When the story begin, it was last year
|
|
|
- Ashley Weaver
- 5 years ago
- Views:
Transcription
1
2 When the story begin, it was last year Mr. Ho, YC 58/ M Ex smoker PMH : HT, hyperlipidaemia Med: adalat retard, lopid and losartan Presented to POH on 17 th Feb., 2016 High fever and URTI symptom
3 On admission Hb: 11.1 WCC : 17.4 increased in neutrophils Plt: 267 Cr: 193 Urea : 27 Total Bil.: 29 Normal LFT INR: 1.3

4
5 He was started on augmentin and tamiflu
6 He has persistent swinging fever Stepped antibiotic to Rocephin MSU : negative Blood culture : negative Sputum: commensal only Urine legionella : negative No diarrhoea, stool no pathogen identified
7 AKI 17/2/ /2/ /2/ /2/2016 Urea Creatinine WCC Hb Plt
8 Work up for AKI Hx of taken NSAID before admission USG : normal sized kidneys, no hydronephrosis RF, ANA, anti ds DNA: negative Low C3, C4 (0.79, 0.13) HBV, HCV, HIV: negative ASOT : negative Ig pattern : normal, SPE: no abnormal band ANCA, anti GBM: negative G6PD: normal
9 MSU : negative Granular cast : positive Urine: no dysmorphic red cell No eosinophils Spot urine TP/ Cr: 0.63 mg/mg
10 Fluid over load on Admitted to ICU in POH for haemodialysis 17/2/ /2/ /2/ /2/ /2/2016 Urea Creatinine LDH WCC Hb Plt
11 Blood film Occ. Schistocytes Occ. Atypical lymphocytes Haptoglobin: 2.50 (not low) Normal LDH, Bil Renal biopsy performed in ICU with plt cover on 22 nd Feb.

12

13

14
15 Renal Biopsy Result 1. Thrombotic microangiopathy, with focal glomerular infarction 2. Acute interstitial nephritis with eosinophils
16 No feature suggestive of intravascular haemolysis, after reviewing the film by haematologist Plasma exchange was started( for renal biopsy show TMA) And steroid for the? NSAID induced interstitial nephritis
17 27 th Feb., 2016 Started on prednisolone 15mg BD Plasma exchange on alternate day 27/2/ /2/2016 2/3/2016 Urea Creatinine LDH WCC Hb Plt
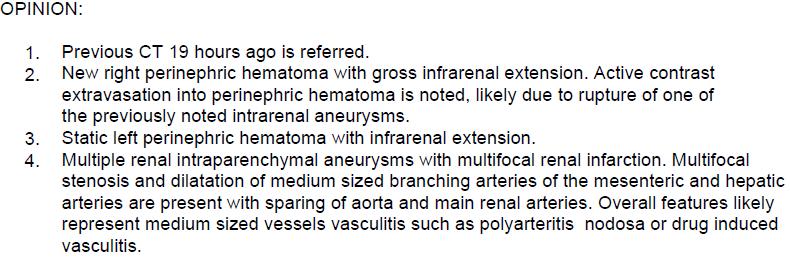
18 3 rd March, 2016 The day after 3 rd PE Acute Lt loin pain Hb drop from 8 to 6 Urgent CT abd

19
20 ?
21 4 th March, 2016 New Rt loin pain and abd distesnsion Hypotension Hb down to 5 4 unit of pack cell transfused Another CT abd

22

23
24

25

26

27
28 Seen by Rheumatologist Suggest pulse steroid then cyclophosphamide Started on pulse steroid on 4 th March (same day) 5 th March: 2 nd dose of pulse steroid 6 th March: high fever and decreased SaO2

29
30 Changed to iv hydrocortisone Cyclophosphamide did not start Back to general ward on 8 th March for con t Mx of the RLL pneumonia Next day. Persistance fever, desaturation and resp failure Intubated and back to ICU
31 After multiple work up Melioidosis pneumonia
32 Started on meropenem But cyclophosphamide was not started Condition improved Extubated, back to general ward Temp HD and active rehab Given 4 weeks of meropenem then changed to septrin for 6 more weeks
33 Noted to have renal recovery and last HD on Just came back Fu last month Urea : 12.7 Cr: 231 Spot urine TP/ Cr: 0.44mg/mg Med : Adalat GITS, pantoloc, NaHCO3, labetalol and prednisolone 5 mg daily

34




35

36 Polyarteritis nodosa (PAN)
37 Polyarteritis nodosa (PAN) Systemic necrotizing vasculitis targeting medium-sized arteries and not associated with glomerulonephritis or small vessel involvement. Anti-neutrophil cytoplasmic antibodies are typically negative. Clinical manifestations of PAN can be systemic or confined to a single organ or systems.
38 Laboratory abnormalities reveal a prominent acute phase response but are non-specific. Histologic confirmation of vasculitis in medium sized arteries is desirable. While renal biopsy are usu normal. If biopsies are negative or cannot be obtained, visceral angiography, may reveal multiple micro-aneurysms supporting the diagnosis of PAN.
39 PAN may be triggered by viral infections: HBV HCV HIV Parvovirus B19 remains idiopathic in most cases. Hernández-Rodríguez J, et al., Diagnosis and classification of polyarteritis nodosa, Journal of Autoimmunity(2014),
40 The American College of Rheumatology (ACR) 1990 criteria for the classification of polyarteritis nodosa Used for patients with known primary systemic vasculitis. These criteria do not differentiate between PAN and microscopic polyangiitis (MPA); both are included under the umbrella of PAN.
41 Three of the following 10 criteria are required: Weight loss 4 kg Livedo reticularis Testicular pain or tenderness Myalgias, weakness, or leg tenderness Mononeuropathy or polyneuropathy Diastolic blood pressure >90 mmhg Elevated urea or creatinine Positivity for hepatitis B virus (HBV) infection Arteriographic abnormality Biopsy of small- or medium-sized artery containing polymorphonuclear leukocytes.
42 French Vasculitis Study Group (FVSG) proposal for diagnostic criteria for polyarteritis nodosa. The FVSG has proposed a set of predictive items to be used as a paradigm for diagnostic criteria. These items were derived from patients with known vasculitis but not from undifferentiated patients. They are used in classification rather than diagnostic criteria. Arthritis Rheum May;58(5): doi: /art
43 The positive predictive items were: Positivity for hepatitis B virus infection Arteriographic abnormalities Mononeuropathy or polyneuropathy. The negative predictive items were: Presence of anti-neutrophil cytoplasmic antibodies (ANCA) Asthma Ear, nose, or throat signs Glomerulopathy Cryoglobulinaemia.

44 Final publication of the guideline anticipated in See more at: Quality/Clinical-Support/Clinical-Practice- Guidelines/Vasculitis#sthash.NWAPpQAB.dpuf
45 Management Based on clinical trials. Current treatment policy includes high-dose corticosteroids, which are combined with immunosuppressive agents (cyclosphosphamide).
46 Recommendations for the Management of Primary Small and Medium Vessel Vasculitis We recommend a combination of cyclophosphamide (intravenous or oral) and glucocorticoids for remissioninduction of generalised primary small and medium vessel vasculitis. [Level of evidence 1A for WG and MPA, Grade of recommendation A] [Level of evidence 1B for PAN and CSS, Grade of recommendation A] Ann Rheum Dis 2009;68(3):
47 In patients with PAN, the combination of cyclophosphamide and glucocorticoid achieves better control of disease as compared to glucocorticoid alone but the long term survival remains unchanged

48 Thrombotic Microangiopathy (TMA)
49 Thrombotic microangiopathy (TMA) is a pathologic condition with abnormalities in the blood vessel walls of arterioles and capillaries resulting in microvascular thrombosis. Clinically TMA is always accompanied by microangiopathic hemolytic anemia (MAHA), a non-immune hemolytic anemia resulting from intravascular red cell fragmentation with schistocytosis and thrombocytopenia due to consumption. But it was not a must.

50

51 Diagnosis?


52

53 And Swine flu

54 Could this 3 things come together?

55

56

57

58
59 Our case : Renal biopsy : TMA Blood smear : not suggestive of haemolysis Haptoglobin not low LDH, Bil : normal TMA without MAHA? TMA = Thrombotic microangiopathy MAHA = Microangiopathic hemolytic anemia Any other cases?
60 Yes! Two patients had a kidney biopsy that showed features of TMA in one patient and TMA and podocyte effacement in another. MAHA was not present in either case (53,55) Chapter 11. Chemotherapy and Kidney Injury, American Society of Nephrology, Onco- Nephrology Curriculum
61 1 st patient A 50-year-old man, diagnosed with advanced renal cell carcinoma (RCC), who was treated with sorafenib as second line treatment. Develop impaired renal function and renal biopsy show TMA feature, without MAHA in blood smear.
62 2 nd patient A 44-year-old woman with a history of malignant skin hidradenoma was started on sunitinib for refractory disease. One month later, proteinuria was discovered at 1.1 g/day whereas serumcreatinine level remained stable at 64μmol/land microhaematuria was undetectable. Biological signs oftma were absent (haemoglobin level 13.3 g/dl, plateletcount /mm3, schistocytes undetectable, LDH: 581IU/l). Guillaume Bollee et al. Thrombotic microangiopathy secondary to VEGF pathway inhibition by sunitinib. Nephrol Dial Transplant (2009) 24:
63 Six months after sunitinib was started, persistance proteinurea. Still, no haematological features of MAHA had been detected. Antigenic dosages in serum of C3, C4, CH50, Factor H, Factor I and CD46/MCP were in the normal range. ADAMTS13 activity was also normal. Renal ultrasound showed normal kidneys.
64 The renal biopsy contained 13 glomeruli, none of which were globally sclerotic. Almost all showed typical features of TMA: with widespread duplication of the glomerular basement membranes, endothelial swelling, focal glomerular capillary thrombosis, mesangiolysis and fibrin deposits


65 Renal biopsy
66
67
68 In a nutshell, Viral infection can associated with TMA and medium vessels vasculitis TMA can occur without MAHA HUS can happened without thrombocytopenia H1N1 induced TMA without MAHA, in a patient with PAN
69 Clear? Not clear?

70 One thing for sure is clear Mr. Ho, did not die of respiratory failure, and now dialysis free.
71 Thank you.
What is meant by Thrombotic Microangiopathy (TMA)?
?") What is meant by Thrombotic Microangiopathy (TMA)? Thrombotic Microangiopathy (TMA) is a group of disorders characterized by injured endothelial cells, microangiopathic hemolytic anemia (MAHA), with its
What is meant by Thrombotic Microangiopathy (TMA)? Thrombotic Microangiopathy (TMA) is a group of disorders characterized by injured endothelial cells, microangiopathic hemolytic anemia (MAHA), with its
Year 2004 Paper one: Questions supplied by Megan
 QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
QUESTION 53 Endothelial cell pathology on renal biopsy is most characteristic of which one of the following diagnoses? A. Pre-eclampsia B. Haemolytic uraemic syndrome C. Lupus nephritis D. Immunoglobulin
Renal failure and thrombocytopaenia? Don t forget TTP/HUS. Jonathan Wala Nephrologist
 Renal failure and thrombocytopaenia? Don t forget TTP/HUS Jonathan Wala Nephrologist Thrombotic microangiopathies Disorders characterized by: thrombocytopaenia microangiopathic haemolytic anaemia (MAHA)
Renal failure and thrombocytopaenia? Don t forget TTP/HUS Jonathan Wala Nephrologist Thrombotic microangiopathies Disorders characterized by: thrombocytopaenia microangiopathic haemolytic anaemia (MAHA)
Case Presentation VASCULITIS. Case Presentation. Case Presentation. Vasculitis
 Case Presentation VASCULITIS The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
Case Presentation VASCULITIS The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
VASCULITIS. Case Presentation. Case Presentation
 VASCULITIS Case Presentation The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
VASCULITIS Case Presentation The patient is a 24 year old woman who presented to the emergency room with left-sided weakness. She was confused and complained of a severe headache. She was noted to have
PAEDIATRIC VASCULITIS
 PAEDIATRIC VASCULITIS Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. OUTLINE Introduction
PAEDIATRIC VASCULITIS Lawrence Owino Okong o, Mmed (UoN); Mphil. (UCT). Lecturer, Department of Paediatrics and Child Health, University of Nairobi. Paediatrician/ Rheumatologist. OUTLINE Introduction
Acute Kidney Injury. I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS
 Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
Acute Kidney Injury I. David Weiner, M.D. Division of Nephrology, Hypertension and Transplantation University of Florida and NF/SGVHS 374-6102 David.Weiner@medicine.ufl.edu www.renallectures.com Concentration
Hemolytic uremic syndrome: Investigations and management
 Hemolytic uremic syndrome: Investigations and management SAWAI Toshihiro M.D., Ph.D. Department of Pediatrics, Shiga University of Medical Science Otsu, JAPAN AGENDA TMA; Thrombotic micro angiopathy STEC-HUS;
Hemolytic uremic syndrome: Investigations and management SAWAI Toshihiro M.D., Ph.D. Department of Pediatrics, Shiga University of Medical Science Otsu, JAPAN AGENDA TMA; Thrombotic micro angiopathy STEC-HUS;
1. INSTRUCTIONS 2. DEFINITION OF HUS
 CQ_IBK_aHUS_01 / version 25/11/09 European Paediatric Research Group for HUS and related disorders Case questionnaire for diarrhoea negative/vtec (STEC) negative cases acute phase 1. INSTRUCTIONS Please
CQ_IBK_aHUS_01 / version 25/11/09 European Paediatric Research Group for HUS and related disorders Case questionnaire for diarrhoea negative/vtec (STEC) negative cases acute phase 1. INSTRUCTIONS Please
Mohammad Reza Shakibi M.D Kerman university of medical sciences (KMU) Shafa Hospital, Rheumatology ward
 Shafa Hospital, Rheumatology ward") VASCULITIS SYNDROMES Mohammad Reza Shakibi M.D Kerman university of medical sciences (KMU) Shafa Hospital, Rheumatology ward ILLUSTRATED CASE 1 A 56 years old lady refered me for prolonged fever, arthritis
VASCULITIS SYNDROMES Mohammad Reza Shakibi M.D Kerman university of medical sciences (KMU) Shafa Hospital, Rheumatology ward ILLUSTRATED CASE 1 A 56 years old lady refered me for prolonged fever, arthritis
A 60 year old woman with altered mental status and thrombotic microangiopathy. Josh Veatch
 A 60 year old woman with altered mental status and thrombotic microangiopathy Josh Veatch Previously healthy 60 year old woman 2 3 months of fatigue following a URI, transient episodes being out of it
A 60 year old woman with altered mental status and thrombotic microangiopathy Josh Veatch Previously healthy 60 year old woman 2 3 months of fatigue following a URI, transient episodes being out of it
AKI Case study -Vasculitis. Sarah Mackie Renal Practice Development Nurse King s College Hospital - London
 AKI Case study -Vasculitis Sarah Mackie Renal Practice Development Nurse King s College Hospital - London What is vasculitis Vasculitis refers to inflammation of the blood vessels, including arteries,
AKI Case study -Vasculitis Sarah Mackie Renal Practice Development Nurse King s College Hospital - London What is vasculitis Vasculitis refers to inflammation of the blood vessels, including arteries,
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated 2- infectious
RaDaR Inclusion and Exclusion Criteria. Diagnosis Inclusion Criteria Exclusion Criteria. Alport Syndrome definite or probable
 Alport Syndrome and Type IV collagenopathies APRT Deficiency Alport Syndrome definite or probable Alport carrier definite or probable Thin basement membrane nephropathy APRT Deficiency confirmed Abolished
Alport Syndrome and Type IV collagenopathies APRT Deficiency Alport Syndrome definite or probable Alport carrier definite or probable Thin basement membrane nephropathy APRT Deficiency confirmed Abolished
DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL
 DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL Rare but fatal disease if unrecognized and untreated Incidence about 1: 1 million in the USA Female preponderance of 2:1 Part
DR V PHILIP CLINICAL HAEMATOLOGY UNIT CHRIS HANI BARAGWANATH ACADEMIC HOSPITAL Rare but fatal disease if unrecognized and untreated Incidence about 1: 1 million in the USA Female preponderance of 2:1 Part
Case report 24 th Summer School of Internal Medicine 2015
 Case report 24 th Summer School of Internal Medicine 2015 Goldmannová D., Horák P., Skácelová M. IIIrd Internal Clinic - endocrinology, diabetology, rheumatology, nephrology University hospital Olomouc,
Case report 24 th Summer School of Internal Medicine 2015 Goldmannová D., Horák P., Skácelová M. IIIrd Internal Clinic - endocrinology, diabetology, rheumatology, nephrology University hospital Olomouc,
monoclonal gammopathy of undetermin Citation Rheumatology international, 33(1),
,") NAOSITE: Nagasaki University's Ac Title Author(s) Renal thrombotic microangiopathies/ in a patient with primary Sjögren's monoclonal gammopathy of undetermin Koga, Tomohiro; Yamasaki, Satoshi; Atsushi;
NAOSITE: Nagasaki University's Ac Title Author(s) Renal thrombotic microangiopathies/ in a patient with primary Sjögren's monoclonal gammopathy of undetermin Koga, Tomohiro; Yamasaki, Satoshi; Atsushi;
Vasculitis. Edward Dwyer, M.D. Division of Rheumatology. Vasculitis
 Edward Dwyer, M.D. Division of Rheumatology VASCULITIS is a primary inflammatory disease process of the vasculature Determinants of the Clinical Manifestations of : Target organ involved Size of vessel
Edward Dwyer, M.D. Division of Rheumatology VASCULITIS is a primary inflammatory disease process of the vasculature Determinants of the Clinical Manifestations of : Target organ involved Size of vessel
Case 3. ACCME/Disclosure. Laboratory results. Clinical history 4/13/2016
 Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
Case 3 Lynn D. Cornell, M.D. Mayo Clinic, Rochester, MN Cornell.Lynn@mayo.edu USCAP Renal Case Conference March 13, 2016 ACCME/Disclosure Dr. Cornell has nothing to disclose Clinical history 57-year-old
DRUG NAME: Eculizumab Brand(s): Soliris DOSAGE FORM/ STRENGTH: 10 mg/ml (300 mg per vial)
: Soliris DOSAGE FORM/ STRENGTH: 10 mg/ml (300 mg per vial)") Preamble: A confirmed diagnosis of atypical hemolytic uremic syndrome (ahus) is required for eculizumab funding. The information below is to provide clinicians with context for how a diagnosis of ahus
Preamble: A confirmed diagnosis of atypical hemolytic uremic syndrome (ahus) is required for eculizumab funding. The information below is to provide clinicians with context for how a diagnosis of ahus
ANCA associated vasculitis in China
 ANCA associated vasculitis in China Min Chen Renal Division, Peking University First Hospital, Beijing 100034, P. R. China 1 General introduction of AAV in China Disease spectrum and ANCA type Clinical
ANCA associated vasculitis in China Min Chen Renal Division, Peking University First Hospital, Beijing 100034, P. R. China 1 General introduction of AAV in China Disease spectrum and ANCA type Clinical
Rejection or Not? Interhospital Renal Meeting 10 Oct Desmond Yap & Sydney Tang Queen Mary Hospital
 Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
Rejection or Not? Interhospital Renal Meeting 10 Oct 2007 Desmond Yap & Sydney Tang Queen Mary Hospital Case Presentation F/61 End stage renal failure due to unknown cause Received HD in private hospital
THROMBOTIC MICROANGIOPATHY. Jun-Ki Park 7/19/11
 THROMBOTIC MICROANGIOPATHY Jun-Ki Park 7/19/11 TMAs are microvascular occlusive disorders characterized by systemic or intrarenal aggregation of platelets, thrombocytopenia, and mechanical injury to erythrocytes.
THROMBOTIC MICROANGIOPATHY Jun-Ki Park 7/19/11 TMAs are microvascular occlusive disorders characterized by systemic or intrarenal aggregation of platelets, thrombocytopenia, and mechanical injury to erythrocytes.
Tell me more about vasculitis. Lisa Willcocks Consultant in Nephrology and Vasculitis, Addenbrooke s Hospital
 Tell me more about vasculitis Lisa Willcocks Consultant in Nephrology and Vasculitis, Addenbrooke s Hospital Talk overview Case study ANCA-associated vasculitis What is ANCA vasculitis? What causes ANCA
Tell me more about vasculitis Lisa Willcocks Consultant in Nephrology and Vasculitis, Addenbrooke s Hospital Talk overview Case study ANCA-associated vasculitis What is ANCA vasculitis? What causes ANCA
SMALL TO MEDIUM VASCULITIS: RENAL ASPECT RATANA CHAWANASUNTORAPOJ UPDATE IN INTERNAL MEDICINE 2018
 SMALL TO MEDIUM VASCULITIS: RENAL ASPECT RATANA CHAWANASUNTORAPOJ UPDATE IN INTERNAL MEDICINE 2018 OUTLINE Renal involvement in vasculitis Curr Rheumatol Rep 2013 Renal involvement in ANCA vasculitis GN***:
SMALL TO MEDIUM VASCULITIS: RENAL ASPECT RATANA CHAWANASUNTORAPOJ UPDATE IN INTERNAL MEDICINE 2018 OUTLINE Renal involvement in vasculitis Curr Rheumatol Rep 2013 Renal involvement in ANCA vasculitis GN***:
A 23 year old Caucasian male presented with shortness of breath, hypertension, bloody sputum, and a history of drug abuse (confirmed by urinalysis).
.") A 23 year old Caucasian male presented with shortness of breath, hypertension, bloody sputum, and a history of drug abuse (confirmed by urinalysis). He was found to have severe kidney injury requiring
A 23 year old Caucasian male presented with shortness of breath, hypertension, bloody sputum, and a history of drug abuse (confirmed by urinalysis). He was found to have severe kidney injury requiring
Dr. E.SUDHA (Fellow in Pediatric Nephrology) DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL
 DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL") Dr. E.SUDHA (Fellow in Pediatric Nephrology) DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL CASE HISTORY 4 yrs old previously well boy Born to 2 nd degree consanguinity Fever x 5 days
Dr. E.SUDHA (Fellow in Pediatric Nephrology) DEPT OF PEDIATRIC NEPHROLOGY & DIALYSIS Dr.MEHTA CHILDRENS HOSPITAL CASE HISTORY 4 yrs old previously well boy Born to 2 nd degree consanguinity Fever x 5 days
Managing Acute Medical Problems, Birmingham Vasculitis. David Jayne. University of Cambridge
 Managing Acute Medical Problems, Birmingham 2016 Vasculitis David Jayne University of Cambridge Disclosures Astra Zeneca, Aurinia, BIOGEN, Boehringer, Chemocentryx, Genzyme/Sanofi, GSK, Lilly, Medimmune,
Managing Acute Medical Problems, Birmingham 2016 Vasculitis David Jayne University of Cambridge Disclosures Astra Zeneca, Aurinia, BIOGEN, Boehringer, Chemocentryx, Genzyme/Sanofi, GSK, Lilly, Medimmune,
DIABETES MELLITUS. Kidney in systemic diseases. Slower the progression: Pathology: Patients with diabetes mellitus are prone to other renal diseases:
 Kidney in systemic diseases Dr. Badri Paudel The kidneys may be directly involved in a number of multisystem diseases or secondarily affected by diseases of other organs. Involvement may be at a prerenal,
Kidney in systemic diseases Dr. Badri Paudel The kidneys may be directly involved in a number of multisystem diseases or secondarily affected by diseases of other organs. Involvement may be at a prerenal,
Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis
 GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
GLOMERULONEPHRITIDES Vivette D Agati Jai Radhakrishnan Approach to Glomerular Diseases: Clinical Presentation Nephrotic Syndrome Nephritis Heavy Proteinuria Renal failure Low serum Albumin Hypertension
Membranous nephropathy. By Mohammed Kamal Nassar, MD Lecturer of Nephrology Mansoura University
 Membranous nephropathy By Mohammed Kamal Nassar, MD Lecturer of Nephrology Mansoura University Membranous nephropathy Definition: Immune complex glomerular disease in which immune deposits of IgG and complement
Membranous nephropathy By Mohammed Kamal Nassar, MD Lecturer of Nephrology Mansoura University Membranous nephropathy Definition: Immune complex glomerular disease in which immune deposits of IgG and complement
Thrombotic microangiopathies and antineoplastic agents
 Thrombotic microangiopathies and antineoplastic agents Paul Coppo paul.coppo@aphp.fr Service d Hématologie - Hôpital Saint-Antoine AP-HP et Université Pierre & Marie Curie Centre de Référence des Microangiopathies
Thrombotic microangiopathies and antineoplastic agents Paul Coppo paul.coppo@aphp.fr Service d Hématologie - Hôpital Saint-Antoine AP-HP et Université Pierre & Marie Curie Centre de Référence des Microangiopathies
RAPIDLY FAILING KIDNEYS. Dr Paul Johny 2 nd yr DNB Medicine Resident
 RAPIDLY FAILING KIDNEYS Dr Paul Johny 2 nd yr DNB Medicine Resident Mr Z 67yrs old Occupation : Retired officer from electricity board Chief complaints : Fever : 5 days Right lower limb swelling and pain
RAPIDLY FAILING KIDNEYS Dr Paul Johny 2 nd yr DNB Medicine Resident Mr Z 67yrs old Occupation : Retired officer from electricity board Chief complaints : Fever : 5 days Right lower limb swelling and pain
Case conference. Welcome Dr. Lawrence Tierney
 Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016
 Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016 Case report 20 months old girl Israeli Arab Muslim family, consanguineous marriage
Let`s go for the diagnosis! Yazeed Toukan, MD Pediatric Pulmonary Institute, Ruth Rappaport Children`s Hospital July 2016 Case report 20 months old girl Israeli Arab Muslim family, consanguineous marriage
Fußzeile (Titel der Präsentation) 1. Thrombotic Microangiopathy: The German Experience 4. Conflictof interest: none
 1. Thrombotic Microangiopathy: The German Experience 4. Conflictof interest: none") Thrombotic Microangiopathy: The German Experience 3 Nephropathology Section, Institute of Pathology, Hamburg, Germany Agenda 1. Difficulties in the diagnosis TMA 2. Previous efforts to reach consensus
Thrombotic Microangiopathy: The German Experience 3 Nephropathology Section, Institute of Pathology, Hamburg, Germany Agenda 1. Difficulties in the diagnosis TMA 2. Previous efforts to reach consensus
Vasculitis local: systemic
 Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated inflammation
Vasculitis Inflammation of the vessel wall. Signs and symptoms: 1- local: according to the involved tissue 2- systemic:(fever, myalgia, arthralgias, and malaise) Pathogenesis 1- immune-mediated inflammation
Non-immune acquired haemolytic anaemias. Dr.Maysem
 Non-immune acquired haemolytic anaemias Dr.Maysem Causes of Non-immune acquired haemolytic anaemias. Infections Infections can cause haemolysis in a variety of ways: -They may precipitate an acute haemolytic
Non-immune acquired haemolytic anaemias Dr.Maysem Causes of Non-immune acquired haemolytic anaemias. Infections Infections can cause haemolysis in a variety of ways: -They may precipitate an acute haemolytic
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS
 CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
CASE 4 A RARE CASE OF INTRALUMINAL GLOMERULAR CAPILLARY DEPOSITS DR ANNIE JOJO, Dr Seethalekshmy N V, Dr Nanda Kachare DEPARTMENT OF PATHOLOGY, AMRITA INSTITUTE OF MEDICAL SCIENCES, KOCHI. 54 yrs female,
Another TB patient with renal failure. Inter-hospital renal meeting 21/3/2007 KWH Drs. SF Chan and SK Mak
 Another TB patient with renal failure Inter-hospital renal meeting 21/3/2007 KWH Drs. SF Chan and SK Mak Case presentation 59/M Chronic smoker, nondrinker History of pulmonary tuberculosis in 2000 completed
Another TB patient with renal failure Inter-hospital renal meeting 21/3/2007 KWH Drs. SF Chan and SK Mak Case presentation 59/M Chronic smoker, nondrinker History of pulmonary tuberculosis in 2000 completed
Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management
 Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management") AKI Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management and indications for RRT Etiology prerenal causes
AKI Definition : Stages : ( RIFLE vs. AKIN ) Causes and classification : Pre-renal Renal Post- renal Clinical manifestations and Complication Management and indications for RRT Etiology prerenal causes
Renal Pathology 1: Glomerulus. With many thanks to Elizabeth Angus PhD for EM photographs
 Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
Renal Pathology 1: Glomerulus With many thanks to Elizabeth Angus PhD for EM photographs Anatomy of the Kidney http://www.yalemedicalgroup.org/stw/page.asp?pageid=stw028980 The Nephron http://www.beltina.org/health-dictionary/nephron-function-kidney-definition.html
A TRICKY PROBLEM. Presenter-Dr Lakshmi PK
 A TRICKY PROBLEM Presenter-Dr Lakshmi PK Patient particulars 33 years old Male Resident of Andhra Pradesh Occupation-soldier Chief compliants Headache- 03 days Headache-global,throbbing type Associated
A TRICKY PROBLEM Presenter-Dr Lakshmi PK Patient particulars 33 years old Male Resident of Andhra Pradesh Occupation-soldier Chief compliants Headache- 03 days Headache-global,throbbing type Associated
Case Studies. Scleroderma Renal Crisis or Thrombotic Thrombocytopenic Purpura: Seeing Through the Masquerade. Patient 1
 Scleroderma Renal Crisis or Thrombotic Thrombocytopenic Purpura: Seeing Through the Masquerade Emily Keeler, DO, 1* Gloria Fioravanti, DO, FACP, 1 Bensson Samuel, MD, PG Dip, 1 Santo Longo, MD 2 Lab Med
Scleroderma Renal Crisis or Thrombotic Thrombocytopenic Purpura: Seeing Through the Masquerade Emily Keeler, DO, 1* Gloria Fioravanti, DO, FACP, 1 Bensson Samuel, MD, PG Dip, 1 Santo Longo, MD 2 Lab Med
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT. J. H. Helderman,MD,FACP,FAST
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT J. H. Helderman,MD,FACP,FAST Vanderbilt University Medical Center Professor of Medicine, Pathology and Immunology Medical Director, Vanderbilt Transplant
Small Vessel Vasculitis
 Small Vessel Vasculitis Paul A Brogan Professor of Vasculitis and Consultant Paediatric Rheumatologist Department of Rheumatology Institute of Child Health and Great Ormond St Hospital, London UK P.brogan@ucl.ac.uk
Small Vessel Vasculitis Paul A Brogan Professor of Vasculitis and Consultant Paediatric Rheumatologist Department of Rheumatology Institute of Child Health and Great Ormond St Hospital, London UK P.brogan@ucl.ac.uk
Management of Acute Vasculitis. CMT teaching 3 rd June 2015 Caroline Wroe
 Management of Acute Vasculitis CMT teaching 3 rd June 2015 Caroline Wroe Vasculitis pub quiz Match the date with the event Dr Peter McBride, Scottish Otolaryngologist describes a disease of rapid destruction
Management of Acute Vasculitis CMT teaching 3 rd June 2015 Caroline Wroe Vasculitis pub quiz Match the date with the event Dr Peter McBride, Scottish Otolaryngologist describes a disease of rapid destruction
Additional file 2: Details of cohort studies and randomised trials
 Reference Randomised trials Ye et al. 2001 Abstract 274 R=1 WD=0 Design, numbers, treatments, duration Randomised open comparison of: (45 patients) 1.5 g for 3, 1 g for 3, then 0.5 to 0.75 g IV cyclophosphamide
Reference Randomised trials Ye et al. 2001 Abstract 274 R=1 WD=0 Design, numbers, treatments, duration Randomised open comparison of: (45 patients) 1.5 g for 3, 1 g for 3, then 0.5 to 0.75 g IV cyclophosphamide
RaDaR Inclusion and Exclusion Criteria. Diagnosis Inclusion Criteria Exclusion Criteria. Alport Syndrome definite or probable
 Alport Syndrome and Type IV collagenopathies APRT Deficiency Alport Syndrome definite or probable Alport carrier definite or probable Thin basement membrane nephropathy APRT Deficiency confirmed Abolished
Alport Syndrome and Type IV collagenopathies APRT Deficiency Alport Syndrome definite or probable Alport carrier definite or probable Thin basement membrane nephropathy APRT Deficiency confirmed Abolished
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Plan of attack: Diagnostic approach to the renal biopsy Differential diagnosis of the clinical syndromes of renal disease Microscopy Step
Protocol Version 2.0 Synopsis
 Protocol Version 2.0 Synopsis Title Short Title Plasma exchange and glucocorticoid dosing in anti-neutrophil cytoplasm antibody associated vasculitis: a randomized controlled trial. PEXIVAS PEXIVAS Clinical
Protocol Version 2.0 Synopsis Title Short Title Plasma exchange and glucocorticoid dosing in anti-neutrophil cytoplasm antibody associated vasculitis: a randomized controlled trial. PEXIVAS PEXIVAS Clinical
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS. Myriam Farah, MD, FRCPC
 ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
ACUTE KIDNEY INJURY A PRIMER FOR PRIMARY CARE PHYSICIANS Myriam Farah, MD, FRCPC Clinical Assistant Professor Division of Nephrology, University of British Columbia November 2016 1. How to recognize acute
Dr Rodney Itaki Lecturer Anatomical Pathology Discipline. University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology
 Vasculitis Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Disease Spectrum Hypersensitivity vasculitis/microscopic
Vasculitis Dr Rodney Itaki Lecturer Anatomical Pathology Discipline University of Papua New Guinea School of Medicine & Health Sciences Division of Pathology Disease Spectrum Hypersensitivity vasculitis/microscopic
Kidney disease associated with autoimmune disease
 Kidney disease associated with autoimmune disease Masaomi Nangaku Division of Nephrology and Endocrinology the University of Tokyo Graduate School of Medicine, Japan M-type Phospholipase A2 Receptor as
Kidney disease associated with autoimmune disease Masaomi Nangaku Division of Nephrology and Endocrinology the University of Tokyo Graduate School of Medicine, Japan M-type Phospholipase A2 Receptor as
Thrombotic Microangiopathies (TMA) / TTP/HUS/αHUS Pathology & Molecular. Genetics
 / TTP/HUS/αHUS Pathology & Molecular. Genetics") Thrombotic Microangiopathies (TMA) / TTP/HUS/αHUS Pathology & Molecular Genetics Helen Liapis, M.D. Senior Consultant Arkana Labs Professor of Pathology & Immunology. retired Washington University School
Thrombotic Microangiopathies (TMA) / TTP/HUS/αHUS Pathology & Molecular Genetics Helen Liapis, M.D. Senior Consultant Arkana Labs Professor of Pathology & Immunology. retired Washington University School
* Renal insufficiencies
 Thrombotic Thrombocytopenic Purpura Behzad Poopak, DCLS PhD. Tehran medical Branch Islamic Azad university bpoopak@yahoo.com Case Summary Ms. X, a 35-year year-old woman Complained of weakness, low grade
Thrombotic Thrombocytopenic Purpura Behzad Poopak, DCLS PhD. Tehran medical Branch Islamic Azad university bpoopak@yahoo.com Case Summary Ms. X, a 35-year year-old woman Complained of weakness, low grade
Some renal vascular disorders
 Some renal vascular disorders Introduction Nearly all diseases of the kidney involve the renal blood vessels secondarily We will discuss: -Hypertension (arterionephrosclerosis in benign HTN & hyperplastic
Some renal vascular disorders Introduction Nearly all diseases of the kidney involve the renal blood vessels secondarily We will discuss: -Hypertension (arterionephrosclerosis in benign HTN & hyperplastic
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Index. electron microscopy, 81 immunofluorescence microscopy, 80 light microscopy, 80 Amyloidosis clinical setting, 185 etiology/pathogenesis,
 A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
A Acute antibody-mediated rejection (Acute AMR) clinical features, 203 clinicopathologic correlations, 206 pathogenesis, 205 206 204 205 light microscopy, 203 204 Acute cellular rejection (ACR) clinical
Case Presentation Turki Al-Hussain, MD
 Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Case Presentation Turki Al-Hussain, MD Director, Renal Pathology Chapter Saudi Society of Nephrology & Transplantation Consultant Nephropathologist & Urological Pathologist Department of Pathology & Laboratory
Nephritic vs. Nephrotic Syndrome
 Page 1 of 18 Nephritic vs. Nephrotic Syndrome Terminology: Glomerulus: A network of blood capillaries contained within the cuplike end (Bowman s capsule) of a nephron. Glomerular filtration rate: The rate
Page 1 of 18 Nephritic vs. Nephrotic Syndrome Terminology: Glomerulus: A network of blood capillaries contained within the cuplike end (Bowman s capsule) of a nephron. Glomerular filtration rate: The rate
Case Presentation. Rafid Asfar, MD
 Case Presentation Rafid Asfar, MD Introduction ANCA associated vasculitis may be localized or systemic, and can involve the eyes Ocular manifestations can occur in the absence of systemic disease in persons
Case Presentation Rafid Asfar, MD Introduction ANCA associated vasculitis may be localized or systemic, and can involve the eyes Ocular manifestations can occur in the absence of systemic disease in persons
Henoch Schonlein Purpura
 CHILDREN S SERVICES Henoch Schonlein Purpura Definition A vasculitic syndrome of small vessels classically characterised by a purpuric rash, abdominal pain, arthritis, and nephritis. Platelet count and
CHILDREN S SERVICES Henoch Schonlein Purpura Definition A vasculitic syndrome of small vessels classically characterised by a purpuric rash, abdominal pain, arthritis, and nephritis. Platelet count and
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome.
 Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Disorders of the kidney. Urine analysis. Nephrotic and nephritic syndrome. Azotemia and Urinary Abnormalities Disturbances in urine volume oliguria, anuria, polyuria Abnormalities of urine sediment red
Plasma exchanges in ANCA-associated vasculitis
 Plasma exchanges in ANCA-associated vasculitis Xavier Puéchal, MD, PhD Centre de Référence des Maladies auto-immunes systémiques rares d Ile de France Hôpital Cochin Université Paris Descartes http://www.vascularites.org
Plasma exchanges in ANCA-associated vasculitis Xavier Puéchal, MD, PhD Centre de Référence des Maladies auto-immunes systémiques rares d Ile de France Hôpital Cochin Université Paris Descartes http://www.vascularites.org
Case report Fever in a patient with ANCA-associated vasculitis
 Case report Fever in a patient with ANCA-associated vasculitis 73 years-old white woman PRIOR MEDICAL HISTORY *Hypertension: Enalapril, Furosemide *Dyslipidemia: Pravastatin *Ischemic heart disease: 2008
Case report Fever in a patient with ANCA-associated vasculitis 73 years-old white woman PRIOR MEDICAL HISTORY *Hypertension: Enalapril, Furosemide *Dyslipidemia: Pravastatin *Ischemic heart disease: 2008
Diabetes, Obesity and Heavy Proteinuria
 Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Diabetes, Obesity and Heavy Proteinuria Clinical Case 41 yo Black woman with heavy proteinuria History 2014: noted to have proteinuria on routine lab testing (1.1g/g). 1+ edema. Blood pressure has been
Dr Ian Roberts Oxford
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing renal failure Highlight diagnostic pitfalls. Crescentic GN: renal
MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS
 MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS Hatim Q. AlMaghrabi, MD, FRCPC Consultant at King Abdulaziz Medical City (NGHA) Jeddah Case Presentation 70 years old female Known hypertensive
MICROSCOPIC HEMATURIA AND DIFFUSE NECROTIZING GLOMERULONEPHRITIS Hatim Q. AlMaghrabi, MD, FRCPC Consultant at King Abdulaziz Medical City (NGHA) Jeddah Case Presentation 70 years old female Known hypertensive
FAQ Identifying and enrolling participants
 FAQ Identifying and enrolling participants WHO IS ELIGIBLE - CASES? Patients with a new diagnosis of primary systemic vasculitis Patients suitable as cases are over 18 years with a new presentation or
FAQ Identifying and enrolling participants WHO IS ELIGIBLE - CASES? Patients with a new diagnosis of primary systemic vasculitis Patients suitable as cases are over 18 years with a new presentation or
62- year-old man presented with-
 62- year-old man presented with- High grade continued fever Extreme anorexia and vomiting 2 months BACKGROUND On 15 th March 2004, presented with- - severe pain, swelling, marked redness of ears, nose,
62- year-old man presented with- High grade continued fever Extreme anorexia and vomiting 2 months BACKGROUND On 15 th March 2004, presented with- - severe pain, swelling, marked redness of ears, nose,
SHO Teaching. Dr. Amir Bhanji Consultant Nephrologist, Q.A hospital, Portsmouth
 SHO Teaching Vasculitis Renal medicine Dr. Amir Bhanji Consultant Nephrologist, Q.A hospital, Portsmouth OUTLINE What is vasculitis Causes Classification Brief look into ANCA Associated Vasculitis (AAV)
SHO Teaching Vasculitis Renal medicine Dr. Amir Bhanji Consultant Nephrologist, Q.A hospital, Portsmouth OUTLINE What is vasculitis Causes Classification Brief look into ANCA Associated Vasculitis (AAV)
Things to never miss in the office. Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC
 Leonard Minuk MD FRCPC") Things to never miss in the office Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC Presenter Disclosure Faculty / Speaker s name: Brett Houston / Leonard Minuk Relationships with commercial
Things to never miss in the office Brett Houston MD FRCPC (PYG-5, hematology) Leonard Minuk MD FRCPC Presenter Disclosure Faculty / Speaker s name: Brett Houston / Leonard Minuk Relationships with commercial
A clinical syndrome, composed mainly of:
 Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Nephritic syndrome We will discuss: 1)Nephritic syndrome: -Acute postinfectious (poststreptococcal) GN -IgA nephropathy -Hereditary nephritis 2)Rapidly progressive GN (RPGN) A clinical syndrome, composed
Soliris (eculizumab) DRUG.00050
 DRUG.00050") Market DC Soliris (eculizumab) DRUG.00050 Override(s) Prior Authorization Approval Duration 1 year Medications Soliris (eculizumab) APPROVAL CRITERIA Paroxysmal Nocturnal Hemoglobinuria I. Initiation of
Market DC Soliris (eculizumab) DRUG.00050 Override(s) Prior Authorization Approval Duration 1 year Medications Soliris (eculizumab) APPROVAL CRITERIA Paroxysmal Nocturnal Hemoglobinuria I. Initiation of
Vasculitis and Vasculitides. OMONDI OYOO Physician/Rheumatologist; Senior Lecturer, Department of Medicine University of Nairobi
 Vasculitis and Vasculitides OMONDI OYOO Physician/Rheumatologist; Senior Lecturer, Department of Medicine University of Nairobi Definition Presence of leucocytes in the vessel wall with reactive damage
Vasculitis and Vasculitides OMONDI OYOO Physician/Rheumatologist; Senior Lecturer, Department of Medicine University of Nairobi Definition Presence of leucocytes in the vessel wall with reactive damage
Monoclonal Gammopathies and the Kidney. Tibor Nádasdy, MD The Ohio State University, Columbus, OH
 Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Monoclonal Gammopathies and the Kidney Tibor Nádasdy, MD The Ohio State University, Columbus, OH Monoclonal gammopathy of renal significance (MGRS) Biopsies at OSU (n=475) between 2007 and 2016 AL or AH
Clinical pathological correlations in AKI
 Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
Clinical pathological correlations in AKI Dr. Rajasekara chakravarthi Director - Nephrology Star Kidney Center, Star Hospitals Renown clinical services India Introduction AKI is common entity Community
Mr. I.K 58 years old
 Mr. I.K 58 years old Hospitalized because of marked pitting peripheral edema (bilateral crural and perimalleolar edema) and uncontrolled blood pressure (BP 150/100 mmhg under treatment). since age 54 years
Mr. I.K 58 years old Hospitalized because of marked pitting peripheral edema (bilateral crural and perimalleolar edema) and uncontrolled blood pressure (BP 150/100 mmhg under treatment). since age 54 years
Retraction Retracted: Anti-GBM of Pregnancy: Acute Renal Failure Resolved after Spontaneous Abortion, Plasma Exchange, Hemodialysis, and Steroids
 Hindawi Publishing Corporation Volume 015, Article ID 369087, 1 page http://dx.doi.org/10.1155/015/369087 Retraction Retracted: Anti-GBM of Pregnancy: Acute Renal Failure Hemodialysis, and Steroids Received
Hindawi Publishing Corporation Volume 015, Article ID 369087, 1 page http://dx.doi.org/10.1155/015/369087 Retraction Retracted: Anti-GBM of Pregnancy: Acute Renal Failure Hemodialysis, and Steroids Received
*HSP is a common vasculitis of small vessels with cutaneous & systemic complications. Its etiology is unknown& often follows URTIs.
 BY Introduction The disease is eponymously named after Eduard heinrich Henoch (1820-1910), a German pediatrician, and his teacher Johann Lukas Schonlein (1793-1864), who described it in the 1860s. Cont
BY Introduction The disease is eponymously named after Eduard heinrich Henoch (1820-1910), a German pediatrician, and his teacher Johann Lukas Schonlein (1793-1864), who described it in the 1860s. Cont
The Sequential Development of Antiglomerular Basement Membrane Nephritis and Myeloperoxidase-antineutrophil Cytoplasmic Antibody-associated Vasculitis
 doi: 10.2169/internalmedicine.8757-16 http://internmed.jp CASE REPORT The Sequential Development of Antiglomerular Basement Membrane Nephritis and Myeloperoxidase-antineutrophil Cytoplasmic Antibody-associated
doi: 10.2169/internalmedicine.8757-16 http://internmed.jp CASE REPORT The Sequential Development of Antiglomerular Basement Membrane Nephritis and Myeloperoxidase-antineutrophil Cytoplasmic Antibody-associated
Patologie da attivazione del complemento G.F.Ferraccioli Istituto di Reumatologia e Scienze Affini Facolta di Medicina Universita Cattolica del sacro
 Patologie da attivazione del complemento G.F.Ferraccioli Istituto di Reumatologia e Scienze Affini Facolta di Medicina Universita Cattolica del sacro Cuore Roma Roma 19.02.2016 TMA: complement disorders
Patologie da attivazione del complemento G.F.Ferraccioli Istituto di Reumatologia e Scienze Affini Facolta di Medicina Universita Cattolica del sacro Cuore Roma Roma 19.02.2016 TMA: complement disorders
ACUTE GLOMERULONEPHRITIS. IAP UG Teaching slides
 ACUTE GLOMERULONEPHRITIS 1 Definition Etiology Pathology/pathogenesis Risk factors Clinical Presentation Investigation Differential Diagnosis Management Outcome/Prognosis Indication for Renal Biopsy Summary
ACUTE GLOMERULONEPHRITIS 1 Definition Etiology Pathology/pathogenesis Risk factors Clinical Presentation Investigation Differential Diagnosis Management Outcome/Prognosis Indication for Renal Biopsy Summary
Atypical IgA Nephropathy
 Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
Atypical IgA Nephropathy Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA XXXIII Chilean Congress of Nephrology, Hypertension and Transplantation Puerto Varas, Chile October 6, 2016 IgA
Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature
 Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature Mouhanna Abu Ghanimeh 1, Omar Abughanimeh 1, Ayman Qasrawi 1, Abdulraheem
Atypical Hemolytic Uremic Syndrome: When the Environment and Mutations Affect Organ Systems. A Case Report with Review of Literature Mouhanna Abu Ghanimeh 1, Omar Abughanimeh 1, Ayman Qasrawi 1, Abdulraheem
Secondary IgA Nephropathy & HSP
 Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Secondary IgA Nephropathy & HSP Anjali Gupta, MD 1/11/11 AKI sec to Hematuria? 65 cases of ARF after an episode of macroscopic hematuria have been reported in the literature in patients with GN. The main
Elevated Serum Creatinine, a simplified approach
 Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Elevated Serum Creatinine, a simplified approach Primary Care Update Creighton University School of Medicine. April 27 th, 2018 Disclosure Slide I have no disclosures and have no conflicts with this presentation.
Crescentic Glomerulonephritis (RPGN)
") Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Crescentic Glomerulonephritis (RPGN) Background Rapidly progressive glomerulonephritis (RPGN) is defined as any glomerular disease characterized by extensive crescents (usually >50%) as the principal histologic
Dr Ian Roberts Oxford. Oxford Pathology Course 2010 for FRCPath Illustration-Cellular Pathology. Oxford Radcliffe NHS Trust
 Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Dr Ian Roberts Oxford Oxford Pathology Course 2010 for FRCPath Present the basic diagnostic features of the commonest conditions causing proteinuria & haematuria Highlight diagnostic pitfalls Nephrotic
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Lapeyraque A-L, Malina M, Fremeaux-Bacchi V, et al. Eculizumab
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Lapeyraque A-L, Malina M, Fremeaux-Bacchi V, et al. Eculizumab
Histopathology: Glomerulonephritis and other renal pathology
 Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Histopathology: Glomerulonephritis and other renal pathology These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you
Management of Rejection
 Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Management of Rejection I have no disclosures Disclosures (relevant or otherwise) Deborah B Adey, MD Professor of Medicine University of California, San Francisco Kidney and Pancreas Transplant Center
Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura
 Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura Kristen Knoph, PharmD, BCPS PGY2 Pharmacotherapy Resident Pharmacy Grand Rounds April 25, 2017 2016 MFMER slide-1 Objectives
Beyond Plasma Exchange: Targeted Therapy for Thrombotic Thrombocytopenic Purpura Kristen Knoph, PharmD, BCPS PGY2 Pharmacotherapy Resident Pharmacy Grand Rounds April 25, 2017 2016 MFMER slide-1 Objectives
Dual positive serology in a case of rapidly progressive glomerulonephritis in a middle aged woman
 CASE REPORT Advance Access publication 20 May 2014 Dual positive serology in a case of rapidly progressive glomerulonephritis in a middle aged woman Rubina Naqvi 1, Muhammed Mubarak 2 1 Department of Nephrology
CASE REPORT Advance Access publication 20 May 2014 Dual positive serology in a case of rapidly progressive glomerulonephritis in a middle aged woman Rubina Naqvi 1, Muhammed Mubarak 2 1 Department of Nephrology
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM. The cases we will cover are:
 THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
THE URINARY SYSTEM The focus of this week s lab will be pathology of the urinary system. Diseases of the kidney can be broken down into diseases that affect the glomeruli, tubules, interstitium, and blood
Risk factors of chronic renal failure after atypical Hemolytic Uremic Syndrome under plasmatherapy
 Risk factors of chronic renal failure after atypical Hemolytic Uremic Syndrome under plasmatherapy Professeur Eric Rondeau Urgences néphrologiques et Transplantation rénale Hôpital Tenon, Paris WWA SFH
Risk factors of chronic renal failure after atypical Hemolytic Uremic Syndrome under plasmatherapy Professeur Eric Rondeau Urgences néphrologiques et Transplantation rénale Hôpital Tenon, Paris WWA SFH
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT
 RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
RECURRENT AND DE NOVO RENAL DISEASES IN THE ALLOGRAFT HISTOPATHOLOGIC DISORDERS AFFECTING THE ALLOGRAFT OTHER THAN REJECTION RECURRENT DISEASE DE NOVO DISEASE TRANSPLANT GLOMERULOPATHY Glomerular Non-glomerular
Primary causes: Complement dysregulation (50% of non-shiga toxin-producing E. coli ) Secondary causes:
 Secondary causes:") General department INTRODUCTION The hemolytic uremic syndrome (HUS): microangiopathic hemolytic anemia, thrombocytopenia, and acute kidney injury One of the main causes of acute kidney injury in children
General department INTRODUCTION The hemolytic uremic syndrome (HUS): microangiopathic hemolytic anemia, thrombocytopenia, and acute kidney injury One of the main causes of acute kidney injury in children