Modified Radical Mastectomy
|
|
|
- Gregory Glenn
- 6 years ago
- Views:
Transcription
, MRM with immediate reconstruction, and breast conservation therapy (BCT).")
1 Modified Radical Mastectomy Valerie L. Staradub, MD, and Monica Morrow, MD S urgical management options for breast cancer include modified radical mastectomy (MRM), MRM with immediate reconstruction, and breast conservation therapy (BCT). Absolute contraindications to BCT include tumor presence in more than one breast quadrant, diffuse suspicious or indeterminate calcifications seen on mammography and contraindications to radiation therapy, such as first or second trimester of pregnancy or history of radiation therapy to the breast field for previous breast cancer or as part of treatment for another condition, such as Hodgkin's disease. 1 Relative contraindications include sufficiently large tumor-to-breast ratio to preclude acceptable cosmesis and collagen vascular disease. The incidence of these contraindications varies with tumor stage. In our experience, 10% of women with stage I breast cancer and 28% of women with stage II breast cancer had contraindications to BeT. 2 In women with contraindications to BCT, MRM is medically necessary. For all others, there is no survival difference between the procedures, and patient preference should be the deciding factor. We have observed that approximately 20% of women who are candidates for BCT opt to undergo MRM. Nationally, MRM remains the most common treatment for patients with stage I and II breast cancer. 3-5 In some situations, MRM is not an appropriate first-line treatment modality, and the patient should be referred for neoadjuvant chemotherapy; these include metastatic breast cancer and locoregionally advanced carcinoma. 6-7 In addition, patients presenting with stage IV carcinoma are surgical candidates only if they develop local complications that cannot be controlled with systemic therapy. MRM always includes removal of the breast tissue, the nipple-areolar complex, and the ipsilateral axillary lymph nodes. Variations of the procedure, including removal of the pectoralis minor muscle or division of its tendon to facilitate axillary exposure, have been described, sq~ In our experience, these are rarely, if ever, necessary, and the technique that we describe keeps the pectoralis minor intact. The original descriptions of MRM included removal of the pectoralis major fascia, because this structure was thought to be a barrier to the lymphatic spread of tumor. Subsequent studies have shown that lymphatic vessels penetrate the pectoral fascia and that this fascia may be preserved when needed to facilitate implant reconstruction, as long as care is taken to meticulously remove all of the breast tissue superficial to the fascia. MRM is an extremely safe operation with a very- low operative mortality rate. This is true even in the elderly population, for which the mortality rate from breast surgery of all types is less than 2% Patient Positioning and Preparation 1"he patient is positioned supine on the operating table with the ipsilateral arm abducted 90 ~ on an arm board. The arm board is padded to prevent subluxation of the shoulder with brachial plexus stretch. The patient is positioned at the edge of the table on the operative side; it may be helpful to place a folded sheet under the ipsilateral shoulder. The axilla is shaved if necessary, and a standard surgical preparation is done. The breast preparation should extend below the mframammary crease, across the midline, and to the supraclavicular fossa in the event that extra skin mobilization is needed to allow closure. The entire ipsilateral arm is prepped to the wrist, the arm board is covered with a Mayo stand cover, and the arm is draped with an impervious stockinet. The field drapes are brought underneath the ipsilateral shoulder so that the entire arm is in the operative field. From the Lynn Sage Comprehensive Breast Center, Department of Surgery, Northwestern University Medical School, Chicago, IL. Address reprint requests to Monica Morrow, MD, Director, Lynn Sage Comprehensive Breast Center, Northwestern Memorial Hospital, 251 E. Huron St., Gaiter , Chicago, IL Copyright by WB. Saunders Company X/00/ /0 doi: /otgn Operative Techniques in General Surgery, Vol 2, No 2 (June), 2000: pp

 is given before the incision is made if the patient has had a prior open biopsy or preoperative")
2 Modified Radical Mastectomy 119 SURGICAL TECHNIQUE 9.:~! = [ A Mastectomy incision after upper biopsy B Mastectomy incision after lower inner biopsy ia x 1 The surgeon stands below the arm board, and the first assistant is positioned cranial to the arm board on the ipsilateral side. A second assistant may be positioned on the contralateral side. An antibiotic with a broad spectrum of gram-positive coverage (eg, a first-generation cephalosporin) is given before the incision is made if the patient has had a prior open biopsy or preoperative chemotherapy or is otherwise immunosuppressed. The incision line is drawn with a marker and includes the nipple-areolar complex, the biopsy site if carcinoma was diagnosed with a surgical biopsy, and any excess breast skin. The incision can be oriented in any way that facilitates inclusion of these structures (A and B). Care is taken to not extend the incision medially to the sternum or laterally off the breast mound, as this will result in unsightly dog-ears. Exposure in these areas is obtained by raising flaps. Tumescence solution, consisting of 1 L of lactated Ringers' solution with 30 ml of 1% lidocaine solution with epinephrine at 1:1000, is used to allow a hemostatic dissection with the knife. This technique was developed for liposuction and is used to reduce blood loss in various plastic surgical flap procedures. When used for mastectomy, it is critical that the skin incision be planned before the infusion of tumescence fluid, because it is difficult to accurately determine the amount of skin that must be removed once the breast has been filled with fluid. Tumescence may be delivered with a pressure infusion system or manually. In pressure infusion, several stab incisions are made with a #15 blade inside the fine of planned resection for insertion of a blunt needle. The tumescence solution is infused into the subcutaneous space over the entire area of the planned dissection and into the deep substance of the breast. The solution is infused until the breast is firm to the touch, which, depending on breast size, may require between 500 ml and 1 L of solution. Care should be taken to avoid injecting the solution directly into the tumor bed itself. When manual injection is used, a spinal needle is attached to a spring-loaded syringe with a 3-way stopcock and intravenous extension tubing. These needles can reach the axillary vein, so care must be taken when injecting in this area.


3 120 Staradub and Morrow Clavicle Sternum iil/il '{ ' Latissimus dorsi?ii;!{!i!i :ili!i : e:= r.:: : { 2, The incision is made with the knife along the previously sketched lines. With skin hooks used to elevate the skin, skin flaps are raised with a #10 blade in the plane deep to the subcutaneous fat and superficial to the breast parenchyma. The thickness of the flap will vary with the amount of subcutaneous fat present. Manual retraction of the breast tissue away from the skin tends to show this plane quite effectively. Surgeons accustomed to determining flap thickness by palpation need to be aware that the use of tumescence solution causes the flaps to feel thicker. Flaps are raised superiorly to the level of the clavicle, medially to the edge of the sternum, inferiorly to the superior aspect of the rectus sheath, and laterally to the latissimus dorsi muscle. Once all flaps have been raised, the pectoralis major fascia is elevated off the muscle with the knife, beginning at the superior aspect of the breast and continuing inferiorly. Perforating vessels along the sternal edge are ligated and divided as they are encountered, and smaller perforators from the muscle are cauterized. The breast is left attached at the inferolateral edge to provide retraction during the axillary dissection. The breast is then freed from the lateral edge of the pectoralis maj or muscle; the medial pectoral bundle should be preserved. The muscle is gently retracted with a small Richardson retractor, and the axillary investing fascia is opened along the edge of the pectoralis minor to allow placement of a retractor beneath it during the axillary dissection.

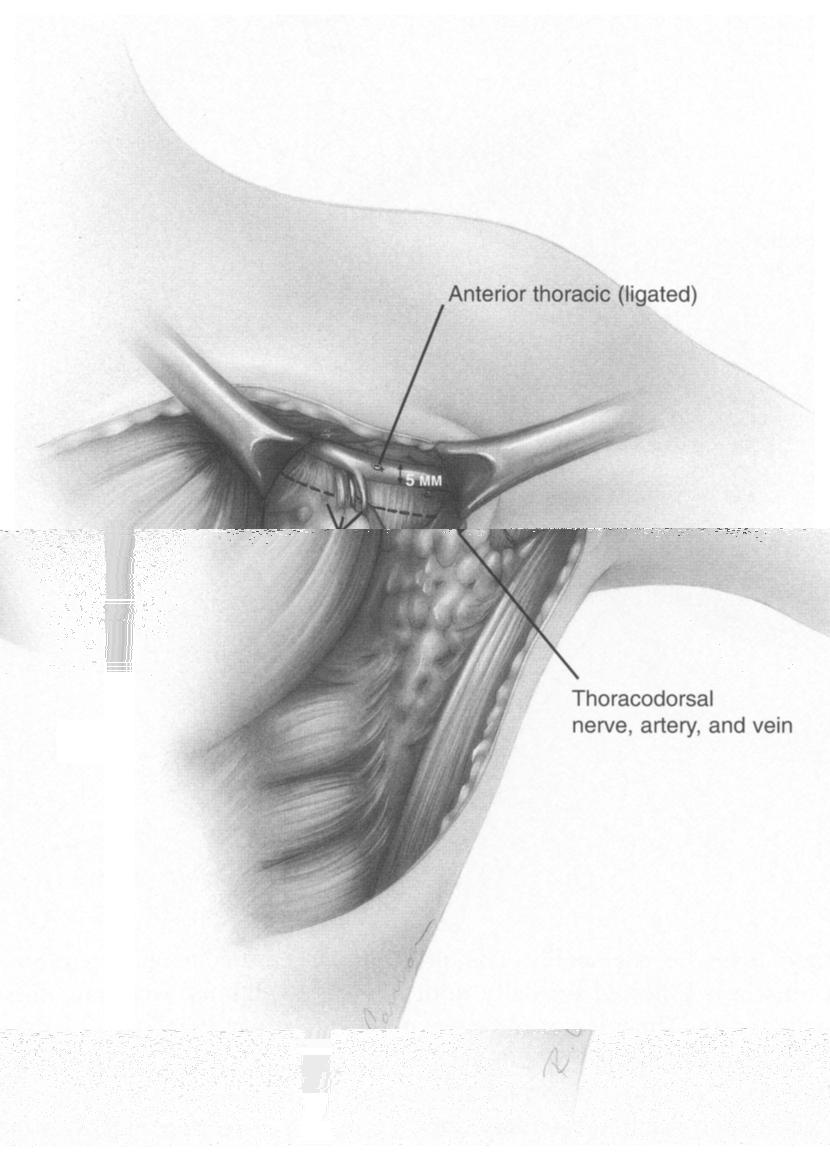
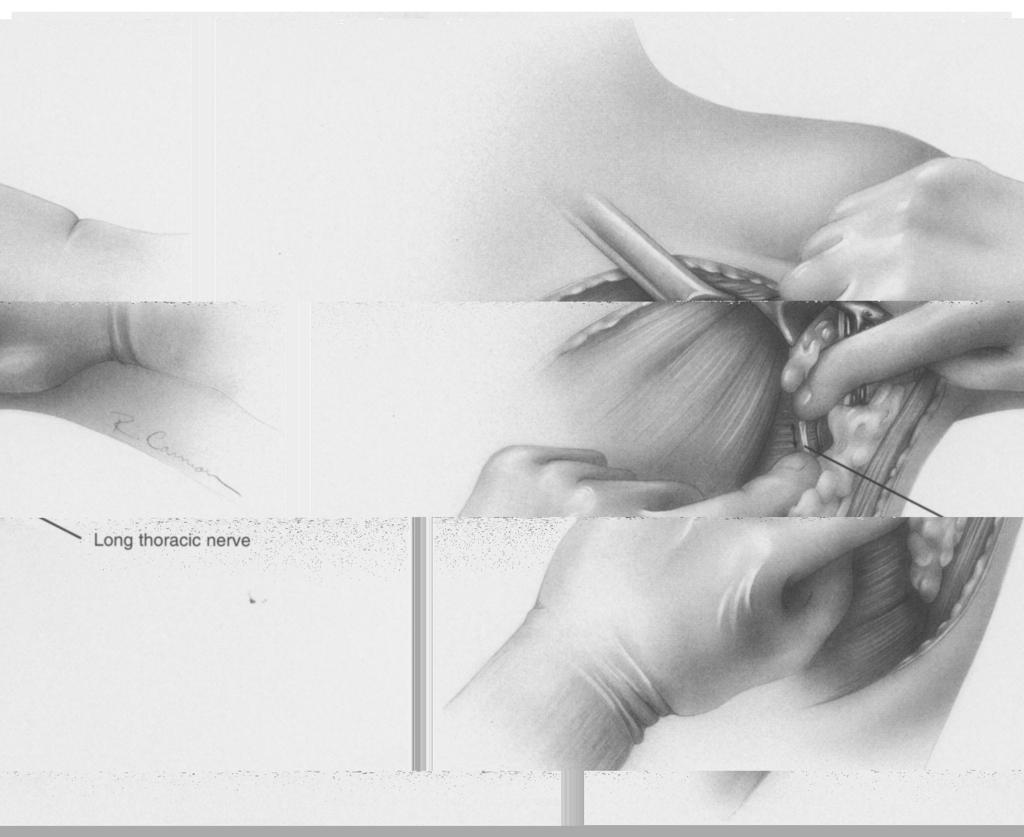
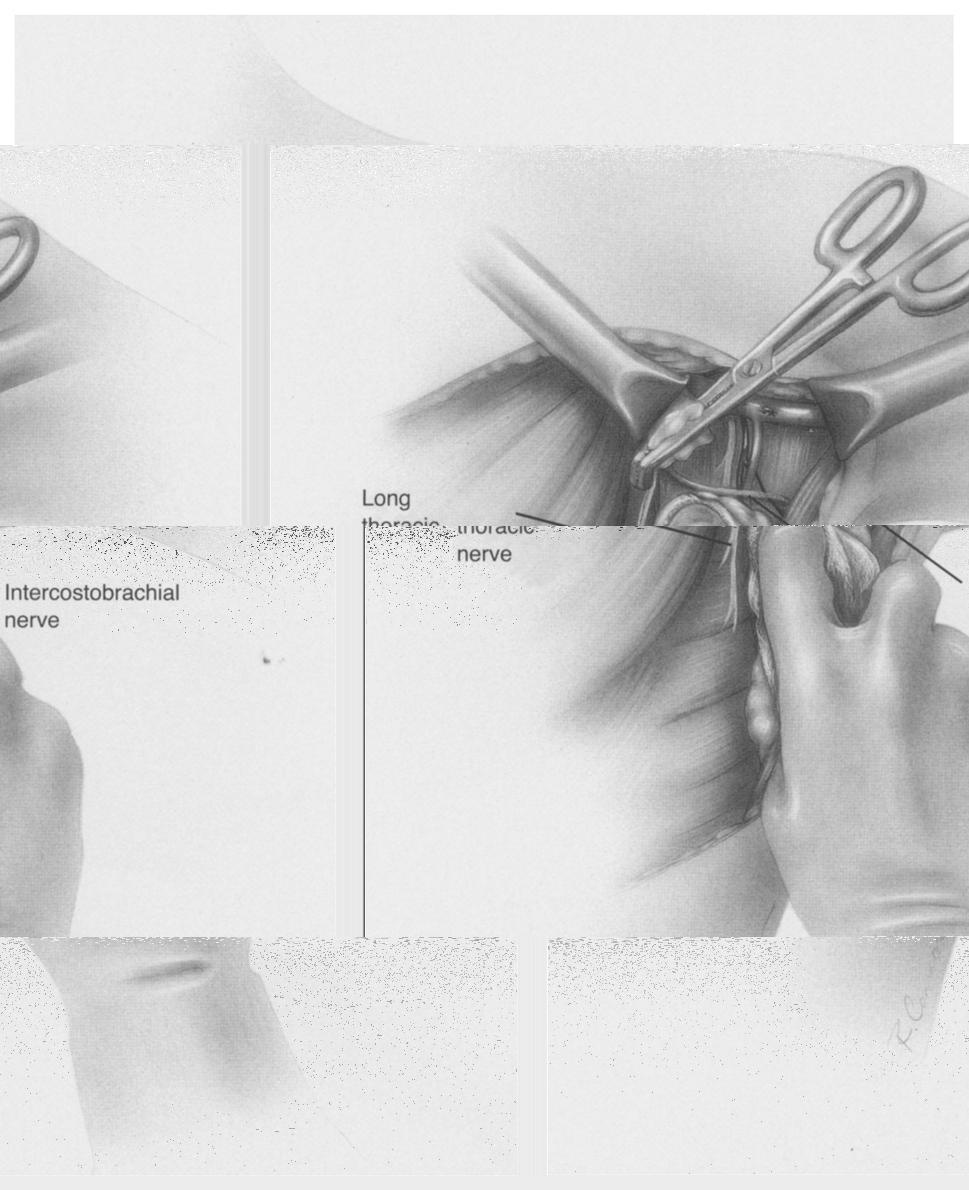
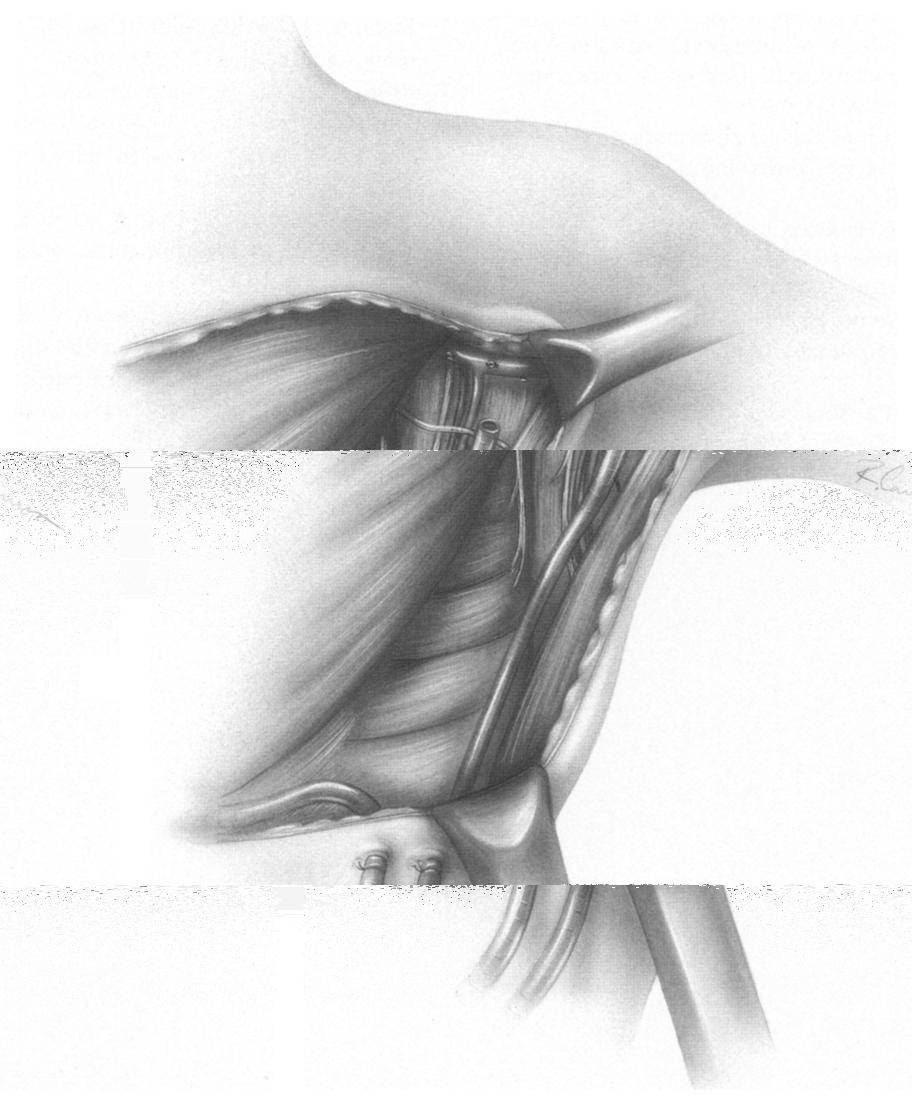
4 Modified Radical Mastectomy 121 Axill ary vein :~i' I i 3 Attention now turns to the axilla. The previously identified edge of the latissimus dorsi muscle is followed cranially until it turns tendinous, where it is crossed by the axillary vein. The intercostobrachial nerves are encountered approximately halfway up the latissimus and are identified during this step and preserved to avoid numbness of the upper inner arm. No other important structures cross this plane of dissection, making it the safest approach to the axillary vein. Once the axillary vein is identified, its overlying fat is divided in a lateral-to-medial fashion. Care is taken to avoid stripping the vein completely of overlying fat and lymphatics, which may increase the potential for lymphedema. Dissection superior to the vein also must be avoided. When the vein has been exposed, dissection once again commences in a lateral-to-medial fashion just below the vein. Dissecting approximately 5 mm below the vein rather than immediately on the inferior surface will avoid creating a side hole in the vein in the event that a branch is inadvertently transected. There is often a large lymphatic vessel traversing parallel to the vein on its inferior surface; this should be preserved, if possible. With the first assistant providing caudal traction on the axillary contents, the surgeon dissects the superficial fat and divides the branches of the axillary vein and ties them with 3-0 silk as they are encountered. An anterior thoracic branch usually overlies the deeper thoracodorsal vein. However, the surgeon should carry out the dissection systematically, layer by layer, rather than attempting to initially identify the deeper vein branches or the thoracodorsal or long thoracic nerves early in the dissection.
5 122

6
7
8

9
Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman
 Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman Breast anatomy: Breast conserving surgery: The aim of wide local excision is to remove all invasive and in situ
Breast conservation surgery and sentinal node biopsy: Dr R Botha Moderator: Dr E Osman Breast anatomy: Breast conserving surgery: The aim of wide local excision is to remove all invasive and in situ
Alexander C Vlantis. Selective Neck Dissection 33
 05 Modified Radical Neck Dissection Type II Alexander C Vlantis Selective Neck Dissection 33 Modified Radical Neck Dissection Type II INCISION Various incisions can be used for a neck dissection. The incision
05 Modified Radical Neck Dissection Type II Alexander C Vlantis Selective Neck Dissection 33 Modified Radical Neck Dissection Type II INCISION Various incisions can be used for a neck dissection. The incision
Advances in Breast Surgery. Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015
 Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
Practice of Axilla Surgery
 Summer School of Breast Disease 2016 Practice of Axilla Surgery Axillary Lymph Node Dissection & Sentinel Lymph Node Biopsy 연세의대외과 박세호 Contents Anatomy of the axilla Axillary lymph node dissection (ALND)
Summer School of Breast Disease 2016 Practice of Axilla Surgery Axillary Lymph Node Dissection & Sentinel Lymph Node Biopsy 연세의대외과 박세호 Contents Anatomy of the axilla Axillary lymph node dissection (ALND)
Advances in Localized Breast Cancer
 Advances in Localized Breast Cancer Melissa Camp, MD, MPH and Fariba Asrari, MD June 18, 2018 Moderated by Elissa Bantug 1 Advances in Surgery for Breast Cancer Melissa Camp, MD June 18, 2018 2 Historical
Advances in Localized Breast Cancer Melissa Camp, MD, MPH and Fariba Asrari, MD June 18, 2018 Moderated by Elissa Bantug 1 Advances in Surgery for Breast Cancer Melissa Camp, MD June 18, 2018 2 Historical
BREAST CANCER SURGERY. Dr. John H. Donohue
 Dr. John H. Donohue HISTORY References to breast surgery in ancient Egypt (ca 3000 BCE) Mastectomy described in numerous medieval texts Petit formulated organized approach in 18 th Century Improvements
Dr. John H. Donohue HISTORY References to breast surgery in ancient Egypt (ca 3000 BCE) Mastectomy described in numerous medieval texts Petit formulated organized approach in 18 th Century Improvements
Forelimb Amputation. Indications. Pre operatively 11/12/2008. Technique Preparing for surgery. Bone neoplasia. Severe trauma/paralysis
 Forelimb Amputation January 10, 2007 Amy Bringardner Becky Pentecost Indications Bone neoplasia Osteosarcoma Fibrosarcoma Chondrosarcoma Severe trauma/paralysis Brachial plexus avulsion Infection Congenital
Forelimb Amputation January 10, 2007 Amy Bringardner Becky Pentecost Indications Bone neoplasia Osteosarcoma Fibrosarcoma Chondrosarcoma Severe trauma/paralysis Brachial plexus avulsion Infection Congenital
BICEPTOR Tenodesis System
 BICEPTOR Tenodesis System Sub-Pectoral Biceps Tenodesis A Shoulder Series Technique Guide As described by: Nikhil N. Verma, MD As described by: Nikhil N. Verma, MD Midwest Orthopedics at Rush Chicago,
BICEPTOR Tenodesis System Sub-Pectoral Biceps Tenodesis A Shoulder Series Technique Guide As described by: Nikhil N. Verma, MD As described by: Nikhil N. Verma, MD Midwest Orthopedics at Rush Chicago,
Essential Anatomy for oncoplastic surgery. Omar Z. Youssef M.D Professor of surgical oncology NCI- Cairo University
 Essential Anatomy for oncoplastic surgery Omar Z. Youssef M.D Professor of surgical oncology NCI- Cairo University Introduction Rationale for anatomical basis for OPS Anatomical considerations: 1. Surface
Essential Anatomy for oncoplastic surgery Omar Z. Youssef M.D Professor of surgical oncology NCI- Cairo University Introduction Rationale for anatomical basis for OPS Anatomical considerations: 1. Surface
Breast Reconstruction Postmastectomy. Using DermaMatrix Acellular Dermis in breast reconstruction with tissue expander.
 Breast Reconstruction Postmastectomy. Using DermaMatrix Acellular Dermis in breast reconstruction with tissue expander. Strong and flexible Bacterially inactivated Provides implant support Breast Reconstruction
Breast Reconstruction Postmastectomy. Using DermaMatrix Acellular Dermis in breast reconstruction with tissue expander. Strong and flexible Bacterially inactivated Provides implant support Breast Reconstruction
Thyroidectomy. Siu Kwan Ng. Modified Radical Neck Dissection Type II 47
 06 Thyroidectomy Siu Kwan Ng Modified Radical Neck Dissection Type II 47 Thyroidectomy STEP 1. EXPOSING THE THYROID GLAND The collar incision Figure 1 (curvilinear skin crease incision) is made at 1.5-2
06 Thyroidectomy Siu Kwan Ng Modified Radical Neck Dissection Type II 47 Thyroidectomy STEP 1. EXPOSING THE THYROID GLAND The collar incision Figure 1 (curvilinear skin crease incision) is made at 1.5-2
Exercise & Breast Cancer Recovery
 Exercise & Breast Cancer Recovery LEARNING OBJECTIVES Demonstrate an understanding of the diagnosis and treatment of breast cancer Demonstrate an understanding of how breast cancer surgery and treatment
Exercise & Breast Cancer Recovery LEARNING OBJECTIVES Demonstrate an understanding of the diagnosis and treatment of breast cancer Demonstrate an understanding of how breast cancer surgery and treatment
Gateway to the upper limb. An area of transition between the neck and the arm.
 Gateway to the upper limb An area of transition between the neck and the arm. Pyramidal space inferior to shoulder @ junction of arm & thorax Distribution center for the neurovascular structures that serve
Gateway to the upper limb An area of transition between the neck and the arm. Pyramidal space inferior to shoulder @ junction of arm & thorax Distribution center for the neurovascular structures that serve
Jake Hutchins, M.D. Aaron Berg, D.O.
 Jake Hutchins, M.D. Aaron Berg, D.O. Jacob Hutchins is on the speaker s bureau, is a consultant, and has received research funding from Pacira Pharmaceuticals He also is a consultant for Insitu Biologics,
Jake Hutchins, M.D. Aaron Berg, D.O. Jacob Hutchins is on the speaker s bureau, is a consultant, and has received research funding from Pacira Pharmaceuticals He also is a consultant for Insitu Biologics,
Clinical examination of the shoulder girdle
 Clinical of the shoulder girdle CHAPTER CONTENTS Symptoms referred to the shoulder girdle........ e72 Symptoms referred from the shoulder girdle...... e72 History........................... e72 Inspection.........................
Clinical of the shoulder girdle CHAPTER CONTENTS Symptoms referred to the shoulder girdle........ e72 Symptoms referred from the shoulder girdle...... e72 History........................... e72 Inspection.........................
Key Relationships in the Upper Limb
 Key Relationships in the Upper Limb This list contains some of the key relationships that will help you identify structures in the lab. They are organized by dissection assignment as defined in the syllabus.
Key Relationships in the Upper Limb This list contains some of the key relationships that will help you identify structures in the lab. They are organized by dissection assignment as defined in the syllabus.
The posterolateral thoracotomy is still probably the
 Posterolateral Thoracotomy Jean Deslauriers and Reza John Mehran The posterolateral thoracotomy is still probably the most commonly used incision in general thoracic surgery. It provides not only excellent
Posterolateral Thoracotomy Jean Deslauriers and Reza John Mehran The posterolateral thoracotomy is still probably the most commonly used incision in general thoracic surgery. It provides not only excellent
Alexander C Vlantis. Total Laryngectomy 57
 07 Total Laryngectomy Alexander C Vlantis Total Laryngectomy 57 Total Laryngectomy STEP 1 INCISION AND POSITION OF STOMA A superiorly based apron flap incision is marked with the horizontal limb placed
07 Total Laryngectomy Alexander C Vlantis Total Laryngectomy 57 Total Laryngectomy STEP 1 INCISION AND POSITION OF STOMA A superiorly based apron flap incision is marked with the horizontal limb placed
STEP 1 INCISION AND ELEVATION OF SKIN FLAP STEP 3 SEPARATE PAROTID GLAND FROM SCM STEP 2 IDENTIFICATON OF GREAT AURICULAR NERVE
 STEP 1 INCISION AND ELEVATION OF SKIN FLAP Create a modified Blair Figure 1 or facelift incision. Figure 2 Raise a superficial cervico-fascial flap between the Superficial Musculo Aponeurotic System (SMAS)
STEP 1 INCISION AND ELEVATION OF SKIN FLAP Create a modified Blair Figure 1 or facelift incision. Figure 2 Raise a superficial cervico-fascial flap between the Superficial Musculo Aponeurotic System (SMAS)
Breast Reconstruction Options
 Breast Reconstruction Options Natural reconstruction using your ABDOMINAL tissue: TRAM Flap (Transverse Rectus Abdominis Myocutaneous) There are various forms of TRAM flap reconstruction that are commonly
Breast Reconstruction Options Natural reconstruction using your ABDOMINAL tissue: TRAM Flap (Transverse Rectus Abdominis Myocutaneous) There are various forms of TRAM flap reconstruction that are commonly
Scapular & Parascapular flap FLAP TERRITORY ANATOMY. is normally accompanied by two venae comitantes.
 Scapular & Parascapular flap FLAP TERRITORY This is a composite flap that is situated over the scapula with various incisional arrangements. It can be harvested as a skin and subcutaneous tissue flap,
Scapular & Parascapular flap FLAP TERRITORY This is a composite flap that is situated over the scapula with various incisional arrangements. It can be harvested as a skin and subcutaneous tissue flap,
Breast Cancer Atlas for Radiation Therapy Planning: Consensus Definitions
 Breast Cancer Atlas for Radiation Therapy Planning: Consensus Definitions 1 Collaborators Julia White 1, An Tai 1, Douglas Arthur 2, Thomas Buchholz 3, Shannon MacDonald 4, Lawrence Marks 5, Lori Pierce
Breast Cancer Atlas for Radiation Therapy Planning: Consensus Definitions 1 Collaborators Julia White 1, An Tai 1, Douglas Arthur 2, Thomas Buchholz 3, Shannon MacDonald 4, Lawrence Marks 5, Lori Pierce
JPRAS Open 3 (2015) 1e5. Contents lists available at ScienceDirect. JPRAS Open. journal homepage:
 1e5. Contents lists available at ScienceDirect. JPRAS Open. journal homepage:") JPRAS Open 3 (2015) 1e5 Contents lists available at ScienceDirect JPRAS Open journal homepage: http://www.journals.elsevier.com/ jpras-open Case report The pedicled transverse partial latissimus dorsi
JPRAS Open 3 (2015) 1e5 Contents lists available at ScienceDirect JPRAS Open journal homepage: http://www.journals.elsevier.com/ jpras-open Case report The pedicled transverse partial latissimus dorsi
The Case FOR Oncoplastic Surgery in Small Breasts. Barbara L. Smith, MD, PhD Massachusetts General Hospital Harvard Medical School Boston, MA USA
 The Case FOR Oncoplastic Surgery in Small Breasts Barbara L. Smith, MD, PhD Massachusetts General Hospital Harvard Medical School Boston, MA USA Changing issues in breast cancer management Early detection
The Case FOR Oncoplastic Surgery in Small Breasts Barbara L. Smith, MD, PhD Massachusetts General Hospital Harvard Medical School Boston, MA USA Changing issues in breast cancer management Early detection
ISSN No: International Journal & Magazine of Engineering, Technology, Management and Research
 Vacuum Sealing Drainage Dressing Versus Negative Pressure Drainage Dressing Used After Modified Radical Mastectomy for Breast Cancer-A Prospective Randomized Clinical Trail Dr.Ninad Yeolkar M.B.B.S,M.S(Gen
Vacuum Sealing Drainage Dressing Versus Negative Pressure Drainage Dressing Used After Modified Radical Mastectomy for Breast Cancer-A Prospective Randomized Clinical Trail Dr.Ninad Yeolkar M.B.B.S,M.S(Gen
EndoBlade Soft Tissue Release System
 Surgical Technique Endoscopic Gastroc Recession Endoscopic Plantar Fascia Release EndoBlade Soft Tissue Release System Endoscopic Gastroc Recession Arthrex has developed a comprehensive, completely disposable
Surgical Technique Endoscopic Gastroc Recession Endoscopic Plantar Fascia Release EndoBlade Soft Tissue Release System Endoscopic Gastroc Recession Arthrex has developed a comprehensive, completely disposable
Breast cancer reconstruction surgery (immediate and delayed) across Ontario: Patient indications and appropriate surgical options
 across Ontario: Patient indications and appropriate surgical options") A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Breast cancer reconstruction surgery (immediate and delayed) across Ontario: Patient indications and appropriate
A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Breast cancer reconstruction surgery (immediate and delayed) across Ontario: Patient indications and appropriate
Posterior Triangle of the Neck By Prof. Dr. Muhammad Imran Qureshi
 Posterior Triangle of the Neck By Prof. Dr. Muhammad Imran Qureshi For the purpose of anatomical description the neck is sub divided into two major triangles, the Anterior and the Posterior by muscle bellies
Posterior Triangle of the Neck By Prof. Dr. Muhammad Imran Qureshi For the purpose of anatomical description the neck is sub divided into two major triangles, the Anterior and the Posterior by muscle bellies
VENOUS DRAINAGE O US F UPPER UPPER LIM B BY dr.fahad Ullah
 VENOUS DRAINAGE OF UPPER LIMB BY dr.fahad Ullah Venous drainage of the supper limb The venous system of the upper limb drains deoxygenated blood from the arm, forearm and hand It can anatomically be divided
VENOUS DRAINAGE OF UPPER LIMB BY dr.fahad Ullah Venous drainage of the supper limb The venous system of the upper limb drains deoxygenated blood from the arm, forearm and hand It can anatomically be divided
Endoscopic Soft Tissue Release System. SafeViewTM 360 Panoramic Visualization Sterile Packaged Fully Disposable
 L O W E R E X T R E M I T Y T E C H N I Q U E G U I D E Endoscopic Soft Tissue Release System SafeViewTM 360 Panoramic Visualization Sterile Packaged Fully Disposable Versatility and Control SafeView is
L O W E R E X T R E M I T Y T E C H N I Q U E G U I D E Endoscopic Soft Tissue Release System SafeViewTM 360 Panoramic Visualization Sterile Packaged Fully Disposable Versatility and Control SafeView is
Region of upper limb attachment to the trunk Proximal segment of limb overlaps parts of the trunk (thorax and back) and lower lateral neck.
 and lower lateral neck.") Region of upper limb attachment to the trunk Proximal segment of limb overlaps parts of the trunk (thorax and back) and lower lateral neck. includes Pectoral Scapular Deltoid regions of the upper limb
Region of upper limb attachment to the trunk Proximal segment of limb overlaps parts of the trunk (thorax and back) and lower lateral neck. includes Pectoral Scapular Deltoid regions of the upper limb
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY
 OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY RECTUS ABDOMINIS FLAP FOR HEAD & NECK RECONSTRUCTION Patrik Pipkorn, Brian Nussenbaum The rectus abdominis flap is based on the deep inferior
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY RECTUS ABDOMINIS FLAP FOR HEAD & NECK RECONSTRUCTION Patrik Pipkorn, Brian Nussenbaum The rectus abdominis flap is based on the deep inferior
Knee Disarticulation Amputation
 Knee Disarticulation Amputation Pre-Op 64 year old man, previous spinal cord injury, diabetes, renal failure, and a history of spasticity with dynamic knee flexion contracture. He had an open left ankle
Knee Disarticulation Amputation Pre-Op 64 year old man, previous spinal cord injury, diabetes, renal failure, and a history of spasticity with dynamic knee flexion contracture. He had an open left ankle
Debate Axillary dissection - con. Prof. Dr. Rodica Anghel Institute of Oncology Bucharest
 Debate Axillary dissection - con Prof. Dr. Rodica Anghel Institute of Oncology Bucharest Summer School of Oncology, third edition Updated Oncology 2015: State of the Art News & Challenging Topics Bucharest,
Debate Axillary dissection - con Prof. Dr. Rodica Anghel Institute of Oncology Bucharest Summer School of Oncology, third edition Updated Oncology 2015: State of the Art News & Challenging Topics Bucharest,
MIAA. Minimally Invasive Anterior Approach Surgical technique
 MIAA Minimally Invasive Anterior Approach Surgical technique Contents Introduction 3 With-Table MIAA technique 4 A1. Patient positioning/draping 4 A2. Skin incision 4 A3. Muscular dissection 4 A4. Muscle
MIAA Minimally Invasive Anterior Approach Surgical technique Contents Introduction 3 With-Table MIAA technique 4 A1. Patient positioning/draping 4 A2. Skin incision 4 A3. Muscular dissection 4 A4. Muscle
Selective salvage of zones 2 and 4 in the pedicled TRAM flap: a focus on reducing fat necrosis and improving aesthetic outcomes
 DOI 10.1186/s40064-016-1714-7 RESEARCH Open Access Selective salvage of zones 2 and 4 in the pedicled TRAM flap: a focus on reducing fat necrosis and improving aesthetic outcomes Chi Sun Yoon and Kyu Nam
DOI 10.1186/s40064-016-1714-7 RESEARCH Open Access Selective salvage of zones 2 and 4 in the pedicled TRAM flap: a focus on reducing fat necrosis and improving aesthetic outcomes Chi Sun Yoon and Kyu Nam
PRINCIPLES OF BREAST SURGERY & COMPLICATIONS
 PRINCIPLES OF BREAST SURGERY & COMPLICATIONS Adam Cichowitz The Royal Melbourne Hospital ANATOMY Lies in subcutaneous tissue Base: midline to midaxillary line, 2nd to 6th rib Overlies pec major, serratus
PRINCIPLES OF BREAST SURGERY & COMPLICATIONS Adam Cichowitz The Royal Melbourne Hospital ANATOMY Lies in subcutaneous tissue Base: midline to midaxillary line, 2nd to 6th rib Overlies pec major, serratus
Breast Restoration Surgery After a mastectomy
 UW MEDICINE PATIENT EDUCATION Breast Restoration Surgery After a mastectomy This handout explains the most common procedures that are used at University of Washington Medical Center (UWMC) to restore a
UW MEDICINE PATIENT EDUCATION Breast Restoration Surgery After a mastectomy This handout explains the most common procedures that are used at University of Washington Medical Center (UWMC) to restore a
Circumareolar Mastopexy
 Circumareolar Mastopexy and Moderate Reduction drien iache n mastopexy the problems created by the doughnut-type excision and scarring are relatively minimal, because the breast tissue is not excised and
Circumareolar Mastopexy and Moderate Reduction drien iache n mastopexy the problems created by the doughnut-type excision and scarring are relatively minimal, because the breast tissue is not excised and
complicanze in chirurgia senologica ricostruttiva Tecniche per la prevenzione delle complicanze nelle mastectomie conservative
 Il trattamento delle complicanze in chirurgia senologica ricostruttiva Tecniche per la prevenzione delle complicanze nelle mastectomie conservative Dr. Christian Rizzetto UOC Chirurgia Senologica - Breast
Il trattamento delle complicanze in chirurgia senologica ricostruttiva Tecniche per la prevenzione delle complicanze nelle mastectomie conservative Dr. Christian Rizzetto UOC Chirurgia Senologica - Breast
X-Plain Breast Cancer Surgery Reference Summary
 X-Plain Breast Cancer Surgery Reference Summary Introduction Breast lumps are a common condition that affects millions of women every year. Breast lumps may be cancerous. Breast cancer occurs in approximately
X-Plain Breast Cancer Surgery Reference Summary Introduction Breast lumps are a common condition that affects millions of women every year. Breast lumps may be cancerous. Breast cancer occurs in approximately
SURGICAL PROCEDURE DESCRIPTIONS
 SURGICAL PROCEDURE DESCRIPTIONS GONADECTOMY: CASTRATION USING SCROTAL METHOD 1. The animal is anesthetized and placed in dorsal recumbency with the tail toward the surgeon. 2. The abdominal and scrotal
SURGICAL PROCEDURE DESCRIPTIONS GONADECTOMY: CASTRATION USING SCROTAL METHOD 1. The animal is anesthetized and placed in dorsal recumbency with the tail toward the surgeon. 2. The abdominal and scrotal
Pectoral region. Lecture 2
 Pectoral region Lecture 2 Muscle Action Each muscle has: Origin Beginning. Insertion End. Body (belly). Law: When a muscle performs its action, its insertion, moves towards its origin. Spring 2016 Dr.
Pectoral region Lecture 2 Muscle Action Each muscle has: Origin Beginning. Insertion End. Body (belly). Law: When a muscle performs its action, its insertion, moves towards its origin. Spring 2016 Dr.
BREAST RECONSTRUCTION POST MASTECTOMY
 UnitedHealthcare Commercial Coverage Determination Guideline BREAST RECONSTRUCTION POST MASTECTOMY Guideline Number: SUR057 Effective Date: January 1, 2019 Table of Contents Page INSTRUCTIONS FOR USE...
UnitedHealthcare Commercial Coverage Determination Guideline BREAST RECONSTRUCTION POST MASTECTOMY Guideline Number: SUR057 Effective Date: January 1, 2019 Table of Contents Page INSTRUCTIONS FOR USE...
Surgical Anatomy of the Hip. Joseph H. Dimon
 Surgical Anatomy of the Hip Joseph H. Dimon The hip joint is a deep joint surrounded by large and powerful muscles necessary for its proper function. Essential neurovascular structures lie in front and
Surgical Anatomy of the Hip Joseph H. Dimon The hip joint is a deep joint surrounded by large and powerful muscles necessary for its proper function. Essential neurovascular structures lie in front and
2. List the 8 pelvic spaces: list one procedure or dissection which involves entering that space.
 Name: Anatomy Quiz: Pre / Post 1. In making a pfannensteil incision you would traverse through the following layers: a) Skin, Camper s fascia, Scarpa s fascia, external oblique aponeurosis, internal oblique
Name: Anatomy Quiz: Pre / Post 1. In making a pfannensteil incision you would traverse through the following layers: a) Skin, Camper s fascia, Scarpa s fascia, external oblique aponeurosis, internal oblique
Jordan University Faculty Of Medicine. Breast. Dr. Ahmed Salman. Assistant professor of anatomy & embryology
 Jordan University Faculty Of Medicine Breast Dr. Ahmed Salman Assistant professor of anatomy & embryology The breasts are specialized accessory glands of the skin that secretes milk. They are situated
Jordan University Faculty Of Medicine Breast Dr. Ahmed Salman Assistant professor of anatomy & embryology The breasts are specialized accessory glands of the skin that secretes milk. They are situated
THE MANAGEMENT OF THE SWOLLEN ARM IN CARCINOMA OF THE BREAST
 THE MANAGEMENT OF THE SWOLLEN ARM IN CARCINOMA OF THE BREAST NORMAN TREVES, M.D. The terms "brawny arm" and "lymphedema" have been given to the swollen arm which may complicate the inoperable, recurrent,
THE MANAGEMENT OF THE SWOLLEN ARM IN CARCINOMA OF THE BREAST NORMAN TREVES, M.D. The terms "brawny arm" and "lymphedema" have been given to the swollen arm which may complicate the inoperable, recurrent,
A Manual Therapy and Exercise Approach to Breast Cancer Rehabilitation Course
 2014 Annual Breast Cancer Rehabilitation Healthcare Provider Event A Manual Therapy and Exercise Approach to Breast Cancer Rehabilitation Course November 7 th and 8 th, 2014 Mercer University, Atlanta,
2014 Annual Breast Cancer Rehabilitation Healthcare Provider Event A Manual Therapy and Exercise Approach to Breast Cancer Rehabilitation Course November 7 th and 8 th, 2014 Mercer University, Atlanta,
BREAST RECONSTRUCTION POST MASTECTOMY
 UnitedHealthcare Commercial Coverage Determination Guideline BREAST RECONSTRUCTION POST MASTECTOMY Guideline Number: SUR057 Effective Date: February 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE...
UnitedHealthcare Commercial Coverage Determination Guideline BREAST RECONSTRUCTION POST MASTECTOMY Guideline Number: SUR057 Effective Date: February 1, 2018 Table of Contents Page INSTRUCTIONS FOR USE...
Tor Chiu. Deep Inferior Epigastric Artery Perforator Flap 161
 18 Deep Inferior Epigastric Artery Perforator Flap Tor Chiu Deep Inferior Epigastric Artery Perforator Flap 161 Deep Inferior Epigastric Artery Perforator Flap FLAP TERRITORY The deep inferior epigastric
18 Deep Inferior Epigastric Artery Perforator Flap Tor Chiu Deep Inferior Epigastric Artery Perforator Flap 161 Deep Inferior Epigastric Artery Perforator Flap FLAP TERRITORY The deep inferior epigastric
Thoracic outlet syndrome: first rib resection
 Review rticle Page 1 of 7 Thoracic outlet syndrome: first rib resection ornelis G. Vos 1, Çag das Ünlü 1, Michiel T. Voûte 2, Rob H. W. van de Mortel 3, Jean-Paul P. M. de Vries 3 1 Department of Surgery,
Review rticle Page 1 of 7 Thoracic outlet syndrome: first rib resection ornelis G. Vos 1, Çag das Ünlü 1, Michiel T. Voûte 2, Rob H. W. van de Mortel 3, Jean-Paul P. M. de Vries 3 1 Department of Surgery,
MUSCLES. Anconeus Muscle
 LAB 7 UPPER LIMBS MUSCLES Anconeus Muscle anconeus origin: distal end of dorsal surface of humerus insertion: lateral surface of ulna from distal margin of the semilunar notch to proximal end of the olecranon
LAB 7 UPPER LIMBS MUSCLES Anconeus Muscle anconeus origin: distal end of dorsal surface of humerus insertion: lateral surface of ulna from distal margin of the semilunar notch to proximal end of the olecranon
3 Mohammad Al-Mohtasib Areej Mosleh
 3 Mohammad Al-Mohtasib Areej Mosleh ***Muscles Connecting the Upper Limb to the Vertebral Column 1.Trapezius Muscle ***The first muscle on the back is trapezius muscle, it s called so according
3 Mohammad Al-Mohtasib Areej Mosleh ***Muscles Connecting the Upper Limb to the Vertebral Column 1.Trapezius Muscle ***The first muscle on the back is trapezius muscle, it s called so according
Transfemoral Amputation
 Transfemoral Amputation Preop This 26 year old male sustained a gunshot wound to the left thigh. He was treated emergently with revascularization and fasciotomies. He was transferred to our regional trauma
Transfemoral Amputation Preop This 26 year old male sustained a gunshot wound to the left thigh. He was treated emergently with revascularization and fasciotomies. He was transferred to our regional trauma
Breast Reconstruction Surgery
 Breast Reconstruction Surgery I. Policy University Health Alliance (UHA) will reimburse for Breast Reconstruction Surgery when it is determined to be medically necessary and when it meets the medical criteria
Breast Reconstruction Surgery I. Policy University Health Alliance (UHA) will reimburse for Breast Reconstruction Surgery when it is determined to be medically necessary and when it meets the medical criteria
This figure (of humerus) is from Dr. Maher's newest slides. -Its added here just for consideration-
 is from Dr. Maher's newest slides. -Its added here just for consideration-") This figure (of humerus) is from Dr. Maher's newest slides. -Its added here just for consideration- Slides of Anatomy Please note : These slides are Dr. Maher Hadidi s slides of spring 2016 and were edited
This figure (of humerus) is from Dr. Maher's newest slides. -Its added here just for consideration- Slides of Anatomy Please note : These slides are Dr. Maher Hadidi s slides of spring 2016 and were edited
Endoscopic assisted harvest of the pedicled pectoralis major muscle flap
 British Journal of Plastic Surgery (2005) 58, 170 174 Endoscopic assisted harvest of the pedicled pectoralis major muscle flap Arif Turkmen*, A. Graeme B. Perks Plastic Surgery Department, Nottingham City
British Journal of Plastic Surgery (2005) 58, 170 174 Endoscopic assisted harvest of the pedicled pectoralis major muscle flap Arif Turkmen*, A. Graeme B. Perks Plastic Surgery Department, Nottingham City
Superior Pedicle Vertical Scar Mammaplasty: Surgical Technique
 Superior Pedicle Vertical Scar Mammaplasty: Surgical Technique 4 Foad Nahai A man honours himself by not displaying all the knowledge he has acquired. Folk Tradition Introduction I first tried the vertical
Superior Pedicle Vertical Scar Mammaplasty: Surgical Technique 4 Foad Nahai A man honours himself by not displaying all the knowledge he has acquired. Folk Tradition Introduction I first tried the vertical
Anatomical Study of Pectoral Nerves and its Implications in Surgery
 DOI: 10.7860/JCDR/2014/8631.4545 Anatomy Section Original Article Anatomical Study of Pectoral Nerves and its Implications in Surgery Prakash KG 1, Saniya K 2 ABSTRACT Introduction: This anatomical study
DOI: 10.7860/JCDR/2014/8631.4545 Anatomy Section Original Article Anatomical Study of Pectoral Nerves and its Implications in Surgery Prakash KG 1, Saniya K 2 ABSTRACT Introduction: This anatomical study
The Thoracic wall including the diaphragm. Prof Oluwadiya KS
 The Thoracic wall including the diaphragm Prof Oluwadiya KS www.oluwadiya.com Components of the thoracic wall Skin Superficial fascia Chest wall muscles (see upper limb slides) Skeletal framework Intercostal
The Thoracic wall including the diaphragm Prof Oluwadiya KS www.oluwadiya.com Components of the thoracic wall Skin Superficial fascia Chest wall muscles (see upper limb slides) Skeletal framework Intercostal
Strattice Reconstructive Tissue Matrix used in the repair of rippling
 Clinical case study Strattice Tissue Matrix Strattice Reconstructive Tissue Matrix used in the repair of rippling Steven Teitelbaum, MD* Santa Monica, CA Case summary A 48-year-old woman with a history
Clinical case study Strattice Tissue Matrix Strattice Reconstructive Tissue Matrix used in the repair of rippling Steven Teitelbaum, MD* Santa Monica, CA Case summary A 48-year-old woman with a history
Septic Bone and Joint Surgery
 Septic Bone and Joint Surgery Bearbeitet von Reinhard Schnettler 1. Auflage 2010. Buch. 328 S. Hardcover ISBN 978 3 13 149031 5 Format (B x L): 19,5 x 27 cm Weitere Fachgebiete > Medizin > Chirurgie >
Septic Bone and Joint Surgery Bearbeitet von Reinhard Schnettler 1. Auflage 2010. Buch. 328 S. Hardcover ISBN 978 3 13 149031 5 Format (B x L): 19,5 x 27 cm Weitere Fachgebiete > Medizin > Chirurgie >
FASCIAL PLANE BLOCKS TOM BARIBEAULT MSN, CRNA
 FASCIAL PLANE BLOCKS TOM BARIBEAULT MSN, CRNA TECHNIQUES Abdominal Wall TAP Rectus Sheath Quadratus Lumborum Erector Spinae Chest PECS I & II Erector Spinae TECHNIQUES Knee Ipack/LIA Hip Fascia Iliaca
FASCIAL PLANE BLOCKS TOM BARIBEAULT MSN, CRNA TECHNIQUES Abdominal Wall TAP Rectus Sheath Quadratus Lumborum Erector Spinae Chest PECS I & II Erector Spinae TECHNIQUES Knee Ipack/LIA Hip Fascia Iliaca
Radiation-induced Brachial Plexopathy: MR Imaging
 Radiation-induced Brachial Plexopathy 85 Chapter 5 Radiation-induced Brachial Plexopathy: MR Imaging Neurological symptoms and signs of brachial plexopathy may develop in patients who have had radiation
Radiation-induced Brachial Plexopathy 85 Chapter 5 Radiation-induced Brachial Plexopathy: MR Imaging Neurological symptoms and signs of brachial plexopathy may develop in patients who have had radiation
Case Scenario 1. 2/15/2011 The patient received IMRT 45 Gy at 1.8 Gy per fraction for 25 fractions.
 Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
ONCOPLASTIC SURGERY. Dr. Sadir Alrawi Director of Surgical Oncology Services. Dr. Humaa Darr Surgical Oncology Fellow
 Hessa St ONCOPLASTIC SURGERY Dr. Sadir Alrawi Director of Surgical Oncology Services Dr. Humaa Darr Surgical Oncology Fellow Al Sufouh Rd AL SUFOUH AL SUFOUH Sharaf DG Mall of the Emirates Mall Of the
Hessa St ONCOPLASTIC SURGERY Dr. Sadir Alrawi Director of Surgical Oncology Services Dr. Humaa Darr Surgical Oncology Fellow Al Sufouh Rd AL SUFOUH AL SUFOUH Sharaf DG Mall of the Emirates Mall Of the
Parenchyma-sparing lung resections are a potential therapeutic
 Lung Segmentectomy for Patients with Peripheral T1 Lesions Bryan A. Whitson, MD, Rafael S. Andrade, MD, and Michael A. Maddaus, MD Parenchyma-sparing lung resections are a potential therapeutic option
Lung Segmentectomy for Patients with Peripheral T1 Lesions Bryan A. Whitson, MD, Rafael S. Andrade, MD, and Michael A. Maddaus, MD Parenchyma-sparing lung resections are a potential therapeutic option
Brachial plexuses and axillary lymph nodes
 Brachial plexuses and axillary lymph nodes Introduction about nervous system nervous system central nervous system periphral nervous system brain spinal cord 31 pairs of spinal nerves 12 paris of cranial
Brachial plexuses and axillary lymph nodes Introduction about nervous system nervous system central nervous system periphral nervous system brain spinal cord 31 pairs of spinal nerves 12 paris of cranial
Upper extremity. Part I
 Part I Upper extremity 1 Fractures of the clavicle Peter V. Giannoudis 1.1 OPEN REDUCTION AND INTERNAL FIXATION (ORIF) OF MIDSHAFT FRACTURES Indications (a) Open fractures. (b) Painful non-union. (c) Associated
Part I Upper extremity 1 Fractures of the clavicle Peter V. Giannoudis 1.1 OPEN REDUCTION AND INTERNAL FIXATION (ORIF) OF MIDSHAFT FRACTURES Indications (a) Open fractures. (b) Painful non-union. (c) Associated
Breast Surgery: Yesterday, Today and Tomorrow
 Breast Surgery: Yesterday, Today and Tomorrow Baptist Hospital Gladys L. Giron, MD, FACS October 11,2014 Homestead Hospital Baptist Children s Hospital Doctors Hospital Baptist Cardiac & Vascular Institute
Breast Surgery: Yesterday, Today and Tomorrow Baptist Hospital Gladys L. Giron, MD, FACS October 11,2014 Homestead Hospital Baptist Children s Hospital Doctors Hospital Baptist Cardiac & Vascular Institute
BREAST AUGMENTATION TECHNIQUES
 BREAST AUGMENTATION TECHNIQUES Breast Augmentation Top Surgical Procedure in 2015 (Worldwide) Surgical Procedure : Breast Augmentation Rank : 1 Total : 1,488,992 Percent of Total Surgical Procedures :
BREAST AUGMENTATION TECHNIQUES Breast Augmentation Top Surgical Procedure in 2015 (Worldwide) Surgical Procedure : Breast Augmentation Rank : 1 Total : 1,488,992 Percent of Total Surgical Procedures :
Anatomical information for intercostobrachial nerve preservation in axillary lymph node dissection for breast cancer
 Anatomical information for intercostobrachial nerve preservation in axillary lymph node dissection for breast cancer J.J. Zhu 1 *, X.F. Liu 1, P.L. Zhang 1, J.Z. Yang 1, J. Wang 2, Y. Qin 1, G.L. Zhang
Anatomical information for intercostobrachial nerve preservation in axillary lymph node dissection for breast cancer J.J. Zhu 1 *, X.F. Liu 1, P.L. Zhang 1, J.Z. Yang 1, J. Wang 2, Y. Qin 1, G.L. Zhang
Frederick J. Duffy, Jr., MD, FACS and Brice W. McKane, MD, FACS BREAST RECONSTRUCTION
 Frederick J. Duffy, Jr., MD, FACS and Brice W. McKane, MD, FACS BREAST RECONSTRUCTION BREAST RECONSTRUCTION: A WOMAN S DECISION Options and Information Our approach to breast reconstruction entails a very
Frederick J. Duffy, Jr., MD, FACS and Brice W. McKane, MD, FACS BREAST RECONSTRUCTION BREAST RECONSTRUCTION: A WOMAN S DECISION Options and Information Our approach to breast reconstruction entails a very
COPE Library Sample
 Breast Anatomy LOBULE LOBE ACINI (MILK PRODUCING UNITS) NIPPLE AREOLA COMPLEX ENLARGEMENT OF DUCT AND LOBE LOBULE SUPRACLAVICULAR NODES INFRACLAVICULAR NODES DUCT DUCT ACINI (MILK PRODUCING UNITS) 8420
Breast Anatomy LOBULE LOBE ACINI (MILK PRODUCING UNITS) NIPPLE AREOLA COMPLEX ENLARGEMENT OF DUCT AND LOBE LOBULE SUPRACLAVICULAR NODES INFRACLAVICULAR NODES DUCT DUCT ACINI (MILK PRODUCING UNITS) 8420
Tips for using shaped implants in breast augmentation
 Tips for using shaped implants in breast augmentation Sientra would like to thank Dr. Patricia McGuire of St. Louis, MO for her significant contributions to Sientra s educational efforts. Dr. McGuire has
Tips for using shaped implants in breast augmentation Sientra would like to thank Dr. Patricia McGuire of St. Louis, MO for her significant contributions to Sientra s educational efforts. Dr. McGuire has
Pectoral region. Lecture 2
 Pectoral region Lecture 2 Muscle Action Each muscle has: Origin Beginning. Insertion End. Body (belly). Law: When a muscle performs its action, its insertion, moves towards its origin. Spring 2016 Dr.
Pectoral region Lecture 2 Muscle Action Each muscle has: Origin Beginning. Insertion End. Body (belly). Law: When a muscle performs its action, its insertion, moves towards its origin. Spring 2016 Dr.
Surgeries of the breast are among the most common operative
 REGIONAL ANESTHESIA AND ACUTE PAIN REVIEW ARTICLE A Qualitative Review of Anatomy and Regional Techniques Glenn E. Woodworth, MD,* Ryan M.J. Ivie, MD,* Sylvia M. Nelson, PhD,* Cameron M. Walker, PhD,*
REGIONAL ANESTHESIA AND ACUTE PAIN REVIEW ARTICLE A Qualitative Review of Anatomy and Regional Techniques Glenn E. Woodworth, MD,* Ryan M.J. Ivie, MD,* Sylvia M. Nelson, PhD,* Cameron M. Walker, PhD,*
Candidate s instructions Look at this cross-section taken at the level of C5. Answer the following questions.
 Section 1 Anatomy Chapter 1. Trachea 1 Candidate s instructions Look at this cross-section taken at the level of C5. Answer the following questions. Pretracheal fascia 1 2 5 3 4 Questions 1. Label the
Section 1 Anatomy Chapter 1. Trachea 1 Candidate s instructions Look at this cross-section taken at the level of C5. Answer the following questions. Pretracheal fascia 1 2 5 3 4 Questions 1. Label the
17 FibulA FlAP Tor Chiu fibula flap 153
 17 Fibula Flap Tor Chiu Fibula Flap 153 Fibula Flap FLAP TERRITORY This flap includes a segment of the fibular bone with or without the overlying skin island on the peroneal/ lateral aspect of the calf.
17 Fibula Flap Tor Chiu Fibula Flap 153 Fibula Flap FLAP TERRITORY This flap includes a segment of the fibular bone with or without the overlying skin island on the peroneal/ lateral aspect of the calf.
Algorithm for Autologous Breast Reconstruction for Partial Mastectomy Defects
 Algorithm for Autologous Breast Reconstruction for Partial Mastectomy Defects Joshua L. Levine, M.D., Nassif E. Soueid, M.D., and Robert J. Allen, M.D. New Orleans, La. Background: The use of lateral thoracic
Algorithm for Autologous Breast Reconstruction for Partial Mastectomy Defects Joshua L. Levine, M.D., Nassif E. Soueid, M.D., and Robert J. Allen, M.D. New Orleans, La. Background: The use of lateral thoracic
JMSCR Volume 03 Issue 01 Page January 2015
 www.jmscr.igmpublication.org Impact Factor 3.79 ISSN (e)-2347-176x Is Surgical Exposure of Scapula Through Direct Lateral Approach Preferable? Authors Dr. Dibakar Ray 1, Dr. Ashoke Kumar Chanda 2, Dr.
www.jmscr.igmpublication.org Impact Factor 3.79 ISSN (e)-2347-176x Is Surgical Exposure of Scapula Through Direct Lateral Approach Preferable? Authors Dr. Dibakar Ray 1, Dr. Ashoke Kumar Chanda 2, Dr.
Breast cancer: an update
 Breast cancer: an update Dr. Sanjeewa Seneviratne M.D, MRCS, Ph.D. Senior Lecturer and Honorary Consultant Surgeon Department of Surgery Faculty of Medicine, Colombo Plan The problem Screening & early
Breast cancer: an update Dr. Sanjeewa Seneviratne M.D, MRCS, Ph.D. Senior Lecturer and Honorary Consultant Surgeon Department of Surgery Faculty of Medicine, Colombo Plan The problem Screening & early
Technique Guide. VersiTomic G-Lok. J. Martin Leland III, M.D. Sub-Pectoral Proximal Biceps Tenodesis
 Technique Guide VersiTomic G-Lok Sub-Pectoral Proximal Biceps Tenodesis J. Martin Leland III, M.D. The opinions expressed are those of Dr. Leland and are not necessarily those of Stryker. Sub-Pectoral
Technique Guide VersiTomic G-Lok Sub-Pectoral Proximal Biceps Tenodesis J. Martin Leland III, M.D. The opinions expressed are those of Dr. Leland and are not necessarily those of Stryker. Sub-Pectoral
Reconstruction of the Breast after Cancer An Overview of Procedures and Options by Karen M. Horton, MD, MSc, FRCSC
 Downloaded from Reconstruction of the Breast after Cancer An Overview of Procedures and Options by Karen M. Horton, MD, MSc, FRCSC What is Breast Reconstruction? Reconstruction of the breast involves recreating
Downloaded from Reconstruction of the Breast after Cancer An Overview of Procedures and Options by Karen M. Horton, MD, MSc, FRCSC What is Breast Reconstruction? Reconstruction of the breast involves recreating
Background & Indications Probe Selection
 Teresa S. Wu, MD, FACEP Director, EM Ultrasound Program & Fellowship Co-Director, Simulation Based Training Program & Fellowship Associate Program Director, EM Residency Program Maricopa Medical Center
Teresa S. Wu, MD, FACEP Director, EM Ultrasound Program & Fellowship Co-Director, Simulation Based Training Program & Fellowship Associate Program Director, EM Residency Program Maricopa Medical Center
Transfemoral Amputation
 Transfemoral Amputation Pre-Op: 42 year old male who sustained severe injuries in a motorcycle accident. Note: he is a previous renal transplant recipient and is on immunosuppressive treatments. His injuries
Transfemoral Amputation Pre-Op: 42 year old male who sustained severe injuries in a motorcycle accident. Note: he is a previous renal transplant recipient and is on immunosuppressive treatments. His injuries
Surgery Under Regional Anesthesia
 Surgery Under Regional Anesthesia Jean Daniel Eloy, MD Assistant Professor Residency Program Director Rutgers-New Jersey Medical School Rutgers The State University of New Jersey Peripheral Nerve Block
Surgery Under Regional Anesthesia Jean Daniel Eloy, MD Assistant Professor Residency Program Director Rutgers-New Jersey Medical School Rutgers The State University of New Jersey Peripheral Nerve Block
ABDOMINAL WALL & RECTUS SHEATH
 ABDOMINAL WALL & RECTUS SHEATH Learning Objectives Describe the anatomy, innervation and functions of the muscles of the anterior, lateral and posterior abdominal walls. Discuss their functional relations
ABDOMINAL WALL & RECTUS SHEATH Learning Objectives Describe the anatomy, innervation and functions of the muscles of the anterior, lateral and posterior abdominal walls. Discuss their functional relations
Augmentation of the Ptotic Breast: Simultaneous Periareolar Mastopexy/Breast Augmentation By: Laurence Kirwan, M.D., F.R.C.S
 Augmentation of the Ptotic Breast: Simultaneous Periareolar Mastopexy/Breast Augmentation By: Laurence Kirwan, M.D., F.R.C.S Background: Submusculofascial augmentation of the ptotic breast can result in
Augmentation of the Ptotic Breast: Simultaneous Periareolar Mastopexy/Breast Augmentation By: Laurence Kirwan, M.D., F.R.C.S Background: Submusculofascial augmentation of the ptotic breast can result in
FUNCTIONAL ANATOMY OF SHOULDER JOINT
 FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
FUNCTIONAL ANATOMY OF SHOULDER JOINT ARTICULATION Articulation is between: The rounded head of the Glenoid cavity humerus and The shallow, pear-shaped glenoid cavity of the scapula. 2 The articular surfaces
The Alvin & Lois Lapidus Cancer Institute BREAST CANCER
 The Alvin & Lois Lapidus Cancer Institute BREAST CANCER What is breast cancer? Breast cancer is a disease in which cancer cells form in the tissues of the breast. The breast is made up of lobes and ducts.
The Alvin & Lois Lapidus Cancer Institute BREAST CANCER What is breast cancer? Breast cancer is a disease in which cancer cells form in the tissues of the breast. The breast is made up of lobes and ducts.
2013 MCT CPC-H Quiz #8 Chapters 13 and 14
 2013 MCT CPC-H Quiz #8 Chapters 13 and 14 Name: Date: Instructor: Score: 1. A female patient presents to the outpatient clinic for excision of a 4.8 cm malignant melanoma of the left inner thigh. A 6 cm
2013 MCT CPC-H Quiz #8 Chapters 13 and 14 Name: Date: Instructor: Score: 1. A female patient presents to the outpatient clinic for excision of a 4.8 cm malignant melanoma of the left inner thigh. A 6 cm
Chapter 2. Simple Nephrectomy. Please Give Three Tips for Laparoscopic Simple Nephrectomy. Dr. de la Rosette
 Chapter 2 Simple Nephrectomy Please Give Three Tips for Laparoscopic Simple Nephrectomy............. 39 How Does One Find the Renal Hilum during Transperitoneal Laparoscopic Nephrectomy?.................
Chapter 2 Simple Nephrectomy Please Give Three Tips for Laparoscopic Simple Nephrectomy............. 39 How Does One Find the Renal Hilum during Transperitoneal Laparoscopic Nephrectomy?.................
Resection of malignant tumors invading the thoracic inlet
 Resection of Superior Sulcus Tumors: Anterior Approach Marc de Perrot, MD, MSc Resection of malignant tumors invading the thoracic inlet represents a technical challenge because of the complex anatomy
Resection of Superior Sulcus Tumors: Anterior Approach Marc de Perrot, MD, MSc Resection of malignant tumors invading the thoracic inlet represents a technical challenge because of the complex anatomy
Upper Limb Muscles Muscles of Axilla & Arm
 Done By : Saleh Salahat Upper Limb Muscles Muscles of Axilla & Arm 1) Muscles around the axilla A- Muscles connecting the upper to thoracic wall (4) 1- pectoralis major Origin:- from the medial half of
Done By : Saleh Salahat Upper Limb Muscles Muscles of Axilla & Arm 1) Muscles around the axilla A- Muscles connecting the upper to thoracic wall (4) 1- pectoralis major Origin:- from the medial half of
G24: Shoulder and Axilla
 G24: Shoulder and Axilla Syllabus - Pg. 2 ANAT 6010- Medical Gross Anatomy David A. Morton, Ph.D. Objectives Upper limb Systemically: Bones (joints) Muscles Nerves Vessels (arteries/veins) Fascial compartments
G24: Shoulder and Axilla Syllabus - Pg. 2 ANAT 6010- Medical Gross Anatomy David A. Morton, Ph.D. Objectives Upper limb Systemically: Bones (joints) Muscles Nerves Vessels (arteries/veins) Fascial compartments
Technique Guide. A natural product for a natural repair. Post-Mastectomy Breast Reconstruction
 A natural product for a natural repair. Acellular Dermal Matrix Tissue In Conjunction With Soft Tissue Repair Technique Guide Post-Mastectomy Breast Reconstruction This Technique Guide contains the opinions
A natural product for a natural repair. Acellular Dermal Matrix Tissue In Conjunction With Soft Tissue Repair Technique Guide Post-Mastectomy Breast Reconstruction This Technique Guide contains the opinions
How can surgeons help the Radiation Oncologists?
 How can surgeons help the Radiation Oncologists? Lorna Weir BC Surgical Oncology fall breast cancer update Oct 24, 2009 Disclosure no conflict of interest Outline Introduction OR reports Marking of surgical
How can surgeons help the Radiation Oncologists? Lorna Weir BC Surgical Oncology fall breast cancer update Oct 24, 2009 Disclosure no conflict of interest Outline Introduction OR reports Marking of surgical
Centerline Carpal Tunnel Release
 Centerline Endoscopic Carpal Tunnel Release Surgical Technique Centerline Carpal Tunnel Release Centerline Endoscopic Carpal Tunnel Release Surgical Set Up The patient is positioned supine on the operating
Centerline Endoscopic Carpal Tunnel Release Surgical Technique Centerline Carpal Tunnel Release Centerline Endoscopic Carpal Tunnel Release Surgical Set Up The patient is positioned supine on the operating