Immunocytochemistry and the diagnosis of cutaneous lymphoma
|
|
|
- Benedict Willis
- 6 years ago
- Views:
Transcription
1 Histopathology 2010, 56, DOI: /j x REVIEW Immunocytochemistry and the diagnosis of cutaneous lymphoma Alistair Robson Department of Dermatopathology, St John s Institute of Dermatology, St Thomas Hospital, London, UK Robson A (2010) Histopathology 56, Immunocytochemistry and the diagnosis of cutaneous lymphoma Cutaneous lymphoid infiltrates may pose some of the most difficult diagnostic problems in dermatopathology. Immunocytochemistry is often employed in an effort to determine whether an infiltrate is neoplastic or, in the case of clearly malignant infiltrates, to provide a specific diagnosis. The rarity of these disorders and the variant immunocytochemical profiles they may present further thwart understanding and sometimes prevent an accurate diagnosis. In this review the common immunocytochemical profiles of various cutaneous lymphomas are presented and potential pitfalls and problems considered. Immunocytochemistry is not a diagnostic test but, as in other areas of histopathology, is a highly valuable tool that requires critical interpretation within a context: so applied, it is an indispensable part of the pathologist s arsenal in evaluating lymphoid infiltrates and defining different lymphomas. Keywords: cutaneous lymphoma, diagnosis, immunocytochemistry, review Abbreviations: AIDS, acquired immunodeficiency syndrome; ALCL, anaplastic large cell lymphoma; ATL, adult T-cell leukaemia lymphoma; CLH, cutaneous lymphoid hyperplasia; DLBCL, diffuse large B-cell lymphoma; DLBCLL, diffuse large B-cell lymphoma, leg type; DLBCLO, diffuse large B-cell lymphoma, other; EBER, Epstein Barr virus-encoded RNA; EBV, Epstein Barr virus; EMA, epithelial membrane antigen; EORTC, European Organization for Research and Treatment of Cancer; FCCL, follicle centre cell lymphoma; Fli-1, Friend leukaemia virus integration-1; ICC, immunocytochemistry; IL, interleukin; LMP, latent membrane protein; LP, lupus profundus; LyP, lymphomatoid papulosis; MF, mycosis fungoides; MZL, marginal zone lymphoma; NK, natural killer; PLEVA, pityriasis lichenoides et varioliformis acuta; SPTCL, subcutaneous panniculitis-like T-cell lymphoma; SS, Sezary syndrome; TCL-1, T-cell leukaemia lymphoma-1; TCR, T-cell receptor; TIA-1, T-cell intracellular antigen-1; WHO, World Health Organization Introduction The World Health Organization European Organization for Research and Treatment of Cancer Consensus (WHO EORTC) classification of cutaneous lymphomas, 2005, 1 stressed the importance of considering primary cutaneous lymphoproliferative diseases as distinct from their more usual nodal counterparts, and the critical roles of clinical, histological and immunocytochemical Address for correspondence: A Robson, Department of Dermatopathology, 2nd floor, south wing, block 7, St John s Institute of Dermatology, St Thomas Hospital, Lambeth Palace Road, London, SE1 7EH, UK. alistair.robson@gstt.nhs.uk appraisal for correct diagnosis. Primary cutaneous lymphoma is not a disease but a group of quite distinct conditions that vary considerably in prognosis and preferred treatment regimens. Immunocytochemistry (ICC) may play one of two not mutually exclusive roles in the evaluation of cutaneous lymphoid infiltrates: the assessment of the likely neoplastic nature of such an infiltrate, and characterizing the specific lymphoma. Since the purpose of this review is a critical analysis of ICC in the evaluation and classification of lymphoproliferative disease, to prevent tedious repetition the importance of careful clinical examination and histological Ó 2010 The Author. Journal compilation Ó 2010 Blackwell Publishing Limited.
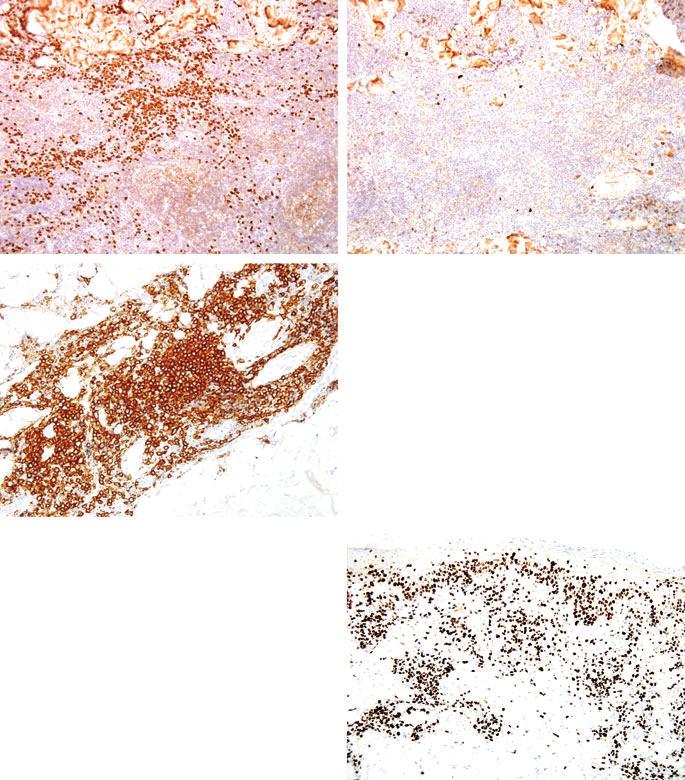
2 72 A Robson evaluation in all cases and that ICC is an adjunct to diagnosis, not an inviolate proof will be accepted as axiomatic. Although, by the time of publication, the Consensus classification will have been incorporated into a single WHO classification for all lymphomas, this cutaneous schema imparts the structure of this review of ICC in cutaneous lymphoid infiltrates, with particular attention to problems that confront dermatopathologists in their practice, and the solutions or otherwise that ICC can offer. Mycosis fungoides Mycosis fungoides (MF) is the most common cutaneous lymphoma, and is characterized by patches, plaques and tumours. The histopathology of these different stages poses distinct problems for the reporting pathologist. Early lesions of MF may have a psoriasiform, lichenoid or even interstitial pattern. There is often a degree of spongiosis, usually very limited, occasionally marked. Cytological atypia and Pautrier microabscesses are seldom conspicuous in the early stages of disease, becoming more evident with disease progression. There is often a dermal lymphocytic infiltrate, but in early disease this is usually dominated by reactive inflammatory cells. Thus, the differential diagnosis may include spongiotic dermatitis (most commonly eczema) and lichenoid dermatoses. ICC is often employed in an attempt to distinguish between a neoplastic and inflammatory lymphocytic infiltrate. The classical immunophenotype of MF is that of a CD4+ memory (CD45RO+) T cell. Unfortunately, the vast majority of dermatoses share this phenotype and, accordingly, ICC may contribute little to this problematic distinction. Both Ki67 and CD30 tend not to be prevalent in the early stages, with rare exceptions. 2 A variety of studies have attempted quantification of CD4+ lymphocytes as a fraction of the CD3+ T-cell population, or in terms of a ratio to the CD8+ infiltrate, to facilitate differentiating MF from dermatoses. Ortonne et al. 3 reported the mean CD8:CD3 was significantly lower in MF in comparison with controls (deliberately avoiding assessing CD4+ cells that inevitably would include the histiocyte population). Other groups have not found the CD8+ fraction of the T-cell population to differ significantly between cases of MF, non-mf and cases of uncertain diagnosis. 4 Studies have suggested that a CD4:CD8 >2 is specific for MF, and that such a ratio is found in 65% of cases. 5 Harvell et al. 6 performed a detailed analysis of lymphocyte subsets in MF and assorted dermatoses. The CD4:CD8 varied from 1 to 6, with values of 1.5 for spongiotic dermatoses, 2.4 in lichen planus, 2.1 in psoriasis, one in lichen sclerosus, and 1.5 in lupus erythematosus. None had greater numbers of CD8+ cells in comparison with CD4+ lymphocytes. Recognizing that, certainly in early MF, most of the neoplastic lymphocytes will be intraepidermal, they then analysed this population in isolation; for spongiotic dermatoses the CD4:CD8 ratio was two, lichen planus 2.1, lichen sclerosus and psoriasis 0.1 in comparison with 6.2 for MF. In practice, even semiquantification of lymphocyte subsets or CD4:CD8 ratios are unlikely to be routinely used; neither are they likely to be sufficiently robust measurements for precise diagnosis. Furthermore, in early MF there may be a CD8+ inflammatory response to the CD4+ neoplastic cells, 7 and deciding which represents the neoplastic population can be impossible. Nevertheless, a few considerations can be practically useful. Actinic reticuloid usually has a predominant CD8+ immunophenotype. So, too, do human immunodeficiency virus dermatitis, 8 pityriasis lichenoides et varioloformis acuta; and, as the results of Harvell s study and others confirm, lichen sclerosus and psoriasis typically have a high proportion of intraepidermal CD8+ lymphocytes. These latter two dermatoses can particularly be morphological mimics of MF. Additional dermatoses that may have substantial populations of CD8+ T cells include lupus erythematosus and other connective tissue diseases. Of more use is the observation of T-cell-associated antigen loss. T-cell-associated antigens (CD2, CD5 and CD7) are usually retained by neoplastic cells in the early stages, perhaps even more so with interstitial forms of MF. 144 Whilst an uncommon finding in early disease, when present it is helpful. The most frequently downregulated antigen is CD7, 2,9 closely followed by CD5. Indeed, antigen loss may occur even in very sparse infiltrates (Figure 1A,B). That inflammatory diseasesfrequently have apparent loss of CD7 expression 10 (and the author has seen at least one case of lichen sclerosus in which the lymphocytes were both CD7) and CD5)) serves to emphasize that this mode of evaluation is not without caveats (Figure 1C E). The evaluation of CD2, CD3, CD4, CD5, CD7, CD8 and CD79a is a reasonable baseline panel for assessing possible early MF. Biopsy specimens from a plaque or tumour of MF are more readily established as neoplastic; there may be obvious Pautrier microabscesses, Indian-filing and cytological atypia, but also dermal involvement by the neoplastic cells. One confounding issue can be the mistaking of Langerhans cell hyperplasia for Pautrier microabscesses. Langerhans cells can express CD4, an observation that may reinforce the error unless confirmatory CD3 and or CD1a are also assessed (Figure 2).
 the loss of T-cell-associated antigens, such as CD2 (B),")
 and CD5 (D) by this case of lichen sclerosus (E) serves as a cautionary caveat.")


3 Immunocytochemistry, cutaneous lymphoma 73 A B C D E Figure 1. Even in a sparse neoplastic infiltrate (A) the loss of T-cell-associated antigens, such as CD2 (B), can be a useful diagnostic clue. The loss of CD7 (C) and CD5 (D) by this case of lichen sclerosus (E) serves as a cautionary caveat. In the later course of MF epidermotropism may be lost, and there is usually obvious atypia; the diagnostic challenge is to categorize the lymphoma. In this respect, the CD4+ CD45RO+ phenotype is helpful, but is by no means specific. Much has been vaunted of the value of CD30 expression with disease progression. It should be clarified that tumour MF has a clinical, not a histological definition, but transformation is a histological judgement predicated on cytology; the two are not synonymous, and neither requires CD30

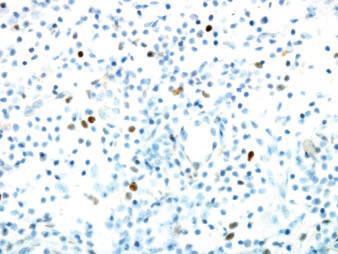
4 74 A Robson Figure 2. Langerhans cell hyperplasia may be confused with Pautrier microabscesses; expression of CD1a can help identify the Langerhans cells. expression. Nevertheless, CD30 positivity in the majority of the neoplastic population is most frequently observed in the later stages of disease, either plaque or, more often, tumour phase. In the author s experience it is less common than widely credited. A potential pitfall is mistaking dense nodules of histiocytes for transformed MF; corroborative CD3 and or CD68 confirm the nature of such a CD4+ population. Despite the CD4+ T-cell lineage of MF, in the later stages the tumour cells not uncommonly express cytotoxic markers, e.g. T-cell intracellular antigen-1 (TIA-1) and granzyme B. 11 With disease progression there is greater expression of Ki67 12 and increasing likelihood of T-cell antigen loss. 13,14 Quick et al. 15 reported an association between increased Friend leukaemia virus integration-1 (Fli-1) expression and progression to tumour stage MF, observing nuclear Fli-1 in lymphocytes in all tumour lesions and 50% of plaques but only 33% at the patch stage. A number of variant immunophenotypes are known to occur in MF, albeit rarely. The most common of these is CD8+ MF, which can be observed in classical forms of disease, but appears to be particularly prevalent in juvenile-onset and or hypopigmented cases Wain et al. 20 documented that 63% of juvenile-onset MF had a CD4+ phenotype, 38% were either CD8+ or CD8) and TIA-1+. Eight of these patients had hypopigmented MF, and 4 7 (57%) of these were CD8+, with one having a CD4 8) CD56+ TIA-1+ profile. Hence, 5 7 had a cytotoxic phenotype. A null phenotype (CD4) CD8)), although not uncommon in advanced disease, 13,14 can be seen in the early patch stage. Hodak et al. reported 18 examples of CD4) CD8) double-negative MF. They defined the cases according to <10% of the CD3+ intraepidermal infiltrate expressing either CD4 or CD8. Almost all (n = 17) were also CD7), but retained CD45RO+. Only eight of 16 tested expressed b-f1. 2 Although double-negative lymphocytes with functionally competent ab T-cell receptors (TCR) have been identified as a lymphocyte subpopulation, 21 the expression of TIA-1 (11 cases) or CD56 (two examples) in this cohort suggested a cytotoxic phenotype in the majority. Interestingly, there appeared to be a greater proportion of unusual clinical phenotypes in the group, including hypopigmented, ichthyosiform and purpuric forms. Cases of MF derived from T cells of the cd rather than ab subclass are described but exceptional indeed. 2,22 Likewise, double CD4+ CD8+ is very rare, and should prompt a consideration of T-cell prolymphocytic leukaemia. Finally, there are certainly cases of subset infidelity, e.g. CD4+ MF recurring or progressing, sometimes after therapy, including bone marrow transplantation, as CD8+ disease, or double-negative MF switching to CD8+. 2 The crucial point is the scant evidence that variant phenotypes have any bearing on the prognosis of MF, 13,14,23,49 underscoring the critical importance of an accurate clinical diagnosis. Erythroderma Patients presenting with clinical erythroderma can pose a challenging problem. Most commonly attributable to eczema, psoriasis or drug-related cause, T-cell lymphoma accounts for <5% of cases. Establishing an erythrodermic infiltrate as neoplastic usually relies on morphology. Loss of CD7 expression does not reliably discriminate between neoplastic and benign erythroderma, 24,25 loss of CD2, CD3 and or CD5 is more specific, but of low sensitivity. 24 Erythrodermic MF and Sezary syndrome (SS) are often histologically indistinguishable, and largely have the same immunoprofile, CD4+ CD45RO+. 17,26 T-cell antigen loss is variable, although CD7 is possibly more often retained in SS in comparison with MF. 27 In addition, the examples of SS with obvious cytological atypia usually have higher Ki67 expression than early MF, and the large cells are often MUM-1+. CD30+ lymphoproliferative disease Encompassing anaplastic large cell lymphoma (ALCL) and lymphomatoid papulosis (LyP) types A, B and C,
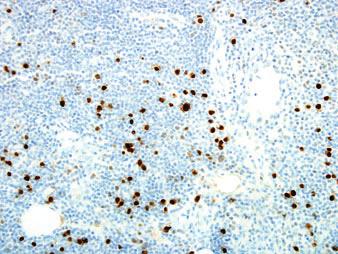
 and primary cutaneous ALCL is facilitated with epithelial membrane antigen (EMA) and ALK-1.")

 systemic ALCL in comparison with cutaneous disease.")
. 29 31 LyP types A and C have the same immunoprofile as ALCL, i.e. CD4+ CD30+ TIA-1+ granzyme B+ and variable loss of CD2, CD3 or CD5.")
5 Immunocytochemistry, cutaneous lymphoma 75 the expression of CD30 by the atypical cells provides the diagnostic criterion (Figure 3A). The distinction between metastatic nodal ( systemic ) and primary cutaneous ALCL is facilitated with epithelial membrane antigen (EMA) and ALK-1. Primary cutaneous ALCL may be EMA+ but almost always ALK-1). 143 In the author s experience, the majority of the handful of examples of putative ALK-1+ primary cutaneous disease have demonstrated convincing cytoplasmic ALK positivity, with or without nuclear expression (Figure 3B). These patterns of reactivity have been associated with variant translocations other than t(2;5) leading to overexpression of the ALK protein. Nuclear survivin may be more commonly expressed by ALK-1) systemic ALCL in comparison with cutaneous disease. 28 Most examples of cutaneous ALCL have the usual CD4+ CD45RO+ T-cell phenotype, are commonly CD25+, with variable antigen loss, 29 CD15 is negative in the large atypical cells. Cytotoxic proteins are commonly positive TIA-1, granzyme B and perforin (Figure 3C) LyP types A and C have the same immunoprofile as ALCL, i.e. CD4+ CD30+ TIA-1+ granzyme B+ and variable loss of CD2, CD3 or CD5. In contrast, infiltrates of LyP type B consist of a population of smaller mononuclear cells, with cerebriform nuclei, resembling the neoplastic population seen in MF, and usually with the same immunoprofile (CD3+ CD2+ CD4+), albeit with variable loss of CD5 and or CD7. 32 Although traditional dogma maintains that these cells do not express CD30, some authors report that both the large A B C D Figure 3. Expression of CD30 is usually strong and diffuse in anaplastic large cell lymphoma (A) with characteristic membranous and cytoplasmic dot positivity. ALK-1 is almost never positive in primary cutaneous disease, and often cytoplasmic when it is expressed (B). Expression of cytotoxic granules, such as T-cell intracellular antigen-1, is common (C). The CD8+ variant of lymphomatoid papulosis (D) is of no consequence other than possibly being more vasculocentric.
6 76 A Robson Table 1. World Health Organization European Organization for Research and Treatment of Cancer classification of cutaneous lymphomas Cutaneous T-cell and NK-cell lymphomas Mycosis fungoides Mycosis fungoides variants and subtypes Folliculotropic mycosis fungoides Pagetoid reticulosis Granulomatous slack skin Sézary syndrome Adult T-cell leukaemia lymphoma Primary cutaneous CD30+ lymphoproliferative disorders Primary cutaneous anaplastic large-cell lymphoma Lymphomatoid papulosis Subcutaneous panniculitis-like T-cell lymphoma Extranodal NK T-cell lymphoma, nasal type Primary cutaneous peripheral T-cell lymphoma, unspecified Primary cutaneous aggressive epidermotropic CD8+ T-cell lymphoma (provisional) Cutaneous cd T-cell lymphoma (provisional) Primary cutaneous CD4+ small medium-sized pleomorphic T-cell lymphoma(provisional) Cutaneous B-cell lymphomas Primary cutaneous marginal zone B-cell lymphoma Primary cutaneous follicle centre lymphoma Primary cutaneous diffuse large B-cell lymphoma, leg type Primary cutaneous diffuse large B-cell lymphoma, other Intravascular large B-cell lymphoma Precursor haematological neoplasm Plasmacytoid dendritic cell neoplasm (formerly CD4+ CD56+ haematodermic neoplasm and blastic NK-cell lymphoma) NK, natural killer. atypical cells of type A LyP and the cerebriform cells in type B express activation markers, including CD30. In practice, biopsy specimens often have features that overlap LyP types A and B, and in the author s experience even the neoplastic cells of type B may express CD30, a reflection, perhaps, of improved antigen retrieval techniques. As with MF, variant immunophenotypes are well documented. Flann et al. 33 documented three cases of CD56+ LyP. Two were type A, and one type B. All had a TIA-1+ granzyme B+ CD8+ profile. Shabrawi-Caelen et al. 34 reported a surprisingly high prevalence of double-negative cases; 25% of type A LyP failed to express CD4 and CD8. They also noted double positivity (CD4+ CD8+) in one of 16 cases. In their hands, half of type B LyPs were double negative, and one expressed CD56. Of three cases of type C disease, one each was CD4+, CD8+ and double positive, while three of six labelled with CD56+. These observations may partly reflect a bias from referral pattern. Such variants probably have no clinical significance, although CD8+ variants may be more vasculo-destructive, 35 (personal observation) (Figure 3D). Various attempts to use immunohistochemistry to distinguish between LyP type C and ALCL have had little success, with most finding blurred quantifiable differences between the groups rather than clear evidence of lineage-specific markers. Thus, fascin expression was observed significantly less in LyP than in ALCL and, interestingly, patients with fascin-positive cases of LyP had a 4.3 odds ratio of subsequently developing lymphoma in comparison with fascin-negative cases. 36 Bax and CD44 are expressed by all forms of cutaneous CD30+ lymphoproliferative disease. 37,38 Similarly, MUM-1, the post-germinal centre activation marker, is expressed by activated large cells in both LyP and ALCL and, in fact, SS and transformed MF. Despite minor differences, these conditions could not be resolved with this marker. It is important to note that biopsy specimens from various inflammatory conditions, e.g. scabies or herpes, may have a significant population of CD30+ cells, an antigen expressed on activated T and B cells. 39,40 In such inflammatory conditions, however, the CD30+ population never forms a majority of the infiltrate, or gather in dense cohesive clusters. Extranodal natural killer T-cell lymphoma Primary cutaneous variants of this lymphoma are rare, although the limited cited cases suggest it might carry a better prognosis when compared with other sites. 142 The neoplastic cells display CD3 cytoplasmic expression but are negative for surface CD3. It should be noted that natural killer (NK) cells do express CD2 and CD7, and these are commonly positive; similarly, NK cells may be CD45RO+ and CD43+ and, therefore, relying
 infection latent membrane protein (LMP) expression by ICC and or Epstein Barr virus-encoded RNA (EBER) in situ hybridization and a cytotoxic")

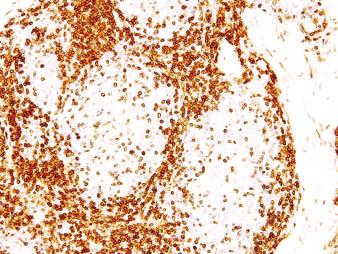
7 Immunocytochemistry, cutaneous lymphoma 77 on this set of markers as indicative of a T-cell lineage may be misleading. 42 Demonstrable evidence of Epstein Barr virus (EBV) infection latent membrane protein (LMP) expression by ICC and or Epstein Barr virus-encoded RNA (EBER) in situ hybridization and a cytotoxic phenotype, viz. CD56+ TIA-1+ granzyme B+ perforin+, are defining features, although the EBV association with cutaneous disease is weaker than the nasal counterpart. It has been suggested that CD30 expression by the neoplastic cells may confer a better prognosis, perhaps through increased p21 expression and subsequent apoptosis. 41,43 Human T lymphotropic virus-1-associated lymphoma Adult T-cell leukaemia lymphoma (ATL) may present an identical histology to MF. The T-cell phenotype is usually CD3+ CD4+ and CD45RO+. Most cases are CD7) CD8) CD20). CD30 may be expressed, and possibly portend a better prognosis. 44 The expression of CD25, a cytokine-stimulated activation marker, is a helpful diagnostic indicator; almost all cases are strongly positive. However, a sizeable proportion of MF cases also express CD25, including CD8+ cases. 30 Indeed, high expression of CD25 in MF has been correlated positively with a therapeutic response to Ontak, an anti-cd25 chemotherapeutic agent. 138 Nevertheless, diffuse and strong CD25 positivity in the vast majority of the neoplastic cells is quite uncommon in MF and ALCL, 45 but is the frequent pattern observed in ATL (Figure 4A,B). Interestingly, there is evidence that CD25 expression might be site dependent. 46 Subcutaneous panniculitis-like T-cell lymphoma Subcutaneous panniculitis-like T-cell lymphoma (SPTCL) is, now by definition, a neoplasm of cytotoxic T cells of the ab receptor class. Thus, the neoplastic cells, typically confined to the subcutis, are CD8+ with variable T-cell-associated antigen loss, TIA-1+, granzyme B+, perforin+ and b-f1+. A common diagnostic difficulty posed is distinguishing between lobular panniculitis, in particular lupus profundus (LP), and SPTCL. Whilst cases of discoid lupus erythematosus may involve the panniculus, the epidermal and dermal features usually allow a confident diagnosis. LP, however, may be confined to the subcutis, have a dense infiltrate, display foci of necrosis and certainly display cytologically atypical lymphocytes. Aside from careful attention to histological nuances, the monomorphic A B Figure 4. It is not uncommon for mycosis fungoides to be CD25+ (A), although seldom as diffuse and strong as is usually seen in adult T-cell leukaemia lymphoma (B). immunoprofile of SPTCL helpfully contrasts with the polymorphic infiltrate in LP. Thus, in LP plasma cells are observed in 91% of cases; lymphoid follicles in 45%, and both CD4+ and CD8+ T cells and B cells. It is not uncommon to find admixed CD56+ and or TIA-1+ cells, 47 indeed, a study of dermatoses found LE to have the highest proportion of CD56+ cells, although never more than 9% of the infiltrate. 6 One useful feature of ICC is in highlighting the adipocyte rimming by T cells. In addition, Ki67 demonstrates a high proliferative fraction almost 100% in the tumour cells rimming the fat spaces, significantly contrasting with a true panniculitis of any form (Figure 5A D). Peripheral T-cell lymphoma not otherwise specified Despite the implicit admission that this group is an undefined farrago of conditions, included are at least
, and have a high proliferative fraction with MIB-1 (C).")

 lymphoma denotes the centrality of CD8 expression in making this diagnosis, although this observation alone is not specific.")
 to memory (CD45RO+) T cells there is up-regulation of the adhesion molecule, CD2, and therefore a reciprocal relationship between these")
8 78 A Robson A B C D Figure 5. By definition, the cells of subcutaneous panniculitis-like T-cell lymphoma (SPTCL) are CD8+ (A), which highlights the adipocyte rimming by neoplastic cells. These usually express cytotoxic markers, e.g. granzyme B (B), and have a high proliferative fraction with MIB-1 (C). Inflammatory infiltrates, such as seen in lupus erythematosus, may have a CD8+ population but do not show the same distribution as SPTCL (D). three rare, probably distinct lymphomas that have yet to gather enough data to warrant a discrete entry in the taxonomy. In most cases the neoplastic nature of the infiltrate is usually clear on the routine sections; it is the categorization of the disease that may be problematic. Aggressive epidermotropic CD8+ ( Berti ) lymphoma denotes the centrality of CD8 expression in making this diagnosis, although this observation alone is not specific. However, many cases have a particular ICC profile; thus, a substantial proportion have a CD2) CD5) CD45RA+ CD45RO) b-f1+ phenotype 48 (Figure 6A D). In the physiological transition from naive (CD45RA+) to memory (CD45RO+) T cells there is up-regulation of the adhesion molecule, CD2, and therefore a reciprocal relationship between these immunomarkers may be expected. Although neoplastic cells in MF are typically memory T cells, in one series approximately 9% of CD4+ MF cases had a CD45RA+ phenotype. In the EORTC collection of examples of CD8+ MF, five of 23 labelled with CD45RA. 49 The markedly pagetoid pattern of infiltration by the neoplastic T cells in Berti s lymphoma is associated with a high proliferative fraction at least 50% of malignant cells Ki67+ in 13 of 17 of the EORTC series, contrasting with the usually low proliferative fraction in epidermotropic (i.e. early ) MF. Interestingly, while there are some clinical and histological similarities to pityriasis lichenoides et varioliformis acuta (PLEVA), a CD8+ dermatosis, the latter has a CD45RO+ rather than CD45RA signature. 50,51 There has been reported a histologically high-grade, although clinically indolent, CD8+ lymphoma with a curious propensity for the ear, less commonly arising

9 Immunocytochemistry, cutaneous lymphoma 79 A B C D Figure 6. Berti s lymphoma typically has a CD8+ (A) CD45RA+ (B) CD2) (C) phenotype with a high intraepidermal proliferative fraction (D). on the nose. Apart from the diffuse and strong CD8 expression by the lymphoblast-like cells, there is a characteristic minority CD20+ population, expression of cytotoxic markers and a low proliferative fraction with Ki67, this latter feature seemingly at odds with the readily observed mitotic figures It is worth recalling that cytotoxic lymphocytes include three cell types: CD8+ cytotoxic T cells, NK cells (a subset of which are CD8+) and CD4+ cytotoxic T cells. 55,56 Of the effector molecules, perforin and granzyme are detectable only in activated cells, while TIA-1 is constitutively expressed. In a series of nodal CD8+ lymphomas granzyme B was expressed by only 2 13 cases, suggesting well-developed cytotoxic granules are not a feature of most peripheral CD8+ lymphomas, in comparison with fully mature cytotoxic cells in inflammatory conditions. 57 Notably, most dermatoses contain a population of TIA-1+ lymphoid cells, a marker that also labels mast cells, neutrophils and eosinophils. 6,58 Cutaneous cd lymphoma. (In the 2008 WHO classification, cutaneous cd lymphoma will be accepted as a definite discrete entity.) Derived from T cells of the cd TCR, the characteristic phenotype of these cells enables a correct diagnosis in an infiltrate that can involve epidermis, dermis and or subcutis. The cells have a CD56+ CD4) CD8) and b-f1) profile, and usually CD5). In rare cases there may be CD56) tumours. TIA-1, granzyme and perforin are usually expressed in contrast to the hepatosplenic variant Furthermore, there is a small minority circulating population of CD8+ cd T cells, and cases of CD8+ cd lymphoma are theoretically possible. The utility of CD56, neural adhesion protein (N-CAM), as a marker for NK cells, or cd lymphoma, deserves a note of caution. Interleukin (IL)-2 and intereron-gamma increase CD56 expression on both CD4+ and CD8+ lymphocytes. 140 Both CD56 expression and a CD4) CD8) phenotype are well recognized in MF, lymphomatoid papulosis and anaplastic lymphoma. 2,62 66 The absence of demonstrable
10 80 A Robson b-f1 expression cannot be simply assumed to indicate a cd phenotype; indeed, the most common explanation for b-f1 negativity is simply loss of antigen expression. A number of studies have been written detailing CD56+ lymphoma implying a single immunophenotypic marker defines a disease. Unsurprisingly, such cases display a range of features. For example, Gniadecki et al. 67 identified three types of CD56+ lymphoma in the skin; blastic, nasal type NK T and SPTCL. Harvell et al. 6 point out that all inflammatory dermatoses they investigated contained a CD56+ population, which in one case of PLEVA had led to a misdiagnosis of NK T-cell lymphoma. Nevertheless, the demonstration of a classical cd immunoprofile is of import, usually predicting a very aggressive clinical course. In Gniadecki s series, median survival was 14 months. Toro et al. 68 analysed 104 biopsy specimens to assess the prognostic value of TCRd1 in primary cutaneous lymphomas; TCR-d1 was considered positive if >80% of cells had membrane expression. There was a statistically significant survival difference between ab and cd. Such findings underscore the inclusion of subcutaneous examples of cd into this disease category rather than SPTCL, a taxonomic shuffle convincingly supported by a consensus EORTC report. 69 In Toro s series, subcutaneous involvement had a worse prognosis in comparison with diseases with epidermal dermal disease, an observation that might reflect the included cases of MF and re-emphasizing the need to consider the clinical diagnosis together with immunophenotype. It is likely that immunocytochemistry has deciphered many cases hitherto diagnosed as Ketron Goodman disease (disseminated pagetoid reticulosis). Originally described in 1931, the report understandably reflected a primarily morphological description of a widespread cutaneous disease with a poor prognosis. Morphologically similar reported cases since the advent of ICC have often detailed either a CD4) CD8) 70,71 or a CD4) CD8+ phenotype. The former almost certainly represents cd and the latter Berti s lymphomas. Undoubtedly, not all cases are so readily accommodated as the reports from Shiozawa et al. and Pagnanelli et al. illustrate, in which they describe an aggressive fatal case of CD4) CD8) CD56) granzyme B+ TIA-1+ b-f1+ lymphoma. 70,72 Small medium cell pleomorphic CD4+ T-cell lymphoma. Perhaps the most controversial of the not otherwise specified category, ICC simply records the predominant population of CD4+ T cells, with variable antigen loss. A common feature of this disease is the background population of B lymphocytes and (polyclonal) plasma cells, and macrophages. ICC therefore demonstrates CD20 and CD68 liberally labelling cells within the infiltrate. MIB-1 typically reveals a low moderate proliferative fraction. 73,74 The most common problem in evaluating this disease is distinguishing between a reactive infiltrate, in which there is also a polymorphous population, and a low proliferative index. At least one putative case of small-medium cell pleomorphic CD4+ T-cell lymphoma with a variant CD8+ phenotype has been reported. B-cell lymphomas With the exception of lymphocytoma cutis, a substantial infiltrate of B cells is a rare feature of reactive processes. Such infiltrates are amongst the most difficult to characterize with confidence. The initial observation of a heavy B-cell population, even of small cells with little or insignificant atypia, is sufficient grounds for suspecting a B-cell lymphoma. Having observed a heavy B-cell population within an infiltrate, the architecture of the infiltrate informs the possible diagnoses, and the interpretation of the ICC. Any B-cell infiltrate may be diffuse or nodular, each with or without true lymphoid follicles. The analysis of such an infiltrate may, therefore, be considered along these two threads. diffuse b-cell infiltrate The principal primary cutaneous B-cell lymphomas with a diffuse architecture include follicle centre cell lymphoma (FCCL), diffuse large B-cell lymphoma, leg type (DLBCLL), and diffuse large B-cell lymphoma, other (DLBCLO). FCCL is the source of much controversy, with adherents of the traditional WHO classification maintaining that diffuse examples of these are best designated as diffuse large B-cell lymphomas (DLBCL). FCCL has a variable cytology; not all consist of large cells, particularly in the early papular lesions. The identification of the B cells as of germinal centre origin is crucial; almost all cases are CD20+ CD79a+ Bcl-6+ Bcl-2), and lack t(14;18) (Figure 7A,B). MUM-1 often labels a minority of cells scattered amongst the infiltrate. The growth fraction elicited with Ki67 is variable. In the absence of a nodular component and or obvious follicular pattern, CD21 expression is unusual, although exceptionally there may be diffuse and strong positivity. The presence of a significant Bcl- 2+ T-cell population may hamper interpretation; sometimes combined immunolabelling may be helpful to demonstrate that the Bcl-6+ germinal centre cells are Bcl-2) (Figure 7C). There is good evidence that
 Bcl-6+ (B) but Bcl-2- phenotype; sometimes this can be hard to discern and combined immunolabelling using two chromogens for Bcl-2 (red) and")

11 Immunocytochemistry, cutaneous lymphoma 81 A B C Figure 7. Diffuse follicle centre cell lymphoma has a CD20+ (A) Bcl-6+ (B) but Bcl-2- phenotype; sometimes this can be hard to discern and combined immunolabelling using two chromogens for Bcl-2 (red) and Bcl-6 (brown) may be useful (C). FCCL and DLBCLL are different entities. Certainly, some studies have failed to support this division. 80 For example, of 32 cases no significant differences were identified in morphology, Bcl-2 or clinical outcome. 81 However, many reinforce the Consensus view. Gene expression profiling suggests two groups within the DLBCL category, identifiable by their ICC signature 82 : germinal centre B cells that label Bcl-6+ CD10+ (FCCL) and other activated post-germinal B cells Bcl-2+ MUM-1+ (DLBCLL). Those patients with a gene expression profile of germinal centre cells have a better prognosis when compared with those with activated B cells; 83 furthermore, leg tumours are more likely to have the activated phenotype. Of the 14 patients analysed in this series, two died, both with leg disease. These findings are in accord with numerous others: Bcl-2, Bcl-6 and MUM-1 have been correlated with disease-specific survival Thus, a diffuse large cell infiltrate with an ICC profile of Bcl-2+ MUM-1+ CD20+, usually diffuse and strong, and lacking a follicular dendritic network is most commonly seen on the leg, 86,87 but in any locale portends a more aggressive disease, and defines DLBCLL. Array-based analysis adds further support for considering DLBCLL as distinct from FCCL. 88 There is a high proliferative fraction, often >90%. However, there is variable Bcl-6 and CD10 expression, suggesting a germinal centre derivation in a subset ,141 Currently, DLBCLO denotes cases with a diffuse infiltrate of large B cells that do not readily fit into these categories. Examples include cases with limited MUM-1 and Bcl-6 expression. nodular/follicular b-cell infiltrates Expression of CD21 and or CD23, labelling the follicular dendritic cell network, establishes whether true lymphoid follicles are present within an infiltrate; these may not be obvious on routine sections. Benign lymphoid follicles may be seen in cutaneous lymphoid hyperplasia (CLH) (syn. lymphocytoma cutis, Spiegler Fendt sarcoid), marginal zone lymphoma (MZL), and in some dermatoses, e.g. LP. In each of these cases the germinal centres have a Bcl-6+ Bcl-2) CD10+ CD10) phenotype and a high proliferative index, i.e. the typical immunophenotype of reactive germinal centres. 86,88,89 It is the interfollicular infiltrate that is neoplastic in MZL, and diffusely Bcl-2+ but Bcl-6) and CD10); aberrant expression of CD43 is helpful. The histological distinction between CLH and MZL may be one of the most challenging problems in dermatopathology. CLH has a variety of recognized antecedents, Borrelia burgdorferi infection being the best characterized, but also vaccination sites, arthropod bites, tattoo sites, and gold therapy. Colli et al. 90 investigated Borrelia-associated lymphocytoma cutis; all had a follicular pattern
12 82 A Robson with CD10+ Bcl-6+ germinal centres and a Ki67 index >90%. Findings that may cause diagnostic difficulty included the observation of interfollicular CD10+ and Bcl-6+ cells in 2 15 and 5 17 cases, respectively, both being features usually associated with malignancy; similar observations may be seen with MUM-1 86,89 (Figure 8A,B) The interfollicular Ki67+ growth fraction is usually low, however. In 20% of biopsy specimens the follicles were confluent and mimicked DLBCL, although all had numerous tingible-body macrophages and, as in the clearly follicular examples, had a CD20+ Bcl-6+ CD10+ profile with CD21+ follicular dendritic cells. The demonstration of light-chain restriction by the lymphoid cells provides proof of clonality and is the ICC arbiter between MZL and LC. This technique is particularly difficult on skin specimens unless there is marked plasmacytoid differentiation. Since j chain is expressed by approximately twice as many B cells as k light chain, there are various thresholds for accepting proof of clonality. Thus, ratios of 3:1 k:j- or 5:1 10:1 j:kexpressing B cells have been touted as evidence of lightchain restriction. The reproducibility of assessing ratios makes this strict approach problematic but, generally, a striking dominance of either k or j expression is grounds for suggesting neoplasia (Figure 8C,D). A minority of FCCL has a follicular architecture, and it is these examples that many authors consider true follicular lymphomas akin to the more common nodal disease. Unfortunately, in most of these cases, whilst the follicles are neoplastic, they are, like the diffuse examples, usually Bcl-6+ Bcl-2), 78,91,92 with a low proliferative fraction. 89 Rare Bcl-2+ cases do occur, although in many instances such a profile denotes secondary cutaneous spread from nodal follicular lymphoma with the characteristic t(14;18). In a series of 24 FCCL, Hoefnagel et al. 86 found Bcl-6+ in CD and Bcl ; in comparison, 3 3 secondary deposits from nodal follicular lymphomas had a Bcl-6+ CD10+ Bcl-2+ profile. This claim that FCCL is distinct from nodal follicular lymphoma is controversial but, although there are studies to support both protagonists, a majority indicate most FCCL to be a CD10), Bcl-2)tumour that lacks t(14;18) 75 78,89,91,93 98 (Figure 8E,F). Lawnicki et al. contend that if cases are chosen for a true follicular network ( a required feature for the diagnosis), then the ICC profile (Bcl-6+ Bcl-2+ CD10+) equates to the more common nodal follicular lymphoma, and such cases are certainly reported This may have some credence, but perhaps misses the point, that most examples of FCCL are diffuse. Lawnicki comments that, given the inclusion of diffuse examples, it is no wonder that there is a lower prevalence of Bcl-2 and CD10 expression, since this is a feature of DLBCL, and these tumours are more properly so designated according to the WHO classification. The prevalence of t(14;18) varies from 0% to 41%. 91,95,96,99,100,102,103,106 In most studies of FCCL no threshold of determining whether a germinal centre is Bcl-2+ or Bcl-2) is given, a finding that shows considerable variability in the literature 91,102 Hoefnagel et al. 86 designated Bcl-2+ if >25% of the constituent follicle cells were positive. Furthermore, Bcl-2 antigen-retrieval methods are not always reported. While it is true, in the author s experience, that strikingly follicular examples of FCCL with a CD21+ follicular dendritic network are more likely to be Bcl-2+ CD10+ and, indeed, have systemic disease on staging, this is not invariable (Figure 8G). Mixed B-cell and T-cell lymphoid populations Even in clear-cut B-cell lymphoma there is usually a heavy T-cell infiltrate, sometimes more numerous than the neoplastic population. Baldassano et al. 107 suggest that a B:T cell ration >3 favours MZL rather than CLH, but many MZL have a heavy T-cell background. Likewise, in many T-cell lymphomas there is often an admixed B-cell population, albeit seldom equal to the neoplastic fraction. Thus, biopsy specimens from reactive conditions, T-cell or B-cell lymphoma, may present a similarly dense lymphoid population, which on initial ICC analysis reveals both lymphocytic subsets. In the absence of clear cytological atypia it is difficult, even unwise, to make a confident diagnosis of lymphoma. T-cell-rich B-cell lymphoma is afforded a separate category in the WHO classification of nodal diseases. Currently, this is not a recognized dermatopathology entity and putative example 108 almost certainly reflect the frequent tendency for cutaneous B-cell lymphomas, particularly MZL and FCCL, to have a heavy inflammatory T-cell population. Rather than Figure 8. Interfollicular Bcl-6+ (A) or MUM-1+ (B) cells are a potential source of confusion, although not uncommon. Light chain restriction is diagnostic; here there is clear j (C) dominance over k (D). The follicular variant of follicle centre cell lymphoma (FCCL) is also CD20+ (E) and Bcl-2) (F); nevertheless, Bcl-2+ cases of primary cutaneous FCCL do occur (G). A high dermal MIB-1 fraction does not usually occur in reactive infiltrates, but there are exceptions (H).

13 Immunocytochemistry, cutaneous lymphoma 83 A B C D E F G H

14 84 A Robson label an infiltrate T-cell-rich B-cell lymphoma, a designation without meaningful prognostic import, it behoves the pathologist to discern the underlying disease and, if this is not possible, to acknowledge this. In such apparently polymorphic infiltrates, Ki67 may be of some use. Inflammatory dermatoses, of any aetiology, do not usually have a sizeable proliferative fraction, although there are exceptions (Figure 8H), and the demonstration of a high Ki67 index is always a suspicious finding for possible neoplasia. Further apparently conflicting results stem from the rare cases of CD20+ T-cell lymphoma. There is a physiological small circulating fraction of T cells that are weakly CD20+ that might account for this rare anomaly, 109,110,139 possibly reflecting activation, 111 and occasionally CD20+ MF can be encountered. Similarly, CD79a may be positive in peripheral T-cell lymphoma, 112 and there is at least one report of coexpression of CD20 and CD79a in T-cell lymphoma. 113 Finally, loss of CD20 expression may be seen as a consequence of rituximab therapy. 114 of post transplantation, acquired immunodeficiency syndrome (AIDS) or immunosuppressive therapy (Table 2). Many are attributable to EBV. Senile EBV-associated B-cell lymphoproliferative disorder is a relatively recently recognized entity. Affecting predominantly the >60 years age group, it is believed that age-related immune impairment allows the proliferation of EBV+ B cells. 115,116 Thus, there is an infiltrate of markedly atypical CD20+ CD79a+ CD30+ cells with demonstration of EBV LMP-1 and EBER using in situ hybridization. In all lymphomas suspected of having an EBV association, EBER in situ hybridization has a much greater sensitivity than LMP-1 and is the investigation of choice (Figure 9A,B). Methotrexate-related lymphoma, in practice, is not so much a discrete disease but the occurrence of a number of lymphomas, most, but not all, EBV- A Immune impairment-related lymphomas Numerous lymphoproliferative disorders arise in the setting of immune impairment, whether in the context Table 2. Cutaneous lymphomas described in the setting of immune impairment EBV+ senile-related lymphoma cd lymphoma Methotrexate-related lymphoma Diffuse large B-cell lymphoma Lymphoplasmacytic infiltrates B Hodgkin s Extranodal NK T-cell lymphoma Peripheral T-cell lymphoma NOS AIDS-related lymphoma Plasmablastic lymphoma MF Sezary syndrome Hodgkin-like lymphoma ALCL EBV, Epstein Barr virus; NK, natural killer; NOS, not otherwise specified; AIDS, acquired immunodeficiency syndrome; MF, mycosis fungoides; ALCL, anaplastic large cell lymphoma. Figure 9. In evaluating potential Epstein Barr virus as a causative factor, in situ hybridization for Epstein Barr virus-encoded RNA (A) is much more sensitive than immunocytochemistry for latent membrane protein (B).

15 Immunocytochemistry, cutaneous lymphoma 85 related, 117 that arise following protracted methotrexate treatment, usually in patients with rheumatoid arthritis. Interestingly, patients with psoriasis under longterm methotrexate therapy have a much lower incidence. 118 The ICC profiles mirror the usual disease except for EBV positivity in the majority. Withdrawal of methotrexate leads to at least partial regression in approximately 60% of cases. 119 Cutaneous presentations of AIDS-related lymphoma tend to fall into two groups: (i) MF Sezary-like, 8,120 and (ii) large-cell CD30+ EBV+ lymphomas. 121 Cutaneous examples of the latter are more likely to have a T-cell phenotype in comparison with the overall B-cell predominance. 121 Plasmablastic lymphoma is often seen in the context of AIDS, usually arising within the oral cavity, but primary cutaneous examples are described, as are cases developing post transplantation 122 and in previously healthy individuals. 123 Human herpes virus 8 and EBV are implicated in this CD79a+ CD138+ CD20) tumour, in which light-chain restriction might be demonstrable. The clinical course varies between self-healing nodules to a fatal outcome. 124 Reports of primary cutaneous post-transplantation EBV+ T-cell ALCL 125,126 underscore the general maxim that, whatever the lymphoma type, if arising in the context of immune suppression EBV should be actively excluded. Plasmacytoid dendritic cell neoplasm This aggressive tumour was formerly known as blastic NK-cell lymphoma and, more recently, CD4+ CD56+ haematodermic neoplasm. 127,128 The infiltrate consists of lymphoblast-like cells, CD4+ CD56+ (Figure 10A,B) but usually negative for other T-cell- A B C D Figure 10. CD4+ (A) and CD56+ (B) are defining features of plasmacytoid dendritic cell neoplasm, some cases of which may express a variety of other antigens, e.g. TdT (C). CD123 (D) is a very useful marker.
16 86 A Robson associated antigens, CD2, CD3, CD5 and CD7. Similarly, CD20, CD79a, CD138, EBV, cytotoxic granules TIA-1, granzyme B and perforin are negative. Whilst in most cases the cells are also negative for leukaemia-associated markers, including myeloperoxidase, lysozyme, CD34 and CD117, there can be focal positivity for some of these, particularly TdT (Figure 10C). 129 Derived from plasmacytoid dendritic cells, expression of CD123 (membranous IL-3 receptor) (Figs) and T-cell leukaemia lymphoma-1 (TCL-1), a cytoplasmic protein that augments cell survival kinase, 130 more specifically characterize the tumour cells (Figure 10D). 129,131,132 Although TCL-1 is negative in most cases of leukaemia cutis, it is commonly positive in T-cell pro-lymphocytic leukaemia associated with t(14;32) 133 and has been found expressed in ALT. 129 There may be expression of CD45RA+ and CD68+, sometimes strong. 134,135 The ICC profile is not always as crisp in practice as suggested in some reports, possibly reflecting individual thresholds for considering a tumour as positive. Thus, examples with focal CD2+ and CD7+ are documented. 129 The author has seen at least one case with focal CD3 expression. The tumour has an uncertain relationship to leukaemia, with marrow and blood involvement common in the later stages, and there are cases that have transformed to a myelomonocytic leukaemia during clinical progression. 136 There is emerging evidence that the ICC profile in this tumour might have therapeutic and prognostic import. Thus, CD303 (BDCA-2) and CD7 expression increases with plasmacytoid dendritic cell maturation, whilst TdT decreases, 137 and it has been suggested that the more mature phenotype, associated with a lower growth fraction, may predict a less chemosensitive tumour. Concluding remarks It is impossible to be comprehensive in discussing such a vast field. Whatever advances and subtle nuances emerge in literature analyses of these largely rare tumours, the time-honoured tenets of basic histopathology practice should never be forgotten. ICC is a critical tool in lymphoid proliferations, but one that requires interpretation within a context. Perhaps less widely appreciated, but at least as important, is the extent to which a dermatological clinical diagnosis can drastically alter the significance of an ICC profile. In approaching the interpretation of ICC in these frequently difficult infiltrates, such wise saws remain pivotal to accurate diagnosis. References 1. Willemze R, Jaffe ES, Burg G et al. WHO-EORTC classification for cutaneous lymphomas. Blood 2005; 105; Hodak E, David M, Maron L et al. CD4 CD8 double-negative epidermotropic cutaneous T-cell lymphoma: an immunohistochemical variant of mycosis fungoides. J. Am. Acad. Dermatol. 2006; 55; Ortonne N, Buyukbabani N, Delfau-Larue MH et al. Value of the CD8-CD3 ratio for the diagnosis of mycosis fungoides. Mod. Pathol. 2003; 16; Bergman R, Faclieru D, Sahar D et al. Immunophenotyping and T-cell receptor gamma gene rearrangement analysis as an adjunct to the histopathologic diagnosis of mycosis fungoides. J. Am. Acad. Dermatol. 1998; 39; Nuckols JD, Shea CR, Horenstein MG et al. Quantitation of intraepidermal T-cell subsets in formalin-fixed, paraffin-embedded tissue helps in the diagnosis of mycosis fungoides. J. Cutan. Pathol. 1999; 26; Harvell JD, Nowfar-Rad M, Sundram U. An immunohistochemical study of CD4, CD8, TIA-1 and CD56 subsets in inflammatory skin disease. J. Cutan. Pathol. 2003; 30; Wood GS, Edinger A, Hoppe RT et al. Mycosis fungoides skin lesions contain CD8+ tumour-infiltrating lymphocytes expressing an activated, MHC-restricted cytotoxic T-lymphocyte phenotype. J. Cutan. Pathol. 1994; 21; Cuitart J, Variakojis D, Kuzel T et al. Cutaneous CD8 T-cell infiltrates in advanced HIV infection. J. Am. Acad. Dermatol. 1999; 41; Ormsby A, Bergfield WF, Tubbs RR et al. Evaluation of a new paraffin-reactive CD7 T-cell deletion marker and a polymerase chain reaction-based T-cell receptor gene rearrangement assay: implications for diagnosis of mycosis fungoides in community practice. J. Am. Acad. Dermatol. 2001; 45; Cerroni L, Kerl H. Diagnostic immunohistology: cutaneous lymphomas and pseudolymphomas. Semin. Cutan. Med. Surg. 1999; 18; Vermeer MH, Geelen FAMJ, Kummer J et al. Expression of cytotoxic proteins by neoplastic T-cells in mycosis fungoides increases with progression from plaque to tumour stage disease. Am. J. Pathol. 1999; 154; Gambichler T, Bischoff S, Bechara FG et al. Expression of proliferation markers and cell cycle regulators in T-cell lymphoproliferative skin disorders. J. Dermatol. Sci. 2008; 49; van der Putte SCJ, Toonstra J, van Wichen DF et al. Aberrant immunophenotypes in mycosis fungoides. Arch. Dermatol. 1988; 124; Ralfkiaer E, Wollf-Sneedorff A, Thomsen K et al. Immunophenotypic studies in cutaneous T-cell lymphoma: clinical implications. Br. J. Dermatol. 1993; 129; Quick CM, Smoller BR, Hiatt KM. Fli-1 expression in mycosis fungoides. J. Cutan. Pathol. 2006; 33; Dummer R, Kamarashev J, Kempf W et al. Junctional CD8+ cutaneous lymphomas with non-aggressive clinical behaviour: a CD8+ variant of mycosis fungoides? Arch. Dermatol. 2002; 138; Kamarashev J, Burg G, Kempf W et al. Comparative analysis of histological and immunohistological features in mycosis fungoides and Sezary syndrome. J. Cutan. Pathol. 1998; 25; Ardigo M, Borroni G, Muscardin L et al. Hypopigmented mycosis fungoides in Caucasian patients: a clinicopathologic study of 7 cases. J. Am. Acad. Dermatol. 2003; 49;
Lymphoma and Pseudolymphoma
 Lymphoma and Pseudolymphoma Laura B. Pincus, MD Co-Director, Cutaneous Lymphoma Clinic Associate Professor Dermatology and Pathology University of California, San Francisco I HAVE NO RELEVANT RELATIONSHIPS
Lymphoma and Pseudolymphoma Laura B. Pincus, MD Co-Director, Cutaneous Lymphoma Clinic Associate Professor Dermatology and Pathology University of California, San Francisco I HAVE NO RELEVANT RELATIONSHIPS
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders
 Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Important Decisions in Dermatopathology: The Clinico- Pathologic Correlation. Dermatopathology Specialists Needed. Changing Trends
 Important Decisions in Dermatopathology: The Clinico- Pathologic Correlation Uma Sundram, MD, PhD Departments of Pathology and Dermatology Stanford University May 29, 2008 Dermatopathology Specialists
Important Decisions in Dermatopathology: The Clinico- Pathologic Correlation Uma Sundram, MD, PhD Departments of Pathology and Dermatology Stanford University May 29, 2008 Dermatopathology Specialists
Michi Shinohara MD Associate Professor University of Washington/Seattle Cancer Care Alliance Dermatology, Dermatopathology
 Michi Shinohara MD Associate Professor University of Washington/Seattle Cancer Care Alliance Dermatology, Dermatopathology Agenda Overview of cutaneous T and B- cell lymphomas Diagnosis, Staging, Prognosis
Michi Shinohara MD Associate Professor University of Washington/Seattle Cancer Care Alliance Dermatology, Dermatopathology Agenda Overview of cutaneous T and B- cell lymphomas Diagnosis, Staging, Prognosis
Immunopathology of Lymphoma
 Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
New Haven, Connecticut
 New Haven, Connecticut Yale University Main Campus Yale mascot: Handsome Dan Cutaneous Lymphomas Tony Subtil, MD, MBA Associate Professor Yale University Cutaneous Lymphomas: 1. Intro 2. CTCL/NK 3. CBCL
New Haven, Connecticut Yale University Main Campus Yale mascot: Handsome Dan Cutaneous Lymphomas Tony Subtil, MD, MBA Associate Professor Yale University Cutaneous Lymphomas: 1. Intro 2. CTCL/NK 3. CBCL
Classification of Cutaneous T cell Lymphomas (CTCLs) Hernani Cualing, MD
 Hernani Cualing, MD") Classification of Cutaneous T cell Lymphomas (CTCLs) Hernani Cualing, MD Pathology and Cell Biology, USF IFLOW, Inc. CTCL, MF, and Sézary syndrome In 1806, mycosis fungoides (MF) was first described 1
Classification of Cutaneous T cell Lymphomas (CTCLs) Hernani Cualing, MD Pathology and Cell Biology, USF IFLOW, Inc. CTCL, MF, and Sézary syndrome In 1806, mycosis fungoides (MF) was first described 1
Review Article. Cutaneous lymphoproliferative disorders. NJ Trendell-Smith
 Hong Kong J. Dermatol. Venereol. (2010) 18, 190-201 Review Article Cutaneous lymphoproliferative disorders NJ Trendell-Smith Cutaneous lymphoproliferative disorders (CLD) include reactive lymphoid hyperplasias,
Hong Kong J. Dermatol. Venereol. (2010) 18, 190-201 Review Article Cutaneous lymphoproliferative disorders NJ Trendell-Smith Cutaneous lymphoproliferative disorders (CLD) include reactive lymphoid hyperplasias,
Lymphocytoma Cutis. Cynthia M. Magro MD. Director of Dermatopathology Weill Medical College of Cornell University New York, New York
 Lymphocytoma Cutis Cynthia M. Magro MD Professor of Pathology Director of Dermatopathology Weill Medical College of Cornell University New York, New York Lymphocytoma Cutis Falls under other designations
Lymphocytoma Cutis Cynthia M. Magro MD Professor of Pathology Director of Dermatopathology Weill Medical College of Cornell University New York, New York Lymphocytoma Cutis Falls under other designations
Hepatic Lymphoma Diagnosis An Algorithmic Approach
 Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Primer of Immunohistochemistry (Leukocytic)
") Primer of Immunohistochemistry (Leukocytic) Paul K. Shitabata, M.D. Dermatopathology Institute Torrance, CA BENIGN LYMPHOID SKIN LESIONS CAPABLE OF SIMULATING LYMPHOMA -Jessner s lymphoid infiltrate -Dermal-subcutaneous
Primer of Immunohistochemistry (Leukocytic) Paul K. Shitabata, M.D. Dermatopathology Institute Torrance, CA BENIGN LYMPHOID SKIN LESIONS CAPABLE OF SIMULATING LYMPHOMA -Jessner s lymphoid infiltrate -Dermal-subcutaneous
Cutaneous Lymphoid Proliferations: A Comprehensive Textbook of Lymphocytic Infiltrates of the Skin
 Cutaneous Lymphoid Proliferations: A Comprehensive Textbook of Lymphocytic Infiltrates of the Skin Magro, Cynthia M., MD ISBN-13: 9780471695981 Table of Contents Chapter One: Introduction to the Classification
Cutaneous Lymphoid Proliferations: A Comprehensive Textbook of Lymphocytic Infiltrates of the Skin Magro, Cynthia M., MD ISBN-13: 9780471695981 Table of Contents Chapter One: Introduction to the Classification
A middle-aged man with self-healing papulonecrotic lesions over the trunk and proximal limbs
 Hong Kong J. Dermatol. Venereol. (2011) 19, 30-34 Case Report A middle-aged man with self-healing papulonecrotic lesions over the trunk and proximal limbs JC Chan, N Trendell-Smith, CK Yeung Lymphomatoid
Hong Kong J. Dermatol. Venereol. (2011) 19, 30-34 Case Report A middle-aged man with self-healing papulonecrotic lesions over the trunk and proximal limbs JC Chan, N Trendell-Smith, CK Yeung Lymphomatoid
Session Summary session 6. Reactive Lymphoproliferations of the skin. Session 6 - case 211
 SH/EAHP Workshop 2011 Los Angeles, California, USA October 27-29, 2011 Session 6 Reactive Lymphoproliferations of the skin Rein Willemze Summary session 6 Atypical T-cell infiltrates (lymphomatoid; pseudo-t-cell
SH/EAHP Workshop 2011 Los Angeles, California, USA October 27-29, 2011 Session 6 Reactive Lymphoproliferations of the skin Rein Willemze Summary session 6 Atypical T-cell infiltrates (lymphomatoid; pseudo-t-cell
Overview of Cutaneous Lymphomas: Diagnosis and Staging. Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology
 Overview of Cutaneous Lymphomas: Diagnosis and Staging Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology Definition of Lymphoma A cancer or malignancy that comes from
Overview of Cutaneous Lymphomas: Diagnosis and Staging Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology Definition of Lymphoma A cancer or malignancy that comes from
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
SH/EAHP Workshop 2011 Los Angeles, California, USA
 SH/EAHP Workshop 2011 Los Angeles, California, USA October 27-29, 2011 Session 3 Non-Mycosis Fungoides CTCL Patty Jansen & Rein Willemze Introduction Submitted: 101 cases + 7 cases group 1: 108 Deactivated
SH/EAHP Workshop 2011 Los Angeles, California, USA October 27-29, 2011 Session 3 Non-Mycosis Fungoides CTCL Patty Jansen & Rein Willemze Introduction Submitted: 101 cases + 7 cases group 1: 108 Deactivated
Disclosures. Advisory Board. Consultant. Investigator. MiRagen, Actelion, Celgene, Therakos. Mindera
 Cutaneous Lymphomas Christiane Querfeld, MD, PhD Director, Cutaneous Lymphoma Program City of Hope ~ How the Experts Treat Hematologic Malignancies Symposium March 10 13, 2017 Disclosures Advisory Board
Cutaneous Lymphomas Christiane Querfeld, MD, PhD Director, Cutaneous Lymphoma Program City of Hope ~ How the Experts Treat Hematologic Malignancies Symposium March 10 13, 2017 Disclosures Advisory Board
Contents. vii. Preface... Acknowledgments... v xiii
 Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
Bone Marrow. Procedures Blood Film Aspirate, Cell Block Trephine Biopsy, Touch Imprint
 Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Non-Hodgkin s Lymphomas Version
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Mycosis Fungoides and Variants
 Mycosis Fungoides and Variants Jennifer Madison McNiff, M.D. Associate Professor, Dermatology and Pathology Yale University School of Medicine Classic mycosis fungoides The most common cutaneous lymphoma
Mycosis Fungoides and Variants Jennifer Madison McNiff, M.D. Associate Professor, Dermatology and Pathology Yale University School of Medicine Classic mycosis fungoides The most common cutaneous lymphoma
Commentary on the 2008 WHO classification of mature T- and NK-cell neoplasms
 J Hematopathol (2009) 2:65 73 DOI 10.1007/s12308-009-0034-z COMMENT Commentary on the 2008 WHO classification of mature T- and NK-cell neoplasms Megan S. Lim & Laurence de Leval & Leticia Quintanilla-Martinez
J Hematopathol (2009) 2:65 73 DOI 10.1007/s12308-009-0034-z COMMENT Commentary on the 2008 WHO classification of mature T- and NK-cell neoplasms Megan S. Lim & Laurence de Leval & Leticia Quintanilla-Martinez
Incidence. Bimodal age incidence 15-40, >55 years Childhood form (0-14) more common in developing countries M:F=1.5:1; in all subtypes except NS
 more common in developing countries M:F=1.5:1; in all subtypes except NS") Hodgkin Lymphoma Hodgkin Lymphoma 30% of all lymphomas Absolute incidence unchanged Arise in lymph node, cervical region Neoplastic tissues usually contain a small number of tumor cells Incidence Bimodal
Hodgkin Lymphoma Hodgkin Lymphoma 30% of all lymphomas Absolute incidence unchanged Arise in lymph node, cervical region Neoplastic tissues usually contain a small number of tumor cells Incidence Bimodal
FOLLICULARITY in LYMPHOMA
 FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
Methotrexate-associated Lymphoproliferative Disorders
 Methotrexate-associated Lymphoproliferative Disorders Definition A lymphoid proliferation or lymphoma in a patient immunosuppressed with methotrexate, typically for treatment of autoimmune disease (rheumatoid
Methotrexate-associated Lymphoproliferative Disorders Definition A lymphoid proliferation or lymphoma in a patient immunosuppressed with methotrexate, typically for treatment of autoimmune disease (rheumatoid
Combinations of morphology codes of haematological malignancies (HM) referring to the same tumour or to a potential transformation
 referring to the same tumour or to a potential transformation") Major subgroups according to the World Health Organisation (WHO) Classification Myeloproliferative neoplasms (MPN) Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB or
Major subgroups according to the World Health Organisation (WHO) Classification Myeloproliferative neoplasms (MPN) Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB or
88-year-old Female with Lymphadenopathy. Faizi Ali, MD
 88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Granulomatous Slack Skin with an unusually aggressive course due to the subsequent development of a CD30-positive Large Cell Lymphoma
 Granulomatous Slack Skin with an unusually aggressive course due to the subsequent development of a CD30-positive Large Cell Lymphoma Alexandra Papoudou-Bai 1, Eleni Kapsali 2, Ioannis Kostas-Agnantis
Granulomatous Slack Skin with an unusually aggressive course due to the subsequent development of a CD30-positive Large Cell Lymphoma Alexandra Papoudou-Bai 1, Eleni Kapsali 2, Ioannis Kostas-Agnantis
Corrigenda. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run
: corrections made in second print run") Corrigenda WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run In addition to corrections of minor typographical errors, corrections
Corrigenda WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues (revised 4th edition): corrections made in second print run In addition to corrections of minor typographical errors, corrections
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Anaplastic Large Cell Lymphoma (of T cell lineage)
") Anaplastic Large Cell Lymphoma (of T cell lineage) Definition T-cell lymphoma comprised of large cells with abundant cytoplasm and pleomorphic, often horseshoe-shaped nuclei CD30+ Most express cytotoxic
Anaplastic Large Cell Lymphoma (of T cell lineage) Definition T-cell lymphoma comprised of large cells with abundant cytoplasm and pleomorphic, often horseshoe-shaped nuclei CD30+ Most express cytotoxic
Malignant Lymphomas Decision Making and Problem Solving
 Malignant Lymphomas Decision Making and Problem Solving Cutaneous T-cell lymphomas (including rare subtypes). Current concepts. II. [haematologica] 2004;89:1372-1388 MARCO PAULLI EMILIO BERTI A B S T R
Malignant Lymphomas Decision Making and Problem Solving Cutaneous T-cell lymphomas (including rare subtypes). Current concepts. II. [haematologica] 2004;89:1372-1388 MARCO PAULLI EMILIO BERTI A B S T R
DETERMINATION OF A LYMPHOID PROCESS
 Chapter 2 Applications of Touch Preparation Cytology to Intraoperative Consultations: Lymph Nodes and Extranodal Tissues for Evaluation of Hematolymphoid Disorders INTRODUCTION As discussed in Chap. 1,
Chapter 2 Applications of Touch Preparation Cytology to Intraoperative Consultations: Lymph Nodes and Extranodal Tissues for Evaluation of Hematolymphoid Disorders INTRODUCTION As discussed in Chap. 1,
Plasma cell myeloma (multiple myeloma)
") Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
CASE 15 Patient: A 41-year-old Thai female Chief Compliant: Generalized papulovesicular rash for 1 month Present Illness: She presented with a 1-week
 CASE 15 Patient: A 41-year-old Thai female Chief Compliant: Generalized papulovesicular rash for 1 month Present Illness: She presented with a 1-week history of the generalized asymptomatic erythematous
CASE 15 Patient: A 41-year-old Thai female Chief Compliant: Generalized papulovesicular rash for 1 month Present Illness: She presented with a 1-week history of the generalized asymptomatic erythematous
Case 3. Ann T. Moriarty,MD
 Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
Many of the hematolymphoid disorders are derived
 REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/2010 holds various files of this Leiden University dissertation. Author: Benner, Marchina Frederika Title: Cutaneous CD30-positive lymphoproliferations
Cover Page The handle http://hdl.handle.net/1887/2010 holds various files of this Leiden University dissertation. Author: Benner, Marchina Frederika Title: Cutaneous CD30-positive lymphoproliferations
Sezary Syndrome(SS) and other malignancies. Hernani Cualing MD Hematopathologist IHCFLOW Lab
 and other malignancies. Hernani Cualing MD Hematopathologist IHCFLOW Lab") Sezary Syndrome(SS) and other malignancies Hernani Cualing MD Hematopathologist IHCFLOW Lab Disclosures IHCFLOW Laboratory:consultant and director NEOGENOMICS: contract consultant USF: contract reviewer
Sezary Syndrome(SS) and other malignancies Hernani Cualing MD Hematopathologist IHCFLOW Lab Disclosures IHCFLOW Laboratory:consultant and director NEOGENOMICS: contract consultant USF: contract reviewer
ISPUB.COM. Primary Cutaneous Anaplastic Large Cell Lymphoma Long-term Management with Low Dose Methotrexate. S Parker INTRODUCTION
 ISPUB.COM The Internet Journal of Dermatology Volume 7 Number 3 Primary Cutaneous Anaplastic Large Cell Lymphoma Long-term Management with Low Dose S Parker Citation S Parker.. The Internet Journal of
ISPUB.COM The Internet Journal of Dermatology Volume 7 Number 3 Primary Cutaneous Anaplastic Large Cell Lymphoma Long-term Management with Low Dose S Parker Citation S Parker.. The Internet Journal of
Immunohistochemical classification of haematolymphoid tumours. Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital
 Immunohistochemical classification of haematolymphoid tumours Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital Malignant lymphoproliferative diseases What are they? Haematolymphoid
Immunohistochemical classification of haematolymphoid tumours Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital Malignant lymphoproliferative diseases What are they? Haematolymphoid
Case Report A Severe Case of Lymphomatoid Papulosis Type E Successfully Treated with Interferon-Alfa 2a
 Hindawi Case Reports in Dermatological Medicine Volume 2017, Article ID 3194738, 5 pages https://doi.org/10.1155/2017/3194738 Case Report A Severe Case of Lymphomatoid Papulosis Type E Successfully Treated
Hindawi Case Reports in Dermatological Medicine Volume 2017, Article ID 3194738, 5 pages https://doi.org/10.1155/2017/3194738 Case Report A Severe Case of Lymphomatoid Papulosis Type E Successfully Treated
U006 Primary Cutaneous Lymphomas: Diagnosis, Staging and When to Refer M. Yadira Hurley, MD
 U006 Primary Cutaneous Lymphomas: Diagnosis, Staging and When to Refer M. Yadira Hurley, MD hurleyy@slu.edu DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Actelion: Speaker Honoraria, Investigator Grants, Consultant
U006 Primary Cutaneous Lymphomas: Diagnosis, Staging and When to Refer M. Yadira Hurley, MD hurleyy@slu.edu DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Actelion: Speaker Honoraria, Investigator Grants, Consultant
2010 Hematopoietic and Lymphoid ICD-O Codes - Alphabetical List THIS TABLE REPLACES ALL ICD-O-3 Codes
 Acute basophilic leukemia 9870/3 Acute biphenotypic leukemia [OBS] 9805/3 Acute erythroid leukemia 9840/3 Acute megakaryoblastic leukemia 9910/3 Acute monoblastic and monocytic leukemia 9891/3 Acute myeloid
Acute basophilic leukemia 9870/3 Acute biphenotypic leukemia [OBS] 9805/3 Acute erythroid leukemia 9840/3 Acute megakaryoblastic leukemia 9910/3 Acute monoblastic and monocytic leukemia 9891/3 Acute myeloid
2012 Hematopoietic and Lymphoid ICD-O Codes - Numerical List THIS TABLE REPLACES ALL ICD-O-3 Codes
 Malignant lymphoma, NOS 9590/3 Non-Hodgkin lymphoma, NOS 9591/3 B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma 9596/3 Primary
Malignant lymphoma, NOS 9590/3 Non-Hodgkin lymphoma, NOS 9591/3 B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma 9596/3 Primary
CASE 35 CLINICAL HISTORY
 Female, 24 Painful ulcerated lesion Left buttock Developed over a few weeks?abscess Excision CASE 35 CLINICAL HISTORY Two months later developed a similar lesion on right buttock CD30 CD3 CD4
Female, 24 Painful ulcerated lesion Left buttock Developed over a few weeks?abscess Excision CASE 35 CLINICAL HISTORY Two months later developed a similar lesion on right buttock CD30 CD3 CD4
Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent
 Int J Clin Exp Med 2014;7(1):307-311 www.ijcem.com /ISSN:1940-5901/IJCEM1311029 Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent Qilin Ao 2, Ying Wang 1, Sanpeng Xu 2,
Int J Clin Exp Med 2014;7(1):307-311 www.ijcem.com /ISSN:1940-5901/IJCEM1311029 Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent Qilin Ao 2, Ying Wang 1, Sanpeng Xu 2,
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies
 Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
3/23/2017. Disclosure of Relevant Financial Relationships. Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?!
 Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?! Judith A. Ferry Massachusetts General Hospital Disclosure of Relevant Financial Relationships USCAP requires that all
Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?! Judith A. Ferry Massachusetts General Hospital Disclosure of Relevant Financial Relationships USCAP requires that all
Blastic NK-Cell Leukemia / Lymphoma
 * * Blastic NK-Cell Leukemia / Lymphoma A Case Report Chun-Ming Lin Shu-Hui Wang Tseng-tong Kuo* Ching-Chi Chi Hsin-Chun Ho Hong-Shang Hong Blastic natural killer (NK) cell lymphoma / leukemia is a rare
* * Blastic NK-Cell Leukemia / Lymphoma A Case Report Chun-Ming Lin Shu-Hui Wang Tseng-tong Kuo* Ching-Chi Chi Hsin-Chun Ho Hong-Shang Hong Blastic natural killer (NK) cell lymphoma / leukemia is a rare
Burkitt lymphoma. Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8
 Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH
 EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH CASE E1 M: 68 yrs Left destructive sinonasal lesion.?lymphoma?adenocarcinoma CD20 CD10 BCL6 MIB1 Answers Diffuse large B cell
EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH CASE E1 M: 68 yrs Left destructive sinonasal lesion.?lymphoma?adenocarcinoma CD20 CD10 BCL6 MIB1 Answers Diffuse large B cell
Non-Hodgkin Lymphoma. Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract.
 Non-Hodgkin Lymphoma Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract. Protocol revision date: January 2005 No AJCC/UICC staging system Procedures Cytology
Non-Hodgkin Lymphoma Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract. Protocol revision date: January 2005 No AJCC/UICC staging system Procedures Cytology
Dermatopathology. Dr. Rafael Botella Estrada. Hospital La Fe de Valencia
 Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
3/24/2017 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS. Disclosure of Relevant Financial Relationships
 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
Primary Cutaneous Acral CD8 þ T-Cell Lymphoma
 Primary Cutaneous Acral CD8 þ T-Cell Lymphoma Vivian M. Hathuc, DO; Alexandra C. Hristov, MD; Lauren B. Smith, MD Primary cutaneous acral CD8 þ T-cell lymphoma is a new provisional entity in the 2016 revision
Primary Cutaneous Acral CD8 þ T-Cell Lymphoma Vivian M. Hathuc, DO; Alexandra C. Hristov, MD; Lauren B. Smith, MD Primary cutaneous acral CD8 þ T-cell lymphoma is a new provisional entity in the 2016 revision
2. Sézary syndrome (SS)
") Go Back to the Top To Order, Visit the Purchasing Page for Details Clinical images are available in hardcopy only. Clinical images are available in Clinical images are available in d e f g h i j Fig..36-2
Go Back to the Top To Order, Visit the Purchasing Page for Details Clinical images are available in hardcopy only. Clinical images are available in Clinical images are available in d e f g h i j Fig..36-2
184 Cutaneous Lymphomas: Morphology, Immunohistochemistry and Molecular Testing. David Cassarino MD, PhD Aaron Auerbach MD
 184 Cutaneous Lymphomas: Morphology, Immunohistochemistry and Molecular Testing David Cassarino MD, PhD Aaron Auerbach MD 2011 Annual Meeting Las Vegas, NV AMERICAN SOCIETY FOR CLINICAL PATHOLOGY 33 W.
184 Cutaneous Lymphomas: Morphology, Immunohistochemistry and Molecular Testing David Cassarino MD, PhD Aaron Auerbach MD 2011 Annual Meeting Las Vegas, NV AMERICAN SOCIETY FOR CLINICAL PATHOLOGY 33 W.
10/31/2017. Immunodeficiencies. Outline. Discuss EBV. Non-destructive Polymorphic Monomorphic Therapies Challenges
 I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Outline Transplant Congenital Autoimmunity T-cell/immune
I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Outline Transplant Congenital Autoimmunity T-cell/immune
11/2/2017. Immunodeficiencies. Joo Y. Song, MD Assistant Professor of Clinical Pathology. I have no financial disclosures.
 I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Transplant Autoimmunity Drugs T-cell dysfunction (Age,
I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Transplant Autoimmunity Drugs T-cell dysfunction (Age,
Common Problem Areas. WHO Classification. Defines separate diseases (entities) with their CLINICAL AGGRESSIVENESS LOW GRADE / HIGH GRADE
 with their CLINICAL AGGRESSIVENESS LOW GRADE / HIGH GRADE") WHO Classification Defines separate diseases (entities) with their CLINICAL AGGRESSIVENESS REVIEW OF MOST COMMON LYMPHOMA ENTITIES Dr Stefan Dojcinov LOW GRADE / HIGH GRADE (June 2014) The Non-Hodgkin
WHO Classification Defines separate diseases (entities) with their CLINICAL AGGRESSIVENESS REVIEW OF MOST COMMON LYMPHOMA ENTITIES Dr Stefan Dojcinov LOW GRADE / HIGH GRADE (June 2014) The Non-Hodgkin
Mimics of Lymphoma in Routine Biopsies. I have nothing to disclose regarding the information to be reported in this talk.
 Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco I have nothing to disclose regarding the information to be reported in this
Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco I have nothing to disclose regarding the information to be reported in this
"CUTANEOUS LYMPHOPROLIFERATIONS - AN UPDATE 2016"
 Chair: Werner Kempf, Co-Chair: Alistair Robson 1. Phil LeBoit: Unusual B cell proliferations 2. Martin Sangueza: From EBV- to HTLV-1-lymphomas 3. Joan Guitart: Aggressive cytotoxic T-cell-lymphomas - the
Chair: Werner Kempf, Co-Chair: Alistair Robson 1. Phil LeBoit: Unusual B cell proliferations 2. Martin Sangueza: From EBV- to HTLV-1-lymphomas 3. Joan Guitart: Aggressive cytotoxic T-cell-lymphomas - the
During past decades, because of the lack of knowledge
 Staging and Classification of Lymphoma Ping Lu, MD In 2004, new cases of non-hodgkin s in the United States were estimated at 54,370, representing 4% of all cancers and resulting 4% of all cancer deaths,
Staging and Classification of Lymphoma Ping Lu, MD In 2004, new cases of non-hodgkin s in the United States were estimated at 54,370, representing 4% of all cancers and resulting 4% of all cancer deaths,
clinical recommendations
 19 (Supplement 2): ii72 ii76, 2008 doi:10.1093/annonc/mdn095 Primary cutaneous lymphoma: ESMO Clinical Recommendations for diagnosis, treatment and follow-up R. Dummer 1 & M. Dreyling 2 On behalf of the
19 (Supplement 2): ii72 ii76, 2008 doi:10.1093/annonc/mdn095 Primary cutaneous lymphoma: ESMO Clinical Recommendations for diagnosis, treatment and follow-up R. Dummer 1 & M. Dreyling 2 On behalf of the
ECP meeting, Lisbon, september 2012 Slide seminar New and old challenges in the diagnosis of peripheral T-cell lymphomas
 ECP meeting, Lisbon, september 2012 Slide seminar New and old challenges in the diagnosis of peripheral T-cell lymphomas Philippe Gaulard, Dept of Pathology, INSERM U955, Hôpital Henri Mondor, 94010 -
ECP meeting, Lisbon, september 2012 Slide seminar New and old challenges in the diagnosis of peripheral T-cell lymphomas Philippe Gaulard, Dept of Pathology, INSERM U955, Hôpital Henri Mondor, 94010 -
Basal cell carcinoma 5/28/2011
 Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Goal of this Presentation A practical approach to the diagnosis of cutaneous carcinomas and their mimics Thaddeus Mully, MD University of California San Francisco To review common non-melanoma skin cancers
Classification of Hematologic Malignancies. Patricia Aoun MD MPH
 Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
LYMPHOMAS an overview of some subtypes of NHLs
 One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
Aggressive B-Cell Lymphomas
 Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
Integrated Hematopathology. Morphology and FCI with IHC
 Integrated Hematopathology Morphology and FCI with IHC FrontMatter.indd i 9/6/2009 9:30:12 PM FrontMatter.indd ii 9/6/2009 9:30:18 PM Integrated Hematopathology Morphology and FCI with IHC Cherie H Dunphy,
Integrated Hematopathology Morphology and FCI with IHC FrontMatter.indd i 9/6/2009 9:30:12 PM FrontMatter.indd ii 9/6/2009 9:30:18 PM Integrated Hematopathology Morphology and FCI with IHC Cherie H Dunphy,
Small B-cell (Histologically Low Grade) Lymphoma
 Lymphoma") Frequency of Lymphoid Neoplasms Small B-cell (Histologically Low Grade) Lymphoma Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital B-cell neoplasms 88% Diffuse large B-cell lymphoma
Frequency of Lymphoid Neoplasms Small B-cell (Histologically Low Grade) Lymphoma Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital B-cell neoplasms 88% Diffuse large B-cell lymphoma
1/14/2018. Objectives
 2018 Pathology CME Cutaneous Hematopathology Maui, HI Jan 18 th 26 th Pseudolymphomas Alejandro A. Gru, M.D. Assistant Professor of Pathology & Dermatology Dermatopathology Division and Fellowship Director
2018 Pathology CME Cutaneous Hematopathology Maui, HI Jan 18 th 26 th Pseudolymphomas Alejandro A. Gru, M.D. Assistant Professor of Pathology & Dermatology Dermatopathology Division and Fellowship Director
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
2016 AAD SUMMER MEETING SYMPOSIUM S011: CLINICOPATHOLOGIC SELF-ASSESSMENT 7/30/16 2:00 PM. Tom Helm, MD
 2016 AAD SUMMER MEETING SYMPOSIUM S011: CLINICOPATHOLOGIC SELF-ASSESSMENT 7/30/16 2:00 PM Tom Helm, MD Case 1 Diagnosis: Pseudoepitheliomatous hyperplasia associated with CD30+ lymphoproliferative disease
2016 AAD SUMMER MEETING SYMPOSIUM S011: CLINICOPATHOLOGIC SELF-ASSESSMENT 7/30/16 2:00 PM Tom Helm, MD Case 1 Diagnosis: Pseudoepitheliomatous hyperplasia associated with CD30+ lymphoproliferative disease
Mimics of Lymphoma in Routine Biopsies. Mixed follicular and paracortical hyperplasia. Types of Lymphoid Hyperplasia
 Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco Types of Lymphoid Hyperplasia Follicular hyperplasia (B-cells) Paracortical
Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco Types of Lymphoid Hyperplasia Follicular hyperplasia (B-cells) Paracortical
T cell lymphoma diagnostics and differential diagnosis to Hodgkin lymphoma
 T cell lymphoma diagnostics and differential diagnosis to Hodgkin lymphoma Sylvia Hartmann Dr. Senckenberg Institute of Pathology Goethe University Frankfurt Overview Borderline ALCL classical HL Borderline
T cell lymphoma diagnostics and differential diagnosis to Hodgkin lymphoma Sylvia Hartmann Dr. Senckenberg Institute of Pathology Goethe University Frankfurt Overview Borderline ALCL classical HL Borderline
Defined lymphoma entities in the current WHO classification
 Defined lymphoma entities in the current WHO classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno Bellinzona, January 29-31, 2016 Evolution of lymphoma classification Rappaport Lukes
Defined lymphoma entities in the current WHO classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno Bellinzona, January 29-31, 2016 Evolution of lymphoma classification Rappaport Lukes
Int J Clin Exp Pathol 2013;6(4): /ISSN: /IJCEP Tadashi Terada
: /ISSN: /IJCEP Tadashi Terada") Int J Clin Exp Pathol 2013;6(4):749-756 www.ijcep.com /ISSN:1936-2625/IJCEP1301060 Case Report Mycosis fungoides in plaque stage with pronounced eosinophilic infiltration, folliculotropism, and concomitant
Int J Clin Exp Pathol 2013;6(4):749-756 www.ijcep.com /ISSN:1936-2625/IJCEP1301060 Case Report Mycosis fungoides in plaque stage with pronounced eosinophilic infiltration, folliculotropism, and concomitant
What s new on the horizon in T-cell lymphoma Elaine S Jaffe National Cancer Institute, Bethesda MD
 What s new on the horizon in T-cell lymphoma Elaine S Jaffe National Cancer Institute, Bethesda MD WHO classification: where are we today? Of 12 monographs planned for 4 th Edition Bluebook series, only
What s new on the horizon in T-cell lymphoma Elaine S Jaffe National Cancer Institute, Bethesda MD WHO classification: where are we today? Of 12 monographs planned for 4 th Edition Bluebook series, only
WHO Classification. B-cell chronic lymphocytic leukemia/small T-cell granular lymphocytic leukemia
 Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
Aggressive B-cell Lymphomas Updated WHO classification Elias Campo
 Aggressive B-cell Lymphomas Updated WHO classification Elias Campo Hospital Clinic, University of Barcelona Diffuse Large B-cell Lymphoma A Heterogeneous Category Subtypes with differing: Histology and
Aggressive B-cell Lymphomas Updated WHO classification Elias Campo Hospital Clinic, University of Barcelona Diffuse Large B-cell Lymphoma A Heterogeneous Category Subtypes with differing: Histology and
Blastic Plasmacytoid Dendritic Cell Neoplasm : Report of Two Cases
 Case Study Blastic Plasmacytoid Dendritic Cell Neoplasm : Report of Two Cases J Clin Exp Hematopathol Vol. 52, No. 1, May 2012 Kanako Tsunoda, 1,2) Takashi Satoh, 2) Kiyomi Akasaka, 1,2) Yuichi Ishikawa,
Case Study Blastic Plasmacytoid Dendritic Cell Neoplasm : Report of Two Cases J Clin Exp Hematopathol Vol. 52, No. 1, May 2012 Kanako Tsunoda, 1,2) Takashi Satoh, 2) Kiyomi Akasaka, 1,2) Yuichi Ishikawa,
HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO
 HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO HODGKIN LYMPHOMA CLASSIFICATION Lukes & Butler Rye WHO-2016 Linphocytic and/or histiocytic Nodular & diffuse Nodular Sclerosis Lymphocyte
HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO HODGKIN LYMPHOMA CLASSIFICATION Lukes & Butler Rye WHO-2016 Linphocytic and/or histiocytic Nodular & diffuse Nodular Sclerosis Lymphocyte
Aggressive B-cell lymphomas and gene expression profiling towards individualized therapy?
 Aggressive B-cell lymphomas and gene expression profiling towards individualized therapy? Andreas Rosenwald Institute of Pathology, University of Würzburg, Germany Barcelona, June 18, 2010 NEW WHO CLASSIFICATION
Aggressive B-cell lymphomas and gene expression profiling towards individualized therapy? Andreas Rosenwald Institute of Pathology, University of Würzburg, Germany Barcelona, June 18, 2010 NEW WHO CLASSIFICATION
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
Microscopic study of the normal skin in cases of mycosis fungoides
 Microscopic study of the normal skin in cases of mycosis fungoides M. El Darouti, S. Marzook, M. Bosseila, O. Abu Zeid, O. El- Safouri, A. Zayed, A. El-Ramly Egyptian Dermatology Online Journal 2 (1):
Microscopic study of the normal skin in cases of mycosis fungoides M. El Darouti, S. Marzook, M. Bosseila, O. Abu Zeid, O. El- Safouri, A. Zayed, A. El-Ramly Egyptian Dermatology Online Journal 2 (1):
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Istodax) Reference Number: CP.PHAR.314 Effective Date: 01.01.17 Last Review Date: 11.18 Line of Business: Medicaid, HIM-Medical Benefit Coding Implications Revision Log See Important
Clinical Policy: (Istodax) Reference Number: CP.PHAR.314 Effective Date: 01.01.17 Last Review Date: 11.18 Line of Business: Medicaid, HIM-Medical Benefit Coding Implications Revision Log See Important
Methods used to diagnose lymphomas
 Institut für Pathologie Institut für Pathologie Methods used to diagnose lymphomas Prof. Dr.Med. Leticia Quintanilla-Fend Molecular techniques NGS histology Cytology AS-PCR Sanger seq. MYC Immunohistochemistry
Institut für Pathologie Institut für Pathologie Methods used to diagnose lymphomas Prof. Dr.Med. Leticia Quintanilla-Fend Molecular techniques NGS histology Cytology AS-PCR Sanger seq. MYC Immunohistochemistry
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU
 Rex K.H. Au-Yeung Department of Pathology, HKU") Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Vorinostat (Zolinza) Reference Number: CP.PHAR.83 Effective Date: 10.01.18 Last Review Date: 07.13.18 Line of Business: Oregon Health Plan Revision Log See Important Reminder at the end
Clinical Policy: Vorinostat (Zolinza) Reference Number: CP.PHAR.83 Effective Date: 10.01.18 Last Review Date: 07.13.18 Line of Business: Oregon Health Plan Revision Log See Important Reminder at the end
Cluster of differentiation (CD) markers in erythrodermic patients: A case series study
 markers in erythrodermic patients: A case series study") Original Article Cluster of differentiation (CD) markers in erythrodermic patients: A case series study Fariba Ghalamkarpour, MD Faranak Niknafs, MD Shima Younespour, PhD Skin Research Center, Shahid Beheshti
Original Article Cluster of differentiation (CD) markers in erythrodermic patients: A case series study Fariba Ghalamkarpour, MD Faranak Niknafs, MD Shima Younespour, PhD Skin Research Center, Shahid Beheshti
Lymphadenopathies mimicking lymphoma and vice versa. Session 3
 Lymphadenopathies mimicking lymphoma and vice versa Session T/ NK Cell System The human and rodent T and NK cell system is characterized by many highly specialized cell suopulations and functions, that
Lymphadenopathies mimicking lymphoma and vice versa Session T/ NK Cell System The human and rodent T and NK cell system is characterized by many highly specialized cell suopulations and functions, that
Classification! Immunohistochemical classification of haematolymphoid tumours. Malignant lymphoproliferative diseases
 Immunohistochemical classification of haematolymphoid tumours Haematolymphoid Neoplasias: Leukaemia vs Lymphoma C L O N A L M A L I G N A N C I E S Stephen Hamilton-Dutoit Institute of Pathology Aarhus
Immunohistochemical classification of haematolymphoid tumours Haematolymphoid Neoplasias: Leukaemia vs Lymphoma C L O N A L M A L I G N A N C I E S Stephen Hamilton-Dutoit Institute of Pathology Aarhus