Castleman Disease. Frits van Rhee, MD, PhD, MRCP(UK), FRCPath Myeloma Center, University of Arkansas for Medical Sciences Little Rock, Arkansas
|
|
|
- Cuthbert Spencer
- 5 years ago
- Views:
Transcription

1 Castleman Disease Frits van Rhee, MD, PhD, MRCP(UK), FRCPath Myeloma Center, University of Arkansas for Medical Sciences Little Rock, Arkansas
2 The Castleman Disease Story



3 1954 The trigger Benjamin Castleman, pathologist in Boston

4 First Description Mediastinal mass in 13 young adults Cancer,1956
5 What is Castleman Disease? Group of rare lymph node disorders which share the same histopathology Unicentric vs multicentric Multicentric disease in some patients, often HIV positive, driven by HHV8 In multicentric disease, symptoms and laboratory abnormalities caused by cytokines especially interleukin-6 (IL6)


6 Dysplastic Germinal Center Increased Blood Vessel Formation Hyaline Vascular Variant

7 Lollipop Follicle in Hyaline Vascular CD


8 Plasmacytic Variant Hyperplastic Follicle Sheets of Plasma Cells Expanded Mantle Zone
9 CD Classification Unicentric Castleman Disease (UCD) Idiopathic; 90% no B- symptoms; occasional to severe symptoms (if it causes paraneoplastic pemphigus or cannot be resected) HHV8 negative Surgical excision is usually curative (>90% 5-year survival rate) HHV8-associated Multicentric Castleman Disease (HHV8 + MCD) HHV8 virus drives cytokine release and causes episodes of B-signs, autoimmune manifestations, and multiple organ system impairment (renal failure, pancytopenia, fluid overload); clinically picture: from mono or sepsis B-cell hosts HHV8, secretes vil6, IL6 Rituximab +/- etoposide +/- antivirals are effective HHV8-negative Idiopathic Multicentric Castleman Disease (imcd) Unknown cause drives the cytokine release and B-signs, autoimmune manifestations, and multiple organ system impairment; like HHV8 Unknown host/pathologic cell type Siltuximab newly approved Rituximab and cytotoxic chemotherapy can be be used off label; relapses common FAJGENBAUM D, VAN RHEE F, NABEL C. BLOOD. 2014;123(19):

10 Age Distribution in 384 HIV- Patients TALAT N, AND SCHULTE K THE ONCOLOGIST 2011;16:
11 Unicentric Castleman Disease (UCD) Single, slow-growing lymph node mass, e.g. neck, chest, abdomen, or groin Symptoms, if any, caused by pressure effect of the enlarging lymph nodes Usually Hyaline vascular type, usually HIV- and HHV8-negative Usually no progression to, or association with other tumors Only 10% have systemic symptoms
12 Relationship Between Centricity and Pathologic Subtype Unicentric Usually Hyaline Vascular type (90%) Hyaline Vascular type Multicentric Mixed Cellularity type Plasmacytic type
13 UCD Therapy Surgery: Curative in > 95% of patients Combined approach: embolization, cryoablation followed by surgery Other (drug) therapy followed by surgery Radiation


14 Large Lymph Node Mass Displacing and Compressing Windpipe

15 Embolization Process Microcatheter injection of internal pudendal showing hypervascular mass

16 Embolization Process


17 10cm, 600g Pelvic Mass Rendered Resectable by Embolization

18 Management of UCD Level 1 Level 2A Level 2B Level 3 Talat Ann Surg 2012 Bowne Cancer 1999 Herrada Ann Intern Med 1998 Safford J Ped Surg 2003 Robert Cardiovasc Intervent Radiol No role for anti-il6 therapy except for rare patients with pro-inflammatory syndrome. 2 Consider pre-surgical embolization in large, vascular masses. 3 CT-scan every 6-12 months. 4 In some cases only significant debulking can be achieved Chronowski Cancer 2001 Neuhof Acta Oncologica 2006





19 Role of IL6 in CD in imcd B Cell Growth Elevated VEGF Increased Th2 Cells Inflammatory Response Overgrowth of B cells and plasma cells Increased size of lymph nodes, lymphoma, myeloma Formation of blood vessels Increased blood supply to tumor Vascular leak syndrome Autoimmune reactions Autoantibodies to organs ESR, CRP, IgG, anemia, hypoalbuminemia B-symptoms VAN RHEE ET AL. CLIN ADV HEM ONC 2010
, hepatosplenomegaly (45/60), pleural")
, hypoalbuminemia (57/63), high IL-6 (57/63), abnormal PLTs (28 high, 14 low), renal dysfunction 3X increased prevalence of malignancy in imcd")
 Patients treated with corticosteroids first line experience worse survival 22% died by follow up (median: 28 months) with median")
20 Clinical Features in Review of 128 imcd Cases imcd HHV8 -? HHV8 + HIV + HHV8 +, HIV - Review revealed ~35% of MCD is HHV8-negative, ~45% is HHV-8-positive, ~20% HHV-8-unknown Fever (51/64), hepatosplenomegaly (45/60), pleural effusion (29/38), edema (26/36) 43 plasmacytic, 26 mixed, and 23 hyaline vasculare163- pathological subtypes Elevated CRP (70/79), anemia (76/90), hyper gammaglobulinemia (63/82), hypoalbuminemia (57/63), high IL-6 (57/63), abnormal PLTs (28 high, 14 low), renal dysfunction 3X increased prevalence of malignancy in imcd cases than age-matched SEER controls Autoantibodies or autoimmune hemolytic anemia reported in 38/128 imcd patients NR (21%), PR (42%), CR (37%) to first-line therapies; 41% failed first line (6mo) Patients treated with corticosteroids first line experience worse survival 22% died by follow up (median: 28 months) with median OS of 26 months Causes of death: septic shock, multi-organ failure, and malignancy LIU A ET AL. LANCET HAEMATOLOGY 2016; 3: E
21 Clinical Course Extremely Varied Mild, virtually asymptomatic Waxing and waning Gradually progressive Massive cytokine flares resulting in organ failure and death


22 Ascites Due to Vascular Leak Syndrome
. The normal left transverse sinus is easily seen (white arrows).")
23 Thrombosis of the right transverse sinus demonstrated by loss of flow signal (red arrows). The normal left transverse sinus is easily seen (white arrows).



24 Castleman Disease with Osteosclerotic Bone Lesions


25 Ethnic Impact on Clinical Manifestations: Skin Lesions in Asian Patients


26 Ethnic Impact on Clinical Manifestations: Interstitial Pneumonitis in Asian patients Patient 1 Patient 2
27 imcd Overall Survival DISPENZIERI, ET AL. AM. J. HEMATOLOGY. 2012;87:
28 Why is the historical outcome of imcd poor? Until recently, no diagnostic criteria or treatment guidelines Orphan disease with incidence of patients in the USA CD is complex with different subtypes and varied clinical presentation Few published systematic studies No uniform response criteria Lack of real world data
29 How Do You Diagnose Idiopathic Castleman Disease?
30 Initial Work-up Critical features Clinical Parameters Laboratory Tests/ History Centricity Unicentric vs Multicentric CT-scans or CT-PET Virology HHV8 positive versus negative qpcr HHV8 PB Pathology HV, MC, PC variety LANA-1, EBER, IgG4 stains Symptoms B-symptomatology Night sweats, fever, weight loss, anorexia Laboratory Features Inflammatory response/organ Function Hb, ESR, CRP, fibrinogen, ferritin, albumin, creatinine, platelet count Cytokine Profile Cytokine storm IL6, VEGF, Interleukin 2 Receptor Co-existent Disorders POEMS, MGUS, Myeloma, Amyloidosis, Autoimmune Disorders Myeloma markers, ANA, endocrine function, bone marrow
31 CDCN Consensus Diagnostic Criteria A. Major criteria (both are required) Histopathologic lymph node features consistent with the imcd spectrum Enlarged lymph nodes ( 1 cm in short-axis diameter) in 2 lymph node stations B. Minor Criteria pertaining to symptoms and laboratory markers Minor Criteria (need at least 2 of 11 criteria with at least 1 laboratory criterion C. Exclusion of diseases that can mimic imcd DAVID C. FAJGENBAUM ET AL. BLOOD 2017;129:
32 CDCN Consensus Diagnostic Criteria: Minor Criteria ( 2 of 11) and at least one lab criterion Laboratory 1. C-Reactive Protein (>10mg/dL) and/or ESR (>15) 2. Anemia (Hgb<12.5 for males, <11.5 for females) 3. Thrombocytopenia or thrombocytosis (< 150K/uL; >400k/uL) 4. Hypoalbuminemia (<3.5 gm/dl ) 5. Renal dysfunction (estimated EGFR<60) or proteinuria >150mg/100ml) 6. Hypergammaglobulinemia (>1700mg/dL) Clinical 1. Constitutional Symptoms: Sweats, fever (>100.5), weight loss, fatigue ( 2 CTCAE score for B- symptoms) 2. Large spleen and/or liver 3. Edema/anasarca, effusions 4. Eruptive Cherry Hemangiomata or violaceous papules 5. Interstitial pneumonitis DAVID C. FAJGENBAUM ET AL. BLOOD 2017;129:


33 Related Conditions Must Be Ruled Out DAVID C. FAJGENBAUM ET AL. BLOOD 2017;129:

34 CDCN Algorithm for the Clinico-Pathological Diagnosis of Castleman Disease Infectionrelated (e.g. acute EBV, HIV, TB) Excisional LN Biopsy Histopathology Consistent with CD CT (chest, abdomen, pelvis) or CT-PET Unicentric Multicentric Active Exclusion of Other Disorders Autoimmune Disease (e.g. SLE, RA) Other LPDs (e.g. ALPS, lymphoma) imcd (using consensus criteria) Confirmed MCD HHV8- associated (LANA-1- positive) MCD ADAPTED FROM DAVID C. FAJGENBAUM ET AL. BLOOD 2017;129: POEMSassociated MCD
35 How Do You Treat Idiopathic Castleman Disease?
36 imcd Therapy Corticosteroids Antibodies Rituximab Anti-IL6 antibody therapy: tocilizumab, siltuximab Chemotherapy: Like for lymphoma: R-CHOP, Like for myeloma: VDT (P) ACE Immunomodulatory agents: a-interferon, ATRA, bortezomib, thalidomide, lenalidomide, cyclosporin, sirolimus, anakinra Stem cell transplantation
37 Is the therapy of Castleman Disease a maze?

38 Rationale for Rituximab Therapy CD20+ B-lymphocytes HYALINE VASCULAR CD STAINED WITH CD20 ANTIBODY


39 MCD Post-Rituximab/Steroids Pre-therapy Improving Normal
40 Which data support the role of rituximab in imcd? Very limited data in imcd (case reports) Systematic studies and prolonged follow-up data lacking Still a favorite for many oncologists: familiar drug, effective in lymphoma and HHV8-associated MCD Limited course of single shot therapy
41 IL6 is a pleiotropic cytokine with multiple functions

42 How Anti-IL6 Antibody Therapy Works
43 Interleukin-6
44 Tocilizumab Reduces Lymphadenopathy NORIHIRO NISHIMOTO ET AL. BLOOD 2005;106:
45 Impact of Tocilizumab on Inflammatory Markers NORIHIRO NISHIMOTO ET AL. BLOOD 2005;106:
46 A Multicenter, Randomized, Double-Blind, Placebo-Controlled Study of the Efficacy and Safety of Siltuximab, an Anti-Interleukin 6 Monoclonal Antibody, in Patients with Multicentric Castleman Disease Raymond S Wong 1, Corey Casper 2*, Nikhil Munshi 3, Xiaoyan Ke 4*, Alexander Fosså 5*, David Simpson 6, Marcelo Capra 7*, Ting Liu 8, Ruey Kuen Hsieh 9*, Yeow Tee Goh 10, Jun Zhu 11*, Seok-Goo Cho 12, Hanyun Ren 13, James Cavet 14*, Rajesh Bandekar 15*, Margaret Rothman 16*, Thomas A Puchalski 15*, Shalini Chaturvedi 15*, Helgi van de Velde 17*, Jessica Vermeulen 18* and Frits van Rhee 19 1 Prince of Wales Hospital, The Chinese University of Hong Kong, Hong Kong, Hong Kong; 2 Fred Hutchinson Cancer Research Center, Seattle, WA; 3 Dana-Farber Cancer Institute, Harvard Medical School, Boston, MA; 4 Peking University Third Hospital, Beijing, China; 5 The Norwegian Radium Hospital, Oslo, Norway; 6 North Shore Hospital, Takapuna Auckland, Auckland, New Zealand; 7 Hospital Mãe de Deus, Porto Alegre, Brazil; 8 Department of Hematology, West China Hospital, Sichuan University, Chengdu, China; 9 Mackay Memorial Hospital, Taipei, Taiwan; 10 Singapore General Hospital, Singapore, Singapore; 11 Beijing Cancer Hospital, Beijing, China; 12 Seoul St. Mary's Hospital, Seoul, South Korea; 13 Peking University First Hospital, Beijing, China; 14 The Christie NHS Foundation Trust/University of Manchester, Manchester, United Kingdom; 15 Janssen Research & Development, Spring House, PA; 16 Janssen Research & Development, Washington, GA; 17 Janssen Research & Development, Beerse, Belgium; 18 Janssen Research & Development, Leiden, Netherlands; 19 Myeloma Institute for Research and Therapy, University of Arkansas for Medical Sciences, Little Rock, AR

47 VAN RHEE F LANCET ONCOL, 2014
48 A Multicenter, Randomized, Double-Blind, Placebo- Controlled Study of Siltuximab in Multicentric Castleman Disease First and only multi-national, randomized, double-blind, placebo-controlled, study in MCD MCD subjects Symptomatic Central confirmed pathology HIV, HHV8 negative Treatment naïve or pretreated 1:2 randomization Stratified for steroid use Placebo* (n=26) Siltuximab* (n=53) Treatment failure open label Siltuximab Treatment failure Discontinue Primary study analysis planned at 48 weeks after last patient enrolled *All patients received best supportive care allowing up to 1mg/kg of prednisone VAN RHEE F LANCET ONCOL, 2014

")
49 Primary Endpoint Analysis: Durable Tumor and Symptom Response p= % CR 50% of patients remained on siltuximab 20 PR % Placebo (N=26) Siltuximab (N=53)
50 Siltuximab Statistically Superior Across Major Efficacy Endpoints Durable tumor and symptom response (Central Review) Durable tumor and symptom response (Investigator) Placebo (n=26) Siltuximab (n=53) p- value 0% 34.0% % 45.3% < Tumor response (Central Review) 3.8% 37.7% Tumor response (Investigator) 0% 50.9% < Hemoglobin increase 1.5 g/dl at Week 13 0% 61%
51 Survival probability Time to Treatment Failure Siltuximab Placebo Median TTF: Placebo: 134 days Siltuximab: not reached HR=0.418 p= Time to treatment failure (Days)
52 Waterfall Plot of Tumor Response Independent Review Investigator Assessment ORR 4% 38% ORR 0% 51%
53 BL C2D1 C3D1 C4D1 C5D1 C6D1 C7D1 C8D1 C10D1 C9D1 C11D1 C12D1 Mean Hemoglobin (g/l) Median Erythrocyte Sedimentation Rate (mm/hr) BL C2D1 C3D1 C4D1 C5D1 C6D1 C7D1 C8D1 C12D1 C16D1 Median CRP Levels (mg/l) Median Fibrinogen Levels (umol/l) Changes in Disease-Related Relevant Laboratory Parameters In siltuximab-treated subjects, improvement in MCD related laboratory abnormalities are observed: CRP, ESR and Fibrinogen levels decrease Hemoglobin and Albumin increases CRP Fibrinogen Placebo Siltuximab 0 Visit 8 BL C4D1 C8D1 C12D1 C16D1 Visit 130 Hemoglobin 60 ESR Visit BL C4D1 C8D1 C12D1 C16D1 Visit CRP = C-REACTIVE PROTEIN; ESR = ERYTHROCYTE SEDIMENTATION RATE VAN RHEE F, ET AL. LANCET ONCOL. 2014;15:966-74; WONG RS ET AL. BLOOD 2013;122:505




54 Anti-IL6 Therapy: Siltuximab At diagnosis After 2.5 years of Siltuximab therapy



55 (Baseline) After 2 doses (12 mg/kg q3wk) After 6 doses Skin Lesions Improving with Siltuximab
56 Limitations of Siltuximab Therapy is life long and not a cure Treatment intervals can eventually be spaced out Relapse occurs on cessation of therapy
57 Can we predict who will respond to siltuximab?








58 Responders to siltuximab have a clear inflammatory response by laboratory markers. BRITISH JOURNAL OF HAEMATOLOGY, IN PRESS
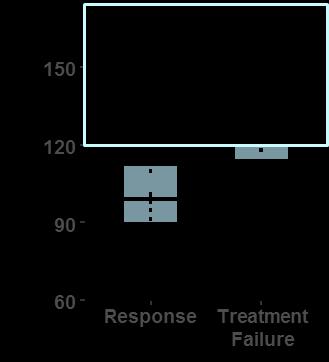
59 Probability Predicted Probability of Response Based on Model Comprising Hb, CRP, IgG and Fibrinogen Response Treatment Failure Correctly classified 15/18 (83%) 19/22 (86%)
60 How to utilize the different therapies?
61 CDCN Criteria for Evaluation of imcd Severity Severe imcd ECOG 2 Stage IV renal dysfunction (egfr < 30; Creatinine >3.0) Anasarca and/or ascites and/or pleural/pericardial effusion (effects of hypercytokinemia/low albumin) Hemoglobin 8.0g/dL Pulmonary involvement /interstitial pneumonitis w/dyspnea VAN RHEE ET AL. BLOOD SEP 4. PII: BLOOD DOI: /BLOOD [EPUB AHEAD OF PRINT]
62 imcd Clinical Case Series of 344 Patients Therapy Patients (n) Response/m* (%) No Response/m* (%) Treatment Failure/m* (%) All Therapies /461 (61) 180/461 (39) 163/367 (44) Corticosteroid Monotherapy /114 (46) 61/114 (54) 62/115 (54) Corticosteroid or Cytotoxic Chemotherapy (not distinguished) Cytotoxic Chemotherapy (any time used) Anti-IL-6 mab (without cytotoxic agent or rituximab) Immunomodulator (without cytotoxic agent) 19 12/19 (63) 7/19 (37) NA /131 (78) 29/131 (22) 44/105 (42) /144 (61) 56/144 (39) 32/100 (32) 27 18/26 (69) 8/26 (31) 10/26 (38) Other 16 8/13 (62) 5/13 (38) 12/15 (80) No treatment/follow-up Only 18 0/14 (0) 14/14 (100) 11/14 (79) m = Total number of regimens evaluated (479) m* = Number regimens assessed for stated outcome van Rhee et al. Blood Sep 4. pii: blood doi: /blood [Epub ahead of print]


63 CDCN Criteria for Evaluation of imcd Severity VAN RHEE ET AL. BLOOD SEP 4. PII: BLOOD DOI: /BLOOD [EPUB AHEAD OF PRINT]

64 State of of imcd Research in in Epidemiology not UpToDate 407 physicians; 32-member SAB; 5 largest ever meetings Limited collaboration, different classifications No First understanding ever R01 for CD of trigger, awarded! cells, 18 pathways studies launched to investigate etiology, cell types, and pathways; 7 more in development Disease model didn t make sense! No Diagnostic diagnostic criteria criteria, published! no treatment ICD-10 guidelines code established! International imcd consensus treatment guidelines published! Published largest series! New subtype described! Promising Siltuximab anti-il-6 approved results! in 2014! No New other disease drugs model or targets guiding in development Research Agenda No animal models or cell lines Over 6,000 patients and loved ones connected! Real-world natural history registry advancing research! No advocacy effort and $0 NIH funding No Identified plan or a strategy promising for therapeutic how studies approach fit together
65 Conclusions Accurate diagnosis of imcd is of paramount importance Tailor therapy to the severity of the disease Severely afflicted patients may require combination chemotherapy On-going research may identify biomarkers for responders to anti-il6 ma therapy. Alternative therapeutic targets for IL6-non-responders
66 Thank You David Fajgenbaum Eric Oksenhendler Sheila Pierson Elaine Jaffé Corey Casper Thomas Uldrick Raymond Wong Peter Voorhees Angela Dispenzieri Makote Ide Katie Stone Amy Greenway Samina Waheed
Simon Haefliger. Pathologie. Fallvorstellung
 Simon Haefliger Pathologie Fallvorstellung Castleman s disease Historical perspective Classification Epidemiology and clinical aspects Microscopic caracteristics Pathogenesis Historical perspective First
Simon Haefliger Pathologie Fallvorstellung Castleman s disease Historical perspective Classification Epidemiology and clinical aspects Microscopic caracteristics Pathogenesis Historical perspective First
Long-term remission in idiopathic Castleman's disease with tocilizumab followed by consolidation with high-dose melphalan-two case studies.
 Long-term remission in idiopathic Castleman's disease with tocilizumab followed by consolidation with high-dose melphalan-two case studies. Jerkeman, Mats; Lindén, Ola Published in: European Journal of
Long-term remission in idiopathic Castleman's disease with tocilizumab followed by consolidation with high-dose melphalan-two case studies. Jerkeman, Mats; Lindén, Ola Published in: European Journal of
Case Report Rituximab Monotherapy in the Management of a Rare Case of an HIV Associated Lymphoproliferative Disorder
 Hindawi Case Reports in Oncological Medicine Volume 2017, Article ID 5235163, 4 pages https://doi.org/10.1155/2017/5235163 Case Report Rituximab Monotherapy in the Management of a Rare Case of an HIV Associated
Hindawi Case Reports in Oncological Medicine Volume 2017, Article ID 5235163, 4 pages https://doi.org/10.1155/2017/5235163 Case Report Rituximab Monotherapy in the Management of a Rare Case of an HIV Associated
Non-Hodgkin s Lymphomas Version
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) n-hodgkin s Lymphomas Version 2.2015 NCCN.g Continue Version 2.2015, 03/03/15 National Comprehensive Cancer Netwk, Inc. 2015, All rights
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) n-hodgkin s Lymphomas Version 2.2015 NCCN.g Continue Version 2.2015, 03/03/15 National Comprehensive Cancer Netwk, Inc. 2015, All rights
About. Castleman s. Disease. First Edition
 About Castleman s Disease First Edition DISCLAMER The About Castleman s Disease booklet is provided for educational purposes only. Consult your own physician regarding the applicability of any opinions
About Castleman s Disease First Edition DISCLAMER The About Castleman s Disease booklet is provided for educational purposes only. Consult your own physician regarding the applicability of any opinions
Patient-reported Outcomes for Multicentric Castleman s Disease in a Randomized, Placebo-controlled Study of Siltuximab
 Patient-reported Outcomes for Multicentric Castleman s Disease in a Randomized, Placebo-controlled Study of Siltuximab The Harvard community has made this article openly available. Please share how this
Patient-reported Outcomes for Multicentric Castleman s Disease in a Randomized, Placebo-controlled Study of Siltuximab The Harvard community has made this article openly available. Please share how this
Unicentric Castleman s disease: An unusual cause of neck swelling
 Komaranchath et al. 5 CASE REPORT PEER REVIEWED OPEN ACCESS Unicentric Castleman s disease: An unusual cause of neck swelling Ashok S. Komaranchath, A.H. Rudresh, Kuntegowdenahalli Lakshmaiah C., Chennagiri
Komaranchath et al. 5 CASE REPORT PEER REVIEWED OPEN ACCESS Unicentric Castleman s disease: An unusual cause of neck swelling Ashok S. Komaranchath, A.H. Rudresh, Kuntegowdenahalli Lakshmaiah C., Chennagiri
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
NON HODGKINS LYMPHOMA: INDOLENT Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and Dr.
DiagnosticUtility of Interleukin-6 Expression by Immunohistochemistry in Differentiating Castleman Disease Subtypes and Reactive Lymphadenopathies
 474 Available online at www.annclinlabsci.org Annals of Clinical & Laboratory Science, vol. 46, no. 5, 2016 DiagnosticUtility of Interleukin-6 Expression by Immunohistochemistry in Differentiating Castleman
474 Available online at www.annclinlabsci.org Annals of Clinical & Laboratory Science, vol. 46, no. 5, 2016 DiagnosticUtility of Interleukin-6 Expression by Immunohistochemistry in Differentiating Castleman
Idiopathic multicentric Castleman s disease: a systematic literature review
 Idiopathic multicentric Castleman s disease: a systematic literature review Amy Y Liu, Christopher S Nabel, Brian S Finkelman, Jason R Ruth, Razelle Kurzrock, Frits van Rhee, Vera P Krymskaya, Dermot Kelleher,
Idiopathic multicentric Castleman s disease: a systematic literature review Amy Y Liu, Christopher S Nabel, Brian S Finkelman, Jason R Ruth, Razelle Kurzrock, Frits van Rhee, Vera P Krymskaya, Dermot Kelleher,
Mantle Cell Lymphoma
 Mantle Cell Lymphoma Clinical Case A 56 year-old woman complains of pain and fullness in the left superior abdominal quadrant for the last 8 months. She has lost 25 kg, and lately has had night sweats.
Mantle Cell Lymphoma Clinical Case A 56 year-old woman complains of pain and fullness in the left superior abdominal quadrant for the last 8 months. She has lost 25 kg, and lately has had night sweats.
Lymphatic System Disorders
 Lymphatic System Disorders Lymphomas Malignant neoplasms involving lymphocyte proliferation in lymph nodes Specific causes not identified // Higher risk in adults who received radiation during childhood
Lymphatic System Disorders Lymphomas Malignant neoplasms involving lymphocyte proliferation in lymph nodes Specific causes not identified // Higher risk in adults who received radiation during childhood
Smoldering Myeloma: Leave them alone!
 Smoldering Myeloma: Leave them alone! David H. Vesole, MD, PhD Co-Director, Myeloma Division Director, Myeloma Research John Theurer Cancer Center Hackensack University Medical Center Prevalence 1960 2002
Smoldering Myeloma: Leave them alone! David H. Vesole, MD, PhD Co-Director, Myeloma Division Director, Myeloma Research John Theurer Cancer Center Hackensack University Medical Center Prevalence 1960 2002
HIV ASSOCIATED LYMPHOMA. Dr N Rapiti
 HIV ASSOCIATED LYMPHOMA Dr N Rapiti HIV ASSOCIATED LYMPHOMA: OVERVIEW Classification Pathogenesis Prognosis cart Chemotherapy/Radiotherapy/SCT Supportive CASE 40 yr old male, Mr BM, p/w Symptomatic anemia
HIV ASSOCIATED LYMPHOMA Dr N Rapiti HIV ASSOCIATED LYMPHOMA: OVERVIEW Classification Pathogenesis Prognosis cart Chemotherapy/Radiotherapy/SCT Supportive CASE 40 yr old male, Mr BM, p/w Symptomatic anemia
Osteosclerotic Myeloma (POEMS Syndrome)
") Osteosclerotic Myeloma (POEMS Syndrome) Osteosclerotic Myeloma (POEMS Syndrome) Synonyms Crow-Fukase syndrome Multicentric Castleman disease Takatsuki syndrome Acronym coined by Bardwick POEMS Scheinker,
Osteosclerotic Myeloma (POEMS Syndrome) Osteosclerotic Myeloma (POEMS Syndrome) Synonyms Crow-Fukase syndrome Multicentric Castleman disease Takatsuki syndrome Acronym coined by Bardwick POEMS Scheinker,
SLIDE SEMINAR NON NEOPLASTIC LYMPH NODE DISORDERS DR SHEILA NAIR CMC, VELLORE
 SLIDE SEMINAR NON NEOPLASTIC LYMPH NODE DISORDERS DR SHEILA NAIR CMC, VELLORE Case 1 34 year old male, mass right cervical region, for 4 years. No other significant findings. Grossly, the mass was well
SLIDE SEMINAR NON NEOPLASTIC LYMPH NODE DISORDERS DR SHEILA NAIR CMC, VELLORE Case 1 34 year old male, mass right cervical region, for 4 years. No other significant findings. Grossly, the mass was well
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: van Rhee F, Wong RS, Munshi N, et al. Siltuximab
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: van Rhee F, Wong RS, Munshi N, et al. Siltuximab
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial
 Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center
 LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center Lymphoma is cancer of the lymphatic system. The lymphatic system is made up of organs all over the body that make up and store cells
LYMPHOMA Joginder Singh, MD Medical Oncologist, Mercy Cancer Center Lymphoma is cancer of the lymphatic system. The lymphatic system is made up of organs all over the body that make up and store cells
How SYLVANT May Help IMPORTANT SAFETY INFORMATION. Multicentric Castleman s Disease.
 SYLVANT (siltuximab) is a prescription medicine used to treat people with Multicentric Castleman s Disease (MCD) who do not have human immunodeficiency virus (HIV) and human herpesvirus-8 (HHV-8) infection.
SYLVANT (siltuximab) is a prescription medicine used to treat people with Multicentric Castleman s Disease (MCD) who do not have human immunodeficiency virus (HIV) and human herpesvirus-8 (HHV-8) infection.
Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma:
 1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
DIAGNOSIS AND TREATMENT OF WALDENSTRÖM S MACROGLOBULINAEMIA IN THE NETHERLANDS. Monique Minnema UMC Utrecht
 DIAGNOSIS AND TREATMENT OF WALDENSTRÖM S MACROGLOBULINAEMIA IN THE NETHERLANDS Monique Minnema UMC Utrecht Organisation of hematological care in the Netherlands Intensive chemotherapy, including acute
DIAGNOSIS AND TREATMENT OF WALDENSTRÖM S MACROGLOBULINAEMIA IN THE NETHERLANDS Monique Minnema UMC Utrecht Organisation of hematological care in the Netherlands Intensive chemotherapy, including acute
ABSTRACT INTRODUCTION
 /, Vol. 6, No. 30 A phase 2, open-label, multicenter study of the long-term safety of siltuximab (an anti-interleukin-6 monoclonal antibody) in patients with multicentric Castleman disease Frits van Rhee
/, Vol. 6, No. 30 A phase 2, open-label, multicenter study of the long-term safety of siltuximab (an anti-interleukin-6 monoclonal antibody) in patients with multicentric Castleman disease Frits van Rhee
Morphology Case Study. Presented by Niamh O Donnell, BSc, MSc. Medical Scientist Haematology Laboratory Cork University Hospital
 Morphology Case Study Presented by Niamh O Donnell, BSc, MSc. Medical Scientist Haematology Laboratory Cork University Hospital 41 year old male presented to GP for routine check-up in May 2011. FBC Results:
Morphology Case Study Presented by Niamh O Donnell, BSc, MSc. Medical Scientist Haematology Laboratory Cork University Hospital 41 year old male presented to GP for routine check-up in May 2011. FBC Results:
Should we treat Smoldering MM patients? María-Victoria Mateos University Hospital of Salamanca Salamanca. Spain
 Should we treat Smoldering MM patients? María-Victoria Mateos University Hospital of Salamanca Salamanca. Spain Should we treat some patients with Stage I MM? Len-dex is a promising and atractive option
Should we treat Smoldering MM patients? María-Victoria Mateos University Hospital of Salamanca Salamanca. Spain Should we treat some patients with Stage I MM? Len-dex is a promising and atractive option
Advances in the Treatment of Hematologic Malignancies. Disclosures
 Advances in the Treatment of Hematologic Malignancies A Review of Newly Approved Drugs Katherine Shah, PharmD, BCOP Clinical Pharmacy Specialist, Hematology/Oncology Emory University Hospital / Winship
Advances in the Treatment of Hematologic Malignancies A Review of Newly Approved Drugs Katherine Shah, PharmD, BCOP Clinical Pharmacy Specialist, Hematology/Oncology Emory University Hospital / Winship
What are the hurdles to using cell of origin in classification to treat DLBCL?
 What are the hurdles to using cell of origin in classification to treat DLBCL? John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical
What are the hurdles to using cell of origin in classification to treat DLBCL? John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical
Treatment of Waldenström s Macroglobulinemia Mayo Consensus
 Treatment of Waldenström s Macroglobulinemia Mayo Consensus Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Mayo Clinic College of Medicine Mayo Clinic Comprehensive Cancer Center Mayo Clinic
Treatment of Waldenström s Macroglobulinemia Mayo Consensus Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Mayo Clinic College of Medicine Mayo Clinic Comprehensive Cancer Center Mayo Clinic
Patient Case Studies & Panel Discussion
 Patient Case Studies & Panel Discussion Panelists: Jeremy S. Abramson, MD, Massachusetts General Hospital Cancer Center; Ranjana H. Advani, MD, Stanford Cancer Institute; Andrew D. Zelenetz, MD, PhD, Memorial
Patient Case Studies & Panel Discussion Panelists: Jeremy S. Abramson, MD, Massachusetts General Hospital Cancer Center; Ranjana H. Advani, MD, Stanford Cancer Institute; Andrew D. Zelenetz, MD, PhD, Memorial
Clinicopathologic analysis of TAFRO syndrome demonstrates a distinct subtype of HHV-8-negative multicentric Castleman disease
 Clinicopathologic analysis of TAFRO syndrome demonstrates a distinct subtype of HHV-8-negative multicentric Castleman disease AJH Noriko Iwaki, 1,2 David C. Fajgenbaum, 3 Christopher S. Nabel, 3 Yuka Gion,
Clinicopathologic analysis of TAFRO syndrome demonstrates a distinct subtype of HHV-8-negative multicentric Castleman disease AJH Noriko Iwaki, 1,2 David C. Fajgenbaum, 3 Christopher S. Nabel, 3 Yuka Gion,
Velcade (bortezomib)
") Velcade (bortezomib) Line(s) of Business: HMO; PPO; QUEST Integration Akamai Advantage Original Effective Date: 03/09/2004 Current Effective Date: 05/01/2017 POLICY A. INDICATIONS The indications below
Velcade (bortezomib) Line(s) of Business: HMO; PPO; QUEST Integration Akamai Advantage Original Effective Date: 03/09/2004 Current Effective Date: 05/01/2017 POLICY A. INDICATIONS The indications below
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
A CRP Breakout Session
 A041202 CRP Breakout Session Jennifer Woyach, MD, A041202 Study Chair Samantha Sublett, A041202 Protocol Coordinator Luke Wilson, A041202 Data Manager Alliance Fall Group Meeting November 5, 2015 Agenda
A041202 CRP Breakout Session Jennifer Woyach, MD, A041202 Study Chair Samantha Sublett, A041202 Protocol Coordinator Luke Wilson, A041202 Data Manager Alliance Fall Group Meeting November 5, 2015 Agenda
Waldenstrom s Macroglobulinemia
 Waldenstrom s Macroglobulinemia : Introduction Waldenstrom s macroglobulinemia (WM) is a lymphoma, or cancer of the lymphatic system. It occurs in a type of white blood cell called a B-lymphocyte or B-cell,
Waldenstrom s Macroglobulinemia : Introduction Waldenstrom s macroglobulinemia (WM) is a lymphoma, or cancer of the lymphatic system. It occurs in a type of white blood cell called a B-lymphocyte or B-cell,
BR for previously untreated or relapsed CLL
 1 Protocol synopsis Title Rationale Study Objectives Multicentre phase II trial of bendamustine in combination with rituximab for patients with previously untreated or relapsed chronic lymphocytic leukemia
1 Protocol synopsis Title Rationale Study Objectives Multicentre phase II trial of bendamustine in combination with rituximab for patients with previously untreated or relapsed chronic lymphocytic leukemia
Hematology 101. Rachid Baz, M.D. 5/16/2014
 Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary)
") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Understanding your diagnosis. Dr Graham Collins Consultant Haemtologist Oxford University Hospitals
 Understanding your diagnosis Dr Graham Collins Consultant Haemtologist Oxford University Hospitals Common questions I get asked What is lymphoma? What subtype do I have and what does that mean? What are
Understanding your diagnosis Dr Graham Collins Consultant Haemtologist Oxford University Hospitals Common questions I get asked What is lymphoma? What subtype do I have and what does that mean? What are
Velcade (bortezomib)
") Velcade (bortezomib) Line(s) of Business: HMO; PPO; QUEST Integration Medicare Advantage Original Effective Date: 03/09/2004 Current Effective Date: 03/01/2018 POLICY A. INDICATIONS The indications below
Velcade (bortezomib) Line(s) of Business: HMO; PPO; QUEST Integration Medicare Advantage Original Effective Date: 03/09/2004 Current Effective Date: 03/01/2018 POLICY A. INDICATIONS The indications below
Clinicopathologic Features of Castleman s disease: Experience at King Hussein Medical Center
 Clinicopathologic Features of Castleman s disease: Experience at King Hussein Medical Center Sura Alrawabdeh, MD*, Ibrahim Jraisat, MD**,Nabeeha Abbasi, MD*, Shadi Aldaoud, MD***, Sami Alhijazien, MD***
Clinicopathologic Features of Castleman s disease: Experience at King Hussein Medical Center Sura Alrawabdeh, MD*, Ibrahim Jraisat, MD**,Nabeeha Abbasi, MD*, Shadi Aldaoud, MD***, Sami Alhijazien, MD***
Case conference. Welcome Dr. Lawrence Tierney
 Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
Idelalisib in the Treatment of Chronic Lymphocytic Leukemia
 Idelalisib in the Treatment of Chronic Lymphocytic Leukemia Jacqueline C. Barrientos, MD Assistant Professor of Medicine Hofstra North Shore LIJ School of Medicine North Shore LIJ Cancer Institute CLL
Idelalisib in the Treatment of Chronic Lymphocytic Leukemia Jacqueline C. Barrientos, MD Assistant Professor of Medicine Hofstra North Shore LIJ School of Medicine North Shore LIJ Cancer Institute CLL
What is a hematological malignancy? Hematology and Hematologic Malignancies. Etiology of hematological malignancies. Leukemias
 Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Case Report Coexistence of Hodgkin s Lymphoma and Castleman s Disease: A Case Report with Successful Response to Chemotherapy and Radiotherapy
 Case Reports in Oncological Medicine Volume 2013, Article ID 487205, 4 pages http://dx.doi.org/10.1155/2013/487205 Case Report Coexistence of Hodgkin s Lymphoma and Castleman s Disease: A Case Report with
Case Reports in Oncological Medicine Volume 2013, Article ID 487205, 4 pages http://dx.doi.org/10.1155/2013/487205 Case Report Coexistence of Hodgkin s Lymphoma and Castleman s Disease: A Case Report with
CLL & SLL: Current Management & Treatment. Dr. Isabelle Bence-Bruckler
 CLL & SLL: Current Management & Treatment Dr. Isabelle Bence-Bruckler Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of white blood cell B lymphocyte Lymphocytic Cancer
CLL & SLL: Current Management & Treatment Dr. Isabelle Bence-Bruckler Chronic Lymphocytic Leukemia Prolonged clinical course Chronic A particular type of white blood cell B lymphocyte Lymphocytic Cancer
Summary. Keywords: Castleman disease, clinical complications, paraneoplastic pemphigus, survival analysis, prognostic factors.
 characterized as unicentric (UCD) and multicentric (MCD). Pathologically, CD can be classified into three variants: hyaline vascular variant (HV), plasmacytic variant (PC) and mixed cellular variant (Mix).
characterized as unicentric (UCD) and multicentric (MCD). Pathologically, CD can be classified into three variants: hyaline vascular variant (HV), plasmacytic variant (PC) and mixed cellular variant (Mix).
Idelalisib treatment is associated with improved cytopenias in patients with relapsed/refractory inhl and CLL
 Idelalisib treatment is associated with improved cytopenias in patients with relapsed/refractory inhl and CLL Susan M O Brien, Andrew J Davies, Ian W Flinn, Ajay K Gopal, Thomas J Kipps, Gilles A Salles,
Idelalisib treatment is associated with improved cytopenias in patients with relapsed/refractory inhl and CLL Susan M O Brien, Andrew J Davies, Ian W Flinn, Ajay K Gopal, Thomas J Kipps, Gilles A Salles,
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma
 Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
Forms Revision: Myeloma Changes
 Sharing knowledge. Sharing hope. Forms Revision: Myeloma Changes J. Brunner, PA-C and A. Dispenzieri, MD February 2013 Disclosures Janet Brunner, PA-C I have no relevant conflicts of interest to disclose.
Sharing knowledge. Sharing hope. Forms Revision: Myeloma Changes J. Brunner, PA-C and A. Dispenzieri, MD February 2013 Disclosures Janet Brunner, PA-C I have no relevant conflicts of interest to disclose.
ClinicalTrials.gov Identifier: NCT
 Efficacy of Daratumumab, Bortezomib, and Dexamethasone Versus Bortezomib and Dexamethasone in Relapsed or Refractory Multiple Myeloma Based on Prior Lines of Therapy: Updated Analysis of CASTOR Maria-Victoria
Efficacy of Daratumumab, Bortezomib, and Dexamethasone Versus Bortezomib and Dexamethasone in Relapsed or Refractory Multiple Myeloma Based on Prior Lines of Therapy: Updated Analysis of CASTOR Maria-Victoria
Fever in Lupus. 21 st April 2014
 Fever in Lupus 21 st April 2014 Fever in lupus Cause of fever N= 487 % SLE fever 206 42 Infection in SLE 265 54.5 Active SLE and infection 8 1.6 Tumor fever 4 0.8 Miscellaneous 4 0.8 Crucial Question Infection
Fever in Lupus 21 st April 2014 Fever in lupus Cause of fever N= 487 % SLE fever 206 42 Infection in SLE 265 54.5 Active SLE and infection 8 1.6 Tumor fever 4 0.8 Miscellaneous 4 0.8 Crucial Question Infection
Successful Treatment with Cyclosporin A in Tocilizumab-resistant TAFRO Syndrome
 CASE REPORT Successful Treatment with Cyclosporin A in Tocilizumab-resistant TAFRO Syndrome Yusuke Yamaga 1, Kiyonobu Tokuyama 1, Takehiro Kato 1,RieYamada 1, Masanori Murayama 1, Tsuneko Ikeda 2, Noriyoshi
CASE REPORT Successful Treatment with Cyclosporin A in Tocilizumab-resistant TAFRO Syndrome Yusuke Yamaga 1, Kiyonobu Tokuyama 1, Takehiro Kato 1,RieYamada 1, Masanori Murayama 1, Tsuneko Ikeda 2, Noriyoshi
Non-Hodgkin lymphoma
 Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
New Targets and Treatments for Follicular Lymphoma
 Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Update on Waldenström Macroglobulinemia (WM)
") Update on Waldenström Macroglobulinemia (WM) Stephen M. Ansell, MD, PhD Professor of Medicine Division of Hematology Mayo Clinic Rochester, MN Update on Waldenström Macroglobulinemia (WM) Disclosures Stephen
Update on Waldenström Macroglobulinemia (WM) Stephen M. Ansell, MD, PhD Professor of Medicine Division of Hematology Mayo Clinic Rochester, MN Update on Waldenström Macroglobulinemia (WM) Disclosures Stephen
M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016
 + M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016 + Disclosures Advisory Boards: AMGEN, Lundbeck, NOVARTIS + Subtypes of Plasma Cell Disorders Increased Plasma
+ M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016 + Disclosures Advisory Boards: AMGEN, Lundbeck, NOVARTIS + Subtypes of Plasma Cell Disorders Increased Plasma
Case 5 15-year-old male
 Case 5 15-year-old male Present illness: Six months ago, abnormality of ECG was incidentally detected by annual health check. His blood level of γ-gtp, HbA1c and norepinephrine were elevated; however,
Case 5 15-year-old male Present illness: Six months ago, abnormality of ECG was incidentally detected by annual health check. His blood level of γ-gtp, HbA1c and norepinephrine were elevated; however,
Warm Autoantibodies in a Patient with Hemophagocytic Lymphohistiocytosis: A Case Report
 Warm Autoantibodies in a Patient with Hemophagocytic Lymphohistiocytosis: A Case Report Emily Coberly, MD Department of Pathology and Anatomical Sciences University of Missouri Columbia April 30, 2013
Warm Autoantibodies in a Patient with Hemophagocytic Lymphohistiocytosis: A Case Report Emily Coberly, MD Department of Pathology and Anatomical Sciences University of Missouri Columbia April 30, 2013
Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113)
") Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the CLL Post-HSCT Data Form. E-mail
Instructions for Chronic Lymphocytic Leukemia Post-HSCT Data (Form 2113) This section of the CIBMTR Forms Instruction Manual is intended to be a resource for completing the CLL Post-HSCT Data Form. E-mail
Overview of Cutaneous Lymphomas: Diagnosis and Staging. Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology
 Overview of Cutaneous Lymphomas: Diagnosis and Staging Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology Definition of Lymphoma A cancer or malignancy that comes from
Overview of Cutaneous Lymphomas: Diagnosis and Staging Lauren C. Pinter-Brown MD, FACP Health Sciences Professor of Medicine and Dermatology Definition of Lymphoma A cancer or malignancy that comes from
Castleman Disease (CD) is a rare and potentially
 is a rare and potentially") doi: http://dx.doi.org/10.11606/issn.1679-9836.v95ispe3p24-29 Rare disease research requires (and benefits from) global collaboration: three examples from the Castleman Disease Collaborative Network Hayley
doi: http://dx.doi.org/10.11606/issn.1679-9836.v95ispe3p24-29 Rare disease research requires (and benefits from) global collaboration: three examples from the Castleman Disease Collaborative Network Hayley
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Maemondo M, Inoue A, Kobayashi K, et al. Gefitinib or chemotherapy
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Maemondo M, Inoue A, Kobayashi K, et al. Gefitinib or chemotherapy
How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES
 How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES How I Choose First Line Treatment in Follicular Lymphoma in 2017? 1. How do I take into account
How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES How I Choose First Line Treatment in Follicular Lymphoma in 2017? 1. How do I take into account
MANTLE CELL LYMPHOMA
 MANTLE CELL LYMPHOMA CLINICAL CASE PRESENTATION Martin Dreyling Medizinische Klinik III LMU München Munich, Germany esmo.org Multicenter Evaluation of MCL Annency Criteria fulfilled event free interval
MANTLE CELL LYMPHOMA CLINICAL CASE PRESENTATION Martin Dreyling Medizinische Klinik III LMU München Munich, Germany esmo.org Multicenter Evaluation of MCL Annency Criteria fulfilled event free interval
88-year-old Female with Lymphadenopathy. Faizi Ali, MD
 88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
Peking University People's Hospital, Peking University Institute of Hematology
 Qian Jiang, M.D. Peking University People's Hospital, Peking University Institute of Hematology No. 11 Xizhimen South Street, Beijing, 100044, China. Phone number: 86-10-66583802 Mobile: 86-13611115100
Qian Jiang, M.D. Peking University People's Hospital, Peking University Institute of Hematology No. 11 Xizhimen South Street, Beijing, 100044, China. Phone number: 86-10-66583802 Mobile: 86-13611115100
Ibrutinib Withdrawal Symptoms in Patients with Waldenström Macroglobulinemia
 Published Ahead of Print on February 22, 2018, as doi:10.3324/haematol.2017.186908. Copyright 2018 Ferrata Storti Foundation. Ibrutinib Withdrawal Symptoms in Patients with Waldenström Macroglobulinemia
Published Ahead of Print on February 22, 2018, as doi:10.3324/haematol.2017.186908. Copyright 2018 Ferrata Storti Foundation. Ibrutinib Withdrawal Symptoms in Patients with Waldenström Macroglobulinemia
This was a multicenter study conducted at 11 sites in the United States and 11 sites in Europe.
 Protocol CAM211: A Phase II Study of Campath-1H (CAMPATH ) in Patients with B- Cell Chronic Lymphocytic Leukemia who have Received an Alkylating Agent and Failed Fludarabine Therapy These results are supplied
Protocol CAM211: A Phase II Study of Campath-1H (CAMPATH ) in Patients with B- Cell Chronic Lymphocytic Leukemia who have Received an Alkylating Agent and Failed Fludarabine Therapy These results are supplied
Background. Approved by FDA and EMEA for CLL and allows for treatment without chemotherapy in all lines of therapy
 Updated Efficacy and Safety From the Phase 3 RESONATE-2 Study: Ibrutinib As First-Line Treatment Option in Patients 65 Years and Older With Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma Abstract
Updated Efficacy and Safety From the Phase 3 RESONATE-2 Study: Ibrutinib As First-Line Treatment Option in Patients 65 Years and Older With Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma Abstract
Relapsed/Refractory Hodgkin Lymphoma
 Relapsed/Refractory Hodgkin Lymphoma Anas Younes, MD Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center New York, New York, United States Case Study 32-year-old woman was diagnosed with stage
Relapsed/Refractory Hodgkin Lymphoma Anas Younes, MD Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center New York, New York, United States Case Study 32-year-old woman was diagnosed with stage
Dr Shankara Paneesha. ASH Highlights Department of Haematology & Stem cell Transplantation
 ASH Highlights 2015 Themes of ASH 2015 Novel therapies - Myeloma AML Lymphoma Pd-L1 & PD-l inhibitors Emerging concepts in biology HIF-1a pathway Cautionary tales ASH Choosing Wisely list IFM/DFCI
ASH Highlights 2015 Themes of ASH 2015 Novel therapies - Myeloma AML Lymphoma Pd-L1 & PD-l inhibitors Emerging concepts in biology HIF-1a pathway Cautionary tales ASH Choosing Wisely list IFM/DFCI
A) PUBLIC HEALTH B) PRESENTATION & DIAGNOSIS
 PUBLIC HEALTH B) PRESENTATION & DIAGNOSIS") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary), April 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Centre, BC Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary), April 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Centre, BC Cancer
Lymphoma Read with the experts
 Lymphoma Read with the experts Marc Seltzer, MD Associate Professor of Radiology Geisel School of Medicine at Dartmouth Director, PET-CT Course American College of Radiology Learning Objectives Recognize
Lymphoma Read with the experts Marc Seltzer, MD Associate Professor of Radiology Geisel School of Medicine at Dartmouth Director, PET-CT Course American College of Radiology Learning Objectives Recognize
DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA
 DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA Ian Flinn, CB Miller, KM Ardeshna, S Tetreault, SE Assouline, PL Zinzani, J Mayer, M Merli, SD Lunin, AR Pettitt,
DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA Ian Flinn, CB Miller, KM Ardeshna, S Tetreault, SE Assouline, PL Zinzani, J Mayer, M Merli, SD Lunin, AR Pettitt,
Large cell immunoblastic Diffuse histiocytic (DHL) Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s
 Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s") Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Case Workshop of Society for Hematopathology and European Association for Haematopathology
 Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
Presentation by Dr. Thomas Yau on behalf of his co-authors
 4078 First presented at the American Society of Clinical Oncology (ASCO) 2016 Annual Meeting, Chicago, Illinois, USA, June 3-7, 2016. Reused with permission from the American Society of Clinical Oncology
4078 First presented at the American Society of Clinical Oncology (ASCO) 2016 Annual Meeting, Chicago, Illinois, USA, June 3-7, 2016. Reused with permission from the American Society of Clinical Oncology
New Evidence reports on presentations given at EHA/ICML Bendamustine in the Treatment of Lymphoproliferative Disorders
 New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
Waldenstrom s Macroglobulinemia
 Waldenstrom s Macroglobulinemia : Monoclonal Antibodies Introduction Waldenstrom s macroglobulinemia (WM) is a lymphoma, or cancer of the lymphatic system. It occurs in a type of white blood cell called
Waldenstrom s Macroglobulinemia : Monoclonal Antibodies Introduction Waldenstrom s macroglobulinemia (WM) is a lymphoma, or cancer of the lymphatic system. It occurs in a type of white blood cell called
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic
 Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Indolent Lymphomas. Dr. Melissa Toupin The Ottawa Hospital
 Indolent Lymphomas Dr. Melissa Toupin The Ottawa Hospital What does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with
Indolent Lymphomas Dr. Melissa Toupin The Ottawa Hospital What does indolent mean? Slow growth Often asymptomatic Chronic disease with periods of relapse (long natural history possible) Incurable with
Larger than Life. Angela Thomae Case Study CHEM 454
 Angela Thomae Case Study CHEM 454 Larger than Life Maria Thomas, a 5 year old girl, was brought to Urgent Care at the hospital because of a painful swelling in her neck. The doctor who was on call that
Angela Thomae Case Study CHEM 454 Larger than Life Maria Thomas, a 5 year old girl, was brought to Urgent Care at the hospital because of a painful swelling in her neck. The doctor who was on call that
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Multiple Myeloma Updates 2007
 Multiple Myeloma Updates 2007 Brian Berryman, M.D. Multiple Myeloma Updates 2007 Goals for today: Understand the staging systems for myeloma Understand prognostic factors in myeloma Review updates from
Multiple Myeloma Updates 2007 Brian Berryman, M.D. Multiple Myeloma Updates 2007 Goals for today: Understand the staging systems for myeloma Understand prognostic factors in myeloma Review updates from
Lymphoma is a cancer that develops in the white blood cells (lymphocytes) of the lymphatic system, which is part of the body's immune system.
 of the lymphatic system, which is part of the body's immune system.") Scan for mobile link. Lymphoma Lymphoma is a cancer that develops in the white blood cells of the lymphatic system. Symptoms may include enlarged lymph nodes, unexplained weight loss, fatigue, night sweats
Scan for mobile link. Lymphoma Lymphoma is a cancer that develops in the white blood cells of the lymphatic system. Symptoms may include enlarged lymph nodes, unexplained weight loss, fatigue, night sweats
Update: New Treatment Modalities
 ASH 2008 Update: New Treatment Modalities ASH 2008: Update on new treatment modalities GA101 Improves tumour growth inhibition in mice and exhibits a promising safety profile in patients with CD20+ malignant
ASH 2008 Update: New Treatment Modalities ASH 2008: Update on new treatment modalities GA101 Improves tumour growth inhibition in mice and exhibits a promising safety profile in patients with CD20+ malignant
Major Diagnostic Criteria
 Multiple Myeloma Elizabeth Ann Coleman, PhD, RNP, AOCN Professor and Chair, Dept. of Nursing Science Cooper Chair in Oncology Nursing, College of Nursing Professor, Dept. of Internal Medicine, College
Multiple Myeloma Elizabeth Ann Coleman, PhD, RNP, AOCN Professor and Chair, Dept. of Nursing Science Cooper Chair in Oncology Nursing, College of Nursing Professor, Dept. of Internal Medicine, College
Non-Hodgkin Lymphoma in Clinically Difficult Situations
 Winship Cancer Institute of Emory University Non-Hodgkin Lymphoma in Clinically Difficult Situations James Armitage, MD Professor, Department of Internal Medicine Joe Shapiro Distinguished Chair of Oncology
Winship Cancer Institute of Emory University Non-Hodgkin Lymphoma in Clinically Difficult Situations James Armitage, MD Professor, Department of Internal Medicine Joe Shapiro Distinguished Chair of Oncology
This was a multi-center study conducted at 44 study centers. There were 9 centers in the United States and 35 centers in Europe.
 Protocol CAM307: A Phase 3 Study to Evaluate the Efficacy and Safety of Frontline Therapy with Alemtuzumab (Campath ) vs Chlorambucil in Patients with Progressive B-Cell Chronic Lymphocytic Leukemia These
Protocol CAM307: A Phase 3 Study to Evaluate the Efficacy and Safety of Frontline Therapy with Alemtuzumab (Campath ) vs Chlorambucil in Patients with Progressive B-Cell Chronic Lymphocytic Leukemia These
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma
 Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Dana-Farber Cancer Institute, Boston, MA, USA; 2. H. Lee Moffitt Cancer Center & Research Institute, Tampa, FL, USA; 3
 The investigational agent MLN9708, an oral proteasome inhibitor, in patients with relapsed and/or refractory multiple myeloma (MM): results from the expansion cohorts of a phase 1 dose-escalation study
The investigational agent MLN9708, an oral proteasome inhibitor, in patients with relapsed and/or refractory multiple myeloma (MM): results from the expansion cohorts of a phase 1 dose-escalation study
Pathology of Hematopoietic and Lymphoid tissue
 Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
All Wales Lymphoma Panel Lymphoma Course April 2015 Wales Millennium Centre Cardiff
 All Wales Lymphoma Panel Lymphoma Course 23-24 April 2015 Wales Millennium Centre Cardiff Case Histories Online slides at: http://dental.uwcm.ac.uk:82/awlp%20course%202015/view.apml? Professor Sebastian
All Wales Lymphoma Panel Lymphoma Course 23-24 April 2015 Wales Millennium Centre Cardiff Case Histories Online slides at: http://dental.uwcm.ac.uk:82/awlp%20course%202015/view.apml? Professor Sebastian
Hematology: Challenging Cases with Your Participation COPYRIGHT
 Hematology: Challenging Cases with Your Participation Reed E. Drews, MD Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Question 1 Question 1 64-year-old man is evaluated during
Hematology: Challenging Cases with Your Participation Reed E. Drews, MD Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Question 1 Question 1 64-year-old man is evaluated during
Diagnosis and patient pathway in lymphomas
 The Royal Marsden Diagnosis and patient pathway in lymphomas Dr Ian Chau Consultant Medical Oncologist The Royal Marsden Hospital London & Surrey Change Presentation title and date in Footer dd.mm.yyyy
The Royal Marsden Diagnosis and patient pathway in lymphomas Dr Ian Chau Consultant Medical Oncologist The Royal Marsden Hospital London & Surrey Change Presentation title and date in Footer dd.mm.yyyy
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014
 Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 TB Case Presentation Andrea Cruz, MD, MPH August 14, 2014 Andrea Cruz, MD, MPH has the following disclosures to
Advanced Management of Patients with Tuberculosis Little Rock, Arkansas August 13 14, 2014 TB Case Presentation Andrea Cruz, MD, MPH August 14, 2014 Andrea Cruz, MD, MPH has the following disclosures to
2012 by American Society of Hematology
 2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
Lymphoma co existing with Tuberculosis granulomatous
 Available online at www.worldscientificnews.com WSN 90 (2017) 265-270 EISSN 2392-2192 SHORT COMMUNICATION Lymphoma co existing with Tuberculosis granulomatous Madeeha Subhan 1, *, Waleed Sadiq 2 1 Ayub
Available online at www.worldscientificnews.com WSN 90 (2017) 265-270 EISSN 2392-2192 SHORT COMMUNICATION Lymphoma co existing with Tuberculosis granulomatous Madeeha Subhan 1, *, Waleed Sadiq 2 1 Ayub