The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
|
|
|
- Ronald Wright
- 5 years ago
- Views:
Transcription
1 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via at:
2 First Line Therapies for UC and Crohn s Disease Douglas C Wolf, MD
3 Ulcera've Coli's Crohn s disease Aminosalicyalates (ASA to mesalamine) Aminosalicyalates (?) oral therapy(diazo bond, ph, controlled release) topical rectal therapy( mesalamine suppository and enema) Cor'costeroids Cor'costeroid systemic-oral, IV ( prednisone) non-systemic-topical po./ rectal (budesonide MMX, Budesonide foam) Immunomodulators thiopurine(aza, 6MP) Mtx (?) Biologic AnM-cytokine: AnM-TNF(IFX, ADA, GOL) AnM-integrin(VEDO) I systemic-oral, IV (prednisone) non-systemic-topical po/ rectal budesonide EC, budesonide foam) Immunomodulators Thiopurine (AZA, 6MP) MTX Biologic AnM-TNF(CZP,IFX,ADA) AnM-integrin (VEDO)


4 Crohn s Disease Algorithm LOW RISK TERMINAL ILEUM+/- right colon COLON Sulfasalazine or Mesalamine NO Prednisone 4-6 weeks Response NO Budesonide Response yes yes yes (AZA/ 6 MP) or MTX Response yes +/- Maintenance Response NO +/- Maintenance yes NO Treat as high risk Maintenance ( AZA/6 MP) or MTX
5 Crohn s Disease Algorithm HIGH RISK Prednisone OR An9 TNF+/- ( AZA/6 MP) or MTX 4-6 weeks +/or Response no Response (AZA/ 6 MP) or MTX no yes no yes Response Maintenance ( AZA/6 MP) or MTX Maintenance anm TNF and (AZA/6MP) or MTX Dose escalate Switch AnM TNF Switch anm metabolite Natalizumab Clinical trial Surgery

6 Moderate-to-Severe Active UC Non-hospitalized Bressler B, Marshall JK, et al. Gastroenterology. 2015;148(5):
7 National Cooperative Crohn s Disease Study
8 Corticosteroids One of the most effecmve CD medicamons Always try to minimize use PotenMal side effects : Mood swings AsepMc necrosis InfecMon Cataracts Hypertension Weight gain Striae Diabetes mellitus Osteoporosis Cushingoid appearance Adrenal suppression(addisons if severe)
9 Antibiotics
10 Immunomodulators Rutgeerts P et al.rev Gastroenterol disord.2004;4(suppl 3):S3-S9) Korelitz BI,Present DH.NEJM.1995;333:
11

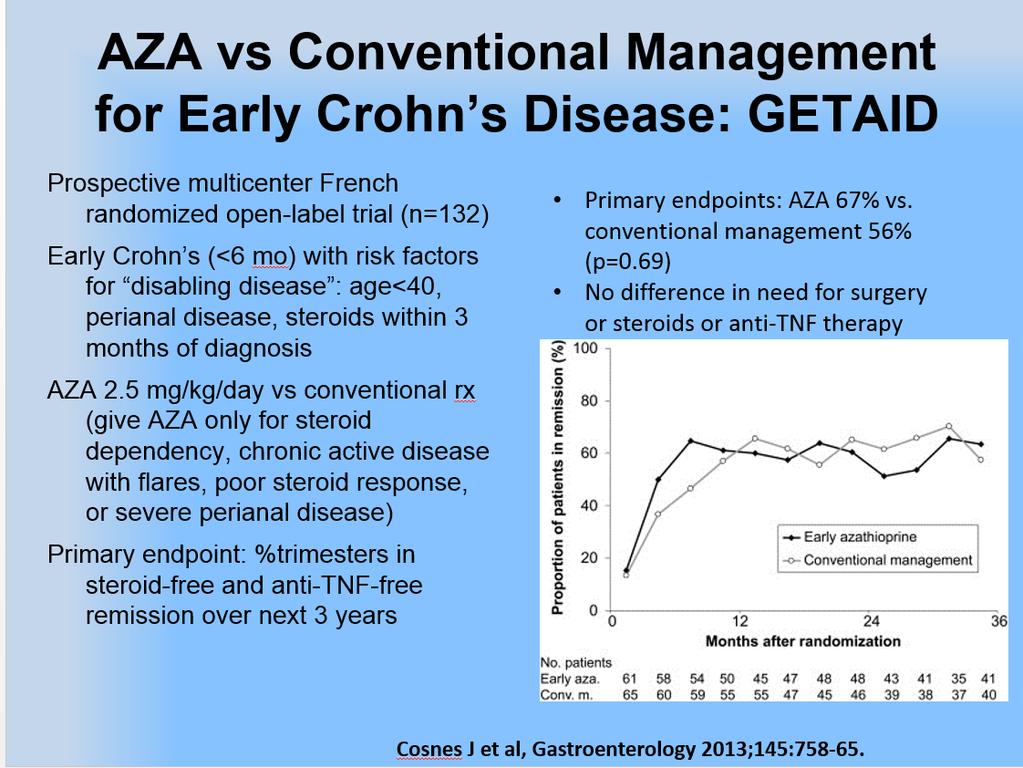
12 Early Crohn s Disease Therapy: Combined Immunosuppressive vs ConvenMonal
13 OpMmizing Thiopurine Therapy Thiopurine Nonresponder Groups Nonadherent Underdosing Thiopurine Resistant Thiopurine Refractory THIOPURINE METABOLITE MEASUREMENTS AND MANAGEMENT Metabolite Profile Low/absent 6-TGN Low/absent 6-MMP Low 6-TGN Low 6-MMP Low 6-TGN High 6-MMP High 6-TGN High 6-MMP Management Pa'ent educa'on Increase thiopurine dose Pa'ent educa'on Switch to another drug. Possibly add allopurinol (special monitoring)* Switch to another drug *WBC must be >4.5x10 4 Allopurinol dose is 100mg and thiopurine dose is reduced 25-50% from the original dose Chevaux J-P, et al. Inflamm Bowel Dis. 2011;17(6):
14 Steroid Sparing and Toxicity of MTX in AcMve CD
15 Indication for Biologic Therapy
16 Indication for Biologic therapy
17 Biologic Induction and Maintenance Dosing
18 Optimizing biologic therapy InducMon- Give a loading dose Give in combinamon with a immunomodulator (6MP,AZA, MTX) OpMmize maintenance dosing Avoid episodic dosing TherapeuMc drug monitoring (TDM)
:A-147.")
19 CHARM: Remission by Disease Duration with Adalimumab at Week 26 Placebo All adalimumab * % Remission ** 14 0 <2 years N = 23, N = 39 <2-5 years N = 36, N = 57 5 years N = 111, N = 233 *P =.002, **P <.001, P =.014, P =.001 all vs placebo Schreiber S, et al. Gastroenterology 2007;132(4 Suppl 2):A-147. Abstract 985.
20 SONIC: CorMcosteroid-Free Clinical Remission at Week 26 Infliximab Naïve to IMM/anM-TNF/Short DuraMon CD Propor'on of Pa'ents (%) P <.001 P =.009 P = /170 75/169 96/169 AZA + placebo IFX + placebo IFX+ AZA Colombel JF, Sandborn WJ, et al. N Engl J Med. 2010; 362:
21 PRECISE 2: Response and Remission by Disease DuraMon with Certolizumab Pegol at Week 26 Response Placebo response Remission Placebo remission PRECiSE trial (certolizumab) <1 year N = 19, 35, 19, 35 1-<2 years N = 20, 22, 20, 22 2-<5 years N = 45, 55, 45, 55 5 years N = 131, 98, 131, 98 Sandborn WJ, et al. Am J Gastroenterol. 2006;101:S Abstract Schreiber S, et al. N Engl J Med. 2007;357(3):
22 Different Release Sites and Release Mechanisms of 5-ASAs Stomach ph 6 Small Intes'ne ph 7 Large Intes'ne Mesalamine in microgranules Mesalamine w/ Eudragit-S Mesalamine MMX Granulated Mesalamine with Delayed and Extended Release Azo bond Oral and Rectal prepara'ons
23 Dose Response at Week 6: Delayed-Release Mesalamine (5-ASA) Patients With Treatment Success at Week 6 (%) P=NS 51 ASCEND I P= Mild to moderate UC (N = 286) Moderate UC (N = 180) P=NS 56 P= g/day 4.8 g/day Delayed-Release Mesalamine 72 Hanauer SB, et al. Can J Gastroenterol. 2007;21(12):
24 MMX Mesalamine in Mild to Moderate UC Patients in Clinical and Endoscopic Remission at Week 8 (%) Placebo P=.01* * P-values represent active treatment vs placebo 1. Kamm MA et al. Gastroenterology. 2007;132(1): Lichtenstein GR, et al. Clin Gastroenterol Hepatol. 2007;5(1): P<.001* 34 P=.007* 41 Kamm, et al 1 Lichtenstein, et al 2 P=.009* g/day 4.8 g/day MMX Mesalamine Dose
25 Budesonide MMX in UC Induces Remission
26 Budesonide Foam is EffecMve for Mild and Moderate UlceraMve ProcMMs and ProctosigmoidiMs
 30 25 Mayo score 4.0 4.")

27 METEOR: Methotrexate vs Placebo in Steroid-dependent UC Week 16: Primary Endpoint Week 16: Secondary Endpoints Baseline Characteris'cs Prednisone equiv. dose (mg/d) Mayo score Mayo Endoscopy score 1 1 Carbonnel F, et al. European Crohn s and ColiMs OrganisaMon, Inflammatory Bowel Diseases. Abstract OP023. February 21, clinicaltrials.gov/ct2/show/study/nct
28 Infliximab in Ulcerative Colitis: Clinical Remission* Percent of Patients ACT Percent of Patients ACT P<0.001 P< Weeks 30 Weeks 0 8 Weeks 30 Weeks Placebo infusions 5 mg/kg infliximab 10 mg/kg infliximab *Clinical remission defined as Mayo score of 2 points, with no individual subscore >1. PaMents with baseline medicamon were conmnued on stable doses. Rutgeerts P, Sandborn WJ, Feagan BG, et al. N Engl J Med. 2005;353:
 60 40 * 40 50 55 37 20 22 24 0 Steroid-free remission Response Mucosal Healing *P<.05 Panaccione R, et al. Gastroentreology. 2014;146(2):392-400.")
29 CombinaMon Therapy with Infliximab and Azathioprine Works Beqer than Either Alone in UC 100 IFX+AZA (n=78) IFX (n=77) AZA (n=66) PaMents (%) * Steroid-free remission Response Mucosal Healing *P<.05 Panaccione R, et al. Gastroentreology. 2014;146(2):
30 Accelerated Infliximab Dosing in UC RetrospecMve analysis 50 hospitalized severe acute UC paments 35 received standard IFX 0,2,6 42 days 15 received 3 doses: median - 24 days Standard inducmon:14/35=40% colectomy Accelerated inducmon:1/15=6.7% colectomy Gibson, et al. CGH. 2015; 13:

31 Fecal Infliximab Loss Brandise JF, et al. Gastroenterology Apr 24 [Epub ahead of print].
32 No Unanimity Regarding IFX Rescue Dosing for Severe UC Herfarth HH, et al. Clin Gastroenterol Hepatol. 2015;13(2):336-8.
33 Vedolizumab in UC Week 6 and 52 PaMents (%) Placebo (n=149) [VALUE] % Week 6 Vedolizumab 300 mg (n=225) P<0.001 [VALUE] % Clinical Response: Week 6 Primary Endpoint Feagan B, et al. NEJM.2013;369: PaMents (%) PaMents (%) Placebo (n=126) Vedolizumab 300 mg q8weeks (n=122) [VALUE] % P=0.008 [VALUE] % Clinical remission at both Weeks 6 and 52 Secondary Endpoint Placebo (n=126) Vedolizumab 300 mg q8weeks (n=122) [VALUE] % P<0.001 [VALUE] % Clinical response at both Weeks 6 and 52 Secondary Endpoint
34 What Is Our Treatment Target? Clinical - asymptomamc Biologic - normal labs, biomarkers Endoscopic - mucosal healing Histologic - deep remission Few of our paments are able to achieve it Cost Convenience Efficacy Side effects
35 What About Safety? Mesalamine rare issues, e.g. renal Immunomodulators Lymphoma, InfecMon Cyclosporine InfecMon AnM-TNF: Monotherapy vs. Dual InfecMon, Malignancy, Lymphoma (HSTL) Vedolizumab: Monotherapy vs. Dual InfecMon, Lymphoma (dual)
36 Conclusion ExisMng strategies are frequently ineffecmve at long term disease control PrognosMc factors are important to determine approach to therapy Careful disease and TherapeuMc Drug Monitoring improve outcomes Need for new agents in UC and CD
September 12, 2015 Millie D. Long MD, MPH, FACG
 Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
Update on Biologic Therapy in 2015 September 12, 2015 Millie D. Long MD, MPH, FACG Assistant Professor of Medicine Inflammatory Bowel Disease Center University of North Carolina-Chapel Hill Outline Crohn
IBD Updates. Themes in IBD IBD management journey. New tools for therapeutic monitoring. First-line treatment in IBD
 IBD Updates Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Themes in IBD 213 First-line treatment in IBD New tools for therapeutic monitoring Biologic therapy for CD and
IBD Updates Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Themes in IBD 213 First-line treatment in IBD New tools for therapeutic monitoring Biologic therapy for CD and
How to Optimize Induction and Maintenance Responses: Definitions and Dosing Advances in Inflammatory Bowel Disease December 6, 2009
 How to Optimize Induction and Maintenance Responses: Definitions and Dosing 2009 Advances in Inflammatory Bowel Disease December 6, 2009 Fernando Velayos MD MPH University of California, San Francisco
How to Optimize Induction and Maintenance Responses: Definitions and Dosing 2009 Advances in Inflammatory Bowel Disease December 6, 2009 Fernando Velayos MD MPH University of California, San Francisco
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Associate Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD
 Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
Efficacy and Safety of Treatment for Pediatric IBD Andrew B. Grossman MD Co-Director, Center for Pediatric Inflammatory Bowel Disease Assistant Professor of Clinical Pediatrics Division of Gastroenterology,
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease. David A. Schwartz, MD
 An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
An Update on the Biologic Treatment for Patients with Inflammatory Bowel Disease David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University
Mono or Combination Therapy with. Individualized Approach
 Mono Combination Therapy with Biologics i in IBD: Developing an Individualized Approach David T. Rubin, MD, FACG Co-Direct, Inflammaty Bowel Disease Center Fellowship Program Direct University of Chicago
Mono Combination Therapy with Biologics i in IBD: Developing an Individualized Approach David T. Rubin, MD, FACG Co-Direct, Inflammaty Bowel Disease Center Fellowship Program Direct University of Chicago
Biologic Therapy for Inflammatory. Is Top-Down Too Top-Heavy? S. Devi Rampertab, MD, FACG, AGAF Associate Professor of Medicine University of Florida
 Biologic Therapy for Inflammatory Bowel Disease: Is Top-Down Too Top-Heavy? S. Devi Rampertab, MD, FACG, AGAF Associate Professor of Medicine University of Florida Learning Objectives Evaluate evidence
Biologic Therapy for Inflammatory Bowel Disease: Is Top-Down Too Top-Heavy? S. Devi Rampertab, MD, FACG, AGAF Associate Professor of Medicine University of Florida Learning Objectives Evaluate evidence
Biologics in IBD. Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College
 Biologics in IBD Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College Case 30 year old man diagnosed with ulcerative proctitis diagnosed in 2003 Had been maintained
Biologics in IBD Brian P. Bosworth, MD, NYSGEF Associate Professor of Medicine Weill Cornell Medical College Case 30 year old man diagnosed with ulcerative proctitis diagnosed in 2003 Had been maintained
Treatment Goals. Current Therapeutic Pyramids Crohn s Disease Ulcerative Colitis 11/14/10
 Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Current Management of IBD: From Conventional Agents to Biologics Stephen B. Hanauer, M.D. University of Chicago Treatment Goals Induce and maintain response/ remission Prevent complications Improve quality
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease
 Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Azathioprine for Induction and Maintenance of Remission in Crohn s Disease William J. Sandborn, MD Chief, Division of Gastroenterology Director, UCSD IBD Center Objectives Azathioprine as induction and
Positioning New Therapies
 Positioning New Therapies Stephen Hanauer, MD Professor of Medicine Medical Director, Digestive Disease Center Northwestern Medicine Chicago, Illinois Speaker Disclosure Stephen Hanauer, MD has disclosed
Positioning New Therapies Stephen Hanauer, MD Professor of Medicine Medical Director, Digestive Disease Center Northwestern Medicine Chicago, Illinois Speaker Disclosure Stephen Hanauer, MD has disclosed
Indications for use of Infliximab
 Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
Indications for use of Infliximab Moscow, June 10 th 2006 Prof. Dr. Dr. Gerhard Rogler Klinik und Poliklinik für Innere Medizin I Universität Regensburg Case report 1989: Diagnosis of Crohn s disease of
CCFA. Crohns Disease vs UC: What is the best treatment for me? November
 CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
CCFA Crohns Disease vs UC: What is the best treatment for me? November 8 2009 Ellen J. Scherl,, MD, FACP,AGAF Roberts Inflammatory Bowel Disease Center Weill Medical College Cornell University New York
Update on Biologics in Ulcerative Colitis. Scott Plevy, MD University of North Carolina Chapel Hill, NC
 Update on Biologics in Ulcerative Colitis Scott Plevy, MD University of North Carolina Chapel Hill, NC Objectives Discuss the latest advances in the pharmacologic management of ulcerative colitis Describe
Update on Biologics in Ulcerative Colitis Scott Plevy, MD University of North Carolina Chapel Hill, NC Objectives Discuss the latest advances in the pharmacologic management of ulcerative colitis Describe
Medical Therapy for Pediatric IBD: Efficacy and Safety
 Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
Medical Therapy for Pediatric IBD: Efficacy and Safety Betsy Maxwell, MD Assistant Professor of Clinical Pediatrics Division of Gastroenterology, Hepatology, and Nutrition Pediatric IBD: Defining Remission
IBD Understanding Your Medications. Thomas V. Aguirre, MD Santa Barbara GI Consultants
 IBD Understanding Your Medications Thomas V. Aguirre, MD Santa Barbara GI Consultants IBD Understanding Your Medications (& Your Doctor) Thomas V. Aguirre, MD Santa Barbara GI Consultants Disclosure I
IBD Understanding Your Medications Thomas V. Aguirre, MD Santa Barbara GI Consultants IBD Understanding Your Medications (& Your Doctor) Thomas V. Aguirre, MD Santa Barbara GI Consultants Disclosure I
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease
 Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
Initiation of Maintenance Treatment in Moderate to Severe New Onset Crohn s Disease The Case for Starting with Anti-TNFα Agents Maria Oliva-Hemker, M.D. Chief, Division of Pediatric Gastroenterology &
Beyond Anti TNFs: positioning of other biologics for Crohn s disease. Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center
 Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Beyond Anti TNFs: positioning of other biologics for Crohn s disease Christina Ha, MD Cedars Sinai Inflammatory Bowel Disease Center Objectives: To define high and low risk patient and disease features
Common Questions in Crohn s Disease Therapy. Case
 Common Questions in Crohn s Disease Therapy Jean-Paul Achkar, MD, FACG Kenneth Rainin Chair for IBD Research Cleveland Clinic Case 23 yo male with 1 year history of diarrhea, abdominal pain and 15 pound
Common Questions in Crohn s Disease Therapy Jean-Paul Achkar, MD, FACG Kenneth Rainin Chair for IBD Research Cleveland Clinic Case 23 yo male with 1 year history of diarrhea, abdominal pain and 15 pound
Crohn's Disease. The What, When, and Why of Treatment
 Crohn's Disease The What, When, and Why of Treatment Gary R. Lichtenstein, MD, FACG Professor of Medicine Director, Inflammatory Bowel Disease Program University of Pennsylvania Philadelphia, PA In my
Crohn's Disease The What, When, and Why of Treatment Gary R. Lichtenstein, MD, FACG Professor of Medicine Director, Inflammatory Bowel Disease Program University of Pennsylvania Philadelphia, PA In my
COPYRIGHT. Inflammatory Bowel Disease What Every Clinician Needs to Know. Adam S. Cheifetz, MD. Director, Center for Inflammatory Bowel Disease
 Inflammatory Bowel Disease What Every Clinician Needs to Know Adam S. Cheifetz, MD Director, Center for Inflammatory Bowel Disease Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard
Inflammatory Bowel Disease What Every Clinician Needs to Know Adam S. Cheifetz, MD Director, Center for Inflammatory Bowel Disease Beth Israel Deaconess Medical Center Associate Professor of Medicine Harvard
Medical Management of Inflammatory Bowel Disease
 Medical Management of Inflammatory Bowel Disease John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University John K. Marshall: Conflicts of Interest Speaker: AbbVie, Allergan, Ferring,
Medical Management of Inflammatory Bowel Disease John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University John K. Marshall: Conflicts of Interest Speaker: AbbVie, Allergan, Ferring,
Moderately to severely active ulcerative colitis
 Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients
Adalimumab in the Treatment of Moderate-to-Severe Ulcerative Colitis: ULTRA 2 Trial Results Sandborn WJ, van Assche G, Reinisch W, et al. Adalimumab induces and maintains clinical remission in patients
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy
 Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
Position of Biologics in IBD Circa 2006: Top Down vs. Step Up Therapy Stephen B. Hanauer, MD University of Chicago Potential Conflicts: Centocor/Schering, Abbott, UCB, Elan, Berlex, PDL Goals of Treatment
Severe IBD: What to Do When Anti- TNFs Don t Work?
 Severe IBD: What to Do When Anti- TNFs Don t Work? David T. Rubin, MD, FACG Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Interim Chief, Section of Gastroenterology, Hepatology and
Severe IBD: What to Do When Anti- TNFs Don t Work? David T. Rubin, MD, FACG Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Interim Chief, Section of Gastroenterology, Hepatology and
Crohn's Disease. The What, When, and Why of Treatment
 Crohn's Disease The What, When, and Why of Treatment Brian Feagan, MD, FACG Professor of Medicine and Epidemiology and Biostatistics Director, Robarts Clinical Trials Robarts Research Institute University
Crohn's Disease The What, When, and Why of Treatment Brian Feagan, MD, FACG Professor of Medicine and Epidemiology and Biostatistics Director, Robarts Clinical Trials Robarts Research Institute University
John F. Valentine, MD Inflammatory Bowel Disease Program University of Utah
 John F. Valentine, MD Inflammatory Bowel Disease Program University of Utah Hawaii 1/20/2017 DISCLOSURES Research Support: NIH, Pfizer, Celgene, AbbVie, Roche/Genentech, Takeda, CCFA OBJECTIVES Review
John F. Valentine, MD Inflammatory Bowel Disease Program University of Utah Hawaii 1/20/2017 DISCLOSURES Research Support: NIH, Pfizer, Celgene, AbbVie, Roche/Genentech, Takeda, CCFA OBJECTIVES Review
Mucosal Healing in Crohn s Disease. Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium
 Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Mucosal Healing in Crohn s Disease Geert D Haens MD, PhD University Hospital Gasthuisberg University of Leuven Leuven, Belgium Mucosal Lesions in CD: General Features CD can affect the entire GI tract
Disclosures. What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists
 What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
What Do I Do When Anti-TNF Therapy Is Not Working Anymore? Fadi Hamid, M.D. Saint Luke s GI Specialists Disclosures No financial relationships to disclose. 1 Learning Objectives Case 24M with ileocolonic
How do I choose amongst medicines for inflammatory bowel disease. Maria T. Abreu, MD
 How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
How do I choose amongst medicines for inflammatory bowel disease Maria T. Abreu, MD Overview of IBD Pathogenesis Bacterial Products Moderately Acutely Inflamed Chronic Inflammation = IBD Normal Gut Mildly
5-ASA Therapy, Steroids and Antibiotics in Inflammatory Bowel Disease
 5-ASA Therapy, Steroids and Antibiotics in Inflammatory Bowel Disease David T. Rubin, MD Associate Professor of Medicine Co-Director, Inflammatory Bowel Disease Center University it of Chicago Medical
5-ASA Therapy, Steroids and Antibiotics in Inflammatory Bowel Disease David T. Rubin, MD Associate Professor of Medicine Co-Director, Inflammatory Bowel Disease Center University it of Chicago Medical
Emerging g therapies for IBD: A practical approach to positioning. Sequential Therapies for IBD
 Emerging g therapies for IBD: A practical approach to positioning Stephen B. Hanauer, MD Sequential Therapies for IBD Disease Severity at Presentation Severe Anti-TNF +/IS Cyclosporine (UC) Colectomy (UC)
Emerging g therapies for IBD: A practical approach to positioning Stephen B. Hanauer, MD Sequential Therapies for IBD Disease Severity at Presentation Severe Anti-TNF +/IS Cyclosporine (UC) Colectomy (UC)
OPTIMAL USE OF IMMUNOMODULATORS AND BIOLOGICS Edward V. Loftus, Jr., MD, FACG
 1C: Advances in Inflammatory Bowel Disease OPTIMAL USE OF IMMUNOMODULATORS AND BIOLOGICS Edward V. Loftus, Jr., MD, FACG narrow interpretation of this presentation topic would A be a discussion of dosing
1C: Advances in Inflammatory Bowel Disease OPTIMAL USE OF IMMUNOMODULATORS AND BIOLOGICS Edward V. Loftus, Jr., MD, FACG narrow interpretation of this presentation topic would A be a discussion of dosing
Dr. Elmer Schabel, MD. Bundesinstitut für Arzneimittel und Medizinprodukte, Bonn, Germany (No conflicts of interest)
") EMA workshop on the development of new medicinal products for the treatment of ulcerative colitis and Crohn s disease Overview of authorised medicines for IBD in Europe - previous regulatory positions
EMA workshop on the development of new medicinal products for the treatment of ulcerative colitis and Crohn s disease Overview of authorised medicines for IBD in Europe - previous regulatory positions
Immunogenicity of Biologic Agents and How to Prevent Sensitization
 Immunogenicity of Biologic Agents and How to Prevent Sensitization William J. Sandborn, MD Professor and Chief, Division of Gastroenterology Director, UCSD IBD Center La Jolla, California, USA Learning
Immunogenicity of Biologic Agents and How to Prevent Sensitization William J. Sandborn, MD Professor and Chief, Division of Gastroenterology Director, UCSD IBD Center La Jolla, California, USA Learning
Anne Griffiths MD, FRCPC. SickKids Hospital, University of Toronto. Buenos Aires, August 16, 2014
 Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
Management and Medical Therapies for Crohn disease: strategies to enhance mucosal healing Anne Griffiths MD, FRCPC SickKids Hospital, University of Toronto Buenos Aires, August 16, 2014 New onset Crohn
Agenda. Predictive markers in IBD. Management of ulcerative colitis. Management of Crohn s disease
 Agenda Predictive markers in IBD Management of ulcerative colitis Management of Crohn s disease 2 Patients With UC (%) Distribution of UC Disease Severity at Presentation 1 Fulminant disease (9%) 8 6 4
Agenda Predictive markers in IBD Management of ulcerative colitis Management of Crohn s disease 2 Patients With UC (%) Distribution of UC Disease Severity at Presentation 1 Fulminant disease (9%) 8 6 4
Latest Meds Approved for IBD: What are they and how do they work?
 Latest Meds Approved for IBD: What are they and how do they work? JAMES LORD, MD PHD BENAROYA RESEARCH INSTITUTE AT VIRGINIA MASON MEDICAL CENTER SEPT 30, 2018 Brief history of IBD Dr. Burrill Crohn JAMA
Latest Meds Approved for IBD: What are they and how do they work? JAMES LORD, MD PHD BENAROYA RESEARCH INSTITUTE AT VIRGINIA MASON MEDICAL CENTER SEPT 30, 2018 Brief history of IBD Dr. Burrill Crohn JAMA
Therapy for Inflammatory Bowel Disease
 Therapy for Inflammatory Bowel Disease Jonathan P. Terdiman, MD Professor of Clinical Medicine Clinical Director, Center for Colitis and Crohn s Disease University of California San Francisco, CA UC: Current
Therapy for Inflammatory Bowel Disease Jonathan P. Terdiman, MD Professor of Clinical Medicine Clinical Director, Center for Colitis and Crohn s Disease University of California San Francisco, CA UC: Current
Biologics in 2016: How Do We Select the Most Appropriate Agent? Gary R. Lichtenstein, MD, FACG University of PA School of Medicine Philadelphia, PA
 Biologics in 2016: How Do We Select the Most Appropriate Agent? Gary R. Lichtenstein, MD, FACG University of PA School of Medicine Philadelphia, PA Overview Indications and Drug Selection Contraindications
Biologics in 2016: How Do We Select the Most Appropriate Agent? Gary R. Lichtenstein, MD, FACG University of PA School of Medicine Philadelphia, PA Overview Indications and Drug Selection Contraindications
Recent Advances in the Management of Refractory IBD
 Recent Advances in the Management of Refractory IBD Raina Shivashankar, M.D. Assistant Professor of Medicine Division of Gastroenterology and Hepatology Thomas Jefferson University Philadelphia, PA Outline
Recent Advances in the Management of Refractory IBD Raina Shivashankar, M.D. Assistant Professor of Medicine Division of Gastroenterology and Hepatology Thomas Jefferson University Philadelphia, PA Outline
Optimal Use of Immunomodulators and Biologics
 3/17/214 Optimal Use of Immunomodulators and Biologics Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic Rochester, Minnesota, U.S.A. Loftus Disclosures
3/17/214 Optimal Use of Immunomodulators and Biologics Edward V. Loftus, Jr., M.D. Professor of Medicine Division of Gastroenterology and Hepatology Mayo Clinic Rochester, Minnesota, U.S.A. Loftus Disclosures
CROHN'S DISEASE/ULCERATIVE COLITIS TREATMENT ALGORITHM
 CROHN'S DISEASE/ULCERATIVE COLITIS TREATMENT ALGORITHM Crohn's Disease Ulcerative Colitis Steroids x 2 No prior AZA/6-MP Biologic Agent AZA/6-MP STEP-UP MANAGEMENT APPROACH Advantages Patients attain remission
CROHN'S DISEASE/ULCERATIVE COLITIS TREATMENT ALGORITHM Crohn's Disease Ulcerative Colitis Steroids x 2 No prior AZA/6-MP Biologic Agent AZA/6-MP STEP-UP MANAGEMENT APPROACH Advantages Patients attain remission
New treatment options in UC. Rob Bryant IBD Consultant Royal Adelaide Hospital
 New treatment options in UC Rob Bryant IBD Consultant Royal Adelaide Hospital Talk Outline 1. Raising expectations 2. Optimising UC therapy 3. Clinical trials 4. What s new on the PBS? 5. Questions 1.
New treatment options in UC Rob Bryant IBD Consultant Royal Adelaide Hospital Talk Outline 1. Raising expectations 2. Optimising UC therapy 3. Clinical trials 4. What s new on the PBS? 5. Questions 1.
Personalized Medicine in IBD
 Personalized Medicine in IBD Anita Afzali MD, MPH Assistant Professor of Medicine Director, Inflammatory Bowel Diseases Program University of Washington Harborview Medical Center CCFA April 2 nd, 2016
Personalized Medicine in IBD Anita Afzali MD, MPH Assistant Professor of Medicine Director, Inflammatory Bowel Diseases Program University of Washington Harborview Medical Center CCFA April 2 nd, 2016
Latest Treatment Updates for Crohn s Disease: Tailoring Therapy David G. Binion, M.D.
 Latest Treatment Updates for Crohn s Disease: Tailoring Therapy David G. Binion, M.D. Co-Director, IBD Center Director, Nutrition Support Service UPMC Presbyterian Hospital Division of Gastroenterology,
Latest Treatment Updates for Crohn s Disease: Tailoring Therapy David G. Binion, M.D. Co-Director, IBD Center Director, Nutrition Support Service UPMC Presbyterian Hospital Division of Gastroenterology,
Emerging Therapies in IBD 2006
 Overview Emerging Therapies in IBD 26 David T. Rubin, MD Assistant Professor of Medicine Inflammatory Bowel Disease Center University of Chicago Describe the unmet needs of therapy in IBD Emerging biologic
Overview Emerging Therapies in IBD 26 David T. Rubin, MD Assistant Professor of Medicine Inflammatory Bowel Disease Center University of Chicago Describe the unmet needs of therapy in IBD Emerging biologic
Selection and use of the non-anti- TNF biological therapies: Who? When? How?
 Selection and use of the non-anti- TNF biological therapies: Who? When? How? Asher Kornbluth, MD Clinical Professor of Medicine The Henry D. Janowitz Division of Gastroenterology The Icahn School of Medicine
Selection and use of the non-anti- TNF biological therapies: Who? When? How? Asher Kornbluth, MD Clinical Professor of Medicine The Henry D. Janowitz Division of Gastroenterology The Icahn School of Medicine
Drug Level Monitoring in IBD. Objectives
 Drug Level Monitoring in IBD Corey A. Siegel, MD, MS Director, Dartmouth-Hitchcock IBD Center Associate Professor of Medicine, Geisel School of Medicine at Dartmouth Objectives Review non-biologic drug
Drug Level Monitoring in IBD Corey A. Siegel, MD, MS Director, Dartmouth-Hitchcock IBD Center Associate Professor of Medicine, Geisel School of Medicine at Dartmouth Objectives Review non-biologic drug
Join the conversation at #GIFORUMCCFA
 1 Join the conversation at #GIFORUMCCFA 2 Disclosures In accordance with the ACCME Standards for Commercial Support of CME, the speakers for this course have been asked to disclose to participants the
1 Join the conversation at #GIFORUMCCFA 2 Disclosures In accordance with the ACCME Standards for Commercial Support of CME, the speakers for this course have been asked to disclose to participants the
Ulcerative Colitis: Refining our Management and Incorporating Newer Concepts
 Ulcerative Colitis: Refining our Management and Incorporating Newer Concepts Asher Kornbluth, MD Clinical Professor of Medicine The Henry D. Janowitz The Mt. Sinai School of Medicine Refining our Management
Ulcerative Colitis: Refining our Management and Incorporating Newer Concepts Asher Kornbluth, MD Clinical Professor of Medicine The Henry D. Janowitz The Mt. Sinai School of Medicine Refining our Management
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 3 October 2012
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 3 October 2012 REMICADE 100 mg, powder for concentrate for solution for infusion B/1 vial (CIP code: 562 070-1) Applicant:
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 3 October 2012 REMICADE 100 mg, powder for concentrate for solution for infusion B/1 vial (CIP code: 562 070-1) Applicant:
Selby Inflamm Bowel Dis. 2008:14:
 Medical Management of Inflammatory Bowel Disease Freddy Caldera D.O. Assistant Professor Division of Gastroenterology Objectives Discuss Crohn s disease and Ulcerative Colitis Discuss Medications for Inflammatory
Medical Management of Inflammatory Bowel Disease Freddy Caldera D.O. Assistant Professor Division of Gastroenterology Objectives Discuss Crohn s disease and Ulcerative Colitis Discuss Medications for Inflammatory
Ali Keshavarzian MD Rush University Medical Center
 Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Treatment: Step Up or Top Down? Ali Keshavarzian MD Rush University Medical Center Questions What medication should IBD be treated with? Can we predict which patients with IBD are high risk? Is starting
Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball
 Looking for the Crystal Ball") Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball Siddharth Singh, MD, MS Assistant Professor of Medicine Division of Gastroenterology Division of Biomedical
Choosing and Positioning Biologic Therapy for Crohn s Disease: (Still) Looking for the Crystal Ball Siddharth Singh, MD, MS Assistant Professor of Medicine Division of Gastroenterology Division of Biomedical
Positioning Biologics in Ulcerative Colitis
 Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
Positioning Biologics in Ulcerative Colitis Bruce E. Sands, MD, MS Acting Chief, Gastrointestinal Unit Massachusetts General Hospital Associate Professor of Medicine Harvard Medical School Sequential Therapies
Latest Treatment Updates for Ulcerative Colitis: Evolving Treatment Goals
 Latest Treatment Updates for Ulcerative Colitis: Evolving Treatment Goals Stephen Hanauer, MD Professor of Medicine Medical Director, Digestive Disease Center Northwestern Medicine Chicago, Illinois Speaker
Latest Treatment Updates for Ulcerative Colitis: Evolving Treatment Goals Stephen Hanauer, MD Professor of Medicine Medical Director, Digestive Disease Center Northwestern Medicine Chicago, Illinois Speaker
Definitions. Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency)
") CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
CROHN S DISEASE Definitions Clinical remission: Resolution of symptoms (stool frequency 3/day, no bleeding and no urgency) Recurrence: The reappearance of lesions after surgical resection Endoscopic remission:
Management of Moderate to Severe Ulcerative Colitis
 Management of Moderate to Severe Ulcerative Colitis Neilanjan Nandi, MD Assistant Professor of Medicine Associate Program Director Division of Gastroenterology Drexel University College of Medicine Hahnemann
Management of Moderate to Severe Ulcerative Colitis Neilanjan Nandi, MD Assistant Professor of Medicine Associate Program Director Division of Gastroenterology Drexel University College of Medicine Hahnemann
Inflammatory Bowel Disease Drug Therapy 2016
 Inflammatory Bowel Disease Drug Therapy 206 David T. Rubin, MD, FACG Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology and Nutrition Objectives Outline the goals of
Inflammatory Bowel Disease Drug Therapy 206 David T. Rubin, MD, FACG Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology and Nutrition Objectives Outline the goals of
How to use infliximab?
 How to use infliximab? Séverine Vermeire, MD, PhD Division of Gastroenterology University Hospital Gasthuisberg Leuven The how to use infliximab rules Before starting IFX: try optimizing chances for response!
How to use infliximab? Séverine Vermeire, MD, PhD Division of Gastroenterology University Hospital Gasthuisberg Leuven The how to use infliximab rules Before starting IFX: try optimizing chances for response!
The Refractory Crohn s Disease
 The Refractory Crohn s Disease Patient David T. Rubin, MD, FACG Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Interim Chief, Section of Gastroenterology, Hepatology and Nutrition
The Refractory Crohn s Disease Patient David T. Rubin, MD, FACG Professor of Medicine Co-Director, Inflammatory Bowel Disease Center Interim Chief, Section of Gastroenterology, Hepatology and Nutrition
WHY HAVE WE NOT FINALLY FIGURED OUT COMBINATION THERAPY?
 WHY HAVE WE NOT FINALLY FIGURED OUT COMBINATION THERAPY? Siew Ng, Professor MBBS, FRCP, (Lon, Edin), PhD (Lond), AGAF, FHKCP, FHKAM (medicine) Department of Medicine and Therapeutics Chinese University
WHY HAVE WE NOT FINALLY FIGURED OUT COMBINATION THERAPY? Siew Ng, Professor MBBS, FRCP, (Lon, Edin), PhD (Lond), AGAF, FHKCP, FHKAM (medicine) Department of Medicine and Therapeutics Chinese University
Crohn s
 Crohn s Disease David T. Rubin, MD, AGAF Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology, and Nutrition Co-Director, Digestive Diseases Center @IBDMD Disclosures
Crohn s Disease David T. Rubin, MD, AGAF Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology, and Nutrition Co-Director, Digestive Diseases Center @IBDMD Disclosures
Managing IBD: Lessons I Have Learned Over the Past. Farraye s Tips
 Managing IBD: Lessons I Have Learned Over the Past 25 Years Francis A. Farraye, MD, MSc Clinical Director Section of Gastroenterology Boston Medical Center Professor of Medicine Boston University School
Managing IBD: Lessons I Have Learned Over the Past 25 Years Francis A. Farraye, MD, MSc Clinical Director Section of Gastroenterology Boston Medical Center Professor of Medicine Boston University School
To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture,
 To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture, click Options in the Message Bar, and then click Enable
To help protect your privacy, PowerPoint prevented this external picture from being automatically downloaded. To download and display this picture, click Options in the Message Bar, and then click Enable
Management of Refractory Crohn s Disease
 Management of Refractory Crohn s Disease @IBDMD David T. Rubin, MD, FACG, FASGE Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology and Nutrition Disclosures Consultant
Management of Refractory Crohn s Disease @IBDMD David T. Rubin, MD, FACG, FASGE Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology and Nutrition Disclosures Consultant
Endpoints for Stopping Treatment in UC
 Endpoints for Stopping Treatment in UC Jana G. Hashash, MD Assistant Professor of Medicine Inflammatory Bowel Disease Center Division of Gastroenterology, Hepatology, and Nutrition University of Pittsburgh
Endpoints for Stopping Treatment in UC Jana G. Hashash, MD Assistant Professor of Medicine Inflammatory Bowel Disease Center Division of Gastroenterology, Hepatology, and Nutrition University of Pittsburgh
Ulcerative Colitis Therapy. Faculty Disclosure. Acknowledgements 28/11/2013. Amy Morse November 30/13
 Ulcerative Colitis Therapy Amy Morse November 30/13 GI for GP s Jasper AB Faculty Disclosure Faculty: Amy Morse Relationships with commercial interests: Grants/Research Support: Therapeutic Fellowship
Ulcerative Colitis Therapy Amy Morse November 30/13 GI for GP s Jasper AB Faculty Disclosure Faculty: Amy Morse Relationships with commercial interests: Grants/Research Support: Therapeutic Fellowship
Από τη θεωρία στη πράξη: Συζήτηση κλινικών περιστατικών. Κωνσταντίνος Κατσάνος Επίκουρος Καθηγητής Γαστρεντερολογίας Πανεπιστήμιο Ιωαννίνων
 Από τη θεωρία στη πράξη: Συζήτηση κλινικών περιστατικών Κωνσταντίνος Κατσάνος Επίκουρος Καθηγητής Γαστρεντερολογίας Πανεπιστήμιο Ιωαννίνων Conflict of interest By means of this, the speaker confirms that
Από τη θεωρία στη πράξη: Συζήτηση κλινικών περιστατικών Κωνσταντίνος Κατσάνος Επίκουρος Καθηγητής Γαστρεντερολογίας Πανεπιστήμιο Ιωαννίνων Conflict of interest By means of this, the speaker confirms that
DENOMINATOR: All patients aged 18 and older with a diagnosis of inflammatory bowel disease
 Measure #270: Inflammatory Bowel Disease (IBD): Preventive Care: Corticosteroid Sparing Therapy National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Measure #270: Inflammatory Bowel Disease (IBD): Preventive Care: Corticosteroid Sparing Therapy National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY
Treating to Achieve a Target and Disease Monitoring in 2015: State of the Art
 Treating to Achieve a Target and Disease Monitoring in 2015: State of the Art David T. Rubin, MD The Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology and Nutrition
Treating to Achieve a Target and Disease Monitoring in 2015: State of the Art David T. Rubin, MD The Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology and Nutrition
Ulcerative Colitis: State of the Art 2006
 Ulcerative Colitis: State of the Art David T. Rubin, MD Assistant Professor of Medicine Inflammatory Bowel Disease Center University of Chicago Improving Management of Ulcerative Colitis (UC) Better classification/diagnostic
Ulcerative Colitis: State of the Art David T. Rubin, MD Assistant Professor of Medicine Inflammatory Bowel Disease Center University of Chicago Improving Management of Ulcerative Colitis (UC) Better classification/diagnostic
Treatment of ulcerative colitis with adalimumab or infliximab: long-term follow-up of a single-centre cohort
 Alimentary Pharmacology and Therapeutics Treatment of ulcerative colitis with adalimumab or infliximab: long-term follow-up of a single-centre cohort N. Gies, K. I. Kroeker, K. Wong & R. N. Fedorak Division
Alimentary Pharmacology and Therapeutics Treatment of ulcerative colitis with adalimumab or infliximab: long-term follow-up of a single-centre cohort N. Gies, K. I. Kroeker, K. Wong & R. N. Fedorak Division
Progress in Inflammatory Bowel Disease
 Progress in Inflammatory Bowel Disease Gary R Lichtenstein, MD Director, Center for IBD University of Pennsylvania School of Medicine Hospital of the University of PA Philadelphia, PA Disclosure Research,
Progress in Inflammatory Bowel Disease Gary R Lichtenstein, MD Director, Center for IBD University of Pennsylvania School of Medicine Hospital of the University of PA Philadelphia, PA Disclosure Research,
Mild-moderate Ulcerative Colitis Sequential & Combined treatments need to be tested. Philippe Marteau, Paris, France
 Mild-moderate Ulcerative Colitis Sequential & Combined treatments need to be tested Philippe Marteau, Paris, France Sequential vs combined treatments When should one switch? Sequential vs combined treatments
Mild-moderate Ulcerative Colitis Sequential & Combined treatments need to be tested Philippe Marteau, Paris, France Sequential vs combined treatments When should one switch? Sequential vs combined treatments
Optimizing the effectiveness of anti-tnf therapy in paediatric IBD
 Optimizing the effectiveness of anti-tnf therapy in paediatric IBD Anne Griffiths MD, FRCPC Co-Lead, Inflammatory Bowel Disease Center Northbridge Chair in IBD Hospital for Sick Children, Professor of
Optimizing the effectiveness of anti-tnf therapy in paediatric IBD Anne Griffiths MD, FRCPC Co-Lead, Inflammatory Bowel Disease Center Northbridge Chair in IBD Hospital for Sick Children, Professor of
Mucosal healing: does it really matter?
 Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does it really matter? Professor Jean-Frédéric Colombel, New York, USA Oxford Inflammatory Bowel Disease MasterClass Mucosal healing: does
When can I stop taking my medications? Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida
 When can I stop taking my medications? Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Post-op low risk patient Uc de-escalation Discuss combo therapy Which one worked IBD
When can I stop taking my medications? Maria T. Abreu, MD University of Miami Miller School of Medicine Miami, Florida Post-op low risk patient Uc de-escalation Discuss combo therapy Which one worked IBD
Understanding Inflammatory Bowel Diseases (IBD):
:") Understanding Inflammatory Bowel Diseases (IBD): What Every Patient Needs to Know William H Holderman, MD Digestive Health Specialists Tacoma, WA Today s Objectives Define IBD, its potential causes and
Understanding Inflammatory Bowel Diseases (IBD): What Every Patient Needs to Know William H Holderman, MD Digestive Health Specialists Tacoma, WA Today s Objectives Define IBD, its potential causes and
Managing Complications of IBD and Its Therapies David T. Rubin, MD, AGAF
 Managing Complications of IBD and Its Therapies David T. Rubin, MD, AGAF Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology and Nutrition University of Chicago Medicine
Managing Complications of IBD and Its Therapies David T. Rubin, MD, AGAF Joseph B. Kirsner Professor of Medicine Chief, Section of Gastroenterology, Hepatology and Nutrition University of Chicago Medicine
Approaches to Inflammatory Bowel Disease
 2:15 3pm Best Approach to Inflammatory Bowel Disease SPEAKER Maria Abreu, MD Presenter Disclosure Information The following relationships exist related to this presentation: Maria Abreu, MD, receives consulting
2:15 3pm Best Approach to Inflammatory Bowel Disease SPEAKER Maria Abreu, MD Presenter Disclosure Information The following relationships exist related to this presentation: Maria Abreu, MD, receives consulting
Title: Author: Journal:
 IMPORTANT COPYRIGHT NOTICE: This electronic article is provided to you by courtesy of Ferring Pharmaceuticals. The document is provided for personal usage only. Further reproduction and/or distribution
IMPORTANT COPYRIGHT NOTICE: This electronic article is provided to you by courtesy of Ferring Pharmaceuticals. The document is provided for personal usage only. Further reproduction and/or distribution
Of Treatment For Inflammatory Bowel Diseases
 Balancing The Risks And Benefits Of Treatment For Inflammatory Bowel Diseases Corey A. Siegel, MD Assistant Professor of Medicine Dartmouth Medical School Director, Inflammatory Bowel Diseases Center Dartmouth-Hitchcock
Balancing The Risks And Benefits Of Treatment For Inflammatory Bowel Diseases Corey A. Siegel, MD Assistant Professor of Medicine Dartmouth Medical School Director, Inflammatory Bowel Diseases Center Dartmouth-Hitchcock
New Perspectives on the Diagnosis and Management of IBD. Disclosures
 New Perspectives on the Diagnosis and Management of IBD Joel R. Rosh, MD Director, Pediatric Gastroenterology Goryeb Children's Hospital/Atlantic Health Professor of Pediatrics Icahn School of Medicine
New Perspectives on the Diagnosis and Management of IBD Joel R. Rosh, MD Director, Pediatric Gastroenterology Goryeb Children's Hospital/Atlantic Health Professor of Pediatrics Icahn School of Medicine
Disease Management Strategies for Moderate to Severe IBD in Adults
 Disease Management Strategies for Moderate to Severe IBD in Adults Alyssa Parian, MD Assistant Professor of Medicine Johns Hopkins University April 21, 2016 Outline Overview of IBD Treatments (Benefits/Risks)
Disease Management Strategies for Moderate to Severe IBD in Adults Alyssa Parian, MD Assistant Professor of Medicine Johns Hopkins University April 21, 2016 Outline Overview of IBD Treatments (Benefits/Risks)
Optimizing Therapies for Severe Ulcerative Colitis October 19, 2014
 Optimizing Therapies for Severe Ulcerative Colitis October 19, 2014 Ellen J. Scherl, MD, FACP, FACG, AGAF, FASGE, NYSGEF Director Jill Roberts Center for Inflammatory Bowel Disease Jill Roberts IBD Research
Optimizing Therapies for Severe Ulcerative Colitis October 19, 2014 Ellen J. Scherl, MD, FACP, FACG, AGAF, FASGE, NYSGEF Director Jill Roberts Center for Inflammatory Bowel Disease Jill Roberts IBD Research
Withdrawal of drug therapy in patients with quiescent Crohn s disease
 Withdrawal of drug therapy in patients with quiescent Crohn s disease DR. JEAN-FRÉDÉRIC COLOMBEL DIRECTOR OF THE IBD CENTER, ICAHN SCHOOL OF MEDICINE AT MOUNT SINAI, NEW YORK, USA Withdrawal of drug therapy
Withdrawal of drug therapy in patients with quiescent Crohn s disease DR. JEAN-FRÉDÉRIC COLOMBEL DIRECTOR OF THE IBD CENTER, ICAHN SCHOOL OF MEDICINE AT MOUNT SINAI, NEW YORK, USA Withdrawal of drug therapy
Achieving Success in Ulcerative Colitis: the Role of Infliximab
 Achieving Success in Ulcerative Colitis: the Role of Infliximab Dr Gill Watermeyer IBD clinic Groote Schuur Hospital 17 th August 2012 Inflammatory Bowel Disease Crohn s disease and ulcerative colitis
Achieving Success in Ulcerative Colitis: the Role of Infliximab Dr Gill Watermeyer IBD clinic Groote Schuur Hospital 17 th August 2012 Inflammatory Bowel Disease Crohn s disease and ulcerative colitis
Personalized Medicine in IBD: Where Are We in 2013
 Personalized Medicine in IBD: Where Are We in 2013 David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University Medical Center What is Personalized
Personalized Medicine in IBD: Where Are We in 2013 David A. Schwartz, MD Director, Inflammatory Bowel Disease Center Associate Professor of Medicine Vanderbilt University Medical Center What is Personalized
ORIGINAL ARTICLE. Abstract. Introduction
 ORIGINAL ARTICLE Annals of Gastroenterology (2014) 27, 1-5 Effectiveness of adalimumab for ambulatory ulcerative colitis patients after failure of infliximab treatment: a first real-life experience in
ORIGINAL ARTICLE Annals of Gastroenterology (2014) 27, 1-5 Effectiveness of adalimumab for ambulatory ulcerative colitis patients after failure of infliximab treatment: a first real-life experience in
Biologic Therapy for Ulcerative Colitis in 2015
 5/6/215 Biologic Therapy for Ulcerative Colitis in 215 John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University Bressler B, Marshall JK, et al. Gastroenterology 215;148: 135-58
5/6/215 Biologic Therapy for Ulcerative Colitis in 215 John K. Marshall MD MSc FRCPC AGAF Division of Gastroenterology McMaster University Bressler B, Marshall JK, et al. Gastroenterology 215;148: 135-58
Submitted by xxxxxxxxxxxxxxxxx, xxxxxxxxx RCP and co-ordinated by xxxxxxxxxxxx, xxxxxxxxxxxxxxxxxxxxxxxxxxxxx, Royal Liverpool University Hospital.
 Royal College of Physicians statement on the appraisal of use of tumour necrosis factor alpha (TNF-α) inhibitors (adalimumab, certolizumab pegol and infliximab) and natalizumab for Crohn's disease Submitted
Royal College of Physicians statement on the appraisal of use of tumour necrosis factor alpha (TNF-α) inhibitors (adalimumab, certolizumab pegol and infliximab) and natalizumab for Crohn's disease Submitted
Best Practices in the Diagnosis and Treatment of Inflammatory Bowel Disease
 Best Practices in the Diagnosis and Treatment of Inflammatory Bowel Disease Mark Lazarev, MD Summary Inflammatory bowel disease (IBD) is a complex disease that is costly both in terms of medical costs
Best Practices in the Diagnosis and Treatment of Inflammatory Bowel Disease Mark Lazarev, MD Summary Inflammatory bowel disease (IBD) is a complex disease that is costly both in terms of medical costs
Edward V. Loftus, Jr., M.D.
 Edward V. Loftus, Jr., M.D. Professor of Medicine Faculty photo will be placed here loftus.edward@mayo.edu 2015 MFMER 3417200-1 Inflammatory Bowel Disease Therapy Edward V. Loftus, Jr., M.D. Gastroenterology
Edward V. Loftus, Jr., M.D. Professor of Medicine Faculty photo will be placed here loftus.edward@mayo.edu 2015 MFMER 3417200-1 Inflammatory Bowel Disease Therapy Edward V. Loftus, Jr., M.D. Gastroenterology
IBD Case Studies. David Rowbotham. Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology & Hepatology Auckland City Hospital
 IBD Case Studies David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology & Hepatology Auckland City Hospital Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust
IBD Case Studies David Rowbotham Clinical Director & Consultant Gastroenterologist Dept of Gastroenterology & Hepatology Auckland City Hospital Dr David Rowbotham The Leeds Teaching Hospitals NHS Trust
IBD in teenagers Biological and Transition
 IBD in teenagers Biological and Transition Dr Warren Hyer Consultant Paediatric Gastroenterologist St Mark s Hospital Chelsea and Westminster Hospital Conflict of Interest None to declare Fee for presentation
IBD in teenagers Biological and Transition Dr Warren Hyer Consultant Paediatric Gastroenterologist St Mark s Hospital Chelsea and Westminster Hospital Conflict of Interest None to declare Fee for presentation
Ulcerative colitis (UC) is a chronic inflammatory
 is a chronic inflammatory") Induction and Maintenance Therapy with Vedolizumab, a Novel Biologic Therapy for Ulcerative Colitis Feagan BG, Rutgeerts P, Sands BE, et al; GEMINI 1 Study Group. Vedolizumab as induction and maintenance
Induction and Maintenance Therapy with Vedolizumab, a Novel Biologic Therapy for Ulcerative Colitis Feagan BG, Rutgeerts P, Sands BE, et al; GEMINI 1 Study Group. Vedolizumab as induction and maintenance
Association Between Plasma Concentrations of Certolizumab Pegol and Endoscopic Outcomes of Patients With Crohn's Disease
 Association Between Plasma Concentrations of Certolizumab Pegol and Endoscopic Outcomes of Patients With Crohn's Disease Jean Frédéric Colombel, William J. Sandborn, Matthieu Allez, Jean Louis Dupas, Olivier
Association Between Plasma Concentrations of Certolizumab Pegol and Endoscopic Outcomes of Patients With Crohn's Disease Jean Frédéric Colombel, William J. Sandborn, Matthieu Allez, Jean Louis Dupas, Olivier