Subarachnoid Hemorrhage (SAH) Disclosures/Relationships. Click to edit Master title style. Click to edit Master title style.
|
|
|
- Elijah Phelps
- 5 years ago
- Views:
Transcription
1 Subarachnoid Hemorrhage (SAH) William J. Jones, M.D. Assistant Professor of Neurology Co-Director, UCH Stroke Program Click to edit Master title style Disclosures/Relationships No conflicts of interest Click to edit Master title style SAH Objectives Recognize and appropriately evaluate suspected SAH Apply appropriate strategies to prevent re-bleeding Apply appropriate strategies to reduce intracranial pressure Use appropriate treatment for seizures or to prevent seizures
2 SS1280 Case 1 28 year old woman, presented to an outside ED Sudden HA while doing kettlebell exercises Sharp right parietal pain, radiating down neck, with limited movement of head and neck due to pain Associated photophobia Described as the worst headache of her life PMH: Migraine Questions What evaluation should she have? Other than the history of migraine she had no significant PMH Neurological examination was reportedly normal Non-contrast head CT was reportedly normal A Spinal tap was not done SS1280 Case 1 Four days later she returned to the kettlebell class and again had sudden similar headache but even worse She returned to the ED with headache, lightheadedness, numbness and tingling, and nausea and vomiting She was treated with IV fluids and anti-emetics in the ED and discharged with a prescription for oxycodone
 and associated with Nausea and vomiting Severe lower back pain Difficulty walking Twelve days after the initial headache she drove from New Mexico to her parents home in Aurora and was seen in the")
3 SS1280 Case 1 Since then she continued to have severe headache, worse with valsalva (sneezing, coughing, etc.) and associated with Nausea and vomiting Severe lower back pain Difficulty walking Twelve days after the initial headache she drove from New Mexico to her parents home in Aurora and was seen in the Neurology Outpatient clinic SS1280 Case 1 She reports a severe headache which is much different than she has ever experienced with migraine Examination: Pain with eye movement and transient bilateral horizontal nystagmus with lateral gaze Intense pain with neck flexion Normal sensory examination SS1280


 Focal neurological deficits (including cranial nerve palsies) Up to 12% die before receiving")
4 SS1280 Case 1 Spinal tap Non-traumatic Cloudy, light pink fluid Tube #1: Bloody, slight xanthochromia 16 WBCs 5184 RBCs Tube #4: Bloody, slight xanthochromia 26 WBCs 3610 RBCs SS1280 Symptoms suspicious for acute SAH The worst headache of my life is described by ~80% of patients who can give a history A warning or sentinel headache is also described by 20% Most intracranial aneurysms remain asymptomatic until they rupture Aneurismal SAH occurs frequently during physical exertion or stress but can occur at any time Other signs and symptoms are often associated with headache: Nausea and/or vomiting (~77%) Stiff neck (~35%) Brief loss of consciousness (~53%) Focal neurological deficits (including cranial nerve palsies) Up to 12% die before receiving medical attention
5 Risk Factors for SAH Hypertension Smoking Heavy alcohol use Sympathomimetic drugs (especially in younger patients) Cocaine Methylphenidate Diabetes does not appear to be a risk factor for SAH Evaluation of suspected acute SAH SAH is a medical emergency and is frequently misdiagnosed A high level of suspicion for SAH should exist in patients with acute onset of severe headache CT scanning for suspected SAH should be performed If the CT is negative lumbar puncture is strongly recommended Selective cerebral angiography should be performed in patients with SAH to document the presence and anatomic features of aneurysms MRA and/or CTA may be considered when conventional angiography cannot be performed in a timely fashion PZ1131 Case 2 78 year old woman presented to outside ED Awoke with 10/10 bitemporal headache, nausea, and vomiting BP 156/79 ( /59-87), HR 122 (73-122) Regular, unlabored, and protecting airway Lethargic but follows directions, pupils pinpoint, grip is weak on the right
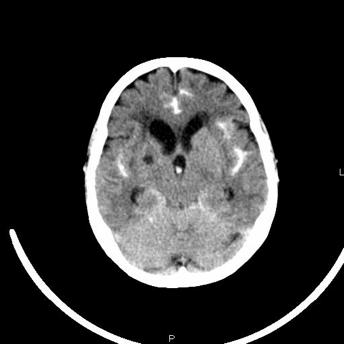
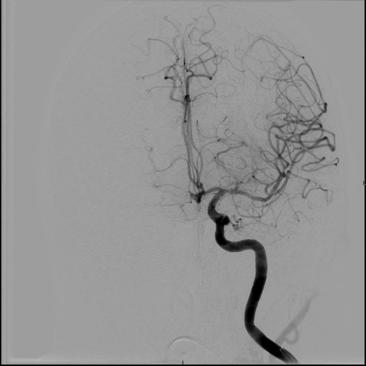
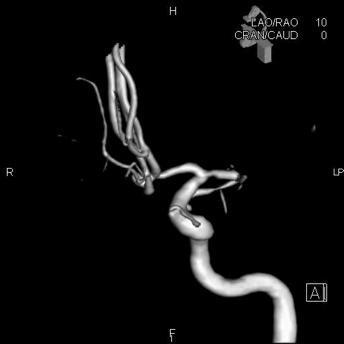
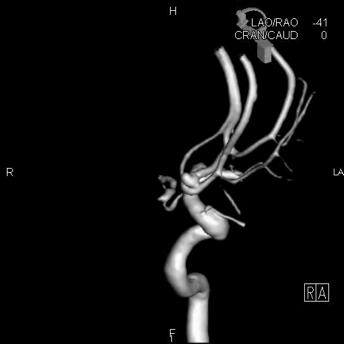
6 PZ1131 PZ1131 PZ1131
7 Questions What are three common and serious cerebral complications of SAH? Re-bleeding Cerebral Vasospasm Typically occurs 3-5 days (up to 14 days) after SAH Nimodipine, 60 mg PO/NG q 4 hours X 21 days After aneurysm is secured Volume expansion Mild-moderate HTN Elevated intracranial pressure (ICP) Question Should empiric anticonvulsant treatment be started? Yes No Hunt and Hess scale for non-traumatic SAH Description Grade Survival Unruptured aneurysm 0 Asymptomatic, mild headache, slight nuchal rigidity 1 70% Moderate to severe headache, nuchal rigidity, no neurologic deficit other than cranial nerve palsy 2 60% Drowsiness / confusion, mild focal neurologic deficit 3 50% Stupor, moderate-severe hemiparesis 4 20% Coma, decerebrate posturing 5 10%
8 Modified Fisher grade classification of SAH on CT scan Grade 1 None evident 2 Less than 1 mm thick 3 More than 1 mm thick Appearance of hemorrhage 4 Any thickness with intraventricular hemorrhage or parenchymal extension World Federation of Neurosurgeons (WFNS) classification of SAH Grade GCS* Focal neurological deficit 1 15 Absent Absent Present Absent of present 5 <7 Absent or present *Glasgow Coma Scale Re-bleeding after initial SAH Re-bleeding is associated with ~ 70% fatality rate Re-bleeding is currently the most treatable cause of poor outcomes ~ 4% of re-bleeding occurs within the first 24 hours ~1-2% per day for the first month With conservative therapy (not clipped or coiled) the risk of re-bleeding is ~ 20-30% within the first month and ~ 3% per year thereafter Risk factors for re-bleeding: Longer interval from hemorrhage to admission and treatment Higher initial blood pressure Worse neurological status on admission (Hunt & Hess, Fisher, WFNS) Recent evidence suggests that ultra-early re-bleeding (within 24 hours of initial SAH) may be as high as 15% ~70% of ultra-early re-bleeds may occur within 2 hours of the initial SAH
9 Prevention of re-bleeding Surgical clipping or endovascular coiling should be performed to reduce the rate of rebleeding after aneurismal SAH Early referral to high-volume centers that have both experienced cerebrovascular surgeons and endovascular specialists is recommended Treat hypertension Antithrombolytics (±) Prevention of re-bleeding (elevated blood pressure) No well-controlled studies of blood pressure control on the rate of re-bleeding Retrospective studies have shown: Re-bleeding is less frequent in patients treated with antihypertensive medication Even though blood pressures were still higher in the treated than non-treated patients An increase in blood pressure immediately before re-bleeding Re-bleeding associated with systolic blood pressure > 150 mm Hg Re-bleeding associated with systolic blood pressure > 160 mm Hg ~ 13.6% of re-bleeds in the ambulance or while still at the referring hospital with a peak incidence within 2 hours of the initial hemorrhage Re-bleeding rate of only 6.9% with no relationship to blood pressure When blood pressure is elevated, short-acting continuous-infusion intravenous agents with a reliable dose-response relationship and favorable safety profile are desirable to reduce SBP <150 mm Hg: Nicardipine, labetalol, and esmolol reportedly best meet these criteria However, sodium nitroprusside is more reliable at quickly and effectively lowering blood pressure but may raise intracranial pressure and causes toxicity with prolonged infusion Prevention of re-bleeding (antifibrinolytics) Antifibrinolytic agents (epsilon-aminocaproic acid, 36 gm/ day; or tranexamic acid, 6 to 12 gm/day): 40-60% reduction in re-bleeding in treated versus control subjects Nearly one third of treated patients in these trials were clinically worse at 14 days Up to 43% increase in the rate of cerebral infarction No difference in re-bleeding between subjects receiving tranexamic acid versus control subjects Similar results have been found with either epsilon-aminocaproic acid (36 gm/d) or tranexamic acid (6 to 12 gm/d) More recently, a prospective, randomized trial of tranexamic acid administered immediately after the diagnosis of SAH followed by early clipping or coiling demonstrated reduced re-bleeding rates and adverse outcomes
10 Prevention of re-bleeding Quiet bed-rest may be helpful but is not sufficient to prevent re-bleeding without being combined with broader treatment strategies Blood pressure should be monitored and controlled to balance the risk of stroke, hypertension-related re-bleeding, and maintenance of cerebral perfusion pressure Within the first 24 hours when risk of vasospasm is low (typically occurs between 3-14 days) and the risk of re-bleeding is highest, SBP should be maintained < 150 mm Hg Recent evidence suggests that early treatment with a short course of antifibrinolytic agents combined with early aneurysm treatment followed by discontinuation of the antifibrinolytic may be reasonable avoid hypovolemia and vasospasm (±) Aminocaproic acid 4-5 gm IV over one hour, then 1 gm IV per hour for 24 hours or until clipped or coiled Increased intracranial pressure Increased ICP is common following SAH may be caused by one or more of: Hydrocephalus May occur with or without intra-ventricular blood Is associated with the amount of cisternal blood when intra-ventricular blood is absent Intra-parenchymal hemorrhage Cerebral edema Increased intracranial pressure Most patient require ICP monitoring Intracranial pressure monitor (bolt) Intra-ventricular drain (s) can also be used to treat hydrocephalus and elevated ICP Mannitol gm/kg will reduce ICP May cause hyponatremia May cause volume depletion and thus decreased cerebral perfusion Hyperventilation temporarily reduces ICP
11 Anticonvulsant treatment The risk and implications of seizures associated with SAH are not well defined, and the need for and efficacy of routinely administered anticonvulsants after SAH are not well established Seizure-like episodes have been associated with aneurismal rupture In retrospective reviews seizures frequency ranges from 6% to 18% Most seizures occurred before medical presentation and in-hospital seizures are rare in patients given prophylactic anticonvulsants The relationship between seizures and outcome is not clear In one series of patients who underwent continuous EEG monitoring found 19% of stuporous or comatose patients had non-convulsive seizures All were receiving prophylactic anticonvulsants, and all died Risk factors for seizures after SAH include: middle cerebral artery aneurysms intraparenchymal hematoma cerebral infarctions history of hypertension Anticonvulsant treatment Anticonvulsants should be administered in patients with seizures Prophylactic anticonvulsants may be considered in the immediate post-hemorrhagic period Dilantin (phenytoin) Typically avoid phenytoin because cardiac rhythm disturbances are common with SAH and phenytoin may also cause arrhythmias Keppra (levetiracetam) mg IV BID Valproic acid mg/kg per day divided TID, may increase up to mg/kg per day SAH recommendations Prevention of re-bleeding Secure aneurysm ASAP Maintain SBP < 150 mm Hg until aneurysm is secured Nicardipine, 3-15 mg per hour IV drip Nipride (nitroprusside), 3-10 mcg/kg per minute IV drip ±Amicar (aminocaproic acid) immediately and for 24 hours or until aneurysm is secured Treatment of ICP ICP monitor or intra-ventricular drain (s) Mannitol gm/kg Anticonvulsants Keppra (levetiracetam), mg BID Depacon (valproate), mg/kg per day, divided TIA
12 Questions
Current State of the Art
 SAH Current State of the Art Thomas C. Steineke, M.D., Ph.D. Director of Neurovascular Surgery NJ Neuroscience Institute JFK Medical Center Introduction Signs and symptoms of a problem What are aneurysms
SAH Current State of the Art Thomas C. Steineke, M.D., Ph.D. Director of Neurovascular Surgery NJ Neuroscience Institute JFK Medical Center Introduction Signs and symptoms of a problem What are aneurysms
Neurosurgical Management of Stroke
 Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Overview Hemorrhagic Stroke Ischemic Stroke Aneurysmal Subarachnoid hemorrhage Neurosurgical Management of Stroke Jesse Liu, MD Instructor, Neurological Surgery Initial management In hospital management
Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY
 Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part B. Objectives Epidemiology of asah Concept: What is a brain
Code Stroke Intervention: Endovascular therapy for asah and management J. DIEGO LOZANO MD INTERVENTIONAL NEURORADIOLOGY Disclosures None Part B. Objectives Epidemiology of asah Concept: What is a brain
Stroke - Intracranial hemorrhage. Dr. Amitesh Aggarwal Associate Professor Department of Medicine
 Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
Stroke - Intracranial hemorrhage Dr. Amitesh Aggarwal Associate Professor Department of Medicine Etiology and pathogenesis ICH accounts for ~10% of all strokes 30 day mortality - 35 45% Incidence rates
PRACTICE GUIDELINE. DEFINITIONS: Mild head injury: Glasgow Coma Scale* (GCS) score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8
 score Moderate head injury: GCS 9-12 Severe head injury: GCS 3-8") PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
PRACTICE GUIDELINE Effective Date: 9-1-2012 Manual Reference: Deaconess Trauma Services TITLE: TRAUMATIC BRAIN INJURY GUIDELINE OBJECTIVE: To provide practice management guidelines for traumatic brain
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage. Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA
 Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Neurointensive Care of Aneurysmal Subarachnoid Hemorrhage Alejandro A. Rabinstein Department of Neurology Mayo Clinic, Rochester, USA The traditional view: asah is a bad disease Pre-hospital mortality
Subarachnoid Hemorrhage and Brain Aneurysm
 Subarachnoid Hemorrhage and Brain Aneurysm DIN Department of Interventional Neurology What is SAH? Subarachnoid Haemorrhage is the sudden leaking (haemorrhage) of blood from the blood vessels of brain.
Subarachnoid Hemorrhage and Brain Aneurysm DIN Department of Interventional Neurology What is SAH? Subarachnoid Haemorrhage is the sudden leaking (haemorrhage) of blood from the blood vessels of brain.
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE
 WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
WHITE PAPER: A GUIDE TO UNDERSTANDING SUBARACHNOID HEMORRHAGE Subarachnoid Hemorrhage is a serious, life-threatening type of hemorrhagic stroke caused by bleeding into the space surrounding the brain,
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications
 Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
Aneurysmal Subarachnoid Hemorrhage Presentation and Complications Sherry H-Y. Chou MD MMSc FNCS Department of Critical Care Medicine, Neurology and Neurosurgery University of Pittsburgh School of Medicine
TCD AND VASOSPASM SAH
 CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
CURRENT TREATMENT FOR CEREBRAL ANEURYSMS TCD AND VASOSPASM SAH Michigan Sonographers Society 2 Nd Annual Fall Vascular Conference Larry N. Raber RVT-RDMS Clinical Manager General Ultrasound-Neurovascular
/ / / / / / Hospital Abstraction: Stroke/TIA. Participant ID: Hospital Code: Multi-Ethnic Study of Atherosclerosis
 Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
Multi-Ethnic Study of Atherosclerosis Participant ID: Hospital Code: Hospital Abstraction: Stroke/TIA History and Hospital Record 1. Was the participant hospitalized as an immediate consequence of this
4/10/2018. The Surgical Treatment of Cerebral Aneurysms. Aneurysm Locations. Aneurysmal Subarachnoid Hemorrhage. Jerone Kennedy, M.D.
 The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
The Surgical Treatment of Cerebral Aneurysms Aneurysmal Subarachnoid Hemorrhage Jerone Kennedy, M.D. Medical Director, Vascular Neurosurgery CentraCare Health-Neurosciences St. Cloud Hospital Aneurysm
11/27/2017. Stroke Management in the Neurocritical Care Unit. Conflict of interest. Karel Fuentes MD Medical Director of Neurocritical Care
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Conflict of interest None Introduction Reperfusion therapy remains the mainstay in the treatment
Sub-arachnoid haemorrhage
 Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
Sub-arachnoid haemorrhage Dr Mary Newton Consultant Anaesthetist The National Hospital for Neurology and Neurosurgery UCL Hospitals NHS Trust mary.newton@uclh.nhs.uk Kiev, Ukraine September 17 th 2009
SAH READMISSIONS TO NCCU
 SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
SAH READMISSIONS TO NCCU Are they preventable? João Amaral Rebecca Gorf Critical Care Outreach Team - NHNN 2015 Total admissions to NCCU =862 Total SAH admitted to NCCU= 104 (93e) (12.0%) Total SAH readmissions=
Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management
 0 0 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management The Department of Health and Social Care in England
0 0 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Guideline scope Subarachnoid haemorrhage caused by a ruptured aneurysm: diagnosis and management The Department of Health and Social Care in England
Preoperative Grading Systems of Spontaneous Subarachnoid Hemorrhage
 KISEP KOR J CEREBROVASCULAR DISEASE March 2000 Vo. 2, No 1, page 24-9 자발성지주막하출혈환자의수술전등급 황성남 Preoperative Grading Systems of Spontaneous Subarachnoid Hemorrhage Sung-Nam Hwang, MD Department of Neurosurgery,
KISEP KOR J CEREBROVASCULAR DISEASE March 2000 Vo. 2, No 1, page 24-9 자발성지주막하출혈환자의수술전등급 황성남 Preoperative Grading Systems of Spontaneous Subarachnoid Hemorrhage Sung-Nam Hwang, MD Department of Neurosurgery,
Standardize comprehensive care of the patient with severe traumatic brain injury
 Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
Trauma Center Practice Management Guideline Iowa Methodist Medical Center Des Moines Management of Patients with Severe Traumatic Brain Injury (GCS < 9) ADULT Practice Management Guideline Contact: Trauma
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM. Vikram Jadhav MD, PhD. 04/12/2018 CentraCare Health St.
 ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
ENDOVASCULAR TREATMENT OF CEREBRAL ANEURYSMS AND MANAGEMENT OF RUPTURED ANEURYSM Vikram Jadhav MD, PhD 04/12/2018 CentraCare Health St. Cloud, MN OBJECTIVES Understand epidemiology and risk factors for
Pre-hospital Response to Trauma and Brain Injury. Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center
 Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Pre-hospital Response to Trauma and Brain Injury Hans Notenboom, M.D. Asst. Medical Director Sacred Heart Medical Center Traumatic Brain Injury is Common 235,000 Americans hospitalized for non-fatal TBI
Intracranial Hemorrhage. Objectives. What Do Need to Know?
 Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
Intracranial Hemorrhage What Do Need to Know? Kerry Brega, MD Associate Professor of Neurosurgery University of Colorado Objectives Know the common types of ICH. Know how they can be differentiated. Know
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes
 and Non- Aneurysmal Causes") Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Diagnosis of Subarachnoid Hemorrhage (SAH) and Non- Aneurysmal Causes By Sheila Smith, MD Swedish Medical Center 1 Disclosures I have no disclosures 2 Course Objectives Review significance and differential
Ruptured Cerebral Aneurysm of the Anterior Circulation
 Original Articles * Division of Neurosurgery Department of Surgery Ruptured Cerebral Aneurysm of the Anterior Circulation Management and Microsurgical Treatment Ossama Al-Mefty, MD* ABSTRACT Based on the
Original Articles * Division of Neurosurgery Department of Surgery Ruptured Cerebral Aneurysm of the Anterior Circulation Management and Microsurgical Treatment Ossama Al-Mefty, MD* ABSTRACT Based on the
THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F.
 THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F. ISHFAQ ZEENAT QURESHI STROKE INSTITUTE AND UNIVERSITY OF TENNESSEE,
THE EFFICACY AND SAFETY OF CILOSTAZOL IN SUBARACHNOID HEMORRHAGE. A META- ANALYSIS OF RANDOMIZED AND NON RANDOMIZED STUDIES DR. MUHAMMAD F. ISHFAQ ZEENAT QURESHI STROKE INSTITUTE AND UNIVERSITY OF TENNESSEE,
presents the fourth annual HONEY BASH GALA The Cira Centre Atrium
 presents the fourth annual HONEY BASH GALA S a t u r d a y, S e p t e m b e r 1 6, 2 0 1 7 The Cira Centre Atrium P H I L A D E L P H I A, P E N N S Y LVA N I A S P O N S O R S H I P & B E N E FA C T O
presents the fourth annual HONEY BASH GALA S a t u r d a y, S e p t e m b e r 1 6, 2 0 1 7 The Cira Centre Atrium P H I L A D E L P H I A, P E N N S Y LVA N I A S P O N S O R S H I P & B E N E FA C T O
Stroke Transfer Checklist
 Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
Stroke Transfer Checklist When preparing to transfer an acute stroke patient to the UF Health Shands Comprehensive Stroke Center, please make every attempt to include the following information: Results
HEADACHE. Dr Nick Pendleton. September Headache
 HEADACHE Dr Nick Pendleton September 2017 Headache Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache Raised ICP
HEADACHE Dr Nick Pendleton September 2017 Headache Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache Raised ICP
Blood Pressure Management in Acute Ischemic Stroke
 Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
Blood Pressure Management in Acute Ischemic Stroke Kimberly Clark, PharmD, BCCCP Clinical Pharmacy Specialist Critical Care, Greenville Health System Adjunct Assistant Professor, South Carolina College
IDPH EMS Region Five. Stroke Education
 IDPH EMS Region Five Stroke Education Time is Brain!!!!! Time is Brain!!!! Stroke refers to any spontaneous damage to the brain caused by an abnormality of the blood supply by means of a clot or bleed.
IDPH EMS Region Five Stroke Education Time is Brain!!!!! Time is Brain!!!! Stroke refers to any spontaneous damage to the brain caused by an abnormality of the blood supply by means of a clot or bleed.
The Worst Headache of My Life Hemorrhagic Stroke
 The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
The Worst Headache of My Life Hemorrhagic Stroke Lindsay Trantum ACNP-BC Neurocritical Care Nurse Practitioner Assistant in Anesthesiology, Division of Critical Care Objectives Identify the risk factors
 www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
www.yassermetwally.com MANAGEMENT OF CEREBRAL HAEMORRHAGE (ICH): A QUICK GUIDE Overview 10% of strokes is caused by ICH. Main Causes: Less than 40 years old: vascular malformations and illicit drug use.
Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici
 Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici Nino Stocchetti Milan University Neuroscience ICU Ospedale Policlinico IRCCS Milano stocchet@policlinico.mi.it Macdonald RL et
Ischemia cerebrale dopo emorragia subaracnoidea Vasospasmo e altri nemici Nino Stocchetti Milan University Neuroscience ICU Ospedale Policlinico IRCCS Milano stocchet@policlinico.mi.it Macdonald RL et
25/09/2018 HEADACHE. Dr Nick Pendleton
 HEADACHE Dr Nick Pendleton September 2018 1 Small Group Work Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache
HEADACHE Dr Nick Pendleton September 2018 1 Small Group Work Tension Type Headache Cranial Nerve Examination Migraine Migraine Treatment Medication Overuse Headache Headache Red Flags Sinusitis Headache
8/29/2011. Brain Injury Incidence: 200/100,000. Prehospital Brain Injury Mortality Incidence: 20/100,000
 Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic Brain Injury Almario G. Jabson MD Section Of Neurosurgery Asian Hospital And Medical Center Brain Injury Incidence: 200/100,000 Prehospital Brain Injury Mortality Incidence: 20/100,000 Hospital
Traumatic brain Injury- An open eye approach
 Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Traumatic brain Injury- An open eye approach Dr. Sunit Dr Sunit, Apollo children's hospital Blah blah Lots of head injury Lot of ill children Various methods of injury Various mechanisms of brain damage
Alan Barber. Professor of Clinical Neurology University of Auckland
 Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Alan Barber Professor of Clinical Neurology University of Auckland Presented with L numbness & slurred speech 2 episodes; 10 mins & 2 hrs Hypertension Type II DM Examination P 80/min reg, BP 160/95, normal
Subarachnoid hemorrhage (SAH) is a common and frequently
 is a common and frequently") AHA/ASA Guideline Guidelines for the Management of Aneurysmal Subarachnoid Hemorrhage A Statement for Healthcare Professionals From a Special Writing Group of the Stroke Council, American Heart Association
AHA/ASA Guideline Guidelines for the Management of Aneurysmal Subarachnoid Hemorrhage A Statement for Healthcare Professionals From a Special Writing Group of the Stroke Council, American Heart Association
What You Should Know About Cerebral Aneurysms
 American Society of Neuroradiology American Society of Interventional & Therapeutic Neuroradiology What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Intervention Committee
American Society of Neuroradiology American Society of Interventional & Therapeutic Neuroradiology What You Should Know About Cerebral Aneurysms From the Cerebrovascular Imaging and Intervention Committee
Vascular Disorders. Nervous System Disorders (Part B-1) Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013
 Module 8 -Chapter 14. Cerebrovascular disease S/S 1/9/2013") Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Nervous System Disorders (Part B-1) Module 8 -Chapter 14 Overview ACUTE NEUROLOGIC DISORDERS Vascular Disorders Infections/Inflammation/Toxins Metabolic, Endocrinologic, Nutritional, Toxic Neoplastic Traumatic
Canadian Best Practice Recommendations for Stroke Care 3.6 Acute Subarachnoid Hemorrhage
 Last Updated: May 21, 2013 Canadian Best Practice Recommendations for Stroke Care Canadian Best Practice Recommendations for Stroke Care 2011-2013 Update Contents Search Strategy... 2 CSN Current Recommendations...Error!
Last Updated: May 21, 2013 Canadian Best Practice Recommendations for Stroke Care Canadian Best Practice Recommendations for Stroke Care 2011-2013 Update Contents Search Strategy... 2 CSN Current Recommendations...Error!
I T IS generally agreed that the surgical risk
 Surgical Risk as Related to Time of Intervention in the Repair of Intracranial Aneurysms WILLIAM E. HUNT, M.D., AND ROBERT M. HESS, M.D. Department of Surgery, Division of Neurological Surgery, Ohio State
Surgical Risk as Related to Time of Intervention in the Repair of Intracranial Aneurysms WILLIAM E. HUNT, M.D., AND ROBERT M. HESS, M.D. Department of Surgery, Division of Neurological Surgery, Ohio State
excellence in care Procedure Neuroprotection For Review Aug 2015
 Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
Neuro Projection HELI.CLI.14 Purpose This procedure outlines the management principles of patients being retrieved with traumatic brain injury (TBI), spontaneous intracranial haemorrhage (including subarachnoid
11/23/2015. Disclosures. Stroke Management in the Neurocritical Care Unit. Karel Fuentes MD Medical Director of Neurocritical Care.
 Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke Management in the Neurocritical Care Unit Karel Fuentes MD Medical Director of Neurocritical Care Disclosures I have no relevant commercial relationships to disclose, and my presentations will not
Stroke in the ED. Dr. William Whiteley. Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian
 Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Stroke in the ED Dr. William Whiteley Scottish Senior Clinical Fellow University of Edinburgh Consultant Neurologist NHS Lothian 2016 RCP Guideline for Stroke RCP guidelines for acute ischaemic stroke
Cerebrovascular Disorders. Blood, Brain, and Energy. Blood Supply to the Brain 2/14/11
 Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
Cerebrovascular Disorders Blood, Brain, and Energy 20% of body s oxygen usage No oxygen/glucose reserves Hypoxia - reduced oxygen Anoxia - Absence of oxygen supply Cell death can occur in as little as
From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council
 American Society of Neuroradiology What Is a Stroke? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall T. Higashida, M.D., Chair
American Society of Neuroradiology What Is a Stroke? From the Cerebrovascular Imaging and Intervention Committee of the American Heart Association Cardiovascular Council Randall T. Higashida, M.D., Chair
Clinical Decision Rules to Rule Out Subarachnoid Hemorrhage for Acute Headache FREE
 Clinical Decision Rules to Rule Out Subarachnoid Hemorrhage for Acute Headache FREE Jeffrey J. Perry, MD, MSc1; Ian G. Stiell, MD, MSc1; Marco L. A. Sivilotti, MD, MSc5,6; Michael J. Bullard, MD11; Corinne
Clinical Decision Rules to Rule Out Subarachnoid Hemorrhage for Acute Headache FREE Jeffrey J. Perry, MD, MSc1; Ian G. Stiell, MD, MSc1; Marco L. A. Sivilotti, MD, MSc5,6; Michael J. Bullard, MD11; Corinne
Emergency Department Management of Acute Ischemic Stroke
 Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
Emergency Department Management of Acute Ischemic Stroke R. Jason Thurman, MD Associate Professor of Emergency Medicine and Neurosurgery Associate Director, Vanderbilt Stroke Center Vanderbilt University,
European Stroke Organization Guidelines for the Management of Intracranial Aneurysms and Subarachnoid Haemorrhage
 https://helda.helsinki.fi European Stroke Organization Guidelines for the Management of Intracranial Aneurysms and Subarachnoid Haemorrhage Steiner, Thorsten 2013 Steiner, T, Juvela, S, Unterberg, A, Jung,
https://helda.helsinki.fi European Stroke Organization Guidelines for the Management of Intracranial Aneurysms and Subarachnoid Haemorrhage Steiner, Thorsten 2013 Steiner, T, Juvela, S, Unterberg, A, Jung,
Update in Diagnosis and Management of Intracranial Aneurysms for Primary Health Care Providers November 15, 2012 Boston, Massachusetts
 Update in Diagnosis and Management of Intracranial Aneurysms for Primary Health Care Providers November 15, 2012 Boston, Massachusetts Educational Partner: Session 1: Update in Diagnosis and Management
Update in Diagnosis and Management of Intracranial Aneurysms for Primary Health Care Providers November 15, 2012 Boston, Massachusetts Educational Partner: Session 1: Update in Diagnosis and Management
Cerebral Aneurysms. U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health
 Cerebral Aneurysms U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health Cerebral Aneurysms What is a cerebral aneurysm? cerebral aneurysm (also known as an
Cerebral Aneurysms U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutes of Health Cerebral Aneurysms What is a cerebral aneurysm? cerebral aneurysm (also known as an
An Introduc+on to Stroke
 An Introduc+on to Stroke Elizabeth Huntoon MS, MD Assistant Professor Department of Physical Medicine and Rehabilita>on Vanderbilt University School of Medicine Defini+on Sudden focal neurologic deficit
An Introduc+on to Stroke Elizabeth Huntoon MS, MD Assistant Professor Department of Physical Medicine and Rehabilita>on Vanderbilt University School of Medicine Defini+on Sudden focal neurologic deficit
Stroke Guidelines. November 19, 2011
 Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
Stroke Guidelines November 19, 2011 Clinical Practice Guidelines American Stroke Association Guidelines are comprehensive statements that provide the highest level of scientific evidence for clinical practice.
TURN IT UP TO 11: LP IN THE DIAGNOSIS OF SAH. Matt Greer February 10 th, 2015
 TURN IT UP TO 11: LP IN THE DIAGNOSIS OF SAH Matt Greer February 10 th, 2015 IN CASE YOU MISSED THE REFERENCE HEADACHES IN THE ED Account for approximately 2% of ED visits 1% of these are due to SAH Approximately
TURN IT UP TO 11: LP IN THE DIAGNOSIS OF SAH Matt Greer February 10 th, 2015 IN CASE YOU MISSED THE REFERENCE HEADACHES IN THE ED Account for approximately 2% of ED visits 1% of these are due to SAH Approximately
MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes
 MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes Stroke is the third leading cause of death and the leading cause of adult disability in the
MCHENRY WESTERN LAKE COUNTY EMS SYSTEM Paramedic, EMT-B and PHRN Optional Continuing Education 2019 #7 Strokes Stroke is the third leading cause of death and the leading cause of adult disability in the
Definition พ.ญ.ส ธ ดา เย นจ นทร. Epidemiology. Definition 5/25/2016. Seizures after stroke Can we predict? Poststroke seizure
 Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
Seizures after stroke Can we predict? พ.ญ.ส ธ ดา เย นจ นทร PMK Epilepsy Annual Meeting 2016 Definition Poststroke seizure : single or multiple convulsive episode(s) after stroke and thought to be related
Chapter 57: Nursing Management: Acute Intracranial Problems
 Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
Chapter 57: Nursing Management: Acute Intracranial Problems NORMAL INTRACRANIAL PRESSURE Intracranial pressure (ICP) is the hydrostatic force measured in the brain CSF compartment. Normal ICP is the total
HEADACHE: Benign or Severe Dr Gobinda Chandra Roy
 HEADACHE: Benign or Severe Dr Gobinda Chandra Roy Associate Professor, Department of Medicine, Shaheed Suhrawardy Medical College and Hospital Outlines 1. Introduction 2. Classification of headache 3.
HEADACHE: Benign or Severe Dr Gobinda Chandra Roy Associate Professor, Department of Medicine, Shaheed Suhrawardy Medical College and Hospital Outlines 1. Introduction 2. Classification of headache 3.
A few Neurosurgical Emergencies. Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015
 A few Neurosurgical Emergencies Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015 Outline Neuroanatomy and physiology (85 slides ) Raised
A few Neurosurgical Emergencies Cathrin Parsch Lyell Mc Ewin Hospital SA Ambulance Service SAAS medstar Spring Seminar on Emergency Medicine 2015 Outline Neuroanatomy and physiology (85 slides ) Raised
Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage
 Romanian Neurosurgery (2016) XXX 4: 461 466 461 DOI: 10.1515/romneu-2016-0074 Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage A. Chiriac, Georgiana Ion*,
Romanian Neurosurgery (2016) XXX 4: 461 466 461 DOI: 10.1515/romneu-2016-0074 Intra-arterial nimodipine for the treatment of vasospasm due to aneurysmal subarachnoid hemorrhage A. Chiriac, Georgiana Ion*,
Guidelines for the management of a patient with a subarachnoid haemorrhage
 Guidelines for the management of a patient with a subarachnoid haemorrhage Item Type Report Authors Health Service Executive (HSE) Citation Health Service Executive. Guidelines for the management of a
Guidelines for the management of a patient with a subarachnoid haemorrhage Item Type Report Authors Health Service Executive (HSE) Citation Health Service Executive. Guidelines for the management of a
Acute stroke imaging
 Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
Acute stroke imaging Aims Imaging modalities and differences Why image acute stroke Clinical correlation to imaging appearance What is stroke Classic definition: acute focal injury to the central nervous
BY: Ramon Medina EMT-LP/RN
 BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
BY: Ramon Medina EMT-LP/RN Discuss types of strokes Discuss the physical and neurological assessment of stroke patients Discuss pertinent historical findings Discuss pre-hospital and emergency management
Lesson. The most important aspect in the assessment of headache is a careful history
 Lesson The most important aspect in the assessment of headache is a careful history Investigation of? SAH Summary A CT scan within 12 hours of presentation is 98% sensitive for SAH CSF >12 hours with spectrophotometric
Lesson The most important aspect in the assessment of headache is a careful history Investigation of? SAH Summary A CT scan within 12 hours of presentation is 98% sensitive for SAH CSF >12 hours with spectrophotometric
(aneurysmal subarachnoid hemorrhage, 17%~60% :SAH. ,asah , 22%~49% : Willis. :1927 Moniz ;(3) 2. ischemic neurological deficit,dind) SAH) SAH ;(6)
 2. ischemic neurological deficit,dind) SAH) SAH ;(6)") ,, 2. : ;,, :(1), (delayed ;(2) ischemic neurological deficit,dind) ;(3) 2. :SAH ;(4) 5-10 10 HT -1-1 ;(5), 10 SAH ;(6) - - 27%~50%, ( cerebral vasospasm ) Glasgow (Glasgow Coma Scale,GCS), [1],, (aneurysmal
,, 2. : ;,, :(1), (delayed ;(2) ischemic neurological deficit,dind) ;(3) 2. :SAH ;(4) 5-10 10 HT -1-1 ;(5), 10 SAH ;(6) - - 27%~50%, ( cerebral vasospasm ) Glasgow (Glasgow Coma Scale,GCS), [1],, (aneurysmal
Nicolas Bianchi M.D. May 15th, 2012
 Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Nicolas Bianchi M.D. May 15th, 2012 New concepts in TIA Differential Diagnosis Stroke Syndromes To learn the new definitions and concepts on TIA as a condition of high risk for stroke. To recognize the
Hypertensives Emergency and Urgency
 Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Hypertensives Emergency and Urgency Budi Yuli Setianto Cardiology Divisision Department of Internal Medicine Faculty of Medicine UGM Sardjito Hospital Yogyakarta Background USA: Hypertension is 30% of
Isolated Cranial Nerve-III Palsy Secondary to Perimesencephalic Subarachnoid Hemorrhage
 Lehigh Valley Health Network LVHN Scholarly Works Department of Medicine Isolated Cranial Nerve-III Palsy Secondary to Perimesencephalic Subarachnoid Hemorrhage Hussam A. Yacoub MD Lehigh Valley Health
Lehigh Valley Health Network LVHN Scholarly Works Department of Medicine Isolated Cranial Nerve-III Palsy Secondary to Perimesencephalic Subarachnoid Hemorrhage Hussam A. Yacoub MD Lehigh Valley Health
Pre-Hospital Stroke Care: Bringing It To The Street. by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center
 Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
Pre-Hospital Stroke Care: Bringing It To The Street by Bob Atkins, NREMT-Paramedic AEMD EMS Director Bedford Regional Medical Center Overview/Objectives Explain the reasons or rational behind the importance
AHA/ASA Guideline. by guest on April 14, 2017
 AHA/ASA Guideline Guidelines for the Management of Aneurysmal Subarachnoid Hemorrhage A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association The American
AHA/ASA Guideline Guidelines for the Management of Aneurysmal Subarachnoid Hemorrhage A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association The American
Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke (2 of 2) Seizures Altered Mental Status (AMS)
 Stroke (2 of 2) Seizures Altered Mental Status (AMS)") 1 2 3 4 5 Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women
1 2 3 4 5 Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women
Overview INTRODUCTION 3/15/2018. Headache Emergencies. Other way to differentiate between them? Is there an easy way to differentiate between them?
 Overview Headache Emergencies Primary versus Secondary headache disorder Red flags 4 cases of unusual headache emergencies Disclaimer: we will not talk about brain bleed as patients usually go the ED.
Overview Headache Emergencies Primary versus Secondary headache disorder Red flags 4 cases of unusual headache emergencies Disclaimer: we will not talk about brain bleed as patients usually go the ED.
Management of Severe Traumatic Brain Injury
 Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Guideline for North Bristol Trust Management of Severe Traumatic Brain Injury This guideline describes the following: Initial assessment and management of the patient with head injury Indications for CT
Risk Management in an Office Setting: Who are we sending home?
 Risk Management in an Office Setting: Who are we sending home? October 1, 2016 Niagara Falls, NY The threat of litigation following a misdiagnosis or improper treatment presents a challenge to healthcare
Risk Management in an Office Setting: Who are we sending home? October 1, 2016 Niagara Falls, NY The threat of litigation following a misdiagnosis or improper treatment presents a challenge to healthcare
Subarachnoid Haemorrhage
 2011 Subarachnoid Haemorrhage Subarachnoid Haemorrhage This pamphlet will briefly describe what may happen to a person who has a subarachnoid haemorrhage (SAH). We would like to encourage you to read this
2011 Subarachnoid Haemorrhage Subarachnoid Haemorrhage This pamphlet will briefly describe what may happen to a person who has a subarachnoid haemorrhage (SAH). We would like to encourage you to read this
Treatment of Acute Hydrocephalus After Subarachnoid Hemorrhage With Serial Lumbar Puncture
 19 Treatment of Acute After Subarachnoid Hemorrhage With Serial Lumbar Puncture Djo Hasan, MD; Kenneth W. Lindsay, PhD, FRCS; and Marinus Vermeulen, MD Downloaded from http://ahajournals.org by on vember,
19 Treatment of Acute After Subarachnoid Hemorrhage With Serial Lumbar Puncture Djo Hasan, MD; Kenneth W. Lindsay, PhD, FRCS; and Marinus Vermeulen, MD Downloaded from http://ahajournals.org by on vember,
Brain abscess rupturing into the lateral ventricle causing meningitis: a case report
 Brain abscess rupturing into the lateral ventricle causing meningitis: a case report Endry Martinez, and Judith Berger SBH Health System, 4422 Third Ave, Bronx, NY 10457 Key words: brain abscess, rupture
Brain abscess rupturing into the lateral ventricle causing meningitis: a case report Endry Martinez, and Judith Berger SBH Health System, 4422 Third Ave, Bronx, NY 10457 Key words: brain abscess, rupture
Subarachnoid Bleeds. Under the Spider via deepthought 1 / 22
 Subarachnoid Bleeds Under the Spider via deepthought 1 / 22 SAH: symptoms worst headache of my life Sudden-onset Severe w max intensity in seconds = thunderclap Sentinel headache in ~10-40% in aneurysmal
Subarachnoid Bleeds Under the Spider via deepthought 1 / 22 SAH: symptoms worst headache of my life Sudden-onset Severe w max intensity in seconds = thunderclap Sentinel headache in ~10-40% in aneurysmal
Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center
 Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center Nothing to disclose Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss
Marcey Osgood, DO Assistant Professor of Neurocritical Care UMASS Medical Center Nothing to disclose Review common neurologic emergencies Ischemic Stroke Hemorrhagic Stroke Subarachnoid Hemorrhage Discuss
CEREBRO VASCULAR ACCIDENTS
 CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
CEREBRO VASCULAR S MICHAEL OPONG-KUSI, DO MBA MORTON CLINIC, TULSA, OK, USA 8/9/2012 1 Cerebrovascular Accident Third Leading cause of deaths (USA) 750,000 strokes in USA per year. 150,000 deaths in USA
8th Annual NKY TBI Conference 3/28/2014
 Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
Closed Head Injury: Headache to Herniation A N T H O N Y T. K R A M E R U N I V E R S I T Y O F C I N C I N N A T I B L U E A S H E M S T E C H N O L O G Y P R O G R A M Objectives Describe the pathological
NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM
 NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM Chairperson Professor Dr Zamzuri Idris Head of Department Members Associate Professor Dato Dr
NEUROSURGICAL EMERGENCY GUIDELINE DEVELOPMENT GROUP P3 NEURO CENTER OF NEUROSCIENCE RESEARCH AND SERVICE USM Chairperson Professor Dr Zamzuri Idris Head of Department Members Associate Professor Dato Dr
TIA: Updates and Management 2008
 TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
TIA: Updates and Management 2008 S. Andrew Josephson, MD Department of Neurology, Neurovascular Division University of California San Francisco Commonly Held TIA Misconceptions TIA is easy to diagnose
ACCESS CENTER:
 ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
ACCESS CENTER: 1-877-367-8855 Emergency Specialty Services: BRAIN ATTACK Criteria: Stroke symptom onset time less than 6 hours Referring Emergency Department Patient Information Data: Time last known normal:
Summary of some of the landmark articles:
 Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
Summary of some of the landmark articles: The significance of unruptured intracranial saccular aneurysms: Weibers et al Mayo clinic. 1987 1. 131 patients with 161 aneurysms were followed up at until death,
Hypertensive Urgency and Emergency. Definitions. Emergency or Urgency?
 Hypertensive Urgency and Emergency Joel Handler MD Kaiser Permanente Care Management Institute/ SCal Region Hypertension Lead Definitions Hypertensive Emergency: -Severe elevation in BP with evidence of
Hypertensive Urgency and Emergency Joel Handler MD Kaiser Permanente Care Management Institute/ SCal Region Hypertension Lead Definitions Hypertensive Emergency: -Severe elevation in BP with evidence of
Chapter 15 Neurological Emergencies Stroke (1 of 2) Stroke (2 of 2) Seizures Altered Mental Status (AMS) Brain Structure and Function
 Stroke (2 of 2) Seizures Altered Mental Status (AMS) Brain Structure and Function") 1 Chapter 15 Neurological Emergencies 2 Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women have
1 Chapter 15 Neurological Emergencies 2 Stroke (1 of 2) Stroke is the leading cause of death in the United States. After heart disease and cancer It is common in geriatric patients. More than women have
Method Hannah Shotton
 #asah Method Hannah Shotton 2 Introduction SAH Rupturing aneurysm Poor outlook Intervention Secure the aneurysm: clipping or coiling Recommended 48 hours Regional Specialist NSC Conservative management
#asah Method Hannah Shotton 2 Introduction SAH Rupturing aneurysm Poor outlook Intervention Secure the aneurysm: clipping or coiling Recommended 48 hours Regional Specialist NSC Conservative management
Hypertensive Haemorrhagic Stroke. Dr Philip Lam Thuon Mine
 Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Hypertensive Haemorrhagic Stroke Dr Philip Lam Thuon Mine Intracerebral Haemorrhage Primary ICH Spontaneous rupture of small vessels damaged by HBP Basal ganglia, thalamus, pons and cerebellum Amyloid
Clinical Analysis of Risk Factors Affecting Rebleeding in Patients with an Aneurysm. Gab Teug Kim, M.D.
 / 119 = Abstract = Clinical Analysis of Risk Factors Affecting Rebleeding in Patients with an Aneurysm Gab Teug Kim, M.D. Department of Emergency Medicine, College of Medicine, Dankook University, Choenan,
/ 119 = Abstract = Clinical Analysis of Risk Factors Affecting Rebleeding in Patients with an Aneurysm Gab Teug Kim, M.D. Department of Emergency Medicine, College of Medicine, Dankook University, Choenan,
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease
 Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Acute stroke update 2016 innovations in managing ischemic and hemorrhagic disease Christopher Koebbe, MD Endovascular Neurosurgeon Florida Spine Institute Director of Neurosciences Northside Hospital Overview
Daniel A Capen MD Downey Orthopedic Group COMPLICATIONS IN CERVICAL AND LUMBAR SPINAL SURGERY
 Daniel A Capen MD Downey Orthopedic Group COMPLICATIONS IN CERVICAL AND LUMBAR SPINAL SURGERY Complications in Spinal Surgery Positioning Complications Approach Complications Procedure Complications Post-surgical
Daniel A Capen MD Downey Orthopedic Group COMPLICATIONS IN CERVICAL AND LUMBAR SPINAL SURGERY Complications in Spinal Surgery Positioning Complications Approach Complications Procedure Complications Post-surgical
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES
 TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
TRAUMATIC CAROTID &VERTEBRAL ARTERY INJURIES ALBERTO MAUD, MD ASSOCIATE PROFESSOR TEXAS TECH UNIVERSITY HEALTH SCIENCES CENTER EL PASO PAUL L. FOSTER SCHOOL OF MEDICINE 18TH ANNUAL RIO GRANDE TRAUMA 2017
Risk Factors for Delayed Diagnosis of Subarachnoid and Intracerebral Hemorrhage
 Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine 1-10-2003 Risk Factors for Delayed Diagnosis of Subarachnoid and Intracerebral
Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine 1-10-2003 Risk Factors for Delayed Diagnosis of Subarachnoid and Intracerebral
David Dredge, MD MGH Child Neurology CME Course September 9, 2017
 David Dredge, MD MGH Child Neurology CME Course September 9, 2017 } 25-40,000 children experience their first nonfebrile seizure each year } AAN/CNS guidelines developed in early 2000s and subsequently
David Dredge, MD MGH Child Neurology CME Course September 9, 2017 } 25-40,000 children experience their first nonfebrile seizure each year } AAN/CNS guidelines developed in early 2000s and subsequently
Neurosurgical decision making in structural lesions causing stroke. Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery)
") Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
Neurosurgical decision making in structural lesions causing stroke Dr Rakesh Ranjan MS, MCh, Dip NB (Neurosurgery) Subarachnoid Hemorrhage Every year, an estimated 30,000 people in the United States experience
UPSTATE Comprehensive Stroke Center. Neurosurgical Interventions Satish Krishnamurthy MD, MCh
 UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
UPSTATE Comprehensive Stroke Center Neurosurgical Interventions Satish Krishnamurthy MD, MCh Regional cerebral blood flow is important Some essential facts Neurons are obligatory glucose users Under anerobic
Subarachnoid Hemorrhage & Vasospasm basic level
 Subarachnoid Hemorrhage & Vasospasm basic level Overview Subarachnoid hemorrhage (SAH) is a serious, lifethreatening type of stroke caused by bleeding into the space surrounding the brain. A stroke occurs
Subarachnoid Hemorrhage & Vasospasm basic level Overview Subarachnoid hemorrhage (SAH) is a serious, lifethreatening type of stroke caused by bleeding into the space surrounding the brain. A stroke occurs
Protocol for IV rtpa Treatment of Acute Ischemic Stroke
 Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Protocol for IV rtpa Treatment of Acute Ischemic Stroke Acute stroke management is progressing very rapidly. Our team offers several options for acute stroke therapy, including endovascular therapy and
Disclosures. Objectives. Critical Care Management of Subarachnoid Hemorrhage. Nothing to disclose
 Critical Care Management of Subarachnoid Hemorrhage Nerissa U. Ko, MD, MAS UCSF Department of Neurology September 7, 2013 Nothing to disclose Disclosures Grant funding from American Heart Association,
Critical Care Management of Subarachnoid Hemorrhage Nerissa U. Ko, MD, MAS UCSF Department of Neurology September 7, 2013 Nothing to disclose Disclosures Grant funding from American Heart Association,