Brachytherapy:General Principles
|
|
|
- Jonas Kelley
- 6 years ago
- Views:
Transcription


1 Brachytherapy:General Principles Dr. S.C.Sharma Professor & Head Department foradiotherapy and Oncology, Regional Cancer Centre, Postgraduate Institute of Medical Education and Research Chandigarh
2 Brachytherapy: The precise answer for tackling cancer Derives from the Greek word brachy meaning short-distance Brachytherapyinvolves placing small radiation sources internally, either into or immediately next to the tumorin a geometrical fashion, allowing precise radiation dose delivery 1 Treating the cancer from the inside, out Brachytherapy works from the inside, out EBRT works from the outside, in 1. Stewart AJ & Jones B. In Devlin Brachytherapy: Applications and techniques
3 Traditional EBRT and brachytherapy EBRT Brachytherapy Treated volume Large Small Dose distribution Homogenous Heterogenous Dose rate High Variable HDR, LDR, (PDR) Fractionation Multiple Few Treatment duration Long; weeks to months Short; hours to days Adapted from Mazeron JJ, Scalliet P, Van Limbergen E et al. In: The GEC ESTRO Handbook of Brachytherapy
4 Key concepts: Dose distribution Unlike EBRT, brachytherapy is able to deliver a highly conformal dose at a high dose rate Smaller volume Higher dose Fewer fractions Short treatment Prevents repopulation of cancer cells Limits toxicity to surrounding tissue Inverse Square Law Gerbaulet A, Ash D, Meertems H et al. In The GEC ESTRO handbook of brachytherapy
5 Brachytherapy:History 1896 Radioactivity was described by Becquerel 1898 Marie curie extracted radium from pitchblende ore 1901 Danlos and Bloc performed first radium implant (1901) 1931 The term brachytherapy proposed first time by Forsell s Co⁶⁰,Ta¹⁸², Cs¹³⁷, Ir¹⁹² first used in brachytherapy Cs¹³⁷ began to replace Ra²²⁶ 1953 Aterloadingtechnique first introduced by Henschkein New York removed hazard of radiation exposure. Also Ir-192 used first time by Henschke
6 Brachytherapy:History Brachytherapy rules were developed and followed 1953 LDR brachytherapy became the gold standard 1968 HDR brachytherapy was introduced 1950s and 1960s New radioactive sources, techniques and equipment, which prevented unnecessary radiation exposure to patients and clinicians led to a renaissance for brachytherapy s Brachytherapy is established as a safe and effective standard of care for many gynecological cancers 5 Present day Brachytherapy a valued treatment option for many types of cancer, with a wealth of supporting evidence 4,5 with maqny advances. 1. Gupta VK. J Medical Physics 1995;20(2): Nag S. American Brachytherapy Society. 3. Aronowitz JN, Aronowitz SV Robison RF. Brachyther 2007;6: Blasko JC, Wallner K, Grimm PD et al. J Urol 1995;154: Viani GA, Manta GB, Stefano EJ et al. J Exp Clin Cancer Res 2009;28:47.
7 History of Brachytherapy Rules for implantation were made for LDR Interstitial Brachytherapy: Surface Mould Manchester system Manchester system Quimby System Memorial System Paris system Intracavitary Brachytherapy: Stockholm system (1914) Paris System (1926) Manchester System (1938) Last 4 decades have seen the emergence of remote after loading system ( selectronmachine LDR machine first time used in 1970 for ca cx) HDR became widely accepted after a long struggle in early 90 s PDR has been developed Now with more sophisticated imaging, hardware and software : image based and image guided brachytherapyhas come up.
8 Advantages 1. High dose of radiation is delivered to tumor in short time. So biologically very effective 2. Normal tissue spared due to rapid dose fall off 3. Better tumor control 4. Radiation morbidity minimal 5. Cosmetic superiority over teletherapy 6. Acute reactions appear when treatment is over; so no treatment breaks. Also radiation reactions localized & manageable 7. Treatment time short reduces risk of tumor repopulation 8. Therapeutic ratio high 9. Also decreased burden on patient & family
9 Limitations 1. Applicable to accessible sites only 2. Application limited to small size tumors ( T1, T2 )
10 Disadvantages 1. Invasive procedure 2. Radiation hazard due to radioisotopes (in olden days due to preloading techniques, now risk decreased ) 3. General anesthesia required 4. Dose inhomogeneity is higher than EBRT (but acceptable if rules followed) 5. Because of greater conformity, small errors in source placement can lead to extreme changes from the intended dose distribution 6. Present day brachytherapy is costly
11 Types of brachytherapy Classification schemes: 1. depending on use/radionuclide position 2. depending on loading pattern 3. depending on duration of irradiation 4. depending on dose rate
12 Types of Brachytherapy Depending on use (surgical approach to target volume) o Source in contact with but superficial to tumor: surface moulds o Source inside the tumor/target Interstitial Intracavitary Intraluminal Intravascular
13 Surface dose applications (plesiocurie/mold therapy) consists of an applicator containing array of radioactive sources designed to deliver a uniform dose distribution to skin/mucosal surface Interstitial brachytherapy surgically implanting small radioactive sources directly into target tissues Intracavitary brachytherapy consists of positioning applicators bearing radioactive sources into the body cavity in close proximity to target tissue Transluminal brachytherapy consists of inserting single line source into a body lumen to treat its surface &adjacent tissue Intravascular brachytherapy
14 Types of Brachytherapy Depending on source loading pattern: Preloaded: inserting needles/tubes containing radioactive material directly into the tumor After loaded: first, the non-radioactive tubes inserted into tumor Manual: Ir 192 wires, sources manipulated into applicator by means of forceps & hand-held tools Computerized remote controlled after loaded: consists of pneumatically or motor-driven source transport system

15 Preloading pattern Advantage: Loose & flexible system(can be inserted even in distorted cervix) Excellent clinical result Cheap Long term results with least morbidity (due to LDR) Disadvantages: Hasty application -Improper geometry in dose distribution Loose system high chance of slipping of applicators improper geometry Application needed special instruments to maintain distance. Radiation hazard Optimization not possible
16 After loading pattern MANUAL AFTERLOADING Advantages 1. Circumvents radiation protection problems of preloading 2. Allows better applicator placement and verification prior to source placement. 3. Radiation hazard can be minimized in the OT / bystanders as patient loaded in ward. 4. Advantages of preloading remain as practised at LDR. Disadvantages: specialized applicators are required.






17 APPLICATORS Gynae Applicators Vaginal Sorbo Esophageal Bougie Nasopharyngeal Applicator Steel Needles Plastic Catheters & Buttons
18 REMOTE AFTERLOADING Advantages : 1. No radiation hazard 2. Accurate applicator placement -ideal geometry maintained -dose homogeneity achieved -better dose distribution 3. Information on source positions available 4. Individualization & optimization of treatment possible 5. Higher precision, better control 6. Decreased treatment time- opd treatment possible 7. Chances of source loss nil. Disadvantages : 1. costly 2. Still some grey areas in dose conversions




19 AfterloadingSystems Selectron MDR Microselectron,Varies Source & Gammamed
20 Types of Brachytherapy Depending on Dose-Rate used Acc. To ICRU REPORT no.38 : Low dose rate (LDR): Gy/hour Hours to days- Confinement to bed LDR A/L: 1970s using Cs 137 Medium dose rate (MDR): 2-12 Gy/hour in Mid 70s Cs137- ROUGHLY LDR 10 Gy/day MDR -10 Gy/hr HDR 10 Gy/min High dose rate (HDR): >12 Gy/hour (0.2 Gy/min) 1 st in 1968-joslin (cathetron) 1984-PGI (Co 60 source drawn to high intensity) Ultra-low dose rate (ULDR): Gy/hour
21 LDR-advantages 1. Clinical effects predictable -large body of data spanning 4-5 decades -experience with various radionuclides 2. Radiobiologically superior -allows continous radiation to tumor as well as simultaneous repair of sublethal damage in normal tissues 3. Long experience -well defined rules for use exist which allow optimum implant dosimetry 4. Less morbidity & best tumor control 5. Cheap 6. Since 1-2 sessions required -intersession variability in dose distribution minimized
22 LDR-disadvantages 1. Treatment continuous and prolonged. -confined to bed 2. Geometry and distribution not properly maintained 3. Limited applicability in elderly patients, with respiratory, cardiac problems 4. Individualization & optimization not possible
 2.")
23 MDR ADVANTAGES : 1. treatment completed in shorter treatment time 2. increased patient convenience 3. considered radiobiologically nearer to LDR brachytherapy DISADVANTAGES : 1. without correction, increased incidence of late complication (20 30 %) 2. few results despite widespread use at one time
24 HDR-advantage 1.Shorter treatment times, resulting in: a) OPD based treatment possible b) Less patient discomfort ( prolonged bed rest is eliminated ) c) Reduced applicator movement during therapy(geometry well maintained) d) Greater displacement of nearby normal tissues. e) Possibility of treating larger number of patients
25 2. Allows use of smaller & thinner applicators than are used in LDR: a) Resulting in lesser tissue trauma b) Reducing the need for dilatation of the cervix and therefore reducing the need for heavy sedation or general anesthesia (allowing treatment for high-risk patients who are unable to tolerate general anesthesia). c) Geometrical sparing can circumvent radio biological disadvantage 3. Tailor dose distribution to target through optimization due to stepping source technique used. 4. Elimination of exposure to personnel

26 HDR-disadvantages 1. Decreased therapeutic ratio -short treatment time-doesn t allow repair of sublethal damage to normal tissues and redistribution & reoxygenation of tumor cells(radiobiologically inferior as normal tissue becomes more sensitive) 2. Multiple sessions -different geometry each time 3. Less time to detect & correct error 4. Limited experience -till recently, no standard guidelines 5. Economic disadvantage -Labour intensive -large capital investment
27 PDR Brachytherapy Series of short HDR treatments ( 10 minute pulse repeated at 1 hr intervals) replacing the continuous LDR treatment lasting several days- PDR BT. Overall time remains same as LDR Source strength : 1 Ci ADVANTAGE: radiobiologically nearer to LDR optimization possible
28 Types of Brachytherapy Depending upon means of controlling dose delivered(duration of irradiation) Temporary/Removable implants when the radioactive source implanted into the tumor tissue is allowed to remain there for definite period. Ex Cs¹³⁷, Ir¹⁹² Permanent implants when the sources are implanted indefinitely ex: Pd¹⁰³, Au¹⁹⁸ These terms used for interstitial form of brachytherapy
29 Permanent implant Advantages : 1. Useful for less accessible sites (e.g. prostate, endovascular) 2. Allows a continuous ultra-low dose rate treatment (maximum biological effectiveness) 3. Allows better normal tissue healing due to low dose rate 4. Cell kill predominantly by alpha damage (KeV photons, PE effect) better efficacy in slow growing and radioresistant tumors. 5. Patient mobility maintained after procedure
30 Disadvantages : 1. Radiation protection issues in case of source being excreted (e.g. urine) 2. Dosimetry uncertain due to short half life latter part of treatment becomes progressively less effective 3. Source migrations known to occur resultant perturbation in dose distributions 4. Sources expensive can t be reused. 5. Complicated implant procedure difficult to maintain geometry esp. for larger tumors. 6. Radiobiologically inferior in rapidly proliferating tumors
31 Radioactive sources Obsolete or historical 226 Ra, 222 Rn Currently used sealed sources 137 Cs, 192 Ir, 60 Co, 125 I, 103 Pd, 198 Au, 90 Sr. Developmental sealed sources 241 Am, 169 Yb, 252 Cf, 131 Cs, 145 Sm.
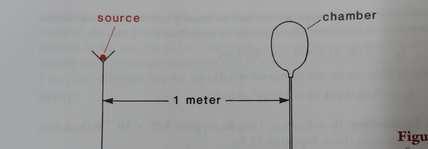
32 Characteristics of a radioisotope Half life- Time required for the activity of the source to decay to half the initial value. Gamma energy Specific activity- Activity per unit mass of a radio nuclide.(ci/gm) Half value layer- Thickness of the material required to decrease the intensity of the incident beam to half of it original value Exposure rate constant- Gamma ray constant Defined as the exposure in R/hr at a point 1 cm from a 1 mci point source.(r cm²/hr/mci) Beta Energy& filtration
33 What is an Ideal Radionuclide? Easily available & Cost effective Gamma ray energy high enough to avoid increased energy deposition in bone by PEE & low enough to minimise radiation protection requirements Preferably monoenergetic: Optimum 300 KeV to 400 KeV(max=600 kev) Absence of charged particle emission or it should be easily screened (Beta energy as low as possible: filtration) Half life such that correction for decay during treatment is minimal Moderate (few years) T1/2 for removable implants Shorter T1/2 for permanent implants Moderate gamma ray constant (determines activity & output) & also determine shielding required.
 to allow fabrication of smaller sources &")
34 What is an Ideal Radionuclide? No daughter product; No gaseous disintegration product to prevent physical damage to source and to avoid source contamination High Specific Activity (Ci/gm) to allow fabrication of smaller sources & to achieve higher output (adequate photon yield) Material available is insoluble & non-toxic form Sources can be made in different shapes & sizes: Tubes, needle, wire, rod, beads etc. Should withstand sterilization process Disposable without radiation hazard to environment Isotropic: same magnitude in all directions around the source No self attenuation
35 Why Ra not used now? Spectrum has >8 photon energies ranging from MeV : gives heterogenous beam & non uniform dose distribution Low specific activity : 1 Ci/gm : large dia of needles will be needed High gamma ray constant: requires more protection High energy: large HVL reqd :high radiation shielding will be reqd Rn 222 being the gaseous daughter product-threat of leaks especialy from long bent needles(long t1/2) Storage & disposal of leaked sources a big problem Ra source costly
 Exposure rate constant Source Form 6.5 3.28 Tubes & Needles 11 13.")
36 RADIUM SUBSTITUTES Currently used sealed sources Element Energy (MeV) Cesium Cs 137 yrs Cobalt 1.25 Co 60 average 5.26 yrs Halflife HVL- Lead (mm) Exposure rate constant Source Form Tubes & Needles Encapsulated spheres Clinical application LDR I/C &temporary Implants HDR I/C Cesium or Cobalt needles,tubes & Pallets
37 Currently used sealed sources Element Energy (MeV) Halflife HVL- Lead (mm) Exposure rate constant Source Form Clinical application Iridium Ir 192 average 73.8 days Seeds in nylon ribbons; Metal wires; Encapsulated source on cable LDR & HDR temporary implants HDR I/C Intravascular


38
39 Currently used Seed sources Element Energy (MeV) Halflife HVL- Lead (mm) Exposure rate constant Source Form Clinical application Gold Au 198 days Seeds Permanent Implants Iodine I 125 days Seeds Permanent Implants Palladiu m Pd 103 days Seeds Permanent Implants
40 Newer Isotopes Name T 1/2 Photon energy (KeV) 10 th VL Comment Samarium 125 Americium 241 Ytterbium days 432 yrs 32 days Sensitization of cells to radiation damage by iodinated deoxyuridine due to photon energy Low specific activity and α emitter Highest specific activity and lower tissue attenuation Californium yrs NA NA Neutron emitter used in brachytherapy and as EBRT source. 2.3 x 10 9 / sec (neutrons)



41 Needle Tube Wire Hair pin Cylinder spherical Beads Pellets Micro pellets SOURCE FORMS
42 Sr. No. Radio-isotopes Used in Radiotherapy and their Physical Charactrestics Radio- Isotope γ-energy (MeV) β-energy (MeV) Gamma Constant Half Lfie 1. Ra R 1620 yrs. 1.4 Needles, tubes I/C,Mou ld,ints. 2. Rn R 3.8 yrs. 1.2 Seeds Ints. HVL (Pb) Form 3. Tn R 115 days 1.2 Wires, pins, ribbon 4. Co R 5.2 yrs. 1.2 Needles, tubes, I/C, teletherapy Mould, sources Ints.,I/L 5. Cs R 30 yrs 0.65 Needles, tubes, pallets 6. Ir R 74.2 days 0.30 Wires,seeds, ribbons 7. I None 1.20 R 60.2 days 0.0 Seeds Ints. 8. An R 2.7 days 0.33 Seeds Ints. 9. P-32 None days 0.01 Plaques I/V Stent Use Ints. -do- -do- I/C Intracavitary, Ints. Interstitial, I/L Intraluminal, I/V Intra-vascular
43 Sr. No. Radio- Isotope Radio-isotopes Used in Radiotherapy and their Physical Chractrestics γ-energy (MeV) β-energy (MeV) Gamma Constant Half Lfie 10. Sr-90 None yrs 0.01 Plaques Plaque HVL (Pb) Form Use 11. Cr & 1.0 Neutron 2.1 & yrs -- Tubes I/C 12. Pd (mean) Sm (mean) Am (mean) Yt (mean) days 0.03 mm days 0.2 mm days 0.42 mm days 3.3 mm Seeds Ints. -- -do- -- -do- -- -do- I/C Intracavitary, Ints. Interstitial, I/L Intraluminal, I/V Intra-vascular
44 Source Strength Specification: Quantities and Units Quantity and Units :- 1. mg Radium or mg radium equivalent. 2. mg hours 3. Roentzen 4. Rads or Centigray Activity :- 1. Curie or mci 2. Air kermastrength Dose Calculations :- 1. Lane s approximation 2. Sievertintegral 3. Computer dose calculations.



45 Radiation Safety Radiation Shield Radio-isotop



46 Calibration of Sources Well Type Chamber



47 Calibration of Sources Zigs
48 Clinical criteria for brachytherapy 1. Small size tumors (3 5 cm) 2. Depth of penetration/thickness < cm 3. Histology: moderately radiosensitive tumors (ca squamous cell);some adenocarcinomas 4. Early stage (localized to organ) 5. No nodal/distant metastasis 6. Location : accessible site with relatively maintained anatomy 7. Absence of local infection & inflammation
49 Indications For radical radiation alone: Skin tumors Head and Neck cancer Oral Cavity Cervical cancer Prostate cancer Penile cancers Ocular tumors Breast cancer As a boost after EBRT ± Chemotherapy: Head and neck cancers Oral Cancer Cervical cancers Breast cancer Esophagus Anal canal
50 Indications In the post-operative setting: Perioperative: Soft tissue sarcomas Breast Postoperative: Endometrium Cervix Breast Palliative setting: Bronchus Bile ducts Selected esophagus Selected recurrent tumors (chest wall, head and neck) Benign tumors: Keloids Pterygium Other indication: Endovascular brachytherapy Radioactive stents
51 Brachytherapy meeting patient s needs Efficacious 2 High cancer cure rates Low toxicity 3 Minimized risk of side effects Short treatment times 4,5 More convenient Precise 1 Highly targeted, individualized dose delivery Patient centered care Many applications 6 Different body sites Brachytherapy offers a precise, highly effective and well tolerated treatment option tailored to the needs of individual patients 1. Stewart AJ & Jones B. In Devlin. Brachytherapy: Applications and Techniques Kupelian PA, Potters L, Khuntia D, et al. Int J Radiat Oncol Biol Phys 2004;58(1): Pisansky TM, Gold DG, Furutani KM, et al. Mayo Clin Proc 2008;83(12): Dickler A, Patel RR, Wazer D. Expert Rev Med Devices 2009;6(3): Viani GA, Manta GB, Stefano EJ, et al. J Exp Clin Cancer Res 2009;28: Sylvester JE, Grimm PD, Blasko JC, et al. Int J Radiat Oncol Biol Phys 2007;67(1):57-64.
52 Brachytherapy: Incorporating advanced imaging and computing technology into planning and treatment 2D Film Based 1 Standardization through protocols Paris system (e.g. breast) and Manchester method (gyn) 3D Volume Based 2 Dose/volume optimization with availability of 3D imaging capabilities (CT/MRI) Dynamic (real-time) dose based placement guidance Image-guided adaptive brachytherapy 1. Meertens H, Briot E. In The GEC ESTRO handbook of brachytherapy Hoskin PJ & Bownes P. Semin Radiat Oncol 2006;16(4):
53 Image-guided planning and delivery Advanced imaging used for virtually every step of the procedure Provisional treatment planning Simulation of treatment and provisional dose calculation Quality control of dose delivery During or after procedure Precision Therapy Image-guided application Accurate placement of applicators Definitive treatment planning 3D virtual patient and optimization of treatment plan Gerbaulet A, Ash D, Meertems H et al. In The GEC ESTRO handbook of brachytherapy
54 Delivering precision treatment Brachytherapy delivers targeted radiation through the combination of computer-based planning, imagery and treatment delivery techniques via specialized applicators Imaging Application insertion Optimizing treatment plan Clinical examination and tumor imaging Source applicators placed in body for accurate positioning Create virtual patient via visualization and refine Delivery Sources delivered to treatment site via applicators
55 Brachytherapy-A multidisciplinary approach Referring clinician Anaesthetist Medical oncologist Specialist nurse Collaborative multi-disciplinary team, providing patient-centred care Radiation oncologist Radiation therapist/ technician Medical physicist
56
Brachytherapy an Overview
 Brachytherapy an Overview Yakov Pipman, D Sc North Shore LIJ Health System Monterrey, Nov30-Dec1, 2007 Brachytherapy A procedure in therapeutic radiology that involves the irradiation of a target with
Brachytherapy an Overview Yakov Pipman, D Sc North Shore LIJ Health System Monterrey, Nov30-Dec1, 2007 Brachytherapy A procedure in therapeutic radiology that involves the irradiation of a target with
Brachytherapy The use of radioactive sources in close proximity to the target area for radiotherapy
 Brachytherapy The use of radioactive sources in close proximity to the target area for radiotherapy Interstitial Seven 192-Ir wires Interstitial implant for breast radiotherapy Intracavitary Three 137-Cs
Brachytherapy The use of radioactive sources in close proximity to the target area for radiotherapy Interstitial Seven 192-Ir wires Interstitial implant for breast radiotherapy Intracavitary Three 137-Cs
Brachytherapy Planning and Quality Assurance
 Brachytherapy Planning and Quality Assurance Classical implant systems Most common clinical applications and modern dosimetry methods Quality assurance Classical implant systems Manchester (Paterson-Parker)
Brachytherapy Planning and Quality Assurance Classical implant systems Most common clinical applications and modern dosimetry methods Quality assurance Classical implant systems Manchester (Paterson-Parker)
Brachytherapy Planning and Quality Assurance w Classical implant systems and modern computerized dosimetry w Most common clinical applications w
 Brachytherapy Planning and Quality Assurance w Classical implant systems and modern computerized dosimetry w Most common clinical applications w Quality assurance Classical implant systems w Manchester
Brachytherapy Planning and Quality Assurance w Classical implant systems and modern computerized dosimetry w Most common clinical applications w Quality assurance Classical implant systems w Manchester
Regulatory Guidelines and Computational Methods for Safe Release of Radioactive Patients II. Brachytherapy
 Regulatory Guidelines and Computational Methods for Safe Release of Radioactive Patients II. Brachytherapy Firas Mourtada, Ph.D., DABR Chief of Clinical Physics Helen F. Graham Cancer Center Christiana
Regulatory Guidelines and Computational Methods for Safe Release of Radioactive Patients II. Brachytherapy Firas Mourtada, Ph.D., DABR Chief of Clinical Physics Helen F. Graham Cancer Center Christiana
Brachytherapy. What is brachytherapy and how is it used?
 Scan for mobile link. Brachytherapy Brachytherapy places radioactive sources inside the patient on a temporary or permanent basis to damage cancer cells DNA and destroy their ability to divide and grow.
Scan for mobile link. Brachytherapy Brachytherapy places radioactive sources inside the patient on a temporary or permanent basis to damage cancer cells DNA and destroy their ability to divide and grow.
INTRODUCTION TO BRACHYTHERAPY, HISTORY AND INDICATIONS. Christine Haie-Meder Brachytherapy Unit
 INTRODUCTION TO BRACHYTHERAPY, HISTORY AND INDICATIONS Christine Haie-Meder Brachytherapy Unit HISTORY OF BRACHYTHERAPY 8/11/1895 Röentgen : X-ray discovery 22/11/1895 Mrs Röentgen s hand X-ray 1896 Becquerel
INTRODUCTION TO BRACHYTHERAPY, HISTORY AND INDICATIONS Christine Haie-Meder Brachytherapy Unit HISTORY OF BRACHYTHERAPY 8/11/1895 Röentgen : X-ray discovery 22/11/1895 Mrs Röentgen s hand X-ray 1896 Becquerel
Definitions. Brachytherapy in treatment of cancer. Implantation Techniques and Methods of Dose Specifications. Importance of Brachytherapy in GYN
 Implantation Techniques and Methods of Dose Specifications Brachytherapy Course Lecture V Krishna Reddy, MD, PhD Assistant Professor, Radiation Oncology Brachytherapy in treatment of cancer GYN Cervical
Implantation Techniques and Methods of Dose Specifications Brachytherapy Course Lecture V Krishna Reddy, MD, PhD Assistant Professor, Radiation Oncology Brachytherapy in treatment of cancer GYN Cervical
ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป
 ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป Brachytherapy การร กษาด วยร งส ระยะใกล Insertion การสอดใส แร Implantation การฝ งแร Surface application การวางแร physical benefit of brachytherapy - very high dose of radiation
ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป Brachytherapy การร กษาด วยร งส ระยะใกล Insertion การสอดใส แร Implantation การฝ งแร Surface application การวางแร physical benefit of brachytherapy - very high dose of radiation
BRACHYTHERAPY IN HEAD & NECK CANCERS DR. GIRI G.V.
 BRACHYTHERAPY IN HEAD & NECK CANCERS DR. GIRI G.V. BASICS High dose to tumor = local control Spare normal structures i.e. salivary gland, mandible and muscles of mastication. Seed 100 Relative dose 10
BRACHYTHERAPY IN HEAD & NECK CANCERS DR. GIRI G.V. BASICS High dose to tumor = local control Spare normal structures i.e. salivary gland, mandible and muscles of mastication. Seed 100 Relative dose 10
Radiotherapy physics & Equipments
 Radiotherapy physics & Equipments RAD 481 Lecture s Title: An Overview of Radiation Therapy for Health Care Professionals Dr. Mohammed Emam Vision :IMC aspires to be a leader in applied medical sciences,
Radiotherapy physics & Equipments RAD 481 Lecture s Title: An Overview of Radiation Therapy for Health Care Professionals Dr. Mohammed Emam Vision :IMC aspires to be a leader in applied medical sciences,
Radioactive sources in brachytherapy
 Radioactive sources in brachytherapy Janez Burger Institute of Oncology, Department of Radiophysics, Brachytherapy Unit, Ljubljana, Slovenia Background. In modern brachytherapy, a great step forward was
Radioactive sources in brachytherapy Janez Burger Institute of Oncology, Department of Radiophysics, Brachytherapy Unit, Ljubljana, Slovenia Background. In modern brachytherapy, a great step forward was
How ICD-10 Affects Radiation Oncology. Presented by, Lashelle Bolton CPC, COC, CPC-I, CPMA
 How ICD-10 Affects Radiation Oncology Presented by, Lashelle Bolton CPC, COC, CPC-I, CPMA ICD-10 ICD-10-CM has added new challenges to the radiation oncology specialty. Approximately 220 ICD-9-CM codes
How ICD-10 Affects Radiation Oncology Presented by, Lashelle Bolton CPC, COC, CPC-I, CPMA ICD-10 ICD-10-CM has added new challenges to the radiation oncology specialty. Approximately 220 ICD-9-CM codes
Chapter 13: Brachytherapy: Physical and Clinical Aspects
 Chapter 13: Brachytherapy: Physical and Clinical Aspects Set of 163 slides based on the chapter authored by N. Suntharalingam, E.B. Podgorsak, H. Tolli of the IAEA publication (ISBN 92-0-107304-6): Radiation
Chapter 13: Brachytherapy: Physical and Clinical Aspects Set of 163 slides based on the chapter authored by N. Suntharalingam, E.B. Podgorsak, H. Tolli of the IAEA publication (ISBN 92-0-107304-6): Radiation
Basics of Cervix Brachytherapy. William Small, Jr., MD Professor and Chairman Loyola University Chicago
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Basics of Cervix Brachytherapy William Small, Jr., MD Professor and Chairman Loyola University Chicago Cervix Cancer Education Symposium, January
Gynecologic Cancer InterGroup Cervix Cancer Research Network Basics of Cervix Brachytherapy William Small, Jr., MD Professor and Chairman Loyola University Chicago Cervix Cancer Education Symposium, January
Comprehensive and Practical Brachytherapy March 04-8 March 2018, Ljubljana, Slovenia Day 1 Sunday 4 March 2018
 Day 1 Sunday 4 March 2018 Welcome and Summary of the course 13:00-13:20 15 introduction 13:20-13:50 30 Radioactivity Radioactivity: What we need to know Characteristics of LDR-PDR-HDR, radiobiological
Day 1 Sunday 4 March 2018 Welcome and Summary of the course 13:00-13:20 15 introduction 13:20-13:50 30 Radioactivity Radioactivity: What we need to know Characteristics of LDR-PDR-HDR, radiobiological
Radiotherapy. Marta Anguiano Millán. Departamento de Física Atómica, Molecular y Nuclear Facultad de Ciencias. Universidad de Granada
 Departamento de Física Atómica, Molecular y Nuclear Facultad de Ciencias. Universidad de Granada Overview Introduction Overview Introduction Brachytherapy Radioisotopes in contact with the tumor Overview
Departamento de Física Atómica, Molecular y Nuclear Facultad de Ciencias. Universidad de Granada Overview Introduction Overview Introduction Brachytherapy Radioisotopes in contact with the tumor Overview
Intravascular Brachytherapy Dosimetry Techniques for Gamma systems
 Intravascular Brachytherapy Dosimetry Techniques for Gamma systems Shirish K. Jani, Ph.D., FACR Scripps Clinic La Jolla, California Physics Parameters-1: IVBT Gamma or X ray Isotopes Energy [ kev ] Half
Intravascular Brachytherapy Dosimetry Techniques for Gamma systems Shirish K. Jani, Ph.D., FACR Scripps Clinic La Jolla, California Physics Parameters-1: IVBT Gamma or X ray Isotopes Energy [ kev ] Half
Radio-isotopes in Clinical Medicine
 Radio-isotopes in Clinical Medicine Radiactive isotopes, whether naturally occurring or artificially produced, have a number of different uses in clinical medicine. These include: (1) Diagnostic and research
Radio-isotopes in Clinical Medicine Radiactive isotopes, whether naturally occurring or artificially produced, have a number of different uses in clinical medicine. These include: (1) Diagnostic and research
FEE RULES RADIATION ONCOLOGY FEE SCHEDULE CONTENTS
 Tel: +27-21-9494060 Fax: +27-21-9494112 E-mail: leon.gouws@cancercare.co.za FEE RULES RADIATION ONCOLOGY FEE SCHEDULE CONTENTS 1. EXTERNAL BEAM RADIATION... 2 2. PLANNING OF TREATMENT... 2 3. DELIVERY
Tel: +27-21-9494060 Fax: +27-21-9494112 E-mail: leon.gouws@cancercare.co.za FEE RULES RADIATION ONCOLOGY FEE SCHEDULE CONTENTS 1. EXTERNAL BEAM RADIATION... 2 2. PLANNING OF TREATMENT... 2 3. DELIVERY
Understanding Radiation Therapy. For Patients and the Public
 Understanding Radiation Therapy For Patients and the Public Introduction to Radiation Oncology Radiation has been an effective tool for treating cancer for more than 100 years. Radiation oncologists are
Understanding Radiation Therapy For Patients and the Public Introduction to Radiation Oncology Radiation has been an effective tool for treating cancer for more than 100 years. Radiation oncologists are
12 Physics and Clinical Aspects of Brachytherapy
 Physics and Clinical Aspects of Brachytherapy 255 12 Physics and Clinical Aspects of Brachytherapy Zuofeng Li CONTENTS 12.1 Introduction 255 12.2 Classifications of Brachytherapy 256 12.2.1 Permanent Versus
Physics and Clinical Aspects of Brachytherapy 255 12 Physics and Clinical Aspects of Brachytherapy Zuofeng Li CONTENTS 12.1 Introduction 255 12.2 Classifications of Brachytherapy 256 12.2.1 Permanent Versus
PRINCIPLES and PRACTICE of RADIATION ONCOLOGY. Matthew B. Podgorsak, PhD, FAAPM Department of Radiation Oncology
 PRINCIPLES and PRACTICE of RADIATION ONCOLOGY Matthew B. Podgorsak, PhD, FAAPM Department of Radiation Oncology OUTLINE Physical basis Biological basis History of radiation therapy Treatment planning Technology
PRINCIPLES and PRACTICE of RADIATION ONCOLOGY Matthew B. Podgorsak, PhD, FAAPM Department of Radiation Oncology OUTLINE Physical basis Biological basis History of radiation therapy Treatment planning Technology
Healthcare Professional Guide
 Healthcare Professional Guide Brachytherapy: The precise answer for tackling gynecological cancers Because life is for living Radiotherapy: a cornerstone of gynecological cancer care Gynecological cancers
Healthcare Professional Guide Brachytherapy: The precise answer for tackling gynecological cancers Because life is for living Radiotherapy: a cornerstone of gynecological cancer care Gynecological cancers
PROSTATE CANCER BRACHYTHERAPY. Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College
 PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
The Future of Brachytherapy. Alex Rijnders Europe Hospitals Brussels, Belgium
 The Future of Brachytherapy Alex Rijnders Europe Hospitals Brussels, Belgium a.rijnders@europehospitals.be Sarajevo, May 21, 2014 Brachytherapy = application of sealed sources inside or in close proximity
The Future of Brachytherapy Alex Rijnders Europe Hospitals Brussels, Belgium a.rijnders@europehospitals.be Sarajevo, May 21, 2014 Brachytherapy = application of sealed sources inside or in close proximity
A Study on Dosimetry of Gynaecological Cancer and Quality Assurance of HDR Brachytherapy in BPKMCH, Nepal
 A Study on Dosimetry of Gynaecological Cancer and Quality Assurance of HDR Brachytherapy in BPKMCH, Nepal SB Chand, PP Chaursia, MP Adhikary, AK Jha, and S Shrestha Dept. of Radiation Oncology, BPKM Cancer
A Study on Dosimetry of Gynaecological Cancer and Quality Assurance of HDR Brachytherapy in BPKMCH, Nepal SB Chand, PP Chaursia, MP Adhikary, AK Jha, and S Shrestha Dept. of Radiation Oncology, BPKM Cancer
Therapeutic Medical Physics. Stephen J. Amadon Jr., Ph.D., DABR
 Therapeutic Medical Physics Stephen J. Amadon Jr., Ph.D., DABR Outline 1. Why physicists are needed in medicine 2. Branches of medical physics 3. Physics in Radiation Oncology 4. Treatment types and Treatment
Therapeutic Medical Physics Stephen J. Amadon Jr., Ph.D., DABR Outline 1. Why physicists are needed in medicine 2. Branches of medical physics 3. Physics in Radiation Oncology 4. Treatment types and Treatment
Clinical Applications of Brachytherapy Radiobiology. Radiobiology is Essential
 Clinical Applications of Brachytherapy Radiobiology Dr Alexandra Stewart University of Surrey St Luke s Cancer Centre Guildford, England Radiobiology is Essential Knowledge of radiobiological principles
Clinical Applications of Brachytherapy Radiobiology Dr Alexandra Stewart University of Surrey St Luke s Cancer Centre Guildford, England Radiobiology is Essential Knowledge of radiobiological principles
BRACHYTHERAPY IN HORSES
 Vet Times The website for the veterinary profession https://www.vettimes.co.uk BRACHYTHERAPY IN HORSES Author : DAVID DONALDSON Categories : Vets Date : June 16, 2014 DAVID DONALDSON BVSc(Hons), DipECVO,
Vet Times The website for the veterinary profession https://www.vettimes.co.uk BRACHYTHERAPY IN HORSES Author : DAVID DONALDSON Categories : Vets Date : June 16, 2014 DAVID DONALDSON BVSc(Hons), DipECVO,
Healthcare Professional Guide. Brachytherapy: The precise answer for tackling cancer. Because life is for living
 Healthcare Professional Guide Brachytherapy: The precise answer for tackling cancer Because life is for living Radiotherapy; a cornerstone of cancer care According to the World Health Organization (WHO),
Healthcare Professional Guide Brachytherapy: The precise answer for tackling cancer Because life is for living Radiotherapy; a cornerstone of cancer care According to the World Health Organization (WHO),
Radiation Biology in Brachytherapy
 Journal of Surgical Oncology 1997;65:66 70 REVIEW ARTICLE Radiation Biology in Brachytherapy DAVID J. BRENNER, DSc Center for Radiological Research, College of Physicians and Surgeons, Columbia University,
Journal of Surgical Oncology 1997;65:66 70 REVIEW ARTICLE Radiation Biology in Brachytherapy DAVID J. BRENNER, DSc Center for Radiological Research, College of Physicians and Surgeons, Columbia University,
RADIOTHERAPY: TECHNOLOGIES AND GLOBAL MARKETS
 RADIOTHERAPY: TECHNOLOGIES AND GLOBAL MARKETS HLC176A February 2015 Neha Maliwal Project Analyst ISBN: 1-62296-043-2 BCC Research 49 Walnut Park, Building 2 Wellesley, MA 02481 USA 866-285-7215 (toll-free
RADIOTHERAPY: TECHNOLOGIES AND GLOBAL MARKETS HLC176A February 2015 Neha Maliwal Project Analyst ISBN: 1-62296-043-2 BCC Research 49 Walnut Park, Building 2 Wellesley, MA 02481 USA 866-285-7215 (toll-free
OPPORTUNITIES IN BRACHYTHERAPY
 OPPORTUNITIES IN BRACHYTHERAPY EDITION 2014 A report written by Paul-Emmanuel Goethals & Richard Zimmermann www.medraysintell.com Brachytherapy THE FIRST COMPREHENSIVE EVALUATION OF THE BRACHYTHERAPY INDUSTRY
OPPORTUNITIES IN BRACHYTHERAPY EDITION 2014 A report written by Paul-Emmanuel Goethals & Richard Zimmermann www.medraysintell.com Brachytherapy THE FIRST COMPREHENSIVE EVALUATION OF THE BRACHYTHERAPY INDUSTRY
NIA MAGELLAN HEALTH RADIATION ONCOLOGY CODING STANDARD. Dosimetry Planning
 NIA MAGELLAN HEALTH RADIATION ONCOLOGY CODING STANDARD Dosimetry Planning CPT Codes: 77295, 77300, 77301, 77306, 77307, 77321, 77316, 77317, 77318, 77331, 77399 Original Date: April, 2011 Last Reviewed
NIA MAGELLAN HEALTH RADIATION ONCOLOGY CODING STANDARD Dosimetry Planning CPT Codes: 77295, 77300, 77301, 77306, 77307, 77321, 77316, 77317, 77318, 77331, 77399 Original Date: April, 2011 Last Reviewed
3D CONFORMATIONAL INTERSTITIAL BRACHYTHERAPY PLANNING FOR SOFT TISSUE SARCOMA
 3D CONFORMATIONAL INTERSTITIAL BRACHYTHERAPY PLANNING FOR SOFT TISSUE SARCOMA Alina TĂNASE 1,3, M. DUMITRACHE 2,3, O. FLOREA 1 1 Emergency Central Military Hospital Dr. Carol Davila Bucharest, Romania,
3D CONFORMATIONAL INTERSTITIAL BRACHYTHERAPY PLANNING FOR SOFT TISSUE SARCOMA Alina TĂNASE 1,3, M. DUMITRACHE 2,3, O. FLOREA 1 1 Emergency Central Military Hospital Dr. Carol Davila Bucharest, Romania,
Pulsed Dose Rate for GYN Brachytherapy
 Pulsed Dose Rate for GYN Brachytherapy Firas Mourtada,, Ph.D. Department of Radiation Physics Dose equivalency to LDR Brief Introduction Radiobiology Dose Distribution: Radial dose function Source anisotropy
Pulsed Dose Rate for GYN Brachytherapy Firas Mourtada,, Ph.D. Department of Radiation Physics Dose equivalency to LDR Brief Introduction Radiobiology Dose Distribution: Radial dose function Source anisotropy
HDR vs. LDR Is One Better Than The Other?
 HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
Varian Acuity BrachyTherapy Suite One Room Integrated Image-Guided Brachytherapy
 Varian Acuity BrachyTherapy Suite One Room Integrated Image-Guided Brachytherapy The Acuity BrachyTherapy Suite Integrating Imaging, Planning, and Treatment in a Single Room Each component draws on the
Varian Acuity BrachyTherapy Suite One Room Integrated Image-Guided Brachytherapy The Acuity BrachyTherapy Suite Integrating Imaging, Planning, and Treatment in a Single Room Each component draws on the
Medical Use of Radioisotopes
 Medical Use of Radioisotopes Therapy Radioisotopes prove to be useful in the application of brachytherapy, the procedure for using temporary irradiation close to the area of disease (i.e. cancer) 10% Medical
Medical Use of Radioisotopes Therapy Radioisotopes prove to be useful in the application of brachytherapy, the procedure for using temporary irradiation close to the area of disease (i.e. cancer) 10% Medical
First, how does radiation work?
 Hello, I am Prajnan Das, Faculty Member in the Department of Radiation Oncology at The University of Texas MD Anderson Cancer Center. We are going to talk today about some of the basic principles regarding
Hello, I am Prajnan Das, Faculty Member in the Department of Radiation Oncology at The University of Texas MD Anderson Cancer Center. We are going to talk today about some of the basic principles regarding
Prostate Cancer Treatment
 Scan for mobile link. Prostate Cancer Treatment Prostate cancer overview Prostate cancer is the most common form of cancer in American men, most prevalent in men over age 65 and fairly common in men 50-64
Scan for mobile link. Prostate Cancer Treatment Prostate cancer overview Prostate cancer is the most common form of cancer in American men, most prevalent in men over age 65 and fairly common in men 50-64
APPLICATIONS OF RADIATION IN MEDICINE. Kirstin Murray BSc (Hons) Radiotherapy & Oncology
 Radiotherapy & Oncology") APPLICATIONS OF RADIATION IN MEDICINE Kirstin Murray BSc (Hons) Radiotherapy & Oncology CONTENTS Principles of Radiation Therapy Radiobiology Radiotherapy Treatment Modalities Special Techniques Nuclear
APPLICATIONS OF RADIATION IN MEDICINE Kirstin Murray BSc (Hons) Radiotherapy & Oncology CONTENTS Principles of Radiation Therapy Radiobiology Radiotherapy Treatment Modalities Special Techniques Nuclear
Fractionation: why did we ever fractionate? The Multiple Fractions School won! Survival curves: normal vs cancer cells
 1 Basic Radiobiology for the Radiotherapy Physicist Colin G. Orton, Ph.D. Professor Emeritus, Wayne State University, Detroit, Michigan, USA Fractionation: why did we ever fractionate? Actually, initially
1 Basic Radiobiology for the Radiotherapy Physicist Colin G. Orton, Ph.D. Professor Emeritus, Wayne State University, Detroit, Michigan, USA Fractionation: why did we ever fractionate? Actually, initially
MEDICAL MANAGEMENT POLICY
 PAGE: 1 of 8 This medical policy is not a guarantee of benefits or coverage, nor should it be deemed as medical advice. In the event of any conflict concerning benefit coverage, the employer/member summary
PAGE: 1 of 8 This medical policy is not a guarantee of benefits or coverage, nor should it be deemed as medical advice. In the event of any conflict concerning benefit coverage, the employer/member summary
GYNECOLOGIC CANCER and RADIATION THERAPY. Jon Anders M.D. Radiation Oncology
 GYNECOLOGIC CANCER and RADIATION THERAPY Jon Anders M.D. Radiation Oncology Brachytherapy Comes from the Greek brakhus meaning short Brachytherapy is treatment at short distance Intracavitary vs interstitial
GYNECOLOGIC CANCER and RADIATION THERAPY Jon Anders M.D. Radiation Oncology Brachytherapy Comes from the Greek brakhus meaning short Brachytherapy is treatment at short distance Intracavitary vs interstitial
 https://patient.varian.com/sit es/default/files/videos/origin al/imrt.mp4 brachy- from Greek brakhys "short" Historically LDR has been used. Cs-137 at 0.4-0.8 Gy/h With optimally placed device, dose
https://patient.varian.com/sit es/default/files/videos/origin al/imrt.mp4 brachy- from Greek brakhys "short" Historically LDR has been used. Cs-137 at 0.4-0.8 Gy/h With optimally placed device, dose
2015 Radiology Coding Survival Guide
 2015 Radiology Coding Survival Guide Chapter 31: Clinical Brachytherapy (77750-77799) Clinical brachytherapy involves applying radioelements into or around a treatment field. CPT guidelines clarify that
2015 Radiology Coding Survival Guide Chapter 31: Clinical Brachytherapy (77750-77799) Clinical brachytherapy involves applying radioelements into or around a treatment field. CPT guidelines clarify that
Advances in Image-guided Brachytherapy
 Advances in Image-guided Brachytherapy Hospital Authority Convention 2016 Terry Wong, Physicist Department of Medical Physics Pamela Youde Nethersole Eastern Hospital Introduction What is Brachytherapy?
Advances in Image-guided Brachytherapy Hospital Authority Convention 2016 Terry Wong, Physicist Department of Medical Physics Pamela Youde Nethersole Eastern Hospital Introduction What is Brachytherapy?
Dose distribution and dosimetry parameters calculation of MED3633 palladium-103 source in water phantom using MCNP
 Iran. J. Radiat. Res., 2006; 4 (1): 15-19 Dose distribution and dosimetry parameters calculation of MED3633 palladium- source in water phantom using MCNP A.A. Mowlavi 1*,A. Binesh 2, H. Moslehitabar 3
Iran. J. Radiat. Res., 2006; 4 (1): 15-19 Dose distribution and dosimetry parameters calculation of MED3633 palladium- source in water phantom using MCNP A.A. Mowlavi 1*,A. Binesh 2, H. Moslehitabar 3
Prostate Cancer. What is prostate cancer?
 Scan for mobile link. Prostate Cancer Prostate cancer is a tumor of the prostate gland, which is located in front of the rectum and below the bladder. Your doctor may perform a physical exam, prostate-specific
Scan for mobile link. Prostate Cancer Prostate cancer is a tumor of the prostate gland, which is located in front of the rectum and below the bladder. Your doctor may perform a physical exam, prostate-specific
MEDICAL POLICY. SUBJECT: BRACHYTHERAPY OR RADIOACTIVE SEED IMPLANTATION FOR PROSTATE CANCER POLICY NUMBER: CATEGORY: Technology Assessment
 MEDICAL POLICY SUBJECT: BRACHYTHERAPY OR PAGE: 1 OF: 5 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy
MEDICAL POLICY SUBJECT: BRACHYTHERAPY OR PAGE: 1 OF: 5 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy
ADVANCES IN RADIATION TECHNOLOGIES IN THE TREATMENT OF CANCER
 ADVANCES IN RADIATION TECHNOLOGIES IN THE TREATMENT OF CANCER Bro. Dr. Collie Miller IARC/WHO Based on trends in the incidence of cancer, the International Agency for Research on Cancer (IARC) and WHO
ADVANCES IN RADIATION TECHNOLOGIES IN THE TREATMENT OF CANCER Bro. Dr. Collie Miller IARC/WHO Based on trends in the incidence of cancer, the International Agency for Research on Cancer (IARC) and WHO
Option D: Medicinal Chemistry
 Option D: Medicinal Chemistry Basics - unstable radioactive nuclei emit radiation in the form of smaller particles alpha, beta, positron, proton, neutron, & gamma are all used in nuclear medicine unstable
Option D: Medicinal Chemistry Basics - unstable radioactive nuclei emit radiation in the form of smaller particles alpha, beta, positron, proton, neutron, & gamma are all used in nuclear medicine unstable
Radiobiological principles of brachytherapy
 Radiobiological principles of brachytherapy Low dose rate (LDR) Medium dose rate (MDR) High dose rate (HDR) The effect of dose rate As the dose rate is decreased, there is more time during irradiation
Radiobiological principles of brachytherapy Low dose rate (LDR) Medium dose rate (MDR) High dose rate (HDR) The effect of dose rate As the dose rate is decreased, there is more time during irradiation
BRACHYTHERAPY FOR TREATMENT OF MISCELLANEOUS CANCERS
 BRACHYTHERAPY FOR TREATMENT OF MISCELLANEOUS CANCERS Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan.
BRACHYTHERAPY FOR TREATMENT OF MISCELLANEOUS CANCERS Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan.
MR-Guided Brachytherapy
 MR-Guided Brachytherapy Joann I. Prisciandaro, Ph.D. The Department of Radiation Oncology University of Michigan Outline Traditional 2D technique for brachytherapy treatment planning Transition to MR-guided
MR-Guided Brachytherapy Joann I. Prisciandaro, Ph.D. The Department of Radiation Oncology University of Michigan Outline Traditional 2D technique for brachytherapy treatment planning Transition to MR-guided
ACCELERATED BREAST IRRADIATION EVOLVING PARADIGM FOR TREATMENT OF EARLY STAGE BREAST CANCER
 ACCELERATED BREAST IRRADIATION EVOLVING PARADIGM FOR TREATMENT OF EARLY STAGE BREAST CANCER KHANH NGUYEN, MD, MA DEPARTMENT OF RADIATION ONCOLOGY BAYHEALTH CANCER CENTER BREAST CANCER STATISTICS Most common
ACCELERATED BREAST IRRADIATION EVOLVING PARADIGM FOR TREATMENT OF EARLY STAGE BREAST CANCER KHANH NGUYEN, MD, MA DEPARTMENT OF RADIATION ONCOLOGY BAYHEALTH CANCER CENTER BREAST CANCER STATISTICS Most common
IAEA-TECDOC Implementation of microsource high dose rate (mhdr) brachytherapy in developing countries
 brachytherapy in developing countries") IAEA-TECDOC-1257 Implementation of microsource high dose rate (mhdr) brachytherapy in developing countries November 2001 The originating Section of this publication in the IAEA was: Applied Radiation Biology
IAEA-TECDOC-1257 Implementation of microsource high dose rate (mhdr) brachytherapy in developing countries November 2001 The originating Section of this publication in the IAEA was: Applied Radiation Biology
Brachytherapy, Radionuclide Therapy Medical Physics in the Clinic. Raymond K. Wu, PhD Chairman AAPM Exchange Scientist Program
 Brachytherapy, Radionuclide Therapy Medical Physics in the Clinic Raymond K. Wu, PhD Chairman AAPM Exchange Scientist Program TG 43 of 1995 New dose calculation formalism for brachytherapy Consensus data
Brachytherapy, Radionuclide Therapy Medical Physics in the Clinic Raymond K. Wu, PhD Chairman AAPM Exchange Scientist Program TG 43 of 1995 New dose calculation formalism for brachytherapy Consensus data
Advances in Treatment of Cancer by Brachytherapy in Kenya, in Particular, Prostate Cancer
 Research Article imedpub Journals www.imedpub.com Journal Of Medical Physics And Applied Sciences ISSN 2574-285X DOI: 1.21767/2574-285X.12 Advances in Treatment of Cancer by Brachytherapy in Kenya, in
Research Article imedpub Journals www.imedpub.com Journal Of Medical Physics And Applied Sciences ISSN 2574-285X DOI: 1.21767/2574-285X.12 Advances in Treatment of Cancer by Brachytherapy in Kenya, in
MEDICAL POLICY SUBJECT: BRACHYTHERAPY OR RADIOACTIVE SEED IMPLANTATION FOR PROSTATE CANCER
 MEDICAL POLICY SUBJECT: BRACHYTHERAPY OR PAGE: 1 OF: 6 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy
MEDICAL POLICY SUBJECT: BRACHYTHERAPY OR PAGE: 1 OF: 6 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy
Brachytherapy, Noncoronary
 Brachytherapy, Noncoronary Policy Number: Original Effective Date: MM.05.004 05/10/2005 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 03/01/2016 Section: Radiology Place(s) of
Brachytherapy, Noncoronary Policy Number: Original Effective Date: MM.05.004 05/10/2005 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 03/01/2016 Section: Radiology Place(s) of
Prostate Cancer. What is prostate cancer?
 Scan for mobile link. Prostate Cancer Prostate cancer is a tumor of the prostate gland, which is located in front of the rectum, below the bladder and above the base of the penis. Your doctor may perform
Scan for mobile link. Prostate Cancer Prostate cancer is a tumor of the prostate gland, which is located in front of the rectum, below the bladder and above the base of the penis. Your doctor may perform
I. Equipments for external beam radiotherapy
 I. Equipments for external beam radiotherapy 5 linear accelerators (LINACs): Varian TrueBeam 6, 10 & 18 MV photons, 6-18 MeV electrons, image-guided (IGRT) and intensity modulated radiotherapy (IMRT),
I. Equipments for external beam radiotherapy 5 linear accelerators (LINACs): Varian TrueBeam 6, 10 & 18 MV photons, 6-18 MeV electrons, image-guided (IGRT) and intensity modulated radiotherapy (IMRT),
Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring)
") Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring) Dr Umesh Mahantshetty, Professor, Radiation Oncology GYN & Urology Disease Management Group (DMG) Member Tata Memorial
Basic Concepts in Image Based Brachytherapy (GEC-ESTRO Target Concept & Contouring) Dr Umesh Mahantshetty, Professor, Radiation Oncology GYN & Urology Disease Management Group (DMG) Member Tata Memorial
Expectations of Physics Knowledge for Certification
 Expectations of Physics Knowledge for Certification Bhudatt Paliwal, Ph.D. University of Wisconsin Medical School Department of Human Oncology Madison, Wisconsin 53792 USA Guiding Principles Test that
Expectations of Physics Knowledge for Certification Bhudatt Paliwal, Ph.D. University of Wisconsin Medical School Department of Human Oncology Madison, Wisconsin 53792 USA Guiding Principles Test that
Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer
 for Gynaecological Cancer") Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer Tan Chek Wee 15 06 2016 National University Cancer Institute, Singapore Clinical Care Education Research
Dosimetric Analysis of 3DCRT or IMRT with Vaginal-cuff Brachytherapy (VCB) for Gynaecological Cancer Tan Chek Wee 15 06 2016 National University Cancer Institute, Singapore Clinical Care Education Research
Healthcare Professional Guide
 Healthcare Professional Guide Brachytherapy: The precise answer for tackling prostate cancer Because life is for living Radiotherapy: a cornerstone of prostate cancer care Prostate cancer is the most commonly
Healthcare Professional Guide Brachytherapy: The precise answer for tackling prostate cancer Because life is for living Radiotherapy: a cornerstone of prostate cancer care Prostate cancer is the most commonly
MultiSource. for a higher standard in HDR brachytherapy.
 MultiSource for a higher standard in HDR brachytherapy www.ibt-bebig.eu MultiSource HDR afterloader Multiple use: The MultiSource radiation sources have two things in common a small size and a favourable
MultiSource for a higher standard in HDR brachytherapy www.ibt-bebig.eu MultiSource HDR afterloader Multiple use: The MultiSource radiation sources have two things in common a small size and a favourable
SCOPE OF ACCREDITATION TO ISO/IEC 17025:2005 & ANSI/NCSL Z
 SCOPE OF ACCREDITATION TO ISO/IEC 17025:2005 & ANSI/NCSL Z540-1-1994 UNIVERSITY OF WISCONSIN RADIATION CALIBRATION LABORATORY Room B1002, WIMR 1111 Highland Avenue Madison, WI 53705-2275 Larry A. DeWerd,
SCOPE OF ACCREDITATION TO ISO/IEC 17025:2005 & ANSI/NCSL Z540-1-1994 UNIVERSITY OF WISCONSIN RADIATION CALIBRATION LABORATORY Room B1002, WIMR 1111 Highland Avenue Madison, WI 53705-2275 Larry A. DeWerd,
A Handbook for Families. Radiation. Therapy ONCOLOGY SERIES
 A Handbook for Families Radiation Therapy ONCOLOGY SERIES A Handbook for Families Radiation Therapy ONCOLOGY SERIES RADIATION THERAPY A HANDBOOK FOR FAMILIES Author Hilda Haynes-Lewis, MS ANP BC AOCNP
A Handbook for Families Radiation Therapy ONCOLOGY SERIES A Handbook for Families Radiation Therapy ONCOLOGY SERIES RADIATION THERAPY A HANDBOOK FOR FAMILIES Author Hilda Haynes-Lewis, MS ANP BC AOCNP
3D ANATOMY-BASED PLANNING OPTIMIZATION FOR HDR BRACHYTHERAPY OF CERVIX CANCER
 SAUDI JOURNAL OF OBSTETRICS AND GYNECOLOGY VOLUME 11 NO. 2 1430 H - 2009 G 3D ANATOMY-BASED PLANNING OPTIMIZATION FOR HDR BRACHYTHERAPY OF CERVIX CANCER DR YASIR BAHADUR 1, DR CAMELIA CONSTANTINESCU 2,
SAUDI JOURNAL OF OBSTETRICS AND GYNECOLOGY VOLUME 11 NO. 2 1430 H - 2009 G 3D ANATOMY-BASED PLANNING OPTIMIZATION FOR HDR BRACHYTHERAPY OF CERVIX CANCER DR YASIR BAHADUR 1, DR CAMELIA CONSTANTINESCU 2,
CHAPTER : 1 INTRODUCTION 1.1 Carcinoma of the Cervix (Cervical Cancer)
") CHAPTER : 1 INTRODUCTION The curative management of carcinoma of the cervix is significantly enhanced when intracavitary Brachytherapy (BT) is used as an integral component in the treatment of cervical
CHAPTER : 1 INTRODUCTION The curative management of carcinoma of the cervix is significantly enhanced when intracavitary Brachytherapy (BT) is used as an integral component in the treatment of cervical
The role and development of afterloading brachytherapy services in the United Kingdom
 Oncology The role and development of afterloading brachytherapy services in the United Kingdom Board of the Faculty of Clinical Oncology The Royal College of Radiologists Contents Foreword 3 1. Introduction
Oncology The role and development of afterloading brachytherapy services in the United Kingdom Board of the Faculty of Clinical Oncology The Royal College of Radiologists Contents Foreword 3 1. Introduction
EORTC Member Facility Questionnaire
 Page 1 of 9 EORTC Member Facility Questionnaire I. Administrative Data Name of person submitting this questionnaire Email address Function Phone Institution Address City Post code Country EORTC No Enter
Page 1 of 9 EORTC Member Facility Questionnaire I. Administrative Data Name of person submitting this questionnaire Email address Function Phone Institution Address City Post code Country EORTC No Enter
Electronics X-ray Sources for Brachytherapy
 Electronics X-ray Sources for Brachytherapy Mieczysław Słapa, Marek Traczyk, Marcin Talejko, Krzysztof Wincel, Barbara Zaręba The Andrzej Sołtan Institute for Nuclear Studies Department of Physics Applications
Electronics X-ray Sources for Brachytherapy Mieczysław Słapa, Marek Traczyk, Marcin Talejko, Krzysztof Wincel, Barbara Zaręba The Andrzej Sołtan Institute for Nuclear Studies Department of Physics Applications
Radioactivity. Alpha particles (α) :
 :") Radioactivity It is the property of an element that causes it to emit radiation Discovered by Becquerel (1896) Radiation comes from the nucleus of the atom There are three types of radiation : alpha particles
Radioactivity It is the property of an element that causes it to emit radiation Discovered by Becquerel (1896) Radiation comes from the nucleus of the atom There are three types of radiation : alpha particles
Brachytherapy, Noncoronary
 Brachytherapy, Noncoronary Policy Number: Original Effective Date: MM.05.004 05/10/2005 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 06/01/2017 Section: Radiology Place(s) of
Brachytherapy, Noncoronary Policy Number: Original Effective Date: MM.05.004 05/10/2005 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 06/01/2017 Section: Radiology Place(s) of
Neutron Interactions Part 2. Neutron shielding. Neutron shielding. George Starkschall, Ph.D. Department of Radiation Physics
 Neutron Interactions Part 2 George Starkschall, Ph.D. Department of Radiation Physics Neutron shielding Fast neutrons Slow down rapidly by scatter in hydrogenous materials, e.g., polyethylene, paraffin,
Neutron Interactions Part 2 George Starkschall, Ph.D. Department of Radiation Physics Neutron shielding Fast neutrons Slow down rapidly by scatter in hydrogenous materials, e.g., polyethylene, paraffin,
Radiation Therapy for Cancer: Questions and Answers
 Radiation Therapy for Cancer: Questions and Answers Key Points Radiation therapy uses ionizing radiation to kill cancer cells and shrink tumors (see Question 1). About half of all people with cancer are
Radiation Therapy for Cancer: Questions and Answers Key Points Radiation therapy uses ionizing radiation to kill cancer cells and shrink tumors (see Question 1). About half of all people with cancer are
PROGRESS IN RADIATION ONCOLOGY. Fox Chase Cancer Center. Jean Holland RN MSN AOCN Department of Radiation Oncology April 2017
 PROGRESS IN RADIATION ONCOLOGY Fox Chase Cancer Center Jean Holland RN MSN AOCN Department of Radiation Oncology April 2017 Radiation Therapy Therapeutic use of electromagnetic energy from a machine or
PROGRESS IN RADIATION ONCOLOGY Fox Chase Cancer Center Jean Holland RN MSN AOCN Department of Radiation Oncology April 2017 Radiation Therapy Therapeutic use of electromagnetic energy from a machine or
Rola brachyterapii w leczeniu wznów nowotworów języka i dna jamy ustnej. The role of brachytherapy in recurrent. oral cavity
 Rola brachyterapii w leczeniu wznów nowotworów języka i dna jamy ustnej The role of brachytherapy in recurrent tumours of the tongue and fundus of the oral cavity Janusz Skowronek, MD, PhD, Ass. Prof.
Rola brachyterapii w leczeniu wznów nowotworów języka i dna jamy ustnej The role of brachytherapy in recurrent tumours of the tongue and fundus of the oral cavity Janusz Skowronek, MD, PhD, Ass. Prof.
Limitations. General Clinical Applications of Brachytherapy Physics. Learning Objectives. Conflicts of Interest. University of Wisconsin - Madison
 General Clinical Applications of Brachytherapy Physics Bruce Thomadsen Limitations Due to file size limitations for this handout, many of the figures have had to be removed. I apologize for the lack of
General Clinical Applications of Brachytherapy Physics Bruce Thomadsen Limitations Due to file size limitations for this handout, many of the figures have had to be removed. I apologize for the lack of
Overview of Clinical and Research Activities at Georgetown University Hospital
 Overview of Clinical and Research Activities at Georgetown University Hospital Dalong Pang, Ph.D. Department of Radiation Medicine Georgetown University Hospital Clinical Operation Two Varian linear accelerators
Overview of Clinical and Research Activities at Georgetown University Hospital Dalong Pang, Ph.D. Department of Radiation Medicine Georgetown University Hospital Clinical Operation Two Varian linear accelerators
1 General Aspects Alain Gerbaulet, Dan Ash, Harm Meertens
 1 General Aspects Alain Gerbaulet, Dan Ash, Harm Meertens 1 History Radioactivity was discovered by Becquerel (Fig 1.1) in 1896 after accidental exposure of a photographic plate to uranium. Two years later
1 General Aspects Alain Gerbaulet, Dan Ash, Harm Meertens 1 History Radioactivity was discovered by Becquerel (Fig 1.1) in 1896 after accidental exposure of a photographic plate to uranium. Two years later
Inter-society standards for the performance of brachytherapy: a joint report from ABS, ACMP and ACRO
 Critical Reviews in Oncology/Hematology 48 (2003) 1 17 Inter-society standards for the performance of brachytherapy: a joint report from ABS, ACMP and ACRO Subir Nag a,, Ralph Dobelbower b, Glenn Glasgow
Critical Reviews in Oncology/Hematology 48 (2003) 1 17 Inter-society standards for the performance of brachytherapy: a joint report from ABS, ACMP and ACRO Subir Nag a,, Ralph Dobelbower b, Glenn Glasgow
Dosimetric Characteristics of the Brachytherapy Sources Based on Monte Carlo Method
 10 Dosimetric Characteristics of the Brachytherapy Sources Based on Monte Carlo Method Mahdi Sadeghi 1, Pooneh Saidi 2 and Claudio Tenreiro 3 1 Agricultural, Medical and Industrial School, P.O. Box 31485-498,
10 Dosimetric Characteristics of the Brachytherapy Sources Based on Monte Carlo Method Mahdi Sadeghi 1, Pooneh Saidi 2 and Claudio Tenreiro 3 1 Agricultural, Medical and Industrial School, P.O. Box 31485-498,
The Canadian National System for Incident Reporting in Radiation Treatment (NSIR-RT) Taxonomy March 11, 2015
 Taxonomy March 11, 2015") The Canadian National System for Incident Reporting in Radiation Treatment (NSIR-RT) Taxonomy March 11, 2015 Taxonomy Data Category Number Description Data Fields and Menu Choices 1. Impact 1.1 Incident
The Canadian National System for Incident Reporting in Radiation Treatment (NSIR-RT) Taxonomy March 11, 2015 Taxonomy Data Category Number Description Data Fields and Menu Choices 1. Impact 1.1 Incident
20 Prostate Cancer Dan Ash
 20 Prostate Cancer Dan Ash 1 Introduction Prostate cancer is a disease of ageing men for which the aetiology remains unknown. The incidence rises up to 30 to 40% in men over 80. The symptoms of localised
20 Prostate Cancer Dan Ash 1 Introduction Prostate cancer is a disease of ageing men for which the aetiology remains unknown. The incidence rises up to 30 to 40% in men over 80. The symptoms of localised
Radiation Protection in Laboratory work. Mats Isaksson, prof. Department of radiation physics, GU
 Radiation Protection in Laboratory work Mats Isaksson, prof. Department of radiation physics, GU mats.isaksson@radfys.gu.se Fundamental principles (ICRP) Justification Optimisation Application of dose
Radiation Protection in Laboratory work Mats Isaksson, prof. Department of radiation physics, GU mats.isaksson@radfys.gu.se Fundamental principles (ICRP) Justification Optimisation Application of dose
Patient Safety Focused QA. LDR Brachytherapy Vrinda Narayana
 Patient Safety Focused QA LDR Brachytherapy Vrinda Narayana D < 2 Gy/h Old LDR Brachytherapy? Ra-226; Cs-137; Ir-192 New Gynecological; interstitial Pd-103; I-125; Cs-131 Prostate implants Eye plaques
Patient Safety Focused QA LDR Brachytherapy Vrinda Narayana D < 2 Gy/h Old LDR Brachytherapy? Ra-226; Cs-137; Ir-192 New Gynecological; interstitial Pd-103; I-125; Cs-131 Prostate implants Eye plaques
PHYS 383: Applications of physics in medicine (offered at the University of Waterloo from Jan 2015)
") PHYS 383: Applications of physics in medicine (offered at the University of Waterloo from Jan 2015) Course Description: This course is an introduction to physics in medicine and is intended to introduce
PHYS 383: Applications of physics in medicine (offered at the University of Waterloo from Jan 2015) Course Description: This course is an introduction to physics in medicine and is intended to introduce
Brachytherapy, Noncoronary
 Brachytherapy, Noncoronary Policy Number: Original Effective Date: MM.05.004 05/10/2005 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 11/21/2014 Section: Radiology Place(s) of
Brachytherapy, Noncoronary Policy Number: Original Effective Date: MM.05.004 05/10/2005 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 11/21/2014 Section: Radiology Place(s) of
National System for Incident Reporting in Radiation Therapy (NSIR-RT) Taxonomy
 Taxonomy") Canadian Partnership for Quality Radiotherapy (CPQR) National System for Incident Reporting in Radiation Therapy (NSIR-RT) National System for Incident Reporting in Radiation Therapy (NSIR-RT) Taxonomy
Canadian Partnership for Quality Radiotherapy (CPQR) National System for Incident Reporting in Radiation Therapy (NSIR-RT) National System for Incident Reporting in Radiation Therapy (NSIR-RT) Taxonomy
RADIATION ONCOLOGY AT UNIVERSITY OF COLORADO HOSPITAL
 RADIATION ONCOLOGY AT UNIVERSITY OF COLORADO HOSPITAL Cancer treatment requires a team effort. The Radiation Oncology team may include radiation oncology doctors, registered nurses, radiation therapists,
RADIATION ONCOLOGY AT UNIVERSITY OF COLORADO HOSPITAL Cancer treatment requires a team effort. The Radiation Oncology team may include radiation oncology doctors, registered nurses, radiation therapists,
A Review of UK Guidelines for Prostate Brachytherapy. Sarah Aldridge. Head of Brachytherapy Physics Guy s & St. Thomas NHS Foundation Trust
 A Review of UK Guidelines for Prostate Brachytherapy Sarah Aldridge Head of Brachytherapy Physics Guy s & St. Thomas NHS Foundation Trust Overview Review of current guidelines for LDR & HDR prostate brachytherapy
A Review of UK Guidelines for Prostate Brachytherapy Sarah Aldridge Head of Brachytherapy Physics Guy s & St. Thomas NHS Foundation Trust Overview Review of current guidelines for LDR & HDR prostate brachytherapy
Oral cavity cancer Post-operative treatment
 Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Interstitial Breast Brachytherapy
 Patient Education Questions? Your questions are important. Call your doctor or health care provider if you have questions or concerns. UWMC clinic staff are also available to help at any time. During normal
Patient Education Questions? Your questions are important. Call your doctor or health care provider if you have questions or concerns. UWMC clinic staff are also available to help at any time. During normal
University Medical Center Utrecht The Netherlands
 University Medical Center Utrecht The Netherlands Metha Maenhout, MD: PHD student Maaike Koelink: Specialist RTT Wilfred de Vries: Physicist Assistant MED-00005 [00] UMC Utrecht Radiotherapy Department
University Medical Center Utrecht The Netherlands Metha Maenhout, MD: PHD student Maaike Koelink: Specialist RTT Wilfred de Vries: Physicist Assistant MED-00005 [00] UMC Utrecht Radiotherapy Department