Uncommon Presentations of Thyroid Dysfunction. Douglas S Ross MD May 16, 2018 Copyrighted slides omitted
|
|
|
- Millicent Randall
- 6 years ago
- Views:
Transcription
1 Uncommon Presentations of Thyroid Dysfunction Douglas S Ross MD May 16, 2018 Copyrighted slides omitted
2 Case 1 53 year old woman Sees her PCP with complaints of fatigue She is sleeping poorly due to hot flashes She has no weight loss or palpitations AP 78, thyroid exam normal Free T4 2.9 (normal ), T3 342 (normal ), TSH <0.01
3 Uncommon cause of abnormal thyroid tests Biotin



4 Prescribed by Hairdressers
5 Biotin No RDA Adequate Intake (AI) 30 mcg Hair Skin and Nails 2,500 mcg tid Biotin 10,000 mcg
6 Prescribed by Neurologists Multiple Sclerosis Ataxia due to Multiple Carboxylase Deficiencies (MCD) Doses are up to 100 mg tid
7 Copyrighted slides withdrawn Figure: biotin effect of direct assays Figure: Standard curve sandwich assay Figure: biotin effect on competitive assays Figure: Standard curve competitive assay Figure: Biotin effect on TBII assay Figure: Time course of biotin effect
8 Case 1 follow up Off Biotin for 2 days Free T4 1.5 (normal ), T3 120 (normal ), TSH 1.4
9 Case 2 60 year old woman on levothyroxine TSH 30, PCP increased the dose 6 weeks later TSH 28.6, dose increased again 6 weeks later free T4 3.2 (normal ), T3 207 (normal ), TSH 29 Referred to endocrinologist
10 Case 2 continued She was taking no other medications or supplements except a multivitamin She was complaining of palpitations and insomnia Repeat blood tests: TSH <0.01, free T4 3.2 ( ), T3 212 (60 181)
11 Copyrighted slide withdrawn Figure: Effect of heterophilic antibodies on sandwich assays
12 Diagnosis of HAMA Human Anti Mouse Antibody Non linearity with dilution suggests interference Add nonimmune homologous mouse immunoglobulins Add Sepharose beads coated with Protein A or G to eliminate all IgG Reagents and detection kits commercially available
13 Rheumatoid Factors Directed against Fc fragment of human IgG Cross reactivity to mouse IgG may occur
14 Case 2 follow up Levothyroxine dose adjusted She is having her thyroid blood tests done through a national reference lab instead of the local hospital
15 Case 3 18 year old stressed out over exams, sleeping poorly, anxious Grandmother on thyroxine, prior radioiodine treatment Sister is being evaluated for a thyroid problem Free T4 2.7 (normal ), TSH 0.9
16 Differential Diagnosis Inappropriate TSH TSH producing pituitary adenoma Thyroid Hormone Resistance Binding Protein Abnormalities
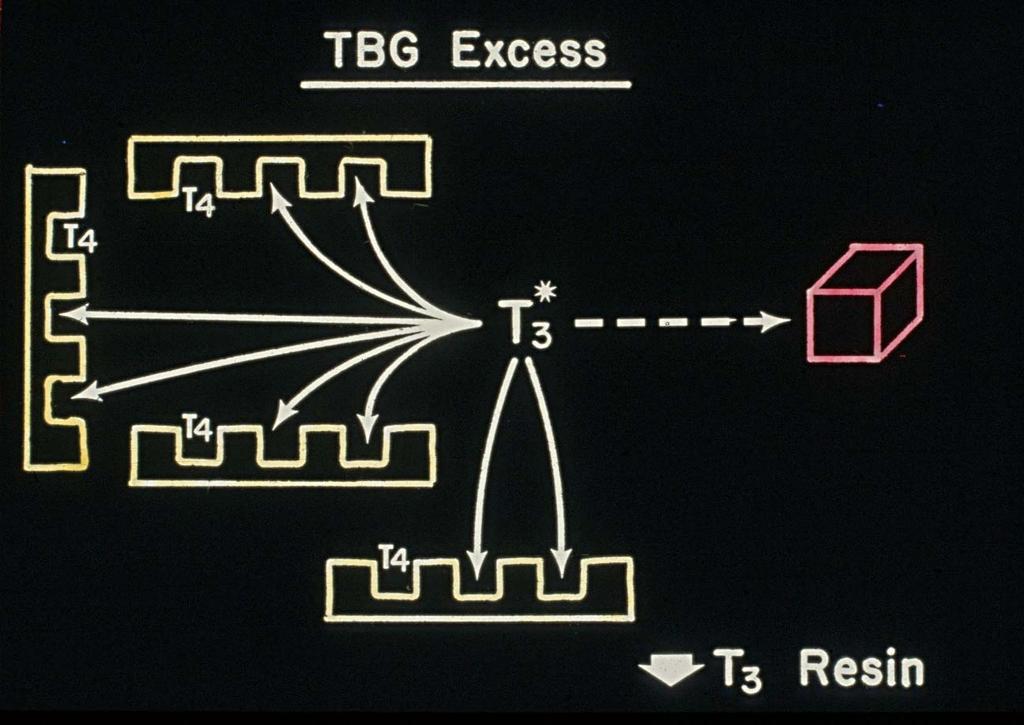
17 Binding Protein Abnormalities (TBG excess) (free T4 should be normal) Familial dysalbuminemic hyperthyroxinemia Abnormal transthyretin Autoantibodies to T4 (or T3)
18 TBG excess Hereditary (x linked) Estrogens, raloxifen, tamoxifen, pregnancy Mild hepatitis 5 FU Perphenazine Clofibrate Heroin and methadone Acute intermittent porphyria
19 Case 3 continued T3 142 ng/ml (normal ) Excludes TBG excess Excludes TSH adenoma and thyroid hormone resistance
20 Differential Diagnosis Familial dysalbuminemic hyperthyroxinemia Abnormal transthyretin Autoantibodies to T4 These should all effect total T4 assays, but shouldn t free T4 assays measure only free T4?
21 Free T4 index direct free T4 assays Free T4 estimates

22

23
24
25 Free T4 index Hyperthyroidism: high T4 x high T3R = high free T4 index TBG excess high T4 x low T3R = normal free T4 index

26
27 Copyrighted slide withdrawn Figure: free T4 assays in patients with FDH
28 Evaluation of T4 binding abnormalities T4 binding panel measures the concentrations of TBG, transthyretin, and albumin and the percent binding of T4 to each protein T4 autoantibodies can be measured by adding labeled T4 and precipitating immunoglobulins with PEG
29 Case 3 follow up The patient s T4 binding panel showed excess binding to albumin consistent with familial dysalbuminemic hyperthyroxinemia More common in Hispanics His grandmother was never hyperthyroid and received RAI unnecessarily
30 Case 4 38 year old woman complains of fatigue TSH 7.4, free T4 4.2 ( ), T3 108 (60 181)
31 Differential Diagnosis? Mild hypothyroidism and Familial dysalbuminemic hyperthyroxinemia Abnormal transthyretin Autoantibodies to T4 With normal T3 a TSH producing pituitary tumor and thyroid hormone resistance are excluded
32 Case 4 continued Free T4 by equilibrium dialysis was normal Free T4 in a two step assay was normal Reduced T4 recovery with PEG precipitation of the patient s serum Anti T4 autoantibodies confirmed by immune assay
33 Copyrighted slides withdrawn Figure: two step free T4 assays Figure: one step labeled antibody free T4 assays
34 Case 4 follow up Patients with anti T4 autoantibodies usually have Hashimoto s thyroiditis TPO antibodies positive 486 The patient was treated with levothyroxine
35 Cases with assay interference Case 1 Biotin Case 2 HAMA Case 3 FDH Case 4 Anti T4 antibodies
36 Case 5 36 year old woman with relapsing remitting multiple sclerosis Treated with alemtuzumab 12 mg daily x 5 days One year later she was given alemtuzumab 12 mg daily x 3 days 18 months after her first dose of alemtuzumab: TSH <0.01, free T4 3.8 ( ), T3 432 (60 181)
37 Alemtuzumab and Immune Reconstitution Syndrome Anti CD52 antibody Depletes lymphocytes binds cells and initiates complement mediated lysis of lymphocytes Followed by reconstitution of immune function Clonal expansion of lymphocytes favors antibody over cellmediated autoimmunity ITP is among the major complications of treatment
38 Alemtuzumab and Thyroid dysfunction 22 % of patients have Graves, of which 23 % spontaneously remit and 15 % become hypothyroid 7 % of patients have hypothyroidism, of which 74 % have TBII 4 % of patients had subacute destructive thyroiditis 34% of patients have thyroid dysfunction Daniels et al JCEM 2014
39 Graves disease and alemtuzumab Treatment Considerations Overall remission rate 78% Methimazole may be more appropriate than definitive therapy with RAI
40 Copyrighted slide withdrawn Figure: Onset of thyroid dysfunction after alemtuzumab
41 Multiple episodes of immune reconstitution syndrome and thyroid dysfunction 30 percent of patients had more than one episode Most common was overt Graves disease initially, then overt hypothyroidism subsequently Some patients had painless thyroiditis followed by Graves disease or overt hypothyroidism Daniels et al JCEM 2014
42 Case 5 follow up She went into remission after 6 months of methimazole Currently euthyroid, but schedule to have her third treatment with alemtuzumab soon
43 Case 6 62 year old man with metastatic melanoma Treated with ipilimumab and nivolumab Free T4 2.2, T3 160, TSH <0.01
44 Immune Checkpoint inhibitors Cytotoxic T lymphocyte associated protein 4 (CTLA 4) Programmed cell death protein 1 inhibitor (PD 1) Programmed cell death ligand inhibitor (PD L1)
45 Copyrighted slides withdrawn Figure: mechanism of check point inhibition Figure: immune related adverse effects of checkpoint inhibitors endocrine
46 Endocrine Dysfunction after Checkpoint Inhibitors Meta analysis of 38 studies and 7551 patients Hypothyroid Hyperthyroid Hypophysitis CTLA 4 Ipilimumab 3.8 % 1.7 % 3.2 % PD 1 Nivolumab PD 1 Pembrolizumab Ipilimumab and Nivolumab PD L1 Atezolizumab <0.1 Barroso Sousa et al JAMA Oncol 2017
47 Copyrighted slides withdrawn Table: destructive thyroiditis with nivolumab Figure: Graves disease from CTLA 4 inhibition
48 Current indications for checkpoint inhibition CTLA 4 Melanoma CTLA 4 + PD 1 Melanoma PD 1 PD L1 Melanoma Bladder Cancer Squamous NSCLC RCC CRC HCC Hodgkin s
49 Thyroid Cancer and Immune Checkpoint Inhibition High PD LI expression in more aggressive cancers PD LI expressed in anaplastic cancer PD LI expressed in BRAF mutated cancers Ongoing clinical trials in thyroid cancer and anaplastic thyroid cancer Nivolumab + ipilumumab Pembrolizumab + levantinib Cunha et al 2013, Ahn et al 2017, Angell et al 2014
50 Case 6 follow up One month later TSH 89, free T4 <0.4 ( ) Patient started on levothyroxine
51 Case 7 49 year old woman with nonresectable hepatocellular carcinoma Treated with sorafenib 400 mg bid 17 weeks into treatment: free T4 2.7 ( ) and TSH <0.01 After 4 months: free T4 0.1 and TSH 86 Anti TPO negative Levothyroxine started
52 Thyroid dysfunction with Tyrosine Kinase Inhibitors (TKIs) Overt hypothyroidism 32 to 85% of patients Transient hyperthyroidism (destructive thyroiditis) 0 to 24% Increased levothyroxine requirements in patients with prior hypothyroidism Onset averages 4 weeks, but reported up to 94 weeks after initial exposure Torino et al Thyroid 2013
53 Mechanism of thyroid dysfunction with TKIs Unlikely due to lymphocytic thyroiditis. Anti TPO antibodies usually negative. Hypothesis: Inhibition of angiogenic pathways: VEGF (vascular endothelial growth factor) PDGFR (platelet derived growth factor receptor) Results in reduced blood flow, ischemic thyroiditis, destruction and atrophy
54 Copyrighted slide withdrawn Figure: CT showing reduction in thyroid size with sorafenib
55 Evidence to support the angiotoxic hypothesis for TKI associated hypothyroidism TKIs that were potent inhibitors of VEGF and PDGFR (e.g. sunitinib) were more likely to cause destructive thyroiditis and hypothyroidism Thyroid vascularity measured by doppler is reduced during sunitinib treatment and increases when sunitinib is discontinued Torino et al Thyroid 2013; Makita et al Thyroid 2010
56 Other potential mechanisms of TKI associated hypothyroidism Impaired iodine uptake (related to reduced blood flow) Increased non deiodination metabolism of thyroxine Increased type 3 (DIO3) deiodination Hershman & Liwanpo Thyroid 2010; de Groot et al Clin Pharmacol Ther 2005; Schlumberger et al J Clin Oncol 2009
57 Case 7 follow up Patient remains euthyroid on levothyroxine
58 Cases of thyroid dysfunction from drug therapies Case 5 Alemtuzumab for relapsingremitting multiple sclerosis Case 6 Immune check point inhibitors Case 7 Tyrosine kinase inhibitors
59 Case 8 27 year old woman, 14 weeks pregnant Chiropractor diagnosed hypothyroidism 2 years ago On Naturethroid 2 grains TSH 0.07, free T4 0.5 (normal )
60 Free T4 in pregnancy non pregnant 1 st 2 nd 3 rd Total T Free T4 index Free T4 A Free T4 B Lee et al Am J Obstet Gynecol 2009
61 Why did the chiropractor prescribe thyroid extract?
62 Copyrighted slide withdrawn Figure: blood levels of T4 and T3 on levothyroxine
63 Normal T4:T3 ratio Approximate average daily requirements (taking into account absorption): T mcg T mcg Normal T4:T3 ratio (in humans) is 14:1
64 Thyroid Extract 1 grain = 38 mcg T4 and 9 mcg T3 T4:T3 ratio 4.2:1 T4:T3 ratio in rats 4:1 T4:T3 ratio in humans 14:1
65 Extract versus L T4 Extract does NOT mimic normal physiology extract L T4 normal mg mcg Free T T TSH Hoang et al JCEM 2013
66 T3 containing thyroid medications Cytomel (liothyronine) Thyroid extract Armour Westhroid Naturethroid W P thyroid Thyrolar (liotrix)
67 Thyroid Extract Probable Harm to Fetus Fetal type 2 deiodinase converts maternal T4 to T3, the primary source of thyroid hormone through week 16 of gestation Maternal T3 does not appear to correlate with fetal T3 levels Thus maternal hypothyroxinemia seen in mothers taking extract may have adverse effects on fetal development
68 Maternal Thyroid Function during Early Pregnancy and Cognitive Functioning in Early Childhood: The Generation R Study Odds Ratio for non verbal cognitive delay Free T4 <10 percentile 1.37 ( ) Free T4 < 5 percentile 2.03 ( ) * Henrichs et al JCEM 2010
69 Low maternal free T4 and IQ in offspring 3727 mother child pairs Thyroid tests before 18 weeks gestation; Non verbal IQ at 6 years Free T4 in lowest 5% ile with normal TSH IQ was 4.3 points lower (CI 6.7 to 1.8, P<0.001) Ghassabian et al JCEM 2014
70 Case 8 follow up Patient refused to take levothyroxine alone Patient is unable to function at work on T4 alone (brain fog) Agreed to levothyroxine and liothyronine at 14:1 ratio She had a non eventful pregnancy
71 Case 9 62 year old woman with a thyroid nodule

72 Toxic adenoma 10 years after radioiodine
73 Radiology report Heterogeneous hypoechoic nodule with macroand microcalcifications, and possible extrathyroidal extension highly suspicious for malignancy.
74 Case 9 14 years earlier Free T4 2.8 ( ), T3 336 (60 181), TSH <0.01 Palpable right nodule Scan 30% uptake, toxic adenoma
75
76 Which Treatment? Surgery Radioiodine Hypothyroid: 20% Hypothyroid: 8% 1 yr, 60% at 20 yrs Re treatment: 1% (Rapid) control of hyperthyroidism: 99% Nerve palsy 1% Hypoparathyroidism 2% Re treatment: 20% Control of hyperthyroidism, 6 mos: 80% Graves disease: 4% PERSISTENT NODULE
77 Treatment of toxic adenoma RAI 75% of patients were no longer hyperthyroid at 3 months, with nodule volume decreased by 35% at 3 months, 45% at 2 years. Risk of an ugly nodule on ultrasound 10 years later Ceccarelli et al Clin Endocrinol. 62:
78 Use of Ultrasound by ATA members in the year 1999 Only 34 % would obtain an ultrasound to evaluate a patient with a solitary nodule. Bennedbaek & Hegedos JCEM 2000
79 Case 9 follow up FNA was read as FLUS due to the presence of microfollicles The patient, at the insistence of her PCP underwent surgery The pathology was a benign adenoma with mixed macro and microfolicular architecture The patient expressed satisfaction with her outcome. She did not want a scar on her neck in her 40s, but this concerns her less in her 60s.
80 Case year old woman Graves diagnosed during her first pregnancy T4 13, T3 292, TSH <0.01 She was managed without ATD Post partum free T4 2.2, T3 320 and methimazole started Rash on methimazole after 4 weeks Off methimazole free T4 1.8, T3 187, TSH <0.01 She is unwilling to take PTU, radioiodine, or have surgery
81 Iodine as Primary Therapy for Graves Disease 44 Japanese patients 66 % controlled for 9 28 years (mean 18 yrs) 39 % achieved a remission after mean 7 years 10% no benefit 25% only transient benefit Okamura et al JCEM 2014
82 Iodine as Primary Therapy 2016 ATA Hyperthyroid Guidelines Potassium iodide may be of benefit in select patients with hyperthyroidism due to GD, who have had adverse reactions to ATD, and have a contraindication or aversion to RAI (or additional RAI) or surgery. Treatment may be more suitable for patients with mild hyperthyroidism, or a prior history of RAI. Insufficient evidence to determine net benefits or risks.
83 Case 10 Patient was started on SSKI one drop daily One month later: free T4 1.2, T3 160, TSH 0.02 Two months later: free T4 0.8, T3 90, TSH 7.23 Dose reduced to one drop every other day One month later: free T4 1.1, T3 148, TSH 2.1 She wants to get pregnant again
84 Use of Iodine during pregnancy 2017 ATA Pregnancy Guidelines Excessive doses of iodine exposure during pregnancy should be avoided, except in preparation for the surgical treatment of GD. Clinicians should carefully weigh the risks and benefits when ordering medications or diagnostic tests that will result in high iodine exposure. Strong recommendation, moderate quality evidence. Excessive = >500 mcg / day 1 drop SSKI = 50 mg
85 2016 ATA Hyperthyroid Guidelines Women with Graves hyperthyroidism who are planning a pregnancy could consider: 1) Changing to PTU prior to conception 2) Changing to PTU when hcg positive 3) Stopping ATD when hcg positive 4) Definitive therapy before conceiving Weak recommendation; low quality evidence. Stopping iodine when hcg positive? Continuing iodine during first trimester?
86 Iodine treatment during pregnancy 283 Japanese woman who stopped methimazole and shifted to iodine first trimester Hyperthyroidism was not as well controlled, but Fewer birth defects 1.53 versus 4.14 % More live births 92 versus 85% Yoshihara et al 2015 Thyroid
87 Iodine treatment during pregnancy 35 Japanese patients taking 6 to 40 mg of iodine daily Only one infant was born with subclinical hypothyroidism Momotani et al 1992 JCEM
88 Case 10 follow up Uneventful pregnancy Iodine was discontinued when she got pregnant Peak T3 343, T4 14, TSH <0.01, TSI 2.56 end of first trimester Then slowly normalized tests: TSH 1.26 by third trimester Post partum T3 228, T4 13 TSH<0.01 T3/T4 ratio suggests post partum thyroiditis
89 Case year old woman with a 70 g nodular goiter She has noted increased dysphagia, and her gland bothers her when she lies on the couch while watching television TSH 0.06, free T4 1.0 ( ), T3 110 (60 181) Ultrasound Multiple spongiform appearing nodules, as large as 3.6 cm Scan 15% uptake, with areas of both increased and reduced isotope concentration

90

91
92 Case 11 continued Surgery discussed with the patient who refuses to consider surgery. Is her RAIU too low to effectively treat her with radioiodine?
93 Low iodine diet rhtsh methimazole Strategies to increase RAIU in patients with nodular goiter
94 rhtsh and radioiodine treatment of nodular goiter 0.3 mg rhtsh versus placebo OFF LABEL RAIU 35 % versus 26 % Goiter size reduced 62 % versus 41 % Hypothyroidism in 62 % versus 11 % Nielsen et al Arch Int Med 2006
95 Methimazole pretreatment to increase RAIU Preliminary Study of 5 women Methimazole 10 to 15 mg given for 2 to 4 months Mean TSH increased from 0.32 to 2.6 RAIU increase from 26 to 49 % Thyroid Volume reduced 46% at 12 months after 30 mci 100 % became hypothyroid Flores Rebollar J Clin Med Res 2013
96 Case 11 follow up Patient received methimazole 20 mg for 3.5 months TSH increased to 7.8 RAIU increased to 48% Patient received 24 mci radioidine Her goiter has regressed by about 40% She is taking levothyroxine for hypothyroidism
97 Questions or Comments Biotin HAMA FDH Anti T4 antibodies Alemtuzumab Immune checkpoint inhibitors Tyrosine kinase inhibitors Thyroid extract in pregnancy Toxic adenoma s/p radioiodine Iodine as primary therapy for Graves Toxic MNG with low RAIU
The Thyroid and Pregnancy OUTLINE OF DISCUSSION 3/19/10. Francis S. Greenspan March 19, Normal Physiology. 2.
 The Thyroid and Pregnancy Francis S. Greenspan March 19, 2010 OUTLINE OF DISCUSSION 1. Normal Physiology 2. Hypothyroidism 3. Hyperthyroidism 4. Thyroid Nodules and Cancer NORMAL PHYSIOLOGY Iodine Requirements:
The Thyroid and Pregnancy Francis S. Greenspan March 19, 2010 OUTLINE OF DISCUSSION 1. Normal Physiology 2. Hypothyroidism 3. Hyperthyroidism 4. Thyroid Nodules and Cancer NORMAL PHYSIOLOGY Iodine Requirements:
Thyrotoxicosis in Pregnancy: Diagnose and Management
 Thyrotoxicosis in Pregnancy: Diagnose and Management Yuanita Asri Langi email: meralday@yahoo.co.id Endocrinology & Metabolic Division, Internal Medicine Department, Prof.dr.R.D. Kandou Hospital/ Sam Ratulangi
Thyrotoxicosis in Pregnancy: Diagnose and Management Yuanita Asri Langi email: meralday@yahoo.co.id Endocrinology & Metabolic Division, Internal Medicine Department, Prof.dr.R.D. Kandou Hospital/ Sam Ratulangi
Hyperthyroidism Diagnosis and Treatment. April Janet A. Schlechte, M.D.
 Hyperthyroidism Diagnosis and Treatment Family Practice Refresher Course April 2015 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any
Hyperthyroidism Diagnosis and Treatment Family Practice Refresher Course April 2015 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any
Lecture title. Name Family name Country
 Lecture title Name Family name Country Nguyen Thy Khue, MD, PhD Department of Endocrinology HCMC University of Medicine and Pharmacy, MEDIC Clinic Hochiminh City, Viet Nam Provided no information regarding
Lecture title Name Family name Country Nguyen Thy Khue, MD, PhD Department of Endocrinology HCMC University of Medicine and Pharmacy, MEDIC Clinic Hochiminh City, Viet Nam Provided no information regarding
Hyperthyroidism: Guidelines and Beyond. Douglas S Ross MD May Copyrighted slides omitted
 Hyperthyroidism: Guidelines and Beyond Douglas S Ross MD May 19 2018 Copyrighted slides omitted Abbott Laboratories Quest Diagnostics Disclosures Diagnosis Biochemical Assessment Biotin Interference Biotinylated
Hyperthyroidism: Guidelines and Beyond Douglas S Ross MD May 19 2018 Copyrighted slides omitted Abbott Laboratories Quest Diagnostics Disclosures Diagnosis Biochemical Assessment Biotin Interference Biotinylated
LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS
 LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS Maryam Tohidi Anatomical & clinical pathologist Research Institute for Endocrine Sciences THYROID GLAND (15-25 gr), (12-20 gr), 2 lobes connected by
LABORATORY TESTS FOR EVALUATION OF THYROID DISORDERS Maryam Tohidi Anatomical & clinical pathologist Research Institute for Endocrine Sciences THYROID GLAND (15-25 gr), (12-20 gr), 2 lobes connected by
Hypothyroidism in pregnancy. Nor Shaffinaz Yusoff Azmi Jabatan Perubatan Hospital Sultanah Bahiyah Kedah
 Hypothyroidism in pregnancy Nor Shaffinaz Yusoff Azmi Jabatan Perubatan Hospital Sultanah Bahiyah Kedah Agenda 1. Epidemiology and clinical characteristics of maternal hypothyroidism 2. Prevention and
Hypothyroidism in pregnancy Nor Shaffinaz Yusoff Azmi Jabatan Perubatan Hospital Sultanah Bahiyah Kedah Agenda 1. Epidemiology and clinical characteristics of maternal hypothyroidism 2. Prevention and
Disorders of Thyroid Function
 Disorders of Thyroid Function Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Thyroid Hormone Axis Hypothalamus TRH
Disorders of Thyroid Function Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Thyroid Hormone Axis Hypothalamus TRH
Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017
 Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017 I will not be discussing this Outline of discussion Laboratory tests for thyroid function Diagnosis of hypothyroidism Treatment of
Sanjay B. Dixit, M.D. BHS Endocrinology Associates November 11, 2017 I will not be discussing this Outline of discussion Laboratory tests for thyroid function Diagnosis of hypothyroidism Treatment of
Thyroid Disease. I have no disclosures. Overview TSH. Matthew Kim, M.D. July, 2012
 Thyroid Disease I have no disclosures Matthew Kim, M.D. July, 2012 Overview Thyroid Function Tests Hyperthyroidism Hypothyroidism Subclinical Thyroid Disease Thyroid Nodules Questions TSH Best single screening
Thyroid Disease I have no disclosures Matthew Kim, M.D. July, 2012 Overview Thyroid Function Tests Hyperthyroidism Hypothyroidism Subclinical Thyroid Disease Thyroid Nodules Questions TSH Best single screening
Disclosures. Learning objectives. Case 1A. Autoimmune Thyroid Disease: Medical and Surgical Issues. I have nothing to disclose.
 Disclosures Autoimmune Thyroid Disease: Medical and Surgical Issues I have nothing to disclose. Chrysoula Dosiou, MD, MS Clinical Assistant Professor Division of Endocrinology Stanford University School
Disclosures Autoimmune Thyroid Disease: Medical and Surgical Issues I have nothing to disclose. Chrysoula Dosiou, MD, MS Clinical Assistant Professor Division of Endocrinology Stanford University School
Virginia ACP Clinical Update Thyroid Clinical Pearls. University of Virginia. Richard J. Santen MD
 Virginia ACP Clinical Update Thyroid Clinical Pearls University of Virginia Richard J. Santen MD Goal Provide a guide to frequently encountered problems in thyroid disease Follow my approach to recently
Virginia ACP Clinical Update Thyroid Clinical Pearls University of Virginia Richard J. Santen MD Goal Provide a guide to frequently encountered problems in thyroid disease Follow my approach to recently
Approach to thyroid dysfunction
 Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Understanding Thyroid Labs
 Understanding Thyroid Labs Chris Sadler, MA, PA-C, CDE, DFAAPA Senior Medical Science Liaison CVM Janssen Scientific Affairs Diabetes and Endocrine Associates La Jolla, CA Disclosures Employee of Janssen
Understanding Thyroid Labs Chris Sadler, MA, PA-C, CDE, DFAAPA Senior Medical Science Liaison CVM Janssen Scientific Affairs Diabetes and Endocrine Associates La Jolla, CA Disclosures Employee of Janssen
Hyperthyroidism. Objectives. Clinical Manifestations. Slide 1. Slide 2. Slide 3. Implications for Primary Care. hyperthyroidism
 1 Hyperthyroidism Implications for Primary Care Laura A. Ruby, DNP, CRNP Wellspan Endocrinology 2 Objectives! Discuss the clinical manifestations of hyperthyroidism! Review the use of the diagnostic studies!
1 Hyperthyroidism Implications for Primary Care Laura A. Ruby, DNP, CRNP Wellspan Endocrinology 2 Objectives! Discuss the clinical manifestations of hyperthyroidism! Review the use of the diagnostic studies!
None. Thyroid Potpourri for the Primary Care Physician. Evaluating Thyroid Function. Disclosures. Learning Objectives
 Thyroid Potpourri for the Primary Care Physician Ramya Vedula DO, MPH, ECNU Endocrinology, Diabetes and Metabolism Princeton Medical Group Assistant Professor of Clinical Medicine Rutgers Robert Wood Johnson
Thyroid Potpourri for the Primary Care Physician Ramya Vedula DO, MPH, ECNU Endocrinology, Diabetes and Metabolism Princeton Medical Group Assistant Professor of Clinical Medicine Rutgers Robert Wood Johnson
Common Issues in Management of Hypothyroidism
 Common Issues in Management of Hypothyroidism Family Medicine Refresher Course April 5, 2018 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Common Issues in Management of Hypothyroidism Family Medicine Refresher Course April 5, 2018 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Update In Hyperthyroidism
 Update In Hyperthyroidism CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
Update In Hyperthyroidism CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
Thyroid Disease in Pregnancy: The Essentials. Elizabeth N. Pearce, MD, MSc
 Thyroid Disease in Pregnancy: The Essentials Elizabeth N. Pearce, MD, MSc None Disclosures Case 1 A 31-year-old woman from Massachusetts is practicing a vegan diet. She is currently planning a pregnancy.
Thyroid Disease in Pregnancy: The Essentials Elizabeth N. Pearce, MD, MSc None Disclosures Case 1 A 31-year-old woman from Massachusetts is practicing a vegan diet. She is currently planning a pregnancy.
B-Resistance to the action of hormones, Hormone resistance characterized by receptor mediated, postreceptor.
 Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
Disorders of the endocrine system 38 Disorders of endocrine system mainly are caused by: A-Deficiency or an excess of a single hormone or several hormones: - deficiency :can be congenital or acquired.
DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT ENDOCRINE SYSTEM AT A GLANCE OBJECTIVES ANATOMY OF THE THYROID
 OBJECTIVES DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT Stephanie Blackburn, MHS, MLS(ASCP) CM LSU Health Shreveport Clinical Laboratory Science Program Discuss the synthesis and action
OBJECTIVES DISORDERS OF THE THYROID GLAND SIGNS, SYMPTOMS, & TREATMENT Stephanie Blackburn, MHS, MLS(ASCP) CM LSU Health Shreveport Clinical Laboratory Science Program Discuss the synthesis and action
BELIEVE MIDWIFERY SERVICES
 TITLE: THYROID DISEASE IN PREGNANCY EFFECTIVE DATE: July, 2013 POLICY STATEMENT: Pregnancy changes significantly the values influenced by the serum thyroid binding hormone level (i.e., total thyroxine,
TITLE: THYROID DISEASE IN PREGNANCY EFFECTIVE DATE: July, 2013 POLICY STATEMENT: Pregnancy changes significantly the values influenced by the serum thyroid binding hormone level (i.e., total thyroxine,
Pregnancy & Thyroid. Zohreh Moosavi Associate professor of Endocriology Imam Reza General Hospital Mashad University. Imam Reza weeky Conferance
 Pregnancy & Thyroid Zohreh Moosavi Associate professor of Endocriology Imam Reza General Hospital Mashad University Imam Reza weeky Conferance Objectives Thyroid Disorders & Pregnancy Normal thyroid phsyiology
Pregnancy & Thyroid Zohreh Moosavi Associate professor of Endocriology Imam Reza General Hospital Mashad University Imam Reza weeky Conferance Objectives Thyroid Disorders & Pregnancy Normal thyroid phsyiology
Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME
 Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME 795-7520 traskla@cmhc.org No disclosures Objectives To have an understanding of hyperthyroidism To have an understanding of the management
Laura Trask, MD FACP Central Maine Endocrinology Lewiston, ME 795-7520 traskla@cmhc.org No disclosures Objectives To have an understanding of hyperthyroidism To have an understanding of the management
Common Causes of Hypothyroidism
 Common Causes of Hypothyroidism Autoimmune thyroidi4s Surgical removal of thyroid gland Medica4on Therapy Iodine and iodine containing medica4ons Neck radia4on Post Partum thyroidi4s Prevalence of Hypothyroidism
Common Causes of Hypothyroidism Autoimmune thyroidi4s Surgical removal of thyroid gland Medica4on Therapy Iodine and iodine containing medica4ons Neck radia4on Post Partum thyroidi4s Prevalence of Hypothyroidism
Thyroid Management. Evolving Controversy - Science, Dogma, Opinion. The Ogden Surgical Medical Society May 2016
 Thyroid Management Evolving Controversy - Science, Dogma, Opinion The Ogden Surgical Medical Society May 2016 Published Guidelines AACE and ATA - Clinical Practice Guidelines in 2012 Guidelines are neither
Thyroid Management Evolving Controversy - Science, Dogma, Opinion The Ogden Surgical Medical Society May 2016 Published Guidelines AACE and ATA - Clinical Practice Guidelines in 2012 Guidelines are neither
ENDOCRINE ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT IMMUNOTHERAPY
 ENDOCRINE ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT IMMUNOTHERAPY Lauren Clarine DO, Renil Rodriguez Martinez MD, Matthew Levine MD, Amy Chang MD, and Megan McGarvey MD May 6, 2017 Immune checkpoint inhibitors
ENDOCRINE ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT IMMUNOTHERAPY Lauren Clarine DO, Renil Rodriguez Martinez MD, Matthew Levine MD, Amy Chang MD, and Megan McGarvey MD May 6, 2017 Immune checkpoint inhibitors
Pitfalls of TFTs Interpretation
 Mohammad Reza Bakhtiari DCLS, PhD Pitfalls of TFTs Interpretation CME July 2006 Vol.24 No.7, http://keck.usc.edu HPT axis physiology Log-linear relationship between TSH and FT4 Patient Specific Set Point
Mohammad Reza Bakhtiari DCLS, PhD Pitfalls of TFTs Interpretation CME July 2006 Vol.24 No.7, http://keck.usc.edu HPT axis physiology Log-linear relationship between TSH and FT4 Patient Specific Set Point
Chapter I.A.1: Thyroid Evaluation Laboratory Testing
 Chapter I.A.1: Thyroid Evaluation Laboratory Testing Jennifer L. Poehls, MD and Rebecca S. Sippel, MD, FACS THYROID FUNCTION TESTS Overview Thyroid-stimulating hormone (TSH) is produced by the anterior
Chapter I.A.1: Thyroid Evaluation Laboratory Testing Jennifer L. Poehls, MD and Rebecca S. Sippel, MD, FACS THYROID FUNCTION TESTS Overview Thyroid-stimulating hormone (TSH) is produced by the anterior
The Presence of Thyroid Autoantibodies in Pregnancy
 The Presence of Thyroid Autoantibodies in Pregnancy Dr. O Sullivan does not have any financial relationships with any commercial interests. KATIE O SULLIVAN, MD FELLOW, ADULT/PEDIATRIC ENDOCRINOLOGY ENDORAMA
The Presence of Thyroid Autoantibodies in Pregnancy Dr. O Sullivan does not have any financial relationships with any commercial interests. KATIE O SULLIVAN, MD FELLOW, ADULT/PEDIATRIC ENDOCRINOLOGY ENDORAMA
OUTLINE. Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis
 THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
THYROID DISEASE OUTLINE Regulation of Thyroid Hormone Production Common Tests to Evaluate the Thyroid Hyperthyroidism - Graves disease, toxic nodules, thyroiditis OUTLINE Hypothyroidism - Hashimoto s thyroiditis,
THYROID DISEASE IN PREGNANCY
 THYROID DISEASE IN PREGNANCY https://www.wddty.com/magazine/2016/june/depression-its-not-your-brain-its-your-thyroid.html Grand Rounds December 5, 2018 Maria Kolojeski, DO (PGY3) REVIEW OF THYROID HORMONES
THYROID DISEASE IN PREGNANCY https://www.wddty.com/magazine/2016/june/depression-its-not-your-brain-its-your-thyroid.html Grand Rounds December 5, 2018 Maria Kolojeski, DO (PGY3) REVIEW OF THYROID HORMONES
Index. Graves disease, 111 thyroid autoantigens, 110 Autoimmune thyroiditis, 11, 58, 180, 181. B Bamforth Lazarus syndrome, 27
 Index A Adrenergic activation, 77 Allan Herndon Dudley syndrome, 31 Ambulatory practice choice of test, 156, 157 screening general population, thyroid dysfunction, 163, 164 targeted population, 164 167
Index A Adrenergic activation, 77 Allan Herndon Dudley syndrome, 31 Ambulatory practice choice of test, 156, 157 screening general population, thyroid dysfunction, 163, 164 targeted population, 164 167
Management of Common Thyroid Disorders
 Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures Cases 68 yr old woman with new atrial fibrillation and no other findings except TSH=0.04,
Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures Cases 68 yr old woman with new atrial fibrillation and no other findings except TSH=0.04,
An Approach to: Thyroid Function Tests. Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital
 An Approach to: Thyroid Function Tests Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital Regulation of Thyroid axis Hypothalamus TRH T3,T4 ---- TRH Median Eminence (base of brain)
An Approach to: Thyroid Function Tests Rinkoo Dalan Consultant Department of Endocrinology Tan Tock Seng Hospital Regulation of Thyroid axis Hypothalamus TRH T3,T4 ---- TRH Median Eminence (base of brain)
NEWBORN FEMALE WITH GOITER PAYAL PATEL, M.D. PEDIATRIC ENDOCRINOLOGY FELLOW FEBRUARY 12, 2015
 NEWBORN FEMALE WITH GOITER PAYAL PATEL, M.D. PEDIATRIC ENDOCRINOLOGY FELLOW FEBRUARY 12, 2015 CHIEF COMPLAINT 35 6/7 week F with goiter, born to a mother with Graves disease (GD) HPI 35 6/7 week F born
NEWBORN FEMALE WITH GOITER PAYAL PATEL, M.D. PEDIATRIC ENDOCRINOLOGY FELLOW FEBRUARY 12, 2015 CHIEF COMPLAINT 35 6/7 week F with goiter, born to a mother with Graves disease (GD) HPI 35 6/7 week F born
John Sutton, DO, FACOI, FACE, CCD. Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989
 John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 No Disclosures Disease Of the Thyroid Iodide Metabolism/Synthesis of Thyroid Hormone Trap Oxidation Organification(catalyzed
John Sutton, DO, FACOI, FACE, CCD Carson Tahoe Endocrinology Carson City, NV KCOM Class of 1989 No Disclosures Disease Of the Thyroid Iodide Metabolism/Synthesis of Thyroid Hormone Trap Oxidation Organification(catalyzed
Thyroid. Dr Jessica Triay November 2018
 Thyroid Dr Jessica Triay November 2018 Hypothyroidism in Pregnancy Clinical update: Hypothyroidism in Pregnancy Take home messages Additional evidence supportive for more relaxed TSH targets for those
Thyroid Dr Jessica Triay November 2018 Hypothyroidism in Pregnancy Clinical update: Hypothyroidism in Pregnancy Take home messages Additional evidence supportive for more relaxed TSH targets for those
Toxic MNG Thyroiditis 5-15
 Hyperthyroidism Facts Prevalence 0.5-1.0%, more common in women Thyrotoxicosis is excess thyroid hormones from endogenous or exogenous sources Hyperthyroidism is excess thyroid hormones from thyroid gland
Hyperthyroidism Facts Prevalence 0.5-1.0%, more common in women Thyrotoxicosis is excess thyroid hormones from endogenous or exogenous sources Hyperthyroidism is excess thyroid hormones from thyroid gland
Diseases of thyroid & parathyroid glands (1 of 2)
") Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
Hypothyroidism. Definition:
 Definition: Hypothyroidism Primary hypothyroidism is characterized biochemically by a high serum thyroidstimulating hormone (TSH) concentration and a low serum free thyroxine (T4) concentration. Subclinical
Definition: Hypothyroidism Primary hypothyroidism is characterized biochemically by a high serum thyroidstimulating hormone (TSH) concentration and a low serum free thyroxine (T4) concentration. Subclinical
Timothy Bilash MD MS OBG Northern Inyo Hospital, Bishop, CA October 20, :30 PM
 Thyroxine Deficiency in Pregnancy Timothy Bilash MD MS OBG Northern Inyo Hospital, Bishop, CA October 20, 2006 1:30 PM WHI Estrogen recap In http://courses.washington.edu/bonephys/opestrogen.html. from:
Thyroxine Deficiency in Pregnancy Timothy Bilash MD MS OBG Northern Inyo Hospital, Bishop, CA October 20, 2006 1:30 PM WHI Estrogen recap In http://courses.washington.edu/bonephys/opestrogen.html. from:
Page 1. Understanding Common Thyroid Disorders. Cases. Topics Covered
 Cases Understanding Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 66 yr old female with 1 yr of fatigue and lassitude and no findings except TSH=8.2,
Cases Understanding Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 66 yr old female with 1 yr of fatigue and lassitude and no findings except TSH=8.2,
Management of Thyroid Nodules. February 2 nd, 2018 Sarah Hopkins
 Management of Thyroid Nodules February 2 nd, 2018 Sarah Hopkins No disclosures Goals: Review Initial Evaluation of Thyroid Nodules Review Indications for Biopsy Approach to Multinodular Goiter Review Management
Management of Thyroid Nodules February 2 nd, 2018 Sarah Hopkins No disclosures Goals: Review Initial Evaluation of Thyroid Nodules Review Indications for Biopsy Approach to Multinodular Goiter Review Management
Update on Gestational Thyroid Disease. Aidan McElduff The Discipline of Medicine, The University of Sydney
 IADPSG 2016 Update on Gestational Thyroid Disease Aidan McElduff The Discipline of Medicine, The University of Sydney IADPSG 2016 DISCLOSURES and AIM Nil to disclose Aim: to provide an overview 2017 Guidelines
IADPSG 2016 Update on Gestational Thyroid Disease Aidan McElduff The Discipline of Medicine, The University of Sydney IADPSG 2016 DISCLOSURES and AIM Nil to disclose Aim: to provide an overview 2017 Guidelines
Pearls and Pitfalls of Thyroid Diagnosis. Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS
 Pearls and Pitfalls of Thyroid Diagnosis Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS Thyroid Anatomy Isthmus of gland located 1 fingerbreadth below cricoid cartilage
Pearls and Pitfalls of Thyroid Diagnosis Todd W. Frieze, MD, FACP, FACE, ECNU, CCD Endocrine Care, Hattiesburg Clinic Biloxi MS Thyroid Anatomy Isthmus of gland located 1 fingerbreadth below cricoid cartilage
Thyroid and Antithyroid Drugs. Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014
 Thyroid and Antithyroid Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed
Thyroid and Antithyroid Drugs Munir Gharaibeh, MD, PhD, MHPE Faculty of Medicine April 2014 Anatomy and histology of the thyroid gland Located in neck adjacent to the 5 th cervical vertebra (C5). Composed
Thyroid Plus. Central Thyroid Regulation & Activity. Peripheral Thyroid Function. Thyroid Auto Immunity. Key Guide. Patient: DOB: Sex: F MRN:
 Thyroid Plus Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4) 127 127
Thyroid Plus Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4) 127 127
THYROID DISEASE AND TESTING. Jack L. Snitzer, D.O., FACOI, FACE, CCD
 THYROID DISEASE AND TESTING Jack L. Snitzer, D.O., FACOI, FACE, CCD MAPA MEETING 2018 JACK L. SNITZER, D.O. 410-572-8848 JACK.SNITZER@PENINSULA.ORG NO CONFLICTS OF INTEREST THYROID THYROID Goiter Hyperthyroidism
THYROID DISEASE AND TESTING Jack L. Snitzer, D.O., FACOI, FACE, CCD MAPA MEETING 2018 JACK L. SNITZER, D.O. 410-572-8848 JACK.SNITZER@PENINSULA.ORG NO CONFLICTS OF INTEREST THYROID THYROID Goiter Hyperthyroidism
Thyroid function testing in pregnancy: 2017 ATA guidelines update. Dr Simon Forehan
 Thyroid function testing in pregnancy: 2017 ATA guidelines update Dr Simon Forehan Several factors are known to tax gravid thyroid economy: Increased plasma volume TBG pool increased Renal clearance Feto-placental
Thyroid function testing in pregnancy: 2017 ATA guidelines update Dr Simon Forehan Several factors are known to tax gravid thyroid economy: Increased plasma volume TBG pool increased Renal clearance Feto-placental
Table 1: Thyroid panel. Result (reference interval) TSH 89.5 miu/l ( ) Total T4 5.2 µg/dl ( ) T3 uptake 39% (22-35)
 TSH 89.5 miu/l ( ) Total T4 5.2 µg/dl ( ) T3 uptake 39% (22-35)") Introduction Thyroid disease is the second most common endocrine disorder (behind diabetes), and its prevalence increases with increasing age. The incidence of newly diagnosed thyroid cancer is increasing
Introduction Thyroid disease is the second most common endocrine disorder (behind diabetes), and its prevalence increases with increasing age. The incidence of newly diagnosed thyroid cancer is increasing
Evaluation and Management of Thyroid Nodules. Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada
 Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Decoding Your Thyroid Tests and Results
 Decoding Your Thyroid Tests and Results Wondering about your thyroid test results? Learn about each test and what low, optimal, and high results may mean so you can work with your doctor to choose appropriate
Decoding Your Thyroid Tests and Results Wondering about your thyroid test results? Learn about each test and what low, optimal, and high results may mean so you can work with your doctor to choose appropriate
Hypothyroidism and Hyperthyroidism. Paul V. Tomasic, MD, MS, FACP, FACE Nevada AACE EFNE & Annual Meeting October 6, 2018
 Hypothyroidism and Hyperthyroidism Paul V. Tomasic, MD, MS, FACP, FACE Nevada AACE EFNE & Annual Meeting October 6, 2018 Disclosures: None related to this program or presentation Objectives: Hypothyroidism
Hypothyroidism and Hyperthyroidism Paul V. Tomasic, MD, MS, FACP, FACE Nevada AACE EFNE & Annual Meeting October 6, 2018 Disclosures: None related to this program or presentation Objectives: Hypothyroidism
Mastering Thyroid Disorders. Douglas C. Bauer, MD UCSF Division of General Internal Medicine
 Mastering Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine Cases 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04, normal free T4 79
Mastering Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine Cases 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04, normal free T4 79
Lothian Guidance for Diagnosis and Management of Thyroid Dysfunction in Pregnancy
 Lothian Guidance for Diagnosis and Management of Thyroid Dysfunction in Pregnancy Early diagnosis and good management of maternal thyroid dysfunction are essential to ensure minimal adverse effects on
Lothian Guidance for Diagnosis and Management of Thyroid Dysfunction in Pregnancy Early diagnosis and good management of maternal thyroid dysfunction are essential to ensure minimal adverse effects on
Iodine 131 thyroid Therapy. Sara G. Johnson, MBA, CNMT, NCT President SNMMI-TS VA Healthcare System San Diego
 Iodine 131 thyroid Therapy Sara G. Johnson, MBA, CNMT, NCT President SNMMI-TS VA Healthcare System San Diego OBJECTIVES Describe the basics of thyroid gland anatomy and physiology Outline the disease process
Iodine 131 thyroid Therapy Sara G. Johnson, MBA, CNMT, NCT President SNMMI-TS VA Healthcare System San Diego OBJECTIVES Describe the basics of thyroid gland anatomy and physiology Outline the disease process
Common Thyroid Disorders
 Common Thyroid Disorders Louie Riesch MSN, MPH, RN, ACNS-BC, CDE Texas Diabetes and Endocrinology Anatomy of the Thyroid Gland Hypothalamic-Pituitary-Thyroid Axis Physiology Hypothalamus TRH Pituitary
Common Thyroid Disorders Louie Riesch MSN, MPH, RN, ACNS-BC, CDE Texas Diabetes and Endocrinology Anatomy of the Thyroid Gland Hypothalamic-Pituitary-Thyroid Axis Physiology Hypothalamus TRH Pituitary
4) Thyroid Gland Defects - Dr. Tara
 Thyroid Gland Defects - Dr. Tara") 4) Thyroid Gland Defects - Dr. Tara Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3, T4 T4 has negative feedback on secretion
4) Thyroid Gland Defects - Dr. Tara Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3, T4 T4 has negative feedback on secretion
Thyroid disorders. Dr Enas Abusalim
 Thyroid disorders Dr Enas Abusalim Thyroid physiology The hypothalamic pituitary thyroid axis And peripheral conversion of T4 to T3, WHERE, AND BY WHAT ENZYME?? Only relatively small concentrations of
Thyroid disorders Dr Enas Abusalim Thyroid physiology The hypothalamic pituitary thyroid axis And peripheral conversion of T4 to T3, WHERE, AND BY WHAT ENZYME?? Only relatively small concentrations of
Checking the Right Box at the Right Age: the Art of Pediatric Endocrine Testing
 Checking the Right Box at the Right Age: the Art of Pediatric Endocrine Testing Jean-Pierre Chanoine, MD Endocrinology and Diabetes Unit British Columbia s Children s Hospital Objectives 1. Interpret the
Checking the Right Box at the Right Age: the Art of Pediatric Endocrine Testing Jean-Pierre Chanoine, MD Endocrinology and Diabetes Unit British Columbia s Children s Hospital Objectives 1. Interpret the
Thyroid gland defects. Dr. Tara Husain
 Thyroid gland defects Dr. Tara Husain Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3,T4 T4 has negative feed back on secretion
Thyroid gland defects Dr. Tara Husain Thyroid Pituitary Axis TRH secreted in the hypothalamus stimulates production and Secretion of TSH TSH stimulates secretion of T3,T4 T4 has negative feed back on secretion
Should every pregnant woman be screened for thyroid disease?
 Should every pregnant woman be screened for thyroid disease? Tal Biron-Shental Rinat Gabbay-Benziv Is there a debate? Thyroid screening Guidelines Targeted case finding criteria Age > 30 years Personal
Should every pregnant woman be screened for thyroid disease? Tal Biron-Shental Rinat Gabbay-Benziv Is there a debate? Thyroid screening Guidelines Targeted case finding criteria Age > 30 years Personal
Management of Common Thyroid Disorders
 Cases Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04,
Cases Management of Common Thyroid Disorders Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04,
Alvin C. Powers, M.D. 1/27/06
 Thyroid Histology Follicular Cells ECF side Apical lumen Thyroid Follicles -200-400 um Parafollicular or C-cells Colloid Photos from University of Manchester and tutorial created by Dr. James Crimando,
Thyroid Histology Follicular Cells ECF side Apical lumen Thyroid Follicles -200-400 um Parafollicular or C-cells Colloid Photos from University of Manchester and tutorial created by Dr. James Crimando,
Thyroid Function. Thyroid Antibodies. Analyte Information
 Thyroid Function Thyroid Antibodies Analyte Information - 1-2013-04-30 Thyroid Antibodies Determination of thyroid autoantibodies are, besides TSH and FT4, one of the most important diagnostic parameters.
Thyroid Function Thyroid Antibodies Analyte Information - 1-2013-04-30 Thyroid Antibodies Determination of thyroid autoantibodies are, besides TSH and FT4, one of the most important diagnostic parameters.
Graves Disease in Pediatrics
 Graves Disease in Pediatrics Graves disease is a common cause of an overactive thyroid. It occurs in about 1 in 5000 children and teens. It occurs more often in females than males. This booklet is designed
Graves Disease in Pediatrics Graves disease is a common cause of an overactive thyroid. It occurs in about 1 in 5000 children and teens. It occurs more often in females than males. This booklet is designed
Canadian Endocrine Review Course 2014
 Canadian Endocrine Review Course 2014 Amiodarone & Thyrotoxicosis Iodine, A Catch 22 Ally P.H. Prebtani Associate Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University
Canadian Endocrine Review Course 2014 Amiodarone & Thyrotoxicosis Iodine, A Catch 22 Ally P.H. Prebtani Associate Professor of Medicine Internal Medicine, Endocrinology & Metabolism McMaster University
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging. Deepa R Biyyam, MD Attending Pediatric Radiologist
 Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Thyroid Screen (Serum)
") Thyroid Screen (Serum) Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4)
Thyroid Screen (Serum) Patient: DOB: Sex: F MRN: Order Number: Completed: Received: Collected: Sample Type - Serum Result Reference Range Units Central Thyroid Regulation & Activity Total Thyroxine (T4)
THYROID DISEASE IN CHILDREN
 THYROID DISEASE IN CHILDREN Michelle Schweiger, D.O. Center for Pediatric and Adolescent Endocrinology Cleveland Clinic Foundation Neither I nor any immediate family members have any financial interests
THYROID DISEASE IN CHILDREN Michelle Schweiger, D.O. Center for Pediatric and Adolescent Endocrinology Cleveland Clinic Foundation Neither I nor any immediate family members have any financial interests
GOITER and Shortness of Breath. Case A: GOITER. Learning Objectives. Common Thyroid Disorders for
 2:25 3:05pm Diagnosing and Treating Thyroid Disorders SPEAKER John Tayek, MD Presenter Disclosure Information The following relationships exist related to this presentation: John Tayek, MD, serves on the
2:25 3:05pm Diagnosing and Treating Thyroid Disorders SPEAKER John Tayek, MD Presenter Disclosure Information The following relationships exist related to this presentation: John Tayek, MD, serves on the
Slide notes: This presentation provides information on Graves disease, a systemic autoimmune disease. Epidemiology, pathology, complications,
 1 This presentation provides information on Graves disease, a systemic autoimmune disease. Epidemiology, pathology, complications, including ophthalmic complications, treatments (both permanent solutions
1 This presentation provides information on Graves disease, a systemic autoimmune disease. Epidemiology, pathology, complications, including ophthalmic complications, treatments (both permanent solutions
HYPERTHYROIDISM. Hypothalamus. Thyrotropin-releasing hormone (TRH) Anterior pituitary gland. Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3
 Anterior pituitary gland. Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3") HYPERTHYROIDISM Hypothalamus Thyrotropin-releasing hormone (TRH) Anterior pituitary gland Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3 In hyperthyroidism, there is an increased production of
HYPERTHYROIDISM Hypothalamus Thyrotropin-releasing hormone (TRH) Anterior pituitary gland Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3 In hyperthyroidism, there is an increased production of
Lothian Guidance for Diagnosis and Management of Thyroid Dysfunction in Pregnancy.
 Lothian Guidance for Diagnosis and Management of Thyroid Dysfunction in Pregnancy. Early diagnosis and good management of maternal thyroid dysfunction is essential to ensure minimal adverse effects on
Lothian Guidance for Diagnosis and Management of Thyroid Dysfunction in Pregnancy. Early diagnosis and good management of maternal thyroid dysfunction is essential to ensure minimal adverse effects on
Thyroid Cancer & rhtsh: When and How?
 Thyroid Cancer & rhtsh: When and How? 8 th Postgraduate Course in Endocrine Surgery Capsis Beach, Crete, September 21, 2006 Quan-Yang Duh, Professor of Surgery, UCSF Increasing Incidence of Thyroid Cancer
Thyroid Cancer & rhtsh: When and How? 8 th Postgraduate Course in Endocrine Surgery Capsis Beach, Crete, September 21, 2006 Quan-Yang Duh, Professor of Surgery, UCSF Increasing Incidence of Thyroid Cancer
Thyroid Disorders Towards a Healthy Endocrine System
 Thyroid Disorders Towards a Healthy Endocrine System What are Thyroid Disorders? The thyroid is a butterfly-shaped gland in the middle of the lower neck. Through the release of hormones, the thyroid regulates
Thyroid Disorders Towards a Healthy Endocrine System What are Thyroid Disorders? The thyroid is a butterfly-shaped gland in the middle of the lower neck. Through the release of hormones, the thyroid regulates
Dianne S Cheung, MD FACE Assistant Clinical Professor UCLA Health David Geffen School of Medicine CA-AACE Chapter Secretary
 Dianne S Cheung, MD FACE Assistant Clinical Professor UCLA Health David Geffen School of Medicine CA-AACE Chapter Secretary No Financial Disclosures Objectives Which thyroid labs to order and interpret?
Dianne S Cheung, MD FACE Assistant Clinical Professor UCLA Health David Geffen School of Medicine CA-AACE Chapter Secretary No Financial Disclosures Objectives Which thyroid labs to order and interpret?
Graves Disease. What is Graves disease?
 Graves Disease What is Graves disease? The thyroid gland s production of thyroid hormones (T 3 and T 4 ) is triggered by thyroidstimulating hormone (TSH), which is made by the pituitary gland. Graves disease,
Graves Disease What is Graves disease? The thyroid gland s production of thyroid hormones (T 3 and T 4 ) is triggered by thyroidstimulating hormone (TSH), which is made by the pituitary gland. Graves disease,
Objectives. How to Investigate Thyroid Nodules like A Pro
 How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
How to Investigate Thyroid Nodules like A Pro Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President ASEPA Disclosures
Updates in Thyroid Disease. Thyroid Outline. Thyroid 10/5/2015. Leila Wing, MD. Endocrinology, Diabetes, and Metabolism
 Updates in Thyroid Disease Leila Wing, MD Endocrinology, Diabetes, and Metabolism Background Hypothyroidism Hyperthyroidism Thyroid nodules Thyroid Cancer Conclusions Resources/References Thyroid Outline
Updates in Thyroid Disease Leila Wing, MD Endocrinology, Diabetes, and Metabolism Background Hypothyroidism Hyperthyroidism Thyroid nodules Thyroid Cancer Conclusions Resources/References Thyroid Outline
19th Century Thyroidology
 1 19th Century Thyroidology Dr. Kinnicutt s patient (1893) A cold, tired, constipated middle aged woman Slow pulse rate Low body temperature From physiology it was likely patient needed thyroid replacement
1 19th Century Thyroidology Dr. Kinnicutt s patient (1893) A cold, tired, constipated middle aged woman Slow pulse rate Low body temperature From physiology it was likely patient needed thyroid replacement
Some Issues in the Management of Hypothyroidism
 Some Issues in the Management of Hypothyroidism Family Medicine Refresher Course April 6, 2016 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Some Issues in the Management of Hypothyroidism Family Medicine Refresher Course April 6, 2016 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships
Understanding thyroid function tests. Dr. Colette George
 Understanding thyroid function tests Dr. Colette George Disclosures No financial disclosure I will present fictitious cases and thyroid function tests (TFTs) that are based on scenarios I commonly encounter.
Understanding thyroid function tests Dr. Colette George Disclosures No financial disclosure I will present fictitious cases and thyroid function tests (TFTs) that are based on scenarios I commonly encounter.
Objectives. 1)To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy
To recall thyroid nodule ultrasound characteristics that increase the risk of malignancy") Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
Evaluation and Management of Thyroid Nodules in Primary Care Chris Sadler, MA, PA C, CDE, DFAAPA Medical Science Outcomes Liaison Intarcia Diabetes and Endocrine Associates La Jolla, CA Past President
The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital
 The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital Presentation Today: Common thyroid problems and treatments Pregnancy related thyroid problems The suppressed
The Number Games and Thyroid Function Arshia Panahloo Consultant Endocrinologist St George s Hospital Presentation Today: Common thyroid problems and treatments Pregnancy related thyroid problems The suppressed
Disorders of the Thyroid Gland
 Disorders of the Thyroid Gland István Takács MD., PhD, 1st Department of Medicine, Semmelweis University Connection to the dentistry: close to each other higher operation risk radiating pain macroglossia
Disorders of the Thyroid Gland István Takács MD., PhD, 1st Department of Medicine, Semmelweis University Connection to the dentistry: close to each other higher operation risk radiating pain macroglossia
THYROID DISEASES. CASE BASED WORKSHOP Z. Henry He, MD, PhD. Endocrinology, Diabetes, & Metabolism Cambridge Health Alliance Harvard Medical School
 THYROID DISEASES CASE BASED WORKSHOP Z. Henry He, MD, PhD Endocrinology, Diabetes, & Metabolism Cambridge Health Alliance Harvard Medical School DISCLOSURE I have no relevant financial disclosure OBJECTIVES
THYROID DISEASES CASE BASED WORKSHOP Z. Henry He, MD, PhD Endocrinology, Diabetes, & Metabolism Cambridge Health Alliance Harvard Medical School DISCLOSURE I have no relevant financial disclosure OBJECTIVES
Iodine and Thyroid Hormones
 Iodine and Thyroid Hormones Iodine and Thyroid Hormones feed-back Iodine Deficiency Characteristics Iodine Deficiency None Mild Mode Severe Median urine iodine >100 50-99 20-49
Iodine and Thyroid Hormones Iodine and Thyroid Hormones feed-back Iodine Deficiency Characteristics Iodine Deficiency None Mild Mode Severe Median urine iodine >100 50-99 20-49
Update In Hypothyroidism
 Update In Hypothyroidism CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
Update In Hypothyroidism CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
Evaluation and Management of Thyroid Nodules. Overview of Thyroid Nodules and Their Management. Thyroid Nodule detection: U/S versus Exam
 Overview of Thyroid Nodules and Their Management Matthew D. Ringel, M.D. Professor of Medicine Divisions of Endocrinology and Oncology, The Ohio State University Co-Director, Thyroid Cancer Unit Arthur
Overview of Thyroid Nodules and Their Management Matthew D. Ringel, M.D. Professor of Medicine Divisions of Endocrinology and Oncology, The Ohio State University Co-Director, Thyroid Cancer Unit Arthur
1 day PTA: vaginal spotting, LE edema LMP 6 weeks ago. OSH Clinic: distended abdomen, (+) urine pregnancy; sent home with iron
 urine pregnancy; sent home with iron") Anila Bindal, MD 1 day PTA: vaginal spotting, LE edema LMP 6 weeks ago OSH Clinic: distended abdomen, (+) urine pregnancy; sent home with iron UCMC ER: abdomen doubled overnight, significant vaginal bleeding,
Anila Bindal, MD 1 day PTA: vaginal spotting, LE edema LMP 6 weeks ago OSH Clinic: distended abdomen, (+) urine pregnancy; sent home with iron UCMC ER: abdomen doubled overnight, significant vaginal bleeding,
Hypothyroidism. Causes. Diagnosis. Christopher Theberge
 Hypothyroidism Pronunciations: (Hypothyroidism) Hypothyroidism (under active thyroid) is a condition where the thyroid gland fails to secrete enough of the thyroid hormones thyroxine (T4) and triiodothyronine
Hypothyroidism Pronunciations: (Hypothyroidism) Hypothyroidism (under active thyroid) is a condition where the thyroid gland fails to secrete enough of the thyroid hormones thyroxine (T4) and triiodothyronine
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Thyroid Disease & Pregnancy Updates and Ongoing Questions
 Thyroid Disease & Pregnancy - 2018 Updates and Ongoing Questions Erik K. Alexander, MD Chief, Thyroid Section, Division of Endocrinology Brigham & Women s Hospital Professor of Medicine, Harvard Medical
Thyroid Disease & Pregnancy - 2018 Updates and Ongoing Questions Erik K. Alexander, MD Chief, Thyroid Section, Division of Endocrinology Brigham & Women s Hospital Professor of Medicine, Harvard Medical
Thyroid Disorders. January 2019
 Thyroid Disorders January 2019 What is the Thyroid? The thyroid is a small butterfly-shaped gland inside the neck, located in front of the trachea (windpipe) and below the larynx (voicebox). It produces
Thyroid Disorders January 2019 What is the Thyroid? The thyroid is a small butterfly-shaped gland inside the neck, located in front of the trachea (windpipe) and below the larynx (voicebox). It produces
Sample Type - Serum Result Reference Range Units. Central Thyroid Regulation Surrey & Activity KT3 4Q. Peripheral Thyroid D Function mark
 Thyroid Plus Sample Type - Serum Result Reference Range Units Central Thyroid Regulation Surrey & Activity KT3 4Q Total Thyroxine (T4)
Thyroid Plus Sample Type - Serum Result Reference Range Units Central Thyroid Regulation Surrey & Activity KT3 4Q Total Thyroxine (T4)
Thyroid Disease. Scott D. Isaacs, MD, FACP, FACE HRT Symposium Savannah GA July 14 16, All Rights Reserved. 1
 Thyroid Disease Scott D. Isaacs, MD, FACP, FACE HRT Symposium Savannah GA July 14 16, 2016 2016. All Rights Reserved. 1 Disclosure Scott D. Isaacs, MD, FACP, FACE, is the Medical Director at Atlanta Center
Thyroid Disease Scott D. Isaacs, MD, FACP, FACE HRT Symposium Savannah GA July 14 16, 2016 2016. All Rights Reserved. 1 Disclosure Scott D. Isaacs, MD, FACP, FACE, is the Medical Director at Atlanta Center
Jim Paoletti BS Pharmacy, FAARM, FIACP, Director of Education, P2P
 presents A Pioneering Functional Technologies Approach For to Hypothyroidism Lifestyle Based Medicine Part 3 of 3 with Jim Paoletti BS Pharmacy, FAARM, FIACP, Director of Education, P2P Clinical Consultant
presents A Pioneering Functional Technologies Approach For to Hypothyroidism Lifestyle Based Medicine Part 3 of 3 with Jim Paoletti BS Pharmacy, FAARM, FIACP, Director of Education, P2P Clinical Consultant
AUGUST 25-27, 2017 UPDATE & BOARD REVIEW. acofp INTENSIVE. Evolving Issues in Endocrinology. Chris Pitsch, DO INNOVATIVE COMPREHENSIVE HANDS-ON
 acofp INTENSIVE UPDATE & BOARD REVIEW AUGUST 25-27, 2017 Loews Chicago O'Hare Hotel Rosemont, IL INNOVATIVE COMPREHENSIVE HANDS-ON Evolving Issues in Endocrinology Chris Pitsch, DO acofp Am eric an College
acofp INTENSIVE UPDATE & BOARD REVIEW AUGUST 25-27, 2017 Loews Chicago O'Hare Hotel Rosemont, IL INNOVATIVE COMPREHENSIVE HANDS-ON Evolving Issues in Endocrinology Chris Pitsch, DO acofp Am eric an College