OSTEOPOROSIS IN MEN. Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO
|
|
|
- Merry Russell
- 5 years ago
- Views:
Transcription
1 OSTEOPOROSIS IN MEN Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Speakers Bureau: Amgen, Radius Consultant: Abbvie, Amgen, Janssen, Radius, Sanofi

2

3 Watts NB et al J Clin Endocrinol Metab 2012;97:

4 OSTEOPOROSIS IN MEN Discuss the skeletal differences between men and women Describe criteria for diagnosing osteoporosis in men Explain the recommended evaluation Construct a plan for nonpharmacologic management Identify available treatments for men with osteoporosis State appropriate monitoring strategies

5 HOW ARE MEN DIFFERENT FROM WOMEN? Men have Higher peak bone mass Larger bones Different geometry Greater muscle mass Less likely to fall No equivalent to menopause Shorter life span


6 WHAT IS THE ECONOMIC BURDEN? The lifetime risk for any clinical fracture at age 60 is 29% in men and 56% in women. 1 U.S. expenditure for osteoporotic fractures in men (2005) was $4.1 billion, 24% of the total cost Jones G Osteoporosis Int 1994; 4: Burge R et al J Bone Miner Res 2007;22:
7 FRACTURES IN MEN AND WOMEN Data from the UK Curtis EM et al Bone 2016;87:19-26
8 FRACTURES IN MEN AND WOMEN Incidence/1,000,000 Person-years 4,000 3,000 2,000 1,000 0 Forearm Spine Hip Women Men Cooper C et al Trends Endocrinol Metab1992;3:224
9 DISTAL FOREARM FRACTURES IN WOMEN AND MEN Women Men Over time Forearm fractures Fewer in women More in men Amin S et al J Bone Miner Res 2014;29:
10 PROXIMAL FEMUR FRACTURES IN WOMEN AND MEN Women Men Over time Hip fractures Fewer in women No change in men Amin S et al J Bone Miner Res 2014;29:
11 VERTEBRAL FRACTURES IN WOMEN AND MEN Women Men Over time Vertebral fractures More in women More in men Amin S et al J Bone Miner Res 2014;29:

12 MORTALITY AFTER FRACTURES IS GREATER IN MEN Bliuc D et al JAMA 2009;301:
13 WHICH MEN SHOULD HAVE A BMD TEST? Men 70 years or older without additional risk factors Younger men (50-69) with low-trauma fractures Men with diseases/conditions/drugs known to cause bone loss Men considering therapy for osteoporosis Men receiving treatment for osteoporosis ISCD. Binkley NC et al J Clin Densitom 2002;5 (suppl):s19-s28 Endo. Watts NB et al J Clin Endocrinol Metab 2012;97: NOF. Cosman F et al Osteoporos Int 2014:25:

14 DXA TESTING IS LOWER FOR MEN THAN FOR WOMEN Ever-enrolled 65+ Part B FFS recipients as reported in the 5% sample of LDS SAF claims Direct Research LLC, Medicare PSPS Master Files and Medicare 5 Percent Sample LDS SAF, analysis by Peter M. Steven, PhD
 patients with primary hyperparathyroidism patients being monitored to assess the")
15 REIMBURSEMENT FOR DXA INTERIM FINAL RULE Effective July 1, 1998, Medicare covers bone densitometry for five indications: estrogen deficient women at clinical risk for osteoporosis patients with vertebral abnormalities patients receiving long-term glucocorticoids (prednisone 5 mg/d or more for 3+ months) patients with primary hyperparathyroidism patients being monitored to assess the response to an approved drug Federal Register June 24, 1998;63: Watts NB J Clin Densitom 1999;2:







16
17 WHEN YOU ORDER A BMD TEST FOR A 70-YEAR- OLD MAN, HOW WOULD YOU GET IT COVERED? If patient has back pain or height loss, consider spine radiographs before DXA; radiographic osteopenia or vertebral fracture would be covered indications If you have a screening tests, such as heel ultrasound or finger DXA, provide that for free; T-score -1.0 or below is osteopenia Have the patient sign a waiver (ABN) so you can bill the patient if Medicare doesn t pay
18 WHO CRITERIA FOR POSTMENOPAUSAL OSTEOPOROSIS The T-score compares an individual s BMD with the mean value for young normal individuals and expresses the difference as a standard deviation score. T-Score NORMAL -1.0 and above OSTEOPENIA -1.0 to -2.5 OSTEOPOROSIS -2.5 and below Kanis JA et al J Bone Miner Res 1994;9:
19 WHY THE WHO CHOSE A T-SCORE CUTOFF OF -2.5 FOR POSTMENOPAUSAL WOMEN "Such a cutoff value identifies approximately 30% of postmenopausal women as having osteoporosis using measurements made at the spine, hip, or forearm. This is approximately equivalent to the lifetime risk of fracture at these sites." "Criteria different from those just mentioned should be applied to men and to younger individuals before skeletal maturity, but there are insufficient data to establish them The use of a female referent for men is inappropriate." Kanis JA et al J Bone Miner Res 1994; 9:1137
20 WHO INTERIM REPORT-1999 The same absolute BMD value (after adjustment for larger body size) can, provisionally, be utilized for men. Genant HK et al Osteoporos Int 1999;10:

21 DXA UNDERESTIMATES BMD OF SMALL BONES AND OVERESTIMATES BMD IN LARGE BONES 3 cm 3.5 cm 3 cm 4 cm Bone mineral content 2.12 g 3.85 g Volume 21.2 cm cm 3 Volumetric density 0.1 g/cm g/cm 3 Projected area 9.0 cm cm 2 Areal density g/cm g/cm 2
22 USE A MALE OR FEMALE DATABASE TO CALCULATE T-SCORES FOR MEN? T-scores for men are lower with a male database than with a female database (~0.3 hip, ~1 SD spine). Some studies suggest that men fracture at the same BMD as women. If so, a female database should be used. Other studies suggest that men fracture at a higher BMD than women. If so, a male data base should be used.
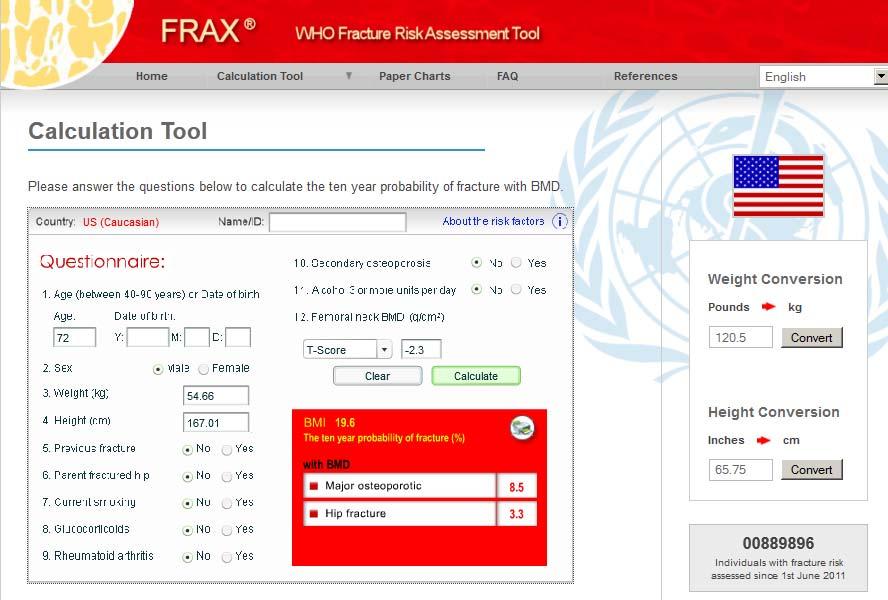
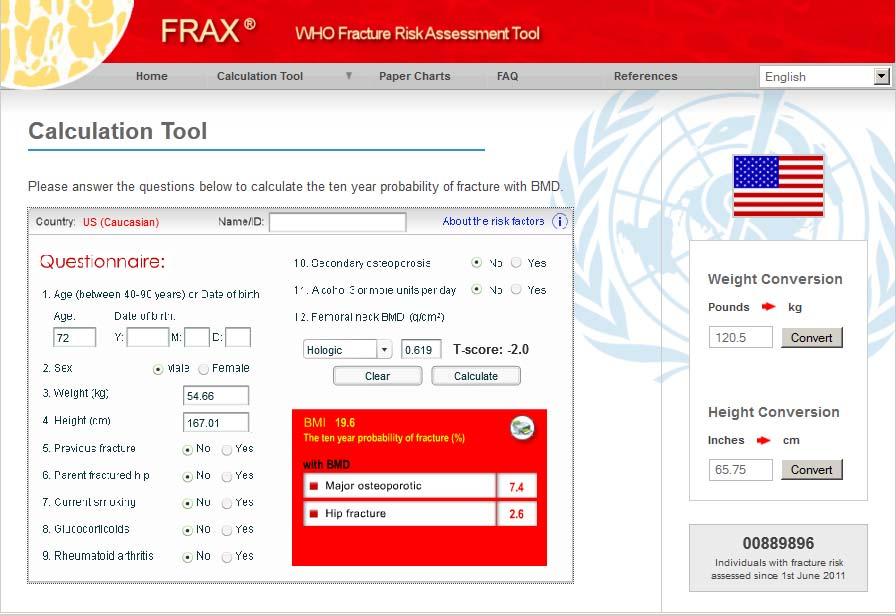
23 USE A MALE OR FEMALE DATABASE TO CALCULATE T-SCORES FOR MEN? Prior to 2013, all DXA manufacturers used a male database for men and a female database for women (and some still do) FRAX uses femoral neck BMD and calculates T-scores using a female database for both men and women (though T-scores in FRAX don t matter FRAX uses BMD to determine fracture risk)

24 4. A uniform Caucasian (non-race adjusted) female reference database should be used to calculate T-scores for men of all ethnic groups. Watts NB et al J Clin Densitom 2013;16:

25
26
27
28
29 NEWER HIP DATA FROM NHANES NHANES III ( ) NHANES Looker AC et al Osteoporos Int 2012;23:
30 SPINE DATA FROM NHANES Looker AC et al Osteoporosis Int 2012:23:






31 MOST MEN WITH FRACTURES DO NOT HAVE OSTEOPOROSIS Rotterdam Study Women Non-vertebral fractures 44% Osteoporosis 13% Normal BMD 21% 18% Men Non-vertebral fractures 43% Low BMD 61% Hip fractures 64% Osteoporosis 5% Normal BMD 31% Low BMD 39% 3% 58% Hip fractures Schuit SCE et al Bone 2004;34:
32 OSTEOPOROSIS PREVALENCE AND FRACTURE RISK IN MEN Prevalence (FN -2.5 and below) Lifetime fracture risk 4% (NHANES female database) 6% (NHANES male database) 6-11% (hip fracture, age 50) 25-30% (any clin fx, age 60) Regardless of whether a male or female database is used, femoral neck T-score cut point of -2.5 identifies only a small proportion of men who will fracture
33 HOW MANY MEN WOULD BE TREATED? 3887 men from MrOs, age % Femoral neck -2.5 or below* 3.2% Spine -2.5 or below* 7.0% Femoral neck OR spine -2.5 or below* 29.0% FRAX 10-year hip fracture risk 3%** 8.3% FRAX 10-year major fracture risk 20%** Meeting any NOF criterion 34% *T-scores calculated using a male database **FRAX risk calculated February 2009 Donaldson MG et al J Bone Miner Res 2010;25:
34 FUNDAMENTAL MEASURES FOR BONE HEALTH Calcium and vitamin D intake Needs in men are similar to women; adequate intake must be ensured Appropriate physical activity Avoid smoking Avoid heavy alcohol use 3 or more units per day (FRAX )
35 SECONDARY OSTEOPOROSIS EVALUATION IN MEN History and physical exam CBC; chemistry profile incl. electrolytes and phosphorus; 25-hydroxyvitamin D; serum testosterone; 24-h urine calcium, sodium and creatinine In selected patients: PTH, SPEP/UPEP,TSH, serum free testosterone, urine free cortisol, skin fibroblast culture, tissue transglutaminase antibodies, IGF-1, histamine metabolites Bone turnover markers Bone biopsy
36 WHICH MEN TO TREAT WITH PHARMACOLOGIC AGENTS? Men with a clinical diagnosis of osteoporosis (spine or hip fracture) 1 Men with a DXA diagnosis of osteoporosis (T-score -2.5 or below) 1 Men at high risk of fracture based on FRAX 1 Where effectiveness of treatment has been shown in clinical trials 2 T-score -2.0 or below Non-spine, non-hip fragility fracture with T-score -1.0 or below 1. Cosman F et al Osteoporos Int 2014:25: Watts NB et al J Clin Endocrinol Metab 2012;97:
37 FDA-APPROVED MEDICATIONS INDICATIONS Postmenopausal Osteoporosis Glucocorticoid-induced Osteoporosis Men Drug Prevention Treatment Prevention Treatment Estrogen Calcitonin (Miacalcin, Fortical ) Raloxifene (Evista ) Ibandronate (Boniva ) Alendronate (Fosamax ) Risedronate (Actonel ) Risedronate (Atelvia ) Zoledronate (Reclast ) Denosumab (Prolia ) Teriparatide (Forteo ) Abaloparatide (Tymlos )
38 FDA-APPROVED MEDICATIONS INDICATIONS Postmenopausal Osteoporosis Glucocorticoid-induced Osteoporosis Men Drug Prevention Treatment Prevention Treatment Estrogen Calcitonin (Miacalcin, Fortical ) Raloxifene (Evista ) Ibandronate (Boniva ) Alendronate (Fosamax ) Risedronate (Actonel ) Risedronate (Atelvia ) Zoledronate (Reclast ) Denosumab (Prolia ) Teriparatide (Forteo ) Abaloparatide (Tymlos )
39 ALENDRONATE INCREASES BMD IN MEN WITH OSTEOPOROSIS 241 men with femoral neck BMD 2.0 or below Men with secondary osteoporosis other than hypogonadism were excluded Lumbar Spine Total Hip Mean BMD (% change from baseline + SE) Alendronate 10 mg/d Placebo Months Mean BMD (% change from baseline + SE) Months Orwoll ES et al N Engl J Med 2000;343:
40 ALENDRONATE INCREASES BMD IN MEN REGARDLESS OF SEX HORMONE LEVELS Change in Lumbar Spine BMD Mean BMD Change (% Over 24 Months) Alendronate < > 126 Quintiles of Free Testosterone (pg/ml) Placebo < > 27 Quintiles of Estradiol (pg/ml) Orwoll ES et al N Engl J Med 2000;343:
41 ALENDRONATE MAY REDUCE VERTEBRAL FRACTURES IN MEN WITH OSTEOPOROSIS men with osteoporosis, age Post hoc analysis Percent with new vertebral fractures over 2 Years *P=0.02 Placebo ALN 10 mg 0-2 Semiquant. Quantitative After data of Orwoll E et al N Engl J Med 2000;343:

42 REDUCTION IN NEW VERTEBRAL FRACTURES ZOLEDRONIC ACID IN MEN 1199 men Median age 66 T-scores -2.2 fem. neck -1.7 total hip ~1/3 had prior VFX Boonen S et al N Engl J Med 2012;367:
43 ONJ AND AFF RISK DIFFERENT FOR MEN vs WOMEN? Swedish Medical Products Agency BP users 2 AFF 1 RR 3 for AFF Men 39, (1.02,18.25) ONJ 1 Women RR 3 for ONJ (0.80, 4.33) 1. Spontaneous reports of AFF and ONJ, excluding non-confirmed cases 2. Bisphosphonate use estimated from Swedish Prescription Register Duration of use similar for men (5 yrs) and women (6 yrs) 3. RR calculated from age-stratified incidence proportions Kharazmi M et al ann Rheum Dis 2014;73:1594
44 EFFECT OF DENOSUMAB ON BMD IN MEN Lumbar Spine Femoral Neck 1/3 Radius D mab 60 mg Q 6 mos Placebo * * * * * *p< vs placebo *p< vs placebo *p< vs placebo Months Months Months Orwoll E et al J Clin Endocrinol Metab 2012;97:
45 REDUCTION IN NEW VERTEBRAL FRACTURES D MAB IN MEN RECEVING ADT 1468 men Median age 75 T-scores -1.5 fem. neck -0.9 total hip ~22% had prior VFx 85% 69% 62% Smith M et al N Engl J Med 2009;361:
46 OSTEOPOROSIS IN MEN: TREATMENT WITH TESTOSTERONE Pharmacologic therapy should be prescribed for men at high risk of fracture, whether testosterone is offered or not, and is effective even if testosterone level is low and not treated Testosterone alone might be considered for Men at high risk for fracture who are not candidates for other agents Candidates for testosterone therapy at borderline risk for fracture Not recommended unless Serum testosterone level is low (<200 ng/ml) Hypogonadism is organic (e.g., pituitary tumor) There are symptoms of hypogonadism (e.g., low libido, erectile dysfunction) Reduce dose or discontinue if there are side effects or no clinical improvement in symptoms
47 EFFECT OF IM TESTOSTERONE ON BMD 70 men age 65 or older Serum testosterone less than 350 ng/dl on two occasions (mean baseline T ~290 ng/dl) Assigned at random to IM testosterone + oral finasteride IM testosterone + oral placebo IM placebo + oral placebo Average serum T with Rx ~750±180 ng/dl Amory JK, Watts NB et al J Clin Endocrinol Metab 2004;89:
48 EFFECT OF IM TESTOSTERONE ON BMD Amory JK, Watts NB et al J Clin Endocrinol Metab 2004;89:
49 EFFECT OF IM TESTOSTERONE ON BTM Amory JK, Watts NB et al J Clin Endocrinol Metab 2004;89:
50 EFFECT OF TESTOSTERONE PATCH ON BMD Conclusion: testosterone doesn t help if the blood level is normal but may increase spine BMD in men with low baseline serum testosterone levels Stratified effect on hip BMD not reported Snyder PJ et al J Clin Endocrinol Metab 1999;84:
51 META-ANALYSIS OF THE EFFECTS OF TESTOSTERONE THERAPY ON BMD Tracz MJ et al J Clin Endocrinol Metab 2006; 91:
52 META-ANALYSIS OF THE EFFECTS OF TESTOSTERONE THERAPY ON BMD Spine Femoral Neck Tracz MJ et al J Clin Endocrinol Metab 2006;91:

53 Geusens PM and van den Bergh JP Nature Rev Rheum 2012;8:

54 Geusens PM and van den Bergh JP Nature Rev Rheum 2012;8:
55 TREATMENT RATES FOR OSTEOPOROSIS ARE LOWER FOR MEN THAN FOR WOMEN van de Velde RY et al Bone 2017;94:50-55
56 OSTEOPOROSIS IN MEN Osteoporosis in men is a serious public health problem BMD testing is recommended for men age 70 and older, as well as younger men at increased risk A female database is recommended to calculate T-scores for men Fracture risk calculation should be done for men with osteopenia (enter femoral neck BMD, not T-score) All men at risk of fracture should be evaluated for cause of secondary osteoporosis Alendronate, risedronate, zoledronate, denosumab and teriparatide are FDA-approved to treat osteoporosis in men Testosterone may be used in limited circumstances

57 Thank you for your attention
CASE 1 WHY IS IT IMPORTANT TO TREAT? FACTS CONCERNS
 4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
4:30-5:15pm Ask the Expert: Osteoporosis SPEAKERS Silvina Levis, MD OSTEOPOROSIS - FACTS 1:3 older women and 1:5 older men will have a fragility fracture after age 50 After 3 years of treatment, depending
Osteoporosis Treatment Overview. Colton Larson RFUMS October 26, 2018
 Osteoporosis Treatment Overview Colton Larson RFUMS October 26, 2018 Burden of Disease Most common bone disease 9.9 million Americans + 43.1 million Americans have low bone mineral density (BMD) Stealthy
Osteoporosis Treatment Overview Colton Larson RFUMS October 26, 2018 Burden of Disease Most common bone disease 9.9 million Americans + 43.1 million Americans have low bone mineral density (BMD) Stealthy
Osteoporosis Agents Drug Class Prior Authorization Protocol
 Osteoporosis Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of
Osteoporosis Agents Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review of
Osteoporosis: A Tale of 3 Task Forces!
 Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
Forteo (teriparatide) Prior Authorization Program Summary
 Prior Authorization Program Summary") Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
Forteo (teriparatide) Prior Authorization Program Summary FDA APPROVED INDICATIONS DOSAGE 1 FDA Indication 1 : Forteo (teriparatide) is indicated for: the treatment of postmenopausal women with osteoporosis
AACE/ACE Osteoporosis Treatment Decision Tool
 AACE/ACE Osteoporosis Treatment Decision Tool What is Osteoporosis? OSTEOPOROSIS is defined as reduced bone strength leading to an increased risk of fracture. Osteoporosis, or porous bones, occurs when
AACE/ACE Osteoporosis Treatment Decision Tool What is Osteoporosis? OSTEOPOROSIS is defined as reduced bone strength leading to an increased risk of fracture. Osteoporosis, or porous bones, occurs when
Osteoporosis Management
 Osteoporosis Management Lisa Voss PA C, CCD Laura Frontiero NP C, CCD Kaiser Healthy Bones Program San Diego Disclosures: Nothing to disclose www.zazzle.com 1 Overview How to diagnose Osteoporosis FRAX
Osteoporosis Management Lisa Voss PA C, CCD Laura Frontiero NP C, CCD Kaiser Healthy Bones Program San Diego Disclosures: Nothing to disclose www.zazzle.com 1 Overview How to diagnose Osteoporosis FRAX
Osteoporosis and Lupus. Andrew Ruthberg, MD University Rheumatologists
 Osteoporosis and Lupus Andrew Ruthberg, MD University Rheumatologists 1 Forget the medical terminology (osteoporosis, osteopenia, low bone mass, DEXA, DXA, T score etc) The bottom line is that you don
Osteoporosis and Lupus Andrew Ruthberg, MD University Rheumatologists 1 Forget the medical terminology (osteoporosis, osteopenia, low bone mass, DEXA, DXA, T score etc) The bottom line is that you don
Osteoporosis: An Overview. Carolyn J. Crandall, MD, MS
 Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Osteoporosis: An Overview Carolyn J. Crandall, MD, MS Professor of Medicine David Geffen School of Medicine at UCLA Objectives Review osteoporosis
TREATING OSTEOPOROSIS IN 2018: WHAT'S OLD, WHAT'S NEW, WHAT'S UNPROVEN AND WHAT'S TRUE. Nelson B. Watts, MD
 TREATING OSTEOPOROSIS IN 2018: WHAT'S OLD, WHAT'S NEW, WHAT'S UNPROVEN AND WHAT'S TRUE Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO Honoraria: Amgen, Radius, Shire Consulting
TREATING OSTEOPOROSIS IN 2018: WHAT'S OLD, WHAT'S NEW, WHAT'S UNPROVEN AND WHAT'S TRUE Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO Honoraria: Amgen, Radius, Shire Consulting
TREATMENT OF OSTEOPOROSIS HOLIDAYS OR NO HOLIDAYS? Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO
 TREATMENT OF OSTEOPOROSIS HOLIDAYS OR NO HOLIDAYS? Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Honoraria: Amgen, Merck, Shire Consulting : AbbVie, Amgen, Merck,
TREATMENT OF OSTEOPOROSIS HOLIDAYS OR NO HOLIDAYS? Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Honoraria: Amgen, Merck, Shire Consulting : AbbVie, Amgen, Merck,
John J. Wolf, DO Family Medicine
 John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
John J. Wolf, DO Family Medicine Objectives: 1. Review incidence & Risk of Osteoporosis 2.Review indications for testing 3.Review current pharmacologic & Non pharmacologic Tx options 4.Understand & Utilize
Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary
 Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary This prior authorization program applies to Commercial, NetResults A series, NetResults F series
Parathyroid Hormone Analog for Osteoporosis Prior Authorization with Quantity Limit Criteria Program Summary This prior authorization program applies to Commercial, NetResults A series, NetResults F series
Current and Emerging Strategies for Osteoporosis
 Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
Current and Emerging Strategies for Osteoporosis I have nothing to disclose. Anne Schafer, MD Assistant Professor of Medicine Division of Endocrinology & Metabolism December 12, 2014 Outline Osteoporosis
Disclosures. Diagnostic Challenges in Osteoporosis: Whom To Treat 9/25/2014
 Disclosures Diagnostic Challenges in Osteoporosis: Whom To Treat Ethel S. Siris, MD Columbia University Medical Center New York, NY Consultant on scientific issues for: AgNovos Amgen Eli Lilly Merck Novartis
Disclosures Diagnostic Challenges in Osteoporosis: Whom To Treat Ethel S. Siris, MD Columbia University Medical Center New York, NY Consultant on scientific issues for: AgNovos Amgen Eli Lilly Merck Novartis
Osteoporosis: A Tale of 3 Task Forces!
 Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
Osteoporosis: A Tale of 3 Task Forces! Robert A. Adler, MD McGuire Veterans Affairs Medical Center Virginia Commonwealth University Richmond, Virginia, USA Disclosures The opinions are those of the speaker
9/9/2015 OSTEOPOROSIS WHAT S NEW AND ON THE HORIZON IN SCREENING, DRUG HOLIDAYS, SUPPLEMENTS, CONSERVATIVE THERAPY DISCLOSURES
 OSTEOPOROSIS WHAT S NEW AND ON THE HORIZON IN SCREENING, DRUG HOLIDAYS, SUPPLEMENTS, CONSERVATIVE THERAPY Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Stock options/holdings,
OSTEOPOROSIS WHAT S NEW AND ON THE HORIZON IN SCREENING, DRUG HOLIDAYS, SUPPLEMENTS, CONSERVATIVE THERAPY Nelson B. Watts, MD OSTEOPOROSIS AND BONE HEALTH SERVICES CINCINNATI, OHIO DISCLOSURES Stock options/holdings,
Osteoporosis/Fracture Prevention
 Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Osteoporosis/Fracture Prevention NATIONAL GUIDELINE SUMMARY This guideline was developed using an evidence-based methodology by the KP National Osteoporosis/Fracture Prevention Guideline Development Team
Pharmacy Management Drug Policy
 SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 9/29/2017 If the member s subscriber contract excludes coverage
Update on Osteoporosis 2016
 WELCOME! Update on Osteoporosis 2016 Jennifer J. Kelly, D.O., F.A.C.E. Associate Professor of Medicine Division of Endocrinology, Diabetes and Metabolism Upstate Medical University Director of the Clinical
WELCOME! Update on Osteoporosis 2016 Jennifer J. Kelly, D.O., F.A.C.E. Associate Professor of Medicine Division of Endocrinology, Diabetes and Metabolism Upstate Medical University Director of the Clinical
Disclosure. Objectives. Osteoporosis. Major Public Health Concern Will I end up like my mother?
 Everything a Pharmacist Needs to Know About Osteoporosis New Mexico Pharmacists Association Mid-Winter Meeting January 27-28, 2018 Albuquerque, NM Consulting Amgen, Radius Speaking Radius Disclosure E.
Everything a Pharmacist Needs to Know About Osteoporosis New Mexico Pharmacists Association Mid-Winter Meeting January 27-28, 2018 Albuquerque, NM Consulting Amgen, Radius Speaking Radius Disclosure E.
Osteoporosis: Are your bones at risk of fracturing? Rachel Wallwork, MD Internal medicine resident Massachusetts General Hospital
 Osteoporosis: Are your bones at risk of fracturing? Rachel Wallwork, MD Internal medicine resident Massachusetts General Hospital What is Osteoporosis? Osteoporosis causes bones to lose density, become
Osteoporosis: Are your bones at risk of fracturing? Rachel Wallwork, MD Internal medicine resident Massachusetts General Hospital What is Osteoporosis? Osteoporosis causes bones to lose density, become
Learning Objectives. Controversies in Osteoporosis Prevention and Management. Etiology. Presenter Disclosure Information. Epidemiology.
 12:45 1:30pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
12:45 1:30pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
Pharmacy Management Drug Policy
 SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide), Boniva injection (Ibandronate) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 10/15/2018 If the member s
SUBJECT: - Forteo (teriparatide), Prolia (denosumab), Tymlos (abaloparatide), Boniva injection (Ibandronate) POLICY NUMBER: Pharmacy-35 EFFECTIVE DATE: 9/07 LAST REVIEW DATE: 10/15/2018 If the member s
Osteoporosis in Men Professor Peter R Ebeling
 Osteoporosis in Men MD FRACP Head, Department of Medicine, School for Clinical Sciences Monash Health Translation Precinct Monash University, Clayton, Victoria 1 MonashHealth Potential Conflicts Departmental
Osteoporosis in Men MD FRACP Head, Department of Medicine, School for Clinical Sciences Monash Health Translation Precinct Monash University, Clayton, Victoria 1 MonashHealth Potential Conflicts Departmental
1
 www.osteoporosis.ca 1 2 Overview of the Presentation Osteoporosis: An Overview Bone Basics Diagnosis of Osteoporosis Drug Therapies Risk Reduction Living with Osteoporosis 3 What is Osteoporosis? Osteoporosis:
www.osteoporosis.ca 1 2 Overview of the Presentation Osteoporosis: An Overview Bone Basics Diagnosis of Osteoporosis Drug Therapies Risk Reduction Living with Osteoporosis 3 What is Osteoporosis? Osteoporosis:
Bone Densitometry Pathway
 Bone Densitometry Pathway The goal of the Bone Densitometry pathway is to manage our diagnosed osteopenic and osteoporotic patients, educate and monitor the patient population at risk for bone density
Bone Densitometry Pathway The goal of the Bone Densitometry pathway is to manage our diagnosed osteopenic and osteoporotic patients, educate and monitor the patient population at risk for bone density
Because the low bone mass and deterioration
 OSTEOPOROSIS A look at recent expert guidelines and key studies in bone health, the findings of which affect your patients young and old Steven R. Goldstein, MD Dr. Goldstein is Professor of Obstetrics
OSTEOPOROSIS A look at recent expert guidelines and key studies in bone health, the findings of which affect your patients young and old Steven R. Goldstein, MD Dr. Goldstein is Professor of Obstetrics
Chau Nguyen, D.O. Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences
 Chau Nguyen, D.O Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences I do not have any relationship with the manufacturer of any commercial products
Chau Nguyen, D.O Rheumatologist Clinical Assistant Professor of Internal Medicine at Western University of Health Sciences I do not have any relationship with the manufacturer of any commercial products
Clinical Practice. Presented by: Internist, Endocrinologist
 Clinical Practice Management of Osteoporosis Presented by: SaeedBehradmanesh, h MD Internist, Endocrinologist Iran, Isfahan, Feb. 2017 Definition: A disease characterized by low bone mass and microarchitectural
Clinical Practice Management of Osteoporosis Presented by: SaeedBehradmanesh, h MD Internist, Endocrinologist Iran, Isfahan, Feb. 2017 Definition: A disease characterized by low bone mass and microarchitectural
Osteoporosis: How to Manage Long- Term Use of Bisphosphonates AKA Now What? David E Feinstein, DO, CCD November 15 th, 2017
 Osteoporosis: How to Manage Long- Term Use of Bisphosphonates AKA Now What? David E Feinstein, DO, CCD November 15 th, 2017 Introduction A fracture due to OP occurs every 3 seconds around the world. 1
Osteoporosis: How to Manage Long- Term Use of Bisphosphonates AKA Now What? David E Feinstein, DO, CCD November 15 th, 2017 Introduction A fracture due to OP occurs every 3 seconds around the world. 1
DXA When to order? How to interpret? Dr Nikhil Tandon Department of Endocrinology and Metabolism All India Institute of Medical Sciences New Delhi
 DXA When to order? How to interpret? Dr Nikhil Tandon Department of Endocrinology and Metabolism All India Institute of Medical Sciences New Delhi Clinical Utility of Bone Densitometry Diagnosis (DXA)
DXA When to order? How to interpret? Dr Nikhil Tandon Department of Endocrinology and Metabolism All India Institute of Medical Sciences New Delhi Clinical Utility of Bone Densitometry Diagnosis (DXA)
Breast Cancer and Bone Loss. One in seven women will develop breast cancer during a lifetime
 Breast Cancer and Bone Loss One in seven women will develop breast cancer during a lifetime Causes of Bone Loss in Breast Cancer Patients Aromatase inhibitors Bil Oophorectomy Hypogonadism Steroids Chemotherapy
Breast Cancer and Bone Loss One in seven women will develop breast cancer during a lifetime Causes of Bone Loss in Breast Cancer Patients Aromatase inhibitors Bil Oophorectomy Hypogonadism Steroids Chemotherapy
OSTEOPOROSIS: AN OPPORTUNITY OR OBLIGATION
 OSTEOPOROSIS: AN OPPORTUNITY OR OBLIGATION Debra L. Sietsema, PhD, RN Director, Bone Health Clinical Operations October 5, 2016 OTA NP/PA Course 1 Osteoporosis Definition A skeletal disorder characterized
OSTEOPOROSIS: AN OPPORTUNITY OR OBLIGATION Debra L. Sietsema, PhD, RN Director, Bone Health Clinical Operations October 5, 2016 OTA NP/PA Course 1 Osteoporosis Definition A skeletal disorder characterized
Management of postmenopausal osteoporosis
 Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
Management of postmenopausal osteoporosis Yeap SS, Hew FL, Chan SP, on behalf of the Malaysian Osteoporosis Society Committee Working Group for the Clinical Guidance on the Management of Osteoporosis,
Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment. William D. Leslie, MD MSc FRCPC
 Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment William D. Leslie, MD MSc FRCPC Case #1 Age 53: 3 years post-menopause Has always enjoyed excellent health with
Module 5 - Speaking of Bones Osteoporosis For Health Professionals: Fracture Risk Assessment William D. Leslie, MD MSc FRCPC Case #1 Age 53: 3 years post-menopause Has always enjoyed excellent health with
The Bare Bones of Osteoporosis. Wendy Rosenthal, PharmD
 The Bare Bones of Osteoporosis Wendy Rosenthal, PharmD Definition A systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase
The Bare Bones of Osteoporosis Wendy Rosenthal, PharmD Definition A systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue, with a consequent increase
Download slides:
 Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
Download slides: https://www.tinyurl.com/m67zcnn https://tinyurl.com/kazchbn OSTEOPOROSIS REVIEW AND UPDATE Boca Raton Regional Hospital Internal Medicine Conference 2017 Benjamin Wang, M.D., FRCPC Division
Fragile Bones and how to recognise them. Rod Hughes Consultant physician and rheumatologist St Peter s hospital Chertsey
 Fragile Bones and how to recognise them Rod Hughes Consultant physician and rheumatologist St Peter s hospital Chertsey Osteoporosis Osteoporosis is a skeletal disorder characterised by compromised bone
Fragile Bones and how to recognise them Rod Hughes Consultant physician and rheumatologist St Peter s hospital Chertsey Osteoporosis Osteoporosis is a skeletal disorder characterised by compromised bone
Osteoporosis. Overview
 v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
v2 Osteoporosis Overview Osteoporosis is defined as compromised bone strength that increases risk of fracture (NIH Consensus Conference, 2000). Bone strength is characterized by bone mineral density (BMD)
Clinician s Guide to Prevention and Treatment of Osteoporosis
 Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
Clinician s Guide to Prevention and Treatment of Osteoporosis Published: 15 August 2014 committee of the National Osteoporosis Foundation (NOF) Tipawan khiemsontia,md outline Basic pathophysiology screening
BAD TO THE BONE. Peter Jones, Rheumatologist QE Health, Rotorua. GP CME Conference Rotorua, June 2008
 BAD TO THE BONE Peter Jones, Rheumatologist QE Health, Rotorua GP CME Conference Rotorua, June 2008 Agenda Osteoporosis in Men Vitamin D and Calcium Long-term treatment with Bisphosphonates Pathophysiology
BAD TO THE BONE Peter Jones, Rheumatologist QE Health, Rotorua GP CME Conference Rotorua, June 2008 Agenda Osteoporosis in Men Vitamin D and Calcium Long-term treatment with Bisphosphonates Pathophysiology
Tymlos (abaloparatide)
") Tymlos (abaloparatide) Policy Number: 5.01.638 Last Review: 11/2018 Origination: 10/2017 Next Review: 11/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Tymlos
Tymlos (abaloparatide) Policy Number: 5.01.638 Last Review: 11/2018 Origination: 10/2017 Next Review: 11/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage for Tymlos
ACP Colorado-Evidence Based Management of Osteoporosis
 ACP Colorado-Evidence Based Management of Osteoporosis Micol S. Rothman, MD Associate Professor of Medicine and Radiology Clinical Director Metabolic Bone Program University of Colorado School of Medicine
ACP Colorado-Evidence Based Management of Osteoporosis Micol S. Rothman, MD Associate Professor of Medicine and Radiology Clinical Director Metabolic Bone Program University of Colorado School of Medicine
Page 1. Current and Emerging Strategies for Osteoporosis. Osteoporosis Warm-Up: Which of the Following is True?
 Current and Emerging Strategies for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures Osteoporosis Warm-Up:
Current and Emerging Strategies for Osteoporosis Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures Osteoporosis Warm-Up:
nogg Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK
 nogg NATIONAL OSTEOPOROSIS GUIDELINE GROUP Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK Produced by J Compston, A Cooper,
nogg NATIONAL OSTEOPOROSIS GUIDELINE GROUP Guideline for the diagnosis and management of osteoporosis in postmenopausal women and men from the age of 50 years in the UK Produced by J Compston, A Cooper,
Page 1. Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco What s
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018? Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco What s
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in ? What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018-19? What s New in Osteoporosis The crisis in treatment and compliance Douglas C. Bauer, MD Professor of Medicine and Epidemiology
Diagnosis and Treatment of Osteoporosis: What s New and Controversial in 2018-19? What s New in Osteoporosis The crisis in treatment and compliance Douglas C. Bauer, MD Professor of Medicine and Epidemiology
Page 1. New Developments in Osteoporosis. What s New in Osteoporosis
 New Developments in Osteoporosis Eliseo J. Pérez-Stable MD Professor of Medicine Division of General Internal Medicine Department of Medicine July 4, 2013 Declaration of full disclosure: No conflict of
New Developments in Osteoporosis Eliseo J. Pérez-Stable MD Professor of Medicine Division of General Internal Medicine Department of Medicine July 4, 2013 Declaration of full disclosure: No conflict of
Pharmacy Management Drug Policy
 Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed medical literature generally recognized by the medical community. Guidelines
Clinical criteria used to make utilization review decisions are based on credible scientific evidence published in peer reviewed medical literature generally recognized by the medical community. Guidelines
What is Osteoporosis?
 What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
What is Osteoporosis? 2000 NIH Definition A skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture. Bone strength reflects the integration of
Prevalence of Osteoporosis 5/3/2017. Rhiannon Anderson, PA-C, FLS Linda Mitchell, PA-C, FLS, DEXA Specialist
 Rhiannon Anderson, PA-C, FLS Linda Mitchell, PA-C, FLS, DEXA Specialist Prevalence of Osteoporosis 1.5 million fractures annually in the U.S. Overall lifetime risk for an osteoporotic fracture is about
Rhiannon Anderson, PA-C, FLS Linda Mitchell, PA-C, FLS, DEXA Specialist Prevalence of Osteoporosis 1.5 million fractures annually in the U.S. Overall lifetime risk for an osteoporotic fracture is about
Objectives. Discuss bone health and the consequences of osteoporosis on patients medical and disability status.
 Objectives Discuss bone health and the consequences of osteoporosis on patients medical and disability status. Discuss the pathophysiology of osteoporosis and major risk factors. Assess the major diagnostic
Objectives Discuss bone health and the consequences of osteoporosis on patients medical and disability status. Discuss the pathophysiology of osteoporosis and major risk factors. Assess the major diagnostic
Osteoporosis in Men Wendy Rosenthal PharmD. This program has been brought to you by PharmCon
 Osteoporosis in Men Wendy Rosenthal PharmD This program has been brought to you by PharmCon Osteoporosis in Men Speaker: Dr. Wendy Rosenthal, President of MedOutcomes, will be the presenter for this webcast.
Osteoporosis in Men Wendy Rosenthal PharmD This program has been brought to you by PharmCon Osteoporosis in Men Speaker: Dr. Wendy Rosenthal, President of MedOutcomes, will be the presenter for this webcast.
Current Issues in Osteoporosis
 Current Issues in Osteoporosis California AACE 18TH Annual Meeting & Symposium Marina del Rey, CA September 15, 2018 Michael R. McClung, MD, FACP,FACE Director, Oregon Osteoporosis Center Portland, Oregon,
Current Issues in Osteoporosis California AACE 18TH Annual Meeting & Symposium Marina del Rey, CA September 15, 2018 Michael R. McClung, MD, FACP,FACE Director, Oregon Osteoporosis Center Portland, Oregon,
This Coverage Policy applies to Individual Health Insurance Marketplace benefit plans only.
 This Coverage Policy applies to Individual Health Insurance Marketplace benefit plans only. INJECTABLE OSTEOPOSIS AGENTS SUBJECT Pharmacologic Agents: Bisphosphonates: Boniva IV (ibandronate) Reclast (zoledronic
This Coverage Policy applies to Individual Health Insurance Marketplace benefit plans only. INJECTABLE OSTEOPOSIS AGENTS SUBJECT Pharmacologic Agents: Bisphosphonates: Boniva IV (ibandronate) Reclast (zoledronic
Interpreting DEXA Scan and. the New Fracture Risk. Assessment. Algorithm
 Interpreting DEXA Scan and the New Fracture Risk Assessment Algorithm Prof. Samir Elbadawy *Osteoporosis affect 30%-40% of women in western countries and almost 15% of men after the age of 50 years. Osteoporosis
Interpreting DEXA Scan and the New Fracture Risk Assessment Algorithm Prof. Samir Elbadawy *Osteoporosis affect 30%-40% of women in western countries and almost 15% of men after the age of 50 years. Osteoporosis
Use of DXA / Bone Density in the Care of Your Patients. Brenda Lee Holbert, M.D. Associate Professor Senior Staff Radiologist
 Use of DXA / Bone Density in the Care of Your Patients Brenda Lee Holbert, M.D. Associate Professor Senior Staff Radiologist Important Websites Resources for Clinicians and Patients www.nof.org www.iofbonehealth.org
Use of DXA / Bone Density in the Care of Your Patients Brenda Lee Holbert, M.D. Associate Professor Senior Staff Radiologist Important Websites Resources for Clinicians and Patients www.nof.org www.iofbonehealth.org
AN OVERVIEW of TREATMENT: WHO and WHEN to TREAT
 AN OVERVIEW of TREATMENT: WHO and WHEN to TREAT Dolores Shoback, MD Professor of Medicine, UCSF San Francisco VA Medical Center July 16, 21 ~ QUESTIONS ~ Who should receive therapy to prevent fractures?
AN OVERVIEW of TREATMENT: WHO and WHEN to TREAT Dolores Shoback, MD Professor of Medicine, UCSF San Francisco VA Medical Center July 16, 21 ~ QUESTIONS ~ Who should receive therapy to prevent fractures?
Reducing the Risk of Fracture in Postmenopausal Women: Guidance for Family Physicians. Please complete the preassessment before the session starts.
 Reducing the Risk of Fracture in Postmenopausal Women: Guidance for Family Physicians Please complete the preassessment before the session starts. Sponsorship and Support This educational activity is jointly
Reducing the Risk of Fracture in Postmenopausal Women: Guidance for Family Physicians Please complete the preassessment before the session starts. Sponsorship and Support This educational activity is jointly
Bone Health Update Susan L. Greenspan, MD Professor of Medicine University of Pittsburgh
 Bone Health Update 2018 Susan L. Greenspan, MD Professor of Medicine University of Pittsburgh The Problem 50% women and 20% of men have an osteoporotic fracture after age 50 2 million fractures annually
Bone Health Update 2018 Susan L. Greenspan, MD Professor of Medicine University of Pittsburgh The Problem 50% women and 20% of men have an osteoporotic fracture after age 50 2 million fractures annually
Kristen M. Nebel, DO PENN/ LGHP Geriatrics. Temple Family Medicine Review
 Kristen M. Nebel, DO PENN/ LGHP Geriatrics 10/3/17 Temple Family Medicine Review OBJECTIVES Define Revised 2017 American College of Physician Recommendations Screening, Prevention and Treatment Application
Kristen M. Nebel, DO PENN/ LGHP Geriatrics 10/3/17 Temple Family Medicine Review OBJECTIVES Define Revised 2017 American College of Physician Recommendations Screening, Prevention and Treatment Application
AETNA BETTER HEALTH Prior Authorization guideline for Injectable Osteoporosis Agents
 AETNA BETTER HEALTH Prior Authorization guideline for Injectable Osteoporosis Agents Injectable Osteoporosis Agents Forteo (teriparatide); zoledronic acid Prolia (denosumab)] Authorization guidelines For
AETNA BETTER HEALTH Prior Authorization guideline for Injectable Osteoporosis Agents Injectable Osteoporosis Agents Forteo (teriparatide); zoledronic acid Prolia (denosumab)] Authorization guidelines For
Controversies in Osteoporosis Management
 Controversies in Osteoporosis Management 2018 Northwest Rheumatism Society Meeting Portland, OR April 28, 2018 Michael R. McClung, MD, FACP Director, Oregon Osteoporosis Center Portland, Oregon, USA Institute
Controversies in Osteoporosis Management 2018 Northwest Rheumatism Society Meeting Portland, OR April 28, 2018 Michael R. McClung, MD, FACP Director, Oregon Osteoporosis Center Portland, Oregon, USA Institute
What is Osteoporosis?
 What is Osteoporosis? Systemic skeletal disease characterized by: low bone mass (T-score < -2.5) biochemically normal bone microarchitectural deterioration of bone tissue Hallmark- Increased bone fragility
What is Osteoporosis? Systemic skeletal disease characterized by: low bone mass (T-score < -2.5) biochemically normal bone microarchitectural deterioration of bone tissue Hallmark- Increased bone fragility
Rheumatology. keeping Joints in Motion. Treating and Preventing Fractures
 Rheumatology keeping Joints in Motion Treating and Preventing Fractures Robin K. Dore, MD Clinical Professor of Medicine David Geffen School of Medicine at UCLA, Los Angeles CA Private practice, Tustin
Rheumatology keeping Joints in Motion Treating and Preventing Fractures Robin K. Dore, MD Clinical Professor of Medicine David Geffen School of Medicine at UCLA, Los Angeles CA Private practice, Tustin
Learning Objectives. Controversies in Osteoporosis Prevention and Management. Definition. Presenter Disclosure Information.
 4 4:45 pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
4 4:45 pm Controversies in Osteoporosis Prevention and Management SPEAKER Carolyn Crandall, MD, MS Presenter Disclosure Information The following relationships exist related to this presentation: Carolyn
FRAX Based Lebanese Osteoporosis Guidelines Second Update for Lebanese Guidelines for Osteoporosis Assessment and Treatment
 These guidelines are endorsed by the following Lebanese Scientific Societies and Associations: Lebanese Society of Endocrinology Diabetes and Lipids, Lebanese Society of Rheumatology, Lebanese Society
These guidelines are endorsed by the following Lebanese Scientific Societies and Associations: Lebanese Society of Endocrinology Diabetes and Lipids, Lebanese Society of Rheumatology, Lebanese Society
TYMLOS (abaloparatide)
") TYMLOS (abaloparatide) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
TYMLOS (abaloparatide) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
Updates in Osteoporosis. I have no conflicts of interest. What Would You Do? Mrs. C. What s New in Osteoporosis. Page 1
 Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Updates in Osteoporosis Jeffrey A. Tice, MD Associate Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in
Osteoporosis. Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective. Old Definition of Osteoporosis
 Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective Dr Dicky T.K. Choy Physician Jockey Club Centre for Osteoporosis Care and Control, CUHK Osteoporosis Global public health
Current Trend in Osteoporosis Management for Elderly in HK- Medical Perspective Dr Dicky T.K. Choy Physician Jockey Club Centre for Osteoporosis Care and Control, CUHK Osteoporosis Global public health
Keeping old bones from breaking: The diagnosis, prevention, and treatment of osteoporosis
 Keeping old bones from breaking: The diagnosis, prevention, and treatment of osteoporosis Balanced data about medications www.rxfacts.org Copyright 2010 by The Alosa Foundation. All rights reserved. www.rxfacts.org
Keeping old bones from breaking: The diagnosis, prevention, and treatment of osteoporosis Balanced data about medications www.rxfacts.org Copyright 2010 by The Alosa Foundation. All rights reserved. www.rxfacts.org
Osteoporosis Update. Greg Summers Consultant Rheumatologist
 Osteoporosis Update Greg Summers Consultant Rheumatologist DEFINITION OSTEOPOROSIS is LOW BONE MASS (& micro-architectural deterioration) causing AN INCREASED RISK OF FRACTURE 23 years 82 years 23 y/o
Osteoporosis Update Greg Summers Consultant Rheumatologist DEFINITION OSTEOPOROSIS is LOW BONE MASS (& micro-architectural deterioration) causing AN INCREASED RISK OF FRACTURE 23 years 82 years 23 y/o
Osteoporosis challenges
 Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
Osteoporosis challenges Osteoporosis challenges Who should have a fracture risk assessment? Who to treat? Drugs, holidays and unusual adverse effects Fracture liaison service? The size of the problem 1
Advanced medicine conference. Monday 20 Tuesday 21 June 2016
 Advanced medicine conference Monday 20 Tuesday 21 June 2016 Osteoporosis: recent advances in risk assessment and management Juliet Compston Emeritus Professor of Bone Medicine Cambridge Biomedical Campus
Advanced medicine conference Monday 20 Tuesday 21 June 2016 Osteoporosis: recent advances in risk assessment and management Juliet Compston Emeritus Professor of Bone Medicine Cambridge Biomedical Campus
Skeletal Manifestations
 Skeletal Manifestations of Metabolic Bone Disease Mishaela R. Rubin, MD February 21, 2008 The Three Ages of Women Gustav Klimt 1905 1 Lecture Outline Osteoporosis epidemiology diagnosis secondary causes
Skeletal Manifestations of Metabolic Bone Disease Mishaela R. Rubin, MD February 21, 2008 The Three Ages of Women Gustav Klimt 1905 1 Lecture Outline Osteoporosis epidemiology diagnosis secondary causes
Osteoporosis Update. Case 2. Case 1: Monday morning, 8:15
 Osteoporosis Update Laura E. Ryan, MD Assistant Director for Special Programs Center for Women s Health Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio
Osteoporosis Update Laura E. Ryan, MD Assistant Director for Special Programs Center for Women s Health Clinical Assistant Professor of Medicine Division of Endocrinology, Diabetes and Metabolism The Ohio
2016 AACE/ACE POSTMENOPAUSAL OSTEOPOROSIS GUIDELINES: Practical Applications. Outline. The Process. Osteoporosis Diagnosis NEW CLINICAL DEFINITION
 2016 AACE/ACE POSTMENOPAUSAL OSTEOPOROSIS GUIDELINES: Practical Applications Steven M. Petak MD, JD, MACE, FACP Associate Clinical Professor Weill-Cornell Medical College Division Head and Chief of Endocrinology
2016 AACE/ACE POSTMENOPAUSAL OSTEOPOROSIS GUIDELINES: Practical Applications Steven M. Petak MD, JD, MACE, FACP Associate Clinical Professor Weill-Cornell Medical College Division Head and Chief of Endocrinology
Osteoporosis for the PCP and consultant COPYRIGHT. Harold Rosen, MD Director- Osteoporosis Prevention and Treatment Center
 Osteoporosis for the PCP and consultant Harold Rosen, MD Director- Osteoporosis Prevention and Treatment Center Beth Israel Deaconess Medical Center Potential conflicts of interest None GOALS When to screen/treat?
Osteoporosis for the PCP and consultant Harold Rosen, MD Director- Osteoporosis Prevention and Treatment Center Beth Israel Deaconess Medical Center Potential conflicts of interest None GOALS When to screen/treat?
Healthy Bones: Osteoporosis Management. Laurel Short, MSN, FNP-C
 Healthy Bones: Osteoporosis Management Laurel Short, MSN, FNP-C Disclosure I have no current affiliation or financial interest with any grantor or commercial interests that may have direct interest in
Healthy Bones: Osteoporosis Management Laurel Short, MSN, FNP-C Disclosure I have no current affiliation or financial interest with any grantor or commercial interests that may have direct interest in
Differentiating Pharmacological Therapies for Osteoporosis
 Differentiating Pharmacological Therapies for Osteoporosis Socrates E Papapoulos Department of Endocrinology & Metabolic Diseases Leiden University Medical Center The Netherlands Competing interests: consulting/speaking
Differentiating Pharmacological Therapies for Osteoporosis Socrates E Papapoulos Department of Endocrinology & Metabolic Diseases Leiden University Medical Center The Netherlands Competing interests: consulting/speaking
8/6/2018. Glucocorticoid induced osteoporosis: overlooked and undertreated? Disclosure. Objectives. Overview
 Disclosure Glucocorticoid induced osteoporosis: overlooked and undertreated? I have no financial disclosure relevant to this presentation Tasma Harindhanavudhi, MD Division of Diabetes and Endocrinology
Disclosure Glucocorticoid induced osteoporosis: overlooked and undertreated? I have no financial disclosure relevant to this presentation Tasma Harindhanavudhi, MD Division of Diabetes and Endocrinology
How to treat osteoporosis With what and for how long?
 How to treat osteoporosis With what and for how long? Professor Neil Gittoes Consultant Endocrinologist & Honorary Professor Where will we be going? Drug therapies Current Indications Contraindications/unmet
How to treat osteoporosis With what and for how long? Professor Neil Gittoes Consultant Endocrinologist & Honorary Professor Where will we be going? Drug therapies Current Indications Contraindications/unmet
Tipping the Balance: Strategies for Enhanced Detection and Treatment of Osteoporosis in Primary Care
 Tipping the Balance: Strategies for Enhanced Detection and Treatment of Osteoporosis in Primary Care February 7, 2013 Fort Lauderdale, Florida Educational Partner: Session 5: Tipping the Balance: Strategies
Tipping the Balance: Strategies for Enhanced Detection and Treatment of Osteoporosis in Primary Care February 7, 2013 Fort Lauderdale, Florida Educational Partner: Session 5: Tipping the Balance: Strategies
Men and Osteoporosis So you think that it can t happen to you
 Men and Osteoporosis So you think that it can t happen to you Jonathan D. Adachi MD, FRCPC Alliance for Better Bone Health Chair in Rheumatology Professor, Department of Medicine Michael G. DeGroote School
Men and Osteoporosis So you think that it can t happen to you Jonathan D. Adachi MD, FRCPC Alliance for Better Bone Health Chair in Rheumatology Professor, Department of Medicine Michael G. DeGroote School
Osteoporosis in Men. CME Away India & Sri Lanka March 23 - April 7, 2018
 Osteoporosis in Men CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright 2017
Osteoporosis in Men CME Away India & Sri Lanka March 23 - April 7, 2018 Richard A. Bebb MD, ABIM, FRCPC Consultant Endocrinologist Medical Subspecialty Institute Cleveland Clinic Abu Dhabi Copyright 2017
Page 1. Updates in Osteoporosis. I have no conflicts of interest. What is osteoporosis? What s New in Osteoporosis
 Updates in Osteoporosis Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in Osteoporosis
Updates in Osteoporosis Jeffrey A. Tice, MD Professor of Medicine Division of General Internal Medicine, University of California, San Francisco I have no conflicts of interest What s New in Osteoporosis
Annual Rheumatology & Therapeutics Review for Organizations & Societies
 Annual Rheumatology & Therapeutics Review for Organizations & Societies Osteoporosis in Men: An Update on the Epidemiology, Clinical Evaluation Current Treatments and Treatments in Development Learning
Annual Rheumatology & Therapeutics Review for Organizations & Societies Osteoporosis in Men: An Update on the Epidemiology, Clinical Evaluation Current Treatments and Treatments in Development Learning
2017 Santa Fe Bone Symposium McClung
 217 Santa Fe Bone Symposium Insights into the Use of Anti-remodeling and Anabolic Agents for Osteoporosis Developing a Long-term Management Plan Michael R., MD, FACP Oregon Osteoporosis Center Portland,
217 Santa Fe Bone Symposium Insights into the Use of Anti-remodeling and Anabolic Agents for Osteoporosis Developing a Long-term Management Plan Michael R., MD, FACP Oregon Osteoporosis Center Portland,
Steven W. Ing, M.D., MSCE Assistant Professor of Internal Medicine
 Osteoporosis Steven W. Ing, M.D., MSCE Assistant Professor of Internal Medicine Department of Internal Medicine Division of Endocrinology, Diabetes, & Metabolism Ohio State University Medical Center Case
Osteoporosis Steven W. Ing, M.D., MSCE Assistant Professor of Internal Medicine Department of Internal Medicine Division of Endocrinology, Diabetes, & Metabolism Ohio State University Medical Center Case
Using the FRAX Tool. Osteoporosis Definition
 How long will your bones remain standing? Using the FRAX Tool Gary Salzman M.D. Director Banner Good Samaritan/ Hayden VAMC Internal Medicine Geriatric Fellowship Program Phoenix, Arizona Using the FRAX
How long will your bones remain standing? Using the FRAX Tool Gary Salzman M.D. Director Banner Good Samaritan/ Hayden VAMC Internal Medicine Geriatric Fellowship Program Phoenix, Arizona Using the FRAX
Osteoporosis update. Dr. Claire Vandevelde Consultant Rheumatologist, LTHT
 Osteoporosis update Dr. Claire Vandevelde Consultant Rheumatologist, LTHT Outline Background BMD Tools for assessing fracture risk Case study Denosumab Treatment breaks BMD BMD predicts fracture risk but
Osteoporosis update Dr. Claire Vandevelde Consultant Rheumatologist, LTHT Outline Background BMD Tools for assessing fracture risk Case study Denosumab Treatment breaks BMD BMD predicts fracture risk but
Hot Topics in Osteoporosis and Fracture Prevention
 Hot Topics in Osteoporosis and Fracture Prevention Sid Feldman, MD CCFP (COE) FCFP Sandra Kim, MD, FRCPC November 15, 2018 Family Medicine Forum, Toronto Faculty/Presenter Disclosure Faculty: Sid Feldman
Hot Topics in Osteoporosis and Fracture Prevention Sid Feldman, MD CCFP (COE) FCFP Sandra Kim, MD, FRCPC November 15, 2018 Family Medicine Forum, Toronto Faculty/Presenter Disclosure Faculty: Sid Feldman
Treatments for Osteoporosis Expected Benefits, Potential Harms and Drug Holidays. Suzanne Morin MD FRCP FACP McGill University May 2014
 Treatments for Osteoporosis Expected Benefits, Potential Harms and Drug Holidays Suzanne Morin MD FRCP FACP McGill University May 2014 Learning Objectives Overview of osteoporosis management Outline efficacy
Treatments for Osteoporosis Expected Benefits, Potential Harms and Drug Holidays Suzanne Morin MD FRCP FACP McGill University May 2014 Learning Objectives Overview of osteoporosis management Outline efficacy
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT
 NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
NEW DEVELOPMENTS IN OSTEOPOROSIS: SCREENING, PREVENTION AND TREATMENT Judith Walsh, MD, MPH Departments of Medicine and Epidemiology and Biostatistics UCSF OSTEOPOROSIS: OVERVIEW Definitions Risk factors
July 2012 CME (35 minutes) 7/12/2016
 7/12/2016") Financial Disclosures Epidemiology and Consequences of Fractures Advisory Board: Amgen Janssen Pharmaceuticals Inc. Ann V. Schwartz, PhD Department of Epidemiology and Biostatistics UCSF Outline Osteoporotic
Financial Disclosures Epidemiology and Consequences of Fractures Advisory Board: Amgen Janssen Pharmaceuticals Inc. Ann V. Schwartz, PhD Department of Epidemiology and Biostatistics UCSF Outline Osteoporotic
Page 1. Osteoporosis Warm-Up: Which of the Following is True? Diagnosis and Treatment of Osteoporosis: What is New in What s New in Osteoporosis
 Diagnosis and Treatment of Osteoporosis: What is New in 2017 Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures Osteoporosis
Diagnosis and Treatment of Osteoporosis: What is New in 2017 Douglas C. Bauer, MD Professor of Medicine and Epidemiology & Biostatistics University of California, San Francisco No Disclosures Osteoporosis
NAMS Practice Pearl. Use of Drug Holidays in Women Taking Bisphosphonates. Released April 1, 2013
 NAMS Practice Pearl Use of Drug Holidays in Women Taking Bisphosphonates Released April 1, 2013 Dima L. Diab, MD 1, and Nelson B. Watts, MD 2 ( 1 Cincinnati VA Medical Center, Cincinnati, OH, 2 Mercy Health
NAMS Practice Pearl Use of Drug Holidays in Women Taking Bisphosphonates Released April 1, 2013 Dima L. Diab, MD 1, and Nelson B. Watts, MD 2 ( 1 Cincinnati VA Medical Center, Cincinnati, OH, 2 Mercy Health
Parathyroid Hormone Analogs
 Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.36 Subject: Parathyroid Hormone Analogs Page: 1 of 6 Last Review Date: September 15, 2017 Parathyroid
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.36 Subject: Parathyroid Hormone Analogs Page: 1 of 6 Last Review Date: September 15, 2017 Parathyroid