GI Polyp syndromes in children. Screening and surveillance, surgery.
|
|
|
- Lauren Atkins
- 5 years ago
- Views:
Transcription

1 Dr Warren Hyer Consultant Paediatric Gastroenterologist St Mark s Hospital, UK GI Polyp syndromes in children Screening and surveillance, surgery. No conflict of interests to declare
2 Objectives Understand the reason for screening and surveillance Understand the genetic basis for different polyposis syndromes Update on how and when adolescents and children should undergo genetic testing and commence colonoscopic surveillance and surgery
3 Classification of Intestinal Polyps Common polyps Juvenile polyps (hamartoma) Inheritable polyposis adenomatous polyps familial adenomatous polyposis coli (FAP) MYH-associated polyposis (MAP) hamartomatous polyps Peutz-Jeghers syndrome (PJS) PTEN hamartoma tumor syndromes Cowden s disease Bannayan-Riley-Ruvalcaba syndrome Juvenile polyposis (JPS)
4

5
6 So why consider screening and surveillance? Solitary colonic polyp to avoid missing others FAP to prevent a CRC PJS to prevent a mid gut intussusception and laparotomy JPS to characterise the condition
7 The solitary isolated colonic polyp

8 Single harmless juvenile colonic polyp Fox at al Clin Gastroenterol Hepatol 8: 796, 2010

9 Not all single polyps are benign
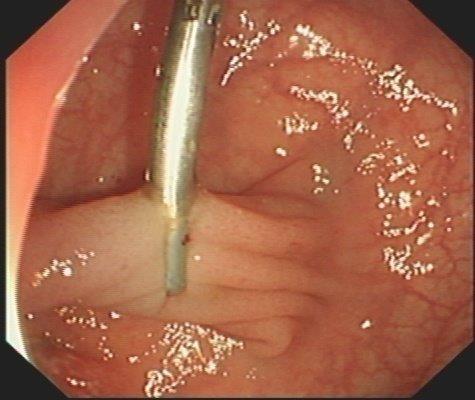
10 Preinjection


11 The surgeon is defunct
12 Bottom Line They are benign nearly always Polypectomy needs waterproof pants Rescoping to know if there are more Consider FH Rescope if bleed Perhaps rescope later if bleeding, FH, uncertain histology
13 FAP - Clinical scenario A 7 year old from a family known to be affected by FAP comes to your clinic with infrequent rectal bleeding. Why and when to screen and start surveillance? Should you perform genetic testing? Should you undertake a colonoscopy?

14 Current practice, start screening in teenage years

15
16

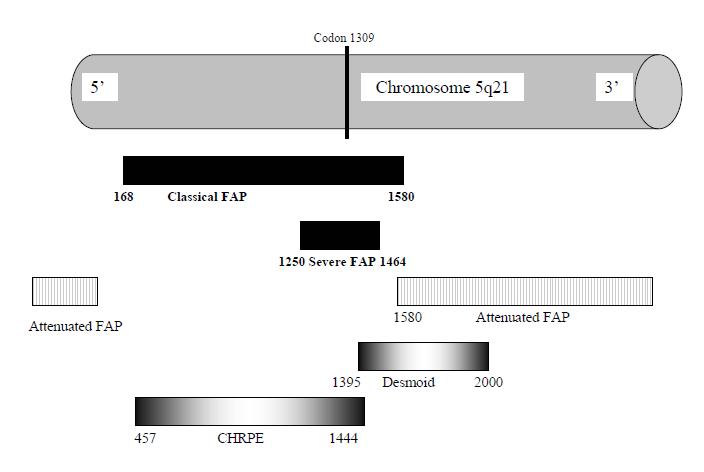
17 Early childhood presentation of FAP No FH Presents with rectal bleeding alone CHRPE Mutation codon 1309 Colectomy sample age 4 years Youngest symptomatic FAP child Symptomatic Polyposis in a Four-Year- Old: The Exception Proves the Rule Will, Phillips, Hyer, Clark.


18 Desmoid disease- codon >1400


19 Commence genetic testing at age of earliest onset of disease Family mutation known Family mutation known Family mutation not known Counsel and genetic testing Counsel and genetic testing No genetic testing Positive result Negative result Annual sigmoidoscopy Full colonoscopy Discharge from follow up
20 Commence genetic testing at age of earliest onset of disease Family mutation known Family mutation known Family mutation not known Counsel and genetic testing Positive result Counsel and genetic testing Presence of bleeding or unfavourable genotype should lead to earlier screening Negative result No genetic testing Annual sigmoidoscopy Full colonoscopy Discharge from follow up


21 Assess adenoma burden in the rectum

22 Assess polyp burden in the colon
23 Annual colonoscopy impacts on surgical choices Cancer risk Cancer risk Complications and sequelae Complications and sequelae IRA < 20 rectal adenomas <1000 colonic adenomas Genotype Density of rectal polyps Access to laparoscopy Family experience Perception of risk Risk of desmoid Schooling, relationships IPAA > 20 rectal adenomas >1000 colonic adenomas Any rectal adenoma >3cms

24 Delay duodenal surveillance until > 20+ Duodenal polyposis Spigelman classification
25 Surveillance for a teenager does not stop after colectomy FAP proband. Genetic testing colonoscopy from age years depending on symptoms. Refer for surgery depending on adenoma burden IRA if rectal adenoma burden permits IPAA if preferable 6 monthly sigmoidoscopy Annual pouchoscopy Long term FU and commence duodenal surveillance (age 20+)
26 Bottom Line Often wait until teenage years Commence earlier screening if bleeding or symptomatic Understand the gene, start earlier if high risk genotype Chemoprevention does not alter timing nor surveillance

27
28
, offer genetic testing prior to age of")
29 So at what age to undertake genetic testing? If the kindred genetic mutation is known (STK11), offer genetic testing prior to age of earliest onset of complications eg infancy
30 Diagnosis confirmed eg mucosal pigmentation, FH, genetics Symptomatic with polyp leading intussusception Asymptomatic affected child Start screening age 5-8 years OGD, VCE and colonoscopy


31 Symptomatic and obstructive symptoms with intussusception get a surgeon
32

33
34 Diagnosis confirmed eg mucosal pigmentation, FH, genetics Symptomatic with polyp leading intussusception Asymptomatic affected child Start screening age 5-8 years OGD, VCE (or MRI) and colonoscopy

35 The risk from surveillance is the polypectomy

36 Post polypectomy check the site

37 Clips and loops to reduce complication from polypectomy

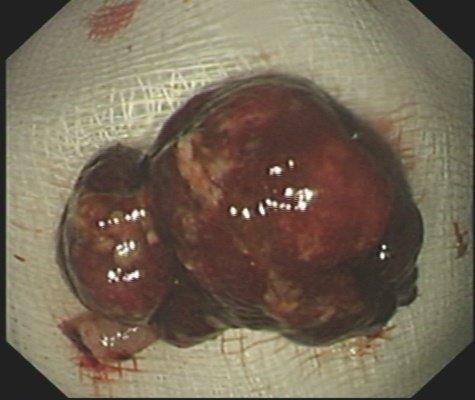
38 Many polyps are massive. Do not feel you should remove endoscopically

39 Beware duodenal polyps
40 Current screening PJS protocol Diagnosis confirmed eg mucosal pigmentation, FH, genetics Symptomatic with polyp leading intussuception Polyps < 5mm Asymptomatic affected child Start screening age 5-8 years OGD, VCE and colonoscopy every 2 yrs Polyps 5-10mm Polyps >15mm Laparoscopy or laparotomy with Intraoperative enteroscopy reduces risk of rpt laparotomy Rpt in 2 years DBE Elective planned polypectomy by DBE, laparoscopy Or laparotomy
41 PJS Bottom Line Symptomatic needs surgery Small bowel surveillance starts at age 5-8 years but respect the risks of polypectomy
42 Classification of Intestinal Polyps Common polyps Juvenile polyps (hamartoma) Inheritable polyposis adenomatous polyps familial adenomatous polyposis coli (FAP) MYH-associated polyposis (MAP) hamartomatous polyps Peutz-Jegher s syndrome PTEN hamartoma tumor syndromes Cowden s disease Bannayan-Riley-Ruvalcaba syndrome Juvenile polyposis

43 Consider a polyposis syndrome in a child with a juvenile polyp...if >3-5 polyps cumulative Dysmorphic features macrocephaly, digital clubbing Concerning family history Possibility of HHT (hereditary haemorrhagic telangiectasia)
44 Interpreting hamartomatous syndromes Genetics Clinical phenotype Pathology Family history Colonoscopic appearance Juvenile polyposis Syndrome (SMAD4 or BMPR1A) Cowdens syndrome (PTEN) Bannayan Riley Ruvalcaba Syndrome (PTEN) Juvenile polyposis Syndrome in infancy
45 Genetic mutation is not identified in 50% of cases PTEN 85% of Cowden 65% of Bannayan Riley Ruvalcaba syndrome SMAD 4 /HHT 20-50% JPS BMPR1A 20-40% of JPS ENG 2-5% of JPS, HHT
46 Endoscopic surveillance Juvenile polyposis syndrome (SMAD4/BMPR1A) 2-3 yearly colonoscopy with polypectomy if bleeding from age about years Consider Ix for HHT GI malignancy risk is very low PTEN eg Cowden or BRRS Other non GI screening is necessary GI malignancy risk is very low
47 Again don t underestimate the polypectomy risk 5cms
48 Juvenile polyposis syndrome Careful assess the phenotype, and interpret genetics with a geneticist CRC risk is still low Modify the surveillance according to phenotype, and symptoms

49 Bottom Line JP The polyps are benign Repeat colonoscopy to know if there are more later in life Consider FH Rescope if bleeding

50 Bottom Line FAP Often wait until teenage years Commence earlier screening if bleeding or symptomatic Understand the gene - start earlier if high risk genotype Chemoprevention does not alter timing nor surveillance
51 Bottom Line PJS Symptomatic needs surgery Small bowel surveillance starts at age 5-8 years but respect the risks of polypectomy

52 Juvenile polyposis syndrome Careful assess the phenotype, and interpret genetics with a geneticist CRC risk is still low Modify the surveillance according to phenotype, and symptoms
53 Why surveillance Solitary colonic polyp to avoid missing others FAP to prevent a CRC PJS to prevent a mid gut intussusception and laparotomy JPS to characterise the condition Be careful with polypectomy esp in PJS. Use the surgeon wisely
54 Annual colonoscopy impacts on surgical choices Cancer risk Cancer risk Complications and sequelae Complications and sequelae IRA < 20 rectal adenomas <1000 colonic adenomas Genotype Density of rectal polyps Access to laparoscopy Family experience Perception of risk Risk of desmoid Schooling, relationships IPAA > 20 rectal adenomas >1000 colonic adenomas Any rectal adenoma >3cms
55 Thank you UK Polyposis team St Mark s Hospital UK: Polyposis Registry, UK Professor Robin Phillips, Kay Neale and Jackie Hawkins Prof Sue Clark Wolfson Academic Dept of Endoscopy, Department of Colorectal Surgery Thank you to the organisers of ESPGHAN and the working group for paediatric polyposis
For identification, support and follow up related to Familial Gastrointestinal Cancer conditions. South Island Cancer Nurses Network September 2013
 For identification, support and follow up related to Familial Gastrointestinal Cancer conditions South Island Cancer Nurses Network September 2013 Who are we? Specialist multidisciplinary team: Nurse coordinators,
For identification, support and follow up related to Familial Gastrointestinal Cancer conditions South Island Cancer Nurses Network September 2013 Who are we? Specialist multidisciplinary team: Nurse coordinators,
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Pathology reports, related operative reports and consult letters must be provided with a request for assessment.
 Page 1 of 6 Polyposis Syndromes Inherited risk for colorectal cancer is associated with a number of polyposis syndromes (genes), some of which are well-defined and others are less common. Identification
Page 1 of 6 Polyposis Syndromes Inherited risk for colorectal cancer is associated with a number of polyposis syndromes (genes), some of which are well-defined and others are less common. Identification
Familial Adenomatous Polyposis
 Familial Adenomatous Polyposis 1 in 10,000 incidence 100 s to 1000 s of colonic adenomas by teens Cancer risk: colon, gastric, duodenum (periampulla), small bowel, pancreas, papillary thyroid, childhood
Familial Adenomatous Polyposis 1 in 10,000 incidence 100 s to 1000 s of colonic adenomas by teens Cancer risk: colon, gastric, duodenum (periampulla), small bowel, pancreas, papillary thyroid, childhood
Timing of surgery in FAP
 Timing of surgery in FAP Sue Clark Consultant Colorectal Surgeon, The Polyposis Registry, St Mark s Hospital, London, UK. 0-5 5-10 10-15 15-20 20-25 25-30 30-35 35-40 40-45 45-50 50-55 55-60 60-65 65-70
Timing of surgery in FAP Sue Clark Consultant Colorectal Surgeon, The Polyposis Registry, St Mark s Hospital, London, UK. 0-5 5-10 10-15 15-20 20-25 25-30 30-35 35-40 40-45 45-50 50-55 55-60 60-65 65-70
YES NO UNKNOWN. Stage I: Rule-Out Dashboard ACTIONABILITY PENETRANCE SIGNIFICANCE/BURDEN OF DISEASE NEXT STEPS. YES ( 1 of above)
") Stage I: Rule-Out Dashboard GENE/GENE PANEL: SMAD4, BMPR1A DISORDER: Juvenile Polyposis Syndrome HGNC ID: 6670, 1076 OMIM ID: 174900, 175050 ACTIONABILITY PENETRANCE 1. Is there a qualifying resource,
Stage I: Rule-Out Dashboard GENE/GENE PANEL: SMAD4, BMPR1A DISORDER: Juvenile Polyposis Syndrome HGNC ID: 6670, 1076 OMIM ID: 174900, 175050 ACTIONABILITY PENETRANCE 1. Is there a qualifying resource,
GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS. Family Health Clinical Genetics. Clinical Genetics department
 GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS Full Title of Guideline: Author (include email and role): Division & Speciality: GUIDELINES FOR THE GENETIC MANAGEMENT OF A FAMILY
GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS Full Title of Guideline: Author (include email and role): Division & Speciality: GUIDELINES FOR THE GENETIC MANAGEMENT OF A FAMILY
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
27
 26 27 28 29 30 31 32 33 34 35 Diagnosis:? Diagnosis: Juvenile Polyposis with BMPR1A Mutation 36 Juvenile Polyposis Syndrome Rare Autosomal Dominant Disorder with Multiple Juvenile Polyps in GI Tract Juvenile
26 27 28 29 30 31 32 33 34 35 Diagnosis:? Diagnosis: Juvenile Polyposis with BMPR1A Mutation 36 Juvenile Polyposis Syndrome Rare Autosomal Dominant Disorder with Multiple Juvenile Polyps in GI Tract Juvenile
GI EMERGENCIES Acute Abdominal Pain
 GI EMERGENCIES Acute Abdominal Pain Marcia Cruz-Correa, MD, PhD, AGAF. FASGE Associate Professor of Medicine, Biochemistry, Surgery Director Translational Research University of Puerto Rico Comprehensive
GI EMERGENCIES Acute Abdominal Pain Marcia Cruz-Correa, MD, PhD, AGAF. FASGE Associate Professor of Medicine, Biochemistry, Surgery Director Translational Research University of Puerto Rico Comprehensive
Michele Bettinelli RN Maria Scholz RN Sandra Scolaro RN
 Michele Bettinelli RN Maria Scholz RN Sandra Scolaro RN Objectives Define Peutz-Jeghers Syndrome (PJS) Describe the management and treatment of PJS Discuss the patient experience associated with the diagnosis
Michele Bettinelli RN Maria Scholz RN Sandra Scolaro RN Objectives Define Peutz-Jeghers Syndrome (PJS) Describe the management and treatment of PJS Discuss the patient experience associated with the diagnosis
Classification of polyposis syndromes two major groups. Adenomatous polyposis syndromes. Hamartomatous polyposis syndromes
 Hereditary polyposis syndromes Classification of polyposis syndromes two major groups adenomatous and non-adenomatous polyposis syndromes Adenomatous polyposis syndromes Familial adenomatous polyposis(fap)
Hereditary polyposis syndromes Classification of polyposis syndromes two major groups adenomatous and non-adenomatous polyposis syndromes Adenomatous polyposis syndromes Familial adenomatous polyposis(fap)
COLON CANCER & GENETICS VERMONT COLORECTAL CANCER SUMMIT NOVEMBER 15, 2014
 COLON CANCER & GENETICS VERMONT COLORECTAL CANCER SUMMIT NOVEMBER 15, 2014 WENDY MCKINNON, MS, CGC CERTIFIED GENETIC COUNSELOR FAMILIAL CANCER PROGRAM UNIVERSIT Y OF VERMONT MEDICAL CENTER 1 CHARACTERISTICS
COLON CANCER & GENETICS VERMONT COLORECTAL CANCER SUMMIT NOVEMBER 15, 2014 WENDY MCKINNON, MS, CGC CERTIFIED GENETIC COUNSELOR FAMILIAL CANCER PROGRAM UNIVERSIT Y OF VERMONT MEDICAL CENTER 1 CHARACTERISTICS
Hereditary Colorectal Cancer Syndromes Miguel A. Rodriguez-Bigas, MD
 Hereditary Colorectal Cancer Syndromes Miguel A. Rodriguez-Bigas, MD Living Beyond Cancer A-Z January 12,2019 Hereditary CRC Syndromes Objectives are to discuss the : Most common Hereditary CRC syndromes
Hereditary Colorectal Cancer Syndromes Miguel A. Rodriguez-Bigas, MD Living Beyond Cancer A-Z January 12,2019 Hereditary CRC Syndromes Objectives are to discuss the : Most common Hereditary CRC syndromes
Genetic Testing for Familial Gastrointestinal Cancer Syndromes. C. Richard Boland, MD La Jolla, CA January 21, 2017
 Genetic Testing for Familial Gastrointestinal Cancer Syndromes C. Richard Boland, MD La Jolla, CA January 21, 2017 Disclosure Information C. Richard Boland, MD I have no financial relationships to disclose.
Genetic Testing for Familial Gastrointestinal Cancer Syndromes C. Richard Boland, MD La Jolla, CA January 21, 2017 Disclosure Information C. Richard Boland, MD I have no financial relationships to disclose.
Colorectal Cancer Syndromes. Barbara Jung, MD AGAF Associate Professor and Chief University of Illinois at Chicago
 Colorectal Cancer Syndromes Barbara Jung, MD AGAF Associate Professor and Chief University of Illinois at Chicago Outline Colon cancer General Genetics, Risk, Screening Specific Syndromes, when to suspect,
Colorectal Cancer Syndromes Barbara Jung, MD AGAF Associate Professor and Chief University of Illinois at Chicago Outline Colon cancer General Genetics, Risk, Screening Specific Syndromes, when to suspect,
ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes
 ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes Sapna Syngal, MD, MPH, FACG, 1,2,3 Randall E. Brand, MD, FACG, 4 James M. Church, MD, FACG, 5,6,7
ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes Sapna Syngal, MD, MPH, FACG, 1,2,3 Randall E. Brand, MD, FACG, 4 James M. Church, MD, FACG, 5,6,7
Colorectal Cancer and Hereditary Colon Cancer Syndromes Carol A. Burke, M.D.
 Colorectal Cancer and Hereditary, FACG, FACP Sanford R. Weiss MD Center for Hereditary Colorectal Neoplasia Digestive Disease Institute Cleveland Clinic, Cleveland, Ohio 1 Objectives Review the molecular
Colorectal Cancer and Hereditary, FACG, FACP Sanford R. Weiss MD Center for Hereditary Colorectal Neoplasia Digestive Disease Institute Cleveland Clinic, Cleveland, Ohio 1 Objectives Review the molecular
Hereditary Gastric Cancer
 Hereditary Gastric Cancer Dr Bastiaan de Boer Consultant Pathologist Department of Anatomical Pathology PathWest Laboratory Medicine, QE II Medical Centre Clinical Associate Professor School of Pathology
Hereditary Gastric Cancer Dr Bastiaan de Boer Consultant Pathologist Department of Anatomical Pathology PathWest Laboratory Medicine, QE II Medical Centre Clinical Associate Professor School of Pathology
Journal of Pediatric Gastroenterology and Nutrition, Publish Ahead of Print
 Journal of Pediatric Gastroenterology and Nutrition, Publish Ahead of Print DOI : 10.1097/MPG.0000000000002247 Management of familial adenomatous polyposis in children and adolescents: Position Paper from
Journal of Pediatric Gastroenterology and Nutrition, Publish Ahead of Print DOI : 10.1097/MPG.0000000000002247 Management of familial adenomatous polyposis in children and adolescents: Position Paper from
PENETRANCE ACTIONABILITY SIGNIFICANCE/BURDEN OF DISEASE NEXT STEPS. YES ( 1 of above) YES (Proceed to Stage II)
 YES (Proceed to Stage II)") Stage I: Binning Dashboard GENE/GENE PANEL: APC ACTIONABILITY 1. Is there a qualifying resource, such as a practice guideline or systematic review, for the genetic condition? 2. Does the practice guideline
Stage I: Binning Dashboard GENE/GENE PANEL: APC ACTIONABILITY 1. Is there a qualifying resource, such as a practice guideline or systematic review, for the genetic condition? 2. Does the practice guideline
Gastrointestinal polyposis syndromes for the general gastroenterologist
 TRAINING MATTERS CURRICULUM BASED CLINICAL REVIEWS Gastrointestinal polyposis syndromes for the general gastroenterologist Joanna J Hurley, 1,2 Iain Ewing, 3 Julian R Sampson, 2 Sunil Dolwani 1 1 Department
TRAINING MATTERS CURRICULUM BASED CLINICAL REVIEWS Gastrointestinal polyposis syndromes for the general gastroenterologist Joanna J Hurley, 1,2 Iain Ewing, 3 Julian R Sampson, 2 Sunil Dolwani 1 1 Department
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
Disclosure. Polyps in Pediatrics. Learning Objectives. Case Presentation I. Case Presentation II
 Disclosure Polyps in Pediatrics I have no relationships with commercial companies to disclose. Sonal Desai, MD Division of Pediatric Gastroenterology May 31, 2013 Pediatric Grand Rounds Learning Objectives
Disclosure Polyps in Pediatrics I have no relationships with commercial companies to disclose. Sonal Desai, MD Division of Pediatric Gastroenterology May 31, 2013 Pediatric Grand Rounds Learning Objectives
Genetic testing all you need to know
 Genetic testing all you need to know Sue Clark Consultant Colorectal Surgeon, St Mark s Hospital, London, UK. Colorectal cancer Familial 33% Polyposis syndromes
Genetic testing all you need to know Sue Clark Consultant Colorectal Surgeon, St Mark s Hospital, London, UK. Colorectal cancer Familial 33% Polyposis syndromes
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
 BUY ONE GENE, GET ONE 30 FREE! G E N E P A N E L T E S T I N G F O R H E R E D I T A R Y C A N C E R : G E T T I N G I T R I G H T THIS COULD BE YOU ONE DAY SOON: Starting out in your new OB/Gyn practice
BUY ONE GENE, GET ONE 30 FREE! G E N E P A N E L T E S T I N G F O R H E R E D I T A R Y C A N C E R : G E T T I N G I T R I G H T THIS COULD BE YOU ONE DAY SOON: Starting out in your new OB/Gyn practice
Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes
 Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Policy Number: 2.04.08 Last Review: 1/2019 Origination: 1/2004 Next Review: 1/2020 Policy Blue Cross and Blue Shield of Kansas
Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Policy Number: 2.04.08 Last Review: 1/2019 Origination: 1/2004 Next Review: 1/2020 Policy Blue Cross and Blue Shield of Kansas
BowelGene. How do I know if I am at risk? Families with hereditary bowel cancer generally show one or more of the following clues:
 BowelGene BowelGene What is hereditary bowel cancer? Bowel cancer (also known as colorectal cancer) is the fourth most common cancer in the UK. Unfortunately 1 in 19 women and 1 in 14 men will develop
BowelGene BowelGene What is hereditary bowel cancer? Bowel cancer (also known as colorectal cancer) is the fourth most common cancer in the UK. Unfortunately 1 in 19 women and 1 in 14 men will develop
Endoscopic techniques for surveillance and treatment of FAP
 Endoscopic techniques for surveillance and treatment of FAP Evelien Dekker MD PhD Department of Gastroenterology & Hepatology Academic Medical Center Amsterdam The Netherlands FAP: endoscopic surveillance
Endoscopic techniques for surveillance and treatment of FAP Evelien Dekker MD PhD Department of Gastroenterology & Hepatology Academic Medical Center Amsterdam The Netherlands FAP: endoscopic surveillance
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
GHUK BowelGene_2017.qxp_Layout 1 22/02/ :22 Page 3 BowelGene
 GHUK BowelGene_2017.qxp_Layout 1 22/02/2017 10:22 Page 3 BowelGene BowelGene What is hereditary bowel cancer? Bowel cancer (also known as colorectal cancer) is the fourth most common cancer in the UK.
GHUK BowelGene_2017.qxp_Layout 1 22/02/2017 10:22 Page 3 BowelGene BowelGene What is hereditary bowel cancer? Bowel cancer (also known as colorectal cancer) is the fourth most common cancer in the UK.
The term juvenile polyp was used in 1957 by Horrilleno. Juvenile Polyps: Recurrence in Patients With Multiple and Solitary Polyps
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:795 799 Juvenile Polyps: Recurrence in Patients With Multiple and Solitary Polyps VICTOR L. FOX,* STEPHEN PERROS,* HONGYU JIANG,*, and JEFFREY D. GOLDSMITH,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:795 799 Juvenile Polyps: Recurrence in Patients With Multiple and Solitary Polyps VICTOR L. FOX,* STEPHEN PERROS,* HONGYU JIANG,*, and JEFFREY D. GOLDSMITH,
Journal of Pediatric Gastroenterology and Nutrition, Publish Ahead of Print
 Journal of Pediatric Gastroenterology and Nutrition, Publish Ahead of Print DOI : 10.1097/MPG.0000000000002248 Management of Peutz-Jeghers syndromes in children and adolescents: A Position Paper from the
Journal of Pediatric Gastroenterology and Nutrition, Publish Ahead of Print DOI : 10.1097/MPG.0000000000002248 Management of Peutz-Jeghers syndromes in children and adolescents: A Position Paper from the
COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University
 Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University") COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University 1. I am a surgeon; of course I have nothing to disclose.
COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University 1. I am a surgeon; of course I have nothing to disclose.
Risk of Colorectal Cancer (CRC) Hereditary Syndromes in GI Cancer GENETIC MALPRACTICE
 Hereditary Syndromes in GI Cancer GENETIC MALPRACTICE") Identifying the Patient at Risk for an Inherited Syndrome Sapna Syngal, MD, MPH, FACG Director, Gastroenterology Director, Familial GI Program Dana-Farber/Brigham and Women s Cancer Center Associate Professor
Identifying the Patient at Risk for an Inherited Syndrome Sapna Syngal, MD, MPH, FACG Director, Gastroenterology Director, Familial GI Program Dana-Farber/Brigham and Women s Cancer Center Associate Professor
B Base excision repair, in MUTYH-associated polyposis and colorectal cancer, BRAF testing, for hereditary colorectal cancer, 696
 Index Note: Page numbers of article titles are in boldface type. A Adenomatous polyposis, familial. See Familial adenomatous polyposis. Anal anastomosis, ileal-pouch, proctocolectomy with, in FAP, 591
Index Note: Page numbers of article titles are in boldface type. A Adenomatous polyposis, familial. See Familial adenomatous polyposis. Anal anastomosis, ileal-pouch, proctocolectomy with, in FAP, 591
Duodenal adenomas Management. Dr Stratis Alexandridis Consultant Gastroenterologist BRI
 Duodenal adenomas Management Dr Stratis Alexandridis Consultant Gastroenterologist BRI Introduction Ampullary and non ampullary polyps of the duodenum are diagnosed within and outside genetic syndromes.
Duodenal adenomas Management Dr Stratis Alexandridis Consultant Gastroenterologist BRI Introduction Ampullary and non ampullary polyps of the duodenum are diagnosed within and outside genetic syndromes.
Colonic polyps and colon cancer. Andrew Macpherson Director of Gastroentology University of Bern
 Colonic polyps and colon cancer Andrew Macpherson Director of Gastroentology University of Bern Improtance of the problem of colon cancers - Epidemiology Lifetime risk 5% Incidence/10 5 /annum (US Detroit
Colonic polyps and colon cancer Andrew Macpherson Director of Gastroentology University of Bern Improtance of the problem of colon cancers - Epidemiology Lifetime risk 5% Incidence/10 5 /annum (US Detroit
Cancer Genomics 101. BCCCP 2015 Annual Meeting
 Cancer Genomics 101 BCCCP 2015 Annual Meeting Objectives Identify red flags in a person s personal and family medical history that indicate a potential inherited susceptibility to cancer Develop a systematic
Cancer Genomics 101 BCCCP 2015 Annual Meeting Objectives Identify red flags in a person s personal and family medical history that indicate a potential inherited susceptibility to cancer Develop a systematic
An Introduction to MUTYH Associated Polyposis (MAP)
") An Introduction to MUTYH Associated Polyposis (MAP) 1 An Introduction to MUTYH Associated Polyposis(MAP) Contents What is MUTYH Associated Polyposis (MAP)? 2 What causes MUTYH Associated Polyposis (MAP)?
An Introduction to MUTYH Associated Polyposis (MAP) 1 An Introduction to MUTYH Associated Polyposis(MAP) Contents What is MUTYH Associated Polyposis (MAP)? 2 What causes MUTYH Associated Polyposis (MAP)?
HEREDITARY COLORECTAL CANCER AND POLYPOSIS SYNDROMES
 gastrointestinal tract and abdomen HEREDITARY COLORECTAL CANCER AND POLYPOSIS SYNDROMES Jose G. Guillem, MD, MPH, FACS, and John B. Ammori, MD* The majority of cases of inherited colorectal cancer (CRC)
gastrointestinal tract and abdomen HEREDITARY COLORECTAL CANCER AND POLYPOSIS SYNDROMES Jose G. Guillem, MD, MPH, FACS, and John B. Ammori, MD* The majority of cases of inherited colorectal cancer (CRC)
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
FINAL HISTOLOGICAL DIAGNOSIS: Villo-adenomatous polyp with in-situ-carcinomatous foci (involving both adenomatous and villous component).
.") SOLITARY VILLO ADENOMATOUS POLYP WITH CARCINOMATOUS CHANGES RECTUM: A Divvya B 1, M. Valluvan 2, Rehana Tippoo 3, P. Viswanathan 4, R. Baskaran 5 HOW TO CITE THIS ARTICLE: Divvya B, M. Valluvan, Rehana
SOLITARY VILLO ADENOMATOUS POLYP WITH CARCINOMATOUS CHANGES RECTUM: A Divvya B 1, M. Valluvan 2, Rehana Tippoo 3, P. Viswanathan 4, R. Baskaran 5 HOW TO CITE THIS ARTICLE: Divvya B, M. Valluvan, Rehana
Colorectal Cancer - Working in Partnership. David Baty Genetics, Ninewells Hospital
 Colorectal Cancer - Working in Partnership David Baty Genetics, Ninewells Hospital Genetics and Pathology National initiatives Colorectal cancer Inherited CRC Sporadic CRC The Liquid Biopsy The future?
Colorectal Cancer - Working in Partnership David Baty Genetics, Ninewells Hospital Genetics and Pathology National initiatives Colorectal cancer Inherited CRC Sporadic CRC The Liquid Biopsy The future?
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population
 Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
Colorectal Neoplasia. Dr. Smita Devani MBChB, MRCP. Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi
 Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
Hereditary GI tumor syndromes ACG guidelines of genetic testing and management. Dr. med. Henrik Csaba Horváth PhD
 Hereditary GI tumor syndromes ACG guidelines of genetic testing and management Dr. med. Henrik Csaba Horváth PhD Genetic testing and management of hereditary GI tumor syndromes June 29, 2016 2 Clinical
Hereditary GI tumor syndromes ACG guidelines of genetic testing and management Dr. med. Henrik Csaba Horváth PhD Genetic testing and management of hereditary GI tumor syndromes June 29, 2016 2 Clinical
Pathology perspective of colonic polyposis syndromes
 Pathology perspective of colonic polyposis syndromes When are too many polyps too many? David Schaeffer Head and Consultant Pathologist, Department of Pathology and Laboratory Medicine, Vancouver General
Pathology perspective of colonic polyposis syndromes When are too many polyps too many? David Schaeffer Head and Consultant Pathologist, Department of Pathology and Laboratory Medicine, Vancouver General
Hereditary Colorectal Polyposis and Cancer Syndromes: A Primer on Diagnosis and Management
 CLINICAL AND SYSTEMATIC S 1509 CME Hereditary Colorectal Polyposis and Cancer Syndromes: A Primer on Diagnosis and Management Pr iyan ka Kant h, M D, M S 1, Jade Grimmett, MS2, 3, Mar j an C hampi ne,
CLINICAL AND SYSTEMATIC S 1509 CME Hereditary Colorectal Polyposis and Cancer Syndromes: A Primer on Diagnosis and Management Pr iyan ka Kant h, M D, M S 1, Jade Grimmett, MS2, 3, Mar j an C hampi ne,
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci. Colon polyps. Colorectal cancer
 Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Management of higher risk of colorectal cancer. Huw Thomas
 Management of higher risk of colorectal cancer Huw Thomas Colorectal Cancer 41,000 new cases pa in UK 16,000 deaths pa 60% 5 year survival Adenoma-carcinoma sequence (Morson) Survival vs stage (Dukes)
Management of higher risk of colorectal cancer Huw Thomas Colorectal Cancer 41,000 new cases pa in UK 16,000 deaths pa 60% 5 year survival Adenoma-carcinoma sequence (Morson) Survival vs stage (Dukes)
During the past decade the genetic etiology of all of. Genetic Testing for Inherited Colon Cancer
 GASTROENTEROLOGY 2005;128:1696 1716 Genetic Testing for Inherited Colon Cancer RANDALL BURT*, and DEBORAH W. NEKLASON*, *Huntsman Cancer Institute, Salt Lake City; and Departments of Medicine and Oncological
GASTROENTEROLOGY 2005;128:1696 1716 Genetic Testing for Inherited Colon Cancer RANDALL BURT*, and DEBORAH W. NEKLASON*, *Huntsman Cancer Institute, Salt Lake City; and Departments of Medicine and Oncological
Adenomatous Polyposis Syndromes (FAP/AFAP and MAP)
") A Patient s Guide to risk assessment Adenomatous Polyposis Syndromes (FAP/AFAP and MAP) Hereditary Cancer Testing: Is it Right for You? This workbook is designed to help you decide if hereditary cancer
A Patient s Guide to risk assessment Adenomatous Polyposis Syndromes (FAP/AFAP and MAP) Hereditary Cancer Testing: Is it Right for You? This workbook is designed to help you decide if hereditary cancer
LIST OF ABBREVIATIONS
 Gastroenter oenterology 2005 Royal College of Physicians of Edinburgh Screening and surveillance for upper and lower gastrointestinal cancer JN Plevris Consultant Gastroenterologist and Honorary Senior
Gastroenter oenterology 2005 Royal College of Physicians of Edinburgh Screening and surveillance for upper and lower gastrointestinal cancer JN Plevris Consultant Gastroenterologist and Honorary Senior
FAMILIAL COLORECTAL CANCER. Lyn Schofield Manager Familial Cancer Registry
 FAMILIAL COLORECTAL CANCER Lyn Schofield Manager Familial Cancer Registry Cancer in WA 2004 4000 3500 ASPR, rate per 100,000 3000 2500 2000 1500 1000 Male incidence Female incidence Male mortality Female
FAMILIAL COLORECTAL CANCER Lyn Schofield Manager Familial Cancer Registry Cancer in WA 2004 4000 3500 ASPR, rate per 100,000 3000 2500 2000 1500 1000 Male incidence Female incidence Male mortality Female
Is Colonoscopy Necessary in Children Suspected of Having Colonic Polyps?
 Gut and Liver, Vol. 4, No. 3, September 2010, pp. 326-331 original article Is Colonoscopy Necessary in Children Suspected of Having Colonic Polyps? Hye Jin Lee, Ji Hyuk Lee, Jong Seung Lee, and Yon Ho
Gut and Liver, Vol. 4, No. 3, September 2010, pp. 326-331 original article Is Colonoscopy Necessary in Children Suspected of Having Colonic Polyps? Hye Jin Lee, Ji Hyuk Lee, Jong Seung Lee, and Yon Ho
Screening & Surveillance Guidelines
 Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Hans F. A. Vasen, Ian Tomlinson and Antoni Castells
 Clinical management of hereditary colorectal cancer syndromes Hans F. A. Vasen, Ian Tomlinson and Antoni Castells REVIEWS Abstract Hereditary factors are involved in the development of a substantial proportion
Clinical management of hereditary colorectal cancer syndromes Hans F. A. Vasen, Ian Tomlinson and Antoni Castells REVIEWS Abstract Hereditary factors are involved in the development of a substantial proportion
Prevention of Bowel Cancer: which patients do I send for colonoscopy?
 Prevention of Bowel Cancer: which patients do I send for colonoscopy? Dr Chris Groves Consultant Gastroenterologist and Honorary Senior Lecturer St George s Hospital and Medical School Director, SW London
Prevention of Bowel Cancer: which patients do I send for colonoscopy? Dr Chris Groves Consultant Gastroenterologist and Honorary Senior Lecturer St George s Hospital and Medical School Director, SW London
ACG Clinical Guideline: Colorectal Cancer Screening
 ACG Clinical Guideline: Colorectal Cancer Screening Douglas K. Rex, MD, FACG 1, David A. Johnson, MD, FACG 2, Joseph C. Anderson, MD 3, Phillip S. Schoenfeld, MD, MSEd, MSc (Epi), FACG 4, Carol A. Burke,
ACG Clinical Guideline: Colorectal Cancer Screening Douglas K. Rex, MD, FACG 1, David A. Johnson, MD, FACG 2, Joseph C. Anderson, MD 3, Phillip S. Schoenfeld, MD, MSEd, MSc (Epi), FACG 4, Carol A. Burke,
Inherited colon cancer and other inherited cancer predispositions. Dr Anne De Leener Centre de Génétique Humaine
 14.20-15.00 Inherited colon cancer and other inherited cancer predispositions Dr Anne De Leener Centre de Génétique Humaine INHERITED COLORECTAL CANCER (CRC) Colorectal cancer 5% 1% 10% 84% Sporadic Familial
14.20-15.00 Inherited colon cancer and other inherited cancer predispositions Dr Anne De Leener Centre de Génétique Humaine INHERITED COLORECTAL CANCER (CRC) Colorectal cancer 5% 1% 10% 84% Sporadic Familial
Peutz Jegher's Syndrome (Gastro-intestinal Polyposis) and Its Complications
 and Its Complications") Peutz Jegher's Syndrome (Gastro-intestinal Polyposis) and Its Complications Pages with reference to book, From 154 To 155 Zakiuddin G. Oonwala, Sina Aziz ( Department of Surgery, Dow Medical College and
Peutz Jegher's Syndrome (Gastro-intestinal Polyposis) and Its Complications Pages with reference to book, From 154 To 155 Zakiuddin G. Oonwala, Sina Aziz ( Department of Surgery, Dow Medical College and
ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes
 PRACTICE GUIDELINES nature publishing group 223 CME ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes Sapna Sy nga l, MD, M PH, FAC G 1, 2, 3, R and
PRACTICE GUIDELINES nature publishing group 223 CME ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes Sapna Sy nga l, MD, M PH, FAC G 1, 2, 3, R and
Objectives. Definitions. Colorectal Cancer Screening 5/8/2018. Payam Afshar, MS, MD Kaiser Permanente, San Diego. Colorectal cancer background
 Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Adenomatous Polyposis Syndromes (FAP/AFAP and MAP)
") A Patient s Guide to risk assessment Adenomatous Polyposis Syndromes (FAP/AFAP and MAP) Hereditary Cancer Testing: Is it Right for You? This workbook is designed to help you decide if hereditary cancer
A Patient s Guide to risk assessment Adenomatous Polyposis Syndromes (FAP/AFAP and MAP) Hereditary Cancer Testing: Is it Right for You? This workbook is designed to help you decide if hereditary cancer
FEP Medical Policy Manual
 FEP Medical Policy Manual Effective Date: July 15, 2018 Related Policies: None Genetic Testing for PTEN Hamartoma Tumor Syndrome Description The PTEN hamartoma tumor syndrome (PHTS) includes several syndromes
FEP Medical Policy Manual Effective Date: July 15, 2018 Related Policies: None Genetic Testing for PTEN Hamartoma Tumor Syndrome Description The PTEN hamartoma tumor syndrome (PHTS) includes several syndromes
The Role of the Surgical Pathologist in the Diagnosis of Rare Polyposis Syndromes 1. Lynch Syndrome
 The Role of the Surgical Pathologist in the Diagnosis of Rare Polyposis Syndromes Dr Christophe Rosty. Envoi Pathology and University of Queensland, Brisbane, QLD, Australia. Email: c.rosty@uq.edu.au Presented
The Role of the Surgical Pathologist in the Diagnosis of Rare Polyposis Syndromes Dr Christophe Rosty. Envoi Pathology and University of Queensland, Brisbane, QLD, Australia. Email: c.rosty@uq.edu.au Presented
A Patient s Guide to risk assessment. Hereditary Colorectal Cancer
 A Patient s Guide to risk assessment Hereditary Colorectal Cancer Hereditary Cancer Testing: Is it Right for You? Overview of Syndromes This workbook is designed to help you decide if hereditary cancer
A Patient s Guide to risk assessment Hereditary Colorectal Cancer Hereditary Cancer Testing: Is it Right for You? Overview of Syndromes This workbook is designed to help you decide if hereditary cancer
Colon polyps can be a
 ASSOCIATE EDITOR SUZANNE M. MAHON, DNSc, RN, AOCN, AGN-BC Downloaded on 12 09 2018. Single-user license only. Copyright 2018 by the Oncology Nursing Society. For permission to post online, reprint, adapt,
ASSOCIATE EDITOR SUZANNE M. MAHON, DNSc, RN, AOCN, AGN-BC Downloaded on 12 09 2018. Single-user license only. Copyright 2018 by the Oncology Nursing Society. For permission to post online, reprint, adapt,
Understanding Your Genetic Test Result. Positive for Two Copies of an MYH Mutation
 Understanding Your Genetic Test Result Positive for Two Copies of an MYH Mutation This workbook is designed to help you understand the results of your genetic test and is best reviewed with your healthcare
Understanding Your Genetic Test Result Positive for Two Copies of an MYH Mutation This workbook is designed to help you understand the results of your genetic test and is best reviewed with your healthcare
FREQUENTLY ASKED QUESTIONS
 FREQUENTLY ASKED QUESTIONS What is CRC? CRC (CRC) is cancer of the large intestine (colon), the lower part of the digestive system. Rectal cancer is cancer of the last several inches of the colon. Together,
FREQUENTLY ASKED QUESTIONS What is CRC? CRC (CRC) is cancer of the large intestine (colon), the lower part of the digestive system. Rectal cancer is cancer of the last several inches of the colon. Together,
Joint Session with ACOFP and Cancer Treatment Centers of America (CTCA): Cancer Screening: Consensus & Controversies. Ashish Sangal, M.D.
: Cancer Screening: Consensus & Controversies. Ashish Sangal, M.D.") Joint Session with ACOFP and Cancer Treatment Centers of America (CTCA): Cancer Screening: Consensus & Controversies Ashish Sangal, M.D. Cancer Screening: Consensus & Controversies Ashish Sangal, MD Director,
Joint Session with ACOFP and Cancer Treatment Centers of America (CTCA): Cancer Screening: Consensus & Controversies Ashish Sangal, M.D. Cancer Screening: Consensus & Controversies Ashish Sangal, MD Director,
The Genetics of Familial Polyposis
 The Genetics of Familial Polyposis Thursday, September 24 th 2015 Kara Semotiuk, MS, (C)CGC & Laura Winter, MSc, CGC Genetic Counsellors at the FGICR Familial Polyposis Familial Can run in the family related
The Genetics of Familial Polyposis Thursday, September 24 th 2015 Kara Semotiuk, MS, (C)CGC & Laura Winter, MSc, CGC Genetic Counsellors at the FGICR Familial Polyposis Familial Can run in the family related
PATIENT BROCHURE. 441 Charmany Dr 1 Madison WI, RX Only
 PATIENT BROCHURE 441 Charmany Dr 1 Madison WI, 53719 844-870- 8870 Cologuard colorectal cancer screening test is a registered trademark of Exact Sciences Corporation. Indications for Use Cologuard is intended
PATIENT BROCHURE 441 Charmany Dr 1 Madison WI, 53719 844-870- 8870 Cologuard colorectal cancer screening test is a registered trademark of Exact Sciences Corporation. Indications for Use Cologuard is intended
Resident Seminar Aug 19 th, 2015 Colon: Neoplastic. Scott Rieder Dr. Colquhoun
 Resident Seminar Aug 19 th, 2015 Colon: Neoplastic Scott Rieder Dr. Colquhoun Objectives Medical Expert: 1. The biologic basis of colon neoplasia 2. Colon cancer screening (guidelines and evidence) 3.
Resident Seminar Aug 19 th, 2015 Colon: Neoplastic Scott Rieder Dr. Colquhoun Objectives Medical Expert: 1. The biologic basis of colon neoplasia 2. Colon cancer screening (guidelines and evidence) 3.
Natural History and Epidemiology of Colorectal Cancer
 Natural History and Epidemiology of Colorectal Cancer Prevent Cancer Foundation 2017 Dialogue for Action April 19, 2017 Roy J. Duhé, Ph.D. Associate Director for Cancer Education; Professor of Pharmacology;
Natural History and Epidemiology of Colorectal Cancer Prevent Cancer Foundation 2017 Dialogue for Action April 19, 2017 Roy J. Duhé, Ph.D. Associate Director for Cancer Education; Professor of Pharmacology;
MEDICAL POLICY SUBJECT: GENETIC TESTING FOR INHERITED SUSCEPTIBILITY TO COLORECTAL CANCER. POLICY NUMBER: CATEGORY: Laboratory Test
 MEDICAL POLICY SUBJECT: GENETIC TESTING FOR INHERITED SUSCEPTIBILITY TO COLORECTAL CANCER POLICY NUMBER: 2.02.11 CATEGORY: Laboratory Test EFFECTIVE DATE: 09/16/99 REVISED DATE: 04/19/01, 05/16/02, 06/19/03,
MEDICAL POLICY SUBJECT: GENETIC TESTING FOR INHERITED SUSCEPTIBILITY TO COLORECTAL CANCER POLICY NUMBER: 2.02.11 CATEGORY: Laboratory Test EFFECTIVE DATE: 09/16/99 REVISED DATE: 04/19/01, 05/16/02, 06/19/03,
The real face of juvenile polyposis syndrome
 Case Report The real face of juvenile polyposis syndrome Beatrix Tam 1, Ágnes Salamon 1, Attila Bajtai 2, Annamária Németh 3, János Kiss 4, László Simon 4, Tamás Molnár 5 1 Department of Gastroenterology,
Case Report The real face of juvenile polyposis syndrome Beatrix Tam 1, Ágnes Salamon 1, Attila Bajtai 2, Annamária Németh 3, János Kiss 4, László Simon 4, Tamás Molnár 5 1 Department of Gastroenterology,
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
EARLY DETECTION OF COLORECTAL CANCER. Epidemiology of CRC
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
FAMILIAL ADENOMATOUS POLYPOSIS (COLORECTAL CANCER) PREFERRED MODEL OF CARE AND CRITERIA FOR REFERENCE CENTRES
 PREFERRED MODEL OF CARE AND CRITERIA FOR REFERENCE CENTRES") FAMILIAL ADENOMATOUS POLYPOSIS (COLORECTAL CANCER) PREFERRED MODEL OF CARE AND CRITERIA FOR REFERENCE CENTRES Coordinator: Alex Kartheuser (Colorectal Surgery, Cliniques universitaires St-Luc, UCL) Authors
FAMILIAL ADENOMATOUS POLYPOSIS (COLORECTAL CANCER) PREFERRED MODEL OF CARE AND CRITERIA FOR REFERENCE CENTRES Coordinator: Alex Kartheuser (Colorectal Surgery, Cliniques universitaires St-Luc, UCL) Authors
Result Navigator. Positive Test Result: PTEN. After a positive test result, there can be many questions about what to do next. Navigate Your Results
 Result Navigator Positive Test Result: PTEN Positive test results identify a change, or misspelling, of DNA that is known or predicted to cause an increased risk for cancer. DNA is the blueprint of life
Result Navigator Positive Test Result: PTEN Positive test results identify a change, or misspelling, of DNA that is known or predicted to cause an increased risk for cancer. DNA is the blueprint of life
Mr Chris Wakeman. General Surgeon University of Otago, Christchurch. 12:15-12:40 Management of Colorectal Cancer
 Mr Chris Wakeman General Surgeon University of Otago, Christchurch 12:15-12:40 Management of Colorectal Cancer Bowel cancer Chris Wakeman Colorectal Surgeon Christchurch Sam Simon (Simpsons) Elizabeth
Mr Chris Wakeman General Surgeon University of Otago, Christchurch 12:15-12:40 Management of Colorectal Cancer Bowel cancer Chris Wakeman Colorectal Surgeon Christchurch Sam Simon (Simpsons) Elizabeth
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
DIGESTIVE SYSTEM SURGICAL PROCEDURES May 1, 2015 INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 Asst Surg Anae") ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
JOURNAL OF CASE REPORTS 2014;4(2):
:") JOURNAL OF CASE REPORTS 2014;4(2):395-399 Juvenile Polyposis Syndrome -Two Case Reports Samuel Essoun 1, Jonathan CB Dakubo 2, Antoinette A Bediako-Bowan 2 From the Department of Surgery, 1 Korle Bu Teaching
JOURNAL OF CASE REPORTS 2014;4(2):395-399 Juvenile Polyposis Syndrome -Two Case Reports Samuel Essoun 1, Jonathan CB Dakubo 2, Antoinette A Bediako-Bowan 2 From the Department of Surgery, 1 Korle Bu Teaching
Rare presentation of Recurrent Multiple Intussusceptions in a case of Post Total Colectomy for Peutz-Jeghers Polyposis
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 14, Issue 3 Ver. VIII (Mar. 2015), PP 06-10 www.iosrjournals.org Rare presentation of Recurrent Multiple
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 14, Issue 3 Ver. VIII (Mar. 2015), PP 06-10 www.iosrjournals.org Rare presentation of Recurrent Multiple
Result Navigator. Positive Test Result: BMPR1A. After a positive test result, there can be many questions about what to do next. Navigate Your Results
 Result Navigator Positive Test Result: BMPR1A Positive test results identify a change, or misspelling, of DNA that is known or predicted to cause an increased risk for cancer. DNA is the blueprint of life
Result Navigator Positive Test Result: BMPR1A Positive test results identify a change, or misspelling, of DNA that is known or predicted to cause an increased risk for cancer. DNA is the blueprint of life
SCREENING FOR BOWEL CANCER USING FLEXIBLE SIGMOIDOSCOPY REVIEW APPRAISAL CRITERIA FOR THE UK NATIONAL SCREENING COMMITTEE
 SCREENING FOR BOWEL CANCER USING FLEXIBLE SIGMOIDOSCOPY REVIEW APPRAISAL CRITERIA FOR THE UK NATIONAL SCREENING COMMITTEE The Condition 1. The condition should be an important health problem Colorectal
SCREENING FOR BOWEL CANCER USING FLEXIBLE SIGMOIDOSCOPY REVIEW APPRAISAL CRITERIA FOR THE UK NATIONAL SCREENING COMMITTEE The Condition 1. The condition should be an important health problem Colorectal
Colorectal Cancer in 2006: New Developments
 James J. Stark, MD Colorectal Cancer in 2006: New Developments Melissa Bennett, MS, CGC Myriad Genetic Laboratories Thomas Duntemann,, MD Ray Ramirez, Jr., MD Hereditary Colon Cancer and Genetic Testing
James J. Stark, MD Colorectal Cancer in 2006: New Developments Melissa Bennett, MS, CGC Myriad Genetic Laboratories Thomas Duntemann,, MD Ray Ramirez, Jr., MD Hereditary Colon Cancer and Genetic Testing
Improving Access to Endoscopy at Safety-Net Hospitals. Lukejohn W. Day MD Assistant Professor of Medicine
 Improving Access to Endoscopy at Safety-Net Hospitals Lukejohn W. Day MD Assistant Professor of Medicine Goals Background Improving Access to Endoscopic Care Electronic referral: ereferral Direct Access
Improving Access to Endoscopy at Safety-Net Hospitals Lukejohn W. Day MD Assistant Professor of Medicine Goals Background Improving Access to Endoscopic Care Electronic referral: ereferral Direct Access
Accepted Manuscript. Utility of Genetic Testing in Persons with Multiple Colorectal Polyps. Natalia Khalaf, MD, MPH, Niloy Jewel Samadder, MD, MS
 Accepted Manuscript Utility of Genetic Testing in Persons with Multiple Colorectal Polyps Natalia Khalaf, MD, MPH, Niloy Jewel Samadder, MD, MS PII: S1542-3565(19)30259-9 DOI: https://doi.org/10.1016/j.cgh.2019.03.007
Accepted Manuscript Utility of Genetic Testing in Persons with Multiple Colorectal Polyps Natalia Khalaf, MD, MPH, Niloy Jewel Samadder, MD, MS PII: S1542-3565(19)30259-9 DOI: https://doi.org/10.1016/j.cgh.2019.03.007
Bowel obstruction and tumors
 Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Genetic/Familial High-Risk Assessment: Colorectal
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Genetic/Familial High-Risk Assessment: Colorectal Version 1.2014 NCCN.org Continue Panel Members Genetic/Familial High-Risk Assessment:
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Genetic/Familial High-Risk Assessment: Colorectal Version 1.2014 NCCN.org Continue Panel Members Genetic/Familial High-Risk Assessment:
Adenoma to Carcinoma Pathway
 It is widely accepted that more than 95% of colorectal cancers arise from adenomatous polyps, which are generally defined as benign lesions with dysplastic epithelium that have variable potential for malignancy.
It is widely accepted that more than 95% of colorectal cancers arise from adenomatous polyps, which are generally defined as benign lesions with dysplastic epithelium that have variable potential for malignancy.
Hamartomatous Polyps A Clinical and Molecular Genetic Study
 PHD THESIS DANISH MEDICAL JOURNAL Hamartomatous Polyps A Clinical and Molecular Genetic Study Anne Marie Jelsig This review has been accepted as a thesis together with six original papers by the University
PHD THESIS DANISH MEDICAL JOURNAL Hamartomatous Polyps A Clinical and Molecular Genetic Study Anne Marie Jelsig This review has been accepted as a thesis together with six original papers by the University
CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING
 CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING This guideline is designed to assist practitioners by providing the framework for colorectal cancer (CRC) screening, and is not intended to replace
CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING This guideline is designed to assist practitioners by providing the framework for colorectal cancer (CRC) screening, and is not intended to replace
Hereditary Colorectal Cancer
 A Patient s Guide to risk assessment Hereditary Colorectal Cancer Hereditary Cancer Testing: Is it Right for You? This workbook is designed to help you decide if hereditary cancer testing is right for
A Patient s Guide to risk assessment Hereditary Colorectal Cancer Hereditary Cancer Testing: Is it Right for You? This workbook is designed to help you decide if hereditary cancer testing is right for
Yes when meets criteria below. Dean Health Plan covers when Medicare also covers the benefit.
 Genetic Testing for Lynch Syndrome MP9487 Covered Service: Prior Authorization Required: Additional Information: Yes when meets criteria below Yes-as shown below Pre and post test genetic counseling is
Genetic Testing for Lynch Syndrome MP9487 Covered Service: Prior Authorization Required: Additional Information: Yes when meets criteria below Yes-as shown below Pre and post test genetic counseling is