Radio(chemo)therapy for head and neck cancer HNSCC: indications and modalities Prof. dr. Sandra Nuyts Radiotherapy-Oncology
|
|
|
- Camron Park
- 6 years ago
- Views:
Transcription

1 Radio(chemo)therapy for head and neck cancer HNSCC: indications and modalities Prof. dr. Sandra Nuyts Radiotherapy-Oncology March 2018
2 > Half million new cases HNC/year in world 50-60% cured not cured local failure Less side effects More organ and function preservation More effective local and systemic treatment distant failure More effective systemic treatment
3 Therapy of Head and Neck Cancer Multidisciplinary! Head and neck surgeon Maxillofacial surgeon Reconstructive surgeon Dietician Speak and language therapist Maxillofacial prosthodontists Nurses Dentist Medical oncologist Radiation-oncologist Radiologist/ nuclear medicine Pathologist Tabacologist Social nurses
4 Current standard treatment for early HNC: radiotherapy or surgery Surgery (organ sparing) Radiotherapy alone Often altered fractionation schedules
5 Current standard treatment for locally advanced HNC: chemoradiotherapy or surgery Inoperabele locally advanced HNC: CRT Operabele locally advanced HNC CRT: Organ and function preservation Surgery + postoperative (C)RT





6 CANCER TREATMENT surgery chemotherapy radiotherapy hormonal therapy immunotherapy






7 linear accelerator Impacting intra-cellular mechanism Damaging molecular structure of DNA Ionizing atoms Cellular level Ion Photon Impacting processes in the human body Molecular level Atomic level Free electrons
8 Increasing the therapeutic ratio in radiotherapy 1.0 Probability of Tumor Control Probability of Normal Tissue Damage Therapeutic Effect (A) 0 Dose (Gy)
9 Advances in radiotherapy for HNC 1. Lessons from randomized trials 2. IMRT: beyond parotid sparing? Tumorbiology Fractionation schedules 3. New approaches Optimise radiotherapy Concomitant Chemo/biotherapy Technological improvement
10 Radiotherapy for HNC Primary setting Chemoradiotherapy Bioradiotherapy Altered fractionation Postoperative setting Chemoradiotherapy Ionising radiation
11 Current standard treatment for locally advanced HNSCC: chemoradiotherapy 1.Primary setting Inoperable locally advanced HNSCC Operable locally advanced HNSCC Organ and function preservation Tumorbiology Fractionation schedules Optimise radiotherapy Concomitant Chemo/biotherapy Technological improvement
12 Concurrent therapy At current: 2 options Chemoradiotherapy (CRT): based on data from thousands of patients Bio radiotherapy (BRT): based on 1 trial
 Inductie CH+ RT of S (n=171) Conc")

13 Intergroup trial RTOG Larynx stadium III-IV, resecabel, exclusie T4 Primair eindpunt larynx preservatie Standaard RT (n=170) Inductie CH+ RT of S (n=171) Conc CH-RT (n=169) 70 Gy 2Gy/fr 7 weken CDDP 100mg/m 2, d1 5FU 1g/m 2, d1-5 X2-3 >= PR: 70Gy <PR: chirurgie 70 Gy,2Gy/fr,7w CDDP 100mg/m 2, d1,22,43 Forastiere, NEJM 2003

14 Intergroup trial RTOG % 0% Years from randomization


15 Intergroup trial RTOG % 88% 74% 85% 71% 69% 64% 59% 54% 53% 0% Years from randomization
16 chemoradiotherapy 4% pts 63 trials Pignon, Lancet 2000
17 Chemoradiotherapy meta-analysis pts 87 trials Pignon et al, R&O 2009
18 Radiochemotherapy Radiotherapy Concomitant Radiotherapy + Chemotherapy pts 87 trials Pignon, Radiother Oncol 2009
19 chemoradiotherapy: which chemotherapy? Only 2 combinations based on randomised studies: Carbo (70mg/m 2 )-5FU (600mg/m 2 x4d) 3 weekly Calais et al JNCI 1999 CDDP 100mg/m 2 3 weekly Bernier et al EORTC NEJM 2004 Cooper et al RTOG NEJM 2004 Forastiere et al Intergroup RTOG91-11 NEJM 2003

20 1373 patients Szturz Oral Oncology 2018
21 CRT results in significant increase in acute toxicity Grade 3+: 77% with CRT vs 34% with RT alone (p<0.001) RCT RT CT Cooper NEJM 2004

22 CRT: late toxicity! Analysis 3 RTOG trials on CRT 230 eligible patients: 43% late toxicity Machtay JCO 2008

23 Newer agents molecular targeting: EGFR Overexpression in % HNC Poor prognostic factor Reduced response to XRT and CT Ang Int J Radiat Oncol Biol Phys 2004
 conventional BID hyperfractionation concom boost Arm 2: XRT + weekly Cetuximab (n=211) NEJM 2006 Lancet Oncol")
24 Phase III studie: Radiotherapie +/- Cetuximab Phase III randomised study Stage III-IV oropharynx, larynx and hypopharynx R A N D O M I S A T I O N Arm 1: XRT (n=213) conventional BID hyperfractionation concom boost Arm 2: XRT + weekly Cetuximab (n=211) NEJM 2006 Lancet Oncol 2010
25 Results: locoregional control RT RT+ C225 P-value Median duration (months) Locoregional control rates 1 year 55% 63% 2 year 41% 50% 3 year 34% 47% <0.01 Bonner, NEJM 2006
26 Results: Survival Median overall survival (months) RT RT+ C225 P-value Survival rates 3 year 45% 55% year 36% 45.6% 0.02



27 Toxicity?
28 16 Correlation of rash and survival after treatment with EGFR targets Survival (months) CRC CRC CRC CRC Pancreatic SCCHN Study: BOND Saltz (2001) 1 Saltz (2004) 2 Cunningham Van Cutsem Xiong (2004) 5 Kies (2002) 6 (2004) 3 (2004) 4 No reaction Grade 1 Grade 2 Grade 3 1 Saltz et al. Proc ASCO Saltz et al. J Clin Oncol Cunningham D Van Cutsem E. N Engl J Med Van Cutsem et al. EORTC/NCI Geneva Xiong H et al. J Clin Oncol Kies et al. Proc ASCO 2002.
29 Update Bonner trial Lancet Oncol 2009
30 Take home message 1: Golden standard locally advanced HNSCC: Radiotherapy+ high dose cisplatin If patient not eligible cisplatin: cetuximab What about early stage disease? Use of altered fractionation
31 altered fractionation Standard fractionation Hyperfractionation scheme Higher total dose Dose/fraction lower Accelerated radiotherapy Total treatment shorter Combination schedules
32 fractionation meta-analysis MARCH group 6515 ptn, 15 trials All fractionationschedules together: 6.4% gain 5yr locoregional control Hyperfractionation schedules: largest benefit: 9.4% Bourhis, Lancet 2006
33 Take home message 2: 70 Gy in 7 weeks alone= perhaps the worst we can do! RT-CT Altered fractionation Induction chemotherapy Cetuximab+ RT +13% +10% +10% +???
34 postoperative XRT 2.Postop setting Reduces locoregional recurrence rates by at least factor 2 Cohort studies Small randomized trials Kokal WA, J Surg Oncol 1988; 38(2): Marcial VA, Semin Oncol 1988; 15(1): Sadeghi A, Otolaryngol Head Neck Surg 1986; 94(5): Huang DT, Int J Radiat Oncol Biol Phys. 1992;23(4): Reduced locoregional control translates in survival benefit
35 Oral cavity: timing PORT In general: within 6 weeks postop
36 postop XRT vs preop XRT? RTOG 73-03: LAHNCC: supraglottic larynx, hypopharynx, oral cavity, oropharynx Preop (50Gy) versus postop (60Gy) OC/OP also had definitive RT arm (65-70Gy) followed by surgery if residual disease 277 patients, 10 yr follow up Improved LRC in postop arm (65%) vs preop (48%, P=0,04) Trend toward improved survival: 38 vs 33% (p=0,1) Surgical and RT complications similar RTOG established 60Gy as postop RT dose Kramer et al, Head Neck Surg 1987;10:19-30 Tupchong et al, IJROBP 1991;20:21-28

37 radiation dose based on risk MDAnderson prospective randomized trial 240 pts resected stage III/IV OC, OP, HP, L
38 radiation dose Locoregional control by risk factors: Peters et al IJROBP 1993;26:3-11
39 radiation dose Patients receiving <54 Gy had significantly higher failure rate. No dose response beyond 57.6 Gy except for patients with extracapsular nodal spread. +ECE needed at least 63 Gy Clusters of two or more of the following also predicted increased risk of failure and need for 63 Gy: oral cavity primary, positive/close margins, nerve invasion, >2 positive nodes, largest node >3 cm, treatment delay >6weeks, Zubrod performance status>2 Moderate to severe complications seen in 7.1%; more if RT dose >63 Gy Dose escalation above 63 Gy does not appear to improve the therapeutic ratio. Peters et al IJROBP 1993;26:3-11
40 radiation dose based on risk Risk factors: > 1 nodal group >= 2 nodes Nodes >3cm Microscopic + margins PNI+ OC ECE -Low risk: no features -Intermediate risk: 1 risk factor (no ECE) -High risk: ECE or >= 2 risk factors Ang et al IJROBP 2001; 51:
41 Locoregional control and survival by risk factors 5 yr LRC and OS : Low risk: 90% and 83% Intermediate risk: 94% and 66% High risk: 68% and 42% Ang et al IJROBP 2001; 51:
42 Indication PORT Risk features: Microscopically positive surgical margins ECE LVI PNI Close margins (0,01-5mm) >= 2 involved neck nodes >1 positive nodal group Oral cavity primary site Nodal diameter>3cm >6 week interval between surgery and XRT Advanced T stage Recurrent disease Tumor spillage Multicentricity Invasion of bone/cartilage/skin or soft tissue of the neck Depth of tumor invasion >3mm (An 2008), >4mm (Fakih 1989, O Brien 2003), >5mm (Fukano 1997) (Tumors 3-9 mm: 44% node+, 7% local recurrence; >9 mm: 53% subclinical node+, 24% local recurrence Head Neck 2002: 24:513-20)
43 PORT- risk group definition RPA (recursive partitioning analysis) 801 patients Class I-intermediate risk (5Y LRC 88%) No N3 nodes Negative margins (>5mm) No extranodal spread (ENS) Class II-high risk (5Y LRC 73%) pn1 ENS Or pt1, pt2 or pt4 with close or + margins Langendijk et al Cancer 2005; 104:
44 PORT- risk group definition RPA (recursive partitioning analysis) Class III-very high risk (5Y LRC 58%) N3 node >= 2 positive lymph nodes with ENS pt3 with close or positive margins No extranodal spread (ENS) Langendijk et al Cancer 2005; 104:
45 Model based on 979 patients OCSCC Validation on 431 patients
46 Postoperative RT: role chemo? 2 important studies NEJM 2004 high risk group:

47

48
49 Overall survival
50 Combined EORTC/RTOG analysis Bernier, Cooper Head Neck 2005;27:843
51 OS for patients WITH positive margin and/or ECE CRT CRT RT RT
52 OS for patients WITHOUT positive margin and/or ECE CRT RT
53 Update: long term follow up RTOG9501 patients WITH positive margin and/or ECE Cooper et al IJROBP 2012
54 Postoperative RT: role chemo? Differences in selection criteria explain variation in impact of chemo 26-27% of population had OC primaries Adjuvant chemo is indicated in Positive margins +ECE Head Neck 2005; 27:
55 Postoperative RT: role chemo? Words of caution: Important increase acute toxicity: doubling acute mucositis gr III/IV (21% vs 41%) 3 toxic deaths in study Only 61% pts received 3 cycles chemo EORTC no pts > 70j, in RTOG trial only 5% of pts > 70j No reduction in distant metastasis in both trials DFS for pts with ECE and/or positive margins still remains poor: 45.2% at 3 yrs and at 35.7% at 5 yrs (Meta-analysis of EORTC and RTOG trial)
56 Take home message 3: Risk Adaptive PORT depending on pathology Risk Features Management Low risk No radiation Intermediate risk (neg margin, no ECE) Radiation alone to 60Gy High risk (pos margin, and/or ECE) Radiation to 60-66Gy with concurrent cisplatin
57 PORT: altered fractionation? Accelerated fractionation in adjuvant setting: no advantage shown Ang et al IJROBP 2001 Suwinkski et al R&O 2008 Hyperfractionated XRT: not systematically investigated in postop setting
58 role OTT
59 Advances in radiotherapy for HNC 1. Lessons from randomized trials 2. IMRT: beyond parotid sparing? 3. New approaches



60 old school



61 current




62 Evolution in RT techniques Technology 2D-RT D-RT 2000 IMRT 2010 Arc 2D-RT 3D-RT IMRT Arc






63 Technological improvement Technology Introduction conformal radiotherapy-imrt




64 Classic Radiotherapy Highly conformal Radiotherapy


65 What is IMRT?




66 CONFORMAL RADIOTHERAPY LINEAR accelerator COLLIMATOR Different angles MULTI-LEAF COLLIMATOR
67 IMRT


68 Xerostomia is one of the most common complications of RT for HNC. Technology Dirix P., Nuyts S. Cancer 2006


69 Head and Neck Cancer: IMRT is golden standard Phase III Multi-Centre Randomised Controlled Trial of Intensity Modulated vs Conventional Radiotherapy in Head and Neck Cancer: PARSPORT Conventional radiotherapy parallel opposed fields IMRT sparing left parotid C. Nutting, et al Lancet Oncology febr 2011


70

71 Evolution in RT techniques 2D-RT 3D-RT IMRT Arc Reduction xerostomia


72 Evolution in RT techniques 2D-RT 3D-RT IMRT Arc Reduction dysphagia superior pharyngeal constrictor muscle middle pcm inferior pcm upper esophageal sphincter esophagus base of tongue supraglottic larynx glottic larynx



73 Intensity modulated arc therapy (VMAT)






74 Radiotherapy for head and neck cancer: past-present-future 2D-RT 3D-CRT IMRT proton Anno 1970 Anno 1990 Anno 2000 Anno 2020
75 Take home message 4: Current radiotherapy techniques offer possibilities to spare critical organs Like parotids, swallowing structures To reduce acute and long term toxicity Quality of radiotherapy is becoming more crucial!
76 Complexity RT increases We are at increased risk of missing very precisely (J. Rosenman)

77 Wuthrick E et al JCO 2014

78 6212 treated patients IMRT treated pats: increased survival if treated by higher volume radiation oncologists For each 5 patients more treated per year: 21 % reduction in all cause mortality
79 Advances in radiotherapy for HNC 1. Lessons from randomized trials 2. IMRT: beyond parotid sparing? 3. New approaches



 Biology")

80 Increase dose to parts of the tumor: Dose-painting on the biological target volume (BTV) Biology CT PET Fusion Galvin J. et al. J Clin Oncol 2007.




81 Molecular imaging-based dose escalation in HPV negative patients with locally advanced squamous cell carcinoma of the oropharynx Biology





82 Adaptive (Biological) Image-guided Radiotherapy Treatment planning Treatment delivery Linac-integrated kv Cone-beam CT technology Correction : Patient positioning Anatomy changes Biology changes Planning biology anatomy Treatment biology anatomy Image registration

83 Use of Hypoxic Radiosensitizers Biology

84 Biologie Radiation resistance: the oxygen fixation hypothesis FMISO-1 FMISO-2 Brown J. & Wilson W. Nat Rev Cancer 2004.



85 Immunotherapy: PD-1/PD-L1 inhibitors


86 protontherapy Robert. R. Wilson ( ) 1946: good things can come from the tragedy of war
87 Physical Aspects Proton Charged particles (+e) Mass: 1,67 x10-27 kg =1836 times the mass m e of an electron Photon Quantum of electromagnetic radiation No charge No mass Energy ~ frequency ~ wavelength Interaction with matter Newhauser et al. Phys. Med. Biol. 60 (2015)


88 Proton Beam Bragg peak Protons stop in solid or liquid matter. Beyond the stopping point the dose is negligible dose Entrance plateau Protons loose kinetic energy gradually when travelling through matter, through multiple collisions with atomic electrons depth The rate at which protons loose energy increases as the proton is slowing down The rate of energy loss or stopping power depends on the energy itself and on the stopping material Pencil beam High ionization density at the end of their range Weak scattering => Low entrance dose plateau followed by the sharp Bragg peak at the end of the proton range


89


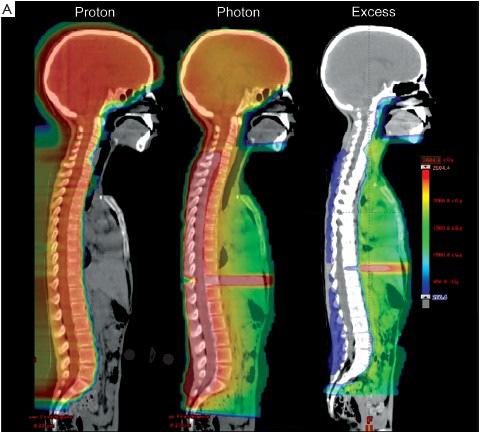
90 Proton vs. photontherapy Photon Proton No dose H&N case Medulloblastoma case


91




92 Leeman et al Lancet Oncol 2014



93 Ongoing studies

94 Conclusion: Radiotherapy for HNC : Enormous progress made Tumorbiology Fractionation schedules Optimise radiotherapy Concomitant Chemo/biotherapy Technological improvement

95
Locally advanced head and neck cancer
 Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Oral Cavity Cancer Combined modality therapy
 Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view. Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium
 HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium DISCLOSURE OF INTEREST Nothing to declare HEAD AND NECK CANCER -HPV
HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium DISCLOSURE OF INTEREST Nothing to declare HEAD AND NECK CANCER -HPV
De-Escalate Trial for the Head and neck NSSG. Dr Eleanor Aynsley Consultant Clinical Oncologist
 De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
State of the art for radiotherapy of SCCHN
 State of the art for radiotherapy of SCCHN Less side effects Cured More organ & function preservation Head & neck cancer = 42 000 new cases / year in Europe Not cured Local failure Distant failure More
State of the art for radiotherapy of SCCHN Less side effects Cured More organ & function preservation Head & neck cancer = 42 000 new cases / year in Europe Not cured Local failure Distant failure More
Oral cavity cancer Post-operative treatment
 Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations
 Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations Troy G. Scroggins Jr. MD Chairman, Department of Radiation Oncology Ochsner Health Systems 1 Association of Postoperative Radiotherapy
Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations Troy G. Scroggins Jr. MD Chairman, Department of Radiation Oncology Ochsner Health Systems 1 Association of Postoperative Radiotherapy
Sequencing Chemo with Radiation therapy Locally Advanced Head and Neck Cancer. Dr P Vijay Anand Reddy Director Apollo Cancer Hospital
 Sequencing Chemo with Radiation therapy Locally Advanced Head and Neck Cancer Dr P Vijay Anand Reddy Director Apollo Cancer Hospital H&N Ca - Disease Burden 15-20% of all cancers in India, 8% worldwide
Sequencing Chemo with Radiation therapy Locally Advanced Head and Neck Cancer Dr P Vijay Anand Reddy Director Apollo Cancer Hospital H&N Ca - Disease Burden 15-20% of all cancers in India, 8% worldwide
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Adjuvant Therapy in Locally Advanced Head and Neck Cancer. Ezra EW Cohen University of Chicago. Financial Support
 Adjuvant Therapy in Locally Advanced Head and Neck Cancer Ezra EW Cohen University of Chicago Financial Support This program is made possible by an educational grant from Eli Lilly Oncology, who had no
Adjuvant Therapy in Locally Advanced Head and Neck Cancer Ezra EW Cohen University of Chicago Financial Support This program is made possible by an educational grant from Eli Lilly Oncology, who had no
SAMO MASTERCLASS HEAD & NECK CANCER. Nicolas Mach, PD Geneva University Hospital
 SAMO MASTERCLASS HEAD & NECK CANCER Nicolas Mach, PD Geneva University Hospital Epidemiology Prevention Best treatment for localized disease Best treatment for relapsed or metastatic disease Introduction
SAMO MASTERCLASS HEAD & NECK CANCER Nicolas Mach, PD Geneva University Hospital Epidemiology Prevention Best treatment for localized disease Best treatment for relapsed or metastatic disease Introduction
RT +/- Surgery. Concurrent ChemoRT +/- Surgery
 Molecular targeted approaches to head and neck cancer Lillian L. Siu Department of Medical Oncology & Hematology Princess Margaret Hospital, University of Toronto Locally Advanced HNSCC Locally Advanced
Molecular targeted approaches to head and neck cancer Lillian L. Siu Department of Medical Oncology & Hematology Princess Margaret Hospital, University of Toronto Locally Advanced HNSCC Locally Advanced
Head and Neck cancer
 Head and Neck cancer Medical Oncologist s Role in Multidisciplinary Teams - Focus on Adjuvant & Neo-adjuvant Therapy - Hye Ryun Kim, M.D. Yonsei Cancer Center, Medical Oncology Contents I. Introduction
Head and Neck cancer Medical Oncologist s Role in Multidisciplinary Teams - Focus on Adjuvant & Neo-adjuvant Therapy - Hye Ryun Kim, M.D. Yonsei Cancer Center, Medical Oncology Contents I. Introduction
Laryngeal Preservation Using Radiation Therapy. Chemotherapy and Organ Preservation
 1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221. Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS
 Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS. Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1.
 RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
Neoplasie del laringe Diagnosi e trattamento
 Neoplasie del laringe Diagnosi e trattamento Venerdì 22 maggio 2015 Alessandria Trattamenti non chirurgici: Preservazione d organo, malattia localmente avanzata Marco C Merlano A.O. S.Croce e Carle, Ospedale
Neoplasie del laringe Diagnosi e trattamento Venerdì 22 maggio 2015 Alessandria Trattamenti non chirurgici: Preservazione d organo, malattia localmente avanzata Marco C Merlano A.O. S.Croce e Carle, Ospedale
HPV POSITIVE OROPHARYNGEAL CARCINOMA the radiation oncologist point of view. Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium
 HPV POSITIVE OROPHARYNGEAL CARCINOMA the radiation oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium HEAD AND NECK CANCER -HPV Change in incidence: HEAD AND NECK
HPV POSITIVE OROPHARYNGEAL CARCINOMA the radiation oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium HEAD AND NECK CANCER -HPV Change in incidence: HEAD AND NECK
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer
 Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
Head and NeckCancer: multi-modal therapeuticintegration
 Head and NeckCancer: multi-modal therapeuticintegration P. Ponticelli, L. Lastrucci, R. De Majo, A. Rampini U.O.C. Radioterapia Ospedale S. Donato ASL 8 -AREZZO Summary Biological considerations Clinical
Head and NeckCancer: multi-modal therapeuticintegration P. Ponticelli, L. Lastrucci, R. De Majo, A. Rampini U.O.C. Radioterapia Ospedale S. Donato ASL 8 -AREZZO Summary Biological considerations Clinical
HALF. Who gets radiotherapy? Who gets radiotherapy? Half of all cancer patients get radiotherapy. By 1899 X rays were being used for cancer therapy
 The Physical and Biological Basis of By 1899 X rays were being used for cancer therapy David J. Brenner, PhD, DSc Center for Radiological Research Department of Radiation Oncology Columbia University Medical
The Physical and Biological Basis of By 1899 X rays were being used for cancer therapy David J. Brenner, PhD, DSc Center for Radiological Research Department of Radiation Oncology Columbia University Medical
Head & Neck Cancer: When to Irradiate
 Head & Neck Cancer: When to Irradiate ESO-ESMO Latin-America 2018 Talented students colleagues 1 > 15 different diseases for RT strategies NC NP OC OP H L 2 HPV Prognostic Marker >2010 Trial Cases Marker
Head & Neck Cancer: When to Irradiate ESO-ESMO Latin-America 2018 Talented students colleagues 1 > 15 different diseases for RT strategies NC NP OC OP H L 2 HPV Prognostic Marker >2010 Trial Cases Marker
Organ-Preservation Strategies in head and neck cancer. Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari
 Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Concurrent Chemo- and Radiotherapy for Ororpharynx Cancer
 Concurrent Chemo- and Radiotherapy for Ororpharynx Cancer Faye Johnson MD, PhD Associate Professor Thoracic/Head and Neck Medical Oncology August 2017 Objectives Review data that support concurrent chemo-
Concurrent Chemo- and Radiotherapy for Ororpharynx Cancer Faye Johnson MD, PhD Associate Professor Thoracic/Head and Neck Medical Oncology August 2017 Objectives Review data that support concurrent chemo-
CALGB Thoracic Radiotherapy for Limited Stage Small Cell Lung Cancer
 CALGB 30610 Thoracic Radiotherapy for Limited Stage Small Cell Lung Cancer Jeffrey A. Bogart Department of Radiation Oncology Upstate Medical University Syracuse, NY Small Cell Lung Cancer Estimated 33,000
CALGB 30610 Thoracic Radiotherapy for Limited Stage Small Cell Lung Cancer Jeffrey A. Bogart Department of Radiation Oncology Upstate Medical University Syracuse, NY Small Cell Lung Cancer Estimated 33,000
MANAGEMENT OF CA HYPOPHARYNX
 MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón
 Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Gastroesophag Gastroesopha eal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. G. H addock Haddock M.D.
 Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部
 肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部 Outline Current status of radiation oncology in lung cancer Focused on stage III non-small cell lung cancer Radiation
肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部 Outline Current status of radiation oncology in lung cancer Focused on stage III non-small cell lung cancer Radiation
Locally advanced disease & challenges in management
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Accepted 28 April 2005 Published online 13 September 2005 in Wiley InterScience ( DOI: /hed.
 DEFINING RISK LEVELS IN LOCALLY ADVANCED HEAD AND NECK CANCERS: A COMPARATIVE ANALYSIS OF CONCURRENT POSTOPERATIVE RADIATION PLUS CHEMOTHERAPY TRIALS OF THE EORTC (#22931) AND RTOG (#9501) Jacques Bernier,
DEFINING RISK LEVELS IN LOCALLY ADVANCED HEAD AND NECK CANCERS: A COMPARATIVE ANALYSIS OF CONCURRENT POSTOPERATIVE RADIATION PLUS CHEMOTHERAPY TRIALS OF THE EORTC (#22931) AND RTOG (#9501) Jacques Bernier,
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Neoadjuvant Chemotherapy in Locally Advanced Squamous Cell Cancer of Head and Neck. Mei Tang, MD
 Neoadjuvant Chemotherapy in Locally Advanced Squamous Cell Cancer of Head and Neck Mei Tang, MD Head and Neck Cancer Worldwide New cases : 644,000 Cancer deaths: 350,000 About 5% of all cancers Local Recurrence:
Neoadjuvant Chemotherapy in Locally Advanced Squamous Cell Cancer of Head and Neck Mei Tang, MD Head and Neck Cancer Worldwide New cases : 644,000 Cancer deaths: 350,000 About 5% of all cancers Local Recurrence:
Emerging Role of Immunotherapy in Head and Neck Cancer
 Emerging Role of Immunotherapy in Head and Neck Cancer Jared Weiss, MD Associate Professor of Medicine and Section Chief of Thoracic and Head/Neck Oncology UNC Lineberger Comprehensive Cancer Center Copyright
Emerging Role of Immunotherapy in Head and Neck Cancer Jared Weiss, MD Associate Professor of Medicine and Section Chief of Thoracic and Head/Neck Oncology UNC Lineberger Comprehensive Cancer Center Copyright
The role of chemoradiotherapy in GE junction and gastric cancer. Karin Haustermans
 The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
Advances in external beam radiotherapy
 International Conference on Modern Radiotherapy: Advances and Challenges in Radiation Protection of Patients Advances in external beam radiotherapy New techniques, new benefits and new risks Michael Brada
International Conference on Modern Radiotherapy: Advances and Challenges in Radiation Protection of Patients Advances in external beam radiotherapy New techniques, new benefits and new risks Michael Brada
Protocol of Radiotherapy for Head and Neck Cancer
 106 年 12 月修訂 Protocol of Radiotherapy for Head and Neck Cancer Indication of radiotherapy Indication of definitive radiotherapy with or without chemotherapy (1) Resectable, but medically unfit, or high
106 年 12 月修訂 Protocol of Radiotherapy for Head and Neck Cancer Indication of radiotherapy Indication of definitive radiotherapy with or without chemotherapy (1) Resectable, but medically unfit, or high
Head and Neck Cancer Update Sandro V Porceddu
 Head and Neck Cancer Update Sandro V Porceddu Director, Radiation Oncology Research Princess Alexandra Hospital, Brisbane Associate Professor, University of Queensland President, Trans Tasman Radiation
Head and Neck Cancer Update Sandro V Porceddu Director, Radiation Oncology Research Princess Alexandra Hospital, Brisbane Associate Professor, University of Queensland President, Trans Tasman Radiation
Combined modality treatment for N2 disease
 Combined modality treatment for N2 disease Dr Clara Chan Consultant in Clinical Oncology 3 rd March 2017 Overview Background The evidence base Systemic treatment Radiotherapy Future directions/clinical
Combined modality treatment for N2 disease Dr Clara Chan Consultant in Clinical Oncology 3 rd March 2017 Overview Background The evidence base Systemic treatment Radiotherapy Future directions/clinical
TREATMENT TIME & TOBACCO: TWIN TERRORS Of H&N Therapy
 TREATMENT TIME & TOBACCO: TWIN TERRORS Of H&N Therapy Anurag K. Singh, MD Professor of Medicine University at Buffalo School of Medicine Professor of Oncology Director of Radiation Research Roswell Park
TREATMENT TIME & TOBACCO: TWIN TERRORS Of H&N Therapy Anurag K. Singh, MD Professor of Medicine University at Buffalo School of Medicine Professor of Oncology Director of Radiation Research Roswell Park
Non-surgical treatment for locally advanced head and neck squamous cell carcinoma: beyond the upper limit
 Editorial Non-surgical treatment for locally advanced head and neck squamous cell carcinoma: beyond the upper limit Hiroto Ishiki, Satoru Iwase Department of Palliative Medicine, The Institute of Medical
Editorial Non-surgical treatment for locally advanced head and neck squamous cell carcinoma: beyond the upper limit Hiroto Ishiki, Satoru Iwase Department of Palliative Medicine, The Institute of Medical
First, how does radiation work?
 Hello, I am Prajnan Das, Faculty Member in the Department of Radiation Oncology at The University of Texas MD Anderson Cancer Center. We are going to talk today about some of the basic principles regarding
Hello, I am Prajnan Das, Faculty Member in the Department of Radiation Oncology at The University of Texas MD Anderson Cancer Center. We are going to talk today about some of the basic principles regarding
Laryngeal and hypopharyngeal cancers
 Laryngeal and hypopharyngeal cancers Induction Chemotherapy in combined modality approaches Atenas 16.09.2017 Ana Ferreira Castro, MD Medical Oncology Centro Hospitalar do Porto Instituto de Ciências Biomédicas
Laryngeal and hypopharyngeal cancers Induction Chemotherapy in combined modality approaches Atenas 16.09.2017 Ana Ferreira Castro, MD Medical Oncology Centro Hospitalar do Porto Instituto de Ciências Biomédicas
State of the Art: Management of Squamous Cell Carcinoma of the Head and Neck. Raul Giglio
 State of the Art: Management of Squamous Cell Carcinoma of the Head and Neck Raul Giglio Disclosures Nothing to disclose SCCHN Outline 1. General considerations: MTD 2. Epidemiology 3. Locoregional disease
State of the Art: Management of Squamous Cell Carcinoma of the Head and Neck Raul Giglio Disclosures Nothing to disclose SCCHN Outline 1. General considerations: MTD 2. Epidemiology 3. Locoregional disease
Laryngeal Conservation
 Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
TOPICS. Primary Radiation Therapy. Targeted Therapy in Oncology. Principles of Radiation Therapy. Principles of Radiation Therapy
 Peter B. Schiff, M.D., Ph.D. Department of Radiation Oncology Columbia University College of Physicians & Surgeons May 4, 2007 Targeted Therapy in Oncology Surgical Oncology Minimal invasive techniques
Peter B. Schiff, M.D., Ph.D. Department of Radiation Oncology Columbia University College of Physicians & Surgeons May 4, 2007 Targeted Therapy in Oncology Surgical Oncology Minimal invasive techniques
Thomas Gernon, MD Otolaryngology THE EVOLVING TREATMENT OF SCCA OF THE OROPHARYNX
 Thomas Gernon, MD Otolaryngology THE EVOLVING TREATMENT OF SCCA OF THE OROPHARYNX Disclosures I have nothing to disclose. 3 Changing Role of Surgery N=42,688 Chen Ay et al. Larygoscope. 2007; 117:16-21
Thomas Gernon, MD Otolaryngology THE EVOLVING TREATMENT OF SCCA OF THE OROPHARYNX Disclosures I have nothing to disclose. 3 Changing Role of Surgery N=42,688 Chen Ay et al. Larygoscope. 2007; 117:16-21
Multimodular treatment in Head and Neck Squamous Cell Carcinoma (HNSCC)
") Multimodular treatment in Head and Neck Squamous Cell Carcinoma (HNSCC) Amanda Psyrri, MD,FACP Attikon University Hospital Athens, Greece Learning objectives After reading and reviewing this material,
Multimodular treatment in Head and Neck Squamous Cell Carcinoma (HNSCC) Amanda Psyrri, MD,FACP Attikon University Hospital Athens, Greece Learning objectives After reading and reviewing this material,
MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS
 MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS Kyle Arneson, MD PhD Avera Medical Group Radiation Oncology Avera Cancer Institute 16 th Annual Oncology Symposium September
MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS Kyle Arneson, MD PhD Avera Medical Group Radiation Oncology Avera Cancer Institute 16 th Annual Oncology Symposium September
Therapy of Locally Advanced Head and Neck Cancer: State of the Art
 Therapy of Locally Advanced Head and Neck Cancer: State of the Art Barbara Burtness, MD Chief, Head and Neck ncology Medical ncology Co-Leader Senior Member Fox Chase Cancer Center Philadelphia, PA Therapy
Therapy of Locally Advanced Head and Neck Cancer: State of the Art Barbara Burtness, MD Chief, Head and Neck ncology Medical ncology Co-Leader Senior Member Fox Chase Cancer Center Philadelphia, PA Therapy
The PARADIGM Study: A Phase III Study Comparing Sequential Therapy (ST) to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer
 to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer") The PARADIGM Study: A Phase III Study Comparing Sequential Therapy (ST) to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer Robert I. Haddad, Guilherme Rabinowits, Roy B. Tishler,
The PARADIGM Study: A Phase III Study Comparing Sequential Therapy (ST) to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer Robert I. Haddad, Guilherme Rabinowits, Roy B. Tishler,
RADIATION THERAPY AND CHEMOTHERAPY IN LOCALLY ADVANCED CANCER OF THE HEAD AND NECK Carlos A. Perez, M.D. Former Chairman/Professor Emeritus
 RADIATION THERAPY AND CHEMOTHERAPY IN LOCALLY ADVANCED CANCER OF THE HEAD AND NECK Carlos A. Perez, M.D. Former Chairman/Professor Emeritus Department of Radiation Oncology Mallinckrodt Institute of Radiology/
RADIATION THERAPY AND CHEMOTHERAPY IN LOCALLY ADVANCED CANCER OF THE HEAD AND NECK Carlos A. Perez, M.D. Former Chairman/Professor Emeritus Department of Radiation Oncology Mallinckrodt Institute of Radiology/
Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer
 Techniques in Head and Neck Cancer") 1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
Comparing Alternative treatment Regimens for intermediate and high risk oropharyngeal cancer CompARE. Prof. Hisham Mehanna.
 Comparing Alternative treatment Regimens for intermediate and high risk oropharyngeal cancer CompARE Prof. Hisham Mehanna Chief investigator: Hisham Mehanna Arm 1: Mehmet Sen Arm2: John Chester/Martin
Comparing Alternative treatment Regimens for intermediate and high risk oropharyngeal cancer CompARE Prof. Hisham Mehanna Chief investigator: Hisham Mehanna Arm 1: Mehmet Sen Arm2: John Chester/Martin
Stereotactic radiotherapy
 Stereotactic radiotherapy Influence of patient positioning and fixation on treatment planning - clinical results Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH
Stereotactic radiotherapy Influence of patient positioning and fixation on treatment planning - clinical results Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER
 CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
Radiation Therapy: From Fallacy to Science
 27 th Annual Management of Colon and Rectal Diseases 2.23.2019 Radiation Therapy: From Fallacy to Science Hadi Zahra, MD, DABR Radiation Oncologist CHI Health Henry Lynch Cancer Center Assistant Clinical
27 th Annual Management of Colon and Rectal Diseases 2.23.2019 Radiation Therapy: From Fallacy to Science Hadi Zahra, MD, DABR Radiation Oncologist CHI Health Henry Lynch Cancer Center Assistant Clinical
Radiotherapy & Cervical Cancer Dr Mary McCormack Consultant Clinical Oncologist University College Hospital, London,UK
 Lead Group Log Radiotherapy & Cervical Cancer Dr Mary McCormack Consultant Clinical Oncologist University College Hospital, London,UK Cervical Cancer treatment Treatment planning should be made on a multidisciplinary
Lead Group Log Radiotherapy & Cervical Cancer Dr Mary McCormack Consultant Clinical Oncologist University College Hospital, London,UK Cervical Cancer treatment Treatment planning should be made on a multidisciplinary
Sarcoma and Radiation Therapy. Gabrielle M Kane MB BCh EdD FRCPC Muir Professorship in Radiation Oncology University of Washington
 Sarcoma and Radiation Therapy Gabrielle M Kane MB BCh EdD FRCPC Muir Professorship in Radiation Oncology University of Washington Objective: Helping you make informed decisions Introduction Process Radiation
Sarcoma and Radiation Therapy Gabrielle M Kane MB BCh EdD FRCPC Muir Professorship in Radiation Oncology University of Washington Objective: Helping you make informed decisions Introduction Process Radiation
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Heterogeneity of N2 disease
 Locally Advanced NSCLC Surgery? No. Ramaswamy Govindan M.D Co-Director, Section of Medical Oncology Alvin J Siteman Cancer Center at Washington University School of Medicine St. Louis, Missouri Heterogeneity
Locally Advanced NSCLC Surgery? No. Ramaswamy Govindan M.D Co-Director, Section of Medical Oncology Alvin J Siteman Cancer Center at Washington University School of Medicine St. Louis, Missouri Heterogeneity
Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma
 Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma Consensus update and recommendations, 2018 Head and Neck Steering Committee P. Gorphe *, F. Nguyen, Y. Tao, P. Blanchard,
Surgical Margins in Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma Consensus update and recommendations, 2018 Head and Neck Steering Committee P. Gorphe *, F. Nguyen, Y. Tao, P. Blanchard,
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy. Julia White MD Professor, Radiation Oncology
 Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
State of the Art Radiotherapy for Pediatric Tumors. Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center
 State of the Art Radiotherapy for Pediatric Tumors Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center Introduction Progress and success in pediatric oncology Examples of low-tech and high-tech
State of the Art Radiotherapy for Pediatric Tumors Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center Introduction Progress and success in pediatric oncology Examples of low-tech and high-tech
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Re-irradiation with or without chemotherapy. Jozsef Lövey National Institute of Oncology, Budapest, Hungary
 Re-irradiation with or without chemotherapy Jozsef Lövey National Institute of Oncology, Budapest, Hungary Disclosures Occasional advisory board and educational activity to Merck, Roche, Nutricia, Takeda,
Re-irradiation with or without chemotherapy Jozsef Lövey National Institute of Oncology, Budapest, Hungary Disclosures Occasional advisory board and educational activity to Merck, Roche, Nutricia, Takeda,
Adjuvant Radiotherapy for completely resected NSCLC
 Adjuvant Radiotherapy for completely resected NSCLC ESMO Preceptorship on lung Cancer Manchester February 2017 Cécile Le Péchoux Radiation Oncology Department IOT Institut d Oncologie Thoracique Local
Adjuvant Radiotherapy for completely resected NSCLC ESMO Preceptorship on lung Cancer Manchester February 2017 Cécile Le Péchoux Radiation Oncology Department IOT Institut d Oncologie Thoracique Local
CANCERS of OROPHARYNX and HYPOPHARYNX. STAGING and TREATMENT
 1 CANCERS of OROPHARYNX and HYPOPHARYNX STAGING and TREATMENT 2 1. Staging 2. General Principles of Treatment 3. Site Specific Treatment Guidelines 4. Selected Abstracts from Relevant Studies 3 1. Staging
1 CANCERS of OROPHARYNX and HYPOPHARYNX STAGING and TREATMENT 2 1. Staging 2. General Principles of Treatment 3. Site Specific Treatment Guidelines 4. Selected Abstracts from Relevant Studies 3 1. Staging
Opportunity for palliative care Research
 Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no
 67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no overlying skin changes, gradually increasing in size. Recent
67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no overlying skin changes, gradually increasing in size. Recent
The Integration and Impact of Modern Radiotherapy Techniques in Clinical Practice. Kian Ang
 The Integration and Impact of Modern Radiotherapy Techniques in Clinical Practice Kian Ang Funding: P01-CA06294, R01-CA84415, GF Fletcher Chair, Imclone (phase III trial) From Bench to Bedside Head and
The Integration and Impact of Modern Radiotherapy Techniques in Clinical Practice Kian Ang Funding: P01-CA06294, R01-CA84415, GF Fletcher Chair, Imclone (phase III trial) From Bench to Bedside Head and
REIRRADIATION OF HEAD & NECK TARGETS
 REIRRADIATION OF HEAD & NECK TARGETS WORKSHOP-Current challenges of patient re-irradiation 6-7 september 2018, Stockholm, Sweden Claes Mercke Karolinska Institute and Karolinska University Hospital STOCKHOLM
REIRRADIATION OF HEAD & NECK TARGETS WORKSHOP-Current challenges of patient re-irradiation 6-7 september 2018, Stockholm, Sweden Claes Mercke Karolinska Institute and Karolinska University Hospital STOCKHOLM
Head and Neck Cancer:
 Head and Neck Cancer: Robert Haddad M.D. Clinical Director Head and Neck Oncology Program Dana Farber Cancer Institute Boston, MA Predictive Biomarkers: HPV Abstract 6003: Survival Outcomes By HPV Status
Head and Neck Cancer: Robert Haddad M.D. Clinical Director Head and Neck Oncology Program Dana Farber Cancer Institute Boston, MA Predictive Biomarkers: HPV Abstract 6003: Survival Outcomes By HPV Status
Demands and Perspectives of Hadron Therapy
 Demands and Perspectives of Hadron Therapy Alexander Lin, M.D. Assistant Professor University of Pennsylvania Direction of Operations Roberts Proton Therapy Center Disclosures Teva Pharmaceuticals: Advisory
Demands and Perspectives of Hadron Therapy Alexander Lin, M.D. Assistant Professor University of Pennsylvania Direction of Operations Roberts Proton Therapy Center Disclosures Teva Pharmaceuticals: Advisory
Adjuvant chemo- and radiotherapy for poor prognosis head and neck squamous cell carcinomas
 Critical Reviews in Oncology/Hematology 56 (2005) 353 364 Adjuvant chemo- and radiotherapy for poor prognosis head and neck squamous cell carcinomas Jacques Bernier a,, David G. Pfister b, Jay S. Cooper
Critical Reviews in Oncology/Hematology 56 (2005) 353 364 Adjuvant chemo- and radiotherapy for poor prognosis head and neck squamous cell carcinomas Jacques Bernier a,, David G. Pfister b, Jay S. Cooper
The Role of Concurrent Chemo-radiotherapy in Patients with Head and Neck Cancers: A Review
 The Role of Concurrent Chemo-radiotherapy in Patients with Head and Neck Cancers: A Review M.D. Al-Sarraf 1 1 Williams Beaumont Hospital, Royal Oak, Michigan, USA Introduction In the past, radiotherapy
The Role of Concurrent Chemo-radiotherapy in Patients with Head and Neck Cancers: A Review M.D. Al-Sarraf 1 1 Williams Beaumont Hospital, Royal Oak, Michigan, USA Introduction In the past, radiotherapy
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Carcinoma del Canale Anale. Approcci RadioChemioterapici. Antonino De Paoli.. Oncologia Radioterapica, CRO Aviano.
 Carcinoma del Canale Anale Approcci RadioChemioterapici Antonino De Paoli.. Oncologia Radioterapica, CRO Aviano. Anal Cancer Epidemiology and Risk Factors Uncommon Disease; 2-4% of all GI Tumors Increasing
Carcinoma del Canale Anale Approcci RadioChemioterapici Antonino De Paoli.. Oncologia Radioterapica, CRO Aviano. Anal Cancer Epidemiology and Risk Factors Uncommon Disease; 2-4% of all GI Tumors Increasing
Radiotherapy for rectal cancer. Karin Haustermans Department of Radiation Oncology
 Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
Adjuvant radiotherapy for completely resected early stage NSCLC
 Adjuvant radiotherapy for completely resected early stage NSCLC ESMO Preceptorship on lung Cancer Manchester March 2018 Cécile Le Péchoux Radiation Oncology Department IOT Institut d Oncologie Thoracique
Adjuvant radiotherapy for completely resected early stage NSCLC ESMO Preceptorship on lung Cancer Manchester March 2018 Cécile Le Péchoux Radiation Oncology Department IOT Institut d Oncologie Thoracique
Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT
 Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT David H. Ilson, MD, PhD Gastrointestinal Oncology Service Memorial Sloan Kettering Cancer Center Disclosure Consulting
Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT David H. Ilson, MD, PhD Gastrointestinal Oncology Service Memorial Sloan Kettering Cancer Center Disclosure Consulting
Are we making progress? Marked reduction in operative morbidity and mortality
 Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Workshop LA RADIOTERAPIA DEI TUMORI RARI I TIMOMI : INDICAZIONI
 XXI CONGRESSO NAZIONALE AIRO Genova, 19-22 novembre 2011 Workshop LA RADIOTERAPIA DEI TUMORI RARI I TIMOMI : INDICAZIONI PIERA NAVARRIA Unità Operativa di Radioterapia e Radiochirurgia Humanitas Cancer
XXI CONGRESSO NAZIONALE AIRO Genova, 19-22 novembre 2011 Workshop LA RADIOTERAPIA DEI TUMORI RARI I TIMOMI : INDICAZIONI PIERA NAVARRIA Unità Operativa di Radioterapia e Radiochirurgia Humanitas Cancer
TOXICITY OF TWO CISPLATIN-BASED RADIOCHEMOTHERAPY REGIMENS FOR THE TREATMENT OF PATIENTS WITH STAGE III/IV HEAD AND NECK CANCER
 ORIGINAL ARTICLE TOXICITY OF TWO CISPLATIN-BASED RADIOCHEMOTHERAPY REGIMENS FOR THE TREATMENT OF PATIENTS WITH STAGE III/IV HEAD AND NECK CANCER Dirk Rades, MD, 1 Fabian Fehlauer, MD, 2 Mashid Sheikh-Sarraf,
ORIGINAL ARTICLE TOXICITY OF TWO CISPLATIN-BASED RADIOCHEMOTHERAPY REGIMENS FOR THE TREATMENT OF PATIENTS WITH STAGE III/IV HEAD AND NECK CANCER Dirk Rades, MD, 1 Fabian Fehlauer, MD, 2 Mashid Sheikh-Sarraf,
Pancreatic Cancer and Radiation Therapy
 Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
Diagnosis and what happens after referral
 Diagnosis and what happens after referral Dr Kate Newbold Consultant in Clinical Oncology The Royal Marsden Women's cancers Breast cancer introduction 1 Treatment Modalities Early stage disease -larynx
Diagnosis and what happens after referral Dr Kate Newbold Consultant in Clinical Oncology The Royal Marsden Women's cancers Breast cancer introduction 1 Treatment Modalities Early stage disease -larynx
Combined Modality Therapy State of the Art. Everett E. Vokes The University of Chicago
 Combined Modality Therapy State of the Art Everett E. Vokes The University of Chicago What we Know Some patients are cured (20%) Induction and concurrent chemoradiotherapy are each superior to radiotherapy
Combined Modality Therapy State of the Art Everett E. Vokes The University of Chicago What we Know Some patients are cured (20%) Induction and concurrent chemoradiotherapy are each superior to radiotherapy
Post-Operative Concurrent Chemoradiation with Mitomycin-C for Advanced Head and Neck Cancer
 Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine 2006 Post-Operative Concurrent Chemoradiation with Mitomycin-C for
Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine 2006 Post-Operative Concurrent Chemoradiation with Mitomycin-C for
New Paradigms for Treatment of. Erminia Massarelli, MD, PHD, MS Clinical Associate Professor
 New Paradigms for Treatment of Head and Neck cancers Erminia Massarelli, MD, PHD, MS Clinical Associate Professor City of Hope Disclosure Statement Grant/Research Support frommerck Bristol Grant/Research
New Paradigms for Treatment of Head and Neck cancers Erminia Massarelli, MD, PHD, MS Clinical Associate Professor City of Hope Disclosure Statement Grant/Research Support frommerck Bristol Grant/Research
Where are we with radiotherapy for biliary tract cancers?
 Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist
 Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Head and Neck Reirradiation: Perils and Practice
 Head and Neck Reirradiation: Perils and Practice David J. Sher, MD, MPH Department of Radiation Oncology Dana-Farber Cancer Institute/ Brigham and Women s Hospital Conflicts of Interest No conflicts of
Head and Neck Reirradiation: Perils and Practice David J. Sher, MD, MPH Department of Radiation Oncology Dana-Farber Cancer Institute/ Brigham and Women s Hospital Conflicts of Interest No conflicts of
Questions may be submitted anytime during the presentation.
 Understanding Radiation Therapy and its Role in Treating Patients with Pancreatic Cancer Presented by Pancreatic Cancer Action Network www.pancan.org August 18, 2014 If you experience technical difficulty
Understanding Radiation Therapy and its Role in Treating Patients with Pancreatic Cancer Presented by Pancreatic Cancer Action Network www.pancan.org August 18, 2014 If you experience technical difficulty
Nasopharynx Cancer. 1 Feb Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar)
 Dr Peter Luk (Pathology Registrar)") Nasopharynx Cancer 1 Feb 2016 Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar) Expert Panels Prof Mo Mo Tin Prof Michael Boyer Dr Raewyn Campbell Prof
Nasopharynx Cancer 1 Feb 2016 Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar) Expert Panels Prof Mo Mo Tin Prof Michael Boyer Dr Raewyn Campbell Prof
Cetuximab/cisplatin and radiotherapy in HNSCC: is there a favorite choice?
 Cent. Eur. J. Med. 9(2) 2014 279-284 DOI: 10.2478/s11536-013-0154-9 Central European Journal of Medicine Cetuximab/cisplatin and radiotherapy in HNSCC: is there a favorite choice? Jacopo Giuliani* 1, Marina
Cent. Eur. J. Med. 9(2) 2014 279-284 DOI: 10.2478/s11536-013-0154-9 Central European Journal of Medicine Cetuximab/cisplatin and radiotherapy in HNSCC: is there a favorite choice? Jacopo Giuliani* 1, Marina
Some Seminal Studies. Chemotherapy Alone is Inadequate. Bladder Cancer Role of Radiation in Bladder Sparing. Primary Radiation for Bladder Cancer
 Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Treatment of Locally Advanced Rectal Cancer: Current Concepts
 Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Self-Assessment Module 2016 Annual Refresher Course
 LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
Practice teaching course on head and neck cancer management
 28-29 October 2016 - Saint-Priest en Jarez, France Practice teaching course on head and neck cancer management IMPROVING THE PATIENT S LIFE LIFE THROUGH MEDICAL MEDICAL EDUCATION EDUCATION www.excemed.org
28-29 October 2016 - Saint-Priest en Jarez, France Practice teaching course on head and neck cancer management IMPROVING THE PATIENT S LIFE LIFE THROUGH MEDICAL MEDICAL EDUCATION EDUCATION www.excemed.org