Objectives. The ability to demonstrate knowledge of the following:
|
|
|
- Solomon Lawrence
- 6 years ago
- Views:
Transcription

1
2 Objectives The ability to demonstrate knowledge of the following: Bone and joints infections presentation Assessment and work up for bone and joint infections Differential diagnosis for bone and joint infections Management of bone and joint infections Complication of bone and joint infections
3 Red Flag Conditions Beware of: 1) Cauda Equina/severe neurologic injury (perianal numbness, decreased rectal tone, loss of movement in the extremeties) 2) Tumour 3) Infection 4) Trauma (open fracture, pelvic fracture) 5) Joint dislocations 6) Compartment syndrome
4 Acute osteomyelitis Classification Duration: Acute Subacute Chronic Route of Infection: Hematogenous Exogenous Host response: Pyogenic Granulomatous
5 Acute osteomyelitis Definition: Osteomyelitis is an inflammation of bone caused by an infecting organism. It may remain: Localized Spread to: Marrow Cortex Periosteum Soft tissue


6 Acute osteomyelitis Definition: Osteomyelitis is an inflammation of bone caused by an infecting organism. It may remain: Localized Spread to: Marrow Cortex Periosteum Soft tissue
7 Acute osteomyelitis Organism: Neonates: Staph aureus, Strep, E coli Children: Staph aureus, E coli, Serratia, Pseudomona ( Hem. Infl < 4 yrs, rare now) Sicklers: Staph aureus, Salmonella (most unique) Drug addicts: Staph aureus, Pseudomonas (most unique)
8 Acute osteomyelitis Organism: the commonest is staph. Aureus Source of infection: Hematogenous, direct extension, direct from outside Incidence: Age: more in children Sex: Boys> Girls Site of infection: metaphysis Bones: LE > UE. commonest are tibia and femur

9

10
11 Pathology Hematogenous colonisation of the bones by bacteria Stage of inflammation Spread of infection with pus formation Formation of subperiosteal abscess Pus tracks towards skin to form a sinus Bone infarction (Sequestrum) Subperiosteal new bone formation (Involucrum)
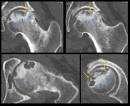
12 Involucrum is seen in the distal fibula
13 Involucrum is seen in the distal fibula

14 This x-rays show sequestra
15 Pathology and age variation Neonates: Extensive bone necrosis Increased ability to absorb large sequestrum Increased ability to remodel Epiphysio-metaphyseal vascular connection Secondary septic arthritis Presence of growth plate growth disturbance
16 Pathology and age variation Adults: No subperiosteal abscess Adherent periosteum Soft tissue abscess Vascular connection with the joint Secondary septic arthritis
17 Clinical Picture History: Fever Psudoparalysis, limping, inability to walk Identified potential source Confirm your most likely diagnosis Exclude other diagnosis
18 Clinical Picture Symptoms: Pain Fever malaise Restlessness Vomiting The limb is held still, loss of function
19 Clinical Picture General signs: Looks ill Fever Tachycardia Local signs: Look, feel and move
20 Laboratory tests CBC: raised WBC ESR: 24-36hrs C-reactive protein: 4-6hrs (most sensitive) Blood cultures (positive up to 50 %) Aspiration (send for Gram stain and C&S)
21 Radiography Plain x-rays (Normal in the first ten days, after that resorption of affected bone and sub-periosteal new bone formation) Bone scan (very sensitive but not specific) Ultrasound CT scan MRI

22 Acute Hematogenous OM Radiographic Changes soft tissue swelling (early) bone demineralization (10-14 days) sequestra dead bone with surrounding granulation tissue late involucrum periosteal new bone late Sequestrum and involucrum are signs of chronic ostemyelitis
23 Acute osteomyelitis
24 Subacute osteomyelitis

25

26 Diagnosis MRI shows changes in bone and bone marrow before plain films decreased T 1 -weighted bone marrow signal intensity increased post gadolinium fatsuppressed T 1 -weighted signal intensity increased T 2 -weighted signal relative to normal fat


27
28 Differential Diagnosis Acute septic arthritis Cellulitis Ewing s Sarcoma, lymphoma Sickle cell bone crisis Acute rheumatoid arthritis

29 Differential Diagnosis
30 Treatment Outline Select appropriate empirical antibiotics Deliver antibiotics to the infected site Identify the organisms Halt tissue destruction
31 Treatment General: Admission Hydration Correction of electrolyte imbalance Analgeics Immobilization Specific: Broad spectrum intravenous antibiotic till final culture Surgery if indicated
32 Empirical Treatment Initial treatment based on presumed infection type clinical findings and patient s age Definitive treatment based on final culture
33 Operative Treatment Started after cultures Indications for operative intervention Drainage of an abscess Débridement of infected tissues to prevent further destruction Refractory cases that show no improvement after nonoperative treatment
34 Complication Septicemia and distant abscesses Septic arthritis Growth disturbance in skeletally immature Pathological fracture Chronic osteomylitis



35 Complication

36 Chronic OM Common in Inappropriately treated acute OM Trauma Immunosuppressed Diabetics IV drug abusers Anatomical classification
37 Chronic OM Features Skin and soft tissues involvement Sinus tract may occasionally develop squamous cell carcinoma Periods of quiescence followed by acute exacerbations Diagnosis Nuclear medicine activity of the disease Best test to identify the organisms Operative sampling of deep specimens from multiple foci
38 Treatment Empirical therapy is not indicated IV antibiotics must be based on deep cultures Most common organisms S. aureus Enterobacteriaceae P. aeruginosa

39 Chronic osteomyelitis Glycocalyx exopolysaccharide coating envelops bacteria enhances bacterial adherence to biologic implants

40


41 Chronic osteomyelitis


42



43
44 Complications Recurrence Pathological fracture Growth disturbance in skeletally immature Squamous cell carcinoma transformation (fistula) Amputation
45 Septic Arthritis May affect any age and any joint The knee and hip are most affected Pathology: hematogenous or from the bone In neonates: transphyseal vessels In joints where the metaphysis is intracapsular (Hip, shoulder, proximal radius and distal fibula)

46
47 Septic Arthritis Symptoms : like AO Signs: hot swollen joint which is painful to any motion, inability to bear weight Joint is fixed in the position of ease


48 Septic Arthritis

49 Investigation Basic lab for infection (CBC,ESR and CRP) and Blood cultures Plain films and Ultrasound Joint aspiration: WBC >50,000 (>90%PMNL), damaged WBC and No crystals Organisms: similar to AO Rx: Admission for Emergency arthrotomy and washout, broad spectrum IV antibiotics and splintage Main DDx: transient synovitis of the hip
50 Acute Monoarthritis Sepsis workup Synovial Fluid Aspiration Positive B/C : 50-70% Smear- Culture Light microscope Leukocytosis ESR & CRP Positive Gram stain: 75% in s. aureus 30-50% in gram (-) Positive Fluid culture: 90% Turbid - Purulent Leukocyte> 50,000/ml (> 90% PMN) Damaged WBC Crystal (-) PCR: partially treated or culture negative

51

52 For simulated cases
53 Differential diagnosis Acute osteomylitis Transient synovitis (<10 years) Reactive arthritis Vasculitis eg: Henoch-Schonlein purpura Traumatic haemoarthrosis Haemophilic arthritis
54 Complication Septicemia Abscess Osteomyelitis Joint destruction Joint subluxation and dislocation Ankylosed joint Avascular necrosis of the femoral head Growth disturbance



55 Complication
56 Reactive arthritis Sterile inflammation secondary to bacterial infection 80% have HLA type B weeks after bacteria in genitalia eg: Chlamydia, or bowel eg (Shigella, Salmonella) Oligoarthritis (large joint of lower limb) Sometimes eye redness and irritation Synovial fluid: WBC <50,000 (PMNL <60%) Treatment: NSAID
57 Transient Synovitis Benign, self-limited disorder Associated with recent URI in 32-50% of children 30-40% of all non-traumatic limps Sterile inflammation causing joint effusion Lasts 2-7 days without intervention Male: Female is > 2:1 Ages 2-6 (typically <4)
58 Transient Synovitis Sudden onset of hip pain (Don t forget knee pain!!) Afebrile/low-grade fever (<38.5) Usually able to ambulate with a limp Antalgic gait Hip is flexed and externally rotated with mildly decreased ROM 5% bilateral presentation 25% with unilateral presentation with effusion on contralateral hip by ultrasound
59 Transient Synovitis Laboratory Evaluation WBC count <12,000 Mildly elevated ESR (<40), CRP (<2) X-Ray Joint space widening Discrepancies >2mm between sides Ultrasound: Joint effusion and/or synovial swelling Bilateral joint effusions in up to 25% of cases of asymtpmatic contralateral hip

60
61 Transient Synovitis Treatment Self-limited after 2-7 days Bed rest (NSAIDS):Ibuprofen Mean duration of pain ibuprofen: 2 days 80% of all patients has resolution by 7 days
62 Vasculitis Henoch-Schonlien purpura: systemic IgA vasculitis Primarily affect children Classic triad: purpura, arthritis and abdominal pain Usually able to ambulate, but with antalgic gait Ankle, knees and elbow mostly affected Purpura starts at posterior aspect of lower limb, buttocks, but can affect rest of the body


63 Henoch-Schonlein purpura Vasculitis: ecchmosis, petechiae Arthralgia: transient and migratory Abdominal pain: Within 8 days of rash (colicky) 20-30% GI bleeding Inussusception is common Renal: hematuria and proteinuria
64 Henoch-Schonlein purpura High urea and creatinine Raised IgA Raised ESR and/or CRP Diagnosis confirmed by biopsy
65 Chronic Non-Specific Bone and Joint Infection Outline: 1. Tuberculosis Causative organism Target Pathology Location of infection Spine T.B Clinical presentation Diagnosis Treatment 2. Other less common infections Brucellosis Syphilis Fungal infection
66 Tuberculosis Causative organism: 1. Mycobacterium tuberculosis 2. Mycobacterium Bovine 3. Mycobacterium africanum
67 Tuberculosis Causative organism: 1. Mycobacterium tuberculosis 2. Mycobacterium Bovine 3. Mycobacterium africanum
68 Mycobacterium Tuberculosis Thin non-motile rod Strictly aerobic Acid fast bacillus Requires enriched culture medium to grow Takes as long as 4-6 weeks to see the colonies
69 Mycobacterium Tuberculosis Known to affect humans from about 5000 BC Discovered by Laennic in the early 18 th century Common in our region and other developing countries Endemic in poor non-developed countries Increasing in developed countries along with the increase in AIDS
70 Tuberculosis Affects: 1. Anyone at any age!! 2. More common in the immunocompromised (AIDS, chronic renal failure, substance abuser) 3. Usually affects young individuals in developing countries while it affects the older in developed countries
71 TB Pathology Inflammation Hyperemia TB Follicles (tubercle): LYPHOCYTE MONOCYTES ENDOTHELIAL CELLS LANGHANS GIANT CELLS Coalesce Caseation

72 TB Follicle
73 Musculoskeletal TB Secondary to other primary TB lesions (Pulm.,Renal, LN) 1-8% of all T.B 50% associated with pulmonary primary site Route of spread: Hematogenous **** Direct (much less) * bone to joint * soft tissue to bone The primary lesion Quiescent Active: (Apparent, Latent)
74 Musculoskeletal TB MSK targets: 1. Spine (50%) Thoracic (50%) Lumbar (25%) Cervical (25%) 2. Pelvis 3. Hip 4. Knee 5. Ankle and shoulder
75 Musculoskeletal TB MSK targets: 1. Spine (50%) Thoracic (50%) Lumbar (25%) Cervical (25%) 2. Pelvis 3. Hip 4. Knee 5. Ankle and shoulder
76 MSK Tuberculosis Spine: Deformity (gibbus, kyphus) Neurological compromise (motor>sensory) Muscle spasm Joints: Swelling Stiffness Locking Loss of function Bones: Ulcers Sinuses Swelling deformity
77 MSK Tuberculosis Presentation: Constitutional symptoms Fever Wt loss Night sweats Anorexia Pain Stiffness deformity
78 Diagnosis Radiology: Plain x-rays: Joints: usually monoarticular Peri-articular osteopenia PHEMISTER S TRIAD Subchondral and peripheral erosions affecting both sides of the joint Loss of joint space

79
80 T.B of The Spine: (Pott s disease) Usually secondary to hematogenous spread Can affect two or more adjacent vertebrae May skip levels Primarily does not affect the disc but eventually the disc is affected
81 T.B of The Spine: (Pott s disease) Affects most commonly the anterior part of the vertebral endplates Causing erosion and destruction and finally anterior wedging of the vertebrae The disc herniates into the weakened and destructed body and narrowing of the disc height follows
82 T.B of The Spine: (Pott s disease) Infection spreads to adjacent level under the longitudinal ligaments and hematologically Eventually a kyphotic deformity occurs Para vertebral abscess is common and may be distant as well Cervical > retropharyngeal abscess Lumbar > psoas abscess Compression of the spinal cord is more likely to occur at the thoracic level
83 T.B of The Spine: (Pott s disease) Neurological deficits occur due to the compression secondary to the deformity or compression from the abscess Paraplegia may occur Reversible if treated early Mostly treated non-surgically

84


85


86

87

88
89 Diagnosis History and physical High risk Constitutional symptoms Atypical clinical picture Blood work: Lymphocytosis Anemia Elevated ESR ELISA PCR Brucella titre
90 Diagnosis Radiology: Plain x-rays: Spine: Erosion and destruction of end plates Narrowing of disc space Soft tissue mass shadow Anterior wedging of vertebrae Kyphus deformity
91 Diagnosis Radiology: Computerized tomography: Further delineate bony destruction and sequestrum Magnetic resonance imaging with contrast: Soft tissue mass, abscess Nerve root, cord status Distant abscess Non-enhanced cold abscess with enhanced peripheral ring
92 Diagnosis Special tests: Mantoux skin test Spine: CT guided needle biopsy Joints: Synovial aspiration---- low yield Should get bone/soft tissue Send for aerobic/non-aerobic bacteria, fungal, AFB, enriched culture media Takes up to 4-6 weeks
93 Treatment Mainstay of treatment is combination anti-microbial agents. Usually 3-4 medications needed Isniazide, Rifampin, Ethambutol, Pyrazinamide are commonly chosen Modify according to culture results Given for prolonged period of time (6 months up-to 18 months)
94 Treatment Indications of surgery: 1. Marked and progressive neurological deficit not responding to medical treatment requiring decompression 2. Spinal instability requiring stabilization 3. Tissue biopsy to confirm diagnosis 4. Joint lavage and removal of rice bodies 5. Abscess drainage if resistant to conservative treatment
95 Brucellosis Milk and milk products Back pain and stiffness Muscle spasms Fever (mild) Sacro-iliac joint Less destructive than TB Brucella titer Antibiotics: e.g. Septrin - Oxytetracycline
96 Take home messages Be aware about red flags Acute osteomyelitis: Empirical wide spectrum IV Abx till final culture Chronic osteomyelitis: IV Abx according to C/S Septic arthritis: Joint aspiration under GA for children Emergency Joint washout Required Immediate wide spectrum IV Abx till final culture Bone and joint infection requires prolonged antibiotic
Mohammad Ashraf. - Bahaa Najjar. - Mousa Al-Abbadi. 1 P a g e
 - 4 - Mohammad Ashraf - Bahaa Najjar - Mousa Al-Abbadi 1 P a g e Fractures (cont d). Healing of fractures: There are a lot of factors determine the proper healing of the fracture. For example: Displaced
- 4 - Mohammad Ashraf - Bahaa Najjar - Mousa Al-Abbadi 1 P a g e Fractures (cont d). Healing of fractures: There are a lot of factors determine the proper healing of the fracture. For example: Displaced
Prof Oluwadiya KS FMCS (Orthop) Consultant Orthopaedic Surgeon / Associate Professor Division of Orthopaedics and Traumatology Department of Surgery
 Consultant Orthopaedic Surgeon / Associate Professor Division of Orthopaedics and Traumatology Department of Surgery") Prof Oluwadiya KS FMCS (Orthop) Consultant Orthopaedic Surgeon / Associate Professor Division of Orthopaedics and Traumatology Department of Surgery College of Health Sciences Ladoke Akintola University
Prof Oluwadiya KS FMCS (Orthop) Consultant Orthopaedic Surgeon / Associate Professor Division of Orthopaedics and Traumatology Department of Surgery College of Health Sciences Ladoke Akintola University
ISPUB.COM. Spectrum Of MRI Findings In Musculoskeletal Tuberculosis: Pictoral Essay. P Chudgar INTRODUCTION SPINE
 ISPUB.COM The Internet Journal of Radiology Volume 8 Number 2 Spectrum Of MRI Findings In Musculoskeletal Tuberculosis: Pictoral Essay P Chudgar Citation P Chudgar.. The Internet Journal of Radiology.
ISPUB.COM The Internet Journal of Radiology Volume 8 Number 2 Spectrum Of MRI Findings In Musculoskeletal Tuberculosis: Pictoral Essay P Chudgar Citation P Chudgar.. The Internet Journal of Radiology.
Objectives. Comprehension of the common spine disorder
 Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Objectives Comprehension of the common spine disorder Disc degeneration/hernia Spinal stenosis Common spinal deformity (Spondylolisthesis, Scoliosis) Osteoporotic fracture Destructive spinal lesions Anatomy
Assessment of limping child (beware the child who does not weight bear at all):
:") Department of Paediatrics Clinical Guideline Acutely Limping Child and Septic Arthritis Assessment of limping child (beware the child who does not weight bear at all): History Careful history of any significant
Department of Paediatrics Clinical Guideline Acutely Limping Child and Septic Arthritis Assessment of limping child (beware the child who does not weight bear at all): History Careful history of any significant
SEPTIC ARTHRITIS. Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA. University of Science and technology Hospital Sanaa Yemen 18/Dec/2014
 SEPTIC ARTHRITIS Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA University of Science and technology Hospital Sanaa Yemen 18/Dec/2014 Objectives be able to define Septic Arthritis know what factors predispose
SEPTIC ARTHRITIS Dr Ahmed Husam Al Ahmed Rheumatologist SYRIA University of Science and technology Hospital Sanaa Yemen 18/Dec/2014 Objectives be able to define Septic Arthritis know what factors predispose
Osteomyelitis in infancy and childhood: A clinical and diagnostic overview M. Mearadji
 Osteomyelitis in infancy and childhood: A clinical and diagnostic overview M. Mearadji International Foundation for Pediatric Imaging Aid Introduction Osteomyelitis is a relative common disease in infancy
Osteomyelitis in infancy and childhood: A clinical and diagnostic overview M. Mearadji International Foundation for Pediatric Imaging Aid Introduction Osteomyelitis is a relative common disease in infancy
Topics. Musculoskeletal Infection Extremities. Detection of Infection. Role of Imaging in Extremity Infection. Detection of Infection
 Topics Musculoskeletal Infection Extremities Nuttaya Pattamapaspong M.D. Department of Radiology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand Role of imaging in extremity infection
Topics Musculoskeletal Infection Extremities Nuttaya Pattamapaspong M.D. Department of Radiology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand Role of imaging in extremity infection
PSOAS ABSCESS. Dr Noman Ullah Wazir
 PSOAS ABSCESS Dr Noman Ullah Wazir Psoas Major muscle The psoas major is a long fusiform muscle located on the side of the lumbar region of the vertebral column and brim of the lesser pelvis. Psoas Major
PSOAS ABSCESS Dr Noman Ullah Wazir Psoas Major muscle The psoas major is a long fusiform muscle located on the side of the lumbar region of the vertebral column and brim of the lesser pelvis. Psoas Major
TUBERCULOSIS OF HIP AND KNEE JOINT
 TUBERCULOSIS OF HIP AND KNEE JOINT TUBERCULOSIS OF HIP JOINT Occurrence-15% of all osteo articular tuber culosis Next common after spinal TB AETIO PATHOGENESIS Most common cause Mycobacterium tuberculosis
TUBERCULOSIS OF HIP AND KNEE JOINT TUBERCULOSIS OF HIP JOINT Occurrence-15% of all osteo articular tuber culosis Next common after spinal TB AETIO PATHOGENESIS Most common cause Mycobacterium tuberculosis
Acute Osteomyelitis: similar to septic arthritis but up to 40% may be afebrile swelling overlying the bone & tenderness
 Osteomyelitis / Bone and Joint Infections Bone infections in children are usually from haematogenous bacterial seeding to a single joint, usually the lower limbs, but may be multifocal. Approximately 10%
Osteomyelitis / Bone and Joint Infections Bone infections in children are usually from haematogenous bacterial seeding to a single joint, usually the lower limbs, but may be multifocal. Approximately 10%
BONES & JOINTS INFECTION BONE TUMOURS
 BONES & JOINTS INFECTION BONE TUMOURS IMPORTANT SERIOUS CONSEQUENCE PLEASE DON T MISS!! EARLY DIAGNOSIS & PROPER TREATMENT HOW?? AWARE of THEIR EXISTENCE (Knowledge) PREPARE for THEIR OCCURRENCE A HIGH
BONES & JOINTS INFECTION BONE TUMOURS IMPORTANT SERIOUS CONSEQUENCE PLEASE DON T MISS!! EARLY DIAGNOSIS & PROPER TREATMENT HOW?? AWARE of THEIR EXISTENCE (Knowledge) PREPARE for THEIR OCCURRENCE A HIGH
MUSCULOSKELETAL INFECTIONS IN CHILDREN. Dr Caren Landes Alder Hey Children s NHS Foundation Trust Liverpool
 MUSCULOSKELETAL INFECTIONS IN CHILDREN Dr Caren Landes Alder Hey Children s NHS Foundation Trust Liverpool MUSCULOSKELETAL INFECTIONS Common and uncommon infections Common and uncommon presentations Imaging
MUSCULOSKELETAL INFECTIONS IN CHILDREN Dr Caren Landes Alder Hey Children s NHS Foundation Trust Liverpool MUSCULOSKELETAL INFECTIONS Common and uncommon infections Common and uncommon presentations Imaging
BONE AND JOINT INFECTION. Dr.Jónás Zoltán Dept.of Orthopaedics
 BONE AND JOINT INFECTION Dr.Jónás Zoltán Dept.of Orthopaedics www.ortopedia.dote.hu Order of verbal exams: The students are able to register for the exam on the Neptun system. The students pick two titles,
BONE AND JOINT INFECTION Dr.Jónás Zoltán Dept.of Orthopaedics www.ortopedia.dote.hu Order of verbal exams: The students are able to register for the exam on the Neptun system. The students pick two titles,
Osteomieliti STEOMIE
 OsteomielitiSTEOMIE Osteomyelitis is the inflammation of bone caused by pyogenic organisms. Major sources of infection: - haematogenous spread - tracking from adjacent foci of infection - direct inoculation
OsteomielitiSTEOMIE Osteomyelitis is the inflammation of bone caused by pyogenic organisms. Major sources of infection: - haematogenous spread - tracking from adjacent foci of infection - direct inoculation
OSTEOMYELITIS. If it occurs in adults, then the axial skeleton is the usual site.
 OSTEOMYELITIS Introduction Osteomyelitis is an acute or chronic inflammatory process of the bone and its structures secondary to infection with pyogenic organisms. Pathophysiology Osteomyelitis may be
OSTEOMYELITIS Introduction Osteomyelitis is an acute or chronic inflammatory process of the bone and its structures secondary to infection with pyogenic organisms. Pathophysiology Osteomyelitis may be
Types of bone/joint infections. Bone and Joint Infections. Septic Arthritis. Pathogenesis. Pathogenesis. Bacterial arthritis: predisposing factors
 Bone and Joint Infections Types of bone/joint infections Arthritis (infective/septic) Osteomyelitis Prosthetic bone and joint infections Septic Arthritis Common destructive athroplasty Mono-articular Poly-articular
Bone and Joint Infections Types of bone/joint infections Arthritis (infective/septic) Osteomyelitis Prosthetic bone and joint infections Septic Arthritis Common destructive athroplasty Mono-articular Poly-articular
Special Imaging MUSCULOSKELETAL INFECTION. Special Imaging. Special Imaging. 18yr old male pt What is it? Additional Imaging
 MUSCULOSKELETAL INFECTION Additional Imaging May assist in diagnosis and, possibly, treatment Help create the picture May help differentiate from neoplasia 18yr old male pt What is it? Lymphoma Ewings
MUSCULOSKELETAL INFECTION Additional Imaging May assist in diagnosis and, possibly, treatment Help create the picture May help differentiate from neoplasia 18yr old male pt What is it? Lymphoma Ewings
Types of osteoarthritis
 ARTHRITIS Osteoarthritis is a degenerative joint disease is the most common joint disorder. It is a frequent part of aging and is an important cause of physical disability in persons older than 65 years
ARTHRITIS Osteoarthritis is a degenerative joint disease is the most common joint disorder. It is a frequent part of aging and is an important cause of physical disability in persons older than 65 years
OBJECTIVE INFECTION OF BONE AND JOINT CONTENT. Case. Case. Make diagnosis and treatment in bone and joint sepsis
 INFECTION OF BONE AND JOINT ธนพจน จ นทร น ม ภาคว ชาออร โธป ด กส โรงพยาบาลรามาธ บด OBJECTIVE Make diagnosis and treatment in bone and joint sepsis Prevent complications i from disease and treatment Use
INFECTION OF BONE AND JOINT ธนพจน จ นทร น ม ภาคว ชาออร โธป ด กส โรงพยาบาลรามาธ บด OBJECTIVE Make diagnosis and treatment in bone and joint sepsis Prevent complications i from disease and treatment Use
Osteo-articular TB in Children
 Osteo-articular TB in Children H Simon Schaaf Desmond Tutu TB Centre, Department of Paediatrics and Child Health, Stellenbosch University, Cape Town, South Africa Questions Spinal TB is the most common
Osteo-articular TB in Children H Simon Schaaf Desmond Tutu TB Centre, Department of Paediatrics and Child Health, Stellenbosch University, Cape Town, South Africa Questions Spinal TB is the most common
The Limping Child: Differential Diagnosis
 The Limping Child: Differential Diagnosis Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics
The Limping Child: Differential Diagnosis Kathryn A Keeler, MD Assistant Professor University of Missouri-Kansas City School of Medicine, Department of Orthopaedic Surgery and Department of Pediatrics
The Child with a Limp
 The Child with a Limp DR S Rajapaksa RCH CHIld with a limp Case: An 11 year old presents to ED with a 4 days history of a painful limp. He had been playing footie over the weekend and had fallen but then
The Child with a Limp DR S Rajapaksa RCH CHIld with a limp Case: An 11 year old presents to ED with a 4 days history of a painful limp. He had been playing footie over the weekend and had fallen but then
The Child With a Limp
 KID WITH A LIMP Common in ED, common in Exams Differential diagnosis is very wide Most causes benign, but mustn't miss Septic arthritis Osteomyelitis Fractures / NAI SUFE (older, heavier children) The
KID WITH A LIMP Common in ED, common in Exams Differential diagnosis is very wide Most causes benign, but mustn't miss Septic arthritis Osteomyelitis Fractures / NAI SUFE (older, heavier children) The
Pediatric Orthopedic Pathology Pathology 2 Dr. Gary Mumaugh
 Pediatric Orthopedic Pathology Pathology 2 Dr. Gary Mumaugh Congenital Defects - Clubfoot (congenital equinovarus) Forefoot is adducted and supinated o Positional equinovarus o Idiopathic congenital equinovarus
Pediatric Orthopedic Pathology Pathology 2 Dr. Gary Mumaugh Congenital Defects - Clubfoot (congenital equinovarus) Forefoot is adducted and supinated o Positional equinovarus o Idiopathic congenital equinovarus
 www.fisiokinesiterapia.biz Peak onset between 20 and 30 years Form of spondyloarthritis (cause inflammation around site of ligament insertion into bone) and association with HLA-B27 Prevalence as high
www.fisiokinesiterapia.biz Peak onset between 20 and 30 years Form of spondyloarthritis (cause inflammation around site of ligament insertion into bone) and association with HLA-B27 Prevalence as high
A Patient s Guide to Limping in Children
 A Patient s Guide to Limping in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled from a variety
A Patient s Guide to Limping in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet is compiled from a variety
Bone and Joint Infections Oh, My
 Bone and Joint Infections Oh, My Dale Jarka, MD,CM, FRCSC The Children s Mercy Hospitals & Clinics The Children's Mercy Hospital 2016 1 Disclosures A: I have no relevant financial relationships with the
Bone and Joint Infections Oh, My Dale Jarka, MD,CM, FRCSC The Children s Mercy Hospitals & Clinics The Children's Mercy Hospital 2016 1 Disclosures A: I have no relevant financial relationships with the
A free online interactive information resource for clinicians.
 A free online interactive information resource for clinicians www.pmmonline.org The limping child Helen Foster Professor of Paediatric Rheumatology Newcastle University Honorary Consultant Great North
A free online interactive information resource for clinicians www.pmmonline.org The limping child Helen Foster Professor of Paediatric Rheumatology Newcastle University Honorary Consultant Great North
Pott disease (spinal tuberculosis): MR and CT imaging
: MR and CT imaging") Pott disease (spinal tuberculosis): MR and CT imaging Poster No.: C-1422 Congress: ECR 2016 Type: Educational Exhibit Authors: G. Beretis, K. Giannaki, M. Fasoula, D. Kypriotis, T. Dagla, T.-P. Mantzouranis;
Pott disease (spinal tuberculosis): MR and CT imaging Poster No.: C-1422 Congress: ECR 2016 Type: Educational Exhibit Authors: G. Beretis, K. Giannaki, M. Fasoula, D. Kypriotis, T. Dagla, T.-P. Mantzouranis;
Epidemiology of Low back pain
 Low Back Pain Definition Pain felt in your lower back may come from the spine, muscles, nerves, or other structures in that region. It may also radiate from other areas like the mid or upper back, a inguinal
Low Back Pain Definition Pain felt in your lower back may come from the spine, muscles, nerves, or other structures in that region. It may also radiate from other areas like the mid or upper back, a inguinal
Spinal infection. Outline ANATOMY 6/2/2017. Anatomy Pathogen
 Outline Spinal infection Pramot Tanutit, M.D. Department of Radiology, Songklanagarind Hospital Faculty of Medicine, Prince of Songkla University Anatomy Pathogen Pyogenic spondylodiscitis Tuberculous
Outline Spinal infection Pramot Tanutit, M.D. Department of Radiology, Songklanagarind Hospital Faculty of Medicine, Prince of Songkla University Anatomy Pathogen Pyogenic spondylodiscitis Tuberculous
 www.fisiokinesiterapia.biz NOTE : THIS PRESENTATION DOES NOT REPLACE ATTENDANCE OR INFORMATION GIVEN IN THE LECTURE.IT IS INTENDED AS A HIGHLIGHT FOR THE TOPIC INTRODUCTION 60-80% of people will have LBP
www.fisiokinesiterapia.biz NOTE : THIS PRESENTATION DOES NOT REPLACE ATTENDANCE OR INFORMATION GIVEN IN THE LECTURE.IT IS INTENDED AS A HIGHLIGHT FOR THE TOPIC INTRODUCTION 60-80% of people will have LBP
ESPID New Bone and Joint Infection Guidelines
 ESPID New Bone and Joint Infection Guidelines Theoklis Zaoutis, MD, MSCE Professor of Pediatrics and Epidemiology Perelman School of Medicine at the University of Pennsylvania Chief, Division of Infectious
ESPID New Bone and Joint Infection Guidelines Theoklis Zaoutis, MD, MSCE Professor of Pediatrics and Epidemiology Perelman School of Medicine at the University of Pennsylvania Chief, Division of Infectious
ACUTE AND CHRONIC OSTEOMYELITIS
 ACUTE AND CHRONIC OSTEOMYELITIS DEFINITION Inflammation of the bone caused by an infecting organism HISTORY In the early 1900 s about 20% of patients with osteomyelitis died and patients who survived had
ACUTE AND CHRONIC OSTEOMYELITIS DEFINITION Inflammation of the bone caused by an infecting organism HISTORY In the early 1900 s about 20% of patients with osteomyelitis died and patients who survived had
Manage TB Dr. Dina Nair National Institute for Research in Tuberculosis, Chennai. Lecture 07 Clinical manifestations of TB Session 02
 Manage TB Dr. Dina Nair National Institute for Research in Tuberculosis, Chennai Lecture 07 Clinical manifestations of TB Session 02 Hello, welcome to the second session on Clinical manifestations of tuberculosis.
Manage TB Dr. Dina Nair National Institute for Research in Tuberculosis, Chennai Lecture 07 Clinical manifestations of TB Session 02 Hello, welcome to the second session on Clinical manifestations of tuberculosis.
P-1 (Former P-1) Are pediatric patients on oral or intravenous steroids at an increased risk of developing septic arthritis?
 Are pediatric patients on oral or intravenous steroids at an increased risk of developing septic arthritis?") Pediatrics Prevention P-1 (Former P-1) Are pediatric patients on oral or intravenous steroids at an increased risk of developing septic arthritis? RESEARCHED BY: Muhammad Amin Chinoy MD, Pakistan Literature:
Pediatrics Prevention P-1 (Former P-1) Are pediatric patients on oral or intravenous steroids at an increased risk of developing septic arthritis? RESEARCHED BY: Muhammad Amin Chinoy MD, Pakistan Literature:
A Patient s Guide to Transient Synovitis of the Hip in Children
 A Patient s Guide to Transient Synovitis of the Hip in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet
A Patient s Guide to Transient Synovitis of the Hip in Children 651 Old Country Road Plainview, NY 11803 Phone: 5166818822 Fax: 5166813332 p.lettieri@aol.com DISCLAIMER: The information in this booklet
12 Interesting MSK Cases
 12 Interesting MSK Cases James F Griffith Department of Imaging and Interventional Radiology Prince of Wales Hospital Case 1: 12-year-old boy Slipped and fell. Anterior knee pain and swelling Knee pain
12 Interesting MSK Cases James F Griffith Department of Imaging and Interventional Radiology Prince of Wales Hospital Case 1: 12-year-old boy Slipped and fell. Anterior knee pain and swelling Knee pain
Pediatric TB Intensive Houston, Texas
 Pediatric TB Intensive Houston, Texas November 13, 2009 Radiographic Manifestations of Pediatric TB Susan D. John, MD, FACR November 13, 2009 Radiologic Presentation of Childhood TB Susan D. John, MD,
Pediatric TB Intensive Houston, Texas November 13, 2009 Radiographic Manifestations of Pediatric TB Susan D. John, MD, FACR November 13, 2009 Radiologic Presentation of Childhood TB Susan D. John, MD,
MRI findings in proven Mycobacterium tuberculosis (TB) spondylitis
 spondylitis") CASE ORIGINAL REPORT ARTICLE MRI findings in proven Mycobacterium tuberculosis (TB) spondylitis D J Kotzé, MB ChB L J Erasmus, MB ChB Department of Diagnostic Radiology, University of the Free State, Bloemfontein
CASE ORIGINAL REPORT ARTICLE MRI findings in proven Mycobacterium tuberculosis (TB) spondylitis D J Kotzé, MB ChB L J Erasmus, MB ChB Department of Diagnostic Radiology, University of the Free State, Bloemfontein
Surgical Care at the District Hospital. EMERGENCY & ESSENTIAL SURGICAL CARE
 Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Surgical Care at the District Hospital 1 18 Orthopedic Trauma Key Points 2 18.1 Upper Extremity Injuries Clavicle Fractures Diagnose fractures from the history and by physical examination Treat with a
Pediatric TB Intensive Houston, Texas October 14, 2013
 Pediatric TB Intensive Houston, Texas October 14, 2013 Radiologic Presentation of Childhood TB Susan D. John, MD, FACR October 14, 2013 Disclosures I have no disclosures or conflicts of interest to report
Pediatric TB Intensive Houston, Texas October 14, 2013 Radiologic Presentation of Childhood TB Susan D. John, MD, FACR October 14, 2013 Disclosures I have no disclosures or conflicts of interest to report
CHAPTER 13 SKELETAL SYSTEM
 CHAPTER 13 SKELETAL SYSTEM Structure and Function Functions of the skeletal system Provides shape and support Protects internal organs Stores minerals and fat Produces blood cells and platelets Assists
CHAPTER 13 SKELETAL SYSTEM Structure and Function Functions of the skeletal system Provides shape and support Protects internal organs Stores minerals and fat Produces blood cells and platelets Assists
Etiology: Pathogenesis Clinical manifestation Investigation Treatment Prognosis
 Etiology: Pathogenesis Clinical manifestation Investigation Treatment Prognosis JIA is the most common rheumatic disease in childhood and a major cause of chronic disability. Etiology: Unknown, but may
Etiology: Pathogenesis Clinical manifestation Investigation Treatment Prognosis JIA is the most common rheumatic disease in childhood and a major cause of chronic disability. Etiology: Unknown, but may
Hths 2231 Laboratory 13 Alterations in Musculoskeletal
 Watch Movie: Osteoporosis Answer the movie questions on the worksheet. Complete activities 1-4. Activity #1: Click on the website link in activity 1 to review the structure and function of bone. Activity
Watch Movie: Osteoporosis Answer the movie questions on the worksheet. Complete activities 1-4. Activity #1: Click on the website link in activity 1 to review the structure and function of bone. Activity
7/1/2012. Repetitive valgus stresses cause microfractures in the apophyseal cartilage (weak link) Common in year olds
 Common in year olds") 1 2 3 4 5 6 7 When growing pains are not growing pains David W. Gray,M.D. Medical Director Orthopedics Differential Diagnosis Fracture Ligament Injury Disloclation Cartilage Injury Apophysitis Inflammation
1 2 3 4 5 6 7 When growing pains are not growing pains David W. Gray,M.D. Medical Director Orthopedics Differential Diagnosis Fracture Ligament Injury Disloclation Cartilage Injury Apophysitis Inflammation
Salisbury Foundation Trust Radiology Department Referral Guidelines for Primary Care: Musculoskeletal Imaging
 Salisbury Foundation Trust Radiology Department Referral Guidelines for Primary Care: Musculoskeletal Imaging These guidelines have been issued in conjunction with the Royal College of Radiology referral
Salisbury Foundation Trust Radiology Department Referral Guidelines for Primary Care: Musculoskeletal Imaging These guidelines have been issued in conjunction with the Royal College of Radiology referral
4/28/2010. Fractures. Normal Bone and Normal Ossification Bone Terms. Epiphysis Epiphyseal Plate (physis) Metaphysis
 Metaphysis") Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Fractures Normal Bone and Normal Ossification Bone Terms Epiphysis Epiphyseal Plate (physis) Metaphysis Diaphysis 1 Fracture Classifications A. Longitudinal B. Transverse C. Oblique D. Spiral E. Incomplete
Case Report Sequential MR Images and Radiographs of Epiphyseal Osteomyelitis in the Distal Femur of an Infant
 Case Reports in Radiology Volume 2013, Article ID 672815, 4 pages http://dx.doi.org/10.1155/2013/672815 Case Report Sequential MR Images and Radiographs of Epiphyseal Osteomyelitis in the Distal Femur
Case Reports in Radiology Volume 2013, Article ID 672815, 4 pages http://dx.doi.org/10.1155/2013/672815 Case Report Sequential MR Images and Radiographs of Epiphyseal Osteomyelitis in the Distal Femur
Musculoskeletal Referral Guidelines
 Musculoskeletal Referral Guidelines Introduction These guidelines have been developed to provide an integrated musculoskeletal service. They are based on reasonable clinical practice and will initially
Musculoskeletal Referral Guidelines Introduction These guidelines have been developed to provide an integrated musculoskeletal service. They are based on reasonable clinical practice and will initially
Case. 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds
 Case 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds Exam I: Swelling over entire tibia extending to foot P: Tenderness
Case 5 year old with 2 weeks leg pain and now refusing to walk + Fevers, lower leg swelling, warmth Denies and history of trauma or wounds Exam I: Swelling over entire tibia extending to foot P: Tenderness
Comprehension of the common spine disorder.
 Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy
Objectives Comprehension of the common spine disorder. Disc degeneration/hernia. Spinal stenosis. Common spinal deformity (Spondylolisthesis, Scoliosis). Osteoporotic fracture. Anatomy Anatomy Anatomy
RED AND AMBER FLAG GUIDANCE ORTHOPAEDIC CONDITIONS
 RED AND AMBER FLAG GUIDANCE ORTHOPAEDIC CONDITIONS Distribution list: Clinical Commissioning Groups / All Worcestershire GP practices; Musculoskeletal Integrated Clinical and Assessment Services; Commissioning
RED AND AMBER FLAG GUIDANCE ORTHOPAEDIC CONDITIONS Distribution list: Clinical Commissioning Groups / All Worcestershire GP practices; Musculoskeletal Integrated Clinical and Assessment Services; Commissioning
Ankle Replacement Surgery
 Ankle Replacement Surgery Ankle replacement surgery is performed to replace the damaged articular surfaces of the three bones of the ankle joint with artificial implants. This procedure is now being preferred
Ankle Replacement Surgery Ankle replacement surgery is performed to replace the damaged articular surfaces of the three bones of the ankle joint with artificial implants. This procedure is now being preferred
Spinal Cord Injuries: The Basics. Kadre Sneddon POS Rounds October 1, 2003
 Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Spinal Cord Injuries: The Basics Kadre Sneddon POS Rounds October 1, 2003 Anatomy Dorsal columntouch, vibration Corticospinal tract- UMN Anterior horn-lmn Spinothalamic tractpain, temperature (contralateral)
Message of the Month for GPs June 2013
 Message of the Month for GPs June 2013 Dr Winn : Consultant Musculoskeletal Radiologist, Manchester Royal Infirmary Imaging of the musculoskeletal system Musculoskeletal pain is a common problem in the
Message of the Month for GPs June 2013 Dr Winn : Consultant Musculoskeletal Radiologist, Manchester Royal Infirmary Imaging of the musculoskeletal system Musculoskeletal pain is a common problem in the
Sue Greenhalgh Consultant Physiotherapist March 18th
 Sue Greenhalgh Consultant Physiotherapist March 18th Caused by the Myobacterium Tuberculosis well known to Hippocrates Sir Percival Pott gave a very good description of the disease in 1779 Consumption
Sue Greenhalgh Consultant Physiotherapist March 18th Caused by the Myobacterium Tuberculosis well known to Hippocrates Sir Percival Pott gave a very good description of the disease in 1779 Consumption
6/23/2017. What do you see? skull fracture
 What do you see? skull fracture 1 Head CT On soft tissue windows, posterior soft tissues swelling and hemorrhage, no definite evidence of fracture Head CT On bone windows, fracture now seen subjacent to
What do you see? skull fracture 1 Head CT On soft tissue windows, posterior soft tissues swelling and hemorrhage, no definite evidence of fracture Head CT On bone windows, fracture now seen subjacent to
Osteoarthrosis, unspecified whether generalized or localized, lower leg. Osteoarthrosis, localized, not specified whether primary or secondary, pelvic
 Page 1 Appendix TABLE E-1 Codes (and Definitions) in Humana Database Used for Study Inclusion and Exclusion of Patients Who Underwent,, or 1 to 2-Level Inclusion ICD-9-P-8154 Total knee replacement ICD-9-D-71596
Page 1 Appendix TABLE E-1 Codes (and Definitions) in Humana Database Used for Study Inclusion and Exclusion of Patients Who Underwent,, or 1 to 2-Level Inclusion ICD-9-P-8154 Total knee replacement ICD-9-D-71596
7th CL Davis Diagnostic Pathology Symposium Diagnostic Orthopaedic Pathology Reno, NV October 19, 2007
 7th CL Davis Diagnostic Pathology Symposium Diagnostic Orthopaedic Pathology Reno, NV October 19, 2007 Roy R. Pool, DVM, PhD Professor of Pathology, Texas A&M Department Veterinary Pathobiology Director
7th CL Davis Diagnostic Pathology Symposium Diagnostic Orthopaedic Pathology Reno, NV October 19, 2007 Roy R. Pool, DVM, PhD Professor of Pathology, Texas A&M Department Veterinary Pathobiology Director
A Patient s Guide to Back Pain in Children
 A Patient s Guide to Back Pain in Children 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled from a variety of
A Patient s Guide to Back Pain in Children 2350 Royal Boulevard Suite 200 Elgin, IL 60123 Phone: 847.931.5300 Fax: 847.931.9072 DISCLAIMER: The information in this booklet is compiled from a variety of
Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections
 Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections Objectives How do you to diagnose, classify and manage DFI? How do you diagnose
Bone and Joint Infections in Diabetics: Diagnosis and Management of Diabetic Foot and Other Common Lower Extremity Infections Objectives How do you to diagnose, classify and manage DFI? How do you diagnose
Primary care referral criteria for musculoskeletal MRI scans
 Appendix 1 Primary care referral criteria for musculoskeletal MRI scans Accepted Criteria for Direct Access MRI Body Part Symptoms Imaging indicated Lumbar Spine Low Back Pain with adverse symptoms or
Appendix 1 Primary care referral criteria for musculoskeletal MRI scans Accepted Criteria for Direct Access MRI Body Part Symptoms Imaging indicated Lumbar Spine Low Back Pain with adverse symptoms or
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 11/17/2012 Radiology Quiz of the Week # 99 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 11/17/2012 Radiology Quiz of the Week # 99 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
TUBERCULOSIS. By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi
 TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
TUBERCULOSIS By Dr. Najaf Masood Assistant Prof Pediatrics Benazir Bhutto Hospital Rawalpindi Tuberculosis Infectious, Systemic, Chronic granulomatous disease caused by mycobacterium tuberculosis DEFINITION
Nuclear medicine and Prosthetic Joint Infections
 Nuclear medicine and Prosthetic Joint Infections Christophe Van de Wiele, M.D., Ph.D. Department of Nuclear Medicine, University Hospital Ghent, Belgium Orthopedic prostheses: world market 1996 Prosthetic
Nuclear medicine and Prosthetic Joint Infections Christophe Van de Wiele, M.D., Ph.D. Department of Nuclear Medicine, University Hospital Ghent, Belgium Orthopedic prostheses: world market 1996 Prosthetic
Original Date: December 2015 Page 1 of 8 FOR CMS (MEDICARE) MEMBERS ONLY
 MEMBERS ONLY") National Imaging Associates, Inc. Clinical guidelines TOTAL JOINT ARTHROPLASTY -Total Hip Arthroplasty -Total Knee Arthroplasty -Replacement/Revision Hip or Knee Arthroplasty CPT4 Codes: Please refer to
National Imaging Associates, Inc. Clinical guidelines TOTAL JOINT ARTHROPLASTY -Total Hip Arthroplasty -Total Knee Arthroplasty -Replacement/Revision Hip or Knee Arthroplasty CPT4 Codes: Please refer to
PREAMBLE GENERAL DIAGNOSTIC RADIOLOGY
 PREAMBLE The General Diagnostic Radiology category is intended to cover the body of knowledge a practicing board certified Diagnostic Radiologist should know. Since the range of content relevant to the
PREAMBLE The General Diagnostic Radiology category is intended to cover the body of knowledge a practicing board certified Diagnostic Radiologist should know. Since the range of content relevant to the
Management of Acute Haematogenous Osteomyelitis. SAPOS ICL 2017 Anthony Robertson
 Management of Acute Haematogenous Osteomyelitis SAPOS ICL 2017 Anthony Robertson Diagnosis Diagnosis RED FLAGS: Nunn, Rollinson;; SAMJ 2007 Acute hip pain in a child Infant with loss of movement in a limb
Management of Acute Haematogenous Osteomyelitis SAPOS ICL 2017 Anthony Robertson Diagnosis Diagnosis RED FLAGS: Nunn, Rollinson;; SAMJ 2007 Acute hip pain in a child Infant with loss of movement in a limb
PITFALLS IN THE DIAGNOSIS OF SKELETAL TUBERCULOSIS IN CHILDREN
 PITFALLS IN THE DIAGNOSIS OF SKELETAL TUBERCULOSIS IN CHILDREN DR.JANANI SANKAR SENIOR CONSULTANT - PEDIATRICS DEPARTMENT OF PEDIATRICS & PEDIATRIC ORTHOPEDICS KANCHI KAMAKOTI CHILDS TRUST HOSPITAL CHENNAI,
PITFALLS IN THE DIAGNOSIS OF SKELETAL TUBERCULOSIS IN CHILDREN DR.JANANI SANKAR SENIOR CONSULTANT - PEDIATRICS DEPARTMENT OF PEDIATRICS & PEDIATRIC ORTHOPEDICS KANCHI KAMAKOTI CHILDS TRUST HOSPITAL CHENNAI,
HKCEM JCM OSCE. 06 March 3013 AED POH
 HKCEM JCM OSCE 06 March 3013 AED POH 1 Case 1 M/52 Walk unaided to AED c/o left foot sprain few days ago during working P/E swelling, tender over dorsum of foot 2 3 Questions What were the X ray findings
HKCEM JCM OSCE 06 March 3013 AED POH 1 Case 1 M/52 Walk unaided to AED c/o left foot sprain few days ago during working P/E swelling, tender over dorsum of foot 2 3 Questions What were the X ray findings
Sacroiliac joint infection
 Case Report Brunei Int Med J. 2015; 11 (2): 110-114 Sacroiliac joint infection Jon CHUA 1, Kamal JAMIL 1, Kamalnizat IBRAHIM 1, Suraya AZIZ 2 1 Department of Orthopaedic and Traumatology, Faculty of Medicine,
Case Report Brunei Int Med J. 2015; 11 (2): 110-114 Sacroiliac joint infection Jon CHUA 1, Kamal JAMIL 1, Kamalnizat IBRAHIM 1, Suraya AZIZ 2 1 Department of Orthopaedic and Traumatology, Faculty of Medicine,
Priorities Forum Statement GUIDANCE
 Priorities Forum Statement Number 21 Subject Knee Arthroscopy including arthroscopic knee washouts Date of decision November 2016 Date refreshed March 2017 Date of review November 2018 Osteoarthritis of
Priorities Forum Statement Number 21 Subject Knee Arthroscopy including arthroscopic knee washouts Date of decision November 2016 Date refreshed March 2017 Date of review November 2018 Osteoarthritis of
Musculoskeletal Development and Sports Injuries in Pediatric Patients
 Dynamic Chiropractic October 21, 2010, Vol. 28, Issue 22 Musculoskeletal Development and Sports Injuries in Pediatric Patients By Deborah Pate, DC, DACBR Physical activity is extremely important for everyone,
Dynamic Chiropractic October 21, 2010, Vol. 28, Issue 22 Musculoskeletal Development and Sports Injuries in Pediatric Patients By Deborah Pate, DC, DACBR Physical activity is extremely important for everyone,
Hypertrophic Osteoarthropathy
 September 2005 Hypertrophic Osteoarthropathy Roxanne Landesman, Harvard Medical School Year III Hypothetical Patient A patient presents with persistent right ankle pain, and no history of trauma. As the
September 2005 Hypertrophic Osteoarthropathy Roxanne Landesman, Harvard Medical School Year III Hypothetical Patient A patient presents with persistent right ankle pain, and no history of trauma. As the
Bone and Joint Infections Case Presentations Pediatric MSK Bootcamp Sept 29, 2019 American Academy of Pediatrics/ Penn State
 Bone and Joint Infections Case Presentations Pediatric MSK Bootcamp Sept 29, 2019 American Academy of Pediatrics/ Penn State Douglas Armstrong MD Darmstrong@hmc.psu.edu Penn State College of Medicine Disclosures
Bone and Joint Infections Case Presentations Pediatric MSK Bootcamp Sept 29, 2019 American Academy of Pediatrics/ Penn State Douglas Armstrong MD Darmstrong@hmc.psu.edu Penn State College of Medicine Disclosures
TB or not TB? That should be the question
 TB or not TB? That should be the question SH Liyanage, CM Gupte ( ), A Cobb, MC Beverly Department of Orthopaedics Ealing University Hospital Uxbridge Rd, Southall, Middlesex UB13HW United Kingdom Correspondence:
TB or not TB? That should be the question SH Liyanage, CM Gupte ( ), A Cobb, MC Beverly Department of Orthopaedics Ealing University Hospital Uxbridge Rd, Southall, Middlesex UB13HW United Kingdom Correspondence:
Joint Injuries and Disorders
 Joint Injuries and Disorders Introduction A joint is where two or more bones come together. Your joints include the knees, hips, elbows and shoulders. There are many types of joint disorders, including
Joint Injuries and Disorders Introduction A joint is where two or more bones come together. Your joints include the knees, hips, elbows and shoulders. There are many types of joint disorders, including
Case Report Sacral Emphysematous Osteomyelitis Caused by Escherichia coli after Arthroscopy of the Knee
 Case Reports in Orthopedics Volume 2016, Article ID 1961287, 4 pages http://dx.doi.org/10.1155/2016/1961287 Case Report Sacral Emphysematous Osteomyelitis Caused by Escherichia coli after Arthroscopy of
Case Reports in Orthopedics Volume 2016, Article ID 1961287, 4 pages http://dx.doi.org/10.1155/2016/1961287 Case Report Sacral Emphysematous Osteomyelitis Caused by Escherichia coli after Arthroscopy of
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH)
") A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) 6565 Fannin Street Houston, TX 77030 Phone: 713-790-3333 DISCLAIMER: The information in this booklet is compiled from a variety of sources.
A Patient s Guide to Diffuse Idiopathic Skeletal Hyperostosis (DISH) 6565 Fannin Street Houston, TX 77030 Phone: 713-790-3333 DISCLAIMER: The information in this booklet is compiled from a variety of sources.
Case 4 Generalised bone pain
 Case 4 Generalised bone pain C A 34- year- old woman presented complaining of multifocal pain in her chest and legs. The pain was intermittent, was aggravated by weight bearing. Initially was alleviated
Case 4 Generalised bone pain C A 34- year- old woman presented complaining of multifocal pain in her chest and legs. The pain was intermittent, was aggravated by weight bearing. Initially was alleviated
DIAGNOSIS CODING ESSENTIALS FOR LONG-TERM CARE: CHAPTER 13, M CODES MUSCULOSKELETAL SYSTEM AND CONNECTIVE TISSUE
 DIAGNOSIS CODING ESSENTIALS FOR LONG-TERM CARE: CHAPTER 13, M CODES MUSCULOSKELETAL SYSTEM AND CONNECTIVE TISSUE Preferred Clinical Services for Leading Age Florida August 26-27, 2015 MUSCULOSKELETAL FUNCTIONS
DIAGNOSIS CODING ESSENTIALS FOR LONG-TERM CARE: CHAPTER 13, M CODES MUSCULOSKELETAL SYSTEM AND CONNECTIVE TISSUE Preferred Clinical Services for Leading Age Florida August 26-27, 2015 MUSCULOSKELETAL FUNCTIONS
Subaxial Cervical Spine Trauma. Introduction. Anatomic Considerations 7/23/2018
 Subaxial Cervical Spine Trauma Sheyan J. Armaghani, MD Florida Orthopedic Institute Assistant Professor USF Dept of Orthopedics Introduction Trauma to the cervical spine accounts for 5 of all spine injuries
Subaxial Cervical Spine Trauma Sheyan J. Armaghani, MD Florida Orthopedic Institute Assistant Professor USF Dept of Orthopedics Introduction Trauma to the cervical spine accounts for 5 of all spine injuries
Introduction to Neuroimaging spine. John J. McCormick MD
 Introduction to Neuroimaging spine John J. McCormick MD Neuroanatomy Netter drawings Radiographic Anatomy Cervical Spine Cervical Spine Oblique View Cervical Spine Dens View Thoracic Spine Lumbar Spine
Introduction to Neuroimaging spine John J. McCormick MD Neuroanatomy Netter drawings Radiographic Anatomy Cervical Spine Cervical Spine Oblique View Cervical Spine Dens View Thoracic Spine Lumbar Spine
3/10/17 Spinal a Injury 1
 Spinal Injury 1 'Paralysed' Watmough vows he'll have the backbone for Game Two after treatment for neck injury Watmough will have cortisone injected into his spine this morning to speed up the recovery
Spinal Injury 1 'Paralysed' Watmough vows he'll have the backbone for Game Two after treatment for neck injury Watmough will have cortisone injected into his spine this morning to speed up the recovery
INFECTION & INFLAMMATION IMAGING
 INFECTION & INFLAMMATION IMAGING Radiopharmaceutical Drug Interactions & Other Interesting Case Studies MICHELLE RUNDIO, CNMT NCT MBA PCI NUCLEAR IN-111 WHITE BLOOD CELL IMAGING Interactions, Imaging Parameters
INFECTION & INFLAMMATION IMAGING Radiopharmaceutical Drug Interactions & Other Interesting Case Studies MICHELLE RUNDIO, CNMT NCT MBA PCI NUCLEAR IN-111 WHITE BLOOD CELL IMAGING Interactions, Imaging Parameters
102 Results RESULTS. Age Mean=S.D Range 42= years -84 years Number % <30 years years >50 years
 102 Results RESULTS A total of 50 cases were studied 39 males and 11females.Their age ranged between 16 years and 84 years (mean 42years). T1 and T2WI were acquired for all cases in sagittal and axial
102 Results RESULTS A total of 50 cases were studied 39 males and 11females.Their age ranged between 16 years and 84 years (mean 42years). T1 and T2WI were acquired for all cases in sagittal and axial
Key Primary CPT Codes: Refer to pages: 7-9 Last Review Date: October 2016 Medical Coverage Guideline Number:
 National Imaging Associates, Inc. Clinical guidelines CERVICAL SPINE SURGERY: ANTERI CERVICAL DECOMPRESSION WITH FUSION CERVICAL POSTERI DECOMPRESSION WITH FUSION CERVICAL ARTIFICIAL DISC CERVICAL POSTERI
National Imaging Associates, Inc. Clinical guidelines CERVICAL SPINE SURGERY: ANTERI CERVICAL DECOMPRESSION WITH FUSION CERVICAL POSTERI DECOMPRESSION WITH FUSION CERVICAL ARTIFICIAL DISC CERVICAL POSTERI
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 11/24/2012 Radiology Quiz of the Week # 100 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 11/24/2012 Radiology Quiz of the Week # 100 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Pathology of pulmonary tuberculosis. Dr: Salah Ahmed
 Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
Pathology of pulmonary tuberculosis Dr: Salah Ahmed Is a chronic granulomatous disease, caused by Mycobacterium tuberculosis (hominis) Usually it involves lungs but may affect any organ or tissue Transmission:
RETROLISTHESIS. Retrolisthesis. is found mainly in the cervical spine and lumbar region but can also be often seen in the thoracic spine
 RETROLISTHESIS A retrolisthesis is a posterior displacement of one vertebral body with respect to adjacent vertebrae Typically a vertebra is to be in retrolisthesis position when it translates backward
RETROLISTHESIS A retrolisthesis is a posterior displacement of one vertebral body with respect to adjacent vertebrae Typically a vertebra is to be in retrolisthesis position when it translates backward
Diagnostic Imaging Exams
 Guide for Chiropractors Diagnostic Imaging Exams CREATED FOR OUR CHIROPRACTIC PARTNERS This document has been prepared by the specialized, board-certified radiologists who interpret patient exams for Center
Guide for Chiropractors Diagnostic Imaging Exams CREATED FOR OUR CHIROPRACTIC PARTNERS This document has been prepared by the specialized, board-certified radiologists who interpret patient exams for Center
Effective Utilization of Imaging. John V. Roberts, M.D. Premier Radiology Abdominal Imaging
 Effective Utilization of Imaging John V. Roberts, M.D. Premier Radiology Abdominal Imaging Safety Contrast and Radiation What to order Abdomen/Pelvis Brain/Spine Chest Musculoskeletal Ob/Gyn Head and Neck
Effective Utilization of Imaging John V. Roberts, M.D. Premier Radiology Abdominal Imaging Safety Contrast and Radiation What to order Abdomen/Pelvis Brain/Spine Chest Musculoskeletal Ob/Gyn Head and Neck
Long Case Set 02. Dr Raviraj Uppoor. Dr Sameer Shamshuddin. Consultant Radiologist Cumberland Infirmary, Carlisle, UK
 Long Case Set 02 www.frcrtutorials.com Dr Raviraj Uppoor MBBS, DMRD, DNB, FRCR Consultant Radiologist Cumberland Infirmary, Carlisle, UK Dr Sameer Shamshuddin MBBS, DMRD, FRCR Consultant Radiologist Royal
Long Case Set 02 www.frcrtutorials.com Dr Raviraj Uppoor MBBS, DMRD, DNB, FRCR Consultant Radiologist Cumberland Infirmary, Carlisle, UK Dr Sameer Shamshuddin MBBS, DMRD, FRCR Consultant Radiologist Royal
Disclosures. Orthopedic infections. Case 1. Pen Barnes MBBS PhD. Clinical Associate Professor Departments of Medicine Pathology and Orthopedics OHSU
 Orthopedic infections Disclosures Pen Barnes MBBS PhD I have nothing to disclose Clinical Associate Professor Departments of Medicine Pathology and Orthopedics OHSU Case 1 48 year old woman presents to
Orthopedic infections Disclosures Pen Barnes MBBS PhD I have nothing to disclose Clinical Associate Professor Departments of Medicine Pathology and Orthopedics OHSU Case 1 48 year old woman presents to
REFERRAL GUIDELINES: ORTHOPAEDIC SURGERY
 All patients referred to specialist clinics are assigned to a priority category based on their clinical need and related psychosocial factors. The examples given are indicative only and the clinician reviewing
All patients referred to specialist clinics are assigned to a priority category based on their clinical need and related psychosocial factors. The examples given are indicative only and the clinician reviewing
Case Report Multicentric Spinal Tuberculosis with Sternoclavicular Joint Involvement: A Rare Presentation
 Case Reports in Pulmonology, Article ID 685406, 4 pages http://dx.doi.org/10.1155/2014/685406 Case Report Multicentric Spinal Tuberculosis with Sternoclavicular Joint Involvement: A Rare Presentation Balaji
Case Reports in Pulmonology, Article ID 685406, 4 pages http://dx.doi.org/10.1155/2014/685406 Case Report Multicentric Spinal Tuberculosis with Sternoclavicular Joint Involvement: A Rare Presentation Balaji
Osteomyelitis and Septic Joints; Practical Considerations. Coleen K. Cunningham
 Osteomyelitis and Septic Joints; Practical Considerations Coleen K. Cunningham Goals/objectives To improve understanding of the diagnosis, treatment, and follow-up of pediatric bone and joint infections
Osteomyelitis and Septic Joints; Practical Considerations Coleen K. Cunningham Goals/objectives To improve understanding of the diagnosis, treatment, and follow-up of pediatric bone and joint infections