Update on Antiretroviral Treatment for HIV Infection 2008
|
|
|
- Kristina Watts
- 5 years ago
- Views:
Transcription


1 Update on Antiretroviral Treatment for HIV Infection 2008 Janet Gilmour MD FRCP(C) Clinical Associate Professor of Medicine University of Calgary November 2008
2 Disclosure and Acknowledgements Disclosure: : Speakers fee from Abbott Consultancy fee from Pfizer Acknowledgements: -UNAIDS 2008 Report on the Global AIDS Epidemic -CDC HIV Mortality Slides -AETC NRC Antiretroviral Treatment Adults and Adolescents

3 Learning Objectives Participants should be able to summarize the indications for antiretroviral therapy for HIV infection according to 2008 guidelines Participants should be aware of factors influencing choice of antiretroviral regimen for an individual patient Participants should be able to list the goals of antiretroviral therapy for HIV infection Participants should be able to discuss the potential benefits and risks of earlier initiation of HAART for HIV infection Participants should be able to identify emerging issues in the treatment of HIV infected persons
4 Outline Review Status of Global HIV Epidemic Impact of Antiretroviral Therapy on HIV morbidity/mortality 2008 HIV Treatment Guidelines Important considerations in ART Goals of ART for HIV Infection Emerging issues in HIV treatment Potential Benefits of earlier ART
5 Global summary of the AIDS epidemic, December 2007 Number of people living with HIV in 2007 Total Adults Women Children under 15 years 33 million [30 36 million] 30.8 million [ million] 15.5 million [ million] 2.0 million [ million] People newly infected with HIV in 2007 Total 2.7 million [ million] Adults 2.3 million [ million] Children under 15 years [ ] AIDS deaths in 2007 Total 2.0 million [ million] Adults 1.8 million [ million] Children under 15 years [ ]
6 Adults and children estimated to be living with HIV, 2007 North America 1.2 million [ million] Caribbean [ ] Latin America 1.7 million [ million] Western & Eastern Europe Central Europe & Central Asia [ million] Middle East & North Africa [ ] Sub-Saharan Africa 22.0 million [ million] 1.5 million [ million] East Asia [ million] South & South-East Asia 4.2 million [3.5 Oceania 5.3 million] [ ] Total: 33 million (30 36 million)
7 Estimated adult and child deaths from AIDS, 2007 North America [ ] Caribbean [ ] Latin America [ ] Western & Eastern Europe Central Europe & Central Asia 8000 [ ] Middle East & North Africa [ ] Sub-Saharan Africa 1.5 million [ million] [ ] East Asia [ ] South & South-East Asia [ Oceania ] 1000 [< ] ( million Total: 2.0 million (
8 Estimated number of adults and children newly infected with HIV, 2007 North America [ ] Caribbean [ ] Latin America [ ] Western & Eastern Europe Central Europe & Central Asia [ ] Middle East & North Africa [ ] Sub-Saharan Africa 1.9 million [ million] [ ] East Asia [ ] South & South-East Asia [ Oceania ] [ ] ( million Total: 2.7 million (
9 Over 7400 new HIV infections a day in 2007 More than 96% are in low and middle income countries About 1000 are in children under 15 years of age About 6300 are in adults aged 15 years and older of whom: almost 50% are among women ( ) about 45% are among young people
10 Number of people receiving antiretroviral drugs in low- and middle income countries, Millions end end end end end end North Africa and the Middle East Eastern Europe and Central Asia East, South and South-East Asia Latin America and the Caribbean Sub-Saharan Africa Year Source: Data provided by UNAIDS & WHO, /19/
11 Estimated number of adult and child deaths due to AIDS globally, Millions Year This bar indicates the range 11/19/
12 Number and percentage of HIV-positive pregnant women receiving antiretroviral prophylaxis, Number of HIV-positive pregnant women receiving antiretrovirals % of HIV-positive pregnant women receiving antiretrovirals Year Source: UNAIDS, UNICEF & WHO, 2008; data provided by countries. 11/19/
13 New infections among children, Year This bar indicates the range 11/19/
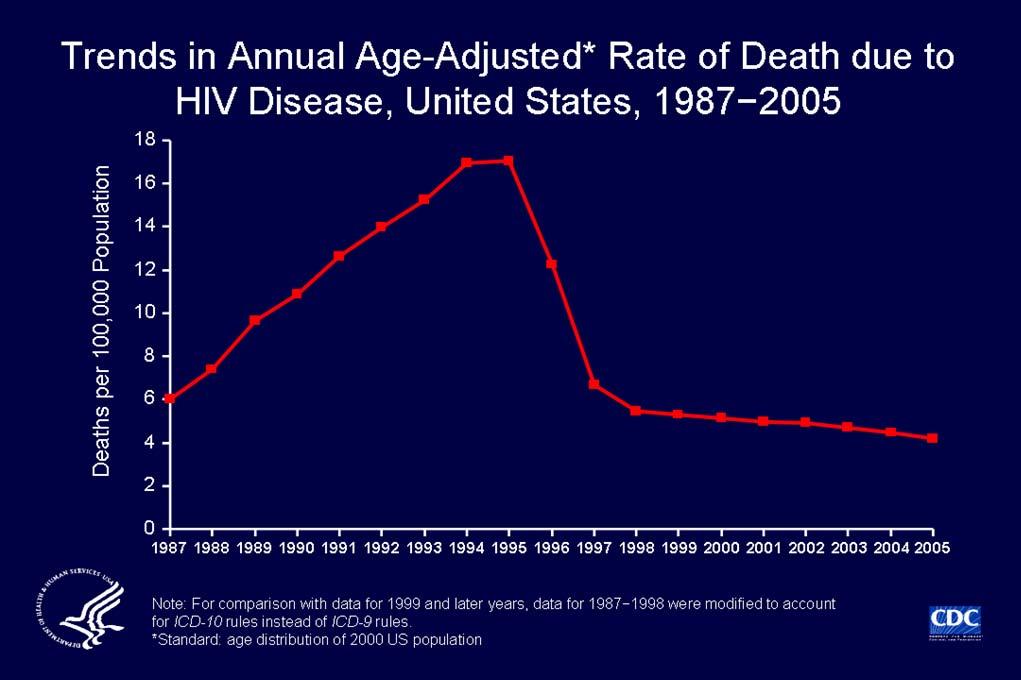
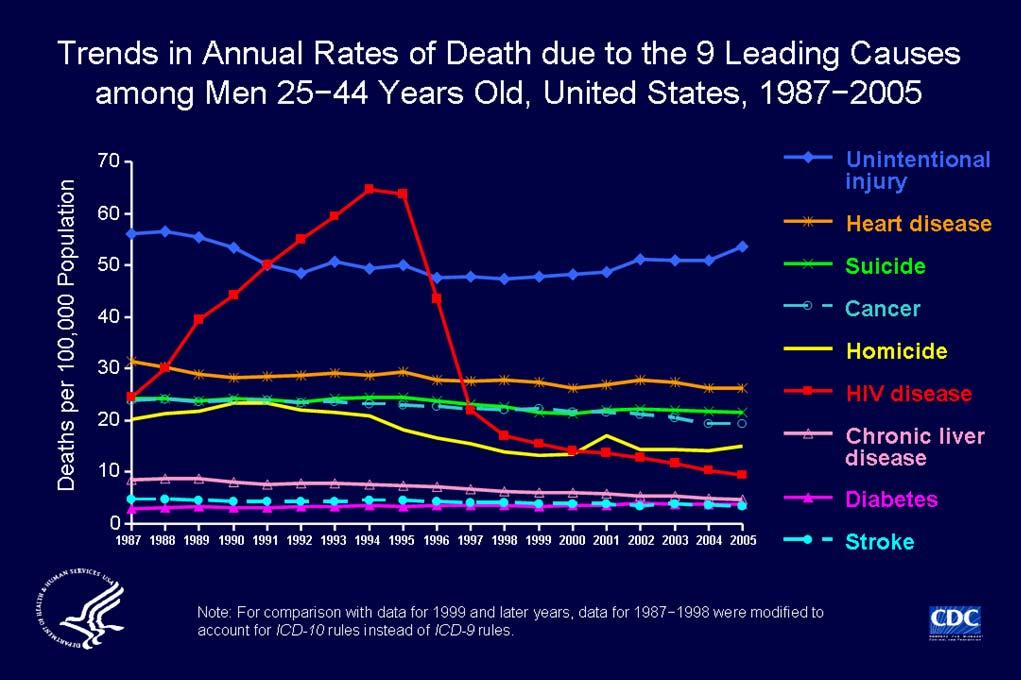
14 Antiretroviral Therapy in High Income Countries 1986 AZT Several NRTIS - DDI, DDC, 3TC, D4T, earlier Rx, use of dual NRTI regimens 1996 First generation Protease Inhibitors SQV, IND, RIT 1996 First generation NNRTIs Nev,, Del, Effav Rapid adoption of HAART with dramatic clinical impact 11/19/
15
16
17 Impact of HAART on Mortality Agence Nationale de Recherches sur le Sida Sida Using pts from 2 french cohorts, calculated SMRs overall and for time with CD4>500 -HIV- Infected Adults With a CD4 Cell Count Greater Than 500 Cells/mm3 on Long-Term Combination Antiretroviral Therapy Reach Same Mortality Rates as the General Population after 6 years of Rx JAIDS Sept 2007 vol ( 46(1 The average number of years remaining for an HIV+ person aged 20 yrs, on HAART is 49 yrs, about 2/3 that of the general population, lower for lower baseline CD4, IDU.- The Lancet 2008 Volume 372:293-99, 99, Antiretroviral Cohort Collaboration NA and Eu
18 Outline Review Status of Global HIV Epidemic Impact of Antiretroviral Therapy on HIV morbidity/mortality 2008 HIV Treatment Guidelines Important considerations in ART Goals of ART for HIV Infection Potential Benefits of earlier ART Emerging issues in HIV treatment
19 Antiretroviral Treatment for HIV Infection- Guidelines DHHS Guidelines for the use of Antiretroviral Agents in HIV Infected Adults and Adolescents January 2008, updated Nov 3, 2008 IAS-USA Panel Recommendation Antiretroviral Treatment of Adult HIV Infection August 2008 BHIVA 2005, updated 2006 WHO Guidelines 2008
20 Indications for Initiating ART: Clinical Category and/or CD4 Count History of AIDS-defining illness CD4 count of <350 cells/µl Pregnant women HIV-associated nephropathy Chronic Infection Hepatitis B coinfection, when HBV treatment is indicated* Recommendation Initiate ART * Treatment with fully suppressive drugs active against both HIV and HBV is recommended.
21 Indications for Initiating ART: Chronic Infection ( 2 ) Clinical Category and/or CD4 Count CD4 count of >350 cells/µl, asymptomatic, without conditions listed above Recommendation Optimal time to initiate ART is not well defined; consider individual patient characteristics and comorbidities
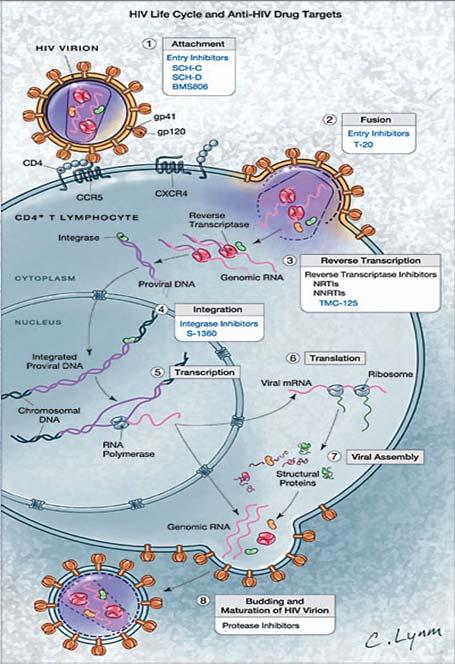
22 NRTI ( ABC ) Abacavir ( ddi ) Didanosine ( FTC ) Emtricitabine ( 3TC ) Lamivudine ( d4t ) Stavudine ( TDF ) Tenofovir Zidovudine (AZT, ZDV) NNRTI ( DLV ) Delavirdine ( EFV ) Efavirenz ( ETV ) Etravirine Nevirapine (NVP) Current ARV Medications PI ( ATV ) Atazanavir ( DRV ) Darunavir ( FPV ) Fosamprenavir Indinavir (IDV) ( LPV ) Lopinavir ( NFV ) Nelfinavir ( RTV ) Ritonavir ( SQV ) Saquinavir Tipranavir (TPV) Fusion Inhibitor ( T-20 Enfuvirtide (ENF, CCR5 Antagonist Maraviroc (MVC) Integrase Inhibitor ( RAL ) Raltegravir
23
24 Initial Treatment: Choosing Regimens 3 main categories: 1 NNRTI + 2 NRTIs 1 PI + 2 NRTIs 3 NRTIs Combination of NNRTI or PI + 2 NRTIs preferred Fusion inhibitor, CCR5 antagonist, integrase inhibitor not recommended in initial ART Few clinical end points to guide choices Advantages and disadvantages to each regimen Individualize treatment
25 Antiretroviral Therapy Considerations Results of drug resistance test Comorbidities (eg,, liver, psychiatric, or cardiovascular disease; ( tuberculosis Adherence potential Dosing convenience (eg( eg,, pill burden, dosing ( frequency Potential adverse effects Potential drug interactions Pregnancy potential Gender and CD4 count, if considering NVP HLA B*5701 testing, if considering ABC
26 Antiretroviral Therapy Considerations Patient readiness/commitment to therapy Adherence Adherence-95% adherence required to avoid development of resistant virus Lifelong therapy should not be interrupted unless serious toxicity or inability to take oral medications interruption ion usually results in immediate viral rebound, CD4 decline CD4 count, VL
27 ARV Components in Initial Therapy: NNRTIs ADVANTAGES Long half-lives lives Less metabolic toxicity (dyslipidemia( dyslipidemia, insulin resistance) than with some PIs PI options preserved for future use DISADVANTAGES Low genetic barrier to resistance single mutation Cross-resistance resistance among most NNRTIs Rash; hepatotoxicity Potential drug interactions ( CYP450 )
28 ARV Components in Initial Therapy: PIs ADVANTAGES Higher genetic barrier to resistance PI resistance uncommon with failure (boosted ( PI NNRTI options preserved for future use DISADVANTAGES Metabolic complications (fat maldistribution, dyslipidemia,, insulin ( resistance GI intolerance Potential for drug interactions (CYP450), especially with RTV
29 ARV Components in Initial Therapy: Dual-NRTI Pairs ADVANTAGES Established backbone of combination therapy Minimal drug interactions DISADVANTAGES Lactic acidosis and hepatic steatosis reported with most NRTIs ( rare ) Mitochondrial toxicity
30 Preferred Components of Initial ART: DHHS Categories Clinical data show optimal efficacy and durability Acceptable tolerability and ease of use Alternative Clinical trial data show efficacy but also show disadvantages in ARV activity, durability, tolerability, or ease of use (compared with preferred ( components May be the best option in select individual patients Other possible options Inferior efficacy or greater or more serious toxicities
31 Initial Treatment: Preferred Components NNRTI Option EFV* OR PI Options ATV + RTV ( BID ) FPV + RTV ( BID ) LPV/RTV + NRTI Options¹ ABC + 3TC² TDF + FTC³ * Avoid in pregnant women and women with significant pregnancy potential ¹ FTC can be used in place of 3TC and vice versa ² For patients who have tested negative for HLA-B*5701 ³ TDF + FTC or 3TC is preferred in patients with HIV/HBV coinfection
32 Initial Treatment: Alternative Components NNRTI Option NVP* PI Options ATV¹ FPV ( daily FPV + RTV (once LPV/RTV (once daily)² SQV + RTV * NVP should not be initiated in women with CD4 counts of >250 cells/µl L or men with CD4 counts of >400 cells/µl ¹ ATV must be boosted with RTV if used with TDF ² May be insufficient if HIV RNA >100,000 copies/ml
33 Initial Treatment: Alternative Components ( 2 ) NRTI Options (in order of ( preference ZDV + 3TC¹ ddi + (FTC or ( 3TC ¹ FTC can be used in place of 3TC and vice versa
34 ARV Medications: Should Not Be Offered at Any Time ARV regimens not recommended Inferior virologic efficacy, rapid development of resistance: Monotherapy with NRTI* Dual-NRTI therapy 3-NRTI regimen (except ABC/3TC/ADV or possibly TDF + 3TC + ZDV, when other regimens are not ( desirable * For pregnant women, see Public Health Service Task Force Recommendations for the Use of Antiretroviral Drugs in Pregnant HIV-Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV Transmission in the United States
35 ARV Medications: Should Not Be Offered at Any Time ( 2 ) Higher incidence of adverse events Potential teratogenicity: avoid during pregnancy (especially 1st trimester) and in women with significant potential for pregnancy* No potential benefit; similar resistance profile ddi + d4t ATV + IDV 2-NNRTI combinations EFV 3TC + FTC * Women who are trying to conceive or who are not using effective and consistent contraception.
36 ARV Medications: Should Not Be Offered at Any Time ( 3 ) Antagonistic effects d4t + ZDV Poor bioavailability SQV ( unboosted )
37 Antiretroviral Therapy Goals of Therapy Reduction HIV morbidity and mortality Improved quality of life Restoration/preservation of immune function Maximal + durable suppression viral load Possible Prevention of transmission -vertical transmission and to sex partners
38 Outline Review Status of Global HIV Epidemic Impact of Antiretroviral Therapy on HIV morbidity/mortality 2008 HIV Treatment Guidelines Important considerations in ART Goals of ART for HIV Infection Emerging issues in HIV treatment Potential Benefits of earlier ART
39 Emerging Issues in HIV Treatment Antiretroviral treatment in pts with CD4> 350 Excess non opportunistic disease and malignancies in HIV+ Cardiac Risk and Abacavir
40 Potential Benefits of Early Antiretroviral Therapy ( CD4>350 ) Maintain higher CD4 count -prevent irreversible immune damage Decrease risk of HIV associated complications (TB, TB, KS, NHL, peripheral neuropathy, HIV associated malignancies and cognitive ( impairment Decrease risk non opportunistic conditions and non AIDS associated conditions (CV,( CV, renal and liver disease, infections, ( malignancies Decrease transmission
41 Potential Risks of Early ARV Therapy ( CD4>350 ) Inadequate time to learn about HIV, treatment and adherence Increase total time on ARVs,, increase risk of treatment fatigue, drug resistance with failure ARV related side effects and toxicities Current therapy may be less effective/more toxic than future options
42 Benefits of Early ART (CD4>350) Maintain higher CD4 count -prevent irreversible immune damage- ATHENA (AIDS Therapy Evaluation Project Netherlands) Pts starting with CD4 > 350 significantly more likely to achieve CD4 > 800 John Hopkins CC Pts starting ART CD4 < 350 significantly less likely to achieve CD4 >500
43 Benefits of Early ART (CD4>350) Decrease risk of HIV associated complications Decrease risk non opportunistic conditions and non AIDS associated conditions NA Accord- (22 research cohorts, part of the 'Intl Epid Databases to Evaluate AIDS Project', 8,374 pts, 24,994 person yrs follow up, data prospectively collected) Showed a 70% Survival benefit for pts initiating HAART CD vs CD4 < 350 (RH 1.7, ) Benefit seen across all subsets. Age, IDU, HCV associated with increased mortality SMART Substudy Found a 5.7% difference in absolute risk of opportunistic disease and serious non-aids events with immediate versus deferred antiretroviral therapy (CD4 >350)
44 Benefits of Early Treatment Decrease transmission- Abstract presented at Intl AIDS Conference 2008 Montaner Prospective cohort of HIV+ and HIV Prospective cohort of HIV+ and HIV- IVDU semi-annual plasma HIV level correlated with HIV incidence rates adjusted for risk behaviours, community HIV RNA level associated with time to seroconversion- Conclusion Treating an HIV infected community may decrease transmission Serodiscordant couples- When VL<1000 c/ml on HAART very low risk of transmission
45 Potential Risks of Early ARV Therapy ( CD4>350 ) ARV related side effects and toxicities HOPS Cohort (Prospective,( dynamic cohort (>8000 ( patients : Early Initiation of HAART Decreases Risk of Toxicities
46 Currently lack clinical trial evidence for earlier initiation of ART, so recommendation remains for CD4> 350 consider on an individual basis Evidence is mounting in favour of earlier initiation of antiretroviral therapy. START Trial - enrolling
47 Emerging Issues in HIV Treatment Antiretroviral treatment in pts with CD4> 350 Excess non opportunistic disease and malignancies in HIV+ Cardiac Risk and Abacavir
48 Comparison of Mortality, National Survey of causes of death in HIV+ pts in France 78,000 pts followed at least 1 year Compared deaths in 2000 (n=964) vs ( n=937 ) In 2005, increased deaths due to malignancies (38% respiratory tract), HCV, cardiovascular While AIDS-related deaths are decline, deaths due to CA, HCV, CV disease are increasing Causes of death 2000 (n=964) and 2005 ( n=937 ) AIDS Cancer HCV Cardiovascular Suicide Non-AIDS Infection Lewden C, et al. 14th CROI, Los Angeles, CA, February 25-28, Abst. 976.
49 Emerging Concerns Non AIDS Malignancies Intl AIDS Conf Mexico % increase risk of non AIDS malig.. in HIV+ pts anal/lung/melanoma/liver Pre HAART < 10% deaths were from cancer, HAART 28% deaths cancer, ADM and non ADM, 4-14 fold inc incidence lung ca HIV+ -not associated with CD4, 10:1 M:F, smoking, usually advanced MST 3-83 mos D:A:D Cohort USA- Risk ADM nonadm increased with decreasing CD4<500, older age, smoking, HBV
50 The most reasonable explanation for the year gap in life expectancy so well documented by the ART-CC study is the previously unrealised clinical mischief of untreated HIV infection Lancet, Volume 372 Cooper
51 Emerging Issues in HIV Treatment Antiretroviral treatment in pts with CD4> 350 Excess non opportunistic disease and malignancies in HIV+ Cardiac Risk and Abacavir
52 Abacavir and Cardiac Risk SMART CD4>350 CD4>350 continuous(virol suppression) vs intermittent (drug conservation) CVD Events in VS group (major clinical MI, silent MI, CVA, CAD Sx,, CVD death) In pts with >5 CRF, or ischaemic changes on EKG HR 3.1 ABC vs other NRTI Similar results NOT seen in GSK trials, HEAT Results significant enough that DHHS have Updated Guidelines Use with caution in pts with increased CRF, or ischaemic disease
53 Websites to Access the Guidelines
54 Case 1 Mr and Mrs S- have been together several years. Mr. S recently diagnosed with HIV, current VL 45,000 c/ml, CD4 362, asymptomatic. Mrs S not infected. Refugees from Africa. Wanting to start a family. You are seeing Mr S in your office regarding management of his HIV. What are his options, what do you recommend?
55 Case 2 20 yo male from Ethiopia, newly diagnosed HIV+, baseline CD4 280, VL 5,000 Recent diagnosis of disseminated TB. Symptomatic with wieght loss, diarrhea What ART regimen would you recommend, and why? (What are the significant concerns with the different options NNRTI vs PI based)
56 Case 3 You are meeting Ms. K for the first time. 36 yo F, advanced HIV, CD4 56, on methadone maintenance therapy. Several prior attempts at ART have been unsuccessful. She is wanting to try again. Medical hx significant for G3P2A1, HBV+ What information do you need to choose ART? What medications should you avoid? What medications should be included? What might increase her liklihood of success?
Comprehensive Guideline Summary
 Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines
 The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
HIV Treatment Update. Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University
 HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
HIV Treatment Update Awewura Kwara, MD, MPH&TM Associate Professor of Medicine and Infectious Diseases Brown University Outline Rationale for highly active antiretroviral therapy (HAART) When to start
Continuing Education for Pharmacy Technicians
 Continuing Education for Pharmacy Technicians HIV/AIDS TREATMENT Michael Denaburg, Pharm.D. Birmingham, AL Objectives: 1. Identify drugs and drug classes currently used in the management of HIV infected
Continuing Education for Pharmacy Technicians HIV/AIDS TREATMENT Michael Denaburg, Pharm.D. Birmingham, AL Objectives: 1. Identify drugs and drug classes currently used in the management of HIV infected
Pharmacological considerations on the use of ARVs in pregnancy
 Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
ART and Prevention: What do we know?
 ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
ART and Prevention: What do we know? Biomedical Issues Trip Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Cornell Medical College New York City ART for Prevention:
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV. Ernesto Parra, M.D., M.P.H.
 Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
Pediatric HIV Infection and the Medical Management of Pregnant Women infected with HIV Ernesto Parra, M.D., M.P.H. Adjunct Associate Professor UTHSCSA Department of Pediatrics and Family and Community
Selected Issues in HIV Clinical Trials
 Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
When to Start ART. Reduction in HIV transmission. ? Reduction in HIV-associated inflammation and associated complications» i.e. CV disease, neuro, etc
 When to Start ART Exact CD4 count at which to initiate therapy not known, but evidence points to starting at higher counts Current recommendation: ART for all patients with CD4 count of
When to Start ART Exact CD4 count at which to initiate therapy not known, but evidence points to starting at higher counts Current recommendation: ART for all patients with CD4 count of
HIV in in Women Women
 HIV in Women Susan L. Koletar, MD The Ohio State University How Many of These Women Have HIV? Answer: I don t really know Google Search: Photos of Groups of Women Pub Med Search: HIV and Women 22,732
HIV in Women Susan L. Koletar, MD The Ohio State University How Many of These Women Have HIV? Answer: I don t really know Google Search: Photos of Groups of Women Pub Med Search: HIV and Women 22,732
I. HIV Epidemiology. HIV Infection A Primer. Objectives. Disclosures 7/18/2014
 Objectives HIV Infection A Primer Discuss the worldwide and domestic epidemiology of HIV infection Review HIV Biology Review HIV Transmission and Prevention Review HIV diagnosis Describe the approaches
Objectives HIV Infection A Primer Discuss the worldwide and domestic epidemiology of HIV infection Review HIV Biology Review HIV Transmission and Prevention Review HIV diagnosis Describe the approaches
HIV basics. Katya Calvo Medical Director of Antimicrobial Stewardship
 HIV basics Katya Calvo Medical Director of Antimicrobial Stewardship Learning Objectives 1. Review of HIV epidemiology worldwide and locally 2. Review of recommendations on whom to screen 3. Work up of
HIV basics Katya Calvo Medical Director of Antimicrobial Stewardship Learning Objectives 1. Review of HIV epidemiology worldwide and locally 2. Review of recommendations on whom to screen 3. Work up of
/AIDS HIV/ HIV Overview. Nelson L. Michael, MD, PhD Division of Retrovirology Walter Reed Army Institute of Research US Military HIV Research Program
 /AIDS HIV/ HIV Overview Nelson L. Michael, MD, PhD Division of Retrovirology Walter Reed Army Institute of Research US Military HIV Research Program www.hivresearch.org 1 WRAIR Tropical Medicine Course
/AIDS HIV/ HIV Overview Nelson L. Michael, MD, PhD Division of Retrovirology Walter Reed Army Institute of Research US Military HIV Research Program www.hivresearch.org 1 WRAIR Tropical Medicine Course
HIV Overview. Mary Marovich, MD, DTMH Division of Retrovirology Walter Reed Army Ins?tute of Research US Military HIV Research Program
 HIV Overview Mary Marovich, MD, DTMH Division of Retrovirology Walter Reed Army Ins?tute of Research US Military HIV Research Program www.hivresearch.org 1 Outline HIV Virology, Transmission, and Pathogenesis
HIV Overview Mary Marovich, MD, DTMH Division of Retrovirology Walter Reed Army Ins?tute of Research US Military HIV Research Program www.hivresearch.org 1 Outline HIV Virology, Transmission, and Pathogenesis
Criteria for Oral PrEP
 Oral PrEP New Drugs Roy M. Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Medical College of Cornell University New York City Safe Criteria for Oral PrEP Penetrates
Oral PrEP New Drugs Roy M. Gulick, MD, MPH Chief, Division of Infectious Diseases Professor of Medicine Weill Medical College of Cornell University New York City Safe Criteria for Oral PrEP Penetrates
Selected Issues in HIV Clinical Trials
 Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Selected Issues in HIV Clinical Trials Judith S. Currier, M.D., MSc Professor of Medicine Division of Infectious Diseases University of California, Los Angeles Issues Evolving Global and Domestic Epidemic
Selecting an Initial Antiretroviral Therapy (ART) Regimen
 Regimen") Selecting an Initial Antiretroviral Therapy (ART) Regimen An HIV Diagnosis is a Call to Action In support of the NYSDOH AIDS Institute s January 2018 call to action for patients newly diagnosed with HIV,
Selecting an Initial Antiretroviral Therapy (ART) Regimen An HIV Diagnosis is a Call to Action In support of the NYSDOH AIDS Institute s January 2018 call to action for patients newly diagnosed with HIV,
Susan L. Koletar, MD
 HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
Structured Treatment Interruption in HIV Positive Patients. Leah Jackson, BScPhm Pharmacy Resident HIV Rotation January 23, 2007
 Structured Treatment Interruption in HIV Positive Patients Leah Jackson, BScPhm Pharmacy Resident HIV Rotation January 23, 2007 Objectives To become re-acquainted with the basics of HAART for HIV infection
Structured Treatment Interruption in HIV Positive Patients Leah Jackson, BScPhm Pharmacy Resident HIV Rotation January 23, 2007 Objectives To become re-acquainted with the basics of HAART for HIV infection
This graph displays the natural history of the HIV disease. During acute infection there is high levels of HIV RNA in plasma, and CD4 s counts
 1 2 This graph displays the natural history of the HIV disease. During acute infection there is high levels of HIV RNA in plasma, and CD4 s counts decreased. This period of acute infection or serocnversion
1 2 This graph displays the natural history of the HIV disease. During acute infection there is high levels of HIV RNA in plasma, and CD4 s counts decreased. This period of acute infection or serocnversion
TB Intensive Tyler, Texas December 2-4, Tuberculosis and HIV Co-Infection. Lisa Y. Armitige, MD, PhD. December 4, 2008.
 TB Intensive Tyler, Texas December 2-4, 2008 Tuberculosis and HIV Co-Infection Lisa Y. Armitige, MD, Ph.D. December 4, 2008 Tuberculosis and HIV Co Infection Lisa Y. Armitige, MD, PhD Assistant Professor
TB Intensive Tyler, Texas December 2-4, 2008 Tuberculosis and HIV Co-Infection Lisa Y. Armitige, MD, Ph.D. December 4, 2008 Tuberculosis and HIV Co Infection Lisa Y. Armitige, MD, PhD Assistant Professor
When to start, when to switch ART and monitoring of ARV side effects
 When to start, when to switch ART and monitoring of ARV side effects Thanomsak Anekthananon, MD Faculty of Medicine Siriraj Hospital September 4, 2009 Recommended Websites Free e-book: HIV Medicine 2007
When to start, when to switch ART and monitoring of ARV side effects Thanomsak Anekthananon, MD Faculty of Medicine Siriraj Hospital September 4, 2009 Recommended Websites Free e-book: HIV Medicine 2007
Sasisopin Kiertiburanakul, MD, MHS
 What s Newin Antiretroviral Therapy? Sasisopin Kiertiburanakul, MD, MHS Division of Infectious Diseases Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University Rotating RCPT,
What s Newin Antiretroviral Therapy? Sasisopin Kiertiburanakul, MD, MHS Division of Infectious Diseases Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University Rotating RCPT,
TB/HIV Co-Infection. Tuberculosis and HIV
 TB Intensive Tyler, Texas June 2-4, 2010 TB/HIV Co-Infection Lisa Y Armitige, MD, PhD June 3, 2010 Tuberculosis and HIV Co-Infection Lisa Y Armitige, MD, PhD Medical Consultant Heartland National TB Center
TB Intensive Tyler, Texas June 2-4, 2010 TB/HIV Co-Infection Lisa Y Armitige, MD, PhD June 3, 2010 Tuberculosis and HIV Co-Infection Lisa Y Armitige, MD, PhD Medical Consultant Heartland National TB Center
Susan L. Koletar, MD
 HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
Principles of Antiretroviral Therapy
 Principles of Antiretroviral Therapy Ten Principles of Antiretroviral Therapy Skills Building Workshop: Clinical Management of HIV Infection and Antiretroviral Therapy, 11 th ICAAP, November 21st, 2011,
Principles of Antiretroviral Therapy Ten Principles of Antiretroviral Therapy Skills Building Workshop: Clinical Management of HIV Infection and Antiretroviral Therapy, 11 th ICAAP, November 21st, 2011,
The Global HIV Epidemic. Jerome Larkin, MD
 The Global HIV Epidemic Jerome Larkin, MD Outline Global Epidemiology Natural History of HIV Antiretroviral Therapy Malaria Tuberculosis Prevention of Mother to Child Transmission Post-Exposure Prophylaxis
The Global HIV Epidemic Jerome Larkin, MD Outline Global Epidemiology Natural History of HIV Antiretroviral Therapy Malaria Tuberculosis Prevention of Mother to Child Transmission Post-Exposure Prophylaxis
Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update
 Frontier AIDS Education and Training Center Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director,
Frontier AIDS Education and Training Center Antiretroviral Therapy During Pregnancy and Delivery: 2015 Update Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director,
POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV
 POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none
POST-EXPOSURE PROPHYLAXIS, PRE-EXPOSURE PROPHYLAXIS, & TREATMENT OF HIV DISCLOSURE Relevant relationships with commercial entities none Potential for conflicts of interest within this presentation none
Treatment strategies for the developing world
 David A Cooper National Centre in HIV Epidemiology and Clinical Research The University of New South Wales Sydney, Australia First line standard of care First line in the developing world First line failure
David A Cooper National Centre in HIV Epidemiology and Clinical Research The University of New South Wales Sydney, Australia First line standard of care First line in the developing world First line failure
Overview of HIV. LTC Paige Waterman
 Overview of HIV LTC Paige Waterman Outline Background and Epidemiology HIV Virology, Transmission, and Pathogenesis Acute HIV infection HIV Diagnostics Management of Health Care Personnel Exposed to HIV
Overview of HIV LTC Paige Waterman Outline Background and Epidemiology HIV Virology, Transmission, and Pathogenesis Acute HIV infection HIV Diagnostics Management of Health Care Personnel Exposed to HIV
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents
 Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Overview of HIV WRAIR- GEIS 'Operational Clinical Infectious Disease' Course
 Overview of HIV WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments - Dr. Christina Polyak - Dr. Julie Ake Disclaimer The views expressed in this presentation are
Overview of HIV WRAIR- GEIS 'Operational Clinical Infectious Disease' Course UNCLASSIFIED Acknowledgments - Dr. Christina Polyak - Dr. Julie Ake Disclaimer The views expressed in this presentation are
Gaps between Policy and Practice in Managing HIV disease in Asia Pacific
 Gaps between Policy and Practice in Managing HIV disease in Asia Pacific Dr. N. Kumarasamy Chief Medical Officer YRGCARE Medical Centre Voluntary Health Services Chief-Chennai Antiviral Research and Treatment
Gaps between Policy and Practice in Managing HIV disease in Asia Pacific Dr. N. Kumarasamy Chief Medical Officer YRGCARE Medical Centre Voluntary Health Services Chief-Chennai Antiviral Research and Treatment
Simplifying HIV Treatment Now and in the Future
 Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
Simplifying HIV Treatment Now and in the Future David M. Hachey, Pharm.D., AAHIVP Professor Idaho State University Department of Family Medicine Nothing Disclosure 1 Objectives List current first line
Management of patients with antiretroviral treatment failure: guidelines comparison
 The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
The editorial staff Management of patients with antiretroviral treatment failure: guidelines comparison A change of therapy should be considered for patients if they experience sustained rebound in viral
Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care
 Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care www.nwaetc.org The Northwest AIDS Education and Training Center (NW AETC), located at the University
Northwest AIDS Education and Training Center Educating health care professionals to provide quality HIV care www.nwaetc.org The Northwest AIDS Education and Training Center (NW AETC), located at the University
0% 0% 0% Parasite. 2. RNA-virus. RNA-virus
 HIV/AIDS and Treatment Manado, Indonesia 16 november HIV [e] EDUCATION HIV is a 1. DNA-virus 2. RNA-virus 3. Parasite 0% 0% 0% DNA-virus RNA-virus Parasite HIV HIV is a RNA-virus. HIV is an RNA virus which
HIV/AIDS and Treatment Manado, Indonesia 16 november HIV [e] EDUCATION HIV is a 1. DNA-virus 2. RNA-virus 3. Parasite 0% 0% 0% DNA-virus RNA-virus Parasite HIV HIV is a RNA-virus. HIV is an RNA virus which
Pediatric Antiretroviral Resistance Challenges
 Pediatric Antiretroviral Resistance Challenges Thanyawee Puthanakit, MD The HIVNAT, Thai Red Cross AIDS research Center The Research Institute for Health Science, Chiang Mai University Outline The burden
Pediatric Antiretroviral Resistance Challenges Thanyawee Puthanakit, MD The HIVNAT, Thai Red Cross AIDS research Center The Research Institute for Health Science, Chiang Mai University Outline The burden
Improving accessibility to antiretroviral drugs: A south-south collaboration
 Improving accessibility to antiretroviral drugs: A south-south collaboration Jaideep A Gogtay MD Cipla Ltd Mumbai jgogtay@cipla.com Adults and children estimated to be living with HIV at the end of 2000
Improving accessibility to antiretroviral drugs: A south-south collaboration Jaideep A Gogtay MD Cipla Ltd Mumbai jgogtay@cipla.com Adults and children estimated to be living with HIV at the end of 2000
Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches
 Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches Harry W. Lampiris, MD Chief, Infectious Disease Section, San Francisco VA Medical Center Professor
Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches Harry W. Lampiris, MD Chief, Infectious Disease Section, San Francisco VA Medical Center Professor
What's new in the WHO ART guidelines How did markets react?
 WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
WHO 2013 ARV Guidelines What's new in the WHO ART guidelines How did markets react? Dr. J. Perriëns Coordinator, HIV Technology and Commodities HIV department, WHO, Geneva When to start in adults Starting
Rajesh T. Gandhi, M.D.
 HIV Treatment Guidelines: 2010 Rajesh T. Gandhi, M.D. Case 29 yo M with 8 weeks of cough and fever. Diagnosed with smear-positive pulmonary TB. HIV-1 antibody positive. CD4 count 361. HIV-1 RNA 23,000
HIV Treatment Guidelines: 2010 Rajesh T. Gandhi, M.D. Case 29 yo M with 8 weeks of cough and fever. Diagnosed with smear-positive pulmonary TB. HIV-1 antibody positive. CD4 count 361. HIV-1 RNA 23,000
0.14 ( 0.053%) UNAIDS 10% (94) ( ) (73-94/6 ) 8,920
 UNAIDS 10% (94) ( ) (73-94/6 ) 8,920") 0.14 UNAIDS 0.053% 2 250 60 10% 94 73 20 73-94/6 8,920 12 43 Public Health Service Task Force Recommendations 5-10% for Use of Antiretroviral Drugs in 10-20% Pregnant HIV-1-Infected Women for Maternal
0.14 UNAIDS 0.053% 2 250 60 10% 94 73 20 73-94/6 8,920 12 43 Public Health Service Task Force Recommendations 5-10% for Use of Antiretroviral Drugs in 10-20% Pregnant HIV-1-Infected Women for Maternal
Somnuek Sungkanuparph, M.D.
 HIV Drug Resistance Somnuek Sungkanuparph, M.D. Associate Professor Division of Infectious Diseases Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University Adjunct Professor
HIV Drug Resistance Somnuek Sungkanuparph, M.D. Associate Professor Division of Infectious Diseases Department of Medicine Faculty of Medicine Ramathibodi Hospital Mahidol University Adjunct Professor
HIV - Therapy Principles
 HIV - Therapy Principles Manuel Battegay and Christine Katlama Basel, Switzerland and Paris, France Disclosure MB has received honoraria for advisory board participation from Gilead, MSD, Pfizer, ViiV
HIV - Therapy Principles Manuel Battegay and Christine Katlama Basel, Switzerland and Paris, France Disclosure MB has received honoraria for advisory board participation from Gilead, MSD, Pfizer, ViiV
HIV Treatment: State of the Art 2013
 HIV Treatment: State of the Art 2013 Daniel R. Kuritzkes, MD Chief, Division of Infectious Diseases Brigham and Women s Hospital Professor of Medicine Harvard Medical School Success of current ART Substantial
HIV Treatment: State of the Art 2013 Daniel R. Kuritzkes, MD Chief, Division of Infectious Diseases Brigham and Women s Hospital Professor of Medicine Harvard Medical School Success of current ART Substantial
Antiretroviral Therapy
 Antiretroviral Therapy Scott M. Hammer, M.D. 1986 1990 ZDV monorx 1990 1995 Alternative NRTI monorx Combination NRTI Rx Introduction of NNRTI s Antiretroviral resistance Pathogenetic concepts Evolution
Antiretroviral Therapy Scott M. Hammer, M.D. 1986 1990 ZDV monorx 1990 1995 Alternative NRTI monorx Combination NRTI Rx Introduction of NNRTI s Antiretroviral resistance Pathogenetic concepts Evolution
Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications
 and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications") Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications Carrie Allen PharmD, CGP, BCPS, BCPP, CCHP Overview - Part 2: HIV
Human Immunodeficiency Virus (HIV) and Acquired Immune Deficiency Syndrome (AIDS) in the Long Term Care Setting Part 2: HIV Medications Carrie Allen PharmD, CGP, BCPS, BCPP, CCHP Overview - Part 2: HIV
ANTIRETROVIRAL TOXICITY Strategies for prevention and treatment
 ANTIRETROVIRAL TOXICITY Strategies for prevention and treatment Francisco Antunes Professor da Faculdade de Medicina da Universidade de Lisboa e Director do Serviço de Doenças Infecciosas do Hospital de
ANTIRETROVIRAL TOXICITY Strategies for prevention and treatment Francisco Antunes Professor da Faculdade de Medicina da Universidade de Lisboa e Director do Serviço de Doenças Infecciosas do Hospital de
HIV Treatment: New and Veteran Drugs Classes
 HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
ART for HIV Prevention:
 ART for HIV Prevention: KENNETH H. MAYER, M.D. Brown University/The Fenway Institute August 22, 2009 APPROACHES TO PREVENT HIV TRANSMISSION DECREASE SOURCE OF INFECTION Barrier Protection Treat STI Antiretroviral
ART for HIV Prevention: KENNETH H. MAYER, M.D. Brown University/The Fenway Institute August 22, 2009 APPROACHES TO PREVENT HIV TRANSMISSION DECREASE SOURCE OF INFECTION Barrier Protection Treat STI Antiretroviral
2 nd Line Treatment and Resistance. Dr Rohit Talwani & Dr Dave Riedel 12 th June 2012
 2 nd Line Treatment and Resistance Dr Rohit Talwani & Dr Dave Riedel 12 th June 2012 Overview Basics of Resistance Treatment failure Strategies to manage treatment failure Mutation Definition: A change
2 nd Line Treatment and Resistance Dr Rohit Talwani & Dr Dave Riedel 12 th June 2012 Overview Basics of Resistance Treatment failure Strategies to manage treatment failure Mutation Definition: A change
Friday afternoon Programme
 Friday afternoon Programme Pharmacology and TDM Dr Marta Boffito Consultant Physician, C&W Resistance to new anti-retrovirals Dr Steve Taylor Consultant Physician, Birmingham HIVPA Annual Conference 2008
Friday afternoon Programme Pharmacology and TDM Dr Marta Boffito Consultant Physician, C&W Resistance to new anti-retrovirals Dr Steve Taylor Consultant Physician, Birmingham HIVPA Annual Conference 2008
When to start: guidelines comparison
 The editorial staff When to start: guidelines comparison The optimal time to begin antiretroviral therapy remains a critical question for the HIV field, and consensus about the appropriate CD4+ cell count
The editorial staff When to start: guidelines comparison The optimal time to begin antiretroviral therapy remains a critical question for the HIV field, and consensus about the appropriate CD4+ cell count
A Fatal Imbalance. Tropical diseases: 18 new drugs (incl. 8 for malaria) 1.3% 21 new drugs for neglected diseases. Tuberculosis: 3 new drugs
 1.3% 21 new drugs for neglected diseases. Tuberculosis: 3 new drugs") ADDRESSING GAPS IN INNOVATION FOR NEGLECTED PATIENTS: DNDI ANDPEDIATRIC HIV/AIDS Rachel Cohen, Regional Executive Director, DNDi North America Proposals for a Global Innovation System that Responds to
ADDRESSING GAPS IN INNOVATION FOR NEGLECTED PATIENTS: DNDI ANDPEDIATRIC HIV/AIDS Rachel Cohen, Regional Executive Director, DNDi North America Proposals for a Global Innovation System that Responds to
13 th Conference on Retroviruses and Opportunistic Infections (CROI)
") REPORT FROM 13 th Conference on Retroviruses and Opportunistic Infections (CROI) February 5 8, 5 2006 Denver, CO 1 Tipranavir Significantly Reduces Concentrations of Other ARVs -10 % change PK -30-50 -70-68
REPORT FROM 13 th Conference on Retroviruses and Opportunistic Infections (CROI) February 5 8, 5 2006 Denver, CO 1 Tipranavir Significantly Reduces Concentrations of Other ARVs -10 % change PK -30-50 -70-68
Cases from the Clinic(ians): Case-Based Panel Discussion
: Case-Based Panel Discussion") Cases from the Clinic(ians): Case-Based Panel Discussion Michael S. Saag, MD Professor of Medicine The University of Alabama at Birmingham EDITED: 03-12-14 Learning Objectives After attending this presentation,
Cases from the Clinic(ians): Case-Based Panel Discussion Michael S. Saag, MD Professor of Medicine The University of Alabama at Birmingham EDITED: 03-12-14 Learning Objectives After attending this presentation,
Pharmacology Update Alice Tseng, Pharm.D., FCSHP Vancouver May 11, 2005
 Pharmacology Update 2005 Alice Tseng, Pharm.D., FCSHP Vancouver May 11, 2005 I m having a Maalox moment!!! Gastric Hypoacidity in HIV 20% incidence in HIV (unrelated to CD 4 ) Antacids, ddi tablets, H2-blockers
Pharmacology Update 2005 Alice Tseng, Pharm.D., FCSHP Vancouver May 11, 2005 I m having a Maalox moment!!! Gastric Hypoacidity in HIV 20% incidence in HIV (unrelated to CD 4 ) Antacids, ddi tablets, H2-blockers
Overview of HIV. Christina Polyak, MD, MPH. Research Physician. U.S. Military HIV Research Program, Walter Reed Army Institute of Research
 Overview of HIV Christina Polyak, MD, MPH Research Physician U.S. Military HIV Research Program, Walter Reed Army Institute of Research The views expressed are those of the authors and should not be construed
Overview of HIV Christina Polyak, MD, MPH Research Physician U.S. Military HIV Research Program, Walter Reed Army Institute of Research The views expressed are those of the authors and should not be construed
Didactic Series. Update: 2012 HIV Treatment Guidelines. Daniel Lee, MD August 30, 2012
 Didactic Series Update: 2012 HIV Treatment Guidelines Daniel Lee, MD August 30, 2012 ACCREDITATION STATEMENT: University of California, San Diego School of Medicine is accredited by the Accreditation Council
Didactic Series Update: 2012 HIV Treatment Guidelines Daniel Lee, MD August 30, 2012 ACCREDITATION STATEMENT: University of California, San Diego School of Medicine is accredited by the Accreditation Council
HIV Pharmacology 101ish - 202ish: New HIV Clinicians Workshop
 HIV Pharmacology 101ish - 202ish: New HIV Clinicians Workshop Parya Saberi, PharmD, MAS The Medical Management of HIV/AIDS December 2012 Objectives What are commonly used ARVs and where do they work in
HIV Pharmacology 101ish - 202ish: New HIV Clinicians Workshop Parya Saberi, PharmD, MAS The Medical Management of HIV/AIDS December 2012 Objectives What are commonly used ARVs and where do they work in
The ART of Managing Drug-Drug Interactions in Patients with HIV
 The ART of Managing Drug-Drug Interactions in Patients with HIV Bradley L. Smith, Pharm.D. smith.bradley1@mayo.edu Pharmacy Grand Rounds December 19, 2017 2017 MFMER slide-1 Presentation Objectives Describe
The ART of Managing Drug-Drug Interactions in Patients with HIV Bradley L. Smith, Pharm.D. smith.bradley1@mayo.edu Pharmacy Grand Rounds December 19, 2017 2017 MFMER slide-1 Presentation Objectives Describe
Medscape's Antiretroviral Pocket Guide for the Treatment of HIV Infection
 Table 3. Characteristics of Nucleoside Reverse Transcriptase Inhibitors (NRTIs) Generic Name (Abbreviation) / Trade Name Abacavir (ABC) / Ziagen Trizivir with ZDV + 3TC Epzicom with 3TC Didanosine (ddi)
Table 3. Characteristics of Nucleoside Reverse Transcriptase Inhibitors (NRTIs) Generic Name (Abbreviation) / Trade Name Abacavir (ABC) / Ziagen Trizivir with ZDV + 3TC Epzicom with 3TC Didanosine (ddi)
HIV in the Brain MANAGING COMORBIDITIES IN PATIENTS WITH HIV
 HIV in the Brain MANAGING COMORBIDITIES IN PATIENTS WITH HIV Shibani S. Mukerji MD, PhD Massachusetts General Hospital, Division of Immunologic, Inflammatory and Infectious Neurological Diseases Dana-Farber
HIV in the Brain MANAGING COMORBIDITIES IN PATIENTS WITH HIV Shibani S. Mukerji MD, PhD Massachusetts General Hospital, Division of Immunologic, Inflammatory and Infectious Neurological Diseases Dana-Farber
HIV/AIDS HIV/AIDS: Outline. Morbidity and Mortality Weekly Report (MMWR)
") HIV/AIDS: Outline HIV/AIDS 2013 Roy M. Gulick, MD, MPH Professor of Medicine Chief, Division of Infectious Diseases Weill Medical College of Cornell University New York City January 31, 2013 Epidemiology
HIV/AIDS: Outline HIV/AIDS 2013 Roy M. Gulick, MD, MPH Professor of Medicine Chief, Division of Infectious Diseases Weill Medical College of Cornell University New York City January 31, 2013 Epidemiology
Second and third line paediatric ART strategies
 Second and third line paediatric ART strategies Dr. Marape Marape Assistant Professor Ohio University School of Health Professions Gaborone, Botswana Marape Marape MB, BCh, BAO, MPH, PhD Assistant Professor
Second and third line paediatric ART strategies Dr. Marape Marape Assistant Professor Ohio University School of Health Professions Gaborone, Botswana Marape Marape MB, BCh, BAO, MPH, PhD Assistant Professor
Case # 1. Case #1 (cont d)
") Antiretroviral Therapy Management: Expert Panel Discussion George Beatty Susa Coffey Steve O Brien December 3, 2011 Moderated by Annie Luetkemeyer Case # 1 38 y.o. man, CD4 =350, VL=340K, new to your clinic
Antiretroviral Therapy Management: Expert Panel Discussion George Beatty Susa Coffey Steve O Brien December 3, 2011 Moderated by Annie Luetkemeyer Case # 1 38 y.o. man, CD4 =350, VL=340K, new to your clinic
Second-Line Therapy NORTHWEST AIDS EDUCATION AND TRAINING CENTER
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Second-Line Therapy David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious Diseases University of Washington Presentation
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Second-Line Therapy David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious Diseases University of Washington Presentation
Nobel /03/28. HIV virus and infected CD4+ T cells
 Mechanism of HIV drug resistance. Rodrigo Brindeiro / Amilcar Tanuri Laboratório de Virologia Molecular UFRJ 2 -Asso ciate Research Scientist, Internatio nal Center fo r Aids Care and Treatment Programs-ICAP,
Mechanism of HIV drug resistance. Rodrigo Brindeiro / Amilcar Tanuri Laboratório de Virologia Molecular UFRJ 2 -Asso ciate Research Scientist, Internatio nal Center fo r Aids Care and Treatment Programs-ICAP,
Advances in HIV Treatment: When to Start Treatment Which Antivirals to Use
 Advances in HIV Treatment: When to Start Treatment Which Antivirals to Use Calvin Cohen MD Harvard Vanguard Medical Associates CRI New England Vice Chair, Science Steering Cmte, INSIGHT Boston MA Learning
Advances in HIV Treatment: When to Start Treatment Which Antivirals to Use Calvin Cohen MD Harvard Vanguard Medical Associates CRI New England Vice Chair, Science Steering Cmte, INSIGHT Boston MA Learning
Antiretroviral Treatment (ART) of Adult HIV Infection*
 of Adult HIV Infection*") Antiretroviral Treatment (ART) of Adult HIV Infection* Prepared by J Montaner for the BC- CfE Therapeutic Guidelines Committee of the British Columbia - Centre for Excellence in HIV/AIDS. *Based on M Thompson,
Antiretroviral Treatment (ART) of Adult HIV Infection* Prepared by J Montaner for the BC- CfE Therapeutic Guidelines Committee of the British Columbia - Centre for Excellence in HIV/AIDS. *Based on M Thompson,
2009 Recommendations for Antiretroviral Therapy in Adults and Adolescents. When to Start and What ART to Use in 1 st and 2 nd Line December 2009
 2009 Recommendations for Antiretroviral Therapy in Adults and Adolescents When to Start and What ART to Use in 1 st and 2 nd Line December 2009 Historic Evolution of CD4 Criteria for ART Initiation in
2009 Recommendations for Antiretroviral Therapy in Adults and Adolescents When to Start and What ART to Use in 1 st and 2 nd Line December 2009 Historic Evolution of CD4 Criteria for ART Initiation in
PHCP 403 by L. K. Sarki
 PHCP 403 by L. K. Sarki objectives To gain insight into the epidemiology of HIV To gain basic understanding of the etiology of HIV disease To know the clinical manifestations of the disease To gain a basic
PHCP 403 by L. K. Sarki objectives To gain insight into the epidemiology of HIV To gain basic understanding of the etiology of HIV disease To know the clinical manifestations of the disease To gain a basic
MEDICAL COVERAGE GUIDELINES ORIGINAL EFFECTIVE DATE: 03/07/18 SECTION: DRUGS LAST REVIEW DATE: 02/19/19 LAST CRITERIA REVISION DATE: ARCHIVE DATE:
 FUZEON (enfuvirtide) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
FUZEON (enfuvirtide) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
Pediatric HIV Update NORTHWEST AIDS EDUCATION AND TRAINING CENTER
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Pediatric HIV Update Christian B. Ramers, MD, MPH Assistant Medical Director, Family Health Centers of San Diego HIV/HCV Distance Education Specialist - NWAETC,
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Pediatric HIV Update Christian B. Ramers, MD, MPH Assistant Medical Director, Family Health Centers of San Diego HIV/HCV Distance Education Specialist - NWAETC,
First-Line Antiretroviral Therapy for Treatment and Prevention:
 First-Line Antiretroviral Therapy for Treatment and Prevention: The Past, Present and Future Best Options Joel Gallant, MD, MPH Johns Hopkins University School of Medicine IAS-USA Guidelines 7/2008: When
First-Line Antiretroviral Therapy for Treatment and Prevention: The Past, Present and Future Best Options Joel Gallant, MD, MPH Johns Hopkins University School of Medicine IAS-USA Guidelines 7/2008: When
Optimizing 2 nd and 3 rd Line Antiretroviral Therapy in Children and Adolescents
 Optimizing 2 nd and 3 rd Line Antiretroviral Therapy in Children and Adolescents Victor Musiime, MBChB, MMED, PhD Senior Lecturer, Makerere University Investigator, Joint Clinical Research Centre (JCRC)
Optimizing 2 nd and 3 rd Line Antiretroviral Therapy in Children and Adolescents Victor Musiime, MBChB, MMED, PhD Senior Lecturer, Makerere University Investigator, Joint Clinical Research Centre (JCRC)
HIV Update. Divya Ahuja, MD Associate Professor of Medicine University of South Carolina School of Medicine
 HIV Update Divya Ahuja, MD Associate Professor of Medicine University of South Carolina School of Medicine Rates of Diagnoses of HIV Infection among Adults and Adolescents, 2012 United States and 6 Dependent
HIV Update Divya Ahuja, MD Associate Professor of Medicine University of South Carolina School of Medicine Rates of Diagnoses of HIV Infection among Adults and Adolescents, 2012 United States and 6 Dependent
Management of Treatment-Experienced Patients: New Agents and Rescue Strategies. Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine
 Management of Treatment-Experienced Patients: New Agents and Rescue Strategies Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine When to Modify Therapy! Studies to date show better responses
Management of Treatment-Experienced Patients: New Agents and Rescue Strategies Joel E. Gallant, MD, MPH Johns Hopkins University School of Medicine When to Modify Therapy! Studies to date show better responses
MDR HIV and Total Therapeutic Failure. Douglas G. Fish, MD Albany Medical College Albany, New York Cali, Colombia March 30, 2007
 MDR HIV and Total Therapeutic Failure Douglas G. Fish, MD Albany Medical College Albany, New York Cali, Colombia March 30, 2007 Objectives Case study Definitions Fitness Pathogenesis of resistant virus
MDR HIV and Total Therapeutic Failure Douglas G. Fish, MD Albany Medical College Albany, New York Cali, Colombia March 30, 2007 Objectives Case study Definitions Fitness Pathogenesis of resistant virus
Approach for the Newly Diagnosed HIV Positive Patient
 Approach for the Newly Diagnosed HIV Positive Patient Jason E. Farley, PhD, MPH, ANP-BC, FAAN, AACRN Associate Professor & NP, Johns Hopkins University School of Nursing & Medicine Director, AETC Adult-Gerontology
Approach for the Newly Diagnosed HIV Positive Patient Jason E. Farley, PhD, MPH, ANP-BC, FAAN, AACRN Associate Professor & NP, Johns Hopkins University School of Nursing & Medicine Director, AETC Adult-Gerontology
Didactic Series. Switching Regimens in the Setting of Virologic Suppression
 Didactic Series Switching Regimens in the Setting of Virologic Suppression Craig Ballard, PharmD, AAHIVP UC San Diego Health Owen Clinic June 14 th, 2018 1 Learning Objectives 1) Describe DHHS guidelines
Didactic Series Switching Regimens in the Setting of Virologic Suppression Craig Ballard, PharmD, AAHIVP UC San Diego Health Owen Clinic June 14 th, 2018 1 Learning Objectives 1) Describe DHHS guidelines
The Eras of the HIV Epidemic
 The Eras of the HIV Epidemic 1930-1980 1981-1986 1987-1995 1996-2005 2nd Gen. HAART 2006-2011 2006: Disproportionate distribution of HIV 2006: Gates and Clinton at International AIDS conference announce
The Eras of the HIV Epidemic 1930-1980 1981-1986 1987-1995 1996-2005 2nd Gen. HAART 2006-2011 2006: Disproportionate distribution of HIV 2006: Gates and Clinton at International AIDS conference announce
HIV Diagnosis and Management 2015 Update. Faria Farhat, MD MedStar Washington Hospital Center
 HIV Diagnosis and Management 2015 Update Faria Farhat, MD MedStar Washington Hospital Center Objectives Describe the epidemiology and pathogenesis of HIV infection Highlight HIV diagnosis algorithm and
HIV Diagnosis and Management 2015 Update Faria Farhat, MD MedStar Washington Hospital Center Objectives Describe the epidemiology and pathogenesis of HIV infection Highlight HIV diagnosis algorithm and
SA HIV Clinicians Society Adult ART guidelines
 SA HIV Clinicians Society Adult ART guidelines In draft format Graeme Meintjes (on behalf of the guidelines committee) Selected topics When to start ART First-line Second-line Third-line Patients with
SA HIV Clinicians Society Adult ART guidelines In draft format Graeme Meintjes (on behalf of the guidelines committee) Selected topics When to start ART First-line Second-line Third-line Patients with
HIV for the Non-ID Pharmacist
 Disclosures HIV for the Non-ID Pharmacist I have nothing to disclose at this time Carmen Faulkner-Fennell, PharmD, BCPS (AQ-ID) Clinical Pharmacy Specialist--Infectious Diseases Greenville Hospital System
Disclosures HIV for the Non-ID Pharmacist I have nothing to disclose at this time Carmen Faulkner-Fennell, PharmD, BCPS (AQ-ID) Clinical Pharmacy Specialist--Infectious Diseases Greenville Hospital System
HIV Testing. HIV Symposium Patient Jane. Outline: 4/13/2010. What are your primary concerns for this patient?
 Patient Jane HIV Symposium 2010 Jess Fogler Waldura, MD Mina Matin, MD National HIV AIDS Clinicians Consultation Center San Francisco General Hospital University of California, San Francisco Referral from
Patient Jane HIV Symposium 2010 Jess Fogler Waldura, MD Mina Matin, MD National HIV AIDS Clinicians Consultation Center San Francisco General Hospital University of California, San Francisco Referral from
Distribution and Effectiveness of Antiretrovirals in the Central Nervous System
 Distribution and Effectiveness of Antiretrovirals in the Central Nervous System Scott Letendre, MD Associate Professor of Medicine HIV Neurobehavioral Research Center and Antiviral Research Center University
Distribution and Effectiveness of Antiretrovirals in the Central Nervous System Scott Letendre, MD Associate Professor of Medicine HIV Neurobehavioral Research Center and Antiviral Research Center University
PAEDIATRIC HIV INFECTION. Dr Ashendri Pillay Paediatric Infectious Diseases Specialist
 PAEDIATRIC HIV INFECTION Dr Ashendri Pillay Paediatric Infectious Diseases Specialist Paediatric HIV Infection Epidemiology Immuno-pathogenesis Antiretroviral therapy Transmission Diagnostics Clinical
PAEDIATRIC HIV INFECTION Dr Ashendri Pillay Paediatric Infectious Diseases Specialist Paediatric HIV Infection Epidemiology Immuno-pathogenesis Antiretroviral therapy Transmission Diagnostics Clinical
HIV infection and Primary Care. HIV Care in /30/2013. It s not the AIDS of 85. Stephen Raffanti MD MPH Vanderbilt University School of Medicine
 HIV infection and Primary Care Stephen Raffanti MD MPH Vanderbilt University School of Medicine HIV Care in 2013 Chronic lifelong treatment with all the associated issues: medication tolerability medication
HIV infection and Primary Care Stephen Raffanti MD MPH Vanderbilt University School of Medicine HIV Care in 2013 Chronic lifelong treatment with all the associated issues: medication tolerability medication
Natural history of HIV Infection
 HIV in Primary Care Joint RCGP/BHIVA Multidisciplinary Conference Dr Ian Williams University College London Medical School Friday 25 January 2013, Royal College of General Practitioners, London HIV Treatment
HIV in Primary Care Joint RCGP/BHIVA Multidisciplinary Conference Dr Ian Williams University College London Medical School Friday 25 January 2013, Royal College of General Practitioners, London HIV Treatment
WESTERN CAPE ART GUIDELINES PRESENTATION 2013
 WESTERN CAPE ART GUIDELINES PRESENTATION 2013 The WC guidelines are based on SA National ART guidelines dated 24th March 2013 Acknowledgement goes to members of the Adult and Paediatric HAST policy advisory
WESTERN CAPE ART GUIDELINES PRESENTATION 2013 The WC guidelines are based on SA National ART guidelines dated 24th March 2013 Acknowledgement goes to members of the Adult and Paediatric HAST policy advisory
Historic Perspective on HIV and TB Research in Pregnant Women
 Historic Perspective on HIV and TB Research in Pregnant Women Lynne M. Mofenson, M.D. Senior HIV Technical Advisor Elizabeth Glaser Pediatric AIDS Foundation High Burden of TB/HIV in Women - 2016 TB HIV
Historic Perspective on HIV and TB Research in Pregnant Women Lynne M. Mofenson, M.D. Senior HIV Technical Advisor Elizabeth Glaser Pediatric AIDS Foundation High Burden of TB/HIV in Women - 2016 TB HIV
Epidemiology Testing Clinical Features Management
 Jason Cronin, MD Epidemiology Testing Clinical Features Management In 1981, 1 the first cases of AIDS were identified among gay men in the US. However, scientists later found evidence that the disease
Jason Cronin, MD Epidemiology Testing Clinical Features Management In 1981, 1 the first cases of AIDS were identified among gay men in the US. However, scientists later found evidence that the disease
THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010
 THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010 The South African Antiretroviral Treatment Guidelines 2010 Goals of the programme Achieve best health outcomes in the most cost-efficient manner
THE SOUTH AFRICAN ANTIRETROVIRAL TREATMENT GUIDELINES 2010 The South African Antiretroviral Treatment Guidelines 2010 Goals of the programme Achieve best health outcomes in the most cost-efficient manner
Supplementary Figure 1. Gating strategy and quantification of integrated HIV DNA in sorted CD4 + T-cell subsets.
 Supplementary information HIV reservoir size and persistence are driven by T-cell survival and homeostatic proliferation. Chomont, N., M. El Far, P. Ancuta, L. Trautmann, F. A. Procopio, B. Yassine-Diab,
Supplementary information HIV reservoir size and persistence are driven by T-cell survival and homeostatic proliferation. Chomont, N., M. El Far, P. Ancuta, L. Trautmann, F. A. Procopio, B. Yassine-Diab,
COMPREHENSIVE ANTIRETROVIRAL TABLE: ADULT DOSING, DOSAGE FORM MODIFICATIONS, ADVERSE REACTIONS and INTERACTION POTENTIAL
 Generic Name COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir)
Generic Name COMPREHENSIVE ANTIRETROVIRAL TABLE: NUCLOESIDE/TIDE REVERSE TRANSCRIPTASE INHIBITORS (N(t)RTIs) Abacavir ABC (Ziagen) Didanosine ddi (Videx EC) Emtricitabine FTC (Emtriva) Lamivudine 3TC (Epivir)
Supplementary information
 Supplementary information Dose-response Curve Slope Sets Class-Specific Limits on Inhibitory Potential of Anti-HIV Drugs Lin Shen 1,2, Susan Peterson 1, Ahmad R. Sedaghat 1, Moira A. McMahon 1,2, Marc
Supplementary information Dose-response Curve Slope Sets Class-Specific Limits on Inhibitory Potential of Anti-HIV Drugs Lin Shen 1,2, Susan Peterson 1, Ahmad R. Sedaghat 1, Moira A. McMahon 1,2, Marc
What s New. In The 2016 Perinatal HIV Treatment Guidelines? Provided by CDC s Elimination of Perinatal HIV Transmission Stakeholders Group
 What s New In The 2016 Perinatal HIV Treatment Guidelines? Provided by CDC s Elimination of Perinatal HIV Transmission Stakeholders Group Guidelines for our Online Meeting Room You will be listening to
What s New In The 2016 Perinatal HIV Treatment Guidelines? Provided by CDC s Elimination of Perinatal HIV Transmission Stakeholders Group Guidelines for our Online Meeting Room You will be listening to