Chris Cameron Clinical pharmacologist & General Physician CCDHB. Oxygen- A prescribing Blindspot?
|
|
|
- Mary Moody
- 5 years ago
- Views:
Transcription
1 Chris Cameron Clinical pharmacologist & General Physician CCDHB Oxygen- A prescribing Blindspot?
2 Ms J, 70yo Lives with partner, who has a recent diagnosis of breast cancer Works 3 days a week Weight 46kg Smoker (80 pack year history) Ex tol about 500m on flat Recent admission (May 17) for IECOPD
3 PMHx Severe COPD ICU admission July Spirometry Sept 2014: FEV litres (31%), FVC 61%, FEV1/FVC 42% Last seen by Resp Sept 2014 CT chest (2014) Moderate centrilobular emphysematous change with hyperinflation of the lungs
4 RxHx Bezafibrate 400mg PO nocte Omeprazole 20mg PO mane Salbutamol 100mcg 2 puffs inh BD and PRN q4h Seretide 125/25 2 puffs inh bd Spiriva 18mcg 1 puff inh od Aspirin E.C. 100mg PO od Cholecalciferol 1.25mg PO monthly Dermol ointment, apply to psoriasis occasionally Ensure liquid 1.5kcal/mL - chocolate, 1 BD
5 ICU admission 2012 Not known to be a CO2 retainer Slow respiratory wean - intubated for 12 days Trial of BiPAP resulted in increased agitation and intolerance and so was stopped. Hypercapnic on further ABG's. Documented ICU note that Ms J has significant respiratory disease (COPD with FEV1 0.77). While she was successfully, though slowly, weaned from mechanical ventilation, her underlying lung pathologies are likely to worsen, especially if she continues to smoke. As such, she would be a poor candidate for ICU therapy if she presented to hospital in a number of months time; although they would be happy to discuss this further if the situation does arise.
6 Blood gases in recent admissions Date & time O2 given pco2 PO2 ph 23 June L 44 (A) L 67 (A) Trial of BiPAP unsuccessful Transferred to ICU, intubated and ventilated L 54 (A) July 2012 Extubated 5 July 2012 Date & time O2 given pco2 po2 ph 13 May 2017 unknown 47 (?V) May 2017 unknown 55 (?V)
7 Final admission July PC: Cough, fever, SOB IECOPD, new paf VBG: ph 7.382, pco2 49.9, HCO Bloods: CRP 9, WCC 8.1, Neuts 6.5 ECG: Sinus tachycardia (132)with frequent PACs/PAF. No acute ischaemic changes. CXR: Heart not enlarged. Significant hyperinflation of the chest but no focal consolidation/evidence of failure. Plan: 1) Admit Gen Med 2) Q2H obs - EWS adjusted 3) Further IVF 4) Continue IV Cefuroxime given Penicillin allergy 5) Prophylactic Clexane 6) Monitor heart rate but if does not settle with ABs and further fluid may need rate control - oral short acting metorpolol tartrate. 7) Ca/PO4 and Mg added to bloods. (Unable to add TFTs - repeat bloods mane with TFTs). 8) NRF form signed in discussion with patient.
8
9 Progress July Ms J was steadily improving HR settling, still some paf SW discussions re care for partner Date & time O2 given pco2 po2 ph 14 July (ED) 45% 50 (V) (HCO3 29.6)

10 Then suddenly..
11
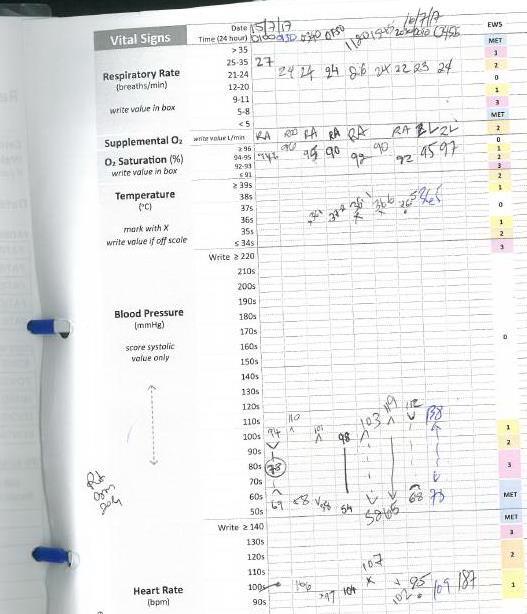
12 What happened? Ms J was started on 2L/min O2 in the early hours of 16 July when her O2 sats were 92% RA After about 4 hours she became restless and HR (AF) She then had a seizure Transferred to HDB Date & time O2 given pco2 po2 ph 16 July L/min 120 (A)

13
14 Time O2 given pco2 po2 ph 0709? 114 (A) L 105 (A)
15 Lessons to be learned No-one appreciated that Ms J was a CO2 retainer This was not on her problem list No O2 therapy was prescribed for her VBGs were used to guide therapy No O2 therapy documented on VBG No Venturi mask was used Signs of CO2 retention not appreciated
16 ABG vs. VBG in COPD Values from VBG: ph ABG=VBG po2 ABG bears no relation to VBG Low po2 can predict CO2 retention pco2 If VBG pco2 <46, then ABG <46 usually If VBG pco2 >46, the ABG pco2 is high, but?how high In COPD patients and others at risk of T2RF, ABGs need to be used to guide O2 therapy. Get some practice. VBGs are not useful in this setting.

17 PML Guidance
18 x 14 July 2017 Venturi Mask 2L-4L/min

19 Do not administer oxygen unless discussed with registrar/smo x
20 Supplemental O2 is an FiO2 > 21% and is a drug (remember RA=21% O2) Type of device Litres O2/minutes FiO2 inhaled When to use Nasal prongs 1L/min 2L/min 3L/min 4L/min 6L/min 24% (0.24) 28% 33% 41% 45% When low flow O2 needed in a patient without CO2 retention. If >4L/min humidification is recommended Hudson mask Venturi mask Non-rebreather mask 4L/min 6L/min 8L/min 2-4L/min 2-4L/min 4-6L/min 6-8L/min 9-10L/min 10-12L/min 12-15L/min 24-28% 31% 35-40% 24% 26% 28% 30% 35% 40% 50% In hypoxic patients without CO2 retention In hypoxic patients with known CO2 retention, or at risk of CO2 retention Upto 15L/min 60-90% In hypoxic patients without CO2 retention
21 Signs of hypercapnia Sedation, comatose Altered mental status, confusion, paranoia, seizures Muscle twitches Vasodilatation of the skin flushed face, strong, bounding pulse Papilloedema Asterixis an easy sign to elicit
22 What did we learn? Supplementary O2 is a drug Supplementary O2 must be prescribed All COPD patients are potential CO2 retainers Education of nursing and junior medical staff is needed
Oxygen and ABG. Dr Will Dooley
 Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Oxygen and ABG G Dr Will Dooley Oxygen and ABGs Simply in 10 cases Recap of: ABG interpretation Oxygen management Some common concerns A-a gradient Base Excess Anion Gap COPD patients CPAP/BiPAP First
Oxygen: Is there a problem? Tom Heaps Acute Physician
 Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
Oxygen: Is there a problem? Tom Heaps Acute Physician Case 1 79-year-old female, diabetic, morbidly obese Admitted with LVF Overnight Reduced GCS?cause 15l NRB in situ ABG showed ph 6.9, pco 2 15.9kPa
Respiratory Medicine. Some pet peeves and other random topics. Kyle Perrin
 Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
Respiratory Medicine Some pet peeves and other random topics Kyle Perrin Overview 1. Acute asthma Severity assessment and management 2. Acute COPD NIV and other management 3. Respiratory problems in the
ALL orders are active unless: 1. Order is manually lined through to inactivate 2. Orders with check boxes ( ) are unchecked DRUG AND TREATMENT ORDERS
 are unchecked DRUG AND TREATMENT ORDERS") DRUG AND TREATMENT Intubation Phase Notify Therapy for STAT intubation Medications SUB Rapid Sequence Induction (SUB)* ***Reminder: Order SUB Rapid Sequence Induction (SUB) on a separate form*** lidocaine
DRUG AND TREATMENT Intubation Phase Notify Therapy for STAT intubation Medications SUB Rapid Sequence Induction (SUB)* ***Reminder: Order SUB Rapid Sequence Induction (SUB) on a separate form*** lidocaine
SIMPLY Arterial Blood Gases Interpretation. Week 4 Dr William Dooley
 SIMPLY Arterial Blood Gases Interpretation Week 4 Dr William Dooley Plan Structure for interpretation 5-step approach Works for majority of cases Case scenarios Some common concerns A-a gradient BE Anion
SIMPLY Arterial Blood Gases Interpretation Week 4 Dr William Dooley Plan Structure for interpretation 5-step approach Works for majority of cases Case scenarios Some common concerns A-a gradient BE Anion
Acute NIV in COPD and what happens next. Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital
 Acute NIV in COPD and what happens next Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital Content Scenarios Evidence based medicine for the first 24 hrs Who should we refer
Acute NIV in COPD and what happens next Dr Rachael Evans PhD Associate Professor, Respiratory Medicine, Glenfield Hospital Content Scenarios Evidence based medicine for the first 24 hrs Who should we refer
Images have been removed from the PowerPoint slides in this handout due to copyright restrictions.
 Arterial Blood Gas Interpretation Routine Assessment Inspection Palpation Auscultation Labs Na 135-145 K 3.5-5.3 Chloride 95-105 CO2 22-31 BUN 10-26 Creat.5-1.2 Glu 80-120 Arterial Blood Gases WBC 5-10K
Arterial Blood Gas Interpretation Routine Assessment Inspection Palpation Auscultation Labs Na 135-145 K 3.5-5.3 Chloride 95-105 CO2 22-31 BUN 10-26 Creat.5-1.2 Glu 80-120 Arterial Blood Gases WBC 5-10K
a. Will not suppress respiratory drive in acute asthma
 Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Status Asthmaticus & COPD with Respiratory Failure - Key Points M.J. Betzner MD FRCPc - NYEMU Toronto 2018 Overview This talk is about the sickest of the sick patients presenting with severe or near death
Tracheostomy Sim Course
 Patients Name: Robert Smith Patients Age / DOB: 45 year old gentleman on medical ward Major Medical Problem Displaced tracheostomy tube Learning Goal Medical Early recognition of displaced tracheostomy
Patients Name: Robert Smith Patients Age / DOB: 45 year old gentleman on medical ward Major Medical Problem Displaced tracheostomy tube Learning Goal Medical Early recognition of displaced tracheostomy
RESPIRATORY FAILURE - CAUSES, CLINICAL INFORMATION, TREATMENT AND CODING CONVENTIONS
 RESPIRATORY FAILURE - CAUSES, CLINICAL INFORMATION, TREATMENT AND CODING CONVENTIONS QUIZ REVIEW The correct answer is in bold font. 1. Hypoxic respiratory failure involves: a. Low oxygen b. High oxygen
RESPIRATORY FAILURE - CAUSES, CLINICAL INFORMATION, TREATMENT AND CODING CONVENTIONS QUIZ REVIEW The correct answer is in bold font. 1. Hypoxic respiratory failure involves: a. Low oxygen b. High oxygen
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
NIV in Acute Respiratory Failure: Where we fail? Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Use of NIV 1998-2010 50 45 40 35 30 25 20 15 10 5 0 1998
Sample Case Study. The patient was a 77-year-old female who arrived to the emergency room on
 Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
Sample Case Study The patient was a 77-year-old female who arrived to the emergency room on February 25 th with a chief complaint of shortness of breath and a deteriorating pulmonary status along with
No Catheter, No CAUTI Scenario 1 Urinary catheter-trauma
 No Catheter, No CAUTI Scenario 1 Urinary catheter-trauma Course lead Colette Laws-Chapman Faculty Course / Curriculum Scenario name No Catheter, No catheter associated urine infection (CAUTI) Scenario
No Catheter, No CAUTI Scenario 1 Urinary catheter-trauma Course lead Colette Laws-Chapman Faculty Course / Curriculum Scenario name No Catheter, No catheter associated urine infection (CAUTI) Scenario
Safer Tracheostomy Care Course
 Patients Name: Samira Patel Patients Age / DOB: 65 year old female on a general ward Major Medical Problem Blocked tracheostomy tube Learning Goal Medical Early recognition of respiratory distress Understanding
Patients Name: Samira Patel Patients Age / DOB: 65 year old female on a general ward Major Medical Problem Blocked tracheostomy tube Learning Goal Medical Early recognition of respiratory distress Understanding
5. What is the cause of this patient s metabolic acidosis? LACTIC ACIDOSIS SECONDARY TO ANEMIC HYPOXIA (HIGH CO LEVEL)
") Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
Self-Assessment RSPT 2350: Module F - ABG Analysis 1. You are called to the ER to do an ABG on a 40 year old female who is C/O dyspnea but seems confused and disoriented. The ABG on an FiO 2 of.21 show:
PHYSICIAN SIGNATURE DATE TIME DRUG ALLERGIES WT: KG
 Available ONLY at: BMC-B BMC-D BMC-N BMC-S Intubation Phase Notify Therapy for STAT intubation SUB Rapid Sequence Induction(SUB)* ***The above subphase is available at the end of the powerplan under the
Available ONLY at: BMC-B BMC-D BMC-N BMC-S Intubation Phase Notify Therapy for STAT intubation SUB Rapid Sequence Induction(SUB)* ***The above subphase is available at the end of the powerplan under the
COPD Challenge CASE PRESENTATION
 Chronic obstructive pulmonary disease (COPD) exacerbations may make up more than 10% of acute medical admissions [1], and they are increasingly recognised as a cause of significant morbidity and mortality
Chronic obstructive pulmonary disease (COPD) exacerbations may make up more than 10% of acute medical admissions [1], and they are increasingly recognised as a cause of significant morbidity and mortality
Allwin Mercer Dr Andrew Zurek
 Allwin Mercer Dr Andrew Zurek 1 in 11 people are currently receiving treatment for asthma (5.4 million people in the UK) Every 10 seconds, someone is having a potentially life-threatening asthma attack
Allwin Mercer Dr Andrew Zurek 1 in 11 people are currently receiving treatment for asthma (5.4 million people in the UK) Every 10 seconds, someone is having a potentially life-threatening asthma attack
ADULT ASTHMA GUIDE SUMMARY. This summary provides busy health professionals with key guidance for assessing and treating adult asthma.
 ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ADULT ASTHMA GUIDE SUMMARY This summary provides busy health professionals with key guidance for assessing and treating adult asthma. Its source document Asthma and Respiratory Foundation NZ Adult Asthma
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv
 Rv") ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) Rv.8.18.18 ACUTE RESPIRATORY DISTRESS SYNDROME (ARDS) SUDDEN PROGRESSIVE FORM OF ACUTE RESPIRATORY FAILURE ALVEOLAR CAPILLARY MEMBRANE BECOMES DAMAGED AND MORE
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX
 MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX") CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX COPD OUTLINE Definition and Overview Pathophysiology Diagnosis and Assessment Therapeutic
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX COPD OUTLINE Definition and Overview Pathophysiology Diagnosis and Assessment Therapeutic
(PLACE PATIENT LABEL HERE) Date: Time: Assessment nurse: Sign: STOP!
 Date: Time: Assessment nurse: Sign: STOP!") ASTHMA BEST CARE BUNDLE P A T H W A Y ADULT ASTHMA Date: Time: Assessment nurse: Sign: INCLUSION CRITERIA Known asthmatic Shortness of breath and / or wheeze EXCLUSION CRITERIA Chronic lung disease other
ASTHMA BEST CARE BUNDLE P A T H W A Y ADULT ASTHMA Date: Time: Assessment nurse: Sign: INCLUSION CRITERIA Known asthmatic Shortness of breath and / or wheeze EXCLUSION CRITERIA Chronic lung disease other
Learning Lessons from Complaints to the Ombudsman Charles Turton. Society for Acute Medicine May 2013
 Learning Lessons from Complaints to the Ombudsman Charles Turton Society for Acute Medicine May 2013 Society for Acute Medicine The Parliamentary and Health Service Ombudsman Final Stage of NHS Complaints
Learning Lessons from Complaints to the Ombudsman Charles Turton Society for Acute Medicine May 2013 Society for Acute Medicine The Parliamentary and Health Service Ombudsman Final Stage of NHS Complaints
Palliative Care In Respirology: Who s job is it, anyway?! Everyones!
 Palliative Care In Respirology: Who s job is it, anyway?! Everyones! Dr. Shalini Nayar MD Respiratory Medicine Palliative Medicine Clinical Assistant Professor, Dept of Medicine, UBC Canadian Cancer Society
Palliative Care In Respirology: Who s job is it, anyway?! Everyones! Dr. Shalini Nayar MD Respiratory Medicine Palliative Medicine Clinical Assistant Professor, Dept of Medicine, UBC Canadian Cancer Society
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo
 62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
62 year old man with a cough! Dr. Aflah Sadikeen Consultant Respiratory Physician Colombo History Mr.KS, a 62 year-old, has been feeling unwell - Worsening cough for the last 5 days - Feels out of breath
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
Management of acute asthma in children in emergency department. Moderate asthma
 152 Moderate asthma SpO2 92% No clinical features of severe asthma NB: If a patient has signs and symptoms across categories, always treat according to their most severe features agonist 2-10 puffs via
152 Moderate asthma SpO2 92% No clinical features of severe asthma NB: If a patient has signs and symptoms across categories, always treat according to their most severe features agonist 2-10 puffs via
Managing Exacerbations of COPD (Version 3.0)
") Managing Exacerbations of COPD (Version 3.0) Guideline Readership This guideline is intended for use in patients with a confirmed diagnosis of a chronic obstructive pulmonary disease (COPD) exacerbation.
Managing Exacerbations of COPD (Version 3.0) Guideline Readership This guideline is intended for use in patients with a confirmed diagnosis of a chronic obstructive pulmonary disease (COPD) exacerbation.
Emergency Department Protocol Initiative
 Emergency Department Protocol Initiative ACUTE ASTHMA MANAGEMENT TOOLKIT March 2006 Provincial Emergency Services Project PHYSICIAN ORDER TEMPLATE FOR CTAS LEVEL 1 ASTHMA ADULT PEDIATRIC Date: Site: Arrival
Emergency Department Protocol Initiative ACUTE ASTHMA MANAGEMENT TOOLKIT March 2006 Provincial Emergency Services Project PHYSICIAN ORDER TEMPLATE FOR CTAS LEVEL 1 ASTHMA ADULT PEDIATRIC Date: Site: Arrival
IDPH ESF-8 Plan: Pediatric and Neonatal Surge Annex Sample Pediatric Admission Orders 2015
 Purpose: To provide guidance to practitioners caring for pediatric patients who need inpatient hospital care during a disaster. Disclaimer: This guideline is not meant to be all inclusive, replace an existing
Purpose: To provide guidance to practitioners caring for pediatric patients who need inpatient hospital care during a disaster. Disclaimer: This guideline is not meant to be all inclusive, replace an existing
COPD exacerbation. Chiara Maruggi, PGY2
 COPD exacerbation Chiara Maruggi, PGY2 Learning objectives At the end of this lecture students will be able to: 1) Critically assess patients for COPD and design a management plan. 2) Develop a step-wise
COPD exacerbation Chiara Maruggi, PGY2 Learning objectives At the end of this lecture students will be able to: 1) Critically assess patients for COPD and design a management plan. 2) Develop a step-wise
OBSERVATION UNIT ASTHMA PATHWAY OUTLINE Westmoreland Hospital PAGE 1 OF 5
 PAGE 1 OF 5 Exclusion Criteria: (Reason to admit to hospital) A. New EKG changes except sinus tachycardia B. Respiratory Rate > 40 C. Signs/symptoms of Heart Failure D. Impending respiratory failure or
PAGE 1 OF 5 Exclusion Criteria: (Reason to admit to hospital) A. New EKG changes except sinus tachycardia B. Respiratory Rate > 40 C. Signs/symptoms of Heart Failure D. Impending respiratory failure or
Non-invasive Ventilation protocol For COPD
 NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
NHS LANARKSHIRE MONKLANDS HOSPITAL Non-invasive Ventilation protocol For COPD April 2017 S Baird Review Date: Oct 2019 Approved by Medical Directorate Indications for Non-Invasive Ventilation (NIV) NIV
Together Everyone Achieves More: Team in Maternity Care Eclamptic Fit
 Together Everyone Achieves More: Team in Maternity Care Eclamptic Fit Course lead Course / Curriculum Scenario name Hannah Rogers / Danielle Nixon Faculty Target Delegates Group Size Newly qualified Nurses
Together Everyone Achieves More: Team in Maternity Care Eclamptic Fit Course lead Course / Curriculum Scenario name Hannah Rogers / Danielle Nixon Faculty Target Delegates Group Size Newly qualified Nurses
Acute respiratory failure
 Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Rita Williams, NP-C, PA PeaceHealth Medical Group Pulmonary & Critical Care Acute respiratory failure Ventilation/perfusion mismatching Most common cause of hypoxemia Normal is 1:1 ratio or 1 Ventilation
Exacerbations of COPD. Dr J Cullen
 Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
CSIM annual meeting Acute respiratory failure. Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018
 CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
CSIM annual meeting - 2018 Acute respiratory failure Dr. John Ronald, FRCPC Int Med, Resp, CCM. October 10, 2018 NRGH affiliated with UBC medicine Disclosures None relevant to this presentation. Also no
Prone ventilation revisited in H1N1 patients
 International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
International Journal of Advanced Multidisciplinary Research ISSN: 2393-8870 www.ijarm.com DOI: 10.22192/ijamr Volume 5, Issue 10-2018 Case Report DOI: http://dx.doi.org/10.22192/ijamr.2018.05.10.005 Prone
2/12/2015. ASTHMA & COPD The Yin &Yang. Asthma General Information. Asthma General Information
 ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
Simulation 1: Two Year-Old Child in Respiratory Distress
 Simulation 1: Two Year-Old Child in Respiratory Distress Opening Scenario (Links to Section 1) You are the respiratory therapist in a 300 bed community hospital working the evening shift. At 8:30 PM you
Simulation 1: Two Year-Old Child in Respiratory Distress Opening Scenario (Links to Section 1) You are the respiratory therapist in a 300 bed community hospital working the evening shift. At 8:30 PM you
Chronic Obstructive Pulmonary Disease (COPD)
") Chronic Obstructive Pulmonary Disease (COPD) Definition of COPD Airflow obstruction that is: o Not fully reversible o Progressive o Does not change markedly over several months Combination of airway and
Chronic Obstructive Pulmonary Disease (COPD) Definition of COPD Airflow obstruction that is: o Not fully reversible o Progressive o Does not change markedly over several months Combination of airway and
Keeping Patients Off the Vent: Bilevel, HFNC, Neither?
 Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Keeping Patients Off the Vent: Bilevel, HFNC, Neither? Robert Kempainen, MD Pulmonary and Critical Care Medicine Hennepin County Medical Center University of Minnesota School of Medicine Objectives Summarize
Asthma Assessment & Review
 ASTHMA RESOURCE PACK Section 5B Asthma Assessment & Review In this section: 1. Primary Care initial assessment and review Asthma Resource Pack Section 5B: Asthma Assessment & Review Version 3.0 Last Updated:
ASTHMA RESOURCE PACK Section 5B Asthma Assessment & Review In this section: 1. Primary Care initial assessment and review Asthma Resource Pack Section 5B: Asthma Assessment & Review Version 3.0 Last Updated:
Disclosure. Learning Objectives. Bernadette Zelaya, RRT. Area Clinical Manager
 High Velocity Nasal Insufflation An Important Therapeutic Approach for Use in the Emergency Department Presented by Vapotherm Accredited for 1 CEU by the American Association for Respiratory Care Provider
High Velocity Nasal Insufflation An Important Therapeutic Approach for Use in the Emergency Department Presented by Vapotherm Accredited for 1 CEU by the American Association for Respiratory Care Provider
Chronic Obstructive Pulmonary Disease (COPD) Measures Document
 Measures Document") Chronic Obstructive Pulmonary Disease (COPD) Measures Document COPD Version: 3 - covering patients discharged between 01/10/2017 and present. Programme Lead: Jo Higgins Clinical Lead: Dr Paul Albert Number
Chronic Obstructive Pulmonary Disease (COPD) Measures Document COPD Version: 3 - covering patients discharged between 01/10/2017 and present. Programme Lead: Jo Higgins Clinical Lead: Dr Paul Albert Number
Mechanical Ventilation Principles and Practices
 Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
Mechanical Ventilation Principles and Practices Dr LAU Chun Wing Arthur Department of Intensive Care Pamela Youde Nethersole Eastern Hospital 6 October 2009 In this lecture, you will learn Major concepts
2 nd Year Revision Respiratory. Michael Hodkinson
 2 nd Year Revision Respiratory Michael Hodkinson Before we start This is a quick run through of topics Obviously there will be more to learn than what s in these slides but hopefully it will provide a
2 nd Year Revision Respiratory Michael Hodkinson Before we start This is a quick run through of topics Obviously there will be more to learn than what s in these slides but hopefully it will provide a
Update in Pulmonology Update in Medicine and Primary Care November 11, 2017
 Update in Pulmonology Update in Medicine and Primary Care November 11, 2017 Denitza P. Blagev, MD Pulmonary & Critical Care Medicine Director, Schmidt Chest Clinic Director, Lung Cancer Screening Program
Update in Pulmonology Update in Medicine and Primary Care November 11, 2017 Denitza P. Blagev, MD Pulmonary & Critical Care Medicine Director, Schmidt Chest Clinic Director, Lung Cancer Screening Program
CASE PRESENTATION VV ECMO
 CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
CASE PRESENTATION VV ECMO Joshua Huelster, MD Fellow in Critical Care Medicine Department of Pulmonary and Critical Care Medicine Hennepin County Medical Center Disclosure There are no conflicts of interest
Printed copies of this document may not be up to date, obtain the most recent version from
 Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Children s Acute Transport Service Clinical Guidelines Acute Severe Asthma Document Control Information Author E Randle Author Position CATS Consultant Document Owner E Polke Document Owner Position Co-ordinator
Salford COPD Treatment Pathway
 Salford COPD Treatment Pathway Development led by Helen Pyne with Salford Asthma and Respiratory Team (SART) Department Respiratory Medicine Salford Royal NHS Foundation Trust Hope Hospital, Stott Lane,
Salford COPD Treatment Pathway Development led by Helen Pyne with Salford Asthma and Respiratory Team (SART) Department Respiratory Medicine Salford Royal NHS Foundation Trust Hope Hospital, Stott Lane,
Pharmaceutical care of patients with infections. Course activities
 Pharmaceutical care of patients with infections Course activities Pharmaceutical care of patients with infections Course activities page 2 Pre-course presentation: Bugs and Drugs 17 Course presentation:
Pharmaceutical care of patients with infections Course activities Pharmaceutical care of patients with infections Course activities page 2 Pre-course presentation: Bugs and Drugs 17 Course presentation:
Thanks to Ben Taylor for his Grand Rounds talk which looks at the problems that may result from whacking on a bit of oxygen.
 EMERGENCY MEDICINE Liverpool Hospital The Weekly Probe 4 th July, 2012 Volume 15, Issue 20 THIS WEEK: 1. Hyperoxia and the perils of oxygen therapy 2. Next week s case 3. Joke of the Week Hyperoxia The
EMERGENCY MEDICINE Liverpool Hospital The Weekly Probe 4 th July, 2012 Volume 15, Issue 20 THIS WEEK: 1. Hyperoxia and the perils of oxygen therapy 2. Next week s case 3. Joke of the Week Hyperoxia The
Acute respiratory failure. Arterial blood gas assessment. finn rasmussen 2011
 Acute respiratory failure Arterial blood gas assessment finn rasmussen 2011 Normal P a CO 2 = 40mmHg Normal P a O 2 = 90-95 mmhg ALVEOLAR VENTILATION Normal HCO 3- = 22-27 mmol/l H + 2 0 CO + 2 H HCO -
Acute respiratory failure Arterial blood gas assessment finn rasmussen 2011 Normal P a CO 2 = 40mmHg Normal P a O 2 = 90-95 mmhg ALVEOLAR VENTILATION Normal HCO 3- = 22-27 mmol/l H + 2 0 CO + 2 H HCO -
Optimize vent weaning and SBT outcomes. Identify underlying causes for SBT failures. Role SBT and weaning protocol have in respiratory care
 Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
Optimize vent weaning and SBT outcomes Identify underlying causes for SBT failures Role SBT and weaning protocol have in respiratory care Lower risk of developing complications Lower risk of VAP, other
WESTMEAD Cardiac QUESTIONS PRACTICE SAQ
 QUESTION 1 A 65-year-old man presents to the emergency department with a history of palpitations. His vital signs are: BP 105/60 mmhg HR 156 beats/min RR 26 /min Temperature 36.2 o C His ECG is on the
QUESTION 1 A 65-year-old man presents to the emergency department with a history of palpitations. His vital signs are: BP 105/60 mmhg HR 156 beats/min RR 26 /min Temperature 36.2 o C His ECG is on the
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES
 DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
DAYTON CHILDREN S HOSPITAL CLINICAL PRACTICE GUIDELINES DISCLAIMER: This Clinical Practice Guideline (CPG) generally describes a recommended course of treatment for patients with the identified health
Candidate. Within the 8 minutes you are required to do the following:
 Candidate You are a member of the paediatrics team. Lisa is a 7 year old girl who has presented to ED with wheeze on a background of known asthma. The emergency department has provided the following information:
Candidate You are a member of the paediatrics team. Lisa is a 7 year old girl who has presented to ED with wheeze on a background of known asthma. The emergency department has provided the following information:
Patient Profile. Patient s details Initials: IF Age: 40 Gender: Male. Weight: 139.7kg Height: 510 metres BMI: >47
 Patient Profile Patient background and medication list Reason for selecting profile Interesting depression case whereby there were several opportunities for intervention as a pharmacist to ensure drug-related
Patient Profile Patient background and medication list Reason for selecting profile Interesting depression case whereby there were several opportunities for intervention as a pharmacist to ensure drug-related
Mechanical Ventilation ศ.พ.ญ.ส ณ ร ตน คงเสร พงศ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล
 Mechanical Ventilation ศ.พ.ญ.ส ณ ร ตน คงเสร พงศ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล Goal of Mechanical Ventilation Mechanical ventilation is any means in which physical device or machines are
Mechanical Ventilation ศ.พ.ญ.ส ณ ร ตน คงเสร พงศ ภาคว ชาว ส ญญ ว ทยา คณะแพทยศาสตร ศ ร ราชพยาบาล Goal of Mechanical Ventilation Mechanical ventilation is any means in which physical device or machines are
ECLS Bridge to Lung Transplantation Optimizing and Ambulating the Recipient
 ECLS Bridge to Lung Transplantation Optimizing and Ambulating the Recipient Shaf Keshavjee MD MSc FRCSC FACS Surgeon-in-Chief, University Health Network James Wallace McCutcheon Chair in Surgery Director,
ECLS Bridge to Lung Transplantation Optimizing and Ambulating the Recipient Shaf Keshavjee MD MSc FRCSC FACS Surgeon-in-Chief, University Health Network James Wallace McCutcheon Chair in Surgery Director,
POST-OP CARDIAC SURGERY PHYSICIAN S ORDER SHEET USE BALLPOINT PEN ONLY. CARDIAC INTENSIVE CARE UNIT
 PHYSICIAN S SHEET Automatically Activate, if not in agreement, cross out and initial Activated by Checking Box ALLERGIES: None known YES Patient s Height: Patient s Weight: ALL MEDICATION and INTRAVENOUS
PHYSICIAN S SHEET Automatically Activate, if not in agreement, cross out and initial Activated by Checking Box ALLERGIES: None known YES Patient s Height: Patient s Weight: ALL MEDICATION and INTRAVENOUS
INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4
 INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4 RESPIRATORY FAILURE Acute respiratory failure is defined by hypoxemia with or without hypercapnia. It is one
INDICATIONS FOR RESPIRATORY ASSISTANCE A C U T E M E D I C I N E U N I T P - Y E A R M B B S 4 RESPIRATORY FAILURE Acute respiratory failure is defined by hypoxemia with or without hypercapnia. It is one
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Objectives. Health care significance of ARF 9/10/15 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION
 TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
TREATMENT OF ACUTE RESPIRATORY FAILURE OF VARIABLE CAUSES: INVASIVE VS. NON- INVASIVE VENTILATION Louisa Chika Ikpeama, DNP, CCRN, ACNP-BC Objectives Identify health care significance of acute respiratory
COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis.
 1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
Lung Transplant Case Presentation
 Lung Transplant Case Presentation Errol L. Bush, MD Assistant Professor of Surgery Heart and Lung Transplantation UCSF Medical Center Update in Advanced Lung Disease May 9, 2015 LP 47y F never smoker w/
Lung Transplant Case Presentation Errol L. Bush, MD Assistant Professor of Surgery Heart and Lung Transplantation UCSF Medical Center Update in Advanced Lung Disease May 9, 2015 LP 47y F never smoker w/
Scenario title. Pear Shaped- prepare for intubation on the ward. Designed for (specific group) ICU MET team. Scenario Design team.
 ICU MET team. Scenario Design team.") Scenario title Pear Shaped- prepare for intubation on the ward Designed for (specific group) ICU MET team Scenario Design team Name Maurice Le Guen Cameron Knott Organisation Austin Hospital Date of creation
Scenario title Pear Shaped- prepare for intubation on the ward Designed for (specific group) ICU MET team Scenario Design team Name Maurice Le Guen Cameron Knott Organisation Austin Hospital Date of creation
Oxygen Workbook Answer book
 Oxygen Workbook Answer book 1 Produced by the Oxygen Steering Group, 2018 2 1. Pre-workbook Quiz 1. Oxygen is a drug? Y N maybe 2. Oxygen is a treatment for? breathlessness hypoxia high carbon dioxide
Oxygen Workbook Answer book 1 Produced by the Oxygen Steering Group, 2018 2 1. Pre-workbook Quiz 1. Oxygen is a drug? Y N maybe 2. Oxygen is a treatment for? breathlessness hypoxia high carbon dioxide
Case Scenarios. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC. Consultant, Critical Care Medicine Medanta, The Medicity
 Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Case Scenarios Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Case 1 A 36 year male with cirrhosis and active GI bleeding is intubated to protect his airway,
Extracorporeal support in acute respiratory failure. Dr Anthony Bastin Consultant in critical care Royal Brompton Hospital, London
 Extracorporeal support in acute respiratory failure Dr Anthony Bastin Consultant in critical care Royal Brompton Hospital, London Objectives By the end of this session, you will be able to: Describe different
Extracorporeal support in acute respiratory failure Dr Anthony Bastin Consultant in critical care Royal Brompton Hospital, London Objectives By the end of this session, you will be able to: Describe different
Bronchodilator Delivery and Nebuliser Trials in Adults
 Bronchodilator Delivery and Nebuliser Trials in Adults Acute Management Favour the use of MDI (+/- Spacer) If considering nebuliser Short term treatment Approx. < 3 weeks See optimisation of inhaled bronchodilators
Bronchodilator Delivery and Nebuliser Trials in Adults Acute Management Favour the use of MDI (+/- Spacer) If considering nebuliser Short term treatment Approx. < 3 weeks See optimisation of inhaled bronchodilators
ACEM Fellowship Examination Emergency Medicine Practice Questions VAQ (Part C)
") ACEM Fellowship Examination Emergency Medicine 2013-14 Practice Questions VAQ (Part C) Question 1 A 67- year- old lady presents to the Emergency Department (ED) with a history of increasing Shortness of
ACEM Fellowship Examination Emergency Medicine 2013-14 Practice Questions VAQ (Part C) Question 1 A 67- year- old lady presents to the Emergency Department (ED) with a history of increasing Shortness of
HEALTH SERVICES POLICY & PROCEDURE MANUAL
 Page 1 of 9 PURPOSE To assure that DOP inmates with Pulmonary Diseases are receiving high quality Primary Care for their condition. POLICY All DOP Primary Care Providers and Chronic Disease Nurses are
Page 1 of 9 PURPOSE To assure that DOP inmates with Pulmonary Diseases are receiving high quality Primary Care for their condition. POLICY All DOP Primary Care Providers and Chronic Disease Nurses are
POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO
 POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO MD (ANAESTHESIOLOGY) FINAL EXAMINATION AUGUST 2013 Date : 2 nd August 2013 Time : 1.00 p.m. 4.00 p.m. Answer any three questions. Answer each question
POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO MD (ANAESTHESIOLOGY) FINAL EXAMINATION AUGUST 2013 Date : 2 nd August 2013 Time : 1.00 p.m. 4.00 p.m. Answer any three questions. Answer each question
Physician Orders ADULT Order Set: Respiratory Failure Orders
 [R] = will be ordered Height: cm Weight: kg Allergies: [ ] No known allergies [ ]Medication allergy(s): [ ] Latex allergy [ ]Other: Admission/Transfer/Discharge [ ] Patient Status Initial Inpatient Attending
[R] = will be ordered Height: cm Weight: kg Allergies: [ ] No known allergies [ ]Medication allergy(s): [ ] Latex allergy [ ]Other: Admission/Transfer/Discharge [ ] Patient Status Initial Inpatient Attending
Permissive hypoxaemia. Mervyn Singer Bloomsbury Institute of Intensive Care Medicine University College London, UK
 Permissive hypoxaemia Mervyn Singer Bloomsbury Institute of Intensive Care Medicine University College London, UK Is mechanical ventilation such a good idea? ventilator-induced lung injury (short- & long-term)
Permissive hypoxaemia Mervyn Singer Bloomsbury Institute of Intensive Care Medicine University College London, UK Is mechanical ventilation such a good idea? ventilator-induced lung injury (short- & long-term)
Approach to type 2 Respiratory Failure
 Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
Approach to type 2 Respiratory Failure Changing Nature of NIV Not longer just the traditional COPD patients Increasingly Obesity Neuromuscular Pneumonias 3 fold increase in patients with Ph 7.25 and below
COPD/Asthma. Prudence Twigg, AGNP
 COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
What is the next best step?
 Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Noninvasive Ventilation William Janssen, M.D. Assistant Professor of Medicine National Jewish Health University of Colorado Denver Health Sciences Center What is the next best step? 65 year old female
Chronic Obstructive Pulmonary Disease Guidelines and updates
 Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
Bronchospasm & SOB. Kim Kilmurray Senior Clinical Teaching Fellow
 Bronchospasm & SOB Kim Kilmurray Senior Clinical Teaching Fellow LEARNING OBJECTIVES Perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identify the spectrum
Bronchospasm & SOB Kim Kilmurray Senior Clinical Teaching Fellow LEARNING OBJECTIVES Perform a comprehensive respiratory examination & link clinical signs to underlying pathology Identify the spectrum
Acid Base Balance by: Susan Mberenga RN, BSN, MSN
 Acid Base Balance by: Susan Mberenga RN, BSN, MSN Acid Base Balance Refers to hydrogen ions as measured by ph Normal range: 7.35-7.45 Acidosis/acidemia: ph is less than 7.35 Alkalosis/alkalemia: ph is
Acid Base Balance by: Susan Mberenga RN, BSN, MSN Acid Base Balance Refers to hydrogen ions as measured by ph Normal range: 7.35-7.45 Acidosis/acidemia: ph is less than 7.35 Alkalosis/alkalemia: ph is
COPD/ Asthma. Dr Heather Lewis Honorary Clinical Lecturer
 COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
Patient demographics Patient name Date of birth Gender NHS number SMITH, Robert (Mr) 01-Feb-1950 Male Verified
 01-Feb-1950 Male Verified") Patient demographics Patient name Date of birth Gender NHS number SMITH, Robert (Mr) 01-Feb-1950 Male Verified - 123 456 7890 Home Address 10 The Lane The Village The County BB22 2CC Phone 01678456789
Patient demographics Patient name Date of birth Gender NHS number SMITH, Robert (Mr) 01-Feb-1950 Male Verified - 123 456 7890 Home Address 10 The Lane The Village The County BB22 2CC Phone 01678456789
Physician Orders ADULT: Asthma and Bronchitis Plan
 Initiate Orders Phase Care Sets/Protocols/PowerPlans Initiate Powerplan Phase, Phase: Asthma and Bronchitis Phase, When to Initiate: Asthma and Bronchitis Phase Non Categorized Problem: Asthma Problem:
Initiate Orders Phase Care Sets/Protocols/PowerPlans Initiate Powerplan Phase, Phase: Asthma and Bronchitis Phase, When to Initiate: Asthma and Bronchitis Phase Non Categorized Problem: Asthma Problem:
Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe )
") PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
PROTOCOL Sedation Hold/Interruption and Weaning Protocol ( Wake-up and Breathe ) Page 1 of 6 Scope: Population: Outcome: Critical care clinicians and providers. All ICU patients intubated or mechanically
Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE
 VAPOTHERM POCKET GUIDE") Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE Indications for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) administration, the patient should be: Spontaneously
Emergency Medicine High Velocity Nasal Insufflation (Hi-VNI) VAPOTHERM POCKET GUIDE Indications for Vapotherm High Velocity Nasal Insufflation (Hi-VNI ) administration, the patient should be: Spontaneously
Index No. All five (05) questions should be answered. All questions carry equal marks.
 questions should be answered. All questions carry equal marks.") POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO POSTGRADUATE DIPLOMA IN TUBERCULOSIS & CHEST DISEASES EXAMINATION - MAY 2016 Date :- 4 th May 2016 PAPER I CASE HISTORIES Time :- 9.00 a.m. -11.00
POSTGRADUATE INSTITUTE OF MEDICINE UNIVERSITY OF COLOMBO POSTGRADUATE DIPLOMA IN TUBERCULOSIS & CHEST DISEASES EXAMINATION - MAY 2016 Date :- 4 th May 2016 PAPER I CASE HISTORIES Time :- 9.00 a.m. -11.00
Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning
 CME article Johnson S, et al: Noninvasive ventilation Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning Saumy Johnson, Ramesh Unnikrishnan * Email: ramesh.unnikrishnan@manipal.edu
CME article Johnson S, et al: Noninvasive ventilation Noninvasive ventilation: Selection of patient, interfaces, initiation and weaning Saumy Johnson, Ramesh Unnikrishnan * Email: ramesh.unnikrishnan@manipal.edu
OXYGEN USE IN PHYSICAL THERAPY PRACTICE. Rebecca H. Crouch, PT,DPT,MS,CCS,FAACVPR
 OXYGEN USE IN PHYSICAL THERAPY PRACTICE Rebecca H. Crouch, PT,DPT,MS,CCS,FAACVPR Supplemental Oxygen Advantages British Medical Research Council Clinical Trial Improved survival using oxygen 15 hrs/day
OXYGEN USE IN PHYSICAL THERAPY PRACTICE Rebecca H. Crouch, PT,DPT,MS,CCS,FAACVPR Supplemental Oxygen Advantages British Medical Research Council Clinical Trial Improved survival using oxygen 15 hrs/day
2/4/2019. GOLD Objectives. GOLD 2019 Report: Chapters
 GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
Diagnosis and Management of Acute Respiratory Failure
 Diagnosis and Management of Acute Respiratory Failure Steven B. Leven, M.D., F.C.C.P. Clinical Professor, Pulmonary/Critical Care Medicine UCI Director MICU and Respiratory Therapy, UCI Medical Center
Diagnosis and Management of Acute Respiratory Failure Steven B. Leven, M.D., F.C.C.P. Clinical Professor, Pulmonary/Critical Care Medicine UCI Director MICU and Respiratory Therapy, UCI Medical Center
If you require this document in another format such as Braille, large print, audio or another language please contact the Trusts Communications Team
 MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) IN ADULTS Summary statement: How does the document support patient care? Staff/stakeholders involved in development: Job titles only Division:
MANAGEMENT OF CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) IN ADULTS Summary statement: How does the document support patient care? Staff/stakeholders involved in development: Job titles only Division:
Haut debit nasal ou BiPAP? Laurent Brochard Toronto
 Haut debit nasal ou BiPAP? Laurent Brochard Toronto Conflicts of interest Our clinical research laboratory has received research grants for clinical trials from the following companies: General Electric
Haut debit nasal ou BiPAP? Laurent Brochard Toronto Conflicts of interest Our clinical research laboratory has received research grants for clinical trials from the following companies: General Electric
Chronic Obstructive Pulmonary Disease (COPD) Copyright 2014 by Mosby, an imprint of Elsevier Inc.
 Copyright 2014 by Mosby, an imprint of Elsevier Inc.") Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic
 COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic Learning Objectives Know the adverse effects of COPD exacerbations Know mainstays
COPD: From Hospital to Home October 5, 2015 Derek Linderman, MD Associate Professor COPD Center Pulmonary Nodule Clinic Learning Objectives Know the adverse effects of COPD exacerbations Know mainstays
BRONCHIOLITIS. See also the PSNZ guideline - Wheeze & Chest Infections in infants under 1 year (www.paediatrics.org.nz)
") Definition What is Bronchiolitis? Assessment Management Flow Chart Admission Guidelines Investigations Management Use of Bronchodilators Other treatments Discharge Planning Bronchiolitis & Asthma References
Definition What is Bronchiolitis? Assessment Management Flow Chart Admission Guidelines Investigations Management Use of Bronchodilators Other treatments Discharge Planning Bronchiolitis & Asthma References
AT TRIAGE. Alberta Acute Childhood Asthma Pathway: Evidence based* recommendations For Emergency / Urgent Care
 1 1 Should the child be placed into the Pathway? Asthma Clinical Score (PRAM) Inclusion Children 1 year and 18 years of age who present with wheezing and respiratory distress, and have been diagnosed by
1 1 Should the child be placed into the Pathway? Asthma Clinical Score (PRAM) Inclusion Children 1 year and 18 years of age who present with wheezing and respiratory distress, and have been diagnosed by
NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP)
") Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive
Introduction NIV - BI-LEVEL POSITIVE AIRWAY PRESSURE (BIPAP) Noninvasive ventilation (NIV) is a method of delivering oxygen by positive pressure mask that allows for the prevention or postponement of invasive