Current State of the Art
|
|
|
- Todd Dennis
- 5 years ago
- Views:
Transcription

1 SAH Current State of the Art Thomas C. Steineke, M.D., Ph.D. Director of Neurovascular Surgery NJ Neuroscience Institute JFK Medical Center
2 Introduction Signs and symptoms of a problem What are aneurysms Why are the bad? Because they rupture and cause Subarachnoid hemorrhage SAH is more a result or sign don t really treat it But do treat the cause And its sequelae

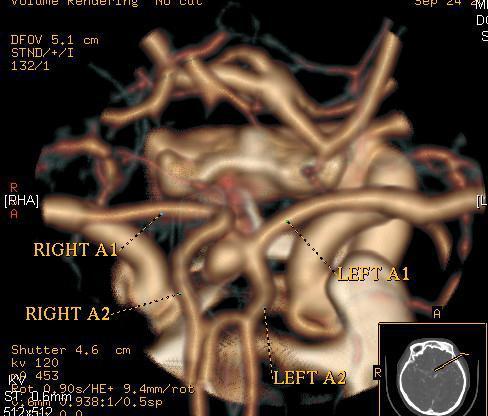
3 Cerebral vasculature

4 Big problem in small packages
5 Pathophysiology Weakness in the wall of an artery, typically at the branch point of a large intracerebral artery Classically thought of as a congenital weakness in the wall of an artery Current leading theory is repeated vascular injury Conditions with increased incidence of aneurysms Atherosclerosis Hypertension High flow vascular lesions Moya Moya Polycystic Kidney Disease Fibromuscular Dysplasia Etc
 Focal neurological symptoms (weakness, numbness, cranial")
6 Signs and Symptoms of a Problem Worst headache of a patient s life Neck stiffness Nausea Vomiting Encephalopathy (confusion) Focal neurological symptoms (weakness, numbness, cranial neuropathies
7 Work-up & Diagnosis Head CT If positive CTA or cerebral angiogram Lumbar Puncture Angio negative SAH Benign perimesencephalic hemorrhage Localilzed vasospasm

8 Subarachnoid Hemorrhage
9 So is this bad?? 10% die before reaching medical attention 50% die within the first month Of the survivors, half will have a permanent neurological deficit
10 What do they look like?? 80 to 90% with signs and symptoms of SAH Worst headache of one s life Meningeal signs Lethargy Nausea/vomitting LOC, altered MS, coma Expanding aneurysm Third nerve palsy (posterior communicating artery aneurysm) Decreased vision (peri-ophthalmic aneurysm)
11 Now What?? SAH considered neurosurgical emergency Without treatment 25 to 50% of patients will have a second rupture with a mortality rate of 85% Immediate treatment Definitive Treatment options Open surgery, and occlusion of the aneurysm Endovascular embolization via cerebral angiography
12 First base Stabilize the patient (not all patients are created equal Treatment really depends on the condition of the patient Hunt & Hess SAH grade is a helpful descriptor and prognosticator
13 Be a doctor History - Get the story Did the patient pass out and fall or fall and pass out Did the patient pass out and run their car into the telephone pole or did they hit the pole and pass out? Premorbid neurological condition Co-morbidities CAD, COPD, CVD, DM etc Medications/Allergies (anticoagulation? Anti-platelett? Metformin?) Family Hx anyone else have an aneurysm?? Any sudden deaths due to brain hemorrhage? Social Hx hx of recreational pharmacology?? Hunt & Hess Grade
14 Hunt & Hess SAH Grade DESCRIPTION GRADE Asymptomatic, mild headache, slight nuchal rigidity 1 Moderate to severe headache, nuchal rigidity, no neurologic deficit other than cranial nerve palsy 2 Drowsiness / confusion, mild focal neurologic deficit 3 Stupor, moderate-severe hemiparesis 4 Coma, decerebrate posturing 5 Some authorities will have a 1A or 2A to indicate grade plus a cranial nerve deficit
15 Rounding 1 st going to 2 nd Depends on grade, CT scan and comordities ICP management HOB > 30 o Mild hyperventilation if intubated EVD if hydrocephalus Seizure prophylaxis Start Nimodipine NS + 20KCl at /hr BP management (generally s) EKG cardiac stun CXR TCDs, DVT prophylaxis, PUD prophylaxis, routine labs
16 Getting to 2 nd base Keep calm! (recommended for both physician and patient!) Try to avoid stimulation Anxiolytics Analgesics May also use steroids that help with headache and nuchal rigidity Trying to prevent
17 Re-rupture! Very high morbidity and mortality rate Incidence is 4% in first 24hrs and about 15-20% in first 7 days Antifibrinolytic therapy Tranexamic acid Reduces rebleed rates but at a cost increased incidence of vasospasm and ischemic events and increased incidence of hydrocephalus therefore use is discouraged. Best prevention is early definitive treatment (the best defense is a strong offense )

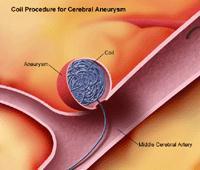
18 Clip vs Coil
19 Coiling Pros less invasive, typically shorter surgeries, can treat aneurysms difficult to surgically clip (basilar tip), less recovery following the procedure Cons aneurysm is more likely to recur and recanalize can occur many years after treatment. Intraprocedural rupture. Not able to remove the blood or substantial hemorrhage


20 Clipping Pros More durable, can treat wide necked aneurysms, less likely to have a residual and recurrence Cons more trauma due to the operation, higher infection rate, more stressful to the body, higher initial complication rate.
21 So what s best?? International Subarachnoid Aneurysm Trial (ISAT), a prospective, randomized trial comparing surgery (craniotomy for clipping) to endovascular therapy (coiling) in the treatment of ruptured intracranial aneurysms Conclusions Craniotomy and clipping had a 30.3 chance of poor outcome at 1 year Coiling had a 23.7 chance of a poor outcome at 1 year Therefore a relative risk reduction of 6.9%
22 Here come the critics Patients case reviewed by a neurovascular team 9,559 with ruptured aneurysms were reviewed for the study Only 2,143 were randomized, namely the neurovascular team felt that either clipping or coiling would be an appropriate treatment 7,416 of patients did not get randomized, the majority of which underwent surgery
 Post op monitoring")
23 Now what?? Once the aneurysm is definitively clipped (or coiled) Post op monitoring Vasospasm ICP or hydrocephalus Seizures Cardiac Pulmonary Renal function
24 Main culprit vasospasm Pathophysiology (theory ) breakdown product of the blood cause irritation in the arterial smooth muscle causing irritability and proliferation/hypertrophy Peak incidence is post bleed day 6-8 Rarely seen before day 3 or after day 17 Most significant cause of morbidity and mortality in patients that survive initial hemorrhage and are stabilized (mortality rate of 7-10%)
25 Diagnosis Clinically In patient s who have a clinical exam Careful monitoring of neurological status Monitoring for development of a new focal deficits Overall decrease in sensorium Intubated patients or those in coma No clinical exam, therefore must depend on diagnostic tools

26 Diagnostic Tools Transcranial Doppler studies Evaluates velocity of blood flow in main arteries of the cerebral vasculature Compared to extracranial ICA as a ratio to correct for hyperdynamic flow CT perfusion studies Cerebral Angiography
27 Treatment Nimodipine Avoidance of hyperventilation Keep normocarbic May need for ICP control however must carefully balance needs/risks Gold standard. Hypertension Hypervolumia Hemodilution Triple H Therapy
28 Need to get physical?? Generally, in patients with subtle initial deficits HHH, generally increasing SBP Typically the deficit will reverse Pharmacology To this point disappointing Some evidence to the benefit of IV Mg If medical therapy fails off to the angio suite
29 Getting tough Intra arterial pharmacological treatment Papavarin Verapamil Often temporal relief of the spasm Needs multiple infusions Angioplasty Gentle dilation of the arterial wall But must push it so that the smooth muscle is torn Therefore permanent treatment of vasospasm But there is risk of arterial rupture
30 On the Horizon General trend to the severity of vasospam the more blood and the worse the clinical exam, the higher risk of vasospasm For this reason, there have been several ideas regarding the reduction of the SAH Some good ideas And of course some not so good

31
32 Promising treatments Implants Nicardipine prolonged release implants Placed intraoperatively into the cisterns Medication leaches into the CSF at the site of the vasospasm had has shown promise Clazosentan selective endothelin IA receptor antagonist reduces frequency and severity of vasospasm Statins 3 small studies have shown benefit
33 And its finally over The take home points SAH is bad very bad To clip or coil not a foregone conclusion Decision best made by a team with expertise in both treatment options The Aftermath Vasospasm major source of morbidity and mortality Monitored through exam, TCDs, perfusion studies Symptomatic vasospam, treated with Nimodipine, HHH, angiography
34 Quiz Questions T or F All ruptured aneurysm are best treated with coiling? What is the most common cause of neurologic morbidity and mortality in a patient who has suffered a SAH and has had definitive treatment of the ruptured aneurysm? T or F In a randomized, double blinded study (funded by Obamacare), snail therapy has been shown to reduce the incidence and severity of vasospasm following aneurysmal SAH, and is quite cost effective
35
TCD AND VASOSPASM SAH
 CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Subarachnoid Hemorrhage (SAH) Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.
 Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.") Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest
Sub-arachnoid haemorrhage
 Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM. Vikram Jadhav MD, PhD. 04/12/2018 CentraCare Health St.
 ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
4/10/2018. The Surgical Treatment of Cerebral Aneurysms. Aneurysm Locations. Aneurysmal Subarachnoid Hemorrhage. Jerone Kennedy, M.D.
 The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Subarachnoid Hemorrhage and Brain Aneurysm
 Subarachnoid Hemorrhage and Brain Aneurysm DIN Department of Interventional Neurology What is SAH? Subarachnoid Haemorrhage is the sudden leaking (haemorrhage) of blood from the blood vessels of brain.
Subarachnoid Hemorrhage and Brain Aneurysm DIN Department of Interventional Neurology What is SAH? Subarachnoid Haemorrhage is the sudden leaking (haemorrhage) of blood from the blood vessels of brain.
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications
 Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease
 Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Neurosurgical decision making in structural lesions causing stroke. Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery)
") Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage
 Romanian Neurosurgery (2016) XXX 4: 461 466 461 DOI: 10.1515/romneu-2016-0074 Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage A. Chiriac, Georgiana Ion*,
Romanian Neurosurgery (2016) XXX 4: 461 466 461 DOI: 10.1515/romneu-2016-0074 Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage A. Chiriac, Georgiana Ion*,
Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici
 Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici Nino Stocchetti Milan University Neuroscience ICU Ospedale Policlinico IRCCS Milano stocchet@policlinico.mi.it Macdonald RL et
Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici Nino Stocchetti Milan University Neuroscience ICU Ospedale Policlinico IRCCS Milano stocchet@policlinico.mi.it Macdonald RL et
What You Should Know About Cerebral Aneurysms
 American Society of Neuroradiology American Society of Interventional & Therapeutic Neuroradiology What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Intervention Committee
American Society of Neuroradiology American Society of Interventional & Therapeutic Neuroradiology What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Intervention Committee
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Subarachnoid Bleeds. Under the Spider via deepthought 1 / 22
 Subarachnoid Bleeds Under the Spider via deepthought 1 / 22 SAH: symptoms worst headache of my life Sudden-onset Severe w max intensity in seconds = thunderclap Sentinel headache in ~10-40% in aneurysmal
Subarachnoid Bleeds Under the Spider via deepthought 1 / 22 SAH: symptoms worst headache of my life Sudden-onset Severe w max intensity in seconds = thunderclap Sentinel headache in ~10-40% in aneurysmal
Update in Diagnosis and Management of Intracranial Aneurysms for Primary Health Care Providers November 15, 2012 Boston, Massachusetts
 Update in Diagnosis and Management of Intracranial Aneurysms for Primary Health Care Providers November 15, 2012 Boston, Massachusetts Educational Partner: Session 1: Update in Diagnosis and Management
Update in Diagnosis and Management of Intracranial Aneurysms for Primary Health Care Providers November 15, 2012 Boston, Massachusetts Educational Partner: Session 1: Update in Diagnosis and Management
Multi-modality management of intracranial aneurysms
 Multi-modality management of intracranial aneurysms Christopher Koebbe, Maj, USAF, MC Staff Neurosurgeon San Antonio Military Medical Consortium Clinical Assistant Professor Department of Neurological
Multi-modality management of intracranial aneurysms Christopher Koebbe, Maj, USAF, MC Staff Neurosurgeon San Antonio Military Medical Consortium Clinical Assistant Professor Department of Neurological
SAH READMISSIONS TO NCCU
 SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
The Endovascular Treatment of Cerebral Aneurysms
 The Endovascular Treatment of Cerebral Aneurysms George P. Teitelbaum, M.D., FSIR Regional Director, Neurointerventional Surgery Providence, California Types of Stroke and Their Causes Ischemic (87%):
The Endovascular Treatment of Cerebral Aneurysms George P. Teitelbaum, M.D., FSIR Regional Director, Neurointerventional Surgery Providence, California Types of Stroke and Their Causes Ischemic (87%):
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
7/18/2018. Cerebral Vasospasm: Current and Emerging Therapies. Disclosures. Objectives
 Cerebral : Current and Emerging Therapies Chad W. Washington MS, MD, MPHS Assistant Professor Department of Neurosurgery Disclosures None Objectives Brief Overview How we got here Review of Trials Meta-analysis
Cerebral : Current and Emerging Therapies Chad W. Washington MS, MD, MPHS Assistant Professor Department of Neurosurgery Disclosures None Objectives Brief Overview How we got here Review of Trials Meta-analysis
Neurosurgical Management of Aneurysmal Subarachnoid Hemorrhage
 Neurosurgical Management of Aneurysmal Subarachnoid Hemorrhage PVHMC STROKE SYMPOSIUM 2018 10/27/18 Srinath Samudrala MD, FACS Epidemiology of Subarachnoid Hemorrhage (SAH) Less than 10% of all stroke
Neurosurgical Management of Aneurysmal Subarachnoid Hemorrhage PVHMC STROKE SYMPOSIUM 2018 10/27/18 Srinath Samudrala MD, FACS Epidemiology of Subarachnoid Hemorrhage (SAH) Less than 10% of all stroke
TREATMENT OF INTRACRANIAL ANEURYSMS
 TREATMENT OF INTRACRANIAL ANEURYSMS Presented by: Dr Nilesh S. Kurwale Introduction Incidence of aneurysm difficult to estimate Prevalence 0.2-7.9 % Half the aneurysms ruptures 2% present during childhood
TREATMENT OF INTRACRANIAL ANEURYSMS Presented by: Dr Nilesh S. Kurwale Introduction Incidence of aneurysm difficult to estimate Prevalence 0.2-7.9 % Half the aneurysms ruptures 2% present during childhood
Monitoring of Regional Cerebral Blood Flow Using an Implanted Cerebral Thermal Perfusion Probe Archived Medical Policy
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
NIH Public Access Author Manuscript J Am Coll Radiol. Author manuscript; available in PMC 2013 June 24.
 NIH Public Access Author Manuscript Published in final edited form as: J Am Coll Radiol. 2010 January ; 7(1): 73 76. doi:10.1016/j.jacr.2009.06.015. Cerebral Aneurysms Janet C. Miller, DPhil, Joshua A.
NIH Public Access Author Manuscript Published in final edited form as: J Am Coll Radiol. 2010 January ; 7(1): 73 76. doi:10.1016/j.jacr.2009.06.015. Cerebral Aneurysms Janet C. Miller, DPhil, Joshua A.
Management of Cerebral Aneurysms in Polycystic Kidney Disease. Dr H Stockley Consultant Neuroradiologist Greater Manchester Neuroscience Centre
 Management of Cerebral Aneurysms in Polycystic Kidney Disease Dr H Stockley Consultant Neuroradiologist Greater Manchester Neuroscience Centre What is a cerebral aneurysm? Developmental degenerative arterial
Management of Cerebral Aneurysms in Polycystic Kidney Disease Dr H Stockley Consultant Neuroradiologist Greater Manchester Neuroscience Centre What is a cerebral aneurysm? Developmental degenerative arterial
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes
 and Non- Aneurysmal Causes") Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Management of the Endovascular Patient and Acute Emergencies in the Angio Suite
 Management of the Endovascular Patient and Acute Emergencies in the Angio Suite June 9, 2015 Bridget Cantrell, APN, CNP Endovascular Neurosurgery Advocate Medical Group No Disclosures The human brain is
Management of the Endovascular Patient and Acute Emergencies in the Angio Suite June 9, 2015 Bridget Cantrell, APN, CNP Endovascular Neurosurgery Advocate Medical Group No Disclosures The human brain is
Subarachnoid Hemorrhage & Vasospasm basic level
 Subarachnoid Hemorrhage & Vasospasm basic level Overview Subarachnoid hemorrhage (SAH) is a serious, lifethreatening type of stroke caused by bleeding into the space surrounding the brain. A stroke occurs
Subarachnoid Hemorrhage & Vasospasm basic level Overview Subarachnoid hemorrhage (SAH) is a serious, lifethreatening type of stroke caused by bleeding into the space surrounding the brain. A stroke occurs
Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part B. Objectives Epidemiology of asah Concept: What is a brain
Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part B. Objectives Epidemiology of asah Concept: What is a brain
Aneurysmal SAH Jenny Fox APN, CCRN, CNRN, ACNP-BC
 Epidemiology of asah Incidence 9.7 to 14.5 per 100,000 in the United States. About 30,000 yearly in North America. Aneurysmal SAH Jenny Fox APN, CCRN, CNRN, ACNP-BC Mean age of onset is 55 years. Most
Epidemiology of asah Incidence 9.7 to 14.5 per 100,000 in the United States. About 30,000 yearly in North America. Aneurysmal SAH Jenny Fox APN, CCRN, CNRN, ACNP-BC Mean age of onset is 55 years. Most
Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management
 0 0 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management The Department of Health and Social Care in England
0 0 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management The Department of Health and Social Care in England
Ruptured Cerebral Aneurysm of the Anterior Circulation
 Original Articles * Division of Neurosurgery Department of Surgery Ruptured Cerebral Aneurysm of the Anterior Circulation Management and Microsurgical Treatment Ossama Al-Mefty, MD* ABSTRACT Based on the
Original Articles * Division of Neurosurgery Department of Surgery Ruptured Cerebral Aneurysm of the Anterior Circulation Management and Microsurgical Treatment Ossama Al-Mefty, MD* ABSTRACT Based on the
Daniel A Capen MD Downey Orthopedic Group COMPLICATIONS IN CERVICAL AND LUMBAR SPINAL SURGERY
 Daniel A Capen MD Downey Orthopedic Group COMPLICATIONS IN CERVICAL AND LUMBAR SPINAL SURGERY Complications in Spinal Surgery Positioning Complications Approach Complications Procedure Complications Post-surgical
Daniel A Capen MD Downey Orthopedic Group COMPLICATIONS IN CERVICAL AND LUMBAR SPINAL SURGERY Complications in Spinal Surgery Positioning Complications Approach Complications Procedure Complications Post-surgical
Paul Gigante HMS IV Gillian Lieberman, MD. Sept Mr. T s T s Headache. Paul Gigante,, Harvard Medical School Year IV Gillian Lieberman, MD
 Sept 2005 Mr. T s T s Headache Paul Gigante,, Harvard Medical School Year IV Mr. T s T s Presentation 45 year-old welder complains of sudden severe headache and witnessed seizure with loss of consciousness
Sept 2005 Mr. T s T s Headache Paul Gigante,, Harvard Medical School Year IV Mr. T s T s Presentation 45 year-old welder complains of sudden severe headache and witnessed seizure with loss of consciousness
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Cerebral Aneurysms. U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health
 Cerebral Aneurysms U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health Cerebral Aneurysms What is a cerebral aneurysm? cerebral aneurysm (also known as an
Cerebral Aneurysms U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health Cerebral Aneurysms What is a cerebral aneurysm? cerebral aneurysm (also known as an
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO
 Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Carotid Artery Disease and What s Pertinent JOSEPH A PAULISIN DO Goal of treatment of carotid disease Identify those at risk of developing symptoms Prevent patients at risk from developing symptoms Prevent
Overview of imaging modalities for cerebral aneurysms
 Overview of imaging modalities for cerebral aneurysms Soroush Zaghi BIDMC PCE: Radiology August 2008 (Images from BIDMC, PACS.) Our Patient: Presentation Our patient is a 57 y/o woman who reports blowing
Overview of imaging modalities for cerebral aneurysms Soroush Zaghi BIDMC PCE: Radiology August 2008 (Images from BIDMC, PACS.) Our Patient: Presentation Our patient is a 57 y/o woman who reports blowing
lek Magdalena Puławska-Stalmach
 lek Magdalena Puławska-Stalmach tytuł pracy: Kliniczne i radiologiczne aspekty tętniaków wewnątrzczaszkowych a wybór metody leczenia Summary An aneurysm is a localized, abnormal distended lumen of the
lek Magdalena Puławska-Stalmach tytuł pracy: Kliniczne i radiologiczne aspekty tętniaków wewnątrzczaszkowych a wybór metody leczenia Summary An aneurysm is a localized, abnormal distended lumen of the
North Oaks Trauma Symposium Friday, November 3, 2017
 Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
Traumatic Intracranial Hemorrhage Aaron C. Sigler, DO, MS Neurosurgery Tulane Neurosciences None Disclosures Overview Anatomy Epidural hematoma Subdural hematoma Cerebral contusions Outline Traumatic ICH
TRANSCRANIAL DOPPLER ULTRASOUND INTRODUCTION TO TCD INTERPRETATION
 TRANSCRANIAL DOPPLER ULTRASOUND INTRODUCTION TO TCD INTERPRETATION ---Rune Aaslid First TCD Publication 1982 WHAT IS TCD? Uses 2 MHz pulsed Doppler ultrasound Passes through cranial windows Provides information
TRANSCRANIAL DOPPLER ULTRASOUND INTRODUCTION TO TCD INTERPRETATION ---Rune Aaslid First TCD Publication 1982 WHAT IS TCD? Uses 2 MHz pulsed Doppler ultrasound Passes through cranial windows Provides information
COMPREHENSIVE SUMMARY OF INSTOR REPORTS
 COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
COMPREHENSIVE SUMMARY OF INSTOR REPORTS Please note that the following chart provides a sampling of INSTOR reports to differentiate this registry s capabilities as a process improvement system. This list
Raw and Quantitative EEG for Identification of Ischemia
 Raw and Quantitative EEG for Identification of Ischemia Susan T. Herman, MD Assistant Professor of Neurology Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Disclosures None relevant
Raw and Quantitative EEG for Identification of Ischemia Susan T. Herman, MD Assistant Professor of Neurology Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Disclosures None relevant
Small UIAs, <7 mm in diameter, uncommonly cause aneurysmal symptoms and are the most frequently detected incidentally.
 Research grant from Stryker Neurovascular Research grant from Covidien/ Medtronic Consultant and proctor for Stryker Neurovascular Consultant and proctor for Covidien/ Medtronic Consultant for Codman Neurovascular
Research grant from Stryker Neurovascular Research grant from Covidien/ Medtronic Consultant and proctor for Stryker Neurovascular Consultant and proctor for Covidien/ Medtronic Consultant for Codman Neurovascular
(aneurysmal subarachnoid hemorrhage, 17%~60% :SAH. ,asah , 22%~49% : Willis. :1927 Moniz ;(3) 2. ischemic neurological deficit,dind) SAH) SAH ;(6)
 2. ischemic neurological deficit,dind) SAH) SAH ;(6)") ,, 2. : ;,, :(1), (delayed ;(2) ischemic neurological deficit,dind) ;(3) 2. :SAH ;(4) 5-10 10 HT -1-1 ;(5), 10 SAH ;(6) - - 27%~50%, ( cerebral vasospasm ) Glasgow (Glasgow Coma Scale,GCS), [1],, (aneurysmal
,, 2. : ;,, :(1), (delayed ;(2) ischemic neurological deficit,dind) ;(3) 2. :SAH ;(4) 5-10 10 HT -1-1 ;(5), 10 SAH ;(6) - - 27%~50%, ( cerebral vasospasm ) Glasgow (Glasgow Coma Scale,GCS), [1],, (aneurysmal
CEREBRAL ANEURYSM. Epidemiology. Number of Case per Year 12/15/2008. Wanarak Watcharasakailp M.D.
 Epidemiology CEREBRAL ANEURYSM Wanarak Watcharasakailp M.D. 5-10% of all stroke 6-7 /100,000 persons/yrs, 20/100,000 in Finland and Japan Female predominant Most in anterior circulation Female->ICA 36.8%
Epidemiology CEREBRAL ANEURYSM Wanarak Watcharasakailp M.D. 5-10% of all stroke 6-7 /100,000 persons/yrs, 20/100,000 in Finland and Japan Female predominant Most in anterior circulation Female->ICA 36.8%
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Risk Management in an Office Setting: Who are we sending home?
 Risk Management in an Office Setting: Who are we sending home? October 1, 2016 Niagara Falls, NY The threat of litigation following a misdiagnosis or improper treatment presents a challenge to healthcare
Risk Management in an Office Setting: Who are we sending home? October 1, 2016 Niagara Falls, NY The threat of litigation following a misdiagnosis or improper treatment presents a challenge to healthcare
Interventions in the Management of Acute Stroke. Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital
 Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
Interventions in the Management of Acute Stroke Dr Md Shafiqul Islam Associate Professor Neurosurgery Dhaka Medical College Hospital Acute stroke intervention Number of stroke patients increasing day by
Coil Embolization for Intracranial Aneurysms
 Ontario Health Technology Assessment Series 2006; Vol. 6, No. 1 Coil Embolization for Intracranial Aneurysms An Evidence-Based Analysis January 2006 Medical Advisory Secretariat Ministry of Health and
Ontario Health Technology Assessment Series 2006; Vol. 6, No. 1 Coil Embolization for Intracranial Aneurysms An Evidence-Based Analysis January 2006 Medical Advisory Secretariat Ministry of Health and
Neuro Quiz 29 Transcranial Doppler Monitoring
 Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Verghese Cherian, MD, FFARCSI Penn State Hershey Medical Center, Hershey Quiz Team Shobana Rajan, M.D Suneeta Gollapudy, M.D Angele Marie Theard, M.D Neuro Quiz 29 Transcranial Doppler Monitoring This
Case Report 1. CTA head. (c) Tele3D Advantage, LLC
 Tele3D Advantage, LLC") Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
Case Report 1 CTA head 1 History 82 YEAR OLD woman with signs and symptoms of increased intra cranial pressure in setting of SAH. CT Brain was performed followed by CT Angiography of head. 2 CT brain Extensive
Management of Acute Ischemic Stroke. Learning Objec=ves. What is a Stroke? Jen Simpson Neurohospitalist
 Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
Management of Acute Ischemic Stroke Jen Simpson Neurohospitalist Learning Objec=ves Iden=fy signs/symptoms of stroke Recognize pa=ents who may be eligible for treatment of acute stroke What is a Stroke?
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Michael Horowitz, MD Pittsburgh, PA
 Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Michael Horowitz, MD Pittsburgh, PA Introduction Cervical Artery Dissection occurs by a rupture within the arterial wall leading to an intra-mural Hematoma. A possible consequence is an acute occlusion
Recombinant Factor VIIa for Intracerebral Hemorrhage
 Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Recombinant Factor VIIa for Intracerebral Hemorrhage January 24, 2006 Justin Lee Pharmacy Resident University Health Network Outline 1. Introduction to patient case 2. Overview of intracerebral hemorrhage
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Shawke A. Soueidan, MD. Riverside Neurology & Sleep Specialists
 Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
Shawke A. Soueidan, MD Riverside Neurology & Sleep Specialists 757-221-0110 Epidemiology of stroke 2018 Affects nearly 800,000 people in the US annually Approximately 600000 first-ever strokes and 185000
NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM
 NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM Chairperson Professor Dr Zamzuri Idris Head of Department Members Associate Professor Dato Dr
NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM Chairperson Professor Dr Zamzuri Idris Head of Department Members Associate Professor Dato Dr
An Introduc+on to Stroke
 An Introduc+on to Stroke Elizabeth Huntoon MS, MD Assistant Professor Department of Physical Medicine and Rehabilita>on Vanderbilt University School of Medicine Defini+on Sudden focal neurologic deficit
An Introduc+on to Stroke Elizabeth Huntoon MS, MD Assistant Professor Department of Physical Medicine and Rehabilita>on Vanderbilt University School of Medicine Defini+on Sudden focal neurologic deficit
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for
 Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Post-op Carotid Complications A Nursing Perspective of What to Watch Out for By Kariss Peterson, ARNP Swedish Medical Center Inpatient Neurology Team 1 Post-op Carotid Management Objectives Review the
Disclosures. Take Home Points 9/6/2014. Endovascular Treatment of Aneurysms and Pseudoaneurysms
 Endovascular Treatment of Aneurysms and Pseudoaneurysms UCSF Stroke and Aneurysm Update CME Saturday September 6, 2014 Steven W. Hetts, MD Associate Professor of Radiology Interventional Neuroradiology
Endovascular Treatment of Aneurysms and Pseudoaneurysms UCSF Stroke and Aneurysm Update CME Saturday September 6, 2014 Steven W. Hetts, MD Associate Professor of Radiology Interventional Neuroradiology
From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council
 American Society of Neuroradiology What Is a Stroke? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall T. Higashida, M.D., Chair
American Society of Neuroradiology What Is a Stroke? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall T. Higashida, M.D., Chair
Comparison of Five Major Recent Endovascular Treatment Trials
 Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
Comparison of Five Major Recent Endovascular Treatment Trials Sample size 500 # sites 70 (100 planned) 316 (500 planned) 196 (833 estimated) 206 (690 planned) 16 10 22 39 4 Treatment contrasts Baseline
THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F.
 THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F. ISHFAQ ZEENAT QURESHI STROKE INSTITUTE AND UNIVERSITY OF TENNESSEE,
THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F. ISHFAQ ZEENAT QURESHI STROKE INSTITUTE AND UNIVERSITY OF TENNESSEE,
Isolated Cranial Nerve-III Palsy Secondary to Perimesencephalic Subarachnoid Hemorrhage
 Lehigh Valley Health Network LVHN Scholarly Works Department of Medicine Isolated Cranial Nerve-III Palsy Secondary to Perimesencephalic Subarachnoid Hemorrhage Hussam A. Yacoub MD Lehigh Valley Health
Lehigh Valley Health Network LVHN Scholarly Works Department of Medicine Isolated Cranial Nerve-III Palsy Secondary to Perimesencephalic Subarachnoid Hemorrhage Hussam A. Yacoub MD Lehigh Valley Health
Overview INTRODUCTION 3/15/2018. Headache Emergencies. Other way to differentiate between them? Is there an easy way to differentiate between them?
 Overview Headache Emergencies Primary versus Secondary headache disorder Red flags 4 cases of unusual headache emergencies Disclaimer: we will not talk about brain bleed as patients usually go the ED.
Overview Headache Emergencies Primary versus Secondary headache disorder Red flags 4 cases of unusual headache emergencies Disclaimer: we will not talk about brain bleed as patients usually go the ED.
Carotid Revascularization
 Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
Options for Carotid Disease Carotid Revascularization Wayne Causey, MD 2 nd Year Vascular Surgery Fellow Best medical therapy, Carotid Endarterectomy, and Carotid Stenting Who benefits from best medical
MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes
 MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes Stroke is the third leading cause of death and the leading cause of adult disability in the
MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes Stroke is the third leading cause of death and the leading cause of adult disability in the
Aneurysmal subarachnoid haemorrhage and the anaesthetist
 British Journal of Anaesthesia 99 (1): 102 18 (2007) doi:10.1093/bja/aem119 Advance Access publication May 23, 2007 Aneurysmal subarachnoid haemorrhage and the anaesthetist H.-J. Priebe* Department of
British Journal of Anaesthesia 99 (1): 102 18 (2007) doi:10.1093/bja/aem119 Advance Access publication May 23, 2007 Aneurysmal subarachnoid haemorrhage and the anaesthetist H.-J. Priebe* Department of
Traumatic Brain Injuries
 Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
Traumatic Brain Injuries Scott P. Sherry, MS, PA-C, FCCM Assistant Professor Department of Surgery Division of Trauma, Critical Care and Acute Care Surgery DISCLOSURES Nothing to disclose Discussion of
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Age-Associated Vasospasm in Aneurysmal Subarachnoid Hemorrhage
 Age-Associated Vasospasm in Aneurysmal Subarachnoid Hemorrhage Sushant P. Kale, MD, MPH,* Randall C. Edgell, MD,* Amer Alshekhlee, MD,* Afshin Borhani Haghighi, MD,* Justin Sweeny, MD, Jason Felton, MD,
Age-Associated Vasospasm in Aneurysmal Subarachnoid Hemorrhage Sushant P. Kale, MD, MPH,* Randall C. Edgell, MD,* Amer Alshekhlee, MD,* Afshin Borhani Haghighi, MD,* Justin Sweeny, MD, Jason Felton, MD,
Epilepsy after two different neurosurgical approaches
 Journal ofneurology, Neurosurgery, and Psychiatry, 1976, 39, 1052-1056 Epilepsy after two different neurosurgical approaches to the treatment of ruptured intracranial aneurysm R. J. CABRAL, T. T. KING,
Journal ofneurology, Neurosurgery, and Psychiatry, 1976, 39, 1052-1056 Epilepsy after two different neurosurgical approaches to the treatment of ruptured intracranial aneurysm R. J. CABRAL, T. T. KING,
Intracranial Hemorrhage. Objectives. What Do Need to Know?
 Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
Tutorials. By Dr Sharon Truter
 Tutorials By Dr Sharon Truter To the Tutorials By Dr Sharon Truter What to expect from the Tutorials What to expect from these tutorials Outlines, structure, guided reading, explanations, mnemonics Begin
Tutorials By Dr Sharon Truter To the Tutorials By Dr Sharon Truter What to expect from the Tutorials What to expect from these tutorials Outlines, structure, guided reading, explanations, mnemonics Begin
Identifying Cerebrovascular Disorders. Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine
 Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
Identifying Cerebrovascular Disorders Wengui Yu, MD, PhD Department of Neurology, University of California, Irvine Objectives Review different types of cerebrovascular disorders. Briefly discuss etiology,
INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU
 CEREBRAL BYPASS An Innovative Treatment for Arteritis INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU CASE 1 q 1 year old girl -recurrent seizure, right side limb weakness, excessive cry and irritability.
CEREBRAL BYPASS An Innovative Treatment for Arteritis INSTITUTE OF NEUROSURGERY & DEPARTMENT OF PICU CASE 1 q 1 year old girl -recurrent seizure, right side limb weakness, excessive cry and irritability.
 Demographic Data Group Study Cohort Control p N 60 20 Age, Mean (years) 36.3 64.4 < 0.001 Age, Median (years) 33.2 64 < 0.001 Male 41 (68.4%) 4 (20%) 0.001 Female 19 (31.6%) 16 (80%) 0.001 Mechanism of
Demographic Data Group Study Cohort Control p N 60 20 Age, Mean (years) 36.3 64.4 < 0.001 Age, Median (years) 33.2 64 < 0.001 Male 41 (68.4%) 4 (20%) 0.001 Female 19 (31.6%) 16 (80%) 0.001 Mechanism of
Classification of Stroke. CNA Neuroscience Nursing Course: Cerebrovascular Disorders. Stroke in Canada
 CNA Neuroscience Nursing Course: Cerebrovascular Disorders Breeda O Farrell RN(EC), MScN, CNN(C) Nurse Practitioner Neurology University Hospital, London Health Science Centre London, ON Deb Bisnaire RN(EC),
CNA Neuroscience Nursing Course: Cerebrovascular Disorders Breeda O Farrell RN(EC), MScN, CNN(C) Nurse Practitioner Neurology University Hospital, London Health Science Centre London, ON Deb Bisnaire RN(EC),
Management of cerebral vasospasm
 Neurosurg Rev DOI 10.1007/s10143-005-0013-5 REVIEW R. Loch Macdonald Management of cerebral vasospasm Received: 5 August 2005 / Revised: 28 October 2005 / Accepted: 4 November 2005 # Springer-Verlag 2005
Neurosurg Rev DOI 10.1007/s10143-005-0013-5 REVIEW R. Loch Macdonald Management of cerebral vasospasm Received: 5 August 2005 / Revised: 28 October 2005 / Accepted: 4 November 2005 # Springer-Verlag 2005
Primary Versus Comprehensive: What is the Difference?
 Primary Versus Comprehensive: What is the Difference? April 26, 2018 Bethann Mercanti, PA-C Director of Clinical Practice Stroke Program Coordinator Cooper Neurological Institute Cooper Bon & Joint Institute
Primary Versus Comprehensive: What is the Difference? April 26, 2018 Bethann Mercanti, PA-C Director of Clinical Practice Stroke Program Coordinator Cooper Neurological Institute Cooper Bon & Joint Institute
Repair of Intracranial Vessel Perforation with Onyx-18 Using an Exovascular Retreating Catheter Technique
 Repair of Intracranial Vessel Perforation with Onyx-18 Using an Exovascular Retreating Catheter Technique Michael Horowitz M.D. Pittsburgh, Pennsylvania Background Iatrogenic intraprocedural rupture rates
Repair of Intracranial Vessel Perforation with Onyx-18 Using an Exovascular Retreating Catheter Technique Michael Horowitz M.D. Pittsburgh, Pennsylvania Background Iatrogenic intraprocedural rupture rates
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins
 ISPUB.COM The Internet Journal of Radiology Volume 18 Number 1 Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins K Kragha Citation K Kragha. Cryptogenic Enlargement Of Bilateral Superior Ophthalmic
ISPUB.COM The Internet Journal of Radiology Volume 18 Number 1 Cryptogenic Enlargement Of Bilateral Superior Ophthalmic Veins K Kragha Citation K Kragha. Cryptogenic Enlargement Of Bilateral Superior Ophthalmic
Definition พ.ญ.ส ธ ดา เย นจ นทร. Epidemiology. Definition 5/25/2016. Seizures after stroke Can we predict? Poststroke seizure
 Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
presents the fourth annual HONEY BASH GALA The Cira Centre Atrium
 presents the fourth annual HONEY BASH GALA S a t u r d a y, S e p t e m b e r 1 6, 2 0 1 7 The Cira Centre Atrium P H I L A D E L P H I A, P E N N S Y LVA N I A S P O N S O R S H I P & B E N E FA C T O
presents the fourth annual HONEY BASH GALA S a t u r d a y, S e p t e m b e r 1 6, 2 0 1 7 The Cira Centre Atrium P H I L A D E L P H I A, P E N N S Y LVA N I A S P O N S O R S H I P & B E N E FA C T O
Stroke: The First Critical Hour. Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP
 Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
Stroke: The First Critical Hour Alina Candal, RN, PCC, MICN Kevin Andruss, MD, FACEP Disclosures We have no actual or potential conflicts of interest in relation to this presentation. Objectives Discuss
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas
 The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
The Importance of Stroke Programs in an Acute Care Setting by Debbie Estes, RN, BSN Stroke Program Coordinator, Medical City of Dallas Objectives Describe the road to the gold Discuss the importance of
Objectives. Stroke Facts 2/27/2015. EMS in Stroke Care: A Critical Partnership
 EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
EMS in Stroke Care: A Critical Partnership Spokane County EMS Objectives Identify the types and time limitations for acute ischemic stroke treatment options Identify the importance of early identification
IDPH EMS Region Five. Stroke Education
 IDPH EMS Region Five Stroke Education Time is Brain!!!!! Time is Brain!!!! Stroke refers to any spontaneous damage to the brain caused by an abnormality of the blood supply by means of a clot or bleed.
IDPH EMS Region Five Stroke Education Time is Brain!!!!! Time is Brain!!!! Stroke refers to any spontaneous damage to the brain caused by an abnormality of the blood supply by means of a clot or bleed.
Required Annual Nursing Education Primary Stroke Center For ICU, Step-Down and Floor
 Required Annual Nursing Education Primary Stroke Center For ICU, Step-Down and Floor Lori Massaro, RN, MSN, CRNP Bethanne McCabe, RN, MSN, CNRN Sue Underwood, RN, MSN, CNRN Requirement RN s caring for
Required Annual Nursing Education Primary Stroke Center For ICU, Step-Down and Floor Lori Massaro, RN, MSN, CRNP Bethanne McCabe, RN, MSN, CNRN Sue Underwood, RN, MSN, CNRN Requirement RN s caring for