VASCULITIS ACOI Robert L. DiGiovanni, DO, FACOI
|
|
|
- Erick Mason
- 5 years ago
- Views:
Transcription
1 VASCULITIS ACOI 2018 Robert L. DiGiovanni, DO, FACOI
2 Disclosures NONE
3 Vasculitis Clinicopathologic process characterized by inflammation of and damage to blood vessels. Vessel lumen is usually compromised leading to possible ischemia and necrosis. This also leads to increased cytokine production and inflammation. Can be confined to one single organ (i.e skin), or it may simultaneously involve several organ systems. The distribution of affected organs may suggest a particular vasculitic disorder, but significant overlap is observed. It is often a serious and sometimes fatal disease that requires prompt recognition and therapy
4 Pathophysiology Multi-factorial: Genetic predisposition Environmental exposure Regulatory mechanisms associated with immune response to certain antigens
5 Conditions that can mimic vasculitis Infectious ds: Neoplasms Bacterial endocarditis Atrial myxoma Disseminated gonoccocal infection Lymphoma Pulmonary histoplasmosis Carcinomatosis Coccidioidomycosis Drug toxicity Syphillis Cocaine Lyme ds Amphetamines Rocky Mountain spotted fever Ergot alkaloids Whipple s ds Arsenic Coagulopathies/thrombotic microangiopathies Sarcoidosis Antiphosphlipid antibody syndrome Atheroembolic ds Thrombotic thrombocytopenic purpura Goodpasture s syndrome Amyloidosis Migraine
6 Large-sized Vessels: Giant Cell Arteritis Takayasu s Arteritis Classification Medium-sized Vessels Polyarteritis Nodosa Kawasaki s Disease Primary Central Nervous system vasculitis
7 Classification Small-sized Vessels ANCA-Associated Granulomatosis with polyangiitis (Wegener s) Microscopic Polyangiitis Eosinophilic granulomatosis with polyangiitis (Churg-Strauss Syndrome) Immune-Complex mediated: Henoch-Schonlein purpura Essential cryoglobulinemic vasculitis Hypersensitivity vasculitis Vasculitis secondary to connective tissue disease Vasculitis secondary to viral infection
8 ANCA-associated antibodies Directed against certain proteins in the cytoplasmic granules of neutrophils and monocytes. Two patterns of ANCA: Cytoplasmic (C-ANCA) Major target is Proteinaise-3 (PR-3) Perinuclear (P-ANCA) Major target is the enzyme myeloperoxidase (MPO).


9 C-ANCA P-ANCA There is heavy staining in the cytoplasm while the multilobulated nuclei (clear zones) are nonreactive. Staining is limited to the perinuclear region and the cytoplasm is nonreactive.
10 More on P-ANCA P-ANCA can be associated to certain medications (drug-induced) that include: Hydralazine, propylthiouracil, minocycline. P-ANCA pattern or atypical pattern has been associated with rheumatic diseases: inflammatory myopathies, reactive arthritis, APS, autoimmune GI disorders, such as ulcerative colitis or chrons ds, also cocaine, infections. Typically anti-mpo antibody is helpful and if present, it is more suggestive of true vasculitis.
11 Churg-Strauss syndrome (EGPA) Eosinophilic Granulomatosis w Polyangiitis Characterized by asthma, peripheral and tissue eosinophilia, extravascular granuloma formation, and vasculitis of multiple organ systems. Uncommon ds with estimated annual incidence of 1-3/ 1,000,000. Can affect any age, except infants with mean age at onset at 48y/o. Female:male 1.2 :1
12 Churg-Strauss syndrome clinical presentation Fever, malaise, anorexia, weight loss (constitutional symptoms), Most predominant: pulmonary: severe asthmatic attacks with presence of pulmonary infiltrates. Mononeuritis multiplex: second most common manifestation (up to 72% pts). Allergic rhinitis and sinusitis (up to 61% pts). Heart ds (14% pts). Skin lesions (51%): purpura, cutaneous and subcutenous nodules. Kidney: less common and generally less-severe than of WG or MPA. Labs: Eosinophilia (>1000 cells/ul in >80%), elevated ESR, fibrinogen, Alpha2-globulins found in >81%. And then organ specific findings. About 48% pts have +ANCA, usually anti-mpo ab.
13 Churg-Strauss syndrome Treatment Prognosis is poor without treatment, with reported 5-year survival of 25%. With treatment, prognosis is favorable, about 72%. Myocardial involvement is the most frequent cause of death and is responsible for 39% of pts mortality. Treatment is with glucocorticoids, immunomodulatory Rx: MTX, Cytoxan Mepolizumab: first FDA approved treatment for EGPA 12/12/17, MOA: MAB against IL-5
14 Wegner s granulomatosis (GPA) Characterized by granulomatous vasculitis of the upper and lower respiratory tracts together with glomerulonephritis. Prevalence: 3/100,000, Extremely rare in blacks compared to whites. Male: female 1:1. 15% pts are <19 y/o, mean age of onset is approximately 40y/o. Rarely occurs before adolescence
15 Wegner s granulomatosis pathogenesis Necrotizing vasculitis of small arteries and veins together with granuloma formation. Lung: multiple bilateral nodular cavitary infiltrates (on biopsy almost always show necrotizing granulomatous vasculitis). Upper airway: sinuses and nasopharynx reveal inflammation, necrosis, granuloma formation, with or without vasculitis. Kidneys: earliest form presents with focal and segmental glomerulonephritis that may evolve into rapidly progressive crescentic glomerulonephritis. Granuloma formation is rarely seen on renal biopsy. No immune complex deposition is found.
16 Wegner s granulomatosis Clinical presentation-1 Upper airway (95% pts): paranasal sinus pain and drainage, purulent or bloody nasal discharge nasal mucosal ulceration nasal septal perforation can lead to saddle nose deformity serous otitis media from eustachian tube blockage subglottic tracheal stenosis from active ds or scarring in up to 16% of pts (can lead to severe airway obstruction). Lower airway (85 to 90%): Cough, hemoptysis, dyspnea, chest discomfort (present in 85-90%). Endobronchial ds (active or as a result of fibrous scarring, can lead to obstruction with atelectasis). Eye involvement (up to 52%): may range from mild conjuctivitis to dacryocystitis, episcleritis, scleritis, granulomatous sclerouveitis, ciliary vessel vasculitis, and retroorbital mass lesions, leading to proptosis.

17 Wegner s granulomatosis saddle nose deformity

18 Wegner s granulomatosis ground glass opacities and cavitary nodule
19 Wegner s granulomatosis Clinical presentation-2 Skin lesions (46% of pts) appear as papules, vesicles, palpable purpura, ulcers, or subcutanous nodules (biopsy shows vasculitis, granuloma or both). Cardiac involvement (8% of pts) as pericarditis, coronary vasculitis or cardiomyopathy. Nervous system manifestations (23%) include cranial neuritis, mononeuritis multiplex, or cerebral vasculitis and/or granuloma. Renal ds (77% of pts) presents with glomerulitis with protenuiria, hematuria, red blood cell casts, but if untreated, then rapidly progressive renal failure ensues. Constitutional symptoms Labs: Elevated ESR, mild anemia, leukocytosis, mild hypergammaglobulinemia (mostly IgA class), could have midly elevated RF, thrombosis. 90% of pts have +anti-pr3 ANCA. In the absence of active ds, the sensitivity drops to approximately 60 to 70%.
20 Wegner s granulomatosis Treatment Mortality reaches 90% in 2 years if untreated. With proper treatment, more than 75% remission. The most effective therapy for life-threatening disease, typically with pulmonary-renal involvement is cyclophosphamide with high dose glucocorticoids Cyclophosphamide-related toxicities include: cystitis (at least 30%), bladder cancer (6%), myelodysplasia (2%), high risk of infertility. Following induction of remission: maintenance therapy with methotrexate, azathioprine or cellcept. TMP-SMX for PJP prophylaxis and also to prevent upper respiratory relapse.
21 Wegner s granulomatosis Treatment For mild ds: consider methotrexate. For pulmonary hemorrhage: plasma exchange For subglottic stenosis: intralesional injection of glucocorticoids in combination with endoscopic dilation may avoid the need for more invasive surgical procedures FDA approved 2011: rituximab (B-cell depletion anti- CD20 monoclonal Ab) for ANCA-associated vasculitis in non-inferiority study compared to cyclophosphmide
22 Microscopic polyangiitis Pts have equivalent vasculitic lesions to those observed in GPA, but, at least at presentation, do not typically have symptomatic or histologic respiratory involvement. Such individuals are considered to have microscopic polyarteritis. ANCA are typically present with anti-mpo ab. Absence of granulomatous inflammation differentiates it from GPA. Renal lesion is identical to that of GPA.
23 Microscopic polyangiitis clinical manifestation Constitutional symptoms Glomerulonephritis occurs in 79% pts and can be rapidly progressive, leading to renal failure. Hemoptysis may be the first symptom of alveaolar hemorrhage, which occurs in 12% of pts. Mononeuritis multiplex. GI tract. Cutanous vasculitis. Upper airway ds and pulmonary nodules are not typically found in microscopic polyangitis (and if present, suggest GPA). Labs: Elevated ESR, anemia, leukocytosis, thrombocytosis, ANCA is present in 75% pts (typically with anti-mpo ab).
24 Microscopic polyangiitis treatment Treatment is similar to GPA, depending on severity. 5-year survival rate is about 74%. Disease-related mortality occurs usually from alveolar hemorrhage or GI, cardiac, or renal ds. Relapse is lower than GPA with about 34% pts relapsing. Limited studies. Most information comes from GPA treatment trials.
25 Does negative ANCA exclude small vessel vasculitis? Up to 40% pts with limited GPA and up to 10% of severe GPA have negative ANCA. Up to 30% of MPA and up to 50% of CSS could have negative ANCA
26 Does increased ANCA titers predict a disease flare? Studies have shown that elevations in titers in ANCA do not predict disease flares. If a pt was ANCA-positive during a period of active disease, a persistently ANCAnegative status is consistent with, but not absolutely proof of remission. Absolute height of antibody titers does not correlate well with disease activity.
27 Should tissue biopsy be done? It depends on the clinical presentation. Predictive value of ANCA testing depends heavily upon clinical presentation of the pt. If the presentation is highly suggestive of WG for example, and C-ANCA with anti PR3 ab is present, tissue biopsy is not necessary before initiation of treatment. However, the recommendation per ACR states that the biopsy should be obtained whenever possible, and it should be a biopsy of involved organ before starting pt on long-term potentially toxic therapy.
28 Giant Cell Arteritis Affects the second- to fifth-order aortic branches, often in the extracranial aa of the head AKA temporal arteritis, cranial arteritis Aged 50+ years, mean age is 72 Women>men Epidemiology Scandinavian countries/n Eur (15-25 cases/100,000) Southern Europeans (6/100,000) Blacks, Hispanics (1-2/100,000) US-Olmsted County, Minnesota (17.8/100,000)

29 Giant Cell Arteritis
30 GCA-Clinical Features Two major symptomatic complexes Vascular insufficiency Usually occlusion, aorta-arterial wall dilatation Systemic inflammation Multiple variants/gca-pmr syndrome Cranial arteritis Large-vessel GCA/aortitis Fever/wasting syndrome Isolated PMR
 CNS ischemia TIA, CVA")
31 Cranial Arteritis Headaches- throbbing, sharp, or dull; unilateral or back of head Scalp tenderness Ischemic optic neuropathy blindness (sudden, painless, irreversible) Amaurosis fugax-intermittent visual blurring or diplopia with heat, exercise or postural changes Jaw claudication-talking, chewing ilicit pain (50%) CNS ischemia TIA, CVA (20-30%) PMR
32 Large-vessel GCA/Aortitis Large-vessel in 10-15% of pts, prefers carotid, subclavian, and axillary aa>femoral aa Usually lack cranial involvement, 50% TA bx-neg Aortic arch syndrome-claudication of the arms, absent or asymmetrical pulses, parasthesias, digital ischemia Aortitis-Aortic valve insufficiency, aortic aneurysm and dissection Risk thoracic aortic aneurysm increased 17-fold Ranges from silent aneurysm to dissection and rupture
33 Fever/Wasting Syndrome Fever and chills (occult presentation-gca is cause of FUO in up to 15% elderly) Need to exclude infection, malignancy Malaise, fatigue, anorexia, weight loss Night sweats Weakness Depression
34 Isolated PMR Pain and stiffness in shoulder and pelvic girdle muscles Peripheral synovitis (uncommon) Malaise, weight loss, sweats, and low-grade fever Elevated ESR and/or CRP, anemia 2-3x more common than GCA, same population Exclude other diagnoses but if Signs of vascular insufficiency i.e. claudication, bruits over aa, and discrepant BP readings high index of suspicion for GCA
35 GCA-Diagnosis Temporal artery Bx: False-negative bx in 10% of pts Short-term steroids (up to 2 weeks) is unlikely to interfere with results Labs: elevated ESR, CRP, IL-6, normochromic or hypochromic anemia, thrombocytosis, elevated Alk phos 25% of patients w/ + temporal bx had normal ESR Imaging-angiography (MRA, CTA, Doppler US)
36 GCA-Treatment Glucocorticoids 60mg of prednisone or equivalent Relief within 12 to 48 hours Cannot reverse intimal hyperplasia, may decrease ischemic complications by decreasing edema Once clinically stable, decrease dose by 10% q 1-2wks DMARDs: MTX not usually steroid-sparing Tocilizumab (anti-il6) FDA approved 5/22/17 ASA mg/day may decrease risk of visual loss and CNS ischemia
37 PMR Very steroid responsive which may help in diagnosis Treatment: steroids, 2/3 respond to prednisone<20mg/day Decrease by 2.5mg q days until 8mg then slower tapering may be required Higher required doses may indicate risk of developing GCA Prognosis good, disease self-limiting Some may develop seronegative RA-type picture requiring DMARDs
38 Takayasu s Arteritis Chronic granulomatous vasculitis characterized by stenosis, occlusion, and sometimes aneurysm of the large elastic arteries, especially aorta and its main branches May also affect coronary and pulmonary arteries AKA Pulseless disease-complete occlusion of upper extremeties AKA Aortic arch syndrome Primarily affects adolescent girls and young women <40yo, can start >40 esp. in Asians Incidence highest in Asia followed by South Americans but occurs in all races
39
40
41 TA-Clinical Features Generalized inflammatory syndrome with fever, night sweats, malaise, anorexia, weight loss, diffuse myalgias Late consequences-ischemic complications Carotid and vertebral- dizziness, tinnitus, HA, syncope, CVA, visual disturbances; facial muscle atrophy Brachiocephalic and subclavian-arm claudication, pulselessness, and discrepant blood pressures, bruits Aorta-Ischemic CAD, arrhythmia, CHF, AR Coronary aa-angina pectoralis Renal-renovascular HTN Mesenteric aa-n/v, ischemic bowel disease
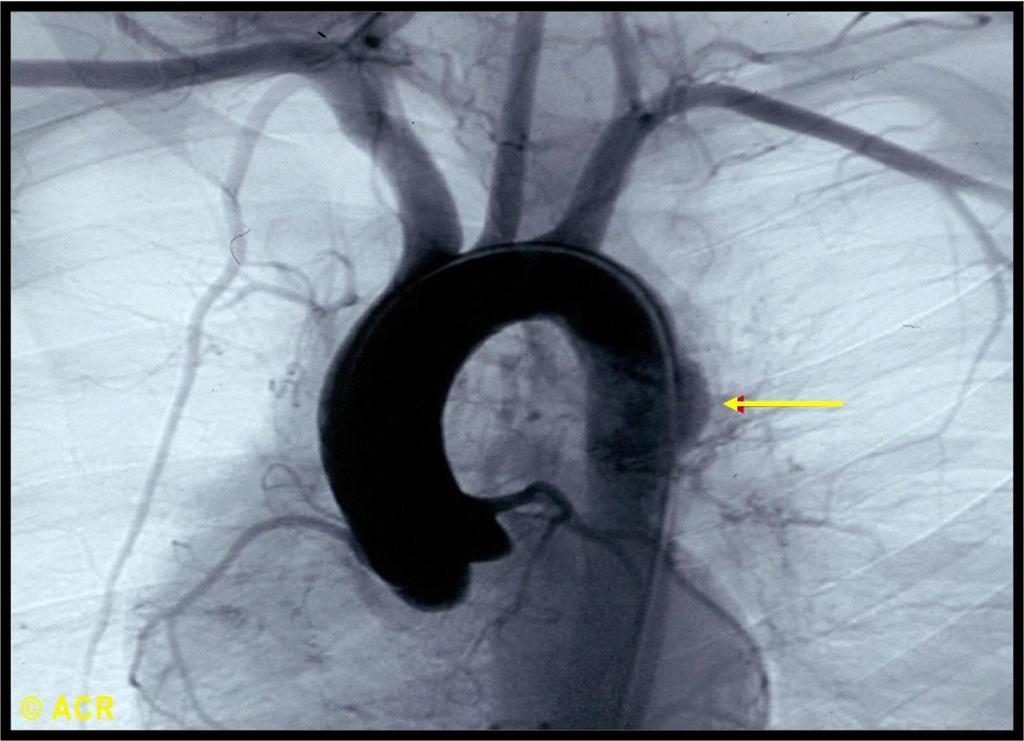
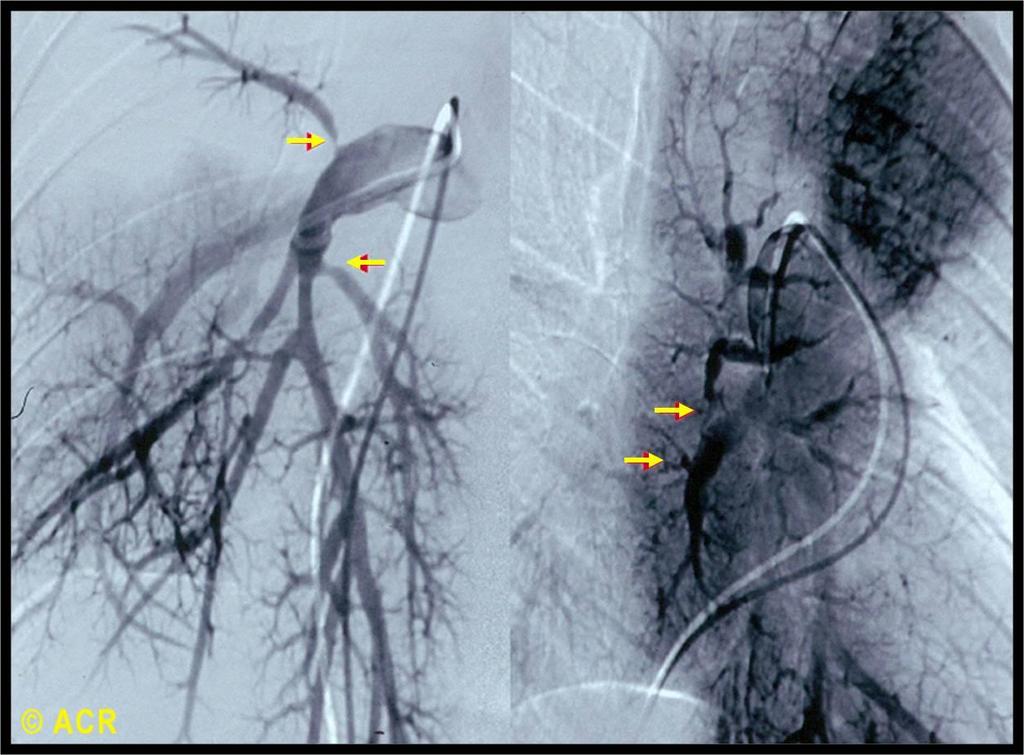
42 TA-Diagnosis High index of suspicion-vaso-occlusive disease and systemic inflammation in a young pt Dx: Angiography-long, smooth taperings of involved vessels, with collateralization in advanced cases MRI/MRA for serial assessments Doppler US for cervical vessels CTA for aorta and proximal vessels
43 TA-Treatment Some cases TA burn out while others have progressive or relapsing/remitting course Glucocorticoids: prednisone 40-60mg/day then taper 5mg/day q2wks until 10mg/day Monitor ESR, CRP but 50% of patients had progressing disease despite normal values ASA or other antiplatelet agent MTX up to 25mg/wk help improve remission and decrease steroids (no randomized trials) Azathioprine, MMF, cyclosponrine, TNF-blockers also success but no controlled studies Stenotic lesions are irreversible-no tx if collaterals Prognosis much improved; death d/t CHF, ischemic HD
44 Polyarteritis Nodosa Systemic vasculitis affects medium-sized arteries that supply the skin, gut, nerve, and kidney, but may affect multiple organs Incidence 2-9 cases per million annually M=F, all races and ages (mostly 40-60) May be p-anca positive but PR3- and MPO-ANCA negative Not associated with glomerulonephritis or pulmonary involvement
45 PAN Presents insidiously with nonspecific symptoms Fever, fatigue, malaise, myalgias, arthralgias Cutaneous involvement possible Diagnosis made when other systemic manifestions occur Associated w/ Hepatitis B infection and possibly hairy cell leukemia 77 per 1 million in a Hep B-hyperendemic Alaskan Eskimo population
46 PAN-Diagnosis Based on characteristic symptoms, PE findings, and lab, angiography and pathologic findings Abdominal angiography or biopsy recommended abdominal arteriography reveals strictures and aneurysms (beading) Differentiate from ANCA-associated vasculitis, cryoglobulinemia, and Buerger s disease R/O viral hepatitis, bacterial endocarditis, or other embolic disease; CTD-SLE, RA, SSc Lab-nonspecific: elevated acute phase reactants, anemia, renal insufficiency EMG/NCV-useful for confirming mononeuritis multiplex
47 PAN-1990 ACR Criteria Weight loss >4kg Livedo reticularis Testicular pain or tenderness Myalgias, weakness, or leg tenderness Mononeuropathy or polyneuropathy Diastolic BP>90mm Hg Elevated BUN (>40 mg/dl) or creatinine (>1.5 mg/dl) Hepatitis B virus Arteriographic abnormality-aneurysms or occlusions Biopsy of small or medium-sized vessel-granulocytes or leukocytes in the artery wall +PAN if 3 of 10 criteria are present Sensitiviyt-82.2%, specificity-86.6%
48 PAN Predelection for certain organs: Arteries to the kidney (70-80%) GI tract (50%) Peripheral nerves (50%) CNS (10%) Skin- livedo reticularis, nodules, ulcerations, ischemia of digits Cutaneous PAN-nodules and ulcers, primarily of lower legs, in crops and very painful

49 This 37 year old woman presented with low-grade fever, abdominal pain, arthralgia, myalgia, anemia, and elevated ESR and C-reactive protein. There are numerous aneurysms in the hepatic, splenic, renal, celiac, superior mesenteric and inferior mesenteric arteries.
50 PAN-Treatment Glucocorticoids-prednisone 1 mg/kg/day Will treat milder forms of the disease Rapidly progressive or organ-threatening cyclophosphamide is added to steroids Daily oral or monthly pulsed IV for 6 to 12 months Maintenance with azathioprine or MTX x 18 mos
51 Hypersensitivity Vasculitis AKA leukocytoclastic vasculitis, hypersensitivity angiitis Small-vessel vasculitis localized to the skin or may manifest in other organs, most commonly the joints, GI tract and kidneys Can be acute or chronic persons per million persons per year M=F, whites more common, any age (HSP in children)
52 LCV-Etiology Drugs: antibiotics, NSAIDs, and diuretics; foreign proteins such as streptokinase and those found in vaccines Infections: URIs, viral hepatitis, HIV, bacterial endocarditis, HCV (?virus or cryoglobulins) Foods, additives CVD in 10-15% of vasculitis cases RA, Sjögren syndrome and SLE; may indicate active dz Inflammatory bowel disease: Crohn s, UC Malignancy (< 1% ) lymphoproliferative diseases are more common, esp. hairy cell leukemia; however any tumor type Treatment of malignancy improves No cause is identified in up to 50% of patients
53 LCV-PE Cutaneous vasculitis-itching, burning, or pain, or they may have asymptomatic lesions May occur in the absence of systemic disease Palpable purpura-most common Round and 1-3 mm or coalesce to form plaques and may ulcerate Symmetric, dependent areas Urticarial lesions can burn more than itch Other rashes: Livedo reticularis, nodular lesions or ulceration Dx: skin biopsy
54 LCV-Treatment Removal of inciting agent, usually resolves in 1-2 weeks May need to stop many meds simultaneously then re-start them gradually Reserve glucocorticoids for patients with fulminant systemic disease May have relapsing/remitting course but restricted to the skin not requiring immunosuppressive tx
55 References Ball et al. Vasculitis, Second Ed. New York, Harris et al. Kelly Textbook of Rheumatology, Seventh Ed Jennette et al. Chapel Hill Consensus Conference on the nomenclature for systemic vasculitides Klippel et al. Primer on the Rheumatic Diseases, Thirteenth Ed. New York,
PAEDIATRIC VASCULITIS
 PAEDIATRIC VASCULITIS Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. OUTLINE Introduction
PAEDIATRIC VASCULITIS Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. OUTLINE Introduction
Dr Rodney Itaki Lecturer Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology
 Vasculitis Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Disease Spectrum Hypersensitivity vasculitis/microscopic
Vasculitis Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Disease Spectrum Hypersensitivity vasculitis/microscopic
Vasculitis. Edward Dwyer, M.D. Division of Rheumatology. Vasculitis
 Edward Dwyer, M.D. Division of Rheumatology VASCULITIS is a primary inflammatory disease process of the vasculature Determinants of the Clinical Manifestations of : Target organ involved Size of vessel
Edward Dwyer, M.D. Division of Rheumatology VASCULITIS is a primary inflammatory disease process of the vasculature Determinants of the Clinical Manifestations of : Target organ involved Size of vessel
Atlas of the Vasculitic Syndromes
 CHAPTER e40 Atlas of the Vasculitic Syndromes Carol A. Langford Anthony S. Fauci Diagnosis of the vasculitic syndromes is usually based upon characteristic histologic or arteriographic findings in a patient
CHAPTER e40 Atlas of the Vasculitic Syndromes Carol A. Langford Anthony S. Fauci Diagnosis of the vasculitic syndromes is usually based upon characteristic histologic or arteriographic findings in a patient
Mohammad Reza Shakibi M.D Kerman university of medical sciences (KMU) Shafa Hospital, Rheumatology ward
 Shafa Hospital, Rheumatology ward") VASCULITIS SYNDROMES Mohammad Reza Shakibi M.D Kerman university of medical sciences (KMU) Shafa Hospital, Rheumatology ward ILLUSTRATED CASE 1 A 56 years old lady refered me for prolonged fever, arthritis
VASCULITIS SYNDROMES Mohammad Reza Shakibi M.D Kerman university of medical sciences (KMU) Shafa Hospital, Rheumatology ward ILLUSTRATED CASE 1 A 56 years old lady refered me for prolonged fever, arthritis
The Vasculitis Syndromes
 The Vasculitis Syndromes Definition Inflammation and damage of blood vessels Single organ skin Several organ systems Primary Secondary Heterogeneity Overlap Primary Vasculitis Syndromes Wegener s granulomatosis
The Vasculitis Syndromes Definition Inflammation and damage of blood vessels Single organ skin Several organ systems Primary Secondary Heterogeneity Overlap Primary Vasculitis Syndromes Wegener s granulomatosis
VASCULITIC SYNDROMES. Howard L. Feinberg, D.O., F.A.C.O.I., F.A.C.R. OPSC 2018
 VASCULITIC SYNDROMES Howard L. Feinberg, D.O., F.A.C.O.I., F.A.C.R. OPSC 2018 2012 REVISED CHAPEL HILL CONSENSUS CONFERENCE Large vessel Takayasu arteritis Giant cell arteritis Medium Vessel Polyarteritis
VASCULITIC SYNDROMES Howard L. Feinberg, D.O., F.A.C.O.I., F.A.C.R. OPSC 2018 2012 REVISED CHAPEL HILL CONSENSUS CONFERENCE Large vessel Takayasu arteritis Giant cell arteritis Medium Vessel Polyarteritis
VASCULITIS. Case Presentation. Case Presentation
 VASCULITIS Case Presentation The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
VASCULITIS Case Presentation The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
Case Presentation VASCULITIS. Case Presentation. Case Presentation. Vasculitis
 Case Presentation VASCULITIS The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
Case Presentation VASCULITIS The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
SHO Teaching. Dr. Amir Bhanji Consultant Nephrologist, Q.A hospital, Portsmouth
 SHO Teaching Vasculitis Renal medicine Dr. Amir Bhanji Consultant Nephrologist, Q.A hospital, Portsmouth OUTLINE What is vasculitis Causes Classification Brief look into ANCA Associated Vasculitis (AAV)
SHO Teaching Vasculitis Renal medicine Dr. Amir Bhanji Consultant Nephrologist, Q.A hospital, Portsmouth OUTLINE What is vasculitis Causes Classification Brief look into ANCA Associated Vasculitis (AAV)
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated inflammation
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated inflammation
Annual Rheumatology & Therapeutics Review for Organizations & Societies
 Annual Rheumatology & Therapeutics Review for Organizations & Societies Update on Granulomatosis with Polyangiitis (Wegener s) Learning Objectives Identify the clinical features of granulomatosis with
Annual Rheumatology & Therapeutics Review for Organizations & Societies Update on Granulomatosis with Polyangiitis (Wegener s) Learning Objectives Identify the clinical features of granulomatosis with
Overview. = inflammation of vessel wall. Symptoms and signs depend on the tissue of which the vessels are affected
 Vasculitis (1+2) Overview = inflammation of vessel wall Symptoms and signs depend on the tissue of which the vessels are affected Often with systemic symptoms fever, myalgia, arthralgia, malaise etc. Most
Vasculitis (1+2) Overview = inflammation of vessel wall Symptoms and signs depend on the tissue of which the vessels are affected Often with systemic symptoms fever, myalgia, arthralgia, malaise etc. Most
Small Vessel Vasculitis
 Banff- Rocky Mountain Barry Kassen, MD, FRCPC,FACP Head, Division of Internal Medicine UBC/VGH/SPH Acting Head, Division of Community Internal Medicine November, 2009 Objectives 1. To understand small
Banff- Rocky Mountain Barry Kassen, MD, FRCPC,FACP Head, Division of Internal Medicine UBC/VGH/SPH Acting Head, Division of Community Internal Medicine November, 2009 Objectives 1. To understand small
A. Smržová. III. Interní klinika FN Olomouc nefrologická, revmatologická a endokrinologická
 A. Smržová III. Interní klinika FN Olomouc nefrologická, revmatologická a endokrinologická Systemic vasculitis destructive inflamatory of the walls of blood vessels. Pathologist Inflammatory destruction
A. Smržová III. Interní klinika FN Olomouc nefrologická, revmatologická a endokrinologická Systemic vasculitis destructive inflamatory of the walls of blood vessels. Pathologist Inflammatory destruction
GIANT CELL ARTERITIS. Page 1 of 6 Reproduction of this material requires written permission of the Vasculitis Foundation. Copyright 2018.
 What is giant cell arteritis (GCA)? Giant cell arteritis (GCA) is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict blood flow and damage
What is giant cell arteritis (GCA)? Giant cell arteritis (GCA) is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict blood flow and damage
Rituximab treatment for ANCA-associated vasculitis in childhood
 Rituximab treatment for ANCA-associated vasculitis in childhood DISCLOSURE I have no relevant financial relationships to disclose Katharine Moore MD Nov 14, 2012 University of Colorado School of Medicine
Rituximab treatment for ANCA-associated vasculitis in childhood DISCLOSURE I have no relevant financial relationships to disclose Katharine Moore MD Nov 14, 2012 University of Colorado School of Medicine
Vasculitides in Surgical Neuropathology Practice
 Vasculitides in Surgical Neuropathology Practice USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Vasculitides in Surgical Neuropathology Practice USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Vasculitis and Vasculitides. OMONDI OYOO Physician/Rheumatologist; Senior Lecturer, Department of Medicine University of Nairobi
 Vasculitis and Vasculitides OMONDI OYOO Physician/Rheumatologist; Senior Lecturer, Department of Medicine University of Nairobi Definition Presence of leucocytes in the vessel wall with reactive damage
Vasculitis and Vasculitides OMONDI OYOO Physician/Rheumatologist; Senior Lecturer, Department of Medicine University of Nairobi Definition Presence of leucocytes in the vessel wall with reactive damage
December 6, 2010 Asthma and Rheumatic Disorders and Vasculitis
 December 6, 2010 Asthma and Rheumatic Disorders and Vasculitis Lanny J. Rosenwasser, M.D. Dee Lyons/Missouri Endowed Chair in Immunology Research Professor of Pediatrics Allergy-Immunology Division Childrens
December 6, 2010 Asthma and Rheumatic Disorders and Vasculitis Lanny J. Rosenwasser, M.D. Dee Lyons/Missouri Endowed Chair in Immunology Research Professor of Pediatrics Allergy-Immunology Division Childrens
Done by: Shatha Khtoum
 Done by: Shatha Khtoum Overview Vasculitis -Vasculitis is a general term for vessel wall inflammation -Symptoms and signs depend on the tissue of which the vessels are affected. (slide 2) -There are usually
Done by: Shatha Khtoum Overview Vasculitis -Vasculitis is a general term for vessel wall inflammation -Symptoms and signs depend on the tissue of which the vessels are affected. (slide 2) -There are usually
9/11/11. Temporal Arteritis. Background. Background. Richard E. Castillo, OD, DO NORTHEASTERN STATE UNIVERSITY Director, Ophthalmic Surgery Service
 Temporal Arteritis Richard E. Castillo, OD, DO NORTHEASTERN STATE UNIVERSITY Director, Ophthalmic Surgery Service 1 Background Giant Cell Arteritis Temporal Arteritis Cranial Arteritis Granulomatous Arteritis
Temporal Arteritis Richard E. Castillo, OD, DO NORTHEASTERN STATE UNIVERSITY Director, Ophthalmic Surgery Service 1 Background Giant Cell Arteritis Temporal Arteritis Cranial Arteritis Granulomatous Arteritis
RARE JUVENILE PRIMARY SYSTEMIC VASCULITIS
 www.pediatric-rheumathology.printo.it RARE JUVENILE PRIMARY SYSTEMIC VASCULITIS WHAT IS IT? Vasculitis is an inflammation of blood vessels. Vasculitides cover a wide group of diseases. Primary vasculitis
www.pediatric-rheumathology.printo.it RARE JUVENILE PRIMARY SYSTEMIC VASCULITIS WHAT IS IT? Vasculitis is an inflammation of blood vessels. Vasculitides cover a wide group of diseases. Primary vasculitis
Rheumatology Primer: What Labs and When
 Rheumatology Primer: What Labs and When Irina Konon, MD Department of Internal Medicine Division of Rheumatology Medical College of Wisconsin Disclosures None 1 Objective Discuss principles of laboratory
Rheumatology Primer: What Labs and When Irina Konon, MD Department of Internal Medicine Division of Rheumatology Medical College of Wisconsin Disclosures None 1 Objective Discuss principles of laboratory
Vasculitis Prof. Dr. med. Katharina Glatz Pathologie
 Vasculitis 08-21-2018 Prof. Dr. med. Katharina Glatz Pathologie Agenda Anatomy and histology Vasculitis: Chapel Hill Classification Examples Giant cell arteritis Single organ vasculitis Artery or Vein?
Vasculitis 08-21-2018 Prof. Dr. med. Katharina Glatz Pathologie Agenda Anatomy and histology Vasculitis: Chapel Hill Classification Examples Giant cell arteritis Single organ vasculitis Artery or Vein?
Vasculitis. Seth Mark Berney, MD Professor of Medicine Chief, Division of Rheumatology University of Arkansas for Medical Sciences
 Vasculitis Seth Mark Berney, MD Professor of Medicine Chief, Division of Rheumatology University of Arkansas for Medical Sciences History A 50 year old white male with a history of intravenous drug use
Vasculitis Seth Mark Berney, MD Professor of Medicine Chief, Division of Rheumatology University of Arkansas for Medical Sciences History A 50 year old white male with a history of intravenous drug use
Small Vessel Vasculitis
 Small Vessel Vasculitis Paul A Brogan Professor of Vasculitis and Consultant Paediatric Rheumatologist Department of Rheumatology Institute of Child Health and Great Ormond St Hospital, London UK P.brogan@ucl.ac.uk
Small Vessel Vasculitis Paul A Brogan Professor of Vasculitis and Consultant Paediatric Rheumatologist Department of Rheumatology Institute of Child Health and Great Ormond St Hospital, London UK P.brogan@ucl.ac.uk
VASCULITIS AND VASCULOPATHY
 VASCULITIS AND VASCULOPATHY Mantosh S. Rattan @CincyKidsRad facebook.com/cincykidsrad Disclosure No relevant financial disclosures Outline Overview Referral pathways MR imaging Case examples Vasculitis
VASCULITIS AND VASCULOPATHY Mantosh S. Rattan @CincyKidsRad facebook.com/cincykidsrad Disclosure No relevant financial disclosures Outline Overview Referral pathways MR imaging Case examples Vasculitis
TAKAYASU S ARTERITIS. Second-stage symptoms include:
 What is Takayasu s arteritis (TAK)? Takayasu s arteritis (TAK) is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict blood flow and damage
What is Takayasu s arteritis (TAK)? Takayasu s arteritis (TAK) is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict blood flow and damage
SMALL TO MEDIUM VASCULITIS: RENAL ASPECT RATANA CHAWANASUNTORAPOJ UPDATE IN INTERNAL MEDICINE 2018
 SMALL TO MEDIUM VASCULITIS: RENAL ASPECT RATANA CHAWANASUNTORAPOJ UPDATE IN INTERNAL MEDICINE 2018 OUTLINE Renal involvement in vasculitis Curr Rheumatol Rep 2013 Renal involvement in ANCA vasculitis GN***:
SMALL TO MEDIUM VASCULITIS: RENAL ASPECT RATANA CHAWANASUNTORAPOJ UPDATE IN INTERNAL MEDICINE 2018 OUTLINE Renal involvement in vasculitis Curr Rheumatol Rep 2013 Renal involvement in ANCA vasculitis GN***:
ANCA associated vasculitis in China
 ANCA associated vasculitis in China Min Chen Renal Division, Peking University First Hospital, Beijing 100034, P. R. China 1 General introduction of AAV in China Disease spectrum and ANCA type Clinical
ANCA associated vasculitis in China Min Chen Renal Division, Peking University First Hospital, Beijing 100034, P. R. China 1 General introduction of AAV in China Disease spectrum and ANCA type Clinical
GRANULOMATOSIS WITH POLYANGIITIS
 What is granulomatosis with polyangiitis (GPA)? Granulomatosis with polyangiitis (GPA) is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict
What is granulomatosis with polyangiitis (GPA)? Granulomatosis with polyangiitis (GPA) is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict
Management of Acute Vasculitis. CMT teaching 3 rd June 2015 Caroline Wroe
 Management of Acute Vasculitis CMT teaching 3 rd June 2015 Caroline Wroe Vasculitis pub quiz Match the date with the event Dr Peter McBride, Scottish Otolaryngologist describes a disease of rapid destruction
Management of Acute Vasculitis CMT teaching 3 rd June 2015 Caroline Wroe Vasculitis pub quiz Match the date with the event Dr Peter McBride, Scottish Otolaryngologist describes a disease of rapid destruction
EUVAS update June 5 th Marinka Twilt
 EUVAS update June 5 th 2012 Marinka Twilt Chapel Hill 2012 Classification Large Vessel Vasculitis (LVV) Medium Vessel Vasculitis (MVV) Small Vessel Vasculitis (SVV) Variable Vessel Vasculitis (VVV) Single
EUVAS update June 5 th 2012 Marinka Twilt Chapel Hill 2012 Classification Large Vessel Vasculitis (LVV) Medium Vessel Vasculitis (MVV) Small Vessel Vasculitis (SVV) Variable Vessel Vasculitis (VVV) Single
Diagnostic Procedures for Vasculitis
 Diagnostic Procedures for Vasculitis Toshiharu Matsumoto, MD Clinical Professor of Department of Diagnostic Pathology Juntendo University Nerima Hospital, Tokyo, Japan Introduction In 1994, the International
Diagnostic Procedures for Vasculitis Toshiharu Matsumoto, MD Clinical Professor of Department of Diagnostic Pathology Juntendo University Nerima Hospital, Tokyo, Japan Introduction In 1994, the International
Scleritis LEN V KOH OD
 Scleritis LEN V KOH OD 2014 PUCO 1 Introduction A painful, destructive, and potentially blinding disorder Highly symptomatic High association with systemic disease Immunosuppresssive agents 2014 PUCO 2
Scleritis LEN V KOH OD 2014 PUCO 1 Introduction A painful, destructive, and potentially blinding disorder Highly symptomatic High association with systemic disease Immunosuppresssive agents 2014 PUCO 2
AN OVERVIEW OF ANCA-ASSOCIATED VASCULITIS
 GRANULOMATOSIS WITH POLYANGIITIS (GPA), MICROSCOPIC POLYANGIITIS (MPA), and EOSINOPHILIC GRANULOMATOSIS WITH POLYANGIITIS (EGPA) AN OVERVIEW OF ANCA-ASSOCIATED VASCULITIS What is ANCA-associated Vasculitis?
GRANULOMATOSIS WITH POLYANGIITIS (GPA), MICROSCOPIC POLYANGIITIS (MPA), and EOSINOPHILIC GRANULOMATOSIS WITH POLYANGIITIS (EGPA) AN OVERVIEW OF ANCA-ASSOCIATED VASCULITIS What is ANCA-associated Vasculitis?
TREATMENT OF ANCA-ASSOCIATED VASCULITIS
 TREATMENT OF ANCA-ASSOCIATED VASCULITIS Loïc Guillevin Hôpital Cochin, Université Paris Descartes Cours DU, 11 mars 2016 1 Disclosure of interest regarding this presentation Roche has provided, in part,
TREATMENT OF ANCA-ASSOCIATED VASCULITIS Loïc Guillevin Hôpital Cochin, Université Paris Descartes Cours DU, 11 mars 2016 1 Disclosure of interest regarding this presentation Roche has provided, in part,
FAQ Identifying and enrolling participants
 FAQ Identifying and enrolling participants WHO IS ELIGIBLE - CASES? Patients with a new diagnosis of primary systemic vasculitis Patients suitable as cases are over 18 years with a new presentation or
FAQ Identifying and enrolling participants WHO IS ELIGIBLE - CASES? Patients with a new diagnosis of primary systemic vasculitis Patients suitable as cases are over 18 years with a new presentation or
CUTANEOUS VASCULITIS. Katharine Warburton ST6 Dermatology
 CUTANEOUS VASCULITIS Katharine Warburton ST6 Dermatology AIMS Clinical cases introduction The theory Categorising cutaneous vasculitis Features presenting in the skin Mimics/pitfalls How to initially manage
CUTANEOUS VASCULITIS Katharine Warburton ST6 Dermatology AIMS Clinical cases introduction The theory Categorising cutaneous vasculitis Features presenting in the skin Mimics/pitfalls How to initially manage
CHECK LIST FORM-SCREENING
 CHECK LIST FORM-SCREENING Participant Initials: Date of Birth: Evaluation Date: Were the following forms completed for this visit? Eligibility Form Done t Done Baseline medical History Form Done t Done
CHECK LIST FORM-SCREENING Participant Initials: Date of Birth: Evaluation Date: Were the following forms completed for this visit? Eligibility Form Done t Done Baseline medical History Form Done t Done
vasculitis Patomorfologia vasculitis (arteritis) caused by infections vasculitis (arteritis) caused by infections
 caused by infections vasculitis (arteritis) caused by infections") Patomorfologia Lecture 12 prof hab. n. med. Andrzej Marszałek VASCULITIS infectious vasculitis non-infectious causes: Aspergillus Rickettsiae vasculitis (arteritis) caused by infections Mucormycosis syphylis
Patomorfologia Lecture 12 prof hab. n. med. Andrzej Marszałek VASCULITIS infectious vasculitis non-infectious causes: Aspergillus Rickettsiae vasculitis (arteritis) caused by infections Mucormycosis syphylis
Shawkat Michel, M.D.
 Vasculitis / Polyarteritis nodosa (PAN) Shawkat Michel, M.D. Case presentation: 87 yo, wf was referred in May 1998 with decreased VA OD and photophobia > one year duration. The patient had been on topical
Vasculitis / Polyarteritis nodosa (PAN) Shawkat Michel, M.D. Case presentation: 87 yo, wf was referred in May 1998 with decreased VA OD and photophobia > one year duration. The patient had been on topical
Tell me more about vasculitis. Lisa Willcocks Consultant in Nephrology and Vasculitis, Addenbrooke s Hospital
 Tell me more about vasculitis Lisa Willcocks Consultant in Nephrology and Vasculitis, Addenbrooke s Hospital Talk overview Case study ANCA-associated vasculitis What is ANCA vasculitis? What causes ANCA
Tell me more about vasculitis Lisa Willcocks Consultant in Nephrology and Vasculitis, Addenbrooke s Hospital Talk overview Case study ANCA-associated vasculitis What is ANCA vasculitis? What causes ANCA
Wegener s Granulomatosis JUN-KI PARK
 Wegener s Granulomatosis JUN-KI PARK Definition History Epidemiology Clinical symptoms Pathophysiology Treatment Wegener granulomatosis (WG) is a complex, immunemediated disorder, which along with microscopic
Wegener s Granulomatosis JUN-KI PARK Definition History Epidemiology Clinical symptoms Pathophysiology Treatment Wegener granulomatosis (WG) is a complex, immunemediated disorder, which along with microscopic
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A ANCA vasculitis. See Antineutrophil cytoplasmic antibody associated (ANCA) vasculitis Angiography 54 Antineutrophil cytoplasmic antibody correlation
Note: Page numbers of article titles are in boldface type. A ANCA vasculitis. See Antineutrophil cytoplasmic antibody associated (ANCA) vasculitis Angiography 54 Antineutrophil cytoplasmic antibody correlation
NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES
 NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES Leslie M. Scoutt, MD, FACR Professor of Diagnostic Radiology & Surgery Vice Chair, Dept of Radiology & Biomedical Imaging Chief, Ultrasound Section
NON-ATHEROSCLEROTIC PATHOLOGY OF THE CAROTID ARTERIES Leslie M. Scoutt, MD, FACR Professor of Diagnostic Radiology & Surgery Vice Chair, Dept of Radiology & Biomedical Imaging Chief, Ultrasound Section
ST - segment Elevation Myocardial Infarction complicating an atypical Kawasaki disease
 ST - segment Elevation Myocardial Infarction complicating an atypical Kawasaki disease Raluca PRISECARU, Marc VINCENT, Steven VERCAUTEREN Brussels Heart Center, Brussels, Belgium Disclosure None Clinical
ST - segment Elevation Myocardial Infarction complicating an atypical Kawasaki disease Raluca PRISECARU, Marc VINCENT, Steven VERCAUTEREN Brussels Heart Center, Brussels, Belgium Disclosure None Clinical
A number of factors point to the likelihood of a person with RA developing RV:
 What is rheumatoid vasculitis (RV)? Rheumatoid vasculitis (RV) is a rare but serious complication of rheumatoid arthritis (RA) an inflammatory disease that causes severe joint pain and damage, and can
What is rheumatoid vasculitis (RV)? Rheumatoid vasculitis (RV) is a rare but serious complication of rheumatoid arthritis (RA) an inflammatory disease that causes severe joint pain and damage, and can
Update in Vasculitis. Anatomy of vasculitis. General Principles of Vasculitis. Not necessarily as rare as one might think
 Black Hole Vasculitis Update in Vasculitis Advances In Internal Medicine 2015 Jonathan Graf, MD Professor of Clinical Medicine, UCSF Division of Rheumatology, SFGH Rare Poorly understood mystery of universe
Black Hole Vasculitis Update in Vasculitis Advances In Internal Medicine 2015 Jonathan Graf, MD Professor of Clinical Medicine, UCSF Division of Rheumatology, SFGH Rare Poorly understood mystery of universe
CHECK LIST FORM-MONTH 27 (Please note Month 27 is from enrolment not randomisation)
") CHECK LIST FORM-MONTH 27 (Please note Month 27 is from enrolment not randomisation) Participant Initials: Date of Birth: Were the following forms completed for this visit? Follow Up Form Done t Done BVASWG
CHECK LIST FORM-MONTH 27 (Please note Month 27 is from enrolment not randomisation) Participant Initials: Date of Birth: Were the following forms completed for this visit? Follow Up Form Done t Done BVASWG
Disclosures. Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies. None
 Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies Sarah Goglin MD Assistant Professor of Medicine Division of Rheumatology Disclosures None 1 [footer
Rheumatological Approaches to Differential Diagnosis, Physical Examination, and Interpretation of Studies Sarah Goglin MD Assistant Professor of Medicine Division of Rheumatology Disclosures None 1 [footer
Takayasu s Arteritis: A Case Report With Global Arterial Involvement
 1 Case Report Takayasu s Arteritis: A Case Report With Global Arterial Involvement Waqas Ahmed, Zeeshan Ahmad* From Shifa International Hospital H-8/4, Islamabad, Pakistan Correspondence: Dr Waqas Ahmed,
1 Case Report Takayasu s Arteritis: A Case Report With Global Arterial Involvement Waqas Ahmed, Zeeshan Ahmad* From Shifa International Hospital H-8/4, Islamabad, Pakistan Correspondence: Dr Waqas Ahmed,
Vasculitis (Polyarteritis Nodosa, Microscopic Polyangiitis, Wegener s Granulomatosis, Henoch- Schönlein Purpura)
") Vasculitis (Polyarteritis Nodosa, Microscopic Polyangiitis, Wegener s Granulomatosis, Henoch- Schönlein Purpura) J. Charles Jennette Ronald J. Falk The kidneys are affected by a variety of systemic vasculitides
Vasculitis (Polyarteritis Nodosa, Microscopic Polyangiitis, Wegener s Granulomatosis, Henoch- Schönlein Purpura) J. Charles Jennette Ronald J. Falk The kidneys are affected by a variety of systemic vasculitides
Vasculitis. Marwan Adwan. 4 th year MBBS. Consultant Rheumatologist. MBChB, MRCPI, MSc, MRCP (rheum)
") Vasculitis 4 th year MBBS Marwan Adwan MBChB, MRCPI, MSc, MRCP (rheum) Consultant Rheumatologist Case 1 A 45 man presents with 3 wk hx of fever, fatigue, malaise, abdo pain and polyarthralgia. He noticed
Vasculitis 4 th year MBBS Marwan Adwan MBChB, MRCPI, MSc, MRCP (rheum) Consultant Rheumatologist Case 1 A 45 man presents with 3 wk hx of fever, fatigue, malaise, abdo pain and polyarthralgia. He noticed
Managing Acute Medical Problems, Birmingham Vasculitis. David Jayne. University of Cambridge
 Managing Acute Medical Problems, Birmingham 2016 Vasculitis David Jayne University of Cambridge Disclosures Astra Zeneca, Aurinia, BIOGEN, Boehringer, Chemocentryx, Genzyme/Sanofi, GSK, Lilly, Medimmune,
Managing Acute Medical Problems, Birmingham 2016 Vasculitis David Jayne University of Cambridge Disclosures Astra Zeneca, Aurinia, BIOGEN, Boehringer, Chemocentryx, Genzyme/Sanofi, GSK, Lilly, Medimmune,
Diagnostic Tests in Rheumatic Disease: What s Old, What s New & What s Useful? COPYRIGHT
 Diagnostic Tests in Rheumatic Disease: What s Old, What s New & What s Useful? Robert H. Shmerling, M.D. Beth Israel Deaconess Medical Center Boston, MA Diagnostic Tests in Rheumatic Disease: What's Old,
Diagnostic Tests in Rheumatic Disease: What s Old, What s New & What s Useful? Robert H. Shmerling, M.D. Beth Israel Deaconess Medical Center Boston, MA Diagnostic Tests in Rheumatic Disease: What's Old,
UNFOLDING NATURE S ORIGAMI: MEDICAL TREATMENT OF TAKAYASU ARTERITIS AND GIANT CELL ARTERITIS
 UNFOLDING NATURE S ORIGAMI: MEDICAL TREATMENT OF TAKAYASU ARTERITIS AND GIANT CELL ARTERITIS CanVasc meeting Montreal Nov 22 2012 Patrick Liang Service de rhumatologie Centre Hospitalier Universitaire
UNFOLDING NATURE S ORIGAMI: MEDICAL TREATMENT OF TAKAYASU ARTERITIS AND GIANT CELL ARTERITIS CanVasc meeting Montreal Nov 22 2012 Patrick Liang Service de rhumatologie Centre Hospitalier Universitaire
CHECK LIST FORM-SCREENING
 CHECK LIST FORM-SCREENING Participant Initials: Date of Birth: Evaluation Date: Were the following forms completed for this visit? Eligibility Form Done t Done Baseline medical History Form Done t Done
CHECK LIST FORM-SCREENING Participant Initials: Date of Birth: Evaluation Date: Were the following forms completed for this visit? Eligibility Form Done t Done Baseline medical History Form Done t Done
Granulomatosis with Polyangiitis (Wegener s)
") August 2011 Granulomatosis with Polyangiitis (Wegener s) Andrew Noll, Harvard Medical School, Year III Agenda Patient presentation Overview of granulomatosis with polyangiitis (Wegener s), abbreviated
August 2011 Granulomatosis with Polyangiitis (Wegener s) Andrew Noll, Harvard Medical School, Year III Agenda Patient presentation Overview of granulomatosis with polyangiitis (Wegener s), abbreviated
*HSP is a common vasculitis of small vessels with cutaneous & systemic complications. Its etiology is unknown& often follows URTIs.
 BY Introduction The disease is eponymously named after Eduard heinrich Henoch (1820-1910), a German pediatrician, and his teacher Johann Lukas Schonlein (1793-1864), who described it in the 1860s. Cont
BY Introduction The disease is eponymously named after Eduard heinrich Henoch (1820-1910), a German pediatrician, and his teacher Johann Lukas Schonlein (1793-1864), who described it in the 1860s. Cont
RAPIDLY FAILING KIDNEYS. Dr Paul Johny 2 nd yr DNB Medicine Resident
 RAPIDLY FAILING KIDNEYS Dr Paul Johny 2 nd yr DNB Medicine Resident Mr Z 67yrs old Occupation : Retired officer from electricity board Chief complaints : Fever : 5 days Right lower limb swelling and pain
RAPIDLY FAILING KIDNEYS Dr Paul Johny 2 nd yr DNB Medicine Resident Mr Z 67yrs old Occupation : Retired officer from electricity board Chief complaints : Fever : 5 days Right lower limb swelling and pain
CENTRAL NERVOUS SYSTEM VASCULITIS
 What is central nervous system (CNS) vasculitis? Central nervous system (CNS) vasculitis is among a family of rare disorders characterized by inflammation of the blood vessels, which restricts blood flow
What is central nervous system (CNS) vasculitis? Central nervous system (CNS) vasculitis is among a family of rare disorders characterized by inflammation of the blood vessels, which restricts blood flow
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
Autoimmune Disease. Autoimmunity. Epidemiology. ACR Criteria for Diagnosis. Signs and Symptoms. Autoreactivity: Reactivity to self antigens:
 Autoimmunity Reactivity to self antigens: Autoreactivity: Autoimmune Disease T cells B cells Leading to tissue damage or dysfunction Occurring in the absence of ongoing infection Epidemiology SLE Pathogenesis
Autoimmunity Reactivity to self antigens: Autoreactivity: Autoimmune Disease T cells B cells Leading to tissue damage or dysfunction Occurring in the absence of ongoing infection Epidemiology SLE Pathogenesis
Preventing blindness: Ultrasound in Giant cell arteritis
 Preventing blindness: Ultrasound in Giant cell arteritis Elizabeth Jernberg, MD Associate Clinical Professor of Medicine Division of Rheumatology University of Washington Virginia Mason Medical Center
Preventing blindness: Ultrasound in Giant cell arteritis Elizabeth Jernberg, MD Associate Clinical Professor of Medicine Division of Rheumatology University of Washington Virginia Mason Medical Center
Autoimmunity. Autoimmune Disease
 Autoimmunity Reactivity to self antigens: T cells B cells Autoimmune Disease Autoreactivity: Leading to tissue damage or dysfunction Occurring in the absence of ongoing infection 1 SLE Pathogenesis Immune
Autoimmunity Reactivity to self antigens: T cells B cells Autoimmune Disease Autoreactivity: Leading to tissue damage or dysfunction Occurring in the absence of ongoing infection 1 SLE Pathogenesis Immune
Disclosures. Objectives. Vasculitis: What The Primary Care Physician Needs To Know. Definition & Classification of Vasculitis
 Vasculitis: What The Primary Care Physician Needs To Know Lynn Fussner, MD Assistant Professor - Clinical Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Vasculitis: What The Primary Care Physician Needs To Know Lynn Fussner, MD Assistant Professor - Clinical Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Vasculitis: What The Primary Care Physician Needs To Know. Lynn Fussner, MD
 Vasculitis: What The Primary Care Physician Needs To Know Lynn Fussner, MD Assistant Professor - Clinical Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Vasculitis: What The Primary Care Physician Needs To Know Lynn Fussner, MD Assistant Professor - Clinical Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Crescentic Glomerulonephritis (RPGN)
") Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Vasculitis of the peripheral nervous system
 4 rd Congress of the European Academy of Neurology Lisbon, Portugal, June 16-19, 2018 Teaching Course 5 Acute emergencies in neuromuscular disease - Level 2 Vasculitis of the peripheral nervous system
4 rd Congress of the European Academy of Neurology Lisbon, Portugal, June 16-19, 2018 Teaching Course 5 Acute emergencies in neuromuscular disease - Level 2 Vasculitis of the peripheral nervous system
RATIONALE. K Without therapy, ANCA vasculitis with GN is associated. K There is high-quality evidence for treatment with
 http://www.kidney-international.org chapter 13 & 2012 KDIGO Chapter 13: Pauci-immune focal and segmental necrotizing glomerulonephritis Kidney International Supplements (2012) 2, 233 239; doi:10.1038/kisup.2012.26
http://www.kidney-international.org chapter 13 & 2012 KDIGO Chapter 13: Pauci-immune focal and segmental necrotizing glomerulonephritis Kidney International Supplements (2012) 2, 233 239; doi:10.1038/kisup.2012.26
Update on nomenclature and classification of vasculitis
 Update on nomenclature and classification of vasculitis Mohammadreza Shakibi M.D. Kerman university of medical sciences (KMU) Shafa Hospital, Rheumatology ward Adolph Kussmaul (1822 1902) First Modern
Update on nomenclature and classification of vasculitis Mohammadreza Shakibi M.D. Kerman university of medical sciences (KMU) Shafa Hospital, Rheumatology ward Adolph Kussmaul (1822 1902) First Modern
Polymyalgia Rheumatica; Giant Cell Arteritis Paul Katzenstein, MD
 Polymyalgia Rheumatica; Giant Cell Arteritis Paul Katzenstein, MD What is it; is it not? How is this thought about, characterized, understood, treated Time honored published clinical experience Clinical
Polymyalgia Rheumatica; Giant Cell Arteritis Paul Katzenstein, MD What is it; is it not? How is this thought about, characterized, understood, treated Time honored published clinical experience Clinical
EDITORIAL. Issue Seventeen, October Editorial Team. Issue Seventeen. Info link
 EDITORIAL, October 2004 Welcome to the Spring 2004 Edition of InfoLink. The feature article in this edition has been written by Dr Rodger Laurent, Head of Department, PaLMS Rheumatology Laboratory. The
EDITORIAL, October 2004 Welcome to the Spring 2004 Edition of InfoLink. The feature article in this edition has been written by Dr Rodger Laurent, Head of Department, PaLMS Rheumatology Laboratory. The
The role of pathology in the diagnosis of systemic vasculitis
 Clinical and Experimental Rheumatology 2007; 25: S52-S56 The role of pathology in the diagnosis of systemic vasculitis J.C. Jennette 1, R.J. Falk 2 1 Brinkhous Distinguished Professor and Chair of Pathology
Clinical and Experimental Rheumatology 2007; 25: S52-S56 The role of pathology in the diagnosis of systemic vasculitis J.C. Jennette 1, R.J. Falk 2 1 Brinkhous Distinguished Professor and Chair of Pathology
KAWASAKI DISEASE. What is Kawasaki disease? Causes
 What is Kawasaki disease? Kawasaki disease is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict blood flow and damage vital organs and
What is Kawasaki disease? Kawasaki disease is a form of vasculitis a family of rare disorders characterized by inflammation of the blood vessels, which can restrict blood flow and damage vital organs and
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Cerebrovascular Disease
 Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
Neuropathology lecture series Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O 2 consumption (resting):
Polymyalgia, Temporal Arteritis and pineapples
 Polymyalgia, Temporal Arteritis and pineapples Rod Hughes Consultant Rheumatologist Ashford St Peter s Hospital Trust Chertsey Wed 11 th May 2011 Meeting aims Pineapples their significance in disease Defining
Polymyalgia, Temporal Arteritis and pineapples Rod Hughes Consultant Rheumatologist Ashford St Peter s Hospital Trust Chertsey Wed 11 th May 2011 Meeting aims Pineapples their significance in disease Defining
Subclavian artery Stenting
 Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
Subclavian artery Stenting Etiology Atherosclerosis Takayasu s arteritis Fibromuscular dysplasia Giant Cell Arteritis Radiation-induced Vascular Injury Thoracic Outlet Syndrome Neurofibromatosis Incidence
Cardiovascular Pathology
 Cardiovascular Pathology Duration: 03 Weeks (15 days) Concepts Objectives Activity Time Department Comments 3/SBM-3/01 Introduction to ischaemia, infarction, thrombosis stenosis / occlusion, embolism Atherosclerosis
Cardiovascular Pathology Duration: 03 Weeks (15 days) Concepts Objectives Activity Time Department Comments 3/SBM-3/01 Introduction to ischaemia, infarction, thrombosis stenosis / occlusion, embolism Atherosclerosis
Lung diseases of Vascular Origin. By: Shefaa Qa qqa
 Lung diseases of Vascular Origin By: Shefaa Qa qqa Pulmonary Hypertension Pulmonary hypertension is defined as a mean pulmonary artery pressure greater than or equal to 25 mm Hg at rest. Based on underlying
Lung diseases of Vascular Origin By: Shefaa Qa qqa Pulmonary Hypertension Pulmonary hypertension is defined as a mean pulmonary artery pressure greater than or equal to 25 mm Hg at rest. Based on underlying
Cardiac Pathology & Rehabilitation
 Cardiac Pathology & Rehabilitation Which of the following best describes the physical activity performed in my leisure time? A. I perform vigorous physical activity 3X/week for 20 minutes each time B.
Cardiac Pathology & Rehabilitation Which of the following best describes the physical activity performed in my leisure time? A. I perform vigorous physical activity 3X/week for 20 minutes each time B.
Review Article. Current concepts in Anti-Neutrophil Cytoplasmic Antibody (ANCA) associated Vasculitis. Milind Aurangabadkar
 associated Vasculitis. Milind Aurangabadkar") Review Article Vidarbha Journal of Internal Medicine Volume 23 July 207 Current concepts in Anti-Neutrophil Cytoplasmic Antibody (ANCA) associated Vasculitis Milind Aurangabadkar ABSTRACT Anti-neutrophil
Review Article Vidarbha Journal of Internal Medicine Volume 23 July 207 Current concepts in Anti-Neutrophil Cytoplasmic Antibody (ANCA) associated Vasculitis Milind Aurangabadkar ABSTRACT Anti-neutrophil
Vasculitis Update. A selective review of what s new. Dr Jonathan Akikusa MBBS FRACP
 Vasculitis Update A selective review of what s new Dr Jonathan Akikusa MBBS FRACP Consultant Paediatric Rheumatologist Royal Children s Hospital, Melbourne Honorary Research Fellow Murdoch Children s Research
Vasculitis Update A selective review of what s new Dr Jonathan Akikusa MBBS FRACP Consultant Paediatric Rheumatologist Royal Children s Hospital, Melbourne Honorary Research Fellow Murdoch Children s Research
Pharmacy Management Drug Policy
 SUBJECT: : Nucala (mepolizumab), Cinqair (reslizumab), & Fasenra (benralizumab) POLICY NUMBER: Pharmacy-62 EFFECTIVE DATE: 12/15 LAST REVIEW DATE: 3/5/2018 If the member s subscriber contract excludes
SUBJECT: : Nucala (mepolizumab), Cinqair (reslizumab), & Fasenra (benralizumab) POLICY NUMBER: Pharmacy-62 EFFECTIVE DATE: 12/15 LAST REVIEW DATE: 3/5/2018 If the member s subscriber contract excludes
Essential Rheumatology. Dr Ellen Bruce Consultant Rheumatologist CMFT
 Essential Rheumatology Dr Ellen Bruce Consultant Rheumatologist CMFT Saving the best for last! Apparently people recall best the first and last thing they re told. Far too difficult to include everything.
Essential Rheumatology Dr Ellen Bruce Consultant Rheumatologist CMFT Saving the best for last! Apparently people recall best the first and last thing they re told. Far too difficult to include everything.
Vasculitis and the Dermatologist: General approach, pitfalls, and pearls
 Vasculitis and the Dermatologist: General approach, pitfalls, and pearls Robert G. Micheletti, MD Assistant Professor of Dermatology and Medicine Director, Cutaneous Vasculitis Clinic, Penn Vasculitis
Vasculitis and the Dermatologist: General approach, pitfalls, and pearls Robert G. Micheletti, MD Assistant Professor of Dermatology and Medicine Director, Cutaneous Vasculitis Clinic, Penn Vasculitis
A prospective study of vasculitis patients collected in a five year period: evaluation of the Chapel Hill nomenclature
 478 Bispebjerg Hospital, 2400 Copenhagen NV, Denmark S F Sørensen Hvidovre Hospital, Hvidovre, Denmark O Slot N Tvede Rigshospitalet, National University Hospital, Copenhagen, Denmark J Petersen Correspondence
478 Bispebjerg Hospital, 2400 Copenhagen NV, Denmark S F Sørensen Hvidovre Hospital, Hvidovre, Denmark O Slot N Tvede Rigshospitalet, National University Hospital, Copenhagen, Denmark J Petersen Correspondence
VCRC-OMERACT ANCA-Vasculitis Outcome Measure Initiative Comparative Outcome Measure Exercise-Training Cases
 Introduction to Training Cases The purpose of this preliminary exercise is to familiarize you with the rules and logistics of the five instruments under study. Please do not read the Training Cases until
Introduction to Training Cases The purpose of this preliminary exercise is to familiarize you with the rules and logistics of the five instruments under study. Please do not read the Training Cases until
29 Glomerular disease: an overview
 29 Glomerular : an overview Renal Extra-renal Neurological changes Clinical syndromes pressure Sore throat (streptococcal) Rash Cardiac valve lesions Hemoptysis Asymptomatic or Acute Glomerulonephritis
29 Glomerular : an overview Renal Extra-renal Neurological changes Clinical syndromes pressure Sore throat (streptococcal) Rash Cardiac valve lesions Hemoptysis Asymptomatic or Acute Glomerulonephritis
Neuropathology lecture series. III. Neuropathology of Cerebrovascular Disease. Physiology of cerebral blood flow
 Neuropathology lecture series III. Neuropathology of Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O
Neuropathology lecture series III. Neuropathology of Cerebrovascular Disease Physiology of cerebral blood flow Brain makes up only 2% of body weight Percentage of cardiac output: 15-20% Percentage of O
Case Presentation. Rafid Asfar, MD
 Case Presentation Rafid Asfar, MD Introduction ANCA associated vasculitis may be localized or systemic, and can involve the eyes Ocular manifestations can occur in the absence of systemic disease in persons
Case Presentation Rafid Asfar, MD Introduction ANCA associated vasculitis may be localized or systemic, and can involve the eyes Ocular manifestations can occur in the absence of systemic disease in persons
Everyday Vasculitis (or what questions do we get asked most!) Lucy Smyth Renal Consultant
 Lucy Smyth Renal Consultant") Everyday Vasculitis (or what questions do we get asked most!) Lucy Smyth Renal Consultant What is it? Why have I got it? How can we treat it? Why do I feel like I do? What do the blood tests mean? Will
Everyday Vasculitis (or what questions do we get asked most!) Lucy Smyth Renal Consultant What is it? Why have I got it? How can we treat it? Why do I feel like I do? What do the blood tests mean? Will
AKI Case study -Vasculitis. Sarah Mackie Renal Practice Development Nurse King s College Hospital - London
 AKI Case study -Vasculitis Sarah Mackie Renal Practice Development Nurse King s College Hospital - London What is vasculitis Vasculitis refers to inflammation of the blood vessels, including arteries,
AKI Case study -Vasculitis Sarah Mackie Renal Practice Development Nurse King s College Hospital - London What is vasculitis Vasculitis refers to inflammation of the blood vessels, including arteries,
APPROACH TO PATIENTS WITH POLYARTHRALGIA
 APPROACH TO PATIENTS WITH POLYARTHRALGIA Scott Vogelgesang, MD Division of Immunology University of Iowa No conflicts of interest DEFINITIONS Arthralgia joint pain with no evidence of inflammation Arthritis
APPROACH TO PATIENTS WITH POLYARTHRALGIA Scott Vogelgesang, MD Division of Immunology University of Iowa No conflicts of interest DEFINITIONS Arthralgia joint pain with no evidence of inflammation Arthritis
Cardiac Sarcoidosis. Millee Singh DO Non Invasive Cardiology First Coast Heart and Vascluar
 Cardiac Sarcoidosis Millee Singh DO Non Invasive Cardiology First Coast Heart and Vascluar Introduction Multisystem granulomatous disease of unknown etiology characterized by noncaseating granulomas in
Cardiac Sarcoidosis Millee Singh DO Non Invasive Cardiology First Coast Heart and Vascluar Introduction Multisystem granulomatous disease of unknown etiology characterized by noncaseating granulomas in
Patient with Daily Headache NTERNATIONAL CLASSIFICATION HEADACHE DISORDERS. R. Allan Purdy, MD, FRCPC,FACP. Professor of Medicine (Neurology)
") Patient with Daily Headache NTERNATIONAL CLASSIFICATION of R. Allan Purdy, MD, FRCPC,FACP HEADACHE DISORDERS Professor of Medicine (Neurology) 2nd edition (ICHD-II) Learning Issues Headaches in the elderly
Patient with Daily Headache NTERNATIONAL CLASSIFICATION of R. Allan Purdy, MD, FRCPC,FACP HEADACHE DISORDERS Professor of Medicine (Neurology) 2nd edition (ICHD-II) Learning Issues Headaches in the elderly