Sub-arachnoid haemorrhage
|
|
|
- Christopher Marsh
- 5 years ago
- Views:
Transcription



1 Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust Kiev, Ukraine September 17 th 2009
2 Sub-arachnoid haemorrhage (SAH) introduction overview of SAH
3 Sub-arachnoid haemorrhage (SAH) introduction overview of SAH aneurysmal SAH
4 Sub-arachnoid haemorrhage (SAH) introduction overview of SAH aneurysmal SAH complications and their treatment
5 Sub-arachnoid haemorrhage (SAH) introduction overview of SAH aneurysmal SAH complications and their treatment occlusion of aneurysm
6 Sub-arachnoid haemorrhage (SAH) introduction overview of SAH aneurysmal SAH complications and their treatment occlusion of aneurysm implications for the anaesthetist
7 Sub-arachnoid haemorrhage prognosis poor early treatment may improve outcome prompt diagnosis appropriate treatment essential
8 Sub-arachnoid haemorrhage presentation worst ever headache / hit at back of head nausea/vomiting/photophobia loss of consciousness (transient/prolonged) seizures (10%) neurological deficit
9 Sub-arachnoid haemorrhage diagnosis/investigations physical examination -ABC -GCS - BP/ temperature - intraocular haemorrhage - neurological deficit
10 Sub-arachnoid haemorrhage diagnosis/investigations full blood count coagulation screen urea/electrolytes blood glucose chest radiography 12 lead ECG
11 Sub-arachnoid haemorrhage diagnosis/investigations early non-contrast computerised tomography (CT) < 12 h miss 2% > 12h < 24 h miss 7 % > 10 days no blood seen
12 Sub-arachnoid haemorrhage diagnosis/investigations -ve CT scan lumbar puncture (LP) >12h - haemoglobin oxyhaemoglobin + bilirubin - spectrophotometry - distinguishes SAH from traumatic LP - + ve for bilirubin >2 weeks
13 Sub-arachnoid haemorrhage diagnosis/investigations + ve diagnosis - refer to specialist centre
14 Sub-arachnoid haemorrhage diagnosis/investigations CTA cerebral angiography
15 Sub-arachnoid haemorrhage causes traumatic (most common) spontaneous

16 Sub-arachnoid haemorrhage aneurysmal SAH
17 Aneurysmal sub-arachnoid haemorrhage prognosis devastating condition 50% mortality by 30 days only 50% survivors return to independent living early diagnosis essential to optimize outcome
18 Aneurysmal sub-arachnoid haemorrhage epidemiology & aetiology 7/ population F:M 3:2 mean age (55 60y) family history, coarctation of aorta, polycystic disease, connective tissue disorder smoking
19 Aneurysmal sub-arachnoid haemorrhage epidemiology & aetiology degenerative changes in tunica media of artery mostly at bifurcation anterior circulation % posterior circulation %
20
21 Aneurysmal sub-arachnoid haemorrhage early mortality/ morbidity may be from; - intracranial and/or - extracranial complications
22 Aneurysmal sub-arachnoid haemorrhage intracranial complications rebleed hydrocephalus vasospasm seizures
23 Aneurysmal sub-arachnoid haemorrhage intracranial complications rebleed - serious risk of death (40%) - highest risk is first 24 hours (10%) - 25% risk rebleed in first 2 weeks - 3% risk per year thereafter
24 Aneurysmal sub-arachnoid haemorrhage intracranial complications rebleed hydrocephalus vasospasm seizures
25 Aneurysmal sub-arachnoid haemorrhage intracranial complications hydrocephalus -early (1 st 24 h) external ventricular drain - late (10%) ventriculo-peritoneal shunt

26
27 Aneurysmal sub-arachnoid haemorrhage intracranial complications rebleed hydrocephalus vasospasm seizures


28 Aneurysmal sub-arachnoid haemorrhage transcranial doppler seizures
29 Aneurysmal sub-arachnoid haemorrhage intracranial complications vasospasm - risk day % angiographic vasospasm - 33% symptomatic ( GCS/neurological deficit) - 20% patients with vasospasm permanent neurological deficit/death

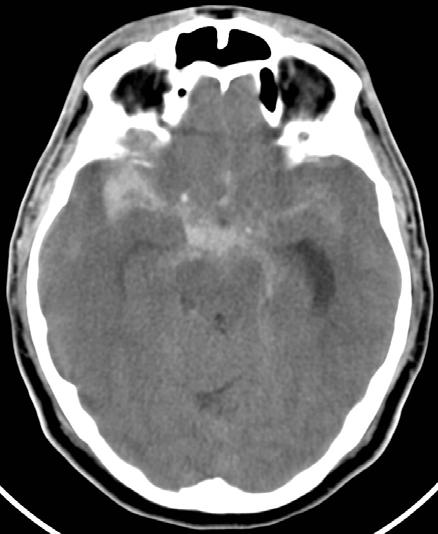
30 CT scan - extensive SAH

31 CT scan - multiple cerebral infarcts after SAH
32 Aneurysmal sub-arachnoid haemorrhage intracranial complications vasospasm - prophylaxis nimodipine 60mg (4 hourly) x 3 weeks well hydrated normotension avoid hyponatraemia
33 Aneurysmal sub-arachnoid haemorrhage intracranial complications vasospasm - treatment for symptomatic patients = triple-h therapy hypertension (* care with unprotected aneurysm) hypervolaemia haemodilution
34 Aneurysmal sub-arachnoid haemorrhage intracranial complications vasospasm - treatment for symptomatic patients no improvement after one hour triple-h therapy? CT (to exclude infarct) angiography balloon angioplasty (segmental spasm) intra-arterial nimodipine (global spasm)
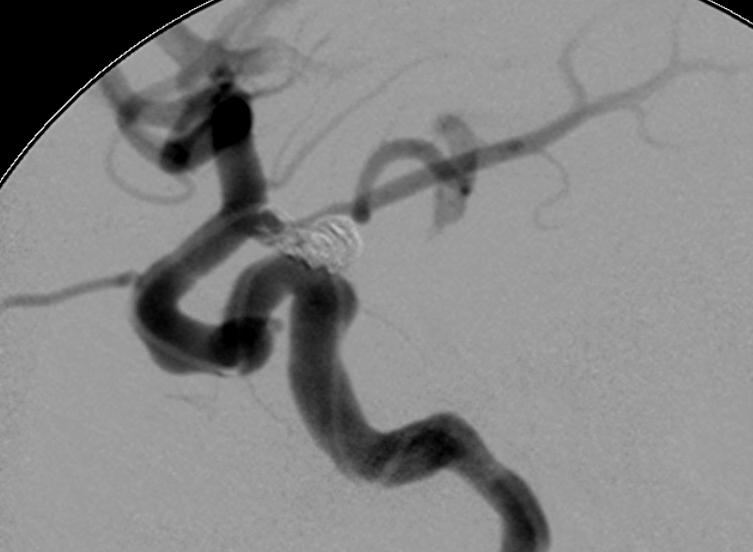
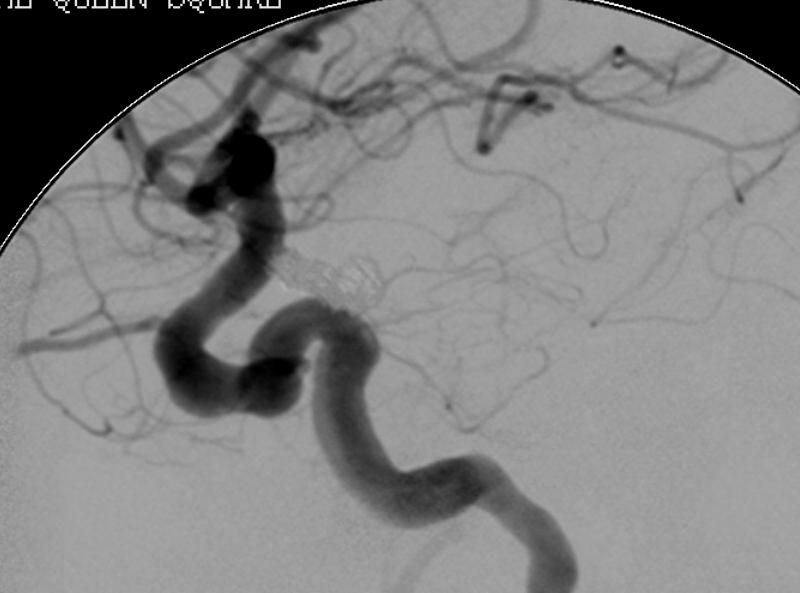
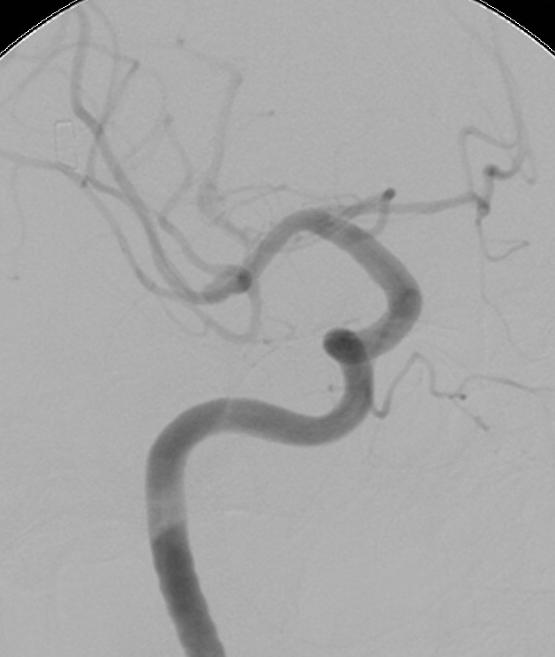
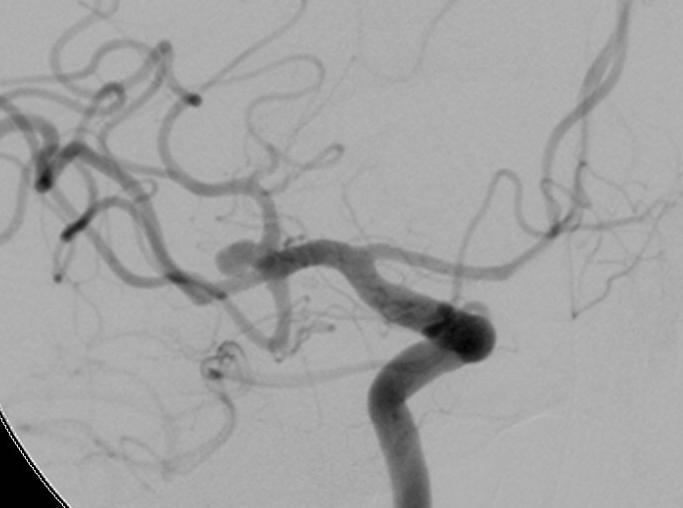
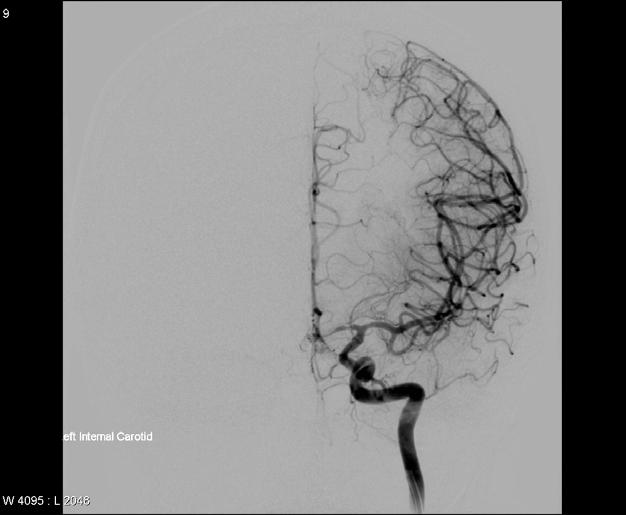
35 Aneurysmal sub-arachnoid haemorrhage vasopasm Pre-nimodipine Post-nimodipine
36 Aneurysmal sub-arachnoid haemorrhage intracranial complications rebleed hydrocephalus vasospasm seizures
37 Aneurysmal sub-arachnoid haemorrhage intracranial complications seizures - low incidence (10%) - no anticonvulsant unless 2nd witnessed fit
38 Aneurysmal sub-arachnoid haemorrhage extracranial complications cardiac dysrhythmias myocardial injury/dysfunction pulmonary complications electrolyte disturbance

39 Aneurysmal sub-arachnoid haemorrhage extracranial complications cardiac dysrhythmias very common % - prolonged QT interval - non-specific ST segment changes
40 Aneurysmal sub-arachnoid haemorrhage extracranial complications ECG changes mostly neurogenic origin proportional to severity of neuronal damage troponin reflects myocardial injury and is associated with poor outcome
41 Aneurysmal sub-arachnoid haemorrhage extracranial complications cardiac dysrhythmias myocardial injury/dysfunction pulmonary complications electrolyte disturbance
42 Aneurysmal sub-arachnoid haemorrhage extracranial complications myocardial injury/dysfunction - approx 10-30% - neurogenic-stunned myocardium is most severe (reversible LV dysfunction + pulmonary oedema)

43 Cardiogenic pulmonary oedema

44 Resolving cardiogenic pulmonary oedema (oesophageal doppler in position)
45 Aneurysmal sub-arachnoid haemorrhage extracranial complications cardiac dysrhythmias myocardial injury/dysfunction pulmonary complications electrolyte disturbance
46 Aneurysmal sub-arachnoid haemorrhage extracranial complications aspiration pneumonia cardiogenic pulmonary oedema neurogenic pulmonary oedema - hydrostatic pressure injury to pulmonary capillaries at time of bleed
47 Aneurysmal sub-arachnoid haemorrhage extracranial complications cardiac dysrhythmias myocardial injury/dysfunction pulmonary complications electrolyte disturbance
48 Aneurysmal sub-arachnoid haemorrhage extracranial complications electrolyte disturbance common Na + (30-40%) SIADH or CSWS Mg 2+ (50%)? vasospasm K +
49 Sub-arachnoid haemorrhage overview of sub-arachnoid haemorrhage (SAH) aneurysmal sub-arachnoid haemorrhage complications and their treatment occlusion of aneurysm implications for the anaesthetist
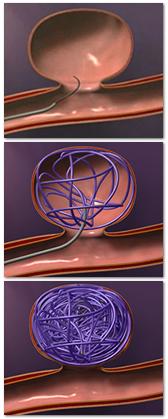
50 Aneurysmal sub-arachnoid haemorrhage occlusion of aneurysm surgical clipping endovascular coiling
51 Aneurysmal sub-arachnoid haemorrhage occlusion of aneurysm International Subarachnoid Aneurysm Trial (ISAT) published 2002 neurosurgical clipping v endovascular coiling many caveats but outcome significantly better with endovascular coiling ISAT Collaborative Group The Lancet 2002; 360:

52
53 Aneurysmal sub-arachnoid haemorrhage occlusion of aneurysm at our hospital multidisciplinary approach most aneurysms coiling (120 in 2008) middle cerebral artery aneurysm (mca) clipping rapid learning curve with coiling treating more and more complicated aneurysms consultant led service
54 Aneurysmal sub-arachnoid haemorrhage coiling implications for the anaesthetist
55 Aneurysmal sub-arachnoid haemorrhage coiling - implications for the anaesthetist consideration of associated medical problems - ECG abnormalities, BP, pulmonary problems wherever possible proceed; secured aneurysm may allow optimization of other conditions coiling probably less challenging if cardiac impairment
56 Aneurysmal sub-arachnoid haemorrhage coiling - implications for the anaesthetist geographically remote (theatres/itu) cramped conditions moving equipment poor light flat table (problem if ICP ) radiation hazard
57 Angiography suite

58 Angiography suite

59 Angiography suite
60 Aneurysmal sub-arachnoid haemorrhage coiling - implications for the anaesthetist general principles of anaesthesia are the same for clipping & coiling ; prevention of rupture CVS stability - maintain CPP - avoid hypertension maintain optimal ICP prevent movement to stimulus
61 Aneurysmal sub-arachnoid haemorrhage coiling - implications for the anaesthetist Induction/maintenance anaesthesia avoid volatile agents if ICP avoid N 2 0 (micro air emboli) aim for PaCO KPa prevent hyperthermia
62 Aneurysmal sub-arachnoid haemorrhage coiling - implications for the anaesthetist nasogastric tube post-induction (aspirin) tracheal intubation i.v. access arterial line no CVP line urinary catheter nasopharyngeal temperature
63 Aneurysmal sub-arachnoid haemorrhage coiling - implications for the anaesthetist specific problems during procedure; - vasospasm (nimodipine) - aneurysm rupture - thrombosis rapid action
64 Aneurysmal sub-arachnoid haemorrhage coiling - implications for the anaesthetist specific problems; - vasospasm (nimodipine) - aneurysm rupture - thrombosis rapid action
65
66 Aneurysmal sub-arachnoid haemorrhage coiling - implications for the anaesthetist aneurysm rupture - closed cranium - massive ICP and CBF - patient often anti-coagulated (heparin) -do notreverse heparin - control BP (propofol) - rapidly continue coiling - urgent CT scan? transfer to theatre
67 Aneurysmal sub-arachnoid haemorrhage coiling - implications for the anaesthetist specific problems; - vasospasm (nimodipine) - aneurysm rupture - thrombosis
68 Aneurysmal sub-arachnoid haemorrhage coiling - implications for the anaesthetist thrombosis - requires rapid action seconds count - usually with last coil (aneurysm secure) - elevate blood pressure -abciximab (glycoprotein IIb/IIIa receptor antagonist)
69 Aneurysmal sub-arachnoid haemorrhage coiling - implications for the anaesthetist emergency situations - successful outcome requires urgent management by experienced team - coiling procedures therefore within normal working hours
70 Sub-arachnoid haemorrhage aneurysmal SAH conclusions aneurysmal SAH has a poor prognosis anaesthetists involved at many stages of a patient s illness early treatment (occlusion) and supportive neurocritical care may improve outcome
71 Thank you for your attention
72

73 AP Projections of Right MCA Aneurysm

74
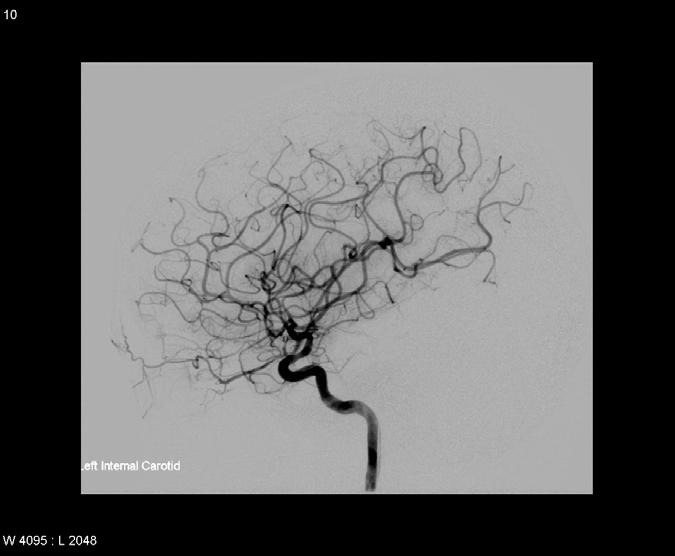
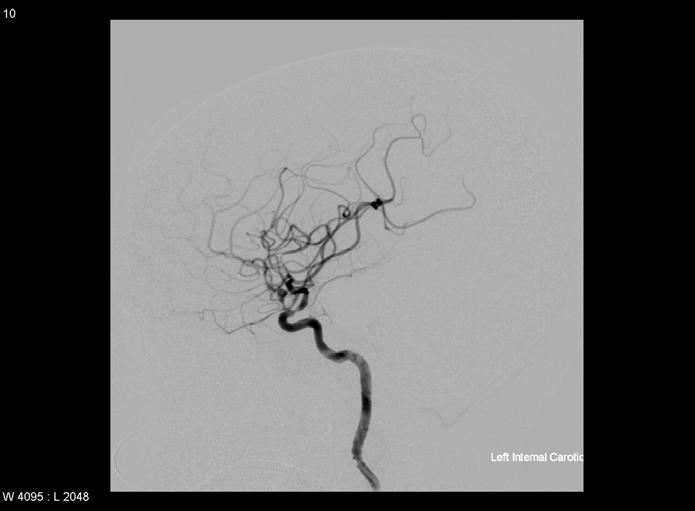
75 Pre-nimodipine Post-nimodipine
76
77 Sub-arachnoid haemorrhage causes traumatic (most common) spontaneous
78 Angiography suite
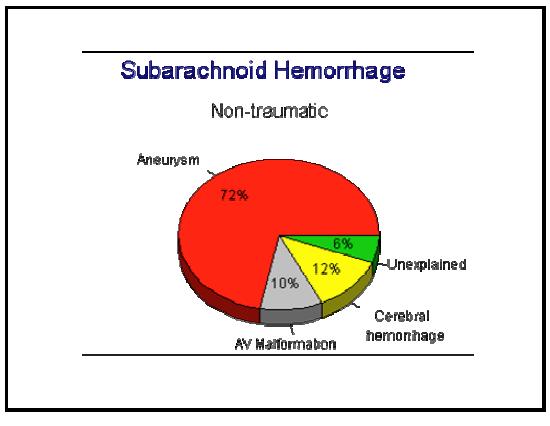
79 Sub-arachnoid haemorrhage diagnosis/investigations aneurysm 72% -ve angiography 10% (perimesencephalic) AVM, tumours, vasculitis etc

80 Angiography suite

81 Meninges Skull Dura mater achnoid Vessel Brain Extradural Subdural

82 Sub-arachnoid space
83 Aneurysmal sub-arachnoid haemorrhage prognosis grading - aids research / prognosis / guides treatment - most common; WFNS (World Federation of Neurological Surgeons) Hunt and Hess
84 Aneurysmal sub-arachnoid haemorrhage WFNS (World Federation of Neurological Surgeons) Grade GCS Motor deficit I 15 absent II absent III present IV 7-12 absent/ present V 3-6 absent/ present
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications
 Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Current State of the Art
 SAH Current State of the Art Thomas C. Steineke, M.D., Ph.D. Director of Neurovascular Surgery NJ Neuroscience Institute JFK Medical Center Introduction Signs and symptoms of a problem What are aneurysms
SAH Current State of the Art Thomas C. Steineke, M.D., Ph.D. Director of Neurovascular Surgery NJ Neuroscience Institute JFK Medical Center Introduction Signs and symptoms of a problem What are aneurysms
SAH READMISSIONS TO NCCU
 SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
Head injuries. Severity of head injuries
 Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Head injuries ED Teaching day 23 rd October Severity of head injuries Minor GCS 14-15 Must not have any of the following: Amnesia 10min Neurological sign or symptom Skull fracture (clinically or radiologically)
Method Hannah Shotton
 #asah Method Hannah Shotton 2 Introduction SAH Rupturing aneurysm Poor outlook Intervention Secure the aneurysm: clipping or coiling Recommended 48 hours Regional Specialist NSC Conservative management
#asah Method Hannah Shotton 2 Introduction SAH Rupturing aneurysm Poor outlook Intervention Secure the aneurysm: clipping or coiling Recommended 48 hours Regional Specialist NSC Conservative management
4/10/2018. The Surgical Treatment of Cerebral Aneurysms. Aneurysm Locations. Aneurysmal Subarachnoid Hemorrhage. Jerone Kennedy, M.D.
 The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
TCD AND VASOSPASM SAH
 CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
Management of Cerebral Aneurysms in Polycystic Kidney Disease. Dr H Stockley Consultant Neuroradiologist Greater Manchester Neuroscience Centre
 Management of Cerebral Aneurysms in Polycystic Kidney Disease Dr H Stockley Consultant Neuroradiologist Greater Manchester Neuroscience Centre What is a cerebral aneurysm? Developmental degenerative arterial
Management of Cerebral Aneurysms in Polycystic Kidney Disease Dr H Stockley Consultant Neuroradiologist Greater Manchester Neuroscience Centre What is a cerebral aneurysm? Developmental degenerative arterial
Aneurysmal subarachnoid haemorrhage and the anaesthetist
 British Journal of Anaesthesia 99 (1): 102 18 (2007) doi:10.1093/bja/aem119 Advance Access publication May 23, 2007 Aneurysmal subarachnoid haemorrhage and the anaesthetist H.-J. Priebe* Department of
British Journal of Anaesthesia 99 (1): 102 18 (2007) doi:10.1093/bja/aem119 Advance Access publication May 23, 2007 Aneurysmal subarachnoid haemorrhage and the anaesthetist H.-J. Priebe* Department of
Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management
 0 0 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management The Department of Health and Social Care in England
0 0 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management The Department of Health and Social Care in England
Subarachnoid Hemorrhage and Brain Aneurysm
 Subarachnoid Hemorrhage and Brain Aneurysm DIN Department of Interventional Neurology What is SAH? Subarachnoid Haemorrhage is the sudden leaking (haemorrhage) of blood from the blood vessels of brain.
Subarachnoid Hemorrhage and Brain Aneurysm DIN Department of Interventional Neurology What is SAH? Subarachnoid Haemorrhage is the sudden leaking (haemorrhage) of blood from the blood vessels of brain.
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM. Vikram Jadhav MD, PhD. 04/12/2018 CentraCare Health St.
 ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part B. Objectives Epidemiology of asah Concept: What is a brain
Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part B. Objectives Epidemiology of asah Concept: What is a brain
Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage
 Romanian Neurosurgery (2016) XXX 4: 461 466 461 DOI: 10.1515/romneu-2016-0074 Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage A. Chiriac, Georgiana Ion*,
Romanian Neurosurgery (2016) XXX 4: 461 466 461 DOI: 10.1515/romneu-2016-0074 Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage A. Chiriac, Georgiana Ion*,
Neurosurgical decision making in structural lesions causing stroke. Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery)
") Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes
 and Non- Aneurysmal Causes") Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
Subarachnoid Hemorrhage (SAH) Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.
 Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.") Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici
 Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici Nino Stocchetti Milan University Neuroscience ICU Ospedale Policlinico IRCCS Milano stocchet@policlinico.mi.it Macdonald RL et
Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici Nino Stocchetti Milan University Neuroscience ICU Ospedale Policlinico IRCCS Milano stocchet@policlinico.mi.it Macdonald RL et
Guidelines for the management of a patient with a subarachnoid haemorrhage
 Guidelines for the management of a patient with a subarachnoid haemorrhage Item Type Report Authors Health Service Executive (HSE) Citation Health Service Executive. Guidelines for the management of a
Guidelines for the management of a patient with a subarachnoid haemorrhage Item Type Report Authors Health Service Executive (HSE) Citation Health Service Executive. Guidelines for the management of a
(aneurysmal subarachnoid hemorrhage, 17%~60% :SAH. ,asah , 22%~49% : Willis. :1927 Moniz ;(3) 2. ischemic neurological deficit,dind) SAH) SAH ;(6)
 2. ischemic neurological deficit,dind) SAH) SAH ;(6)") ,, 2. : ;,, :(1), (delayed ;(2) ischemic neurological deficit,dind) ;(3) 2. :SAH ;(4) 5-10 10 HT -1-1 ;(5), 10 SAH ;(6) - - 27%~50%, ( cerebral vasospasm ) Glasgow (Glasgow Coma Scale,GCS), [1],, (aneurysmal
,, 2. : ;,, :(1), (delayed ;(2) ischemic neurological deficit,dind) ;(3) 2. :SAH ;(4) 5-10 10 HT -1-1 ;(5), 10 SAH ;(6) - - 27%~50%, ( cerebral vasospasm ) Glasgow (Glasgow Coma Scale,GCS), [1],, (aneurysmal
Update in Diagnosis and Management of Intracranial Aneurysms for Primary Health Care Providers November 15, 2012 Boston, Massachusetts
 Update in Diagnosis and Management of Intracranial Aneurysms for Primary Health Care Providers November 15, 2012 Boston, Massachusetts Educational Partner: Session 1: Update in Diagnosis and Management
Update in Diagnosis and Management of Intracranial Aneurysms for Primary Health Care Providers November 15, 2012 Boston, Massachusetts Educational Partner: Session 1: Update in Diagnosis and Management
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Subarachnoid Hemorrhage & Vasospasm basic level
 Subarachnoid Hemorrhage & Vasospasm basic level Overview Subarachnoid hemorrhage (SAH) is a serious, lifethreatening type of stroke caused by bleeding into the space surrounding the brain. A stroke occurs
Subarachnoid Hemorrhage & Vasospasm basic level Overview Subarachnoid hemorrhage (SAH) is a serious, lifethreatening type of stroke caused by bleeding into the space surrounding the brain. A stroke occurs
10. Severe traumatic brain injury also see flow chart Appendix 5
 10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
10. Severe traumatic brain injury also see flow chart Appendix 5 Introduction Severe traumatic brain injury (TBI) is the leading cause of death in children in the UK, accounting for 15% of deaths in 1-15
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Summary of some of the landmark articles:
 Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE
 2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
2018 UPDATE QUICK SHEET 2018 American Heart Association GUIDELINES FOR THE EARLY MANAGEMENT OF PATIENTS WITH ACUTE ISCHEMIC STROKE A Summary for Healthcare Professionals from the American Heart Association/American
Canadian Best Practice Recommendations for Stroke Care 3.6 Acute Subarachnoid Hemorrhage
 Last Updated: May 21, 2013 Canadian Best Practice Recommendations for Stroke Care Canadian Best Practice Recommendations for Stroke Care 2011-2013 Update Contents Search Strategy... 2 CSN Current Recommendations...Error!
Last Updated: May 21, 2013 Canadian Best Practice Recommendations for Stroke Care Canadian Best Practice Recommendations for Stroke Care 2011-2013 Update Contents Search Strategy... 2 CSN Current Recommendations...Error!
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F.
 THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F. ISHFAQ ZEENAT QURESHI STROKE INSTITUTE AND UNIVERSITY OF TENNESSEE,
THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F. ISHFAQ ZEENAT QURESHI STROKE INSTITUTE AND UNIVERSITY OF TENNESSEE,
Subarachnoid haemorrhage: the management of neurogenic pulmonary oedema
 Subarachnoid haemorrhage: the management of neurogenic pulmonary oedema Clinical problem and domain I chose this case because I had not encountered neurogenic pulmonary oedema previously and was unfamiliar
Subarachnoid haemorrhage: the management of neurogenic pulmonary oedema Clinical problem and domain I chose this case because I had not encountered neurogenic pulmonary oedema previously and was unfamiliar
NIH Public Access Author Manuscript J Am Coll Radiol. Author manuscript; available in PMC 2013 June 24.
 NIH Public Access Author Manuscript Published in final edited form as: J Am Coll Radiol. 2010 January ; 7(1): 73 76. doi:10.1016/j.jacr.2009.06.015. Cerebral Aneurysms Janet C. Miller, DPhil, Joshua A.
NIH Public Access Author Manuscript Published in final edited form as: J Am Coll Radiol. 2010 January ; 7(1): 73 76. doi:10.1016/j.jacr.2009.06.015. Cerebral Aneurysms Janet C. Miller, DPhil, Joshua A.
Epidemiology And Treatment Of Cerebral Aneurysms At An Australian Tertiary Level Hospital
 ISPUB.COM The Internet Journal of Neurosurgery Volume 9 Number 2 Epidemiology And Treatment Of Cerebral Aneurysms At An Australian Tertiary Level Hospital A Granger, R Laherty Citation A Granger, R Laherty.
ISPUB.COM The Internet Journal of Neurosurgery Volume 9 Number 2 Epidemiology And Treatment Of Cerebral Aneurysms At An Australian Tertiary Level Hospital A Granger, R Laherty Citation A Granger, R Laherty.
Interventions in the Management of Acute Stroke. Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital
 Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
Emergency Room Procedure The first few hours in hospital...
 Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Emergency Room Procedure The first few hours in hospital... ER 5 level Emergency Severity Index SOP s for Stroke Stroke = Level 2 Target Time = 1 Hour 10 min from door 2 Doctor 25 min from door 2 CT 60
Assessment of Vasospasm and Delayed Cerebral Ischemia after Subarachnoid Hemorrhage: Current concepts and Value of CT Perfusion and CT Angiography
 Assessment of Vasospasm and Delayed Cerebral Ischemia after Subarachnoid Hemorrhage: Current concepts and Value of CT Perfusion and CT Angiography Poster No.: C-2563 Congress: ECR 2012 Type: Educational
Assessment of Vasospasm and Delayed Cerebral Ischemia after Subarachnoid Hemorrhage: Current concepts and Value of CT Perfusion and CT Angiography Poster No.: C-2563 Congress: ECR 2012 Type: Educational
HEAD INJURY. Dept Neurosurgery
 HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
HEAD INJURY Dept Neurosurgery INTRODUCTION PATHOPHYSIOLOGY CLINICAL CLASSIFICATION MANAGEMENT - INVESTIGATIONS - TREATMENT INTRODUCTION Most head injuries are due to an impact between the head and another
Paul Gigante HMS IV Gillian Lieberman, MD. Sept Mr. T s T s Headache. Paul Gigante,, Harvard Medical School Year IV Gillian Lieberman, MD
 Sept 2005 Mr. T s T s Headache Paul Gigante,, Harvard Medical School Year IV Mr. T s T s Presentation 45 year-old welder complains of sudden severe headache and witnessed seizure with loss of consciousness
Sept 2005 Mr. T s T s Headache Paul Gigante,, Harvard Medical School Year IV Mr. T s T s Presentation 45 year-old welder complains of sudden severe headache and witnessed seizure with loss of consciousness
NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM
 NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM Chairperson Professor Dr Zamzuri Idris Head of Department Members Associate Professor Dato Dr
NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM Chairperson Professor Dr Zamzuri Idris Head of Department Members Associate Professor Dato Dr
lek Magdalena Puławska-Stalmach
 lek Magdalena Puławska-Stalmach tytuł pracy: Kliniczne i radiologiczne aspekty tętniaków wewnątrzczaszkowych a wybór metody leczenia Summary An aneurysm is a localized, abnormal distended lumen of the
lek Magdalena Puławska-Stalmach tytuł pracy: Kliniczne i radiologiczne aspekty tętniaków wewnątrzczaszkowych a wybór metody leczenia Summary An aneurysm is a localized, abnormal distended lumen of the
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Acute management of aneurysmal subarachnoid haemorrhage
 Acute management of aneurysmal subarachnoid haemorrhage Astri Luoma MBChB FRCA Ugan Reddy BSc MBChB FRCA FFICM Matrix reference 2F01, 2A12 Key points Subarachnoid haemorrhage (SAH) accounts for only around
Acute management of aneurysmal subarachnoid haemorrhage Astri Luoma MBChB FRCA Ugan Reddy BSc MBChB FRCA FFICM Matrix reference 2F01, 2A12 Key points Subarachnoid haemorrhage (SAH) accounts for only around
Definition พ.ญ.ส ธ ดา เย นจ นทร. Epidemiology. Definition 5/25/2016. Seizures after stroke Can we predict? Poststroke seizure
 Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
Clinical manifestations, diagnosis and medical management of
 Clinical manifestations, diagnosis and medical management of aneurysmal SAH David Bervini, MD MAdvSurg Department of Neurosurgery Inselspital University of Bern Switzerland 1 2 3 Aneurysmal SAH Incidence:
Clinical manifestations, diagnosis and medical management of aneurysmal SAH David Bervini, MD MAdvSurg Department of Neurosurgery Inselspital University of Bern Switzerland 1 2 3 Aneurysmal SAH Incidence:
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine
 Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
Vivek R. Deshmukh, MD Director, Cerebrovascular and Endovascular Neurosurgery Chairman, Department of Neurosurgery Providence Brain and Spine Institute The Oregon Clinic Disclosure I declare that neither
AEROMEDICAL DECISION MAKING IN CEREBRAL ANEURYSMS. Pooshan Navāthé Michael Drane Peter Clem David Fitzgerald
 AEROMEDICAL DECISION MAKING IN CEREBRAL ANEURYSMS Pooshan Navāthé Michael Drane Peter Clem David Fitzgerald Disclaimer I receive a salary from the Commonwealth of Australia. I have no financial relationships
AEROMEDICAL DECISION MAKING IN CEREBRAL ANEURYSMS Pooshan Navāthé Michael Drane Peter Clem David Fitzgerald Disclaimer I receive a salary from the Commonwealth of Australia. I have no financial relationships
Ruptured Cerebral Aneurysm of the Anterior Circulation
 Original Articles * Division of Neurosurgery Department of Surgery Ruptured Cerebral Aneurysm of the Anterior Circulation Management and Microsurgical Treatment Ossama Al-Mefty, MD* ABSTRACT Based on the
Original Articles * Division of Neurosurgery Department of Surgery Ruptured Cerebral Aneurysm of the Anterior Circulation Management and Microsurgical Treatment Ossama Al-Mefty, MD* ABSTRACT Based on the
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
North Oaks Trauma Symposium Friday, November 3, 2017
 Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Subarachnoid Haemorrhage
 2011 Subarachnoid Haemorrhage Subarachnoid Haemorrhage This pamphlet will briefly describe what may happen to a person who has a subarachnoid haemorrhage (SAH). We would like to encourage you to read this
2011 Subarachnoid Haemorrhage Subarachnoid Haemorrhage This pamphlet will briefly describe what may happen to a person who has a subarachnoid haemorrhage (SAH). We would like to encourage you to read this
Anesthetic Considerations for Cerebrovascular Neurosurgery
 Anesthetic Considerations for Cerebrovascular Neurosurgery Ajith J. Thomas, MD Associate Professor of Neurosurgery BIDMC Brain Aneurysm Institute Mohamed M. Salem, MD Krishnan Ravindran MD Neurovascular
Anesthetic Considerations for Cerebrovascular Neurosurgery Ajith J. Thomas, MD Associate Professor of Neurosurgery BIDMC Brain Aneurysm Institute Mohamed M. Salem, MD Krishnan Ravindran MD Neurovascular
Stroke/TIA. Tom Bedwell
 Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Stroke/TIA Tom Bedwell tab1g11@soton.ac.uk The Plan Definitions Anatomy Recap Aetiology Pathology Syndromes Brocas / Wernickes Investigations Management Prevention & Prognosis TIAs Key Definitions Transient
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08)
") Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Thrombolysis for acute ischaemic stroke Rapid Assessment Protocol NORTHERN IRELAND Regional Protocol (Version 002 July 08) Patient Details Time of onset? Capillary Blood glucose 2.8-22.2 mmol/l? Blood
Stroke in adults with Sickle Cell Disease
 Stroke in adults with Sickle Cell Disease Dr Paul Holmes Consultant Neurologist Guy s and St Thomas Hospitals Stroke and SCD Children and adults with SCA (haemoglobin SS) have a high prevalence (4.01%)
Stroke in adults with Sickle Cell Disease Dr Paul Holmes Consultant Neurologist Guy s and St Thomas Hospitals Stroke and SCD Children and adults with SCA (haemoglobin SS) have a high prevalence (4.01%)
CEREBRAL ANEURYSM. Epidemiology. Number of Case per Year 12/15/2008. Wanarak Watcharasakailp M.D.
 Epidemiology CEREBRAL ANEURYSM Wanarak Watcharasakailp M.D. 5-10% of all stroke 6-7 /100,000 persons/yrs, 20/100,000 in Finland and Japan Female predominant Most in anterior circulation Female->ICA 36.8%
Epidemiology CEREBRAL ANEURYSM Wanarak Watcharasakailp M.D. 5-10% of all stroke 6-7 /100,000 persons/yrs, 20/100,000 in Finland and Japan Female predominant Most in anterior circulation Female->ICA 36.8%
Classification of Stroke. CNA Neuroscience Nursing Course: Cerebrovascular Disorders. Stroke in Canada
 CNA Neuroscience Nursing Course: Cerebrovascular Disorders Breeda O Farrell RN(EC), MScN, CNN(C) Nurse Practitioner Neurology University Hospital, London Health Science Centre London, ON Deb Bisnaire RN(EC),
CNA Neuroscience Nursing Course: Cerebrovascular Disorders Breeda O Farrell RN(EC), MScN, CNN(C) Nurse Practitioner Neurology University Hospital, London Health Science Centre London, ON Deb Bisnaire RN(EC),
TREATMENT OF INTRACRANIAL ANEURYSMS
 TREATMENT OF INTRACRANIAL ANEURYSMS Presented by: Dr Nilesh S. Kurwale Introduction Incidence of aneurysm difficult to estimate Prevalence 0.2-7.9 % Half the aneurysms ruptures 2% present during childhood
TREATMENT OF INTRACRANIAL ANEURYSMS Presented by: Dr Nilesh S. Kurwale Introduction Incidence of aneurysm difficult to estimate Prevalence 0.2-7.9 % Half the aneurysms ruptures 2% present during childhood
7/18/2018. Cerebral Vasospasm: Current and Emerging Therapies. Disclosures. Objectives
 Cerebral : Current and Emerging Therapies Chad W. Washington MS, MD, MPHS Assistant Professor Department of Neurosurgery Disclosures None Objectives Brief Overview How we got here Review of Trials Meta-analysis
Cerebral : Current and Emerging Therapies Chad W. Washington MS, MD, MPHS Assistant Professor Department of Neurosurgery Disclosures None Objectives Brief Overview How we got here Review of Trials Meta-analysis
What You Should Know About Cerebral Aneurysms
 American Society of Neuroradiology American Society of Interventional & Therapeutic Neuroradiology What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Intervention Committee
American Society of Neuroradiology American Society of Interventional & Therapeutic Neuroradiology What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Intervention Committee
Cerebrovascular Disease
 Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
An Introduction to Imaging the Brain. Dr Amy Davis
 An Introduction to Imaging the Brain Dr Amy Davis Common reasons for imaging: Clinical scenarios: - Trauma (NICE guidelines) - Stroke - Tumours - Seizure - Neurological degeneration memory, motor dysfunction,
An Introduction to Imaging the Brain Dr Amy Davis Common reasons for imaging: Clinical scenarios: - Trauma (NICE guidelines) - Stroke - Tumours - Seizure - Neurological degeneration memory, motor dysfunction,
TURN IT UP TO 11: LP IN THE DIAGNOSIS OF SAH. Matt Greer February 10 th, 2015
 TURN IT UP TO 11: LP IN THE DIAGNOSIS OF SAH Matt Greer February 10 th, 2015 IN CASE YOU MISSED THE REFERENCE HEADACHES IN THE ED Account for approximately 2% of ED visits 1% of these are due to SAH Approximately
TURN IT UP TO 11: LP IN THE DIAGNOSIS OF SAH Matt Greer February 10 th, 2015 IN CASE YOU MISSED THE REFERENCE HEADACHES IN THE ED Account for approximately 2% of ED visits 1% of these are due to SAH Approximately
excellence in care Procedure Neuroprotection For Review Aug 2015
 Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
2. Subarachnoid Hemorrhage
 Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Causes: 2. Subarachnoid Hemorrhage A. Saccular (berry) aneurysm - Is the most frequent cause of clinically significant subarachnoid hemorrhage is rupture of a saccular (berry) aneurysm. B. Vascular malformation
Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship
 Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship CLINICAL PROBLEMS IN VASCULAR SURGERY 1. ABDOMINAL AORTIC ANEURYSM A 70 year old man presents in the emergency department with
Learning Objectives for Rotations in Vascular Surgery Year 3 Basic Clerkship CLINICAL PROBLEMS IN VASCULAR SURGERY 1. ABDOMINAL AORTIC ANEURYSM A 70 year old man presents in the emergency department with
Operation Stroke. How to Reduce the Risk of Stroke Complications
 Operation Stroke How to Reduce the Risk of Stroke Complications Objectives Focus on Acute Stroke as an active disease Discuss the most common stroke complications Describe how first 72 hours sets the stage
Operation Stroke How to Reduce the Risk of Stroke Complications Objectives Focus on Acute Stroke as an active disease Discuss the most common stroke complications Describe how first 72 hours sets the stage
ATTENDING PHYSICIAN'S STATEMENT STROKE / BRAIN ANEURYSM SURGERY OR CEREBRAL SHUNT INSERTION / CAROTID ARTERY SURGERY
 ATTENDING PHYSICIAN'S STATEMENT STROKE / BRAIN ANEURYSM SURGERY OR CEREBRAL SHUNT INSERTION / CAROTID ARTERY SURGERY A) Patient s Particulars Name of Patient Gender NRIC/FIN or Passport No. Date of Birth
ATTENDING PHYSICIAN'S STATEMENT STROKE / BRAIN ANEURYSM SURGERY OR CEREBRAL SHUNT INSERTION / CAROTID ARTERY SURGERY A) Patient s Particulars Name of Patient Gender NRIC/FIN or Passport No. Date of Birth
LOSS OF CONSCIOUSNESS & ASSESSMENT. Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT
 LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
LOSS OF CONSCIOUSNESS & ASSESSMENT Sheba Medical Center Acute Medicine Department MATTHEW WRIGHT OUTLINE Causes Head Injury Clinical Features Complications Rapid Assessment Glasgow Coma Scale Classification
Endovascular Treatment of Cerebral Arteriovenous Malformations. Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh
 Endovascular Treatment of Cerebral Arteriovenous Malformations Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh Stroke Vascular Malformations of the Brain Epidemiology: - Incidence: 0.1%,
Endovascular Treatment of Cerebral Arteriovenous Malformations Bs. Nguyễn Ngọc Pi Doanh- Bs Đặng Ngọc Dũng Khoa Ngoại Thần Kinh Stroke Vascular Malformations of the Brain Epidemiology: - Incidence: 0.1%,
Ventriculo-Peritoneal/ Lumbo-Peritoneal Shunts
 Ventriculo-Peritoneal/ Lumbo-Peritoneal Shunts Exceptional healthcare, personally delivered Ventriculo-Peritoneal/ Lumbo-Peritoneal Shunts What is hydrocephalus? Hydrocephalus is the build up of an excess
Ventriculo-Peritoneal/ Lumbo-Peritoneal Shunts Exceptional healthcare, personally delivered Ventriculo-Peritoneal/ Lumbo-Peritoneal Shunts What is hydrocephalus? Hydrocephalus is the build up of an excess
Impact of a Protocol for Acute Antifibrinolytic Therapy on Aneurysm Rebleeding After Subarachnoid Hemorrhage
 Impact of a Protocol for Acute Antifibrinolytic Therapy on Aneurysm Rebleeding After Subarachnoid Hemorrhage Robert M. Starke, BA; Grace H. Kim, MD; Andres Fernandez, MD; Ricardo J. Komotar, MD; Zachary
Impact of a Protocol for Acute Antifibrinolytic Therapy on Aneurysm Rebleeding After Subarachnoid Hemorrhage Robert M. Starke, BA; Grace H. Kim, MD; Andres Fernandez, MD; Ricardo J. Komotar, MD; Zachary
Concurrent Subarachnoid Hemorrhage and Acute Myocardial Infarction: A Case Report
 Concurrent subarachnoid hemorrhage and AMI 155 Concurrent Subarachnoid Hemorrhage and Acute Myocardial Infarction: A Case Report Chen-Chuan Cheng 1, Wen-Shiann Wu 1, Chun-Yen Chiang 1, Tsuei-Yuang Huang
Concurrent subarachnoid hemorrhage and AMI 155 Concurrent Subarachnoid Hemorrhage and Acute Myocardial Infarction: A Case Report Chen-Chuan Cheng 1, Wen-Shiann Wu 1, Chun-Yen Chiang 1, Tsuei-Yuang Huang
WHI Form Report of Cardiovascular Outcome Ver (For items 1-11, each question specifies mark one or mark all that apply.
 WHI Form - Report of Cardiovascular Outcome Ver. 6. COMMENTS To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: OMB# 095-044 Exp: 4/06 -Affix label here- Clinical Center/ID:
WHI Form - Report of Cardiovascular Outcome Ver. 6. COMMENTS To be completed by Physician Adjudicator Date Completed: - - (M/D/Y) Adjudicator Code: OMB# 095-044 Exp: 4/06 -Affix label here- Clinical Center/ID:
Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]
![Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]](/thumbs/87/96512765.jpg "Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical]") Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
Children s Acute Transport Service Clinical Guidelines Acute Neurosurgical Emergency Transfer [see also CATS SOP neurosurgical] Document Control Information Author D Lutman Author Position Head of Clinical
HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM
 REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
REVIEW DATE REVIEWER'S ID HEART AND SOUL STUDY OUTCOME EVENT - MORBIDITY REVIEW FORM : DISCHARGE DATE: RECORDS FROM: Hospitalization ER Please check all that may apply: Myocardial Infarction Pages 2, 3,
The "filling defect" sign helps localise the site of intracranial aneurysm rupture on an unenhanced CT
 The "filling defect" sign helps localise the site of intracranial aneurysm rupture on an unenhanced CT Poster No.: C-3380 Congress: ECR 2010 Type: Topic: Authors: Keywords: DOI: Educational Exhibit Neuro
The "filling defect" sign helps localise the site of intracranial aneurysm rupture on an unenhanced CT Poster No.: C-3380 Congress: ECR 2010 Type: Topic: Authors: Keywords: DOI: Educational Exhibit Neuro
Extracranial to intracranial bypass for intracranial atherosclerosis
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Extracranial to intracranial bypass for intracranial atherosclerosis In cerebrovascular disease, blood vessels
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Interventional procedure consultation document Extracranial to intracranial bypass for intracranial atherosclerosis In cerebrovascular disease, blood vessels
Neuro Quiz 29 Transcranial Doppler Monitoring
 Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Overview of imaging modalities for cerebral aneurysms
 Overview of imaging modalities for cerebral aneurysms Soroush Zaghi BIDMC PCE: Radiology August 2008 (Images from BIDMC, PACS.) Our Patient: Presentation Our patient is a 57 y/o woman who reports blowing
Overview of imaging modalities for cerebral aneurysms Soroush Zaghi BIDMC PCE: Radiology August 2008 (Images from BIDMC, PACS.) Our Patient: Presentation Our patient is a 57 y/o woman who reports blowing
The Worst Headache of My Life Hemorrhagic Stroke
 The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
PARA210 SUMMARY Hyperglycaemia (DKA & HHS) Brain & Nervous System Anatomy & Physiology Degenerative Neurological Disorders
 Brain & Nervous System Anatomy & Physiology Degenerative Neurological Disorders") PARA210 SUMMARY Page Topic 01-03 Diabetes Mellitus 04-05 Hyperglycaemia (DKA & HHS) 06-13 Toxicology 14-18 12 Lead ECG 19-21 Brain & Nervous System Anatomy & Physiology 22-24 Degenerative Neurological
PARA210 SUMMARY Page Topic 01-03 Diabetes Mellitus 04-05 Hyperglycaemia (DKA & HHS) 06-13 Toxicology 14-18 12 Lead ECG 19-21 Brain & Nervous System Anatomy & Physiology 22-24 Degenerative Neurological
はじめに 対象と方法 39: , 2017 SAH 183 WFNS
 39:107 原 著 39: 107 112, 2017 1 2 1 1 1 1 要旨 SAH 2010 1 2013 12 SAH 253 183 64 70 WFNS I III 72.7 Fisher CT 3 86.3 19.9 16.6 GR MD 73.2 73.1 80 WFNS Key words: subarachnoid hemorrhage, prognosis, rate of
39:107 原 著 39: 107 112, 2017 1 2 1 1 1 1 要旨 SAH 2010 1 2013 12 SAH 253 183 64 70 WFNS I III 72.7 Fisher CT 3 86.3 19.9 16.6 GR MD 73.2 73.1 80 WFNS Key words: subarachnoid hemorrhage, prognosis, rate of
Michael Horowitz, MD Pittsburgh, PA
 Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Major Vascular Anaesthesia where is the challenge. Dr B Brandner Consultant in Anaesthesia and Pain Management UCLH, London
 Major Vascular Anaesthesia where is the challenge Dr B Brandner Consultant in Anaesthesia and Pain Management UCLH, London Preoperative challenge Patient selection Patient optimisation Effective multidisciplinary
Major Vascular Anaesthesia where is the challenge Dr B Brandner Consultant in Anaesthesia and Pain Management UCLH, London Preoperative challenge Patient selection Patient optimisation Effective multidisciplinary
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Bleeding in the brain: haemorrhagic stroke
 Call the Stroke Helpline: 0303 3033 100 or email: info@stroke.org.uk Bleeding in the brain: haemorrhagic stroke Some strokes are due to bleeding in or around the brain, and are known as haemorrhagic strokes.
Call the Stroke Helpline: 0303 3033 100 or email: info@stroke.org.uk Bleeding in the brain: haemorrhagic stroke Some strokes are due to bleeding in or around the brain, and are known as haemorrhagic strokes.
Flow-diverting stents (in the Treatment of intracranial aneurysms)
") National Hospital for Neurology and Neurosurgery Flow-diverting stents (in the Treatment of intracranial aneurysms) Lysholm Department of Neuroradiology If you would like this document in another language
National Hospital for Neurology and Neurosurgery Flow-diverting stents (in the Treatment of intracranial aneurysms) Lysholm Department of Neuroradiology If you would like this document in another language
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage. By: Shifaa AlQa qa
 CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
CENTRAL NERVOUS SYSTEM TRAUMA and Subarachnoid Hemorrhage By: Shifaa AlQa qa Subarachnoid Hemorrhage Causes: Rupture of a saccular (berry) aneurysm Vascular malformation Trauma Hematologic disturbances
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Intracranial Hemorrhage. Objectives. What Do Need to Know?
 Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
Perioperative Management Of Extra-Ventricular Drains (EVD)
") Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
Perioperative Management Of Extra-Ventricular Drains (EVD) Dr. Vijay Tarnal MBBS, FRCA Clinical Assistant Professor Division of Neuroanesthesiology Division of Head & Neck Anesthesiology Michigan Medicine
R Adams Cowley Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland.
 R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
R Adams Cowley 1917 -- 1991 Founder of the R Adams Cowley Shock Trauma Center and Maryland EMS System in Baltimore, Maryland. ...That the primary purpose of medicine was to save lives, that every critically
Carotid Revascularization
 Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage
 Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University
Cronicon OPEN ACCESS EC PAEDIATRICS Case Report Brain AVM with Accompanying Venous Aneurysm with Intracerebral and Intraventricular Hemorrhage Dimitrios Panagopoulos* Neurosurgical Department, University