
 Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Rationale for VEGFR-targeted Therapy in RCC
 Rationale for VEGFR-targeted Therapy in RCC EIKCS, Budapest, May 2013 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial Management Group Honoraria Astra Zeneca + + + Astellas
Rationale for VEGFR-targeted Therapy in RCC EIKCS, Budapest, May 2013 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial Management Group Honoraria Astra Zeneca + + + Astellas
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER
 GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
Localized Prostate Cancer Have we finally got it right? Shingai Mutambirwa Professor & Chair-Division Urology DGMAH & SMU Pretoria SOUTH AFRICA
 Localized Prostate Cancer Have we finally got it right? Shingai Mutambirwa Professor & Chair-Division Urology DGMAH & SMU Pretoria SOUTH AFRICA ESMO Cape Town 14 Feb 2018 Disclosures Advisory boards/lecturer/consultant-
Localized Prostate Cancer Have we finally got it right? Shingai Mutambirwa Professor & Chair-Division Urology DGMAH & SMU Pretoria SOUTH AFRICA ESMO Cape Town 14 Feb 2018 Disclosures Advisory boards/lecturer/consultant-
When PSA fails. Urology Grand Rounds Alexandra Perks. Rising PSA after Radical Prostatectomy
 When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
Follow-up Care of Breast Cancer Patients
 Follow-up Care of Breast Cancer Patients Dr. Simon D. Baxter, MD, FRCPC Medical Oncologist BC Cancer Kelowna Clinical Instructor, Dept of Medicine University of British Columbia 24 November 2018 Disclosures
Follow-up Care of Breast Cancer Patients Dr. Simon D. Baxter, MD, FRCPC Medical Oncologist BC Cancer Kelowna Clinical Instructor, Dept of Medicine University of British Columbia 24 November 2018 Disclosures
How to deal with patients with isolated peritoneal metastases
 ESMO Preceptorship Programme Colorectal Valencia 18-19 May 2018 Michel DUCREUX, MD, PhD Gustave Roussy Cancer Centre, Grand Paris, FRANCE How to deal with patients with isolated peritoneal metastases DISCLOSURE
ESMO Preceptorship Programme Colorectal Valencia 18-19 May 2018 Michel DUCREUX, MD, PhD Gustave Roussy Cancer Centre, Grand Paris, FRANCE How to deal with patients with isolated peritoneal metastases DISCLOSURE
NUMERATOR: Reports that include the pt category, the pn category and the histologic grade
 Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Breast Cancer Basics. Clinical Oncology for Public Health Professionals. Ben Ho Park, MD, PhD
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
Cytoreductive Nephrectomy
 Cytoreductive Nephrectomy Stephen H. Culp, M.D., Ph.D. Assistant Professor, Department of Urology Outline The Historics of CN The current status of CN The importance of patient selection Cytoreductive
Cytoreductive Nephrectomy Stephen H. Culp, M.D., Ph.D. Assistant Professor, Department of Urology Outline The Historics of CN The current status of CN The importance of patient selection Cytoreductive
RCC in Adolescents and Young Adults (AYAs): Diagnosis and Management
: Diagnosis and Management") RCC in Adolescents and Young Adults (AYAs): Diagnosis and Management Nicholas G. Cost, M.D. Assistant Professor, Department of Surgery, Division of Urology University of Colorado Cancer Center Fifteenth
RCC in Adolescents and Young Adults (AYAs): Diagnosis and Management Nicholas G. Cost, M.D. Assistant Professor, Department of Surgery, Division of Urology University of Colorado Cancer Center Fifteenth
Bladder Cancer Guidelines
 Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Renal Mass Biopsy Should be Used for Most SRM - PRO
 Renal Mass Biopsy Should be Used for Most SRM - PRO Tony Finelli, MD, MSc, FRCSC Head, Division of Urology GU Site Lead, Princess Margaret Cancer Center GU Cancer Lead, Cancer Care Ontario Associate Professor,
Renal Mass Biopsy Should be Used for Most SRM - PRO Tony Finelli, MD, MSc, FRCSC Head, Division of Urology GU Site Lead, Princess Margaret Cancer Center GU Cancer Lead, Cancer Care Ontario Associate Professor,
Gynecologic Cancer Surveillance and Survivorship: Informing Practice and Policy
 Gynecologic Cancer Surveillance and Survivorship: Informing Practice and Policy Stephanie Yap, M.D. University Gynecologic Oncology Northside Cancer Institute Our Learning Objectives Review survival rates,
Gynecologic Cancer Surveillance and Survivorship: Informing Practice and Policy Stephanie Yap, M.D. University Gynecologic Oncology Northside Cancer Institute Our Learning Objectives Review survival rates,
By: Tania Cortas, MD Arizona Oncology 03/10/2015
 By: Tania Cortas, MD Arizona Oncology 03/10/2015 Epidemiology In the United States, CRC incidence rates have declined about 2 to 3 percent per year over the last 15 years Death rates from CRC have declined
By: Tania Cortas, MD Arizona Oncology 03/10/2015 Epidemiology In the United States, CRC incidence rates have declined about 2 to 3 percent per year over the last 15 years Death rates from CRC have declined
NUMERATOR: Reports that include the pt category, the pn category and the histologic grade
 Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Optimal Treatment of ct1b Renal Mass in Patient with Normal GFR: a Role for Radical Nephrectomy?
 Optimal Treatment of ct1b Renal Mass in Patient with Normal GFR: a Role for Radical Nephrectomy? Steven C. Campbell, MD, PhD Program Director, Vice Chairman Department of Urology Center for Urologic Oncology
Optimal Treatment of ct1b Renal Mass in Patient with Normal GFR: a Role for Radical Nephrectomy? Steven C. Campbell, MD, PhD Program Director, Vice Chairman Department of Urology Center for Urologic Oncology
Case Based Urology Learning Program
 Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 18 CBULP 2011 041 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 18 CBULP 2011 041 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
GUIDELINES ON TESTICULAR CANCER
 38 (Text updated March 2005) P. Albers (chairman), W. Albrecht, F. Algaba, C. Bokemeyer, G. Cohn-Cedermark, A. Horwich, O. Klepp, M.P. Laguna, G. Pizzocaro Introduction Compared with other types of cancer
38 (Text updated March 2005) P. Albers (chairman), W. Albrecht, F. Algaba, C. Bokemeyer, G. Cohn-Cedermark, A. Horwich, O. Klepp, M.P. Laguna, G. Pizzocaro Introduction Compared with other types of cancer
Recruiting Active; not recruiting Completed Suspended Terminated. The biological sex of the patient. Female Unknown
 Clinical Data Form Kidney Carcinoma Clinical Trial Sequencing Project Page 1 The Clinical Data Form (CDF) should be completed for every case. This form can be completed at the time the samples are submitted,
Clinical Data Form Kidney Carcinoma Clinical Trial Sequencing Project Page 1 The Clinical Data Form (CDF) should be completed for every case. This form can be completed at the time the samples are submitted,