Birthday: 1952/07/31 Date of admission:1999/12/30 Age:48 y/o Past medication:esrd under regular HD for 5+ years; denied DM and HTN
|
|
|
- Roger Smith
- 6 years ago
- Views:
Transcription
1 Birthday: 1952/07/31 Date of admission:1999/12/30 Age:48 y/o Past medication:esrd under regular HD for 5+ years; denied DM and HTN
2 Chief Complaint : 1)intermittent LLQ cramping pain for 2 months 2) LGI from LMD showed irregular shadow at splenic flexure
3 Present illness 48 y/o female under regular HD Intermittent left periumbilical cramping pain for 2 months, at first, AGE was impressed Additionally, constipation became severe
4 So lower GI was performed in 新竹惠民醫院 Irregular shadows at T-colon splenic flexure, mucosal thickening, and multiple strictured intestine segments without definite obstructive lesions were noted
5 1999/12/23:D&C 1999/12/30:adissiom 1999/12/31:coloscope 2000/01/03:lower GI angiography 2000/01/05:abdominal CT 2000/01/06:ERCP 2000/01/10:exploratory laparotomy 2000/01/21:discharge
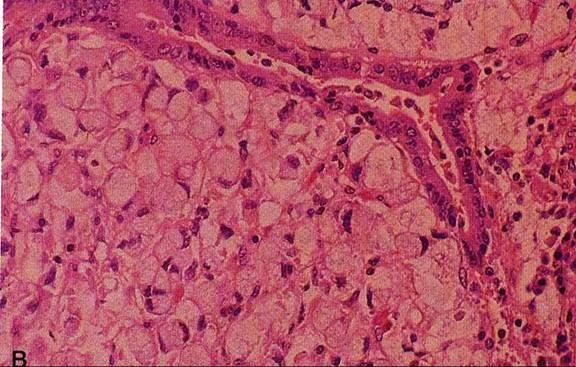
6 1999/12/23:D&C Currettage specimen show endometrium and myometrial tissue with signet-ring cell carcinoma DX: metastatic signet ring cell adenocarcinoma


7 Chest X-ray and KUB: no special finding

8 1999/12/31:coloscope Hyperemic, nodular swelling mucosa change of colon was noted at 50 cm from anal verge, so the scope can t pass through Biopsy: nonspecific chronic inflammatory

9 Angiography


10 Angiography Multilpe hyperemic area was noted over the rectosigmoid and splenic flexure regions, mucosal erotic chronic bleeding was susupected


11 Lower GI Multiple segmental strictures with mucosal tethering at recto-sigmoid, sigmoid-descending junction and the splenic flexure


12 IMP: tumor seeding to the colon is highly suggested

13

14 Abdominal CT (1) Pre-contrast

15
16 89/01/05:abdominal CT Inhomogenous infiltrative mass at retrogastric space, with invation to the pancreas tail, T-colon, descending colon and left pararenal space Bilateral renal atrophy IMP: infiltrative mass at retrogastric space DDX: gastric ca, pancreatic ca; associated with peritoneal seeding


17 89/01/06:ERCP Nonspecific finding
18 89/01/10:exploratory laparotomy Pre-op DX: Abd. Pain r/o carcinomatosis Post-op DX: advanced gastric ca + multiple tumor seeding included peritonum, douglaus pouch, sigmoid and mesentary Path. DX: metastatic adenocarcinoma with scattering signet-ring cells
19 Different diagnosis Gastric adenocarcinoma with peritoneal metastasis -most likely Pancreatic cancer Gastric lymphoma Metastic cancer from unknown
20 Gastric adenocarcinoma
21 S/S of Gastric adenocarcinoma Abdominal pain Unexplained weight loss Anorexia Early satiety Anemia or upper GI bleeding -none is sensitive or specific
22 Morphology 1. polypoid/ fungating carcinoma 2. Ulcerating/ penetrating carcinoma( 70% ) 3. Infiltating / scirrhous carcinoma = linitis plastica( 5~15% ) 4. Superficial spreading carcinoma = confined to mucosa / submucosa; 5-year survival of 90% 5. Advanced carcinoma
23 linitis plastica 1. histo: frequently signet ring cell type+ increase fibrous tissue 2. Firmness, rigidity, reduced capacity of stomach, aperistalsis in involved area 3. Granular/ polypoid fold with encircling growth
 Type II : superficial type< 0.")
24 Early gastric cancer (20%)=invasion limited to mucosa+ submucosa( T1 lesion ) Type I: protruded type> 0.5 cm height with protrusion into gastric lumen(10~20%) Type II : superficial type< 0.5 cm height IIa: slightly elevated surface ( 10~20% ) IIb: flat/ almost unrecognizable ( 2% ) IIc: slightly depressed surface(50~60%) Type III : excavated type ( 5~10 %)

25 Advanced gastric cancer( T2 lesion and higher) Bormann classification: Type 1 : broad- based elevated polypoid lesion Type 2 : elevated lesion + ulceration + well-demarcated margin Type 3 : elevation + ulceration + ill-defined margin Type 4 : ill-defined flat lesion Type 5 : unclassified, no apparent elevation
26 Evidence of metastatic cancer Abdominal mass, ascites or jaundice Enlarged Virchow s node( supraclavicular n.) Sister Mary Joseph s node(infiltration of the umbilicus) Blumer s shelf( a mass in pelvic cul-de-sac) Krukenberg s tumor( enlarged ovaries on PE)

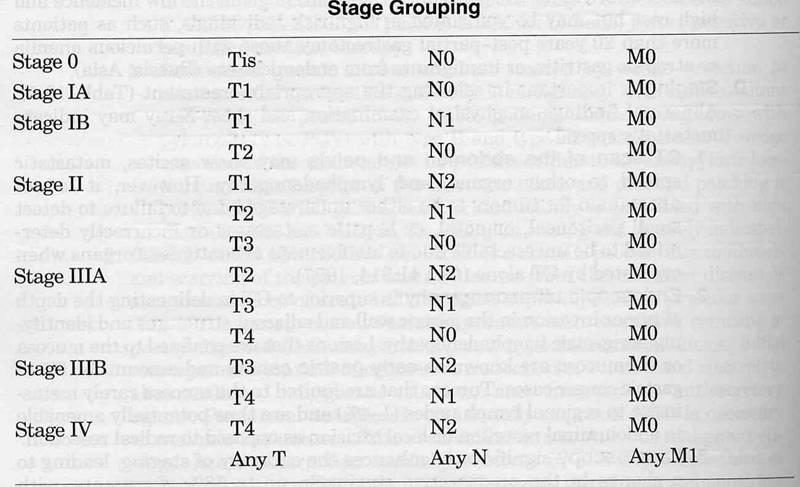
27 Stage -importment in selecting the appropriate treatment
28
29 Prognosis Overall 5-year survival rate of 5~18%, mean survival time of 7~8 months 5-year survival in stage T1: 85% 5-year survival in stage T2: 52% 5-year survival in stage T3: 47% 5-year survival in stage N1~2: 17% 5-year survival in stage N3: 5%

30 Prognostic parameters of gastric carcinoma
31 Classification of lymphoma A. Primary lymphoma of bowel- localized or diffuse B. Secondary intestinal lymphoma- as part of generalized systemic process Histo: predominantly NHL( lymphosarcoma, reticulum cell sarcoma); 15% Hodgkin disease May be associated with: enlarged extraabdominal lymph nodes or spleen, malabsorption
32 Radiographic types of lymphoma (A) Polypoid / nodular ( 47% ) Enlarged nodular folds (B) Ulcerative( 42% ) Ulcerative lesions, may be complicated by performation Aneurysmal configuration (c) Diffuse infiltrating( 11% ) Decreased / absent peristalsis
33 CT staging Stage I : tumor confined to bowel wall Stage II : limited to local nodes Stage III : widespread nodal disease Stage IV : disseminated to bone marrow, liver, other organs
34 Prognosis of lymphoma 71~82% 2 year survival rate in isolated bowel lymphoma 0% 2 year survival rate in stage IV with bowel involvement
35 Pancreatic neoplasm 1. Epithelial origin 2. Acinar cell origin- ex. acinar cell carcinoma 3. Nonepithelial origin- ex.lymphoma or metastases
General Data. Age: 75y/o Sex: female Date of admission:
 General Data Age: 75y/o Sex: female Date of admission: 87-10-31 Chief complaint Poor oral intake, hunger pain for months and body weight loss about 10kg in 3 months Present Illness Quit healthy before
General Data Age: 75y/o Sex: female Date of admission: 87-10-31 Chief complaint Poor oral intake, hunger pain for months and body weight loss about 10kg in 3 months Present Illness Quit healthy before
General Data. Gender : Male Birthday and age : 12/07/24,80 y/o Occupation : 無 Date of Admission :
 General Data Gender : Male Birthday and age : 12/07/24,80 y/o Occupation : 無 Date of Admission : 92-07-09 1 Chief complaint Upper abdominal fullness 30 minutes after having foods with sometimes epigastralgia
General Data Gender : Male Birthday and age : 12/07/24,80 y/o Occupation : 無 Date of Admission : 92-07-09 1 Chief complaint Upper abdominal fullness 30 minutes after having foods with sometimes epigastralgia
By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ.
 Professor of Surgery, Taibah Univ.") By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ. Objectives Types Incidence Risk factors (& prevention) Pathology: Gross, microscopic, spread, staging,
By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ. Objectives Types Incidence Risk factors (& prevention) Pathology: Gross, microscopic, spread, staging,
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Patient. Male 76 year old C.C: abdominal pain
 Patient Male 76 year old C.C: abdominal pain Bowel stool retention Suspected pulmonary TB at right upper lung Infiltration in right lower lung Pleural thickening at the Right chest Localized dilated small
Patient Male 76 year old C.C: abdominal pain Bowel stool retention Suspected pulmonary TB at right upper lung Infiltration in right lower lung Pleural thickening at the Right chest Localized dilated small
Guidelines for Assigning Summary Stage 2000
 Guidelines for Assigning Summary Stage 2000 Mary Lewis, CTR National Program of Cancer Registries 2014 NCRA Annual Meeting May 17, 2014 National Center for Chronic Disease Prevention and Health Promotion
Guidelines for Assigning Summary Stage 2000 Mary Lewis, CTR National Program of Cancer Registries 2014 NCRA Annual Meeting May 17, 2014 National Center for Chronic Disease Prevention and Health Promotion
General history. Basic Data : Age :62y/o Date of admitted: Married status : Married
 General history Basic Data : Age :62y/o Date of admitted:940510 Married status : Married General history Chief Complain : bilateral ovarian cyst incidentally being found out during pap smear. Present Illness
General history Basic Data : Age :62y/o Date of admitted:940510 Married status : Married General history Chief Complain : bilateral ovarian cyst incidentally being found out during pap smear. Present Illness
CT EVALUATION OF GASTRIC LESIONS:
 CT EVALUATION OF GASTRIC LESIONS: Pictural essay Hasni Bouraoui I, Kahloun A, Jemni H, Elouni F, Moulahi H, Daadoucha A, Ben Ali A, Sriha B, Tlili Graies K Departments of Radiology, Gastro enterology,
CT EVALUATION OF GASTRIC LESIONS: Pictural essay Hasni Bouraoui I, Kahloun A, Jemni H, Elouni F, Moulahi H, Daadoucha A, Ben Ali A, Sriha B, Tlili Graies K Departments of Radiology, Gastro enterology,
METASTASES FROM GASTRIC CARCINOMA TO COLON LESIONS: A CASE REPORT IN THE FORM OF MULTIPLE FLAT ELEVATED CASE PRESENTATION
 H.C. Lee, M.T. Yang, K.Y. Lin, et al METASTASES FROM GASTRIC CARCINOMA TO COLON IN THE FORM OF MULTIPLE FLAT ELEVATED LESIONS: A CASE REPORT Hsi-Chang Lee, Min-Ta Yang, 1 Kuang-Yang Lin, 1 Hsing-Yang Tu,
H.C. Lee, M.T. Yang, K.Y. Lin, et al METASTASES FROM GASTRIC CARCINOMA TO COLON IN THE FORM OF MULTIPLE FLAT ELEVATED LESIONS: A CASE REPORT Hsi-Chang Lee, Min-Ta Yang, 1 Kuang-Yang Lin, 1 Hsing-Yang Tu,
IMAGING GUIDELINES - COLORECTAL CANCER
 IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
GENERAL DATA. Sex : female Age : 40 years old Marriage status : married
 GENERAL DATA Sex : female Age : 40 years old Marriage status : married CHIEF COMPLAINT Bilateral ovarian tumors discovered by sonography accidentally PRESENT ILLNESS 2003-06-26 :bilateral ovarian tumors
GENERAL DATA Sex : female Age : 40 years old Marriage status : married CHIEF COMPLAINT Bilateral ovarian tumors discovered by sonography accidentally PRESENT ILLNESS 2003-06-26 :bilateral ovarian tumors
Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22
 Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22 Chief complaint Unknown fever for one month Hand tremor and left huge renal tumor was noted Present illness Suffered from fever for one month, hand
Sex: 女 Age: 51 Occupation: 無 Admission date:92/07/22 Chief complaint Unknown fever for one month Hand tremor and left huge renal tumor was noted Present illness Suffered from fever for one month, hand
Disorders of Cell Growth & Neoplasia. Histopathology Lab
 Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Disorders of Cell Growth & Neoplasia Histopathology Lab Paul Hanna April 2010 Case #84 Clinical History: 5 yr-old, West Highland White terrier. skin mass from axillary region. has been present for the
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
CASE STUDY. Presented by: Jessica Pizzo. CFCC Sonography student Class of 2018
 CASE STUDY Presented by: Jessica Pizzo CFCC Sonography student Class of 2018 Case Presentation April 4, 2017 56 yr old woman presented to ED with lower abdominal pain & swelling, along with constipation.
CASE STUDY Presented by: Jessica Pizzo CFCC Sonography student Class of 2018 Case Presentation April 4, 2017 56 yr old woman presented to ED with lower abdominal pain & swelling, along with constipation.
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 Final Pathology:
 Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Q: In order to use the code 8461/3 (serous surface papillary) for ovary, does it have to say the term "surface" on the path report?
 for ovary, does it have to say the term surface on the path report?") Q&A Session for Collecting Cancer Data: Ovary Q: In order to use the code 8461/3 (serous surface papillary) for ovary, does it have to say the term "surface" on the path report? A: We reviewed both the
Q&A Session for Collecting Cancer Data: Ovary Q: In order to use the code 8461/3 (serous surface papillary) for ovary, does it have to say the term "surface" on the path report? A: We reviewed both the
Pre-operative assessment of patients for cytoreduction and HIPEC
 Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Case Study: #3: Gallbladder Carcinoma?
 Case Study: #3: Gallbladder Carcinoma? By: Megan Wyatt K. SON Wyatt 225 2B1 RDMS, RVT Patient: Male 85 YOA Caucasian Indication: Elevated Alkaline Phosphatase History Annual physical showed elevated alkaline
Case Study: #3: Gallbladder Carcinoma? By: Megan Wyatt K. SON Wyatt 225 2B1 RDMS, RVT Patient: Male 85 YOA Caucasian Indication: Elevated Alkaline Phosphatase History Annual physical showed elevated alkaline
Gastrointestinal Tract Cancer
 Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Alison Douglass Gillian Lieberman, MD. November. Colon Cancer. Alison Douglass, Harvard Medical School Year III Gillian Lieberman, MD
 November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Paris classification (2003) 삼성의료원내과이준행
 삼성의료원내과이준행") Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
The surface mucous cells and the cardiac and pyloric glands secrete mucus which protects the stomach from self-digestion.
 PATHOLOGY OF THE STOMACH Stomach mucosa Gastric mucosa is covered by a layer of mucus. The mucosal glands comprise the cardiac glands, the fundic glands in the fundus and body of the stomach, and the pyloric
PATHOLOGY OF THE STOMACH Stomach mucosa Gastric mucosa is covered by a layer of mucus. The mucosal glands comprise the cardiac glands, the fundic glands in the fundus and body of the stomach, and the pyloric
Title: Linitis plastica of the colon due to metastases of invasive lobular breast carcinoma
 Title: Linitis plastica of the colon due to metastases of invasive lobular breast carcinoma Authors: David Viso Vidal, Rafael Villanueva Pavón, Francisco Jorquera Plaza DOI: 10.17235/reed.2019.6065/2018
Title: Linitis plastica of the colon due to metastases of invasive lobular breast carcinoma Authors: David Viso Vidal, Rafael Villanueva Pavón, Francisco Jorquera Plaza DOI: 10.17235/reed.2019.6065/2018
X-Ray Corner. Imaging of the Stomach. Pantongrag-Brown L
 THAI J 178 Imaging of the Stomach GASTROENTEROL 2014 X-Ray Corner Imaging of the Stomach Pantongrag-Brown L Imaging modalities used in stomach include plain radiographs, UGI study, US, CT, PET CT and MRI.
THAI J 178 Imaging of the Stomach GASTROENTEROL 2014 X-Ray Corner Imaging of the Stomach Pantongrag-Brown L Imaging modalities used in stomach include plain radiographs, UGI study, US, CT, PET CT and MRI.
Polyps in general: is a descriptive term of forming a mass that is exophytic & polypoid.
 ميحرلا نمحرلا هللا مسب Gastric Tumors: Benign tumours & tumor-like conditions: -Mucosal: Gastric polyps (they are uncommon) -Mesenchymal tumours: Leiomyoma & Lipoma (can occur anywhere in the body) Malignant:
ميحرلا نمحرلا هللا مسب Gastric Tumors: Benign tumours & tumor-like conditions: -Mucosal: Gastric polyps (they are uncommon) -Mesenchymal tumours: Leiomyoma & Lipoma (can occur anywhere in the body) Malignant:
A Case of Colon Cancer Metastasizing to the Spleen
 Jpn. J. Clin. Oncol. J984, 14 (3), 425 ~ 430 A Case of Colon Cancer Metastasizing to the Spleen SEISHIRO INABA, M.D., TSUGUO TANAKA, M.D., H1SAKAZU YAMAGISHI, M.D., KIMIO IGUCHI, M.D., HIDEAKI KURIOKA,
Jpn. J. Clin. Oncol. J984, 14 (3), 425 ~ 430 A Case of Colon Cancer Metastasizing to the Spleen SEISHIRO INABA, M.D., TSUGUO TANAKA, M.D., H1SAKAZU YAMAGISHI, M.D., KIMIO IGUCHI, M.D., HIDEAKI KURIOKA,
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Patient underwent hemicolectomy: 7 x 4.5 cm intusscepted segment of ileum in colon - mucosal
 Extranodal Lymphomas Rena Buckstein Odette Cancer Center Case: JT 69 yo male COO software company PMHx: basal cell back, cholesterol Presents to ER with severe abdominal pain, bloody diarrhea x 2d In ER
Extranodal Lymphomas Rena Buckstein Odette Cancer Center Case: JT 69 yo male COO software company PMHx: basal cell back, cholesterol Presents to ER with severe abdominal pain, bloody diarrhea x 2d In ER
Abstracting Hematopoietic Neoplasms
 CASE 1: LYMPHOMA PHYSICAL EXAMINATION 43yo male with a history of lower gastrointestinal bleeding and melena undergoing colonoscopy and biopsy to rule out neoplasm versus inflammation. Patient had no other
CASE 1: LYMPHOMA PHYSICAL EXAMINATION 43yo male with a history of lower gastrointestinal bleeding and melena undergoing colonoscopy and biopsy to rule out neoplasm versus inflammation. Patient had no other
HIPEC Controversies in the Indications and Application of Regional Chemotherapy for Peritoneal Surface Malignancies
 HIPEC Controversies in the Indications and Application of Regional Chemotherapy for Peritoneal Surface Malignancies Crescent City Cancer Update: GI and HPB Saturday September 24, 2016 George M. Fuhrman,
HIPEC Controversies in the Indications and Application of Regional Chemotherapy for Peritoneal Surface Malignancies Crescent City Cancer Update: GI and HPB Saturday September 24, 2016 George M. Fuhrman,
GASTRIC CANCER DR AMIR ASHRAFI
 GASTRIC CANCER DR AMIR ASHRAFI Epidemiology Aetiologic factors Classification Clinical features Investigations Staging Treatment EPIDEMIOLOGY AND FACTS ü Worldwide, gastric cancer is the fourth most common
GASTRIC CANCER DR AMIR ASHRAFI Epidemiology Aetiologic factors Classification Clinical features Investigations Staging Treatment EPIDEMIOLOGY AND FACTS ü Worldwide, gastric cancer is the fourth most common
MULTIPLE PRIMARY CANCERS: PRIMARY MALIGNANT LYMPHOMAS AND CARCINOMAS OF THE INTESTINAL TRACT IN THE SAME PATIENT
 J. clin. Path. (1960), 13, 483. MULTIPLE PRIMARY CANCERS: PRIMARY MALIGNANT LYMPHOMAS AND CARCINOMAS OF THE INTESTINAL TRACT IN THE SAME PATIENT BY JOHN S. CORNES From the Vincent Square Laboratories,
J. clin. Path. (1960), 13, 483. MULTIPLE PRIMARY CANCERS: PRIMARY MALIGNANT LYMPHOMAS AND CARCINOMAS OF THE INTESTINAL TRACT IN THE SAME PATIENT BY JOHN S. CORNES From the Vincent Square Laboratories,
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Multiple Primary Quiz
 Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Gastric Cancer in a Young Postpartum Female. Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012
 Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM
 OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES CASE 1: FEMALE REPRODUCTIVE
 Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES PHYSICAL EXAMINATION CASE 1: FEMALE REPRODUCTIVE 3/5 Patient presents through the emergency room with
Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES PHYSICAL EXAMINATION CASE 1: FEMALE REPRODUCTIVE 3/5 Patient presents through the emergency room with
Case Scenario 1. 1/2/13 History: 64-year-old white female presented with right leg swelling and redness, abdominal pain.
 Case Scenario 1 1/2/13 History: 64-year-old white female presented with right leg swelling and redness, abdominal pain. 1/02/13 CT Abdomen/Pelvis: Abnormal area of nodular mesenteric and left anterior
Case Scenario 1 1/2/13 History: 64-year-old white female presented with right leg swelling and redness, abdominal pain. 1/02/13 CT Abdomen/Pelvis: Abnormal area of nodular mesenteric and left anterior
Cancer of the Stomach
 Cancer of the Stomach Review of Consecutive Ten Year Intervals KENNETH ADASHEK, M.D.,* JAMES SANGER, M.D.,t WILLIAM P. LONGMIRE, JR., M.D.* Records were reviewed for all patients who underwent primary
Cancer of the Stomach Review of Consecutive Ten Year Intervals KENNETH ADASHEK, M.D.,* JAMES SANGER, M.D.,t WILLIAM P. LONGMIRE, JR., M.D.* Records were reviewed for all patients who underwent primary
Bowel obstruction and tumors
 Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Sarah Burton. Lead Gynae Oncology Nurse Specialist Cancer Care Cymru
 Sarah Burton Lead Gynae Oncology Nurse Specialist Cancer Care Cymru Gynaecological Cancers Cervical Cancers Risk factors Presentation Early sexual activity Multiple sexual partners Smoking Human Papiloma
Sarah Burton Lead Gynae Oncology Nurse Specialist Cancer Care Cymru Gynaecological Cancers Cervical Cancers Risk factors Presentation Early sexual activity Multiple sexual partners Smoking Human Papiloma
Gastric Tumors Dr. Taha
 Gastric Tumors Dr. Taha BENIGN TUMORS: Leiomyomas: smooth muscle tumors, equal in men /women, typically located in the middle &distal stomach. Can grow into the lumen with secondary ulceration & bleeding.
Gastric Tumors Dr. Taha BENIGN TUMORS: Leiomyomas: smooth muscle tumors, equal in men /women, typically located in the middle &distal stomach. Can grow into the lumen with secondary ulceration & bleeding.
Autoimmune Pancreatitis: A Great Imitator
 Massachusetts General Hospital Harvard Medical School Autoimmune Pancreatitis: A Great Imitator Dushyant V Sahani MD dsahani@partners.org Autoimmune Pancreatitis: Learning Objectives Clinical manifestations
Massachusetts General Hospital Harvard Medical School Autoimmune Pancreatitis: A Great Imitator Dushyant V Sahani MD dsahani@partners.org Autoimmune Pancreatitis: Learning Objectives Clinical manifestations
Case Scenario 1. Pathology report Specimen from mediastinoscopy Final Diagnosis : Metastatic small cell carcinoma with residual lymphatic tissue
 Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
AJCC 7 th Edition Staging Disease Site Webinar Colorectum
 AJCC 7 th Edition Staging Disease Site Webinar Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310
AJCC 7 th Edition Staging Disease Site Webinar Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310
7 th Edition Staging. AJCC 7 th Edition Staging. Disease Site Webinar. Colorectum. Overview. This webinar is sponsored by
 AJCC 7 th Edition Staging Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers
AJCC 7 th Edition Staging Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers
2009 USCAP Gyn Pathology Evening Session Case #3. Richard J. Zaino, MD Hershey Medical Center Penn State University Hershey, PA
 2009 USCAP Gyn Pathology Evening Session Case #3 Richard J. Zaino, MD Hershey Medical Center Penn State University Hershey, PA rzaino@psu.edu Clinical history Middle aged woman with an exophytic mass of
2009 USCAP Gyn Pathology Evening Session Case #3 Richard J. Zaino, MD Hershey Medical Center Penn State University Hershey, PA rzaino@psu.edu Clinical history Middle aged woman with an exophytic mass of
Case Discussion Splenic Abscess
 Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Case Discussion Splenic Abscess Personal Data Gender: male Birth Date: 1928/Mar/06th Allergy: Mefenamic Smoking: 0.5 PPD for 55 years Alcohol: negative (?) 4 Months Ago Abdominal pain: epigastric area
Imaging techniques in the diagnosis, staging and follow up of GI cancers. Moderators: Banke Agarwal, MD and Paul Schultz, MD
 Imaging techniques in the diagnosis, staging and follow up of GI cancers Moderators: Banke Agarwal, MD and Paul Schultz, MD Panelists Axel Grothey, MD Professor of Oncology Division of Medical Oncology
Imaging techniques in the diagnosis, staging and follow up of GI cancers Moderators: Banke Agarwal, MD and Paul Schultz, MD Panelists Axel Grothey, MD Professor of Oncology Division of Medical Oncology
Case Scenario 1. 1/2/13 History: 64-year-old white female presented with right leg swelling and redness, abdominal pain.
 Case Scenario 1 1/2/13 History: 64-year-old white female presented with right leg swelling and redness, abdominal pain. 1/02/13 CT Abdomen/Pelvis: Abnormal area of nodular mesenteric and left anterior
Case Scenario 1 1/2/13 History: 64-year-old white female presented with right leg swelling and redness, abdominal pain. 1/02/13 CT Abdomen/Pelvis: Abnormal area of nodular mesenteric and left anterior
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
... Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment.
 Definition Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment. " Epidemiology Humans represent the main reservoir of Clostridium difficile, which is not part of the
Definition Inflammatory disorder of the colon that occurs as a complication of antibiotic treatment. " Epidemiology Humans represent the main reservoir of Clostridium difficile, which is not part of the
H&E, IHC anti- Cytokeratin
 Cat No: OVC2281 - Ovary cancer tissue array Lot# Cores Size Cut Format QA/QC OVC228101 228 1.1mm 4um 12X19 H&E, IHC anti- Cytokeratin Recommended applications: For Research use only. RNA or protein ovary
Cat No: OVC2281 - Ovary cancer tissue array Lot# Cores Size Cut Format QA/QC OVC228101 228 1.1mm 4um 12X19 H&E, IHC anti- Cytokeratin Recommended applications: For Research use only. RNA or protein ovary
NAACCR Webinar Series 1 Q&A. Fabulous Prizes. Collecting Cancer Data: Ovary 11/3/2011. Collecting Cancer Data: Ovary
 NAACCR 2011 2012 Webinar Series Collecting Cancer Data: Ovary Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
NAACCR 2011 2012 Webinar Series Collecting Cancer Data: Ovary Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
CASE REPORT GASTRIC ADENOCARCINOMA METASTASIS TO THE BREAST- A DIFFERENTIAL DIAGNOSIS WITH PRIMARY BREAST ADENOCARCINOMA AND REVIEW OF LITERATURE.
 GASTRIC ADENOCARCINOMA METASTASIS TO THE BREAST- A DIFFERENTIAL DIAGNOSIS WITH PRIMARY BREAST ADENOCARCINOMA AND REVIEW OF LITERATURE. Ashwin Hebbar.K 1, Shashidar. K 2, Kamal Kishor 3, Manjunath 4, Shivakumar.H.
GASTRIC ADENOCARCINOMA METASTASIS TO THE BREAST- A DIFFERENTIAL DIAGNOSIS WITH PRIMARY BREAST ADENOCARCINOMA AND REVIEW OF LITERATURE. Ashwin Hebbar.K 1, Shashidar. K 2, Kamal Kishor 3, Manjunath 4, Shivakumar.H.
SEER Summary Stage Still Here!
 SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
3/22/2011. Inflammatory Bowel Disease. Inflammatory Bowel Disease Objectives: Appendicitis. Lemone and Burke Chapter 26
 Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Inflammatory Bowel Disease Lemone and Burke Chapter 26 Inflammatory Bowel Disease Objectives: Discuss etiology, patho and clinical manifestations of Appendicitis Peritonitis Ulcerative Colitis Crohn s
Anatomy of the biliary tract
 Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Basic Data. Birthday: Gender:Female Admission date:
 Basic Data Birthday:1951-07-02 Gender:Female Admission date:2004-06-28 Chief Complaint A protruding mass over RLQ abdomen for many years. Present Illness & Past History Pseudomyxoma peritonei s/p laparotomy
Basic Data Birthday:1951-07-02 Gender:Female Admission date:2004-06-28 Chief Complaint A protruding mass over RLQ abdomen for many years. Present Illness & Past History Pseudomyxoma peritonei s/p laparotomy
GALLBLADDER CANCER. Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011
 GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
Chapter 3. Neoplasms. Copyright 2015 Cengage Learning.
 Chapter 3 Neoplasms Terminology Related to Neoplasms and Tumors Neoplasm New growth Tumor Swelling or neoplasm Leukemia Malignant disease of bone marrow Hematoma Bruise or contusion Classification of Neoplasms
Chapter 3 Neoplasms Terminology Related to Neoplasms and Tumors Neoplasm New growth Tumor Swelling or neoplasm Leukemia Malignant disease of bone marrow Hematoma Bruise or contusion Classification of Neoplasms
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam
 Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
Safe Answers For The American Board of Surgery Certifying Exam & Recertifying Exam By Sarmad Aji, MD., FACS. A comprehensive review of the most commonly asked questions on the American Board of Surgery
The Paris classification of colonic lesions
 The Paris classification of colonic lesions Training to improve the interobserver agreement among international experts Sascha van Doorn, MD, PhD-student in CRC-reserach group of Evelien Dekker Introduction
The Paris classification of colonic lesions Training to improve the interobserver agreement among international experts Sascha van Doorn, MD, PhD-student in CRC-reserach group of Evelien Dekker Introduction
Gastrointestinal Disorders. Disorders of the Esophagus 3/7/2013. Congenital Abnormalities. Achalasia. Not an easy repair. Types
 Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
Gastrointestinal Disorders Congenital Abnormalities Disorders of the Esophagus Types Stenosis Atresia Fistula Newborn aspirates while feeding. Pneumonia Not an easy repair Achalasia Lack of relaxation
Follow up CT Findings of Various Types of Recurrence after Curative Gastric Surgery 1
 Follow up T Findings of Various Types of Recurrence after urative Gastric Surgery 1 Hye-Jeong Lee, M.D., Myeong-Jin Kim, M.D., Joon Seok Lim, M.D., Ki Whang Kim, M.D. lthough the detection of recurred
Follow up T Findings of Various Types of Recurrence after urative Gastric Surgery 1 Hye-Jeong Lee, M.D., Myeong-Jin Kim, M.D., Joon Seok Lim, M.D., Ki Whang Kim, M.D. lthough the detection of recurred
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
A218 : Esophagus cancer tissues. (formalin fixed)
") (formalin fixed) For research use only Specifications: No. of cases: 40 Tissue type: Esophagus cancer tissues No. of spots: 2 spots from each cancer case (80 spots) 4 non-neoplastic spots (4 spots) Total
(formalin fixed) For research use only Specifications: No. of cases: 40 Tissue type: Esophagus cancer tissues No. of spots: 2 spots from each cancer case (80 spots) 4 non-neoplastic spots (4 spots) Total
MPH Quiz. 1. How many primaries are present based on this pathology report? 2. What rule is this based on?
 MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Case presentation. Eran Zittan. MD Mount Sinai Hospital, Toronto, Canada. Emek Medical Center, Afula, Israel. March, 2016
 Case presentation Eran Zittan. MD Mount Sinai Hospital, Toronto, Canada. Emek Medical Center, Afula, Israel. March, 2016 60 y/o man with long standing UC+PSC. Last 10 years on clinical and endoscopic remission.
Case presentation Eran Zittan. MD Mount Sinai Hospital, Toronto, Canada. Emek Medical Center, Afula, Israel. March, 2016 60 y/o man with long standing UC+PSC. Last 10 years on clinical and endoscopic remission.
Nasogastric tube. Stomach. Pylorus. Duodenum 1. Duodenum 2. Duodenum 3. Duodenum 4
 Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
T of patients with malignant melanoma
 ~~ RADIOGRAPHIC: EVALUATION OF METASTATIC MELANOMA JACK E. MEYER, MD*+$ Malignant melanoma can potentially involve any organ system in the body once it metastasizes beyond the regional lymph nodes. A survey
~~ RADIOGRAPHIC: EVALUATION OF METASTATIC MELANOMA JACK E. MEYER, MD*+$ Malignant melanoma can potentially involve any organ system in the body once it metastasizes beyond the regional lymph nodes. A survey
Evaluation of Suspected Pancreatic Cancer
 Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
TUMOR AND TUMOR-LIKE CONDITIONS OF THE PERITONEUM AND OMENTUM/MESENTERY 40 th. Annual Meeting SCBTMR September 9-13, 2017, Nashville, Tennessee
 TUMOR AND TUMOR-LIKE CONDITIONS OF THE PERITONEUM AND OMENTUM/MESENTERY 40 th. Annual Meeting SCBTMR September 9-13, 2017, Nashville, Tennessee Isaac R Francis University of Michigan Department of Radiology
TUMOR AND TUMOR-LIKE CONDITIONS OF THE PERITONEUM AND OMENTUM/MESENTERY 40 th. Annual Meeting SCBTMR September 9-13, 2017, Nashville, Tennessee Isaac R Francis University of Michigan Department of Radiology
We are IntechOpen, the first native scientific publisher of Open Access books. International authors and editors. Our authors are among the TOP 1%
 We are IntechOpen, the first native scientific publisher of Open Access books 3,350 108,000 1.7 M Open access books available International authors and editors Downloads Our authors are among the 151 Countries
We are IntechOpen, the first native scientific publisher of Open Access books 3,350 108,000 1.7 M Open access books available International authors and editors Downloads Our authors are among the 151 Countries
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R
 Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
ABDOMINAL PAIN AND DIARRHEA - IT S NOT (ALWAYS) WHAT YOU THINK. Yakov Wainer, MD Gastroenterology and Hepatology Meir Medical Center
 WHAT YOU THINK. Yakov Wainer, MD Gastroenterology and Hepatology Meir Medical Center") ABDOMINAL PAIN AND DIARRHEA - IT S NOT (ALWAYS) WHAT YOU THINK Yakov Wainer, MD Gastroenterology and Hepatology Meir Medical Center 1 ST ADMISSION - 2015 38 y/o female Abdominal pain, diarrhea - intermittent
ABDOMINAL PAIN AND DIARRHEA - IT S NOT (ALWAYS) WHAT YOU THINK Yakov Wainer, MD Gastroenterology and Hepatology Meir Medical Center 1 ST ADMISSION - 2015 38 y/o female Abdominal pain, diarrhea - intermittent
FY 2016 MCRCEDP Approved ICD-10 Code List
 Approved List C18.0 Malignant neoplasm of cecum C18.1 Malignant neoplasm of appendix C18.2 Malignant neoplasm of ascending colon C18.3 Malignant neoplasm of hepatic flexure C18.4 Malignant neoplasm of
Approved List C18.0 Malignant neoplasm of cecum C18.1 Malignant neoplasm of appendix C18.2 Malignant neoplasm of ascending colon C18.3 Malignant neoplasm of hepatic flexure C18.4 Malignant neoplasm of
In-situ and invasive carcinoma of the colon in patients with ulcerative colitis
 Gut, 1972, 13, 566-570 In-situ and invasive carcinoma of the colon in patients with ulcerative colitis D. J. EVANS AND D. J. POLLOCK From the Departments of Pathology, Royal Postgraduate Medical School
Gut, 1972, 13, 566-570 In-situ and invasive carcinoma of the colon in patients with ulcerative colitis D. J. EVANS AND D. J. POLLOCK From the Departments of Pathology, Royal Postgraduate Medical School
Chief Complain. Liver lesion found in routine health check 41 days ago
 Chief Complain Liver lesion found in routine health check 41 days ago Present Illness On 2005-7-26 at 台北署立醫院 he underwent a health check for the first time. Abdominal US showed suspicious of a 6*5 cm hepatoma,
Chief Complain Liver lesion found in routine health check 41 days ago Present Illness On 2005-7-26 at 台北署立醫院 he underwent a health check for the first time. Abdominal US showed suspicious of a 6*5 cm hepatoma,
Rectal biopsy as an aid to cancer control in ulcerative colitis
 Rectal biopsy as an aid to cancer control in ulcerative colitis B. C. MORSON AND LILLIAN S. C. PANG From the Research Department, St. Mark's Hospital, London Gut, 1967, 8, 423 EDITORIAL COMMENT This is
Rectal biopsy as an aid to cancer control in ulcerative colitis B. C. MORSON AND LILLIAN S. C. PANG From the Research Department, St. Mark's Hospital, London Gut, 1967, 8, 423 EDITORIAL COMMENT This is
What s your diagnosis?
 What s your diagnosis? Signalment: 9 year old MC 2.7 kg Papillion Presenting Complaint: Presented for work up of anorexia and vomiting History: He had presented to cardiology for work up of a grad IV/VI
What s your diagnosis? Signalment: 9 year old MC 2.7 kg Papillion Presenting Complaint: Presented for work up of anorexia and vomiting History: He had presented to cardiology for work up of a grad IV/VI
Clinical Management of Obscure- Overt Gastrointestinal Bleeding. Presented by Dr. 張瀚文
 Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
Clinical Management of Obscure- Overt Gastrointestinal Bleeding Presented by Dr. 張瀚文 Definition Obscure: : hard to understand; not clear. Overt: : public; not secret. Occult: : hidden from the knowledge
2nd week. preexam. GIT system. Atyaf group. Qs team
 2nd week preexam GIT system Qs team 2nd week 2009 Atyaf group بسم االله الرحمن الرحيم 1) a patient with autoimmune gastritis. He is not likely to develop: A. H.pylori colonization. B. pernicious anemia.
2nd week preexam GIT system Qs team 2nd week 2009 Atyaf group بسم االله الرحمن الرحيم 1) a patient with autoimmune gastritis. He is not likely to develop: A. H.pylori colonization. B. pernicious anemia.
Patient Information. Age: 8 y/o Sex: Female. Date of Admission: Date of Discharge:
 Patient Information Age: 8 y/o Sex: Female Date of Admission: 92-10-08 Date of Discharge: 92-10-18 Chief Complaint Severe admominal pain and vomiting with dysuria since last afternoon Present Illness Lower
Patient Information Age: 8 y/o Sex: Female Date of Admission: 92-10-08 Date of Discharge: 92-10-18 Chief Complaint Severe admominal pain and vomiting with dysuria since last afternoon Present Illness Lower
Subepithelial Lesions of the Gut: When Should I Worry?
 Subepithelial Lesions of the Gut: When Should I Worry? President, ASGE Chairman, GI & Hepatology Scottsdale, AZ Faigel.douglas@mayo.edu Case 55 yo male with reflux EGD for Barrett s Screening SET, mucosal
Subepithelial Lesions of the Gut: When Should I Worry? President, ASGE Chairman, GI & Hepatology Scottsdale, AZ Faigel.douglas@mayo.edu Case 55 yo male with reflux EGD for Barrett s Screening SET, mucosal
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Lower GI bleeding. Aliu Sanni, MD Long Island College Hospital 17 th June, 2010
 Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.
Lower GI bleeding Aliu Sanni, MD Long Island College Hospital 17 th June, 2010 Case Presentation CC: Hematochezia HPI: 28yr old male presents with 1 day episode of bloody stools. Denies any abdominal pain.