Extrapulmonary Tuberculosis. E. Ann Misch, MD Assistant Professor Division of Infectious Diseases Department of Medicine
|
|
|
- Teresa Cook
- 5 years ago
- Views:
Transcription

1 Extrapulmonary Tuberculosis E. Ann Misch, MD Assistant Professor Division of Infectious Diseases Department of Medicine
2 OBJECTIVES 1. Introduction pathogenesis of EPTB epidemiology of EP TB 2. Clinical features and diagnosis in-depth discussion of a case (with audience questions) other presentations of EP TB 3. Summary
3 TB pathogenesis
4 tuberculosis pathogenesis Droplet Inhalation Lung 1 Infection Alveolar Mf Spread to LN Bacillemia Primary Progressive 10% No Infection 90% Latent inapparent infection that is aborted?? positive skin test (PPD) Ghon Complex on CXR positive IGRA

5 Mf=macrophage primary focus in lung: o 85% within 1 cm of pleural surface o 66% in lower half of lungs o multiplication within Mfs in granuloma o Mf death bacilli escape to local Lymph nodes hilar focus 2-3 wks post infxn: o hematogenous seeding from primary foci to sites in body: brain apical posterior lung kidneys vertebrae epiphyses 3-4 wks post infxn: o cell mediated immunity arrests 1, 2 nd foci



6 old, healed TB of lung Ghon /Ranke Complex
7 Q1: what is the estimated rate of latent tuberculosis among foreign-born individuals in the United States? 1. 4% 2. 10% 3. 20% 4. 40% 5. 60% Miramontes R (2015). PLoS ONE 10(11): e


8 pathogenesis: reactivation modified by immune suppression/hiv Latency early reactivation 5% in first 2 yrs late reactivation 5% over rest of lifetime 80% Lung Apex Pulmonary Dz Seed Organs Disseminated Miliary R. Hewlett NEJM (2004) Meninges & Brain

9 reactivation of pulmonary tuberculosis classic reactivation tuberculosis with apical cavity ( post primary tuberculosis )
 Extrapulmonary Pleural (16%) Other (23%) Bone/joint (10%) Genitourinary (5%) Peritoneal (6%) Meningeal")
10 Extrapulmonary Sites of Disease CDC Reported TB Cases, United States, 2016 All PTB 70% 20% EP/PTB EP Lymphatic (36%) Extrapulmonary Pleural (16%) Other (23%) Bone/joint (10%) Genitourinary (5%) Peritoneal (6%) Meningeal (4%)
11 Extrapulmonary TB: effect of ethnicity Dutch population subgroups PTB (%) EP TB (%) Total (%) p Total population 8,216 (62.0) 5,042 (38.0) 13,258 (100) Country of origin <0.01 Europe, central and eastern 395 (85) 70 (15) 465 (100) Turkey 449 (68) 212 (32) ethnic Dutch 3,800 (70) 1,882 (33) other 435 (67) 211 (33) 661 (100) Africa 789 (63) 456 (37) 1,267 (100) Morocco 758 (60) 509 (40) 1,692 (100) Asia 895 (56) 705 (44) 1,600 (100) Somalia 695 (41) 997 (59) 646 (100) te Beek, LA (2006) Emerging Infect Dis 12 (9): doi: /eid
. Epidemiology of Extrapulmonary Tuberculosis in the United States, 1993 2006.")
12 Extrapulmonary TB: effect of HIV population subgroup, U.S. OR, EPTB 1 vs PTB p OR, EPTB 2 vs PTB P HIV-positive 1.1 < <0.001 HIV-negative ref ref Foreign-born 1.5 < U.S.-born ref ref EPTB 1, extrapulmonary TB, without concomitant pulmonary or disseminated TB. EPTB 2, extrapulmonary TB with either concomitant pulmonary or disseminated TB Adapted from Peto H (2009). Epidemiology of Extrapulmonary Tuberculosis in the United States, Clin Infect Dis 49:1350 7
13 Extrapulmonary TB: other risk factors Tumor necrosis factor (TNF) blockers Corticosteroids Malignancy Female gender Nonsmoker Organ transplantation Houston A (2014). Medicine 42: 18 22; Canet E (2011). Nephrol Dial Transplant 26: ; Epstein (2018). Infect Dis Clin N Am 32: Peto H (2009). Clin Infect Dis 49:1350 7
14 Case 1 MARCH year old Hmong male with hypertension, diabetes and renal failure. PPD negative: 10/29/2012 Admitted to local hospital in March 2016 with dry cough x three months, shortness of breath and chest pain after dialysis earlier that day. No fever. Diagnosed with pulmonary emboli (blood clots in lung arteries) CT of chest: loculated, moderate pleural effusion on right Echocardiogram: severe diasotolic dysfunction (stiff, noncompliant heart) Discharged home
15 Case 1 Q2 what percent of Wisconsin s non-us-born TB cases come from the Hmong community (ten year average: ) what is the relative risk of TB in Hmong population compared to the white population in Wisconsin? 1. 10% 17x higher 2. 18% 143x higher 3. 40% 17x higher 4. 65% 143x higher 5. 85% 17x higher Active TB rates per 100,000 population Hmong in WI Caucasian in WI 0.15 overall, WI 0.42 overall, U.S. 2.90
16 Case 1 Q3: In end-stage renal disease, what is sensitivity and specificity for tuberculin skin test for predicting progression to active disease? 1. TST in DIALYSIS PATIENTS sensitivity: 43% specificity: 74% Eleftheriadis T (2011). Hippokiratia 15: PPV: 12% NPV: 94% Caveat: anergy reported in 30-40% of dialysis patients Woeltje KF (1998). Am J Kidney Dis. 31: Fang HC (2002). Nephron. 91: Poduval RD (2003). Clin Nephrol. 59: Eleftheriadis T (2005). Am J Kidney Dis. 46:
.")
17 Does a positive TST predict future tuberculosis in dialysis patients? * Campbell JR (2016). Int J Tuberc Lung Dis 20: *incidence rate ratio of active TB
18 Case 1, cont d APRIL weeks later admitted with shortness of breath and hypoxia (87% on room air) CT shows large, loculated pleural effusion involving right lung patchy infiltrates in left lower lobe lobes. Enlarged heart. calcified granulomas within the mediastinum and hilum 3 L of fluid removed at dialysis breathing at baseline Discharged home (plans for outpatient thoracentesis)

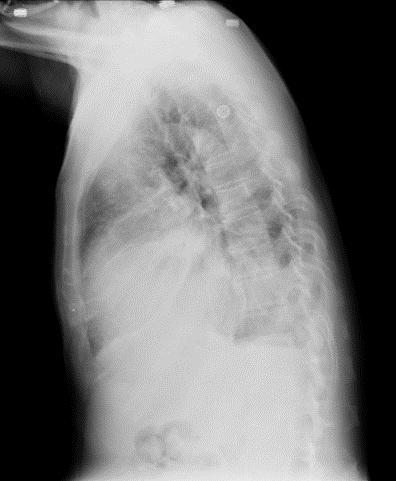


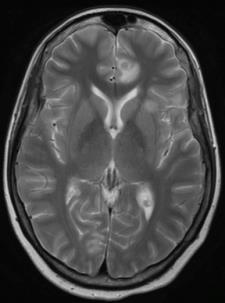
19 Case 1, cont d
20 Case 1 Q4: what TB risk factors does this patient have? Risk factor for Acquisition (latent TB infection) 1. Born in a TB-endemic country Risk Factor for Progression to Active Disease 2. Diabetes 3. End-stage renal disease 4. Signs of old TB on chest X ray, with no history of treatment
21 Risk Factors for TB Progression, 1 RISK FACTOR RR close contact with person with active TB 6.1 old, healed TB on imaging, not treated mg prednisone per day 2.8 underweight (>10%) 1.6 smoking 1.5 Horsburgh (2011). N Engl J Med 364:
22 Risk Factors for TB Progression, 2 Risk Factor Head and Neck Cancer Silicosis Jejunoileal bypass pregnancy Kidney Transplant TNF- blockade Heart Transplant Chronic Renal Failure Cirrhosis HIV Gastrectomy Diabetes Mellitus Relative Risk* (RR) [SIR] [HR] Am Rev Respir Dis Mar;143(3):501-4 (RR=26, pregnant females): Int J Epidemiol Dec;22(6): (RR=8.3); Barber et al. Medicine (Baltimore) Nov;69(6): (9 patients and lit review: can present with mycobacteremia); Tuber Lung Dis Jun;75(3): (RR=3.1); Tuber Lung Dis Feb;76(1):11-6. (RR=11.5) Cote d Ivoire; AIDS Mar;10(3): (RR=7.1; age and sex adjusted); Trans R Soc Trop Med Hyg Sep-Oct;94(5):500-3 (RR= 7.1); Int J Epidemiol Apr;27(2): (RR=9.1 for CD4 count <200 vs. 500) patients with HIV; Med Pregl. 2004;57 Suppl 1:53-8. most estimates in slide (nonhiv) come from this abstract; cirrhosis risk: Lin YT Am J Epidemiol Jul 1;180(1): [hazard ratio reported]
 b 50% upper limit of normal serum value [8.5]) c Aggarwal AN (2016). Int J Tuberc Lung Dis.")
23 Case 1: pleural fluid analysis (4/28/2016) component Normal range Patient value Glucose 60 mg/dl 67 LDH 120 a 2,535 PROTEIN 4.25 b 5.4 CYTOLOGY no atypical cells No cancerous cells ph > 7.30 Not done Adenosine deaminase < 40 IU/L c Not done a 60% of upper limit of normal serum value [200]) b 50% upper limit of normal serum value [8.5]) c Aggarwal AN (2016). Int J Tuberc Lung Dis. 20(10):1386. Bacterial gram stain and culture: negative Fungal smear and culture: negative AFB smear and culture: negative
 Clin Infect Dis 64:111-115. doi: 10.")
24 Case 1 Q5: which tissue has the lowest sensitivity for detection of AFB organisms on smear? 1. Pleural fluid 2. Pleural tissue 3. Cerebrospinal fluid 4. Pericardial fluid 5. Peritoneal fluid 1. Pleural fluid: 0-10% 2. Pleural tissue: 14-39% 3. CSF: 10-30% 4. Pericardial fluid: 0-42% 5. Peritoneal fluid: <5% Lewinsohn DM (2017) Clin Infect Dis 64: doi: /cid/ciw778.


25 JUNE 2016 renal transplant June 4 immune suppression (basilixumab, belatacept, mycophenolate, tacrolimus) SEPTEMBER 2016 Admitted for trauma after motor vehicle accident 9/15/2016


 Placed on")
26 Case 1 OCTOBER 2016 Re-admitted with fever and diagnosed with pulmonary and disseminated blastomycosis Involvement of skin, CNS, knee (infected joint) Placed on amphotericin voriconazole



27
28 Case 1 Interferon gamma release assay 10/14/2016 test component normal range patient values TB minus NIL 0.34 IU/mL 0.01 MITOGEN minus NIL NIL 8.00 IU/mL 0.05 Interpretation: NEGATIVE
29 Case 1 Q6: Does a very high interferon-gamma level on the IGRA predict greater likelihood of progression to active disease? 1. Yes 2. No 3. Maybe At the individual level, not very well. However, two recent studies suggest that higher IFN-gamma levels might be associated with greater risk of progression to active tuberculosis
 negative at 18 24 weeks of age followed over subsequent 6-24 months for IGRA conversion and")
30 Do interferon-gamma levels predict future active disease? 2,512 HIV-negative infants in South Africa HIGH INCIDENCE SETTING IGRA (QFT) negative at weeks of age followed over subsequent 6-24 months for IGRA conversion and active tuberculosis higher rates of tuberculosis in those who converted and had interferon-gamma levels of > 4.00 IU/ml

31 LOW INCIDENCE SETTING population-based, prospective cohort of 44, 875 Norwegians QFT results linked with diagnosis and LTBI prescription data from national registries outcome: TB diagnosis >3 months after QFT testing Only tests with IFN-γ levels <10.0 IU/mL were included (levels >10 IU not quantified by lab)

32 Do interferon-gamma levels predict active disease? 90% of individuals had only a single test no data on whether positive test represented conversions 25% of Norwegian-born were receiving immune suppression very low levels of HIV (1-3%) foreign-born: 43%
33 Summary: Do interferon-γ levels predict active disease? 1. At the population level, maybe 2. at the individual level, magnitude of the IFN-γ response has poor positive predictive value for active TB meta-analysis: PPV 2.7% TB contacts: PPV 2.4% 28.6% immunocompromised: PPV 7% 8% 3. None of this applies to patients with end-stage renal disease 1. Diel R. Chest 2012;142:63 75 (meta-analysis) 2. Zellweger JP. Am J Respir Crit Care Med 2015; 191: (low-incidence) 3. Hermansen TS. Thorax 2016;71:652 8 (low-incidence) 4. Diel R. Am J Respir Crit Care Med 2011;183:88 95 (TB contacts) 5. Sloot R. Am J Respir Crit Care Med 2014;190: (TB contacts) 6. Aichelburg MC. Clinical Infectious Diseases 2009;48: (IC host)



34 Case 1 DECEMBER 2016-JUNE 2017: IMPROVED AUGUST 2017 Skin lesions healed; still on voriconazole Temperature noted to be 99.4 F through interpreter, relates feeling well. However, noted to be "wearing blankets" in the waiting room, and admits to being "a little warm" and perhaps a little chilly in the clinic waiting room.
35 OCTOBER 2017 Followed up again in ID clinic on Temperature noted again to be 99.4 F. Denied fevers, chills, night sweats, hallucinations, transplant problems tolerating medications, new clinic visit, neuropathic 8/3/17 complaints. Noted some loss of appetite. Disseminated blastomycosis clinic visit, 10/19/17


36 Absence of breath sounds right lower lung fields. ID clinician noted prior history of effusion, since March Became concerned about reactivation of latent TB. Patient refused CT and went home.
37 7 days later, admitted to outside (local) hospital Felt unwell, burning sensation all over body. Temp 97.8 F. Glucose in 600s. Insulin increased and discharged. ID clinician spoke to inpatient hospitalist to request chest CT and thoracentesis. This was not done. NOVEMBER 2017 Admitted again to local hospital, with complaint of increasing weakness, intermittent diarrhea, intermittent fevers, dehydration, body aches. Temp 96.5 F. Hydrated and discharged.



38 DECEMBER 2017 Represented 12/14/2017 to local hospital with fever, progressive weakness, anorexia, all over body pain. Son moved home from St paul, MN to provide care over past month. Vitals: T F, pulse 107 BP 129/65, 96% RA Exam notable for sweating, weakness, muscle wasting Transferred to UW hospital. Placed on TB precautions
39 Case 1 Q7: what TB diagnostic studies can be sent on bodily fluids, incl pleural fluid? 1. Xpert MTB/RIF and culture 2. Culture only 3. Free interferon-gamma level 4. IL-1β 5. Lipoarabinomannan 6. Adenosine de-aminase urine/blood only
40 Case 1 Thoracentesis: Pleural fluid culture: AFB smear+, MTD probe positive, culture positive (drug susceptible) Blood cultures: MTB culture-positive (drug susceptible) Sputum cultures: > 9 AFB stain, MTB probe-positive, MTB culture-positive (drug susceptible)
41 Case 1 Interferon gamma release assay 12/16/2017 test component normal range patient values TB minus NIL 0.34 IU/mL 0.73 MITOGEN minus NIL NIL 8.00 IU/mL 0.59 Interpretation: POSITIVE
42 Case 1 Taken to OR 12/18/2017 for decortication of right lung, bronchoscopy, and mediastinal lymph node biopsy Pathology of right pleura: suppurative inflammation, fibrosis and non-necrotizing granulomas. AFB and GMS stain negative Stain/culture of pleural tissue: >9 AFB, MTB culturepositive Pathology of mediastinal lymph node: necrotizing and non-necrotizing granulomas. Stain/culture of Lymph node: Stain positive for acid-fast bacilli. AFB culture positive Bronchoalevolar lavage: Multiple black submucosal endobronchial lesions noted. +broad-based yeast. 1-9 AFB, MTB culture-positive
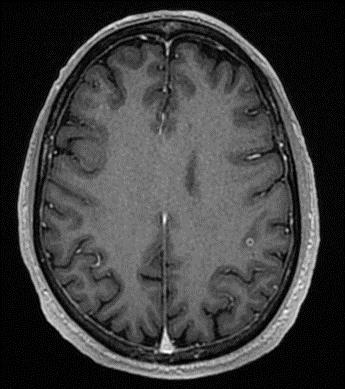
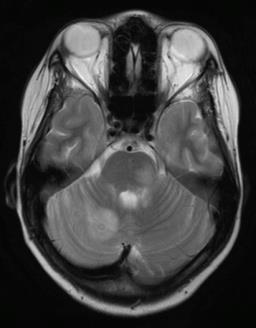
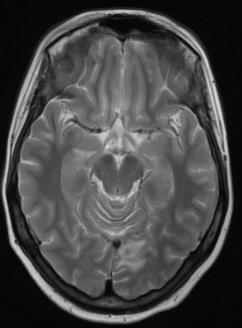
43 Case 1 Presumed CSF involvement CSF Normal Range Patient Data nucleated cells 0-5 /ul 73 differential 97% lymphocytes red blood cells 0-0 /ul 3 GLUCOSE mg/dl 97 PROTEIN mg/dl 266 CSF AFB smear negative, culture negative diagnosis: disseminated TB with pulmonary and extrapulmonary involvement
44 Notable features of case 1. overlooked risk factor for infection: birth in Laos 2. multiple risk factors for progression also overlooked: diabetes, renal failure, radiographic evidence of old, untreated TB and immune suppression 3. neither active TB nor LTBI was aggressively investigated prior to transplant 4. Diagnostic delay 5. Atypical presentation (fever was intermittent; weight loss, anorexia, body pain, persistent loculated effusion were prominent) 6. extrapulmonary and disseminated disease
45 Extrapulmonary tuberculosis: clinical spectrum


46 pleural tuberculosis


47 pleural TB loculated effusion loculated effusion thickened pleura

48 lymphadenitis 43 yo male with cervical LN swelling x 4 wks. No fever, cough. Exposure: No TB contacts. Born in Afghanistan exam: Unilateral enlarged, nontender, submandibular LN. PPD 10 mm. CXR: NL

49 Chris Spitters, MD, MPH

50 Chris Spitters, MD, MPH scrofula

51 scrofula


52 GI TB: often involves ileo-cecal junction, mimicking inflammatory bowel disease Sharma (2016). Indian J Radiol Imaging 26:
.")
53 pancreatic tuberculosis mass at head of pancreas Li (2011). Gut 60:1086


54 Genitourinary tuberculosis credit: Chris Spitters, MD, MPH, Loren Denlinger, MD

55 Genitourinary tuberculosis prostate abscess Chris Spitters, MD, MPH

56 spinal tuberculosis Diskitis, osteomyelitis +/- paraspinous abscess Chris Spitters, MD, MPH, King Country TB program, Washington state


57 Chris Spitters, MD, MPH
58 Extrapulomary tuberculosis: diagnosis
59 symptoms
60 Los Angeles county, California: April-Sept consecutive cases of confirmed tuberculosis identified prospectively 526 sent questionnaires 313 completed predominantly male (64%), non-white (90%), foreign-born (71.4%), few HIV + (12%), pulmonary TB (80%) significant symptoms within past 2 years: cough for >2 weeks weight loss fever for >2 weeks hemoptysis Miller LG (2000). Clin Infect Dis 30: 293 9

61 Loren G Miller et al (2000). Clinical Infectious Diseases 30:293 9
62 Trait Ethnicity overall No. (%) No. (%) with significant sxs Multivariate Analysis OR Asian 74 (23.9) 30 (42.2) 0.17 < Black 38 (12.3) 28 (73.7) 0.43 White 32 (10.4) 25 (78.1) 0.84 Hispanic 153 (49.5) 124 (81.0) 0.96 No Insurance 147 (51.2) 120 (82.8) 3.60 ( ) Homeless 26 (8.6) 23 (88.5) 0.71 Incarceration 83 (27.3 ) 65 (78.3) 0.74 TB diagnosed because of Symptoms 216 (70.1) 177 (81.9) 5.89 ( ) < Screening 92 (29.9) 37 (42.0) Skin Test Positive 218 (83.5) 144 (67.0) 6.40 ( ) 0.02 Negative 43 (16.5) 39 (92.9) P
. Clinical Microbiology Reviews 27: 3-20.")
63 attenuated symptoms immune suppression Adapted from Pai M (2014). Clinical Microbiology Reviews 27: 3-20.
64 Diagnosis of Extra Pulmonary TB: tissue sampling Send respiratory samples even if chest imaging is negative. Bronchoscopy if cannot obtain sputum biopsy biopsy enlarged lymph nodes use CT or MRI to find extrapulmonary lesions that can serve as biopsy targets for pleural TB, pleural biopsy is often required tissue should be sent for AFB stain and culture, as well as PCR/probe testing (may need to be a reference lab)
65 Non-culture-based methods Bacteria or bacterial product is detected oin-situ hybridization (probe) o DNA/RNA amplification = NAAT PCR rtpcr omaldi-tof ourine Lipoarabinomannan Host response is measured oin principle, gene expression signature
66 Nucleic Acid Amplification Tests (NAAT) Versions Amplified MTD (GenProbe) GeneXpert Mtb/RIF (Cepheid) Non FDA-Approved MTBDR Plus (Hain) Others When to Use Directly on processed (unfixed) specimen No current TB rx >7 days No prior TB rx within past 12 months
67 Sensitivity and speed of various methods of TB identification Method Sensitivity (# bugs required) Speed AFB Smear 10 4 Hours Conventional Culture 10 3 Weeks Radiometric/MGIT Days DNA Probe Days (min?) RNA Probe Days (min?) PCR (MTD) + Probe 10 0(?) Days (hours) PCR + DNA sequencing 10 0(?) Days Loren Denlinger, MD
68 Summary: clinical features and diagnosis 1. the key to making the diagnosis is understanding the host 2. classic symptoms (fever, cough, night sweats, weight loss, hemoptysis) may be absent or attenutate 3. diagnostic delay is common 4. certain ethnic groups may be more likely to present with extrapulmonary disease
69 Summary: clinical features and diagnosis 5. PPD and IGRAs have relatively poor positive predictive value for active disease 6. EPTB is typically a paucibacillary disease. Thus, smear and culture are less sensitive than for pulmonary TB. 7. Molecular methods are critical to making a microbiologic diagnosis. PCR is currently the most reliable non-culture-based diagnostic tool
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis
 Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Mycobacterial Infections: What the Primary Provider Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Diagnosis of active TB Screening
Diagnosis and Medical Management of Latent TB Infection
 Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Diagnosis and Medical Management of Latent TB Infection Marsha Majors, RN September 7, 2017 TB Contact Investigation 101 September 6 7, 2017 Little Rock, AR EXCELLENCE EXPERTISE INNOVATION Marsha Majors,
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016
 Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
Latent Tuberculosis Infections Controversies in Diagnosis and Management Update 2016 Randy Culpepper, MD, MPH Deputy Heath Officer/Medical Director Frederick County Health Department March 16, 2016 2 No
TUBERCULOSIS. Pathogenesis and Transmission
 TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TUBERCULOSIS Pathogenesis and Transmission TUBERCULOSIS Pathogenesis and Transmission Infection to Disease Diagnostic & Isolation Updates Treatment Updates Pathogenesis Droplet nuclei of 5µm or less are
TB Intensive Houston, Texas. Childhood Tuberculosis Kim Connelly Smith. November 12, 2009
 TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
TB Intensive Houston, Texas November 10-12, 12 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 Childhood Tuberculosis Kim Connelly Smith MD, MPH November 12, 2009 1 OUTLINE Stages
Tuberculosis Tools: A Clinical Update
 Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
Tuberculosis Tools: A Clinical Update CAPA Conference 2014 JoAnn Deasy, PA-C. MPH, DFAAPA jadeasy@sbcglobal.net Adjunct Faculty Touro PA Program Learning Objectives Outline the pathogenesis of active pulmonary
The Diagnosis of Active TB. Deborah McMahan, MD TB Intensive September 28, 2017
 The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
The Diagnosis of Active TB Deborah McMahan, MD TB Intensive September 28, 2017 Agenda Epidemiology Big picture Conditions that Should Make You Suspicious Which test? Eeenie meenie miny mo Radiographic
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Global Impact of TB
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Epidemiology Common disease presentations Diagnosis of active TB Screening
TB Intensive Houston, Texas
 TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
TB Intensive Houston, Texas October 15-17, 17 2013 Diagnosis of TB: Radiology Rosa M Estrada-Y-Martin, MD MSc FCCP October 16, 2013 Rosa M Estrada-Y-Martin, MD MSc FCCP, has the following disclosures to
What the Primary Physician Should Know about Tuberculosis. Topics for Discussion. Life Cycle of M. tuberculosis
 What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
What the Primary Physician Should Know about Tuberculosis Henry F. Chambers, M.D Professor of Medicine, UCSF Topics for Discussion Microbiology Epidemiology Common disease presentations Diagnosis of active
TB In Detroit 2011* Early TB: Smudge Sign. Who is at risk for exposure to or infection with TB? Who is at risk for TB after exposure or infection?
 Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
Those oral antibiotics are just not working! Inpatient Standards of Care & Discharge Planning S/He s in the Hospital: Now What Do I Do? Dana G. Kissner, MD TB Intensive Workshop, Lansing, MI 2012 Objectives:
TB Nurse Case Management San Antonio, Texas July 18 20, 2012
 TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas July 18 20, 2012 Pediatric TB Kim Smith, MD, MPH July 19, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
TB Nurse Case Management San Antonio, Texas March 7 9, Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012
 TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Nurse Case Management San Antonio, Texas March 7 9, 2012 Pediatric TB Kim Connelly Smith, MD, MPH March 8, 2012 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict of interests
Tuberculosis Pathogenesis
 Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
Tuberculosis Pathogenesis Renuka Khurana, MD, MPH May 12, 2015 TB for Community Providers May 12, 2015 Phoenix, Arizona EXCELLENCE EXPERTISE INNOVATION Renuka Khurana, MD, MPH has the following disclosures
TB: Management in an era of multiple drug resistance. Bob Belknap M.D. Denver Public Health November 2012
 TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB: Management in an era of multiple drug resistance Bob Belknap M.D. Denver Public Health November 2012 Objectives: 1. Explain the steps for diagnosing latent and active TB role of interferon-gamma release
TB Intensive San Antonio, Texas December 1-3, 2010
 TB Intensive San Antonio, Texas December 1-3, 2010 TB Pathogenesis and Transmission Lynn Horvath, MD; TCID December 1, 2010 Tuberculosis Pathogenesis Lynn L. Horvath, MD, FACP, FIDSA Associate Professor
TB Intensive San Antonio, Texas December 1-3, 2010 TB Pathogenesis and Transmission Lynn Horvath, MD; TCID December 1, 2010 Tuberculosis Pathogenesis Lynn L. Horvath, MD, FACP, FIDSA Associate Professor
Diagnosis & Medical Case Management of TB Disease. Lisa Armitige, MD, PhD October 22, 2015
 Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Diagnosis & Medical Case Management of TB Disease Lisa Armitige, MD, PhD October 22, 2015 Comprehensive Care of Patients with Tuberculosis and Their Contacts October 19 22, 2015 Wichita, KS EXCELLENCE
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Childhood Tuberculosis Kim Smith, MD, MPH April 6, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive
 Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Tuberculosis Intensive San Antonio, Texas April 3 6, 2012 Tuberculosis Pathogenesis Lynn Horvath, MD April 3, 2012 Lynn Horvath, MD has the following disclosures to make: No conflict of interests No relevant
Pathology of pulmonary tuberculosis. Dr: Salah Ahmed
 Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Pediatric TB Lisa Armitige, MD, PhD September 28, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Pediatric TB Lisa Armitige, MD, PhD September 28, 2011 Lisa Armitige, MD, PhD has the following disclosures to make: No conflict of interest.
LTBI: Who to Test & When to Treat
 LTBI: Who to Test & When to Treat TB Intensive May 10 th, 2016 David Horne, MD, MPH Harborview Medical Center University of Washington DISCLOSURES I have no disclosures or conflicts of interest to report
LTBI: Who to Test & When to Treat TB Intensive May 10 th, 2016 David Horne, MD, MPH Harborview Medical Center University of Washington DISCLOSURES I have no disclosures or conflicts of interest to report
Diagnosis of tuberculosis in children
 Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Diagnosis of tuberculosis in children H Simon Schaaf Desmond Tutu TB Centre Department of Paediatrics and Child Health, Stellenbosch University, and Tygerberg Children s Hospital (TCH) Estimated TB incidence
Tuberculosis and Diabetes Mellitus. Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant
 Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
Tuberculosis and Diabetes Mellitus Lana Kay Tyer, RN MSN WA State Department of Health TB Nurse Consultant Learning Objectives Understand the impact of uncontrolled diabetes mellitus (DM) on TB infection
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE
 DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
DIAGNOSIS AND MEDICAL MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH Assistant Professor University of Texas Health Science Center Staff Physician, Texas Center for Infectious Diseases TB Nurse Case
has the following disclosures to make:
 CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
CLINICAL DIAGNOSIS AND MANAGEMENT OF TB DISEASE Annie Kizilbash MD, MPH September 22, 2015 TB Nurse Case Management September 22 24, 2015 San Antonio. TX EXCELLENCE EXPERTISE INNOVATION Annie Kizilbash
Fundamentals of Tuberculosis (TB)
") TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
TB in the United States Fundamentals of Tuberculosis (TB) From 1953 to 1984, reported cases decreased by approximately 5.6% each year From 1985 to 1992, reported cases increased by 20% 25,313 cases reported
Interpretation of Chest Radiographs Paul Christensen, MD 10/21/09. Diagnostic Evaluation. Medical Evaluation & CXR Interpretation.
 Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
Diagnostic Evaluation Medical Evaluation & CXR Interpretation University of Michigan TB Consultant Washtenaw County Medical history Physical examination Testing for TB exposure (previously covered) Radiologic
10/3/2017. Updates in Tuberculosis. Global Tuberculosis, WHO 2015 report. Objectives. Disclosures. I have nothing to disclose
 Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Disclosures Updates in Tuberculosis I have nothing to disclose Chris Keh, MD Assistant Clinical Professor, Division of Infectious Diseases, UCSF TB Controller, TB Prevention and Control Program, Population
Clinical and Public Health Impact of Nucleic Acid Amplification Tests (NAATs) for Tuberculosis
 for Tuberculosis") Clinical and Public Health Impact of Nucleic Acid Amplification Tests (NAATs) for Tuberculosis Amit S. Chitnis, MD, MPH; Pennan M. Barry, MD, MPH; Jennifer M. Flood, MD, MPH. California Tuberculosis Controllers
Clinical and Public Health Impact of Nucleic Acid Amplification Tests (NAATs) for Tuberculosis Amit S. Chitnis, MD, MPH; Pennan M. Barry, MD, MPH; Jennifer M. Flood, MD, MPH. California Tuberculosis Controllers
Diagnosis and Medical Management of TB Disease. Quratulian Annie Kizilbash, MD, MPH March 17, 2015
 Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Diagnosis and Medical Management of TB Disease Quratulian Annie Kizilbash, MD, MPH March 17, 2015 TB Nurse Case Management March 17 19, 2015 San Antonio, Texas EXCELLENCE EXPERTISE INNOVATION Quratulian
Tuberculosis: A Provider s Guide to
 Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Tuberculosis: A Provider s Guide to Diagnosis and Treatment of Active Tuberculosis (TB) Disease and Screening and Treatment of Latent Tuberculosis Infection (LTBI) Alameda County Health Care Services Agency
Dr Francis Ogaro MTRH ELDORET
 Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
Dr Francis Ogaro MTRH ELDORET TB in children often severe, disseminated and can progress rapidly and with poor outcome TB diagnosis in children has relied on clinical, imaging, microscopy and TST findings.
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Madhukar Pai, MD, PhD Author and Series Editor Camilla Rodrigues, MD co-author Abstract Most individuals who get exposed
Rehuka Khurana, MD, MPH has the following disclosures to make:
 Case Presentation Steps to a Systematic Approach to Diagnosis of TB Case Presentation Steps to a Systematic Approach to Diagnosis of TB Renuka Khurana, MD, MPH March 13, 2015 TB for Pulmonologist March
Case Presentation Steps to a Systematic Approach to Diagnosis of TB Case Presentation Steps to a Systematic Approach to Diagnosis of TB Renuka Khurana, MD, MPH March 13, 2015 TB for Pulmonologist March
ANNUAL TUBERCULOSIS REPORT OREGON Oregon Health Authority Public Health Division TB Program November 2012
 ANNUAL TUBERCULOSIS REPORT OREGON 211 Oregon Health Authority Public Health Division TB Program November 212 Page 2 Table of Contents Charts Chart 1 TB Incidence in the US and Oregon, 1985-211... page
ANNUAL TUBERCULOSIS REPORT OREGON 211 Oregon Health Authority Public Health Division TB Program November 212 Page 2 Table of Contents Charts Chart 1 TB Incidence in the US and Oregon, 1985-211... page
Tuberculosis - clinical forms. Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases
 Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Tuberculosis - clinical forms Dr. A.Torossian,, M.D., Ph. D. Department of Respiratory Diseases 1 TB DISEASE Primary Post-primary (Secondary) Common primary forms Primary complex Tuberculosis of the intrathoracic
Diagnosis and Treatment of Tuberculosis, 2011
 Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
Diagnosis of TB Diagnosis and Treatment of Tuberculosis, 2011 Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Diagnosis of TB, 2011 Diagnosis follows Suspicion When should we Think TB? Who is
TB in the Patient with HIV
 TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
TB in the Patient with HIV Lisa Y. Armitige, MD, PhD May 11, 2017 TB Intensive May 9 12, 2017 San Antonio, TX EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD, has the following disclosures to
TB & HIV CO-INFECTION IN CHILDREN. Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012
 TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
TB & HIV CO-INFECTION IN CHILDREN Reené Naidoo Paediatric Infectious Diseases Broadreach Healthcare 19 April 2012 Introduction TB & HIV are two of the leading causes of morbidity & mortality in children
Pediatric TB Intensive Houston, Texas October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Pediatric TB Intensive Houston, Texas October 14, 2013 Diagnosis and Management of Tuberculosis in Adolescents Andrea T. Cruz, MD, MPH Sections of Infectious Diseases & Emergency Medicine October 14, 2013
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017
 Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
Pediatric Tuberculosis Lisa Y. Armitige, MD, PhD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Lisa Y. Armitige, MD, PhD has the following disclosures
My heart is racing. Managing Complex Cases. Case 1. Case 1
 Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
Managing Complex Cases My heart is racing Amee Patrawalla, MD April 7, 2017 Case 1 Rutgers, The State University of New Jersey Rutgers, The State University of New Jersey Case 1 29 year old physician from
Tuberculosis. By: Shefaa Q aqa
 Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
Tuberculosis By: Shefaa Q aqa Tuberculosis is a communicable chronic granulomatous disease caused by Mycobacterium tuberculosis. It usually involves the lungs but may affect any organ or tissue in the
TB in Children. Rene De Gama Block 10 Lectures 2012
 TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
TB in Children Rene De Gama Block 10 Lectures 2012 Contents Epidemiology Transmission and pathogenesis Diagnosis of TB TB and HIV Management Epidemiology The year 2000 8.3 million new TB cases diagnosed
Errors in Dx and Rx of TB
 Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Errors in Dx and Rx of TB David Schlossberg, MD, FACP Professor of Medicine Temple University School of Medicine Medical Director, TB Control Program Philadelphia Department of Public Health TB Still a
Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011
 TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
TB Nurse Case Management Davenport, Iowa September 27 28, 2011 Diagnosis and Management of TB Disease Lisa Armitige, MD, PhD September 27, 2011 Lisa Armitige, MD, PhD has the following disclosures to make:
INDEX CASE INFORMATION
 Instructions for Completing the MDH Tuberculosis Contact Investigation Report Form Please provide as much information as possible. Each field represents information that is important to the contact investigation.
Instructions for Completing the MDH Tuberculosis Contact Investigation Report Form Please provide as much information as possible. Each field represents information that is important to the contact investigation.
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013
 Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
Tuberculosis in Primary Care COC GTA Spring Symposium Dr Elizabeth Rea April 2013 1 TB in Toronto - risk groups Diagnosis of active TB LTBI diagnosis and management Infection control 2 TB in Toronto Case
TB is Global. Latent TB Infection (LTBI) Sharing the Care: Working Together. September 24, 2014
 Sharing the Care: Working Together. September 24, 2014") Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Sharing the Care: Working Together to Meet the Challenge of TB Presented by: Barbara Cole, RN, PHN, MSN Director, Disease Control County of Riverside Department of Public Health Curry International TB
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010
 Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Understanding and Managing Latent TB Infection Arnold, Missouri October 5, 2010 What is Latent TB Infection (LTBI)? Traci Hadley, RN October 5, 2010 LTBI or TB Disease? Presented by : Traci Hadley, RN
Diagnosis Latent Tuberculosis. Disclosures. Case
 Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
Diagnosis Latent Tuberculosis Neha Shah MD MPH Field Medical Officer Tuberculosis Control Branch California Department of Public Health Centers for Disease Control and Prevention September 2016 1 Disclosures
An Introduction to Radiology for TB Nurses
 An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
An Introduction to Radiology for TB Nurses Garold O. Minns, MD September 14, 2017 TB Nurse Case Management September 12 14, 2017 EXCELLENCE EXPERTISE INNOVATION Garold O. Minns, MD has the following disclosures
Northwestern Polytechnic University
 Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
Clinical Tuberculosis Assessment by Health Care Provider Clinicians should review and verify the information in the Tuberculosis (TB) Screening Questionnaire (attached). Persons answering YES to any questions
CHAPTER 3: DEFINITION OF TERMS
 CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
CHAPTER 3: DEFINITION OF TERMS NOTE: TB bacteria is used in place of Mycobacterium tuberculosis and Mycobacterium tuberculosis complex in most of the definitions presented here. 3.1 Acid-fast bacteria
Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining
 Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining of PBMCs. Forward scatter area (FSC-A) versus side scatter area (SSC-A) was used to select lymphocytes followed
Supplemental Figure 1. Gating strategies for flow cytometry and intracellular cytokinestaining of PBMCs. Forward scatter area (FSC-A) versus side scatter area (SSC-A) was used to select lymphocytes followed
CHAPTER:1 TUBERCULOSIS. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
CHAPTER:1 TUBERCULOSIS BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY GLOBAL EMERGENCY: * Tuberculosis kills 5,000 people a day! * 2.3 million die each year!
Learning Objectives: Case 1 11/12/2015. Tuberculosis: Focus on Transmission and Pathogenesis. TB: Some Important Terms
 A 11/12/2015 Learning Objectives: Tuberculosis: Focus on Transmission and Pathogenesis Henry Fraimow, M ivision of Infectious iseases ooper School of Medicine at Rowan University Medical onsultant, Southern
A 11/12/2015 Learning Objectives: Tuberculosis: Focus on Transmission and Pathogenesis Henry Fraimow, M ivision of Infectious iseases ooper School of Medicine at Rowan University Medical onsultant, Southern
Contracts Carla Chee, MHS May 8, 2012
 Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Moving Past the Basics of Tuberculosis Phoenix, Arizona May 8-10, 2012 Contracts Carla Chee, MHS May 8, 2012 Carla Chee, MHS has the following disclosures to make: No conflict of interests No relevant
Annual Tuberculosis Report Oregon 2007
 Annual Tuberculosis Report Oregon 7 Oregon Department of Human Services Public Health Division TB Program April 8 Page 2 Table of Contents Charts Chart 1 TB Incidence in the US and Oregon, 1985-7.. page
Annual Tuberculosis Report Oregon 7 Oregon Department of Human Services Public Health Division TB Program April 8 Page 2 Table of Contents Charts Chart 1 TB Incidence in the US and Oregon, 1985-7.. page
I. Demographic Information GENDER NUMBER OF CASES PERCENT OF CASES. Male % Female %
 San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
San Joaquin County (SJC) in 03, (N=43) County Rate = 6. Cases per 00,000 Population I. Demographic Information Table I-A: TB cases by gender, SJC, 03 (N=43) GENDER NUMBER OF CASES Male 6 60.5% Female 7
Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and Infectious Disease UT Health Northeast
 Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
Practical Aspects for Using the Interferon Gamma Release Assay (IGRA) Test Live Webinar July 14, 2017 Barbara J Seaworth MD Medical Director, Heartland National TB Center Professor, Internal Medicine and
A look at medical factors that increase the risk for TB disease
 A look at medical factors that increase the risk for TB disease Mark Lobato, MD New England TB Consultant Division of Tuberculosis Elimination CDC Overview The spectrum of M. tuberculosis infection Immune
A look at medical factors that increase the risk for TB disease Mark Lobato, MD New England TB Consultant Division of Tuberculosis Elimination CDC Overview The spectrum of M. tuberculosis infection Immune
Approaches to LTBI Diagnosis
 Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
Approaches to LTBI Diagnosis Focus on LTBI October 8 th, 2018 Michelle Haas, M.D. Associate Director Denver Metro Tuberculosis Program Denver Public Health DISCLOSURES I have no disclosures or conflicts
PREVENTION OF TUBERCULOSIS. Dr Amitesh Aggarwal
 PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
PREVENTION OF TUBERCULOSIS Dr Amitesh Aggarwal 25 to 50 % of persons exposed to intimate contact with active PTB - latent infection with TB. Exposure to index case for 12 hours - high risk of infection.
of clinical laboratory diagnosis in Extra-pulmonary Tuberculosis
 New approaches and the importance of clinical laboratory diagnosis in Extra-pulmonary Tuberculosis Bahrmand.AR, Hadizadeh Tasbiti.AR, Saifi.M, Yari.SH, Karimi.A, Fateh.A, Tuberculosis Dept. Pasteur Institute
New approaches and the importance of clinical laboratory diagnosis in Extra-pulmonary Tuberculosis Bahrmand.AR, Hadizadeh Tasbiti.AR, Saifi.M, Yari.SH, Karimi.A, Fateh.A, Tuberculosis Dept. Pasteur Institute
TUBERCULOSIS. By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi
 TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
Diagnosis of Tuberculosis Infection and Disease
 Diagnosis of Tuberculosis Infection and Disease David E. Griffith, M.D. Assistant Medical Director Heartland National TB Center The Medical Evaluation for Diagnosing Tuberculosis Traditional Approach Patient
Diagnosis of Tuberculosis Infection and Disease David E. Griffith, M.D. Assistant Medical Director Heartland National TB Center The Medical Evaluation for Diagnosing Tuberculosis Traditional Approach Patient
TB Classification (ATS/CDC)
") bits and pieces Lisa Chen, MD UCSF Pulmonary/Critical Care Curry International Tuberculosis Center 10/2017 TB Classification (ATS/CDC) TB0 No tuberculosis exposure, not infected TB1 Tuberculosis exposure,
bits and pieces Lisa Chen, MD UCSF Pulmonary/Critical Care Curry International Tuberculosis Center 10/2017 TB Classification (ATS/CDC) TB0 No tuberculosis exposure, not infected TB1 Tuberculosis exposure,
Targeted Testing and the Diagnosis of. Latent Tuberculosis. Infection and Tuberculosis Disease
 Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Self-Study Study Modules on Tuberculosis Targeted Testing and the Diagnosis of Latent Tuberculosis Infection and Tuberculosis Disease 1 Module 3: Objectives At completion of this module, learners will
Making the Diagnosis of Tuberculosis
 Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
Making the Diagnosis of Tuberculosis Alfred Lardizabal, MD NJMS Global Tuberculosis Institute Testing for TB Infection Targeted Testing: Key Points Test only if plan for ensuring treatment De-emphasizes
The diagnosis of active TB
 The diagnosis of active TB Faculty/Presenter Disclosure Faculty: Martha Ainslie Relationships with commercial interests: Speakers Bureau/Honoraria: Boehringer Ingelheim Mitigating Potential Bias I have
The diagnosis of active TB Faculty/Presenter Disclosure Faculty: Martha Ainslie Relationships with commercial interests: Speakers Bureau/Honoraria: Boehringer Ingelheim Mitigating Potential Bias I have
TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014
 TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014 Catalina Navarro, BSN, RN has the following disclosures to make: No conflict of interests No relevant financial relationships with
TB Skin Test Practicum Houston, Texas Region 6/5 South September 23, 2014 Catalina Navarro, BSN, RN has the following disclosures to make: No conflict of interests No relevant financial relationships with
ESCMID Online Lecture Library. by author
 Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Tuberculosis prevention in immunodepressed patients M. Carmen Fariñas Álvarez Infectious Diseases.H.U.Marqués de Valdecilla University of Cantabria, Spain DISCLOSURES I have no potential conflicts with
Disclosures. Updates in TB for the PCP: Opportunities for Prevention. Objectives PART 1: WHY TEST? 4/14/2016. None
 Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
Disclosures Updates in TB for the PCP: Opportunities for Prevention None Pennan Barry, MD, MPH Chief, Surveillance and Epidemiology, California TB Control Branch Assistant Clinical Professor, Division
New Tuberculosis Guidelines. Jason Stout, MD, MHS
 New Tuberculosis Guidelines Jason Stout, MD, MHS Two New Sets of Guidelines Treatment of Drug-Susceptible Tuberculosis Clinical Infectious Diseases 2016; 63(7): e147-e195 Diagnosis of Tuberculosis in Adults
New Tuberculosis Guidelines Jason Stout, MD, MHS Two New Sets of Guidelines Treatment of Drug-Susceptible Tuberculosis Clinical Infectious Diseases 2016; 63(7): e147-e195 Diagnosis of Tuberculosis in Adults
Screening and Treatment Recommendations for Persons Exposed to MDR TB
 Screening and Treatment Recommendations for Persons Exposed to MDR TB Although all persons at increased risk of tuberculosis (TB) infection should be screened for TB infection per USPTF/CDC guidelines
Screening and Treatment Recommendations for Persons Exposed to MDR TB Although all persons at increased risk of tuberculosis (TB) infection should be screened for TB infection per USPTF/CDC guidelines
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS
 CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
CLINICAL FEATURES IN PULMONARY TUBERCULOSIS Dr. Amitesh Aggarwal Department of Medicine Tuberculosis Captain of all the Men of Death Great White Plague devastating effect on society 100 years ago one in
TB in Corrections Phoenix, Arizona
 TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
TB in Corrections Phoenix, Arizona March 24, 2011 Treatment of Latent TB Infection Renuka Khurana MD, MPH March 24, 2011 Renuka Khurana, MD, MPH has the following disclosures to make: No conflict of interests
Pediatric TB Intensive Houston, Texas October 14, Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict
Pediatric TB Intensive Houston, Texas October 14, 2013 Extrapulmonary TB in Children Kim Connelly Smith, MD, MPH October 14, 2013 Kim Connelly Smith, MD, MPH has the following disclosures to make: No conflict
Chapter 22. Pulmonary Infections
 Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Chapter 22 Pulmonary Infections Objectives State the incidence of pneumonia in the United States and its economic impact. Discuss the current classification scheme for pneumonia and be able to define hospital-acquired
Diagnosis of TB: Radiology David Finlay, MD
 TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
TB Intensive Tyler, Texas June 2-4, 2010 Diagnosis of TB: Radiology David Finlay, MD June 3, 2010 2stages stages- Tuberculosis 1. primary infection 2. reactivation, or post primary disease 2 1 Primary
TB Intensive San Antonio, Texas November 29-December 2, 2011
 TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
TB Intensive San Antonio, Texas November 29-December 2, 2011 Diagnosis of TB: Radiology Michael McCarthy, MD, FACR November 30, 2011 Michael McCarthy, MD, FACR has the following disclosures to make: No
Identifying TB co-infection : new approaches?
 Identifying TB co-infection : new approaches? Charoen Chuchottaworn MD. Senior Medical Advisor, Central Chest Institute of Thailand, Department of Medical Services, MoPH Primary tuberculosis Natural history
Identifying TB co-infection : new approaches? Charoen Chuchottaworn MD. Senior Medical Advisor, Central Chest Institute of Thailand, Department of Medical Services, MoPH Primary tuberculosis Natural history
Let s Talk TB A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year
 A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
A Series on Tuberculosis, A Disease That Affects Over 2 Million Indians Every Year Barry Rabinovitch, MD, FRCP(C) Author Madhukar Pai, MD, PhD co-author and Series Editor Barry Rabinovitch is an assistant
Latent Tuberculosis Best Practices
 Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
Latent Tuberculosis Best Practices Last Updated September 7, 2016 LTBI Demographics in the US o 13million people in the US with LTBI (estimate) o In 2014, approximately 66% of TB cases in the United States
TB: A Supplement to GP CLINICS
 TB: A Supplement to GP CLINICS Chapter 10: Childhood Tuberculosis: Q&A For Primary Care Physicians Author: Madhukar Pai, MD, PhD Author and Series Editor What is Childhood TB and who is at risk? India
TB: A Supplement to GP CLINICS Chapter 10: Childhood Tuberculosis: Q&A For Primary Care Physicians Author: Madhukar Pai, MD, PhD Author and Series Editor What is Childhood TB and who is at risk? India
TUBERCULOSIS CONTACT INVESTIGATION
 TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE TUBERCULOSIS CONTACT INVESTIGATION LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the criteria used
TB CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE TUBERCULOSIS CONTACT INVESTIGATION LEARNING OBJECTIVES Upon completion of this session, participants will be able to: 1. Describe the criteria used
Case 1. Background. Presenting Symptoms. Schecter Case1 Differential Diagnosis of TB 1
 TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
TB or Not TB? Case 1 Gisela Schecter, M.D., M.P.H. California Department of Public Health Background 26 year old African American male Born and raised in Bay Area of California Convicted of cocaine trafficking
Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)
") Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)-750-5496 Local health care providers, including physicians offices, labs and hospitals, are required by law to
Tuberculosis Reporting, Waco-McLennan County Public Health District TB Control WMCPHD (254)-750-5496 Local health care providers, including physicians offices, labs and hospitals, are required by law to
TUBERCULOSIS. Presented By: Public Health Madison & Dane County
 TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
TUBERCULOSIS Presented By: Public Health Madison & Dane County What is Tuberculosis? Tuberculosis, or TB, is a disease caused by a bacteria called Mycobacterium tuberculosis. The bacteria can attack any
Tuberculosis What you need to know. James Zoretic M.D., M.P.H. Regions 2 and 3 Director
 Tuberculosis What you need to know James Zoretic M.D., M.P.H. Regions 2 and 3 Director What is Tuberculosis? Tuberculosis, (TB) is a communicable disease caused by the Mycobacterium tuberculosis bacillus
Tuberculosis What you need to know James Zoretic M.D., M.P.H. Regions 2 and 3 Director What is Tuberculosis? Tuberculosis, (TB) is a communicable disease caused by the Mycobacterium tuberculosis bacillus
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University
 Lloyd Friedman, M.D. Milford Hospital Yale University") Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
Targeted Tuberculin Testing and Treatment of Latent Tuberculosis Infection (LTBI) Lloyd Friedman, M.D. Milford Hospital Yale University Tuberculosis Estimates USA World Infection 15,000,000 2,000,000,000
TB the basics. (Dr) Margaret (DHA) and John (INZ)
 Margaret (DHA) and John (INZ)") TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
TB the basics (Dr) Margaret (DHA) and John (INZ) Question 1 The scientist who discovered M. tuberculosis was: A: Louis Pasteur B: Robert Koch C: Jean-Antoine Villemin D: Calmette and Guerin Question 2
TB Intensive San Antonio, Texas August 7-10, 2012
 TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
TB Intensive San Antonio, Texas August 7-10, 2012 An Introduction to Childhood Tuberculosis Kim Smith, MD, MPH August 10, 2012 Kim Smith, MD, MPH has the following disclosures to make: No conflict of interests
What you need to know about diagnosing and treating TB: a preventable, fatal disease. Bob Belknap M.D. Denver Public Health November 2013
 What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
What you need to know about diagnosing and treating TB: a preventable, fatal disease Bob Belknap M.D. Denver Public Health November 2013 Case 1: 52 y/o male Born in the Pacific Islands; some travel in
Tuberculosis and cancer
 Tuberculosis and cancer David P. Holland, MD, MHS Chief Clinical Officer, CDPB Fulton County Department of Health and Wellness Assistant Professor, Emory University Disclosures No relevant financial disclosures
Tuberculosis and cancer David P. Holland, MD, MHS Chief Clinical Officer, CDPB Fulton County Department of Health and Wellness Assistant Professor, Emory University Disclosures No relevant financial disclosures