IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and Diabetes Atlas -sixth Edition: IDF 2013
|
|
|
- Kimberly Taylor
- 6 years ago
- Views:
Transcription
1
2 IDF Regions and global projections of the number of people with diabetes (20-79 years), 2013 and 2035 Diabetes Atlas -sixth Edition: IDF 2013
3 Diabetes Atlas -sixth Edition: IDF 2013
4
5 Chronic complications 400 Diab. Patients (HMC) Retinopathy Nephropathy Neuropathy Cardiovascular Qatar Medical Journal, Vol. 12. No. 2, Dec. 2003
6 Diabetes Atlas -sixth Edition: IDF 2013
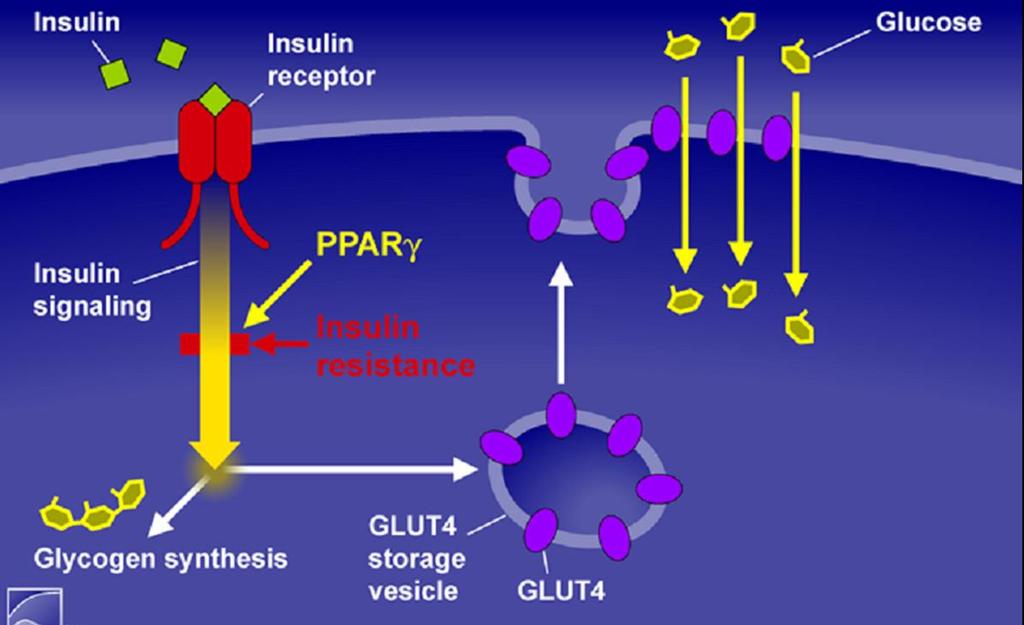
 Glucose output Glucose uptake Liver Blood glucose Muscle Adipose")
7 Insulin and Glucagon Regulate Normal Glucose Homeostasis Fasting state Glucagon (α cell) Fed state Pancreas Insulin (β cell) Glucose output Glucose uptake Liver Blood glucose Muscle Adipose tissue
8 Major Pathophysiologic Defects in Type 2 Diabetes Islet-cell Dysfunction Glucagon (α cell) Pancreas Hepatic glucose output Liver Insulin (β cell) Hyperglycemia Insulin resistance Glucose uptake Muscle Adipose tissue




9 Proportion Not Experiencing Secondary Failure SECONDARY FAILURE OF ETFORMIN MONOTHERAPY (N=1051) BY DURATION OF DIABETES AT METFORMIN INITIATION Months 21.4% year 0-3 Months 12.2% year 4-11 Months 17.7% year Months 18.4% year 0.2 > 36 Months 21.9% year Months on Metformin Brown et al, Diabetes Care 33: , 2010
 Alvarsson (n=48) RECORD (n=272) Hanefeld (n=250) Charbonnel (n=313) UKPDS (n=1,573) Chicago (n=230) ADOPT (n=1,441) PERISCOPE (n=181) Tan (n=297) 0 1 2 3 4 5 6 10 TIME")
10 Change in HbA1c (%) DURABILITY OF GLYCEMIC CONTROL WITH Sulfonylurea Glyburide Glimepiride SU Glyburide GLY SU Gliclazide Glyburide Gliclazide Glyburide Alvarsson (n=39) Alvarsson (n=48) RECORD (n=272) Hanefeld (n=250) Charbonnel (n=313) UKPDS (n=1,573) Chicago (n=230) ADOPT (n=1,441) PERISCOPE (n=181) Tan (n=297) TIME (years)
11 SULFONYLUREAS and coronary disease outcomes sulfonylurea and metformin monotherapy on cardiovascular events in type 2 diabetes mellitus: Retrospective cohort study CVD outcomes (acute myocardial infarction and stroke) or death. Among patients initiating treatment ( with sulfonylurea therapy and with metformin therapy composite outcome were 18.2 per 1000 person-years in sulfonylurea users and 10.4 per 1000 person-years in metformin. More CVD events with sulfonylureas per 1000 person-years; adjusted hazard ratio [ahr], 1.21 [CI, 1.13 to 1.30]). Results were consistent for both glyburide (ahr, 1.26 [CI, 1.16 to 1.37]) and glipizide (ahr, 1.15 [CI, 1.06 to 1.26]) Ann Intern Med. 2012
12 SULFONYLUREAS and coronary disease outcomes : Newer sulfonylureas All Danish residents>20 years, initiating single-agent sulfonylurea or metformin between 1997 and 2006 were followed for up to 9 years (median 3.3 years) A total of subjects were included, of whom 9607 had previous MI. CONCLUSION: Monotherapy with glimepiride, glibenclamide, glipizide, seems to be associated with increased mortality and cardiovascular risk compared with metformin. Gliclazide and repaglinide appear to be associated with a lower risk than others Eur Heart J. 2011
13 Sulphonylurea

14 TREATMENT OF TYPE 2 DIABETES Metformin TZDs Impaired Insulin Secretion Sulfonylureas TZDs Hyperglycemia Increased Lipolysis TZDs TZDs Metformin Increased HGP
15 Change in HbA1c (%) DURABILITY OF GLYCEMIC CONTROL WITH THIAZOLIDINEDIONES 1 0 Hanefeld (n=250) Charbonnel (n=317) PERISCOPE (n=178) RECORD (n=301) PIO Chicago (n=232) ADOPT (n=1,456) Rosenstock (n=115) Tan (n=249) Rosiglitazone -1 PIO ROSI PIO PIO PIO TIME (years)
16
17
18 Kaplan-Meier Event Rate PIOGLITAZONE & CARDIOVASCULAR EVENTS PROACTIVE (n=5238): TIME TO DEATH, MI, OR STROKE META-ANALYSIS OF CLINICAL TRIALS Plc PIO # Events Year Estimate 14.4% 12.3% Placebo P=0.027 HR = 0.84 Pioglitazone TIME (months) (n = 5,203) Comparator CI = Pioglitazone (n = 5,944) TIME (weeks) HR= 0.75 LANCET 366: ,2005 FDA and Center for Drug Evaluation & Research; July 30,2007
19 Pioglitazone and risk of bladder cancer among diabetic patients in France population-based cohort study. The French national health insurance information system Age: 40 to 79 years, follow for up to 42 months 1,491,060 diabetic patients, 155,535 of whom were exposed to pioglitazone. Incidence rates were 49.4 and 42.8 per 100,000 person-years, respectively. Pioglitazone exposure was significantly associated with bladder cancer incidence (adjusted HR 1.22 [95% CI 1.05, 1.43]). Dose-effect relationship, with a significantly increased risk for high cumulative doses and long duration of exposure ( 24 months) Diabetologia. 2012
20 Risk of bladder cancer among diabetic patients treated with pioglitazone: Interim report of a longitudinal cohort study. 193,099 patients in the Kaiser Permanente Northern California diabetes registry who were 40 years of age between 1997 and pioglitazone treated comprised 30,173 patients. There were 90 cases of bladder cancer among pioglitazone users and 791 cases of bladder cancer among nonpioglitazone users. Overall, pioglitazone was not associated with risk of bladder cancer (HR 1.2 [95% CI ]), with similar results in men and women. category of>24 months of therapy, there was an increased risk (1.4 [ ]). Diabetes Care. 2011



21 Major pathophysiologic defects in Type 2 DM: Impaired Insulin Secretion Insulin Resistance Lipotoxicity Hepatic overproduction of Glucose HYPERGLYCEMIA Reduced Incretin Effect
22 Insulin (pmol/l) Glucose (mmol/l) The Incretin Effect 10 iv oral 5 70 % of post-glucose insulin secretion is due to the incretin effects Incretin effect 0 Time





23 INCRETIN HORMONE PHYSIOLOGY Gastric emptying K-cells L-cells Satiety Fullnes s + GIP Glucagon GLP Insulin
24 Degradation of GLP-1 DPP-4 Enzymatic cleavage of GLP-1 by DPP-4 inactivates GLP-1 GLP Des-HA-GLP-1 (inactive) Two possible solutions to utilize GLP-1 action therapeutically: 1) Long-acting DPP-4-resistant GLP-1 analogues / incretin mimetics 2) DPP-4 inhibitors / incretin enhancers Mentlein et al. Eur J Biochem. 1993; Gallwitz et al. Eur J Biochem. 1994
25 GLP-1 enhancement GLP-1 secretion is impaired in Type 2 diabetes Natural GLP-1 has extremely short half-life Add GLP-1 analogues with longer half-life: exenatide liraglutide Injectables Block DPP-4, the enzyme that degrades GLP-1: sitagliptin vildagliptin Oral agents Drucker. Curr Pharm Des. 2001; Drucker. Mol Endocrinol. 2003
26
27 Adverse effects DPP4 inhibitors Hepatic function Although uncommon, cases of hepatic dysfunction (liver enzyme elevations, hepatitis) have been reported in patients taking vildagliptin and alogliptin., Liver function tests should be evaluated prior to initiation of vildagliptin and alogliptin, and at three-month intervals during the first year of therapy. Skin- In post-marketing reports, sitagliptin, saxagliptin, and alogliptin have been associated with hypersensitivity reactions including anaphylaxis, angioedema, and exfoliative skin conditions, including Stevens-Johnson syndrome.
28 Cardiovascular effects DPP4 inhibitors In one trial, 16,492 patients with type 2 diabetes and either a history of cardiovascular disease or multiple risk factors for vascular disease were randomly assigned to saxagliptin or placebo, in addition to other diabetes medications. After a median follow-up of two years, the primary endpoint (a composite endpoint of cardiovascular death, nonfatal myocardial infarction, or nonfatal ischemic stroke) occurred in a similar proportion of patients (7.3 and 7.2 percent in the saxagliptin and placebo groups, respectively Significantly more patients in the saxagliptin group were hospitalized for heart failure, HR 1.27, 95% CI ). N Engl J Med. 2013









29 Pathogenesis of Type 2 Diabetes Multiple defects contribute to the progression of type 2 diabetes mellitus Decreased Incretin Effect Decreased Insulin Secretion Increased Lipolysis Increased Glucagon Secretion Islet-a cell Hyperglycaemia Increased Glucose Reabsorption PHEM/MET/1212/1245 Increased Hepatic Glucose Production Neurotransmitter Dysfunction Decreased Glucose Uptake Adapted from DeFronzo RA. Diabetes. 2009;58:

30 Renal Glucose Reabsorption in the Proximal Tubule Glomerulus Proximal tubule S1 S2 GLUCOSE FILTRATION S3 ~90% Collecting duct GLUCOSE REABSORPTION ~10% NO GLUCOSE Glucose is freely filtered at the glomerulus and is reabsorbed via active transport mechanisms in the proximal convoluted tubule 1 Up to 180 g glucose filtered/24 h 2 PHEM/MET/1212/1245 Adapted from: Bays H. Curr Med Res Opin. 2009;25: Wright EM, et al. J Int Med. 2007;261:32 43.
31 Sodium-Glucose Co-Transporters (SGLTs) SGLT1 SGLT2 Site Intestines and kidney Almost exclusively kidney Sugar specificity Glucose or galactose Glucose Affinity for glucose High K m = 0.4 mm Low K m = 2.0 mm Capacity for glucose transport Low High Role Dietary (intestinal) glucose absorption Renal glucose reabsorption Renal glucose reabsorption PHEM/MET/1212/1245 Lee YJ, et al. Kidney Int Suppl. 2007;72:S27 S35
32 Renal Glucose Transport S1 and S2 Segments of Proximal Renal Tubule SGLT2 accounts for ~ 90% renal glucose reabsorption Tubular lumen Blood Na + SGLT2 Na+ K + Na + K+ Na+ Na + /K + ATPase pump Glucose High capacity Low affinity Glucose Glucose Glucose GLUT2 PHEM/MET/1212/1245 Adapted from: Nair S, Wilding JP. J Clin Endocrinol Metab. 2010;95:34 42 Marsenic O. Am J Kidney Dis. 2009;53:875 83
33 Urinary Glucose Excretion (g/day) The Renal Glucose Threhold (RT G ) is Increased in Subjects with Type 2 Diabetes Below RT G minimal glucosuria occurs Above RT G glucosuria occurs Healthy RT G T2DM RT G 50 ~10 mmol/l ~13.8 mmol/l Plasma Glucose (mmol/l) Renal glucose reabsorption is increased in diabetes, which could contribute to further increasing plasma glucose levels RTG, renal threshold for glucose excretion. PHEM/MET/1212/1245 Adapted from Polidori D, et al. Diabetologia 2010;53[Suppl1]:S350 [Poster 875]; Sha S, et al. Diabetes Obes Metab 2011;13: ; Devineni D, et al. Diabetes Obes Metab 2012;14:

34 Dapagliflozin Add-on to Insulin Results Summary PHEM/MET/1212/1245 Rohwedder K, et al. Diabetologia 2012:55[Suppl1]:S309 [Poster 753]

35 Dapagliflozin Add-on to Insulin Results Summary PHEM/MET/1212/1245 Rohwedder K, et al. Diabetologia 2012:55[Suppl1]:S309 [Poster 753]
36 SGLT2 Inhibitors Canagliflozin: is taken orally before the first meal of the day. The initial dose is 100 mg once daily, and it can be increased to 300 mg daily. In patients with moderate renal impairment (estimated glomerular filtration rate [egfr] 45 to 59 ml/min), the dose should not exceed 100 mg daily. should not be given to patients with egfr <45 ml/min or in patients with severe hepatic impairment. No dose adjustment is needed in patients with mild or moderate hepatic impairment. Dapagliflozin:(10 mg once daily) can be taken any time of day, with or without food. It is not recommended for use in patients with egfr <60 ml/min. For patients with severely reduced liver function, a starting dose of 5 mg is recommended
37 SGLT2 Inhibitors: Overview of Adverse Events Increases in mycotic genital infections; these AEs were generally mild to moderate in severity and led to few study discontinuations Small increase in urinary tract infections, but most infections were mild to moderate, and rarely resulted in discontinuation from treatment Some reports of symptoms attributable to osmotic diuresis No evidence of renal impairment Stenlof K et al. Diabetologia (2012) 55:[Suppl1] S312. [Poster766]; Niskanen L et al. Diabetologia (2012) 55:[Suppl1]S314. [Poster763]; Shernthaner G et al. poster presented at the 4th World Congress on Controversies to Consensus in Diabetes, Obesity and Hypertension (CODHy); 2012; Nov 8-11: Barcelona; Spain. P70; Wilding J et al. Diabetologia (2012) 55:[Suppl1]S315. [Poster766]; Forst T et al. poster presented at the 4th World Congress on Controversies to Consensus in Diabetes, Obesity and Hypertension (CODHy); 2012; Nov 8-11: Barcelona; Spain. P64 ; Matthews D et al. Diabetologia (2012) 55:[Suppl1]S314. [Poster764]; Dapagliflozin; EU Summary of Product Characteristics, December 2012 PHEM/MET/1212/1245
38 SURGICAL TREATMENT OF OBESITY one-year trial, 120 obese patients (BMI 30 to 39.9) with type 2 diabetes (mean duration nine years) who were participating in an intensive lifestyle and medically-managed weight control program were randomly assigned to receive Roux-en-Y gastric bypass surgery while continuing the lifestyle program or to continue the lifestyle program alone After one year, a greater proportion of patients in the gastric bypass group achieved the composite outcome (A1C <7 percent, low-density lipoprotein [LDL] cholesterol <100 mg/dl, and systolic blood pressure less than 130 mmhg, 49 verus 19 percent, odds ratio [OR] 4.8, 95% CI ). The mean percentage weight loss was 26.1 and 7.9 percent, respectively Serious adverse events were more frequent in the gastric bypass group (22 versus 15 events). JAMA. Jun,2013
39
40


41 Diabetes Management(HMC)
42
43
44
45
46 Multifactorial Interventionon. N Engl J Med 2008;358:
47 HbA 1c, % Earlier Use of Combination Therapy May Improve Treating to Target Compared with Conventional Therapy Diet and OAD exercise monotherapy OAD OAD up-titration combination OAD plus basal insulin OAD plus multiple daily insulin injections 10 9 Mean HbA 1c of patients Time Duration of Diabetes 18


48
What to add after metformin: primary care conference 2016
 objectives What to add after metformin: primary care conference 216 Dr. Tsang Man Wo Specialist in Endocrinology, Diabetes & Metabolism Medical Director, United Medical Practice. Consultant (P), M+G department,
objectives What to add after metformin: primary care conference 216 Dr. Tsang Man Wo Specialist in Endocrinology, Diabetes & Metabolism Medical Director, United Medical Practice. Consultant (P), M+G department,
Newer Drugs in the Management of Type 2 Diabetes Mellitus
 Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Newer Drugs in the Management of Type 2 Diabetes Mellitus Dr. C. Dinesh M. Naidu Professor of Pharmacology, Kamineni Institute of Medical Sciences, Narketpally. 1 Presentation Outline Introduction Pathogenesis
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy
 Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Oral Hypoglycemics and Risk of Adverse Cardiac Events: A Summary of the Controversy Jeffrey Boord, MD, MPH Advances in Cardiovascular Medicine Kingston, Jamaica December 7, 2012 VanderbiltHeart.com Outline
Management of Type 2 Diabetes
 Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Management of Type 2 Diabetes Pathophysiology Insulin resistance and relative insulin deficiency/ defective secretion Not immune mediated No evidence of β cell destruction Increased risk with age, obesity
Oral Agents. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
Oral Agents Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What would your ideal diabetes drug do? Effective in lowering HbA1c No hypoglycaemia No effect on weight/ weight
GLP-1. GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4.
 GLP-1 GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4 Food intake éinsulin Gut églucose uptake Pancreas Beta cells Alpha cells
GLP-1 GLP-1 is produced by the L-cells of the gut after food intake in two biologically active forms It is rapidly degraded by DPP-4 Food intake éinsulin Gut églucose uptake Pancreas Beta cells Alpha cells
GLP 1 agonists Winning the Losing Battle. Dr Bernard SAMIA. KCS Congress: Impact through collaboration
 GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
GLP 1 agonists Winning the Losing Battle Dr Bernard SAMIA KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures I have
SESSION 4 12:30pm 1:45pm
 SESSION 4 12:30pm 1:45pm Addressing Renal-Mediated Glucose Homeostasis: Diabetes and the Kidney SPEAKER Davida Kruger, MSN, BC-ADM, APRN Presenter Disclosure Information The following relationships exist
SESSION 4 12:30pm 1:45pm Addressing Renal-Mediated Glucose Homeostasis: Diabetes and the Kidney SPEAKER Davida Kruger, MSN, BC-ADM, APRN Presenter Disclosure Information The following relationships exist
Hanyang University Guri Hospital Chang Beom Lee
 Hanyang University Guri Hospital Chang Beom Lee Meal prayer, Van Brekelenkam 17 th C Introduction 2012 ADA/EASD Position Statement Proper Patients for Pioglitazone β-cell Preservation by Pioglitazone Benefit
Hanyang University Guri Hospital Chang Beom Lee Meal prayer, Van Brekelenkam 17 th C Introduction 2012 ADA/EASD Position Statement Proper Patients for Pioglitazone β-cell Preservation by Pioglitazone Benefit
SGLT2 Inhibition in the Management of T2DM: Potential Impact on CVD Risk
 Managing Diabetes & CVD: Expling New Evidence & Opptunities ESC Congress, London, UK 30 August, 2015 SGLT2 Inhibition in the Management of T2DM: Potential Impact on CVD Risk Silvio E. Inzucchi MD Yale
Managing Diabetes & CVD: Expling New Evidence & Opptunities ESC Congress, London, UK 30 August, 2015 SGLT2 Inhibition in the Management of T2DM: Potential Impact on CVD Risk Silvio E. Inzucchi MD Yale
Medical therapy advances London/Manchester RCP February/June 2016
 Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Medical therapy advances London/Manchester RCP February/June 2016 Advances in medical therapies for diabetes mellitus Duality of interest: The speaker or institutions with which he is associated has received
Chief of Endocrinology East Orange General Hospital
 Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Targeting the Incretins System: Can it Improve Our Ability to Treat Type 2 Diabetes? Darshi Sunderam, MD Darshi Sunderam, MD Chief of Endocrinology East Orange General Hospital Age-adjusted Percentage
Non-insulin treatment in Type 1 DM Sang Yong Kim
 Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
Non-insulin treatment in Type 1 DM Sang Yong Kim Chosun University Hospital Conflict of interest disclosure None Committee of Scientific Affairs Committee of Scientific Affairs Insulin therapy is the mainstay
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE. Single Technology Appraisal. Canagliflozin in combination therapy for treating type 2 diabetes
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE Single Technology Appraisal Canagliflozin in combination therapy for Final scope Remit/appraisal objective To appraise the clinical and cost effectiveness
LATE BREAKING STUDIES IN DM AND CAD. Will this change the guidelines?
 LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
LATE BREAKING STUDIES IN DM AND CAD Will this change the guidelines? Objectives 1. Discuss current guidelines for prevention of CHD in diabetes. 2. Discuss the FDA Guidance for Industry regarding evaluating
01/09/2017. Outline. SGLT 2 inhibitor? Diabetes Patients: Complex and Heterogeneous. Association between diabetes and cardiovascular events
 MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
MICROVASCULAR COMPLICATIONS Incidence of outcome g 1 Cardioprotective Effects of SGLT2s Relevant for Which T2 Diabetes Patient? SGLT 2 inhibitor? 58 year old, waist circumference 5 cm, PMH: IHD On statin,
Management of Type 2 Diabetes. Why Do We Bother to Achieve Good Control in DM2. Insulin Secretion. The Importance of BP and Glucose Control
 Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Insulin Secretion Management of Type 2 Diabetes DG van Zyl Why Do We Bother to Achieve Good Control in DM2 % reduction 0-5 -10-15 -20-25 -30-35 -40 The Importance of BP and Glucose Control Effects of tight
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol
 Inhibitors Drug Class Prior Authorization Protocol") Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has
Sulfoniluree e glinidi: pro e contro
 Sulfoniluree e glinidi: pro e contro Giorgio Sesti Università Magna Graecia di Catanzaro ITALY T2DM anti-hyperglycaemic therapy: general recommendations Diabetes Care 35:1364-1379, 2012; Diabetologia 55:1577-1596,
Sulfoniluree e glinidi: pro e contro Giorgio Sesti Università Magna Graecia di Catanzaro ITALY T2DM anti-hyperglycaemic therapy: general recommendations Diabetes Care 35:1364-1379, 2012; Diabetologia 55:1577-1596,
Diabetes update - Diagnosis and Treatment
 Diabetes update - Diagnosis and Treatment Eugene J Barrett, MD,PhD Madge Jones Professor of Medicine Director, University of Virginia Diabetes Center Disclosures - None Case 1 - Screening for Diabetes
Diabetes update - Diagnosis and Treatment Eugene J Barrett, MD,PhD Madge Jones Professor of Medicine Director, University of Virginia Diabetes Center Disclosures - None Case 1 - Screening for Diabetes
The EMPA-REG OUTCOME trial: Design and results. David Fitchett, MD University of Toronto, Canada
 The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
The EMPA-REG OUTCOME trial: Design and results David Fitchett, MD University of Toronto, Canada Asian Cardio Diabetes Forum April 23 24, 2016 Kuala Lumpur, Malaysia Life Expectancy Is Reduced by ~12 Years
New and Emerging Therapies for Type 2 DM
 Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Dale Clayton MHSc, MD, FRCPC Dalhousie University/Capital Health April 28, 2011 New and Emerging Therapies for Type 2 DM The science of today, is the technology of tomorrow. Edward Teller American Physicist
Drug Class Monograph
 Drug Class Monograph Class: Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drugs: alogliptin, alogliptin/metformin, Januvia (sitagliptin), Janumet (sitagliptin/metformin), Janumet XR (sitagliptin/metformin),
Drug Class Monograph Class: Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drugs: alogliptin, alogliptin/metformin, Januvia (sitagliptin), Janumet (sitagliptin/metformin), Janumet XR (sitagliptin/metformin),
GLP-1 agonists. Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK
 GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
GLP-1 agonists Ian Gallen Consultant Community Diabetologist Royal Berkshire Hospital Reading UK What do GLP-1 agonists do? Physiology of postprandial glucose regulation Meal ❶ ❷ Insulin Rising plasma
Drug Class Monograph
 Class: Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Monograph Drugs: alogliptin, Januvia (sitagliptin), Janumet (sitagliptin/metformin), Janumet XR (sitagliptin/metformin), Jentadueto (linagliptin/metformin),
Class: Dipeptidyl-Peptidase 4 (DPP-4) Inhibitors Drug Class Monograph Drugs: alogliptin, Januvia (sitagliptin), Janumet (sitagliptin/metformin), Janumet XR (sitagliptin/metformin), Jentadueto (linagliptin/metformin),
Ambrish Mithal MD, DM
 Ambrish Mithal MD, DM Chairman, Division of Endocrinology and Diabetes Medanta The Medicity Padma Bhushan Awardee 2015, Member Governing Council, Indian Council of Medical Research (ICMR) Dr Mithal is
Ambrish Mithal MD, DM Chairman, Division of Endocrinology and Diabetes Medanta The Medicity Padma Bhushan Awardee 2015, Member Governing Council, Indian Council of Medical Research (ICMR) Dr Mithal is
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs
 Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
Clinical Relevance of Blood Pressure Lowering Effect of Modern Antidiabetic Drugs Professor Guntram Schernthaner Medical University of Vienna, Austria guntram.schernthaner@meduniwien.ac.at Agenda Glucose
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Proposed Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Dapagliflozin in combination therapy for the Final scope Remit/appraisal objective To appraise the clinical and
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Dapagliflozin in combination therapy for the Final scope Remit/appraisal objective To appraise the clinical and
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS
 IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
IMPROVED DIAGNOSIS OF TYPE 2 DIABETES AND TAILORING MEDICATIONS Dr Bidhu Mohapatra, MBBS, MD, FRACP Consultant Physician Endocrinology and General Medicine Introduction 382 million people affected by diabetes
Peter Stein, MD Janssen Research and Development
 New Agents and Technologies in the Pipeline for the Treatment of Patients with Diabetes Peter Stein, MD Janssen Research and Development Agents in Phase 3 Development for T2DM Long-acting GLP-1 analogues
New Agents and Technologies in the Pipeline for the Treatment of Patients with Diabetes Peter Stein, MD Janssen Research and Development Agents in Phase 3 Development for T2DM Long-acting GLP-1 analogues
No Increased Cardiovascular Risk for Lixisenatide in ELIXA
 ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
ON ISSUES IN THE MANAGEMENT OF TYPE 2 DIABETES JUNE 2015 Coverage of data from ADA 2015, June 5 9 in Boston, Massachusetts No Increased Cardiovascular Risk for Lixisenatide in ELIXA First Cardiovascular
Hypoglycemic Therapy :What to start & stop
 The Cork Diabetes & Endocrinology Clinic CDEC.IE Bon Secours Hospital, Cork Hypoglycemic Therapy :What to start & stop Maeve C. Durkan MBBS.FACP, Mmed.Ed Consultant in Diabetes, Endocrinology & Metabolism
The Cork Diabetes & Endocrinology Clinic CDEC.IE Bon Secours Hospital, Cork Hypoglycemic Therapy :What to start & stop Maeve C. Durkan MBBS.FACP, Mmed.Ed Consultant in Diabetes, Endocrinology & Metabolism
Type 2 Diabetes: Where Do We Start with Treatment? DIABETES EDUCATION. Diabetes Mellitus: Complications and Co-Morbid Conditions
 Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Diabetes Mellitus: Complications and Co-Morbid Conditions ADA Guidelines for Glycemic Control: 2016 Retinopathy Between 2005-2008, 28.5% of patients with diabetes 40 years and older diagnosed with diabetic
Professor Rudy Bilous James Cook University Hospital
 Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Professor Rudy Bilous James Cook University Hospital Rate per 100 patient years Rate per 100 patient years 16 Risk of retinopathy progression 16 Risk of developing microalbuminuria 12 12 8 8 4 0 0 5 6
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications
 Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
Cardiovascular Benefits of Two Classes of Antihyperglycemic Medications Nathan Woolever, Pharm.D., Resident Pharmacist Pharmacy Grand Rounds November 6 th, 2018 Franciscan Healthcare La Crosse, WI 2017
The Many Faces of T2DM in Long-term Care Facilities
 The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
The Many Faces of T2DM in Long-term Care Facilities Question #1 Which of the following is a risk factor for increased hypoglycemia in older patients that may suggest the need to relax hyperglycemia treatment
Multiple Small Feedings of the Mind: Diabetes. Sonja K Fredrickson, MD, BC-ADM March 7, 2014
 Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Multiple Small Feedings of the Mind: Diabetes Sonja K Fredrickson, MD, BC-ADM March 7, 2014 Question 1: Setting A1c Goals Describe the evidence based approach to determining the target HgbA1c in different
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable?
 Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Diabetes Guidelines in View of Recent Clinical Trials Are They Still Applicable? Jay S. Skyler, MD, MACP Division of Endocrinology, Diabetes, and Metabolism and Diabetes Research Institute University of
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes. Overview. Prevalence of Overweight in the U.S.
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Overview Underlying defects with Type 2 diabetes Importance of managing postprandial glucose
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes
 Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
Modulating the Incretin System: A New Therapeutic Strategy for Type 2 Diabetes Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy Clinical Associate, Medical
TREATMENTS FOR TYPE 2 DIABETES. Susan Henry Diabetes Specialist Nurse
 TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
TREATMENTS FOR TYPE 2 DIABETES Susan Henry Diabetes Specialist Nurse How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management
How can we improve outcomes in Type 2 diabetes?
 How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
How can we improve outcomes in Type 2 diabetes? Earlier diagnosis Better patient education Stress central role of lifestyle management Identify and treat all risk factors Use rational pharmacological therapy
Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure?
 UCSD Hawaii 2017 Symposium Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure? Gregg C. Fonarow, MD, FACC, FAHA Elliot Corday Professor of Cardiovascular Medicine UCLA Division of Cardiology
UCSD Hawaii 2017 Symposium Can Treating Diabetes with SGLT2 inhibitors Prevent Heart Failure? Gregg C. Fonarow, MD, FACC, FAHA Elliot Corday Professor of Cardiovascular Medicine UCLA Division of Cardiology
What s New on the Horizon: Diabetes Medication Update
 What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
What s New on the Horizon: Diabetes Medication Update Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors, and what s coming Revised ADA/EASD and AACE guidelines:
GLYXAMBI (empagliflozin-linagliptin) oral tablet
 oral tablet") GLYXAMBI (empagliflozin-linagliptin) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This
GLYXAMBI (empagliflozin-linagliptin) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This
Diabetes Mellitus: Implications of New Clinical Trials and New Medications
 Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Diabetes Mellitus: Implications of New Clinical Trials and New Medications Estimates of Diagnosed Diabetes in Adults, 2005 Alka M. Kanaya, MD Asst. Professor of Medicine UCSF, Primary Care CME October
Metabolic Karma. - Essential Solution in Type2 DM - Eun Gyoung Hong, M.D., Ph.D
 2014 ICDM Breakfast Symposium. Oct 18, 2014 Grand Hilton, Seoul Metabolic Karma - Essential Solution in Type2 DM - Eun Gyoung Hong, M.D., Ph.D Department of Endocrinology and Metabolism, Hallym University
2014 ICDM Breakfast Symposium. Oct 18, 2014 Grand Hilton, Seoul Metabolic Karma - Essential Solution in Type2 DM - Eun Gyoung Hong, M.D., Ph.D Department of Endocrinology and Metabolism, Hallym University
DPP-4/SGLT2 inhibitor combined therapy for type 2 diabetes
 THERAPY REVIEW DPP-4/SGLT2 inhibitor combined therapy for type 2 diabetes STEVE CHAPLIN SPL DPP-4 inhibitors and SGLT2 inhibitors lower blood glucose by complementary mechanisms of action, and two fixeddose
THERAPY REVIEW DPP-4/SGLT2 inhibitor combined therapy for type 2 diabetes STEVE CHAPLIN SPL DPP-4 inhibitors and SGLT2 inhibitors lower blood glucose by complementary mechanisms of action, and two fixeddose
DIABETES DEBATE - IS NEW BETTER?
 DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
DIABETES DEBATE - IS NEW BETTER? WHAT MEDICATION CLASS AFTER METFORMIN TO CONTROL BLOOD SUGAR Dr. Lydia Hatcher, MD, CCFP, FCFP, CHE, D-CAPM Associate Clinical Professor of Family Medicine, McMaster Chief
NEW DIABETES CARE MEDICATIONS
 NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
NEW DIABETES CARE MEDICATIONS James Bonucchi DO, ECNU, FACE Adult Medicine and Endocrinology Specialists Disclosures Speakers bureau Sanofi AZ BI Diabetes Diabetes cost ADA 2017 data Ever increasing disorder.
Multi-factor approach to reduce cardiovascular risk in diabetes
 Multi-factor approach to reduce cardiovascular risk in diabetes Prof. Nicola Napoli, MD PhD Division of Endocrinology and Diabetes Università Campus Bio-Medico di Roma Washington University in St Louis
Multi-factor approach to reduce cardiovascular risk in diabetes Prof. Nicola Napoli, MD PhD Division of Endocrinology and Diabetes Università Campus Bio-Medico di Roma Washington University in St Louis
What s New on the Horizon: Diabetes Medication Update. Michael Shannon, MD Providence Endocrinology, Olympia WA
 What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
What s New on the Horizon: Diabetes Medication Update Michael Shannon, MD Providence Endocrinology, Olympia WA 1 Outline of Talk Newly released and upcoming medications: the incretins, DPP-IV inhibitors,
DPP-4 inhibitor. The new class drug for Diabetes
 DPP-4 inhibitor The new class drug for Diabetes 1 Cause of Death in Korea 1 st ; Neoplasm 2 nd ; Cardiovascular Disease 3 rd ; Cerebrovascular Disease Diabetes 2 Incidence of Fatal or Nonfatal MI During
DPP-4 inhibitor The new class drug for Diabetes 1 Cause of Death in Korea 1 st ; Neoplasm 2 nd ; Cardiovascular Disease 3 rd ; Cerebrovascular Disease Diabetes 2 Incidence of Fatal or Nonfatal MI During
What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital
 What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning
What s New in Type 2? Peter Hammond Consultant Physician Harrogate District Hospital Therapy considerations in T2DM Thiazoledinediones DPP IV inhibitors GLP 1 agonists Insulin Type Delivery Horizon scanning
Wayne Gravois, MD August 6, 2017
 Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Wayne Gravois, MD August 6, 2017 Americans with Diabetes (Millions) 40 30 Source: National Diabetes Statistics Report, 2011, 2017 Millions 20 10 0 1980 2009 2015 2007 - $174 Billion 2015 - $245 Billion
Type 2 Diabetes and Cancer: Is there a link?
 Type 2 Diabetes and Cancer: Is there a link? Sonali Thosani, MD Assistant Professor Department of Endocrine Neoplasia & Hormonal Disorders MD Anderson Cancer Center No relevant financial disclosures Objectives
Type 2 Diabetes and Cancer: Is there a link? Sonali Thosani, MD Assistant Professor Department of Endocrine Neoplasia & Hormonal Disorders MD Anderson Cancer Center No relevant financial disclosures Objectives
The Alphabet Soup of Diabetes. Egils Bogdanovics M.D. Hungerford Diabetes Center
 The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
The Alphabet Soup of Diabetes Egils Bogdanovics M.D. Hungerford Diabetes Center Insulin: January 11, 1922 12 year old Leonard Thompson, on a starvation diet for 2 years received his first insulin injection
Pharmacology Updates. Quang T Nguyen, FACP, FACE, FTOS 11/18/17
 Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Pharmacology Updates Quang T Nguyen, FACP, FACE, FTOS 11/18/17 14 Classes of Drugs Available for the Treatment of Type 2 DM in the USA ### Class A1c Reduction Hypoglycemia Weight Change Dosing (times/day)
Oral and Injectable Non-insulin Antihyperglycemic Agents
 Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Appendix 5: Diabetes Education and Medical Management in Adults with Diabetes Oral and Injectable Non-insulin s This directive will be implemented by RPhs, RNs or RDs who have been deemed authorized implementers.
Drug Class Monograph
 Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Drug Class Monograph Class: Sodium-Glucose Co-Transporter 2 (SGLT-2) Inhibitors Drugs: Farxiga (dapagliflozin), Invokamet (canagliflozin/metformin), Invokana (canagliflozin), Jardiance (empagliflozin),
Disclosures. Type 2 Diabetes. The New Epidemic: How Did We Get Here and What's to Come? Summary:
 Type 2. The New Epidemic: How Did We Get Here and What's to Come? Robert J. Rushakoff, MD Professor of Medicine University of California, San Francisco None Disclosures robert.rushakoff@ucsf.edu Type 2.
Type 2. The New Epidemic: How Did We Get Here and What's to Come? Robert J. Rushakoff, MD Professor of Medicine University of California, San Francisco None Disclosures robert.rushakoff@ucsf.edu Type 2.
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC
 Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Choosing the Right Agent for your Patient with diabetes: Individualizing type 2 diabetes management in light of the expanding therapies
Canadian Society of Internal Medicine Annual Meeting 2016 Montreal, QC Choosing the Right Agent for your Patient with diabetes: Individualizing type 2 diabetes management in light of the expanding therapies
T2DM is a global epidemic with
 : a new option for the management of type 2 diabetes Marc Evans MRCP, MD, Consultant Diabetologist, Llandough Hospital, Cardiff Incretin-based therapies for the treatment of diabetes mellitus (T2DM) present
: a new option for the management of type 2 diabetes Marc Evans MRCP, MD, Consultant Diabetologist, Llandough Hospital, Cardiff Incretin-based therapies for the treatment of diabetes mellitus (T2DM) present
A New Therapeutic Strategey for Type II Diabetes: Update 2008
 Live, One Hour Webinar A New Therapeutic Strategey for Type II Diabetes: Update 2008 Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy in Grundy, Virginia.
Live, One Hour Webinar A New Therapeutic Strategey for Type II Diabetes: Update 2008 Geneva Clark Briggs, PharmD, BCPS Adjunct Professor at University of Appalachia College of Pharmacy in Grundy, Virginia.
Diabetes Mellitus: Overview and Guidelines
 Diabetes Mellitus: Overview and Guidelines Rezvan Salehidoost, M.D., Endocrinologist Abidi Diabetes Master Class IMPORTANCE? Why is it interesting to do research in diabetes J. Olefsky, JAMA 2001:285:628-632
Diabetes Mellitus: Overview and Guidelines Rezvan Salehidoost, M.D., Endocrinologist Abidi Diabetes Master Class IMPORTANCE? Why is it interesting to do research in diabetes J. Olefsky, JAMA 2001:285:628-632
Diabetic Management of the Cardiac Patient
 Diabetic Management of the Cardiac Patient Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Disclosures Grants/Research Support:
Diabetic Management of the Cardiac Patient Dr Peter A Senior BMedSci MBBS PhD FRCP(E) Associate Professor, Director Division of Endocrinology, University of Alberta Disclosures Grants/Research Support:
Joslin Diabetes Center Joslin Diabetes Forum 2013: The Impact of Comorbidities on Glucose Control Scenario 2: Reduced Renal Function
 Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
Scenario 2: Reduced Renal Function 62 y.o. white man with type 2 diabetes for 18 years Hypertension and hypercholesterolemia Known proliferative retinopathy Current medications: Metformin 1000 mg bid Glyburide
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
Disclosure. Learning Objectives. Case. Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare
 Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Disclosure Diabetes Update: Incretin Agents in Diabetes-When to Use Them? I have no disclosures to declare Spring Therapeutics Update 2011 CSHP BC Branch Anar Dossa BScPharm Pharm D CDE April 20, 2011
Dept of Diabetes Main Desk
 Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Dept of Diabetes Main Desk 01202 448060 Glucose management in Type 2 Diabetes in Adults The natural history of type 2 diabetes is for HbA1c to deteriorate with time. A stepwise approach to treatment is
Treatment Options for Diabetes: An Update
 Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Treatment Options for Diabetes: An Update A/Prof. Marg McGill Manager, Diabetes Centre Dr. Ted Wu Staff Specialist Endocrinologist Diabetes Centre Centre of Health Professional Education Education Provider
Metformin. Sulfonylurea. Thiazolidinedione. Insulin
 동아의대내분비내과박미경 Metformin Sulfonylurea Thiazolidinedione Insulin 요약 markers of inflammation (hs-crp, TNF-a) markers of impaired endothelial function (VFW, scams, tpa, PAI-1) LDL-C, fasting and postprandial
동아의대내분비내과박미경 Metformin Sulfonylurea Thiazolidinedione Insulin 요약 markers of inflammation (hs-crp, TNF-a) markers of impaired endothelial function (VFW, scams, tpa, PAI-1) LDL-C, fasting and postprandial
Should Psychiatrists be diagnosing (and treating) metabolic syndrome
 metabolic syndrome") Should Psychiatrists be diagnosing (and treating) metabolic syndrome David Hopkins Clinical Director, Diabetes King s College Hospital, London Diabetes prevalence (thousands) Diabetes in the UK: 1995-2010
Should Psychiatrists be diagnosing (and treating) metabolic syndrome David Hopkins Clinical Director, Diabetes King s College Hospital, London Diabetes prevalence (thousands) Diabetes in the UK: 1995-2010
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes
 Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Obesity, Insulin Resistance, Metabolic Syndrome, and the Natural History of Type 2 Diabetes Genetics, environment, and lifestyle (obesity, inactivity, poor diet) Impaired fasting glucose Decreased β-cell
Il blocco del cotrasportatore. della terapia antiiperglicemica. Anna Solini
 Il blocco del cotrasportatore sodioglucosio come target della terapia antiiperglicemica Anna Solini Dipartimento di Patologia Chirurgica, Medica, Molecolare e dell Area Critica Università di Pisa Grant
Il blocco del cotrasportatore sodioglucosio come target della terapia antiiperglicemica Anna Solini Dipartimento di Patologia Chirurgica, Medica, Molecolare e dell Area Critica Università di Pisa Grant
Clinical Overview of Combination Therapy with Sitagliptin and Metformin
 Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
Clinical Overview of Combination Therapy with Sitagliptin and Metformin 1 Contents Pathophysiology of type 2 diabetes and mechanism of action of sitagliptin Clinical data overview of sitagliptin: Monotherapy
YOU HAVE DIABETES. Angie O Connor Community Diabetes Nurse Specialist 25th September 2013
 YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
YOU HAVE DIABETES Angie O Connor Community Diabetes Nurse Specialist 25th September 2013 Predicated 2015 figures are already met 1 in 20 have diabetes:1in8 over 60years old Definite Diagnosis is key Early
Practical Diabetes. Nic Crook. (and don t use so many charts) Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua
 Kuirau Specialists 1239 Ranolf Street Rotorua. Rotorua Hospital Private Bag 3023 Rotorua") Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Practical Diabetes (and don t use so many charts) Nic Crook Rotorua Hospital Private Bag 3023 Rotorua Kuirau Specialists 1239 Ranolf Street Rotorua Worldwide rates of diabetes mellitus: predictions 80
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series. Diabetes Update July 6, :00pm 1:00pm
 Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Diabetes Update July 6, 2017 12:00pm 1:00pm Jennifer Pennock Holst, MD Endocrinology, Diabetes & Metabolism AHN Center for
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Diabetes Update July 6, 2017 12:00pm 1:00pm Jennifer Pennock Holst, MD Endocrinology, Diabetes & Metabolism AHN Center for
Early treatment for patients with Type 2 Diabetes
 Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Israel Society of Internal Medicine Kibutz Hagoshrim, June 22, 2012 Early treatment for patients with Type 2 Diabetes Eduard Montanya Hospital Universitari Bellvitge-IDIBELL CIBERDEM University of Barcelona
Current Diabetes Care for Internists:2011
 Current Diabetes Care for Internists:2011 Petch Rawdaree, DM, MSc, DLSHTM Faculty of Medicine Vajira Hospital University of Bangkok Metropolis 19 th January 2011 ก ก 1. ก ก ก ก 2. ก ก ก ก ก 3. ก ก ก ก
Current Diabetes Care for Internists:2011 Petch Rawdaree, DM, MSc, DLSHTM Faculty of Medicine Vajira Hospital University of Bangkok Metropolis 19 th January 2011 ก ก 1. ก ก ก ก 2. ก ก ก ก ก 3. ก ก ก ก
CANA DAPA EMPA. Change in Baseline Body Weight (kg) *Doses evaluated in studies cited: CANA=100 or 300 mg, DAPA=5 or 10 mg, EMPA=10 or 25 mg.
 *Doses evaluated in studies cited: CANA=100 or 300 mg, DAPA=5 or 10 mg, EMPA=10 or 25 mg.") CANA DAPA EMPA Change in Baseline Body Weight (kg) 2 1 0-1 -2-3 -4-5 PBO SGLT2 inhibitor (low dose)* SGLT2 inhibitor (high dose)* *Doses evaluated in studies cited: CANA=100 or 300 mg, DAPA=5 or 10 mg,
CANA DAPA EMPA Change in Baseline Body Weight (kg) 2 1 0-1 -2-3 -4-5 PBO SGLT2 inhibitor (low dose)* SGLT2 inhibitor (high dose)* *Doses evaluated in studies cited: CANA=100 or 300 mg, DAPA=5 or 10 mg,
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials
 Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
Case Studies in Type 2 Diabetes Mellitus: Focus on Cardiovascular Outcomes Trials Louis Kuritzky MD Clinical Assistant Professor Emeritus Department of Community Health and Family Medicine College of Medicine
COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP Policy agreed by (Vale of York CCG/date)
") Drug, Treatment, Device name ( Vipidia; Takeda) COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP Policy agreed by (Vale of York CCG/date) Licensed indication To improve glycaemic control in
Drug, Treatment, Device name ( Vipidia; Takeda) COMMISSIONING POLICY RECOMMENDATION TREATMENT ADVISORY GROUP Policy agreed by (Vale of York CCG/date) Licensed indication To improve glycaemic control in
Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville
 Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville Pathogenesis of Diabetes Mellitus (DM) Criteria for the diagnosis
Mae Sheikh-Ali, M.D. Assistant Professor of Medicine Division of Endocrinology University of Florida College of Medicine- Jacksonville Pathogenesis of Diabetes Mellitus (DM) Criteria for the diagnosis
Type 2 Diabetes Mellitus 2011
 2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
2011 Michael T. McDermott MD Director, Endocrinology and Diabetes Practice University of Colorado Hospital Michael.mcdermott@ucdenver.edu Diabetes Mellitus Diagnosis 2011 Diabetes Mellitus Fasting Glucose
Alia Gilani Health Inequalities Pharmacist
 Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
Alia Gilani Health Inequalities Pharmacist THE SOUTH ASIAN HEALTH FOUNDATION (U.K.) (Registered Charity No. 1073178) 1. Case Study 2. Factors influencing prescribing 3. Special Considerations 4. Prescribing
New Treatments for Type 2 diabetes. Nandini Seevaratnam April 2016 Rushcliffe Patient Forum
 New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
New Treatments for Type 2 diabetes Nandini Seevaratnam April 2016 Rushcliffe Patient Forum Overview Growing population of Type 2 diabetes Basic science on what goes wrong Current treatments Why there is
Oral Agents in Type 2 DM
 Oral Agents in Type 2 DM CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
Oral Agents in Type 2 DM CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care
 Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
Hot Topics: The Future of Diabetes Management Cutting Edge Medication and Technology-Based Care Mary Jean Christian, MA, MBA, RD, CDE Diabetes Program Coordinator UC Irvine Health Hot Topics: Diabetes
National Horizon Scanning Centre. Saxagliptin (BMS ) for type 2 diabetes. April 2008
 for type 2 diabetes. April 2008") Saxagliptin (BMS 477118) for type 2 diabetes This technology summary is based on information available at the time of research and a limited literature search. It is not intended to be a definitive statement
Saxagliptin (BMS 477118) for type 2 diabetes This technology summary is based on information available at the time of research and a limited literature search. It is not intended to be a definitive statement
Update on Agents for Type 2 Diabetes
 Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
Update on Agents for Type 2 Diabetes This presentation will: Outline the clinical considerations in the selection of pharmacotherapy for type 2 diabetes, including degree of A1C lowering achieved, patient-specific
6/1/2018. Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE
 Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
Lou Haenel, IV, DO, FACE, FACOI Endocrinology Roper St Francis Charleston, SC THE OMINOUS OCTET: HOW PATHOPHYSIOLOGY AND THERAPY MERGE 1 2 3 Sulfonylureas Glipizide Glyburide Glimeperide 4 Metformin Gold
COPYRIGHT. Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely?
 Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely? Martin J. Abrahamson, MD FACP Associate Professor of Medicine, Harvard
Treatment of Type 2 Diabetes: What To Do When Treatment with Metformin is Inadequate? Can We Achieve Therapeutic Goals More Safely? Martin J. Abrahamson, MD FACP Associate Professor of Medicine, Harvard
New Approaches for Treating Challenging Patients with Diabetes
 New Approaches for Treating Challenging Patients with Diabetes Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs Disclosure of Potential Conflicts of Interest
New Approaches for Treating Challenging Patients with Diabetes Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs Disclosure of Potential Conflicts of Interest
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes
 Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
Pharmacology Update for the Adult Patient - Newer Oral Medications for Diabetes Brooke Hudspeth, PharmD, CDE, MLDE Director of Diabetes Prevention, Kroger Pharmacy Adjunct Assistant Professor, University
The Role Of SGLT-2 Inhibitors In Clinical Practice. Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs
 The Role Of SGLT-2 Inhibitors In Clinical Practice Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs Disclosure of Potential Conflicts of Interest Consultantship
The Role Of SGLT-2 Inhibitors In Clinical Practice Anne Peters, MD Professor, USC Keck School of Medicine Director, USC Clinical Diabetes Programs Disclosure of Potential Conflicts of Interest Consultantship
Glucose Control drug treatments
 Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Glucose Control drug treatments It should be noted that glitazones are under suspicion of precipitating acute cardiac events and current recommendations contraindicate the use of glitazones in patients
Diabete: terapia nei pazienti a rischio cardiovascolare
 Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
Diabete: terapia nei pazienti a rischio cardiovascolare Giorgio Sesti Università Magna Graecia di Catanzaro Cardiovascular mortality in relation to diabetes mellitus and a prior MI: A Danish Population
The ABCs (A1C, BP and Cholesterol) of Diabetes
 of Diabetes") The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department