Intercepting PAD. Playbook for Cardiovascular Care 2018 February 24, Jonathan D Woody, MD, FACS. University Surgical Vascular
|
|
|
- Colin Wheeler
- 5 years ago
- Views:
Transcription
1 Intercepting PAD Playbook for Cardiovascular Care 2018 February 24, 2018 Jonathan D Woody, MD, FACS University Surgical Vascular Attending Vascular Surgeon - Piedmont Athens Regional Adjunct Clinical Associate Professor Faculty of Medical Sciences College of Public Health University of Georgia

2 2 nd and 26
3 Disclosure I have no relevant financial disclosures
4 Outline Definition Risk Factors Diagnosis Treatment Claudication (IC) Critical Limb Ischemia (CLI) Acute Ischemia Summary Quiz
5 What is PAD Peripheral Arterial Disease Atherosclerosis of the peripheral arterial system Most commonly lower extremities Rule of Three for PAD Symptoms Claudication Rest Pain Tissue Loss

6 Society for Vascular Surgery Practice Guidelines for Atherosclerotic Occlusive Disease of the Lower Extremities: Management of Asymptomatic Disease and Claudication Journal of Vascular Surgery March 2016 Supplement Volume 61, Issue 3, p 1S-74S
7 Intermittent Claudication Exercise induced discomfort in a specific muscle group Relieved by rest Consistent and reproducible Typically involves calf, may affect any leg muscle group thigh / buttock Caused by arterial obstruction proximal to affected muscle bed Leads to transient muscle ischemia On demand ischemic muscle pain Angina of the leg
8 Grades of Recommendation Assessment, Development, and Evaluation (GRADE) Grade the Strength of Recommendations & to Rate the Quality of Evidence (confidence in the estimates) Grade 1 (strong) or Grade 2 (weak) Grade 1: Benefit Clearly Outweighs Risk Grade 2: Benefits and Risks Are More Closely Matched Level of Evidence: A (high quality), B (moderate quality), and C (low quality)
9 Epidemiology and Risk Factors
10 Patients with PAD 8 to 12 million Americans are affected by PAD Prevalence of PAD is expected to increase in the U.S. and worldwide as the population ages, cigarette smoking persists, and the epidemic of diabetes mellitus, hypertension, and obesity grows
11 Risk Factors for PAD Reduced Increased Smoking Diabetes Hypertension Hypercholesterolemia Hyperhomocysteinemia C-Reactive Protein Relative Risk Hirsch AT, et al. J Am Coll Cardiol. 2006;47:e1-e192.
12 Patients at Increased Risk of PAD Age 65 Age with risk factors for atherosclerosis (e.g., diabetes mellitus, history of smoking, hyperlipidemia, hypertension) or family history of PAD Age < 50 with diabetes mellitus and 1 additional risk factor for atherosclerosis Individuals with known atherosclerotic disease in another vascular bed (e.g., coronary, carotid, subclavian, renal, mesenteric artery stenosis, or AAA)
13 Rarely progresses to CLI High risk of M&M Society for Vascular Surgery practice guidelines for atherosclerotic occlusive disease of the lower extremities: Management of asymptomatic disease and claudication Conte, Michael S. et al. Journal of Vascular Surgery, Volume 61, Issue 3, 2S - 41S.e1
14 Diagnosis

15 The First Tool to Establish the PAD Diagnosis: A Standardized Physical Examination Pulses should be assessed and recorded When all else fails, examine the patient
16 Vascular Examination Most sensitive tool for pulse exam is WNL = we never looked Only contraindication to pulse exam is absence of a finger
17 History and/or Physical Examination Findings Suggestive of PAD History Claudication Non joint-related exertional lower extremity symptoms Impaired walking function Ischemic rest pain Physical Examination Abnormal lower extremity pulse examination Nonhealing lower extremity wound Lower extremity gangrene Other suggestive lower extremity physical findings (e.g., elevation pallor/dependent rubor)
18 Diagnosis of Peripheral Arterial Disease (PAD) Recommendation Grade LOE 2.1. We recommend using the ABI as the first-line noninvasive test to establish a diagnosis of PAD in individuals with symptoms or signs suggestive of disease. When the ABI is borderline or normal (>0.9) and symptoms of claudication are suggestive, we recommend an exercise ABI We suggest against routine screening for lower extremity PAD in the absence of risk factors, history, signs, or symptoms of PAD For asymptomatic individuals who are at elevated risk, such as those aged >70, smokers, diabetic patients, those with an abnormal pulse examination, or other established cardiovascular disease, screening for lower extremity PAD is reasonable if used to improve risk stratification, preventive care, and medical management. 1 A 2 C 2 C 2.4. In symptomatic patients who are being considered for revascularization, we suggest using physiologic noninvasive studies, such as segmental pressures and pulse volume recordings, to aid in the quantification of arterial insufficiency and help localize the level of obstruction In symptomatic patients in whom revascularization treatment is being considered, we recommend anatomic imaging studies, such as arterial duplex ultrasound, CTA, MRA, and contrast arteriography. 2 C 1 B ABI, Ankle-brachial index; CTA, computed tomography angiography; MRA, magnetic resonance angiography; LOE, Level of Evidence.
19 Ankle Brachial Index ABI no symptoms claudication < 0.4 rest pain, ulceration, gangrene ABI = % of normal blood flow

20 Segmental Pressures (mm Hg) 150 Brachial ABI 0.44

21 Pulse Volume Recordings
22 Management of Asymptomatic Patients with PAD
23 Management of Asymptomatic Disease Recommendation Grade LOE 3.1. We recommend multidisciplinary comprehensive smoking cessation interventions for patients with asymptomatic PAD who use tobacco (repeatedly until tobacco use has stopped). 1 A 3.2. We recommend providing education about the signs and symptoms of PAD progression to asymptomatic patients with PAD We recommend against invasive treatments for PAD in the absence of symptoms, regardless of hemodynamic measures or imaging findings demonstrating PAD. 1 Ungraded 1 B PAD, Peripheral arterial disease; LOE, Level of Evidence.
24 Medical / Non-Interventional Management of the Patient with IC
25 Medical Treatment for Intermittent Claudication (IC) Recommendation Grade LOE 4.1. We recommend multidisciplinary comprehensive smoking cessation interventions 1 A for patients with IC (repeatedly until tobacco use has stopped) We recommend statin therapy in patients with symptomatic PAD. 1 A 4.3. We recommend optimizing diabetes control (hemoglobin A1c goal of <7.0%) in 1 B patients with IC if this goal can be achieved without hypoglycemia We recommend the use of indicated β-blockers (eg, for hypertension, cardiac 1 B indications) in patients with IC. There is no evidence supporting concerns about worsening claudication symptoms In patients with IC due to atherosclerosis, we recommend antiplatelet therapy with 1 A aspirin ( mg daily) We recommend clopidogrel in doses of 75 mg daily as an effective alternative to 1 B aspirin for antiplatelet therapy in patients with IC In patients with IC due to atherosclerosis, we suggest against using warfarin for the 1 C sole indication of reducing the risk of adverse cardiovascular events or vascular occlusions We suggest against using folic acid and vitamin B12 supplements as a treatment of 2 C IC In patients with IC who do not have congestive heart failure, we suggest a 3- month 2 A trial of cilostazol (100 mg twice daily) to improve pain-free walking In patients with IC who cannot tolerate or have contraindications for cilostazol, we suggest a trial of pentoxifylline (400 mg thrice daily) to improve pain-free walking. 2 B ACEI, Angiotensin-converting enzyme inhibitor; PAD, Peripheral arterial disease; LOE, Level of Evidence.
26 Cilostazol, Pentoxifylline, and Chelation Therapy COR LOE Recommendations Cilostazol I A Cilostazol is an effective therapy to improve symptoms and increase walking distance in patients with claudication. Pentoxifylline III: No Pentoxifylline is not effective for treatment of B-R Benefit claudication. Chelation Therapy III: No Chelation therapy (e.g., ethylenediaminetetraacetic B-R Benefit acid) is not beneficial for treatment of claudication.
27 Exercise Therapy Recommendation Grade LOE We recommend as first-line therapy a supervised exercise program consisting of walking a minimum of three times per week (30-60 min/session) for at least 12 weeks to all suitable patients with IC We recommend home-based exercise, with a goal of at least 30 minutes of walking three to five times per week when a supervised exercise program is unavailable or for long-term benefit after a supervised exercise program is completed In patients who have undergone revascularization therapy for IC, we recommend exercise (either supervised or home based) for adjunctive functional benefits We recommend that patients with IC be followed up annually to assess compliance with lifestyle measures (smoking cessation, exercise) and medical therapies as well as to determine if there is evidence of progression in symptoms or signs of PAD. Yearly ABI testing may be of value to provide objective evidence of disease progression. 1 A 1 B 1 B 1 C ABI, Ankle-brachial index; IC, intermittent claudication; PAD, peripheral arterial disease; LOE, Level of Evidence.
28 Change in Treadmill Walking Distance (%) Effects of Exercise Training on Claudication Meta-analysis of 21 Studies * * Exercise Training Control 20 0 Onset of Claudication Pain Maximal Claudication Pain * P < 0.05 Gardner AW, Poehlman ET. JAMA. 1995;274:
29 The Role of Revascularization for IC
30 Rule of Three Revascularization 1. Endovascular 2. Endarterectomy 3. Bypass

31 Angioplasty / Stenting

32

33

34

35 Open Surgery
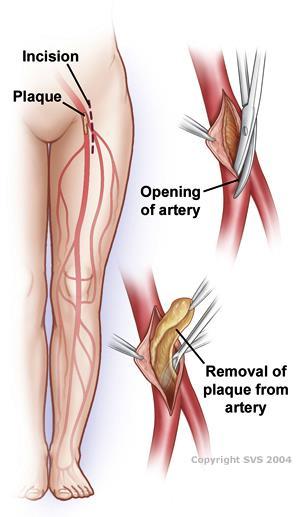
36 Endarterectomy

37 Endarterectomy

38 Bypass

39 Bypass

40 Aortobifemoral Bypass
41 General Considerations on Invasive Treatment for Intermittent Claudication (IC) Recommendation Grade LOE 5.1. We recommend EVT or surgical treatment of IC for patients with significant functional or lifestyle-limiting disability when there is a reasonable likelihood of symptomatic improvement with treatment, when pharmacologic or exercise therapy, or both, have failed, and when the benefits of treatment outweigh the potential risks We recommend an individualized approach to select an invasive treatment for IC. The modality offered should provide a reasonable likelihood of sustained benefit to the patient (>50% likelihood of clinical efficacy for at least 2 years). For revascularization, anatomic patency (freedom from hemodynamically significant restenosis) is considered a prerequisite for sustained efficacy. 1 B 1 C EVT, Endovascular therapy; LOE, Level of Evidence.
42 Interventions for Aortoiliac Occlusive Disease (AIOD) in Intermittent Claudication (IC) (Part 1) Recommendation Grade LOE 5.3. We recommend endovascular procedures over open surgery for focal AIOD causing IC. 1 B 5.4. We recommend endovascular interventions as first-line revascularization therapy for most patients with common iliac artery or external iliac artery occlusive disease causing IC We recommend the selective use of BMS or covered stents for aortoiliac angioplasty for common iliac artery or external iliac artery occlusive disease, or both, due to improved technical success and patency We recommend the use of covered stents for treatment of AIOD in the presence of severe calcification or aneurysmal changes where the risk of rupture may be increased after unprotected dilation For patients with diffuse AIOD (eg, extensive aortic disease, disease involving both common and external iliac arteries) undergoing revascularization, we suggest either endovascular or surgical intervention as first-line approaches. Endovascular interventions that may impair the potential for subsequent AFB in surgical candidates should be avoided EVT of AIOD in the presence of aneurysmal disease should be undertaken cautiously. We recommend that the modality used should either achieve concomitant aneurysm exclusion or should not jeopardize the conduct of any future open or endovascular aneurysm repair In all patients undergoing revascularization for AIOD, we recommend assessing the CFA. If hemodynamically significant CFA disease is present, we recommend surgical therapy (endarterectomy) as first-line treatment. 1 B 1 B 1 C 2 B 1 C 1 B BMS, Bare-metal stent; CFA, common femoral artery; CT, computed tomography; EVT, endovascular therapy; LOE, Level of Evidence.
43 Interventions for Aortoiliac Occlusive Disease (AIOD) in Intermittent Claudication (IC) - (Part 2) Recommendation Grade LOE In patients with iliac artery disease and involvement of the CFA, we recommend hybrid procedures combining femoral endarterectomy with iliac inflow correction We recommend direct surgical reconstruction (bypass, endarterectomy) in patients with reasonable surgical risk and diffuse AIOD not amenable to an endovascular approach, after one or more failed attempts at EVT, or in patients with combined occlusive and aneurysmal disease In younger patients (age <50 years) with IC, we recommend a shared decisionmaking approach to engage patients and inform them of the possibility of inferior outcomes with either endovascular or surgical interventions We recommend either axial imaging (eg, CT, MR) or catheter-based angiography for evaluation and planning of surgical revascularization for AIOD. 1 B 1 B 2 C 1 Ungraded When performing surgical bypass for aortoiliac disease, concomitant aneurysmal disease of the aorta or iliac arteries should be treated as appropriate (exclusion) and is a contraindication to end-to-side proximal anastomoses. 1 Ungraded For any bypass graft originating from the CFA, the donor iliac artery must be free of hemodynamically significant disease or any pre-existing disease should be corrected before performing the bypass graft. 1 Ungraded BMS, Bare-metal stent; CFA, common femoral artery; CT, computed tomography; EVT, endovascular therapy; LOE, Level of Evidence.
44 Intervention for Femoropopliteal Occlusive Disease (FPOD) in Intermittent Claudication (IC) Recommendation Grade LOE We recommend endovascular procedures over open surgery for focal occlusive disease of the SFA artery not involving the origin at the femoral bifurcation For focal lesions (<5 cm) in the SFA that have unsatisfactory technical results with balloon angioplasty, we suggest selective stenting For intermediate-length lesions (5-15 cm) in the SFA, we recommend the adjunctive use of self expanding nitinol stents (with or without paclitaxel) to improve the midterm patency of angioplasty We suggest the use of preoperative ultrasound vein mapping to establish the availability and quality of autogenous vein conduit in patients being considered for infrainguinal bypass for the treatment of IC We recommend against EVT of isolated infrapopliteal disease for IC because this treatment is of unproven benefit and possibly harmful We recommend surgical bypass as an initial revascularization strategy for patients with diffuse FP disease, small caliber (<5 mm), or extensive calcification of the SFA, if they have favorable anatomy for bypass (popliteal artery target, good runoff) and have average or low operative risk We recommend using the saphenous vein as the preferred conduit for infrainguinal bypass grafts In the absence of suitable vein, we suggest using prosthetic conduit for FP bypass in claudicant patients, if the above-knee popliteal artery is the target vessel and good runoff is present. 1 C 2 C 1 B 2 C 1 C 1 B 1 A 2 C EVT, Endovascular therapy; SFA, superficial femoral artery; LOE, Level of Evidence.
45 Postinterventional medical therapy in Intermittent Claudication (IC) Recommendation Grade LOE In all patients after endovascular or open surgical intervention for claudication, we recommend optimal medical therapy (antiplatelets agents, statins, antihypertensives, control of glycemia, smoking cessation). 1 A In patients undergoing lower extremity bypass (venous or prosthetic), we suggest treatment with antiplatelet therapy (aspirin, clopidogrel, or aspirin plus clopidogrel) In patients undergoing infrainguinal endovascular intervention for claudication, we suggest treatment with aspirin and clopidogrel for at least 30 days. 2 B 2 B LOE, Level of Evidence.

46 Which Treatment is Best


47 Patient Preference
48 Treatment Open vs Endo Clinical guidelines remain vague regarding indications for and appropriate use of revascularization strategies Ultimately, clinicians must weigh risks and benefits in determining which patients have the greatest chance for success with revascularization
49 Surveillance After Revascularization for IC




50 PAD Surveillance
51 Surveillance After Revascularization for Intermittent Claudication (IC) Recommendation Grade LOE 6.1. We suggest that patients treated with open or endovascular interventions for IC be monitored with a clinical surveillance program that consists of an interval history to detect new symptoms, ensure compliance with medical therapies, record subjective functional improvements, pulse examination, and measurement of resting and, if possible, post exercise ABIs We suggest that patients treated with lower extremity vein grafts for IC be monitored with a surveillance program that consists of clinical follow-up and duplex scanning 2 C 2 C 6.3. We suggest that patients who have previously undergone vein bypass surgery for IC and have developed a significant graft stenosis on DUS be considered for prophylactic reintervention (open or endovascular) to promote long-term bypass graft patency 1 C ABI, Ankle-brachial index; DUS, duplex ultrasound; LOE, Level of Evidence.
52 Critical Limb Ischemia
53 Critical Limb Ischemia Rest Pain Tissue Loss CLI is BAD Severe ischemia Continuous pain Dependent rubor Gangrene spontaneous necrosis of severely ischemic tissue Non healing wound Infection


54 Critical Limb Ischemia Non-healing wound Gangrene


55 Wound, Ischemia, Foot Infection WIFI Classification
56 Critical Limb Ischemia (CLI) Fate of Patients With CLI After Initial Treatment Summary of 6-month outcomes from 19 studies Alive with amputation 35% Dead 20% Alive without amputation 45% CLI is bad Dormandy JA, Rutherford RB. J Vasc Surg. 2000;31:S1-S296.

57 Don t Wait Until It s Too Late
58 Acute Ischemia
59 The 6 Ps of Acute Ischemia Pulselessness Pain Pallor Poikilothermia Paresthesia Paralysis EMERGENCY
60 Remember This
61 Take Home Message PAD is manifestation of systemic atherosclerosis - confers higher risk of MI, stroke, death Aggressive risk factor modification Exercise program Claudication rarely progresses to amputation Intervention for appropriate patients Minimally invasive is maximally preferred Old fashioned surgery is still the gold standard Surveillance is mandatory Critical Limb Ischemia is BAD Acute ischemia is BAD You can t diagnose it if you don t think of it Treat your PAD patient ALL IN save a limb, save a life!!!
62 Quiz Time


63 Real News or Fake News
64 Smoking Diabetes Hyperlipidemia Hypertension Cancer Risk Factors for PAD

65 Smoking Diabetes Hyperlipidemia Hypertension Cancer Risk Factors for PAD
66 Symptoms of PAD Claudication Rest pain Tissue Loss Leg swelling

67 Claudication Rest pain Tissue Loss Leg swelling Symptoms of PAD
68 Treatment of PAD Smoking cessation Risk factor modification Anti-platelet therapy Exercise program Endovascular procedure Open surgery


69 Treatment of PAD Smoking cessation Risk factor modification Anti-platelet therapy Exercise program Endovascular procedure Open surgery




70 Medal Ceremony





71 UNC University of National Champions 1957, 1982, 1993, 2005, 2009, 2017
Introduction. Risk factors of PVD 5/8/2017
 PATHOPHYSIOLOGY AND CLINICAL FEATURES OF PERIPHERAL VASCULAR DISEASE Dr. Muhamad Zabidi Ahmad Radiologist and Section Chief, Radiology, Oncology and Nuclear Medicine Section, Advanced Medical and Dental
PATHOPHYSIOLOGY AND CLINICAL FEATURES OF PERIPHERAL VASCULAR DISEASE Dr. Muhamad Zabidi Ahmad Radiologist and Section Chief, Radiology, Oncology and Nuclear Medicine Section, Advanced Medical and Dental
Imaging Strategy For Claudication
 Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
Guidelines for Management of Peripheral Arterial Disease
 Guidelines for Management of Peripheral Arterial Disease Subhash Banerjee, MD, FACC, FSCAI Professor of Medicine, Univ. of Texas Southwestern Medical Center Chief, Division of Cardiology, VA North Texas
Guidelines for Management of Peripheral Arterial Disease Subhash Banerjee, MD, FACC, FSCAI Professor of Medicine, Univ. of Texas Southwestern Medical Center Chief, Division of Cardiology, VA North Texas
Peripheral Arterial Disease (PAD): Presentation, Diagnosis, and Treatment
: Presentation, Diagnosis, and Treatment") Peripheral Arterial Disease (PAD): Presentation, Diagnosis, and Treatment Prepared and Presented by Jon Manocchio, Pharm D Blanchard Valley Hospital October 2011 Introduction PAD is a condition that is
Peripheral Arterial Disease (PAD): Presentation, Diagnosis, and Treatment Prepared and Presented by Jon Manocchio, Pharm D Blanchard Valley Hospital October 2011 Introduction PAD is a condition that is
Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI?
 Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI? Peter F. Lawrence, M.D. Gonda Vascular Center Division of Vascular Surgery
Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI? Peter F. Lawrence, M.D. Gonda Vascular Center Division of Vascular Surgery
Recommendations for Follow-up After Vascular Surgery Arterial Procedures SVS Practice Guidelines
 Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division
 John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
Garland Green, MD Interventional Cardiologist. Impact of PAD: Prevalence, Risk Factors, Testing, and Medical Management
 Garland Green, MD Interventional Cardiologist Impact of PAD: Prevalence, Risk Factors, Testing, and Medical Management Peripheral Arterial Disease Affects over 8 million Americans Affects 12% of the general
Garland Green, MD Interventional Cardiologist Impact of PAD: Prevalence, Risk Factors, Testing, and Medical Management Peripheral Arterial Disease Affects over 8 million Americans Affects 12% of the general
PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014
 PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014 Van Crisco, MD, FACC, FSCAI First Coast Heart and Vascular Center, PLLC Jacksonville, FL 678-313-6695 Conflict of Interest Bayer Healthcare
PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014 Van Crisco, MD, FACC, FSCAI First Coast Heart and Vascular Center, PLLC Jacksonville, FL 678-313-6695 Conflict of Interest Bayer Healthcare
Evidence-Based Optimal Treatment for SFA Disease
 Evidence-Based Optimal Treatment for SFA Disease Endo first Don t burn surgical bridge Don t stent if possible Javairiah Fatima, MD Assistant Professor of Surgery Division of Vascular and Endovascular
Evidence-Based Optimal Treatment for SFA Disease Endo first Don t burn surgical bridge Don t stent if possible Javairiah Fatima, MD Assistant Professor of Surgery Division of Vascular and Endovascular
Peripheral Vascular Disease
 Peripheral artery disease (PAD) results from the buildup of plaque (atherosclerosis) in the arteries of the legs. For people with PAD, symptoms may be mild, requiring no treatment except modification of
Peripheral artery disease (PAD) results from the buildup of plaque (atherosclerosis) in the arteries of the legs. For people with PAD, symptoms may be mild, requiring no treatment except modification of
The Struggle to Manage Stroke, Aneurysm and PAD
 The Struggle to Manage Stroke, Aneurysm and PAD In this article, Dr. Salvian examines the management of peripheral arterial disease, aortic aneurysmal disease and cerebrovascular disease from symptomatology
The Struggle to Manage Stroke, Aneurysm and PAD In this article, Dr. Salvian examines the management of peripheral arterial disease, aortic aneurysmal disease and cerebrovascular disease from symptomatology
Objectives. Abdominal Aortic Aneuryms 11/16/2017. The Vascular Patient: Diagnosis and Conservative Treatment
 The Vascular Patient: Diagnosis and Conservative Treatment Ferrell-Duncan Clinic Zachary C. Schmittling, M.D., F.A.C.S. Vascular and General Surgery Ferrell-Duncan Clinic Cox Health Systems Objectives
The Vascular Patient: Diagnosis and Conservative Treatment Ferrell-Duncan Clinic Zachary C. Schmittling, M.D., F.A.C.S. Vascular and General Surgery Ferrell-Duncan Clinic Cox Health Systems Objectives
Role of ABI in Detecting and Quantifying Peripheral Arterial Disease
 Role of ABI in Detecting and Quantifying Peripheral Arterial Disease Difference in AAA size between US and Surgeon 2 1 0-1 -2-3 0 1 2 3 4 5 6 7 Mean AAA size between US and Surgeon Kathleen G. Raman MD,
Role of ABI in Detecting and Quantifying Peripheral Arterial Disease Difference in AAA size between US and Surgeon 2 1 0-1 -2-3 0 1 2 3 4 5 6 7 Mean AAA size between US and Surgeon Kathleen G. Raman MD,
Introduction to Peripheral Arterial Disease. Stacey Clegg, MD Interventional Cardiology August
 Introduction to Peripheral Arterial Disease Stacey Clegg, MD Interventional Cardiology August 20 2014 Outline (and for the ABIM board exam * ** ***) Prevalence* Definitions Lower Extremity: Aorta*** Claudication***
Introduction to Peripheral Arterial Disease Stacey Clegg, MD Interventional Cardiology August 20 2014 Outline (and for the ABIM board exam * ** ***) Prevalence* Definitions Lower Extremity: Aorta*** Claudication***
Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia
 Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia Albeir Mousa, MD., FACS.,MPH., MBA Professor of Vascular and Endovascular Surgery West Virginia University Disclosure None What you
Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia Albeir Mousa, MD., FACS.,MPH., MBA Professor of Vascular and Endovascular Surgery West Virginia University Disclosure None What you
Treatment Strategies For Patients with Peripheral Artery Disease
 Treatment Strategies For Patients with Peripheral Artery Disease Presented by Schuyler Jones, MD Duke University Medical Center & Duke Clinical Research Institute AHRQ Comparative Effectiveness Review
Treatment Strategies For Patients with Peripheral Artery Disease Presented by Schuyler Jones, MD Duke University Medical Center & Duke Clinical Research Institute AHRQ Comparative Effectiveness Review
Hypothesis: When compared to conventional balloon angioplasty, cryoplasty post-dilation decreases the risk of SFA nses in-stent restenosis
 Cryoplasty or Conventional Balloon Post-dilation of Nitinol Stents For Revascularization of Peripheral Arterial Segments Background: Diabetes mellitus is associated with increased risk of in-stent restenosis
Cryoplasty or Conventional Balloon Post-dilation of Nitinol Stents For Revascularization of Peripheral Arterial Segments Background: Diabetes mellitus is associated with increased risk of in-stent restenosis
Practical Point in Diabetic Foot Care 3-4 July 2017
 Diabetic Foot Ulcer : Role of Vascular Surgeon Practical Point in Diabetic Foot Care 3-4 July 2017 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai University
Diabetic Foot Ulcer : Role of Vascular Surgeon Practical Point in Diabetic Foot Care 3-4 July 2017 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai University
Imaging for Peripheral Vascular Disease
 Imaging for Peripheral Vascular Disease James G. Jollis, MD Director, Rex Hospital Cardiovascular Imaging Imaging for Peripheral Vascular Disease 54 year old male with exertional calf pain in his right
Imaging for Peripheral Vascular Disease James G. Jollis, MD Director, Rex Hospital Cardiovascular Imaging Imaging for Peripheral Vascular Disease 54 year old male with exertional calf pain in his right
Diagnosis and Endovascular Treatment of Critical Limb Ischemia: What You Need to Know S. Jay Mathews, MD, MS, FACC
 Diagnosis and Endovascular Treatment of Critical Limb Ischemia: What You Need to Know S. Jay Mathews, MD, MS, FACC Interventional Cardiologist/Endovascular Specialist Bradenton Cardiology Center Bradenton,
Diagnosis and Endovascular Treatment of Critical Limb Ischemia: What You Need to Know S. Jay Mathews, MD, MS, FACC Interventional Cardiologist/Endovascular Specialist Bradenton Cardiology Center Bradenton,
Larry Diaz, MD, FSCAI Mehdi H. Shishehbor, DO, FSCAI
 PAD Diagnosis Larry Diaz, MD, FSCAI Metro Health / University of Michigan Health, Wyoming, MI Mehdi H. Shishehbor, DO, FSCAI University Hospitals Harrington Heart & Vascular Institute, Cleveland, OH PAD:
PAD Diagnosis Larry Diaz, MD, FSCAI Metro Health / University of Michigan Health, Wyoming, MI Mehdi H. Shishehbor, DO, FSCAI University Hospitals Harrington Heart & Vascular Institute, Cleveland, OH PAD:
Peripheral arterial disease for primary care Ed Aboian, MD
 Peripheral arterial disease for primary care Ed Aboian, MD Division of Vascular and Endovascular Surgery Palo Alto Medical Foundation, Burlingame Ca Disclosures Nothing to disclose Clinical presentation
Peripheral arterial disease for primary care Ed Aboian, MD Division of Vascular and Endovascular Surgery Palo Alto Medical Foundation, Burlingame Ca Disclosures Nothing to disclose Clinical presentation
Guidelines for Ultrasound Surveillance
 Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
Guidelines for Ultrasound Surveillance Carotid & Lower Extremity by Ian Hamilton, Jr, MD, MBA, RPVI, FACS Corporate Medical Director BlueCross BlueShield of Tennessee guidelines for ultrasound surveillance
Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE)
") Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE) Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University Health System,
Comparison Of Primary Long Stenting Versus Primary Short Stenting For Long Femoropopliteal Artery Disease (PARADE) Young-Guk Ko, M.D. Severance Cardiovascular Hospital, Yonsei University Health System,
Index. cardiology.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ABI. See Ankle-brachial index (ABI). Afterload, deconstructing of, in ventricular vascular interaction in heart failure, 449 Air plethysmography
Index Note: Page numbers of article titles are in boldface type. A ABI. See Ankle-brachial index (ABI). Afterload, deconstructing of, in ventricular vascular interaction in heart failure, 449 Air plethysmography
Peripheral Arterial Disease: Who has it and what to do about it?
 Peripheral Arterial Disease: Who has it and what to do about it? Seth Krauss, M.D. Alaska Annual Nurse Practitioner Conference September 16, 2011 Scope of the Problem Incidence: 20%
Peripheral Arterial Disease: Who has it and what to do about it? Seth Krauss, M.D. Alaska Annual Nurse Practitioner Conference September 16, 2011 Scope of the Problem Incidence: 20%
John E. Campbell, MD. Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division
 John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
Current Vascular and Endovascular Management in Diabetic Vasculopathy
 Current Vascular and Endovascular Management in Diabetic Vasculopathy Yang-Jin Park Associate professor Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine Peripheral artery
Current Vascular and Endovascular Management in Diabetic Vasculopathy Yang-Jin Park Associate professor Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine Peripheral artery
Surgical Options for revascularisation P E T E R S U B R A M A N I A M
 Surgical Options for revascularisation P E T E R S U B R A M A N I A M The goal Treat pain Heal ulcer Preserve limb Preserve life The options Conservative Endovascular Surgical bypass Primary amputation
Surgical Options for revascularisation P E T E R S U B R A M A N I A M The goal Treat pain Heal ulcer Preserve limb Preserve life The options Conservative Endovascular Surgical bypass Primary amputation
Steven Hadesman, MD Chief Medical Officer, MeridianRx Internal Medicine Physician, St. John Hospital
 Steven Hadesman, MD Chief Medical Officer, MeridianRx Internal Medicine Physician, St. John Hospital Deep Venous Thrombosis Varicose Veins Venous insufficiency Phlebitis Lymphedema Elephantiasis nostras
Steven Hadesman, MD Chief Medical Officer, MeridianRx Internal Medicine Physician, St. John Hospital Deep Venous Thrombosis Varicose Veins Venous insufficiency Phlebitis Lymphedema Elephantiasis nostras
Peripheral Arterial Disease Extremity
 Peripheral Arterial Disease Lower Extremity 05 Contributor Dr Steven Chong Advisors Dr Ashish Anil Dr Tay Jam Chin Introduction Risk Factors Clinical Presentation Classification History PHYSICAL examination
Peripheral Arterial Disease Lower Extremity 05 Contributor Dr Steven Chong Advisors Dr Ashish Anil Dr Tay Jam Chin Introduction Risk Factors Clinical Presentation Classification History PHYSICAL examination
Maximally Invasive Vascular Surgery for the Treatment of Critical Limb Ischemia
 Maximally Invasive Vascular Surgery for the Treatment of Critical Limb Ischemia Traci A. Kimball, MD Department of Surgery Grand Rounds Septemember 13, 2010 Overview Defining Critical Limb Ischemia Epidemiology
Maximally Invasive Vascular Surgery for the Treatment of Critical Limb Ischemia Traci A. Kimball, MD Department of Surgery Grand Rounds Septemember 13, 2010 Overview Defining Critical Limb Ischemia Epidemiology
Subclavian artery Stenting
 Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
BC Vascular Day. Contents. November 3, Abdominal Aortic Aneurysm 2 3. Peripheral Arterial Disease 4 6. Deep Venous Thrombosis 7 8
 BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
Disclosures. Talking Points. An initial strategy of open bypass is better for some CLI patients, and we can define who they are
 An initial strategy of open bypass is better for some CLI patients, and we can define who they are Fadi Saab, MD, FASE, FACC, FSCAI Metro Heart & Vascular Metro Health Hospital, Wyoming, MI Assistant Clinical
An initial strategy of open bypass is better for some CLI patients, and we can define who they are Fadi Saab, MD, FASE, FACC, FSCAI Metro Heart & Vascular Metro Health Hospital, Wyoming, MI Assistant Clinical
RevIewS. Interventions for lower extremity peripheral artery disease
 RevIewS Interventions for lower extremity peripheral artery disease Jade S. Hiramoto 1, Martin Teraa 2, Gert J. de Borst 2 and Michael S. Conte 1 * Abstract Peripheral artery disease (PAD) of the lower
RevIewS Interventions for lower extremity peripheral artery disease Jade S. Hiramoto 1, Martin Teraa 2, Gert J. de Borst 2 and Michael S. Conte 1 * Abstract Peripheral artery disease (PAD) of the lower
Disclosures. Critical Limb Ischemia. Vascular Testing in the CLI Patient. Vascular Testing in Critical Limb Ischemia UCSF Vascular Symposium
 Disclosures Vascular Testing in the CLI Patient None 2015 UCSF Vascular Symposium Warren Gasper, MD Assistant Professor of Surgery UCSF Division of Vascular Surgery Critical Limb Ischemia Chronic Limb
Disclosures Vascular Testing in the CLI Patient None 2015 UCSF Vascular Symposium Warren Gasper, MD Assistant Professor of Surgery UCSF Division of Vascular Surgery Critical Limb Ischemia Chronic Limb
9/7/2018. Disclosures. CV and Limb Events in PAD. Challenges to Revascularization. Challenges. Answering the Challenge
 Disclosures State-of-the-Art Endovascular Lower Extremity Revascularization Promotional Speaker Jansen Pharmaceutical Promotional Speaker Amgen Pharmaceutical C. Michael Brown, MD, FACC al Cardiology Associate
Disclosures State-of-the-Art Endovascular Lower Extremity Revascularization Promotional Speaker Jansen Pharmaceutical Promotional Speaker Amgen Pharmaceutical C. Michael Brown, MD, FACC al Cardiology Associate
V.A. is a 62-year-old male who presents in referral
 , LLC an HMP Communications Holdings Company Clinical Case Update Latest Trends in Critical Limb Ischemia Imaging Amit Srivastava, MD, FACC, FABVM Interventional Cardiologist Bay Area Heart Center St.
, LLC an HMP Communications Holdings Company Clinical Case Update Latest Trends in Critical Limb Ischemia Imaging Amit Srivastava, MD, FACC, FABVM Interventional Cardiologist Bay Area Heart Center St.
Managing Conditions Resulting from Untreated Cardiometabolic Syndrome
 Managing Conditions Resulting from Untreated Cardiometabolic Syndrome Matthew P. Namanny DO, FACOS Vascular/Endovascular Surgery Saguaro Surgical/AZ Vascular Specialist Tucson Medical Center Critical Limb
Managing Conditions Resulting from Untreated Cardiometabolic Syndrome Matthew P. Namanny DO, FACOS Vascular/Endovascular Surgery Saguaro Surgical/AZ Vascular Specialist Tucson Medical Center Critical Limb
Hybrid Procedures for Peripheral Obstructive Disease - Step by Step -
 Hybrid Procedures for Peripheral Obstructive Disease - Step by Step - Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name:..holger Staab... I have
Hybrid Procedures for Peripheral Obstructive Disease - Step by Step - Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name:..holger Staab... I have
LIMB SALVAGE IN THE DIABETIC PATIENT
 LIMB SALVAGE IN THE DIABETIC PATIENT WHO? HOW? BEST? DISCLOSURES Educational grant from Cook Inc OBJECTIVES Review risk stratification and staging schemes for the threatened limb Discuss current concepts
LIMB SALVAGE IN THE DIABETIC PATIENT WHO? HOW? BEST? DISCLOSURES Educational grant from Cook Inc OBJECTIVES Review risk stratification and staging schemes for the threatened limb Discuss current concepts
Disclosures. In-Stent Restenosis: The Tail IS Wagging the Dog 4/15/2016. Restenosis: The Continuing Challenge for Peripheral Vascular Intervention
 In-Stent Restenosis: The Tail IS Wagging the Dog Disclosures NONE Michael S. Conte MD Division of Vascular and Endovascular Surgery UCSF Heart and Vascular Center UCSF Vascular Symposium 2016 IF YOU WERE
In-Stent Restenosis: The Tail IS Wagging the Dog Disclosures NONE Michael S. Conte MD Division of Vascular and Endovascular Surgery UCSF Heart and Vascular Center UCSF Vascular Symposium 2016 IF YOU WERE
Peripheral Arterial Disease. Westley Smith MD Vascular Fellow
 Peripheral Arterial Disease Westley Smith MD Vascular Fellow Background (per 10,000) Goodney P, et al. Regional intensity of vascular care and lower extremity amputation rates. JVS. 2013; 6: 1471-1480.
Peripheral Arterial Disease Westley Smith MD Vascular Fellow Background (per 10,000) Goodney P, et al. Regional intensity of vascular care and lower extremity amputation rates. JVS. 2013; 6: 1471-1480.
Hybrid surgical treatment of bilateral aorto-femoral occlusion: a clinical case
 Hybrid surgical treatment of bilateral aorto-femoral occlusion: a clinical case Chernyavskiy M.,MD,PhD, Chernova D., Zherdev N., Chernov A. Almazov National Medical Research Centre, St.Petersburg, Russia
Hybrid surgical treatment of bilateral aorto-femoral occlusion: a clinical case Chernyavskiy M.,MD,PhD, Chernova D., Zherdev N., Chernov A. Almazov National Medical Research Centre, St.Petersburg, Russia
What s New in the Management of Peripheral Arterial Disease
 What s New in the Management of Peripheral Arterial Disease Sibu P. Saha, MD, MBA Professor of Surgery Chairman, Directors Council Gill Heart Institute University of Kentucky Lexington, KY Disclosure My
What s New in the Management of Peripheral Arterial Disease Sibu P. Saha, MD, MBA Professor of Surgery Chairman, Directors Council Gill Heart Institute University of Kentucky Lexington, KY Disclosure My
Aortoiliac occlusive disease
 Role of endovascular therapy in TASC II C & D inflow disease Per the TASC II Document: Surgery is the treatment of choice for type D lesions Aortoiliac occlusive disease Bala Ramanan, MBBS 1 st year vascular
Role of endovascular therapy in TASC II C & D inflow disease Per the TASC II Document: Surgery is the treatment of choice for type D lesions Aortoiliac occlusive disease Bala Ramanan, MBBS 1 st year vascular
Step by step Hybrid procedures in peripheral obstructive disease. Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery
 Step by step Hybrid procedures in peripheral obstructive disease Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name: H.H. Staab I have the following
Step by step Hybrid procedures in peripheral obstructive disease Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name: H.H. Staab I have the following
Peripheral Artery Disease Role of Exercise, Endovascular and Surgical Options
 Peripheral Artery Disease Role of Exercise, Endovascular and Surgical Options Jeffrey W. Olin, D.O., F.A.C.C., F.A.H.A. Professor of Medicine (Cardiology) Director of Vascular Medicine & the Vascular Diagnostic
Peripheral Artery Disease Role of Exercise, Endovascular and Surgical Options Jeffrey W. Olin, D.O., F.A.C.C., F.A.H.A. Professor of Medicine (Cardiology) Director of Vascular Medicine & the Vascular Diagnostic
Disclosures. Carotid artery stenting. Surveillance after Endovascular Intervention: When to Re-Intervene and What s the Evidence
 Disclosures Surveillance after Endovascular Intervention: When to Re-Intervene and What s the Evidence None 2015 UCSF Vascular Symposium Warren Gasper, MD Assistant Professor of Surgery UCSF Division of
Disclosures Surveillance after Endovascular Intervention: When to Re-Intervene and What s the Evidence None 2015 UCSF Vascular Symposium Warren Gasper, MD Assistant Professor of Surgery UCSF Division of
Endovascular Is The Way To Go: Revascularize As Many Vessels As You Can
 Rafael Malgor, MD Assistant Professor of Surgery The University of Oklahoma, Tulsa Endovascular Is The Way To Go: Revascularize As Many Vessels As You Can Background Lower extremity anatomy (below the
Rafael Malgor, MD Assistant Professor of Surgery The University of Oklahoma, Tulsa Endovascular Is The Way To Go: Revascularize As Many Vessels As You Can Background Lower extremity anatomy (below the
Disclosures. TASC, AHA, SVS: What s Happening with the Guidelines? How Are They Relevant? Purpose of Practice Guidelines
 TASC, AHA, SVS: What s Happening with the Guidelines? How Are They Relevant? Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center UCSF Medical
TASC, AHA, SVS: What s Happening with the Guidelines? How Are They Relevant? Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center UCSF Medical
The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions
 The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Dr. Sven Bräunlich Department of Angiology University-Hospital Leipzig, Germany Disclosure Speaker
The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Dr. Sven Bräunlich Department of Angiology University-Hospital Leipzig, Germany Disclosure Speaker
Resident Teaching Conference 3/12/2010
 Resident Teaching Conference 3/12/2010 Goals Definition and Classification of Acute Limb Ischemia Clinical Assessment of the Vascular Patient History and Physical Diagnostic Modalities Management of Acute
Resident Teaching Conference 3/12/2010 Goals Definition and Classification of Acute Limb Ischemia Clinical Assessment of the Vascular Patient History and Physical Diagnostic Modalities Management of Acute
Vascular claudication: How to individualize treatment
 REVIEW BRUCE H. GRAY, DO Codirector, Peripheral Interventional Laboratory, Cleveland Clinic. TIMOTHY M. SULLIVAN, MD Codirector, Peripheral Interventional Laboratory, Cleveland Clinic. Vascular claudication:
REVIEW BRUCE H. GRAY, DO Codirector, Peripheral Interventional Laboratory, Cleveland Clinic. TIMOTHY M. SULLIVAN, MD Codirector, Peripheral Interventional Laboratory, Cleveland Clinic. Vascular claudication:
Practical Point in Holistic Diabetic Foot Care 3 March 2016
 Diabetic Foot Ulcer : Vascular Management Practical Point in Holistic Diabetic Foot Care 3 March 2016 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai
Diabetic Foot Ulcer : Vascular Management Practical Point in Holistic Diabetic Foot Care 3 March 2016 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai
Lower Extremity Arterial Disease
 Lower Extremity Arterial Disease Circulating the Facts About Peripheral Disease Brought to you by the Education Committee of the Society for 1 www.svnnet.org Peripheral Artery Disease (PAD) Many people
Lower Extremity Arterial Disease Circulating the Facts About Peripheral Disease Brought to you by the Education Committee of the Society for 1 www.svnnet.org Peripheral Artery Disease (PAD) Many people
Endovascular Should Be Considered First Line Therapy
 Revascularization of Patients with Critical Limb Ischemia Endovascular Should Be Considered First Line Therapy Michael Conte David Dawson David L. Dawson, MD Revised Presentation Title A Selective Approach
Revascularization of Patients with Critical Limb Ischemia Endovascular Should Be Considered First Line Therapy Michael Conte David Dawson David L. Dawson, MD Revised Presentation Title A Selective Approach
PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA. Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE
 PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE Disclosure Speaker name: DR. Manar Trab I have the following potential
PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE Disclosure Speaker name: DR. Manar Trab I have the following potential
Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2)
") Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2) Definition Vascular surgery is the specialty concerned with the diagnosis and management of congenital and acquired diseases of the
Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2) Definition Vascular surgery is the specialty concerned with the diagnosis and management of congenital and acquired diseases of the
Limb Salvage in Diabetic Ischemic Foot. Kritaya Kritayakirana, MD, FACS Assistant Professor Chulalongkorn University April 30, 2017
 Limb Salvage in Diabetic Ischemic Foot Kritaya Kritayakirana, MD, FACS Assistant Professor Chulalongkorn University April 30, 2017 Case Male 67 years old Underlying DM, HTN, TVD Present with gangrene
Limb Salvage in Diabetic Ischemic Foot Kritaya Kritayakirana, MD, FACS Assistant Professor Chulalongkorn University April 30, 2017 Case Male 67 years old Underlying DM, HTN, TVD Present with gangrene
Peripheral Arterial Occlusive Disease- The Challenge in patients with diabetes
 Peripheral Arterial Occlusive Disease- The Challenge in patients with diabetes Ashok Handa Reader in Surgery and Consultant Surgeon Nuffield Department of Surgery University of Oxford Introduction Vascular
Peripheral Arterial Occlusive Disease- The Challenge in patients with diabetes Ashok Handa Reader in Surgery and Consultant Surgeon Nuffield Department of Surgery University of Oxford Introduction Vascular
Peripheral Arterial Disease: A Practical Approach
 Peripheral Arterial Disease: A Practical Approach Sanjoy Kundu BSc, MD, FRCPC, DABR, FASA, FCIRSE, FSIR The Scarborough Hospital Toronto Endovascular Centre The Vein Institute of Toronto Scarborough Vascular
Peripheral Arterial Disease: A Practical Approach Sanjoy Kundu BSc, MD, FRCPC, DABR, FASA, FCIRSE, FSIR The Scarborough Hospital Toronto Endovascular Centre The Vein Institute of Toronto Scarborough Vascular
Case Discussion. Disclosures. Critical Limb Ischemia: A Selective Approach to Revascularization Works Best 4/28/2012. None. 58 yo M, DM, CAD, HTN
 Critical Limb Ischemia: A Selective Approach to Revascularization Works Best None Disclosures Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center
Critical Limb Ischemia: A Selective Approach to Revascularization Works Best None Disclosures Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center
Lower Extremity Artery: Physiologic Testing
 Master Title Ultrasound for Initial Evaluation of Lower Extremity Arterial Occlusive Disease: WHY? Gregory L. Moneta MD Professor and Chief Knight Cardiovascular Institute Division of Vascular Surgery
Master Title Ultrasound for Initial Evaluation of Lower Extremity Arterial Occlusive Disease: WHY? Gregory L. Moneta MD Professor and Chief Knight Cardiovascular Institute Division of Vascular Surgery
Interventional Treatment First for CLI
 Interventional Treatment First for CLI Patrick Alexander, MD, FACC, FSCAI Interventional Cardiology Medical Director, Critical Limb Clinic Providence Heart Institute, Southfield MI 48075 Disclosures Consultant
Interventional Treatment First for CLI Patrick Alexander, MD, FACC, FSCAI Interventional Cardiology Medical Director, Critical Limb Clinic Providence Heart Institute, Southfield MI 48075 Disclosures Consultant
The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Preliminary report
 The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Preliminary report G. Biro, M. Bosiers on behalf of ZILVERPASS Study Group Disclosure Speaker
The ZILVERPASS study a randomized study comparing ZILVER PTX stenting with Bypass in femoropopliteal lesions Preliminary report G. Biro, M. Bosiers on behalf of ZILVERPASS Study Group Disclosure Speaker
Boca Raton Regional Hospital Grand Rounds September 13, 2016
 Boca Raton Regional Hospital Grand Rounds September 13, 2016 W. Anthony Lee, MD, FACS Chief, BocaCare Vascular Surgery Christine E. Lynn Heart and Vascular Institute Boca Raton, Florida Disclosures No
Boca Raton Regional Hospital Grand Rounds September 13, 2016 W. Anthony Lee, MD, FACS Chief, BocaCare Vascular Surgery Christine E. Lynn Heart and Vascular Institute Boca Raton, Florida Disclosures No
National Vascular Registry
 National Vascular Registry Bypass Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or postcode.
National Vascular Registry Bypass Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or postcode.
Clinical Approach to CLI and Related Diagnostics: What You Need to Know
 Clinical Approach to CLI and Related Diagnostics: What You Need to Know Ido Weinberg, MD Assistant Professor of Medicine Harvard Medical School Massachusetts General Hospital None Disclosures Critical
Clinical Approach to CLI and Related Diagnostics: What You Need to Know Ido Weinberg, MD Assistant Professor of Medicine Harvard Medical School Massachusetts General Hospital None Disclosures Critical
Cath Lab Essentials : Peripheral Vascular Disease in Patients with CAD
 Cath Lab Essentials : Peripheral Vascular Disease in Patients with CAD Pranav M. Patel, MD, FACC, FSCAI Interim Chief & Associate Professor of Medicine Director, Cardiac Catheterization Lab University
Cath Lab Essentials : Peripheral Vascular Disease in Patients with CAD Pranav M. Patel, MD, FACC, FSCAI Interim Chief & Associate Professor of Medicine Director, Cardiac Catheterization Lab University
ACCF/AHA Practice Guidelines
 ACCF/AHA Practice Guidelines Management of Patients With Peripheral Artery Disease (Compilation of 2005 and 2011 ACCF/AHA Guideline Recommendations) A Report of the American College of Cardiology Foundation/American
ACCF/AHA Practice Guidelines Management of Patients With Peripheral Artery Disease (Compilation of 2005 and 2011 ACCF/AHA Guideline Recommendations) A Report of the American College of Cardiology Foundation/American
Cardiovascular Update for Primary Care Providers. Peripheral Vascular Disease October 4 th 2014 Roberto A. Corpus Jr., MD
 Cardiovascular Update for Primary Care Providers Peripheral Vascular Disease October 4 th 2014 Roberto A. Corpus Jr., MD Agenda Lower Extremity pain Initial evaluation Treatment options of noncritical
Cardiovascular Update for Primary Care Providers Peripheral Vascular Disease October 4 th 2014 Roberto A. Corpus Jr., MD Agenda Lower Extremity pain Initial evaluation Treatment options of noncritical
Carotid Stenosis (carotid artery disease)
") 1 Carotid Stenosis (carotid artery disease) Overview Carotid stenosis is a narrowing of the carotid arteries, the two major arteries that carry oxygenrich blood from the heart to the brain. Also called
1 Carotid Stenosis (carotid artery disease) Overview Carotid stenosis is a narrowing of the carotid arteries, the two major arteries that carry oxygenrich blood from the heart to the brain. Also called
Peripheral Arterial Disease: Screening, Evaluation and Management. Mitchel Sklar, MD, FACC, FSCAI. Cardiovascular Associates of R.I.
 Peripheral Arterial Disease: Screening, Evaluation and Management Mitchel Sklar, MD, FACC, FSCAI Cardiovascular Associates of R.I. Natural History of Intermittent Claudication/PAD: Peripheral to what?
Peripheral Arterial Disease: Screening, Evaluation and Management Mitchel Sklar, MD, FACC, FSCAI Cardiovascular Associates of R.I. Natural History of Intermittent Claudication/PAD: Peripheral to what?
Peripheral Arterial Disease: Objectives. Disclosure. Definition: Peripheral Arterial Disease (PAD)
") Geriatric Grand Rounds Tuesday, April 21, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this
Geriatric Grand Rounds Tuesday, April 21, 2009 12:00 noon Dr. Bill Black Auditorium Glenrose Rehabilitation Hospital In keeping with Glenrose Rehabilitation Hospital policy, speakers participating in this
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 6/30/2012 Radiology Quiz of the Week # 79 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 6/30/2012 Radiology Quiz of the Week # 79 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
MINIMALLY-INVASIVE TREATMENT OF VASCULAR DISEASE
 CLINIC PROFILE MINIMALLY-INVASIVE TREATMENT OF VASCULAR DISEASE The Section of Vascular Surgery at Dartmouth- Hitchcock Medical Center is committed to outstanding care of patients with vascular disease,
CLINIC PROFILE MINIMALLY-INVASIVE TREATMENT OF VASCULAR DISEASE The Section of Vascular Surgery at Dartmouth- Hitchcock Medical Center is committed to outstanding care of patients with vascular disease,
Patient Brochure. Clearstream Technologies, Ltd. Moyne Upper Enniscorthy Co. Wexford, Ireland. PK Rev. 0 05/17
 Patient Brochure Clearstream Technologies, Ltd. Moyne Upper Enniscorthy Co. Wexford, Ireland PK1411100 Rev. 0 05/17 LIFESTREAM Patient Brochure If you or a member of your family has been diagnosed with
Patient Brochure Clearstream Technologies, Ltd. Moyne Upper Enniscorthy Co. Wexford, Ireland PK1411100 Rev. 0 05/17 LIFESTREAM Patient Brochure If you or a member of your family has been diagnosed with
Non-invasive examination
 Non-invasive examination Segmental pressure and Ankle-Brachial Index (ABI) The segmental blood pressure (SBP) examination is a simple, noninvasive method for diagnosing and localizing arterial disease.
Non-invasive examination Segmental pressure and Ankle-Brachial Index (ABI) The segmental blood pressure (SBP) examination is a simple, noninvasive method for diagnosing and localizing arterial disease.
Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI
 Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI 1 Disclosures I have no financial disclosures related to this talk Objectives 1. Discuss indications for intervention
Intervention for Lower Extremity PAD: When, why and what?! Robert F Cuff, MD FACS RVT RPVI 1 Disclosures I have no financial disclosures related to this talk Objectives 1. Discuss indications for intervention
Endovascular and Hybrid Treatment of TASC C & D Aortoiliac Occlusive Disease
 Endovascular and Hybrid Treatment of TASC C & D Aortoiliac Occlusive Disease Arash Bornak, MD FACS Vascular & Endovascular Surgery University of Miami Miller School of Medicine No disclosure BACKGROUND
Endovascular and Hybrid Treatment of TASC C & D Aortoiliac Occlusive Disease Arash Bornak, MD FACS Vascular & Endovascular Surgery University of Miami Miller School of Medicine No disclosure BACKGROUND
Lower Extremity Peripheral Arterial Disease: Less is Sometimes More. Spence M Taylor, M.D.
 Lower Extremity Peripheral Arterial Disease: Less is Sometimes More Spence M Taylor, M.D. President, Greenville Health System Clinical University Senior Associate Dean for Academic Affairs and Diversity
Lower Extremity Peripheral Arterial Disease: Less is Sometimes More Spence M Taylor, M.D. President, Greenville Health System Clinical University Senior Associate Dean for Academic Affairs and Diversity
Global Vascular Guideline on the Management of Chronic Limb Threatening Ischemia -a new foundation for evidence-based care
 Global Vascular Guideline on the Management of Chronic Limb Threatening Ischemia -a new foundation for evidence-based care Michael S. Conte MD Professor and Chief, Division of Vascular and Endovascular
Global Vascular Guideline on the Management of Chronic Limb Threatening Ischemia -a new foundation for evidence-based care Michael S. Conte MD Professor and Chief, Division of Vascular and Endovascular
Registry Assessment of Peripheral Interventional Devices (RAPID)
") Registry Assessment of Peripheral Interventional Devices (RAPID) Adding Data Sources May 2, 2018 W. Schuyler Jones, MD Duke Clinical Research Institute Duke Heart Center Disclosures Research Grants: Agency
Registry Assessment of Peripheral Interventional Devices (RAPID) Adding Data Sources May 2, 2018 W. Schuyler Jones, MD Duke Clinical Research Institute Duke Heart Center Disclosures Research Grants: Agency
Abdominal Aortic Aneurysms. A Surgeons Perspective Dr. Derek D. Muehrcke
 Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
Abdominal Aortic Aneurysms A Surgeons Perspective Dr. Derek D. Muehrcke Aneurysm Definition The abnormal enlargement or bulging of an artery caused by an injury or weakness in the blood vessel wall A localized
2-YEAR DATA SUPERA POPLITEAL REAL WORLD
 2-YEAR DATA SUPERA POPLITEAL REAL WORLD Enrique M. San Norberto. Angiology and Vascular Surgery. Valladolid University Hospital. Valladolid. Spain. Disclosure Speaker name: ENRIQUE M. SAN NORBERTO I have
2-YEAR DATA SUPERA POPLITEAL REAL WORLD Enrique M. San Norberto. Angiology and Vascular Surgery. Valladolid University Hospital. Valladolid. Spain. Disclosure Speaker name: ENRIQUE M. SAN NORBERTO I have
The present status of selfexpanding. for CLI: Why and when to use. Sean P Lyden MD Cleveland Clinic Cleveland, Ohio
 The present status of selfexpanding and balloonexpandable tibial BMS and DES for CLI: Why and when to use Sean P Lyden MD Cleveland Clinic Cleveland, Ohio Disclosure Speaker name: Sean Lyden, MD I have
The present status of selfexpanding and balloonexpandable tibial BMS and DES for CLI: Why and when to use Sean P Lyden MD Cleveland Clinic Cleveland, Ohio Disclosure Speaker name: Sean Lyden, MD I have
Endovascular treatment (EVT) has markedly advanced,
 has markedly advanced,") Ann Vasc Dis Vol. 6, No. 3; 2013; pp 573 577 Online August 12, 2013 2013 Annals of Vascular Diseases doi:10.3400/avd.oa.13-00055 Original Article A Review of Surgically Treated Patients with Obstruction
Ann Vasc Dis Vol. 6, No. 3; 2013; pp 573 577 Online August 12, 2013 2013 Annals of Vascular Diseases doi:10.3400/avd.oa.13-00055 Original Article A Review of Surgically Treated Patients with Obstruction
Peripheral Arterial Disease
 Peripheral Arterial Disease Presentation Prevention Treatment Cardiovascular and Stroke Summit 1 June 2018 Mary MacDonald CD MD PhD FRCSC RPVI Vascular Surgeon Thunder Bay Regional Health Sciences Centre
Peripheral Arterial Disease Presentation Prevention Treatment Cardiovascular and Stroke Summit 1 June 2018 Mary MacDonald CD MD PhD FRCSC RPVI Vascular Surgeon Thunder Bay Regional Health Sciences Centre
National Vascular Registry
 National Vascular Registry Angioplasty Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or
National Vascular Registry Angioplasty Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS
 VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
PAD Characterization Within A Healthcare System" RAPID Face-to-Face Meeting Schuyler Jones, MD September 14, 2016
 PAD Characterization Within A Healthcare System" RAPID Face-to-Face Meeting Schuyler, MD September 14, 2016 Interventional Cardiology and Cath Labs Disclosures Research Grants: Agency for Healthcare Research
PAD Characterization Within A Healthcare System" RAPID Face-to-Face Meeting Schuyler, MD September 14, 2016 Interventional Cardiology and Cath Labs Disclosures Research Grants: Agency for Healthcare Research
SPINACH Making Limb Salvage Salad from Spinach alone
 SPINACH Making Limb Salvage Salad from Spinach alone Surgical reconstruction versus Peripheral Intervention in patients with critical limb ischemia prospective multicenter registry in Japan Nobuyoshi Azuma,
SPINACH Making Limb Salvage Salad from Spinach alone Surgical reconstruction versus Peripheral Intervention in patients with critical limb ischemia prospective multicenter registry in Japan Nobuyoshi Azuma,
Learning About. Peripheral Artery Disease
 SM A C P S P E C I A L R E P O R T Learning About Peripheral Artery Disease What Is Peripheral Artery Disease? Peripheral artery disease (PAD) is a form of atherosclerosis the hardening and narrowing of
SM A C P S P E C I A L R E P O R T Learning About Peripheral Artery Disease What Is Peripheral Artery Disease? Peripheral artery disease (PAD) is a form of atherosclerosis the hardening and narrowing of
3-year results of the OLIVE registry:
 3-year results of the OLIVE registry: A prospective multicenter study in patients with critical limb ischemia Osamu Iida, MD Kansai Rosai Hospital Cardiovascular Center Amagasaki, Hyogo, Japan Disclosure
3-year results of the OLIVE registry: A prospective multicenter study in patients with critical limb ischemia Osamu Iida, MD Kansai Rosai Hospital Cardiovascular Center Amagasaki, Hyogo, Japan Disclosure
Disclosures. Objectives. Bypass vs. Endo for SFA Disease: Reaching Consensus on a Rational Approach. Christopher D. Owens, MD 4/23/2009
 Disclosures Bypass vs. Endo for SFA Disease: Reaching Consensus on a Rational Approach No disclosures No conflicts of interest Christopher D. Owens, MD Objectives Changing face of our patients presenting
Disclosures Bypass vs. Endo for SFA Disease: Reaching Consensus on a Rational Approach No disclosures No conflicts of interest Christopher D. Owens, MD Objectives Changing face of our patients presenting
- Lecture - Recommandations ESC : messages importants P. MEYER (Saint Laurent du Var) - Controverse - Qui doit faire l'angioplastie périphérique?
 - Controverse - Qui doit faire l'angioplastie périphérique?") - Lecture - Recommandations ESC : messages importants P. MEYER (Saint Laurent du Var) - Controverse - Qui doit faire l'angioplastie périphérique? Un chirurgien E. DUCASSE (Bordeaux) Un interventionnel
- Lecture - Recommandations ESC : messages importants P. MEYER (Saint Laurent du Var) - Controverse - Qui doit faire l'angioplastie périphérique? Un chirurgien E. DUCASSE (Bordeaux) Un interventionnel