Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation
|
|
|
- Gregory Wright
- 5 years ago
- Views:
Transcription
1 Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015


2 G O lobal Initiative for Chronic bstructive L D ung isease
. Limited body of data Nonrandomized trials Observational studies.")
3 Description of Levels of Evidence Evidence Category A B C D Sources of Evidence Randomized controlled trials (RCTs). Rich body of data Randomized controlled trials (RCTs). Limited body of data Nonrandomized trials Observational studies. Panel consensus judgment
4 Definition of COPD COPD, a common preventable and treatable disease, is characterized by persistent airflow limitation that is usually progressive and associated with an enhanced chronic inflammatory response in the airways and the lung to noxious particles or gases. Exacerbations and comorbidities contribute to the overall severity in individual patients.

5 Mechanisms Underlying Airflow Limitation in COPD Small Airways Disease Airway inflammation Airway fibrosis, luminal plugs Increased airway resistance Parenchymal Destruction Loss of alveolar attachments Decrease of elastic recoil AIRFLOW LIMITATION
6 Heterogeneity of COPD - Genetic Phenotypes - Although smoking is the major risk factor for the development of COPD, the development of airflow obstruction in smokers is highly variable. Severe 1 antitrypsin deficiency is a proven genetic risk factor for COPD. - Familial aggregation of airflow obstruction within families of COPD patients has also been demonstrated. - A recent association study comprising 8300 patients and 7 separate cohorts found that a minor allele SNP of MMP12 (rs ) associated with decreased MMP-12 expression has a positive effect on lung function in children with asthma and in adult smokers. - Recent genome-wide association studies have identified several COPD loci, including a region near the hedgehog interacting protein (HHIP) gene on chromosome 4 and a cluster of genes on chromosome 15 that likely contain COPD susceptibility determinants. - Barreiro E. Update in Chronic Obstructive Pulmonary Disease Am J Respir Crit Care Med 2014;189:
7 Heterogeneity of COPD - Allergy Phenotypes: - In the National Health and Nutrition Survey III (NHANES III), individuals with an allergic phenotype were more likely to wheeze and have chronic cough and phlegm and increased risk of exacerbations. - In the COPD and Domestic Endotoxin (CODE) cohort, sensitized subjects reported more wheeze, coughinduced nocturnal awakenings and exacerbations and acute health visits. - Active allergic symptoms may worsen the course of COPD. - Allergen avoidance or pharmacologic treatment of allergic disease is warranted in specific subjects with COPD. - Barreiro E. Update in Chronic Obstructive Pulmonary Disease Am J Respir Crit Care Med 2014;189:
8 Heterogeneity of COPD
9 Heterogeneity of COPD - Clinical Phenotypes COPD: clinical phenotypes
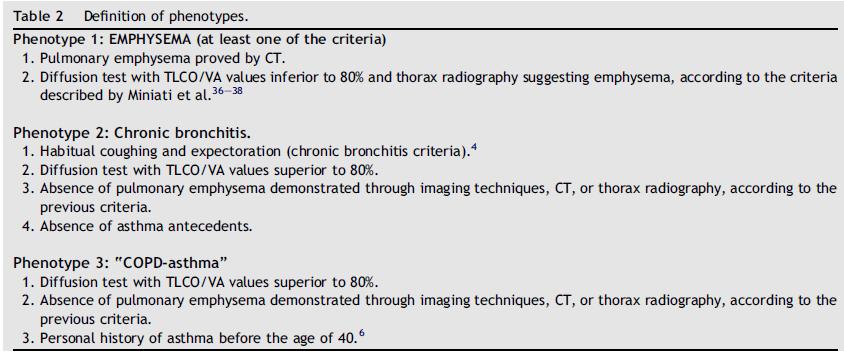
10 Heterogeneity of COPD - Clinical Phenotypes - Soriano JB. Chest. 2003;124(2): Non-proportional Venn diagram of COPD showing subsets of patients with chronic bronchitis, emphysema, and asthma. The subsets comprising COPD are shaded. Patients with asthma whose airflow obstruction is completely reversible (9) are not considered to have COPD. Patients with unremitting asthma are classified as having COPD (6, 7, and 8). Chronic bronchitis and emphysema with airflow obstruction usually occur together (5), and some patients may have asthma associated with these two disorders (8).
.")
11 Heterogeneity of COPD - Clinical Phenotypes - Soriano JB. Chest. 2003;124(2): Those with asthma, exposed to cigarette smoke, may develop chronic productive cough, which is a feature of chronic bronchitis (6). Such patients often are referred as having asthmatic bronchitis or the asthmatic form of COPD. Persons with chronic bronchitis and/or emphysema without airflow obstruction (1, 2, and 11) are not classified as having COPD. Patients with airway obstruction due to diseases with other specific pathology, e.g., cystic fibrosis or obliterative bronchiolitis (10), are not included in this definition.

12 Type 1 Type 2 Type 3 COPD-asthma: 12.1% CB: 44.7% E: 43.2%
13 Heterogeneity of COPD FEV1 (forced expiratory volume in 1 sec) is the hallmark of COPD because it is affected by inflammation and remodeling of the small airways as well as by emphysematous destruction of the terminal airspaces; however, defining a disease as COPD so heterogeneous exclusively based on the patient s FEV1 may not always be adequate.. - Coxson HO. Using Pulmonary Imaging to Move COPD Beyond FEV1. Am J Respir Crit Care Med 2014 May 29.
14 Heterogeneity of COPD COPD is a diverse disease with many clinical, radiological, and genomic features that may designate several different phenotypes that may have prognostic as well as therapeutic implications. Chest CT uses lung structure to characterize the COPD population into emphysema or airwaypredominant phenotypes that may provide keen insight into disease progression and response to therapy.. - Barreiro E. Update in Chronic Obstructive Pulmonary Disease Am J Respir Crit Care Med 2014;189:


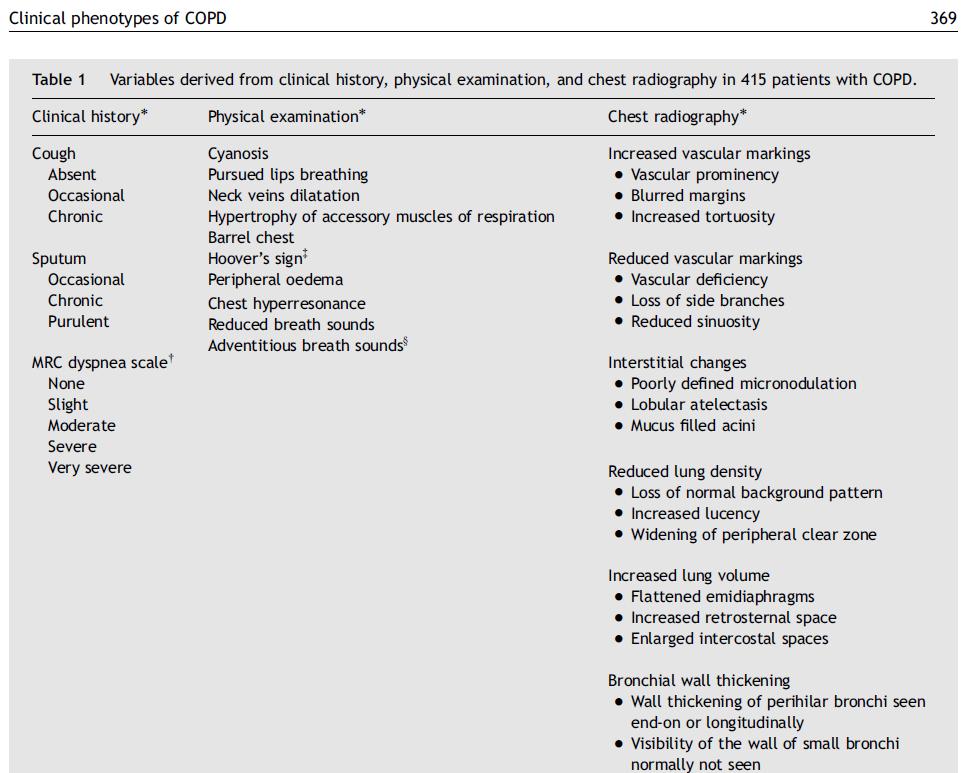
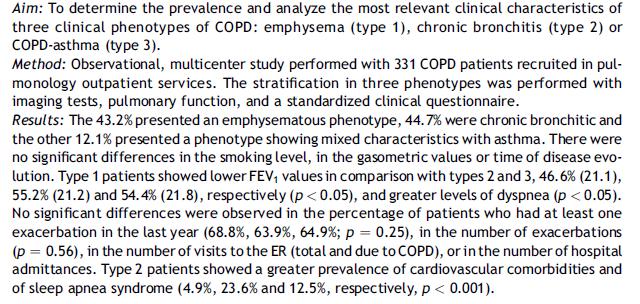
15 Heterogeneity of COPD Radiological phenotypes: Emphysema-predominant and airway-predominant E A M - Pistolesi M. Identification of a predominant COPD phenotype in clinical practice. Respir Med. 2008;102(3):
16 Heterogeneity of COPD

17 Heterogeneity of COPD - Stable moderate-to-severe COPD patients A : absence or with little emphysema but with or without bronchial wall thickening (BWT); E : emphysema without BWT; M : mixed type, emphysema with BWT - Kitaguchi Y. Characteristics of COPD phenotypes classified according to the findings of HRCT. Respir Med. 2006;100(10):

18 Heterogeneity of COPD - Kitaguchi Y. Characteristics of COPD phenotypes classified according to the findings of HRCT. Respir Med. 2006;100(10):
19 Heterogeneity of COPD
20 Heterogeneity of COPD
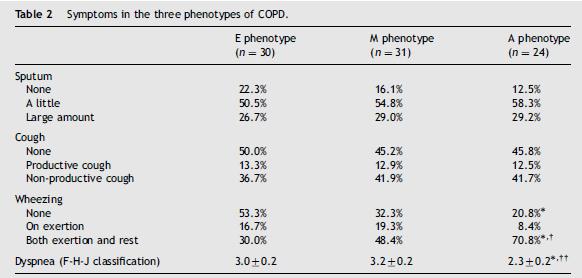
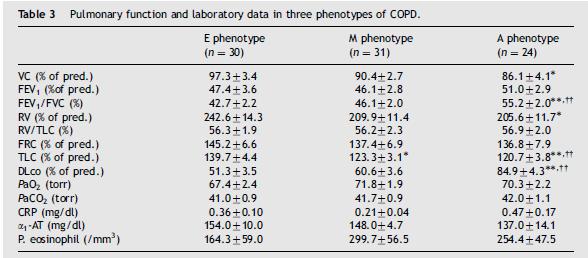
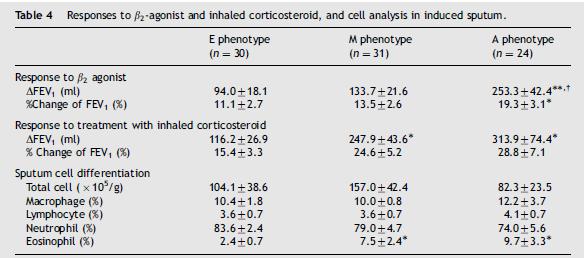
21 Heterogeneity of COPD The A type showed a higher prevalence of non-smoker and patients with wheezing both on exertion and at rest, higher values of DL CO, milder lung hyperinflation, and greater reversibility of airflow obstruction responsive to inhaled 2- agonist as compared with the E phenotype. The E type showed a significantly lower preference of BMI, declined DL CO, and poor response to inhaled 2-agnoist among three groups. The M type showed a higher prevalence of patients complaining of large amounts of sputum, productive cough and wheezing not only on exertion but also at rest, higher rate of acute exacerbation or hospitalization and greater reversibility of airflow obstruction responsive to inhaled 2-agnoist as compared with the E phenotype. - Kitaguchi Y. Characteristics of COPD phenotypes classified according to the findings of HRCT. Respir Med. 2006;100(10):
22 Heterogeneity of COPD The degree of emphysema was significantly associated with Brinkman (smoking) index, lower BMI, a decrease in DL CO, lower FEV1/FVC values. The presence of bronchial wall thickening in A - and M - phenotype was significantly associated with reversibility responsive to treatment with inhaled corticosteroid and sputum eosinophilia. These findings indicated that the morphological phenotypes of COPD classified according to dominancy of emphysema and the presence of BWT showed several clinical characteristics and different bronchodilator responses. - Kitaguchi Y. Characteristics of COPD phenotypes classified according to the findings of HRCT. Respir Med. 2006;100(10):

23 Heterogeneity of COPD COPD with E: - More severe PFT - More airway inflammation - Serious systemic dysfunction COPD with BE - Probable pathogenic bacterial culture - AE/year - Mortality COPD with BWT - Correlate with reversibility to BD - Bafadhel M. The role of CT scanning in multidimensional phenotyping of COPD. Chest. 2011;140(3):


24 Global Strategy for Diagnosis, Management and Prevention of COPD, 2014: Chapters Definition and Overview Diagnosis and Assessment Therapeutic Options Manage Stable COPD Manage Exacerbations Manage Comorbidities Updated 2014 Asthma COPD Overlap Syndrome (ACOS)
25 Diagnosis and Assessment: Key Points A clinical diagnosis of COPD should be considered in any patient who has dyspnea, chronic cough or sputum production, and a history of exposure to risk factors for the disease. Spirometry is required to make the diagnosis; the presence of a post-bronchodilator FEV 1 /FVC < 0.70 confirms the presence of persistent airflow limitation and thus of COPD.
26 Diagnosis and Assessment: Key Points The goals of COPD assessment are to determine the severity of the disease, including (1) the severity of airflow limitation, (2) the impact on the patient s health status, and (3) the risk of future exacerbations, in order to guide therapy. The risk of future exacerbations: estimated by the severity of airflow limitation and the history of previous exacerbations. Comorbidities occur frequently in COPD patients, and should be actively looked for and treated appropriately if present.


27 Diagnosis of COPD SYMPTOMS shortness of breath chronic cough sputum EXPOSURE TO RISK FACTORS tobacco occupation indoor/outdoor pollution SPIROMETRY: Required to establish diagnosis
28 Assessment of Airflow Limitation: Spirometry Spirometry should be performed after the administration of an adequate dose of a shortacting inhaled bronchodilator to minimize variability. A post-bronchodilator FEV 1 /FVC < 0.70 confirms the presence of airflow limitation. Where possible, values should be compared to age-related normal values to avoid overdiagnosis of COPD in the elderly.
29 Spirometry: Normal Trace Showing FEV 1 and FVC 5 FVC Volume, liters FEV 1 = 4L FVC = 5L FEV 1 /FVC = Time, sec
30 Spirometry: Obstructive Disease 5 Normal 4 Volume, liters FEV 1 = 1.8L FVC = 3.2L FEV 1 /FVC = 0.56 Obstructive Time, seconds
31 Assessment of COPD: Goals Determine the severity of the disease, its impact on the patient s health status and the risk of future events (for example exacerbations) to guide therapy. Consider the following aspects of the disease separately: current level of patient s symptoms severity of the spirometric abnormality frequency of exacerbations presence of comorbidities. S-S-E-C

32 Assessment of COPD Assess symptoms Assess degree of airflow limitation using spirometry Assess risk of exacerbations Assess comorbidities
33 Symptoms of COPD The characteristic symptoms of COPD are chronic and progressive dyspnea, cough, and sputum production that can be variable from day-to-day. Dyspnea: Progressive, persistent and characteristically worse with exercise. Chronic cough: May be intermittent and may be unproductive. Chronic sputum production: COPD patients commonly cough up sputum.
 or mmrc Breathlessness scale")
34 Assessment of COPD Assess symptoms: Assess degree of airflow limitation using spirometry COPD Assessment Test (CAT) Assess risk of exacerbations Assess comorbidities or Clinical COPD Questionnaire (CCQ) or mmrc Breathlessness scale
35 Assessment of Symptoms COPD Assessment Test (CAT): An 8-item measure of health status impairment in COPD ( Clinical COPD Questionnaire (CCQ): Selfadministered questionnaire developed to measure clinical control in patients with COPD (


36 The equivalent cutpoint for the CAT is 10
37 CCQ questionnaire Calculation of scores: CCQ total score = (item )/10; Symptom = (item )/4; Functional state = (item )/4; Mental state = (item 3 + 4)/2. The equivalent cutpoint for the CCQ is
 Questionnaire: - relates well to other measures of health status and predicts future mortality")
38 Assessment of Symptoms Breathlessness Measurement using the Modified British Medical Research Council (mmrc) Questionnaire: - relates well to other measures of health status and predicts future mortality risk.
39 Modified MRC (mmrc) Questionnaire Less breathlessness More breathlessness

40 Assessment of COPD Assess symptoms Assess degree of airflow limitation using spirometry Assess risk of exacerbations Use spirometry for grading severity Assess comorbidities according to spirometry, using four grades split at 80%, 50% and 30% of predicted value
41 Classification of Severity of Airflow Limitation in COPD* In patients with FEV 1 /FVC < 0.70: GOLD 1: Mild GOLD 2: Moderate GOLD 3: Severe FEV 1 > 80% predicted 50% < FEV 1 < 80% predicted 30% < FEV 1 < 50% predicted GOLD 4: Very Severe FEV 1 < 30% predicted *Based on Post-Bronchodilator FEV 1

42 - Jones PW. Health status and the spiral of decline. COPD 2009;6(1):59-63.

43 Assessment of COPD Assess symptoms Assess degree of airflow limitation using spirometry Assess risk of exacerbations Assess comorbidities An exacerbation of COPD is defined as an acute event characterized by a worsening of the patient s respiratory symptoms that is beyond normal day-to-day variations and leads to a change in medication.

44 Assess Risk of Exacerbations To assess risk of exacerbations use history of exacerbations and spirometry: Two or more exacerbations within the last year or an FEV 1 < 50 % of predicted value are indicators of high risk. One or more hospitalizations for COPD exacerbation should be considered high risk.
45 Exacerbations increase the decline in lung function, deterioration in health status and risk of death, the assessment of exacerbation risk can also be seen as an assessment of the risk of poor outcomes in general.
46 Combined Assessment of COPD Assess symptoms Assess degree of airflow limitation using spirometry Assess risk of exacerbations Combine these assessments for the purpose of improving management of COPD
47 Risk (GOLD Classification of Airflow Limitation)) Risk (Exacerbation history) Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD 4 3 (C) (D) 2 or > 1 leading to hospital admission 2 1 (A) (B) CAT < 10 CAT > 10 Symptoms mmrc 0 1 mmrc > 2 Breathlessness 1 (not leading to hospital admission) 0
48 Combined Assessment of COPD Assess symptoms first (C) (A) (D) (B) If CAT < 10 or mmrc 0-1: Less Symptoms/breathlessness (A or C) If CAT > 10 or mmrc > 2: More Symptoms/breathlessness (B or D) CAT < 10 CAT > 10 Symptoms mmrc 0 1 mmrc > 2 Breathlessness
49 Risk (GOLD Classification of Airflow Limitation) Risk (Exacerbation history) Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD Assess risk of exacerbations next 4 3 (C) (D) 2 or > 1 leading to hospital admission If GOLD 3 or 4 or 2 exacerbations per year or > 1 leading to hospital admission: High Risk (C or D) 2 1 (A) (B) CAT < 10 CAT > 10 1 (not leading to hospital admission) 0 If GOLD 1 or 2 and only 0 or 1 exacerbations per year (not leading to hospital admission): Low Risk (A or B) Symptoms mmrc 0 1 mmrc > 2 Breathlessness
 (B) CAT < 10 CAT > 10 Symptoms mmrc 0 1 mmrc > 2 Breathlessness 1 (not leading to hospital admission) 0 When assessing risk, choose the highest risk according to GOLD")
50 Risk (GOLD Classification of Airflow Limitation)) Risk (Exacerbation history) Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD 4 3 (C) (D) 2 or > 1 leading to hospital admission 2 1 (A) (B) CAT < 10 CAT > 10 Symptoms mmrc 0 1 mmrc > 2 Breathlessness 1 (not leading to hospital admission) 0 When assessing risk, choose the highest risk according to GOLD spirometric grade or exacerbation history. history.


51 Global Strategy for Diagnosis, Management and Prevention of COPD Combined Assessment of COPD When assessing risk, choose the highest risk according to GOLD grade or exacerbation history. (One or more hospitalizations for COPD exacerbations should be considered high risk) Patient Characteristic Spirometric Classification Exacerbations per year CAT mmrc A B C D Low Risk Less Symptoms Low Risk More Symptoms High Risk Less Symptoms High Risk More Symptoms GOLD < GOLD > 10 > 2 GOLD 3-4 > 2 < GOLD 3-4 > 2 > 10 > 2
 Patient Recommended First Choice Alternative Choice Other Possible Treatments A SAMA prn or SABA prn LAMA or LABA or SABA and SAMA Theophylline B LAMA or LABA LAMA and LABA SABA and/or SAMA")
52 Manage Stable COPD: Pharmacologic Therapy (Medications in each box are mentioned in alphabetical order, and therefore not necessarily in order of preference.) Patient Recommended First Choice Alternative Choice Other Possible Treatments A SAMA prn or SABA prn LAMA or LABA or SABA and SAMA Theophylline B LAMA or LABA LAMA and LABA SABA and/or SAMA Theophylline C ICS + LABA or LAMA LAMA and LABA or LAMA and PDE4-inh. or LABA and PDE4-inh. SABA and/or SAMA Theophylline D ICS + LABA and/or LAMA ICS + LABA and LAMA or ICS+LABA and PDE4-inh. or LAMA and LABA or LAMA and PDE4-inh. Carbocysteine SABA and/or SAMA Theophylline
53
54

 may be at")
55 Patients with symptoms disproportionate to the severity of obstruction (subgroup B) may be at higher risk of death!

56 Evidence to support this classification system Patients with a high risk of exacerbations tend to be in GOLD categories 3 and 4 (Severe or Very Severe airflow limitation) and can be identified quite reliably from the their own past history. Higher exacerbation rates are associated with faster loss of FEV1, and greater worsening of health status. Hospitalization for a COPD exacerbation is associated with poor prognosis. CAT score 10 are associated with significantly impaired health status.

57 Assess COPD Comorbidities COPD patients are at increased risk for: Cardiovascular diseases Osteoporosis, skeletal muscle dysfunction Respiratory infections Anxiety and Depression Diabetes, metabolic syndrome Lung cancer Bronchiectasis These comorbid conditions may influence mortality and hospitalizations and should be looked for routinely, and treated appropriately.
 Symptoms vary from day to day Symptoms worse at night/early morning Allergy, rhinitis, and/or eczema also present Family history of")
58 Differential Diagnosis: COPD and Asthma COPD Onset in mid-life Symptoms slowly progressive Long smoking history ASTHMA Onset early in life (often childhood) Symptoms vary from day to day Symptoms worse at night/early morning Allergy, rhinitis, and/or eczema also present Family history of asthma
 of the chest : Might help in D.D. when concomitant diseases exist. Lung Volumes and Diffusing Capacity: Help to characterize severity, but not essential to patient management.")
59 Additional Investigations Imaging. Chest X-ray: Seldom diagnostic but valuable to exclude alternative diagnoses and establish presence of significant comorbidities. Computed tomography (CT) of the chest : Might help in D.D. when concomitant diseases exist. Lung Volumes and Diffusing Capacity: Help to characterize severity, but not essential to patient management. Oximetry and Arterial Blood Gases: Pulse oximetry can be used to evaluate a patient s oxygen saturation and need for supplemental oxygen therapy. Alpha-1 Antitrypsin Deficiency Screening: Perform when COPD develops in patients of Caucasian descent under 45 years or with a strong family history of COPD Global Initiative for Chronic Obstructive Lung Disease

60 Additional Investigations Exercise Testing: Objectively measured exercise impairment, assessed by a reduction in self-paced walking distance (such as the 6 min walking test) or during incremental exercise testing in a laboratory, is a powerful indicator of health status impairment and predictor of prognosis. Composite Scores: Several variables (FEV 1, exercise tolerance assessed by walking distance or peak oxygen consumption, weight loss and reduction in the arterial oxygen tension) identify patients at increased risk for mortality. The BODE (BMI, Obstruction, Dyspnea, and Exercise) index is a better predictor of subsequent survival Global Initiative for Chronic Obstructive Lung Disease
61 Consequences Of COPD Exacerbations Negative Impact on Quality of Life Impact on Symptoms and Lung Function Accelerated Lung Function Decline EXACERBATIONS Increased Mortality Increased Socioeconomic Costs
62 Manage Exacerbations: Assessments Arterial blood gas measurements (in hospital): PaO 2 < 60 mmhg with or without PaCO 2 > 50 mmhg when breathing room air indicates respiratory failure. Chest radiograph: useful to exclude alternative diagnoses. ECG: may aid in the diagnosis of coexisting cardiac problems. Whole blood count: identify polycythemia, anemia or bleeding. Purulent sputum: during an exacerbation: indication to begin empirical antibiotic treatment. Biochemical tests: detect electrolyte disturbances, diabetes, and poor nutrition. Spirometric tests: not recommended during an exacerbation.

63 Manage Exacerbations: Assessments The best predictor of exacerbations is a history of exacerbations!

64 Manage Exacerbations: Assessments
65 Manage Exacerbations: Treatment Options Oxygen: titrate to improve the patient s hypoxemia with a target saturation of 88-92%. Bronchodilators: Short-acting inhaled beta 2 -agonists with or without short-acting anticholinergics are preferred. Systemic Corticosteroids: Shorten recovery time, improve lung function (FEV 1 ) and arterial hypoxemia (PaO 2 ), and reduce the risk of early relapse, treatment failure, and length of hospital stay. A dose of 40 mg prednisone per day for 5 days is recommended.
66 Manage Exacerbations: Treatment Options Antibiotics should be given to patients with: Three cardinal symptoms: increased dyspnea, increased sputum volume, and increased sputum purulence. Who require mechanical ventilation.

67 Manage Exacerbations: Indications for Hospital Admission Marked increase in intensity of symptoms Severe underlying COPD Onset of new physical signs Failure of an exacerbation to respond to initial medical management Presence of serious comorbidities Frequent exacerbations Older age Insufficient home support


68 Thanks for your attention!
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
COPD: Current Medical Therapy
 COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis.
 1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
Asthma COPD Overlap (ACO)
") Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
2/4/2019. GOLD Objectives. GOLD 2019 Report: Chapters
 GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline. MedStar Health
 Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES
 MANAGEMENT GUIDELINES") JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
Differential diagnosis
 Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Life-long asthma and its relationship to COPD. Stephen T Holgate School of Medicine University of Southampton
 Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
Life-long asthma and its relationship to COPD Stephen T Holgate School of Medicine University of Southampton Definitions COPD is a preventable and treatable disease with some significant extrapulmonary
Defining COPD. Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist
 Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
Chronic Obstructive Pulmonary Disease (COPD) Clinical Guideline
 Clinical Guideline") Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Disclosure and Conflict of Interest 8/15/2017. Pharmacist Objectives. At the conclusion of this program, the pharmacist will be able to:
 Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX
 MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX") CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX COPD OUTLINE Definition and Overview Pathophysiology Diagnosis and Assessment Therapeutic
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX COPD OUTLINE Definition and Overview Pathophysiology Diagnosis and Assessment Therapeutic
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING 10/16/2018 DISCLOSURES I have no financial or other disclosures
 OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
Guideline for the Diagnosis and Management of COPD
 Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Karen Meyerson, MSN, APRN, NP C, AE C
 Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) June 2015 Karen Meyerson, MSN, APRN, NP C, AE C Patient Education The goal of all patient education is to help patients take the actions
Webinar for Michigan Center for Clinical Systems Improvement (Mi-CCSI) June 2015 Karen Meyerson, MSN, APRN, NP C, AE C Patient Education The goal of all patient education is to help patients take the actions
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015
 David CL Lam Department of Medicine University of Hong Kong October, 2015") Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
CHRONIC OBSTRUCTIVE LUNG DISEASE (COPD), BRONCHIAL ASTHMA
, BRONCHIAL ASTHMA") CHRONIC OBSTRUCTIVE LUNG DISEASE (COPD), BRONCHIAL ASTHMA GOLD GINA Chronic Obstructive Pulmonary Disease (COPD) COPD is currently the fourth leading cause of death in the world.1 COPD is projected to
CHRONIC OBSTRUCTIVE LUNG DISEASE (COPD), BRONCHIAL ASTHMA GOLD GINA Chronic Obstructive Pulmonary Disease (COPD) COPD is currently the fourth leading cause of death in the world.1 COPD is projected to
What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university
 What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university Management stable COPD Relieve symptoms Improve exercise tolerance Improve health status Prevent
What s new in COPD? Apichart Khanichap MD. Department of Medicine, Faculty of Medicine, Thammasat university Management stable COPD Relieve symptoms Improve exercise tolerance Improve health status Prevent
COPD GOLD Guidelines & Barnet inhaler choices. Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust
 COPD GOLD Guidelines & Barnet inhaler choices Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust GOLD 2017 Report: Chapters 1. Definition and Overview 2. Diagnosis and Initial
COPD GOLD Guidelines & Barnet inhaler choices Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust GOLD 2017 Report: Chapters 1. Definition and Overview 2. Diagnosis and Initial
COPD exacerbation. Chiara Maruggi, PGY2
 COPD exacerbation Chiara Maruggi, PGY2 Learning objectives At the end of this lecture students will be able to: 1) Critically assess patients for COPD and design a management plan. 2) Develop a step-wise
COPD exacerbation Chiara Maruggi, PGY2 Learning objectives At the end of this lecture students will be able to: 1) Critically assess patients for COPD and design a management plan. 2) Develop a step-wise
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
How to treat COPD? What is the mechanism of dyspnea? Smoking cessation
 : The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
: The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
COPD. Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS
 IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
COPD/Asthma. Prudence Twigg, AGNP
 COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
People with asthma who smoke. The combination of asthma, a chronic airway disease, and smoking increases the risk of COPD even more.
 COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
Curriculum Vitae. Head of Public Wing HCU - RSCM. Head of ICU Sari Asih Ciledug Hospital
 Curriculum Vitae Name : Dr. Ceva W. Pitoyo,SpPD,K-P,KIC,FINASIM POB / DOB : Jakarta, March 8th 1968 Education : o General Practitioner : FKUI 1993 o Internist : FKUI 2002 o Pulmonology Consultant : PAPDI-UI
Curriculum Vitae Name : Dr. Ceva W. Pitoyo,SpPD,K-P,KIC,FINASIM POB / DOB : Jakarta, March 8th 1968 Education : o General Practitioner : FKUI 1993 o Internist : FKUI 2002 o Pulmonology Consultant : PAPDI-UI
AECOPD: Management and Prevention
 Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
Neil MacIntyre MD Duke University Medical Center Durham NC Professor P.J. Barnes, MD, National Heart and Lung Institute, London UK Professor Peter J. Barnes, MD National Heart and Lung Institute, London
CARE OF THE ADULT COPD PATIENT
 CARE OF THE ADULT COPD PATIENT Target Audience: The target audience for this clinical guideline is all MultiCare providers and staff including those associated with our Clinically Integrated Network. The
CARE OF THE ADULT COPD PATIENT Target Audience: The target audience for this clinical guideline is all MultiCare providers and staff including those associated with our Clinically Integrated Network. The
Chronic obstructive pulmonary disease
 0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
COPD: Preventable and Treatable. Lecture Outline. Diagnosis of COPD. COPD: Defining Terms
 COPD: Preventable and Treatable Christopher H. Fanta, M.D. Partners Asthma Center Pulmonary and Critical Care Division Brigham and Women s Hospital Harvard Medical School Lecture Outline I. Diagnosis and
COPD: Preventable and Treatable Christopher H. Fanta, M.D. Partners Asthma Center Pulmonary and Critical Care Division Brigham and Women s Hospital Harvard Medical School Lecture Outline I. Diagnosis and
Lecture Notes. Chapter 4: Chronic Obstructive Pulmonary Disease (COPD)
") Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
How to distinguish between uncontrolled and severe asthma
 How to distinguish between uncontrolled and severe asthma Watch patient using their inhaler. Discuss adherence and barriers to use Compare inhaler technique with a devicespecific checklist, and correct
How to distinguish between uncontrolled and severe asthma Watch patient using their inhaler. Discuss adherence and barriers to use Compare inhaler technique with a devicespecific checklist, and correct
BPCO: dalle novità patogenetiche alla terapia
 BPCO: dalle novità patogenetiche alla terapia Gianna Camiciottoli Dip. Di Scienze Biomediche, Sperimentali e Cliniche Mario Serio Università degli Studi di Firenze Firenze, 11 novembre 2016 Conflict of
BPCO: dalle novità patogenetiche alla terapia Gianna Camiciottoli Dip. Di Scienze Biomediche, Sperimentali e Cliniche Mario Serio Università degli Studi di Firenze Firenze, 11 novembre 2016 Conflict of
Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research
 Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research Concord Hospital Woolcock Institute of Medical Research Joe has asthma What
Asthma and COPD in older people lumping or splitting? Christine Jenkins Concord Hospital Woolcock Institute of Medical Research Concord Hospital Woolcock Institute of Medical Research Joe has asthma What
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
Provider Respiratory Inservice
 Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
COPD Management in LTC: Presented By: Jessica Denney RRT
 COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
Chronic Obstructive Pulmonary Disease Guidelines and updates
 Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
Asthma ASTHMA. Current Strategies for Asthma and COPD
 Current Strategies for Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco,
Current Strategies for Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor of Medicine Chair, Department of Medicine University of California San Francisco (UCSF) San Francisco,
Basic mechanisms disturbing lung function and gas exchange
 Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Supplementary Online Content
 Supplementary Online Content Regan EA, Lynch DA, Curran-Everett D, et al; Genetic Epidemiology of COPD (COPDGene) Investigators. Clinical and radiologic disease in smokers with normal spirometry. Published
Supplementary Online Content Regan EA, Lynch DA, Curran-Everett D, et al; Genetic Epidemiology of COPD (COPDGene) Investigators. Clinical and radiologic disease in smokers with normal spirometry. Published
COPD/ Asthma. Dr Heather Lewis Honorary Clinical Lecturer
 COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
Current Approaches to Asthma & COPD
 10/11/18 Current Approaches to Asthma & COPD Lekshmi Santhosh, M.D. Assistant Professor, Pulm/Critical Care & Hosp Med Primary Care Medicine: Principles & Practice 10.11.2018 Revisiting the Dutch Hypothesis:
10/11/18 Current Approaches to Asthma & COPD Lekshmi Santhosh, M.D. Assistant Professor, Pulm/Critical Care & Hosp Med Primary Care Medicine: Principles & Practice 10.11.2018 Revisiting the Dutch Hypothesis:
CHRONIC OBSTRUCTIVE PULMONARY DISEASE
 CHRONIC OBSTRUCTIVE PULMONARY DISEASE DEFINITION Chronic obstructive pulmonary disease (COPD) is a common preventable and treatable disease characterized by airflow limitation that is usually progressive
CHRONIC OBSTRUCTIVE PULMONARY DISEASE DEFINITION Chronic obstructive pulmonary disease (COPD) is a common preventable and treatable disease characterized by airflow limitation that is usually progressive
Chronic Obstructive Pulmonary Disease (COPD).
.") Chronic Obstructive Pulmonary Disease (COPD). Linde: Living healthcare 02 03 Chronic Obstructive Pulmonary Disease (COPD). A pocket guide for healthcare professionals. COPD the facts Moderate to severe
Chronic Obstructive Pulmonary Disease (COPD). Linde: Living healthcare 02 03 Chronic Obstructive Pulmonary Disease (COPD). A pocket guide for healthcare professionals. COPD the facts Moderate to severe
THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable
 THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. COPD in the United States Third leading cause
THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. COPD in the United States Third leading cause
Pulmonary Function Testing: Concepts and Clinical Applications. Potential Conflict Of Interest. Objectives. Rationale: Why Test?
 Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
GOLD UPDATE on COPD and the Importance of Accurate Dyspnea Evaluation
 GOLD UPDATE on COPD and the Importance of Accurate Dyspnea Evaluation George Anderson, PhD Sr. Medical Science Liaison MA-AZAP ML-4006-US-0212 Approved 11/16 Glob al Strategy for the Diagnosis, Management,
GOLD UPDATE on COPD and the Importance of Accurate Dyspnea Evaluation George Anderson, PhD Sr. Medical Science Liaison MA-AZAP ML-4006-US-0212 Approved 11/16 Glob al Strategy for the Diagnosis, Management,
Chronic Obstructive Pulmonary Disease (COPD) Copyright 2014 by Mosby, an imprint of Elsevier Inc.
 Copyright 2014 by Mosby, an imprint of Elsevier Inc.") Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
COPD and Asthma Update. April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute
 COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
COPD and Asthma Update April 29 th, 2017 Rachel M Taliercio, DO Staff, Respiratory Institute What we ll be talking about COPD: diagnosis, management of stable COPD, COPD exacerbations Asthma: diagnosis,
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
9/22/2015 CONFLICT OF INTEREST OBJECTIVES. Understanding COPD - Recent Research and the Evolving Definition of COPD for MNACVPR
 Understanding COPD - Recent Research and the Evolving Definition of COPD for MNACVPR by Scott Cerreta, BS, RRT Director of Education www.copdfoundation.org scerreta@copdfoundation.org CONFLICT OF INTEREST
Understanding COPD - Recent Research and the Evolving Definition of COPD for MNACVPR by Scott Cerreta, BS, RRT Director of Education www.copdfoundation.org scerreta@copdfoundation.org CONFLICT OF INTEREST
Understanding COPD - Recent Research and the Evolving Definition of COPD for MNACVPR
 Understanding COPD - Recent Research and the Evolving Definition of COPD for MNACVPR by Scott Cerreta, BS, RRT Director of Education www.copdfoundation.org scerreta@copdfoundation.org CONFLICT OF INTEREST
Understanding COPD - Recent Research and the Evolving Definition of COPD for MNACVPR by Scott Cerreta, BS, RRT Director of Education www.copdfoundation.org scerreta@copdfoundation.org CONFLICT OF INTEREST
Known Allergies: Shellfish. Symptoms: abdominal pain, nausea, diarrhea, or vomiting. congestion, trouble breathing, or wheezing.
 CSTAR CASE STUDIES: BLOCK B Asthma or COPD? Setting: Walk in clinic. Dan: I havi g that cough thi g agai HPI: Dan is a 49-year-old male teacher who reports having had episodes of cough with mucus production
CSTAR CASE STUDIES: BLOCK B Asthma or COPD? Setting: Walk in clinic. Dan: I havi g that cough thi g agai HPI: Dan is a 49-year-old male teacher who reports having had episodes of cough with mucus production
Changing Landscapes in COPD New Zealand Respiratory Conference
 Changing Landscapes in COPD New Zealand Respiratory Conference Dr Robert Young BMedSc MBChB DPhil (Oxon) FRACP FRCP Associate Professor Consultant Physician Changing Landscapes in COPD: Summary 1. Overview
Changing Landscapes in COPD New Zealand Respiratory Conference Dr Robert Young BMedSc MBChB DPhil (Oxon) FRACP FRCP Associate Professor Consultant Physician Changing Landscapes in COPD: Summary 1. Overview
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD
 Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor
Primary Care Medicine: Concepts and Controversies Wed., February 17, 2010 Fiesta Americana Puerto Vallarta, Mexico Update on Asthma and COPD Talmadge E. King, Jr., M.D. Krevins Distinguished Professor
Pathophysiology of COPD 건국대학교의학전문대학원
 Pathophysiology of COPD 건국대학교의학전문대학원 내과학교실 유광하 Rate per 100 0,000 population 550 500 450 400 350 300 250 200 150 100 50 0 Heart disease Cancer Stroke 1970 1974 1978 1982 1986 1990 1994 1998 2002 Year of
Pathophysiology of COPD 건국대학교의학전문대학원 내과학교실 유광하 Rate per 100 0,000 population 550 500 450 400 350 300 250 200 150 100 50 0 Heart disease Cancer Stroke 1970 1974 1978 1982 1986 1990 1994 1998 2002 Year of
Fact. Objectives 1/6/2016. Reducing Hospital Readmissions for Chronic Obstructive Pulmonary Disease (COPD)
") Reducing Hospital Readmissions for Chronic Obstructive Pulmonary Disease (COPD) Jin S. Oh, PharmD Larkin Community Hospital January 10, 2016 Fact COPD is the third leading cause of death in the United
Reducing Hospital Readmissions for Chronic Obstructive Pulmonary Disease (COPD) Jin S. Oh, PharmD Larkin Community Hospital January 10, 2016 Fact COPD is the third leading cause of death in the United
Take My Breath Away: COPD Update. Jason Henderson D.O. Warren Clinic Pulmonary & Critical Care
 Take My Breath Away: Update Jason Henderson D.O. Warren Clinic Pulmonary & Critical Care Objectives 1. Recognize clinical signs and symptoms associated with chronic bronchitis and emphysema. 2. Describe
Take My Breath Away: Update Jason Henderson D.O. Warren Clinic Pulmonary & Critical Care Objectives 1. Recognize clinical signs and symptoms associated with chronic bronchitis and emphysema. 2. Describe
Treatment Responses. Ronald Dahl, Aarhus University Hospital, Denmark
 Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
Asthma and COPD: Are They a Spectrum Treatment Responses Ronald Dahl, Aarhus University Hospital, Denmark Pharmacological Treatments Bronchodilators Inhaled short-acting β -Agonist (rescue) Inhaled short-acting
COPD as a comorbidity of heart failure in elderly patients
 COPD as a comorbidity of heart failure in elderly patients Professor Mitja Lainscak, MD, PhD, FESC, FHFA Departments of Cardiology and Research&Education, General Hospital Celje Faculty of Medicine, University
COPD as a comorbidity of heart failure in elderly patients Professor Mitja Lainscak, MD, PhD, FESC, FHFA Departments of Cardiology and Research&Education, General Hospital Celje Faculty of Medicine, University
Pulmonary Pearls. Medical Pearls. Case 1: Case 1 (cont.): Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):
: Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):") Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
You ve come a long way, baby.
 COPD Dr Badri Paudel Dept of Medicine GMC/CHRC 4/22/12 badri@gmc 2 You ve come a long way, baby. Wayne McLaren Former Marlboro Man 4/22/12 badri@gmc 3 Age 30 a robust young man Age 51 riding into the sunset
COPD Dr Badri Paudel Dept of Medicine GMC/CHRC 4/22/12 badri@gmc 2 You ve come a long way, baby. Wayne McLaren Former Marlboro Man 4/22/12 badri@gmc 3 Age 30 a robust young man Age 51 riding into the sunset
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene
 Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene Emily S. Wan, John E. Hokanson, James R. Murphy, Elizabeth A. Regan, Barry J. Make, David A. Lynch, James D. Crapo, Edwin K.
Clinical and radiographic predictors of GOLD-Unclassified smokers in COPDGene Emily S. Wan, John E. Hokanson, James R. Murphy, Elizabeth A. Regan, Barry J. Make, David A. Lynch, James D. Crapo, Edwin K.
PFT s / 2017 Pulmonary Update. Eric S. Papierniak, DO University of Florida NF/SG VHA
 PFT s / 2017 Pulmonary Update Eric S. Papierniak, DO University of Florida NF/SG VHA Outline Overview of pulmonary function testing Uses/indications/limitations Technical aspects Basics of interpretation
PFT s / 2017 Pulmonary Update Eric S. Papierniak, DO University of Florida NF/SG VHA Outline Overview of pulmonary function testing Uses/indications/limitations Technical aspects Basics of interpretation
Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD)
 Instructions for the Pulmonary Diagnosis Form (PLD)") Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD) A Pulmonary Diagnosis Form is filled out by the reviewer for all medical records that are sent to them for review by the CSCC.
Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD) A Pulmonary Diagnosis Form is filled out by the reviewer for all medical records that are sent to them for review by the CSCC.
Disclosure Statement. Epidemiological Data
 EVALUATION OF THE MEDICATION UTILIZATION OF COPD PATIENTS AT THE MIAMI VA HEALTHCARE SYSTEM Simone Edgerton, PharmD. PGY 1 Pharmacy Resident Miami VA Healthcare System Miami, Florida Simone.edgerton2@va.gov
EVALUATION OF THE MEDICATION UTILIZATION OF COPD PATIENTS AT THE MIAMI VA HEALTHCARE SYSTEM Simone Edgerton, PharmD. PGY 1 Pharmacy Resident Miami VA Healthcare System Miami, Florida Simone.edgerton2@va.gov
Course Handouts & Disclosure
 COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
2017 GOLD Report. Is it worth its weight in GOLD??? CSHP-NB Fall Education Day September 30, 2017
 2017 GOLD Report Is it worth its weight in GOLD??? CSHP-NB Fall Education Day September 30, 2017 Lauren Munro; BSc(Pharm) Amanda Burns; BSc(Pharm) Pharmacy Residents The Moncton Hospital Objectives Explain
2017 GOLD Report Is it worth its weight in GOLD??? CSHP-NB Fall Education Day September 30, 2017 Lauren Munro; BSc(Pharm) Amanda Burns; BSc(Pharm) Pharmacy Residents The Moncton Hospital Objectives Explain
Objectives. Advances in Managing COPD Patients
 4:45 5:30pm Advances in Managing Patients SPEAKER Nicola Hanania, MD, FCCP, FRCP, FACP Presenter Disclosure Information The following relationships exist related to this presentation: Nicola Hanania, MD,
4:45 5:30pm Advances in Managing Patients SPEAKER Nicola Hanania, MD, FCCP, FRCP, FACP Presenter Disclosure Information The following relationships exist related to this presentation: Nicola Hanania, MD,
COPD or not COPD, that is the question.
 COPD or not COPD, that is the question. Asthma-COPD Overlap Syndrome: ACOS Do we really need this? Michelle Harkins Disclosure Slide Slide help - William Busse, MD Organizational Interests ATS, ACCP, ACP
COPD or not COPD, that is the question. Asthma-COPD Overlap Syndrome: ACOS Do we really need this? Michelle Harkins Disclosure Slide Slide help - William Busse, MD Organizational Interests ATS, ACCP, ACP
If you require this document in another format such as Braille, large print, audio or another language please contact the Trusts Communications Team
 MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) IN ADULTS Summary statement: How does the document support patient care? Staff/stakeholders involved in development: Job titles only Division:
MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) IN ADULTS Summary statement: How does the document support patient care? Staff/stakeholders involved in development: Job titles only Division:
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
HQO s Episode of Care for Chronic Obstructive Pulmonary Disease
 HQO s Episode of Care for Chronic Obstructive Pulmonary Disease Dr. Chaim Bell, MD PhD FRCPC Ontario Hospital Association Webcast October 23, 2013 Objectives 1. Describe the rationale and methodology for
HQO s Episode of Care for Chronic Obstructive Pulmonary Disease Dr. Chaim Bell, MD PhD FRCPC Ontario Hospital Association Webcast October 23, 2013 Objectives 1. Describe the rationale and methodology for
COPD: GOLD guidelines Ijlal Babar, MD Medical Director Pulmonary CCM, Pulmonary Hypertension Center SRHS
 COPD: GOLD guidelines 2017 Ijlal Babar, MD Medical Director Pulmonary CCM, Pulmonary Hypertension Center SRHS Introduction The Global Initiative for Chronic Obstructive Lung Disease (GOLD) program was
COPD: GOLD guidelines 2017 Ijlal Babar, MD Medical Director Pulmonary CCM, Pulmonary Hypertension Center SRHS Introduction The Global Initiative for Chronic Obstructive Lung Disease (GOLD) program was
At-A-Glance Outpatient Management Reference for Chronic Obstructive Pulmonary Disease (COPD)
") At-A-Glance Outpatient Management Reference f Chronic Obstructive Pulmonary Disease (COPD) BASED ON THE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT AND PREVENTION OF COPD GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE
At-A-Glance Outpatient Management Reference f Chronic Obstructive Pulmonary Disease (COPD) BASED ON THE GLOBAL STRATEGY FOR DIAGNOSIS, MANAGEMENT AND PREVENTION OF COPD GLOBAL INITIATIVE FOR CHRONIC OBSTRUCTIVE
Asthma Pathophysiology and Treatment. John R. Holcomb, M.D.
 Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
Asthma Pathophysiology and Treatment John R. Holcomb, M.D. Objectives Definition of Asthma Epidemiology and risk factors of Asthma Pathophysiology of Asthma Diagnostics test of Asthma Management of Asthma
COPD. Helen Suen & Lexi Smith
 COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
COPD, Asthma, Or Something In Between? Sharon R. Rosenberg Assistant Professor of Medicine Northwestern University December 4, 2013
 COPD, Asthma, Or Something In Between? Sharon R. Rosenberg Assistant Professor of Medicine Northwestern University December 4, 2013 None Disclosures Definitions Asthma Asthma is a chronic inflammatory
COPD, Asthma, Or Something In Between? Sharon R. Rosenberg Assistant Professor of Medicine Northwestern University December 4, 2013 None Disclosures Definitions Asthma Asthma is a chronic inflammatory
Advancing COPD treatment strategies with evidencebased. 17:15 19:15 Monday 11 September 2017 ERS 2017, Milan, Italy
 Advancing COPD treatment strategies with evidencebased approaches 17:15 19:15 Monday 11 September 2017 ERS 2017, Milan, Italy Increasing understanding of COPD and the effect on guideline evolution. GOLD
Advancing COPD treatment strategies with evidencebased approaches 17:15 19:15 Monday 11 September 2017 ERS 2017, Milan, Italy Increasing understanding of COPD and the effect on guideline evolution. GOLD
Up in FLAMES: Stable Chronic Obstructive Pulmonary Disease (COPD) Management. Colleen Sakon, PharmD BCPS September 27, 2018
 Management. Colleen Sakon, PharmD BCPS September 27, 2018") Up in FLAMES: Stable Chronic Obstructive Pulmonary Disease (COPD) Management Colleen Sakon, PharmD BCPS September 27, 2018 Disclosures I have no actual or potential conflicts of interest 2 Objectives Summarize
Up in FLAMES: Stable Chronic Obstructive Pulmonary Disease (COPD) Management Colleen Sakon, PharmD BCPS September 27, 2018 Disclosures I have no actual or potential conflicts of interest 2 Objectives Summarize
7/7/2015. Somboon Chansakulporn, MD. History of variable respiratory symptoms. 1. Documented excessive variability in PFT ( 1 test)
") Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
Definition of Asthma GINA 2010: Chronic inflammatory disorder of the airways Airway hyper-responsiveness Recurrent wheezing, breathlessness, chest tightness, coughing Variable, reversible airflow obstruction
Over the last several years various national and
 Recommendations for the Management of COPD* Gary T. Ferguson, MD, FCCP Three sets of guidelines for the management of COPD that are widely recognized (from the European Respiratory Society [ERS], American
Recommendations for the Management of COPD* Gary T. Ferguson, MD, FCCP Three sets of guidelines for the management of COPD that are widely recognized (from the European Respiratory Society [ERS], American
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo
 62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
UPDATE ON GOLD GUIDELINES IN COPD
 UPDATE ON GOLD GUIDELINES IN COPD GERARD J. CRINER, MD, FACP, FACCP PROFESSOR, THORACIC MEDICINE & SURGERY TEMPLE UNIVERSITY SCHOOL OF MEDICINE PHILADELPHIA, PA Gerard J. Criner, MD, is Professor and Founding
UPDATE ON GOLD GUIDELINES IN COPD GERARD J. CRINER, MD, FACP, FACCP PROFESSOR, THORACIC MEDICINE & SURGERY TEMPLE UNIVERSITY SCHOOL OF MEDICINE PHILADELPHIA, PA Gerard J. Criner, MD, is Professor and Founding
CLINICAL PATHWAY. Acute Medicine. Chronic Obstructive Pulmonary Disease
 CLINICAL PATHWAY Acute Medicine Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease Table of Contents (tap to jump to page) INTRODUCTION 1 Scope of this Pathway 1 Pathway Contacts
CLINICAL PATHWAY Acute Medicine Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease Table of Contents (tap to jump to page) INTRODUCTION 1 Scope of this Pathway 1 Pathway Contacts
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline. MedStar Health
 Global Strategy f the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Global Strategy f the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Update on COPD John Hurst PhD FRCP
 Update on COPD John Hurst PhD FRCP Reader / Consultant in Respiratory Medicine UCL / Royal Free London NHS Foundation Trust Director, UCL Royal Free COPD Centre j.hurst@ucl.ac.uk Questions 1. What is the
Update on COPD John Hurst PhD FRCP Reader / Consultant in Respiratory Medicine UCL / Royal Free London NHS Foundation Trust Director, UCL Royal Free COPD Centre j.hurst@ucl.ac.uk Questions 1. What is the
Are your COPD patients benefiting from best practices? Spirometry makes the diagnosis and determines therapy choices, yet it is vastly underused
 For mass reproduction, content licensing and permissions contact Dowden Health Media. FAMILY Dean Gianakos, MD, and Rafal (Ralph) Kaczynski, MD Lynchburg Family Medicine Residency, Lynchburg, VA deangianakos@yahoo.com
For mass reproduction, content licensing and permissions contact Dowden Health Media. FAMILY Dean Gianakos, MD, and Rafal (Ralph) Kaczynski, MD Lynchburg Family Medicine Residency, Lynchburg, VA deangianakos@yahoo.com
Decramer 2014 a &b [21]
![Decramer 2014 a &b [21]](/thumbs/90/101390504.jpg "Decramer 2014 a &b [21]") Buhl 2015 [19] Celli 2014 [20] Decramer 2014 a &b [21] D Urzo 2014 [22] Maleki-Yazdi 2014 [23] Inclusion criteria: Diagnosis of chronic obstructive pulmonary disease; 40 years of age or older; Relatively
Buhl 2015 [19] Celli 2014 [20] Decramer 2014 a &b [21] D Urzo 2014 [22] Maleki-Yazdi 2014 [23] Inclusion criteria: Diagnosis of chronic obstructive pulmonary disease; 40 years of age or older; Relatively
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ
 Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
Amanda Hess, MMS, PA-C President-Elect, AAPA-AAI Arizona Asthma and Allergy Institute Scottsdale, AZ Financial Disclosures Advanced Practiced Advisory Board for Circassia Learning Objectives 1. Briefly
Lead team presentation: Roflumilast for treating chronic obstructive pulmonary disease [ID984]
![Lead team presentation: Roflumilast for treating chronic obstructive pulmonary disease [ID984]](/thumbs/85/91889043.jpg "Lead team presentation: Roflumilast for treating chronic obstructive pulmonary disease [ID984]") Lead team presentation: Roflumilast for treating chronic obstructive pulmonary disease [ID984] 1 st Appraisal Committee meeting Background & Clinical Effectiveness John McMurray 11 th January 2016 For
Lead team presentation: Roflumilast for treating chronic obstructive pulmonary disease [ID984] 1 st Appraisal Committee meeting Background & Clinical Effectiveness John McMurray 11 th January 2016 For
This is a cross-sectional analysis of the National Health and Nutrition Examination
 SUPPLEMENTAL METHODS Study Design and Setting This is a cross-sectional analysis of the National Health and Nutrition Examination Survey (NHANES) data 2007-2008, 2009-2010, and 2011-2012. The NHANES is
SUPPLEMENTAL METHODS Study Design and Setting This is a cross-sectional analysis of the National Health and Nutrition Examination Survey (NHANES) data 2007-2008, 2009-2010, and 2011-2012. The NHANES is
THE COPD-ASTHMA OVERLAP SYNDROME
 THE COPD-ASTHMA OVERLAP SYNDROME NICOLA A. HANANIA, MD, MS, FRCP(C), FCCP, FACP ASSOCIATE PROFESSOR OF MEDICINE DIRECTOR OF ASTHMA & COPD CLINICAL RESEARCH CENTER BAYLOR COLLEGE OF MEDICINE HOUSTON, TX
THE COPD-ASTHMA OVERLAP SYNDROME NICOLA A. HANANIA, MD, MS, FRCP(C), FCCP, FACP ASSOCIATE PROFESSOR OF MEDICINE DIRECTOR OF ASTHMA & COPD CLINICAL RESEARCH CENTER BAYLOR COLLEGE OF MEDICINE HOUSTON, TX
Turning Science into Real Life Roflumilast in Clinical Practice. Roland Buhl Pulmonary Department Mainz University Hospital
 Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe