Prima linea: dovremmo evitare i PI nella terapia di prima linea per i loro effetti non desiderati? Giuseppina Liuzzi
|
|
|
- Curtis Fields
- 5 years ago
- Views:
Transcription


1 6 th INFECtivology TOday Paestum maggio 2014 Prima linea: dovremmo evitare i PI nella terapia di prima linea per i loro effetti non desiderati? Giuseppina Liuzzi Istituto Nazionale per le Malattie Infettive IRCCS Lazzaro Spallanzani Roma
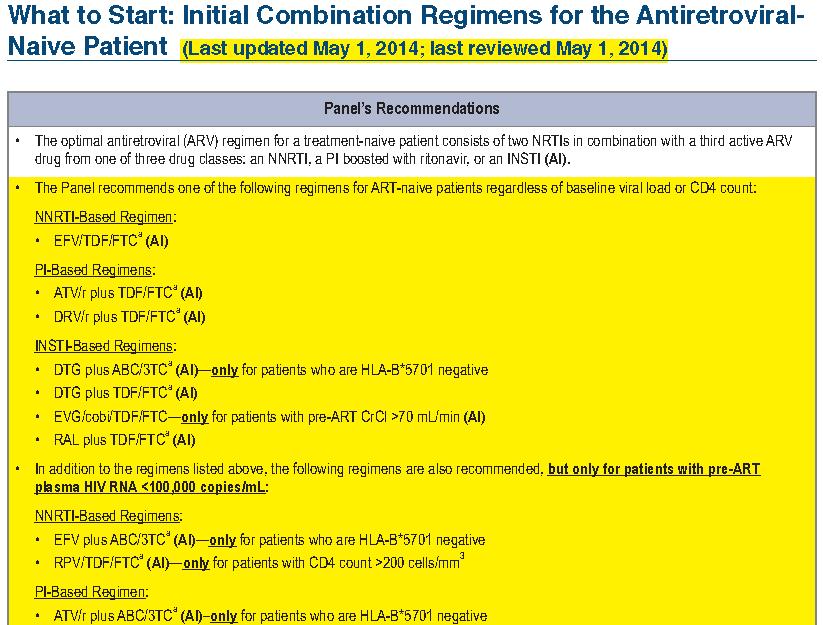
2 Recommendations for ART Initiation ART is recommended for all HIV-infected ART-naive pts to reduce risk of disease progression and transmission Strength of recommendation varies by CD4+ cell count and risk group (perinatal, heterosexual, other) Pts should be ready to commit to ART and understand benefits and risks of therapy and importance of adherence; individual pts may elect to defer ART Selection of a regimen should be individualized on the basis of virologic efficacy, toxicity, pill burden, dosing frequency, drug drug interaction potential, resistance testing results, and comorbid conditions DHHS Guidelines. May 2014.
3 Considerations When Selecting Firstline Antiretroviral Therapy Baseline CD4+ cell count/ HIV-1 RNA level Age Sex Patient/Viral Factors Occupation (eg, work schedule) Comorbid conditions (eg, CV risk, renal abnormalities) Plans for pregnancy Access to care Concurrent medications Adherence to other medications Genetics (eg, HLA-B*5701) Viral tropism Antiretroviral Drug Factors Efficacy Baseline drug resistance Tolerability Long-term toxicity/metabolic effects Drug drug interactions Dosing frequency Pill burden Pharmacokinetics Cost
4 Individualizing First-line Therapy: Specific Circumstances Circumstance No genotype High HIV-1 RNA Renal disease Dyslipidemia CV risk factors Pregnancy Chronic HBV infection Decreased BMD Concerns about CNS effects Agents Use boosted PI Caution with ABC, RPV Caution with TDF, ATV/RTV; monitoring complicated with COBI and DTG RAL, DTG, RPV most lipid neutral Possible association with ABC, ddi, LPV/RTV No data for DRV/RTV, INSTIs, MVC Preferred: ZDV/3TC + NVP, LPV/RTV, or ATV/RTV EFV can be used after first 5-6 wks Preferred TDF + 3TC or FTC Alternative is entecavir Caution with TDF Caution with EFV for at least first mo
5
6
7 Concerns Regarding NRTIs ABC Decreased potency compared with TDF in those with high HIV-1 RNA levels (> 100,000 copies/ml) when combined with EFV and ATV + RTV Variable results regarding relationship with CV events Avoid in patients with positive HLA-B*5701 test TDF Associated with greater decline in bone mineral density than ABC Associated with variable decline in renal function compared with other NRTIs
8 Selecting the Third Drug in a First-line Regimen

9 Readiness for Therapy: A Key Decision Point Potential options PI-based therapy NNRTI- and RAL-based strategies Simple regimen (1 pill, once daily) Regimens to avoid Complicated regimens: frequent dosing, food requirements Regimens with more adverse events: may affect adherence Regimens with higher risk of resistance at failure
10 Which Patient for EFV? Considerations in Favor Coformulation; 1 pill QD [1] Effective across HIV-1 RNA, CD4+ strata [2] Most experience of all NNRTIs Most experience of all preferred drugs Considerations Against High risk of resistance at virologic failure [3] CNS effects [1] Potential for teratogenesis in early pregnancy [4] Drug drug interactions with other drugs metabolized by CYP system [1] Increases in lipids [5] 1. TDF/FTC/EFV [package insert]. 2. Ribaudo HJ, et al. J Infect Dis. 2008;197: Gallant J, et al. N Engl J Med. 2006;354: DHHS Perinatal Guidelines. July Daar E, et al. Ann Intern Med. 2011;154:
11 Efficacy and Tolerability of Atazanavir, Raltegravir, or Darunavir with FTC/TDF: ACTG A5257 Landovitz RJ, Ribaudo HJ, Ofotokun I, Wang H, Baugh BP, Leavitt RY, Rooney JF, Seekins D, Currier JS, and Lennox JL for the A5257 Study Team
12 A5257 Study Design* HIV-infected patients, 18 yr, with no previous ART, VL 1000 c/ml at US Sites Randomized 1:1:1 to Open Label Therapy Stratified by screening HIV-1 RNA level ( vs < 100,000 c/ml), A5260s metabolic substudy participation, cardiovascular risk ATV 300 mg QD + RTV 100mg QD + FTC/TDF 200/300 mg QD RAL 400 mg BID + FTC/TDF 200/300 mg QD DRV 800 mg QD + RTV 100 mg QD + FTC/TDF 200/300 mg QD Study Conclusion 96 weeks after final participant enrolled Follow-up continued for 96 weeks after randomization of last subject (range 2-4 years) regardless of status on randomized ART *With the exception of RTV, all ART drugs were provided by the study
13 Participants Excluded 1 acute illness, 1 prior ART and 3 prior ART + resistance Participants Enrolled 1814 Participants Eligible 1809 ATV/r 605 (5 never started ART) RAL 603 (4 never started ART) DRV/r 601 (4 never started ART) 556 (92%) Completed 96 Weeks 560 (93%) Completed 96 Weeks 546 (91%) Completed 96 Weeks
 -20-10 0 10 20 ATV/r vs RAL 3.4% (-0.7%, 7.4%) DRV/r vs RAL 5.6% (1.3%, 9.9%) ATV/r vs DRV/r -2.")
14 Cumulative Incidence of Virologic Failure Difference in 96 wk cumulative incidence (97.5% CI) ATV/r vs RAL 3.4% (-0.7%, 7.4%) DRV/r vs RAL 5.6% (1.3%, 9.9%) ATV/r vs DRV/r -2.2% (-6.7%, 2.3%)
15 Cumulative Incidence of Tolerability Failure Difference in 96 wk cumulative incidence (97.5% CI) Favors RAL ATV/r vs RAL 13% (9.4%, 16%) DRV/r vs RAL 3.6% (1.4%, 5.8%) Favors DRV/r ATV/r vs DRV/r 9.2% (5.5%, 13%)
16 Cumulative Incidence of Virologic or Tolerability Failure Difference in 96 wk cumulative incidence (97.5% CI) Favors RAL Favors RAL Favors DRV/r ATV/r vs RAL 15% (10%, 20%) DRV/r vs RAL 7.5% (3.2%, 12%) ATV/r vs DRV/r 7.5% (2.3%, 13%) *Consistent results seen with TLOVR at a 200 copies/ml threshold
17 Tolerability Failure Toxicity Associated Discontinuation of randomized ART * ATV/r (N=605) RAL (N=603) DRV/r (N=601) Any toxicity discontinuation 95 (16%) 8 (1%) 32 (5%) Gastrointestinal toxicity Jaundice/Hyperbilirubinemia Other hepatic toxicity Skin toxicity Metabolic toxicity Renal toxicity (all nephrolithiasis) Abnormal chem/heme (excl. LFTs) Other toxicity *Participants allowed to switch therapy for intolerable toxicity
 RAL: 288 (272, 304) DRV/r: 256 (240, 271) Lipid and Bone")

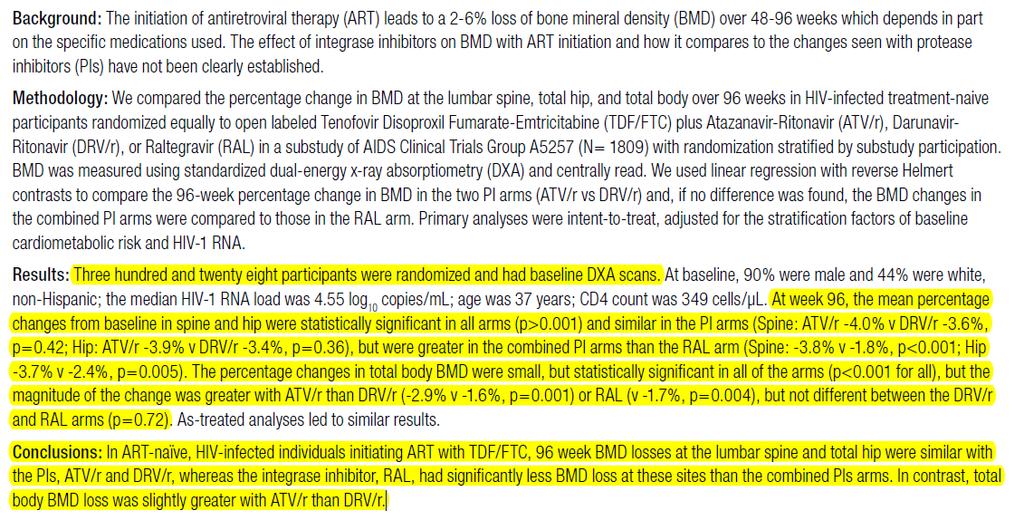
18 Additional Clinical Outcomes Mean change in CD4 count from baseline ATV/r: 284 (269,300) RAL: 288 (272, 304) DRV/r: 256 (240, 271) Lipid and Bone Changes Both PI/r arms had greater increases in LDL and triglycerides than the RAL-arm (p<0.001) Lipids: Poster 746 (Ofotokun et al) Bone: Poster 779LB (Brown et al)
19
20

21 BONE RESULTS
22 Conclusions ATV/r, RAL, and DRV/r were equivalent for virologic efficacy ATV/r was less well tolerated than DRV/r or RAL Largely due to cosmetic hyperbilirubinemia RAL was superior to both PI/r regimens for combined tolerability and virologic efficacy DRV/r was superior to ATV/r VF with resistance was rare More frequently observed with RAL Analyses are ongoing to evaluate: Cardiovascular, metabolic, skeletal, fat, inflammatory biomarkers, behavior, adherence, and key subgroup differences
23 Guidelines for Initial Therapy: Time for a Change? In 2009, DHHS listed 4 regimens as preferred ; no changes since Since then, several new agents have been approved: RPV, EVG/COBI, DTG What do the clinical trials of these agents show? Current Preferred Regimens NRTIs Third Agent EFV ATV/RTV TDF/FTC + DRV/RTV RAL
24 HIV-1 RNA < 50 c/ml at Wk 96 (ITT-TLOVR) ECHO/THRIVE: Rilpivirine Noninferior to Efavirenz Through Wk n = 686 RPV 682 EFV More virologic failures with RPV vs EFV: 14% vs 8% Difference due to more failures between Wks 0-48; failures comparable between arms from Wks Development of NRTI mutations more common with RPV vs EFV E138K mutation with RPV cross-resistance with ETR Discontinuation for AEs more common with EFV vs RPV: 9% vs 4% Pooled Data Cohen CJ, et al. AIDS. 2013;27:
25 HIV-1 RNA < 50 copies/ml (%) ECHO/THRIVE Post Hoc Analysis: Wk 96 Efficacy by Baseline VL and CD4+ Count 100 Rilpivirine Efavirenz n = n = k > 100k - > 500k 500k By Baseline HIV-1 RNA (copies/ml) Cohen CJ, et al. AIDS. 2013;27: < < 200 < 350 By Baseline CD4+ Count (cells/mm 3 ) 350
26 Pooled ECHO/THRIVE Analysis: Wk 96 Safety Adverse Event, % Most common adverse events of interest Any neurologic Dizziness Any psychiatric Abnormal dreams/nightmares Rash (any type) Grade 2-4 laboratory abnormality Total cholesterol LDL-C AST ALT *P <.0001 vs rilpivirine. P =.0039 vs rilpivirine. Rilpivirine (n = 686) Efavirenz (n = 682) 38* 27* 24* 13 15* 22* 18* Cohen CJ, et al. AIDS. 2013;27:
27 HIV-1 RNA < 50 c/ml (%) Open-Label STaR Trial: RPV/TDF/FTC Non inferior to EFV/TDF/FTC at Wk 48 RPV/TDF/FTC noninferior to EFV/TDF/FTC in overall population and in pts with baseline HIV-1 RNA > 100,000 c/ml RPV/TDF/FTC superior to EFV/TDF/FTC in pts with baseline HIV-1 RNA 100,000 c/ml RPV/TDF/FTC (n = 394) Δ: 4.1% (95% CI: -1.1 to 9.2) Δ : 7.2% (95% CI: ) Δ : -1.8% EFV/TDF/FTC (n = 392) (95% CI: to 7.5) Post Hoc Analysis n/n = 0 338/ 394 All Pts 320/ / / 250 VL 100k Cohen C, et al. Glasgow Abstract O / 134 VL > 100k 116/ / 98 96/ 117 VL > 100k - 500k 26/ 36 20/ 25 VL > 500k
28 Summary of Results From Phase III Studies of RPV vs EFV More virologic failures, especially with HIV-1 RNA > 100k [1,2] Difference reduced in open-label study, suggesting importance of adherence, food effect [2] DHHS: RPV is not recommended in patients with pretreatment HIV-1 RNA > 100,000 copies/ml; higher rate of virologic failures reported in patients with pre-art CD4+ count < 200 cells/mm 3 who were treated with RPV + 2 NRTIs [3] RPV resistance mutation (E138K) causes cross-resistance with ETR [1,2] Fewer drug discontinuations with RPV than EFV [1,2] Fewer rash, CNS events; better lipids [1,2] 1. Cohen CJ, et al. AIDS. 2013;27: Cohen C, et al. Glasgow Abstract O DHHS Guidelines. February 2013.
29 Which Patient for RPV? Considerations in Favor Coformulated/1 pill daily Superior vs EFV at lower VL [1] Fewer CNS adverse events than EFV [2] Considerations Against Less effective at high BL VL [2] (not recommended at high VL and low CD4+) [3] Food requirement [4] Restricted use with PPIs or H2 blockers [4] High risk of resistance and cross-resistance with other NNRTIs at VF [2] 1. Cohen C, et al. Glasgow Abstract O Cohen C, et al. AIDS. 2013;27: DHHS Guidelines. February TDF/FTC/RPV [package insert].
30 HIV-1 RNA < 50 c/ml (%) Elvitegravir/Cobicistat/TDF/FTC Noninferior to Efavirenz/TDF/FTC Through Wk 144 EVG/COBI/TDF/FTC (n = 348) Δ: 3.6% (95% CI: -1.6 to 8.8) Δ: 2.7% (95% CI: -2.9 to 8.3) EFV/TDF/FTC (n = 352) Δ: 4.9% (95% CI: -1.3 to 11.1) Results consistent across subgroups: BL HIV-1 RNA, CD4+ count, age, sex, race Resistance at VF detected in 8 pts per arm through Wk 48, plus 2 additional pts per arm through Wk 96 rates similar btwn arms; no additional pts on EVG/COBI developed resistance after Wk 96 In those on EVG/COBI, 9/10 pts had primary integrase and 10/10 had NRTI resistance mutations In those on EFV, 10/10 had NNRTI and 3/10 had NRTI resistance mutations 0 Wk 48 Wk 96 Wk 144 Zolopa A, et al. J Acquir Immune Defic Syndr. 2013;63: Sax PE, et al. Lancet. 2012;379: Wohl D, et al. ICAAC Abstract H-672a.
31 HIV-1 RNA < 50 c/ml (%) EVG/COBI/TDF/FTC Non inferior to ATV/RTV + TDF/FTC Through Wk 96 EVG/COBI/TDF/FTC (n = 353) Δ: 2.7% (95% CI: -2.1 to 7.5) ATV/RTV + TDF/FTC (n = 355) Δ: 1.1% (95% CI: -4.5 to 6.7) Results consistent across subgroups: BL HIV-1 RNA, CD4+ count, adherence, age, sex, race In EVG/COBI arm, resistance at VF detected in 5 pts through Wk 48, plus 1 additional pt through Wk 96 vs 0 pts in ATV/RTV arm 5/6 had primary integrase and 5/6 had NRTI resistance mutations 0 Wk 48 Wk 96 Rockstroh J, et al. J Acquir Immune Defic Syndr. 2013;62: De Jesus E, et al. Lancet. 2012;379:
32 Adverse Events With EVG/COBI/TDF/FTC vs ATV/RTV + TDF/FTC Adverse Events > 10% in Either Group Overall Discontinuation Rate EVG/COBI/ TDF/FTC (n = 353) ATV/RTV + TDF/FTC (n = 355) EVG/COBI/ TDF/FTC (n = 353) ATV/RTV + TDF/FTC (n = 355) Diarrhea Nausea Upper respiratory infection Headache Fatigue Ocular icterus 1 14 Overall 4 5 Diarrhea 1 < 1 Nausea < 1 1 Vomiting < 1 1 Ocular icterus 0 1 Jaundice 0 1 Drug eruption 0 1 Discontinuation rates due to renal adverse events were identical in both arms (0.3%) DeJesus E, et al. Lancet. 2012;379:
33 Change From BL at Wk 48 (mg/dl) EVG/COBI/TDF/FTC vs EFV or ATV/RTV: Lipid Changes P < P = EVG/COBI/TDF/FTC EFV/TDF/FTC P = P = P = Total LDL HDL Triglycerides Total LDL HDL Triglycerides Cholesterol Cholesterol Conclusion: Whereas some lipid fractions better with EVG/COBI/TDF/FTC than EFV or ATV/RTV, overall differences were modest and unlikely to be of clinical significance Sax P, et al. Lancet. 2012;379: DeJesus E, et al. Lancet. 2012;379: Sax P, et al. CROI Abstract P = EVG/COBI/TDF/FTC ATV/RTV + TDF/FTC P = P =
34 EVG/COBI/TDF/FTC vs EFV/TDF/FTC: Common Adverse Events Treatment Emergent Adverse Events in 10% of Subjects, % EVG/COBI/TDF/FTC (n = 348) EFV/TDF/FTC (n = 352) Diarrhea Nausea* Abnormal dreams Upper respiratory infection Headache Fatigue Insomnia* 9 14 Depression 9 11 Dizziness 7 24 Rash 6 12 *P <.05 P <.001 P =.009 Sax P, et al. Lancet. 2012;379:
35 Summary of Results From Tx-Naïve Phase III Studies of EVG/COBI/TDF/FTC Virologic outcomes noninferior to EFV/TDF/FTC and ATV/RTV + TDF/FTC Activity sustained in high VL stratum 2% failed with resistance, usually to both NRTIs and EVG Adverse events vs EFV: fewer CNS, rash events; better lipids; more nausea vs ATV/RTV: less jaundice Small, rapid increase in serum creatinine related to inhibition of tubular secretion of creatinine 5 pts (0.7% of total) developed tubulopathy, likely from TDF
36 Which Patient for TDF/FTC/EVG/COBI? Considerations in Favor Coformulated/1 pill dally Once-daily INSTI regimen Noninferior to EFV and ATV/RTV across HIV-1 RNA, CD4+ strata [1,2] Fewer CNS AEs than EFV [1] Considerations Against Includes pharmacologic booster High risk of resistance at VF [1-4] Cross resistance with RAL [5] Drug drug interactions [6] Concerns about monitoring renal function with COBI [6] 1. Zolopa A, et al. J Acquir Immune Defic Syndr. 2013;63: Rockstroh J, et al. J Acquir Immune Defic Syndr. 2013;62: Sax PE, et al. Lancet. 2012;379: DeJesus E, et al. Lancet. 2012;379: DeJesus E, et al. IAS Abstract TUPEB TDF/FTC/EVG/COBI [package insert].
37 HIV-1 RNA < 50 c/ml (%) SPRING-2: Dolutegravir QD Non inferior to Raltegravir BID Through Wk 96 DTG 50 mg QD (n = 411) RAL 400 mg BID (n = 411) NRTIs: investigator chosen ABC/3TC (40%) or TDF/FTC 60%) DTG non inferior to RAL at Wk 48 [1] and Wk 96 [2] Adverse events and discontinuation rates similar No resistance at VF with DTG vs 1 subject with integrase resistance and 4 with NRTI resistance in RAL group Wk 48 Wk 96 Raffi F, et al. Lancet. 2013;381: Raffi F, et al. IAS Abstract TULBPE17.
38 SPRING-2: Wk 48 Safety and Tolerability Outcome Treatment-emergent adverse events, % Nausea Headache Nasopharyngitis Diarrhea Dolutegravir 50 mg QD (n = 411) Raltegravir 400 mg BID (n = 411) Serious adverse events, % 7 8 Withdrawals due to adverse events, % 2 2 Mean change in creatinine clearance, ml/min Median change in lipids, mg/dl Total cholesterol Triglycerides All patients received either TDF/FTC or ABC/3TC. Raffi F, et al. IAC Abstract ThLBB
39 HIV-1 RNA < 50 c/ml at Wk 48 (%) SINGLE: DTG + ABC/3TC Superior to EFV/TDF/FTC at Wk Difference 7.4% (95% CI: +2.5 to +12.3; P =.003) 88 DTG 50 mg + ABC/3TC QD (n = 414) 81 EFV/TDF/FTC QD (n = 419) DTG superior to EFV at Wk 48 primary efficacy endpoint 4% on each arm with protocoldefined VF Among pts with VF in EFV arm, 1 pt with NRTI and 4 with NNRTI resistance vs 0 pts with resistance in DTG arm Treatment-related study discontinuation in 10% on EFV vs 2% on DTG CNS events and rash more common with EFV Walmsley S, et al. ICAAC Abstract H-556b.
40 SINGLE Study: Wk 48 Safety and Tolerability Outcome, % Treatment-emergent adverse events Dizziness Headache Somnolence Insomnia Abnormal dreams DTG 50 mg + ABC/3TC QD (n = 414) EFV/TDF/FTC QD (n = 419) Serious adverse events < 1 2 Withdrawals due to adverse events 2 10 Liver changes ALT > 3 x ULN Total bilirubin > 1.5 ULN Alkaline phosphatase > 1.5 x ULN *P <.001 P =.029 Walmsley S, et al. ICAAC Abstract H-556b. 1 < 1 < 1 35* * 4 < 1 5
41 HIV-1 RNA < 50 c/ml at Wk 48 (%) FLAMINGO: DTG + NRTIs Superior to DRV/RTV + NRTIs at Wk Difference 7.1% (95% CI: +0.9 to +13.2; P =.025) DTG 50 mg QD + NRTIs (n = 242) DRV/RTV 800/100 mg QD + NRTIs (n = 242) Feinberg J, et al. ICAAC Abstract H1464a. DTG superior to DRV/RTV (both with TDF/FTC or ABC/3TC) at Wk 48 primary efficacy endpoint VF: 2 pts (1%) on each arm No treatment-emergent resistance in either arm Treatment-related study discontinuation in 1% of DTG pts and 4% of DRV/RTV pts More diarrhea with DRV/RTV; more headache with DTG
42 Summary of Results From Tx-Naïve Phase III Studies of DTG DTG + NRTIs noninferior to RAL + NRTIs; superior to DRV/RTV + NRTIs; DTG + ABC/3TC superior to EFV/TDF/FTC More drug discontinuations in EFV and DRV/RTV arms No DTG resistance mutations as yet detected with virologic failure DTG well tolerated with low rates of study drug discontinuation Fewer CNS and rash events compared with EFV Less diarrhea than DRV/RTV Small rapid increase in serum creatinine related to inhibition of tubular secretion of creatinine No drug-related renal events
43 Which Patient for DTG? Considerations in Favor Once-daily INSTI without boosting Superior efficacy vs EFV and DRV/RTV [1,2] Potentially less resistance at VF [1,3] Effective at high VL with both ABC/3TC and TDF/FTC [3] Well tolerated [1-3] Few drug drug interactions [4] Considerations Against Not yet available as coformulation Concerns about monitoring renal function [4] No guideline recommendation at this time 1. Walmsley S, et al. ICAAC Abstract H-556b. 2. Feinberg J, et al. ICAAC Abstract H-1464a. 3. Raffi F, et al. Lancet. 2013;381: Dolutegravir [package insert].
44
45 Potential Benefits of New Treatment Options for HIV Rilpivirine Elvitegravir/Cobicistat Dolutegravir Smallest single-tablet regimen Fewer CNS and rash events vs EFV Better lipids than EFV Superior to EFV if HIV-1 RNA < 100k Single-tablet regimen Maintains comparable virologic activity to EFV, ATV across low and high HIV-1 RNA Fewer CNS and rash events vs EFV Better lipids than EFV, comparable to ATV/RTV Less jaundice than ATV/RTV Superior to EFV/TDF/FTC and DRV/RTV Maintains at least comparable virologic activity to EFV, RAL, DRV/RTV across low and high HIV-1 RNA Fewer CNS and rash events vs EFV Better lipids than EFV No resistance detected with virologic failure Fewer drug drug interactions than boosted PIs, EVG/COBI
46 Lipid Comparisons in Clinical Trials ARV Comparisons RPV [1] vs EFV at Wk 48 Smaller changes in TC, HDL-C, LDL-C, TG (all P <.0001) COBI [2] EVG/COBI TDF/FTC [3-5] vs RTV at Wk 48 when combined with ATV Similar changes in lipids in all fractions vs EFV at Wk 48 Smaller changes in TC (P <.001), HDL-C, LDL-C (both P =.001) Similar changes in TG between arms vs ATV/RTV at Wk 48 Similar changes in TC, HDL-C, LDL-C Smaller change in TG (P =.006) DTG [6] vs RAL at Wk 48 Similar small changes in lipids in all fractions vs EFV at Wk 48 Smaller changes in TC, HDL-C, LDL-C 1. Cohen C, et al. AIDS. 2013;27: Gallant J, et al. J Infect Dis. 2013;208: Sax P, et al. Lancet. 2012;379: DeJesus E, et al. Lancet. 2012;379: Sax P, et al. CROI Abstract Dolutegravir [package insert].
47 Drug Drug Interactions With BOC and TVR Antiretroviral Interactions With Boceprevir Interactions With Telaprevir RPV [1,2] No clinically relevant interactions No clinically relevant interactions EVG/COBI No data No clinically relevant interactions TDF/FTC [3] DTG [4] No clinically relevant interactions No clinically relevant interactions ATV/RTV [5] DRV/RTV [5] EFV [5] Coadministration not recommended Coadministration not recommended Coadministration not recommended Coadministration not recommended Coadministration not recommended Increase TVR dose to 1125 mg q8h RAL [5] No clinically relevant interactions No clinically relevant interactions 1. Rhee E, et al. CROI Abstract Rilpivirine [package insert]. 3. Custodio J, et al. ICAAC Abstract A Dolutegravir [package insert]. 5. DHHS Adult Guidelines. February 2013.
48 % of follow-up COMPACT: Italy Adherence and Clinical Outcomes of STR vs. Multi-Pill Regimens % Patients Evaluation of outcomes in observational, retrospective cohort of 1,604 HIV+ pts ( ) Non-Adherence to cart Regimens (days) Viral Load and CD4 at End of Follow-Up (n=709) STR PI NNRTI RAL n=159 n=878 n=523 n=44 Complete Non-Adherence Selective Non-Adherence STR PI NNRTI RAL CD4 > 500 cells/mm 3 HIV-1 RNA <50c/mL STR was associated with higher adherence vs. multi-pill regimens and with greater rates of virologic suppression and CD4 > 500 cells/mm 3 Antinori A, et al. HIV ; Glasgow. P14
49 What s Available as Fixed-Dose Combinations, and What s Coming? Available Now Efavirenz/tenofovir DF/ emtricitabine Rilpivirine/tenofovir DF/ emtricitabine Elvitegravir/cobicistat/ tenofovir DF/emtricitabine Future Options Darunavir/cobicistat Darunavir/cobicistat/ emtricitabine/tenofovir alafenamide (GS-7340) Atazanavir/cobicistat Dolutegravir/abacavir/ lamivudine Dolutegravir will be initially available as single tablet, not fixed-dose combination
50 Conclusions Currently many simple and easy-to-administer first-line antiretroviral regimens The decision as to which regimen to select first is based upon efficacy, safety, and select characteristics Concerns regarding adherence Virologic characteristic (eg, baseline HIV-1 RNA, drug resistance) Comorbid conditions (eg, cardiovascular disease, hepatitis coinfection, renal disease)
HIV Update Allegra CPD Day Program Port Elizabeth Dr L E Nojoko
 HIV Update 2014 Allegra CPD Day Program Port Elizabeth 12-02-2014 Dr L E Nojoko Global estimates for adults and children 2011 People living with HIV 34.0 million [31.4 million 35.9 million] New HIV infections
HIV Update 2014 Allegra CPD Day Program Port Elizabeth 12-02-2014 Dr L E Nojoko Global estimates for adults and children 2011 People living with HIV 34.0 million [31.4 million 35.9 million] New HIV infections
Disclosures. Update on HIV Drug Therapy: A Case based Discussion. Case # 1: Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv
 Disclosures Update on HIV Drug Therapy: A Case based Discussion Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv Philip Grant Assistant Professor Division of Infectious Diseases
Disclosures Update on HIV Drug Therapy: A Case based Discussion Dr. Grant has received grant support from BMS, Gilead, Janssen, and Viiv Philip Grant Assistant Professor Division of Infectious Diseases
Antiretroviral Therapy: What to Start
 FLOWED: 05-14-2015 Chicago, IL: May 18, 2015 Antiretroviral Therapy: What to Start Eric S. Daar, MD Professor of Medicine David Geffen School of Medicine University of California Los Angeles Los Angeles,
FLOWED: 05-14-2015 Chicago, IL: May 18, 2015 Antiretroviral Therapy: What to Start Eric S. Daar, MD Professor of Medicine David Geffen School of Medicine University of California Los Angeles Los Angeles,
HIV Treatment Update. Anton Pozniak Consultant Physician, Director of HIV Services Chelsea and Westminster Hospital, London
 HIV Treatment Update Anton Pozniak Consultant Physician, Director of HIV Services Chelsea and Westminster Hospital, London Guidelines Nuke sparing Nukes Efavirenz placement as the gold standard ARV Role
HIV Treatment Update Anton Pozniak Consultant Physician, Director of HIV Services Chelsea and Westminster Hospital, London Guidelines Nuke sparing Nukes Efavirenz placement as the gold standard ARV Role
More Options, Some Opinions Initial Therapies for HIV Judith S. Currier, MD
 More Options, Some Opinions Initial Therapies for HIV Judith S. Currier, MD More Options, Some Opinions: Initial Therapies for HIV Judith S. Currier, MD University of California Los Angeles Los Angeles,
More Options, Some Opinions Initial Therapies for HIV Judith S. Currier, MD More Options, Some Opinions: Initial Therapies for HIV Judith S. Currier, MD University of California Los Angeles Los Angeles,
Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches
 Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches Harry W. Lampiris, MD Chief, Infectious Disease Section, San Francisco VA Medical Center Professor
Switching ARV Regimens: Managing Toxicity and Improving Tolerability; Switches & Class-Sparing Approaches Harry W. Lampiris, MD Chief, Infectious Disease Section, San Francisco VA Medical Center Professor
HIV - Therapy Principles
 HIV - Therapy Principles Manuel Battegay and Christine Katlama Basel, Switzerland and Paris, France Disclosure MB has received honoraria for advisory board participation from Gilead, MSD, Pfizer, ViiV
HIV - Therapy Principles Manuel Battegay and Christine Katlama Basel, Switzerland and Paris, France Disclosure MB has received honoraria for advisory board participation from Gilead, MSD, Pfizer, ViiV
STRIBILD (aka. The Quad Pill)
") NORTHWEST AIDS EDUCATION AND TRAINING CENTER STRIBILD (aka. The Quad Pill) Brian R. Wood, MD Medical Director, NW AETC ECHO Assistant Professor of Medicine, University of Washington Presentation prepared
NORTHWEST AIDS EDUCATION AND TRAINING CENTER STRIBILD (aka. The Quad Pill) Brian R. Wood, MD Medical Director, NW AETC ECHO Assistant Professor of Medicine, University of Washington Presentation prepared
Are the current doses of ARV correct. Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine
 Are the current doses of ARV correct Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine Can we lower doses of HIV meds safely? Consensus Panel in Alexandria
Are the current doses of ARV correct Richard Elion MD Associate Adjunct Clinical Professor of Medicine Johns Hopkins School of Medicine Can we lower doses of HIV meds safely? Consensus Panel in Alexandria
L infettivologia del 3 millennio: AIDS ed altro
 L infettivologia del 3 millennio: AIDS ed altro VI Convegno Nazionale 15-16 -17 maggio 2014 Centro Congressi Hotel Ariston Paestum (SA) Nuove molecole ad azione anti-hiv Annalisa Saracino Clinica Malattie
L infettivologia del 3 millennio: AIDS ed altro VI Convegno Nazionale 15-16 -17 maggio 2014 Centro Congressi Hotel Ariston Paestum (SA) Nuove molecole ad azione anti-hiv Annalisa Saracino Clinica Malattie
Antiretroviral Treatment Strategies: Clinical Case Presentation
 Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
Antiretroviral Treatment Strategies: Clinical Case Presentation Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan Chia-Jui, Yang M.D Disclosure No conflicts of interests.
HIV Treatment: State of the Art 2013
 HIV Treatment: State of the Art 2013 Daniel R. Kuritzkes, MD Chief, Division of Infectious Diseases Brigham and Women s Hospital Professor of Medicine Harvard Medical School Success of current ART Substantial
HIV Treatment: State of the Art 2013 Daniel R. Kuritzkes, MD Chief, Division of Infectious Diseases Brigham and Women s Hospital Professor of Medicine Harvard Medical School Success of current ART Substantial
Antiretroviral Treatment 2014
 Activity Code FM285 Antiretroviral Treatment 2014 Rajesh Gandhi, MD Masssachusetts General Hospital Disclosures: Educational grants to my institution from Janssen, Viiv, Abbott Learning Objectives Upon
Activity Code FM285 Antiretroviral Treatment 2014 Rajesh Gandhi, MD Masssachusetts General Hospital Disclosures: Educational grants to my institution from Janssen, Viiv, Abbott Learning Objectives Upon
Comprehensive Guideline Summary
 Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
Comprehensive Guideline Summary Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents AETC NRC Slide Set Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and
The next generation of ART regimens
 The next generation of ART regimens By Gary Maartens Presented by Dirk Hagemeister Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN KAAPSTAD Current state
The next generation of ART regimens By Gary Maartens Presented by Dirk Hagemeister Division of Clinical Pharmacology UNIVERSITY OF CAPE TOWN IYUNIVESITHI YASEKAPA UNIVERSITEIT VAN KAAPSTAD Current state
ART: The New, The Old and The Ugly
 ART: The New, The Old and The Ugly Our Current ARVS The Nucleoside/ Nucleotide Reverse Transcriptase Inhibitors (NRTIs/ NtRTIs) Abacavir Emtricitabine Lamivudine Stavudine Tenofovir Zidovudine The Non-Nucleoside
ART: The New, The Old and The Ugly Our Current ARVS The Nucleoside/ Nucleotide Reverse Transcriptase Inhibitors (NRTIs/ NtRTIs) Abacavir Emtricitabine Lamivudine Stavudine Tenofovir Zidovudine The Non-Nucleoside
Third Agent Advantages Disadvantages. Component Tenofovir/emtricitabine (TDF/FTC) 300/200 mg (coformulated with EFV as Atripla) 1 tab once daily
 300/200 mg (coformulated with EFV as Atripla) 1 tab once daily") Table I. Recommended and Alternative Antiretroviral Regimens (DHHS Guidelines, May 1, 2014) Recommended Regimens Nucleoside Analog Reverse Transcriptase Inhibitor (NRTI) Third Agent Advantages Disadvantages
Table I. Recommended and Alternative Antiretroviral Regimens (DHHS Guidelines, May 1, 2014) Recommended Regimens Nucleoside Analog Reverse Transcriptase Inhibitor (NRTI) Third Agent Advantages Disadvantages
Didactic Series. CROI 2014 Update. March 27, 2014
 Didactic Series CROI 2014 Update Christian Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director,
Didactic Series CROI 2014 Update Christian Ramers, MD, MPH Family Health Centers of San Diego Ciaccio Memorial Clinic Jacqueline Peterson Tulsky, MD UCSF Positive Health Program at SFGH Medical Director,
Antiretroviral Therapy: Current Recommendations, New Drugs, and Novel Strategies. Joel Gallant, MD, MPH Johns Hopkins University School of Medicine
 Antiretroviral Therapy: Current Recommendations, New Drugs, and Novel Strategies Joel Gallant, MD, MPH Johns Hopkins University School of Medicine Initial Regimen: DHHS Guidelines 3/27/2012 Preferred Regimens
Antiretroviral Therapy: Current Recommendations, New Drugs, and Novel Strategies Joel Gallant, MD, MPH Johns Hopkins University School of Medicine Initial Regimen: DHHS Guidelines 3/27/2012 Preferred Regimens
SINGLE. Efficacy and safety of dolutegravir (DTG) in treatment-naïve subjects
 in treatment-naïve subjects") SINGLE Efficacy and safety of dolutegravir (DTG) in treatment-naïve subjects SE/HIV/0023/14 January 2014 PHASE III DTG TRIALS IN TREATMENT-NAÏVE ADULT SUBJECTS WITH HIV SINGLE 1 N=833 Phase III non-inferiority,
SINGLE Efficacy and safety of dolutegravir (DTG) in treatment-naïve subjects SE/HIV/0023/14 January 2014 PHASE III DTG TRIALS IN TREATMENT-NAÏVE ADULT SUBJECTS WITH HIV SINGLE 1 N=833 Phase III non-inferiority,
Professor Jeffery Lennox
 BHIVA AUTUMN CONFERENCE 2014 Including CHIVA Parallel Sessions Professor Jeffery Lennox Emory University School of Medicine Atlanta, Georgia, USA 9-10 October 2014, Queen Elizabeth II Conference Centre,
BHIVA AUTUMN CONFERENCE 2014 Including CHIVA Parallel Sessions Professor Jeffery Lennox Emory University School of Medicine Atlanta, Georgia, USA 9-10 October 2014, Queen Elizabeth II Conference Centre,
Antiretroviral Therapy: When and What to Start. Joe Eron, MD University of North Carolina at Chapel Hill School of Medicine
 Antiretroviral Therapy: When and What to Start Joe Eron, MD University of North Carolina at Chapel Hill School of Medicine Learning Objectives As a results of participating in this activity participants
Antiretroviral Therapy: When and What to Start Joe Eron, MD University of North Carolina at Chapel Hill School of Medicine Learning Objectives As a results of participating in this activity participants
Qué anuncian los nuevos trials?
 Qué anuncian los nuevos trials? XVII Curso Nacional VIH/SIDA Sociedad Chilena de Infectología Agosto 2014 Dr. Carlos Beltrán Hospital Barros Luco Trudeau Universidad de Santiago Grupo SidaChile El presente
Qué anuncian los nuevos trials? XVII Curso Nacional VIH/SIDA Sociedad Chilena de Infectología Agosto 2014 Dr. Carlos Beltrán Hospital Barros Luco Trudeau Universidad de Santiago Grupo SidaChile El presente
TDF containing ART: Efficacy and Safety. Dr Lloyd B. Mulenga Adult Infectious Diseases Centre University Teaching Hospital Lusaka, Zambia
 TDF containing ART: Efficacy and Safety Dr Lloyd B. Mulenga Adult Infectious Diseases Centre University Teaching Hospital Lusaka, Zambia 1 Indications Treatment of HIV-1 in combination with other antiretroviral
TDF containing ART: Efficacy and Safety Dr Lloyd B. Mulenga Adult Infectious Diseases Centre University Teaching Hospital Lusaka, Zambia 1 Indications Treatment of HIV-1 in combination with other antiretroviral
INTERGRASE INHIBITORS- WHAT S NEW?
 INTERGRASE INHIBITORS- WHAT S NEW? Professor Margaret Johnson Royal Free London Foundation Trust October 2018 Targeting the HIV life-cycle NEW HIV VIRON MATURATION CO-RECEPTOR BINDING FUSION BUDDING CD4
INTERGRASE INHIBITORS- WHAT S NEW? Professor Margaret Johnson Royal Free London Foundation Trust October 2018 Targeting the HIV life-cycle NEW HIV VIRON MATURATION CO-RECEPTOR BINDING FUSION BUDDING CD4
HIV Treatment: New and Veteran Drugs Classes
 HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
HIV Treatment: New and Veteran Drugs Classes Jonathan M Schapiro, MD National Hemophilia Center Stanford University School of Medicine Rome, March 2013 Overview Many excellent antiretroviral agents are
Clinical support for reduced drug regimens. David A Cooper The University of New South Wales Sydney, Australia
 Clinical support for reduced drug regimens David A Cooper The University of New South Wales Sydney, Australia Clinical support for reduced drug regimens First line optimisation Virological failure New
Clinical support for reduced drug regimens David A Cooper The University of New South Wales Sydney, Australia Clinical support for reduced drug regimens First line optimisation Virological failure New
2017 NSTC Annual Meeting Eric Daar April 18, 2017
 Antiretroviral Therapy Update for TB Clinicians Eric S. Daar, M.D. Chief, Division of HIV Medicine Harbor-UCLA Medical Center Professor of Medicine David Geffen School of Medicine at UCLA Grants Consultant
Antiretroviral Therapy Update for TB Clinicians Eric S. Daar, M.D. Chief, Division of HIV Medicine Harbor-UCLA Medical Center Professor of Medicine David Geffen School of Medicine at UCLA Grants Consultant
BHIVA Best of CROI Feedback Meetings. London Birmingham North West England Cardiff Gateshead Edinburgh
 BHIVA Best of CROI Feedback Meetings London Birmingham North West England Cardiff Gateshead Edinburgh BHIVA Best of CROI Feedback Meetings 2010 ANTIRETROVIRAL TREATMENT STRATEGIES AND NEW DRUGS A5202:
BHIVA Best of CROI Feedback Meetings London Birmingham North West England Cardiff Gateshead Edinburgh BHIVA Best of CROI Feedback Meetings 2010 ANTIRETROVIRAL TREATMENT STRATEGIES AND NEW DRUGS A5202:
The Use of Integrase Inhibitors In Latin America: From Guidelines to the Real World Ernesto Martínez B., MD Internal Medicine, Infectious Diseases
 De afbeelding kan niet worden weergegeven. The Use of Integrase Inhibitors In Latin America: From Guidelines to the Real World Ernesto Martínez B., MD Internal Medicine, Infectious Diseases DISCLOSURE
De afbeelding kan niet worden weergegeven. The Use of Integrase Inhibitors In Latin America: From Guidelines to the Real World Ernesto Martínez B., MD Internal Medicine, Infectious Diseases DISCLOSURE
State of the ART: Integrase Inhibitors Clinical Data. Juan Berenguer Hospital General Universitario Gregorio Marañón (IiSGM) Madrid, Spain
 Madrid, Spain") State of the ART: Integrase Inhibitors Clinical Data Juan Berenguer Hospital General Universitario Gregorio Marañón (IiSGM) Madrid, Spain Disclosures Consulting fees and honoraria Gilead, Janssen, MSD,
State of the ART: Integrase Inhibitors Clinical Data Juan Berenguer Hospital General Universitario Gregorio Marañón (IiSGM) Madrid, Spain Disclosures Consulting fees and honoraria Gilead, Janssen, MSD,
Antiretroviral Therapy in 2016
 Antiretroviral Therapy in 2016 Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, NM University of New Mexico School of Medicine Johns Hopkins University School of Medicine Disclosures Consulting, Advisory
Antiretroviral Therapy in 2016 Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, NM University of New Mexico School of Medicine Johns Hopkins University School of Medicine Disclosures Consulting, Advisory
Terapia del paciente naive con un régimen de Inhibidor de la proteasa Dr. Jose R Arribas IX Curso de avances en Infección VIH y hepatitis virales
 Terapia del paciente naive con un régimen de Inhibidor de la proteasa Dr. Jose R Arribas IX Curso de avances en Infección VIH y hepatitis virales clinicaloptions.com/hiv Eficacia en Ensayos Clínicos pivotales
Terapia del paciente naive con un régimen de Inhibidor de la proteasa Dr. Jose R Arribas IX Curso de avances en Infección VIH y hepatitis virales clinicaloptions.com/hiv Eficacia en Ensayos Clínicos pivotales
Simplifying Antiretroviral Therapy Regimens: It s not so simple
 Simplifying Antiretroviral Therapy Regimens: It s not so simple Jonathan Colasanti, MD, MSPH Division of Infectious Diseases Emory University School of Medicine Disclosures No Financial Disclosures Parts
Simplifying Antiretroviral Therapy Regimens: It s not so simple Jonathan Colasanti, MD, MSPH Division of Infectious Diseases Emory University School of Medicine Disclosures No Financial Disclosures Parts
DRUGS IN PIPELINE. Pr JC YOMBI UCL-AIDS REFERENCE CENTRE BREACH Sept 27, 2015
 DRUGS IN PIPELINE Pr JC YOMBI UCL-AIDS REFERENCE CENTRE BREACH Sept 27, 2015 N(t)RTI The Development of TAF TAF Delivers the High Potency of TDF While Minimizing Off- Target Kidney and Bone Side Effects
DRUGS IN PIPELINE Pr JC YOMBI UCL-AIDS REFERENCE CENTRE BREACH Sept 27, 2015 N(t)RTI The Development of TAF TAF Delivers the High Potency of TDF While Minimizing Off- Target Kidney and Bone Side Effects
HIV Treatment Update 8/3/2015. When to Start. Disclosures
 8/3/215 HIV Treatment Update Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, NM University of New Mexico School of Medicine Johns Hopkins University School of Medicine Disclosures Consulting, Advisory
8/3/215 HIV Treatment Update Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, NM University of New Mexico School of Medicine Johns Hopkins University School of Medicine Disclosures Consulting, Advisory
Bon Usage des Antirétroviraux dans l Infection par le VIH
 Bon Usage des Antirétroviraux dans l Infection par le VIH Pr. Jean-Michel Molina CHU St Louis, Assistance Publique Hôpitaux de Paris, INSERM U941 et Université Paris 7 Diderot, France 1 Liens d Intérêt
Bon Usage des Antirétroviraux dans l Infection par le VIH Pr. Jean-Michel Molina CHU St Louis, Assistance Publique Hôpitaux de Paris, INSERM U941 et Université Paris 7 Diderot, France 1 Liens d Intérêt
Drug toxicities: Safest PIs. Michelle Moorhouse 14 Apr 2016
 Drug toxicities: Safest PIs Michelle Moorhouse 14 Apr 2016 Impact of PIs on AIDS mortality CDC.gov. Epidemiology of HIV infection. Evolution of PIs http://www.clinicaloptions.com/hiv/treatment%20updates/boosted%20pis/interactive%20virtual%20presentation/slideset.aspx
Drug toxicities: Safest PIs Michelle Moorhouse 14 Apr 2016 Impact of PIs on AIDS mortality CDC.gov. Epidemiology of HIV infection. Evolution of PIs http://www.clinicaloptions.com/hiv/treatment%20updates/boosted%20pis/interactive%20virtual%20presentation/slideset.aspx
Virological suppression and PIs. Diego Ripamonti Malattie Infettive - Bergamo
 Virological suppression and PIs Diego Ripamonti Malattie Infettive - Bergamo Ritonavir-boosted PIs Boosted PIs: 3 drugs in one The intrinsic antiretroviral activity Viral suppression and high baseline
Virological suppression and PIs Diego Ripamonti Malattie Infettive - Bergamo Ritonavir-boosted PIs Boosted PIs: 3 drugs in one The intrinsic antiretroviral activity Viral suppression and high baseline
SELECTING THE BEST ART FOR EACH PATIENT
 SELECTING THE BEST ART FOR EACH PATIENT Corklin R Steinhart, MD, PhD Head, Global Medical Directors ViiV Healthcare CNVX/HIVP/0025/16 5th Asian Conference on Hepatitis & AIDS 第五届亚洲肝炎与艾滋病学术会议 28-29 May
SELECTING THE BEST ART FOR EACH PATIENT Corklin R Steinhart, MD, PhD Head, Global Medical Directors ViiV Healthcare CNVX/HIVP/0025/16 5th Asian Conference on Hepatitis & AIDS 第五届亚洲肝炎与艾滋病学术会议 28-29 May
Switching antiretroviral therapy to safer strategies based on integrase inhibitors
 Switching antiretroviral therapy to safer strategies based on integrase inhibitors Dr Paddy Mallon UCD HIV Molecular Research Group UCD School of Medicine paddy.mallon@ucd.ie UCD School of Medicine & Medical
Switching antiretroviral therapy to safer strategies based on integrase inhibitors Dr Paddy Mallon UCD HIV Molecular Research Group UCD School of Medicine paddy.mallon@ucd.ie UCD School of Medicine & Medical
Update on HIV Drug Resistance. Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School
 Update on HIV Drug Resistance Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Learning Objectives Upon completion of this presentation, learners
Update on HIV Drug Resistance Daniel R. Kuritzkes, MD Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Learning Objectives Upon completion of this presentation, learners
Individual Study Table Referring to the Dossier SYNOPSIS. Final Clinical Study Report for Study AI424138
 Name of Sponsor/Company: Bristol-Myers Squibb Name of Finished Product: Reyataz Name of Active Ingredient: Atazanavir () Individual Study Table Referring to the Dossier (For National Authority Use Only)
Name of Sponsor/Company: Bristol-Myers Squibb Name of Finished Product: Reyataz Name of Active Ingredient: Atazanavir () Individual Study Table Referring to the Dossier (For National Authority Use Only)
HIV: Approach to the Treatment-Naïve Patient
 HIV: Approach to the Treatment-Naïve Patient Paul E. Sax, M.D. Clinical Director, Division of Infectious Diseases Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Approach
HIV: Approach to the Treatment-Naïve Patient Paul E. Sax, M.D. Clinical Director, Division of Infectious Diseases Brigham and Women s Hospital Associate Professor of Medicine Harvard Medical School Approach
ART Treatment. ART Treatment
 Naïve Experienced Strategies ARV in pregnancy ART Treatment Naïve studies: ART Treatment Abstract 37 Atazanavir/r vs Lopinavir/r: Castle study Abstract 774 Kivexa vs Truvada: HEAT study Abstract 775 Lopinavir/r
Naïve Experienced Strategies ARV in pregnancy ART Treatment Naïve studies: ART Treatment Abstract 37 Atazanavir/r vs Lopinavir/r: Castle study Abstract 774 Kivexa vs Truvada: HEAT study Abstract 775 Lopinavir/r
Integrase Inhibitors in the Treatment HIV-Infection. Andrew Zolopa, MD Stanford University
 Integrase Inhibitors in the Treatment HIV-Infection Andrew Zolopa, MD Stanford University 1 IAS-USA 212 Guidelines Updated Recommendations When to start ART is now recommended for all patients, regardless
Integrase Inhibitors in the Treatment HIV-Infection Andrew Zolopa, MD Stanford University 1 IAS-USA 212 Guidelines Updated Recommendations When to start ART is now recommended for all patients, regardless
Switching antiretroviral therapy to safer strategies based on integrase inhibitors. Pedro Cahn
 Switching antiretroviral therapy to safer strategies based on integrase inhibitors Pedro Cahn Disclosures Research Grants: Abbvie-Merck-Richmond-ViiV Advisory boards: Merck-Sandoz-ViiV Switching in Virologically
Switching antiretroviral therapy to safer strategies based on integrase inhibitors Pedro Cahn Disclosures Research Grants: Abbvie-Merck-Richmond-ViiV Advisory boards: Merck-Sandoz-ViiV Switching in Virologically
Antiretroviral Therapy in Joel Gallant, MD, MPH Johns Hopkins University School of Medicine
 Antiretroviral Therapy in 2013 Joel Gallant, MD, MPH Johns Hopkins University School of Medicine When to Start When to Start: DHHS Guidelines, February 2013 ART recommended for all HIV+ individuals to
Antiretroviral Therapy in 2013 Joel Gallant, MD, MPH Johns Hopkins University School of Medicine When to Start When to Start: DHHS Guidelines, February 2013 ART recommended for all HIV+ individuals to
CROI 2017 Review: Novel ART Strategies
 Mountain West AIDS Education and Training Center CROI 2017 Review: Novel ART Strategies Brian R. Wood, MD Assistant Professor of Medicine Medical Director, Mountain West AETC ECHO Telehealth March 2, 2017
Mountain West AIDS Education and Training Center CROI 2017 Review: Novel ART Strategies Brian R. Wood, MD Assistant Professor of Medicine Medical Director, Mountain West AETC ECHO Telehealth March 2, 2017
Introduction. Cahn et al. Andean Pacific HIV Clinical Forum 2017; Santiago, Chile. Abstract 2.
 Efficacy of Dolutegravir/Abacavir/Lamivudine (DTG/ABC/3TC) Fixed Dose Combination (FDC) Compared With Ritonavir- Boosted Atazanavir (ATV/r) Plus Tenofovir Disoproxil Fumarate/Emtricitabine (TDF/FTC) in
Efficacy of Dolutegravir/Abacavir/Lamivudine (DTG/ABC/3TC) Fixed Dose Combination (FDC) Compared With Ritonavir- Boosted Atazanavir (ATV/r) Plus Tenofovir Disoproxil Fumarate/Emtricitabine (TDF/FTC) in
Highlights of AIDS 2012 CCO Official Conference Coverage of the XIX International AIDS Conference
 Highlights of AIDS 2012 CCO Official Conference Coverage of the XIX International AIDS Conference July 22-27, 2012 Washington, DC Sylvia Ojoo, MRCP UK Clinical Assistant Professor of Medicine University
Highlights of AIDS 2012 CCO Official Conference Coverage of the XIX International AIDS Conference July 22-27, 2012 Washington, DC Sylvia Ojoo, MRCP UK Clinical Assistant Professor of Medicine University
1/13/16. Updated April 2015
 Bernadette Jakeman, PharmD, PhC, BCPS, AAHIVP Assistant Professor UNM College of Pharmacy bjakeman@salud.unm.edu Pharmacist objectives: 1. Summarize key updates to the DHHS treatment guidelines. 2. Identify
Bernadette Jakeman, PharmD, PhC, BCPS, AAHIVP Assistant Professor UNM College of Pharmacy bjakeman@salud.unm.edu Pharmacist objectives: 1. Summarize key updates to the DHHS treatment guidelines. 2. Identify
Selecting an Initial Antiretroviral Therapy (ART) Regimen
 Regimen") Selecting an Initial Antiretroviral Therapy (ART) Regimen An HIV Diagnosis is a Call to Action In support of the NYSDOH AIDS Institute s January 2018 call to action for patients newly diagnosed with HIV,
Selecting an Initial Antiretroviral Therapy (ART) Regimen An HIV Diagnosis is a Call to Action In support of the NYSDOH AIDS Institute s January 2018 call to action for patients newly diagnosed with HIV,
Case # 1. Case #1 (cont d)
") Antiretroviral Therapy Management: Expert Panel Discussion George Beatty Susa Coffey Steve O Brien December 3, 2011 Moderated by Annie Luetkemeyer Case # 1 38 y.o. man, CD4 =350, VL=340K, new to your clinic
Antiretroviral Therapy Management: Expert Panel Discussion George Beatty Susa Coffey Steve O Brien December 3, 2011 Moderated by Annie Luetkemeyer Case # 1 38 y.o. man, CD4 =350, VL=340K, new to your clinic
TUESDAY AM HIV DISCUSSION SERIES. 8/25/2015 Management of Treatment-Naïve Patients Ellen Kitchell, M.D.
 TUESDAY AM HIV DISCUSSION SERIES 8/25/2015 Management of Treatment-Naïve Patients Ellen Kitchell, M.D. HAART Initiation/HIV Treatment for Antiretroviral-Naïve Patients Ellen Kitchell, M.D. The Art of HAART
TUESDAY AM HIV DISCUSSION SERIES 8/25/2015 Management of Treatment-Naïve Patients Ellen Kitchell, M.D. HAART Initiation/HIV Treatment for Antiretroviral-Naïve Patients Ellen Kitchell, M.D. The Art of HAART
Treating HIV: When the Guidelines Don t Fit. Joel Gallant, MD, MPH. Southwest CARE Center Santa Fe, New Mexico
 Treating HIV: When the Guidelines Don t Fit Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, New Mexico Johns Hopkins University School of Medicine University of New Mexico School of Medicine Disclosures
Treating HIV: When the Guidelines Don t Fit Joel Gallant, MD, MPH Southwest CARE Center Santa Fe, New Mexico Johns Hopkins University School of Medicine University of New Mexico School of Medicine Disclosures
VIKING STUDIES Efficacy and safety of dolutegravir in treatment-experienced subjects
 VIKING STUDIES Efficacy and safety of dolutegravir in treatment-experienced subjects IL/DLG/0040/14 June 2014 GSK (Israel) Ltd. Basel 25, Petach Tikva. Tel-03-9297100 Medical information service: il.medinfo@gsk.com
VIKING STUDIES Efficacy and safety of dolutegravir in treatment-experienced subjects IL/DLG/0040/14 June 2014 GSK (Israel) Ltd. Basel 25, Petach Tikva. Tel-03-9297100 Medical information service: il.medinfo@gsk.com
12th European AIDS Conference / EACS ARV Therapies and Therapeutic Strategies A CME Newsletter
 EACS 2009 11-14, November 2009 Cologne, Germany Course Director Jürgen K. Rockstroh, MD Co-Chairman, 12th European AIDS Conference Professor, University of Bonn Bonn, Germany Faculty Calvin Cohen, MD,
EACS 2009 11-14, November 2009 Cologne, Germany Course Director Jürgen K. Rockstroh, MD Co-Chairman, 12th European AIDS Conference Professor, University of Bonn Bonn, Germany Faculty Calvin Cohen, MD,
Treatment strategies for the developing world
 David A Cooper National Centre in HIV Epidemiology and Clinical Research The University of New South Wales Sydney, Australia First line standard of care First line in the developing world First line failure
David A Cooper National Centre in HIV Epidemiology and Clinical Research The University of New South Wales Sydney, Australia First line standard of care First line in the developing world First line failure
Second-Line Therapy NORTHWEST AIDS EDUCATION AND TRAINING CENTER
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Second-Line Therapy David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious Diseases University of Washington Presentation
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Second-Line Therapy David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, Division of Infectious Diseases University of Washington Presentation
Antiretroviral Drugs
 Antiretroviral Drugs Dr Paddy Mallon UCD HIV Molecular Research Group Associate Dean for Research and Innovation UCD School of Medicine and Medical Science paddy.mallon@ucd.ie UCD School of Medicine &
Antiretroviral Drugs Dr Paddy Mallon UCD HIV Molecular Research Group Associate Dean for Research and Innovation UCD School of Medicine and Medical Science paddy.mallon@ucd.ie UCD School of Medicine &
ARVs in Development: Where do they fit?
 The picture can't be displayed. ARVs in Development: Where do they fit? Daniel R. Kuritzkes, M.D. Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Disclosures The speaker
The picture can't be displayed. ARVs in Development: Where do they fit? Daniel R. Kuritzkes, M.D. Division of Infectious Diseases Brigham and Women s Hospital Harvard Medical School Disclosures The speaker
Crafting an ART Regimen for Initiation or Salvage: Are NRTI s Necessary?
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Crafting an ART Regimen for Initiation or Salvage: Are NRTI s Necessary? Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Crafting an ART Regimen for Initiation or Salvage: Are NRTI s Necessary? Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical
Real Life Experience of Dolutegravir and Lamivudine Dual Therapy As a Switching Regimen in HIVTR Cohort
 Real Life Experience of Dolutegravir and Lamivudine Dual Therapy As a Switching Regimen in HIVTR Cohort Yagci-Caglayik D 1, Gokengin D 2, Inan A 3, Ozkan-Ozdemir H 4, Inan D 5, Akbulut A 6, Korten V 1,
Real Life Experience of Dolutegravir and Lamivudine Dual Therapy As a Switching Regimen in HIVTR Cohort Yagci-Caglayik D 1, Gokengin D 2, Inan A 3, Ozkan-Ozdemir H 4, Inan D 5, Akbulut A 6, Korten V 1,
The BATAR Study Boosted Atazanavir Truvada vs. Atazanavir Raltegravir
 The BATAR Study Boosted Atazanavir Truvada vs. Atazanavir Raltegravir A Pilot Study of the Novel Antiretroviral Combination of Atazanavir and Raltegravir in HIV-1 Infected Subjects with Virologic Suppression
The BATAR Study Boosted Atazanavir Truvada vs. Atazanavir Raltegravir A Pilot Study of the Novel Antiretroviral Combination of Atazanavir and Raltegravir in HIV-1 Infected Subjects with Virologic Suppression
BHIVA guidelines on the treatment of HIV-1-positive adults with antiretroviral therapy. START & other changes
 BHIVA guidelines on the treatment of HIV-1-positive adults with antiretroviral therapy START & other changes Contents Introduction & treatment aims Major changes When to start What to start BHIVA: what
BHIVA guidelines on the treatment of HIV-1-positive adults with antiretroviral therapy START & other changes Contents Introduction & treatment aims Major changes When to start What to start BHIVA: what
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines
 The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy, M. Boucher and D. Money For and
Antiretroviral Therapy: Panel Discussion
 disclosures Antiretroviral Therapy: Panel Discussion Medical Management of HIV December 9, 217 Panelists: Harry Lampiris, MD; Annie Luetkemeyer, MD; Carina Marquez, MD Moderator: Oliver Bacon, MD none
disclosures Antiretroviral Therapy: Panel Discussion Medical Management of HIV December 9, 217 Panelists: Harry Lampiris, MD; Annie Luetkemeyer, MD; Carina Marquez, MD Moderator: Oliver Bacon, MD none
Josep Mallolas Hospital Clínic Barcelona
 Nuevos paradigmas en la infección VIH Josep Mallolas Hospital Clínic Barcelona 1. Do you believe, I have to start ARV therapy? Incidence and Mortality of AIDS in Spain HIV and NON-AIDS complications HIV
Nuevos paradigmas en la infección VIH Josep Mallolas Hospital Clínic Barcelona 1. Do you believe, I have to start ARV therapy? Incidence and Mortality of AIDS in Spain HIV and NON-AIDS complications HIV
Case 1 continued. Case 1 (cont) 12/8/16. MMAH Debate Panel Thursday, December 8, Case 1
 12/8/16. MMAH Debate Panel Thursday, December 8, Case 1") MMAH Debate Panel Thursday, December 8, 2016 Case 1 HPI 55 yo man with newly diagnosed HIV initiates care in your clinic. His CD4+ cell count is 600, with HIV VL=90,000 copies/ml. He is asymptomatic at
MMAH Debate Panel Thursday, December 8, 2016 Case 1 HPI 55 yo man with newly diagnosed HIV initiates care in your clinic. His CD4+ cell count is 600, with HIV VL=90,000 copies/ml. He is asymptomatic at
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents
 Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Guidelines for the Use of Antiretroviral Agents in HIV-1-Infected Adults and Adolescents Visit the AIDSinfo website to access the most up-to-date guideline. Register for e-mail notification of guideline
Advances in HIV Treatment: When to Start Treatment Which Antivirals to Use
 Advances in HIV Treatment: When to Start Treatment Which Antivirals to Use Calvin Cohen MD Harvard Vanguard Medical Associates CRI New England Vice Chair, Science Steering Cmte, INSIGHT Boston MA Learning
Advances in HIV Treatment: When to Start Treatment Which Antivirals to Use Calvin Cohen MD Harvard Vanguard Medical Associates CRI New England Vice Chair, Science Steering Cmte, INSIGHT Boston MA Learning
The results of the ARTEN study. Vicente Soriano Hospital Carlos III, Madrid, Spain
 The results of the ARTEN study Vicente Soriano Hospital Carlos III, Madrid, Spain Nevirapine: a well-defined efficacy and tolerability profile High efficacy levels 1 3 Well-defined safety profile 4 Favourable
The results of the ARTEN study Vicente Soriano Hospital Carlos III, Madrid, Spain Nevirapine: a well-defined efficacy and tolerability profile High efficacy levels 1 3 Well-defined safety profile 4 Favourable
Susan L. Koletar, MD
 HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
HIV/AIDS Susan L. Koletar, MD Division Director, Infectious Diseases Professor of Internal Medicine Department of Internal Medicine The Ohio State University Wexner Medical Center HIV through the Decades
First-Line Antiretroviral Therapy for Treatment and Prevention:
 First-Line Antiretroviral Therapy for Treatment and Prevention: The Past, Present and Future Best Options Joel Gallant, MD, MPH Johns Hopkins University School of Medicine IAS-USA Guidelines 7/2008: When
First-Line Antiretroviral Therapy for Treatment and Prevention: The Past, Present and Future Best Options Joel Gallant, MD, MPH Johns Hopkins University School of Medicine IAS-USA Guidelines 7/2008: When
HIV Update. On The Cutting Edge A Chronic Disease. Rhett M Shirley, MD
 HIV Update On The Cutting Edge A Chronic Disease Rhett M Shirley, MD CDC Mid-point life expectancy estimates at age 20 years in three calendar periods, overall and by sociodemographic characteristics,
HIV Update On The Cutting Edge A Chronic Disease Rhett M Shirley, MD CDC Mid-point life expectancy estimates at age 20 years in three calendar periods, overall and by sociodemographic characteristics,
Antiretroviral Treatment: What's in the Pipeline
 Antiretroviral Treatment: What's in the Pipeline Joseph P. McGowan, MD, FACP, FIDSA Professor of Medicine Hofstra North Shore-LIJ School of Medicine October 14, 2015 Which describes best how HIV Maturation
Antiretroviral Treatment: What's in the Pipeline Joseph P. McGowan, MD, FACP, FIDSA Professor of Medicine Hofstra North Shore-LIJ School of Medicine October 14, 2015 Which describes best how HIV Maturation
Abstract PS8/2. Double-blind treatment phase D/C/F/TAF. + matching D/C + F/TDF placebo D/C/F/TAF. D/C + F/TDF + matching D/C/F/TAF placebo
 WEEK 8 RESULTS OF AMBER: A PHASE 3, RANDOMISED, DOUBLE-BLIND TRIAL IN ANTIRETROVIRAL TREATMENT (ART)-NAÏVE HIV--INFECTED ADULTS TO EVALUATE THE EFFICACY AND SAFETY OF THE ONCE-DAILY, SINGLE-TABLET REGIMEN
WEEK 8 RESULTS OF AMBER: A PHASE 3, RANDOMISED, DOUBLE-BLIND TRIAL IN ANTIRETROVIRAL TREATMENT (ART)-NAÏVE HIV--INFECTED ADULTS TO EVALUATE THE EFFICACY AND SAFETY OF THE ONCE-DAILY, SINGLE-TABLET REGIMEN
First line ART Rilpirivine A New NNRTI. Chris Jack Physician, Durdoc Centre ethekwini
 First line ART Rilpirivine A New NNRTI Chris Jack Physician, Durdoc Centre ethekwini Overview: Rilpirivine an option for ARV Naïve patients History Current guidelines Efficacy and Safety Tolerability /
First line ART Rilpirivine A New NNRTI Chris Jack Physician, Durdoc Centre ethekwini Overview: Rilpirivine an option for ARV Naïve patients History Current guidelines Efficacy and Safety Tolerability /
D:A:D: Cumulative Exposure to DRV/r Increase MI Risk
 D:A:D: Cumulative Exposure to DRV/r Increase MI Risk 20.0-15.0-10.0-5.0-4.0-3.0-2.0-1.0- Unadjusted CVD rate ratios per 5 years additional exposure: ATV/r 1.25 [1.10-1.43] and DRV/r 1.93 [1.63-2.28] Adjusted*
D:A:D: Cumulative Exposure to DRV/r Increase MI Risk 20.0-15.0-10.0-5.0-4.0-3.0-2.0-1.0- Unadjusted CVD rate ratios per 5 years additional exposure: ATV/r 1.25 [1.10-1.43] and DRV/r 1.93 [1.63-2.28] Adjusted*
Pharmacological considerations on the use of ARVs in pregnancy
 Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
Pharmacological considerations on the use of ARVs in pregnancy 11 th Residential Course on Clinical Pharmacology of Antiretrovirals Torino, 20-22 January 2016 Prof. David Burger, PharmD, PhD david.burger@radboudumc.nl
Didactic Series. CROI New Antiretroviral Therapies. Daniel Lee, MD Clinical Professor of Medicine UCSD Medical Center Owen Clinic July 14, 2016
 Didactic Series CROI 2016 - New Antiretroviral Therapies Daniel Lee, MD Clinical Professor of Medicine UCSD Medical Center Owen Clinic July 14, 2016 This project is supported by the Health Resources and
Didactic Series CROI 2016 - New Antiretroviral Therapies Daniel Lee, MD Clinical Professor of Medicine UCSD Medical Center Owen Clinic July 14, 2016 This project is supported by the Health Resources and
Tenofovir Alafenamide (TAF)
") Frontier AIDS Education and Training Center Tenofovir Alafenamide (TAF) Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director, Frontier AETC ECHO January 28, 2016
Frontier AIDS Education and Training Center Tenofovir Alafenamide (TAF) Brian R. Wood, MD Assistant Professor of Medicine, University of Washington Medical Director, Frontier AETC ECHO January 28, 2016
New HIV EACS and Italian Guidelines
 Original Article HIV correlated pathologies and other infections Marco Borderi New HIV EACS and Italian Guidelines Infectious Disease Unit - S. Orsola-Hospital - University of Bologna Corresponding author:
Original Article HIV correlated pathologies and other infections Marco Borderi New HIV EACS and Italian Guidelines Infectious Disease Unit - S. Orsola-Hospital - University of Bologna Corresponding author:
Perspectivesconcernantles InhibiteursNon Nucléosidiquesde la Transcriptase Inverse (INNTI)
") Perspectivesconcernantles InhibiteursNon Nucléosidiquesde la Transcriptase Inverse (INNTI) Gianni Di Perri Dept. de Maladies Infectieuses Universitè de Turin Ospedale Amedeo di Savoia Fusion inhibitors
Perspectivesconcernantles InhibiteursNon Nucléosidiquesde la Transcriptase Inverse (INNTI) Gianni Di Perri Dept. de Maladies Infectieuses Universitè de Turin Ospedale Amedeo di Savoia Fusion inhibitors
IAC Analyst Presentation
 IAC Analyst Presentation David Redfern Chairman, ViiV Healthcare Chief Strategy Officer, GSK July 27, 2012 1 ViiV Healthcare Dr Dominique Limet CEO, ViiV Healthcare July 27, 2012 2 Equity split of 85%
IAC Analyst Presentation David Redfern Chairman, ViiV Healthcare Chief Strategy Officer, GSK July 27, 2012 1 ViiV Healthcare Dr Dominique Limet CEO, ViiV Healthcare July 27, 2012 2 Equity split of 85%
COMPETING INTEREST OF FINANCIAL VALUE
 BHIVA AUTUMN CONFERENCE 2012 Including CHIVA Parallel Sessions Dr Ian Williams University College London Medical School COMPETING INTEREST OF FINANCIAL VALUE > 1,000: Speaker Name Statement Ian Williams
BHIVA AUTUMN CONFERENCE 2012 Including CHIVA Parallel Sessions Dr Ian Williams University College London Medical School COMPETING INTEREST OF FINANCIAL VALUE > 1,000: Speaker Name Statement Ian Williams
2/16/2017. Management and Prevention of HIV Infection: Case Discussion. Case 1. Case 1
 Management and Prevention of HIV Infection: Case Discussion Eric S. Daar, M.D. Chief, Division of HIV Medicine Harbor-UCLA Medical Center Professor of Medicine David Geffen School of Medicine at UCLA Grant
Management and Prevention of HIV Infection: Case Discussion Eric S. Daar, M.D. Chief, Division of HIV Medicine Harbor-UCLA Medical Center Professor of Medicine David Geffen School of Medicine at UCLA Grant
Faculty. Robert LoNigro, MD, MS SVP and Chief Clinical Officer Envolve PeopleCare Austin, TX
 Learning Objectives Investigate the impact of antiretroviral therapy selection on factors that influence therapeutic effectiveness in patients with HIV, such as adherence, drug resistance, and safety.
Learning Objectives Investigate the impact of antiretroviral therapy selection on factors that influence therapeutic effectiveness in patients with HIV, such as adherence, drug resistance, and safety.
Cases from the Clinic(ians): Case-Based Panel Discussion
: Case-Based Panel Discussion") Cases from the Clinic(ians): Case-Based Panel Discussion Michael S. Saag, MD Professor of Medicine The University of Alabama at Birmingham EDITED: 03-12-14 Learning Objectives After attending this presentation,
Cases from the Clinic(ians): Case-Based Panel Discussion Michael S. Saag, MD Professor of Medicine The University of Alabama at Birmingham EDITED: 03-12-14 Learning Objectives After attending this presentation,
CROI 2018 Report Back
 CROI 2018 Report Back Monika Roy, MD MAS Assistant Professor Division of HIV, Infectious Diseases, and Global Medicine bayareaaetc.org 1 Disclosures and Conflicts of Interest Nothing to report bayareaaetc.org
CROI 2018 Report Back Monika Roy, MD MAS Assistant Professor Division of HIV, Infectious Diseases, and Global Medicine bayareaaetc.org 1 Disclosures and Conflicts of Interest Nothing to report bayareaaetc.org
Didactic Series. Switching Regimens in the Setting of Virologic Suppression
 Didactic Series Switching Regimens in the Setting of Virologic Suppression Craig Ballard, PharmD, AAHIVP UC San Diego Health Owen Clinic June 14 th, 2018 1 Learning Objectives 1) Describe DHHS guidelines
Didactic Series Switching Regimens in the Setting of Virologic Suppression Craig Ballard, PharmD, AAHIVP UC San Diego Health Owen Clinic June 14 th, 2018 1 Learning Objectives 1) Describe DHHS guidelines
Stribild, a Single Tablet Regimen for the Treatment of HIV Disease
 Comb Prod Ther (2013) 3:1 8 DOI 10.1007/s13556-013-0001-y REVIEW Stribild, a Single Tablet Regimen for the Treatment of HIV Disease Cynthia Brinson To view enhanced content go to www.combitherapy-open.com
Comb Prod Ther (2013) 3:1 8 DOI 10.1007/s13556-013-0001-y REVIEW Stribild, a Single Tablet Regimen for the Treatment of HIV Disease Cynthia Brinson To view enhanced content go to www.combitherapy-open.com
Eviplera: New First-Line Treatment Options for patients with HIV (own clinical experience in Izrael) Itsik Levy MD
 Itsik Levy MD") Eviplera: New First-Line Treatment Options for patients with HIV (own clinical experience in Izrael) Itsik Levy MD Population: 8,000,000 Ethnic groups: 75% Jewish 20% Arabs 5% Others HCS PPC 3.5/1000 NPC
Eviplera: New First-Line Treatment Options for patients with HIV (own clinical experience in Izrael) Itsik Levy MD Population: 8,000,000 Ethnic groups: 75% Jewish 20% Arabs 5% Others HCS PPC 3.5/1000 NPC
Management of ART Failure. EACS Advanced HIV Course 2015 Dr Nicky Mackie
 Management of ART Failure EACS Advanced HIV Course 2015 Dr Nicky Mackie Outline Defining treatment success Defining treatment failure Reasons for ART failure Management of ART failure Choice of second
Management of ART Failure EACS Advanced HIV Course 2015 Dr Nicky Mackie Outline Defining treatment success Defining treatment failure Reasons for ART failure Management of ART failure Choice of second
Professor José Arribas
 19 th Annual Conference of the British HIV Association (BHIVA) Professor José Arribas Hospital La Paz, Madrid, Spain 16-19 April 2013, Manchester Central Convention Complex Can we live without nucleosides?
19 th Annual Conference of the British HIV Association (BHIVA) Professor José Arribas Hospital La Paz, Madrid, Spain 16-19 April 2013, Manchester Central Convention Complex Can we live without nucleosides?
Single Pill Combinations Versus Generics: Prescribing Practices in a New Healthcare Era
 Activity Code FM285 Single Pill Combinations Versus Generics: Prescribing Practices in a New Healthcare Era Monica Gandhi MD, MPH Clinic Director, Ward 86 HIV Clinic, SFGH/UCSF Learning Objectives Upon
Activity Code FM285 Single Pill Combinations Versus Generics: Prescribing Practices in a New Healthcare Era Monica Gandhi MD, MPH Clinic Director, Ward 86 HIV Clinic, SFGH/UCSF Learning Objectives Upon
GS-1489: STUDY DESIGN
 A PHASE 3 RANDOMIZED CONTROLLED CLINICAL TRIAL OF BICTEGRAVIR IN A FIXED DOSE COMBINATION,, VS ABC/DTG/3TC IN TREATMENT-NAÏVE ADULTS AT WEEK 48 J. Gallant, A. Lazzarin, A. Mills, C. Orkin, D. Podzamczer,
A PHASE 3 RANDOMIZED CONTROLLED CLINICAL TRIAL OF BICTEGRAVIR IN A FIXED DOSE COMBINATION,, VS ABC/DTG/3TC IN TREATMENT-NAÏVE ADULTS AT WEEK 48 J. Gallant, A. Lazzarin, A. Mills, C. Orkin, D. Podzamczer,
Integrase Strand Transfer Inhibitors on the Horizon
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Integrase Strand Transfer Inhibitors on the Horizon David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, University of Washington Presentation
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Integrase Strand Transfer Inhibitors on the Horizon David Spach, MD Clinical Director, Northwest AETC Professor of Medicine, University of Washington Presentation
The Integrase Inhibitor Drug Class: A Comparative Clinical Review
 The Integrase Inhibitor Drug Class: A Comparative Clinical Review Ian Frank Professor of Medicine University of Pennsylvania Philadelphia, PA USA franki@pennmedicine.upenn.edu Disclosure Gilead, ViiV/GlaxoSmithKline:
The Integrase Inhibitor Drug Class: A Comparative Clinical Review Ian Frank Professor of Medicine University of Pennsylvania Philadelphia, PA USA franki@pennmedicine.upenn.edu Disclosure Gilead, ViiV/GlaxoSmithKline: