Ablation Update and Case Studies. Lawrence Nair, MD, FACC Director of Electrophysiology Presbyterian Heart Group
|
|
|
- Richard Stone
- 6 years ago
- Views:
Transcription
1 Ablation Update and Case Studies Lawrence Nair, MD, FACC Director of Electrophysiology Presbyterian Heart Group
2 Disclosures No financial relationships to disclose
3 Objectives At the conclusion of this activity, participants will be able to: 1.Recognize the indications for an ablation. 2. Identify the alternatives, risks and success rate of an ablation procedure. 3. Compare case studies of various arrhythmias, including SVT, atrial flutter and atrial fibrillation.
4 Intracardiac Electrograms

5
6 Indications for Ablation Common Arrhythmias SVT Atrial Flutter Atrial Fibrillation PVCs/Ventricular Tachycardia Risks and Benefits Alternatives Introduction
7 Classifications of Recommendations and Level of Evidence Class I Benefit>>>Risk Treatment should be performed Class IIa Benefit >>Risk Reasonable to Perform Class IIb Benefit >Risk Treatment may Be considered Class III No Benefit, possible harm Level A Multiple randomized clinical trials Recommendation that treatment is effective Recommendation in favor of treatment Some conflicting evidence Recommendation for treatment less well established. Greater conflicting evidence Recommendation that treatment is not useful and may be harmful Level B Single randomized trial or nonrandomized studies Recommendation that treatment is effective Recommendation in favor of treatment Some conflicting evidence Recommendation for treatment less well established. Greater conflicting evidence Recommendation that treatment is not useful and may be harmful Level C Consensus opinion, case studies, standard of care Recommendation that treatment is effective Recommendation in favor of treatment Some conflicting evidence Recommendation for treatment less well established. Greater conflicting evidence Recommendation that treatment is not useful and may be harmful
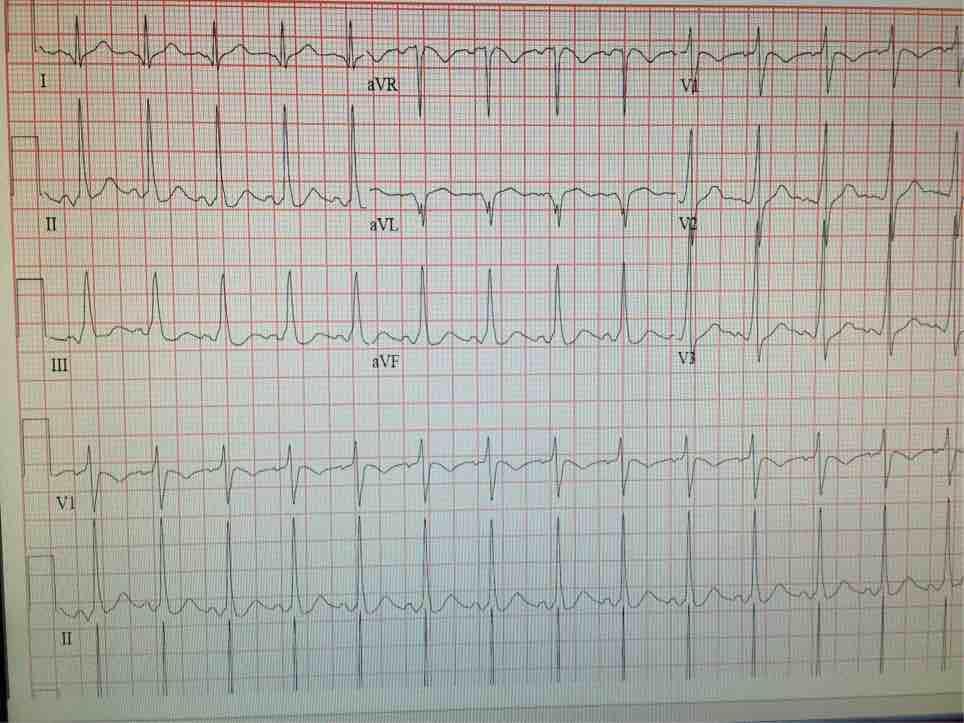
8 SVT 69 year old man presents to the ED with 90 minutes of palpitations and dizziness. He reports 3 similar episodes over the past two years. These episodes are typically associated with polyuria. Physical exam is notable for cannon a waves in his jugular veins. ECG reveals a narrow complex tachycardia with no evidence of P waves. Vagal maneuvers are ineffective. SVT is terminated with 6 mg of IV adenosine.
9 Narrow QRS Tachycardia No Visible P Waves Yes Yes Regular Tachycardia No Afib or aflutter with variable conduction AVNRT A rate > V rate No RP < PR (P after QRS) Yes No Aflutter or Atrial tach Yes RP < 90 msec Atrial tach, Atypical AVNRT, or PJRT Yes AVNRT No AVRT, Atypical AVNRT, or Atrial tach
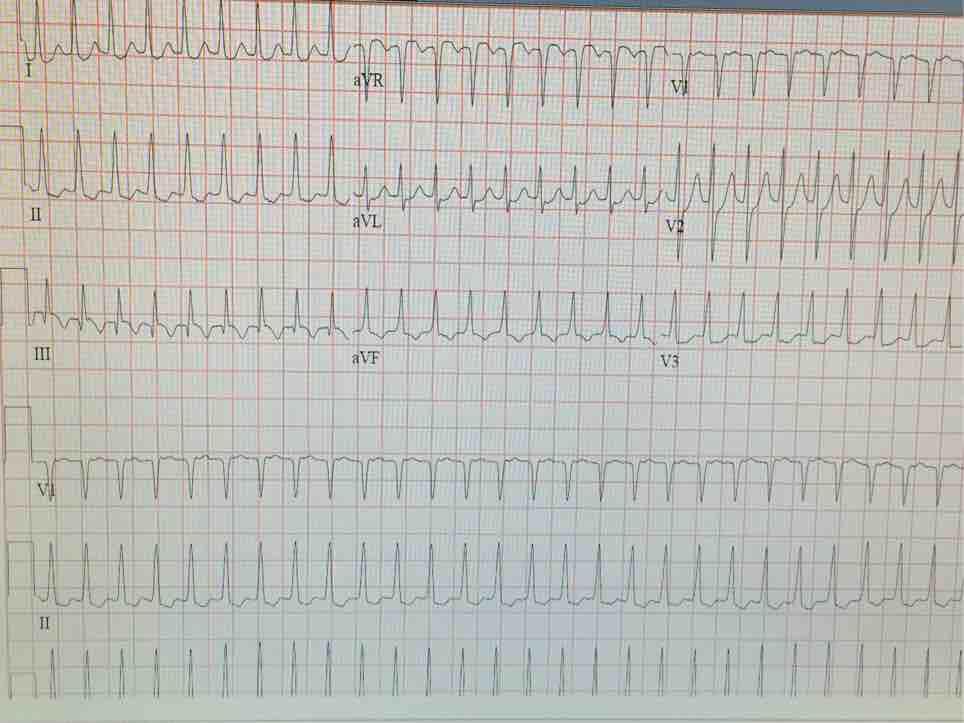
10 Ecg
11 AVNRT Mechanism Atrium Fast pathway Ag Slow pathway Left Ventricle Right Ventricle
12 Acute Treatment of AVNRT AVNRT Vagal maneuvers and/or IV adenosine (Class 1) If Ineffective Hemodynamically Stable Yes IV Beta blocker, diltiazem or verapamil (Class IIa) If Ineffective IV amiodarone (Class IIb) No Synchronized Cardioversion (Class I)
13 Management of AVNRT AVNRT Symptomatic Yes No Clinical follow-up (Class IIa) Yes Ablation Candidate Patient prefers ablation No Slow pathway Catheter ablation (Class I) Beta blockers, diltiazem or verapamil (Class 1) Flecainide or Propafenone (Class IIa) Amiodarone, digoxin, dofetilide, or sotalol (Class IIb) If Ineffective

14 AVNRT - Slow pathway Jump 434ms 497ms

15 AVNRT Ablation Proprietary and confidential do not distribute Junctional beats during ablation Sinus
16 SVT 28 year old woman with a history of palpitations since early childhood. Episodes have been increasing in frequency and duration, up to an hour in length. Typical triggers include bending over and laying on her left side. Episodes can be terminated with a Valsalva maneuver. Her aunt has known SVT.

17
18 AVRT Right Atrium Left Atrium AV Node Accessory Pathway Right Ventricle Left Ventricle
19 Acute Treatment of AVRT Orthodromic AVRT Vagal maneuvers Or IV adenosine (Class 1) Hemodynamically stable IV Beta blockers, Diltiazem or Verapamil (Class IIa) Synchronized cardioversion (Class I) If Ineffective
 Catheter Ablation (Class I) Beta blockers, diltiazem, or verapamil (Class I) Dofetilide, sotalol, digoxin, or amiodarone (Class")
20 Management of AVRT Orthodromic AVRT Yes Pre-excitation on resting ECG No No Yes Yes No Flecainide or propafenone (no structural heart disease) (Class IIa) Dofetilide, sotalol, or amiodarone (Class IIb) Catheter Ablation (Class I) Beta blockers, diltiazem, or verapamil (Class I) Dofetilide, sotalol, digoxin, or amiodarone (Class IIb)
21 WPW Prevalence of manifest accessory pathways 0.1 to 0.3% of the population Ten year risk of sudden cardiac death is 0.15% to 0.24%. Highest risk in the first two decades of life. Low risk profile associated with intermittent loss of pre-excitation on an ECG or ambulatory monitor, or abrupt loss during exercise testing (Class I). EP testing for risk stratification. High risk profile: induced AVRT, AP ERP < 240 ms, R-R interval with induced AF < 250 ms, multiple APs, AVRT triggered AF. Ablation is reasonable with high risk findings or when WPW precludes employment (Class IIa) Observation without treatment (Class IIa)
22 WPW 21 year old male with several year history of rapid palpitations and syncope was diagnosed with WPW one year ago. He declined ablation or medical therapy. Admitted following VF arrest requiring CPR and DC shock for treatment. ECG revealed pre-excitation c/w left lateral accessory pathway location. At EP study three separate pathways were found. Afib with rapid conduction down the AP was easily inducible with R-R interval < 250 ms, as well as ORT. All three pathways underwent successful RF ablation.
23 Ecg

24 Termination of Accessory Pathway during RF ablation Proprietary and confidential do not distribute

25 Termination of Accessory Pathway during RF ablation Proprietary and confidential do not distribute
26 Success and Complication Rates for SVT Ablation Arrhythmia Acute Success Recurrence Rate Complications AVNRT 96-97% 5% Overall 3% PPM 0.7% Groin comp 1-2 % AVRT/AP 93% 8% Overall 2.8% Tamponade 0.4% PPM 0.3% Proprietary and confidential do not distribute
27 Atrial Flutter 56 year old man with a history of HTN, smoking, and COPD complains of 6 weeks of fatigue, exertional intolerance, dyspnea and cough. He was seen in urgent care, diagnosed with bronchitis and treated with a 5 day course of azithromycin. His symptoms persisted and came to his PCP, where and ECG revealed atrial flutter. Exam notable for JVD, a rapid irregular pulse, and bibasilar rales. Echo revealed global hypokinesis with an LVEF of 35%.

28
29 Typical Atrial Flutter Right Atrium AV Node Right Ventricle
30 Management of Atrial Flutter Atrial Flutter Treatment Strategy Rate Control Rhythm Control* Beta-blocker, diltiazem, or verapamil (Class I) Catheter Ablation (Class I) *After adequate anticoagulation or TEE to exclude LAA thrombus Flecainide or propafenone (in the absence of SHD, combine with AV nodal blocking agents) (Class IIb) Sotalol, dofetilide, or amiodarone (Class IIa)

31 Proprietary and confidential do not distribute Mapping Atrial Flutter

32 Atrial Flutter Propagation Map

33 Ablation of the Cavotricuspid Isthmus

34 Termination of Atrial Flutter with RF ablation Proprietary and confidential do not distribute
35 Atrial Fibrillation 68 year old man with obesity, HTN, and sleep apnea notes 6 years of palpitations, lasing up to 12 hours in duration. Event monitor has demonstrated paroxysmal atrial fibrillation. He experiences fatigue and dyspnea during episodes of palpitations. His symptoms have been refractory to metoprolol and flecainide. He has been maintained on chronic anticoagulation with Xarelto.

36
37 Atrial Fibrillation Right superior pulmonary vein Left Atrium Left superior pulmonary vein Left inferior pulmonary vein Right inferior pulmonary vein Left Ventricle
38 Atrial Fibrillation Management Atrial Fibrillation No Structural Heart Disease Structural Heart Disease Flecainide Propafenone Dofetilide Dronedarone Sotalol Catheter Ablation* Dofetilide Dronedarone Sotalol CAD Catheter Ablation* Heart Failure Amiodarone Dofetilide Amiodarone Amiodarone * Class I for paroxysmal AF, Class IIa for persistent AF, Class IIb for long-standing persistent AF (refractory or intolerant of at least one Class 1 or Class III AAA)
39 AF Catheter Ablation Recommendations Class I 1. Symptomatic paroxysmal AF refractory or intolerant to at least one class I or class III antiarrhythmic agent. Class IIa 1. Symptomatic persistent AF refractory intolerant to at least one class I or class III antiarrhythmic agent. 2. Symptomatic paroxysmal AF prior to a trial of antiarrhythmic drug therapy. Class IIb 1. Symptomatic longstanding (>12 mo) persistent AF refractory or intolerant to at least one class I or class III antiarrhythmic agent. 2. Symptomatic persistent AF prior to a trial of antiarrhythmic drug therapy. Class III 1. AF catheter ablation should not be performed in patients who cannot be anticoagulated during or after the procedure. 2. AF catheter ablation should not be performed with the sole intent of obviating the need for anticoagulation.


40 3D Reconstructed CT of the Heart

41 AF Ablation via Radiofrequency (RF) LIPV Pre ablation LIPV Post ablation Pulmonary vein potential Proprietary and confidential do not distribute Fairfield V signal Only Fairfield V Isolated LIPV


42 AF Radiofrequency Ablation Pre and Post Pre Ablation Voltage Post ablation Voltage with ablation lesions Proprietary and confidential do not distribute

43 Cryoballoon catheter Cryoballoon

44 Cryoballoon structure Cryoballoon

45 Cryoballoon Deployment Inflation to Occlude PV Ostium

46 Right Superior Pulmonary Vein Cryo AF ablation RSPV With Contrast Cryo Balloon Proprietary and confidential do not distribute

47 Left Superior Pulmonary Vein Cryo AF ablation Proprietary and confidential do not distribute Balloon LSPV

48 Cryo AF Ablation Voltage Map Pre Voltage Post Voltage Pre Ablation Post Ablation Proprietary and confidential do not distribute

49 Cryo AF with Termination During Ablation AF Sinus Proprietary and confidential do not distribute
50 Success and Complication Rates for Aflutter and Afib Arrhythmia Acute Success Recurrence Rates Complications Typical Atrial Flutter 97% 10.6% Overall 2.5% PPM 0.2% Tamponade 0.3% Atrial Fibrillation 70% 33% Overall 4.5% Tamponade 1.3% CVA/TIA 0.94% A-E Fistula 0.04% Death 0.15%
51 Proprietary and confidential do not distribute PVC/Ventricular Tachycardia 28 year old woman with frequent palpitations, dizziness and exertional intolerance Episodes occur throughout the day, most notable at rest and when trying to sleep ECG shows frequent PVCs with a LBBB morphology and inferior axis Holter monitor reveals 33% burden of ventricular ectopy, with short runs of NSVT, up to 5 beats in duration Echo with LVEF 45% and borderline LV enlargement No efficacy with beta-blockers or flecainide, and associated with increasing fatigue

52
53 RVOT/LVOT and Idiopathic Left Ventricular Tachycardia Pulmonary Artery Aorta Right Atrium Left Ventricle Right Ventricle
54 Management of VT in Structurally Normal Hearts Class I Catheter ablation is useful in patients with symptomatic drug-refractory VT, or in patients drug intolerant or who do not desire long-term drug therapy Class II EP testing is reasonable for diagnostic evaluation in patients with palpitations and suspected outflow tract VT Drug therapy with beta-blockers, calcium channel blocker, or type Ic agents can be useful with symptomatic VT. ICD implantation can be considered for sustained VT with drug refractory VT

55 Focal VT Sinus VT Proprietary and confidential do not distribute

56 Focal VT VT, ablation on Termination at 5 seconds Sinus Rhythm Proprietary and confidential do not distribute
57 Success and Complication Rates for PVC/NSVT Ablation Arrhythmia Acute Success Recurrence Rate Complications RVOT 90-95% 5-8% Tamponade 1% LVOT 85-95% 5-10% Coronary artery injury 0.5%, CVA 0.5% ILVT 85-95% 5-10% CVA 0.5%, CHB 0.5-1% Proprietary and confidential do not distribute
58 Summary AVNRT, AVRT, Atrial Flutter and normal heart PVCs/VT can generally be cured with ablation (90% or higher) AF can be effectively controlled by ablation in up to 70% of patients Treatment options are always patient specific
What s new in my specialty?
 What s new in my specialty? Jon Melman, MD Heart Rhythm Specialists McKay-Dee Hospital some would say some would say my specialty 1 some would say my specialty First pacemaker 1958 some would say my specialty
What s new in my specialty? Jon Melman, MD Heart Rhythm Specialists McKay-Dee Hospital some would say some would say my specialty 1 some would say my specialty First pacemaker 1958 some would say my specialty
APPROACH TO TACHYARRYTHMIAS
 APPROACH TO TACHYARRYTHMIAS PROF.DR.MD.ZAKIR HOSSAIN PROFESSOR AND HEAD DEPARTMENT OF MEDICINE SZMCH TACHYARRYTHMIA Cardiac arrythmia is a disturbance of electrical rhythm of heart. Cardac arrythmia with
APPROACH TO TACHYARRYTHMIAS PROF.DR.MD.ZAKIR HOSSAIN PROFESSOR AND HEAD DEPARTMENT OF MEDICINE SZMCH TACHYARRYTHMIA Cardiac arrythmia is a disturbance of electrical rhythm of heart. Cardac arrythmia with
Dysrhythmias 11/7/2017. Disclosures. 3 reasons to evaluate and treat dysrhythmias. None. Eliminate symptoms and improve hemodynamics
 Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Dysrhythmias CYDNEY STEWART MD, FACC NOVEMBER 3, 2017 Disclosures None 3 reasons to evaluate and treat dysrhythmias Eliminate symptoms and improve hemodynamics Prevent imminent death/hemodynamic compromise
Case-Based Practical ECG Interpretation for the Generalist
 Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Case-Based Practical ECG Interpretation for the Generalist Paul D. Varosy, MD, FACC, FAHA, FHRS Director of Cardiac Electrophysiology VA Eastern Colorado Health Care System Associate Professor of Medicine
Jay Simonson, MD, FACC, FHRS Medical Director, Cardiac Electrophysiology Park Nicollet Heart and Vascular Center
 Jay Simonson, MD, FACC, FHRS Medical Director, Cardiac Electrophysiology Park Nicollet Heart and Vascular Center A-Fib Facts Yes, you may be able to blame your parents It is more of a nuisance than a
Jay Simonson, MD, FACC, FHRS Medical Director, Cardiac Electrophysiology Park Nicollet Heart and Vascular Center A-Fib Facts Yes, you may be able to blame your parents It is more of a nuisance than a
Supraventricular Tachycardia: From Fetus to Adult. Mohamed Hamdan, MD
 Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
Supraventricular Tachycardia: From Fetus to Adult Mohamed Hamdan, MD Learning Objectives Define type of SVT by age Describe clinical approach Describe prenatal and postnatal management of SVT 2 SVT Across
Case #1. 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136
 Tachycardias Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136 Initial Assessment Check Telemetry screen if pt on tele Telemetry
Tachycardias Case #1 73 y/o man with h/o HTN and CHF admitted with dizziness and SOB Treated for CHF exacerbation with Lasix Now HR 136 Initial Assessment Check Telemetry screen if pt on tele Telemetry
WPW syndrome and AVRT
 WPW syndrome and AVRT Myung-Yong Lee, MD, PhD Division of Cardiology Department of Internal Medicine School of Medicine Dankook University, Cheonan, Korea Supraventricular tachycardia (SVT) Paroxysmal
WPW syndrome and AVRT Myung-Yong Lee, MD, PhD Division of Cardiology Department of Internal Medicine School of Medicine Dankook University, Cheonan, Korea Supraventricular tachycardia (SVT) Paroxysmal
Supraventricular Tachycardia (SVT)
") Supraventricular Tachycardia (SVT) Bruce Stambler, MD Piedmont Heart Atlanta, GA Supraventricular Tachycardia Objectives Types and mechanisms AV nodal reentrant tachycardia (AVNRT) AV reciprocating tachycardia
Supraventricular Tachycardia (SVT) Bruce Stambler, MD Piedmont Heart Atlanta, GA Supraventricular Tachycardia Objectives Types and mechanisms AV nodal reentrant tachycardia (AVNRT) AV reciprocating tachycardia
3/25/2017. Program Outline. Classification of Atrial Fibrillation
 Alternate Strategies to Antiarrhythmic Therapy: The Role of Ablation Jennifer El Aile, MS, AGPCNP-BC Electrophysiology Nurse Practitioner Clinical Lecturer at the University of Michigan Program Outline
Alternate Strategies to Antiarrhythmic Therapy: The Role of Ablation Jennifer El Aile, MS, AGPCNP-BC Electrophysiology Nurse Practitioner Clinical Lecturer at the University of Michigan Program Outline
Pediatrics ECG Monitoring. Pediatric Intensive Care Unit Emergency Division
 Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
Pediatrics ECG Monitoring Pediatric Intensive Care Unit Emergency Division 1 Conditions Leading to Pediatric Cardiology Consultation 12.7% of annual consultation Is arrhythmias problems Geggel. Pediatrics.
ECGs and Arrhythmias: Family Medicine Board Review 2009
 Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Rate Rhythm Intervals Hypertrophy ECGs and Arrhythmias: Family Medicine Board Review 2009 Axis Jess (Fogler) Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Ischemia Overview
Tachycardias II. Štěpán Havránek
 Tachycardias II Štěpán Havránek Summary 1) Supraventricular (supraventricular rhythms) Atrial fibrillation and flutter Atrial ectopic tachycardia / extrabeats AV nodal reentrant a AV reentrant tachycardia
Tachycardias II Štěpán Havránek Summary 1) Supraventricular (supraventricular rhythms) Atrial fibrillation and flutter Atrial ectopic tachycardia / extrabeats AV nodal reentrant a AV reentrant tachycardia
ECG Workshop. Carolyn Shepherd And Anya Horne UWE Principles of Cardiac Care
 ECG Workshop Carolyn Shepherd And Anya Horne UWE Principles of Cardiac Care ECG workshop case study1 44 Year old male. Reports SOB, Lethargy, tiredness. PMH: Hypertension, nil else. What tests? What treatment?
ECG Workshop Carolyn Shepherd And Anya Horne UWE Principles of Cardiac Care ECG workshop case study1 44 Year old male. Reports SOB, Lethargy, tiredness. PMH: Hypertension, nil else. What tests? What treatment?
Arrhythmias (I) Supraventricular Tachycardias. Disclosures
 Supraventricular Tachycardias. Disclosures") Arrhythmias (I) Supraventricular Tachycardias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Short R-P Tachycardia REGULAR with 1:1 P/R relationship
Arrhythmias (I) Supraventricular Tachycardias Amy Leigh Miller, MD, PhD Cardiovascular Electrophysiology, Brigham & Women s Hospital Disclosures None Short R-P Tachycardia REGULAR with 1:1 P/R relationship
ECGs and Arrhythmias: Family Medicine Board Review 2012
 Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Overview ECGs and Arrhythmias: Family Medicine Board Review 2012 Jess Waldura, MD University of California, San Francisco walduraj@nccc.ucsf.edu Bundle branch blocks Quick review of ischemia Arrhythmias
Antiarrhythmic Drugs
 Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
Antiarrhythmic Drugs DR ATIF ALQUBBANY A S S I S T A N T P R O F E S S O R O F M E D I C I N E / C A R D I O L O G Y C O N S U L T A N T C A R D I O L O G Y & I N T E R V E N T I O N A L E P A C H D /
TACHYARRHYTHMIAs. Pawel Balsam, MD, PhD
 TACHYARRHYTHMIAs Pawel Balsam, MD, PhD SupraVentricular Tachycardia Atrial Extra Systole Sinus Tachycardia Focal A. Tachycardia AVRT AVNRT Atrial Flutter Atrial Fibrillation Ventricular Tachycardia Ventricular
TACHYARRHYTHMIAs Pawel Balsam, MD, PhD SupraVentricular Tachycardia Atrial Extra Systole Sinus Tachycardia Focal A. Tachycardia AVRT AVNRT Atrial Flutter Atrial Fibrillation Ventricular Tachycardia Ventricular
AF and arrhythmia management. Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire
 AF and arrhythmia management Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire Atrial fibrillation Paroxysmal AF recurrent AF (>2 episodes) that
AF and arrhythmia management Dr Rhys Beynon Consultant Cardiologist and Electrophysiologist University Hospital of North Staffordshire Atrial fibrillation Paroxysmal AF recurrent AF (>2 episodes) that
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014
 Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Rhythm Control: Is There a Role for the PCP? Blake Norris, MD, FACC BHHI Primary Care Symposium February 28, 2014 Financial disclosures Consultant Medtronic 3 reasons to evaluate and treat arrhythmias
Tehran Arrhythmia Center
 Tehran Arrhythmia Center The Worst Scenario A 4 year old kid High heart rates first noted by parents at 20 months of age. Family physician detected rates as high as 220 bpm at that age. He was visited,
Tehran Arrhythmia Center The Worst Scenario A 4 year old kid High heart rates first noted by parents at 20 months of age. Family physician detected rates as high as 220 bpm at that age. He was visited,
Chapter 16: Arrhythmias and Conduction Disturbances
 Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Complete the following. Chapter 16: Arrhythmias and Conduction Disturbances 1. Cardiac arrhythmias result from abnormal impulse, abnormal impulse, or both mechanisms together. 2. is the ability of certain
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: WPW Revised: 11/2013
 Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: WPW Revised: 11/2013 Wolff-Parkinson-White syndrome (WPW) is a syndrome of pre-excitation of the
Emergency Medical Training Services Emergency Medical Technician Paramedic Program Outlines Outline Topic: WPW Revised: 11/2013 Wolff-Parkinson-White syndrome (WPW) is a syndrome of pre-excitation of the
Ectopic Atrial Tachycardia
 Europace Madrid, 26-29 June 2011 Ectopic Atrial Tachycardia P. Loh, MD, PhD University of Utrecht Division Heart & Lungs Epidemiology Nonsustained atrial tachycardia Frequent finding on holter registrations
Europace Madrid, 26-29 June 2011 Ectopic Atrial Tachycardia P. Loh, MD, PhD University of Utrecht Division Heart & Lungs Epidemiology Nonsustained atrial tachycardia Frequent finding on holter registrations
Antony French Consultant Cardiologist & Electrophysiologist
 Antony French Consultant Cardiologist & Electrophysiologist Palpitations Unpleasant awareness of rapid or forceful heart beat Not all tachycardias cause palpitations, and not all palpitations are due to
Antony French Consultant Cardiologist & Electrophysiologist Palpitations Unpleasant awareness of rapid or forceful heart beat Not all tachycardias cause palpitations, and not all palpitations are due to
Atrial Fibrillation and Common Supraventricular Tachycardias. Sunil Kapur MD
 Atrial Fibrillation and Common Supraventricular Tachycardias Sunil Kapur MD Cardiac Electrophysiology Brigham and Women s Hospital Instructor, Harvard Medical School No disclosures Cardiac Conduction:
Atrial Fibrillation and Common Supraventricular Tachycardias Sunil Kapur MD Cardiac Electrophysiology Brigham and Women s Hospital Instructor, Harvard Medical School No disclosures Cardiac Conduction:
Emergency treatment to SVT Evidence-based Approach. Tran Thao Giang
 Emergency treatment to SVT Evidence-based Approach Tran Thao Giang Description ECG manifestations: HR is extremely rapid and regular (240bpm ± 40) P wave is: usually invisible When visible: anormal P axis,
Emergency treatment to SVT Evidence-based Approach Tran Thao Giang Description ECG manifestations: HR is extremely rapid and regular (240bpm ± 40) P wave is: usually invisible When visible: anormal P axis,
ECGs on the acute admission ward. - Cardiology Update -
 ECGs on the acute admission ward - Cardiology Update - Dr Simon Fynn Consultant Cardiologist Papworth Hospital, Cambridge RCP London Oct 2017 ECG 1 1. AF with BBB 2. Pre-excited AF 3. SVT with BBB 4.
ECGs on the acute admission ward - Cardiology Update - Dr Simon Fynn Consultant Cardiologist Papworth Hospital, Cambridge RCP London Oct 2017 ECG 1 1. AF with BBB 2. Pre-excited AF 3. SVT with BBB 4.
CVD: Cardiac Arrhythmias. 1. Final Cardiac Arrhythmias_BMP. 1.1 Cardiovascular Disease. Notes:
 CVD: Cardiac Arrhythmias 1. Final Cardiac Arrhythmias_BMP 1.1 Cardiovascular Disease 1.2 Directions for taking this course 1.3 Content Experts 1.4 Disclosures 1.5 Accreditation Information 1.6 Learning
CVD: Cardiac Arrhythmias 1. Final Cardiac Arrhythmias_BMP 1.1 Cardiovascular Disease 1.2 Directions for taking this course 1.3 Content Experts 1.4 Disclosures 1.5 Accreditation Information 1.6 Learning
Repetitive narrow QRS tachycardia in a 61-year-old female patient with recent palpitations
 Journal of Geriatric Cardiology (2018) 15: 193 198 2018 JGC All rights reserved; www.jgc301.com Case Report Open Access Repetitive narrow QRS tachycardia in a 61-year-old female patient with recent palpitations
Journal of Geriatric Cardiology (2018) 15: 193 198 2018 JGC All rights reserved; www.jgc301.com Case Report Open Access Repetitive narrow QRS tachycardia in a 61-year-old female patient with recent palpitations
Dos and Don t in Cardiac Arrhythmia. Case 1 -ECG. Case 1. Management. Emergency Admissions. Reduction of TE risk -CHADS 2 score. Hospital Admissions
 Emergency Admissions Dos and Don t in Cardiac Arrhythmia Tom Wong, MD, FESC Consultant Cardiologist, Honorary Senior Lecturer Royal Brompton & Harefield Hospitals National Heart and Lung Institute, Imperial
Emergency Admissions Dos and Don t in Cardiac Arrhythmia Tom Wong, MD, FESC Consultant Cardiologist, Honorary Senior Lecturer Royal Brompton & Harefield Hospitals National Heart and Lung Institute, Imperial
Chapter 9. Learning Objectives. Learning Objectives 9/11/2012. Cardiac Arrhythmias. Define electrical therapy
 Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Chapter 9 Cardiac Arrhythmias Learning Objectives Define electrical therapy Explain why electrical therapy is preferred initial therapy over drug administration for cardiac arrest and some arrhythmias
Supraventricular Tachycardia (SVT)
") Supraventricular Tachycardia (SVT) Daniel Frisch, MD Cardiology Division, Electrophysiology Section Thomas Jefferson University Hospital daniel.frisch@jefferson.edu Short RP Are these the Mid same RP tachycardias?
Supraventricular Tachycardia (SVT) Daniel Frisch, MD Cardiology Division, Electrophysiology Section Thomas Jefferson University Hospital daniel.frisch@jefferson.edu Short RP Are these the Mid same RP tachycardias?
Atrial Fibrillation 10/2/2018. Depolarization & ECG. Atrial Fibrillation. Hemodynamic Consequences
 Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Depolarization & ECG Atrial Fibrillation How to make ORDER out of CHAOS Julia Shih, VMD, DACVIM (Cardiology) October 27, 2018 Depolarization & ECG Depolarization & ECG Atrial Fibrillation Hemodynamic Consequences
Asymptomatic WPW Syndrome; Observation or Ablation? 전남대학교병원순환기내과 박형욱
 Asymptomatic WPW Syndrome; Observation or Ablation? 전남대학교병원순환기내과 박형욱 Let It Be? Vs. Just Do It? Natural history of asymptomatic WPW Incidence of sudden cardiac death in natural history studies involving
Asymptomatic WPW Syndrome; Observation or Ablation? 전남대학교병원순환기내과 박형욱 Let It Be? Vs. Just Do It? Natural history of asymptomatic WPW Incidence of sudden cardiac death in natural history studies involving
Atrial fibrillation: Who should be referred for ablation therapy for atrial fibrillation?. September 12 th, 2015
 Atrial fibrillation: Who should be referred for ablation therapy for atrial fibrillation?. September 12 th, 2015 MMMMMMM MMMMMMM MMMMMMM Sohail Hassan MD FACC, FHRS Director, Cardiac Electrophysiology
Atrial fibrillation: Who should be referred for ablation therapy for atrial fibrillation?. September 12 th, 2015 MMMMMMM MMMMMMM MMMMMMM Sohail Hassan MD FACC, FHRS Director, Cardiac Electrophysiology
«Aσθενής με ασυμπτωματικό WPW και παροξυσμική κολπική μαρμαρυγή» Χάρης Κοσσυβάκης Επιμελητής A Καρδιολογικό Τμήμα Γ.Ν.Α. «Γ.
 «Aσθενής με ασυμπτωματικό WPW και παροξυσμική κολπική μαρμαρυγή» Χάρης Κοσσυβάκης Επιμελητής A Καρδιολογικό Τμήμα Γ.Ν.Α. «Γ. ΓΕΝΝΗΜΑΤΑΣ» the primary mechanism of SCD in patients with WPW is the rapid conduction
«Aσθενής με ασυμπτωματικό WPW και παροξυσμική κολπική μαρμαρυγή» Χάρης Κοσσυβάκης Επιμελητής A Καρδιολογικό Τμήμα Γ.Ν.Α. «Γ. ΓΕΝΝΗΜΑΤΑΣ» the primary mechanism of SCD in patients with WPW is the rapid conduction
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology
 Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
Huseng Vefali MD St. Luke s University Health Network Department of Cardiology Learning Objectives Establish Consistent Approach to Interpreting ECGs Review Essential Cases for Paramedics and first responders
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material
 1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
1 Cardiology Acute Care Day 22 April 2013 Arrhythmia Tutorial Course Material Arrhythmia recognition This tutorial builds on the ECG lecture and provides a framework for approaching any ECG to allow the
AF :RHYTHM CONTROL BY DR-MOHAMMED SALAH ASSISSTANT LECTURER CARDIOLOGY DEPARTMENT
 AF :RHYTHM CONTROL BY DR-MOHAMMED SALAH ASSISSTANT LECTURER CARDIOLOGY DEPARTMENT 5-2014 Atrial Fibrillation therapeutic Approach Rhythm Control Thromboembolism Prevention: Recommendations Direct-Current
AF :RHYTHM CONTROL BY DR-MOHAMMED SALAH ASSISSTANT LECTURER CARDIOLOGY DEPARTMENT 5-2014 Atrial Fibrillation therapeutic Approach Rhythm Control Thromboembolism Prevention: Recommendations Direct-Current
A request for a log book extension must be put in writing and sent to BHRS, Unit 6B, Essex House, Cromwell Business Park, Chipping Norton,
 7 7. A request for a log book extension must be put in writing and sent to BHRS, Unit 6B, Essex House, Cromwell Business Park, Chipping Norton, Oxfordshire OX7 5SR. E-mail: admin@bhrs.com. Tel: 01789 867
7 7. A request for a log book extension must be put in writing and sent to BHRS, Unit 6B, Essex House, Cromwell Business Park, Chipping Norton, Oxfordshire OX7 5SR. E-mail: admin@bhrs.com. Tel: 01789 867
2015 Atrial Fibrillation Therapy Meds, Shock, or Ablate? D. Scott Kirby MD, FACC Cardiac Electrophysiologist
 2015 Atrial Fibrillation Therapy Meds, Shock, or Ablate? D. Scott Kirby MD, FACC Cardiac Electrophysiologist Todays Objectives Atrial Fibrillation evaluation and treatment from an EP perspective Multimodal
2015 Atrial Fibrillation Therapy Meds, Shock, or Ablate? D. Scott Kirby MD, FACC Cardiac Electrophysiologist Todays Objectives Atrial Fibrillation evaluation and treatment from an EP perspective Multimodal
You Don t Want to Miss This One! Focus on can t miss EKG tracings
 You Don t Want to Miss This One! Focus on can t miss EKG tracings Renaissance St. Louis Grand Hotel Convention Center October 23, 2014 David K. Tan, M.D., EMT-T, FAAEM EMS Section Chief, Division of Emergency
You Don t Want to Miss This One! Focus on can t miss EKG tracings Renaissance St. Louis Grand Hotel Convention Center October 23, 2014 David K. Tan, M.D., EMT-T, FAAEM EMS Section Chief, Division of Emergency
Basics of Atrial Fibrillation. By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY
 Basics of Atrial Fibrillation By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY Atrial Fibrillation(AF) is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation
Basics of Atrial Fibrillation By Mini Thannikal NP-BC Mount Sinai St Luke s Hospital New York, NY Atrial Fibrillation(AF) is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation
Ventricular Tachycardia in Structurally Normal Hearts (Idiopathic VT) Patient Information
 Patient Information") Melbourne Heart Rhythm Ventricular Tachycardia in Structurally Normal Hearts (Idiopathic VT) Patient Information What is Ventricular Tachycardia? Ventricular tachycardia (VT) is an abnormal rapid heart
Melbourne Heart Rhythm Ventricular Tachycardia in Structurally Normal Hearts (Idiopathic VT) Patient Information What is Ventricular Tachycardia? Ventricular tachycardia (VT) is an abnormal rapid heart
3. AV Block 1. First-degree AV block 1. Delay in AV node 2. Long PR interval 3. QRS complex follows each P wave 4. Benign, no tx
 1. Rhythms & arrhythmias SA nodal rhythms Sinus rhythm Sinus tachycardia Sinus bradycardia Sinus arrhythmia Sick sinus syndrome SA block Sinus arrest AV blocks First-degree Second-degree Mobitz Type I
1. Rhythms & arrhythmias SA nodal rhythms Sinus rhythm Sinus tachycardia Sinus bradycardia Sinus arrhythmia Sick sinus syndrome SA block Sinus arrest AV blocks First-degree Second-degree Mobitz Type I
Anti arrhythmic drugs. Hilal Al Saffar College of medicine Baghdad University
 Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
Anti arrhythmic drugs Hilal Al Saffar College of medicine Baghdad University Mechanism of Arrhythmia Abnormal heart pulse formation Abnormal heart pulse conduction Classification of Arrhythmia Abnormal
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif
 Heart Arrhythmias 2 - Dr. Abdullah Sharif") 2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
2) Heart Arrhythmias 2 - Dr. Abdullah Sharif Rhythms from the Sinus Node Sinus Tachycardia: HR > 100 b/m Causes: o Withdrawal of vagal tone & Sympathetic stimulation (exercise, fight or flight) o Fever
Case 1 Left Atrial Tachycardia
 Case 1 Left Atrial Tachycardia A 16 years old woman was referred to our institution because of recurrent episodes of palpitations and dizziness despite previous ablation procedure( 13 years ago) of postero-septal
Case 1 Left Atrial Tachycardia A 16 years old woman was referred to our institution because of recurrent episodes of palpitations and dizziness despite previous ablation procedure( 13 years ago) of postero-septal
How does the heart work? The heart is muscle whose main function is a pump; to push blood the rest of your body.
 1 You have a condition called atrial fibrillation. I would like you to learn more about this condition. You should read about it below, and can also watch an Internet program about it. After reading about
1 You have a condition called atrial fibrillation. I would like you to learn more about this condition. You should read about it below, and can also watch an Internet program about it. After reading about
LONG RP TACHYCARDIA MAPPING AND RF ABLATION
 LONG RP TACHYCARDIA MAPPING AND RF ABLATION Dr. Hayam Eldamanhoury Ain shams univeristy Arrhythmia is a too broad topic SVT is broadly defined as narrow complex ( unless aberrant conduction ) Requires
LONG RP TACHYCARDIA MAPPING AND RF ABLATION Dr. Hayam Eldamanhoury Ain shams univeristy Arrhythmia is a too broad topic SVT is broadly defined as narrow complex ( unless aberrant conduction ) Requires
Management of Arrhythmias The General Practitioners role
 Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
Management of Arrhythmias The General Practitioners role Rohan Gunawardena MD, FRCP, FCCP, FACC Consultant Cardiac Electrophysiologist National Hospital of Sri Lanka Arrhythmias not common Palpitations
I have nothing to disclose.
 I have nothing to disclose. Antiarrhythmic Therapy in Pregnancy Prof. Ali Oto,MD,FESC,FACC,FHRS Department of Cardiology Hacettepe University,Faculty of Medicine Ankara Arrhythmias in pregnancy An increased
I have nothing to disclose. Antiarrhythmic Therapy in Pregnancy Prof. Ali Oto,MD,FESC,FACC,FHRS Department of Cardiology Hacettepe University,Faculty of Medicine Ankara Arrhythmias in pregnancy An increased
Atrial Fibrillation: Rate vs. Rhythm. Michael Curley, MD Cardiac Electrophysiology
 Atrial Fibrillation: Rate vs. Rhythm Michael Curley, MD Cardiac Electrophysiology I have no relevant financial disclosures pertaining to this topic. A Fib Epidemiology #1 Most common heart rhythm disturbance
Atrial Fibrillation: Rate vs. Rhythm Michael Curley, MD Cardiac Electrophysiology I have no relevant financial disclosures pertaining to this topic. A Fib Epidemiology #1 Most common heart rhythm disturbance
Palpitations and Management of Arrhythmias. Palpitations. Differential Diagnosis. Differential Diagnosis. Differential Diagnosis
 Palpitations and Management of Arrhythmias Fernando Vega, M.D. 7/8/2011 Fernando Vega, M.D. 1 7/8/2011 Fernando Vega, M.D. 2 Palpitations A sensory symptom An unpleasant awareness of the forceful, rapid
Palpitations and Management of Arrhythmias Fernando Vega, M.D. 7/8/2011 Fernando Vega, M.D. 1 7/8/2011 Fernando Vega, M.D. 2 Palpitations A sensory symptom An unpleasant awareness of the forceful, rapid
Differential diagnosis and pacing in maneuvers narrow QRS tachycardia. Richard Schilling
 Differential diagnosis and pacing in maneuvers narrow QRS tachycardia Richard Schilling Differential diagnosis of narrow complex QRS tachycardia Anything that activates the ventricle normally via the His
Differential diagnosis and pacing in maneuvers narrow QRS tachycardia Richard Schilling Differential diagnosis of narrow complex QRS tachycardia Anything that activates the ventricle normally via the His
PEDIATRIC SVT MANAGEMENT
 PEDIATRIC SVT MANAGEMENT 1 INTRODUCTION Supraventricular tachycardia (SVT) can be defined as an abnormally rapid heart rhythm originating above the ventricles, often (but not always) with a narrow QRS
PEDIATRIC SVT MANAGEMENT 1 INTRODUCTION Supraventricular tachycardia (SVT) can be defined as an abnormally rapid heart rhythm originating above the ventricles, often (but not always) with a narrow QRS
Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC
 Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC Professor of Medicine Director of Cardiac Electrophysiology Temple University Health System Plumbing Electrical System Bradyarrhythmias Sinus Node
Arrhythmia Management Joshua M. Cooper, MD, FHRS, FACC Professor of Medicine Director of Cardiac Electrophysiology Temple University Health System Plumbing Electrical System Bradyarrhythmias Sinus Node
Clinical Cardiac Electrophysiology
 Clinical Cardiac Electrophysiology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of
Clinical Cardiac Electrophysiology Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of
EP WIRE on Management Preexcitation syndromes
 EP WIRE on Management Preexcitation syndromes 1. Is your Institution: A University Hospital 70.7% 41 A Private Hospital 13.8% 8 Other Type of Hospital 15.5% 9 Institution name: 50 answered question 58
EP WIRE on Management Preexcitation syndromes 1. Is your Institution: A University Hospital 70.7% 41 A Private Hospital 13.8% 8 Other Type of Hospital 15.5% 9 Institution name: 50 answered question 58
Current Guideline for AF Treatment. Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine
 Current Guideline for AF Treatment Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine Case 1 59 year-old lady Sudden palpitation and breathlessness for 12 hours
Current Guideline for AF Treatment Young Keun On, MD, PhD, FHRS Samsung Medical Center Sungkyunkwan University School of Medicine Case 1 59 year-old lady Sudden palpitation and breathlessness for 12 hours
Management strategies for atrial fibrillation Thursday, 20 October :27
 ALTHOUGH anyone who has had to run up a flight of steps or has had a frightening experience is quite familiar with a racing heartbeat, for the more than 2 million Americans who suffer from atrial fibrillation
ALTHOUGH anyone who has had to run up a flight of steps or has had a frightening experience is quite familiar with a racing heartbeat, for the more than 2 million Americans who suffer from atrial fibrillation
The most common. hospitalized patients. hypotension due to. filling time Rate control in ICU patients may be difficult as many drugs cause hypotension
 Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
Arrhythmias in the critically ill ICU patients: Approach for rapid recognition & management Objectives Be able to identify and manage: Atrial fibrillation with a rapid ventricular response Atrial flutter
5/5/2010. World incidence 720, 000 new cases / year. World prevalence 5.55 million AF prevalence increasing with aging of population
 Atrial Fibrillation: Guidelines through clinical cases and 2010 updates Samy Claude ELAYI Cardiac Clinical Pacing and Electrophysiology UK World incidence 720, 000 new cases / year World prevalence 5.55
Atrial Fibrillation: Guidelines through clinical cases and 2010 updates Samy Claude ELAYI Cardiac Clinical Pacing and Electrophysiology UK World incidence 720, 000 new cases / year World prevalence 5.55
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION
 ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
ATRIAL FIBRILLATION: REVISITING CONTROVERSIES IN AN ERA OF INNOVATION Frederick Schaller, DO, MACOI,FACP Adjunct Clinical Professor Touro University Nevada DISCLOSURES I have no financial relationships
Practical Approaches to Atrial Fibrillation Management Answers to Your Everyday Questions
 Practical Approaches to Atrial Fibrillation Management Answers to Your Everyday Questions H. Mark Guo, MD, FACC, FHRS Clinical Cardiac Electrophysiology Oregon Heart & Vascular Institute hguo@peacehealth.org
Practical Approaches to Atrial Fibrillation Management Answers to Your Everyday Questions H. Mark Guo, MD, FACC, FHRS Clinical Cardiac Electrophysiology Oregon Heart & Vascular Institute hguo@peacehealth.org
CSI Skills Lab #5: Arrhythmia Interpretation and Treatment
 CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
CSI 202 - Skills Lab #5: Arrhythmia Interpretation and Treatment Origins of the ACLS Approach: CSI 202 - Skills Lab 5 Notes ACLS training originated in Nebraska in the early 1970 s. Its purpose was to
Drugs Controlling Myocyte Excitability and Conduction at the AV node Singh and Vaughan-Williams Classification
 Drugs Controlling Myocyte Excitability and Conduction at the AV node Singh and Vaughan-Williams Classification Class I Na Channel Blockers Flecainide Propafenone Class III K channel Blockers Dofetilide,
Drugs Controlling Myocyte Excitability and Conduction at the AV node Singh and Vaughan-Williams Classification Class I Na Channel Blockers Flecainide Propafenone Class III K channel Blockers Dofetilide,
BHRS Prep course Pub style Quiz NOT A
 BHRS Prep course Pub style Quiz NOT A Round 1 Quiz questions Common ECG s in CRM Colin Cunnington Over the past 3 months, a 24-yearold man who works as a truck driver has had frequent episodes of pre-syncope
BHRS Prep course Pub style Quiz NOT A Round 1 Quiz questions Common ECG s in CRM Colin Cunnington Over the past 3 months, a 24-yearold man who works as a truck driver has had frequent episodes of pre-syncope
ECG S: A CASE-BASED APPROACH December 6,
 ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
ECG S: A CASE-BASED APPROACH December 6, 2018 1 Faculty Disclosure Faculty: Lorne Gula MD, FRCPC Professor, Western University Cardiologist, Hearth Rhythm Specialist Director, Electrophysiology Laboratory,
Catheter Ablation for Atrial Fibrillation: Patient Selection and Outcomes
 Catheter Ablation for Atrial Fibrillation: Patient Selection and Outcomes Francis Marchlinski, MD Richard T and Angela Clark President s Distinguished Professor Director Cardiac Electrophysiolgy University
Catheter Ablation for Atrial Fibrillation: Patient Selection and Outcomes Francis Marchlinski, MD Richard T and Angela Clark President s Distinguished Professor Director Cardiac Electrophysiolgy University
Core Content In Urgent Care Medicine
 Palpitations/Arrhythmias Ebrahim Barkoudah, MD Clinical Instructor in Internal Medicine Harvard Medical School Assistant in Internal Medicine & Pediatrics Massachusetts General Hospital MGH Chelsea Chelsea,
Palpitations/Arrhythmias Ebrahim Barkoudah, MD Clinical Instructor in Internal Medicine Harvard Medical School Assistant in Internal Medicine & Pediatrics Massachusetts General Hospital MGH Chelsea Chelsea,
Mission Statement for our Arrhythmia Care
 Mission Statement for our Arrhythmia Care We are dedicated to provide a compassionate and an outstanding care for patients with cardiac arrhythmias. We will be utilizing the cutting edge and the most advanced
Mission Statement for our Arrhythmia Care We are dedicated to provide a compassionate and an outstanding care for patients with cardiac arrhythmias. We will be utilizing the cutting edge and the most advanced
Arrhythmic Complications of MI. Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine
 Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Arrhythmic Complications of MI Teferi Mitiku, MD Assistant Clinical Professor of Medicine University of California Irvine Objectives Brief overview -Pathophysiology of Arrhythmia ECG review of typical
Catheter Ablation for AF: Patients, Procedures, Outcomes
 Catheter Ablation for AF: Patients, Procedures, Outcomes John Sapp Director Heart Rhythm, QEII Health Sciences Centre Professor of Medicine, Dalhousie University Atrial Fibrillation Atrial Fibrillation
Catheter Ablation for AF: Patients, Procedures, Outcomes John Sapp Director Heart Rhythm, QEII Health Sciences Centre Professor of Medicine, Dalhousie University Atrial Fibrillation Atrial Fibrillation
ANTI-ARRHYTHMICS AND WARFARIN. Dr Nithish Jayakumar
 ANTI-ARRHYTHMICS AND WARFARIN Dr Nithish Jayakumar Contents 1. Anti-arrhythmics Pacemaker and myocardial potentials Drug classes mechanisms; s/e; contra-indications Management of common arrhythmias 2.
ANTI-ARRHYTHMICS AND WARFARIN Dr Nithish Jayakumar Contents 1. Anti-arrhythmics Pacemaker and myocardial potentials Drug classes mechanisms; s/e; contra-indications Management of common arrhythmias 2.
Supplementary Online Content
 Supplementary Online Content Morillo CA, Verma A, Connolly SJ, et al. Radiofrequency ablation vs antiarrhythmic drugs as first-line Treatment of Paroxysmal Atrial Fibrillation (RAAFT-2): a randomzied clinical
Supplementary Online Content Morillo CA, Verma A, Connolly SJ, et al. Radiofrequency ablation vs antiarrhythmic drugs as first-line Treatment of Paroxysmal Atrial Fibrillation (RAAFT-2): a randomzied clinical
Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD
 Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD OBJECTIVES 1. Identify the basic electrophysiology of the four causes of wide complex tachycardia. 2. Develop a simple framework for acute management
Nathan Cade, MD Brandon Fainstad, MD Andrew Prouse, MD OBJECTIVES 1. Identify the basic electrophysiology of the four causes of wide complex tachycardia. 2. Develop a simple framework for acute management
Arrhythmia 341. Ahmad Hersi Professor of Cardiology KSU
 Arrhythmia 341 Ahmad Hersi Professor of Cardiology KSU Objectives Epidemiology and Mechanisms of AF Evaluation of AF patients Classification of AF Treatment and Risk stratification of AF Identify other
Arrhythmia 341 Ahmad Hersi Professor of Cardiology KSU Objectives Epidemiology and Mechanisms of AF Evaluation of AF patients Classification of AF Treatment and Risk stratification of AF Identify other
EHRA Accreditation Exam - Sample MCQs Invasive cardiac electrophysiology
 EHRA Accreditation Exam - Sample MCQs Invasive cardiac electrophysiology Dear EHRA Member, Dear Colleague, As you know, the EHRA Accreditation Process is becoming increasingly recognised as an important
EHRA Accreditation Exam - Sample MCQs Invasive cardiac electrophysiology Dear EHRA Member, Dear Colleague, As you know, the EHRA Accreditation Process is becoming increasingly recognised as an important
Asymptomatic patient with WPW
 Asymptomatic patient with WPW Dimosthenis Avramidis, MD. Arrythmiologist Mitera Children s Hospital Athens Greece Scientific Associate 1st Cardiology Dpt Evangelismos Hospital Athens Greece Preexcitation
Asymptomatic patient with WPW Dimosthenis Avramidis, MD. Arrythmiologist Mitera Children s Hospital Athens Greece Scientific Associate 1st Cardiology Dpt Evangelismos Hospital Athens Greece Preexcitation
Atrial Fibrillation New Approaches, Techniques, and Technology
 New Cardiovascular Horizons 2015 May 28, 2015 New Orleans, Louisiana Atrial Fibrillation New Approaches, Techniques, and Technology State of the Art - - 2015 Richard Abben, M D Director, Cardiac Arrhythmia
New Cardiovascular Horizons 2015 May 28, 2015 New Orleans, Louisiana Atrial Fibrillation New Approaches, Techniques, and Technology State of the Art - - 2015 Richard Abben, M D Director, Cardiac Arrhythmia
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient September 25, 2009
 Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Management of the Hospitalized Patient September 25, 2009 ECG Refresher and Update 2009 Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare with
Heart Rhythm Disorders
 Heart Rhythm Disorders Dr Husain Shabeeh Consultant Cardiologist & Cardiac Electrophysiologist Croydon University Hospital and King s College Hospital My interests Diagnosis and management of heart rhythm
Heart Rhythm Disorders Dr Husain Shabeeh Consultant Cardiologist & Cardiac Electrophysiologist Croydon University Hospital and King s College Hospital My interests Diagnosis and management of heart rhythm
Atrial Fibrillation Ablation: in Whom and How
 Update on Consensus Statement on Management of Atrial Fibrillation: EHRA 2012 Atrial Fibrillation Ablation: in Whom and How Update of HRS/EHRA AF/ECAS Ablation Document 2012 Anne M Gillis MD FHRS Professor
Update on Consensus Statement on Management of Atrial Fibrillation: EHRA 2012 Atrial Fibrillation Ablation: in Whom and How Update of HRS/EHRA AF/ECAS Ablation Document 2012 Anne M Gillis MD FHRS Professor
Understanding Atrial Fibrillation Management. Roy Lin, MD
 Understanding Atrial Fibrillation Management Roy Lin, MD Disclosure None Definition of atrial fibrillation Atrial fibrillation is a supraventricular tachyarrhythmia characterized by uncoordinated atrial
Understanding Atrial Fibrillation Management Roy Lin, MD Disclosure None Definition of atrial fibrillation Atrial fibrillation is a supraventricular tachyarrhythmia characterized by uncoordinated atrial
Tachy. Induction tachycardia lead ECG during Tachy /25/2009. Sinus Rhythm Single His
 12-lead ECG during Tachy 10.30.31 Sinus Rhythm Single His 11.20.02 Induction tachycardia 11.23.23 Tachy 11.25.23 1 I This finding excludes: (a) AVNRT (either typical or atypical) Tachy: Alternating cycle
12-lead ECG during Tachy 10.30.31 Sinus Rhythm Single His 11.20.02 Induction tachycardia 11.23.23 Tachy 11.25.23 1 I This finding excludes: (a) AVNRT (either typical or atypical) Tachy: Alternating cycle
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A AADs. See Antiarrhythmic drugs (AADs) ACE inhibitors. See Angiotensin-converting enzyme (ACE) inhibitors ACP in transseptal approach to
Index Note: Page numbers of article titles are in boldface type. A AADs. See Antiarrhythmic drugs (AADs) ACE inhibitors. See Angiotensin-converting enzyme (ACE) inhibitors ACP in transseptal approach to
Interesting EP Cases Catheter ablation to treat congestive heart failure (CHF)
") Interesting EP Cases Catheter ablation to treat congestive heart failure (CHF) Yiming WU, MD, PhD. Alaska heart and vascular institute. ywu@alaskaheart.com 907-561-3211 19 yo man transferred for out side
Interesting EP Cases Catheter ablation to treat congestive heart failure (CHF) Yiming WU, MD, PhD. Alaska heart and vascular institute. ywu@alaskaheart.com 907-561-3211 19 yo man transferred for out side
Atrial Fibrillation: Guidelines through clinical cases and 2010 updates
 Atrial Fibrillation: Guidelines through clinical cases and 2010 updates Samy Claude ELAYI Cardiac Clinical Pacing and Electrophysiology World incidence 720, 000 new cases / year World prevalence 5.5 million
Atrial Fibrillation: Guidelines through clinical cases and 2010 updates Samy Claude ELAYI Cardiac Clinical Pacing and Electrophysiology World incidence 720, 000 new cases / year World prevalence 5.5 million
AF Today: W. For the majority of patients with atrial. are the Options? Chris Case
 AF Today: W hat are the Options? Management strategies for patients with atrial fibrillation should depend on the individual patient. Treatment with medications seems adequate for most patients with atrial
AF Today: W hat are the Options? Management strategies for patients with atrial fibrillation should depend on the individual patient. Treatment with medications seems adequate for most patients with atrial
AF ABLATION Concepts and Techniques
 AF ABLATION Concepts and Techniques Antony F Chu, M.D. Director of Complex Ablation Arrhythmia Services Section Division of Cardiology at the Rhode Island and Miriam Hospital HIGHLIGHTS The main indications
AF ABLATION Concepts and Techniques Antony F Chu, M.D. Director of Complex Ablation Arrhythmia Services Section Division of Cardiology at the Rhode Island and Miriam Hospital HIGHLIGHTS The main indications
Fibs and Flutters: The Heart of the Matter
 Fibs and Flutters: The Heart of the Matter Anita Ralstin, CNP By the Numbers Atrial Fibrillation Hospital Discharges /quarter for 2012 -- 116,500 Average Length of Stay 4 days Projected that 20% of those
Fibs and Flutters: The Heart of the Matter Anita Ralstin, CNP By the Numbers Atrial Fibrillation Hospital Discharges /quarter for 2012 -- 116,500 Average Length of Stay 4 days Projected that 20% of those
How do arrhythmias occur?
 How do arrhythmias occur? An arrhythmia is an abnormal heart rhythm (= dysrhythmia). Can be fast (tachy) or slow (brady). Brady arrhythmias are usually due to conduc;on block, while tachyarrhythmias are
How do arrhythmias occur? An arrhythmia is an abnormal heart rhythm (= dysrhythmia). Can be fast (tachy) or slow (brady). Brady arrhythmias are usually due to conduc;on block, while tachyarrhythmias are
INTERESTING ECGS. Wide-complex tachycardias 11/13/ yr male with acute ant wall MI, S/P primary PTCA
 INTERESTING ECGS V S Prakash Prof, & Head Dept. of Cardiology M S Ramaiah Hospitals 50 yr male with acute ant wall MI, S/P primary PTCA Pt. underwent successful PAMI An hour later,in the CCU Ventricular
INTERESTING ECGS V S Prakash Prof, & Head Dept. of Cardiology M S Ramaiah Hospitals 50 yr male with acute ant wall MI, S/P primary PTCA Pt. underwent successful PAMI An hour later,in the CCU Ventricular
Atrial Fibrillation Cases. Dr Paul Broadhurst Consultant Cardiologist
 Atrial Fibrillation Cases Dr Paul Broadhurst Consultant Cardiologist November 2011 Mr TH age 72 Routine medical for hypertension check Denies any symptoms despite close questioning PMH: hypertension, MI,
Atrial Fibrillation Cases Dr Paul Broadhurst Consultant Cardiologist November 2011 Mr TH age 72 Routine medical for hypertension check Denies any symptoms despite close questioning PMH: hypertension, MI,
EHRA Accreditation Exam - Sample MCQs Cardiac Pacing and ICDs
 EHRA Accreditation Exam - Sample MCQs Cardiac Pacing and ICDs Dear EHRA Member, Dear Colleague, As you know, the EHRA Accreditation Process is becoming increasingly recognised as an important step for
EHRA Accreditation Exam - Sample MCQs Cardiac Pacing and ICDs Dear EHRA Member, Dear Colleague, As you know, the EHRA Accreditation Process is becoming increasingly recognised as an important step for
(living in the fast lane)
") (living in the fast lane) Presented by M.D. Cardiology IT S A group of ECG and Electrophysiological abnormalities in which The atrial impulses are conducted partly or completely, PREMATURELY, to the ventricles
(living in the fast lane) Presented by M.D. Cardiology IT S A group of ECG and Electrophysiological abnormalities in which The atrial impulses are conducted partly or completely, PREMATURELY, to the ventricles
Cost and Prevalence of A fib. Atrial Fibrillation: Guideline Directed Treatment. Prevalence of A Fib. Risk Factors for A Fib. Risk Factors for A Fib
 Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Atrial Fibrillation: Guideline Directed Treatment Melissa Wendell, FNP-C, MSN Heart Failure - Lead Nurse Practitioner, Aspirus Wausau Hospital and Aspirus Cardiology Cost and Prevalence of A fib 33.5 million
Return to Basics. ECG Rate and Rhythm. Management of the Hospitalized Patient October 4, 2007
 Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare
Management of the Hospitalized Patient October 4, 2007 ECG Refresher for the Hospitalists Return to Basics Determine rate and rhythm Determine intervals and axes Define morphology of P-QRS-T-U Compare