A case of struma carcinoid and Graves disease
|
|
|
- Claire Banks
- 6 years ago
- Views:
Transcription
1 AACE Clinical Case Reports Rapid Electronic Articles in Press Rapid Electronic Articles in Press are preprinted manuscripts that have been reviewed and accepted for publication, but have yet to be edited, typeset and finalized. This version of the manuscript will be replaced with the final, published version after it has been published in the print edition of the journal. The final, published version may differ from this proof. Case Report A case of struma carcinoid and Graves disease ACCR Asha K. Pathak, MD 1 ; Gregory M. Cheeney, MD 2 ; Mara H. Rendi, MD, PhD 2 ; Renata R. Urban, MD 3 ; Richard A. Failor, MD 1 ; Alan Chait, MD 1 From: University of Washington, Seattle, Washington, USA; 1 Department of Medicine, Division of Metabolism, Endocrinology, and Nutrition; 2 Department of Pathology; 3 Department of Obstetrics and Gynecology, Division of Gynecologic Oncology Corresponding Author and Address: Alan Chait, MD University of Washington, Division of Metabolism, Endocrinology and Nutrition 1959 NE Pacific St., Box Seattle, WA achait@uw.edu
2 Abstract Objective: We describe a case of coexisting Graves disease and struma carcinoid in a woman with an ovarian mass and history of hyperthyroidism. Methods: Patient history, presentation, diagnostic studies, and treatment are described. Results: A 59 year old female with an antecedent history of hyperthyroidism was scheduled for resection of a 4.1 cm left ovarian mass. Pre-operative labs demonstrated TSH <0.007, free T pg/ml ( pg/ml), and free T ng/dl ( ng/dl). Radioactive iodine uptake (RAIU) was 0 % in the neck at both 4 and 24 hours. A functioning strumal tumor was suspected. In preparation for surgery, propranolol 40 mg three times a day was initiated. Pathology of the left ovary was consistent with struma carcinoid. Hyperthryoidism persisted on post-op follow up. Repeat RAIU with scan at 6 months post-op demonstrated 4- and 24-hour uptake in the neck of 10.4% (4-20%) and 23.6% (10-30%), with diffuse, minimally inhomogeneous uptake in the thyroid lobes bilaterally and uptake visualized in the pyramidal lobe. There was no uptake outside the neck on whole body imaging. Thyroid stimulating immunoglobulin level was 329% (<= 122%). Taken together these findings were consistent with Graves disease. The patient was treated with radioactive iodine ablation (16.02 mci). Six weeks post-ablation she developed hypothyroidism (TSH ), and levothyroxine was initiated. Conclusion: To our knowledge this is the first reported case of Graves disease co-existing with struma carcinoid. Graves disease may be diagnosed after resection of strumal tumors in patients with persistent or recurrent hyperthyroidism.
3 Abbreviations: RAIU = Radioactive iodine uptake; TSH = Thyroid stimulating hormone. Case Report Introduction Struma ovarii are monodermal teratomas containing a predominance of thyroid tissue (1-3). When both thyroid and carcinoid components are identified within the ovary, the tumor is described as struma carcinoid (1-3). Patients with struma carcinoid may present with a pelvic mass or, less commonly, with carcinoid syndrome or hyperthyroidism (3,4). Hyperthyroidism has been described in less than 10% of cases, similar to that reported with struma ovarii (1-3). Hyperthyroidism may be related to autonomous function of thyroid tissue in the ovary, or responsiveness of this tissue to circulating TSH receptor antibodies, as has been described in patients with Graves disease and struma ovarii (2,5-7). Additionally, excess thyroid hormone production by the thyroid gland may occur in the setting of both functioning and nonfunctioning struma ovarii (8,9). We present a case of struma carcinoid coexisting with Graves disease, which to our knowledge has not previously been reported. Case Description A 59 year old female was undergoing pre-operative evaluation for pelvic surgery to remove a 4.1 cm left ovarian mass associated with abdominal pain. She was referred to endocrinology clinic because of an antecedent history of thyroid nodules and hyperthyroidism. Her previous medical history was significant for chronic anxiety, nephrolithiasis, and fibromyalgia. Her medications included sertraline, amitriptyline, alprazolam, and cyclobenzaprine. She had never taken thyroid medications, undergone thyroid uptake
4 and scan or biopsy, or been exposed to significant radiation. There was no family history of thyroid disease. Review of systems was positive for heat intolerance, anxiety, hand tremor, and postmenopausal hot flashes. There were no features concerning for carcinoid syndrome. Serum CA-125 was 31.5 U/mL (0-35 U/mL). Thyroid ultrasound identified a heterogeneous, nodular gland with a dominant solid right mid lobe nodule measuring 1.0 x 1.1 x 1.5 cm. Physical examination demonstrated a nontender thyroid gland normal in size, a palpable right thyroid nodule, and bilateral hand tremor. Laboratory studies demonstrated TSH <0.007 μiu/ml ( μiu/ml), free T pg/ml ( pg/ml), and free T ng/dl ( ng/dl). Radioactive iodine uptake (RAIU) was 0% in the neck at both 4 and 24 hours. Unfortunately, concurrent abdominal and pelvic scans were not obtained to evaluate for extra-cervical concentration of radioactive iodine. However, based on lack of uptake in the neck, a functioning strumal tumor was suspected. In preparation for surgery, propranolol 40 mg three times a day was initiated. Intraoperatively, a smooth mass was identified emanating from the left ovary, interpreted on frozen section as a low grade epithelial neoplasm. Bilateral salpingo-oophorectomy, total hysterectomy, lymph node dissection, and omental biopsy were performed. On pathology, the left ovary was found to contain a 4.0 cm teratoma with components of thyroid tissue and low grade neuroendocrine neoplasm, consistent with struma carcinoid (Figure 1). Nuclei were relatively uniform, and mitotic rate was low. Immunohistochemistry in the carcinoid component was positive for chromogranin (1+; 5-24% of cells) and synaptophysin (3+; >75% of cells) (2). Staining in the thyroid component was positive for TTF-1 and thyroglobulin (2). Incidental cervical intermediate grade squamous intraepithelial neoplasia (CIN 2) was noted. Remaining tissues and peritoneal wash were negative for malignant cells or neoplasm. The patient was seen in clinic 2 weeks post-operatively, at which time she was feeling well. TSH was
5 0.024 μiu/ml and serum chromogranin A level was 123 ng/ml (<93). At 6 weeks post-op TSH was μiu/ml, free T4 1.0 ng/dl and total T3 113 ng/dl ( ng/dl). Five months post-op her TSH remained suppressed at μiu/ml, with elevated free T4 1.7 ng/dl and total T3 202 ng/dl. She described heat intolerance, fatigue, and anxiety. Blood count and electrolyte values were within normal limits. On physical examination her thyroid gland was near upper limit of normal in size, and repeat thyroid ultrasound demonstrated bilateral subcentimeter nodules with otherwise normal thyroid echogenicity, vascularity, and lymph node morphology. Repeat RAIU and scan at 6 months post-op (Figure 2) demonstrated 4- and 24-hour uptake in the neck of 10.4% (4-20%) and 23.6% (10-30%), with diffuse, minimally inhomogeneous uptake in the thyroid lobes bilaterally. Uptake was also visualized in the pyramidal lobe. There was no uptake outside the neck on whole body imaging. Thyroid stimulating immunoglobulin level was 329% (<= 122%). Taken together these findings were consistent with Graves disease, and the patient was treated with radioactive iodine ablation (16.02 mci). Six weeks postablation TSH was μiu/ml, with free T ng/dl and total T ng/dl. Levothyroxine was initiated. The patient continues to be followed, 1.5 years after initial evaluation, and is doing well. Discussion We present a case of concurrent struma carcinoid and Graves disease in a 59 year old woman presenting with hyperthyroidism and an ovarian mass. Fewer than 20 cases of coexisting Graves disease and struma ovarii have been described (5,6). To our knowledge, this is the first report of coexisting Graves disease and struma carcinoid. Hyperthyroidism in the setting of an ovarian mass may be related to excess thyroid hormone production by the thyroid gland and/or thyroid tissue within the ovary (8). RAIU and scans are useful in localizing site of thyroid hormone production, both during initial evaluation and investigation of recurrent or persistent hyperthyroidism. Extracervical scans can help identify an ectopic focus of thyroid hormone
6 production in cases of hyperthyroidism with diminished uptake in the neck. Several reports have described diagnosis of struma ovarii in the setting of recurrent or persistent hyperthyroidism after treatment for Graves disease or toxic adenoma based on abdominopelvic radioactive iodine concentration (5-9). In the present case, while abdominopelvic scans were not obtained after the first 123 I adminstration pre-operatively, a strumal tumor was suspected as the source of excess thyroid hormone, given 0% uptake in the neck and presence of an ovarian mass. Our patient demonstrated persistent hyperthyroidism after resection of struma carcinoid, leading to subsequent diagnosis of Graves disease based on laboratory evaluation and findings on the second RAIU and accompanying scans. Pathologic evaluation of the struma carcinoid in this case demonstrated a thyroid component with benign features and normal morphology, and no high-grade features within the carcinoid component. However cancer may be identified in either component of these tumors, originating within the ovary or metastatic from a primary site (2,3,10). Thyroid tissue demonstrating typical appearance and contained within the ovary is usually benign (2). Spread within the peritoneum identified at surgery, known as peritoneal strumosis, is also usually benign, although patients should continue to be followed, as recurrence would instead suggest a diagnosis of minimal deviation follicular thyroid-type carcinoma (2). Rare cases of thyroid-type carcinoma originating in strumal tumors have been described, and may metastasize; additionally, thyroid cancer can metastasize to the ovary (2,11,12). Carcinoid within the ovary is subtyped histologically as insular, trabecular, or mucinous, and more than one subtype may be present (2,3,8). Atypical features or primary carcinoma with or without metastasis may be found, and carcinoid may also metastasize to the ovary from a primary site (10,11,13).
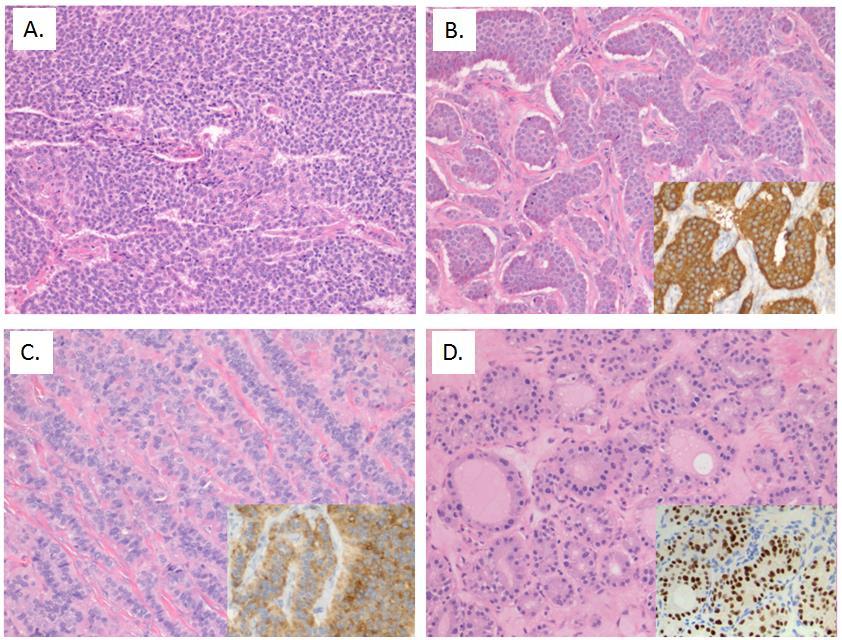
7 In summary, we describe a case of persistent hyperthyroidism after resection of struma carcinoid in a 59 year old woman, leading to diagnosis of Graves disease. To our knowledge this is the first reported case of co-existing struma carcinoid and Graves disease, and emphasizes the importance of monitoring thyroid function after resection of ovarian tumors containing thyroid tissue. Figure 1. Ovarian mass pathology specimen. Photomicrographs and inserts at 200X magnification. Staining performed with hematoxylin and eosin, and as otherwise described. A-C. Neuroendocrine component (ovarian carcinoid), low-grade neoplasm. Neuroendocrine cells with uniform nuclei and low mitotic rate demonstrate solid (A), insular (B), and trabecular (C) patterns, with staining positive for chromogranin (part B inset) and synaptophysin (part C inset). D. Thyroid component (struma ovarii), benign. Thyroid tissue within the ovarian mass demonstrates normal colloid follicles, with staining positive for TTF-1 (inset) and thyroglobulin (not shown). Taken together, these findings are consistent with struma carcinoid.
8


9 Figure 2. Thyroid and whole body uptake and scan 6 months after struma carcinoid resection. A. Cervical scan. The thyroid gland demonstrates diffusely increased, minimally inhomogeneous 123 I uptake bilaterally and in the pyramidal lobe. RAO: right anterior oblique. LAO: left anterior oblique. B. Whole body 123 I scan (anterior, left; posterior, right). Physiologic uptake is demonstrated in the neck, with expected concentration in the gastrointestintal tract and bladder. No pathologic uptake is seen in the abdomen or pelvis. A. B.
10 References 1. Clement PB and Young RH, eds. Atlas of Gynecologic Pathology. 3rd ed. London, UK: Saunders Elsevier, Roth LM, Talerman A. The enigma of struma ovarii. Pathology. 2007;39: Mutter GL and Prat JD, eds. Pathology of the Female Reproductive Tract. 3rd ed. Edinburgh, UK: Churchill Livingstone, Gorin I, Sastre-Garau X. Struma carcinoid of the ovary. J Clin Oncol. 2008;26: Sitasuwan T, Hanamornroongruang S, Peerapatdit T, Thongtang N. Coexistence of Graves disease and unilateral functioning struma ovarii: a case report. BMC Endocr Disord. 2015;15: Anastasilakis AD, Ruggeri RM, Polyzos SA, et al. Coexistence of Graves disease, papillary thyroid cancer and unilateral benign struma ovarii: case report and review of the literature. Metabolism. 2013:62: Teale E, Gouldesbrough DR, Peacey SR. Graves disease and coexisting struma ovarii: struma expression of thyrotropin receptors and the presence of thyrotropin receptor stimulating antibodies. Thyroid. 2006;16: Mimura Y, Kishida M, Masuyama H, et al. Coexistence of Graves disease and struma ovarii: case report and literature review. Endocr J. 2001;48: Ciccarelli A, Valdes-Socin H, Parma J et al. Thyrotoxic adenoma followed by atypical hyperthyroidism due to struma ovarii: clinical and genetic studies. Eur J Endocr. 2004;150: Lenicek T, Tomas D, Soljacić-Vranes H, et al. Struma carcinoid of the ovary: report of two cases. Acta Clin Croat. 2012;51: Robboy SJ, Scully RE. Strumal carcinoid of the ovary: An analysis of 50 cases of a distinctive tumor composed of thyroid tissue and carcinoid. Cancer. 1980;46:
11 12. Armes JE, Ostor AG. A case of malignant struma carcinoid. Gynecol Oncol. 1993;51: Baker PM, Oliva E, Young RH, Talerman A, Scully RE. Ovarian mucinous carcinomas including some with a carcinomatous component. Am J Surg Pathol. 2001;25:
Case Report A Hormonally Active Malignant Struma Ovarii
 Case Reports in Oncological Medicine Volume 2016, Article ID 2643470, 4 pages http://dx.doi.org/10.1155/2016/2643470 Case Report A Hormonally Active Malignant Struma Ovarii Carolina Lara, 1 Dalia Cuenca,
Case Reports in Oncological Medicine Volume 2016, Article ID 2643470, 4 pages http://dx.doi.org/10.1155/2016/2643470 Case Report A Hormonally Active Malignant Struma Ovarii Carolina Lara, 1 Dalia Cuenca,
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Department of Pathology, Breast, and Gynecologic Pathology, Magee-Womens Hospital of UPMC, PA 15213, USA
 Case Reports in Obstetrics and Gynecology Volume 2012, Article ID 269489, 5 pages doi:10.1155/2012/269489 Case Report Malignant Transformation of a Mature Cystic Ovarian Teratoma into Thyroid Carcinoma,
Case Reports in Obstetrics and Gynecology Volume 2012, Article ID 269489, 5 pages doi:10.1155/2012/269489 Case Report Malignant Transformation of a Mature Cystic Ovarian Teratoma into Thyroid Carcinoma,
PROLIFERATIVE HIGHLY DIFFERENTIATED FOLLICULAR CARCINOMA OF OVARIAN ORIGIN (HDFCO) PRESENTING LONG AFTER BILATERAL OOPHORECTOMY
 PRESENTING LONG AFTER BILATERAL OOPHORECTOMY") Case Report PROLIFERATIVE HIGHLY DIFFERENTIATED FOLLICULAR CARCINOMA OF OVARIAN ORIGIN (HDFCO) PRESENTING LONG AFTER BILATERAL OOPHORECTOMY Natalie M. Liu, BS 1 ; Neda Moatamed, MD 1 ; Racquel S. Bueno,
Case Report PROLIFERATIVE HIGHLY DIFFERENTIATED FOLLICULAR CARCINOMA OF OVARIAN ORIGIN (HDFCO) PRESENTING LONG AFTER BILATERAL OOPHORECTOMY Natalie M. Liu, BS 1 ; Neda Moatamed, MD 1 ; Racquel S. Bueno,
5/3/2017. Ahn et al N Engl J Med 2014; 371
 Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Alan Failor, M.D. Clinical Professor of Medicine Division of Metabolism, Endocrinology and Nutrition University of Washington April 20, 2017 No disclosures to report 1. Appropriately evaluate s in adult
Case Report Poorly Differentiated Thyroid Carcinoma Arising in Struma Ovarii
 Hindawi Publishing Corporation Case Reports in Pathology Volume 2015, Article ID 826978, 6 pages http://dx.doi.org/10.1155/2015/826978 Case Report Poorly Differentiated Thyroid Carcinoma Arising in Struma
Hindawi Publishing Corporation Case Reports in Pathology Volume 2015, Article ID 826978, 6 pages http://dx.doi.org/10.1155/2015/826978 Case Report Poorly Differentiated Thyroid Carcinoma Arising in Struma
A rare case of solitary toxic nodule in a 3yr old female child a case report
 Volume 3 Issue 1 2013 ISSN: 2250-0359 A rare case of solitary toxic nodule in a 3yr old female child a case report *Chandrasekaran Maharajan * Poongkodi Karunakaran *Madras Medical College ABSTRACT A three
Volume 3 Issue 1 2013 ISSN: 2250-0359 A rare case of solitary toxic nodule in a 3yr old female child a case report *Chandrasekaran Maharajan * Poongkodi Karunakaran *Madras Medical College ABSTRACT A three
An Unexpected Cause of Hypoglycemia
 An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination
 Endocrine Journal 2008, 55 (5), 889 894 Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination YASUHIRO ITO, TOMONORI
Endocrine Journal 2008, 55 (5), 889 894 Distant and Lymph Node Metastases of Thyroid Nodules with No Pathological Evidence of Malignancy: A Limitation of Pathological Examination YASUHIRO ITO, TOMONORI
A Rare Case of Peritoneal Spread of Benign Struma Ovarii with Thyrotoxicosis
 Case Report www.jbcrs.org A Rare Case of Peritoneal Spread of Benign Struma Ovarii with Thyrotoxicosis Abhijeet Ingle *, Vijaya Gattu, Suhela Rachakonda, Sachin Subhash Marda Yashoda Hospital, Hyderabad,
Case Report www.jbcrs.org A Rare Case of Peritoneal Spread of Benign Struma Ovarii with Thyrotoxicosis Abhijeet Ingle *, Vijaya Gattu, Suhela Rachakonda, Sachin Subhash Marda Yashoda Hospital, Hyderabad,
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging. Deepa R Biyyam, MD Attending Pediatric Radiologist
 Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Imaging in Pediatric Thyroid disorders: US and Radionuclide imaging Deepa R Biyyam, MD Attending Pediatric Radiologist Imaging in Pediatric Thyroid disorders: Imaging modalities Outline ACR-SNM-SPR guidelines
Thyroid Nodule. Disclosure. Learning Objectives P A P A P A 3/18/2014. Nothing to disclose.
 Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Thyroid Nodule Evaluating the patient with a thyroid nodule and some management options. Miguel V. Valdez PA C Disclosure Nothing to disclose. Learning Objectives Examination of thyroid gland Options for
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Evaluation and Management of Thyroid Nodules. Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada
 Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Thyroid Nodules. Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA
 Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
Thyroid Nodules ENDOCRINOLOGY DIVISION ENDOCRINOLOGY DIVISION Dr. HAKIMI, SpAK Dr. MELDA DELIANA, SpAK Dr. SISKA MAYASARI LUBIS, SpA Anatomical Considerations The Thyroid Nodule Congenital anomalies Thyroglossal
ASJ. Spinal Metastasis from Struma Ovarii: Case Report and Review of the Literature. Asian Spine Journal. Introduction
 Asian Spine Journal Asian Spine Case Journal Report Asian Spine J 2015;9(2):281-285 Thoracic http://dx.doi.org/10.4184/asj.2015.9.2.281 metastasis of struma ovarii 281 Spinal Metastasis from Struma Ovarii:
Asian Spine Journal Asian Spine Case Journal Report Asian Spine J 2015;9(2):281-285 Thoracic http://dx.doi.org/10.4184/asj.2015.9.2.281 metastasis of struma ovarii 281 Spinal Metastasis from Struma Ovarii:
Adjuvant therapy for thyroid cancer
 Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Case Scenario 1. Pathology report Specimen from mediastinoscopy Final Diagnosis : Metastatic small cell carcinoma with residual lymphatic tissue
 Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Thyroid pathology Practical part
 Thyroid pathology Practical part My Algorithm After a good macroscopy and a microscopic overview of the lesion, I especially look at the capsule and the thyroid just above and just beneath the capsule.
Thyroid pathology Practical part My Algorithm After a good macroscopy and a microscopic overview of the lesion, I especially look at the capsule and the thyroid just above and just beneath the capsule.
Differentiated Thyroid Cancer: Initial Management
 Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Page 1 ATA HOME GIVE ONLINE ABOUT THE ATA JOIN THE ATA MEMBER SIGN-IN INFORMATION FOR PATIENTS FIND A THYROID SPECIALIST Home Management Guidelines for Patients with Thyroid Nodules and Differentiated
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Ovarian Lesion Benign vs Malignant?
 Ovarian Lesion Benign vs Malignant? Michele Keenan 1,2 Bernice Dunne 2 Mary Moran 1 Therese Herlihy 1 1. Radiography and Diagnostic Imaging, School of Medicine, University College Dublin, Ireland 2. Midland
Ovarian Lesion Benign vs Malignant? Michele Keenan 1,2 Bernice Dunne 2 Mary Moran 1 Therese Herlihy 1 1. Radiography and Diagnostic Imaging, School of Medicine, University College Dublin, Ireland 2. Midland
Chapter 2: Initial treatment for endometrial cancer (including histologic variant type)
") Chapter 2: Initial treatment for endometrial cancer (including histologic variant type) CQ01 Which surgical techniques for hysterectomy are recommended for patients considered to be stage I preoperatively?
Chapter 2: Initial treatment for endometrial cancer (including histologic variant type) CQ01 Which surgical techniques for hysterectomy are recommended for patients considered to be stage I preoperatively?
Malignant transformation in benign cystic teratomas, dermoids of the ovary
 European JournalofObstetrics& Gynecology andreproductivebiology, 29 (1988) 197-206 197 Elsevier EJO 00716 Malignant transformation in benign cystic teratomas, dermoids of the ovary S. Chadha 1 and A. Schaberg
European JournalofObstetrics& Gynecology andreproductivebiology, 29 (1988) 197-206 197 Elsevier EJO 00716 Malignant transformation in benign cystic teratomas, dermoids of the ovary S. Chadha 1 and A. Schaberg
Mandana Moosavi 1 and Stuart Kreisman Background
 Case Reports in Endocrinology Volume 2016, Article ID 6471081, 4 pages http://dx.doi.org/10.1155/2016/6471081 Case Report A Case Report of Dramatically Increased Thyroglobulin after Lymph Node Biopsy in
Case Reports in Endocrinology Volume 2016, Article ID 6471081, 4 pages http://dx.doi.org/10.1155/2016/6471081 Case Report A Case Report of Dramatically Increased Thyroglobulin after Lymph Node Biopsy in
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Thyroid nodules - medical and surgical management. Endocrinology and Endocrine Surgery Manchester Royal Infirmary
 Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
Thyroid nodules - medical and surgical management JRE Davis NR Parrott Endocrinology and Endocrine Surgery Manchester Royal Infirmary Thyroid nodules - prevalence Thyroid nodules common, increase with
STRUMAL CARCINOID OF THE OVARY: REPORT OF TWO CASES *
 Acta Clin Croat 2012; 51:649-653 Case Report STRUMAL CARCINOID OF THE OVARY: REPORT OF TWO CASES * Tanja Leniček 1, Davor Tomas 1,3, Hrvojka Soljačić-Vraneš 2, Zdenko Kraljević 2, Petar Klarić 2, Milan
Acta Clin Croat 2012; 51:649-653 Case Report STRUMAL CARCINOID OF THE OVARY: REPORT OF TWO CASES * Tanja Leniček 1, Davor Tomas 1,3, Hrvojka Soljačić-Vraneš 2, Zdenko Kraljević 2, Petar Klarić 2, Milan
Disclosures. Learning objectives. Case 1A. Autoimmune Thyroid Disease: Medical and Surgical Issues. I have nothing to disclose.
 Disclosures Autoimmune Thyroid Disease: Medical and Surgical Issues I have nothing to disclose. Chrysoula Dosiou, MD, MS Clinical Assistant Professor Division of Endocrinology Stanford University School
Disclosures Autoimmune Thyroid Disease: Medical and Surgical Issues I have nothing to disclose. Chrysoula Dosiou, MD, MS Clinical Assistant Professor Division of Endocrinology Stanford University School
Article begins on next page
 Pseudopapillary Granulosa Cell Tumor: A Case of This Rare Subtype Rutgers University has made this article freely available. Please share how this access benefits you. Your story matters. [https://rucore.libraries.rutgers.edu/rutgers-lib/50622/story/]
Pseudopapillary Granulosa Cell Tumor: A Case of This Rare Subtype Rutgers University has made this article freely available. Please share how this access benefits you. Your story matters. [https://rucore.libraries.rutgers.edu/rutgers-lib/50622/story/]
Medical Sciences, 4301 W Markham Street, Little Rock, AR 72205, USA. Correspondence should be addressed to Syed A. Abid;
 Case Reports in Endocrinology, Article ID 584513, 6 pages http://dx.doi.org/10.1155/2014/584513 Case Report Metastatic Follicular Thyroid Carcinoma Secreting Thyroid Hormone and Radioiodine Avid without
Case Reports in Endocrinology, Article ID 584513, 6 pages http://dx.doi.org/10.1155/2014/584513 Case Report Metastatic Follicular Thyroid Carcinoma Secreting Thyroid Hormone and Radioiodine Avid without
Approach to Thyroid Nodules
 Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Management guideline for patients with differentiated thyroid cancer. Teeraporn Ratanaanekchai ENT, KKU 17 October 2007
 Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
AN INTRODUCTION TO NUCLEAR MEDICINE
 AN INTRODUCTION TO NUCLEAR MEDICINE WITH RESPECT TO THYROID DISORDERS By: B.Shafiei MD Nuclear Physician Taleghani Medical Center Radioactive: An element with Unstable Nucleus (Excess Energy), can achieve
AN INTRODUCTION TO NUCLEAR MEDICINE WITH RESPECT TO THYROID DISORDERS By: B.Shafiei MD Nuclear Physician Taleghani Medical Center Radioactive: An element with Unstable Nucleus (Excess Energy), can achieve
Case 5: Thyroid cancer in 42 yr-old woman with Graves disease
 Case 5: Thyroid cancer in 42 yr-old woman with Graves disease Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) Thyroid cancer in 42 yr-old woman with
Case 5: Thyroid cancer in 42 yr-old woman with Graves disease Giuliano Mariani Regional Center of Nuclear Medicine, University of Pisa Medical School, Pisa (Italy) Thyroid cancer in 42 yr-old woman with
Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
 yroid Research, Article ID 818134, 4 pages http://dx.doi.org/10.1155/2014/818134 Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
yroid Research, Article ID 818134, 4 pages http://dx.doi.org/10.1155/2014/818134 Research Article Papillary Thyroid Cancer, Macrofollicular Variant: The Follow-Up and Analysis of Prognosis of 5 Patients
Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms
 Hindawi Publishing Corporation Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
Hindawi Publishing Corporation Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
Medullary Thyroid Carcinoma. This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands
 Medullary Thyroid Carcinoma This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands ADS-01504 Rev. 001 2016 Hologic, Inc. All rights reserved. Overview Medullary Thyroid Carcinoma
Medullary Thyroid Carcinoma This case was provided by Treant Hospital, Bethesda, Hoogeveen, The Netherlands ADS-01504 Rev. 001 2016 Hologic, Inc. All rights reserved. Overview Medullary Thyroid Carcinoma
Thyroid Cancer: Imaging Techniques (Nuclear Medicine)
") Thyroid Cancer: Imaging Techniques (Nuclear Medicine) Andrei Iagaru, MD MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology Introduction Ø There are
Thyroid Cancer: Imaging Techniques (Nuclear Medicine) Andrei Iagaru, MD MIPS Molecular Imaging Program at Stanford Stanford University School of Medicine Department of Radiology Introduction Ø There are
Thyrotoxicosis from Metastatic Lung Cancer to the Thyroid Gland: A case report
 CLINICAL VIGNETTE Thyrotoxicosis from Metastatic Lung Cancer to the Thyroid Gland: A case report Archana Sadhu, MD and Dorothy Martinez, MD Introduction Thyrotoxicosis from secondary thyroid cancer metastases
CLINICAL VIGNETTE Thyrotoxicosis from Metastatic Lung Cancer to the Thyroid Gland: A case report Archana Sadhu, MD and Dorothy Martinez, MD Introduction Thyrotoxicosis from secondary thyroid cancer metastases
Thyroid nodules. Most thyroid nodules are benign
 Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Thyroid nodules Postgraduate Course in General Surgery Jessica E. Gosnell MD Assistant Professor March 22, 2011 Most thyroid nodules are benign thyroid nodules occur in 77% of the world s population palpable
Calcitonin. 1
 Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
Calcitonin Medullary thyroid carcinoma (MTC) is characterized by a high concentration of serum calcitonin. Routine measurement of serum calcitonin concentration has been advocated for detection of MTC
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
Thyroid Cancer (Carcinoma)
") Information for Patients Thyroid Cancer (Carcinoma) Prepared by the American Association of Clinical Endocrinologists (AACE), a not-for-profit national organization of highly qualified specialists in hormonal
Information for Patients Thyroid Cancer (Carcinoma) Prepared by the American Association of Clinical Endocrinologists (AACE), a not-for-profit national organization of highly qualified specialists in hormonal
Pitfalls in thyroid tumor pathology. Prof.Valdi Pešutić-Pisac MD, PhD
 Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Pitfalls in thyroid tumor pathology Prof.Valdi Pešutić-Pisac MD, PhD Too many or... Tumour herniation through a torn capsule simulating capsular invasion fibrous capsule with a sharp discontinuity, suggestive
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases
 Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
Women s Health in General Practice Symposium 2015 Thyroid & Parathyroid Cases Bill Fleming Epworth Freemasons Hospital 1 Common Endocrine Presentations anatomical problems thyroid nodule / goitre embryological
HYPERTHYROIDISM. Hypothalamus. Thyrotropin-releasing hormone (TRH) Anterior pituitary gland. Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3
 Anterior pituitary gland. Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3") HYPERTHYROIDISM Hypothalamus Thyrotropin-releasing hormone (TRH) Anterior pituitary gland Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3 In hyperthyroidism, there is an increased production of
HYPERTHYROIDISM Hypothalamus Thyrotropin-releasing hormone (TRH) Anterior pituitary gland Thyroid-stimulating hormone (TSH) Thyroid gland T4, T3 In hyperthyroidism, there is an increased production of
Port-Site Metastases After Robotic Surgery for Gynecologic Malignancy
 SCIENTIFIC PAPER Port-Site Metastases After Robotic Surgery for Gynecologic Malignancy Noah Rindos, MD, Christine L. Curry, MD, PhD, Rami Tabbarah, MD, Valena Wright, MD ABSTRACT Background and Objectives:
SCIENTIFIC PAPER Port-Site Metastases After Robotic Surgery for Gynecologic Malignancy Noah Rindos, MD, Christine L. Curry, MD, PhD, Rami Tabbarah, MD, Valena Wright, MD ABSTRACT Background and Objectives:
Survival Analysis and Prognosis for Patients with Serous and Mucinous Borderline Ovarian Tumors: 14-Year Experience from a Tertiary Center in Iran
 ORIGINAL ARTICLE Survival Analysis and Prognosis for Patients with Serous and Mucinous Borderline Ovarian Tumors: 14-Year Experience from a Tertiary Center in Iran Katayoun Ziari, Ebrahim Soleymani, and
ORIGINAL ARTICLE Survival Analysis and Prognosis for Patients with Serous and Mucinous Borderline Ovarian Tumors: 14-Year Experience from a Tertiary Center in Iran Katayoun Ziari, Ebrahim Soleymani, and
THYROID CANCER IN CHILDREN. Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine
 THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
THYROID CANCER IN CHILDREN Humberto Lugo-Vicente MD FACS FAAP Professor Pediatric Surgery UPR School of Medicine Thyroid nodules Rare Female predominance 4-fold as likely to be malignant Hx Radiation exposure?
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines
 2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
2015 American Thyroid Association Thyroid Nodule and Cancer Guidelines Angela M. Leung, MD, MSc, ECNU November 5, 2016 Outline Workup of nontoxic thyroid nodule(s) Ultrasound FNAB Management of FNAB results
Nuclear Medicine Head and Neck Region. Bán Zsuzsanna, MD University of Pécs, Department of Nuclear Medicine
 Nuclear Medicine Head and Neck Region Bán Zsuzsanna, MD University of Pécs, Department of Nuclear Medicine Thyroid scintigraphy Parathyroid scintigraphy F18-FDG PET examinations in head and neck cancer
Nuclear Medicine Head and Neck Region Bán Zsuzsanna, MD University of Pécs, Department of Nuclear Medicine Thyroid scintigraphy Parathyroid scintigraphy F18-FDG PET examinations in head and neck cancer
- RET/PTC rearrangement: 20% papillary thyroid cancer - RET: medullary thyroid cancer
 Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Thyroid Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: 1. Lenvina is the first line therapy with powerful durable response and superior PFS in pts with RAI-refractory disease.
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Chapter 8 Adenocarcinoma
 Page 80 Chapter 8 Adenocarcinoma Overview In Japan, the proportion of squamous cell carcinoma among all cervical cancers has been declining every year. In a recent survey, non-squamous cell carcinoma accounted
Page 80 Chapter 8 Adenocarcinoma Overview In Japan, the proportion of squamous cell carcinoma among all cervical cancers has been declining every year. In a recent survey, non-squamous cell carcinoma accounted
Approach to thyroid dysfunction
 Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Approach to thyroid dysfunction Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or
Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms
 Case Reports in Pathology Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
Case Reports in Pathology Volume 2015, Article ID 153932, 5 pages http://dx.doi.org/10.1155/2015/153932 Case Report Tumor-to-Tumor Metastasis: Lung Carcinoma Metastasizing to Thyroid Neoplasms Shiuan-Li
Thyroid nodules 3/22/2011. Most thyroid nodules are benign. Thyroid nodules: differential diagnosis
 Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
Most thyroid nodules are benign Thyroid nodules Postgraduate Course in General Surgery thyroid nodules occur in 77% of the world s population palpable thyroid nodules occur in about 5% of women and 1%
American Journal of Oral Medicine and Radiology
 American Journal of Oral Medicine and Radiology e - ISSN - XXXX-XXXX ISSN - 2394-7721 Journal homepage: www.mcmed.us/journal/ajomr ULTRASONOGRAPHIC EVALUATION OF ADNEXAL MASSES Nageswar Rao* Professor,
American Journal of Oral Medicine and Radiology e - ISSN - XXXX-XXXX ISSN - 2394-7721 Journal homepage: www.mcmed.us/journal/ajomr ULTRASONOGRAPHIC EVALUATION OF ADNEXAL MASSES Nageswar Rao* Professor,
Nuclear medicine in endocrinology
 Nuclear medicine in endocrinology Thyroid gland: anatomy, function, inflammation, Nuclear medicine in endocrinology tumor dignitiy Parathyroid gland: localisation Adrenal cortex: function Adrenal medulla:
Nuclear medicine in endocrinology Thyroid gland: anatomy, function, inflammation, Nuclear medicine in endocrinology tumor dignitiy Parathyroid gland: localisation Adrenal cortex: function Adrenal medulla:
Index. radiologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
Index Note: Page numbers of article titles are in boldface type. A ACC. See Adrenal cortical carcinoma. Acromegaly and the pituitary gland, 551 Acute suppurative thyroiditis, 405, 406 Addison, Thomas and
THYROID AWARENESS. By: Karen Carbone. January is thyroid awareness month. At least 30 million Americans
 THYROID AWARENESS By: Karen Carbone January is thyroid awareness month. At least 30 million Americans have a thyroid disorder and half-15 million-are silent sufferers who are undiagnosed, according to
THYROID AWARENESS By: Karen Carbone January is thyroid awareness month. At least 30 million Americans have a thyroid disorder and half-15 million-are silent sufferers who are undiagnosed, according to
بسم هللا الرحمن الرحيم. Prof soha Talaat
 بسم هللا الرحمن الرحيم Ovarian tumors The leading indication for gynecologic surgery. Preoperative characterization of complex solid and cystic adnexal masses is crucial for informing patients about possible
بسم هللا الرحمن الرحيم Ovarian tumors The leading indication for gynecologic surgery. Preoperative characterization of complex solid and cystic adnexal masses is crucial for informing patients about possible
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS
 AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
AGGRESSIVE VARIANTS OF PAPILLARY THYROID CARCINOMA DIAGNOSIS AND PROGNOSIS PAPILLARY THYROID CARCINOMA Clinical Any age Microscopic to large Female: Male= 2-4:1 Radiation history Lymph nodes Prognosis
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer
 Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
Ultrasound for Pre-operative Evaluation of Well Differentiated Thyroid Cancer Its Not Just About the Nodes AACE Advances in Medical and Surgical Management of Thyroid Cancer - 2017 Robert A. Levine, MD,
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
An asymptomatic malignant Struma ovarii at saint pierre clinic of Ottignies, Belgium
 An asymptomatic malignant Struma ovarii at saint pierre clinic of Ottignies, Belgium Guy Mulinganya, Renaud Poncin, Georgette Mulinganya, Anne-Philippe Draguet, Col Vincent, Longueville Etienne To cite
An asymptomatic malignant Struma ovarii at saint pierre clinic of Ottignies, Belgium Guy Mulinganya, Renaud Poncin, Georgette Mulinganya, Anne-Philippe Draguet, Col Vincent, Longueville Etienne To cite
Diseases of thyroid & parathyroid glands (1 of 2)
") Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
Diseases of thyroid & parathyroid glands (1 of 2) Thyroid diseases Thyrotoxicosis Hypothyroidism Thyroiditis Graves disease Goiters Neoplasms Chronic Lymphocytic (Hashimoto) Thyroiditis Subacute Granulomatous
Case Report Ovarian Metastasis from Lung Cancer: A Rare Entity
 Case Reports in Obstetrics and Gynecology Volume 2013, Article ID 378438, 4 pages http://dx.doi.org/10.1155/2013/378438 Case Report Ovarian Metastasis from Lung Cancer: A Rare Entity Huseyin Cengiz, Fükrü
Case Reports in Obstetrics and Gynecology Volume 2013, Article ID 378438, 4 pages http://dx.doi.org/10.1155/2013/378438 Case Report Ovarian Metastasis from Lung Cancer: A Rare Entity Huseyin Cengiz, Fükrü
One of the commonest gynecological cancers,especially in white Americans.
 Gynaecology Dr. Rozhan Lecture 6 CARCINOMA OF THE ENDOMETRIUM One of the commonest gynecological cancers,especially in white Americans. It is a disease of postmenopausal women with a peak incidence in
Gynaecology Dr. Rozhan Lecture 6 CARCINOMA OF THE ENDOMETRIUM One of the commonest gynecological cancers,especially in white Americans. It is a disease of postmenopausal women with a peak incidence in
PEDIATRIC Ariel Katz MD
 PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
PEDIATRIC Ariel Katz MD Dept. Otolaryngology Head &Neck Surgery Wolfson Medical Center Holon, Israel OBJECTIVES Overview/Background Epidemiology/Etiology Intro to Guidelines Workup Treatment Follow-Up
Page 289. Corresponding Author: Dr. Nitya Subramanian, Volume 3 Issue - 5, Page No
 ISSN- O: 2458-868X, ISSN P: 2458 8687 Index Copernicus Value: 49. 23 PubMed - National Library of Medicine - ID: 101731606 SJIF Impact Factor: 4.956 International Journal of Medical Science and Innovative
ISSN- O: 2458-868X, ISSN P: 2458 8687 Index Copernicus Value: 49. 23 PubMed - National Library of Medicine - ID: 101731606 SJIF Impact Factor: 4.956 International Journal of Medical Science and Innovative
A case of extremely rare ovarian tumor: Primary ovarian adenomyoma
 Kawasaki Medical Journal 233 A case of extremely rare ovarian tumor: Primary ovarian adenomyoma Shoji KAKU, Takuya MORIYA, Naoki KANOMATA, Tsuyoshi ISHIDA Yangsil CHANG, Norichika USHIODA, Yuichiro NAKAI
Kawasaki Medical Journal 233 A case of extremely rare ovarian tumor: Primary ovarian adenomyoma Shoji KAKU, Takuya MORIYA, Naoki KANOMATA, Tsuyoshi ISHIDA Yangsil CHANG, Norichika USHIODA, Yuichiro NAKAI
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Prostate Case Scenario 1
 Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Management of Thyroid Nodules
 Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
Management of Thyroid Nodules 38 y/o female with solid 1.5 cm right Thyroid nodule. TSH=0.68 Vincent J. Reid, MD., FACS Thyroid Cancer Incidence & Mortality 1974 to 2004 Overall Women Men Mortality 1 Cancer
5/18/2013. Most thyroid nodules are benign. Thyroid nodules: new techniques in evaluation
 Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
Most thyroid nodules are benign Thyroid nodules: new techniques in evaluation Incidence Etiology Risk factors Diagnosis Gene classification system Treatment Postgraduate Course in General Surgery Jessica
Tania Gallant MD, FRCPC Internal Medicine Update April
 Tania Gallant MD, FRCPC Internal Medicine Update April 28 2017 Disclosures Honoraria/Ad board: Sanofi-Aventis, Janssen, Merck Frosst, Eli-Lilly, Astra Zeneca, Boehringer-Ingelheim Objectives By the end
Tania Gallant MD, FRCPC Internal Medicine Update April 28 2017 Disclosures Honoraria/Ad board: Sanofi-Aventis, Janssen, Merck Frosst, Eli-Lilly, Astra Zeneca, Boehringer-Ingelheim Objectives By the end
Thyroid Nodules. Family Medicine Refresher Course Geeta Lal MD, FACS April 2, No financial disclosures
 Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
Thyroid Nodules Family Medicine Refresher Course Geeta Lal MD, FACS April 2, 2014 No financial disclosures Objectives Review epidemiology Work up of Thyroid nodules Indications for FNAB Evolving role of
THYROID FUNCTION TEST and RADIONUCLIDE THERAPY
 THYROID FUNCTION TEST and RADIONUCLIDE THERAPY Ajalaya Teyateeti, M.D. Division of Nuclear Medicine Department of Radiology I. Thyroid function test OUTLINE Application and interpretation of in vitro TFT
THYROID FUNCTION TEST and RADIONUCLIDE THERAPY Ajalaya Teyateeti, M.D. Division of Nuclear Medicine Department of Radiology I. Thyroid function test OUTLINE Application and interpretation of in vitro TFT
Role of peritoneal washing cytology in ovarian malignancies: correlation with histopathological parameters
 Naz et al. World Journal of Surgical Oncology (2015) 13:315 DOI 10.1186/s12957-015-0732-1 WORLD JOURNAL OF SURGICAL ONCOLOGY RESEARCH Open Access Role of peritoneal washing in ovarian malignancies: correlation
Naz et al. World Journal of Surgical Oncology (2015) 13:315 DOI 10.1186/s12957-015-0732-1 WORLD JOURNAL OF SURGICAL ONCOLOGY RESEARCH Open Access Role of peritoneal washing in ovarian malignancies: correlation
AACE 2018 Advanced Endocrine Neck Ultrasound and UGFNA Course
 AACE 2018 Advanced Endocrine Neck Ultrasound and UGFNA Course Describe the sonographic appearance of diffuse thyroid diseases: autoimmune thyroid disease Review non thyroidal findings that can be encountered
AACE 2018 Advanced Endocrine Neck Ultrasound and UGFNA Course Describe the sonographic appearance of diffuse thyroid diseases: autoimmune thyroid disease Review non thyroidal findings that can be encountered
Alvin C. Powers, M.D. 1/27/06
 Thyroid Histology Follicular Cells ECF side Apical lumen Thyroid Follicles -200-400 um Parafollicular or C-cells Colloid Photos from University of Manchester and tutorial created by Dr. James Crimando,
Thyroid Histology Follicular Cells ECF side Apical lumen Thyroid Follicles -200-400 um Parafollicular or C-cells Colloid Photos from University of Manchester and tutorial created by Dr. James Crimando,
BRANCHIAL CLEFT CYST AS THE INITIAL IMPRESSION OF A METASTATIC THYROID PAPILLARY CARCINOMA: TWO CASE REPORTS
 RCHIL CLEFT CYST S THE IITIL IMPRESSIO OF METSTTIC THYROID PPILLRY CRCIOM: TWO CSE REPORTS Hung-Sheng Chi, 1 Ling-Feng Wang, 1 Feng-Yu Chiang, 1,2 Wen-Rei Kuo, 1,2 and Ka-Wo Lee 1,2 1 Department of Otolaryngology,
RCHIL CLEFT CYST S THE IITIL IMPRESSIO OF METSTTIC THYROID PPILLRY CRCIOM: TWO CSE REPORTS Hung-Sheng Chi, 1 Ling-Feng Wang, 1 Feng-Yu Chiang, 1,2 Wen-Rei Kuo, 1,2 and Ka-Wo Lee 1,2 1 Department of Otolaryngology,
Decoding Your Thyroid Tests and Results
 Decoding Your Thyroid Tests and Results Wondering about your thyroid test results? Learn about each test and what low, optimal, and high results may mean so you can work with your doctor to choose appropriate
Decoding Your Thyroid Tests and Results Wondering about your thyroid test results? Learn about each test and what low, optimal, and high results may mean so you can work with your doctor to choose appropriate
Shadow because the air
 Thyroid Ultrasound Thyroid US examination needs: 1. high frequency transducer 2. extended patient's neck 3. check all the neck area because the swelling could be in areas other than the thyroid such as
Thyroid Ultrasound Thyroid US examination needs: 1. high frequency transducer 2. extended patient's neck 3. check all the neck area because the swelling could be in areas other than the thyroid such as
Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events
 Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events Sandrine Rorive, M.D., PhD. Erasme Hospital - Université Libre de Bruxelles (ULB) INTRODUCTION The assessment of thyroid nodules
Ultrasound-Guided Fine-Needle Aspiration of Thyroid Nodules: New events Sandrine Rorive, M.D., PhD. Erasme Hospital - Université Libre de Bruxelles (ULB) INTRODUCTION The assessment of thyroid nodules
Unusual Osteoblastic Secondary Lesion as Predominant Metastatic Disease Spread in Two Cases of Uterine Leiomyosarcoma
 49 Unusual Osteoblastic Secondary Lesion as Predominant Metastatic Disease Spread in Two Cases of Uterine Leiomyosarcoma Loredana Miglietta a Maria Angela Parodi b Luciano Canobbio b Luca Anselmi c a Medical
49 Unusual Osteoblastic Secondary Lesion as Predominant Metastatic Disease Spread in Two Cases of Uterine Leiomyosarcoma Loredana Miglietta a Maria Angela Parodi b Luciano Canobbio b Luca Anselmi c a Medical
REPORT. Introduction. Dongbin Ahn 1, Jin Ho Sohn 1 and Ji Young Park 2
 C A S E REPORT ISSN: 2005-162X J Korean Thyroid Assoc 2013 May 6(1): 80-84 http://dx.doi.org/10.11106/jkta.2013.6.1.80 A Case of Concurrent Papillary and Medullary Thyroid Carcinomas Detected as Recurrent
C A S E REPORT ISSN: 2005-162X J Korean Thyroid Assoc 2013 May 6(1): 80-84 http://dx.doi.org/10.11106/jkta.2013.6.1.80 A Case of Concurrent Papillary and Medullary Thyroid Carcinomas Detected as Recurrent
SEER Summary Stage Still Here!
 SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
Appendix cancer mimicking ovarian cancer
 Int J Gynecol Cancer 2002, 12, 768 772 CORRESPONDENCE AND BRIEF REPORTS Appendix cancer mimicking ovarian cancer P. A. GEHRIG *, J. F. BOGGESS*, D. W. OLLILA, P. A. GROBEN & L. VAN LE* *Division of Gynecologic
Int J Gynecol Cancer 2002, 12, 768 772 CORRESPONDENCE AND BRIEF REPORTS Appendix cancer mimicking ovarian cancer P. A. GEHRIG *, J. F. BOGGESS*, D. W. OLLILA, P. A. GROBEN & L. VAN LE* *Division of Gynecologic
Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES CASE 1: FEMALE REPRODUCTIVE
 Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES PHYSICAL EXAMINATION CASE 1: FEMALE REPRODUCTIVE 3/5 Patient presents through the emergency room with
Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES PHYSICAL EXAMINATION CASE 1: FEMALE REPRODUCTIVE 3/5 Patient presents through the emergency room with
Subacute Thyroiditis with Coexisting Papillary Carcinoma
 C A S E REPORT J Korean Thyroid Assoc Vol. 4, No. 1, May 2011 Subacute Thyroiditis with Coexisting Papillary Carcinoma Pil-Soo Sung, MD 1, Min-Hee Kim, MD 1, Dong-Jun Lim, MD 1, Yoon-Hee Choi, MD 1, Moo-Il
C A S E REPORT J Korean Thyroid Assoc Vol. 4, No. 1, May 2011 Subacute Thyroiditis with Coexisting Papillary Carcinoma Pil-Soo Sung, MD 1, Min-Hee Kim, MD 1, Dong-Jun Lim, MD 1, Yoon-Hee Choi, MD 1, Moo-Il
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS. BY: Shifaa Qa qa
 NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
NEOPLASMS OF THE THYROID PATHOLOGY OF PARATHYROID GLANDS BY: Shifaa Qa qa Neoplasmas of the thyroid thyroid nodules Neoplastic ---- benign, malignant Non neoplastic Solitary nodules ----- neoplastic Nodules
AACE/ACE Principles of Endocrine Neck Sonography Course
 AACE/ACE Principles of Endocrine Neck Sonography Course Primary objective of thyroid ultrasound: assess for malignant disease Nodular Disease Benign Malignant Goiter Iodine deficient Thyroiditis Organification
AACE/ACE Principles of Endocrine Neck Sonography Course Primary objective of thyroid ultrasound: assess for malignant disease Nodular Disease Benign Malignant Goiter Iodine deficient Thyroiditis Organification
Case Scenario 1. 4/19/13 Bone Scan: No scintigraphic findings to suggest skeletal metastases.
 Case Scenario 1 3/8/13 H&P 68 YR W/M presents w/elevated PSA. Patient is a non-smoker, current alcohol use. Physical Exam: On digital rectal exam the sphincter tone is normal and there is a 1 cm nodule
Case Scenario 1 3/8/13 H&P 68 YR W/M presents w/elevated PSA. Patient is a non-smoker, current alcohol use. Physical Exam: On digital rectal exam the sphincter tone is normal and there is a 1 cm nodule
Issue Date Right.
 NAOSITE: Nagasaki University's Ac Title Aggressive ovarian plasmacytoma res Author(s) Yamasaki, Kentaro; Miura, Kiyonori; Citation Acta medica Nagasakiensia, 58(1), p Issue Date 2013-04 URL http://hdl.handle.net/10069/32064
NAOSITE: Nagasaki University's Ac Title Aggressive ovarian plasmacytoma res Author(s) Yamasaki, Kentaro; Miura, Kiyonori; Citation Acta medica Nagasakiensia, 58(1), p Issue Date 2013-04 URL http://hdl.handle.net/10069/32064