COPD. Yesterday and Today; Achievements and Challenges. Zurab Gurul MD, PhD
|
|
|
- Rolf Patrick
- 5 years ago
- Views:
Transcription
1 COPD Yesterday and Today; Achievements and Challenges Zurab Gurul MD, PhD
2 The history of COPD The evolution of knowledge concerning COPD and its components emphysema, chronic bronchitis, and asthmatic bronchitis covers 200 years. Some of the earliest references to the description of emphysema include: Bonet s description of voluminous lungs in 1679 (Bonet 1679); Morgagni s (1769) description of 19 cases in which the lungs were turgid, particularly from air; and Baille s illustrations of the emphysematous lung, thought to be that of Samuel Johnson (Baillie 1789). The beginnings of our clinical understanding of the chronic bronchitis component of COPD can be traced to Badham (1814), who used the word catarrh to refer to the chronic cough and mucus hypersecretion that are cardinal symptoms. He described bronchiolitis and chronic bronchitis as disabling disorders
3 The emphysema component of disease was beautifully described by Laënnec (1821) in his Treatise of diseases of the chest. Laënnec, a clinician, pathologist, and inventor of the stethoscope, did careful dissections of patients that he had studied during life. He recognized that emphysema lungs were hyperinflated and did not empty well. John Hutchinson invented the spirometer in Hutchinson s instrument only measured vital capacity. It took another 100 years for Tiffeneauto add the concept of timed vital capacity as a measure of airflow, for spirometryto become complete as a diagnostic instrument
4 In 1944, one of the great teachers of emphysema, Ronald Christie, suggested that The diagnosis should be considered certain when dyspnea on exertion, of insidious onset, not due to bronchospasm, or left ventricular failure, appears in a patient who has some physical signs of emphysema together with chronic bronchitis and asthma. Barach and Bickerman(1956) edited the first comprehensive text book, Pulmonary emphysema, which nicely describes the treatment of the era. These two physicians were early champions of treatment for emphysema. Contributors to this book included Dickerson Richards, Nobel Laureate, who wrote on the pulmonary circulation and cor pulmonale.
5 Other acronyms that predated the COPD designation were chronic obstructive bronchopulmonary disease, chronic airflow obstruction, chronic obstructive lung disease, nonspecific chronic pulmonary disease, and diffuse obstructive pulmonary syndrome. William Briscoe is believed to be the first person to use the term COPD in discussion at the 9th Aspen Emphysema Conference. This term became established and today we refer to COPD as the designation of this growing health problem (Briscoe and Nash 1965). Today, COPD is a steadily growing global healthcare problem, with increasing morbidity and mortality
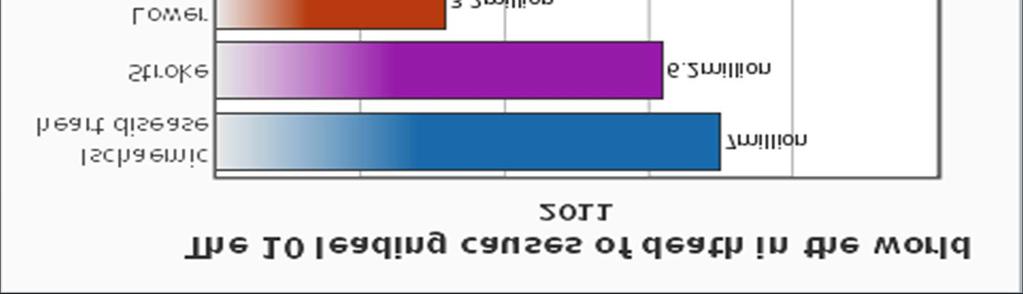
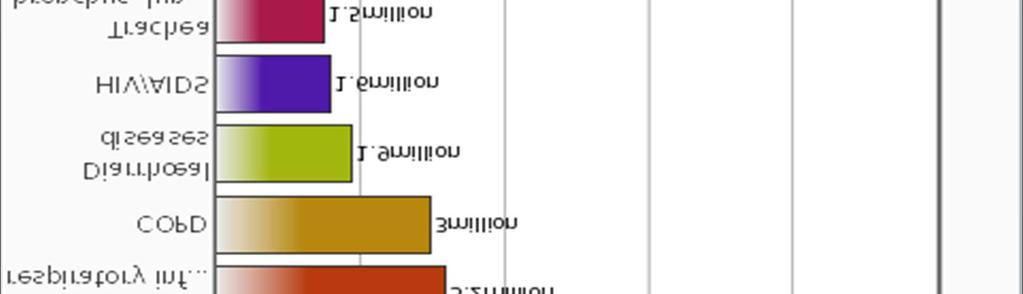
6 COPD Statistics: Worldwide, COPD affects 329 million people or nearly 5% of the population. In 2011, it ranked as the fourth-leading cause of death, killing over 3 million people It resulted in an estimated economic cost of $2.1 trillion in 2010
7
8 In the US COPD is the 4th leading cause of death, following lung cancer, heart disease and strokes. In the US, over 120,000 people die a year from COPD. Most of them were smokers. COPD claims the lives of around 30,000 people in the UK. Smoking is the biggest risk factor for developing COPD. Female deaths from COPD have now overtaken male deaths since the year In the US in 2002, more than 61,000 females died of COPD compared to 59,000 males. Women who smoke are 13 times as likely to die of COPD than women who have never smoked.
9 Men who smoke are 13 times as likely to die of COPD than men who have never smoked. There are more female sufferers of chronic bronchitis than male sufferers (50% more). Around 55% of emphysema sufferers are male and 45% are female. However, the trends seem to be reversing, as the number of female sufferers is increasing (around 5%) and the number of male sufferers is decreasing (around 10%). Around 600,000 people have been diagnosed with COPD in the UK. Heavy smokers are 30 times as likely to develop COPD.
10 The relative and absolute risks of death from smoking continue to increase among female smokers The relative risks of death from lung cancer, COPD, ischemic heart disease, any type of stroke, and all causes are now nearly identical for female and male smokers. women who smoke like men die like men.
11 Other causes of COPD Air pollution People who live in large cities have a higher rate of COPD compared to people who live in rural areas Occupational exposures Intense and prolonged exposure to workplace dusts, chemicals and fumes increase the risk of COPD in both smokers and nonsmokers. coal mining, gold mining, cotton textile industry, occupations involving cadmium and isocyanates, and fumes from welding. The negative effects of dust exposure and cigarette smoke exposure appear to be additive or possibly more than additive
12 Genetics Currently, the only clearly inherited risk factor is alpha 1-antitrypsin deficiency This risk is particularly high if someone deficient in alpha 1-antitrypsin also smokes It is responsible for about 1-5% of cases and the condition is present in about 3-4 in 10,000 people. Other genetic factors are being investigated
13 Cystic Fibrosis ( mucous plugging of secretions leading to pneumonia) Bronchiectasis (localized destruction and dilation of bronchial walls from chronic bronchopneumonia) Bronchiolitis obliterans (destruction of bronchioles occurring with ARDS, viral pneumonia, collagen vascular disease, inhalation of NO2, or graft-vs-host disease from bone marrow transplantation) Tracheal stenosis (<5mm, from ischemia of tracheal mucosa following prolonged intubation)


14 Chronic bronchitis is irritation and inflammation (swelling) of the lining in the bronchial tubes. The irritation causes coughing and an excess amount of mucus in the airways. The swelling makes it difficult to get air in and out of the lungs. The cilia are then unable to help clean mucus from the airways.
15 Chronic Bronchitis Diagnosis : presence of productive cough on most days of 3 consecutive months occurring for >2 consecutive years Symptoms : frequent pneumonia, bronchospasm, chronic hypoxia, erythrocytosis, pulmonary hipertension, cor pulmonale Patients often tolerate hypoxia without dyspnea Blue Bloater

16 Emphysema Irreversible destruction of distal airways with loss of septae, usually secondary to smoking
17 Symptoms: Hyperinflated lungs, cysts, bullae, and destruction of pulmonary capillaries. The patients have less of a tendency to develop cor pulmonale or erythrocytosis Patients are tachypneic in an attempt to maintain a more normal PaO2 Pink Puffer
18 Diagnostic Methods: The diagnosis of COPD should be considered in anyone over the age of 35 to 40 who has shortness of breath, a chronic cough, sputum production, or frequent winter colds and a history of exposure to risk factors for the disease. Spirometry is used to confirm the diagnosis. Spirometry is fundamental to making a diagnosis of COPD and a confident diagnosis of COPD can only be made with spirometry Spirometry measures the amount of airflow obstruction present and is generally carried out after the use of a bronchodilator,
19 Two main components are measured to make the diagnosis: the forced expiratory volume in one second (FEV 1 ), and the forced vital capacity (FVC) A diagnosis of airflow obstruction can be made if the FEV1/FVC < 0.7 (i.e. 70%) and FEV1 < 80% predicted. Spirometry is a poor predictor of disability and quality of life in COPD Spirometry predicts prognosis in COPD Spirometry contributes to the assessment of the severity of COPD
20 Spirometry alone cannot separate asthma from COPD The values for the post-bronchodilator forced expiratory volume in 1 second (FEV1) and forced vital capacity (FVC) must be compared with the predicted normal values which depend on the individual's age, height and sex International GOLD guidelines note that specific spirometric cut-points (e.g., post-bronchodilator FEV1/FVC ratio < 0.70 or FEV1 < 80,50, or 30% predicted) are used for purposes of simplicity, but that these cut-points have not been clinically validated
21 COPD is defined by the presence of airflow limitation that is not fully reversible and does not change markedly over several months While post-bronchodilator FEV1/FVC and FEV1 measurements are recommended for the diagnosis and assessment of severity of COPD, the degree of reversibility of airflow limitation (e.g., change in FEV1 after bronchodilator or glucocorticosteroids) is not recommended for diagnosis, or for predicting the response to long-term treatment with bronchodilators or glucocorticosteroids In most cases the diagnosis of COPD is suggested by the combination of the clinical history, signs and baseline spirometry
22 COPD is heterogeneous disorder, so no single measure can give an adequate assessment of the true severity of the disease in an individual patient. Severity assessment is important because it has implications for therapy and relates to prognosis. Using spirometry alone may underestimate the impact of the disease in some patients and overestimate it in others. Different thresholds for defining mild, moderate and severe airflow obstruction have been recommended. Thresholds of 80%, 50% and 30% are used to define the boundaries as these have implications both for therapy and prognosis and harmonise with the values recommended in the GOLD and the ATS/ERS guidelines. BMI and exercise capacity also reflect the impact of the disease in an individual and predict prognosis
23 GOLD Criteria for COPD The GOLD classifications are the main method to describe the severity of chronic obstructive pulmonary disease (COPD). GOLD is short for the Global Initiative for Chronic Obstructive Lung Disease, a collaboration between the National Institutes of Health and the World Health Organization. The GOLD guidelines suggest dividing people into four categories based on symptoms assessment and airflow limitation.
24 GOLD grade Severity FEV 1 % predicted Mild (GOLD 1) 80 Moderate (GOLD 2) Severe (GOLD 3) Very severe (GOLD 4) <30 or chronic respiratory failure
25 Beyond office spirometry, complete pulmonary function testing may show increased total lung capacity, functional residual capacity, and residual volume. A substantial loss of lung surface area available for effective oxygen exchange causes diminished carbon monoxide diffusion in the lung (DLCO) in patients with emphysema. This finding may help distinguish COPD from asthma, because patients with asthma typically have normal DLCO values. Arterial blood gas measurement is recommended to rule out significant hypoxemia (partial pressure of oxygen less than 60 mm Hg) or hypercapnia in patients with more severe disease. This is based on FEV1 (less than 40 percent of predicted value), signs of right-sided heart failure, and signs of hypoxemia.
26 Testing for α1-antitrypsin deficiency is appropriate in selected patients. testing involves measuring circulating α1-antitrypsin levels followed by phenotype testing if levels are abnormal. Patients with severe α1-antitrypsin deficiency usually are of European descent and develop clinical evidence of COPD approximately 10 years earlier than patients who are not α1- antitrypsin deficient. Lung changes associated with severe α1-antitrypsin deficiency usually include lower lung field predilection. α1-antitrypsin deficiency also may cause otherwise unexplained cirrhosis of the liver. Clinical circumstances in which testing for α1-antitrypsin deficiency should be considered include COPD in never-smokers, idiopathic cirrhosis, family history of α1-antitrypsin deficiency, predominantly lower lung emphysema, premature COPD, and refractory asthma at a young age.


27 Chest X-ray A lateral chest x-ray of a person with emphysema. Note the barrel chest and flat diaphragm.


28 Chest X-Ray A severe case of bullous emphysema


29 CT Scan Axial CT image of the lung of a person with endstage bullous emphysema.
 is")

30 Measurement of the Diameters of the Pulmonary Artery and Aorta CT-detected pulmonary artery enlargement (a PA:A ratio of >1) is independently associated with acute exacerbations of COPD and identifies a sub- population at high risk for hospitalization for these events.
31 COPD and Impaired Left Ventricular Filling Very severe chronic obstructive pulmonary disease causes cor pulmonale with elevated pulmonary vascular resistance and secondary reductions in left ventricular filling, stroke volume, and cardiac output. Moderately severe COPD is associated with significant decrements in left ventricular filling and cardiac output. The magnitude of these associations are greater among participants with a history of smoking, but the associations with percent emphysema are also present among participants who had never smoked.
32 COPD as a Systemic Disease COPD increasingly is considered a systemic disorder with important non-pulmonary components. Weight loss in patients with COPD may be related to increased circulating levels of inflammatory mediators (e.g., tumor necrosis factor alpha, inflammatory cytokines). Pulmonary cachexia associated with severe COPD also causes profound weight loss, which is a predictor of increased mortality risk independent of lung function. Respiratory and skeletal muscle abnormalities accompany COPD. The respiratory muscles of patients with COPD are chronically overworked and fatigued, whereas the extremity muscles tend to be underworked and atrophied.
33 Treatment (Bronchodilators) Inhaled bronchodilators are the primary medications used and result in a small overall benefit. There are two major types, β 2 agonists and anticholinergics; both exist in long-acting and short-acting forms. They reduce shortness of breath, wheeze and exercise limitation, resulting in an improved quality of life. It is unclear if they change the progression of the underlying disease. In those with mild disease, short-acting agents are recommended on an as needed basis. In those with more severe disease, long-acting agents are recommended
34 There are several short-acting β 2 agonists available including salbutamol (Ventolin) and terbutaline. They provide some relief of symptoms for four to six hours. Long-acting β 2 agonists such as salmeterol and formoterol are often used as maintenance therapy. Long-term use appears safe in COPD with adverse effects include shakiness and heart palpitations. When used with inhaled steroids they increase the risk of pneumonia.
35 There are two main anticholinergics used in COPD, ipratropium and tiotropium. Ipratropium is a short-acting agent while tiotropium is longacting. Tiotropium is associated with a decrease in exacerbations and improved quality of life, and tiotropium provides those benefits better than ipratropium. It does not appear to affect mortality or the over all hospitalization rate. Anticholinergics can cause dry mouth and urinary tract symptoms.they are also associated with increased risk of heart disease and stroke.
36 Corticosteroids Corticosteroids are usually used in inhaled form but may also be used as tablets to treat and prevent acute exacerbations. While inhaled corticosteroids (ICS) have not shown benefit for people with mild COPD, they decrease acute exacerbations in those with either moderate or severe disease. When used in combination with a LABA they decrease mortality more than either ICS or LABA alone. By themselves they have no effect on overall one-year mortality and are associated with increased rates of pneumonia. It is unclear if they affect the progression of the disease. Long-term treatment with steroid tablets is associated with significant side effects
37 Other medications Methylxanthine drugs such as aminophylline and theophylline are recommended for use in patients who have acute exacerbations (episodes) of chronic obstructive pulmonary disease, particularly for patients unresponsive to standard therapies. The studies do not give a clear indication of whether there was benefit in terms of reduced symptoms or hospital admissions, but side effects were found to be more common with methylxanthines. Given current evidence, methylxanthines should not be used for acute exacerbations of chronic obstructive pulmonary disease.
38 Long-term antibiotics, specifically those from the macrolide class such as erythromycin, reduce the frequency of exacerbations in those who have two or more a year. (concerns include that of antibiotic resistance and hearing problems with azithromycin). Mucolytics may be useful in some people who have very thick mucous but are generally not needed. Cough medicines are not recommended.
39 Oxygen Supplemental oxygen is recommended in those with low oxygen levels at rest (a partial pressure of oxygen of less than mmhg or oxygen saturations of less than 88%). In this group of people it decreases the risk of heart failure and death if used 15 hours per day and may improve people's ability to exercise. During acute exacerbations, many require oxygen therapy; the use of high concentrations of oxygen without taking into account a person's oxygen saturations, may lead to increased levels of carbon dioxide and worsened outcomes. In those at high risk of high carbon dioxide levels, oxygen saturations of 88 92% are recommended, while for those without this risk recommended levels are 94-98%.


40 Lung volume reduction surgery Vanishing lung syndrome, otherwise known as idiopathic giant bullous emphysema. A 41-year-old man with a smoking history of 30 packyears presented with chronic chest pain, dyspnea, and cough.
41 Preoperative care for the patient with COPD Determine the type of COPD, its severity, and the chronicity of symptoms. Optimize medical management a) Treat any underlying respiratory infections; b) Optimize bronchodilator therapy; c) Facilitate pulmonary toilet; d) Initiate patient participation ( weight loss, incentive spirometry, exercise) e) Smoking cessation ( effective only if >6-8 weeks)
42 Deleterious effects of smoking: Nicotine causes sympathetic stimulation with tachycardia and has been implicated with impaired wound healing. Carbon monoxide (CO) can also cause: a) Negative inotropy; b) Leftward shift of the O2-Hgb dissociation curve ( The half-life of CO is 4-6 hours, so normalization of CO levels 1% in nonsmokers vs. 6% in smokers occurs within 12 hours following cessation of smoking). Acute discontinuation of smoking has not been shown to be helpful. In fact, it may cause airway irritability and actually lead to to an increased incidence of postop atelectasis, pneumonia, pulmonary dysfunction, and DVT s.
43 How to assess the pt s COPD? H/P ( focusing on symptoms of cough, dyspnea, exercise tolerance, cyanosis, clubbing, pneumonia, hospitalizations and medications). PE ( Respiratory pattern, RR, use of accessory muscles, signs of RV failure hepatosplenomegaly, edema, JVD) Labs: CBC (erythrocytosis), CXR, EKG (RVH); ABG ( hypoxemia and hypercarbia), and electrolytes ( metabolic alcalosis for hypercarbia).
44 What is the significance of a increased RR? It depends on the pt s baseline RR and whether he/she has emphysema or chronic bronchitis. A) With chronic emphysema, the RR is faster than with chronic bronchitis due to a preserved drive to maintain normal PaO2 and PaCO2 values. B) With chronic bronchitis, patients are more tolerant of hypercarbia and hypoxemia and tachypnea is often late sign of distress. C) Tachypnea can also be due to pain or anxiety.
45 Which spirometric studies are most The most basic one is FEV1. helpful? Patients with a FEV1<50% may be at risk for failing extubation or developing postop respiratory complication. For pneumonectomies, a preop FEV1 of 1600 cc is often cited as necessary to achieve a predicted postpneumonectomyfev1 of 800 cc; However, such values depend on body size and are not without exception. As an anestesiologist, I rarely order spirometry, despite the long list of theoretical reasons for doing so.
46 Why Not? The reasons for ordering FEV1 of FVC cited in textbooks can often be obtained by H/P. To determine the response to bronchodilators, simply ask the patient if he/she were taking bronchodilator and whether they were of any benefit. To assess the severity of disease and predict whether someone can be extubated, one can depend on good H/P. While it is true that patients with preop FEV1<50% predicted are most likely to require postop mechanical ventilation, such predictions depends entirely on the type and course of surgery.
47 There is no best technique The choice o anesthetic depends on the: a) Type and duration of surgery; b) Preferences of the surgeon,, patient and anesthesiologist; c) Perioperative goals ( extubation, etc.) Is epidural always safe? Even though a motor blockade above T6 does not usually affect TV in normal individuals ( the diaphragm (C3-5) is the major muscle of respiration), it may impair respiration in COPD patients depend on active expiration.
48 How to ventilate the patient with COPD? Since the pathophysiology of COPD involves increased airway resistance that impedes exhalation, goals are to minimize this resistance and allow adequate gas emptying. a) Slow respiratory rates; b) Minimize peak airway pressures; c) Humidification of gases; d) 100% )2 if hypoxemia (PaO2<60 %) were present; Attempting to achieve normocapnia in a chronic CO2 retainer may cause alkalosis!
49 How to reduce the chances of postop respiratory complications? Good pain control Adequate Chest physiotherapy and incentive spirometry Bronchodilators should be continued, or if needed, begun Conservative fluid management ( to minimize the chances of pulmonary edema)
50 Chronic obstructive pulmonary disease is a common disease with a high incidence and a medico-economical impact which should not be underestimated. The extensive comorbidity of COPD patients as well as the impairment of the respiratory system make COPD a key challenge for every physician. Knowledge of the pathogenesis, course and prognosis, and new approaches to therapy have dramatically improved our understanding of this important clinical entity. Early identification and prevention, and adequate treatment of emerging stages of disease promises to change the outcome.
Lecture Notes. Chapter 4: Chronic Obstructive Pulmonary Disease (COPD)
") Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Lecture Notes Chapter 4: Chronic Obstructive Pulmonary Disease (COPD) Objectives Define COPD Estimate incidence of COPD in the US Define factors associated with onset of COPD Describe the clinical features
Basic mechanisms disturbing lung function and gas exchange
 Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Basic mechanisms disturbing lung function and gas exchange Blagoi Marinov, MD, PhD Pathophysiology Department, Medical University of Plovdiv Respiratory system 1 Control of breathing Structure of the lungs
Chronic Obstructive Pulmonary Disease (COPD) Clinical Guideline
 Clinical Guideline") Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
Chronic Obstructive Pulmonary Disease (COPD) Clinical These clinical guidelines are designed to assist clinicians by providing an analytical framework for the evaluation and treatment of patients. They
COPD. Helen Suen & Lexi Smith
 COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
COPD Helen Suen & Lexi Smith What is COPD? Chronic obstructive pulmonary disease: a non reversible, long term lung disease Characterized by progressively limited airflow and an inability to perform full
COPD. Breathing Made Easier
 COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
COPD Breathing Made Easier Catherine E. Cooke, PharmD, BCPS, PAHM Independent Consultant, PosiHleath Clinical Associate Professor, University of Maryland School of Pharmacy This program has been brought
Chronic Obstructive Pulmonary Disease (COPD) Copyright 2014 by Mosby, an imprint of Elsevier Inc.
 Copyright 2014 by Mosby, an imprint of Elsevier Inc.") Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
Chronic Obstructive Pulmonary Disease () 8.18.18 Copyright 2014 by Mosby, an imprint of Elsevier Inc. Description Airflow limitation not fully reversible progressive Abnormal inflammatory response of lungs
Respiratory Disease. Dr Amal Damrah consultant Neonatologist and Paediatrician
 Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
Respiratory Disease Dr Amal Damrah consultant Neonatologist and Paediatrician Signs and Symptoms of Respiratory Diseases Cardinal Symptoms Cough Sputum Hemoptysis Dyspnea Wheezes Chest pain Signs and Symptoms
You ve come a long way, baby.
 COPD Dr Badri Paudel Dept of Medicine GMC/CHRC 4/22/12 badri@gmc 2 You ve come a long way, baby. Wayne McLaren Former Marlboro Man 4/22/12 badri@gmc 3 Age 30 a robust young man Age 51 riding into the sunset
COPD Dr Badri Paudel Dept of Medicine GMC/CHRC 4/22/12 badri@gmc 2 You ve come a long way, baby. Wayne McLaren Former Marlboro Man 4/22/12 badri@gmc 3 Age 30 a robust young man Age 51 riding into the sunset
Chronic obstructive lung disease. Dr/Rehab F.Gwada
 Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
Chronic obstructive lung disease Dr/Rehab F.Gwada Obstructive lung diseases Problem is in the expiratory phase Lung disease Restrictive lung disease Restriction may be with, or within the chest wall Problem
COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis.
 1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
1 Definition of COPD: COPD is a syndrome of chronic limitation in expiratory airflow encompassing emphysema or chronic bronchitis. Airflow obstruction may be accompanied by airway hyper-responsiveness
2/4/2019. GOLD Objectives. GOLD 2019 Report: Chapters
 GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
GOLD Objectives To provide a non biased review of the current evidence for the assessment, diagnosis and treatment of patients with COPD. To highlight short term and long term treatment objectives organized
Lecture Notes. Chapter 3: Asthma
 Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Lecture Notes Chapter 3: Asthma Objectives Define asthma and status asthmaticus List the potential causes of asthma attacks Describe the effect of asthma attacks on lung function List the clinical features
Pulmonary Pathophysiology
 Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Pulmonary Pathophysiology 1 Reduction of Pulmonary Function 1. Inadequate blood flow to the lungs hypoperfusion 2. Inadequate air flow to the alveoli - hypoventilation 2 Signs and Symptoms of Pulmonary
Chronic Obstructive Pulmonary Disease
 Scope of Problem Chronic Obstructive Pulmonary Disease Marianne J. Davies, RN, MSN, APRN Yale University School of Medicine Yale Comprehensive Cancer Center Nevada Cancer Institute 2005 Hospitalizations
Scope of Problem Chronic Obstructive Pulmonary Disease Marianne J. Davies, RN, MSN, APRN Yale University School of Medicine Yale Comprehensive Cancer Center Nevada Cancer Institute 2005 Hospitalizations
Chronic obstructive pulmonary disease
 0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
0 Chronic obstructive pulmonary disease Implementing NICE guidance June 2010 NICE clinical guideline 101 What this presentation covers Background Scope Key priorities for implementation Discussion Find
RESPIRATORY EMERGENCIES. Michael Waters MD April 2004
 RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
RESPIRATORY EMERGENCIES Michael Waters MD April 2004 ASTHMA Asthma is a chronic inflammatory disease of the airways with variable or reversible airway obstruction Characterized by increased sensitivity
Differential diagnosis
 Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
Differential diagnosis The onset of COPD is insidious. Pathological changes may begin years before symptoms appear. The major differential diagnosis is asthma, and in some cases, a clear distinction between
People with asthma who smoke. The combination of asthma, a chronic airway disease, and smoking increases the risk of COPD even more.
 COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
COPD Chronic obstructive pulmonary disease (COPD) is a chronic inflammatory lung disease that causes obstructed airflow from the lungs. Symptoms include breathing difficulty, cough, sputum (phlegm) production
Course Handouts & Disclosure
 COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
COPD: Disease Trajectory and Hospice Eligibility Terri L. Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Hospice Education Network Course Handouts & Disclosure To download presentation
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation
 Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
Update on heterogeneity of COPD, evaluation of COPD severity and exacerbation Yung-Yang Liu, MD Taipei Veterans General Hospital Aug 29, 2015 G O lobal Initiative for Chronic bstructive L D ung isease
COPD: A Renewed Focus. Disclosures
 COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
COPD: A Renewed Focus Heath Latham, MD Assistant Professor Division of Pulmonary and Critical Care Medicine Disclosures No Business Interests No Consulting No Speakers Bureau No Off Label Use to Discuss
Decramer 2014 a &b [21]
![Decramer 2014 a &b [21]](/thumbs/90/101390504.jpg "Decramer 2014 a &b [21]") Buhl 2015 [19] Celli 2014 [20] Decramer 2014 a &b [21] D Urzo 2014 [22] Maleki-Yazdi 2014 [23] Inclusion criteria: Diagnosis of chronic obstructive pulmonary disease; 40 years of age or older; Relatively
Buhl 2015 [19] Celli 2014 [20] Decramer 2014 a &b [21] D Urzo 2014 [22] Maleki-Yazdi 2014 [23] Inclusion criteria: Diagnosis of chronic obstructive pulmonary disease; 40 years of age or older; Relatively
COPD/ Asthma. Dr Heather Lewis Honorary Clinical Lecturer
 COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
COPD/ Asthma Dr Heather Lewis Honorary Clinical Lecturer Objectives To understand the pathogenesis of asthma/ COPD To recognise the clinical features of asthma/ COPD To know how to diagnose asthma/ COPD
COPD Management in LTC: Presented By: Jessica Denney RRT
 COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
COPD Management in LTC: Presented By: Jessica Denney RRT Sponsored by Z & D Medical Services, Diamond Sponsor Seizing Opportunities to Provide Individualized Treatment and Device Selection for your COPD
Chronic obstructive pulmonary disease
 Chronic obstructive pulmonary disease By: Dr. Fatima Makee AL-Hakak () University of kerbala College of nursing Out lines What is the? Overview Causes of Symptoms of What's the difference between and asthma?
Chronic obstructive pulmonary disease By: Dr. Fatima Makee AL-Hakak () University of kerbala College of nursing Out lines What is the? Overview Causes of Symptoms of What's the difference between and asthma?
COPD. Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS
 IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
IN THE NAME OF GOD COPD Dr.O.Paknejad Pulmonologist Shariati Hospital TUMS Definition of COPD* COPD is a preventable and treatable chronic lung disease characterized by airflow limitation that is not fully
COPD exacerbation. Chiara Maruggi, PGY2
 COPD exacerbation Chiara Maruggi, PGY2 Learning objectives At the end of this lecture students will be able to: 1) Critically assess patients for COPD and design a management plan. 2) Develop a step-wise
COPD exacerbation Chiara Maruggi, PGY2 Learning objectives At the end of this lecture students will be able to: 1) Critically assess patients for COPD and design a management plan. 2) Develop a step-wise
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES
 MANAGEMENT GUIDELINES") JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
JOINT CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MANAGEMENT GUIDELINES Authors Dr Ian Benton Respiratory Consultant COCH Penny Rideal Respiratory Nurse COCH Kirti Burgul Respiratory Pharmacist COCH Pam
Fariba Rezaeetalab Associate Professor,Pulmonologist
 Fariba Rezaeetalab Associate Professor,Pulmonologist rezaitalabf@mums.ac.ir Patient related risk factors Procedure related risk factors Preoperative risk assessment Risk reduction strategies Age Obesity
Fariba Rezaeetalab Associate Professor,Pulmonologist rezaitalabf@mums.ac.ir Patient related risk factors Procedure related risk factors Preoperative risk assessment Risk reduction strategies Age Obesity
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline. MedStar Health
 Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Global Strategy for the Diagnosis, Management and Prevention of COPD 2016 Clinical Practice Guideline MedStar Health These guidelines are provided to assist physicians and other clinicians in making decisions
Chronic Obstructive Pulmonary Disease
 Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease 07 Contributor Dr David Tan Hsien Yung Definition, Diagnosis and Risk Factors for (COPD) Differential Diagnoses Goals of Management Management of COPD THERAPY AT EACH
Chronic Obstructive Pulmonary Disease
 136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
136 PHYSIOLOGY CASES AND PROBLEMS Case 24 Chronic Obstructive Pulmonary Disease Bernice Betweiler is a 73-year-old retired seamstress who has never been married. She worked in the alterations department
Exacerbations of COPD. Dr J Cullen
 Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
Exacerbations of COPD Dr J Cullen Definition An AECOPD is a sustained worsening of the patient s clinical condition from their stable state that is beyond their usual day-to-day variation is acute in onset
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss?
 ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
ASTHMA-COPD OVERLAP SYNDROME 2018: What s All the Fuss? Randall W. Brown, MD MPH AE-C Association of Asthma Educators Annual Conference July 20, 2018 Phoenix, Arizona FACULTY/DISCLOSURES Randall Brown,
What do pulmonary function tests tell you?
 Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
Pulmonary Function Testing Michael Wert, MD Assistant Professor Clinical Department of Internal Medicine Division of Pulmonary, Critical Care, and Sleep Medicine The Ohio State University Wexner Medical
2/12/2015. ASTHMA & COPD The Yin &Yang. Asthma General Information. Asthma General Information
 ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
ASTHMA & COPD The Yin &Yang Arizona State Association of Physician Assistants March 6, 2015 Sedona, Arizona Randy D. Danielsen, PhD, PA-C, DFAAPA Dean & Professor A.T. Still University Asthma General Information
Advances in Chronic Obstructive Pulmonary Disease
 Advances in Chronic Obstructive Pulmonary Disease By Dave C. Todd, MD; and Darcy D. Marciniuk, MD, FRCPC The case of Nina Nina, 64, presents to the clinic with a three- to fouryear history of progressive,
Advances in Chronic Obstructive Pulmonary Disease By Dave C. Todd, MD; and Darcy D. Marciniuk, MD, FRCPC The case of Nina Nina, 64, presents to the clinic with a three- to fouryear history of progressive,
Integrated Cardiopulmonary Pharmacology Third Edition
 Integrated Cardiopulmonary Pharmacology Third Edition Chapter 13 Pharmacologic Management of Asthma, Chronic Bronchitis, and Emphysema Multimedia Directory Slide 7 Slide 12 Slide 60 COPD Video Passive
Integrated Cardiopulmonary Pharmacology Third Edition Chapter 13 Pharmacologic Management of Asthma, Chronic Bronchitis, and Emphysema Multimedia Directory Slide 7 Slide 12 Slide 60 COPD Video Passive
Chronic Obstructive Lung Disease - Dr. Kawa Chronic Bronchitis & Emphysema
 Chronic Obstructive Lung Disease - Dr. Kawa Chronic Bronchitis & Emphysema COPD Definition COPD is a chronic, slowly progressive disorder characterized by airflow obstruction. (FEV1 is less than 80% of
Chronic Obstructive Lung Disease - Dr. Kawa Chronic Bronchitis & Emphysema COPD Definition COPD is a chronic, slowly progressive disorder characterized by airflow obstruction. (FEV1 is less than 80% of
Chronic Obstructive Pulmonary Disease Guidelines and updates
 Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
Chronic Obstructive Pulmonary Disease Guidelines and updates October 20, 2018 Saratoga Springs, NY COPD (Chronic obstructive pulmonary disease) is a major cause of mortality and morbidity in the United
COPD: Current Medical Therapy
 COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
COPD: Current Medical Therapy Angela Golden, DNP, FNP-C, FAANP Owner, NP from Home, LLC Outcomes As a result of this activity, learners will be able to: 1. List the appropriate classes of medications for
COPD: Preventable and Treatable. Lecture Outline. Diagnosis of COPD. COPD: Defining Terms
 COPD: Preventable and Treatable Christopher H. Fanta, M.D. Partners Asthma Center Pulmonary and Critical Care Division Brigham and Women s Hospital Harvard Medical School Lecture Outline I. Diagnosis and
COPD: Preventable and Treatable Christopher H. Fanta, M.D. Partners Asthma Center Pulmonary and Critical Care Division Brigham and Women s Hospital Harvard Medical School Lecture Outline I. Diagnosis and
Function of the Respiratory System. Exchange CO2 (on expiration) for O2 (on inspiration)
 for O2 (on inspiration)") Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
Function of the Respiratory System Exchange CO2 (on expiration) for O2 (on inspiration) Upper Respiratory Tract Includes: Nose Mouth Pharynx Larynx Function: Warms and humidifies the inspired air Filters
COPD/Asthma. Prudence Twigg, AGNP
 COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
COPD/Asthma Prudence Twigg, AGNP COPD/Asthma Qualifying Diagnosis Known diagnosis of COPD/asthma or CXR showing COPD with hyperinflated lungs and no infiltrates + two or more: Wheezing, SOB, increased
RESPIRATORY PHYSIOLOGY Pre-Lab Guide
 RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
RESPIRATORY PHYSIOLOGY Pre-Lab Guide NOTE: A very useful Study Guide! This Pre-lab guide takes you through the important concepts that where discussed in the lab videos. There will be some conceptual questions
Pulmonary Function Testing: Concepts and Clinical Applications. Potential Conflict Of Interest. Objectives. Rationale: Why Test?
 Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
Pulmonary Function Testing: Concepts and Clinical Applications David M Systrom, MD Potential Conflict Of Interest Nothing to disclose pertinent to this presentation BRIGHAM AND WOMEN S HOSPITAL Harvard
ASTHMA. Epidemiology. Pathophysiology. Diagnosis. IAP UG Teaching slides
 BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
BRONCHIAL ASTHMA ASTHMA Epidemiology Pathophysiology Diagnosis 2 CHILDHOOD ASTHMA Childhood bronchial asthma is characterized by Airway obstruction which is reversible Airway inflammation Airway hyper
PULMONARY FUNCTION TESTS
 Chapter 4 PULMONARY FUNCTION TESTS M.G.Rajanandh, Department of Pharmacy Practice, SRM College of Pharmacy, SRM University. OBJECTIVES Review basic pulmonary anatomy and physiology. Understand the reasons
Chapter 4 PULMONARY FUNCTION TESTS M.G.Rajanandh, Department of Pharmacy Practice, SRM College of Pharmacy, SRM University. OBJECTIVES Review basic pulmonary anatomy and physiology. Understand the reasons
The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE
 The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE RHYS JEFFERIES ARTP education Learning Objectives Examine the clinical features of airways disease to distinguish
The role of lung function testing in the assessment of and treatment of: AIRWAYS DISEASE RHYS JEFFERIES ARTP education Learning Objectives Examine the clinical features of airways disease to distinguish
Lab 4: Respiratory Physiology and Pathophysiology
 Lab 4: Respiratory Physiology and Pathophysiology This exercise is completed as an in class activity and including the time for the PhysioEx 9.0 demonstration this activity requires ~ 1 hour to complete
Lab 4: Respiratory Physiology and Pathophysiology This exercise is completed as an in class activity and including the time for the PhysioEx 9.0 demonstration this activity requires ~ 1 hour to complete
How to treat COPD? What is the mechanism of dyspnea? Smoking cessation
 : The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
: The Increasing Role of the FP Alan Kaplan, MD, CCFP(EM) Presented at the Primary Care Today: Education Conference and Medical Exposition, Toronto, Ontario, May 2006. Chronic obstructive pulmonary disease
Guideline for the Diagnosis and Management of COPD
 Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Guideline for the Diagnosis and Management of COPD Introduction Chronic obstructive pulmonary disease (COPD) is a respiratory disorder largely caused by smoking. It is characterized by progressive, partially
Pathophysiology of COPD 건국대학교의학전문대학원
 Pathophysiology of COPD 건국대학교의학전문대학원 내과학교실 유광하 Rate per 100 0,000 population 550 500 450 400 350 300 250 200 150 100 50 0 Heart disease Cancer Stroke 1970 1974 1978 1982 1986 1990 1994 1998 2002 Year of
Pathophysiology of COPD 건국대학교의학전문대학원 내과학교실 유광하 Rate per 100 0,000 population 550 500 450 400 350 300 250 200 150 100 50 0 Heart disease Cancer Stroke 1970 1974 1978 1982 1986 1990 1994 1998 2002 Year of
CHRONIC OBSTRUCTIVE PULMONARY DISEASE
 CHRONIC OBSTRUCTIVE PULMONARY DISEASE DEFINITION Chronic obstructive pulmonary disease (COPD) is a common preventable and treatable disease characterized by airflow limitation that is usually progressive
CHRONIC OBSTRUCTIVE PULMONARY DISEASE DEFINITION Chronic obstructive pulmonary disease (COPD) is a common preventable and treatable disease characterized by airflow limitation that is usually progressive
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING 10/16/2018 DISCLOSURES I have no financial or other disclosures
 OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
OPTIMIZING MANAGEMENT OF COPD IN THE PRACTICE SETTING J. Michael Fuller, MD, MEd, FACP, FCCP Associate Professor of Medicine University of South Carolina Greenville DISCLOSURES I have no financial or other
Emphysema. Lungs The lungs help us breathe in oxygen and breathe out carbon dioxide. Everyone is born with 2 lungs: a right lung and a left lung.
 Emphysema Introduction Emphysema is a type of chronic obstructive pulmonary disease, or COPD. COPD affects millions of people worldwide. Emphysema involves damage to the air sacs in the lungs. This makes
Emphysema Introduction Emphysema is a type of chronic obstructive pulmonary disease, or COPD. COPD affects millions of people worldwide. Emphysema involves damage to the air sacs in the lungs. This makes
Defining COPD. Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist
 Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
Defining COPD Georgina Grantham Community Respiratory Team Leader/ Respiratory Nurse Specialist Defining COPD Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease
They are updated regularly as new NICE guidance is published. To view the latest version of this NICE Pathway see:
 bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
bring together everything NICE says on a topic in an interactive flowchart. are interactive and designed to be used online. They are updated regularly as new NICE guidance is published. To view the latest
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX
 MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX") CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX COPD OUTLINE Definition and Overview Pathophysiology Diagnosis and Assessment Therapeutic
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) MOUSTAPHA ABIDALI, DO CRITICAL CARE FELLOW UNIVERSITY OF ARIZONA- PHOENIX COPD OUTLINE Definition and Overview Pathophysiology Diagnosis and Assessment Therapeutic
Author(s): Frank Madore (Hennepin County Medical Center), MD 2012
: Frank Madore (Hennepin County Medical Center), MD 2012") Project: Ghana Emergency Medicine Collaborative Document Title: COPD in the Emergency Department Author(s): Frank Madore (Hennepin County Medical Center), MD 2012 License: Unless otherwise noted, this
Project: Ghana Emergency Medicine Collaborative Document Title: COPD in the Emergency Department Author(s): Frank Madore (Hennepin County Medical Center), MD 2012 License: Unless otherwise noted, this
Overview of COPD INTRODUCTION
 Overview of COPD INTRODUCTION Chronic obstructive pulmonary disease (COPD) is a common lung disease that affects millions of people, and it is the fourth leading cause of death in the United States. It
Overview of COPD INTRODUCTION Chronic obstructive pulmonary disease (COPD) is a common lung disease that affects millions of people, and it is the fourth leading cause of death in the United States. It
CARE OF THE ADULT COPD PATIENT
 CARE OF THE ADULT COPD PATIENT Target Audience: The target audience for this clinical guideline is all MultiCare providers and staff including those associated with our Clinically Integrated Network. The
CARE OF THE ADULT COPD PATIENT Target Audience: The target audience for this clinical guideline is all MultiCare providers and staff including those associated with our Clinically Integrated Network. The
Respiratory Medicine
 Respiratory Medicine This document is based on the handout from the Medicine for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical examinations.
Respiratory Medicine This document is based on the handout from the Medicine for Finals course. The notes provided here summarise key aspects, focusing on areas that are popular in clinical examinations.
Chronic Obstructive Pulmonary Disease (COPD)
") Chronic Obstructive Pulmonary Disease (COPD) Definition of COPD Airflow obstruction that is: o Not fully reversible o Progressive o Does not change markedly over several months Combination of airway and
Chronic Obstructive Pulmonary Disease (COPD) Definition of COPD Airflow obstruction that is: o Not fully reversible o Progressive o Does not change markedly over several months Combination of airway and
Asthma COPD Overlap (ACO)
") Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
Asthma COPD Overlap (ACO) Dr Thomas Brown Consultant Respiratory Physician Thomas.Brown@porthosp.nhs.uk Dr Hitasha Rupani Consultant Respiratory Physician Hitasha.rupani@porthosp.nhs.uk What is Asthma
BPCO/COPD. Andrea Bellone UOC di Pronto Soccorso Ospedale Sant'Anna di Como
 BPCO/COPD Andrea Bellone UOC di Pronto Soccorso Ospedale Sant'Anna di Como Definition of COPD (1) COPD is a preventable and treatable disease state characterised by airflow limitation that is not fully
BPCO/COPD Andrea Bellone UOC di Pronto Soccorso Ospedale Sant'Anna di Como Definition of COPD (1) COPD is a preventable and treatable disease state characterised by airflow limitation that is not fully
COPD- pulmonary hyperinflation- the diaphragms are at the level of the eleventh posterior ribs and appear flat.
 COPD COPD Hallmark symptom - Dyspnea Chronic productive cough Minor hemoptysis pink puffer blue bloater COPD- pulmonary hyperinflation- the diaphragms are at the level of the eleventh posterior ribs and
COPD COPD Hallmark symptom - Dyspnea Chronic productive cough Minor hemoptysis pink puffer blue bloater COPD- pulmonary hyperinflation- the diaphragms are at the level of the eleventh posterior ribs and
Running head: BEST-PRACTICE NURSING CARE FOR PATIENTS WITH 1 CHRONIC OBSTRUCTIVE PULMONARY DISEASE
 Running head: BEST-PRACTICE NURSING CARE FOR PATIENTS WITH 1 CHRONIC OBSTRUCTIVE PULMONARY DISEASE Best-Practice Nursing Care for Patients with Chronic Obstructive Pulmonary Disease Jessica N. Anderson,
Running head: BEST-PRACTICE NURSING CARE FOR PATIENTS WITH 1 CHRONIC OBSTRUCTIVE PULMONARY DISEASE Best-Practice Nursing Care for Patients with Chronic Obstructive Pulmonary Disease Jessica N. Anderson,
RESPIRATORY CARE IN GENERAL PRACTICE
 RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
RESPIRATORY CARE IN GENERAL PRACTICE Definitions of Asthma and COPD Asthma is due to inflammation of the air passages in the lungs and affects the sensitivity of the nerve endings in the airways so they
Unconscious exchange of air between lungs and the external environment Breathing
 Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Respiration Unconscious exchange of air between lungs and the external environment Breathing Two types External Exchange of carbon dioxide and oxygen between the environment and the organism Internal Exchange
Overview of Obstructive Diseases of the Lung, Lung Physiology and Imaging Modalities
 Overview of Obstructive Diseases of the Lung, Lung Physiology and Imaging Modalities Jann Mortensen Final Phil meeting, 29 april 2004 Obstructive disease Definition Epidemiologi Mechanisms Natural history
Overview of Obstructive Diseases of the Lung, Lung Physiology and Imaging Modalities Jann Mortensen Final Phil meeting, 29 april 2004 Obstructive disease Definition Epidemiologi Mechanisms Natural history
Over the last several years various national and
 Recommendations for the Management of COPD* Gary T. Ferguson, MD, FCCP Three sets of guidelines for the management of COPD that are widely recognized (from the European Respiratory Society [ERS], American
Recommendations for the Management of COPD* Gary T. Ferguson, MD, FCCP Three sets of guidelines for the management of COPD that are widely recognized (from the European Respiratory Society [ERS], American
Clinical Pathological Correlation of Chronic Obstructive Pulmonary Disease (COPD)*
*") Clinical Pathological Correlation of Chronic Obstructive Pulmonary Disease (COPD)* ORHAN MUREN, M.D. Associate Professor of Medicine and Anesthesiology, Medical College of Virginia, Health Sciences Division
Clinical Pathological Correlation of Chronic Obstructive Pulmonary Disease (COPD)* ORHAN MUREN, M.D. Associate Professor of Medicine and Anesthesiology, Medical College of Virginia, Health Sciences Division
DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 2: ATELECTASIS AND EMPHYSEMA
 DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 2: ATELECTASIS AND EMPHYSEMA INTRODUCTION In this lecture we will discuss atelectasis which is a complication of several medical and surgical
DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 2: ATELECTASIS AND EMPHYSEMA INTRODUCTION In this lecture we will discuss atelectasis which is a complication of several medical and surgical
Asthma - Chronic. Presentations of asthma Cough Wheeze Breathlessness Chest tightness
 Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Asthma - Chronic Definition of asthma Chronic inflammatory disease of the airways 3 components: o Reversible and variable airflow obstruction o Airway hyper-responsiveness to stimuli o Inflammation of
Paramedic Rounds. Pre-Hospital Continuous Positive Airway Pressure (CPAP)
") Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
Paramedic Rounds Pre-Hospital Continuous Positive Airway Pressure (CPAP) Morgan Hillier MD Class of 2011 Dr. Mike Peddle Assistant Medical Director SWORBHP Objectives Outline evidence for pre-hospital
DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 3: CHRONIC BRNCHITIS AND BRONCHIECTASIS
 DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 3: CHRONIC BRNCHITIS AND BRONCHIECTASIS INTRDUCTION In the last lecture we discussed the difference between restrictive and obstructive lung
DISEASES OF THE RESPIRATORY SYSTEM 2018 DR HEYAM AWAD LECTURE 3: CHRONIC BRNCHITIS AND BRONCHIECTASIS INTRDUCTION In the last lecture we discussed the difference between restrictive and obstructive lung
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Chronic obstructive pulmonary disease: the management of adults with chronic obstructive pulmonary disease in primary and secondary
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Chronic obstructive pulmonary disease: the management of adults with chronic obstructive pulmonary disease in primary and secondary
The Respiratory System
 130 20 The Respiratory System 1. Define important words in this chapter 2. Explain the structure and function of the respiratory system 3. Discuss changes in the respiratory system due to aging 4. Discuss
130 20 The Respiratory System 1. Define important words in this chapter 2. Explain the structure and function of the respiratory system 3. Discuss changes in the respiratory system due to aging 4. Discuss
COPD. Definitionn. make. when (bronchioles) in. the lungs. Wheezing Chest tightness. your lungs. greenish. Lack of energy
 in. the lungs. Wheezing Chest tightness. your lungs. greenish. Lack of energy") COPD Definitionn Emphysema and chronic bronchitis are the two most common conditions thatt make up COPD. Chronic bronchitis is an inflammation of the lining of your bronchial tubes, which carry air to
COPD Definitionn Emphysema and chronic bronchitis are the two most common conditions thatt make up COPD. Chronic bronchitis is an inflammation of the lining of your bronchial tubes, which carry air to
Pulmonary Pearls. Medical Pearls. Case 1: Case 1 (cont.): Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):
: Case 1: What is the Most Likely Diagnosis? Case 1 (cont.):") Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Pulmonary Pearls Christopher H. Fanta, MD Pulmonary and Critical Care Division Brigham and Women s Hospital Partners Asthma Center Harvard Medical School Medical Pearls Definition: Medical fact that is
Respiratory diseases in Ostrołęka County
 Respiratory diseases in Ostrołęka County 4400 persons underwent examination 950 persons were given referrals to more detailed investigation 600 persons were examined so far The results of more detailed
Respiratory diseases in Ostrołęka County 4400 persons underwent examination 950 persons were given referrals to more detailed investigation 600 persons were examined so far The results of more detailed
Anyone who smokes and/or has shortness of breath and sputum production could have COPD
 COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
COPD DIAGNOSIS AND MANAGEMENT CHECKLIST Anyone who smokes and/or has shortness of breath and sputum production could have COPD Confirm Diagnosis Presence and history of symptoms: Shortness of breath Cough
Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD)
 Instructions for the Pulmonary Diagnosis Form (PLD)") Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD) A Pulmonary Diagnosis Form is filled out by the reviewer for all medical records that are sent to them for review by the CSCC.
Question by Question (QXQ) Instructions for the Pulmonary Diagnosis Form (PLD) A Pulmonary Diagnosis Form is filled out by the reviewer for all medical records that are sent to them for review by the CSCC.
A Place For Airway Clearance Therapy In Today s Healthcare Environment
 A Place For Airway Clearance Therapy In Today s Healthcare Environment Michigan Society for Respiratory Care 2015 Fall Conference K. James Ehlen, MD October 6, 2015 Objectives Describe patients who will
A Place For Airway Clearance Therapy In Today s Healthcare Environment Michigan Society for Respiratory Care 2015 Fall Conference K. James Ehlen, MD October 6, 2015 Objectives Describe patients who will
Introduction and Overview of Acute Respiratory Failure
 Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Introduction and Overview of Acute Respiratory Failure Definition: Acute Respiratory Failure Failure to oxygenate Inadequate PaO 2 to saturate hemoglobin PaO 2 of 60 mm Hg ~ SaO 2 of 90% PaO 2 of 50 mm
Air Flow Limitation. In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation.
 Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Asthma Air Flow Limitation In most serious respiratory disease, a key feature causing morbidity and functional disruption is air flow imitation. True whether reversible, asthma and exercise-induced bronchospasm,
Internal medicine. Lec #: 4 Date: COPD-Definition
 Internal medicine Topic: COPD Dr: mousa malkawy Lec #: 4 Date: 26-10-2009 COPD-Definition A disease state characterized by airflow limitation that is not fully reversible and usually it is progressive
Internal medicine Topic: COPD Dr: mousa malkawy Lec #: 4 Date: 26-10-2009 COPD-Definition A disease state characterized by airflow limitation that is not fully reversible and usually it is progressive
Pulmonary Function Testing The Basics of Interpretation
 Pulmonary Function Testing The Basics of Interpretation Jennifer Hale, M.D. Valley Baptist Family Practice Residency Objectives Identify the components of PFTs Describe the indications Develop a stepwise
Pulmonary Function Testing The Basics of Interpretation Jennifer Hale, M.D. Valley Baptist Family Practice Residency Objectives Identify the components of PFTs Describe the indications Develop a stepwise
PATHOPHYSIOLOGICAL PROCESS TEMPLATE
 1 PATHOPHYSIOLOGICAL PROCESS TEMPLATE DISEASE: Chronic obstructive pulmonary disease (COPD) DEFINITION: COPD can be defined as a disease in which there is a significant damage to the lungs thus reducing
1 PATHOPHYSIOLOGICAL PROCESS TEMPLATE DISEASE: Chronic obstructive pulmonary disease (COPD) DEFINITION: COPD can be defined as a disease in which there is a significant damage to the lungs thus reducing
HASPI Medical Anatomy & Physiology 14b Lab Activity
 HASPI Medical Anatomy & Physiology 14b Lab Activity Name(s): Period: Date: Respiratory Distress Respiratory distress is a broad medical term that applies to any type of breathing difficulty and the associated
HASPI Medical Anatomy & Physiology 14b Lab Activity Name(s): Period: Date: Respiratory Distress Respiratory distress is a broad medical term that applies to any type of breathing difficulty and the associated
3. Identify the importance in the prehospital setting for the administration of nebulized bronchodilator.
 TERMINAL OBJECTIVE At the end of this lesson, the EMT-Basic will be able to utilize the assessment findings to formulate a field impression of bronchospasm and understand the administration of nebulized
TERMINAL OBJECTIVE At the end of this lesson, the EMT-Basic will be able to utilize the assessment findings to formulate a field impression of bronchospasm and understand the administration of nebulized
COPD. Stan Kellar, MD. Physiology 11/4/2014. Chief of Clinical Affairs, BH NLR Pulmonary Medicine Sleep Medicine
 Stan Kellar, MD Chief of Clinical Affairs, BH NLR Pulmonary Medicine Sleep Medicine COPD Physiology The lungs are filters Filter in oxygen Filter out carbon dioxide (Vascular filter, not part of this discussion)
Stan Kellar, MD Chief of Clinical Affairs, BH NLR Pulmonary Medicine Sleep Medicine COPD Physiology The lungs are filters Filter in oxygen Filter out carbon dioxide (Vascular filter, not part of this discussion)
PATHOPHYSIOLOGY OF RESPIRATION 2
 PATHOPHYSIOLOGY OF RESPIRATION 2 Obstructive disorders R. Benacka Department of Pathophysiology, Medical faculty, P.J. Safarik University Košice Respiratory diseases Obstructive diseases (OPD) - restricted
PATHOPHYSIOLOGY OF RESPIRATION 2 Obstructive disorders R. Benacka Department of Pathophysiology, Medical faculty, P.J. Safarik University Košice Respiratory diseases Obstructive diseases (OPD) - restricted
Significance. Asthma Definition. Focus on Asthma
 Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
Focus on Asthma (Relates to Chapter 29, Nursing Management: Obstructive Pulmonary Diseases, in the textbook) Asthma Definition Chronic inflammatory disorder of airways Causes airway hyperresponsiveness
COPD: Applying New Guidelines to Optimizing Evaluation and Treatment
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Chronic Obstructive Pulmonary Disease:
 Chronic Obstructive Pulmonary Disease: THE BASICS PROF.G.E. ERHABOR Consultant Chest Physician Obafemi Awolowo University Teaching Hospital Complex, Ile-Ife, Nigeria. 1 BASICS IS THE ESSENCE OF GREATNESS,
Chronic Obstructive Pulmonary Disease: THE BASICS PROF.G.E. ERHABOR Consultant Chest Physician Obafemi Awolowo University Teaching Hospital Complex, Ile-Ife, Nigeria. 1 BASICS IS THE ESSENCE OF GREATNESS,
& Guidelines. For The Management Of. Chronic Obstructive Air Way Disease (COPD)
") Guidelines For The Management Of Chronic Obstructive Air Way Disease (COPD) By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Dr.Layla Al-Shahrabani F.R.C.P (UK) Director of Clinical Affairs
Guidelines For The Management Of Chronic Obstructive Air Way Disease (COPD) By Dr. Sinan Butrus F.I.C.M.S Clinical Standards & Guidelines Dr.Layla Al-Shahrabani F.R.C.P (UK) Director of Clinical Affairs
Chronic Obstructive Pulmonary Disease
 Page 1 of 5 Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease (COPD) is an 'umbrella' term for people with chronic bronchitis, emphysema, or both. With COPD the airflow to the
Page 1 of 5 Chronic Obstructive Pulmonary Disease Chronic Obstructive Pulmonary Disease (COPD) is an 'umbrella' term for people with chronic bronchitis, emphysema, or both. With COPD the airflow to the
Spirometry: Introduction
 Spirometry: Introduction Dr. Badri Paudel 1 2 GMC Spirometry Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after a maximal expiration.
Spirometry: Introduction Dr. Badri Paudel 1 2 GMC Spirometry Spirometry is a method of assessing lung function by measuring the volume of air the patient can expel from the lungs after a maximal expiration.