Global Vascular Guideline on the Management of Chronic Limb Threatening Ischemia -a new foundation for evidence-based care
|
|
|
- Florence Barnett
- 5 years ago
- Views:
Transcription
 Symic, Inc.")
1 Global Vascular Guideline on the Management of Chronic Limb Threatening Ischemia -a new foundation for evidence-based care Michael S. Conte MD Professor and Chief, Division of Vascular and Endovascular Surgery Disclosures Co-editor, Global Vascular Guidelines Writing Group Abbott Vascular (advisory board) Symic, Inc. (advisory board) UCSF Vascular Symposium 2018: Global Vascular Guidelines on CLTI 1
2 The Global Vascular Guidelines (GVG) initiative is sponsored by an international consortium of vascular societies, led by the European Society for Vascular Surgery (ESVS), the Society for Vascular Surgery (SVS), and the World Federation of Vascular Societies () Definitions: CLTI The term critical limb ischemia (CLI) is outdated and fails to encompass the full spectrum of patients who are evaluated and treated for limb-threatening ischemia in modern practice Instead, the term chronic limb-threatening ischemia (CLTI) is proposed, in order to include a broader and more heterogeneous group of patients with varying degrees of ischemia that can often delay wound healing and increase amputation risk. 2
3 CLTI: criteria for diagnosis Objectively documented atherosclerotic PAD Ischemic rest pain typically described as pain in the mid- and forefoot at rest, often worse with recumbency and relieved by dependency, present for more than 2 weeks ABPI <0.4 (using higher of the DP / PT) Absolute highest ankle pressure <50 mmhg Absolute toe pressure <30 mmhg TcP02 <20 Torr Flat pulse volume recording waveforms Tissue Loss diabetic foot ulcer, nonhealing lower limb or foot ulceration of at least 2 weeks duration, any gangrene WIfI ischemia score 1 CLTI: exclusions Absence of any significant PAD, eg, WIfI ischemia grade=0 May be unique circumstances of impaired local perfusion (angiosome) not reflected by the WIfI ischemia grade for the limb as a whole Lower extremity wounds that are a direct result of acute trauma Ulcers of primarily venous origin Acute limb ischemia (onset 14 days) Impaired tissue perfusion related to non-atherosclerotic conditions 3


4 Need for Structured Decision Making in CLTI PLAN: Patient Risk Limb threat severity: WIfI Staging Anatomic pattern of disease: GLASS system 4

5 Risk stratification tools High Risk defined as expected perioperative mortality >5% OR expected 2 year survival <50% Importance of Limb Staging in CLTI Broad spectrum of complexity and risk for limb loss Complicates analysis of outcomes and treatment decisions Previous classification systems inadequately capture the full range of neuro-ischemic compromise Fallacy of a specific hemodynamic threshold for critical ischemia SVS Wound, Ischemia, Foot Infection (WIfI) system Characterizes each of the three major components Grouped into 4 stages based on estimated risk for limb loss Multiple validation reports 5
6 Definitions: WIfI WIfI stratifies amputation risk according to the Wound, the degree of Ischemia, and presence and severity of foot Infection WIfI scores and clinical stages appear to strongly correlate with important clinical outcomes, including those included in SVS Objective Performance Goals (OPG): limb amputation, 1 year amputation free survival, and wound healing time WIfI is currently being evaluated in Multi center trials in the US UK NIR HTA funded BASIL 2 and BASIL 3 trial SVS VQI (Vascular Quality Initiative) Registry of lower extremity interventions. Wound Grade Clinical Category Grade Clinical Description 0 Ischemic rest pain; Pre gangrenous skin change, without frank ulcer or gangrene (Pedis or UT Class 0) 1 Minor tissue loss: small shallow ulceration) < 5 cm 2 on foot or distal leg (Pedis or UT Class 1); no exposed bone unless limited to distal phalanx 2 Major tissue loss: deeper ulceration(s) with exposed bone, joint or tendon, ulcer 5 10 cm 2 not involving calcaneus (Pedis or UT Classes 2 and 3); gangrenous changes limited to digits. Salvageable with multiple digital amps or standard TMA + skin coverage 3 Extensive ulcer/gangrene > 10 cm 2 involving forefoot or midfoot; full thickness heel ulcer > 5 cm 2 + calcaneal involvement. Salvageable only with complex foot reconstruction, nontraditional TMA (Chopart/Lisfranc); flap coverage or complex wound management needed 6
7 Ischemia Grade Noninvasive Assessment Grade ABI Ankle SP TP 0 > 0.80 > 100 mm Hg > 60 mm Hg mmhg mm Hg mm Hg mm Hg 3 < 0.40 < 50 mm Hg < 30 mm Hg ABI=ankle brachial index; SP= systolic pressure; TP=toe pressure 7



8 Risk of Amputation Benefit of Revascularization? Note: These are NOT Concordant There Is a Free App for That: 8
9 Risk of amputation versus WIfI Stage: Compilation of published data Study (year): # Limbs at Risk Stage 1 Stage 2 Stage 3 Stage 4 Cull (2014): (3%) 63 (10%) 43 (23%) 8 (40%) Zhan (2015): (0%) 50 (0%) 53 (8%) 59 (64%)* Darling (2015): (0%) 111 (10%) 222 (11%) 213 (24%) Causey (2016): (0%) 48 (8%) 42 (5%) 49 (20%) Beropoulis (2016): (0%) 42 (2%) 29 (3%) 26 (12%) Ward (2016): 98 5 (0%) 21 (14%) 14 (21%) 58 (34%) Darling (2017): (0%) 293 (4%) 249 (4%) 438 (21%) Robinson (2017): (4%) 67 (16%) 64 (10%) 83 (22%) Mathioudakis (2017): (6.5%) 33 (6%) 87 (8%)** 64 (6%)*** N = 2820 (weighted mean) 291 (3.2%) 728 (6.8%) 803 (8.5%) 998 (24%) Median (% 1 year amputation) 0% 8% 8% 22% Limb staging and appropriateness of revascularization CLTI represents a range of limb severity and ischemia as described in WIfI staging. Severe ischemia (WIfI ischemia grade 3) mandates revascularization for limb salvage With increased stages of limb threat (WIfI stages 3, 4) moderate degrees of ischemia (grades 1, 2) may be appropriate to address Low risk limbs (WIfI Stage 1) should be treated with wound care; revascularization should be reserved for failure to heal (50% within 4 6 weeks) or clinical signs of deterioration Not indicated for Ischemia grade 0 9
10 Benefit of revascularization varies with severity of limb threat and ischemia 3 N/A High benefit Severity of Ischemia (WIfI Ischemia Grade) N/A Low/Nil benefit Limb Severity (WIfI Stage) Rationale for a new anatomic staging system in CLTI Schemes focused on individual lesions (e.g. TASC) or overall burden of disease (e.g. Bollinger) are not useful for defining evidence-based revascularization in CLTI Restoration of in-line flow to the foot is a primary technical goal of revascularization in CLTI, particularly in patients with tissue loss Factors that determine clinical success for endovascular and open bypass surgery are intrinsically different 10
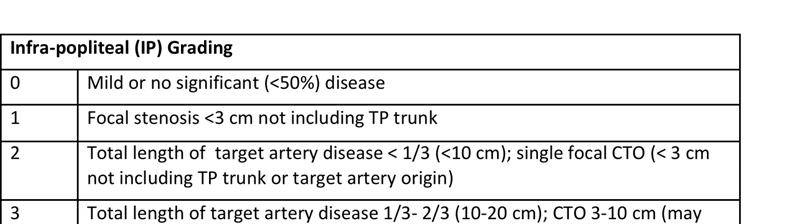
11 GLASS*: Assumptions and Approach Focus on Infrainguinal Disease (SFA origin to foot) Clinician defines the primary Target Artery Path (TAP) Femoro-popliteal (FP) and Infra-popliteal (IP) segments separately graded (0-4), then combined into Three GLASS Stages for the limb (I-III) Infra-malleolar (pedal) disease graded; used as a modifier only Calcification graded as Severe or not; simplified system *Global Limb Anatomic Staging System GLASS: Target Artery Path and Limb-Based Patency Restoration of in line flow to the ankle and foot is a primary goal Target artery path (TAP): the selected continuous route of in line flow from groin to ankle TAP usually involves the least diseased IP artery; may be angiosomebased Limb based patency (LBP): maintained patency of the TAP. Lost when: Occlusion, critical stenosis, or re intervention affecting any portion of the TAP (anatomical failure), and/or: Fall in ABI ( 0.15) or TBI ( 0.10), or 50% stenosis in the TAP, in the presence of recurrent or unresolved clinical symptoms (e.g. rest pain, worsening/persistent tissue loss; signifying hemodynamic failure) 11

12 12

13 GLASS: Consensus Staging of TAP Complexity for Endovascular Intervention 13



14 Pedal disease modifier not included in overall limb stage assignment at present due to insufficient data on relationship to treatment outcomes Examples of the GLASS system 14






15 FP grading: Total length of SFA disease: cm Popliteal disease: <5cm does not involve trifurcation Calcification + 1 FP grade = 4 IP grading: TAP= peroneal artery Peroneal: stenosis TP trunk IP grade = 2 GLASS Stage = III 15





16 FP grading: SFA single stenosis/occlusion approx 5 cm Popliteal: no significant stenosis FP grade = 1 IP grading: TAP = ATA ATA: 2 focal stenosis, <1/3 (<10cm) IP grade = 2 GLASS Stage = II FP grading: SFA: no significant stenosis Popliteal: no significant stenosis FP grade = 0 IP grading: TAP = peroneal artery Peroneal: CTO 3 10cm IP grade = 3 GLASS Stage = II 16

17 FP grading: SFA: no significant stenosis Popliteal: CTO extending into trifurcation FP grade = 4 IP grading: TAP = ATA ATA: CTO target artery origin IP grade = 3 GLASS Stage = III Factors Determining Clinical Success Differ High patient risk More severe limb threat (e.g. WIfI Stage 4) Greater target lesion/path complexity of occlusive disease Prior failed implant Poor runoff Good quality vein available Good quality vein not available FAVORS MORE Bypass Endo

 III II")

18 Preferred initial revascularization strategy for infrainguinal disease, in average risk CLTI patients with adequate autogenous vein for bypass Anatomic Complexity (GLASS Stage) III II I Open Bypass Indeterminate Endovascular No Revascularization Limb Severity (WIfI Stage) 18
 Bypass versus")

19 Funded by NHLBI in 2013 Compare initial Endo vs initial Bypass in CLI Parallel trial, stratified design Target 2100 patients, approximately 120 centers Current enrollment approximately 900 BASIL 2 (BTK) Bypass versus Angioplasty / Stenting in Severe Ischaemia of the Leg due to BTK Disease Trial Andrew W. Bradbury Sampson Gamgee Professor of Vascular Surgery University of Birmingham, UK Heart of England NHS Foundation Trust, Birmingham, UK 19
20 20
GLOBAL VASCULAR GUIDELINES: A NEW PATHWAY FOR LIMB SALVAGE
 GLOBAL VASCULAR GUIDELINES: A NEW PATHWAY FOR LIMB SALVAGE Michael S. Conte MD Professor and Chief, Vascular and Endovascular Surgery Co-Director, Center for Limb Preservation Co-Director, Heart and Vascular
GLOBAL VASCULAR GUIDELINES: A NEW PATHWAY FOR LIMB SALVAGE Michael S. Conte MD Professor and Chief, Vascular and Endovascular Surgery Co-Director, Center for Limb Preservation Co-Director, Heart and Vascular
LIMB SALVAGE IN THE DIABETIC PATIENT
 LIMB SALVAGE IN THE DIABETIC PATIENT WHO? HOW? BEST? DISCLOSURES Educational grant from Cook Inc OBJECTIVES Review risk stratification and staging schemes for the threatened limb Discuss current concepts
LIMB SALVAGE IN THE DIABETIC PATIENT WHO? HOW? BEST? DISCLOSURES Educational grant from Cook Inc OBJECTIVES Review risk stratification and staging schemes for the threatened limb Discuss current concepts
Validation and Clinical Utility of the SVS WIfI Threatened Limb Classification
 Validation and Clinical Utility of the SVS WIfI Threatened Limb Classification PRESENTED BY: 11 th Houston Aortic Symposium 15 February 2018 Joseph L. Mills, Sr., M.D. Reid Endowed Professor of Surgery
Validation and Clinical Utility of the SVS WIfI Threatened Limb Classification PRESENTED BY: 11 th Houston Aortic Symposium 15 February 2018 Joseph L. Mills, Sr., M.D. Reid Endowed Professor of Surgery
Clasificación WIFI: Finalmente hablaremos el mismo idioma! WIfI: Wound, Ischemia, foot Infection The SVS Threatened Limb Classification
 Clasificación WIFI: Finalmente hablaremos el mismo idioma! WIfI: Wound, Ischemia, foot Infection The SVS Threatened Limb Classification Joseph L. Mills, Sr., M.D. Professor of Surgery, Chief, Vascular
Clasificación WIFI: Finalmente hablaremos el mismo idioma! WIfI: Wound, Ischemia, foot Infection The SVS Threatened Limb Classification Joseph L. Mills, Sr., M.D. Professor of Surgery, Chief, Vascular
Acknowledgements. No tengo conflictos de interés que revelar. I have no conflicts of interest to disclose. Michael S. Conte. David G.
 No tengo conflictos de interés que revelar I have no conflicts of interest to disclose. Critical Limb Ischemia : The Need for a New System to Define Disease Burden and Stratify Amputation Risk and Need
No tengo conflictos de interés que revelar I have no conflicts of interest to disclose. Critical Limb Ischemia : The Need for a New System to Define Disease Burden and Stratify Amputation Risk and Need
Case Discussion. Disclosures. Critical Limb Ischemia: A Selective Approach to Revascularization Works Best 4/28/2012. None. 58 yo M, DM, CAD, HTN
 Critical Limb Ischemia: A Selective Approach to Revascularization Works Best None Disclosures Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center
Critical Limb Ischemia: A Selective Approach to Revascularization Works Best None Disclosures Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center
Disclosures. Talking Points. An initial strategy of open bypass is better for some CLI patients, and we can define who they are
 An initial strategy of open bypass is better for some CLI patients, and we can define who they are Fadi Saab, MD, FASE, FACC, FSCAI Metro Heart & Vascular Metro Health Hospital, Wyoming, MI Assistant Clinical
An initial strategy of open bypass is better for some CLI patients, and we can define who they are Fadi Saab, MD, FASE, FACC, FSCAI Metro Heart & Vascular Metro Health Hospital, Wyoming, MI Assistant Clinical
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division
 John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
John E. Campbell, MD Assistant Professor of Surgery and Medicine Department of Vascular Surgery West Virginia University, Charleston Division John Campbell, MD For the 12 months preceding this CME activity,
Maximally Invasive Vascular Surgery for the Treatment of Critical Limb Ischemia
 Maximally Invasive Vascular Surgery for the Treatment of Critical Limb Ischemia Traci A. Kimball, MD Department of Surgery Grand Rounds Septemember 13, 2010 Overview Defining Critical Limb Ischemia Epidemiology
Maximally Invasive Vascular Surgery for the Treatment of Critical Limb Ischemia Traci A. Kimball, MD Department of Surgery Grand Rounds Septemember 13, 2010 Overview Defining Critical Limb Ischemia Epidemiology
Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI?
 Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI? Peter F. Lawrence, M.D. Gonda Vascular Center Division of Vascular Surgery
Stratifying Management Options for Patients with Critical Limb Ischemia: When Should Open Surgery Be the Initial Option for CLI? Peter F. Lawrence, M.D. Gonda Vascular Center Division of Vascular Surgery
Practical Point in Holistic Diabetic Foot Care 3 March 2016
 Diabetic Foot Ulcer : Vascular Management Practical Point in Holistic Diabetic Foot Care 3 March 2016 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai
Diabetic Foot Ulcer : Vascular Management Practical Point in Holistic Diabetic Foot Care 3 March 2016 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai
Practical Point in Diabetic Foot Care 3-4 July 2017
 Diabetic Foot Ulcer : Role of Vascular Surgeon Practical Point in Diabetic Foot Care 3-4 July 2017 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai University
Diabetic Foot Ulcer : Role of Vascular Surgeon Practical Point in Diabetic Foot Care 3-4 July 2017 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai University
Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia
 Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia Albeir Mousa, MD., FACS.,MPH., MBA Professor of Vascular and Endovascular Surgery West Virginia University Disclosure None What you
Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia Albeir Mousa, MD., FACS.,MPH., MBA Professor of Vascular and Endovascular Surgery West Virginia University Disclosure None What you
Lower Extremity Peripheral Arterial Disease: Its All About the Pulse. Spence M Taylor, M.D.
 Lower Extremity Peripheral Arterial Disease: Its All About the Pulse Spence M Taylor, M.D. President, Greenville Health System Clinical University Senior Associate Dean for Academic Affairs and Diversity
Lower Extremity Peripheral Arterial Disease: Its All About the Pulse Spence M Taylor, M.D. President, Greenville Health System Clinical University Senior Associate Dean for Academic Affairs and Diversity
Disclosures. Critical Limb Ischemia. Vascular Testing in the CLI Patient. Vascular Testing in Critical Limb Ischemia UCSF Vascular Symposium
 Disclosures Vascular Testing in the CLI Patient None 2015 UCSF Vascular Symposium Warren Gasper, MD Assistant Professor of Surgery UCSF Division of Vascular Surgery Critical Limb Ischemia Chronic Limb
Disclosures Vascular Testing in the CLI Patient None 2015 UCSF Vascular Symposium Warren Gasper, MD Assistant Professor of Surgery UCSF Division of Vascular Surgery Critical Limb Ischemia Chronic Limb
Disclosures. TASC, AHA, SVS: What s Happening with the Guidelines? How Are They Relevant? Purpose of Practice Guidelines
 TASC, AHA, SVS: What s Happening with the Guidelines? How Are They Relevant? Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center UCSF Medical
TASC, AHA, SVS: What s Happening with the Guidelines? How Are They Relevant? Michael S. Conte MD, FACS Division of Vascular and Endovascular Surgery Co-Director, Heart and Vascular Center UCSF Medical
Angiosome concept myth or truth? Does it make a real difference in real world cases?
 Angiosome concept myth or truth? Does it make a real difference in real world cases? Osamu Iida, MD, FACC Kansai Rosai Hospital Amagasaki, Hyogo, Japan Disclosure Speaker name:... I have the following
Angiosome concept myth or truth? Does it make a real difference in real world cases? Osamu Iida, MD, FACC Kansai Rosai Hospital Amagasaki, Hyogo, Japan Disclosure Speaker name:... I have the following
Interventional Treatment First for CLI
 Interventional Treatment First for CLI Patrick Alexander, MD, FACC, FSCAI Interventional Cardiology Medical Director, Critical Limb Clinic Providence Heart Institute, Southfield MI 48075 Disclosures Consultant
Interventional Treatment First for CLI Patrick Alexander, MD, FACC, FSCAI Interventional Cardiology Medical Director, Critical Limb Clinic Providence Heart Institute, Southfield MI 48075 Disclosures Consultant
Critical Limb Ischemia A Collaborative Approach to Patient Care. Christopher LeSar, MD Vascular Institute of Chattanooga July 28, 2017
 Critical Limb Ischemia A Collaborative Approach to Patient Care Christopher LeSar, MD Vascular Institute of Chattanooga July 28, 2017 Surgeons idea Surgeons idea represents the final stage of peripheral
Critical Limb Ischemia A Collaborative Approach to Patient Care Christopher LeSar, MD Vascular Institute of Chattanooga July 28, 2017 Surgeons idea Surgeons idea represents the final stage of peripheral
UC SF. Disclosures. Vascular Assessment of the Diabetic Foot. What are the best predictors of wound healing? None. Non-Invasive Vascular Studies
 Disclosures Vascular Assessment of the Diabetic Foot What are the best predictors of wound healing? None Shant Vartanian MD Assistant Professor of Vascular Surgery UCSF Vascular Symposium April 20, 2013
Disclosures Vascular Assessment of the Diabetic Foot What are the best predictors of wound healing? None Shant Vartanian MD Assistant Professor of Vascular Surgery UCSF Vascular Symposium April 20, 2013
Due to Perimed s commitment to continuous improvement of our products, all specifications are subject to change without notice.
 A summary Disclaimer The information contained in this document is intended to provide general information only. It is not intended to be, nor does it constitute, medical advice. Under no circumstances
A summary Disclaimer The information contained in this document is intended to provide general information only. It is not intended to be, nor does it constitute, medical advice. Under no circumstances
Fluorescent Angiography: Practical uses in the Clinical Setting
 Fluorescent Angiography: Practical uses in the Clinical Setting Charles Andersen MD, FACS, MAPWCA Chief Vascular/Endovascular/ Limb Preservation Surgery Service (Emeritus) Chief of Wound Care Service Madigan
Fluorescent Angiography: Practical uses in the Clinical Setting Charles Andersen MD, FACS, MAPWCA Chief Vascular/Endovascular/ Limb Preservation Surgery Service (Emeritus) Chief of Wound Care Service Madigan
Peripheral Artery Disease Interventions Utilizing the Angiosomal Approach to the Complex Wound
 Peripheral Artery Disease Interventions Utilizing the Angiosomal Approach to the Complex Wound Craig M. Walker, MD, FACC, FACP Chairman, New Cardiovascular Horizons Clinical Professor of Medicine Tulane
Peripheral Artery Disease Interventions Utilizing the Angiosomal Approach to the Complex Wound Craig M. Walker, MD, FACC, FACP Chairman, New Cardiovascular Horizons Clinical Professor of Medicine Tulane
Objective assessment of CLI patients Hemodynamic parameters
 Objective assessment of CLI patients Hemodynamic parameters Worth anything in end stage patients? Marianne Brodmann Angiology, Medical University Graz, Austria Disclosure Speaker name: Marianne Brodmann
Objective assessment of CLI patients Hemodynamic parameters Worth anything in end stage patients? Marianne Brodmann Angiology, Medical University Graz, Austria Disclosure Speaker name: Marianne Brodmann
Diagnosis and Endovascular Treatment of Critical Limb Ischemia: What You Need to Know S. Jay Mathews, MD, MS, FACC
 Diagnosis and Endovascular Treatment of Critical Limb Ischemia: What You Need to Know S. Jay Mathews, MD, MS, FACC Interventional Cardiologist/Endovascular Specialist Bradenton Cardiology Center Bradenton,
Diagnosis and Endovascular Treatment of Critical Limb Ischemia: What You Need to Know S. Jay Mathews, MD, MS, FACC Interventional Cardiologist/Endovascular Specialist Bradenton Cardiology Center Bradenton,
Peripheral arterial disease for primary care Ed Aboian, MD
 Peripheral arterial disease for primary care Ed Aboian, MD Division of Vascular and Endovascular Surgery Palo Alto Medical Foundation, Burlingame Ca Disclosures Nothing to disclose Clinical presentation
Peripheral arterial disease for primary care Ed Aboian, MD Division of Vascular and Endovascular Surgery Palo Alto Medical Foundation, Burlingame Ca Disclosures Nothing to disclose Clinical presentation
Disclosures. In-Stent Restenosis: The Tail IS Wagging the Dog 4/15/2016. Restenosis: The Continuing Challenge for Peripheral Vascular Intervention
 In-Stent Restenosis: The Tail IS Wagging the Dog Disclosures NONE Michael S. Conte MD Division of Vascular and Endovascular Surgery UCSF Heart and Vascular Center UCSF Vascular Symposium 2016 IF YOU WERE
In-Stent Restenosis: The Tail IS Wagging the Dog Disclosures NONE Michael S. Conte MD Division of Vascular and Endovascular Surgery UCSF Heart and Vascular Center UCSF Vascular Symposium 2016 IF YOU WERE
Limb Salvage in Diabetic Ischemic Foot. Kritaya Kritayakirana, MD, FACS Assistant Professor Chulalongkorn University April 30, 2017
 Limb Salvage in Diabetic Ischemic Foot Kritaya Kritayakirana, MD, FACS Assistant Professor Chulalongkorn University April 30, 2017 Case Male 67 years old Underlying DM, HTN, TVD Present with gangrene
Limb Salvage in Diabetic Ischemic Foot Kritaya Kritayakirana, MD, FACS Assistant Professor Chulalongkorn University April 30, 2017 Case Male 67 years old Underlying DM, HTN, TVD Present with gangrene
Current Vascular and Endovascular Management in Diabetic Vasculopathy
 Current Vascular and Endovascular Management in Diabetic Vasculopathy Yang-Jin Park Associate professor Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine Peripheral artery
Current Vascular and Endovascular Management in Diabetic Vasculopathy Yang-Jin Park Associate professor Vascular Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine Peripheral artery
Will it heal? How to assess the probability of wound healing
 Will it heal? How to assess the probability of wound healing Richard F. Neville, M.D. Professor of Surgery Chief, Division of Vascular Surgery George Washington University Limb center case 69 yr old male
Will it heal? How to assess the probability of wound healing Richard F. Neville, M.D. Professor of Surgery Chief, Division of Vascular Surgery George Washington University Limb center case 69 yr old male
Perfusion Assessment in Chronic Wounds
 Perfusion Assessment in Chronic Wounds American Society of Podiatric Surgeons Surgical Conference September 22, 2018 Michael Maier, DPM, FACCWS Cardiovascular Medicine Cleveland Clinic Disclosures Speaker,
Perfusion Assessment in Chronic Wounds American Society of Podiatric Surgeons Surgical Conference September 22, 2018 Michael Maier, DPM, FACCWS Cardiovascular Medicine Cleveland Clinic Disclosures Speaker,
PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA. Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE
 PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE Disclosure Speaker name: DR. Manar Trab I have the following potential
PATIENT SPECIFIC STRATEGIES IN CRITICAL LIMB ISCHEMIA Dr. Manar Trab Consultant Vascular Surgeon European Vascular Clinic DMCC Dubai, UAE Disclosure Speaker name: DR. Manar Trab I have the following potential
Surgical Options for revascularisation P E T E R S U B R A M A N I A M
 Surgical Options for revascularisation P E T E R S U B R A M A N I A M The goal Treat pain Heal ulcer Preserve limb Preserve life The options Conservative Endovascular Surgical bypass Primary amputation
Surgical Options for revascularisation P E T E R S U B R A M A N I A M The goal Treat pain Heal ulcer Preserve limb Preserve life The options Conservative Endovascular Surgical bypass Primary amputation
Role of ABI in Detecting and Quantifying Peripheral Arterial Disease
 Role of ABI in Detecting and Quantifying Peripheral Arterial Disease Difference in AAA size between US and Surgeon 2 1 0-1 -2-3 0 1 2 3 4 5 6 7 Mean AAA size between US and Surgeon Kathleen G. Raman MD,
Role of ABI in Detecting and Quantifying Peripheral Arterial Disease Difference in AAA size between US and Surgeon 2 1 0-1 -2-3 0 1 2 3 4 5 6 7 Mean AAA size between US and Surgeon Kathleen G. Raman MD,
Endovascular Should Be Considered First Line Therapy
 Revascularization of Patients with Critical Limb Ischemia Endovascular Should Be Considered First Line Therapy Michael Conte David Dawson David L. Dawson, MD Revised Presentation Title A Selective Approach
Revascularization of Patients with Critical Limb Ischemia Endovascular Should Be Considered First Line Therapy Michael Conte David Dawson David L. Dawson, MD Revised Presentation Title A Selective Approach
Ron Fairman, MD Vice-President of the Society for Vascular Surgery MedCAC 2015
 Ron Fairman, MD Vice-President of the Society for Vascular Surgery MedCAC 2015 Ron Fairman, MD No Disclosures The SVS represents more than 5,000 practicing vascular surgeons across the US. The nation s
Ron Fairman, MD Vice-President of the Society for Vascular Surgery MedCAC 2015 Ron Fairman, MD No Disclosures The SVS represents more than 5,000 practicing vascular surgeons across the US. The nation s
Distal hybrids - an option in long SFA CTO accompanied by severely compromized crural runoff
 Distal hybrids - an option in long SFA CTO accompanied by severely compromized crural runoff P. Kuryanov, A. Lipin, A. Antropov, K. Atmadzas, A. Atmadzas, Y. Eminov, A. Borisov, R. Sobolev, A.Orlov Limb
Distal hybrids - an option in long SFA CTO accompanied by severely compromized crural runoff P. Kuryanov, A. Lipin, A. Antropov, K. Atmadzas, A. Atmadzas, Y. Eminov, A. Borisov, R. Sobolev, A.Orlov Limb
Guidelines for Management of Peripheral Arterial Disease
 Guidelines for Management of Peripheral Arterial Disease Subhash Banerjee, MD, FACC, FSCAI Professor of Medicine, Univ. of Texas Southwestern Medical Center Chief, Division of Cardiology, VA North Texas
Guidelines for Management of Peripheral Arterial Disease Subhash Banerjee, MD, FACC, FSCAI Professor of Medicine, Univ. of Texas Southwestern Medical Center Chief, Division of Cardiology, VA North Texas
Francisco Acín, César Varela, Ignacio López de Maturana, Joaquín de Haro, Silvia Bleda, and Javier Rodriguez-Padilla
 International Journal of Vascular Medicine, Article ID 27539, 13 pages http://dx.doi.org/1.1155/214/27539 Clinical Study Results of Infrapopliteal Endovascular Procedures Performed in Diabetic Patients
International Journal of Vascular Medicine, Article ID 27539, 13 pages http://dx.doi.org/1.1155/214/27539 Clinical Study Results of Infrapopliteal Endovascular Procedures Performed in Diabetic Patients
SUPERSUB Trial: 1-yr outcomes of SUPERa SUBintimal stenting in CLI Patients
 SUPERSUB Trial: 1-yr outcomes of SUPERa SUBintimal stenting in CLI Patients Dr. L.M. Palena, MD Interventional Radiology Unit Foot & Ankle Clinic Policlinico Abano Terme (PD), ITALY Disclosure I have the
SUPERSUB Trial: 1-yr outcomes of SUPERa SUBintimal stenting in CLI Patients Dr. L.M. Palena, MD Interventional Radiology Unit Foot & Ankle Clinic Policlinico Abano Terme (PD), ITALY Disclosure I have the
Evidence-Based Optimal Treatment for SFA Disease
 Evidence-Based Optimal Treatment for SFA Disease Endo first Don t burn surgical bridge Don t stent if possible Javairiah Fatima, MD Assistant Professor of Surgery Division of Vascular and Endovascular
Evidence-Based Optimal Treatment for SFA Disease Endo first Don t burn surgical bridge Don t stent if possible Javairiah Fatima, MD Assistant Professor of Surgery Division of Vascular and Endovascular
BEST-CLI Trial Study Concept and Current Status
 BEST-CLI Trial Study Concept and Current Status Kenneth Rosenfield, MD, MHCDS National Co-PI BEST-CLI Trial Section Head, Vascular Medicine and Intervention Institute for Heart, Vascular, and Stroke Care
BEST-CLI Trial Study Concept and Current Status Kenneth Rosenfield, MD, MHCDS National Co-PI BEST-CLI Trial Section Head, Vascular Medicine and Intervention Institute for Heart, Vascular, and Stroke Care
Managing Conditions Resulting from Untreated Cardiometabolic Syndrome
 Managing Conditions Resulting from Untreated Cardiometabolic Syndrome Matthew P. Namanny DO, FACOS Vascular/Endovascular Surgery Saguaro Surgical/AZ Vascular Specialist Tucson Medical Center Critical Limb
Managing Conditions Resulting from Untreated Cardiometabolic Syndrome Matthew P. Namanny DO, FACOS Vascular/Endovascular Surgery Saguaro Surgical/AZ Vascular Specialist Tucson Medical Center Critical Limb
Critical Limb Ischemia: Diagnosis and Current Management
 Research Article Joseph Karam, MD Elliot J. Stephenson, MD From: Minneapolis Heart Institutet at Abbott Northwestern Hospital, Minneapolis, MN Address for correspondence: Joseph Karam, MD Minneapolis Heart
Research Article Joseph Karam, MD Elliot J. Stephenson, MD From: Minneapolis Heart Institutet at Abbott Northwestern Hospital, Minneapolis, MN Address for correspondence: Joseph Karam, MD Minneapolis Heart
The SVS WIfI Classification: Does It Predict Amputation in Diabetic Patients?
 The SVS WIfI Classification: Does It Predict Amputation in Diabetic Patients? Christopher J. Abularrage, MD, FACS The Bertram M. Bernheim Associate Professor of Surgery Division of Vascular Surgery and
The SVS WIfI Classification: Does It Predict Amputation in Diabetic Patients? Christopher J. Abularrage, MD, FACS The Bertram M. Bernheim Associate Professor of Surgery Division of Vascular Surgery and
Clinical Approach to CLI and Related Diagnostics: What You Need to Know
 Clinical Approach to CLI and Related Diagnostics: What You Need to Know Ido Weinberg, MD Assistant Professor of Medicine Harvard Medical School Massachusetts General Hospital None Disclosures Critical
Clinical Approach to CLI and Related Diagnostics: What You Need to Know Ido Weinberg, MD Assistant Professor of Medicine Harvard Medical School Massachusetts General Hospital None Disclosures Critical
PUT YOUR BEST FOOT FORWARD
 PUT YOUR BEST FOOT FORWARD Bala Ramanan, MBBS 1 st year vascular surgery fellow Introduction The epidemic of diabetes and ageing of our population ensures critical limb ischemia will continue to grow.
PUT YOUR BEST FOOT FORWARD Bala Ramanan, MBBS 1 st year vascular surgery fellow Introduction The epidemic of diabetes and ageing of our population ensures critical limb ischemia will continue to grow.
PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014
 PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014 Van Crisco, MD, FACC, FSCAI First Coast Heart and Vascular Center, PLLC Jacksonville, FL 678-313-6695 Conflict of Interest Bayer Healthcare
PAD and CRITICAL LIMB ISCHEMIA: EVALUATION AND TREATMENT 2014 Van Crisco, MD, FACC, FSCAI First Coast Heart and Vascular Center, PLLC Jacksonville, FL 678-313-6695 Conflict of Interest Bayer Healthcare
Is there still any space left for DES in the BTK area??? (Angiolite BTK trial, 6 month Data)
") Is there still any space left for DES in the BTK area??? (Angiolite BTK trial, 6 month Data) (Angiolite BTK DES, IVascular) P. Goverde MD, K. Taeymans MD, K. Lauwers MD Vascular Clinic ZNA Antwerp,Belgium
Is there still any space left for DES in the BTK area??? (Angiolite BTK trial, 6 month Data) (Angiolite BTK DES, IVascular) P. Goverde MD, K. Taeymans MD, K. Lauwers MD Vascular Clinic ZNA Antwerp,Belgium
OMNIA case results: Lumee Oxygen measurements representative for CLI wound healing prognosis. M Werner 1 Feb 2018
 OMNIA case results: Lumee Oxygen measurements representative for CLI wound healing prognosis M Werner 1 Feb 2018 Disclosure Speaker name:... I have the following potential conflicts of interest to report:
OMNIA case results: Lumee Oxygen measurements representative for CLI wound healing prognosis M Werner 1 Feb 2018 Disclosure Speaker name:... I have the following potential conflicts of interest to report:
SPINACH Making Limb Salvage Salad from Spinach alone
 SPINACH Making Limb Salvage Salad from Spinach alone Surgical reconstruction versus Peripheral Intervention in patients with critical limb ischemia prospective multicenter registry in Japan Nobuyoshi Azuma,
SPINACH Making Limb Salvage Salad from Spinach alone Surgical reconstruction versus Peripheral Intervention in patients with critical limb ischemia prospective multicenter registry in Japan Nobuyoshi Azuma,
Imaging Strategy For Claudication
 Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
Who are the Debators? Imaging Strategy For Claudication Duplex Ultrasound Alone is Adequate to Select Patients for Endovascular Intervention - Pro: Dennis Bandyk MD No Disclosures PRO - Vascular Surgeon
My Diabetic Patient Has No Pulses; What Should I Do?
 Emily Malgor, MD Assistant Professor of Surgery University of Oklahoma, Oklahoma City My Diabetic Patient Has No Pulses; What Should I Do? There are no disclosures. Background Diabetes affects 387 million
Emily Malgor, MD Assistant Professor of Surgery University of Oklahoma, Oklahoma City My Diabetic Patient Has No Pulses; What Should I Do? There are no disclosures. Background Diabetes affects 387 million
Lower Extremity Artery: Physiologic Testing
 Master Title Ultrasound for Initial Evaluation of Lower Extremity Arterial Occlusive Disease: WHY? Gregory L. Moneta MD Professor and Chief Knight Cardiovascular Institute Division of Vascular Surgery
Master Title Ultrasound for Initial Evaluation of Lower Extremity Arterial Occlusive Disease: WHY? Gregory L. Moneta MD Professor and Chief Knight Cardiovascular Institute Division of Vascular Surgery
Pedal Bypass With Deep Venous Arterialization:
 Pedal Bypass With Deep Venous Arterialization: Long Term Result For Critical Limb Ischemia With Unreconstructable Distal Arteries Pramook Mutirangura Professor of Vascular Surgery Faculty of Medicine Siriraj
Pedal Bypass With Deep Venous Arterialization: Long Term Result For Critical Limb Ischemia With Unreconstructable Distal Arteries Pramook Mutirangura Professor of Vascular Surgery Faculty of Medicine Siriraj
USWR 23: Outcome Measure: Non Invasive Arterial Assessment of patients with lower extremity wounds or ulcers for determination of healing potential
 USWR 23: Outcome Measure: Non Invasive Arterial Assessment of patients with lower extremity wounds or ulcers for determination of healing potential MEASURE STEWARD: The US Wound Registry [Note: This measure
USWR 23: Outcome Measure: Non Invasive Arterial Assessment of patients with lower extremity wounds or ulcers for determination of healing potential MEASURE STEWARD: The US Wound Registry [Note: This measure
Current Status of Endovascular Therapies for Critical Limb Ischemia
 Current Status of Endovascular Therapies for Critical Limb Ischemia Bulent Arslan, MD Associate Professor of Radiology Director, Vascular & Interventional Radiology Rush University Medical Center bulent_arslan@rush.edu
Current Status of Endovascular Therapies for Critical Limb Ischemia Bulent Arslan, MD Associate Professor of Radiology Director, Vascular & Interventional Radiology Rush University Medical Center bulent_arslan@rush.edu
3-year results of the OLIVE registry:
 3-year results of the OLIVE registry: A prospective multicenter study in patients with critical limb ischemia Osamu Iida, MD Kansai Rosai Hospital Cardiovascular Center Amagasaki, Hyogo, Japan Disclosure
3-year results of the OLIVE registry: A prospective multicenter study in patients with critical limb ischemia Osamu Iida, MD Kansai Rosai Hospital Cardiovascular Center Amagasaki, Hyogo, Japan Disclosure
9/7/2018. Disclosures. CV and Limb Events in PAD. Challenges to Revascularization. Challenges. Answering the Challenge
 Disclosures State-of-the-Art Endovascular Lower Extremity Revascularization Promotional Speaker Jansen Pharmaceutical Promotional Speaker Amgen Pharmaceutical C. Michael Brown, MD, FACC al Cardiology Associate
Disclosures State-of-the-Art Endovascular Lower Extremity Revascularization Promotional Speaker Jansen Pharmaceutical Promotional Speaker Amgen Pharmaceutical C. Michael Brown, MD, FACC al Cardiology Associate
Use of Laser In BTK Disease (CLI)
") Use of Laser In BTK Disease (CLI) Click to edit academic affiliation, practice or hospital logo(s) of preference. Product and/or sponsor logos not permitted, per CME guidelines. Richard Kovach, MD, FACC,
Use of Laser In BTK Disease (CLI) Click to edit academic affiliation, practice or hospital logo(s) of preference. Product and/or sponsor logos not permitted, per CME guidelines. Richard Kovach, MD, FACC,
Endovascular Is The Way To Go: Revascularize As Many Vessels As You Can
 Rafael Malgor, MD Assistant Professor of Surgery The University of Oklahoma, Tulsa Endovascular Is The Way To Go: Revascularize As Many Vessels As You Can Background Lower extremity anatomy (below the
Rafael Malgor, MD Assistant Professor of Surgery The University of Oklahoma, Tulsa Endovascular Is The Way To Go: Revascularize As Many Vessels As You Can Background Lower extremity anatomy (below the
Lower Extremity Peripheral Arterial Disease: Less is Sometimes More. Spence M Taylor, M.D.
 Lower Extremity Peripheral Arterial Disease: Less is Sometimes More Spence M Taylor, M.D. President, Greenville Health System Clinical University Senior Associate Dean for Academic Affairs and Diversity
Lower Extremity Peripheral Arterial Disease: Less is Sometimes More Spence M Taylor, M.D. President, Greenville Health System Clinical University Senior Associate Dean for Academic Affairs and Diversity
Are RCT always needed: Experience with objective performance criteria (OPC)
") Are RCT always needed: Experience with objective performance criteria (OPC) Peter A. Schneider, MD Krishna Rocha-Singh, MD Kaiser Foundation Hospital Honolulu, Hawaii Prarie Heart Institute Springfield,
Are RCT always needed: Experience with objective performance criteria (OPC) Peter A. Schneider, MD Krishna Rocha-Singh, MD Kaiser Foundation Hospital Honolulu, Hawaii Prarie Heart Institute Springfield,
Distal By-Pass procedures can reduce limb loss
 Conventional treatment of the diabetic foot Distal By-Pass procedures can reduce limb loss Dr. Nikolaos Melas, PhD Vascular and Endovascular Surgeon Military Doctor Associate in 1st department of Surgery,
Conventional treatment of the diabetic foot Distal By-Pass procedures can reduce limb loss Dr. Nikolaos Melas, PhD Vascular and Endovascular Surgeon Military Doctor Associate in 1st department of Surgery,
Intercepting PAD. Playbook for Cardiovascular Care 2018 February 24, Jonathan D Woody, MD, FACS. University Surgical Vascular
 Intercepting PAD Playbook for Cardiovascular Care 2018 February 24, 2018 Jonathan D Woody, MD, FACS University Surgical Vascular Attending Vascular Surgeon - Piedmont Athens Regional Adjunct Clinical Associate
Intercepting PAD Playbook for Cardiovascular Care 2018 February 24, 2018 Jonathan D Woody, MD, FACS University Surgical Vascular Attending Vascular Surgeon - Piedmont Athens Regional Adjunct Clinical Associate
The present status of selfexpanding. for CLI: Why and when to use. Sean P Lyden MD Cleveland Clinic Cleveland, Ohio
 The present status of selfexpanding and balloonexpandable tibial BMS and DES for CLI: Why and when to use Sean P Lyden MD Cleveland Clinic Cleveland, Ohio Disclosure Speaker name: Sean Lyden, MD I have
The present status of selfexpanding and balloonexpandable tibial BMS and DES for CLI: Why and when to use Sean P Lyden MD Cleveland Clinic Cleveland, Ohio Disclosure Speaker name: Sean Lyden, MD I have
4/23/2009. Vein Bypass Remains the Gold Standard AND We Can Improve Outcomes. Lower Extremity Revascularization Options: Key Factors to Consider
 Vein Bypass Remains the Gold Standard AND We Can Improve Outcomes Lower Extremity Revascularization Options: Key Factors to Consider General health of the patient Michael S. Conte MD Division of Vascular
Vein Bypass Remains the Gold Standard AND We Can Improve Outcomes Lower Extremity Revascularization Options: Key Factors to Consider General health of the patient Michael S. Conte MD Division of Vascular
DCB in my practice: How the evidence influences my strategy. Yang-Jin Park
 DCB in my practice: How the evidence influences my strategy Yang-Jin Park Associate Professor Division of Vascular Surgery, Department of Surgery Samsung Medical Center Sungkyunkwan University School of
DCB in my practice: How the evidence influences my strategy Yang-Jin Park Associate Professor Division of Vascular Surgery, Department of Surgery Samsung Medical Center Sungkyunkwan University School of
National Clinical Conference 2018 Baltimore, MD
 National Clinical Conference 2018 Baltimore, MD No relevant financial relationships to disclose Wound Care Referral The patient has been maximized from a vascular standpoint. She has no other options.
National Clinical Conference 2018 Baltimore, MD No relevant financial relationships to disclose Wound Care Referral The patient has been maximized from a vascular standpoint. She has no other options.
EVALUATION OF THE VASCULAR STATUS OF DIABETIC WOUNDS Travis Littman, MD NorthWest Surgical Specialists
 EVALUATION OF THE VASCULAR STATUS OF DIABETIC WOUNDS Travis Littman, MD NorthWest Surgical Specialists Nothing To Disclosure DISCLOSURES I have no outside conflicts of interest, financial incentives, or
EVALUATION OF THE VASCULAR STATUS OF DIABETIC WOUNDS Travis Littman, MD NorthWest Surgical Specialists Nothing To Disclosure DISCLOSURES I have no outside conflicts of interest, financial incentives, or
Garland Green, MD Interventional Cardiologist. Impact of PAD: Prevalence, Risk Factors, Testing, and Medical Management
 Garland Green, MD Interventional Cardiologist Impact of PAD: Prevalence, Risk Factors, Testing, and Medical Management Peripheral Arterial Disease Affects over 8 million Americans Affects 12% of the general
Garland Green, MD Interventional Cardiologist Impact of PAD: Prevalence, Risk Factors, Testing, and Medical Management Peripheral Arterial Disease Affects over 8 million Americans Affects 12% of the general
Update on Tack Optimized Balloon Angioplasty (TOBA) Below the Knee. Marianne Brodmann, MD Medical University Graz Graz, Austria
 Below the Knee. Marianne Brodmann, MD Medical University Graz Graz, Austria") Update on Tack Optimized Balloon Angioplasty (TOBA) Below the Knee Marianne Brodmann, MD Medical University Graz Graz, Austria Critical Limb Ischemia Infrapopliteal arterial disease is a leading source
Update on Tack Optimized Balloon Angioplasty (TOBA) Below the Knee Marianne Brodmann, MD Medical University Graz Graz, Austria Critical Limb Ischemia Infrapopliteal arterial disease is a leading source
Vascular screening in diabetic patients: how aggressive should we be and when to intervene?
 Vascular screening in diabetic patients: how aggressive should we be and when to intervene? Roberto Ferraresi Peripheral Interventional Unit Bergamo Italy Disclosure Speaker name: ROBERTO FERRARESI X X
Vascular screening in diabetic patients: how aggressive should we be and when to intervene? Roberto Ferraresi Peripheral Interventional Unit Bergamo Italy Disclosure Speaker name: ROBERTO FERRARESI X X
Arterial Studies And The Diabetic Foot Patient
 Arterial Studies And The Patient George L. Berdejo, BA, RVT, FSVU gberdejo@wphospital.org Disclosures I have nothing to disclose! Diabetes mellitus continues to grow in global prevalence and to consume
Arterial Studies And The Patient George L. Berdejo, BA, RVT, FSVU gberdejo@wphospital.org Disclosures I have nothing to disclose! Diabetes mellitus continues to grow in global prevalence and to consume
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS
 VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
VASCULAR DISEASE: THREE THINGS YOU SHOULD KNOW JAMES A.M. SMITH, D.O. KANSAS VASCULAR MEDICINE, P.A. WICHITA, KANSAS KANSAS ASSOCIATION OF OSTEOPATHIC MEDICINE ANNUAL CME CONVENTION APRIL 13, 2018 THREE
Non-invasive examination
 Non-invasive examination Segmental pressure and Ankle-Brachial Index (ABI) The segmental blood pressure (SBP) examination is a simple, noninvasive method for diagnosing and localizing arterial disease.
Non-invasive examination Segmental pressure and Ankle-Brachial Index (ABI) The segmental blood pressure (SBP) examination is a simple, noninvasive method for diagnosing and localizing arterial disease.
CRITICAL LIMB ISCHEMIA UNITED STATES EPIDEMIOLOGY TABLE OF CONTENTS
 CRITICAL LIMB ISCHEMIA UNITED STATES EPIDEMIOLOGY TABLE OF CONTENTS CRITICAL LIMB ISCHEMIA... 1 CONCLUSION... 9 U.S. CRITICAL LIMB ISCHEMIA PREVALENCE... 9 MARKET OPPORTUNITY ENDOVASCULAR... 9 MARKET OPPORTUNITY
CRITICAL LIMB ISCHEMIA UNITED STATES EPIDEMIOLOGY TABLE OF CONTENTS CRITICAL LIMB ISCHEMIA... 1 CONCLUSION... 9 U.S. CRITICAL LIMB ISCHEMIA PREVALENCE... 9 MARKET OPPORTUNITY ENDOVASCULAR... 9 MARKET OPPORTUNITY
Aggressive BTK Revascularization and Advanced Wound Care - Patient Specific Therapy Concepts
 Aggressive BTK Revascularization and Advanced Wound Care - Patient Specific Therapy Concepts Dr Steven Kum MBBS MMed FRCS FAMS Vascular & Endovascular Surgeon Vascular Centre Department of Surgery Changi
Aggressive BTK Revascularization and Advanced Wound Care - Patient Specific Therapy Concepts Dr Steven Kum MBBS MMed FRCS FAMS Vascular & Endovascular Surgeon Vascular Centre Department of Surgery Changi
PAD Characterization Within A Healthcare System" RAPID Face-to-Face Meeting Schuyler Jones, MD September 14, 2016
 PAD Characterization Within A Healthcare System" RAPID Face-to-Face Meeting Schuyler, MD September 14, 2016 Interventional Cardiology and Cath Labs Disclosures Research Grants: Agency for Healthcare Research
PAD Characterization Within A Healthcare System" RAPID Face-to-Face Meeting Schuyler, MD September 14, 2016 Interventional Cardiology and Cath Labs Disclosures Research Grants: Agency for Healthcare Research
Disclosures. Tips and Tricks for Tibial Intervention. Tibial intervention overview
 Tips and Tricks for Tibial Intervention Donald L. Jacobs, MD C Rollins Hanlon Endowed Professor and Chair Chair of Surgery Saint Louis University SSM-STL Saint Louis University Hospital Disclosures Abbott
Tips and Tricks for Tibial Intervention Donald L. Jacobs, MD C Rollins Hanlon Endowed Professor and Chair Chair of Surgery Saint Louis University SSM-STL Saint Louis University Hospital Disclosures Abbott
Introduction. Risk factors of PVD 5/8/2017
 PATHOPHYSIOLOGY AND CLINICAL FEATURES OF PERIPHERAL VASCULAR DISEASE Dr. Muhamad Zabidi Ahmad Radiologist and Section Chief, Radiology, Oncology and Nuclear Medicine Section, Advanced Medical and Dental
PATHOPHYSIOLOGY AND CLINICAL FEATURES OF PERIPHERAL VASCULAR DISEASE Dr. Muhamad Zabidi Ahmad Radiologist and Section Chief, Radiology, Oncology and Nuclear Medicine Section, Advanced Medical and Dental
Nurse and Technician Forum Part II Critical Limb Ischemia: Optimal care, an interdisciplinary challenge
 L E I P Z I G I N T E R V E N T I O N A L C O U R S E 2017 Nurse and Technician Forum Part II Critical Limb Ischemia: Optimal care, an interdisciplinary challenge Markus Haumer Landesklinikum Baden-Mödling
L E I P Z I G I N T E R V E N T I O N A L C O U R S E 2017 Nurse and Technician Forum Part II Critical Limb Ischemia: Optimal care, an interdisciplinary challenge Markus Haumer Landesklinikum Baden-Mödling
Infection/ischaemia/amputation: how to build a multidisciplinary center for limb salvage
 Infection/ischaemia/amputation: how to build a multidisciplinary center for limb salvage Roberto Ferraresi Peripheral Interventional Unit Bergamo Italy ferraresi.md@gmail.com Disclosure Roberto Ferraresi,
Infection/ischaemia/amputation: how to build a multidisciplinary center for limb salvage Roberto Ferraresi Peripheral Interventional Unit Bergamo Italy ferraresi.md@gmail.com Disclosure Roberto Ferraresi,
FOR THE 18 MILLION INDIVIDUALS with diabetes mellitus in
 11 Evaluation and Management of Peripheral Arterial Disease Joseph L. Mills, Sr., MD FOR THE 18 MILLION INDIVIDUALS with diabetes mellitus in the United States, foot problems ulceration, infection, and
11 Evaluation and Management of Peripheral Arterial Disease Joseph L. Mills, Sr., MD FOR THE 18 MILLION INDIVIDUALS with diabetes mellitus in the United States, foot problems ulceration, infection, and
Recommendations for Follow-up After Vascular Surgery Arterial Procedures SVS Practice Guidelines
 Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Access strategy for chronic total occlusions (CTOs) is crucial
 is crucial") Learn How Access Strategy Impacts Complex CTO Crossing Arthur C. Lee, MD The Cardiac & Vascular Institute, Gainesville, Florida VASCULAR DISEASE MANAGEMENT 2018;15(3):E19-E23. Key words: chronic total
Learn How Access Strategy Impacts Complex CTO Crossing Arthur C. Lee, MD The Cardiac & Vascular Institute, Gainesville, Florida VASCULAR DISEASE MANAGEMENT 2018;15(3):E19-E23. Key words: chronic total
Larry Diaz, MD, FSCAI Mehdi H. Shishehbor, DO, FSCAI
 PAD Diagnosis Larry Diaz, MD, FSCAI Metro Health / University of Michigan Health, Wyoming, MI Mehdi H. Shishehbor, DO, FSCAI University Hospitals Harrington Heart & Vascular Institute, Cleveland, OH PAD:
PAD Diagnosis Larry Diaz, MD, FSCAI Metro Health / University of Michigan Health, Wyoming, MI Mehdi H. Shishehbor, DO, FSCAI University Hospitals Harrington Heart & Vascular Institute, Cleveland, OH PAD:
6/6/2016. Pedal Loop Reconstruction: A Crash Course in 60 minutes. Pedal-Plantar Anatomy. Anand Prasad, MD, FACC, FSCAI, RPVI.
 6/6/2016 Pedal Loop Reconstruction: A Crash Course in 60 minutes Pedal-Plantar Anatomy Anand Prasad, MD, FACC, FSCAI, RPVI Associate Professor of Medicine Freeman Heart Association Endowed Professor in
6/6/2016 Pedal Loop Reconstruction: A Crash Course in 60 minutes Pedal-Plantar Anatomy Anand Prasad, MD, FACC, FSCAI, RPVI Associate Professor of Medicine Freeman Heart Association Endowed Professor in
Step by step Hybrid procedures in peripheral obstructive disease. Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery
 Step by step Hybrid procedures in peripheral obstructive disease Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name: H.H. Staab I have the following
Step by step Hybrid procedures in peripheral obstructive disease Holger Staab, MD University Hospital Leipzig, Germany Clinic for Vascular Surgery Disclosure Speaker name: H.H. Staab I have the following
Angiosome revascularization strategies in real world practice: how much difference does it make?
 Angiosome revascularization strategies in real world practice: how much difference does it make? Peter A. Schneider, MD Kaiser Foundation Hospital Honolulu, Hawaii Disclosure Peter A. Schneider... I have
Angiosome revascularization strategies in real world practice: how much difference does it make? Peter A. Schneider, MD Kaiser Foundation Hospital Honolulu, Hawaii Disclosure Peter A. Schneider... I have
Fluorescence Angiography in Limb Salvage
 Fluorescence Angiography in Limb Salvage Ryan H. Fitzgerald, DPM, FACFAS Associate Professor of Surgery-University Of South Carolina School of Medicine, Greenville Etiology of Lower extremity wounds Neuropathy
Fluorescence Angiography in Limb Salvage Ryan H. Fitzgerald, DPM, FACFAS Associate Professor of Surgery-University Of South Carolina School of Medicine, Greenville Etiology of Lower extremity wounds Neuropathy
The Final Triumph Of Endovascular Therapy In SFA Treatment
 The Final Triumph Of Endovascular Therapy In SFA Treatment MEET 07 Mark W. Mewissen, M.D. Director, St Lukes Vascular Center Milwaukee, WI Endovascular Therapy In SFA Treatment: Works In Progress! Mark
The Final Triumph Of Endovascular Therapy In SFA Treatment MEET 07 Mark W. Mewissen, M.D. Director, St Lukes Vascular Center Milwaukee, WI Endovascular Therapy In SFA Treatment: Works In Progress! Mark
Disclosures. Objectives. Bypass vs. Endo for SFA Disease: Reaching Consensus on a Rational Approach. Christopher D. Owens, MD 4/23/2009
 Disclosures Bypass vs. Endo for SFA Disease: Reaching Consensus on a Rational Approach No disclosures No conflicts of interest Christopher D. Owens, MD Objectives Changing face of our patients presenting
Disclosures Bypass vs. Endo for SFA Disease: Reaching Consensus on a Rational Approach No disclosures No conflicts of interest Christopher D. Owens, MD Objectives Changing face of our patients presenting
How to manage leg ulcers in the elderly
 How to manage leg ulcers in the elderly David Riding Clinical Research Fellow / Specialty Registrar in Vascular Surgery University of Manchester / MFT British Geriatric Society Trainees Meeting 2018 Objectives
How to manage leg ulcers in the elderly David Riding Clinical Research Fellow / Specialty Registrar in Vascular Surgery University of Manchester / MFT British Geriatric Society Trainees Meeting 2018 Objectives
Now That You Have the Tools
 blockosu@gmail.com Now That You Have the Tools Alan Jay Block, DPM, MS, FASPS, FACFAS Assistant Professor Dept Of Orthopeadics The Ohio State University Medical Board Kent State University Editor-in -Chief
blockosu@gmail.com Now That You Have the Tools Alan Jay Block, DPM, MS, FASPS, FACFAS Assistant Professor Dept Of Orthopeadics The Ohio State University Medical Board Kent State University Editor-in -Chief
The relation of 2D perfusion angiography after BTK intervention and wound healing in patient with CLI - Single center prospective study -
 The relation of 2D perfusion angiography after BTK intervention and wound healing in patient with CLI - Single center prospective study - Shinya Sasaki, MD. Saka General Hospital Miyagi, JAPAN Disclosure
The relation of 2D perfusion angiography after BTK intervention and wound healing in patient with CLI - Single center prospective study - Shinya Sasaki, MD. Saka General Hospital Miyagi, JAPAN Disclosure
Peripheral Arterial Disease: Who has it and what to do about it?
 Peripheral Arterial Disease: Who has it and what to do about it? Seth Krauss, M.D. Alaska Annual Nurse Practitioner Conference September 16, 2011 Scope of the Problem Incidence: 20%
Peripheral Arterial Disease: Who has it and what to do about it? Seth Krauss, M.D. Alaska Annual Nurse Practitioner Conference September 16, 2011 Scope of the Problem Incidence: 20%
Boca Raton Regional Hospital Grand Rounds September 13, 2016
 Boca Raton Regional Hospital Grand Rounds September 13, 2016 W. Anthony Lee, MD, FACS Chief, BocaCare Vascular Surgery Christine E. Lynn Heart and Vascular Institute Boca Raton, Florida Disclosures No
Boca Raton Regional Hospital Grand Rounds September 13, 2016 W. Anthony Lee, MD, FACS Chief, BocaCare Vascular Surgery Christine E. Lynn Heart and Vascular Institute Boca Raton, Florida Disclosures No
Chronic lower Extremity Peripheral Arterial Disease: The Relentless Pursuit of Mediocrity
 Chronic lower Extremity Peripheral Arterial Disease: The Relentless Pursuit of Mediocrity Spence M Taylor, MD Assistant Dean for Academic Affairs Greenville Hospital System University Medical Center, Chairman
Chronic lower Extremity Peripheral Arterial Disease: The Relentless Pursuit of Mediocrity Spence M Taylor, MD Assistant Dean for Academic Affairs Greenville Hospital System University Medical Center, Chairman