COPD A Breath of Fresh Air. Clare Hawkins, MD, FAAFP SW Regional Medical Officer Aspire Healthcare/Anthem
|
|
|
- Lester Quinn
- 5 years ago
- Views:
Transcription
1 COPD A Breath of Fresh Air Clare Hawkins, MD, FAAFP SW Regional Medical Officer Aspire Healthcare/Anthem
2 Speaker Disclosure Dr. Hawkins has disclosed that he has no actual or potential conflict of interest in relation to this topic.
3 Learning Objectives By the end of this activity, the participant should be better able to: 1. Evaluate patients who are current or former smokers, and those who develop frequent viral infections, for symptoms that may indicate COPD or related conditions 2. Interpret and validate results in symptomatic patients 3. Prepare treatment plans that include a combination approach to therapy for patients who have COPD. 4. Counsel patients who have COPD on the importance of quitting smoking and receiving annual vaccinations for influenza and pneumonia.
4 Epidemiology of COPD Third leading cause of death in the US % of adults had a diagnosis of COPD in $36 billion dollars annually in 2010, and costs are expected to rise to $49 billion for medical costs alone by Worldwide, an estimated 74 million deaths were caused by COPD in CDC 2016, 2 Adeloye et al 2015, 3 Ford et al, 2015, 4 WHO Fact sheet 2016
5 COPD Phenotypes Chronic Bronchitis Emphysema Overlapping Some COPD without classic features Asthma No Phenotype 5
6 2. Testing for COPD Physical Exam * Office Spirometry Other Pulmonary Function Testing Chest X ray & CT ECG * Holleman 1995
7 Diagnosis Spirometry as the mainstay of diagnosis Simple, inexpensive, but sometimes confusing Spirometry classification of COPD patients by GOLD COPD has utility but does not easily explain illness trajectory Health Status Measures assist (CAT and MRC dyspnea Scale)
8 FVC: Forced Vital Capacity Three Numbers FEV1: Amount breathed out in 1 second FEV1/FVC: How much of your lung s air can be exhaled in the first second Measure of caliber or function of airway NOT A COMPARISON TO REFERENCE VALUES More accurate than Peak Flow
9 Lung Volumes (ERV + RV = Functional Residual Capacity) Vital Capacity Inspiratory Capacity Tidal Volume Expiratory Reserve Volume Residual Volume
10 Dynamic Hyperinflation Vital Capacity Inspiratory Capacity Tidal Volume Expiratory Reserve Volume Residual Volume
11 Severity of Obstruction (GOLD) FEV1 % of predicted Mild >80 Moderate 50 to 79 Severe 30 to 49 Very severe <30 * Severity of Restriction FVC % of predicted Mild >65 to 80 Moderate >50 to 64 Severe <50
12 FEV 1 Thresholds (GOLD) Grade 1: Mild FEV1 > 80% Grade 2: Moderate 50% < FEV1 < 80% Grade 3: Severe 30% < FEV1 < 50% Grade 4: Very Severe FEV1 < 30% Compared with predicted values in patients with post bronchodilator FEV1/FVC < 70
13 FEV1/FVC 70 Caveat Overestimates COPD diagnosis in Elderly Underestimates COPD diagnosis in those under age 45
14 Normal Flow Volume Curve (Expiratory) PEFR 8 Flow (L/sec) 6 4 FEV Volume (L)
15 Normal, Obstructed, & Restrictive Curves Normal Obstruction Restriction Flow (L/sec) Volume (L)
16 Audience Polling #1 The most common cause of an Obstructive Pattern is 1. Pleural Effusion 2. Pulmonary Fibrosis 3. COPD and Asthma 4. Pulmonary Embolus
17 Inspiratory Volume Loop Expiratory Flattened Inspiratory Loop Indicating possible Extrathoracic Obstruction
18 Is FEV 1 / FVC Ratio Low? (<70%) Yes Obstructive Defect Is FVC Low? (<80% pred) Yes Combined Defect of Obstruction and Restriction /or Hyperinflation No Pure Obstruction Reversible Obstruction with ß agonist Reversible Obstruction and improved FVC with ß agonist No Further Testing with Full PFT s Yes Yes Suspect Asthma No Suspect COPD Adapted with permission from J S Lowry
19 Common Obstructive Disorders Diffuse Airway Disease Asthma COPD Bronchiectasis Cystic Fibrosis Upper Airway Obstruction Foreign Body Neoplasm Tracheal Stenosis Tracheomalacia Vocal Cord Paralysis
20 Diagnostic Flow Diagram, Restriction Is FEV 1 / FVC Ratio Low? (<70%) Yes No Is FVC Low?(<80% predicted) No Restrictive Defect Further Testing with Full PFT s and consider referral Normal Spirometry
21 Common Restrictive Disorders Parenchymal Interstitial Lung Diseases Fibrosis Granulomatosis (TB) Pneumoconiosis Pneumonitis (lupus) Loss of Functioning Tissue Atelectasis Large Neoplasm Resection Pleural Effusion Fibrosis Chest Wall Kyphoscoliosis Neuromuscular Disease Trauma Extrathoracic Abdominal Distension Obesity
22 Coding and Reimbursement Diagnosis ICD 9 ICD 10 Cough R05 Simple chronic bronchitis J41.0 Mucopurulent chronic bronchitis without J44.9 exac Acute bronchitis J20.9 Chronic obstructive pulmonary disease w J44.1 exac Shortness of breath/dyspnea R06.00 Pulmonary Fibrosis 515 J84.10 Asthma J45.909
23 Coding and Reimbursement Procedure CPT Code Reimbursement* Single spirometry $32.82 Pre post spirometry $57.71 Pulmonary stress test simple $71.77 Medication administration bronchodilator supply separate $13.34 Demonstration / instruction $14.79 Smoking Cessation <8x/ yr $12.98 Equipment Cost Office spirometer $1,500 2,500 Reimbursements based on Medicare payments 2009 Trailblazer Spirometry cost estimated from several vendors
24 COPD Assessment Test (CAT): CAT: An 8 item measure of health status impairment in COPD CCQ: Clinical COPD Questionnaire (CCQ): Self administered questionnaire developed to measure clinical control in patients with COPD ( mmrc dyspnea: Breathlessness Measurement using the Modified British Medical Research Council: Relates well to other measures of health status and predicts future mortality risk
25 CAT (COPD Assessment Test) I never cough I cough all the time I have no phlegm in my chest at My chestis full of phlegm all My chest does not feel tight at all My chest feels very tight When I walk up a hill or one flight of stairs I am not breathless I am not limited doing any activities at home I am confident leaving my home despite my lung condition When I walk up a hill or one flight of stairs I am very breathless I am very limited doing activities at home I am not at all confident leaving my home because of my lung condition I sleep soundly I don t sleep soundly because of my lung condition I have lots of energy I have no energy at all
26 CAT Score Impact level <10 Low Medium Possible management considerations Smoking Cessation Annual influenza vaccination Reduce exposure to exacerbation risk factors Therapy as warranted by further clinical assessment. Reviewing maintenance therapy is it optimal? Referral for pulmonary rehabilitation Ensuring best approaches to minimizing and managing exacerbations Reviewing aggravating factors still smoking? High Referral to specialist care (if you are in general practice) Additional pharmacological treatments
27 mmrc Dyspnea Scale 0 I only get breathless with strenuous exercise 1 I get short of breath when hurrying on the level or walking up a slight hill 2 I walk slower than people of the same age on the level because of my breathlessness, or I have to stop for breath when walking on my own pace on the level 3 I stop for breath after walking about 100 meters or a few minutes on the level 4 I am too breathless to leave the house or I am breathless when dressing or undressing

28 Prognosis Model in COPD
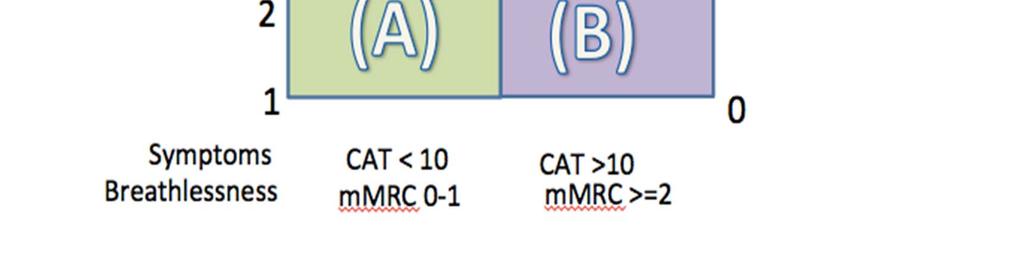
29 A B C D Characteristics Low Risk, Less Symptoms Low Risk, More Symptoms High Risk, Less Symptoms High Risk, More Symptoms Spirometric Class Exac/ yr CAT mmrc Gold 1 2 <1 < Gold 1 2 <1 >10 >2 Gold 3 4 >2 < Gold 3 4 >2 >10 >2
30 3. Treatment Plans Medications for stable COPD Medications for COPD exacerbations Pulmonary rehabilitation Oxygen therapy Comorbidities End of life care
31 GOALS Relieving symptoms Slowing disease progression Enhancing exercise tolerance and functional status Preventing and treating complications Improving overall health
32 Grade 1 Mild Grade 2 Moderate Grade 3 Severe Grade 4 Very Severe FEV1 > 80 FEV FEV FEV1 < 30 Or < 50 with Cor Pulmonale PCV 23,13 Influenza & SABA 3. Treatment Plans: Stable COPD LABA and/or LAMA ICS for recurrent exacerbations Pulmonary Rehab Oxygen & LVRS?
33 Medication Categories Short Acting Beta Agonist (SABA) Short Acting Anticholinergic Long Acting Anticholinergic (LAMA) Long Acting Beta Agonist (LABA) Inhaled Corticosteroid (ICS)
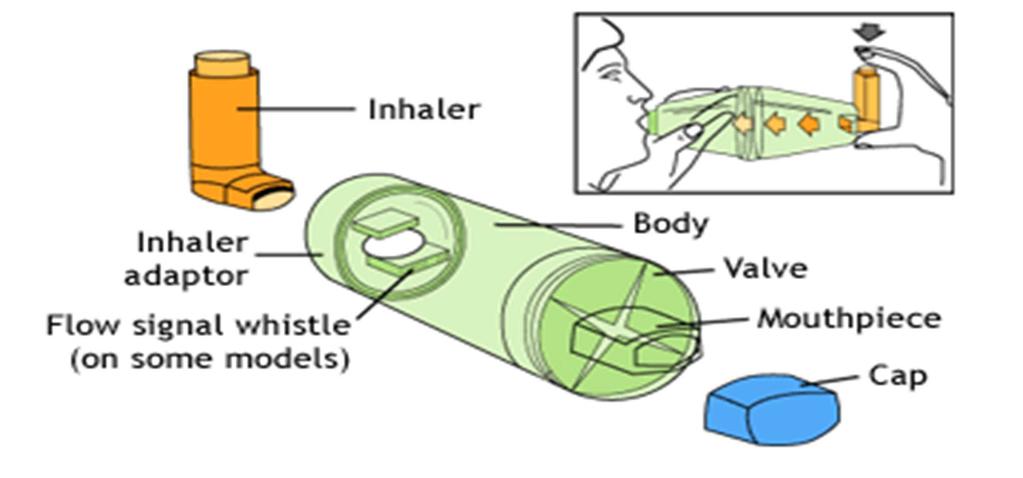
34 Spacer
35 Long Acting Beta Agonists LABA SERAVENT diskus, (salmeterol) DPI device FORADIL Aerolizer, (formoterol) DPI BROVANA, (arformoteral) nebulized PERFORMIST, (salmeterol) DPI STRIVERDI Respimat, (olodaterol) DPI ARCAPTA Neohaler, (indacaterol) DPI
36 Inhaled Corticosteroid, ICS FLOVENT MDI or Diskus (44, 110, 220 fluticasone) DPI Device QVAR MDI (40 & 80 beclomethasone) HFA MDI ASMANEX Twisthaler PULMICORT Tubohaler, (200 budesonide) (DPI Device) PULMICORT Flexhaler, (90 & 180 budesonide) DPI Device PULMICORT Respules (budesonide) Neb bid AEROSPAN Aerosol, (80 & 160 flunisolide) HFA MDI ALVESCO Aerosol, (80 & 160 ciclesonide) HFA MDI ASMANEX HFA MDI, (100 & 200 mometasone) DPI ARNUITY Ellipta, (100 & 200 fluticasone) DPI
37 Combo LABA & ICS ADVAIR Diskus, salmeterol & fluticasone, 250/50, (230/21 bid MDI) SYMBICORT, formoterol & budesonide) (80/45, 160/45 BREO Ellipta, daily (vilanterol & fluticasone) DULERA Aerosol, (100/5 and 200/5 ii bid (formoterol & mometasone)
38 Anticholinergic LAMA SPIRIVA Handihaler or Respimat, tiotropium DPI INCRUSE Ellipta, (umeclidinium) DPI SEEBRI Neohaler, (glycopyrrolate) DPI
39 LAMA & LABA ANORO Ellipta (umeclidinium & vilanterol) STIOLTO Respimat (tiotropium & olodaterol) UTIBRON Neohaler (glycopyrrolate & indacaterol) BEVESPI Aerosphere (formoterol & glycopyrrolate)
40 ICS, LAMA, LABA? TRELIGY: Fluticasone, Umeclidinium, vilanterol
41 Inhaler Technique 50% of people use their inhaler incorrectly Many health care providers can t demonstrate Have them line up their inhalers Have them contrast rescue from maintenance Have them store or d/c ones from previous formulary Have them take them out and show you how they use them (and how often)
42 Medication Adherence Review dose counter to see if on track LABA & LAMA don t have immediate effect that patients expect Outline refill rate. Is it monthly? Review donut hole and formulary issues Consider using needy meds or low income subsidy
43 MDI vs. NEBS Nebulized medications may be necessary if patient has severely limited inspiratory capacity Beta Agonist excess = Tremor, Anxiety, Tachycardia (But similar to popular caffeine supplement drinks) Part B Medicare not Part D, so can be used in the donut hole I.e. Arformoterol LABA ~ $800/month

44 Audience Polling Case COPD Exacerbation 58 yo Asian Male COPD x 5 years Continues to smoke Dyspnea with minimal exertion Increased cough with sputum Increased sputum purulence Three similar exacerbations in past 12 months AdobeStock License #
45 Audience Polling #2 The best treatment for this exacerbation is? 1. Tapering dosage of methylprednisolone 2. Guerilla cillin in high doses 3. Prednisone 40 mg daily x 5 days 4. Immediate hospital admission
46 3. Treatment Plan: Exacerbations Oral Steroids = IV steroids within 1 hour. Prednisone 40 mg daily 5 days 1 Antibiotics: Amox/Clav, Doxycycline, TMP/SMX, Quinolone, or others Bronchodilators Oxygen +/ hospitalization if desaturating 1 Leuppi 2013
47 COPD Interventions #1 E kit Prednisone 40 mg daily x 5 days No other doses, no Medrol dose pack,. Antibiotic of choice Bactrim, Doxycycline, Azithromycin, Amox Clav Fill Prescription Keep in fridge Begin if; change in volume or purulence Change in dyspnea
48 Infectious vs. Non Infectious Exacerbations 2/3 will need antibiotics If no change in sputum or fever, but only dyspnea, and no evidence of pneumothorax then may just need steroid Anthonisen 1987
49 Preventing Recurrent Exacerbations LABA/LAMA therapy with good technique Macrolide therapy daily or 3 x per week Antibiotic resistance, hearing loss, QT interval PDE4 Inhibitor Roflumilast Diarrhea, weight loss, nausea, headache, back pain, influenza, insomnia, dizziness, decreased appetite 1, 2 1 Chong 2013, 2 Martinez 2015
50 Evidence equivocal Oxygen If < 88% sat > h per day for decreased mortality For exercise desaturation? Improves exercise duration, no improvement in outcomes 1 GOLD 2018
51 What is Pulmonary Rehab Comprehensive, interdisciplinary intervention that includes; Supervised exercise training Patient education Behavioral therapy Lifestyle management Programs last from 8 to 12 weeks, with 2 to 3 weekly sessions Some evidence for home based rehab especially for maintenance
52 Pulmonary Rehabilitation Should be prescribed for symptomatic patients with FEV1 < 50%, (SORT A) Could be considered for symptomatic or exercise limited patients FEV1 > 50% (SORT B) Pulmonary rehabilitation improved quality of life dyspnea, and exercise capacity compared to standard care. (SORT A) ACP Updates Guideline on Diagnosis and Management of Stable COPD Aug 2, 2011, Roman et al. 2013
53 3. Treatment Plans: Comorbidities Cardiovascular Disease Heart Failure Atrial Fibrillation Hypertension Osteoporosis Anxiety & Depression Diabetes Impaired cognitive function
54 3. Treatment Plans: End of Life Care COPD as third most common cause of death A story without a (well defined), beginning, middle or end Dyspnea at rest Frequent exacerbations Weight loss Recurrent intubation/ventilation
55 Case II Roger Roger is a 65 yo with advanced COPD, who you have seen for many years, and treated with multiple inhalers, oxygen and a few hospitalizations for exacerbations He has begun to lose weight and has severe exercise restriction in spite of maximal treatment Can you enter a conversation about prognosis? How?


56 Case II Roger 65 COPD D Adobe Stock License # Multiple inhalers, oxygen and a few hospitalizations for exacerbations Has begun to lose weight and has severe exercise restriction in spite of maximal treatment How would you bring up the topic?
57 Audience Polling #3 How would you bring up the topic? 1. Tell him, there is nothing more medicine can do 2. Discuss how if he is intubated he will never come off the ventilator 3. Say, I m worried about you because I see signs that your disease is getting much worse
58 Illness Trajectory: Chronic Illness Organ Failure COPD or CHF Exacerbation
59 Introducing the Topic After looking at what has been going on in the past year, I think we should talk about where this appears to be going How do you feel about continuing to go to the hospital? When this happens again do you want to go on a breathing machine? Since we know that COPD will likely take your life, have you thought what it will be like to die?
60 Audience Polling #4 The only thing which changes the natural history of COPD is 1. Anti inflammatory therapy 2. Smoking cessation 3. Combined LABA and LAMA therapy 4. Pulmonary rehabilitation
61 Adapted from: Fletcher C, Peto R. The natural history of chronic airflow obstruction. Br Med J 1977; 1:
62 4. Smoking Cessation & Vaccination Ask: At every visit about smoking status Advise: The hazards and impact of smoking Assess: Readiness to quit, set a quit date Assist: Prescribe Arrange: Follow up in person, telephonic or on line
63 Medical Assistance with Quitting Nicotine Replacement (17% patch, 12.5% lozenges/gum, 2.4% spray/inhaler ) Varenicline (7.9%) Bupropion XL 150 / d 300 mg / d 2.7% Quitting Smoking Among Adults United States, , MMRW. January 6, 2017 / 65(52);
64 Varenicline Initiate regimen 1 week before quit smoking date Days 1 3: 0.5 mg PO qday Days 4 7: 0.5 mg PO BID Day 8 to end of treatment: 1 mg PO BID If quitting is successful after 12 weeks, continue another 12 weeks at 1 mg q12hr
65 Varenicline SLOW QUIT METHOD: Reduce smoking by 50% from baseline within the first 4 weeks, by an additional 50% in the next 4 weeks Side Effects Psychiatric relative contraindication (depression/ suicide) Seizure contraindication Reduce dose if GFR < mg/d increase to bid If on hemodialysis; maximum 0.5 mg/d
66 Vaccinations PCV 13 Pneumococcal Conjugate PCV 23 Pneumococcal Polysaccharide Before and second dose after 65 (five years apart) One year between Conjugate and Polysaccharide Influenza Annually
67 Recommendations 1. Spirometry should be used to diagnose symptomatic patients (SOR A) 2. Spirometry should not be used to screen asymptomatic patients (SOR A) 3. Bronchodilators should be used for those with FEV % predicted (SOR B) 4. Bronchodilators should be used for those with FEV1 < 60% (SOR A)
68 Recommendations 5. Oral Steroids = IV steroids within 1 hour. Prednisone 40 mg daily 5 days 1 (SOR A) 6. Macrolide daily or 3 x week can reduce exacerbation frequency for those with FEV1 < 60% (SOR B) 2 7. Pulmonary Rehabilitation should be offered for those with FEV1 < 60% predicted 3 1 Lueppi REDUCE 2013, 2 GOLD Pradella 2015
69 GOLD COPD 2018 References reports/ Accessed Aug 5, 2018 Holleman DR, Jr, Simel DL. Does the clinical examination predict airflow limitation? JAMA. 1995;273(4): Pradella CO, Belmonte GM, Maia MN, Delgado CS, Luise AP, Nascimento OA, et al. Home Based Pulmonary Rehabilitation for Subjects With COPD: A Randomized Study. Respiratory Care. 2015;60(4):
70 References Centers For Disease Control and Prevention. Chronic obstructive pulmonary disease (COPD) Accessed at on 15 May Adeloye D, Chua S, Lee C, Basquill C, Papana A, Theodoratou E, et al. Global and regional estimates of COPD prevalence: Systematic review and meta analysis. J Glob Health. 2015;5(2): Ford E, Murphy LB, Khavjou O, Giles WH, Holt JB, Croft JB. Total and state specific medical and absenteeism costs of COPD among adults aged 18 years in the United States for 2010 and projections through CHEST. 2015;147(1): World Health Organization. Chronic obstructive pulmonary disease (COPD): Fact Sheet Accessed at on 15 May 2017.
71 References Leuppi JD. Short term vs. Conventional Glucocorticoid Therapy in Acute Exacerbations of Chronic Obstructive Pulmonary Disease The REDUCE Randomized Clinical Trial. JAMA. 2013;309(21): Roman M, Larraz C, Gomez A, Ripoll J, Mir I, Miranda EZ, et al. Efficacy of pulmonary rehabilitation in patients with moderate chronic obstructive pulmonary disease: a randomized controlled trial. BMC Family Practice. 2013;14:21.
72 References Wellington Respiratory Study. Thorax. 2008;63:761 7 ACP Updates Guideline on Diagnosis and Management of Stable COPD Aug 2, Armstrong C. ACP guideline on stable COPD. Am Fam Physician Jan 15;85(2):
73 References Lee H, Kim J, Tagmazyan K. Treatment of stable COPD: the GOLD guidelines. Am Fam Physician. 2013;88(10): Lenney J, Innes JA, Crompton GK. Inappropriate inhaler use: assessment of use and patient preference of seven inhalation devices. Respir Med. 2000;94(5):
74 References Chong J, Leung B, Poole P. Phosphodiesterase 4 inhibitors for chronic obstructive pulmonary disease. Cochrane Database of Systematic Reviews. 2013;11:CD Martinez FJ, Calverley PM, Goehring UM, Brose M, Fabbri LM, Rabe KF. Effect of roflumilast on exacerbations in patients with severe chronic obstructive pulmonary disease uncontrolled by combination therapy (REACT): a multicenter randomized controlled trial. Lancet. 2015;385(9971): Anthonisen NR, et al. Antibiotic therapy in exacerbations of chronic obstructive pulmonary disease. Ann Intern Med Feb;106(2):
75 References Qaseem A, WT, Weinberger SE, Hanania NA, Criner G, van der Molen T, Marciniuk DD, Denberg, T, Schünemann H, Wedzicha W, MacDonald R, Shekelle P; American College of Physicians; American College of Chest Physicians; American Thoracic Society; European Respiratory Society. Diagnosis and management of stable chronic obstructive pulmonary disease: a clinical practice guideline update from the American College of Physicians, American College of Chest Physicians, American Thoracic Society, and European Respiratory Society. Ann Intern Med Aug 2;155(3): Fletcher C, Peto R. The natural history of chronic airflow obstruction. Br Med J. 1977; 1:
76 Contact
Individualizing and Optimizing Asthma Care. CFW 2018 Friday, April 13, 9:45 11:15 am Renaissance Austin Hotel in Austin, Texas
 Individualizing and Optimizing Asthma Care CFW 2018 Friday, April 13, 9:45 11:15 am Renaissance Austin Hotel in Austin, Texas Speaker Disclosure Dr. Hawkins has disclosed that he has no actual or potential
Individualizing and Optimizing Asthma Care CFW 2018 Friday, April 13, 9:45 11:15 am Renaissance Austin Hotel in Austin, Texas Speaker Disclosure Dr. Hawkins has disclosed that he has no actual or potential
Up in FLAMES: Stable Chronic Obstructive Pulmonary Disease (COPD) Management. Colleen Sakon, PharmD BCPS September 27, 2018
 Management. Colleen Sakon, PharmD BCPS September 27, 2018") Up in FLAMES: Stable Chronic Obstructive Pulmonary Disease (COPD) Management Colleen Sakon, PharmD BCPS September 27, 2018 Disclosures I have no actual or potential conflicts of interest 2 Objectives Summarize
Up in FLAMES: Stable Chronic Obstructive Pulmonary Disease (COPD) Management Colleen Sakon, PharmD BCPS September 27, 2018 Disclosures I have no actual or potential conflicts of interest 2 Objectives Summarize
STRIVERDI RESPIMAT (olodaterol hcl) aerosol
 aerosol") STRIVERDI RESPIMAT (olodaterol hcl) aerosol Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
STRIVERDI RESPIMAT (olodaterol hcl) aerosol Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy
TRELEGY ELLIPTA (fluticasone-umeclidinium-vilanterol) aerosol powder
 aerosol powder") TRELEGY ELLIPTA (fluticasone-umeclidinium-vilanterol) aerosol powder Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
TRELEGY ELLIPTA (fluticasone-umeclidinium-vilanterol) aerosol powder Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
COPD Update. Plus New and Improved Products for Inhaled Therapy. Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor
 COPD Update Plus New and Improved Products for Inhaled Therapy Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose concerning possible financial
COPD Update Plus New and Improved Products for Inhaled Therapy Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose concerning possible financial
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide
 VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
VA/DoD Clinical Practice Guideline Management of COPD Pocket Guide MODULE A: MAAGEMET OF COPD 1 2 Patient with suspected or confirmed COPD presents to primary care [ A ] See sidebar A Perform brief clinical
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline. MedStar Health
 Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
A Visual Approach to Simplifying Respiratory Drug Regimens
 A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP 3 Main Categories Inhaled Respiratory Drugs Binds to beta-2 receptors Relaxation of smooth muscles in the lung
A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP 3 Main Categories Inhaled Respiratory Drugs Binds to beta-2 receptors Relaxation of smooth muscles in the lung
Disclosure and Conflict of Interest 8/15/2017. Pharmacist Objectives. At the conclusion of this program, the pharmacist will be able to:
 Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
Digging for GOLD Rebecca Young, PharmD, BCACP, Roosevelt University College of Pharmacy Assistant Professor of Clinical Sciences Practice Site Advocate Medical Group-Nesset Pavilion Disclosure and Conflict
A Visual Approach to Simplifying Respiratory Drug Regimens
 Adverse Effects of Inhaled Medications A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP June 28, 2017 Drug Category Beta 2 agonists antagonists Adverse Effects
Adverse Effects of Inhaled Medications A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP June 28, 2017 Drug Category Beta 2 agonists antagonists Adverse Effects
A Visual Approach to Simplifying Respiratory Drug Regimens
 A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP October 23, 2017 Learning Objectives Be able to list at least 3 major adverse effects of inhaled medications
A Visual Approach to Simplifying Respiratory Drug Regimens Stephanie Cheng, PharmD, MPH, BCGP October 23, 2017 Learning Objectives Be able to list at least 3 major adverse effects of inhaled medications
COPD: Preventable and Treatable. Lecture Outline. Diagnosis of COPD. COPD: Defining Terms
 COPD: Preventable and Treatable Christopher H. Fanta, M.D. Partners Asthma Center Pulmonary and Critical Care Division Brigham and Women s Hospital Harvard Medical School Lecture Outline I. Diagnosis and
COPD: Preventable and Treatable Christopher H. Fanta, M.D. Partners Asthma Center Pulmonary and Critical Care Division Brigham and Women s Hospital Harvard Medical School Lecture Outline I. Diagnosis and
Test Your Inhaler Knowledge
 A Breath of Fresh Air: Updates in COPD Management Jennifer Austin Szwak, PharmD, BCPS, DPLA University of Chicago Medicine The speaker has nothing to disclose Abbreviations COPD: Chronic obstructive pulmonary
A Breath of Fresh Air: Updates in COPD Management Jennifer Austin Szwak, PharmD, BCPS, DPLA University of Chicago Medicine The speaker has nothing to disclose Abbreviations COPD: Chronic obstructive pulmonary
COPD. Stan Kellar, MD. Physiology 11/4/2014. Chief of Clinical Affairs, BH NLR Pulmonary Medicine Sleep Medicine
 Stan Kellar, MD Chief of Clinical Affairs, BH NLR Pulmonary Medicine Sleep Medicine COPD Physiology The lungs are filters Filter in oxygen Filter out carbon dioxide (Vascular filter, not part of this discussion)
Stan Kellar, MD Chief of Clinical Affairs, BH NLR Pulmonary Medicine Sleep Medicine COPD Physiology The lungs are filters Filter in oxygen Filter out carbon dioxide (Vascular filter, not part of this discussion)
COPD: Current Medical Therapy
 COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
Three s Company - The role of triple therapy in chronic obstructive pulmonary
 Three s Company - The role of triple therapy in chronic obstructive pulmonary disease (COPD) October 26 th, 2018 Zahava Picado, PharmD PGY1 Pharmacy Resident Central Texas Veterans Healthcare System Zahava.Picado@va.gov
Three s Company - The role of triple therapy in chronic obstructive pulmonary disease (COPD) October 26 th, 2018 Zahava Picado, PharmD PGY1 Pharmacy Resident Central Texas Veterans Healthcare System Zahava.Picado@va.gov
Inhaled Corticosteroids Drug Class Prior Authorization Protocol
 Inhaled Corticosteroids Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Inhaled Corticosteroids Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Inhaled Corticosteroids Drug Class Prior Authorization Protocol
 Inhaled Corticosteroids Drug Class Prior Authorization Protocol Line of Business: Medi-Cal P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Inhaled Corticosteroids Drug Class Prior Authorization Protocol Line of Business: Medi-Cal P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been developed through review
Turning Science into Real Life Roflumilast in Clinical Practice. Roland Buhl Pulmonary Department Mainz University Hospital
 Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
Turning Science into Real Life Roflumilast in Clinical Practice Roland Buhl Pulmonary Department Mainz University Hospital Therapy at each stage of COPD I: Mild II: Moderate III: Severe IV: Very severe
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
Clinical Policy: Roflumilast (Daliresp) Reference Number: CP.PMN.46 Effective Date: Last Review Date: 08.18
 Reference Number: CP.PMN.46 Effective Date: Last Review Date: 08.18") Clinical Policy: (Daliresp) Reference Number: CP.PMN.46 Effective Date: 11.01.11 Last Review Date: 08.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Daliresp) Reference Number: CP.PMN.46 Effective Date: 11.01.11 Last Review Date: 08.18 Line of Business: Medicaid Revision Log See Important Reminder at the end of this policy for important
Drug Class Monograph
 Drug Class Monograph Class: Inhaled Corticosteroids Drugs: Aerospan (flunisolide), Advair Diskus, Advair HFA (fluticasone/salmeterol), Alvesco (ciclesonide), Arnuity Ellipta (fluticasone furoate), Asmanex
Drug Class Monograph Class: Inhaled Corticosteroids Drugs: Aerospan (flunisolide), Advair Diskus, Advair HFA (fluticasone/salmeterol), Alvesco (ciclesonide), Arnuity Ellipta (fluticasone furoate), Asmanex
Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines
 Treatment Guidelines") Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines Where appropriate the following should be offered before commencing inhaled treatment: Offer treatment and support to stop smoking. Smoking
Chronic Obstructive Pulmonary Disease (COPD) Treatment Guidelines Where appropriate the following should be offered before commencing inhaled treatment: Offer treatment and support to stop smoking. Smoking
COPD: Treatment Update Property of Presenter. Not for Reproduction. Barry Make, MD Professor of Medicine National Jewish Health
 COPD: Treatment Update Barry Make, MD Professor of Medicine National Jewish Health Disclosures Advisory board, consultant, multi-center trial, research funding, Data Safety Monitoring Board (DSMB), or
COPD: Treatment Update Barry Make, MD Professor of Medicine National Jewish Health Disclosures Advisory board, consultant, multi-center trial, research funding, Data Safety Monitoring Board (DSMB), or
Algorithm for the use of inhaled therapies in COPD Version 2 May 2017
 Algorithm for the use of inhaled therapies in COPD This document has been revised by the Berkshire West Respiratory Network to support clinicians in selecting the most appropriate, cost effective treatments
Algorithm for the use of inhaled therapies in COPD This document has been revised by the Berkshire West Respiratory Network to support clinicians in selecting the most appropriate, cost effective treatments
Select Inhaled Respiratory Agents
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Michelle Zeidler, MD, MS
 7/1/18 Chronic Obstructive Pulmonary Disease: Optimizing Outpatient Care & Reducing Exacerbations Michelle Zeidler, MD, MS Professor of Medicine, Pulmonary, Critical Care Medicine & Sleep Medicine, VA
7/1/18 Chronic Obstructive Pulmonary Disease: Optimizing Outpatient Care & Reducing Exacerbations Michelle Zeidler, MD, MS Professor of Medicine, Pulmonary, Critical Care Medicine & Sleep Medicine, VA
Take My Breath Away: COPD Update. Jason Henderson D.O. Warren Clinic Pulmonary & Critical Care
 Take My Breath Away: Update Jason Henderson D.O. Warren Clinic Pulmonary & Critical Care Objectives 1. Recognize clinical signs and symptoms associated with chronic bronchitis and emphysema. 2. Describe
Take My Breath Away: Update Jason Henderson D.O. Warren Clinic Pulmonary & Critical Care Objectives 1. Recognize clinical signs and symptoms associated with chronic bronchitis and emphysema. 2. Describe
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES
 MANAGEMENT GUIDELINES") JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
Algorithm for the use of inhaled therapies in COPD
 Berkshire West Integrated Care System Representing Berkshire West Clinical Commisioning Group Royal Berkshire NHS Foundation Trust Berkshire Healthcare NHS Foundation Trust Berkshire West Primary Care
Berkshire West Integrated Care System Representing Berkshire West Clinical Commisioning Group Royal Berkshire NHS Foundation Trust Berkshire Healthcare NHS Foundation Trust Berkshire West Primary Care
THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable
 THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. COPD in the United States Third leading cause
THE CHALLENGES OF COPD MANAGEMENT IN PRIMARY CARE An Expert Roundtable This activity is supported by an educational grant from Sunovion Pharmaceuticals Inc. COPD in the United States Third leading cause
Medical Directive. Activation Date: April 24, 2013 Review due by: December 1, Medical Director: Date: December 1, 2017
 Medical Directive Pre and Post Bronchodilator Spirometry Testing and Treatment Initiation Assigned Number: Activation Date: April 24, 2013 Review due by: December 1, 2019 23 Approval Signature & Date Medical
Medical Directive Pre and Post Bronchodilator Spirometry Testing and Treatment Initiation Assigned Number: Activation Date: April 24, 2013 Review due by: December 1, 2019 23 Approval Signature & Date Medical
Ferris State University College of Pharmacy MPA CE Symposium 2016 Paul Thill, PharmD, BCPS
 Ferris State University College of Pharmacy MPA CE Symposium 2016 Paul Thill, PharmD, BCPS Objectives Categorize the new asthma and COPD inhalers in to existing or newly created categories Discuss the
Ferris State University College of Pharmacy MPA CE Symposium 2016 Paul Thill, PharmD, BCPS Objectives Categorize the new asthma and COPD inhalers in to existing or newly created categories Discuss the
Chronic Obstructive Pulmonary Disease (COPD) Clinical Guideline
 Clinical Guideline") Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Guideline for the Diagnosis and Management of COPD
 Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
If you require this document in another format such as Braille, large print, audio or another language please contact the Trusts Communications Team
 MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) IN ADULTS Summary statement: How does the document support patient care? Staff/stakeholders involved in development: Job titles only Division:
MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) IN ADULTS Summary statement: How does the document support patient care? Staff/stakeholders involved in development: Job titles only Division:
Balanced information for better care. Helping patients with COPD breathe easier
 Balanced information for better care Helping patients with COPD breathe easier COPD is the third-leading cause of death in the U.S., following cancer and heart disease 1 FIGURE 1. Women now have a higher
Balanced information for better care Helping patients with COPD breathe easier COPD is the third-leading cause of death in the U.S., following cancer and heart disease 1 FIGURE 1. Women now have a higher
How to treat COPD? What is the mechanism of dyspnea? Smoking cessation
 : The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
: The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
Provider Respiratory Inservice
 Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
Provider Respiratory Inservice 2 Welcome Opening Remarks We will cover: Definition of Asthma & COPD Evidence based guidelines for diagnosis, evaluation, and management of asthma Evidence based guidelines
2/4/2019. GOLD Objectives. GOLD 2019 Report: Chapters
 GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
COPD GOLD Guidelines & Barnet inhaler choices. Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust
 COPD GOLD Guidelines & Barnet inhaler choices Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust GOLD 2017 Report: Chapters 1. Definition and Overview 2. Diagnosis and Initial
COPD GOLD Guidelines & Barnet inhaler choices Dr Dean Creer, Respiratory Consultant, Royal Free London NHS Foundation Trust GOLD 2017 Report: Chapters 1. Definition and Overview 2. Diagnosis and Initial
Asthma & COPD Medication Review. Hutchison Disclosures 2/16/2017. Objectives
 Asthma & COPD Medication Review Anna Meador, PharmD, BCACP Assistant Professor/ Pharmacy Director McWhorter School of Pharmacy/ Christ Health Center Amber Hutchison, PharmD, BCPS Assistant Clinical Professor
Asthma & COPD Medication Review Anna Meador, PharmD, BCACP Assistant Professor/ Pharmacy Director McWhorter School of Pharmacy/ Christ Health Center Amber Hutchison, PharmD, BCPS Assistant Clinical Professor
MEDICAL COVERAGE GUIDELINES ORIGINAL EFFECTIVE DATE: 07/05/18 SECTION: DRUGS LAST REVIEW DATE: LAST CRITERIA REVISION DATE: ARCHIVE DATE:
 CINQAIR (reslizumab) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
CINQAIR (reslizumab) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015
 David CL Lam Department of Medicine University of Hong Kong October, 2015") Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
Advances in the management of chronic obstructive lung diseases (COPD) David CL Lam Department of Medicine University of Hong Kong October, 2015 Chronic obstructive pulmonary disease (COPD) COPD in Hong
COPD Robert Schilz DO, PhD Pulmonary, Critical Care and Sleep Medicine University Hospitals Case Medical Center
 COPD 2018 GOLD 2017 Report Global Initiative for Chronic Obstructive Lung D isease COPYRIGHTED MATERIAL- DO NOT COPY OR DISTRIBUTE GLOBAL STRATEGY FOR THE DIAGNOSIS, MANAGEMENT, AND PREVENTION OF CHRONIC
COPD 2018 GOLD 2017 Report Global Initiative for Chronic Obstructive Lung D isease COPYRIGHTED MATERIAL- DO NOT COPY OR DISTRIBUTE GLOBAL STRATEGY FOR THE DIAGNOSIS, MANAGEMENT, AND PREVENTION OF CHRONIC
COPD Medications Coverage Summary Non-Insured Health Benefits Coverage SABA Bricanyl turbuhaler Yes Yes
 COPD Medications Coverage Summary Drug Non-Insured Health Benefits Coverage SABA Bricanyl turbuhaler Yes Yes Ventolin MDI + generics Yes Yes Ventolin Diskus NO NO Yukon Pharmacare/Chronic Disease Program
COPD Medications Coverage Summary Drug Non-Insured Health Benefits Coverage SABA Bricanyl turbuhaler Yes Yes Ventolin MDI + generics Yes Yes Ventolin Diskus NO NO Yukon Pharmacare/Chronic Disease Program
QUANTITY LIMIT CRITERIA. BROVANA (arformoterol tartrate) SEREVENT DISKUS (salmeterol) STRIVERDI RESPIMAT (olodaterol)
 SEREVENT DISKUS (salmeterol) STRIVERDI RESPIMAT (olodaterol)") Carelirst. +.V Family of health care plans DRUG CLASS COMBINATIONS QUANTITY LIMIT CRITERIA LONG ACTING BETA2-ADRENERGIC AGONIST, ORAL INHALATION BRAND NAME (generic) LONG-ACTING BETA2-ADRENERGIC AGONISTS:
Carelirst. +.V Family of health care plans DRUG CLASS COMBINATIONS QUANTITY LIMIT CRITERIA LONG ACTING BETA2-ADRENERGIC AGONIST, ORAL INHALATION BRAND NAME (generic) LONG-ACTING BETA2-ADRENERGIC AGONISTS:
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline. MedStar Health
 Global Strategy f the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Global Strategy f the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Drug Effectiveness Review Project Summary Report
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Changing Landscapes in COPD New Zealand Respiratory Conference
 Changing Landscapes in COPD New Zealand Respiratory Conference Dr Robert Young BMedSc MBChB DPhil (Oxon) FRACP FRCP Associate Professor Consultant Physician Changing Landscapes in COPD: Summary 1. Overview
Changing Landscapes in COPD New Zealand Respiratory Conference Dr Robert Young BMedSc MBChB DPhil (Oxon) FRACP FRCP Associate Professor Consultant Physician Changing Landscapes in COPD: Summary 1. Overview
Surveillance report Published: 6 April 2016 nice.org.uk. NICE All rights reserved.
 Surveillance report 2016 Chronic obstructive pulmonary disease in over 16s: diagnosis and management (2010) NICE guideline CG101 Surveillance report Published: 6 April 2016 nice.org.uk NICE 2016. All rights
Surveillance report 2016 Chronic obstructive pulmonary disease in over 16s: diagnosis and management (2010) NICE guideline CG101 Surveillance report Published: 6 April 2016 nice.org.uk NICE 2016. All rights
Asthma COPD Update 2018
 Asthma COPD Update 2018 Roger Hefflinger, Pharm.D. Clinical Associate Professor ISU COP Clinical Teaching Pharmacist Family Medicine Residency of Idaho In support of improving patient care, Idaho State
Asthma COPD Update 2018 Roger Hefflinger, Pharm.D. Clinical Associate Professor ISU COP Clinical Teaching Pharmacist Family Medicine Residency of Idaho In support of improving patient care, Idaho State
COPD: GOLD guidelines Ijlal Babar, MD Medical Director Pulmonary CCM, Pulmonary Hypertension Center SRHS
 COPD: GOLD guidelines 2017 Ijlal Babar, MD Medical Director Pulmonary CCM, Pulmonary Hypertension Center SRHS Introduction The Global Initiative for Chronic Obstructive Lung Disease (GOLD) program was
COPD: GOLD guidelines 2017 Ijlal Babar, MD Medical Director Pulmonary CCM, Pulmonary Hypertension Center SRHS Introduction The Global Initiative for Chronic Obstructive Lung Disease (GOLD) program was
What is COPD? COPD Pharmacotherapy. COPD Mortality Is Increasing
 COPD Pharmacotherapy Chronic Bronchitis What is COPD? 75% 17.5% Emphysema Laura C. Feemster, MD, MS Assistant Professor University of Washington Division of Pulmonary & Critical Care April 23,2015 COPD
COPD Pharmacotherapy Chronic Bronchitis What is COPD? 75% 17.5% Emphysema Laura C. Feemster, MD, MS Assistant Professor University of Washington Division of Pulmonary & Critical Care April 23,2015 COPD
Update in Pulmonology Update in Medicine and Primary Care November 11, 2017
 Update in Pulmonology Update in Medicine and Primary Care November 11, 2017 Denitza P. Blagev, MD Pulmonary & Critical Care Medicine Director, Schmidt Chest Clinic Director, Lung Cancer Screening Program
Update in Pulmonology Update in Medicine and Primary Care November 11, 2017 Denitza P. Blagev, MD Pulmonary & Critical Care Medicine Director, Schmidt Chest Clinic Director, Lung Cancer Screening Program
12/18/2017. Disclosures. Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Chronic Obstructive Pulmonary Disease Guidelines and updates
 Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
MDI Bonanza. Dwayne Griffin, DO
 MDI Bonanza Dwayne Griffin, DO Bonanza 3. A MDI costing $200 - $500 per month SISYPHUS MDI Griffin Mountain Evolution of Deliver Systems for COPD in the US 2003 2009 2011 2013 2004 2012 2014 Prescribing
MDI Bonanza Dwayne Griffin, DO Bonanza 3. A MDI costing $200 - $500 per month SISYPHUS MDI Griffin Mountain Evolution of Deliver Systems for COPD in the US 2003 2009 2011 2013 2004 2012 2014 Prescribing
CHRONIC OBSTRUCTIVE PULMONARY DISEASE
 CHRONIC OBSTRUCTIVE PULMONARY DISEASE INCIDENCE UP TO 380,000 PEOPLE IN IRELAND HSE FIGURES 110,000 DIAGNOSED AND 200,000 UNDIAGNOSED. AFFECTS MORE MEN THAN WOMEN BUT RATES ARE RISING 1500 DEATHS PER YEAR
CHRONIC OBSTRUCTIVE PULMONARY DISEASE INCIDENCE UP TO 380,000 PEOPLE IN IRELAND HSE FIGURES 110,000 DIAGNOSED AND 200,000 UNDIAGNOSED. AFFECTS MORE MEN THAN WOMEN BUT RATES ARE RISING 1500 DEATHS PER YEAR
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease CareOregon Pharmacy Abridged sample of presentation content Home Equipment Pathophysiology Exacerbations Guidelines Lifestyle Modification Medication Management Sample
Chronic Obstructive Pulmonary Disease CareOregon Pharmacy Abridged sample of presentation content Home Equipment Pathophysiology Exacerbations Guidelines Lifestyle Modification Medication Management Sample
Breaking Down Barriers to Pulmonary Therapies: Patient Education, Teach Back, and More
 Breaking Down Barriers to Pulmonary Therapies: Patient Education, Teach Back, and More Char Raley, RRT Brandon Johnson, PharmD, BCPS Pulmonary and Critical Care Symposium June 12 th, 2015 We have had no
Breaking Down Barriers to Pulmonary Therapies: Patient Education, Teach Back, and More Char Raley, RRT Brandon Johnson, PharmD, BCPS Pulmonary and Critical Care Symposium June 12 th, 2015 We have had no
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing
 Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
Asthma Management Updates: A Focus on Long-acting Muscarinic Antagonists and Intermittent Inhaled Corticosteroid Dosing Diana M. Sobieraj, PharmD, BCPS Assistant Professor University of Connecticut School
What is New in COPD: Times Are Changing! Meredith Chiasson, MD, FRCPC April 6, 2018
 What is New in COPD: Times Are Changing! Meredith Chiasson, MD, FRCPC April 6, 2018 No disclosures Disclosures objectives How to diagnose & Assess severity Treatment: Pharmacologic Non-Pharmacologic Maintenance
What is New in COPD: Times Are Changing! Meredith Chiasson, MD, FRCPC April 6, 2018 No disclosures Disclosures objectives How to diagnose & Assess severity Treatment: Pharmacologic Non-Pharmacologic Maintenance
Prescribing guidelines: Management of COPD in Primary Care
 Prescribing guidelines: Management of COPD in Primary Care Establish diagnosis of COPD in patients 35 years with appropriate symptoms with history, examination and spirometry (FEV1/FVC ratio < 70%) Establish
Prescribing guidelines: Management of COPD in Primary Care Establish diagnosis of COPD in patients 35 years with appropriate symptoms with history, examination and spirometry (FEV1/FVC ratio < 70%) Establish
Defining COPD. Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist
 Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING 10/16/2018 DISCLOSURES I have no financial or other disclosures
 OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
AIRDUO RESPICLICK (fluticasone-salmeterol) aerosol DULERA (mometasone furoate and formoterol fumarate dihydrate) aerosol
 aerosol DULERA (mometasone furoate and formoterol fumarate dihydrate) aerosol") DULERA (mometasone furoate and formoterol fumarate dihydrate) aerosol Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
DULERA (mometasone furoate and formoterol fumarate dihydrate) aerosol Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific
CHARM Guidelines for the diagnosis and
 \ CHARM Guidelines for the diagnosis and management of COPD City and Hackney CCG Homerton University Hospital NHS Foundation Trust Written by: Miss Hetal Dhruve, Specialist Pharmacist Respiratory Medicine,
\ CHARM Guidelines for the diagnosis and management of COPD City and Hackney CCG Homerton University Hospital NHS Foundation Trust Written by: Miss Hetal Dhruve, Specialist Pharmacist Respiratory Medicine,
THE COPD PRESCRIBING TOOL
 THE COPD PRESCRIBING TOOL Revised edition, 2017 www.bpac.org.nz/copd CLASSIFICATION The COPD prescribing tool This tool provides pharmacological treatment options for patients with COPD based on their
THE COPD PRESCRIBING TOOL Revised edition, 2017 www.bpac.org.nz/copd CLASSIFICATION The COPD prescribing tool This tool provides pharmacological treatment options for patients with COPD based on their
Improving Outcomes in COPD
 Neil MacIntyre MD Duke University Durham NC Current treatment guidelines f COPD focus Barriers to providing optimal treatment Diagnosis of COPD EXPOSURE TO RISK FACTORS AND/ OR SYMPTOMS sputum cough dyspnea
Neil MacIntyre MD Duke University Durham NC Current treatment guidelines f COPD focus Barriers to providing optimal treatment Diagnosis of COPD EXPOSURE TO RISK FACTORS AND/ OR SYMPTOMS sputum cough dyspnea
Medications for Managing COPD in Hospice Patients. Jim Joyner, PharmD, CGP Director of Clinical Operations Outcome Resources
 Medications for Managing COPD in Hospice Patients Jim Joyner, PharmD, CGP Director of Clinical Operations Outcome Resources Goal of medications in COPD Decrease symptoms and/or complications Reduce frequency
Medications for Managing COPD in Hospice Patients Jim Joyner, PharmD, CGP Director of Clinical Operations Outcome Resources Goal of medications in COPD Decrease symptoms and/or complications Reduce frequency
Wirral COPD Prescribing Guidelines
 Wirral COPD Prescribing Guidelines (To be read in conjunction with the Wirral COPD Supplementary Information) STEP 1: Assess symptoms COPD Assessment Test (CAT) [Link for CAT-test Online] is a patient-completed
Wirral COPD Prescribing Guidelines (To be read in conjunction with the Wirral COPD Supplementary Information) STEP 1: Assess symptoms COPD Assessment Test (CAT) [Link for CAT-test Online] is a patient-completed
FASENRA (benralizumab)
") FASENRA (benralizumab) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
FASENRA (benralizumab) Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices and drugs
Question I was one of the first dry power devices available in the US Flovent, Serevent and Advair are all available in this device
 What Device am I Class Side Effects History Potpourri Monitoring Tools 10 10 10 10 10 20 20 20 20 20 30 30 30 30 30 40 40 40 40 40 50 50 50 50 50 WHAT KIND OF DEVICE AM I? I was one of the first dry power
What Device am I Class Side Effects History Potpourri Monitoring Tools 10 10 10 10 10 20 20 20 20 20 30 30 30 30 30 40 40 40 40 40 50 50 50 50 50 WHAT KIND OF DEVICE AM I? I was one of the first dry power
Chronic Obstructive Pulmonary Disease
 Quality Department Guidelines for Clinical Care Ambulatory COPD Guideline Team Team Leader Davoren A Chick, MD General Medicine Team Members Paul J Grant, MD General Medicine R Van Harrison, PhD Learning
Quality Department Guidelines for Clinical Care Ambulatory COPD Guideline Team Team Leader Davoren A Chick, MD General Medicine Team Members Paul J Grant, MD General Medicine R Van Harrison, PhD Learning
Anyone who smokes and/or has shortness of breath and sputum production could have COPD
 COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis.
 1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
Chronic Obstructive Pulmonary Disease: What s New in Therapeutic Management?
 Chronic Obstructive Pulmonary Disease: What s New in Therapeutic Management? Sabrina Sherwood, PharmD PGY2 Internal Medicine Resident University of Utah Health September 29, 2018 Disclosures Relevant disclosures
Chronic Obstructive Pulmonary Disease: What s New in Therapeutic Management? Sabrina Sherwood, PharmD PGY2 Internal Medicine Resident University of Utah Health September 29, 2018 Disclosures Relevant disclosures
COPD. Understanding. An educational health series from National Jewish Health IN THIS ISSUE. What is COPD? 2. How is COPD Managed?
 Understanding COPD The Mount Sinai National Jewish Health Respiratory Institute was formed by the nation s leading respiratory hospital National Jewish Health, based in Denver, and top ranked academic
Understanding COPD The Mount Sinai National Jewish Health Respiratory Institute was formed by the nation s leading respiratory hospital National Jewish Health, based in Denver, and top ranked academic
Incorporating Newer Therapies and Strategies to Improve COPD Outcomes: A Practical Guide for Pharmacists. Learning Objectives.
 Incorporating Newer Therapies and Strategies to Improve COPD Outcomes: A Practical Guide for Pharmacists Learning Objectives Identify the risk factors for COPD and the clinical features that differentiate
Incorporating Newer Therapies and Strategies to Improve COPD Outcomes: A Practical Guide for Pharmacists Learning Objectives Identify the risk factors for COPD and the clinical features that differentiate
Chronic obstructive pulmonary disease
 0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
PFT s / 2017 Pulmonary Update. Eric S. Papierniak, DO University of Florida NF/SG VHA
 PFT s / 2017 Pulmonary Update Eric S. Papierniak, DO University of Florida NF/SG VHA Outline Overview of pulmonary function testing Uses/indications/limitations Technical aspects Basics of interpretation
PFT s / 2017 Pulmonary Update Eric S. Papierniak, DO University of Florida NF/SG VHA Outline Overview of pulmonary function testing Uses/indications/limitations Technical aspects Basics of interpretation
REVISED RESPIRATORY MEDICATION USE QUESTIONNAIRE
 REVISED RESPIRATORY MEDICATION USE QUESTIONNAIRE ID NUMBER: 0a) Date of Collection / / 0b) Staff Code Instructions: This form should be completed during the participant s clinic visit. 1) Are you regularly
REVISED RESPIRATORY MEDICATION USE QUESTIONNAIRE ID NUMBER: 0a) Date of Collection / / 0b) Staff Code Instructions: This form should be completed during the participant s clinic visit. 1) Are you regularly
SABA: VENTOLIN EVOHALER (SALBUTAMOL) SAMA: ATROVENT IPRATROPIUM. Offer LAMA (discontinue SAMA) OR LABA
 SAMA: ATROVENT IPRATROPIUM. Offer LAMA (discontinue SAMA) OR LABA") COPD GUIDELINES DIAGNOSIS >35 years of age Symptoms of cough, breathlessness, sputum, wheeze, Risk factor (SMOKING) Spirometry (post bronchodilator) FEV1/FVC = 0.7 ENCOURAGE PATIENTS TO BRING INHALERS
COPD GUIDELINES DIAGNOSIS >35 years of age Symptoms of cough, breathlessness, sputum, wheeze, Risk factor (SMOKING) Spirometry (post bronchodilator) FEV1/FVC = 0.7 ENCOURAGE PATIENTS TO BRING INHALERS
Co. Durham & Darlington Respiratory Network COPD Treatment Guide
 Co. Durham & Darlington Respiratory Network COPD Treatment Guide Age > 35, Productive cough, Breathless, Smoking Hx Spirometry (post-bronchodilator) COPD Advice Intensive smoking cessation support Vaccination
Co. Durham & Darlington Respiratory Network COPD Treatment Guide Age > 35, Productive cough, Breathless, Smoking Hx Spirometry (post-bronchodilator) COPD Advice Intensive smoking cessation support Vaccination
COPD/Asthma. Prudence Twigg, AGNP
 COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
Pharmacotherapy for COPD
 10/3/2017 Topics to be covered Pharmacotherapy for chronic treatment Pharmacotherapy for COPD Dr. W C Yu 3rd September 2017 Commonly used drugs Guidelines for their use Inhaled corticosteroids (ICS) in
10/3/2017 Topics to be covered Pharmacotherapy for chronic treatment Pharmacotherapy for COPD Dr. W C Yu 3rd September 2017 Commonly used drugs Guidelines for their use Inhaled corticosteroids (ICS) in
Asthma/COPD Update with Inhaler Workshop
 Asthma/COPD Update with Inhaler Workshop October 8, 2017 Nathan Samsa, DO, Pharm D, RPh, FACOI None Disclosures Agenda Asthma Updates COPD Updates Inhaler Workshop Medication Acronyms SABA: Short acting
Asthma/COPD Update with Inhaler Workshop October 8, 2017 Nathan Samsa, DO, Pharm D, RPh, FACOI None Disclosures Agenda Asthma Updates COPD Updates Inhaler Workshop Medication Acronyms SABA: Short acting
What is this patient s diagnosis?
 Asthma and COPD KANTA VELAMURI, MD ASSOCIATE PROFESSOR OF MEDICINE PULMONARY, CRITICAL CARE AND SLEEP MEDICINE SECTION MICHAEL E. DEBAKEY VA MEDICAL CENTER BAYLOR COLLEGE OF MEDICINE Disclosures None Case
Asthma and COPD KANTA VELAMURI, MD ASSOCIATE PROFESSOR OF MEDICINE PULMONARY, CRITICAL CARE AND SLEEP MEDICINE SECTION MICHAEL E. DEBAKEY VA MEDICAL CENTER BAYLOR COLLEGE OF MEDICINE Disclosures None Case
Pharmacist Objectives. Pulmonary Update. Outline. Technician Objectives. GOLD Guidelines. COPD Diagnosis 9/22/2017
 Pharmacist Objectives Pulmonary Update Patty Marshik, PharmD Associate Professor University of New Mexico College of Pharmacy pmarshik@salud.unm.edu Discuss the new Global Initiative for Chronic Obstructive
Pharmacist Objectives Pulmonary Update Patty Marshik, PharmD Associate Professor University of New Mexico College of Pharmacy pmarshik@salud.unm.edu Discuss the new Global Initiative for Chronic Obstructive
Abbreviated Class Review: Chronic Obstructive Pulmonary Disease (COPD)
") Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119 Executive summary: Month/Year of Review: February
Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119 Executive summary: Month/Year of Review: February
reslizumab (Cinqair )
") Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
What do pulmonary function tests tell you?
 Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
GINA. At-A-Glance Asthma Management Reference. for adults, adolescents and children 6 11 years. Updated 2017
 GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
GINA At-A-Glance Asthma Management Reference for adults, adolescents and children 6 11 years Updated 2017 This resource should be used in conjunction with the Global Strategy for Asthma Management and
11/27/18. Challenges in Pulmonary and Critical Care: COPD So Much is New! Faculty. Disclosures
 Challenges in Pulmonary and Critical Care: 2018 COPD So Much is New! 1 Faculty Anas Hadeh, MD, FCCP Director, Pulmonary and Critical Care Medicine Fellowship Program Affiliate Assistant Professor of Clinical
Challenges in Pulmonary and Critical Care: 2018 COPD So Much is New! 1 Faculty Anas Hadeh, MD, FCCP Director, Pulmonary and Critical Care Medicine Fellowship Program Affiliate Assistant Professor of Clinical
II: Moderate Worsening airflow limitations Dyspnea on exertion, cough, and sputum production; patient usually seeks medical
 Table 3.1. Classification of COPD Severity Stage Pulmonary Function Test Findings Symptoms I: Mild Mild airflow limitations +/ Chronic cough and sputum production; patient unaware of abnormal FEV 1 80%
Table 3.1. Classification of COPD Severity Stage Pulmonary Function Test Findings Symptoms I: Mild Mild airflow limitations +/ Chronic cough and sputum production; patient unaware of abnormal FEV 1 80%
Asthma/COPD Update with Inhaler Workshop
 Asthma/COPD Update with Inhaler Workshop October 8, 2017 Nathan Samsa, DO, Pharm D, RPh, FACOI None Disclosures Agenda Asthma Updates COPD Updates Inhaler Workshop Asthma Updates Asthma Updates SMART Trial
Asthma/COPD Update with Inhaler Workshop October 8, 2017 Nathan Samsa, DO, Pharm D, RPh, FACOI None Disclosures Agenda Asthma Updates COPD Updates Inhaler Workshop Asthma Updates Asthma Updates SMART Trial
COPD Prescribing Guidelines
 Cannock Chase Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford and Surrounds Clinical Commissioning Group East Staffordshire Clinical Commissioning
Cannock Chase Clinical Commissioning Group South East Staffordshire and Seisdon Peninsula Clinical Commissioning Group Stafford and Surrounds Clinical Commissioning Group East Staffordshire Clinical Commissioning
New and Novel Medications for Respiratory Care
 New and Novel Medications for Respiratory Care JASON MOORE, PHARM.D. BCCCP CLINICAL STAFF PHARMACIST STORMONT-VAIL HEALTH Objectives Quick overview of the newest FDA-approved repiratory-related medications
New and Novel Medications for Respiratory Care JASON MOORE, PHARM.D. BCCCP CLINICAL STAFF PHARMACIST STORMONT-VAIL HEALTH Objectives Quick overview of the newest FDA-approved repiratory-related medications