Dianne S Cheung, MD FACE Assistant Clinical Professor UCLA Health David Geffen School of Medicine CA-AACE Chapter Secretary
|
|
|
- Annabel Hensley
- 5 years ago
- Views:
Transcription
1 Dianne S Cheung, MD FACE Assistant Clinical Professor UCLA Health David Geffen School of Medicine CA-AACE Chapter Secretary
2 No Financial Disclosures
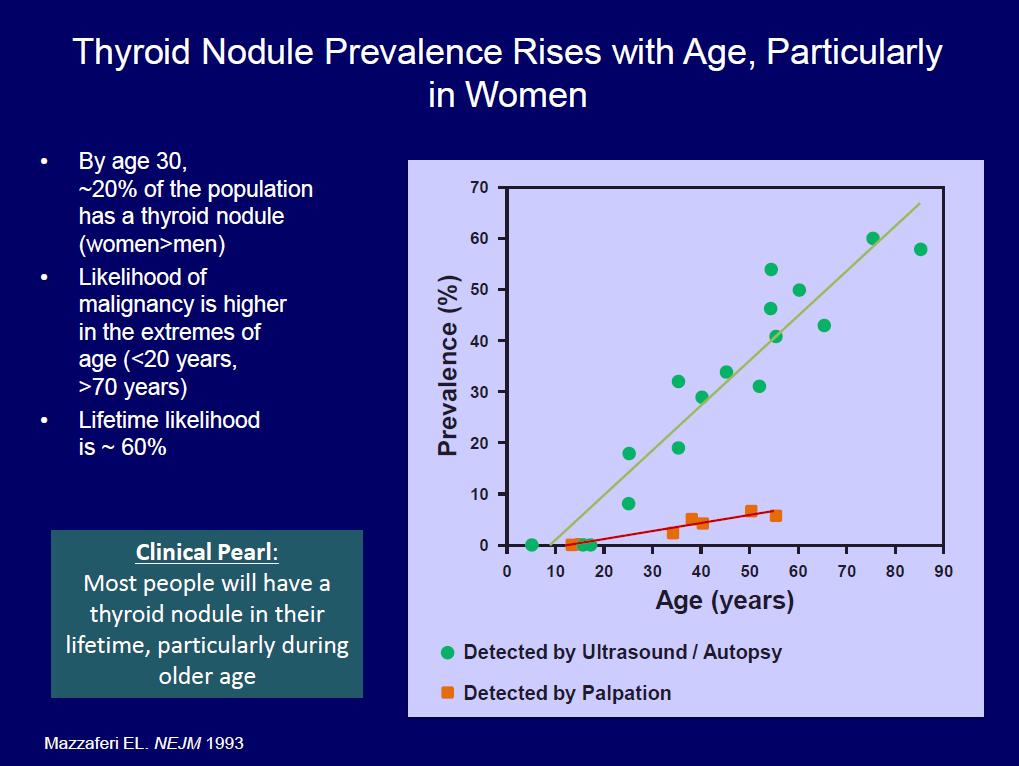
3 Objectives Which thyroid labs to order and interpret? Hot topic - Interference of biotin in our thyroid lab assays Thyroid ultrasound real time versus reports RAIU scans are they important? Thyroid cases Pregnancy Subclinical Hypothyroidism Subacute thyroiditis Hyperthyroidism Incidental Thyroid Nodule
 deiodinase 4.")

4 Thyroid Action 1. TRH TSH 2. T3 and T4 3. T4 T3 tissues (liver/muscle) deiodinase 4. Some T4 and T3 conjugated liver, excreted in bile, partially hydrolyzed in intestine ATA
5 Total Thyroid hormones Relies on binding proteins Total T4 = Bound to TBG, albumin, or TBPA (99.97% serum T4) cannot uptake into cells (storage pool) Total T3 = Bound more tightly to albumin (less tightly to TBG or TBPA) (99.7%)
6 Total Thyroid hormones Raises serum TBG Estrogens Tamoxifen Raloxifen Methadone 5-flurouracil Clofibrate Heroin Mitotane Lowers serum TBG Androgens Danaxol Glucocorticoids Slow-release niacin I-asparaginase
7 Free thyroid hormones Free Hormone Hypothesis Only free hormone metabolically active and determines thyroid status (not total which is largely bound to binding proteins) 4 ways to measure T4 (free T4 estimates) Gold standard: Equilibrium Dialysis for T4 (expensive) Measures distribution of Free T4 at equilibrium across a dialysis membrane Direct free T4 (most common it s automated) Takes some binding abnormalities into account Free T4 index (thyroid hormone binding ratio via T3 resin uptake) takes into account some binding protein abnormalities but not all Total T4/TBG 2 ways to measure T3 Direct T3 (automated) not as reliable levels can vary Free T3 index
8 Typical thyroid labs normal ranges vary with lab Thyroid lab description interpretation or use Pitfalls examples TSH (3 rd gen) Free T4 auto Free T3 auto Initial lab for function Estimate of free T4 Estimate of free T3 TSH low = hyperthyroid TSH high = hypothyroid Can use for thyrotoxic patient If TSH high can use to look at degree of hyothyroidism Useful if hypoth from pituitary/hypothalamic dz Can use for thyrotoxic patient High in patients on T3 Low TSH in pituitary injury/disease High in TSHoma TSH lags recent hyper/graves treated Resistance to thyroid hormone Sick euthyroid Unreliable pregnancy can be falsely low (use TT4 or FT4 index) but can use if there is trimester specific ranges available NOT useful to dose LT4 Not reliable alone Total T4 Total bound and free T4 available Can use in pregnancy, Total T4 (and TT3) rise approximately 50% first half pregnancy and plateaus at 20 weeks NOT for hypothyroid assessment Drugs/illness alter binding protein levels In pregnancy TBG increase 2-fold higher than nonpregnant state Drugs can raise or lower TBG Total T3 Total bound and free T3 available Useful for thyrotoxic assessment NOT for hypothyroid assessment Drugs/illness alter binding protein levels In pregnancy TBG increase 2-fold higher than nonpregnant state Drugs can raise or lower TBG
9 Nonthyroidal illness and Reverse T3 D3 deiodinase induced in critical illness especially hypoxemia/ischemia clearance of rt3 to diiodothyronine (T2) is reduced in nonthyroidal illness because of inhibition of the 5'-monodeiodinase activity (D1) RT3 high in nonthyroidal illness Can use to differientiate central hypothyrodism from nonthryoidal illness Not useful to diagnose hypothyroidism or dosing thyroid medication as can be normal, high or low (variable) People with hypothyroid may have low RT3 but also still have enough T4 to convert to RT3 and be normal Burmeister. Thyroid 1995
10 So what lab to order? 1. Screening (assuming normal hypoth-pit axis) TSH first, if normal you re done TSH high order free T4 to determine degree of hypothyroidism TSH low order free T3 to determine degree of hyperthyrodism 2. If already on levothyroxine (LT4) order TSH to adjust dose If secondary to pituitary or hypothalmic disease, when TSH secretion impaired, use free T4 to titrate dose 3. If early hyperthyroid treatment TSH lags behind for weeks or months sometimes, check free T4 and free T3

11 Cure for Hair loss?

12 Or Thyroid lab confusion?
: 30 µg/day 10-15")
13 What is Biotin (Vitamin B7)? Water soluble vitamin Naturally found in meat, fish, eggs, dairy Action: catalyst for carboxylase enzymes important in macronutrient metabolism Recommended Daily Allowance (RDA): 30 µg/day mg/day or 333-fold of RDA found in biotin supplements that are popular for presumptive health benefits Popular for (Li et al, JAMA 2017;318) Hair and nails Multiple sclerosis Diabetic neuropathy Lipid disorders Images from
14 Biotin (Vitamin B7): FDA Safety Communication 11/28/17 Biotin in blood or other samples taken from patients who are ingesting high levels of biotin in dietary supplements can cause clinically significant incorrect lab test results. The FDA has seen an increase in the number of reported adverse events, including one death, related to biotin interference with lab tests. Death was a patient who was ingesting high levels of biotin supplement showing low troponin who suffered MI had falsely low troponin levels attributed to biotin interference (
15 Biotin (Vitamin B7): FDA Safety Communication 11/28/17 Biotin in patient samples can cause falsely high or falsely low results, depending on the test. Incorrect test results may lead to inappropriate patient management or misdiagnosis. For example, a falsely low result for troponin, a clinically important biomarker to aid in the diagnosis of heart attacks, may lead to a missed diagnosis and potentially serious clinical implications. The FDA has received a report that one patient taking high levels of biotin died following falsely low troponin test results when a troponin test known to have biotin interference was used. (
16 Biotin (Vitamin B7): FDA Safety Communication 11/28/17 Most of the published research on biotin interference covers hormone tests, such as Intact parathyroid hormone (PTH) thyroid stimulating hormone (TSH) T4 and T3 tests (total and free) Troponin However, because biotin is used in so many immunoassays, scientists say it could interfere with many others (HCG, FSH, LH, prolactin, vitamin D25OH, etc)
17 Biotin (Vitamin B7): Interference Biotin technology in many automated assays Biotinylated antibodies and analogues strongly bind to streptavidin Depends on Assay If sandwich assay where analyte is sandwiched between two antibodies result may be falsely lowered due to inference If competitive assay where analyte competes with labeled analyte for binding, may be falsely elevated due to intereference Image from Thermofisher labs
18 Thyroid Assays using biotin Thyroid lab Type Assay Result TSH Sandwich or immunometric Falsely low FT4, Total T4 Competitive Falsely high FT3, Total T3 Competitive Falsely high TBII Competitive Falsely high

19 Is it Graves? Kids on High dose Biotin Kummer S et al NEJM 375;7 August 18, 2016
20 Recommendations Hold all biotin containing vitamins for hours prior to lab draw Vitamins can include MVI Prenatal vitamins Hair and Nail vitamins B complex

21
22 Case 1 32 yo female who is G1P0 approximately 11 weeks pregnant was referred to endocrinology by her OB following initial screening test showing TSH 0.09 ng/dl for 2 nd opinion. Patient has lost approximately 8-lbs in the last 4-weeks She is tachycardic with HR 100 bpm She reports pale, tremor, anxiety and heat intolerance On exam she has nontender slightly enlarged thyroid gland, no palpable nodules, no proptosis or lid lag She was seen by another MD and told to start PTU immediately for the treatment of Graves disease in pregnancy Ultrasound was ordered to evaluate for nodules


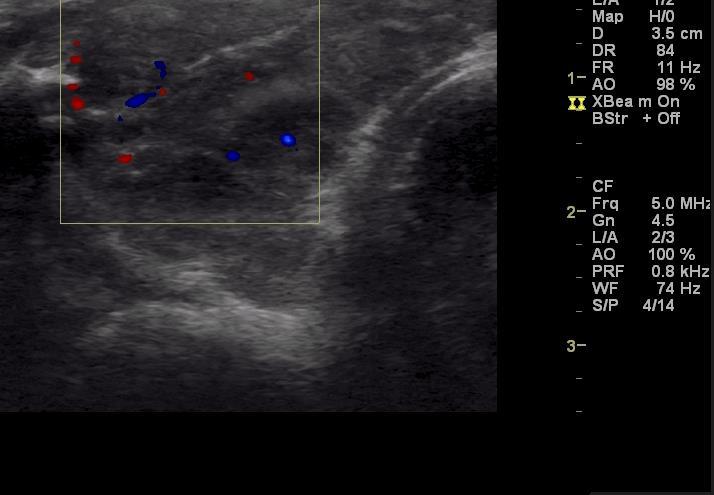
23 Case 1 US report highly vascular heterogenous enlarged thyorid gland
24 Case 1 PTU yes or no? What else do you want to know?
25 Case 1 On further questioning Patient reports nauseated and severe vomiting in the last 4-weeks She is not able to eat more than just a few bites of food and has not been hydrating Labs were ordered showing TT3, TT4, and free T4 index normal TSRAbs: TSI negative and TBII negative antitpo negative Tg Ab negative

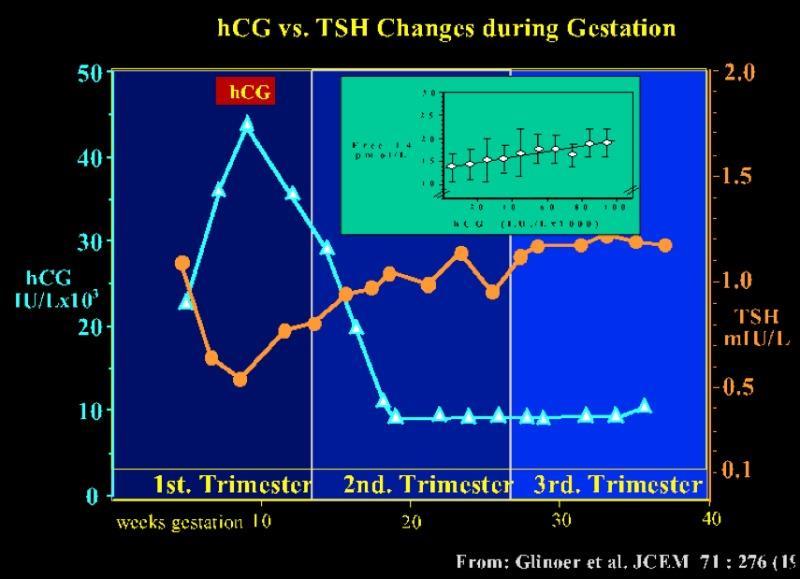
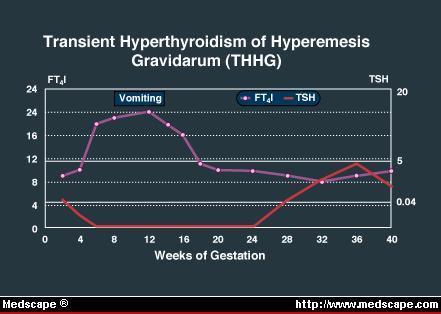
26 HCG and TSH Homology Human chorionic gonadotropin (hcg) is one of a family of glycoprotein hormones, including TSH, with a common alpha subunit and a unique beta subunit. There is considerable homology between the beta subunits of hcg and TSH. As a result, hcg has weak thyroid-stimulating activity Thyroid-stimulating activity in sera of normal pregnant women correlates with serum hcg levels Thyroid gland of normal pregnant women may be stimulated by hcg to secrete slightly excessive quantities of T4 Maternal thyroid glands may secrete more thyroid hormone during early pregnancy in response to the thyrotropic activity of hcg that overrides the normal operation of the hypothalamic-pituitary-thyroid feedback system. Biochemical hyperthyroidism associated with hyperemesis gravidarum has been attributed to hcg. Yoshimura et al. Thyroid Oct;5(5):
27
28
29 Case 1 things to know Alexander EK et al ATA guidelines for the diagnosis and management of thyroid disease in during pregnancy and postpartum TSH may be decreased in 1 st trimester of normal pregnancy due to HCG stimulating effect on TSH receptor Peak HCG level occurs at 7-11 weeks gestation Serum TSH <0.1 mu/l may be present in approximately 5% of women by week 11 of pregnancy Any subnormal TSH level should be evaluated with serum TT4 (0r FT4) and T3 values Biochemical overt hyperthyroidism is confirmed in presence of suppressed or undectable TSH and inappropriately elevated serum TT4, FT4, or T3
30 Case 1 - What to ask? Alexander EK et al ATA guidelines for the diagnosis and management of thyroid disease in during pregnancy and postpartum Take a good history Physical exam Measure maternal serum FT4 or TT4 Measure maternal serum TRAbs and TT3
31 Case 1 Gestational Transient Thyrotoxicosis Alexander EK et al ATA guidelines for the diagnosis and management of thyroid disease in during pregnancy and postpartum Depends on severity symptoms If hyperemesis gravidum control vomiting and treat dehydration Antithyroidal drugs (ATDs) not indicated because serum T4 returns to normal at weeks gestation and early ATD use increase risk of birth defects Small beta blocker dose can be used over limited time In some isolated cases ATDs have been used for symptomatic relief without improvement in OB outcomes compared to supportive care but no studies comparing the two have been reported.
32 Case 2 62 yo male with who presented to his primary care MD for annual physical, was found on screening to have TSH 6.7 (normal lab miu/l) He denies fatigue, weight gain, or cold intolerance He reports that thyroid problem with my mom but I don t know what Patient is reporting hard time losing weight with BMI 42 On physical exam his thyroid gland was small and unremarkable Patient is here to ask if he should take thyroid medication to lose weight due to the TSH elevation
33 Case 2 On redraw TSH again was slightly elevated at 7.0 antitpo was negative Thyroid ultrasound showed normal appearing homogenous gland without nodules or increase in vascularity Do we treat?
34 Subclinical Hypothyroidism (SHypo) Defined as usually normal T4 levels TSH outside of upper limit normal reference range for lab but <10 miu/l Most patients are asymptomatic Strong expert support for treatment of patients with serum TSH concentrations >10 miu/l However the routine treatment of asymptomatic patients with TSH values between 4.5 and 10 miu/l remains controversial
:76. Epub 2007 Nov 8.")
35 Subclinical Hypothyroidism Biondi B, Cooper DS SO Endocr Rev. 2008;29(1):76. Epub 2007 Nov 8.

36 Severity of primary hypothyroidism symptoms

37 What is the cut off for normal TSH?

38 Age and TSH
 than controls Biondi B, Cooper DS SO Endocr Rev. 2008;29(1):76.")
39 Cardiac benefits of treating SHypo Subclinically hypothyroid patients had a more prolonged isovolumetric relaxation time and an impaired time-to-peak filling rate (which are parameters of altered left ventricular diastolic function) than controls Biondi B, Cooper DS SO Endocr Rev. 2008;29(1):76. Epub 2007 Nov 8.
40 Case 2 Garber et al. ATA/AACE Guidelines for Hypothyroidism in Adults Endocr Pract.2012;18(No. 6) The prevalence of SHypo has been reported to be between 4 and 10% of adult population samples thus common SHypo is more frequent in areas of iodine sufficiency 4.2% in iodine-deficient areas compared with 23.9% in areas of abundant iodine intake Depends on the cutoff used to define SHypo and differences in age, gender, and dietary iodine intake in the populations studied.


41 Case 2 Garber et al. ATA/AACE Guidelines for Hypothyroidism in Adults Endocr Pract.2012;18(No. 6)
42 Case 3 19 year old female college student developed severe strep throat with painful tender thyroid gland She presents with difficulty swallowing, weight loss of 5-lbs in 2-weeks, insomnia, tremor, and heat intolerance She was given antibiotics for presumed strep throat, but her thyroid gland continues to be enlarged and tender to the touch despite finishing course What does she have?
43 Subclinical thyroiditis Cause: viral or postviral, typically with h/o URI 2-8 weeks prior to thryoiditis Presents: pain 96% time, tender gland Mechanism: inflammation damages thyroid follicles activating protelysis of thyroglobulin in follicles leading to upregulated release of T4 and T3 Continues until depletes thyroglobulin stores Phases: HYPER NORMAL HYPO NORMAL Each phase lasts 2-8 weeks Recovery usually complete
44 Subclinical thyroiditis Self limiting Some due get severely hyperthyroid Labs: Suppressed TSH, high T3 and T4 High sed rate or CRP Can get RAIU scan Typically avoid FNA unless concern about lymphoma, abscess, cancer though waiting for thyroiditis to improve is best for quality of FNA result Ultrasound thyroid gland rule out thyroid nodules or masses Doppler color flow low flow = thyroiditis versus high flow = Graves
45 Subclinical thyroiditis RAIU scan usually shows low uptake in thyroiditis <1-3% Singh K. NucRadshare.com
46 Subacute thyroiditis treatment Pain relief (no observational studies, just clinical experience so no correct way) NSAIDs: naproxen mg twice daily, ibuprofen up to 800mg qid Prednisone: start 40mg daily and reduce 5-10mg every 5-7 days Pain should get better after 1-2 days, if severe pain returns after dose lowered, go back up to the higher dose and maintain for 1-2 weeks dose and taper again You can taper faster or slower based on symptoms but goal is to use the lowest dose of steroids to achieve symptom relief Sympotmatic thyroiditis Can use beta blockers but avoid thionamidies (PTU or methimazole) since hyperthyrodism is not due to thryoid hormone synthesis excess Radioactive iodine is not effective or indicated = remember RAIU scan uptake is very low, so it would not work
47 Case 4 30 yo female physician presents to me with 4-month history of anxiety, palpitaitons, and weight loss (10-lbs) She also noted right upper neck swelling for approximately 6-months but denies compressive symptoms She is a radiologist and had a her colleague at the hospital proceed to do ultrasound guided fine needle aspiration The pathology came back indeterminate despite multiple needle passes and bloody, the patient is now concerned she may have a thyroid malignancy which is causing her symptoms She was told that based on the indeterminant FNA (follicular lesion unknown significance) she had a 5-15% chance of malignancy
48 Case 4 She has no lab work, said she is fine and just wanted another FNA On physical exam HR 102 bpm, palpable right approximately 2cm soft and mobile nodule, nontender, overall gland is enlarged 2 times normal Patient has hand tremor and is diaphoretic I proceeded to ultrasound her first
49 Case 4 Seshadri KG 2017 IJEM


50 Case 4
51 Case 4 What do we do next? FNA? Labs? Radioactive iodine uptake scan? surgery since previous FNA was Indeterminant?
52 Case 4 I advised the patient I would like to order thyroid labs as her nodule is quite vascular to rule out hyperthyroidism TSH 0.02 Free T3 (2x ULN) Free T4 (1.5x ULN) TRAbs (TSI, TBII negative) antitpo and TgAb negative

53 Case 4 radioactive iodine uptake scan
54 Case American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and other causes of Thyrotoxicosis Ross, Burch, et al., Thyroid. Oct 2016, 26(10): Beta-adrenergic blockade is recommended in all patients with symptomatic thyrotoxicosis Strong recommendation, moderate-quality evidence patients with overtly Toxic multinodular goiter or toxic adenoma be treated with RAI therapy or thyroidectomy. On occasion, long-term, low-dose treatment with MMI may be appropriate. Weak recommendation, moderate-quality evidence
55 Case American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and other causes of Thyrotoxicosis Ross, Burch, et al., Thyroid. Oct 2016, 26(10): For patients with single toxic nodule the risk of treatment failure is < 1% after surgical resection (ipsilateral thyroid lobectomy or isthmusectomy). Typically, euthyroidism is achieved within days after surgery. The prevalence of hypothyroidism varies from 2% to 3% following lobectomy for TA For patients with TA who receive RAI therapy there is a 6% 18% risk of persistent hyperthyroidism and a 3% 5.5% risk of recurrent hyperthyroidism There is a 75% response rate by 3 months and 89% rate by 1 year following RAI therapy for TA
56 Case American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and other causes of Thyrotoxicosis Ross, Burch, et al., Thyroid. Oct 2016, 26(10): Nonfunctioning nodules on radionuclide scintigraphy or nodules with suspicious ultrasound characteristics should be managed according to published guidelines regarding thyroid nodules in euthyroid individuals. Strong recommendation, moderate-quality evidence (ATA 2015 thyroid nodules guidelines) If surgery is chosen as treatment for TMNG or TA, patients with overt hyperthyroidism should be rendered euthyroid prior to the procedure with MMI pretreatment, with or without b-adrenergic blockade. Preoperative iodine should not be used in this setting. Strong recommendation, low-quality evidence.
57 Case American Thyroid Association Guidelines for Diagnosis and Management of Hyperthyroidism and other causes of Thyrotoxicosis Ross, Burch, et al., Thyroid. Oct 2016, 26(10): Patient wished to proceed with surgery Pre-surgery ultrasound did not show ipsilateral nodule(s) Patient was given methimazole 20mg daily and propranolol 10mg tid She was rendered euthyroid prior to surgery Proceeded with right thyroidectomy Pathology was benign thyroid nodule Patient did not require thyroid hormone replacement post surgery
58 Case 5 62 yo male presents with concerns that he has a tumor sticking out of my neck he has noticed only in the last few months Radiology report patient brought of recent thyroid ultrasound identified 4.5 cm right mid thyroid nodule which is partially cystic and smaller 1.5 cm right lower solid nodule but no parathyroid adenoma noted reading He presented to me for possible ultrasound guidedbiopsy of both nodules
59 When to FNA thyroid nodule? Is it based on size of nodule? Does appearance matter? Ultrasound guidance? Radioactive iodine uptake scan needed? Cold or hot nodule important?
60
61
62
63

64 Case 5 real time ultrasound


65 Case 5 Ultrasound report did not mention parathyroid adenoma Note polar artery and echogenic line
66 Case 5 -Additional studies and history TSH was 1.20 ipth 130, Ca , ionized Ca 1.40, VitD25 OH 32 Does report being told by other MDs to stop taking calcium or avoid dairy DEXA bone density done T -2.6 AP spine
67 Case 5 Right inferior parathyroid adenoma confirmed on 4D CT-parathyroid scan Ultrasound guided FNA done of right 4.5 cm nodule was benign adenoma with cystic degeneration Patient proceeded to right inferior parathyroidectomy and right lobectomy
68 Case 5 - Lessons Review the ultrasound report If you can, do one yourself or view the images If uncertain ask for real-time ultrasound to be done by radiologist or endocrinologist Determine based on ultrasound characteristics if thyroid nodules need to be biopsied Always take a good history

69
Approach to thyroid dysfunction
 Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Hyperthyroidism Diagnosis and Treatment. April Janet A. Schlechte, M.D.
 Hyperthyroidism Diagnosis and Treatment Family Practice Refresher Course April 2015 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any
Hyperthyroidism Diagnosis and Treatment Family Practice Refresher Course April 2015 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any
Thyrotoxicosis in Pregnancy: Diagnose and Management
 Thyrotoxicosis in Pregnancy: Diagnose and Management Yuanita Asri Langi email: meralday@yahoo.co.id Endocrinology & Metabolic Division, Internal Medicine Department, Prof.dr.R.D. Kandou Hospital/ Sam Ratulangi
Thyrotoxicosis in Pregnancy: Diagnose and Management Yuanita Asri Langi email: meralday@yahoo.co.id Endocrinology & Metabolic Division, Internal Medicine Department, Prof.dr.R.D. Kandou Hospital/ Sam Ratulangi
Disorders of Thyroid Function
 Disorders of Thyroid Function Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Thyroid Hormone Axis Hypothalamus TRH
Disorders of Thyroid Function Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Thyroid Hormone Axis Hypothalamus TRH
Understanding Thyroid Labs
 Understanding Thyroid Labs Chris Sadler, MA, PA-C, CDE, DFAAPA Senior Medical Science Liaison CVM Janssen Scientific Affairs Diabetes and Endocrine Associates La Jolla, CA Disclosures Employee of Janssen
Understanding Thyroid Labs Chris Sadler, MA, PA-C, CDE, DFAAPA Senior Medical Science Liaison CVM Janssen Scientific Affairs Diabetes and Endocrine Associates La Jolla, CA Disclosures Employee of Janssen
Chapter I.A.1: Thyroid Evaluation Laboratory Testing
 Chapter I.A.1: Thyroid Evaluation Laboratory Testing Jennifer L. Poehls, MD and Rebecca S. Sippel, MD, FACS THYROID FUNCTION TESTS Overview Thyroid-stimulating hormone (TSH) is produced by the anterior
Chapter I.A.1: Thyroid Evaluation Laboratory Testing Jennifer L. Poehls, MD and Rebecca S. Sippel, MD, FACS THYROID FUNCTION TESTS Overview Thyroid-stimulating hormone (TSH) is produced by the anterior
Lecture title. Name Family name Country
 Lecture title Name Family name Country Nguyen Thy Khue, MD, PhD Department of Endocrinology HCMC University of Medicine and Pharmacy, MEDIC Clinic Hochiminh City, Viet Nam Provided no information regarding
Lecture title Name Family name Country Nguyen Thy Khue, MD, PhD Department of Endocrinology HCMC University of Medicine and Pharmacy, MEDIC Clinic Hochiminh City, Viet Nam Provided no information regarding
LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS
 LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS Maryam Tohidi Anatomical & clinical pathologist Research Institute for Endocrine Sciences THYROID GLAND (15-25 gr), (12-20 gr), 2 lobes connected by
LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS Maryam Tohidi Anatomical & clinical pathologist Research Institute for Endocrine Sciences THYROID GLAND (15-25 gr), (12-20 gr), 2 lobes connected by
Disclosures. Learning objectives. Case 1A. Autoimmune Thyroid Disease: Medical and Surgical Issues. I have nothing to disclose.
 Disclosures Autoimmune Thyroid Disease: Medical and Surgical Issues I have nothing to disclose. Chrysoula Dosiou, MD, MS Clinical Assistant Professor Division of Endocrinology Stanford University School
Disclosures Autoimmune Thyroid Disease: Medical and Surgical Issues I have nothing to disclose. Chrysoula Dosiou, MD, MS Clinical Assistant Professor Division of Endocrinology Stanford University School
Hyperthyroidism. Objectives. Clinical Manifestations. Slide 1. Slide 2. Slide 3. Implications for Primary Care. hyperthyroidism
 1 Hyperthyroidism Implications for Primary Care Laura A. Ruby, DNP, CRNP Wellspan Endocrinology 2 Objectives! Discuss the clinical manifestations of hyperthyroidism! Review the use of the diagnostic studies!
1 Hyperthyroidism Implications for Primary Care Laura A. Ruby, DNP, CRNP Wellspan Endocrinology 2 Objectives! Discuss the clinical manifestations of hyperthyroidism! Review the use of the diagnostic studies!
Update In Hyperthyroidism
 Update In Hyperthyroidism CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
Update In Hyperthyroidism CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
Thyroid Disease. I have no disclosures. Overview TSH. Matthew Kim, M.D. July, 2012
 Thyroid Disease I have no disclosures Matthew Kim, M.D. July, 2012 Overview Thyroid Function Tests Hyperthyroidism Hypothyroidism Subclinical Thyroid Disease Thyroid Nodules Questions TSH Best single screening
Thyroid Disease I have no disclosures Matthew Kim, M.D. July, 2012 Overview Thyroid Function Tests Hyperthyroidism Hypothyroidism Subclinical Thyroid Disease Thyroid Nodules Questions TSH Best single screening
Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017
 Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017 I will not be discussing this Outline of discussion Laboratory tests for thyroid function Diagnosis of hypothyroidism Treatment of
Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017 I will not be discussing this Outline of discussion Laboratory tests for thyroid function Diagnosis of hypothyroidism Treatment of
Pregnancy & Thyroid. Zohreh Moosavi Associate professor of Endocriology Imam Reza General Hospital Mashad University. Imam Reza weeky Conferance
 Pregnancy & Thyroid Zohreh Moosavi Associate professor of Endocriology Imam Reza General Hospital Mashad University Imam Reza weeky Conferance Objectives Thyroid Disorders & Pregnancy Normal thyroid phsyiology
Pregnancy & Thyroid Zohreh Moosavi Associate professor of Endocriology Imam Reza General Hospital Mashad University Imam Reza weeky Conferance Objectives Thyroid Disorders & Pregnancy Normal thyroid phsyiology
Table 1: Thyroid panel. Result (reference interval) TSH 89.5 miu/l ( ) Total T4 5.2 µg/dl ( ) T3 uptake 39% (22-35)
 TSH 89.5 miu/l ( ) Total T4 5.2 µg/dl ( ) T3 uptake 39% (22-35)") Introduction Thyroid disease is the second most common endocrine disorder (behind diabetes), and its prevalence increases with increasing age. The incidence of newly diagnosed thyroid cancer is increasing
Introduction Thyroid disease is the second most common endocrine disorder (behind diabetes), and its prevalence increases with increasing age. The incidence of newly diagnosed thyroid cancer is increasing
None. Thyroid Potpourri for the Primary Care Physician. Evaluating Thyroid Function. Disclosures. Learning Objectives
 Thyroid Potpourri for the Primary Care Physician Ramya Vedula DO, MPH, ECNU Endocrinology, Diabetes and Metabolism Princeton Medical Group Assistant Professor of Clinical Medicine Rutgers Robert Wood Johnson
Thyroid Potpourri for the Primary Care Physician Ramya Vedula DO, MPH, ECNU Endocrinology, Diabetes and Metabolism Princeton Medical Group Assistant Professor of Clinical Medicine Rutgers Robert Wood Johnson
HYPERTHYROIDISM. Hypothalamus. Thyrotropin-releasing hormone (TRH) Anterior pituitary gland. Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3
 Anterior pituitary gland. Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3") HYPERTHYROIDISM Hypothalamus Thyrotropin-releasing hormone (TRH) Anterior pituitary gland Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3 In hyperthyroidism, there is an increased production of
HYPERTHYROIDISM Hypothalamus Thyrotropin-releasing hormone (TRH) Anterior pituitary gland Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3 In hyperthyroidism, there is an increased production of
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging. Deepa R Biyyam, MD Attending Pediatric Radiologist
 Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Thyroid disorders. Dr Enas Abusalim
 Thyroid disorders Dr Enas Abusalim Thyroid physiology The hypothalamic pituitary thyroid axis And peripheral conversion of T4 to T3, WHERE, AND BY WHAT ENZYME?? Only relatively small concentrations of
Thyroid disorders Dr Enas Abusalim Thyroid physiology The hypothalamic pituitary thyroid axis And peripheral conversion of T4 to T3, WHERE, AND BY WHAT ENZYME?? Only relatively small concentrations of
Understanding thyroid function tests. Dr. Colette George
 Understanding thyroid function tests Dr. Colette George Disclosures No financial disclosure I will present fictitious cases and thyroid function tests (TFTs) that are based on scenarios I commonly encounter.
Understanding thyroid function tests Dr. Colette George Disclosures No financial disclosure I will present fictitious cases and thyroid function tests (TFTs) that are based on scenarios I commonly encounter.
Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME
 Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME 795-7520 traskla@cmhc.org No disclosures Objectives To have an understanding of hyperthyroidism To have an understanding of the management
Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME 795-7520 traskla@cmhc.org No disclosures Objectives To have an understanding of hyperthyroidism To have an understanding of the management
OUTLINE. Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis
 THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
Thyroid Nodules. Objectives. Clinical Practice Guidelines for the Management of Thyroid Disorders
 9:45 1:45am Clinical Practice Guidelines for the Management of Thyroid Disorders SPEAKER Gregory Brent, MD Presenter Disclosure Information The following relationships exist related to this presentation:
9:45 1:45am Clinical Practice Guidelines for the Management of Thyroid Disorders SPEAKER Gregory Brent, MD Presenter Disclosure Information The following relationships exist related to this presentation:
Management of Thyroid Nodules. February 2 nd, 2018 Sarah Hopkins
 Management of Thyroid Nodules February 2 nd, 2018 Sarah Hopkins No disclosures Goals: Review Initial Evaluation of Thyroid Nodules Review Indications for Biopsy Approach to Multinodular Goiter Review Management
Management of Thyroid Nodules February 2 nd, 2018 Sarah Hopkins No disclosures Goals: Review Initial Evaluation of Thyroid Nodules Review Indications for Biopsy Approach to Multinodular Goiter Review Management
Common Issues in Management of Hypothyroidism
 Common Issues in Management of Hypothyroidism Family Medicine Refresher Course April 5, 2018 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Common Issues in Management of Hypothyroidism Family Medicine Refresher Course April 5, 2018 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases
 Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
THYROID DISEASES. CASE BASED WORKSHOP Z. Henry He, MD, PhD. Endocrinology, Diabetes, & Metabolism Cambridge Health Alliance Harvard Medical School
 THYROID DISEASES CASE BASED WORKSHOP Z. Henry He, MD, PhD Endocrinology, Diabetes, & Metabolism Cambridge Health Alliance Harvard Medical School DISCLOSURE I have no relevant financial disclosure OBJECTIVES
THYROID DISEASES CASE BASED WORKSHOP Z. Henry He, MD, PhD Endocrinology, Diabetes, & Metabolism Cambridge Health Alliance Harvard Medical School DISCLOSURE I have no relevant financial disclosure OBJECTIVES
Decoding Your Thyroid Tests and Results
 Decoding Your Thyroid Tests and Results Wondering about your thyroid test results? Learn about each test and what low, optimal, and high results may mean so you can work with your doctor to choose appropriate
Decoding Your Thyroid Tests and Results Wondering about your thyroid test results? Learn about each test and what low, optimal, and high results may mean so you can work with your doctor to choose appropriate
THYROID DISEASE IN CHILDREN
 THYROID DISEASE IN CHILDREN Michelle Schweiger, D.O. Center for Pediatric and Adolescent Endocrinology Cleveland Clinic Foundation Neither I nor any immediate family members have any financial interests
THYROID DISEASE IN CHILDREN Michelle Schweiger, D.O. Center for Pediatric and Adolescent Endocrinology Cleveland Clinic Foundation Neither I nor any immediate family members have any financial interests
Common Causes of Hypothyroidism
 Common Causes of Hypothyroidism Autoimmune thyroidi4s Surgical removal of thyroid gland Medica4on Therapy Iodine and iodine containing medica4ons Neck radia4on Post Partum thyroidi4s Prevalence of Hypothyroidism
Common Causes of Hypothyroidism Autoimmune thyroidi4s Surgical removal of thyroid gland Medica4on Therapy Iodine and iodine containing medica4ons Neck radia4on Post Partum thyroidi4s Prevalence of Hypothyroidism
5/3/2017. Ahn et al N Engl J Med 2014; 371
 Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Alvin C. Powers, M.D. 1/27/06
 Thyroid Histology Follicular Cells ECF side Apical lumen Thyroid Follicles -200-400 um Parafollicular or C-cells Colloid Photos from University of Manchester and tutorial created by Dr. James Crimando,
Thyroid Histology Follicular Cells ECF side Apical lumen Thyroid Follicles -200-400 um Parafollicular or C-cells Colloid Photos from University of Manchester and tutorial created by Dr. James Crimando,
BELIEVE MIDWIFERY SERVICES
 TITLE: THYROID DISEASE IN PREGNANCY EFFECTIVE DATE: July, 2013 POLICY STATEMENT: Pregnancy changes significantly the values influenced by the serum thyroid binding hormone level (i.e., total thyroxine,
TITLE: THYROID DISEASE IN PREGNANCY EFFECTIVE DATE: July, 2013 POLICY STATEMENT: Pregnancy changes significantly the values influenced by the serum thyroid binding hormone level (i.e., total thyroxine,
DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT ENDOCRINE SYSTEM AT A GLANCE OBJECTIVES ANATOMY OF THE THYROID
 OBJECTIVES DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT Stephanie Blackburn, MHS, MLS(ASCP) CM LSU Health Shreveport Clinical Laboratory Science Program Discuss the synthesis and action
OBJECTIVES DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT Stephanie Blackburn, MHS, MLS(ASCP) CM LSU Health Shreveport Clinical Laboratory Science Program Discuss the synthesis and action
The Thyroid and Pregnancy OUTLINE OF DISCUSSION 3/19/10. Francis S. Greenspan March 19, Normal Physiology. 2.
 The Thyroid and Pregnancy Francis S. Greenspan March 19, 2010 OUTLINE OF DISCUSSION 1. Normal Physiology 2. Hypothyroidism 3. Hyperthyroidism 4. Thyroid Nodules and Cancer NORMAL PHYSIOLOGY Iodine Requirements:
The Thyroid and Pregnancy Francis S. Greenspan March 19, 2010 OUTLINE OF DISCUSSION 1. Normal Physiology 2. Hypothyroidism 3. Hyperthyroidism 4. Thyroid Nodules and Cancer NORMAL PHYSIOLOGY Iodine Requirements:
Thyroid nodules 3/22/2011. Most thyroid nodules are benign. Thyroid nodules: differential diagnosis
 Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Thyroid nodules. Most thyroid nodules are benign
 Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
THE THYROID BOOK. Medical and Surgical Treatment of Thyroid Problems
 THE THYROID BOOK Medical and Surgical Treatment of Thyroid Problems Trouble with Your Thyroid Gland The thyroid is a small gland in your neck that plays a big role in how your body functions. It impacts
THE THYROID BOOK Medical and Surgical Treatment of Thyroid Problems Trouble with Your Thyroid Gland The thyroid is a small gland in your neck that plays a big role in how your body functions. It impacts
Virginia ACP Clinical Update Thyroid Clinical Pearls. University of Virginia. Richard J. Santen MD
 Virginia ACP Clinical Update Thyroid Clinical Pearls University of Virginia Richard J. Santen MD Goal Provide a guide to frequently encountered problems in thyroid disease Follow my approach to recently
Virginia ACP Clinical Update Thyroid Clinical Pearls University of Virginia Richard J. Santen MD Goal Provide a guide to frequently encountered problems in thyroid disease Follow my approach to recently
Hypothyroidism. Definition:
 Definition: Hypothyroidism Primary hypothyroidism is characterized biochemically by a high serum thyroidstimulating hormone (TSH) concentration and a low serum free thyroxine (T4) concentration. Subclinical
Definition: Hypothyroidism Primary hypothyroidism is characterized biochemically by a high serum thyroidstimulating hormone (TSH) concentration and a low serum free thyroxine (T4) concentration. Subclinical
Hyperthyroidism: Guidelines and Beyond. Douglas S Ross MD May Copyrighted slides omitted
 Hyperthyroidism: Guidelines and Beyond Douglas S Ross MD May 19 2018 Copyrighted slides omitted Abbott Laboratories Quest Diagnostics Disclosures Diagnosis Biochemical Assessment Biotin Interference Biotinylated
Hyperthyroidism: Guidelines and Beyond Douglas S Ross MD May 19 2018 Copyrighted slides omitted Abbott Laboratories Quest Diagnostics Disclosures Diagnosis Biochemical Assessment Biotin Interference Biotinylated
Case 1: 24 yo pregnant female presenting with abnormal TFTs and tachycardia RAJESH JAIN ENDORAMA 3/16/2017
 Case 1: 24 yo pregnant female presenting with abnormal TFTs and tachycardia RAJESH JAIN ENDORAMA 3/16/2017 Chief Complaint The ER calls about a 24 year old, 12 weeks pregnant. She presented with tachycardia
Case 1: 24 yo pregnant female presenting with abnormal TFTs and tachycardia RAJESH JAIN ENDORAMA 3/16/2017 Chief Complaint The ER calls about a 24 year old, 12 weeks pregnant. She presented with tachycardia
5/18/2013. Most thyroid nodules are benign. Thyroid nodules: new techniques in evaluation
 Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
THYROID AWARENESS. By: Karen Carbone. January is thyroid awareness month. At least 30 million Americans
 THYROID AWARENESS By: Karen Carbone January is thyroid awareness month. At least 30 million Americans have a thyroid disorder and half-15 million-are silent sufferers who are undiagnosed, according to
THYROID AWARENESS By: Karen Carbone January is thyroid awareness month. At least 30 million Americans have a thyroid disorder and half-15 million-are silent sufferers who are undiagnosed, according to
Thyroid Disease in Pregnancy: The Essentials. Elizabeth N. Pearce, MD, MSc
 Thyroid Disease in Pregnancy: The Essentials Elizabeth N. Pearce, MD, MSc None Disclosures Case 1 A 31-year-old woman from Massachusetts is practicing a vegan diet. She is currently planning a pregnancy.
Thyroid Disease in Pregnancy: The Essentials Elizabeth N. Pearce, MD, MSc None Disclosures Case 1 A 31-year-old woman from Massachusetts is practicing a vegan diet. She is currently planning a pregnancy.
1 day PTA: vaginal spotting, LE edema LMP 6 weeks ago. OSH Clinic: distended abdomen, (+) urine pregnancy; sent home with iron
 urine pregnancy; sent home with iron") Anila Bindal, MD 1 day PTA: vaginal spotting, LE edema LMP 6 weeks ago OSH Clinic: distended abdomen, (+) urine pregnancy; sent home with iron UCMC ER: abdomen doubled overnight, significant vaginal bleeding,
Anila Bindal, MD 1 day PTA: vaginal spotting, LE edema LMP 6 weeks ago OSH Clinic: distended abdomen, (+) urine pregnancy; sent home with iron UCMC ER: abdomen doubled overnight, significant vaginal bleeding,
B-Resistance to the action of hormones, Hormone resistance characterized by receptor mediated, postreceptor.
 Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
Thyroid Disease in Pregnancy. Justin Moore, MD
 Thyroid Disease in Pregnancy Justin Moore, MD Case 1 22 yr old G1P0 female at 14 2/7 weeks presents with tremor Weight stable since first positive pregnancy test Some nausea, rare vomiting TSH 0.02 miu/l,
Thyroid Disease in Pregnancy Justin Moore, MD Case 1 22 yr old G1P0 female at 14 2/7 weeks presents with tremor Weight stable since first positive pregnancy test Some nausea, rare vomiting TSH 0.02 miu/l,
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Gland. Patient Information
 Thyroid Gland Patient Information Contact details for Endocrine and Thyroid Clinics Hawke s Bay Fallen Soldiers Memorial Hospital Villa 16 Phone: 06 8788109 ext 5891 Text: 0274 102 559 Email: endoclinic@hbdhb.govt.nz
Thyroid Gland Patient Information Contact details for Endocrine and Thyroid Clinics Hawke s Bay Fallen Soldiers Memorial Hospital Villa 16 Phone: 06 8788109 ext 5891 Text: 0274 102 559 Email: endoclinic@hbdhb.govt.nz
Update on Gestational Thyroid Disease. Aidan McElduff The Discipline of Medicine, The University of Sydney
 IADPSG 2016 Update on Gestational Thyroid Disease Aidan McElduff The Discipline of Medicine, The University of Sydney IADPSG 2016 DISCLOSURES and AIM Nil to disclose Aim: to provide an overview 2017 Guidelines
IADPSG 2016 Update on Gestational Thyroid Disease Aidan McElduff The Discipline of Medicine, The University of Sydney IADPSG 2016 DISCLOSURES and AIM Nil to disclose Aim: to provide an overview 2017 Guidelines
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
TANJA KEMP INTERNAL MEDICINE: ENDOCRINOLOGY
 ENDOCRINE DISORDERS IN THE ELDERLY (part 2) TANJA KEMP INTERNAL MEDICINE: ENDOCRINOLOGY Pituitary axis Target organs of the pituitary gland Negative feedback Hypothalamus-Pituitary-Thyroid axis Thyroid
ENDOCRINE DISORDERS IN THE ELDERLY (part 2) TANJA KEMP INTERNAL MEDICINE: ENDOCRINOLOGY Pituitary axis Target organs of the pituitary gland Negative feedback Hypothalamus-Pituitary-Thyroid axis Thyroid
Evaluation and Management of Thyroid Nodules. Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada
 Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Updates in Thyroid Disease. Thyroid Outline. Thyroid 10/5/2015. Leila Wing, MD. Endocrinology, Diabetes, and Metabolism
 Updates in Thyroid Disease Leila Wing, MD Endocrinology, Diabetes, and Metabolism Background Hypothyroidism Hyperthyroidism Thyroid nodules Thyroid Cancer Conclusions Resources/References Thyroid Outline
Updates in Thyroid Disease Leila Wing, MD Endocrinology, Diabetes, and Metabolism Background Hypothyroidism Hyperthyroidism Thyroid nodules Thyroid Cancer Conclusions Resources/References Thyroid Outline
Thyroid Function TSH Analyte Information
 Thyroid Function TSH Analyte Information 1 2013-05-01 Thyroid-stimulating hormone (TSH) Introduction Thyroid-stimulating hormone (thyrotropin, TSH) is a glycoprotein with molecular weight of approximately
Thyroid Function TSH Analyte Information 1 2013-05-01 Thyroid-stimulating hormone (TSH) Introduction Thyroid-stimulating hormone (thyrotropin, TSH) is a glycoprotein with molecular weight of approximately
Hyperthyroidism, Inflammatory Disorders
 Hyperthyroidism, Inflammatory Disorders free T4 Howard J. Sachs, MD www.12daysinmarch.com Hyperthyroidism, Inflammatory Disorders The total T4 may be elevated in pregnancy and with OCP use Graves I 123
Hyperthyroidism, Inflammatory Disorders free T4 Howard J. Sachs, MD www.12daysinmarch.com Hyperthyroidism, Inflammatory Disorders The total T4 may be elevated in pregnancy and with OCP use Graves I 123
Slide notes: This presentation provides information on Graves disease, a systemic autoimmune disease. Epidemiology, pathology, complications,
 1 This presentation provides information on Graves disease, a systemic autoimmune disease. Epidemiology, pathology, complications, including ophthalmic complications, treatments (both permanent solutions
1 This presentation provides information on Graves disease, a systemic autoimmune disease. Epidemiology, pathology, complications, including ophthalmic complications, treatments (both permanent solutions
university sciences of Isfahan university Com
 Introduce R. Gholamnezhad Lecturer of school of nursing & midwifery of Iran university Ph.D student tof Immunology, Sh School of medical sciences of Isfahan university E-Mail: Gholami278@gmail. Com Interpreting
Introduce R. Gholamnezhad Lecturer of school of nursing & midwifery of Iran university Ph.D student tof Immunology, Sh School of medical sciences of Isfahan university E-Mail: Gholami278@gmail. Com Interpreting
Pearls and Pitfalls of Thyroid Diagnosis. Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS
 Pearls and Pitfalls of Thyroid Diagnosis Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS Thyroid Anatomy Isthmus of gland located 1 fingerbreadth below cricoid cartilage
Pearls and Pitfalls of Thyroid Diagnosis Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS Thyroid Anatomy Isthmus of gland located 1 fingerbreadth below cricoid cartilage
Diseases of thyroid & parathyroid glands (1 of 2)
") Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
Toxic MNG Thyroiditis 5-15
 Hyperthyroidism Facts Prevalence 0.5-1.0%, more common in women Thyrotoxicosis is excess thyroid hormones from endogenous or exogenous sources Hyperthyroidism is excess thyroid hormones from thyroid gland
Hyperthyroidism Facts Prevalence 0.5-1.0%, more common in women Thyrotoxicosis is excess thyroid hormones from endogenous or exogenous sources Hyperthyroidism is excess thyroid hormones from thyroid gland
4) Thyroid Gland Defects - Dr. Tara
 Thyroid Gland Defects - Dr. Tara") 4) Thyroid Gland Defects - Dr. Tara Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3, T4 T4 has negative feedback on secretion
4) Thyroid Gland Defects - Dr. Tara Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3, T4 T4 has negative feedback on secretion
Thyroid Plus. Central Thyroid Regulation & Activity. Peripheral Thyroid Function. Thyroid Auto Immunity. Key Guide. Patient: DOB: Sex: F MRN:
 Thyroid Plus Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4) 127 127
Thyroid Plus Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4) 127 127
Thyroiditis Diagnosis and Management issues. Prof. Md. Enamul Karim Professor of Medicine Dhaka Medical College
 Thyroiditis Diagnosis and Management issues Prof. Md. Enamul Karim Professor of Medicine Dhaka Medical College Definition Thyroiditis is a general term that refers to inflammation of the thyroid gland.
Thyroiditis Diagnosis and Management issues Prof. Md. Enamul Karim Professor of Medicine Dhaka Medical College Definition Thyroiditis is a general term that refers to inflammation of the thyroid gland.
An Approach to: Thyroid Function Tests. Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital
 An Approach to: Thyroid Function Tests Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital Regulation of Thyroid axis Hypothalamus TRH T3,T4 ---- TRH Median Eminence (base of brain)
An Approach to: Thyroid Function Tests Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital Regulation of Thyroid axis Hypothalamus TRH T3,T4 ---- TRH Median Eminence (base of brain)
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 No Disclosures Disease Of the Thyroid Iodide Metabolism/Synthesis of Thyroid Hormone Trap Oxidation Organification(catalyzed
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 No Disclosures Disease Of the Thyroid Iodide Metabolism/Synthesis of Thyroid Hormone Trap Oxidation Organification(catalyzed
Approach to Thyroid Nodules
 Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Sample Type - Serum Result Reference Range Units. Central Thyroid Regulation Surrey & Activity KT3 4Q. Peripheral Thyroid D Function mark
 Thyroid Plus Sample Type - Serum Result Reference Range Units Central Thyroid Regulation Surrey & Activity KT3 4Q Total Thyroxine (T4)
Thyroid Plus Sample Type - Serum Result Reference Range Units Central Thyroid Regulation Surrey & Activity KT3 4Q Total Thyroxine (T4)
AUGUST 25-27, 2017 UPDATE & BOARD REVIEW. acofp INTENSIVE. Evolving Issues in Endocrinology. Chris Pitsch, DO INNOVATIVE COMPREHENSIVE HANDS-ON
 acofp INTENSIVE UPDATE & BOARD REVIEW AUGUST 25-27, 2017 Loews Chicago O'Hare Hotel Rosemont, IL INNOVATIVE COMPREHENSIVE HANDS-ON Evolving Issues in Endocrinology Chris Pitsch, DO acofp Am eric an College
acofp INTENSIVE UPDATE & BOARD REVIEW AUGUST 25-27, 2017 Loews Chicago O'Hare Hotel Rosemont, IL INNOVATIVE COMPREHENSIVE HANDS-ON Evolving Issues in Endocrinology Chris Pitsch, DO acofp Am eric an College
The Thyroid: No mystery. Just need all the pieces to the puzzle.
 The Thyroid: No mystery. Just need all the pieces to the puzzle. Todd Chennell, MS, RN ANP-C Endocrine surgery University of Rochester 2018 1 According to the American Thyroid Association, 12 percent of
The Thyroid: No mystery. Just need all the pieces to the puzzle. Todd Chennell, MS, RN ANP-C Endocrine surgery University of Rochester 2018 1 According to the American Thyroid Association, 12 percent of
Pitfalls of TFTs Interpretation
 Mohammad Reza Bakhtiari DCLS, PhD Pitfalls of TFTs Interpretation CME July 2006 Vol.24 No.7, http://keck.usc.edu HPT axis physiology Log-linear relationship between TSH and FT4 Patient Specific Set Point
Mohammad Reza Bakhtiari DCLS, PhD Pitfalls of TFTs Interpretation CME July 2006 Vol.24 No.7, http://keck.usc.edu HPT axis physiology Log-linear relationship between TSH and FT4 Patient Specific Set Point
Thyroid gland defects. Dr. Tara Husain
 Thyroid gland defects Dr. Tara Husain Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3,T4 T4 has negative feed back on secretion
Thyroid gland defects Dr. Tara Husain Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3,T4 T4 has negative feed back on secretion
Pathophysiology of Thyroid Disorders. PHCL 415 Hadeel Alkofide April 2010
 Pathophysiology of Thyroid Disorders PHCL 415 Hadeel Alkofide April 2010 1 Learning Objectives Understand the pathophysiology of hyperthyroidism & hypothyroidism Describe the signs & symptoms of hyperthyroidism
Pathophysiology of Thyroid Disorders PHCL 415 Hadeel Alkofide April 2010 1 Learning Objectives Understand the pathophysiology of hyperthyroidism & hypothyroidism Describe the signs & symptoms of hyperthyroidism
Thyroid nodules - medical and surgical management. Endocrinology and Endocrine Surgery Manchester Royal Infirmary
 Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Some Issues in the Management of Hypothyroidism
 Some Issues in the Management of Hypothyroidism Family Medicine Refresher Course April 6, 2016 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Some Issues in the Management of Hypothyroidism Family Medicine Refresher Course April 6, 2016 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Graves Disease in Pediatrics
 Graves Disease in Pediatrics Graves disease is a common cause of an overactive thyroid. It occurs in about 1 in 5000 children and teens. It occurs more often in females than males. This booklet is designed
Graves Disease in Pediatrics Graves disease is a common cause of an overactive thyroid. It occurs in about 1 in 5000 children and teens. It occurs more often in females than males. This booklet is designed
Thyroid function testing in pregnancy: 2017 ATA guidelines update. Dr Simon Forehan
 Thyroid function testing in pregnancy: 2017 ATA guidelines update Dr Simon Forehan Several factors are known to tax gravid thyroid economy: Increased plasma volume TBG pool increased Renal clearance Feto-placental
Thyroid function testing in pregnancy: 2017 ATA guidelines update Dr Simon Forehan Several factors are known to tax gravid thyroid economy: Increased plasma volume TBG pool increased Renal clearance Feto-placental
Strange thyroid function tests: biological pitfall or real pathology? Fleur Wolff, LHUB-ULB, September 2017
 Strange thyroid function tests: biological pitfall or real pathology? Fleur Wolff, LHUB-ULB, September 2017 Introduction o Immunoassays widely used in laboratory practice High throughput measurement Rapidity
Strange thyroid function tests: biological pitfall or real pathology? Fleur Wolff, LHUB-ULB, September 2017 Introduction o Immunoassays widely used in laboratory practice High throughput measurement Rapidity
Iodine 131 thyroid Therapy. Sara G. Johnson, MBA, CNMT, NCT President SNMMI-TS VA Healthcare System San Diego
 Iodine 131 thyroid Therapy Sara G. Johnson, MBA, CNMT, NCT President SNMMI-TS VA Healthcare System San Diego OBJECTIVES Describe the basics of thyroid gland anatomy and physiology Outline the disease process
Iodine 131 thyroid Therapy Sara G. Johnson, MBA, CNMT, NCT President SNMMI-TS VA Healthcare System San Diego OBJECTIVES Describe the basics of thyroid gland anatomy and physiology Outline the disease process
Amiodarone Induced Thyrotoxicosis Treatment? (AIT)
") Amiodarone Induced Thyrotoxicosis Treatment? (AIT) Presentation of a Case Report Annelies Tonnelier Brigitte Velkeniers 14-12-2013 1 1. Background 1. Case report 2. Investigations 3. Diagnosis 4. Treatment
Amiodarone Induced Thyrotoxicosis Treatment? (AIT) Presentation of a Case Report Annelies Tonnelier Brigitte Velkeniers 14-12-2013 1 1. Background 1. Case report 2. Investigations 3. Diagnosis 4. Treatment
25/10/56. Hypothyroidism Myxedema in adults Cretinism congenital deficiency of thyroid hormone Hashimoto thyroiditis. Simple goiter (nontoxic goiter)
") THERAPEUTIC USES OF THYROID HORMONE Supeecha Wittayalertpunya Wannarasmi Ketchart Nov 2013 Hyperthyroidism (Thyrotoxicosis) Grave s disease (diffuse toxic goiter) Toxic uninodular & Toxic multinodular
THERAPEUTIC USES OF THYROID HORMONE Supeecha Wittayalertpunya Wannarasmi Ketchart Nov 2013 Hyperthyroidism (Thyrotoxicosis) Grave s disease (diffuse toxic goiter) Toxic uninodular & Toxic multinodular
Approach to Thyroid Dysfunction in the Elderly
 Approach to Thyroid Dysfunction in the Elderly Fernando Melaragno Endocrinology Objective The objective of this lecture is to review the epidemiology, clinical presentation, risks and complications, and
Approach to Thyroid Dysfunction in the Elderly Fernando Melaragno Endocrinology Objective The objective of this lecture is to review the epidemiology, clinical presentation, risks and complications, and
Hypothyroidism and Hyperthyroidism. Paul V. Tomasic, MD, MS, FACP, FACE Nevada AACE EFNE & Annual Meeting October 6, 2018
 Hypothyroidism and Hyperthyroidism Paul V. Tomasic, MD, MS, FACP, FACE Nevada AACE EFNE & Annual Meeting October 6, 2018 Disclosures: None related to this program or presentation Objectives: Hypothyroidism
Hypothyroidism and Hyperthyroidism Paul V. Tomasic, MD, MS, FACP, FACE Nevada AACE EFNE & Annual Meeting October 6, 2018 Disclosures: None related to this program or presentation Objectives: Hypothyroidism
Thyroid. Dr Jessica Triay November 2018
 Thyroid Dr Jessica Triay November 2018 Hypothyroidism in Pregnancy Clinical update: Hypothyroidism in Pregnancy Take home messages Additional evidence supportive for more relaxed TSH targets for those
Thyroid Dr Jessica Triay November 2018 Hypothyroidism in Pregnancy Clinical update: Hypothyroidism in Pregnancy Take home messages Additional evidence supportive for more relaxed TSH targets for those
Hypothalamo-Pituitary-Thyroid Axis
 SMGr up Hypothalamo-Pituitary-Thyroid Axis Orluwene Chituru Godwill 1 * and Ohiri John U 1 1 Chemical Pathology Department, University of Port Harcourt Teaching Hospital, Nigeria *Corresponding author:
SMGr up Hypothalamo-Pituitary-Thyroid Axis Orluwene Chituru Godwill 1 * and Ohiri John U 1 1 Chemical Pathology Department, University of Port Harcourt Teaching Hospital, Nigeria *Corresponding author:
Thyroid and Antithyroid Drugs. Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014
 Thyroid and Antithyroid Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed
Thyroid and Antithyroid Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed
19th Century Thyroidology
 1 19th Century Thyroidology Dr. Kinnicutt s patient (1893) A cold, tired, constipated middle aged woman Slow pulse rate Low body temperature From physiology it was likely patient needed thyroid replacement
1 19th Century Thyroidology Dr. Kinnicutt s patient (1893) A cold, tired, constipated middle aged woman Slow pulse rate Low body temperature From physiology it was likely patient needed thyroid replacement
The Presence of Thyroid Autoantibodies in Pregnancy
 The Presence of Thyroid Autoantibodies in Pregnancy Dr. O Sullivan does not have any financial relationships with any commercial interests. KATIE O SULLIVAN, MD FELLOW, ADULT/PEDIATRIC ENDOCRINOLOGY ENDORAMA
The Presence of Thyroid Autoantibodies in Pregnancy Dr. O Sullivan does not have any financial relationships with any commercial interests. KATIE O SULLIVAN, MD FELLOW, ADULT/PEDIATRIC ENDOCRINOLOGY ENDORAMA
Thyroid Management. Evolving Controversy - Science, Dogma, Opinion. The Ogden Surgical Medical Society May 2016
 Thyroid Management Evolving Controversy - Science, Dogma, Opinion The Ogden Surgical Medical Society May 2016 Published Guidelines AACE and ATA - Clinical Practice Guidelines in 2012 Guidelines are neither
Thyroid Management Evolving Controversy - Science, Dogma, Opinion The Ogden Surgical Medical Society May 2016 Published Guidelines AACE and ATA - Clinical Practice Guidelines in 2012 Guidelines are neither
Page 1. Understanding Common Thyroid Disorders. Cases. Topics Covered
 Cases Understanding Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 66 yr old female with 1 yr of fatigue and lassitude and no findings except TSH=8.2,
Cases Understanding Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 66 yr old female with 1 yr of fatigue and lassitude and no findings except TSH=8.2,
Thyroid Disorders. January 2019
 Thyroid Disorders January 2019 What is the Thyroid? The thyroid is a small butterfly-shaped gland inside the neck, located in front of the trachea (windpipe) and below the larynx (voicebox). It produces
Thyroid Disorders January 2019 What is the Thyroid? The thyroid is a small butterfly-shaped gland inside the neck, located in front of the trachea (windpipe) and below the larynx (voicebox). It produces
Thyroid disorder for Resident
 Thyroid disorder for Resident Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Topics Abnormal thyroid function test Euthyroid
Thyroid disorder for Resident Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health Topics Abnormal thyroid function test Euthyroid
THYROID HORMONES: An Overview
 1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY PBL SEMINAR MBBS III; BMLS & BDS Year 3 What are the Thyroid Hormones? THYROID
1 SCHOOL OF MEDICINE AND HEALTH SCIENCES DIVISION OF BASIC MEDICAL SCIENCES DISCIPLINE OF BIOCHEMISTRY AND MOLECULAR BIOLOGY PBL SEMINAR MBBS III; BMLS & BDS Year 3 What are the Thyroid Hormones? THYROID
The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital
 The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital Presentation Today: Common thyroid problems and treatments Pregnancy related thyroid problems The suppressed
The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital Presentation Today: Common thyroid problems and treatments Pregnancy related thyroid problems The suppressed
Requesting and Management of abnormal TFTs.
 Requesting and Management of abnormal TFTs. At the request of a number of GPs I have produced summary guidelines surrounding thyroid testing. These have been agreed with our Endocrinology leads Dr Bell
Requesting and Management of abnormal TFTs. At the request of a number of GPs I have produced summary guidelines surrounding thyroid testing. These have been agreed with our Endocrinology leads Dr Bell
Understanding Your Blood Tests by Larry Levin, MD
 Bulletin #42 GRAVES DISEASE & THYROID FOUNDATION Educate * Encourage * Empower P.O. Box 2793 Rancho Santa Fe, CA 92067 (877) 643-3123 www.gdatf.org info@gdatf.org Understanding Your Blood Tests by Larry
Bulletin #42 GRAVES DISEASE & THYROID FOUNDATION Educate * Encourage * Empower P.O. Box 2793 Rancho Santa Fe, CA 92067 (877) 643-3123 www.gdatf.org info@gdatf.org Understanding Your Blood Tests by Larry
Effect of thyroid hormones of metabolism Thyroid Diseases
 Effect of thyroid hormones of metabolism Thyroid Diseases Medical Perspective Aspects That Will Be Addressed Regulation of thyroid hormone secretion Basic physiology Hyperthyroidism Hypothyroidism Thyroiditis
Effect of thyroid hormones of metabolism Thyroid Diseases Medical Perspective Aspects That Will Be Addressed Regulation of thyroid hormone secretion Basic physiology Hyperthyroidism Hypothyroidism Thyroiditis
NSC 830: Drugs Affecting the Thyroid BROOKE BENTLEY, PHD, APRN
 NSC 830: Drugs Affecting the Thyroid BROOKE BENTLEY, PHD, APRN Hypothalamus-Pituitary-Thyroid Hormone Axis TSH: Normal = 0.5-5 mu/l Free T4: 1.3-3.8 ng/dl 1 Hypothyroidism: Thyroid Agents Natural Health
NSC 830: Drugs Affecting the Thyroid BROOKE BENTLEY, PHD, APRN Hypothalamus-Pituitary-Thyroid Hormone Axis TSH: Normal = 0.5-5 mu/l Free T4: 1.3-3.8 ng/dl 1 Hypothyroidism: Thyroid Agents Natural Health
The department of Endocrinology and metabolism Huashan Hospital, Fudan University Dr. Hongying Ye
 The department of Endocrinology and metabolism Huashan Hospital, Fudan University Dr. Hongying Ye dryehongying@hotmail.com Main contents Basic knowledge of thyroid Overview of thyroid diseases Hyperthyroidism/Graves
The department of Endocrinology and metabolism Huashan Hospital, Fudan University Dr. Hongying Ye dryehongying@hotmail.com Main contents Basic knowledge of thyroid Overview of thyroid diseases Hyperthyroidism/Graves