Case Report Acquired Elliptocytosis as a Manifestation of Myelodysplastic Syndrome with Ring Sideroblasts and Multilineage Dysplasia
|
|
|
- Alexandrina Goodman
- 5 years ago
- Views:
Transcription
1 Hindawi Case Reports in Hematology Volume 2017, Article ID , 5 pages Case Report Acquired Elliptocytosis as a Manifestation of Myelodysplastic Syndrome with Ring Sideroblasts and Multilineage Dysplasia Jacob D. Kjelland, 1 Denis M. Dwyre, 2 and Brian A. Jonas 3,4 1 Department of Internal Medicine, University of California Davis Medical Center, Sacramento, CA 98517, USA 2 Department of Pathology, University of California Davis Medical Center, Sacramento, CA 98517, USA 3 Department of Internal Medicine, Division of Hematology and Oncology, University of California Davis Medical Center, Sacramento, CA 98517, USA 4 VA Northern California Health Care System, Mather, CA 95655, USA Correspondence should be addressed to Brian A. Jonas; bajonas@ucdavis.edu Received 18 July 2017; Accepted 11 September 2017; Published 11 October 2017 Academic Editor: Sudhir Tauro Copyright 2017 Jacob D. Kjelland et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Acquired elliptocytosis is a known but rarely described abnormality in the myelodysplastic syndromes (MDS). Here we report the case of an elderly male who was admitted to the hospital with chest pain, dyspnea, and fatigue and was found to be anemic with an elliptocytosis that had only recently been noted on peripheral smears of his blood. After bone marrow biopsy he was diagnosed with MDS with ring sideroblasts and multilineage dysplasia and acquired elliptocytosis. Here we report a rare case of acquired elliptocytosis cooccurring with MDS with ring sideroblasts and multilineage dysplasia. 1. Introduction The myelodysplastic syndromes (MDS) are a heterogeneous group of clonal myeloid hemopathies that result in ineffective development of one or more hematopoietic lineages. The genetic alterations and other pathologic processes in the bone marrow causing dysfunctional hematopoiesis lead to a wide range of disease phenotypes which can range from mild single lineage cytopenia to severe pancytopenia or transformation to acute leukemia. Similarly diverse are the microscopic characteristics of the dysplastic cells in the bone marrow and peripheral blood. Inthisreport,wepresentthecaseofanelderlymale who was diagnosed with MDS after being admitted to our hospital for symptomatic anemia. Review of his bone marrow biopsy showed two morphological findings of particular note. The first finding was ring sideroblasts, which are present in about 25% of cases of MDS [1]. Ring sideroblasts are erythroid precursor cells in which iron is unable to be exported from the mitochondria due to one of a variety of defects. This leads to an excess of iron within the mitochondria, which stains with Prussian blue, revealing the so-called ring sideroblast. As with most findings in MDS, ring sideroblasts are not specific to MDS but are found in numerous congenital and acquired conditions encompassing many genetic and acquired defects. Recently, mutations in a gene coding for a portion of the U2 snrnp have been linked to the development of ring sideroblasts in MDS. In one study, SF3B1, located on chromosome 2 ( was found to be mutated in 20% of all MDS cases and 65% of those with ring sideroblasts [2]. In another recent study, 81% of MDS subtypes with ring sideroblasts had SF3B1 mutations [3]. It has been speculated that the mutated protein may cause generalized downregulation of several core pathways within the mitochondria, potentially accounting for the higher frequency of ring sideroblasts observed in patients with mutated SF3B1 [2]. The second finding in our case was elliptocytosis, a finding which can be hereditary or can be acquired. Hereditary elliptocytosis is caused by mutations in in structural components of the erythrocyte cell membrane. Mutations in genes coding for protein 4.1, alpha spectrin, beta spectrin, band 3, and Glycophorin C have all been implicated in hereditary elliptocytosis [4, 5]. Of note, other hereditary conditions, such as sickle cell
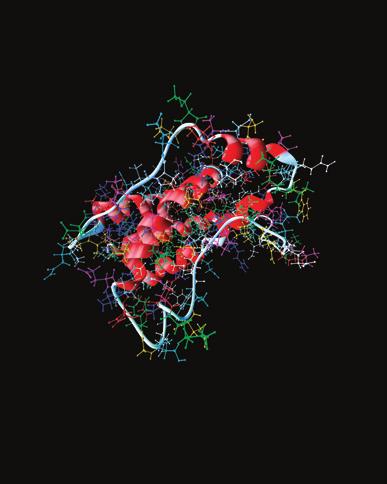
![2 Case Reports in Hematology anemia, thalassemias, and pyruvate kinase deficiency can have elliptocytosis as a feature [4].](/docs-images/89/97495790/images/2-0.jpg "Acquired elliptocytosis is sometimes seen in myeloid malignancies (including MDS) as well as in iron deficiency anemia, megaloblastic anemias, polycythemia, and myelofibrosis [5]. 2.")
2 2 Case Reports in Hematology anemia, thalassemias, and pyruvate kinase deficiency can have elliptocytosis as a feature [4]. Acquired elliptocytosis is sometimes seen in myeloid malignancies (including MDS) as well as in iron deficiency anemia, megaloblastic anemias, polycythemia, and myelofibrosis [5]. 2. Case A 70-year-old Caucasian male immigrant from Eastern Europe with a 6-year history of anemia and an 8-year history of thrombocytopenia was admitted to our hospital for chest pain and dyspnea. At the time of his admission, his exam was notable for mild scleral icterus and a palpable spleen 2 cm below the costal margin. He had undergone prior workup for his cytopenias without a clear diagnosis. There was no family history of anemia. He did not use alcohol. His medications included amiodarone and ranolazine (medications associated with bone marrow suppression), but no other medications known to affect hematopoiesis. Records obtained documenting the outpatient workup included studies showing normal vitamin B12 and folate levels, decreased haptoglobin with a negative Coombs test, and a bone marrow biopsy performed 2 years earlier which showed a hypercellular marrow, moderate erythroid hyperplasia, a deletion of chromosome 20q by cytogenetics, 3-4% ring sideroblasts, and normal flow cytometry studies. Based on these findings, there was concern for a pre-mds state, such as clonal cytopenia of undetermined significance (CCUS). One month prior to admission, a peripheral smear showed elliptocytosis. Physician s notes from the outpatient workup indicate that a peripheral smear was reviewed 2 years earlier and there was no mention of elliptocytosis or spherocytosis at that time. At time of admission, the patient s hemoglobin was 7.6g/dL with an MCV of 91.1μm 3, a platelet count of 28,000/mm 3, white blood cell count of 5,200/mm 3, and absoluteneutrophilcountof4,600/mm 3.Hehad6.7%reticulocytes with an absolute reticulocyte count of 190,000/mm 3. His total bilirubin was elevated at 4.5 mg/dl with direct bilirubin of 2.4 mg/dl. Transaminases were normal. LDH was elevated at 349 U/L, but haptoglobin levels were normal and a direct Coombs test was negative. Methylmalonic acid level was slightly elevated at 0.48 μmol/l (normal up to 0.40 μmol/l). Thyroid studies and vitamin B12 levels were normal. Folate was not checked. Ferritin was 540 ng/ml, with normal serum iron and transferrin levels. No paroxysmal nocturnal hemoglobinuria clone was detected by peripheral blood flow cytometry. Osmotic fragility was tested and found to be normal. HIV screen was negative. Hematology was consulted for diagnostic assistance. Review of the peripheral smear showed marked elliptocytosis (Figure 1). A bone marrow biopsy was performed which showed a hypercellular marrow with erythroid hyperplasia, dyserythropoiesis and dysmegakaryopoiesis, and adequate stainable iron with >15% ring sideroblasts and 3% blasts (Figure 2). Cytogenetic analysis showed 46,XY,del(20)(q11.2q13.3)/47,idem,+del(20) [6]. Based on these findings, the patient was diagnosed with MDS with ring sideroblasts and multilineage dysplasia Figure 1: Peripheral blood smear (Wright-Giemsa stained, 100x): peripheral smear showing anemia, with numerous elliptocytes and thrombocytopenia. (MDS-RS-MLD). His IPSS-R score was 5.5, stratifying him to the high risk IPSS-R group, with an estimated median overall survival of 1.6 years [7]. During his hospital stay he received a total of 2 units of packed red blood cells and 1 unit of platelets, with resolution of his chest pain and dyspnea. Prior to this time, he had not required transfusion for his marrow disorder and had only received blood product transfusions in the postoperative setting (distant open heart surgery and others). He was discharged on hospital day 6 with a follow-up appointment in hematology clinic scheduled. He rescheduled the appointment for unknown reasons and, unfortunately, passed away at home approximately three weeks after discharge. No autopsy was performed. 3. Discussion Over the last 4 decades, understanding of the pathophysiology of MDS has advanced considerably. As a result, there have been revisions in classification and risk scoring of MDS leading to improvements in the ability of clinicians to offer a more accurate prognosis for affected patients. Still, with the considerable heterogeneity and incomplete understanding of MDS, additional investigations into the mechanisms underlying the development of MDS will likely yield new information and insight into disease progression and refinements to MDS classification. This case report describes a unique case of acquired elliptocytosis presumably related to MDS, with a high percentage of ring sideroblasts. MDS with ring sideroblasts is a relatively common subtype of MDS, found in approximately 25% of all MDS cases [1]. Acquired elliptocytosis in MDS, however, is rare.only14suchcasesareavailableintheliteraturetodate (Table 1). According to the 2016 WHO guidelines, a majority of previously reported cases of acquired elliptocytosis in MDS would be classified as either MDS with single lineage dysplasia or multilineage dysplasia (10 of 14 cases) [8]. The case reported in this paper is classified as MDS with ring sideroblasts and multilineage dysplasia (MDS-RS-MLD) and is now the 15th documented case of acquired elliptocytosis in MDS. Of the 15 cases of MDS with an acquired elliptocytosis,
.")
 Bone marrow aspirate (Iron stain, 100x). The iron stained aspirate shows multiple ring sideroblasts (>15%) (arrows).")
 leading to acquisition of elliptocytosis in cases of MDS have not been definitively identified, several cases have noted decreased levels of human erythroid protein 4.")
3 Case Reports in Hematology 3 (a) (b) (c) Figure 2: (a) Bone marrow aspirate (Wright-Giemsa stain, 100x). High magnification of the bone marrow aspirate shows a marrow with erythroid hyperplasia, megaloblastic maturation, and a dysplastic erythroid cell (arrow). (b) Bone marrow aspirate (Wright-Giemsa stained, 100x). High magnification of the bone marrow aspirate shows a dysplastic megakaryocyte with separate lobes. (c) Bone marrow aspirate (Iron stain, 100x). The iron stained aspirate shows multiple ring sideroblasts (>15%) (arrows). 14 reported cytogenetics, and, of those 14 patients, 11 had deletions of chromosome 20q. While the causal factor(s) leading to acquisition of elliptocytosis in cases of MDS have not been definitively identified, several cases have noted decreased levels of human erythroid protein 4.1 in association with del(20q) [9 11]. This protein is a major cytoskeleton component in erythrocytes and reductions in its levels are implicated in a small percentage of cases of hereditary elliptocytosis [4, 5]. Interestingly, the EPB41 gene, which codes for human erythroid protein 4.1 is found on chromosome 1 ( [9]. Since the common location of lost genetic material in most of the cases of MDS with acquired elliptocytosis is on chromosome 20, it has been hypothesized that the association between del(20q) and reduced levels of human erythroid protein 4.1 is a consequence of loss of factors affecting transcription or splicing of the EPB41 gene s mrna [9]. Of note, among the 14 known patients with MDS and acquired elliptocytosis who have cytogenetic data available, only one had a chromosome 1 abnormality and this patient also had adeletiononchromosome20[12].wecanspeculatethat there may be a role for cooperating mutations, possibly involving splice factors such as the one coded for by SF3B1 and downregulation of EPB41 or another gene coding for an erythrocyte membrane protein, leading to peripheral elliptocytosis in MDS. Such a mechanism would provide an explanation for the development of elliptocytosis in MDS and at the same time link the seemingly unrelated observations of decreased levels of human erythroid protein 4.1 and deletion of chromosome 20q in MDS with acquired elliptocytosis [9 11]. To evaluate this idea, future cases of MDS with acquired elliptocytosis should be studied using techniques such as next-generation sequencing based myeloid mutation profiling, RNA-sequencing to evaluate mrna expression, and gene expression profiling. A correlation between deletions on the long arm of chromosome 20 and acquisition of elliptocytosis in MDS has emerged since the first patient with acquired elliptocytosis in what we now call MDS was reported by Hartz et al. in 1984 (then called preleukemic syndrome) and the first such case where cytogenetic studies were performed by Rummens et al.in1986[13,14].thefocusofthisreportisonarareand interesting finding, but it should be noted that chromosome 20 deletions are not uncommon in MDS. Chromosome 20 deletions were found in 7% of MDS cases in one large case series and are common enough to be included as a variable in the IPSS-R for MDS [7, 15]. While del(20q) has been shown to confer good cytogenetic risk, the impact of acquired elliptocytosis on prognosis is unknown and may benefit from further study [16]. The observation that acquired elliptocytosis seems to be related to del(20q) in MDS leads one to question why acquired elliptocytosis is so rare, given that 20q deletions are relatively common in MDS. To our knowledge, this question has yet to be addressed. Future research aimed at resolving this paradox may help to further refine the categorization or risk stratification for patients with MDS if a causative link between del(20q) and acquired elliptocytosis can be established.
4 4 Case Reports in Hematology Table 1: Characteristics of the current and previously published cases of myelodysplastic syndrome with acquired elliptocytosis. Age and gender FAB classification 2016 WHO classification 81, male RA MDS-like CMML 46,XY,i(14)(q10)[5]/46,XY[35] Cytogenetics IPSS-R score Reported outcome Reference number 3-4 (blasts <5% but NR [6] 67, female RA-EB MDS-EB-2 del(20)(q11q13)[20] 5 NR [17] 72, male RA MDS-MLD NR 75, male RA MDS-MLD Del(20q)(q11.2) 59, male RA MDS-MLD 44,XY;-3,-5,12p+,-15,17pand45,XY;-5, 12p+, -15,17p 0 5 (cytogenetics NR, blasts <5% but may be >2%) 2-3 (blasts <5% but 60, male RA-EB MDS-EB-1 Del(20q) 4 82, male RA MDS-SLD or MLD 46 XY, del(20q)(q11.2) 79, male RA MDS-SLD or MLD 46 XY, del(20q)(q11.2) 78, male RA MDS-SLD or MLD Del(20)(q11.2) 74, female RA MDS-SLD or MLD t(14) 77, male RA MDS-SLD or MLD Del(20q) Death, 8 years after diagnosis [13] NR [18] 7 NR [14] (blasts <5% but may be >2%, ANC NR) (blasts <5% but 1-2 (blasts <5% but 3-4 (blasts <5% but 1-2 (blasts <5% but 66, male RA MDS-UorCCUS 46,XY,del(20)(q11.2)[20] (ANC NR) 59, male RA MDS-MLD Del(20q) (platelets NR, blasts <5% but may be >2%) 72, male RA MDS-SLD +1,der(1;5)(q10;p10),t(1;5)(p10;q10),del(20)(q11) 5 70, male RARS MDS RS-MLD 46,XY,del(20)(q11.2q13.3)/47,idem,+del(20) 5.5 Progressed to AML within 1 year of MDS diagnosis, death 1 year later [14] NR [19] NR [19] NR [9] NR [9] NR [9] Progressed to RA-EB, achieved remission with therapy [10] NR [11] Reported to have remained wellfor18monthsat publication Death, 1 month after diagnosis [12] Currently reported case FAB and 2016 WHO classifications were determined using data from published cases. Where data are not sufficient to determine classification, the possible classifications based on available information are shown. IPSS-R score calculated using data from published cases. Where insufficient data is available, the range of possible scores is presented with missing information noted in parentheses. General abbreviations:anc: absolute neutrophil count, MPN: myeloproliferative neoplasm, NA: not applicable, NR: not reported, FAB abbreviations: RA: refractory anemia, RA-EB: refractory anemia with excess blasts, RARS: refractory anemia with ring sideroblasts. WHO 2016 abbreviations: MDS-SLD: MDS with single lineage dysplasia, MDS-MLD: MDS with multilineage dysplasia, MDS-MLD-RS: MDS with multilineage dysplasia and ring sideroblasts, MDS-EB-1/2: MDS with excess blasts 1 or 2, MDS-U: MDS unclassifiable, AML: acute myeloid leukemia, CMML: chronic myelomonocytic leukemia, CCUS: clonal cytopenia of unclear significance. One case not included in this report was classified as MDS/MPN when published in 2008 but would now be classified as AML based on 25% blasts on bone marrow biopsy. Molecular data available for this case; reported findings included no mutation in JAK2, CALR, ormpl.
5 Case Reports in Hematology 5 Disclosure The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Conflicts of Interest The authors declare that there are no conflicts of interest regarding the publication of this article. Authors Contributions Jacob D. Kjelland and Brian A. Jonas designed the study. Denis M. Dwyre contributed the images. Jacob D. Kjelland, DenisM.Dwyre,andBrianA.Jonaswroteandeditedthe manuscript. All authors agree on the final manuscript. Acknowledgments Brian A. Jonas is supported by the National Cancer Institute of the National Institutes of Health under Award no. K12CA References [1] I. Navarro, M. A. Ruiz, A. Cabello et al., Classification and scoring systems in myelodysplastic syndromes: a retrospective analysis of 311 patients, Leukemia Research, vol.30,no.8,pp , [2] E. Papaemmanuil, M. Cazzola, J. Boultwood et al., Somatic SF3B1 Mutation in Myelodysplasia with Ring Sideroblasts, The New England Medicine,vol.365,no.15,pp , [3] L.Malcovati,M.Karimi,E.Papaemmanuiletal., SF3B1mutation identifies a distinct subset of myelodysplastic syndrome with ring sideroblasts, Blood, vol. 126, no. 2, pp , [4] P. G. Gallagher, Hereditary elliptocytosis: spectrin and protein 4.1R, Seminars in Hematology, vol. 41, no. 2, pp , [5] W.T.TseandS.E.Lux, Redbloodcellmembranedisorders, British Haematology,vol.104,no.1,pp.2 13,1999. [6]M.G.Boavida,P.Ambrósio,D.Dhermy,C.Silva,andM.E. Correia Jr., Isochromosome 14q in refractory anemia, Cancer Genetics and Cytogenetics, vol. 97, no. 2, pp , [7]P.L.Greenberg,H.Tuechler,J.Schanzetal., Revisedinternational prognostic scoring system for myelodysplastic syndromes, Blood, vol. 120, no. 12, pp , [8] D.A.Arber,A.Orazi,R.Hasserjianetal., The2016revision to the World Health Organization classification of myeloid neoplasms and acute leukemia, Blood,vol.127,no.20,pp , [9] C. Alanio-Bréchot, P.-O. Schischmanoff, M. Fénéant-Thibault et al., Association between myeloid malignancies and acquired deficit in protein 4.1R: a retrospective analysis of six patients, American Hematology, vol.83,no.4,pp , [10] M. Hur, K. M. Lee, H. C. Cho et al., Protein 4.1 deficiency and deletion of chromosome 20q are associated with acquired elliptocytosis in myelodysplastic syndrome, Clinical and Laboratory Haematology,vol.26,no.1,pp.69 72,2004. [11] H. Ideguchi, Y. Yamada, S. Kondo, K. Tamura, S. Makino, and N. Hamasaki, Abnormal erythrocyte band 4.1 protein in myelodysplastic syndrome with elliptocytosis, British Journal of Haematology,vol.85,no.2,pp ,1993. [12] F. Ishida, S. Shimodaira, H. Kobayashi et al., Elliptocytosis in myelodysplastic syndrome associated with translocation (1;5)(p10;q10) and deletion of 20q, Cancer Genetics and Cytogenetics,vol.108,no.2,pp ,1999. [13] J.W.Hartz,D.H.Buss,D.R.White,M.G.Bond,andM.Scharyj, Marked elliptocytosis and schistocytosis in hematopoietic dysplasia, American Clinical Pathology, vol. 82, no. 3, pp , [14] J. L. Rummens, C. Verfaillie, A. Criel et al., Elliptocytosis and schistocytosis in myelodysplasia: report of two cases, Acta Haematologica,vol.75,no.3,pp ,1986. [15] D. Haase, U. Germing, J. Schanz et al., New insights into the prognostic impact of the karyotype in MDS and correlation with subtypes: evidence from a core dataset of 2124 patients, Blood,vol.110,no.13,pp ,2007. [16] J. Schanz, H. Tüchler, F. Solé et al., New comprehensive cytogenetic scoring system for primary myelodysplastic syndromes (MDS) and oligoblastic acute myeloid leukemia after MDS derived from an international database merge, Clinical Oncology,vol.30,no.8,pp ,2012. [17] R. Boutault and M. Eveillard, Acquired elliptocytosis in the setting of a refractory anemia with excess blasts and del(20q), Blood,vol.127,no.21,p.2646,2016. [18] J. Knight and D. R. Czuchlewski, Acquired elliptocytosis of myelodysplastic syndrome, Blood, vol. 121, no. 4, p. 572, [19] M. Baweja, A. Moreno-Aspitia, D. Menke et al., Marked elliptocytosis in myelodysplastic syndromes (MDS) is associated to deletion of chromosome 20q, Blood, vol. 106, article4927, 2005.
















6 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Correspondence should be addressed to Anas Khanfar;
 Case Reports in Oncological Medicine, Article ID 949515, 4 pages http://dx.doi.org/10.1155/2014/949515 Case Report Durable Hematological and Major Cytogenetic Response in a Patient with Isolated 20q Deletion
Case Reports in Oncological Medicine, Article ID 949515, 4 pages http://dx.doi.org/10.1155/2014/949515 Case Report Durable Hematological and Major Cytogenetic Response in a Patient with Isolated 20q Deletion
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls
 Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
2013 AAIM Pathology Workshop
 2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed
 MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
What is MDS? Epidemiology, Diagnosis, Classification & Risk Stratification
 What is MDS? Epidemiology, Diagnosis, Classification & Risk Stratification Rami Komrokji, MD Clinical Director Malignant Hematology Moffitt Cancer Center Normal Blood and Bone Marrow What is MDS Myelodysplastic
What is MDS? Epidemiology, Diagnosis, Classification & Risk Stratification Rami Komrokji, MD Clinical Director Malignant Hematology Moffitt Cancer Center Normal Blood and Bone Marrow What is MDS Myelodysplastic
When Cancer Looks Like Something Else: How Does Mutational Profiling Inform the Diagnosis of Myelodysplasia?
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Changes to the 2016 WHO Classification for the Diagnosis of MDS
 Changes to the 2016 WHO Classification for the Diagnosis of MDS Welcome to Managing MDS. I am Dr. Ulrich Germing, and today, I will provide highlights from the 14th International Symposium on MDS in Valencia,
Changes to the 2016 WHO Classification for the Diagnosis of MDS Welcome to Managing MDS. I am Dr. Ulrich Germing, and today, I will provide highlights from the 14th International Symposium on MDS in Valencia,
Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Policy Specific Section:
 Medical Policy Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Type: Medical Necessity and Investigational / Experimental Policy Specific Section:
Medical Policy Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Type: Medical Necessity and Investigational / Experimental Policy Specific Section:
MDS: Who gets it and how is it diagnosed?
 MDS: Who gets it and how is it diagnosed? October 16, 2010 Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine Weill Medical College of Cornell University The New York Presbyterian
MDS: Who gets it and how is it diagnosed? October 16, 2010 Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine Weill Medical College of Cornell University The New York Presbyterian
Myelodysplastic Syndrome: Let s build a definition
 1 MDS: Diagnosis and Treatment Update Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine Weill Medical College of Cornell University The New York Presbyterian Hospital Myelodysplastic
1 MDS: Diagnosis and Treatment Update Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine Weill Medical College of Cornell University The New York Presbyterian Hospital Myelodysplastic
MDS 101. What is bone marrow? Myelodysplastic Syndrome: Let s build a definition. Dysplastic? Syndrome? 5/22/2014. What does bone marrow do?
 101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
MYELODYSPLASTIC SYNDROMES
 MYELODYSPLASTIC SYNDROMES Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra university hospital, Isfahan university of medical sciences Key Features ESSENTIALS OF DIAGNOSIS Cytopenias
MYELODYSPLASTIC SYNDROMES Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra university hospital, Isfahan university of medical sciences Key Features ESSENTIALS OF DIAGNOSIS Cytopenias
Hematology Unit Lab 2 Review Material
 Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Myelodysplastic syndromes
 Myelodysplastic syndromes Robert P Hasserjian Massachusetts General Hospital, Boston, MA Disclosure of Relevant Financial Relationships Dr. Hasserjian declares he has no conflict(s) of interest to disclose.
Myelodysplastic syndromes Robert P Hasserjian Massachusetts General Hospital, Boston, MA Disclosure of Relevant Financial Relationships Dr. Hasserjian declares he has no conflict(s) of interest to disclose.
Table 1: biological tests in SMD
 Table 1: biological tests in SMD Tests Mandatory Recommended Under validation Morphology Marrow aspirate Marrow biopsy 1 Iron staining Quantification of dysplasia WHO 2008 Classification Cytogenetics Conventional
Table 1: biological tests in SMD Tests Mandatory Recommended Under validation Morphology Marrow aspirate Marrow biopsy 1 Iron staining Quantification of dysplasia WHO 2008 Classification Cytogenetics Conventional
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms
 & Myeloproliferative neoplasms") Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
NOVEL APPROACHES IN THE CLASSIFICATION AND RISK ASSESSMENT OF PATIENTS WITH MYELODYSPLASTIC SYNDROMES-CLINICAL IMPLICATION
 ORIGINAL ARTICLES NOVEL APPROACHES IN THE CLASSIFICATION AND RISK ASSESSMENT OF PATIENTS WITH MYELODYSPLASTIC SYNDROMES-CLINICAL IMPLICATION Ilina Micheva 1, Rosen Rachev 1, Hinco Varbanov 1, Vladimir
ORIGINAL ARTICLES NOVEL APPROACHES IN THE CLASSIFICATION AND RISK ASSESSMENT OF PATIENTS WITH MYELODYSPLASTIC SYNDROMES-CLINICAL IMPLICATION Ilina Micheva 1, Rosen Rachev 1, Hinco Varbanov 1, Vladimir
Heme 9 Myeloid neoplasms
 Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data
 Post-HCT Data") Instructions for Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data (Form 2114) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Myelodysplasia/Myeloproliferative
Instructions for Myelodysplasia/Myeloproliferative Neoplasms (MDS/MPN) Post-HCT Data (Form 2114) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the Myelodysplasia/Myeloproliferative
CASE 106. Pancytopenia in the setting of marrow hypoplasia, a PNH clone, and a DNMT3A mutation
 CASE 106 Pancytopenia in the setting of marrow hypoplasia, a PNH clone, and a DNMT3A mutation Gabriel C. Caponetti, MD University of Pennsylvania, US Clinical history 69, F peripheral neuropathy, refractory
CASE 106 Pancytopenia in the setting of marrow hypoplasia, a PNH clone, and a DNMT3A mutation Gabriel C. Caponetti, MD University of Pennsylvania, US Clinical history 69, F peripheral neuropathy, refractory
Hematology 101. Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD
 Hematology 101 Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD Hematocrits Plasma White cells Red cells Normal, Hemorrhage, IDA, Leukemia,
Hematology 101 Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD Hematocrits Plasma White cells Red cells Normal, Hemorrhage, IDA, Leukemia,
Juvenile Myelomonocytic Leukemia (JMML)
") Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
Myelodysplastic syndromes and the new WHO 2016 classification
 Myelodysplastic syndromes and the new WHO 2016 classification 32nd General Annual Meeting of the Belgian Hematology Society 10-11 February 2017 Gregor Verhoef, Departement of Hematology, University Hospital
Myelodysplastic syndromes and the new WHO 2016 classification 32nd General Annual Meeting of the Belgian Hematology Society 10-11 February 2017 Gregor Verhoef, Departement of Hematology, University Hospital
CHALLENGING CASES PRESENTATION
 CHALLENGING CASES PRESENTATION Michael C. Wiemann, MD, FACP Program Co-Chair and Vice President Indy Hematology Education President, Clinical St. John Providence Physician Network Detroit, Michigan 36
CHALLENGING CASES PRESENTATION Michael C. Wiemann, MD, FACP Program Co-Chair and Vice President Indy Hematology Education President, Clinical St. John Providence Physician Network Detroit, Michigan 36
Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas. James J. Stark, MD, FACP
 Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS
Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS
RAEB-2 2 Transforming to Acute Erythroleukemia Case # 165
 RAEB-2 2 Transforming to Acute Erythroleukemia Case # 165 Sebastian J. Sasu, M.D. UCLA Medical Center, Hematopathology Los Angeles, CA and Saint John s s Health Center Santa Monica, CA Clinical History
RAEB-2 2 Transforming to Acute Erythroleukemia Case # 165 Sebastian J. Sasu, M.D. UCLA Medical Center, Hematopathology Los Angeles, CA and Saint John s s Health Center Santa Monica, CA Clinical History
Treatment of low risk MDS
 Treatment of low risk MDS Matteo G Della Porta Cancer Center IRCCS Humanitas Research Hospital & Humanitas University Rozzano Milano, Italy matteo.della_porta@hunimed.eu International Prognostic Scoring
Treatment of low risk MDS Matteo G Della Porta Cancer Center IRCCS Humanitas Research Hospital & Humanitas University Rozzano Milano, Italy matteo.della_porta@hunimed.eu International Prognostic Scoring
NUMERATOR: Patients who had baseline cytogenetic testing performed on bone marrow
 Quality ID #67 (NQF 0377): Hematology: Myelodysplastic Syndrome (MDS) and Acute Leukemias: Baseline Cytogenetic Testing Performed on Bone Marrow National Quality Strategy Domain: Effective Clinical Care
Quality ID #67 (NQF 0377): Hematology: Myelodysplastic Syndrome (MDS) and Acute Leukemias: Baseline Cytogenetic Testing Performed on Bone Marrow National Quality Strategy Domain: Effective Clinical Care
ACCME/Disclosures. History. Hematopathology Specialty Conference Case #4 4/13/2016
 Hematopathology Specialty Conference Case #4 Sherrie L. Perkins MD, PhD University of Utah ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose
Hematopathology Specialty Conference Case #4 Sherrie L. Perkins MD, PhD University of Utah ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose
A prospective, multicenter European Registry for newly diagnosed patients with Myelodysplastic Syndromes of IPSS low and intermediate-1 subtypes.
 Protocol Synopsis Study Title A prospective, multicenter European Registry for newly diagnosed patients with Myelodysplastic Syndromes of IPSS low and intermediate-1 subtypes. Short Title European MDS
Protocol Synopsis Study Title A prospective, multicenter European Registry for newly diagnosed patients with Myelodysplastic Syndromes of IPSS low and intermediate-1 subtypes. Short Title European MDS
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms. Curtis A. Hanson, MD
 Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
SESSION 1 Reactive cytopenia and dysplasia
 SESSION 1 Reactive cytopenia and dysplasia Falko Fend, Tübingen & Alexandar Tzankov, Basel 1 Disclosure of speaker s interests (Potential) conflict of interest none Potentially relevant company relationships
SESSION 1 Reactive cytopenia and dysplasia Falko Fend, Tübingen & Alexandar Tzankov, Basel 1 Disclosure of speaker s interests (Potential) conflict of interest none Potentially relevant company relationships
Myelodysplastic Syndrome Case 158
 Myelodysplastic Syndrome Case 158 Dong Chen MD PhD Division of Hematopathology Mayo Clinic Clinical History 86 year old man Persistent borderline anemia and thrombocytopenia. His past medical history was
Myelodysplastic Syndrome Case 158 Dong Chen MD PhD Division of Hematopathology Mayo Clinic Clinical History 86 year old man Persistent borderline anemia and thrombocytopenia. His past medical history was
Chronic Myelomonocytic Leukemia with molecular abnormalities SH
 Chronic Myelomonocytic Leukemia with molecular abnormalities SH2017-0351 Madhu P. Menon MD,PhD, Juan Gomez MD, Kedar V. Inamdar MD,PhD and Kristin Karner MD Madhu P Menon, MD, PhD Henry Ford Hospital Patient
Chronic Myelomonocytic Leukemia with molecular abnormalities SH2017-0351 Madhu P. Menon MD,PhD, Juan Gomez MD, Kedar V. Inamdar MD,PhD and Kristin Karner MD Madhu P Menon, MD, PhD Henry Ford Hospital Patient
Myeloid neoplasms. Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories:
 Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms. Daniel A. Arber, MD Stanford University
 Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms Daniel A. Arber, MD Stanford University What is an integrated approach? What is an integrated approach? Incorporating all diagnostic
Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms Daniel A. Arber, MD Stanford University What is an integrated approach? What is an integrated approach? Incorporating all diagnostic
Myelodysplastic Syndromes Myeloproliferative Disorders
 Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD. Part 4 MYELOID NEOPLASMS
 HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
Participants Identification No. % Evaluation. Mitotic figure Educational Erythrocyte precursor, abnormal 1 0.
 Cell Identification Mitotic figure 212 99.5 Educational Erythrocyte precursor, abnormal BMD-02 The arrowed cell is a mitotic figure. It was correctly identified by 99.5% of the participants. A cell containing
Cell Identification Mitotic figure 212 99.5 Educational Erythrocyte precursor, abnormal BMD-02 The arrowed cell is a mitotic figure. It was correctly identified by 99.5% of the participants. A cell containing
Myelodysplastic Syndromes
 Please complete our online survey at NCCN GUIDELINES FOR PATIENTS NCCN.org/patients/survey 2018 Myelodysplastic Syndromes Presented with support from: Available online at NCCN.org/patients Ü Myelodysplastic
Please complete our online survey at NCCN GUIDELINES FOR PATIENTS NCCN.org/patients/survey 2018 Myelodysplastic Syndromes Presented with support from: Available online at NCCN.org/patients Ü Myelodysplastic
Myelodysplastic syndromes: revised WHO classification and distinction from non-neoplastic conditions
 Myelodysplastic syndromes: revised WHO classification and distinction from non-neoplastic conditions Robert P Hasserjian, MD Associate Professor Massachusetts General Hospital and Harvard Medical School
Myelodysplastic syndromes: revised WHO classification and distinction from non-neoplastic conditions Robert P Hasserjian, MD Associate Professor Massachusetts General Hospital and Harvard Medical School
June 11, Ella Noel, D.O., FACOI 1717 West Broadway Madison, WI
 June 11, 2018 Ella Noel, D.O., FACOI 1717 West Broadway Madison, WI 53713 policycomments@wpsic.com RE: Draft Local Coverage Determination: MolDX: MDS FISH (DL37772) Dear Dr. Noel Thank you for the opportunity
June 11, 2018 Ella Noel, D.O., FACOI 1717 West Broadway Madison, WI 53713 policycomments@wpsic.com RE: Draft Local Coverage Determination: MolDX: MDS FISH (DL37772) Dear Dr. Noel Thank you for the opportunity
Case Presentation No. 075
 Case Presentation No. 075 Session 4. Myelodysplastic Syndrome Cristina Montalvo, MD Baylor College of Medicine Houston, Texas 2007 Workshop of Society for Hematopathology and European Association for Haematopathology
Case Presentation No. 075 Session 4. Myelodysplastic Syndrome Cristina Montalvo, MD Baylor College of Medicine Houston, Texas 2007 Workshop of Society for Hematopathology and European Association for Haematopathology
Hematology Measure #1: Myelodysplastic Syndrome (MDS) and Acute Leukemias: Baseline Cytogenetic Testing Performed on Bone Marrow
 and Acute Leukemias: Baseline Cytogenetic Testing Performed on Bone Marrow") Hematology Measure #1: Myelodysplastic Syndrome (MDS) and Acute Leukemias: Baseline Cytogenetic Testing Performed on Bone Marrow This measure may be used as an Accountability measure Clinical Performance
Hematology Measure #1: Myelodysplastic Syndrome (MDS) and Acute Leukemias: Baseline Cytogenetic Testing Performed on Bone Marrow This measure may be used as an Accountability measure Clinical Performance
Disclosures. Myeloproliferative Neoplasms: A Case-Based Approach. Objectives. Myeloproliferative Neoplasms. Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure
 Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Etiology. Definition MYELODYSPLASTIC SYNDROMES. De novo. Secondary MDS (10 years earlier than primary) transformation
 transformation") MYELODYSPLASTIC SYNDROMES Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics The University of Texas M.D. Anderson Cancer Center Houston, Texas No relevant COIs to
MYELODYSPLASTIC SYNDROMES Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics The University of Texas M.D. Anderson Cancer Center Houston, Texas No relevant COIs to
74y old Female with chronic elevation of Platelet count. August 18, 2005 Faizi Ali, MD Hematopathology Fellow
 74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
APPROACH TO MYELODYSPLASTIC SYNDROMES IN THE ERA OF PRECISION MEDICINE
 APPROACH TO MYELODYSPLASTIC SYNDROMES IN THE ERA OF PRECISION MEDICINE Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics Department of Hematopathology The University
APPROACH TO MYELODYSPLASTIC SYNDROMES IN THE ERA OF PRECISION MEDICINE Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics Department of Hematopathology The University
SWOG ONCOLOGY RESEARCH PROFESSIONAL (ORP) MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017
 MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017") LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
Let s Look at Our Blood
 Let s Look at Our Blood Casey O Connell, MD Associate Professor of Clinical Medicine Jane Anne Nohl Division of Hematology Keck School of Medicine of USC 10,000,000,000 WBCs/day Bone Marrow: The Blood
Let s Look at Our Blood Casey O Connell, MD Associate Professor of Clinical Medicine Jane Anne Nohl Division of Hematology Keck School of Medicine of USC 10,000,000,000 WBCs/day Bone Marrow: The Blood
Myelodysplastic syndromes: 2018 update on diagnosis, risk-stratification and management
 Received: 2 October 2017 Accepted: 2 October 2017 DOI: 10.1002/ajh.24930 ANNUAL CLINICAL UPDATES IN HEMATOLOGICAL MALIGNANCIES Myelodysplastic syndromes: 2018 update on diagnosis, risk-stratification and
Received: 2 October 2017 Accepted: 2 October 2017 DOI: 10.1002/ajh.24930 ANNUAL CLINICAL UPDATES IN HEMATOLOGICAL MALIGNANCIES Myelodysplastic syndromes: 2018 update on diagnosis, risk-stratification and
Pathology. #11 Acute Leukemias. Farah Banyhany. Dr. Sohaib Al- Khatib 23/2/16
 35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
HEMATOLOGIC MALIGNANCIES BIOLOGY
 HEMATOLOGIC MALIGNANCIES BIOLOGY Failure of terminal differentiation Failure of differentiated cells to undergo apoptosis Failure to control growth Neoplastic stem cell FAILURE OF TERMINAL DIFFERENTIATION
HEMATOLOGIC MALIGNANCIES BIOLOGY Failure of terminal differentiation Failure of differentiated cells to undergo apoptosis Failure to control growth Neoplastic stem cell FAILURE OF TERMINAL DIFFERENTIATION
DISCLOSURE Luca Malcovati, MD. No financial relationships to disclose
 ICUS, CCUS and CHIP Luca Malcovati, MD Department of Molecular Medicine, University of Pavia Medical School, & Department of Hematology Oncology, IRCCS Policlinico S. Matteo Foundation, Pavia, Italy DISCLOSURE
ICUS, CCUS and CHIP Luca Malcovati, MD Department of Molecular Medicine, University of Pavia Medical School, & Department of Hematology Oncology, IRCCS Policlinico S. Matteo Foundation, Pavia, Italy DISCLOSURE
About Myelodysplastic Syndromes
 About Myelodysplastic Syndromes Overview and Types If you have been diagnosed with a myelodysplastic syndrome or are worried about it, you likely have a lot of questions. Learning some basics is a good
About Myelodysplastic Syndromes Overview and Types If you have been diagnosed with a myelodysplastic syndrome or are worried about it, you likely have a lot of questions. Learning some basics is a good
Chronic Idiopathic Myelofibrosis (CIMF)
") Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Kaaren Reichard Mayo Clinic Rochester
 Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester Reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Present
Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester Reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Present
Myelodysplastic Syndromes: Hematopathology. Analysis of SHIP1 as a potential biomarker of Disease Progression
 Myelodysplastic Syndromes: Hematopathology. Analysis of SHIP1 as a potential biomarker of Disease Progression Carlos E. Bueso-Ramos, M.D., Ph.D Department of Hematopathology The University of Texas M.
Myelodysplastic Syndromes: Hematopathology. Analysis of SHIP1 as a potential biomarker of Disease Progression Carlos E. Bueso-Ramos, M.D., Ph.D Department of Hematopathology The University of Texas M.
Overview of guidelines on iron chelation therapy in patients with myelodysplastic syndromes and transfusional iron overload
 Int J Hematol (2008) 88:24 29 DOI 10.1007/s12185-008-0118-z PROGRESS IN HEMATOLOGY Transfusional iron overload and iron chelation therapy Overview of guidelines on iron chelation therapy in patients with
Int J Hematol (2008) 88:24 29 DOI 10.1007/s12185-008-0118-z PROGRESS IN HEMATOLOGY Transfusional iron overload and iron chelation therapy Overview of guidelines on iron chelation therapy in patients with
CLINICAL STUDY REPORT SYNOPSIS
 CLINICAL STUDY REPORT SYNOPSIS Document No.: EDMS-PSDB-5412862:2.0 Research & Development, L.L.C. Protocol No.: R115777-AML-301 Title of Study: A Randomized Study of Tipifarnib Versus Best Supportive Care
CLINICAL STUDY REPORT SYNOPSIS Document No.: EDMS-PSDB-5412862:2.0 Research & Development, L.L.C. Protocol No.: R115777-AML-301 Title of Study: A Randomized Study of Tipifarnib Versus Best Supportive Care
Tim R. Randolph. PhD, MT(ASCP) Chair and Associate Professor Department of Biomedical Laboratory Science Saint Louis University
 Chair and Associate Professor Department of Biomedical Laboratory Science Saint Louis University") Tim R. Randolph. PhD, MT(ASCP) Chair and Associate Professor Department of Biomedical Laboratory Science Saint Louis University Anemias Over 30 types Myeloproliferative Neoplasm Polycythemia Leukemia AML:M6
Tim R. Randolph. PhD, MT(ASCP) Chair and Associate Professor Department of Biomedical Laboratory Science Saint Louis University Anemias Over 30 types Myeloproliferative Neoplasm Polycythemia Leukemia AML:M6
MYELODYSPLASTIC SYNDROME. Vivienne Fairley Clinical Nurse Specialist Sheffield
 MYELODYSPLASTIC SYNDROME Vivienne Fairley Clinical Nurse Specialist Sheffield MDS INCIDENCE 1/100,000/YEAR 3,250/YEAR MEDIAN AGE 70 MDS HYPO OR HYPERCELLULAR BONE MARROW BLOOD CYTOPENIAS (EARLY STAGES
MYELODYSPLASTIC SYNDROME Vivienne Fairley Clinical Nurse Specialist Sheffield MDS INCIDENCE 1/100,000/YEAR 3,250/YEAR MEDIAN AGE 70 MDS HYPO OR HYPERCELLULAR BONE MARROW BLOOD CYTOPENIAS (EARLY STAGES
CLINICO-PATHOLOGICAL CONFERENCE CLASS OF 2007/2012 PHASE IIIB SESSION 2010/2012
 CLINICO-PATHOLOGICAL CONFERENCE CLASS OF 2007/2012 PHASE IIIB SESSION 2010/2012 PRESENTATION OF CASE A 62-year-old woman was seen in the outpatient cancer center of this hospital because of anemia and
CLINICO-PATHOLOGICAL CONFERENCE CLASS OF 2007/2012 PHASE IIIB SESSION 2010/2012 PRESENTATION OF CASE A 62-year-old woman was seen in the outpatient cancer center of this hospital because of anemia and
Session II: Summary. Robert P Hasserjian, MD Professor of Pathology Massachusetts General Hospital and Harvard Medical School
 Session II: Summary Robert P Hasserjian, MD Professor of Pathology Massachusetts General Hospital and Harvard Medical School Disclosure of speaker s interests (Prefix and Last Name) (Potential) conflict
Session II: Summary Robert P Hasserjian, MD Professor of Pathology Massachusetts General Hospital and Harvard Medical School Disclosure of speaker s interests (Prefix and Last Name) (Potential) conflict
Guidelines for diagnosis and management of Adult Myelodysplastic Syndromes (MDS)
") Guidelines for diagnosis and management of Adult Myelodysplastic Syndromes (MDS) Author: Dr A Pillai, Consultant Haematologist On behalf of the Haematology CNG Re- Written: February 2011, Version 2 Revised:
Guidelines for diagnosis and management of Adult Myelodysplastic Syndromes (MDS) Author: Dr A Pillai, Consultant Haematologist On behalf of the Haematology CNG Re- Written: February 2011, Version 2 Revised:
Erythropoiesis Stimulating Agents (ESA)
") Erythropoiesis Stimulating Agents (ESA) Policy Number: Original Effective Date: MM.04.008 04/15/2007 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 06/01/2015 Section: Prescription
Erythropoiesis Stimulating Agents (ESA) Policy Number: Original Effective Date: MM.04.008 04/15/2007 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 06/01/2015 Section: Prescription
Acute haemolysis and appearance of PNH-like clones in patients with vitamin B12 deficiency and iron deficiency after iron dextran administration
 Acute haemolysis and appearance of PNH-like clones in patients with vitamin B12 deficiency and iron deficiency after iron dextran administration Chun-Liang Lin 1, Chin-Chan Lin 1,Wen-Jyi Lo 2,Yu-Chien
Acute haemolysis and appearance of PNH-like clones in patients with vitamin B12 deficiency and iron deficiency after iron dextran administration Chun-Liang Lin 1, Chin-Chan Lin 1,Wen-Jyi Lo 2,Yu-Chien
Introduction and Approach to Anemia
 2 nd lecture in Hematology by Dr.Alaa Fadhil Alwan Introduction and Approach to Anemia Anemia is defined clinically as a blood hemoglobin or hematocrit value that is below the appropriate reference range
2 nd lecture in Hematology by Dr.Alaa Fadhil Alwan Introduction and Approach to Anemia Anemia is defined clinically as a blood hemoglobin or hematocrit value that is below the appropriate reference range
MDS - Diagnosis and Treatments. Dr Helen Enright, Adelaide and Meath Hospital Dr Catherine Flynn, St James Hospital
 MDS - Diagnosis and Treatments Dr Helen Enright, Adelaide and Meath Hospital Dr Catherine Flynn, St James Hospital Overview What is myelodysplasia? Symptoms Diagnosis and prognosis Myelodysplasia therapy
MDS - Diagnosis and Treatments Dr Helen Enright, Adelaide and Meath Hospital Dr Catherine Flynn, St James Hospital Overview What is myelodysplasia? Symptoms Diagnosis and prognosis Myelodysplasia therapy
MDS-004 Study: REVLIMID (lenalidomide) versus Placebo in Myelodysplastic Syndromes with Deletion (5q) Abnormality
 versus Placebo in Myelodysplastic Syndromes with Deletion (5q) Abnormality") MDS-4 Study: REVLIMID (lenalidomide) versus Placebo in Myelodysplastic Syndromes with Deletion (5q) Abnormality TABLE OF CONTENTS Section 1. Executive Summary Section 2. Background Section
MDS-4 Study: REVLIMID (lenalidomide) versus Placebo in Myelodysplastic Syndromes with Deletion (5q) Abnormality TABLE OF CONTENTS Section 1. Executive Summary Section 2. Background Section
The Power of Peripheral Blood Smears: Apparent Diagnostic Clues (Part 1) (Wednesday, October 19, 2011)
 (Wednesday, October 19, 2011)") The Power of Peripheral Blood Smears: Apparent Diagnostic Clues (Part 1) (Wednesday, October 19, 2011) By Gene Gulati, Ph.D., SH(ASCP) Conflict of Interest None Plan for the Course Review blood smears,
The Power of Peripheral Blood Smears: Apparent Diagnostic Clues (Part 1) (Wednesday, October 19, 2011) By Gene Gulati, Ph.D., SH(ASCP) Conflict of Interest None Plan for the Course Review blood smears,
Border between aplastic anemia and myelodysplastic syndrome
 Int J Hematol (2013) 97:558 563 DOI 10.1007/s12185-013-1324-x PROGRESS IN HEMATOLOGY Advances in the management of acquired aplastic anemia (AA) Border between aplastic anemia and myelodysplastic syndrome
Int J Hematol (2013) 97:558 563 DOI 10.1007/s12185-013-1324-x PROGRESS IN HEMATOLOGY Advances in the management of acquired aplastic anemia (AA) Border between aplastic anemia and myelodysplastic syndrome
Rory McCulloch. Specialty Trainee Haematology Royal Devon & Exeter Hospital
 Rory McCulloch Specialty Trainee Haematology Royal Devon & Exeter Hospital Anaemia 1 Haematological disorders Anaemia 2 Non-haematological disorders Substrates: Iron, folate, vitamin B12 Red cell mass
Rory McCulloch Specialty Trainee Haematology Royal Devon & Exeter Hospital Anaemia 1 Haematological disorders Anaemia 2 Non-haematological disorders Substrates: Iron, folate, vitamin B12 Red cell mass
Myelodyplastic Syndromes Paul J. Shami, M.D.
 Myelodyplastic Syndromes Paul J. Shami, M.D. Professor of Hematology, University of Utah Member, Huntsman Cancer Institute Objectives Define Myelodysplastic Syndromes (MDS) Explain how MDS are diagnosed
Myelodyplastic Syndromes Paul J. Shami, M.D. Professor of Hematology, University of Utah Member, Huntsman Cancer Institute Objectives Define Myelodysplastic Syndromes (MDS) Explain how MDS are diagnosed
Impact of Comorbidity on Quality of Life and Clinical Outcomes in MDS
 Current Therapeutic and Biologic Advances in MDS A Symposium of The MDS Foundation ASH 2014 Impact of Comorbidity on Quality of Life and Clinical Outcomes in MDS Peter Valent Medical University of Vienna
Current Therapeutic and Biologic Advances in MDS A Symposium of The MDS Foundation ASH 2014 Impact of Comorbidity on Quality of Life and Clinical Outcomes in MDS Peter Valent Medical University of Vienna
Understanding & Treating Myelodysplastic Syndrome (MDS)
") Understanding & Treating Myelodysplastic Syndrome (MDS) Casey O Connell, MD Associate Professor of Clinical Medicine Jane Anne Nohl Division of Hematology Keck School of Medicine of USC Let s Look at Our
Understanding & Treating Myelodysplastic Syndrome (MDS) Casey O Connell, MD Associate Professor of Clinical Medicine Jane Anne Nohl Division of Hematology Keck School of Medicine of USC Let s Look at Our
2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228
 2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228 Vishnu V. B Reddy, MD University of Alabama at Birmingham Birmingham, AL USA 11/03/07
2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228 Vishnu V. B Reddy, MD University of Alabama at Birmingham Birmingham, AL USA 11/03/07
Outline. Case Study 5/17/2010. Treating Lower-Risk Myelodysplastic Syndrome (MDS) Tapan M. Kadia, MD Department of Leukemia MD Anderson Cancer Center
 Tapan M. Kadia, MD Department of Leukemia MD Anderson Cancer Center") Treating Lower-Risk Myelodysplastic Syndrome (MDS) Tapan M. Kadia, MD Department of Leukemia MD Anderson Cancer Center Outline Case Study What is lower-risk MDS? Classification systems Prognosis Treatment
Treating Lower-Risk Myelodysplastic Syndrome (MDS) Tapan M. Kadia, MD Department of Leukemia MD Anderson Cancer Center Outline Case Study What is lower-risk MDS? Classification systems Prognosis Treatment
Myelodysplastic Syndrome Early Detection, Diagnosis, and Staging
 Myelodysplastic Syndrome Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that
Myelodysplastic Syndrome Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that
WHO Update to Myeloproliferative Neoplasms
 WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
Better Prognosis for Patients With Del(7q) Than for Patients With Monosomy 7 in Myelodysplastic Syndrome
 Than for Patients With Monosomy 7 in Myelodysplastic Syndrome") Better Prognosis for Patients With Del(7q) Than for Patients With Monosomy 7 in Myelodysplastic Syndrome Iris Cordoba, MD 1 ; José R. González-Porras, MD 1 ; Benet Nomdedeu, MD 2 ; Elisa Luño, MD 3 ; Raquel
Better Prognosis for Patients With Del(7q) Than for Patients With Monosomy 7 in Myelodysplastic Syndrome Iris Cordoba, MD 1 ; José R. González-Porras, MD 1 ; Benet Nomdedeu, MD 2 ; Elisa Luño, MD 3 ; Raquel
Myelodysplastic syndromes in adults aged less than 50 years: Incidence and clinicopathological data
 JBUON 2014; 19(4): 999-1005 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Myelodysplastic syndromes in adults aged less than 50 years: Incidence
JBUON 2014; 19(4): 999-1005 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Myelodysplastic syndromes in adults aged less than 50 years: Incidence
Acute myeloid leukemia. M. Kaźmierczak 2016
 Acute myeloid leukemia M. Kaźmierczak 2016 Acute myeloid leukemia Malignant clonal disorder of immature hematopoietic cells characterized by clonal proliferation of abnormal blast cells and impaired production
Acute myeloid leukemia M. Kaźmierczak 2016 Acute myeloid leukemia Malignant clonal disorder of immature hematopoietic cells characterized by clonal proliferation of abnormal blast cells and impaired production
Myelodysplastic Syndrome
 Myelodysplastic Syndrome A Family-Oriented Approach on Diagnosis and Treatment Options Cecilia Arana Yi, MD Assistant Professor MDS Patient & Family/Caregiver Forum March 3, 2018 Quote of the Day There
Myelodysplastic Syndrome A Family-Oriented Approach on Diagnosis and Treatment Options Cecilia Arana Yi, MD Assistant Professor MDS Patient & Family/Caregiver Forum March 3, 2018 Quote of the Day There
Concise Review for Primary-Care Physicians
 Concise Review for Primary-Care Physicians Myelodysplastic (Preleukemia) Syndromes: The Bone Marrow Factory Failure Problem H. CLARK HOAGLAND, M.D. The myelodysplastic syndromes are a group of hematologic
Concise Review for Primary-Care Physicians Myelodysplastic (Preleukemia) Syndromes: The Bone Marrow Factory Failure Problem H. CLARK HOAGLAND, M.D. The myelodysplastic syndromes are a group of hematologic
Anemia. A case-based approach. David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017
 Anemia A case-based approach David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017 Recognizing trends Learning Objectives MCV, RDW, Ferritin, LDH, Reticulocytes Managing complex patients 1.
Anemia A case-based approach David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017 Recognizing trends Learning Objectives MCV, RDW, Ferritin, LDH, Reticulocytes Managing complex patients 1.
MORPHOLOGY IN ACTION. Description MINI-CASE ONE OBJECTIVES. Differential Diagnosis. Laboratory Results
 MORPHOLOGY IN ACTION Mini-case studies using morphology Bernadette Rodak, MS, MT, SH(ASCP) Professor emeritus Indiana University brodak@iupui.edu Description Mini-case studies will be used to integrate
MORPHOLOGY IN ACTION Mini-case studies using morphology Bernadette Rodak, MS, MT, SH(ASCP) Professor emeritus Indiana University brodak@iupui.edu Description Mini-case studies will be used to integrate
Abstracting Hematopoietic Neoplasms
 CASE 1: LYMPHOMA PHYSICAL EXAMINATION 43yo male with a history of lower gastrointestinal bleeding and melena undergoing colonoscopy and biopsy to rule out neoplasm versus inflammation. Patient had no other
CASE 1: LYMPHOMA PHYSICAL EXAMINATION 43yo male with a history of lower gastrointestinal bleeding and melena undergoing colonoscopy and biopsy to rule out neoplasm versus inflammation. Patient had no other
Darbepoetin alfa (Aranesp) for treatment of anaemia in adults with low or intermediate-1-risk myelodysplastic syndromes
 for treatment of anaemia in adults with low or intermediate-1-risk myelodysplastic syndromes") NIHR Innovation Observatory Evidence Briefing: August 2017 Darbepoetin alfa (Aranesp) for treatment of anaemia in adults with low or intermediate-1-risk myelodysplastic syndromes NIHRIO (HSRIC) ID: 13763
NIHR Innovation Observatory Evidence Briefing: August 2017 Darbepoetin alfa (Aranesp) for treatment of anaemia in adults with low or intermediate-1-risk myelodysplastic syndromes NIHRIO (HSRIC) ID: 13763
Myelodysplastic Syndromes
 Myelodysplastic Syndromes Attilio Orazi, MD, FRCPath, 1 and Magdalena B. Czader, MD, PhD 2 Key Words: Myelodysplastic syndrome; Refractory cytopenia with unilineage dysplasia; Refractory anemia with ring
Myelodysplastic Syndromes Attilio Orazi, MD, FRCPath, 1 and Magdalena B. Czader, MD, PhD 2 Key Words: Myelodysplastic syndrome; Refractory cytopenia with unilineage dysplasia; Refractory anemia with ring
Case Report Immune Thrombocytopenia and JAK2V617F Positive Essential Thrombocythemia: Literature Review and Case Report
 Hindawi Case Reports in Hematology Volume 2017, Article ID 3725089, 4 pages https://doi.org/10.1155/2017/3725089 Case Report Immune Thrombocytopenia and JAK2V617F Positive Essential Thrombocythemia: Literature
Hindawi Case Reports in Hematology Volume 2017, Article ID 3725089, 4 pages https://doi.org/10.1155/2017/3725089 Case Report Immune Thrombocytopenia and JAK2V617F Positive Essential Thrombocythemia: Literature
Myelodysplastic scoring system with flow cytometry. G Detry B Husson
 Myelodysplastic scoring system with flow cytometry G Detry B Husson Myelodysplastic syndroms Clonal haematopoietic stem cell disease characterized by dysplasia in one or more of the myeloid cell lines
Myelodysplastic scoring system with flow cytometry G Detry B Husson Myelodysplastic syndroms Clonal haematopoietic stem cell disease characterized by dysplasia in one or more of the myeloid cell lines
Ordering Physician CLIENT,CLIENT. Collected REVISED REPORT
 HPWET Hematopathology Consultation, MML Embed Client Hematopathology Consult REVISED INAL DIAGNOSIS Interpretation Peripheral blood, bone marrow aspirate and biopsies, bilateral iliac crests: 1. Normocellular
HPWET Hematopathology Consultation, MML Embed Client Hematopathology Consult REVISED INAL DIAGNOSIS Interpretation Peripheral blood, bone marrow aspirate and biopsies, bilateral iliac crests: 1. Normocellular
Welcome to Master Class for Oncologists. Session 3: 9:15 AM - 10:00 AM
 Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Primary myelofibrosis
 - It s a bone marrow fibrosis Primary myelofibrosis - It's type of myeloproliferative disease i.e. neoplastic proliferation of mature cell of myloid linage. - Its similar to chronic myloid leukemia (CML).
- It s a bone marrow fibrosis Primary myelofibrosis - It's type of myeloproliferative disease i.e. neoplastic proliferation of mature cell of myloid linage. - Its similar to chronic myloid leukemia (CML).
Overview of Aplastic Anemia. Overview of Aplastic Anemia. Epidemiology of aplastic anemia. Normal hematopoiesis 10/6/2017
 Overview of Aplastic Anemia Overview of Aplastic Anemia Peter Westervelt, MD, PhD Professor of Medicine Chief, BMT/Leukemia Section Washington University School of Medicine Epidemiology Normal hematopoiesis
Overview of Aplastic Anemia Overview of Aplastic Anemia Peter Westervelt, MD, PhD Professor of Medicine Chief, BMT/Leukemia Section Washington University School of Medicine Epidemiology Normal hematopoiesis
Myeloproliferative Disorders in the Elderly: Clinical Presentation and Role of Bone Marrow Examination
 Myeloproliferative Disorders in the Elderly: Clinical Presentation and Role of Bone Marrow Examination Arati V. Rao, M.D. Division of Medical Oncology and Geriatrics Duke University Medical Center Durham
Myeloproliferative Disorders in the Elderly: Clinical Presentation and Role of Bone Marrow Examination Arati V. Rao, M.D. Division of Medical Oncology and Geriatrics Duke University Medical Center Durham
Year 2003 Paper two: Questions supplied by Tricia
 QUESTION 65 A 36-year-old man presents in a post-ictal state after an observed generalised seizure. Full blood investigation shows: haemoglobin 0 g/l [128-175] mean corpuscular volume (MCV) 106 fl [80-7]
QUESTION 65 A 36-year-old man presents in a post-ictal state after an observed generalised seizure. Full blood investigation shows: haemoglobin 0 g/l [128-175] mean corpuscular volume (MCV) 106 fl [80-7]
12 Dynamic Interactions between Hematopoietic Stem and Progenitor Cells and the Bone Marrow: Current Biology of Stem Cell Homing and Mobilization
 Table of Contents: PART I: Molecular and Cellular Basis of Hematology 1 Anatomy and Pathophysiology of the Gene 2 Genomic Approaches to Hematology 3 Regulation of Gene Expression, Transcription, Splicing,
Table of Contents: PART I: Molecular and Cellular Basis of Hematology 1 Anatomy and Pathophysiology of the Gene 2 Genomic Approaches to Hematology 3 Regulation of Gene Expression, Transcription, Splicing,