Thyroid disorder for Resident
|
|
|
- Jacob Burns
- 6 years ago
- Views:
Transcription
1 Thyroid disorder for Resident Chaicharn Deerochanawong M.D. Diabetes and Endocrinology Unit Department of Medicine Rajavithi Hospital, Ministry of Public Health
2 Topics Abnormal thyroid function test Euthyroid sick syndrome Difficult cases of thyrotoxicosis Amiodarone induce thyroid disorder Monitor thyroid function after treatment thyroid disorder Subclinical thyroid disorders
3 Usual Interpretation of TFT FT4 ( T4 ) FT3 ( T3 ) TSH ส ง ส ง ต ำ Dx Thyrotoxicosis ต ำ ต ำ หร อ ปกต ต ำ หร อ ปกต หร อส งเล กน อย Secondary hypothyroidism ต ำ ต ำ หร อ ปกต ส ง Primary hypothyroidism
4 Unusual Thyrotoxicosis T3 toxicosis - early or mild thyrotoxicosis - toxic multinodular goiter - iodine deficiency area T4 toxicosis - idodine induce thyrotoxicosis - thyrotoxicosis in severe med illness - thyroiditis
5 Unusual Thyrotoxicosis Thyrotoxicosis with normal or elevated TSH - Lab TSH error - TSH producing tumor - Selective pituitary resistance to thyroid hormone
6 Hyperthyroxinemia with non-suppressed TSH Clinical thyrotoxicosis Rare TSH producing tumor Thyroid hormone resistance Clinical features TSH-omas RTH Familial cases - + CT scan or MRI lesions + +/- High a-subunit + - High a-subunit/tsh ratio + - Elevates TSH after TRH - + T 3 suppression test - +
7 Unusual Thyrotoxicosis Thyrotoxicosis with low iodine uptake - Subacute thyroiditis - Painless thyroiditis - Iodine induced thyrotoxicosis - Factitious thyrotoxicosis - Struma ovarii - Metastatic functioning thyroid CA
8 A 30 years old woman presents with palpitation for 2 weeks. Her thyroid gland diffuse enlarge 30 gm. Her TFT has increase T3 and T4 and TSH 0.10 What is the likely cause of hyperthyroid in this patient? What questions that we should ask more in this patient?
9 Answers Painless thyroiditis History of postpartum, bruit of thyroid gland, consistency of gland Subacute thyroiditis Fever, pain at the thyroid gland
10 Graves vs Painless thyroiditis Graves Painless T. 1. Onset Vary < 2 months 2. Opthalmopathy 10% NO 3. Bruit of thyroid + / Consistency of gl. Vary Firm 5. I 131 uptake High Low 6. Doppler USG ( blood flow ) Increase Decrease 7. TSH R Ab + / - -
11 Euthyroid Hyperthyroxinemia Abnormal thyroid binding protein Acute psychiatric illness Antibody to thyroid hormone Gen thyroid hormone resistance syndrome Sick euthyroid syndrome Drugs
12
13 Euthyroid Hyperthyroxinemia Abnormal thyroid binding protein Acute psychiatric illness Antibody to thyroid hormone Gen thyroid hormone resistance syndrome Sick euthyroid syndrome Drugs
14 TFT changes in acute psyciatric illness 16 % increased thyroid hormone with raised or normal TSH Found in schizophrenia, affective psychosis, and amphetamine abuse Rarely persists beyond 14 days Unknown mechanism Trends in Endocrinol Metab 1997;8:282-7
15 Euthyroid Hyperthyroxinemia Abnormal thyroid binding protein Acute psychiatric illness Antibody to thyroid hormone Gen. thyroid hormone resistance syndrome Sick euthyroid syndrome
16 TBG Circulating binding inhibition TSH ปกต ต ำ ส ง
17 Sick Euthyroid Syndrome T 3 T 4 Reverse T 3 T 2
18 Sick Euthyroid Syndrome Low T3 with Normal T4 Low T4 High T4 TSH may be low, normal or high (<15mIU/L )
19 Change in Thyroid Tests in The course of NTI
20 Euthyroid Hyperthyroxinemia Abnormal thyroid binding protein Acute psychiatric illness Antibody to thyroid hormone Gen thyroid hormone resistance syndrome Sick euthyroid syndrome Drugs
21 Drugs affecting TFT (1) Effect May cause hypothyroidism May cause hyperthyroidism Reduce conversion of T 4 to T 3 Suppress thyroid stimulating hormone Increase clearance of T 4 Drugs Lithium, iodine (all forms, including kelp, contrast media, etc.), interleukin-2, interferon-alpha Iodine, interleukins, interferons Glucocorticods, iodine, propythiouracil, beta-blockers, amiodarone Dopamine, dobutamine, glucocorticoids, phenytoin, bromocriptine, octreotide Carbamazepine, phenytoin, rifampin, phenobarbitol
22 Drugs affecting TFT (2) Effect Reduce binding of T 4 to thyroid-binding globulin Cause increased thyroid-binding globulin Reduce thyroidbinding globulin Influence absorption of thyroxine Drugs Salsalate, salicylates, nonsteroidal antiinflammatory drugs, furosemide, heparin Estrogens, tamoxifen, methadone, heroin, 5-fluorouracil, clofibrate, perphenazine, mitotane Androgens, glucocorticoids, aspariginase Cholestyramine, aluminum hydroxide, ferrous sulfate, sucralfate, cation exchange resins
23 Amiodarone induced thyroid dysfunction Euthyroid : FT4 may be elevated FT3 may be reduced TSH normal Thyrotoxicosis: FT4 elevated, TSH low, FT3 may be high normal Hypothyroid : TSH high FT4 may be low normal
24 Amiodarone induced thyrotoxicosis Feature Type 1 thyrotoxicosis Type 2 thyrotoxicosis Mechanism Excess iodine Destructive, inflammation Thyroid Ab Often present Usually absent IL 6 normal high %Iodine uptake Low but may be normal < 5% Doppler USG Hypervascular Reduced flow Treatment High dose PTU (K perchlorate ) Steroid
25 TFT for Diagnosis and Follow-up Treatment of Thyrotoxicosis Diagnosis FT 4, TSH or FT 3, TSH Critical illness : FT 4, FT 3, TSH Follow-up treatment FT 3, FT 4 in early treatment FT 4, TSH if suspect of overtreatment FT 3 if suspect of relapse

26 DURING TREATMENT OF HYPERTHYROIDISM TSH, FT 4, FT 3 FT 4, FT 3 FT 4, FT 3 Hyperthyroid Transition Euthyroid FT 3 FT 4 Normal range TSH Mo TSH require several months to return to normal after euthyroid
27 ผ ป วยหญ ง อำย 54 ป มำตรวจด วยเร องเหน อยง ำย ตรวจพบม heart rate 122 / นำท AF, thyroid gland diffuse enlarge 40 grams, no bruit ผลกำรตรวจฮอร โมน FT pg/ml ( ) FT ng/dl ( ) TSH miu/l ( )
28 Follow-up treatment Month FT 3 (pg/ml) ( ) FT 4 ( ) TSH ( ) MMI (mg/d)
29 Follow-up treatment Month FT 3 (pg/ml) ( ) FT 4 ( ) TSH ( ) MMI (mg/d)
30 Laboratory Diagnosis of Hypothyroidism Earliest change of TFT in previous Graves disease with ablative treatment decreased FT 4, then increased TSH Earliest change of TFT in previous euthyroid patient increased TSH
 Recommendation of FT 4, TSH if suspected of noncompliance with T 4 treatment Noncompliance : normal FT4 + high TSH or high FT 4 + high")
31 Monitoring Treatment of Hypothyroidism Central hypothyroidism : FT4 Aim : FT 4 in upper third of normal range Primary hypothyroidism : TSH ( + FT4 ) Recommendation of FT 4, TSH if suspected of noncompliance with T 4 treatment Noncompliance : normal FT4 + high TSH or high FT 4 + high TSH
32 Screening TSH for thyroid disease TSH alone : Normal TSH euthyroid status Misleading Low TSH, but not thyrotoxicosis Normal TSH, but not euthyroid High TSH, but not primary hypothyroidism
33 Low TSH but not thyrotoxicosis Prengancy first and early second trimester Euthyroid sick syndrome Euthyroid Graves disease Remission phase of Graves disease On eltroxin suppresive therapy Long standing MNG with autonomous function of gland Drugs Secondary hypothyroidism
34 Conditions with TSH alone might bemisleading Common Recent treatment of thyrotoxicosis Pituitary disease Non-thyroidal illness Drugs Rare TSH-secreting pituitary adenoma Thyroid hormone resistance
35 Option to consider in interpreting thyroid function 1. Repeat laboratory test (consider laboratory error, wrong patient, etc) 2. Clinical correlation/status 3. Patient occupation, past medical history, family history 4. Medications 5. Consider alternate tests 6. Consider common etiologies first 7. Endocrine consult


36 FT3 normal in pregnancy period First trimester to early second trimester TSH ปกต หร อ Third trimester FT 4 ปกต หร อ
37 TRANSIENT HYPERTHYROXINEMIA IN HYPEREMESIS GRAVIDARUM : Hyperemesis gravidarum, early pregnancy : Palpitations, sinus tachycardia, goiter +/- : No clinical evidence of Graves disease : No ophthalmopathy : No family history of thyroid disease : Thyroid antibodies are negative : Common in Asian women : Excessive hcg stimulation results in transiently elevated T 4, FT 4 and low TSH : Supportive treatment Ref. Chong et al Postgrad Med J 1997;73:
38 Subclinical Thyroid Disorders Subclinical hyperthyroidism TSH low and normal FT4, FT3 Subclinical hypothyroidism TSH high and normal FT4,FT3
39 Fact Subclinical thyroid disease: common Associated with complications?? Fair to good evidence only TSH < 0.1 ( osteoporosis, atrial fibrillation ) or >10 ( hypercholesterol, atherosclerosis ) Benefit from treatment: in some selected patients Screening for general population: not recommend Aggressive case findings: Reasonable
40 Treatment Subclinical Hyperthyroidism Persistent TSH < 0.1mIU/L + > 1 risk factor - age > 60 yr - menopausal woman with osteoporosis - tachyarrhythmia eg. AF - patient with heart disease - RAIU high
41 Treatment Subclinical Hyothyroidism Persistent TSH > 10 miu/l + Positive thyroid auto Ab TSH > upper limit in pregnant woman or woman who plan to pregnant
42 The Adrenal Incidentaloma For Internist Chaicharn Deerochanawong M.D. Professor of Medicine, Rangsit Medical University Diabetes and Endocrinology unit, Department of Medine Rajavithi Hospital, Ministry of Public Health

43 Adrenal Incidentaloma Definition Rule out functioning tumor Benigh vs Malignant - Imaging Phenotype - Effect of Size - Role for FNA Biopsy
44 Definition An adrenal mass discovered serendipitously by radiologic examination In the absence of symptoms or clinical findings suggestive of adrenal disease and 1-cm in diameter

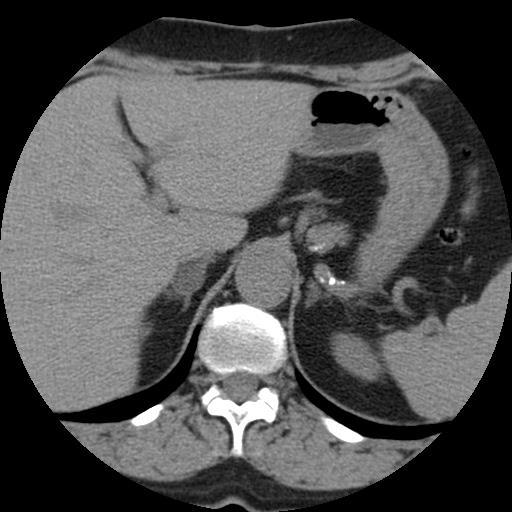
45 IVC Aorta Stomach Liver Spleen Vertebra




46 What to do?

47 Prevalence, % Prevalence by Age -- Autopsy Data 7 6 7%! ' s 30s 40s 50s 60s >70 Age, years Kloos et al., Endo Rev 16:460, 1995

48 Most = Nonfunctioning Cortical Adenomas In a recent review* (9 studies with 1800 patients) the overall mean % of dx were: Malignant = 3% Primary adrenal carcinoma 2% Metastases 1% Benign = 97% Nonfunctioning 90% Subclinical Cushing syndrome 6% Pheochromocytoma 3% Primary aldosteronism 1% *Cawood et al. Eur J of Endo 2009;161:
49 Adrenal Incidentaloma Definition Rule out functioning tumor Benigh vs Malignant - Imaging Phenotype - Effect of Size - Role for FNA Biopsy
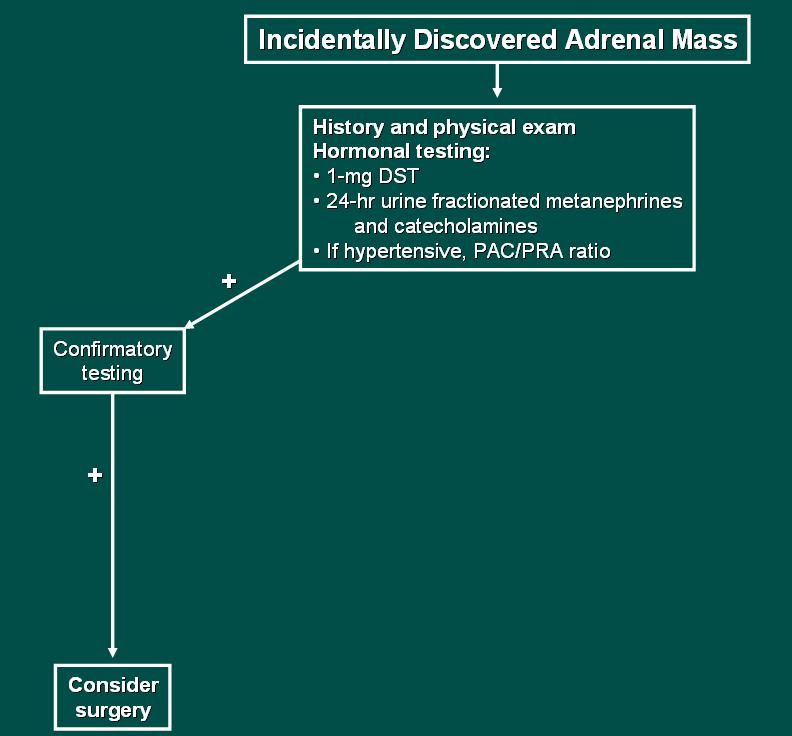
50 Incidentally Discovered Adrenal Mass History and physical exam Hormonal testing: 1-mg DST 24-hr urine fractionated metanephrines and catecholamines If hypertensive, PAC/PRA ratio + Confirmatory testing
51 Adrenal Incidentaloma Definition Rule out functioning tumor Benigh vs Malignant - Imaging Phenotype - Effect of Size - Role for FNA Biopsy




52 Suspicious Imaging Phenotype: large (> 4-cm) irregular margins inhomogeneous dense/vascular precontrast HU >20 <50% contrast Suspicious washout at 10 min Suspicious Suspicious





53 Benign Imaging Phenotype: small (< 3-cm) smooth margins homogeneous hypodense < 10 HU precontrast > 50% contrast Benign washout 10 min Benign Benign
54 Hounsfield Unit (HU) Density +60 HU Less lipid ACCa Met Pheo Lipid-poor adenoma More lipid Benign -20 HU
55 Adrenal Incidentaloma -- Size Factor Accuracy in diagnosis of ACCa N = 1,004 incidentalomas (36 ACCa):* > 4-cm > 5-cm Sensitivity 88% 74% Specificity 75% 91% Positive PV 44% 67% Negative PV 97% 94% *Angeli et al.: Horm Res 47: , 1997.


56 Adrenal Incidentaloma -- Size Factor Adrenal Mass > 4-cm and Young Age

57 CT-Guided FNA Biopsy
58 CT-Guided FNA Biopsy What it CAN tells us: Infection: eg.tb, Fungus Metastatic disease Lyphoma What it CAN T tell us: It cannot distinguish between primary adrenal cortical benign vs malignant hopefully with advances in histopathology, this will be possible in the future
59
60 Incidentally Discovered Adrenal Mass Confirmatory testing + - History and physical exam Hormonal testing: 1-mg DST 24-hr urine fractionated metanephrines and catecholamines If hypertensive, PAC/PRA ratio - Imaging phenotype Suspicious imaging phenotype: nonenhanced CT attenuation >10 HU CT contrast medium washout <50% at 10 min Consider: FNA biopsy if metastatic disease or infection suspected Surgery Close follow-up (e.g. repeat imaging at 3 months)
61 Incidentally Discovered Adrenal Mass History and physical exam Hormonal testing: 1-mg DST 24-hr urine fractionated metanephrines and catecholamines If hypertensive, PAC/PRA ratio - Imaging phenotype Benign imaging phenotype: nonenhanced CT attenuation <10 HU CT contrast medium washout >50% at 10 min Consider: Repeat imaging at 6, 12, and 24 months Repeat hormonal testing annually x 4 years Surgery if 4-cm in diameter
62 Incidentally Discovered Adrenal Mass History and physical exam Hormonal testing: 1-mg DST 24-hr urine fractionated metanephrines and catecholamines If hypertensive, PAC/PRA ratio - Imaging phenotype Benign imaging phenotype: nonenhanced CT attenuation <10 HU CT contrast medium washout >50% at 10 min This is where all of the Consider surgery Growth 1-cm Hormonal autonomy Consider: Repeat imaging at 6, 12, and 24 months Repeat hormonal testing annually x 4 years Surgery if 4-cm in diameter uncertainty and debate lie
Pitfalls of TFTs Interpretation
 Mohammad Reza Bakhtiari DCLS, PhD Pitfalls of TFTs Interpretation CME July 2006 Vol.24 No.7, http://keck.usc.edu HPT axis physiology Log-linear relationship between TSH and FT4 Patient Specific Set Point
Mohammad Reza Bakhtiari DCLS, PhD Pitfalls of TFTs Interpretation CME July 2006 Vol.24 No.7, http://keck.usc.edu HPT axis physiology Log-linear relationship between TSH and FT4 Patient Specific Set Point
Thyroid Disease. I have no disclosures. Overview TSH. Matthew Kim, M.D. July, 2012
 Thyroid Disease I have no disclosures Matthew Kim, M.D. July, 2012 Overview Thyroid Function Tests Hyperthyroidism Hypothyroidism Subclinical Thyroid Disease Thyroid Nodules Questions TSH Best single screening
Thyroid Disease I have no disclosures Matthew Kim, M.D. July, 2012 Overview Thyroid Function Tests Hyperthyroidism Hypothyroidism Subclinical Thyroid Disease Thyroid Nodules Questions TSH Best single screening
Disorders of Thyroid Function
 Disorders of Thyroid Function Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Thyroid Hormone Axis Hypothalamus TRH
Disorders of Thyroid Function Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Thyroid Hormone Axis Hypothalamus TRH
Hyperthyroidism. Objectives. Clinical Manifestations. Slide 1. Slide 2. Slide 3. Implications for Primary Care. hyperthyroidism
 1 Hyperthyroidism Implications for Primary Care Laura A. Ruby, DNP, CRNP Wellspan Endocrinology 2 Objectives! Discuss the clinical manifestations of hyperthyroidism! Review the use of the diagnostic studies!
1 Hyperthyroidism Implications for Primary Care Laura A. Ruby, DNP, CRNP Wellspan Endocrinology 2 Objectives! Discuss the clinical manifestations of hyperthyroidism! Review the use of the diagnostic studies!
ADRENAL INCIDENTALOMA. Jamii St. Julien
 ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
ADRENAL INCIDENTALOMA Jamii St. Julien Outline Definition Differential Evaluation Treatment Follow up Questions Case Definition The phenomenon of detecting an otherwise unsuspected adrenal mass on radiologic
Hyperthyroidism Diagnosis and Treatment. April Janet A. Schlechte, M.D.
 Hyperthyroidism Diagnosis and Treatment Family Practice Refresher Course April 2015 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any
Hyperthyroidism Diagnosis and Treatment Family Practice Refresher Course April 2015 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any
Endocrine MR. Jan 30, 2015 Michael LaFata, MD
 Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Endocrine MR Jan 30, 2015 Michael LaFata, MD Brief case 55-year-old female in ED PMH: HTN, DM2, HLD, GERD CC: Epigastric/LUQ abdominal pain, N/V x2 days AF, HR 103, BP 155/85, room air CMP: Na 133, K 3.6,
Lecture title. Name Family name Country
 Lecture title Name Family name Country Nguyen Thy Khue, MD, PhD Department of Endocrinology HCMC University of Medicine and Pharmacy, MEDIC Clinic Hochiminh City, Viet Nam Provided no information regarding
Lecture title Name Family name Country Nguyen Thy Khue, MD, PhD Department of Endocrinology HCMC University of Medicine and Pharmacy, MEDIC Clinic Hochiminh City, Viet Nam Provided no information regarding
Decoding Your Thyroid Tests and Results
 Decoding Your Thyroid Tests and Results Wondering about your thyroid test results? Learn about each test and what low, optimal, and high results may mean so you can work with your doctor to choose appropriate
Decoding Your Thyroid Tests and Results Wondering about your thyroid test results? Learn about each test and what low, optimal, and high results may mean so you can work with your doctor to choose appropriate
Evaluation of Thyroid Nodules
 Evaluation of Thyroid Nodules Stephan Kowalyk, MD January 25 28, 2018 1 Primary goal Exclude malignancy Incidental thyroid nodules If found on CT, MRI, PET scan, carotid Doppler ULTRASOUND!! January 25
Evaluation of Thyroid Nodules Stephan Kowalyk, MD January 25 28, 2018 1 Primary goal Exclude malignancy Incidental thyroid nodules If found on CT, MRI, PET scan, carotid Doppler ULTRASOUND!! January 25
Understanding thyroid function tests. Dr. Colette George
 Understanding thyroid function tests Dr. Colette George Disclosures No financial disclosure I will present fictitious cases and thyroid function tests (TFTs) that are based on scenarios I commonly encounter.
Understanding thyroid function tests Dr. Colette George Disclosures No financial disclosure I will present fictitious cases and thyroid function tests (TFTs) that are based on scenarios I commonly encounter.
LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS
 LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS Maryam Tohidi Anatomical & clinical pathologist Research Institute for Endocrine Sciences THYROID GLAND (15-25 gr), (12-20 gr), 2 lobes connected by
LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS Maryam Tohidi Anatomical & clinical pathologist Research Institute for Endocrine Sciences THYROID GLAND (15-25 gr), (12-20 gr), 2 lobes connected by
The Work-up and Treatment of Adrenal Nodules
 The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
The Work-up and Treatment of Adrenal Nodules Lawrence Andrew Drew Shirley, MD, MS, FACS Assistant Professor of Surgical-Clinical Department of Surgery Division of Surgical Oncology The Ohio State University
Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017
 Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017 I will not be discussing this Outline of discussion Laboratory tests for thyroid function Diagnosis of hypothyroidism Treatment of
Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017 I will not be discussing this Outline of discussion Laboratory tests for thyroid function Diagnosis of hypothyroidism Treatment of
Approach to thyroid dysfunction
 Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Pearls and Pitfalls of Thyroid Diagnosis. Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS
 Pearls and Pitfalls of Thyroid Diagnosis Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS Thyroid Anatomy Isthmus of gland located 1 fingerbreadth below cricoid cartilage
Pearls and Pitfalls of Thyroid Diagnosis Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS Thyroid Anatomy Isthmus of gland located 1 fingerbreadth below cricoid cartilage
Case Based Urology Learning Program
 Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Case Based Urology Learning Program Resident s Corner: UROLOGY Case Number 4 CBULP 2010 004 Case Based Urology Learning Program Editor: Associate Editors: Manager: Case Contributors: Steven C. Campbell,
Understanding Thyroid Labs
 Understanding Thyroid Labs Chris Sadler, MA, PA-C, CDE, DFAAPA Senior Medical Science Liaison CVM Janssen Scientific Affairs Diabetes and Endocrine Associates La Jolla, CA Disclosures Employee of Janssen
Understanding Thyroid Labs Chris Sadler, MA, PA-C, CDE, DFAAPA Senior Medical Science Liaison CVM Janssen Scientific Affairs Diabetes and Endocrine Associates La Jolla, CA Disclosures Employee of Janssen
university sciences of Isfahan university Com
 Introduce R. Gholamnezhad Lecturer of school of nursing & midwifery of Iran university Ph.D student tof Immunology, Sh School of medical sciences of Isfahan university E-Mail: Gholami278@gmail. Com Interpreting
Introduce R. Gholamnezhad Lecturer of school of nursing & midwifery of Iran university Ph.D student tof Immunology, Sh School of medical sciences of Isfahan university E-Mail: Gholami278@gmail. Com Interpreting
Update In Hyperthyroidism
 Update In Hyperthyroidism CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
Update In Hyperthyroidism CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
Toxic MNG Thyroiditis 5-15
 Hyperthyroidism Facts Prevalence 0.5-1.0%, more common in women Thyrotoxicosis is excess thyroid hormones from endogenous or exogenous sources Hyperthyroidism is excess thyroid hormones from thyroid gland
Hyperthyroidism Facts Prevalence 0.5-1.0%, more common in women Thyrotoxicosis is excess thyroid hormones from endogenous or exogenous sources Hyperthyroidism is excess thyroid hormones from thyroid gland
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 No Disclosures Disease Of the Thyroid Iodide Metabolism/Synthesis of Thyroid Hormone Trap Oxidation Organification(catalyzed
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 No Disclosures Disease Of the Thyroid Iodide Metabolism/Synthesis of Thyroid Hormone Trap Oxidation Organification(catalyzed
Update on Gestational Thyroid Disease. Aidan McElduff The Discipline of Medicine, The University of Sydney
 IADPSG 2016 Update on Gestational Thyroid Disease Aidan McElduff The Discipline of Medicine, The University of Sydney IADPSG 2016 DISCLOSURES and AIM Nil to disclose Aim: to provide an overview 2017 Guidelines
IADPSG 2016 Update on Gestational Thyroid Disease Aidan McElduff The Discipline of Medicine, The University of Sydney IADPSG 2016 DISCLOSURES and AIM Nil to disclose Aim: to provide an overview 2017 Guidelines
An Approach to: Thyroid Function Tests. Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital
 An Approach to: Thyroid Function Tests Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital Regulation of Thyroid axis Hypothalamus TRH T3,T4 ---- TRH Median Eminence (base of brain)
An Approach to: Thyroid Function Tests Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital Regulation of Thyroid axis Hypothalamus TRH T3,T4 ---- TRH Median Eminence (base of brain)
Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME
 Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME 795-7520 traskla@cmhc.org No disclosures Objectives To have an understanding of hyperthyroidism To have an understanding of the management
Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME 795-7520 traskla@cmhc.org No disclosures Objectives To have an understanding of hyperthyroidism To have an understanding of the management
Thyrotoxicosis in Pregnancy: Diagnose and Management
 Thyrotoxicosis in Pregnancy: Diagnose and Management Yuanita Asri Langi email: meralday@yahoo.co.id Endocrinology & Metabolic Division, Internal Medicine Department, Prof.dr.R.D. Kandou Hospital/ Sam Ratulangi
Thyrotoxicosis in Pregnancy: Diagnose and Management Yuanita Asri Langi email: meralday@yahoo.co.id Endocrinology & Metabolic Division, Internal Medicine Department, Prof.dr.R.D. Kandou Hospital/ Sam Ratulangi
Chapter I.A.1: Thyroid Evaluation Laboratory Testing
 Chapter I.A.1: Thyroid Evaluation Laboratory Testing Jennifer L. Poehls, MD and Rebecca S. Sippel, MD, FACS THYROID FUNCTION TESTS Overview Thyroid-stimulating hormone (TSH) is produced by the anterior
Chapter I.A.1: Thyroid Evaluation Laboratory Testing Jennifer L. Poehls, MD and Rebecca S. Sippel, MD, FACS THYROID FUNCTION TESTS Overview Thyroid-stimulating hormone (TSH) is produced by the anterior
None. Thyroid Potpourri for the Primary Care Physician. Evaluating Thyroid Function. Disclosures. Learning Objectives
 Thyroid Potpourri for the Primary Care Physician Ramya Vedula DO, MPH, ECNU Endocrinology, Diabetes and Metabolism Princeton Medical Group Assistant Professor of Clinical Medicine Rutgers Robert Wood Johnson
Thyroid Potpourri for the Primary Care Physician Ramya Vedula DO, MPH, ECNU Endocrinology, Diabetes and Metabolism Princeton Medical Group Assistant Professor of Clinical Medicine Rutgers Robert Wood Johnson
Southern Derbyshire Shared Care Pathology Guidelines. Hyperthyroidism
 Southern Derbyshire Shared Care Pathology Guidelines Hyperthyroidism Purpose of Guideline The management and referral criteria of patients with newly diagnosed hyperthyroidism. Background Hyperthyroidism
Southern Derbyshire Shared Care Pathology Guidelines Hyperthyroidism Purpose of Guideline The management and referral criteria of patients with newly diagnosed hyperthyroidism. Background Hyperthyroidism
Common Thyroid Disorders
 Common Thyroid Disorders Louie Riesch MSN, MPH, RN, ACNS-BC, CDE Texas Diabetes and Endocrinology Anatomy of the Thyroid Gland Hypothalamic-Pituitary-Thyroid Axis Physiology Hypothalamus TRH Pituitary
Common Thyroid Disorders Louie Riesch MSN, MPH, RN, ACNS-BC, CDE Texas Diabetes and Endocrinology Anatomy of the Thyroid Gland Hypothalamic-Pituitary-Thyroid Axis Physiology Hypothalamus TRH Pituitary
B-Resistance to the action of hormones, Hormone resistance characterized by receptor mediated, postreceptor.
 Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
Alvin C. Powers, M.D. 1/27/06
 Thyroid Histology Follicular Cells ECF side Apical lumen Thyroid Follicles -200-400 um Parafollicular or C-cells Colloid Photos from University of Manchester and tutorial created by Dr. James Crimando,
Thyroid Histology Follicular Cells ECF side Apical lumen Thyroid Follicles -200-400 um Parafollicular or C-cells Colloid Photos from University of Manchester and tutorial created by Dr. James Crimando,
Thyroid and Antithyroid Drugs. Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014
 Thyroid and Antithyroid Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed
Thyroid and Antithyroid Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed
The Thyroid and Pregnancy OUTLINE OF DISCUSSION 3/19/10. Francis S. Greenspan March 19, Normal Physiology. 2.
 The Thyroid and Pregnancy Francis S. Greenspan March 19, 2010 OUTLINE OF DISCUSSION 1. Normal Physiology 2. Hypothyroidism 3. Hyperthyroidism 4. Thyroid Nodules and Cancer NORMAL PHYSIOLOGY Iodine Requirements:
The Thyroid and Pregnancy Francis S. Greenspan March 19, 2010 OUTLINE OF DISCUSSION 1. Normal Physiology 2. Hypothyroidism 3. Hyperthyroidism 4. Thyroid Nodules and Cancer NORMAL PHYSIOLOGY Iodine Requirements:
Management of Common Thyroid Disorders
 Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures Cases 68 yr old woman with new atrial fibrillation and no other findings except TSH=0.04,
Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures Cases 68 yr old woman with new atrial fibrillation and no other findings except TSH=0.04,
Management of Common Thyroid Disorders
 Cases Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04,
Cases Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04,
Diseases of thyroid & parathyroid glands (1 of 2)
") Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
Thyroid disorders. Dr Enas Abusalim
 Thyroid disorders Dr Enas Abusalim Thyroid physiology The hypothalamic pituitary thyroid axis And peripheral conversion of T4 to T3, WHERE, AND BY WHAT ENZYME?? Only relatively small concentrations of
Thyroid disorders Dr Enas Abusalim Thyroid physiology The hypothalamic pituitary thyroid axis And peripheral conversion of T4 to T3, WHERE, AND BY WHAT ENZYME?? Only relatively small concentrations of
The Management of adrenal incidentaloma
 The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
The Management of adrenal incidentaloma Dimitrios Linos, MD Director of Surgery, Hygeia Hospital, Athens, Greece Consultant in Surgery, Massachusetts General Hospital, Boston, USA 8 th Postgraduate Course
OUTLINE. Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis
 THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
Mastering Thyroid Disorders. Douglas C. Bauer, MD UCSF Division of General Internal Medicine
 Mastering Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine Cases 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04, normal free T4 79
Mastering Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine Cases 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04, normal free T4 79
Laboratory assessment of thyroid function. Nahid Shirazian MD. Internist, Endocrinologist
 Laboratory assessment of thyroid function Nahid Shirazian MD. Internist, Endocrinologist Physiology Thyroid gland produces Thyroxine Converted to active form T3 in tissue Scattered dc cells within ihi
Laboratory assessment of thyroid function Nahid Shirazian MD. Internist, Endocrinologist Physiology Thyroid gland produces Thyroxine Converted to active form T3 in tissue Scattered dc cells within ihi
Thyroid Function TSH Analyte Information
 Thyroid Function TSH Analyte Information 1 2013-05-01 Thyroid-stimulating hormone (TSH) Introduction Thyroid-stimulating hormone (thyrotropin, TSH) is a glycoprotein with molecular weight of approximately
Thyroid Function TSH Analyte Information 1 2013-05-01 Thyroid-stimulating hormone (TSH) Introduction Thyroid-stimulating hormone (thyrotropin, TSH) is a glycoprotein with molecular weight of approximately
Clinical evaluation of. Thyroid function tests
 In the name of God Dr.m.omidi Endocrinologist Assistant stant professor of medicine 25 APR 2012 Clinical evaluation of Thyroid function tests Goal of TFT Evaluation of function of thyroid Monitoring
In the name of God Dr.m.omidi Endocrinologist Assistant stant professor of medicine 25 APR 2012 Clinical evaluation of Thyroid function tests Goal of TFT Evaluation of function of thyroid Monitoring
Thyroid Disease in Pregnancy: The Essentials. Elizabeth N. Pearce, MD, MSc
 Thyroid Disease in Pregnancy: The Essentials Elizabeth N. Pearce, MD, MSc None Disclosures Case 1 A 31-year-old woman from Massachusetts is practicing a vegan diet. She is currently planning a pregnancy.
Thyroid Disease in Pregnancy: The Essentials Elizabeth N. Pearce, MD, MSc None Disclosures Case 1 A 31-year-old woman from Massachusetts is practicing a vegan diet. She is currently planning a pregnancy.
Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone
 Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Disease of the Adrenals 1 Zona Glomerulosa Mineralocorticoids: aldosterone Angiotensin II/renin regulation by sympathetic tone; High potassium will stimulate and ACTH Increase in aldosterone leads to salt
Endocrine. Endocrine as it relates to the kidney. Sarah Elfering, MD University of Minnesota
 Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
Endocrine Sarah Elfering, MD University of Minnesota Endocrine as it relates to the kidney Parathyroid gland Vitamin D Endocrine causes of HTN Adrenal adenoma PTH Bone Kidney Intestine 1, 25 OH Vitamin
The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital
 The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital Presentation Today: Common thyroid problems and treatments Pregnancy related thyroid problems The suppressed
The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital Presentation Today: Common thyroid problems and treatments Pregnancy related thyroid problems The suppressed
DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT ENDOCRINE SYSTEM AT A GLANCE OBJECTIVES ANATOMY OF THE THYROID
 OBJECTIVES DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT Stephanie Blackburn, MHS, MLS(ASCP) CM LSU Health Shreveport Clinical Laboratory Science Program Discuss the synthesis and action
OBJECTIVES DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT Stephanie Blackburn, MHS, MLS(ASCP) CM LSU Health Shreveport Clinical Laboratory Science Program Discuss the synthesis and action
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases
 Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Take Home Messages in Endocrinology
 Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
Conflict of Interest/Disclosures Take Home Messages in Endocrinology None Carolyn Becker, MD 2 Diabetes Thyroid Pituitary Adrenal Hypoglycemia Overview Diagnostic Criteria for T2DM Diabetes should be diagnosed
Dharma Lindarto Div. Endokrin-Metabolisme dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM Medan
 HYPERTHYROIDISM Dharma Lindarto Div. Endokrin-Metabolisme dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM Medan Anatomy of the Thyroid Gland Tiroid Disease Multi N Aspect fungtion morphology eutiroid,
HYPERTHYROIDISM Dharma Lindarto Div. Endokrin-Metabolisme dan Diabetes. Dep Ilmu Penyakit Dalam FK USU / RSUP HAM Medan Anatomy of the Thyroid Gland Tiroid Disease Multi N Aspect fungtion morphology eutiroid,
Amiodarone Induced Thyrotoxicosis Treatment? (AIT)
") Amiodarone Induced Thyrotoxicosis Treatment? (AIT) Presentation of a Case Report Annelies Tonnelier Brigitte Velkeniers 14-12-2013 1 1. Background 1. Case report 2. Investigations 3. Diagnosis 4. Treatment
Amiodarone Induced Thyrotoxicosis Treatment? (AIT) Presentation of a Case Report Annelies Tonnelier Brigitte Velkeniers 14-12-2013 1 1. Background 1. Case report 2. Investigations 3. Diagnosis 4. Treatment
Endocrine part two. Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy
 Endocrine part two Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy Cushing's disease: increased secretion of adrenocorticotropic
Endocrine part two Presented by Dr. Mohammad Saadeh The requirements for the Clinical Chemistry Philadelphia University Faculty of pharmacy Cushing's disease: increased secretion of adrenocorticotropic
Disclosures. Learning objectives. Case 1A. Autoimmune Thyroid Disease: Medical and Surgical Issues. I have nothing to disclose.
 Disclosures Autoimmune Thyroid Disease: Medical and Surgical Issues I have nothing to disclose. Chrysoula Dosiou, MD, MS Clinical Assistant Professor Division of Endocrinology Stanford University School
Disclosures Autoimmune Thyroid Disease: Medical and Surgical Issues I have nothing to disclose. Chrysoula Dosiou, MD, MS Clinical Assistant Professor Division of Endocrinology Stanford University School
Approach to Adrenal Incidentaloma. Alice Y.Y. Cheng, MD, FRCP
 Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Approach to Adrenal Incidentaloma Alice Y.Y. Cheng, MD, FRCP Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form
Underactive Thyroid. Diagnosis, Treatment & Controversies
 Underactive Thyroid Diagnosis, Treatment & Controversies Dr. Asif Malik Humayun Consultant Endocrinologist Milton Keynes University Hospital NHS Foundation Trust Thyroid Hormone Control of metabolism
Underactive Thyroid Diagnosis, Treatment & Controversies Dr. Asif Malik Humayun Consultant Endocrinologist Milton Keynes University Hospital NHS Foundation Trust Thyroid Hormone Control of metabolism
Endocrine Surgery When to Refer and What We Do
 Endocrine Surgery When to Refer and What We Do None Disclosures W. Heath Giles, M.D., F.A.C.S. Surgery Residency Program Director Assistant Professor of Surgery What is Endocrine Surgery? Who performs
Endocrine Surgery When to Refer and What We Do None Disclosures W. Heath Giles, M.D., F.A.C.S. Surgery Residency Program Director Assistant Professor of Surgery What is Endocrine Surgery? Who performs
Effect of thyroid hormones of metabolism Thyroid Diseases
 Effect of thyroid hormones of metabolism Thyroid Diseases Medical Perspective Aspects That Will Be Addressed Regulation of thyroid hormone secretion Basic physiology Hyperthyroidism Hypothyroidism Thyroiditis
Effect of thyroid hormones of metabolism Thyroid Diseases Medical Perspective Aspects That Will Be Addressed Regulation of thyroid hormone secretion Basic physiology Hyperthyroidism Hypothyroidism Thyroiditis
Common Thyroid Disorders
 8/29/16 Anatomy of the Thyroid Gland Common Thyroid Disorders Heather Cuevas PhD, RN, ACNS- BC Texas Diabetes and Endocrinology The University of Texas at Austin School of Nursing Hypothalamic- Pituitary-
8/29/16 Anatomy of the Thyroid Gland Common Thyroid Disorders Heather Cuevas PhD, RN, ACNS- BC Texas Diabetes and Endocrinology The University of Texas at Austin School of Nursing Hypothalamic- Pituitary-
Pregnancy & Thyroid. Zohreh Moosavi Associate professor of Endocriology Imam Reza General Hospital Mashad University. Imam Reza weeky Conferance
 Pregnancy & Thyroid Zohreh Moosavi Associate professor of Endocriology Imam Reza General Hospital Mashad University Imam Reza weeky Conferance Objectives Thyroid Disorders & Pregnancy Normal thyroid phsyiology
Pregnancy & Thyroid Zohreh Moosavi Associate professor of Endocriology Imam Reza General Hospital Mashad University Imam Reza weeky Conferance Objectives Thyroid Disorders & Pregnancy Normal thyroid phsyiology
Thyroid Nodules. Objectives. Clinical Practice Guidelines for the Management of Thyroid Disorders
 9:45 1:45am Clinical Practice Guidelines for the Management of Thyroid Disorders SPEAKER Gregory Brent, MD Presenter Disclosure Information The following relationships exist related to this presentation:
9:45 1:45am Clinical Practice Guidelines for the Management of Thyroid Disorders SPEAKER Gregory Brent, MD Presenter Disclosure Information The following relationships exist related to this presentation:
GOITER and Shortness of Breath. Case A: GOITER. Learning Objectives. Common Thyroid Disorders for
 2:25 3:05pm Diagnosing and Treating Thyroid Disorders SPEAKER John Tayek, MD Presenter Disclosure Information The following relationships exist related to this presentation: John Tayek, MD, serves on the
2:25 3:05pm Diagnosing and Treating Thyroid Disorders SPEAKER John Tayek, MD Presenter Disclosure Information The following relationships exist related to this presentation: John Tayek, MD, serves on the
AUGUST 25-27, 2017 UPDATE & BOARD REVIEW. acofp INTENSIVE. Evolving Issues in Endocrinology. Chris Pitsch, DO INNOVATIVE COMPREHENSIVE HANDS-ON
 acofp INTENSIVE UPDATE & BOARD REVIEW AUGUST 25-27, 2017 Loews Chicago O'Hare Hotel Rosemont, IL INNOVATIVE COMPREHENSIVE HANDS-ON Evolving Issues in Endocrinology Chris Pitsch, DO acofp Am eric an College
acofp INTENSIVE UPDATE & BOARD REVIEW AUGUST 25-27, 2017 Loews Chicago O'Hare Hotel Rosemont, IL INNOVATIVE COMPREHENSIVE HANDS-ON Evolving Issues in Endocrinology Chris Pitsch, DO acofp Am eric an College
Endocrine Topic Review. Sethanant Sethakarun, MD
 Endocrine Topic Review Sethanant Sethakarun, MD Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
Endocrine Topic Review Sethanant Sethakarun, MD Definition Cushing's syndrome comprises a large group of signs and symptoms that reflect prolonged and in appropriately high exposure of tissue to glucocorticoids
Page 1. Understanding Common Thyroid Disorders. Cases. Topics Covered
 Cases Understanding Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 66 yr old female with 1 yr of fatigue and lassitude and no findings except TSH=8.2,
Cases Understanding Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 66 yr old female with 1 yr of fatigue and lassitude and no findings except TSH=8.2,
Invecchiamento e Tiroide
 Simposio La patologia Tiroidea nell Anziano Invecchiamento e Tiroide Fabio Monzani Sezione Geriatria, Dipartimento di Medicina Clinica & Sperimentale, Università di Pisa THE EFFECT OF AGING ON THYROID
Simposio La patologia Tiroidea nell Anziano Invecchiamento e Tiroide Fabio Monzani Sezione Geriatria, Dipartimento di Medicina Clinica & Sperimentale, Università di Pisa THE EFFECT OF AGING ON THYROID
Index. radiologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
Endocrine system pathology
 Endocrine system pathology Central endocrine system peripheral endocrine system: thyroid gland parathyroid gland pancreas adrenal glands Thyroid gland. the weight of normal thyroid gland is about 15 grams.
Endocrine system pathology Central endocrine system peripheral endocrine system: thyroid gland parathyroid gland pancreas adrenal glands Thyroid gland. the weight of normal thyroid gland is about 15 grams.
molecular brothers David Pfisterer Lucerne, Switzerland ESIM 2011
 molecular brothers David Pfisterer Lucerne, Switzerland ESIM 2011 Case Vignette A 25-year old man was admitted to our hospital because of fever, productive cough, nausea and weight loss. The patient had
molecular brothers David Pfisterer Lucerne, Switzerland ESIM 2011 Case Vignette A 25-year old man was admitted to our hospital because of fever, productive cough, nausea and weight loss. The patient had
Pathology. Hyperthyroidism (Overactive Thyroid), Graves Disease (Basedow Disease) and more. Definitions. See online here
, Graves Disease (Basedow Disease) and more. Definitions. See online here") Pathology Hyperthyroidism (Overactive Thyroid), Graves Disease (Basedow Disease) and more See online here Hyperthyroidism is caused by the excess of thyroid hormones T3 and T4. Graves disease is the most
Pathology Hyperthyroidism (Overactive Thyroid), Graves Disease (Basedow Disease) and more See online here Hyperthyroidism is caused by the excess of thyroid hormones T3 and T4. Graves disease is the most
Hypothyroidism. Definition:
 Definition: Hypothyroidism Primary hypothyroidism is characterized biochemically by a high serum thyroidstimulating hormone (TSH) concentration and a low serum free thyroxine (T4) concentration. Subclinical
Definition: Hypothyroidism Primary hypothyroidism is characterized biochemically by a high serum thyroidstimulating hormone (TSH) concentration and a low serum free thyroxine (T4) concentration. Subclinical
Canadian Endocrine Review Course 2014
 Canadian Endocrine Review Course 2014 Amiodarone & Thyrotoxicosis Iodine, A Catch 22 Ally P.H. Prebtani Associate Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University
Canadian Endocrine Review Course 2014 Amiodarone & Thyrotoxicosis Iodine, A Catch 22 Ally P.H. Prebtani Associate Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University
Euthyroid sick syndrome
 Euthyroid sick syndrome Background Euthyroid sick syndrome can be described as abnormal findings on thyroid function tests that occur in the setting of a nonthyroidal illness (NTI) without preexisting
Euthyroid sick syndrome Background Euthyroid sick syndrome can be described as abnormal findings on thyroid function tests that occur in the setting of a nonthyroidal illness (NTI) without preexisting
Table 1: Thyroid panel. Result (reference interval) TSH 89.5 miu/l ( ) Total T4 5.2 µg/dl ( ) T3 uptake 39% (22-35)
 TSH 89.5 miu/l ( ) Total T4 5.2 µg/dl ( ) T3 uptake 39% (22-35)") Introduction Thyroid disease is the second most common endocrine disorder (behind diabetes), and its prevalence increases with increasing age. The incidence of newly diagnosed thyroid cancer is increasing
Introduction Thyroid disease is the second most common endocrine disorder (behind diabetes), and its prevalence increases with increasing age. The incidence of newly diagnosed thyroid cancer is increasing
Adrenal incidentaloma guideline for Northern Endocrine Network
 Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Adrenal incidentaloma guideline for Northern Endocrine Network Definition of adrenal incidentaloma Adrenal mass detected on an imaging study done for indications that are not related to an adrenal problem
Challenging TFTs (Definition)
") Thyroid Function Tests (Interpretation Challenges) Mohammad Reza Bakhtiari, DCLS, PhD 1/80 Challenging TFTs (Definition) Discordant Results vs. Clinical Picture Inharmonious Results 2/80 1 Challenging
Thyroid Function Tests (Interpretation Challenges) Mohammad Reza Bakhtiari, DCLS, PhD 1/80 Challenging TFTs (Definition) Discordant Results vs. Clinical Picture Inharmonious Results 2/80 1 Challenging
Virginia ACP Clinical Update Thyroid Clinical Pearls. University of Virginia. Richard J. Santen MD
 Virginia ACP Clinical Update Thyroid Clinical Pearls University of Virginia Richard J. Santen MD Goal Provide a guide to frequently encountered problems in thyroid disease Follow my approach to recently
Virginia ACP Clinical Update Thyroid Clinical Pearls University of Virginia Richard J. Santen MD Goal Provide a guide to frequently encountered problems in thyroid disease Follow my approach to recently
Thyroid and Antithyroid Drugs. Dr. Alia Shatanawi Feb,
 Thyroid and Antithyroid Drugs Dr. Alia Shatanawi Feb, 24 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed of epithelial cells which
Thyroid and Antithyroid Drugs Dr. Alia Shatanawi Feb, 24 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed of epithelial cells which
Adrenal Incidentaloma Management
 Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
Adrenal Incidentaloma Management Full Title of Guideline: Author Management of Incidentally-discovered Adrenal Lesions ( Incidentalomas ) Mr David Chadwick Consultant Endocrine Surgeon david.chadwick2@nuh.nhs.uk
Adrenal gland Incidentaloma
 Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
Adrenal gland Incidentaloma Topic review 17 sep 2008 Anatomy 1 Anatomical consideration Blood supply Artery: small branches from Inf. phrenic, renal artery and aorta Vein: Rt : medial aspect to IVC Lt
The Thyroid: No mystery. Just need all the pieces to the puzzle.
 The Thyroid: No mystery. Just need all the pieces to the puzzle. Todd Chennell, MS, RN ANP-C Endocrine surgery University of Rochester 2018 1 According to the American Thyroid Association, 12 percent of
The Thyroid: No mystery. Just need all the pieces to the puzzle. Todd Chennell, MS, RN ANP-C Endocrine surgery University of Rochester 2018 1 According to the American Thyroid Association, 12 percent of
ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE
 ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE DR ANJU SAHDEV READER AND CONSULTANT RADIOLOGIST QUEEN MARY UNIVERSITY AND ST BARTHOLOMEW S HOSPITAL BARTS HEALTH, LONDON, UK DISCLOSURE OF CONFLICT
ADRENAL MEDULLARY DISORDERS: PHAEOCHROMOCYTOMAS AND MORE DR ANJU SAHDEV READER AND CONSULTANT RADIOLOGIST QUEEN MARY UNIVERSITY AND ST BARTHOLOMEW S HOSPITAL BARTS HEALTH, LONDON, UK DISCLOSURE OF CONFLICT
Disorders of the Thyroid Gland
 Disorders of the Thyroid Gland István Takács MD., PhD, 1st Department of Medicine, Semmelweis University Connection to the dentistry: close to each other higher operation risk radiating pain macroglossia
Disorders of the Thyroid Gland István Takács MD., PhD, 1st Department of Medicine, Semmelweis University Connection to the dentistry: close to each other higher operation risk radiating pain macroglossia
Nuclear medicine in endocrinology
 Nuclear medicine in endocrinology Thyroid gland: anatomy, function, inflammation, Nuclear medicine in endocrinology tumor dignitiy Parathyroid gland: localisation Adrenal cortex: function Adrenal medulla:
Nuclear medicine in endocrinology Thyroid gland: anatomy, function, inflammation, Nuclear medicine in endocrinology tumor dignitiy Parathyroid gland: localisation Adrenal cortex: function Adrenal medulla:
Requesting and Management of abnormal TFTs.
 Requesting and Management of abnormal TFTs. At the request of a number of GPs I have produced summary guidelines surrounding thyroid testing. These have been agreed with our Endocrinology leads Dr Bell
Requesting and Management of abnormal TFTs. At the request of a number of GPs I have produced summary guidelines surrounding thyroid testing. These have been agreed with our Endocrinology leads Dr Bell
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Common Causes of Hypothyroidism
 Common Causes of Hypothyroidism Autoimmune thyroidi4s Surgical removal of thyroid gland Medica4on Therapy Iodine and iodine containing medica4ons Neck radia4on Post Partum thyroidi4s Prevalence of Hypothyroidism
Common Causes of Hypothyroidism Autoimmune thyroidi4s Surgical removal of thyroid gland Medica4on Therapy Iodine and iodine containing medica4ons Neck radia4on Post Partum thyroidi4s Prevalence of Hypothyroidism
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging. Deepa R Biyyam, MD Attending Pediatric Radiologist
 Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
TANJA KEMP INTERNAL MEDICINE: ENDOCRINOLOGY
 ENDOCRINE DISORDERS IN THE ELDERLY (part 2) TANJA KEMP INTERNAL MEDICINE: ENDOCRINOLOGY Pituitary axis Target organs of the pituitary gland Negative feedback Hypothalamus-Pituitary-Thyroid axis Thyroid
ENDOCRINE DISORDERS IN THE ELDERLY (part 2) TANJA KEMP INTERNAL MEDICINE: ENDOCRINOLOGY Pituitary axis Target organs of the pituitary gland Negative feedback Hypothalamus-Pituitary-Thyroid axis Thyroid
Approach to Thyroid Dysfunction in the Elderly
 Approach to Thyroid Dysfunction in the Elderly Fernando Melaragno Endocrinology Objective The objective of this lecture is to review the epidemiology, clinical presentation, risks and complications, and
Approach to Thyroid Dysfunction in the Elderly Fernando Melaragno Endocrinology Objective The objective of this lecture is to review the epidemiology, clinical presentation, risks and complications, and
The interpretation and management of thyroid disorders
 Journal of Endocrinology, Metabolism and Diabetes of South Africa 2015 ; 20(2) http://dx.doi.org/10.1080/16089677.2015.1056468 Open Access article distributed under the terms of the Creative Commons License
Journal of Endocrinology, Metabolism and Diabetes of South Africa 2015 ; 20(2) http://dx.doi.org/10.1080/16089677.2015.1056468 Open Access article distributed under the terms of the Creative Commons License
1 day PTA: vaginal spotting, LE edema LMP 6 weeks ago. OSH Clinic: distended abdomen, (+) urine pregnancy; sent home with iron
 urine pregnancy; sent home with iron") Anila Bindal, MD 1 day PTA: vaginal spotting, LE edema LMP 6 weeks ago OSH Clinic: distended abdomen, (+) urine pregnancy; sent home with iron UCMC ER: abdomen doubled overnight, significant vaginal bleeding,
Anila Bindal, MD 1 day PTA: vaginal spotting, LE edema LMP 6 weeks ago OSH Clinic: distended abdomen, (+) urine pregnancy; sent home with iron UCMC ER: abdomen doubled overnight, significant vaginal bleeding,
Grave s disease (1 0 )
") THYROID DYSFUNCTION Grave s disease (1 0 ) Autoimmune - activating AB s to TSH receptor High concentrations of circulating thyroid hormones Weight loss, tachycardia, tiredness Diffuse goitre - TSH stimulating
THYROID DYSFUNCTION Grave s disease (1 0 ) Autoimmune - activating AB s to TSH receptor High concentrations of circulating thyroid hormones Weight loss, tachycardia, tiredness Diffuse goitre - TSH stimulating
NIH Public Access Author Manuscript Ther Drug Monit. Author manuscript; available in PMC 2013 April 14.
 NIH Public Access Author Manuscript Published in final edited form as: Ther Drug Monit. 2006 February ; 28(1): 8 11. Thyroid Function Testing in Pregnancy and Thyroid Disease: Trimester-specific Reference
NIH Public Access Author Manuscript Published in final edited form as: Ther Drug Monit. 2006 February ; 28(1): 8 11. Thyroid Function Testing in Pregnancy and Thyroid Disease: Trimester-specific Reference
THE WORK-UP OF ADRENAL INCIDENTALOMA
 THE WORK-UP OF ADRENAL INCIDENTALOMA Maria Cristina De Martino Dipartimento di Medicina Clinica e Chirurgia, Sezione di Endocrinologia Università Federico II di Napoli Definition and epidemiology Most
THE WORK-UP OF ADRENAL INCIDENTALOMA Maria Cristina De Martino Dipartimento di Medicina Clinica e Chirurgia, Sezione di Endocrinologia Università Federico II di Napoli Definition and epidemiology Most
BELIEVE MIDWIFERY SERVICES
 TITLE: THYROID DISEASE IN PREGNANCY EFFECTIVE DATE: July, 2013 POLICY STATEMENT: Pregnancy changes significantly the values influenced by the serum thyroid binding hormone level (i.e., total thyroxine,
TITLE: THYROID DISEASE IN PREGNANCY EFFECTIVE DATE: July, 2013 POLICY STATEMENT: Pregnancy changes significantly the values influenced by the serum thyroid binding hormone level (i.e., total thyroxine,
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA
 AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
AVS and IPSS: The Basics and the Pearls William F. Young, Jr., MD, MSc Professor of Medicine Mayo Clinic College of Medicine Rochester, MN, USA 2016 Mayo Foundation for Medical Education and Research.
The Effect of Medications on Thyroid Function Tests
 The Effect of Medications on Thyroid Function Tests Priya Kundra, MD a,b, *, Kenneth D. Burman, MD a,b KEYWORDS Thyroid function Medication Hormone Euthyroid state Abnormal results of thyroid function
The Effect of Medications on Thyroid Function Tests Priya Kundra, MD a,b, *, Kenneth D. Burman, MD a,b KEYWORDS Thyroid function Medication Hormone Euthyroid state Abnormal results of thyroid function
William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA
 The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education
The Year in Adrenal William F. Young, Jr., MD, MSc Professor of Medicine, Mayo Clinic, Rochester, MN USA Division of ENDOCRINOLOGY, DIABETES, METABOLISM & NUTRITION 2018 Mayo Foundation for Medical Education