INHALED ANTIBIOTICS THERAPY IN NON-CF LUNG DISEASE
|
|
|
- Norma McKenzie
- 5 years ago
- Views:
Transcription





1 INHALED ANTIBIOTICS THERAPY IN NON-CF LUNG DISEASE Hannah Blau MBBS Pulmonary Institute and Graub CF Center SCHNEIDER CHILDREN S MEDICAL CENTER OF ISRAEL Chipap 18 th February 2015

2 Inhaled antibiotic therapy: Direct delivery to the airways High local drug concentration Low systemic concentration more efficacious With less side effects

3 Inhaled antibiotics Standard treatment for CF with chronic PA colonization Up to 25% non CF bronchiectasis are colonized with PA thus this may be a good therapy. Far less advanced studies or clinical experience
4 At Schneider s, used for many years for non CF lung disease
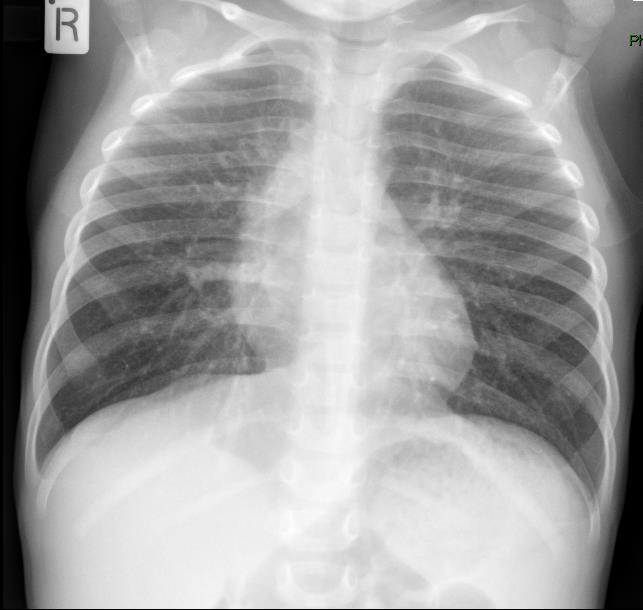
5 Case 1 At 10 months, malignant ependymoma posterior fossa resected + radiation Vocal cord paralysis, no gag reflex Tracheostomy, PEG Chronic severe lung disease: O2 saturation dropped to 70%, Oxygen dependent Sputum culture: P. aeruginosa, P. putida, S. aureus, S.pneumonia, K. pneumonia, S. maltophilia

6

7 18 months inhaled colistin 1 X10 6 units x2/day Oral Cipro/cefuroxime/ flagyl Occasional hospitalizations For IV antibiotics Physiotherapy Ventolin, aerovent, budes 2011

8 No longer oxygen dependent Gag returned Still vocal cord paralysis Still on intermittent Cipro And inhaled colistin - thus avoids hospitalization Chronic lung disease 2014
9 Case 2 Diagnosed in infancy with pseudohypoaldosteronism type 1 (ENaC, epithelial sodium channel defect). PICU with RSV at age 2 months. Ventilated 2 more PICU admissions Recurrent severe respiratory distress. Frequent hospitalizations Sputum: P. mirabilis, chronic P. aeruginosa, K. oxytoca, S. aureus, Providencia

10 Severe hyperinflation, atelectasis during RSV Life threatening hyperkalemia Treatment: Kexalate IV antibiotics Then maintained on: Inhaled colistin Oral ciprofloxacint Physiotherapy Hypertonic saline inh aerovent

11 Chronic lung disease Inhlaed colistin for 20 months And later, intermittent
12 Nov 2014
13 Aim: to review inhaled antibiotic use at Schneider s Included: patients followed in Pulmonary Unit non-cf chronic lung disease Chose colistin inhalation as the index drug Excluded: single consults e.g. oncology, inpatients; those where prescribed but not taken; those without bacterial culture Sputum cultures: by expectoration, or induced sputum with suction + physiotherapy
14 Demographics 29 patients, 18 male 14 chronic therapy (>2 months) 5 recurrent intermittent, 1-2 mths each cycle 10 short term (< 2 months)
15 Age range: y
16 Diagnoses, n=29 Bronchiectasis: 14 PCD: 6 Post adenovirus: 2 Post liver transplant: 1 Idiopathic: 3 Pseudohypoaldosteronism: 2 Immune disorder: 3 Recurrent aspiration pneumonia 12 Congenital myopathy: 4 Neurodegenerative or HIE: 6 Vocal chord paralysis 1 FD: 1
17 Diagnoses <5y (n=10) Myopathy 2 Neurodegenerative 3 Vocal cord paralysis (ependymoma) 1 Immune deficiency 2 Pseudohypoaldost 2
18 Bacterial infection P. aeruginosa 28/29 Co-infection or subsequent cultures: K. pneumonia Enterobacter Acinetobacter S. aureus, S. pneumonia, H. influenza S. maltophilia P. mirabilis Serratia
19 months of therapy 70 Months of Inhaled Colistin: patients with chronic P. aeruginosa subjects
20 Eradication of P. aeruginosa Of 14 with short term or intermittent infection, 11 were eradicated Of 15 with persistent or chronic infection, only 9 were eradicated Subjective improvement: In most cases, at least temporarily

21 Non- CF Bronchiectasis - common: 1:20,000 in the young to 1:200 >75yo - underdiagnosed ( asthma, COPD ) - high morbidity - reduced HrQoL - management: few RCT mainly from consensus expert opinion or extrapolated from CF


22 Vicious cycle impaired mucociliary clearance chronic infection and colonization inflammatory response that persists even after infection has been controlled progressive small airways obstruction
23 Dysregulation of both innate and adaptive immunity A complex series of inter-related events leading to increased airway pro-inflammatory cytokines (e.g. TNF-α, IL-1 and IL-8), neutrophil recruitment and migration.
24 Antibiotics for bronchiectasis: British Thoracic Society guidelines Cornerstone of treatment for Acute exacerbations Prophylaxis to prevent exacerbations Sputum cultures are important Colonization / chronic infection = same microorganism, > 3 cultures >1 mth apart over 6mth H. influenza and S. Pneumonia are common S. aureus and P. aeruginosa if present must be addressed

25 Antibiotics for bronchiectasis (British Guidelines, 2010) For acute exacerbations with P. aeruginosa: d p.o.. - Give IV if no response or sensitive only to IV antibiotics - Suggested protocol to eradicate PA:
26 Long term nebulized antibiotics in non CF bronchiectasis British Guidelines 2010 Patients with chronic PA: admissions, QOL and may have accelerated FEV1 Aim: improve symptoms reduce exacerbations deliver high dose directly to airway, little systemic toxicity bacterial burden, disrupt vicious cycle infection- inflammation choice of antibiotic guided by sensitivities Need further studies.
27 Development chronic Pseudomonas aeruginosa lung infection Mucoid strain Birth 1 st infection Negative sputum cultures Antibiotics Repeated infections Poorer prognosis Recurrent infection Chronic infection



28 Infection James A. Sullivan
29

30 Evolutionary Role for Biofilms? A mechanism for anchoring to a solid surface and facilitating persistence in a turbulent aqueous environment
31 Mechanisms of Colonization Impaired mucociliary clearance Impaired antimicrobial activity Antibacterial proteins Increased adherence CFTR Impaired phagocytosis
32 The Inflammatory Response in CF pmn IL-8 IL-6 macrophage Elastase MPO IL-8 TNF- IL-8 IL-1 respiratory epithelium
33 Inhaled antibiotics for non-cf bronchiectases Previously: extrapolation from evidence in CF Recently: several large randomized trials in Bx Phase 3 trials for colistin, aztreonam
34 Inhaled antibiotics for stable non CF bronchiectasis. ERJ review. Brodt AM, June 2014 Meta-analysis of RCT including Cochrane airways group register 12 RCT in 1264 adults (5 unpublished) 8 RCT in 590 adults were used Inhaled amikacin, aztreonam ciprofloxacin, gentamicin, colistin or tobramycin for 4w 12mth
35 Inhaled antibiotics for stable non CF bronchiectasis. ERJ review. Brodt AM, June 2014 sputum bacterial load log10 CFU/g Eradicated bacteria : risk ratio 4.2, 95% CI exacerbations: risk ratio 0.72, 95% CI Bronchospasm in 10% (controls 2.3%) but same withdrawal rate due to adverse events Emerging resistance: 7.8% vs 3.5% in controls (NS)
36 Effect on reduction of PA sputum load
37 Inhaled antibiotics and PA eradication
38 Inhaled antibiotics for stable non CF bronchiectasis. ERJ review. Brodt AM, June 2014 Concluded: Inhaled antibiotics may provide an effective suppressive therapy with acceptable safety profile in adults with stable non CF bronchiectasis and chronic bronchial infection
39 Nebulized antibiotics for bronchiectases Tobramycin shown to be effective reduce PA colony density; improve symptoms; decrease hospitalizations and LOS; variable rates of prolonged eradication Recurrence of PA on withdrawal almost universal
40 Inhaled Gentamicin in non CF bronchiectasis. Murray MP. Am J Resp Crit Care Med 2011 RPCT, n= 65, gentamicin 80mg bid fo r 12mth Reduced sputum bacterial density 30.8% eradication PA, 92.8% for other pathogens; less sputum purulence (p<0.0001) Fewer exacerbations: 0 vs 1.5; increased time to 1 st exacerbation: 120 vs 61.5d, p=0.02 Improved LCQ and StGeorge Resp Q (p<0.004) No difference in lung function No resistance developed At follow up all returned to baseline. Needs to be continuous


41 Inhaled dual release inhaled liposomal ciprofloxacin for non-cf bronchiectasis. Bilton D, Thorax 2013 Phase II, 24w, ANZ multicenter RDBPCT; N=42 adults with >2 exacerbations in past yr and Cipro-sensitive PA Cipro qd for 3, 28d on/off cycles over 6m Primary outcome: bacterial density dropped 4.2 log10 vs -0.08, p=0.002, at 28d Secondary outcomes: well tolerated; Time to 1 st exacerbation 134 vs 58d (p=0.06)
42 AIR-Bx trials, Gilead. Inh aztreonam 75mg tid via eflow, Lancet Resp Sep 2014, Barker AF Multicenter multinational, RDBPCT 2 on/off cycles of 28 days vs placebo BX1, n=266 ( 134 Az); BX2, n= 274 (136 Az); Bacterial load decreased BUT Primary outcome: change in QOL-B to day 28 Secondary outcome: change in QOL-B to day 84; time to 1 st exacerbation Not significant. Increased adverse events
43 Why did the aztreonam study fail when it succeeded in CF Bronchiectasis, losing the battle but winning the war. JD Chalmers. Lancet Resp. Sep 2014 editorial QOL Bx RSS: is this the best outcome? Very mixed population (1/3 had COPD in aztreonam group and only 19% in placebo gp) Different gram negative bacteria Range of patient severity Underpowered to detect frequency of exacerbations too short; 1/3 of patients had no exacerbations previous year
44 Colistin RCT for non cf N=140,RPCT, colistin 1 million IU BD for 6mth within 21d of anti PA exacerbation Rx using I- neb, breath activated vibrating mesh with adherence download. PA bacterial density Well tolerated QOL improvement Just failed to meet primary end point: time to next exacerbation, (placebo group had less exacerbations than expected; underpowered) bronchiectases
45 Nebulized colistin for non cf bronchiectasis. Déjà vu all over again? Matersky and O Donnell,Editorial AJRCCM 2014 There are no drugs approved by the FDA for non CF bronchiectasis.. In contrast to CF where several agents improve survival, QOL and exacerbations We can t just extrapolate BUT
46 Suggested causes of failure: Slavishly following CF care models not applicable to NCFB Heterogeneity of population Optimal endpoints not found yet Bacterial density does not necessarily reflect clinical outcome e.g. symptoms; exacerbations Lack of basic and translational research in NCFB No animal model
47 Causes for optimism Increasing recognition fo the worldwide scope of the problem More publications recently Guidelines for evaluation and care New delivery devices for less toxicity
48 Lessons learned for future studies Need high quality phenotype to identify populations that can benefit and tolerate inhaled antibiotics Probably best to target more severe, most likely to benefit (recent: bronchiectasis severity index) COPD related bronchiectasis needs better definition and characterisation Need international registries e.g COPD foundation s bronchiectasis research registry in the USA ERS s EMBARC registry
49 Finally Bronchiectasis is not cystic fibrosis Dnase, effective in CF, caused increased exacerbations and drop in FEV1 in bronchiectasis TOBI failed because of toxicity May need different antibiotic doses
50 Speaking practically.. clinicians should personalize care, combining antibiotics with different therapies and including airway clearance
51
CCLI. Bronchiectasis Treatment Antibiotics. Charles Haworth. Physician / Patient Conference, Georgetown University, May 2017
 Physician / Patient Conference, Georgetown University, May 2017 Bronchiectasis Treatment Antibiotics Charles Haworth CCLI Cambridge Centre for Lung Infection Disclosures Educational talks and / or consultancy
Physician / Patient Conference, Georgetown University, May 2017 Bronchiectasis Treatment Antibiotics Charles Haworth CCLI Cambridge Centre for Lung Infection Disclosures Educational talks and / or consultancy
Inhaled Antibiotics in Non-CF. Dr Michael Loebinger Host Defence Unit Royal Brompton Hospital London, United Kingdom
 Inhaled Antibiotics in Non-CF Dr Michael Loebinger Host Defence Unit Royal Brompton Hospital London, United Kingdom Advantages Increased drug concentrations locally Reduced systemic adverse effects Home
Inhaled Antibiotics in Non-CF Dr Michael Loebinger Host Defence Unit Royal Brompton Hospital London, United Kingdom Advantages Increased drug concentrations locally Reduced systemic adverse effects Home
Update on bronchiectasis guidelines. James Chalmers MD, PhD, FRCPE, FERS University of Dundee, UK
 Update on bronchiectasis guidelines James Chalmers MD, PhD, FRCPE, FERS University of Dundee, UK University of Dundee Bronchiectasis guidelines 2017 2010 2006 2008 2015 2015 Currently valid guidelines
Update on bronchiectasis guidelines James Chalmers MD, PhD, FRCPE, FERS University of Dundee, UK University of Dundee Bronchiectasis guidelines 2017 2010 2006 2008 2015 2015 Currently valid guidelines
Efficacy of Pseudomonas aeruginosa eradication regimens in bronchiectasis
 Efficacy of Pseudomonas aeruginosa eradication regimens in bronchiectasis Vallières, E., Tumelty, K., Tunney, M. M., Hannah, R., Hewitt, O., Elborn, J. S., & Downey, D. G. (2017). Efficacy of Pseudomonas
Efficacy of Pseudomonas aeruginosa eradication regimens in bronchiectasis Vallières, E., Tumelty, K., Tunney, M. M., Hannah, R., Hewitt, O., Elborn, J. S., & Downey, D. G. (2017). Efficacy of Pseudomonas
Bronchiectasis exacerbations; differences and management. Michael Loebinger Royal Brompton Imperial College
 Bronchiectasis exacerbations; differences and management Michael Loebinger Royal Brompton Imperial College Plan Bronchiectasis background and burden Exacerbation and Management Longer term Management Cases
Bronchiectasis exacerbations; differences and management Michael Loebinger Royal Brompton Imperial College Plan Bronchiectasis background and burden Exacerbation and Management Longer term Management Cases
Dr Conroy Wong. Professor Richard Beasley. Dr Sarah Mooney. Professor Innes Asher
 Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
Professor Richard Beasley University of Otago Director Medical Research Institute of New Zealand Wellington Dr Sarah Mooney Physiotherapy Advanced Clinician Counties Manukau Health NZ Respiratory and Sleep
Appendix D Clinical specialist statement template
 Appendix D Colistimethate sodium powder and tobramycin powder for inhalation for the treatment of pseudomonas lung infection in cystic fibrosis Thank you for agreeing to give us a statement on your organisation
Appendix D Colistimethate sodium powder and tobramycin powder for inhalation for the treatment of pseudomonas lung infection in cystic fibrosis Thank you for agreeing to give us a statement on your organisation
Inhalational antibacterial regimens in non-cystic fibrosis patients. Jeff Alder Bayer HealthCare
 Inhalational antibacterial regimens in non-cystic fibrosis patients Jeff Alder Bayer HealthCare Alder - Inhaled therapy for non-cf - EMA 25-26 Oct 2012 1 Inhalational antibacterials: two approaches 1.
Inhalational antibacterial regimens in non-cystic fibrosis patients Jeff Alder Bayer HealthCare Alder - Inhaled therapy for non-cf - EMA 25-26 Oct 2012 1 Inhalational antibacterials: two approaches 1.
Cystic Fibrosis the future
 Cystic Fibrosis the future Pathophysiologic cascade Abnormal Gene Abnormal CFTR Therapy Gene replacement Protein replacement Gene read through therapy Abnormal sodium chloride & water movement through
Cystic Fibrosis the future Pathophysiologic cascade Abnormal Gene Abnormal CFTR Therapy Gene replacement Protein replacement Gene read through therapy Abnormal sodium chloride & water movement through
Bronchiectasis it s effects on the NZ population and what we can do to address this
 NZ Respiratory Conference - 2017 Bronchiectasis it s effects on the NZ population and what we can do to address this Conroy Wong Middlemore Hospital Auckland, NZ Bronchiectasis in NZ and new developments
NZ Respiratory Conference - 2017 Bronchiectasis it s effects on the NZ population and what we can do to address this Conroy Wong Middlemore Hospital Auckland, NZ Bronchiectasis in NZ and new developments
Inhaled antibiotics for stable non-cystic fibrosis bronchiectasis: a systematic review
 ORIGINAL ARTICLE BRONCHIECTASIS Inhaled antibiotics for stable non-cystic fibrosis bronchiectasis: a systematic review Alessandra Monteiro Brodt 1, Elizabeth Stovold 2 and Linjie Zhang 1 Affiliations:
ORIGINAL ARTICLE BRONCHIECTASIS Inhaled antibiotics for stable non-cystic fibrosis bronchiectasis: a systematic review Alessandra Monteiro Brodt 1, Elizabeth Stovold 2 and Linjie Zhang 1 Affiliations:
What is Cystic Fibrosis? CYSTIC FIBROSIS. Genetics of CF
 What is Cystic Fibrosis? CYSTIC FIBROSIS Lynne M. Quittell, M.D. Director, CF Center Columbia University Chronic, progressive and life limiting autosomal recessive genetic disease characterized by chronic
What is Cystic Fibrosis? CYSTIC FIBROSIS Lynne M. Quittell, M.D. Director, CF Center Columbia University Chronic, progressive and life limiting autosomal recessive genetic disease characterized by chronic
Cystic fibrosis: From childhood to adulthood. Eitan Kerem Department of Pediatrics and CF Center Hadassah University Hospital Jerusalem Israel
 Cystic fibrosis: From childhood to adulthood Eitan Kerem Department of Pediatrics and CF Center Hadassah University Hospital Jerusalem Israel Vas deference H 2 O Cl - Na + H 2 O Na + Cl - Cl - Cl -
Cystic fibrosis: From childhood to adulthood Eitan Kerem Department of Pediatrics and CF Center Hadassah University Hospital Jerusalem Israel Vas deference H 2 O Cl - Na + H 2 O Na + Cl - Cl - Cl -
Journal Club The ELITE Trial. Sandra Katalinic, Pharmacy Resident University Hospital of Northern British Columbia April 28, 2010
 Journal Club The ELITE Trial Sandra Katalinic, Pharmacy Resident University Hospital of Northern British Columbia April 28, 2010 Overview Journal article Title, journal, authors, funding Abstract Introduction
Journal Club The ELITE Trial Sandra Katalinic, Pharmacy Resident University Hospital of Northern British Columbia April 28, 2010 Overview Journal article Title, journal, authors, funding Abstract Introduction
"Management and Treatment of Patients with Cystic fibrosis (CF)
") "Management and Treatment of Patients with Cystic fibrosis (CF) Dr. Malena Cohen-Cymberknoh Pediatric Pulmonology and CF Center Hadassah Hebrew-University Medical Center Jerusalem, Israel Afula, March
"Management and Treatment of Patients with Cystic fibrosis (CF) Dr. Malena Cohen-Cymberknoh Pediatric Pulmonology and CF Center Hadassah Hebrew-University Medical Center Jerusalem, Israel Afula, March
NON-CF BRONCHIECTASIS IN ADULTS
 Séminaire de Pathologie Infectieuse Jeudi 25 juin 2008 Cliniques Universitaires UCL de Mont-Godinne, Yvoir NON-CF BRONCHIECTASIS IN ADULTS Dr Robert Wilson Royal Brompton Hospital, London, UK Aetiology
Séminaire de Pathologie Infectieuse Jeudi 25 juin 2008 Cliniques Universitaires UCL de Mont-Godinne, Yvoir NON-CF BRONCHIECTASIS IN ADULTS Dr Robert Wilson Royal Brompton Hospital, London, UK Aetiology
Bronchiectasis. Grant Waterer. Professor of Medicine, University of Western Australia Adjunct Professor of Medicine, Northwestern University, Chicago
 Bronchiectasis Grant Waterer MBBS PhD MBA FRACP FCCP Professor of Medicine, University of Western Australia Adjunct Professor of Medicine, Northwestern University, Chicago Conflicts of Interest I have
Bronchiectasis Grant Waterer MBBS PhD MBA FRACP FCCP Professor of Medicine, University of Western Australia Adjunct Professor of Medicine, Northwestern University, Chicago Conflicts of Interest I have
Conference Bronchiectasis A Growing Problem
 Conference 2015 Bronchiectasis A Growing Problem Bronchiectasis (in Children) What is it? Why such a concern in NZ? What to look out for? Management Positives? Just a note that the bar for diagnosis, referral
Conference 2015 Bronchiectasis A Growing Problem Bronchiectasis (in Children) What is it? Why such a concern in NZ? What to look out for? Management Positives? Just a note that the bar for diagnosis, referral
HOW DISEASE ALTERING THERAPY IS CHANGING THE GOALS OF TREATMENT IN CF
 HOW DISEASE ALTERING THERAPY IS CHANGING THE GOALS OF TREATMENT IN CF Peter D. Sly MBBS, MD, FRACP, DSc OUTLINE Goals of CF treatment Drivers of early disease neutrophilic inflammation oxidative stress
HOW DISEASE ALTERING THERAPY IS CHANGING THE GOALS OF TREATMENT IN CF Peter D. Sly MBBS, MD, FRACP, DSc OUTLINE Goals of CF treatment Drivers of early disease neutrophilic inflammation oxidative stress
Management of bronchiectasis in adults
 STATE OF THE ART MANAGEMENT OF BRONCHIECTASIS IN ADULTS Management of bronchiectasis in adults James D. Chalmers 1, Stefano Aliberti 2 and Francesco Blasi 3 Affiliations: 1 Tayside Respiratory Research
STATE OF THE ART MANAGEMENT OF BRONCHIECTASIS IN ADULTS Management of bronchiectasis in adults James D. Chalmers 1, Stefano Aliberti 2 and Francesco Blasi 3 Affiliations: 1 Tayside Respiratory Research
Marcos I. Restrepo, MD, MSc, FCCP
 Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
Thank you for viewing this presentation. We would like to remind you that this material is the property of the author. It is provided to you by the ERS for your personal use only, as submitted by the author.
The management of bronchiectasis in Europe
 The management of bronchiectasis in Europe Data from the European Bronchiectasis Registry James Chalmers University of Dundee, UK Presenter disclosures Clinical Trials AstraZeneca, Aradigm corporation,
The management of bronchiectasis in Europe Data from the European Bronchiectasis Registry James Chalmers University of Dundee, UK Presenter disclosures Clinical Trials AstraZeneca, Aradigm corporation,
Clinical Study Synopsis
 Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
You Can Observe a Lot By Just Watching. Wayne J. Morgan, MD, CM
 You Can Observe a Lot By Just Watching Wayne J. Morgan, MD, CM Disclosures Genentech Epidemiological Study of Cystic Fibrosis, Scientific Advisory Group CF Foundation Data Safety Monitoring Board Registry/Comparative
You Can Observe a Lot By Just Watching Wayne J. Morgan, MD, CM Disclosures Genentech Epidemiological Study of Cystic Fibrosis, Scientific Advisory Group CF Foundation Data Safety Monitoring Board Registry/Comparative
Bronchiectasis Domiciliary treatment. Prof. Adam Hill Royal Infirmary and University of Edinburgh
 Bronchiectasis Domiciliary treatment Prof. Adam Hill Royal Infirmary and University of Edinburgh Plan of talk Background of bronchiectasis Who requires IV antibiotics Domiciliary treatment Results to date.
Bronchiectasis Domiciliary treatment Prof. Adam Hill Royal Infirmary and University of Edinburgh Plan of talk Background of bronchiectasis Who requires IV antibiotics Domiciliary treatment Results to date.
CYSTIC FIBROSIS OBJECTIVES NO CONFLICT OF INTEREST TO DISCLOSE
 CYSTIC FIBROSIS Madhu Pendurthi MD MPH Staff Physician, Mercy Hospital Springfield, MO NO CONFLICT OF INTEREST TO DISCLOSE OBJECTIVES Epidemiology of Cystic Fibrosis (CF) Genetic basis and pathophysiology
CYSTIC FIBROSIS Madhu Pendurthi MD MPH Staff Physician, Mercy Hospital Springfield, MO NO CONFLICT OF INTEREST TO DISCLOSE OBJECTIVES Epidemiology of Cystic Fibrosis (CF) Genetic basis and pathophysiology
Cystic Fibrosis: Progress in Treatment Management. Patrick A. Flume, M.D. Medical University of South Carolina
 Cystic Fibrosis: Progress in Treatment Management Patrick A. Flume, M.D. Medical University of South Carolina Disclosures Grant support Mpex Pharmaceuticals, Inc Gilead Sciences, Inc Bayer Healthcare AG
Cystic Fibrosis: Progress in Treatment Management Patrick A. Flume, M.D. Medical University of South Carolina Disclosures Grant support Mpex Pharmaceuticals, Inc Gilead Sciences, Inc Bayer Healthcare AG
Shared Care Guideline
 Shared Care Guideline Gentamicin for Nebulisation For the long term prophylaxis of chronic lung infections in non CF bronchiectasis Executive Summary Indication Nebulised gentamicin is indicated in patients
Shared Care Guideline Gentamicin for Nebulisation For the long term prophylaxis of chronic lung infections in non CF bronchiectasis Executive Summary Indication Nebulised gentamicin is indicated in patients
Respiratory Pharmacology: Treatment of Cystic Fibrosis
 Respiratory Pharmacology: Treatment of Cystic Fibrosis Dr. Tillie-Louise Hackett Department of Anesthesiology, Pharmacology and Therapeutics University of British Columbia Associate Head, Centre of Heart
Respiratory Pharmacology: Treatment of Cystic Fibrosis Dr. Tillie-Louise Hackett Department of Anesthesiology, Pharmacology and Therapeutics University of British Columbia Associate Head, Centre of Heart
Inhaled antibiotics to treat NTM* lung infections
 Inhaled antibiotics to treat NTM* lung infections *Nontuberculous Mycobacteria Lung Infection October 17, 2017 thofmann@qrumpharma.com Topics Why inhaled abx? - History in TB/NTM - Obstacles - Challenges
Inhaled antibiotics to treat NTM* lung infections *Nontuberculous Mycobacteria Lung Infection October 17, 2017 thofmann@qrumpharma.com Topics Why inhaled abx? - History in TB/NTM - Obstacles - Challenges
Pseudomonas aeruginosa eradication guideline
 SCOTTISH PAEDIATRIC CYSTIC FIBROSIS MCN Pseudomonas aeruginosa eradication guideline Date Created: 27 th June 2013 Date Approved by Steering Group: 30 th May 2014 Date of Review: 31 st May 2016 Lead Author:
SCOTTISH PAEDIATRIC CYSTIC FIBROSIS MCN Pseudomonas aeruginosa eradication guideline Date Created: 27 th June 2013 Date Approved by Steering Group: 30 th May 2014 Date of Review: 31 st May 2016 Lead Author:
Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012
 Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012 INTRODUCTION PNEUMOTHORAX HEMOPTYSIS RESPIRATORY FAILURE Cystic Fibrosis Autosomal Recessive Genetically
Cystic Fibrosis Complications ANDRES ZIRLINGER, MD STANFORD UNIVERSITY MEDICAL CENTER MARCH 3, 2012 INTRODUCTION PNEUMOTHORAX HEMOPTYSIS RESPIRATORY FAILURE Cystic Fibrosis Autosomal Recessive Genetically
Bronchiectasis. What is bronchiectasis? What causes bronchiectasis?
 This factsheet explains what bronchiectasis is, what causes it, and how it is diagnosed and managed. More detailed information is available on the Bronchiectasis Patient Priorities website: www.europeanlunginfo.org/bronchiectasis
This factsheet explains what bronchiectasis is, what causes it, and how it is diagnosed and managed. More detailed information is available on the Bronchiectasis Patient Priorities website: www.europeanlunginfo.org/bronchiectasis
How To Assess Severity and Prognosis
 How To Assess Severity and Prognosis Gregory Tino, M.D. Chief, Department of Medicine Penn Presbyterian Medical Center Associate Professor of Medicine Perelman School of Medicine at the University of Pennsylvania
How To Assess Severity and Prognosis Gregory Tino, M.D. Chief, Department of Medicine Penn Presbyterian Medical Center Associate Professor of Medicine Perelman School of Medicine at the University of Pennsylvania
A Place For Airway Clearance Therapy In Today s Healthcare Environment
 A Place For Airway Clearance Therapy In Today s Healthcare Environment Michigan Society for Respiratory Care 2015 Fall Conference K. James Ehlen, MD October 6, 2015 Objectives Describe patients who will
A Place For Airway Clearance Therapy In Today s Healthcare Environment Michigan Society for Respiratory Care 2015 Fall Conference K. James Ehlen, MD October 6, 2015 Objectives Describe patients who will
Palliative and Supportive Care in Cystic Fibrosis
 Palliative and Supportive Care in Cystic Fibrosis Dr William Flight Consultant in Respiratory Medicine Oxford Adult Cystic Fibrosis Centre 27 th January 2017 Overview 1. Cystic Fibrosis Clinical Aspects
Palliative and Supportive Care in Cystic Fibrosis Dr William Flight Consultant in Respiratory Medicine Oxford Adult Cystic Fibrosis Centre 27 th January 2017 Overview 1. Cystic Fibrosis Clinical Aspects
Clinical Commissioning Policy: Levofloxacin nebuliser solution for chronic Pseudomonas lung infection in cystic fibrosis (all ages)
") Clinical Commissioning Policy: Levofloxacin nebuliser solution for chronic Pseudomonas lung infection in cystic fibrosis (all ages) NHS England Reference: 1732P NHS England INFORMATION READER BOX Directorate
Clinical Commissioning Policy: Levofloxacin nebuliser solution for chronic Pseudomonas lung infection in cystic fibrosis (all ages) NHS England Reference: 1732P NHS England INFORMATION READER BOX Directorate
New Medicine Assessment
 September 2015 New Medicine Assessment Colistimethate sodium/colistin sulfomethate sodium (Colomycin ) Non-Cystic Fibrosis in Patients with Bronchiectasis Colonised with Pseudomonas Aeruginosa Recommendation:
September 2015 New Medicine Assessment Colistimethate sodium/colistin sulfomethate sodium (Colomycin ) Non-Cystic Fibrosis in Patients with Bronchiectasis Colonised with Pseudomonas Aeruginosa Recommendation:
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE 1 Guideline title SCOPE Bronchiolitis: diagnosis and management of bronchiolitis in children. 1.1 Short title Bronchiolitis in children 2 The remit The
NON-CYSTIC FIBROSIS BRONCHIECTASIS
 NON-CYSTIC FIBROSIS BRONCHIECTASIS MARK L. METERSKY, MD PROFESSOR OF MEDICINE UNIVERSITY OF CONNECTICUT SCHOOL OF MEDICINE FARMINGTON, CT Mark Metersky, MD, FCCP, FACP is a Professor of Medicine at the
NON-CYSTIC FIBROSIS BRONCHIECTASIS MARK L. METERSKY, MD PROFESSOR OF MEDICINE UNIVERSITY OF CONNECTICUT SCHOOL OF MEDICINE FARMINGTON, CT Mark Metersky, MD, FCCP, FACP is a Professor of Medicine at the
National Horizon Scanning Centre. Mannitol dry powder for inhalation (Bronchitol) for cystic fibrosis. April 2008
 for cystic fibrosis. April 2008") Mannitol dry powder for inhalation (Bronchitol) for cystic fibrosis April 2008 This technology summary is based on information available at the time of research and a limited literature search. It is not
Mannitol dry powder for inhalation (Bronchitol) for cystic fibrosis April 2008 This technology summary is based on information available at the time of research and a limited literature search. It is not
COPD Bronchiectasis Overlap Syndrome.
 COPD Bronchiectasis Overlap Syndrome. John R Hurst 1, J Stuart Elborn 2, and Anthony De Soyza 3 on Behalf of the BRONCH-UK Consortium (D Bilton, J Bradley, JS Brown, J Duckers, F Copeland, A Floto, J Foweraker,
COPD Bronchiectasis Overlap Syndrome. John R Hurst 1, J Stuart Elborn 2, and Anthony De Soyza 3 on Behalf of the BRONCH-UK Consortium (D Bilton, J Bradley, JS Brown, J Duckers, F Copeland, A Floto, J Foweraker,
C.S. HAWORTH 1, A. WANNER 2, J. FROEHLICH 3, T. O'NEAL 3, A. DAVIS 4, I. GONDA 3, A. O'DONNELL 5
 Inhaled Liposomal Ciprofloxacin in Patients With Non-Cystic Fibrosis Bronchiectasis and Chronic Pseudomonas aeruginosa: Results From Two Parallel Phase III Trials (ORBIT-3 and -4) C.S. HAWORTH 1, A. WANNER
Inhaled Liposomal Ciprofloxacin in Patients With Non-Cystic Fibrosis Bronchiectasis and Chronic Pseudomonas aeruginosa: Results From Two Parallel Phase III Trials (ORBIT-3 and -4) C.S. HAWORTH 1, A. WANNER
Goals Basic defect Pathophysiology Clinical i l signs and symptoms Therapy
 CYSTIC FIBROSIS Lynne M. Quittell, M.D. Director, CF Center Columbia University Goals Basic defect Pathophysiology Clinical i l signs and symptoms Therapy What is Cystic Fibrosis? Chronic, progressive
CYSTIC FIBROSIS Lynne M. Quittell, M.D. Director, CF Center Columbia University Goals Basic defect Pathophysiology Clinical i l signs and symptoms Therapy What is Cystic Fibrosis? Chronic, progressive
JUERGEN FROEHLICH, JANICE DAHMS, DAVID CIPOLLA,
 Reduction in Frequency of Pulmonary Exacerbations With Inhaled ARD-315 in Non-Cystic Fibrosis Bronchiectasis (NCFB) Patients is Independent of Pseudomonas aeruginosa Susceptibility at Baseline JUERGEN
Reduction in Frequency of Pulmonary Exacerbations With Inhaled ARD-315 in Non-Cystic Fibrosis Bronchiectasis (NCFB) Patients is Independent of Pseudomonas aeruginosa Susceptibility at Baseline JUERGEN
Bronchiectasis. Introduction. Key points
 15 Bronchiectasis Introduction i Key points Patients with bronchiectasis typically have chronic airway infection, punctuated by acute exacerbations and accompanied by progressive airflow obstruction. Bronchiectasis
15 Bronchiectasis Introduction i Key points Patients with bronchiectasis typically have chronic airway infection, punctuated by acute exacerbations and accompanied by progressive airflow obstruction. Bronchiectasis
Development of novel inhaled antibiotic regimens in patients with cystic fibrosis (CF) and patients with non-cf bronchiectasis (BE)
 and patients with non-cf bronchiectasis (BE)") Development of novel inhaled antibiotic regimens in patients with cystic fibrosis (CF) and patients with non-cf bronchiectasis (BE) Dr. Juliane Bernholz, Novartis (Coordinator) Dr. Andrea Appenzeller,
Development of novel inhaled antibiotic regimens in patients with cystic fibrosis (CF) and patients with non-cf bronchiectasis (BE) Dr. Juliane Bernholz, Novartis (Coordinator) Dr. Andrea Appenzeller,
The Role of CPET (cardiopulmonary exercise testing) in Assessing Lung Disease in CF
 in Assessing Lung Disease in CF") The Role of CPET (cardiopulmonary exercise testing) in Assessing Lung Disease in CF Dr. Meir Mei-Zahav Kathy and Lee Graub CF Center Schneider CMCI 1 תאריך Exercise in CF You are probably quite sure that
The Role of CPET (cardiopulmonary exercise testing) in Assessing Lung Disease in CF Dr. Meir Mei-Zahav Kathy and Lee Graub CF Center Schneider CMCI 1 תאריך Exercise in CF You are probably quite sure that
without the permission of the author Not to be copied and distributed to others
 Emperor s Castle interior-prato What is the Role of Inhaled Polymyxins for Treatment of Respiratory Tract Infections? Helen Giamarellou CONCLUSIONS: Patients with Pseudomonas and Acinetobacter VAP may
Emperor s Castle interior-prato What is the Role of Inhaled Polymyxins for Treatment of Respiratory Tract Infections? Helen Giamarellou CONCLUSIONS: Patients with Pseudomonas and Acinetobacter VAP may
Nebulised anti-pseudomonal antibiotics for cystic fibrosis (Review)
") Nebulised anti-pseudomonal antibiotics for cystic fibrosis (Review) Ryan G, Mukhopadhyay S, Singh M This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published
Nebulised anti-pseudomonal antibiotics for cystic fibrosis (Review) Ryan G, Mukhopadhyay S, Singh M This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published
Clinical Commissioning Policy Proposition: Dornase alfa inhaled therapy for primary ciliary dyskinesia (all ages)
") Clinical Commissioning Policy Proposition: Dornase alfa inhaled therapy for primary ciliary dyskinesia (all ages) Reference: NHS England E03X05/01 Information Reader Box (IRB) to be inserted on inside
Clinical Commissioning Policy Proposition: Dornase alfa inhaled therapy for primary ciliary dyskinesia (all ages) Reference: NHS England E03X05/01 Information Reader Box (IRB) to be inserted on inside
The team. Medical staff Dr Adam Hill Vacant post- Dr Lithgow Dr Ruzanna Frangulyan Specialist Trainee
 Bronchiectasis The team Medical staff Dr Adam Hill Vacant post- Dr Lithgow Dr Ruzanna Frangulyan Specialist Trainee Specialist staff Kim Turnbull Denise Gillian Jenny Scott Jo Pentland Research nurses
Bronchiectasis The team Medical staff Dr Adam Hill Vacant post- Dr Lithgow Dr Ruzanna Frangulyan Specialist Trainee Specialist staff Kim Turnbull Denise Gillian Jenny Scott Jo Pentland Research nurses
Eradication regimens for early or recurrent Pseudomonas aeruginosa infection
 Eradication regimens for early or recurrent Pseudomonas aeruginosa infection The Leeds Method of Management. April, 2008. Cystic fibrosis and eradication therapy for early or recurrent Pseudomonas aeruginosa
Eradication regimens for early or recurrent Pseudomonas aeruginosa infection The Leeds Method of Management. April, 2008. Cystic fibrosis and eradication therapy for early or recurrent Pseudomonas aeruginosa
Nebulised hypertonic saline for cystic fibrosis.
 Revista: Cochrane Database Syst Rev. 2003;(1):CD001506. Nebulised hypertonic saline for cystic fibrosis. Autor: Wark PA, McDonald V. Source: Department of Respiratory Medicine, John Hunter Hospital, Locked
Revista: Cochrane Database Syst Rev. 2003;(1):CD001506. Nebulised hypertonic saline for cystic fibrosis. Autor: Wark PA, McDonald V. Source: Department of Respiratory Medicine, John Hunter Hospital, Locked
Cystic Fibrosis Foundation Patient Registry 2013
 5/9/2015 Targeting CFTR to Treat Cystic Fibrosis: Small Molecule Therapy Mary Ellen Kleinhenz, MD Director, UCSF Adult Cystic Fibrosis Program Professor of Medicine UCSF Division of Pulmonary, Critical
5/9/2015 Targeting CFTR to Treat Cystic Fibrosis: Small Molecule Therapy Mary Ellen Kleinhenz, MD Director, UCSF Adult Cystic Fibrosis Program Professor of Medicine UCSF Division of Pulmonary, Critical
Treatment of lung infection in patients with cystic fibrosis: Current and future strategies,
 Journal of Cystic Fibrosis 11 (2012) 461 479 www.elsevier.com/locate/jcf Review Treatment of lung infection in patients with cystic fibrosis: Current and future strategies, Gerd Döring a,, Patrick Flume
Journal of Cystic Fibrosis 11 (2012) 461 479 www.elsevier.com/locate/jcf Review Treatment of lung infection in patients with cystic fibrosis: Current and future strategies, Gerd Döring a,, Patrick Flume
Non-CF bronchiectasis: Alexander Duarte, MD Pulmonary, Critical Care & Sleep Medicine University of Texas Medical Branch Galveston, TX
 Non-CF bronchiectasis: Alexander Duarte, MD Pulmonary, Critical Care & Sleep Medicine University of Texas Medical Branch Galveston, TX Pioneer of Respiratory Medicine 2016 marked 200th anniversary of his
Non-CF bronchiectasis: Alexander Duarte, MD Pulmonary, Critical Care & Sleep Medicine University of Texas Medical Branch Galveston, TX Pioneer of Respiratory Medicine 2016 marked 200th anniversary of his
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
Medical / Microbiology
 Medical / Microbiology Pseudomonas aeruginosa biofilms in the lungs of Cystic Fibrosis Patients Thomas Bjarnsholt, PhD, Associate professor 1,2, Peter Østrup Jensen, PhD 2 and Niels Høiby, MD, Dr. Med,
Medical / Microbiology Pseudomonas aeruginosa biofilms in the lungs of Cystic Fibrosis Patients Thomas Bjarnsholt, PhD, Associate professor 1,2, Peter Østrup Jensen, PhD 2 and Niels Høiby, MD, Dr. Med,
CYSTIC FIBROSIS FOUNDATION INFO-POD Information You Need to Make Benefits Decisions
 CYSTIC FIBROSIS FOUNDATION INFO-POD Information You Need to Make Benefits Decisions Issue 1: Hypertonic Saline Summary: Preserving lung function is a crucial element in the care of the individual with
CYSTIC FIBROSIS FOUNDATION INFO-POD Information You Need to Make Benefits Decisions Issue 1: Hypertonic Saline Summary: Preserving lung function is a crucial element in the care of the individual with
10/05/2017. Learning Objectives. Etiology and Prevalence. Diagnosis of Cystic Fibrosis. Disease of Childhood? Survival in Cystic Fibrosis
 Management of the Cystic Fibrosis Patient Jessica Goggin, MAS, RN Nurse Manager UC San Diego Adult Cystic Fibrosis Program Learning Objectives 1. Describe the symptoms associated with Cystic Fibrosis (CF).
Management of the Cystic Fibrosis Patient Jessica Goggin, MAS, RN Nurse Manager UC San Diego Adult Cystic Fibrosis Program Learning Objectives 1. Describe the symptoms associated with Cystic Fibrosis (CF).
Novel Therapies for NTM
 NTM Lecture Series for Providers Novel Therapies for NTM Kenneth N Olivier, MD, MPH Laboratory of Chronic Airway Infection Chief, Pulmonary Branch/DIR October 20, 2017 Disclosures Past: Cooperative Research
NTM Lecture Series for Providers Novel Therapies for NTM Kenneth N Olivier, MD, MPH Laboratory of Chronic Airway Infection Chief, Pulmonary Branch/DIR October 20, 2017 Disclosures Past: Cooperative Research
Overview of Cystic fibrosis in children. Apeksha Sathyaprasad, MD Pediatric pulmonologist
 Overview of Cystic fibrosis in children Apeksha Sathyaprasad, MD Pediatric pulmonologist No conflicts of interest OBJECTIVES Review pathophysiology of pulmonary disease in cystic fibrosis Review diagnostic
Overview of Cystic fibrosis in children Apeksha Sathyaprasad, MD Pediatric pulmonologist No conflicts of interest OBJECTIVES Review pathophysiology of pulmonary disease in cystic fibrosis Review diagnostic
Pneumococcal pneumonia
 Pneumococcal pneumonia Wei Shen Lim Consultant Respiratory Physician & Honorary Professor of Medicine Nottingham University Hospitals NHS Trust University of Nottingham Declarations of interest Unrestricted
Pneumococcal pneumonia Wei Shen Lim Consultant Respiratory Physician & Honorary Professor of Medicine Nottingham University Hospitals NHS Trust University of Nottingham Declarations of interest Unrestricted
Bronchiectasis (non-cystic fibrosis), acute exacerbation: antimicrobial prescribing
, acute exacerbation: antimicrobial prescribing") National Institute for Health and Care Excellence Bronchiectasis (non-cystic fibrosis), acute exacerbation: antimicrobial prescribing Evidence review NICE guideline NG117 December 2018 Disclaimer The
National Institute for Health and Care Excellence Bronchiectasis (non-cystic fibrosis), acute exacerbation: antimicrobial prescribing Evidence review NICE guideline NG117 December 2018 Disclaimer The
Active Cycle of Breathing Technique
 Active Cycle of Breathing Technique Full Title of Guideline: Author (include email and role): Division & Speciality: Version: 3 Ratified by: Scope (Target audience, state if Trust wide): Review date (when
Active Cycle of Breathing Technique Full Title of Guideline: Author (include email and role): Division & Speciality: Version: 3 Ratified by: Scope (Target audience, state if Trust wide): Review date (when
PULMONARY EMERGENCIES
 EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
EMERGENCIES I. Pneumonia A. Bacterial Pneumonia (most common cause of a focal infiltrate) 1. Epidemiology a. Accounts for up to 10% of hospital admissions in the U.S. b. Most pneumonias are the result
Abbreviated Class Review: Inhaled Antibiotics and Dornase Alfa for Cystic Fibrosis
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35, Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Fungal (Aspergillus and Candida) infections in Cystic fibrosis
 infections in Cystic fibrosis") Fungal (Aspergillus and Candida) infections in Cystic fibrosis Malena Cohen-Cymberknoh, MD CF Center Hadassah-Hebrew University Medical Center Jerusalem, Israel Israeli Annual CF Conference, Herzlyia,
Fungal (Aspergillus and Candida) infections in Cystic fibrosis Malena Cohen-Cymberknoh, MD CF Center Hadassah-Hebrew University Medical Center Jerusalem, Israel Israeli Annual CF Conference, Herzlyia,
Clinical Commissioning Policy: Dornase alfa inhaled therapy for primary ciliary dyskinesia (all ages)
") Clinical Commissioning Policy: Dornase alfa inhaled therapy for primary ciliary dyskinesia (all ages) Reference: NHS England: 16029/P NHS England INFORMATION READER BOX Directorate Medical Operations and
Clinical Commissioning Policy: Dornase alfa inhaled therapy for primary ciliary dyskinesia (all ages) Reference: NHS England: 16029/P NHS England INFORMATION READER BOX Directorate Medical Operations and
Aerosolized Antibiotics in Mechanically Ventilated Patients
 Aerosolized Antibiotics in Mechanically Ventilated Patients Gerald C Smaldone MD PhD Introduction Topical Delivery of Antibiotics to the Lung Tracheobronchitis Aerosolized Antibiotic Delivery in the Medical
Aerosolized Antibiotics in Mechanically Ventilated Patients Gerald C Smaldone MD PhD Introduction Topical Delivery of Antibiotics to the Lung Tracheobronchitis Aerosolized Antibiotic Delivery in the Medical
Transformational Treatments. PRESTON W. CAMPBELL, III, M.D. Executive Vice President for Medical Affairs
 Transformational Treatments PRESTON W. CAMPBELL, III, M.D. Executive Vice President for Medical Affairs Symptom-based CF Therapies 45 Median Predicted Survival Age of US Patients with Cystic Fibrosis 41
Transformational Treatments PRESTON W. CAMPBELL, III, M.D. Executive Vice President for Medical Affairs Symptom-based CF Therapies 45 Median Predicted Survival Age of US Patients with Cystic Fibrosis 41
Evaluation of Patients with Diffuse Bronchiectasis
 Evaluation of Patients with Diffuse Bronchiectasis Dr. Patricia Eshaghian, MD Assistant Clinical Professor of Medicine Director, UCLA Adult Cystic Fibrosis Affiliate Program UCLA Division of Pulmonary
Evaluation of Patients with Diffuse Bronchiectasis Dr. Patricia Eshaghian, MD Assistant Clinical Professor of Medicine Director, UCLA Adult Cystic Fibrosis Affiliate Program UCLA Division of Pulmonary
TREAMENT OF RECURRENT VIRUS-INDUCED WHEEZING IN YOUNG CHILDREN. Dr Lại Lê Hưng Respiratory Department
 TREAMENT OF RECURRENT VIRUS-INDUCED WHEEZING IN YOUNG CHILDREN Dr Lại Lê Hưng Respiratory Department Literature review current through: Feb 2013. This topic last updated: Aug 14, 2012 INTRODUCTION Wheezing
TREAMENT OF RECURRENT VIRUS-INDUCED WHEEZING IN YOUNG CHILDREN Dr Lại Lê Hưng Respiratory Department Literature review current through: Feb 2013. This topic last updated: Aug 14, 2012 INTRODUCTION Wheezing
Pulmonary Exacerbations:
 Pulmonary Exacerbations: Better Understanding Needed Michael Tracy, MD Clinical Assistant Professor Pediatric Pulmonary CF Pulmonary Exacerbations Definition Importance Causes Treatment Research opportunities
Pulmonary Exacerbations: Better Understanding Needed Michael Tracy, MD Clinical Assistant Professor Pediatric Pulmonary CF Pulmonary Exacerbations Definition Importance Causes Treatment Research opportunities
Clinical Commissioning Policy Proposition: Levofloxacin nebuliser solution for chronic Pseudomonas lung infection in cystic fibrosis (Adults)
") Clinical Commissioning Policy Proposition: Levofloxacin nebuliser solution for chronic Pseudomonas lung infection in cystic fibrosis (Adults) Reference: NHS England 1621 First published: Month Year Prepared
Clinical Commissioning Policy Proposition: Levofloxacin nebuliser solution for chronic Pseudomonas lung infection in cystic fibrosis (Adults) Reference: NHS England 1621 First published: Month Year Prepared
Chapter 10 Respiratory System J00-J99. Presented by: Jesicca Andrews
 Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Chapter 10 Respiratory System J00-J99 Presented by: Jesicca Andrews 1 Respiratory System 2 Respiratory Infections A respiratory infection cannot be assumed from a laboratory report alone; physician concurrence
Exacerbations. Ronald Dahl, Aarhus University Hospital, Denmark
 1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark The health professional that care for patients with asthma exacerbation must be able to Identificafy
1st WAO Allied Health Session - Asthma: Diagnosi Exacerbations Ronald Dahl, Aarhus University Hospital, Denmark The health professional that care for patients with asthma exacerbation must be able to Identificafy
Arikace (Preclinical Summary)
") Full analyses of data from two phase II blinded and placebo-controlled studies of nebulized liposomal amikacin for inhalation (Arikace ) in the treatment of cystic fibrosis patients with chronic Pseudomonas
Full analyses of data from two phase II blinded and placebo-controlled studies of nebulized liposomal amikacin for inhalation (Arikace ) in the treatment of cystic fibrosis patients with chronic Pseudomonas
ANWICU knowledge
 ANWICU knowledge www.anwicu.org.uk This presenta=on is provided by ANWICU We are a collabora=ve associa=on of ICUs in the North West of England. Permission to provide this presenta=on has been granted
ANWICU knowledge www.anwicu.org.uk This presenta=on is provided by ANWICU We are a collabora=ve associa=on of ICUs in the North West of England. Permission to provide this presenta=on has been granted
PNEUMONIA. I. Background 6 th most common cause of death in U.S. Most common cause of infection related mortality
 Page 1 of 8 September 4, 2001 Donald P. Levine, M.D. University Health Center Suite 5C Office: 577-0348 dlevine@intmed.wayne.edu Assigned reading: pages 153-160; 553-563 PNEUMONIA the most widespread and
Page 1 of 8 September 4, 2001 Donald P. Levine, M.D. University Health Center Suite 5C Office: 577-0348 dlevine@intmed.wayne.edu Assigned reading: pages 153-160; 553-563 PNEUMONIA the most widespread and
an inflammation of the bronchial tubes
 BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
BRONCHITIS DEFINITION Bronchitis is an inflammation of the bronchial tubes (or bronchi), which are the air passages that extend from the trachea into the small airways and alveoli. Triggers may be infectious
Summary A pharmaceutical company which develops therapeutic products for
 Innovative products for respiratory diseases Annual General Meeting October 2012 Pharmaxis - company overview Summary A pharmaceutical company which develops therapeutic products for human chronic respiratory
Innovative products for respiratory diseases Annual General Meeting October 2012 Pharmaxis - company overview Summary A pharmaceutical company which develops therapeutic products for human chronic respiratory
Cystic fibrosis: hitting the target
 Cystic fibrosis: hitting the target Heartland Collaborative Annual Meeting Friday, October 5, 2012 Thomas Ferkol MD 1938 1953 Cystic fibrosis: a historical timeline Cystic fibrosis (CF) of the pancreas
Cystic fibrosis: hitting the target Heartland Collaborative Annual Meeting Friday, October 5, 2012 Thomas Ferkol MD 1938 1953 Cystic fibrosis: a historical timeline Cystic fibrosis (CF) of the pancreas
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER
 MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
MAYA RAMAGOPAL M.D. DIVISION OF PULMONOLOGY & CYSTIC FIBROSIS CENTER 16 year old female with h/o moderate persistent asthma presents to the ED after 6 hours of difficulty breathing, cough, and wheezing
LRI Children s Hospital
 Title: Prescribing in Cystic Fibrosis Page 1 of 10 LRI Children s Hospital Prescribing in Cystic Fibrosis Staff relevant to: Clinical staff working within the UHL Children s Hospital. Team & AWP approval
Title: Prescribing in Cystic Fibrosis Page 1 of 10 LRI Children s Hospital Prescribing in Cystic Fibrosis Staff relevant to: Clinical staff working within the UHL Children s Hospital. Team & AWP approval
TRANSPARENCY COMMITTEE OPINION. 15 October Date of Marketing Authorisation (national procedure): 16 April 1997, variation of 18 February 2008
: 16 April 1997, variation of 18 February 2008") The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 15 October 2008 MERONEM 1 g, powder for solution for IV Injection Box of 10 vials (CIP: 387 830-6) Applicant: ASTRAZENECA
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 15 October 2008 MERONEM 1 g, powder for solution for IV Injection Box of 10 vials (CIP: 387 830-6) Applicant: ASTRAZENECA
TR Protocol Number: TR02-107
 TR02-107 A PLACEBO CONTROLLED, RANDOMIZED, PARALLEL COHORT, SAFETY AND TOLERABILITY STUDY OF TWO DOSE LEVELS OF LIPOSOMAL AMIKACIN FOR INHALATION (ARIKACE ) IN PATIENTS WITH BRONCHIECTASIS COMPLICATED
TR02-107 A PLACEBO CONTROLLED, RANDOMIZED, PARALLEL COHORT, SAFETY AND TOLERABILITY STUDY OF TWO DOSE LEVELS OF LIPOSOMAL AMIKACIN FOR INHALATION (ARIKACE ) IN PATIENTS WITH BRONCHIECTASIS COMPLICATED
Cystic Fibrosis. Jennifer McDaniel, BS, RRT-NPS
 Cystic Fibrosis Jennifer McDaniel, BS, RRT-NPS Overview Cystic fibrosis is the most common fatal, inherited disease in the U. S. CF results from a defective autosomal recessive gene One copy of gene =
Cystic Fibrosis Jennifer McDaniel, BS, RRT-NPS Overview Cystic fibrosis is the most common fatal, inherited disease in the U. S. CF results from a defective autosomal recessive gene One copy of gene =
SAVARA CORPORATE PRESENTATION (NASDAQ: SVRA) NOVEMBER 2018
 NOVEMBER 2018") SAVARA CORPORATE PRESENTATION (NASDAQ: SVRA) NOVEMBER 2018 SAFE HARBOR STATEMENT Savara Inc. ( Savara or the Company ) cautions you that statements in this presentation that are not a description of historical
SAVARA CORPORATE PRESENTATION (NASDAQ: SVRA) NOVEMBER 2018 SAFE HARBOR STATEMENT Savara Inc. ( Savara or the Company ) cautions you that statements in this presentation that are not a description of historical
The objectives of this presentation are to
 1 The objectives of this presentation are to 1. Review the mechanics of airway clearance 2. Understand the difference between secretion mobilization and secretion clearance 3. Identify conditions that
1 The objectives of this presentation are to 1. Review the mechanics of airway clearance 2. Understand the difference between secretion mobilization and secretion clearance 3. Identify conditions that
4.6 Small airways disease
 4.6 Small airways disease Author: Jean-Marc Fellrath 1. INTRODUCTION Small airways are defined as any non alveolated and noncartilaginous airway that has an internal diameter of 2 mm. Several observations
4.6 Small airways disease Author: Jean-Marc Fellrath 1. INTRODUCTION Small airways are defined as any non alveolated and noncartilaginous airway that has an internal diameter of 2 mm. Several observations
COPD. Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS
 IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
Guidelines for the use of Nebulised Colistemethate Sodium (Colomycin) Injection () in Pseudomonas aeruginosa Lung Infections in Adults
 Injection () in Pseudomonas aeruginosa Lung Infections in Adults") Index No: MMG41 Guidelines for the use of Nebulised Colistemethate Sodium (Colomycin) Injection () in Pseudomonas Version: 2 Date ratified: November 2017 Ratified by: (Name of Committee) Name of originator/author,
Index No: MMG41 Guidelines for the use of Nebulised Colistemethate Sodium (Colomycin) Injection () in Pseudomonas Version: 2 Date ratified: November 2017 Ratified by: (Name of Committee) Name of originator/author,
Management of the Symptomatic PCD
 Management of the Symptomatic PCD Andrew Bush MD FRCP FRCPCH FERS Imperial College & Royal Brompton Hospital a.bush@imperial.ac.uk Conflict of Interest AB has no financial or other COI There will be discussion
Management of the Symptomatic PCD Andrew Bush MD FRCP FRCPCH FERS Imperial College & Royal Brompton Hospital a.bush@imperial.ac.uk Conflict of Interest AB has no financial or other COI There will be discussion
Bronchiectasis in Adults - Suspected
 Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
Bronchiectasis in Adults - Suspected Clinical symptoms which may indicate bronchiectasis for patients Take full respiratory history including presenting symptoms, past medical & family history Factors
Asthma in Pediatric Patients. DanThuy Dao, D.O., FAAP. Disclosures. None
 Asthma in Pediatric Patients DanThuy Dao, D.O., FAAP Disclosures None Objectives 1. Discuss the evaluation and management of asthma in a pediatric patient 2. Accurately assess asthma severity and level
Asthma in Pediatric Patients DanThuy Dao, D.O., FAAP Disclosures None Objectives 1. Discuss the evaluation and management of asthma in a pediatric patient 2. Accurately assess asthma severity and level
Session Guidelines. This is a 15 minute webinar session for CNC physicians and staff
 Respiratory Disease Session Guidelines This is a 15 minute webinar session for CNC physicians and staff CNC holds webinars monthly to address topics related to risk adjustment documentation and coding
Respiratory Disease Session Guidelines This is a 15 minute webinar session for CNC physicians and staff CNC holds webinars monthly to address topics related to risk adjustment documentation and coding
Current Concepts in VAP: Stress Ulcer Prophylaxis & Probiotics. Deborah Cook
 Current Concepts in VAP: Stress Ulcer Prophylaxis & Probiotics Deborah Cook Objectives VAP The Old: Gastropulmonary route of infection The New: Microbiome modification Role of acid suppression Influence
Current Concepts in VAP: Stress Ulcer Prophylaxis & Probiotics Deborah Cook Objectives VAP The Old: Gastropulmonary route of infection The New: Microbiome modification Role of acid suppression Influence