Adenoma to Carcinoma Pathway
|
|
|
- Sarah Freeman
- 5 years ago
- Views:
Transcription
1


2
3 It is widely accepted that more than 95% of colorectal cancers arise from adenomatous polyps, which are generally defined as benign lesions with dysplastic epithelium that have variable potential for malignancy. This adenoma-carcinoma sequel can take many years to fully manifest after a stepwise accumulation of genetic alterations and appear benign endoscopically but poses a difficult and often controversial clinical scenario. (Aarons et al; World J Gastroenterol.2014) The probability of carcinoma is related to: 1. The size of the polyp. 2. The relative proportion of its villous features. 3. The presence of significant dysplasia in cells.



4 Adenoma to Carcinoma Pathway Normal Adenoma Cancer APC loss K-ras mutation Chrom 18 loss p53 loss Normal Epithelium Hyperproliferation Early Adenoma Intermediate Adenoma Late Adenoma Cancer
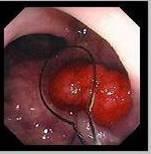
5 Emphasis should be focused on the endoscopic assessment. As Colonoscopy is the diagnostic procedure of choice for: *- accurate detection of polyps of all sizes *- Allows immediate biopsy or polypectomy. Most polyps found during colonoscopy can be completely and safely resected. Scientific studies now conclusively show that resecting adenomatous polyps prevents colorectal cancer. (Bond. AJG; 2000) (Aarons et al; World J Gastroenterol.2014)

6

7

8



9 Type Ip: Pedunculated polyp


10 Type Isp: Semiedunculated polyp

")
11 Type Is: Sessile polyp (Is)



12 Type IIa: Slightly elevated lesions




13


14 Type IIb: Flat lesions


15 Type IIc: Slightly depressed lesions

16 Singh et al; Journal of Clinical and Diagnostic Research. 2015
17 NICE Classification for D.D. of polyps NBI International Colorectal Endoscopic classification is based on narrow-band images of colon polyps using staining, vascular patterns, and surface patterns to distinguish between polyps. Although it is linked to the Olympus company s endoscopes, similar differential-diagnostic approaches have also been reported for devices manufactured by other companies. Clinically, the classification is used for small polyps (< 5 mm or < 10 mm). (Ladabaum et al; Gastroenterol ) (Schachschal et al; Gut. 2014)




18 Type I CHARACTERISTIC FOR HYPERPLASTIC POLYP Color Lighter than or similar to the surroundings Vessels Surface pattern small vessels or a sparse network, with no recognizable pattern circular pattern with small dots pattern with a darker area in the center, surrounded by lighter mucosa




19 Type II CHARACTERISTIC FOR ADENOMATOUS POLYP Color Darker (browner) than the surroundings Vessels A Lighter area in the center, surrounded by thicker brown vessls Surface pattern Oval, tubular, gyrate presence of tubuli, linear or bundled, with light area in center


20 Type III CHARACTERISTIC FOR MALIGNANT POLYP Color Vessels Darker than the surroundings brownish, sometimes with lighter patches areas with interrupted or absent vessels Surface pattern amorphous or no surface pattern
21
22
23




24 Hyperplastic serrated polyp



25
26

27
28
29
30
31 Surveillance and Treatment Endoscopic examination of the colon and upper gastrointestinal tract is recommended every two to three years in patients with JP. In patients with polyps, endoscopic screening should be performed yearly, until the patient is polyp free. Patients with mild polyposis can be managed by frequent endoscopic examinations and polypectomy, Brosens et al; Current Molecular Medicine, 2007
32
33
34
35
36

37
38 Brosens et al; Current Molecular Medicine, 2007

39 Familial polyposis coli (FPC)
 Genetic defect of Adenomatous polyposis coli (APC). APC gene located on the long arm of chromosome 5 (5q21).")

40 Familial Polyposis Syndrome genetic tendencies to develop neoplastic polyps. Familial polyposis coli (FPC) Genetic defect of Adenomatous polyposis coli (APC). APC gene located on the long arm of chromosome 5 (5q21). APC gene is a tumor suppressor gene Innumerable neoplastic polyps in the colon (500 to 2500) Polyps are also found elsewhere in alimentary tract Most polyps are tubular adenomas The risk of colorectal cancer is 100% by midlife. Gardener s syndrome Polyposis coli, multiple osteomas, epidermal cysts, and fibromatosis. Turcot syndrome Polyposis coli, glioma and fibromatosis
41
42

43 Haggitt et al; Gastroenterology 1985

44 Kudo et al; Endoscopy 1993, and Kikuchi et al;. Dis Colon Rectum 1995


45 Colorectal polyps can be diagnosed by endoscopy or barium radiography. When there is an indication to examine the entire large bowel, colonoscopy is the diagnostic procedure of choice. It is the most accurate method of detecting polyps of all sizes and it allows immediate biopsy or polypectomy. Most polyps found during colonoscopy can be completely and safely resected. Scientific studies now conclusively show that resecting adenomatous polyps prevents colorectal cancer. (Bond. AJG; 2000)
46 The role of the radiologist in the diagnosis and evaluation of intestinal polyposis syndromes cannot be overemphasized, as missed polyps are potentially missed cancers. For polyps larger than 1 cm, the sensitivity of single- and double-contrast barium enema (DCBE) examination is 90-95%. DCBE is more sensitive in the detection of polyps smaller than 1 cm.


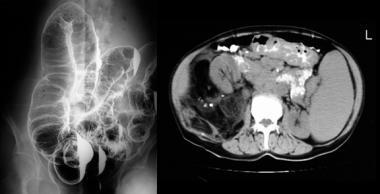
47
48 CT and MR colonography allow an analysis in both the cross-sectional and virtual endoscopic formats. both offer the capability of imaging extra-intestinal disease associated with many of the colon polyposis syndromes. MR colonography shares several limitations with its CT counterpart. Inadequate colon distention, contrast opacification, and the presence of air bubbles and fecal masses may potentially cause problems in interpretation. None of the above techniques are useful in differentiating hamartomatous polyps from adenomatous polyps.


49 Conventional colonoscopy is a little bit ahead in front of virtual colonoscopy, yet the results are more or less comparable to each other.
50 The main critics of virtual colonoscopy were: It cannot detect small polyps with enough certainty. Methodologically it cannot detect small flat adenomas. It is incapable of obtaining information about the etiology even when a small polyp is detected, patients must undergo flexible endoscopy with biopsy anyway. It does not depict early inflammatory changes or allow recognition of small ulcerations, since the surface is artificial and includes no information about the mucosa. It fails to provide information on movement or motility. Mucus and stool residues cannot be removed during the examination. It goes hand in hand with ionizing radiation. It necessitates interpretation of large amount of data; thus consuming lot of time and effort.
51 Supporters of virtual colonoscopy for the following points:- It can be implemented simply and reliably. It boasts high patient acceptance, since the complete examination lasts only a few minutes. It is much less painful, since the mechanical manipulation is limited. It requires no sedation, eliminating the associated risks. It bears no noteworthy risk of perforation (flexible diagnostic endoscopy: 1:1000 1:5000). It is cheaper than flexible endoscopy in various western countries. It does not only offer to see the bowels from within, but also complete abdominal assessment with the possibility of detecting side findings; staging can be accomplished simultaneously. It can accurately detect the exact site of the colonic lesion. It is a high technology examination and expected to improvements in the near future. Virtual colonoscopy has the advantage of assessment of the colon proximal to occlusive stenotic lesions, which is not available in several cases in conventional colonoscopy. The used low dose techniques in virtual colonoscopy decline the hazards of ionizing radiation. With advance of medical systems and experience the data analysis time is 10 min. The clinical significance of small polyps is doubtful. Also the gold standard, i.e. flexible endoscopy, has a 27% margin of error for polyps smaller than 5 mm. Furthermore several centers are reporting excellent virtual colonoscopy sensitivity for smaller polyps. Flat adenomas are very rare tumors and relatively more prevalent in Japan. They are also difficult to recognize in flexible endoscopy, and special techniques are necessary.
52 CT colonography has high specificity but hetrogenous sensitivity. In most cases it is not as sensitive as conventional colonoscopy, therefore be useful as a screening test for high risk patients.

53 CT colonography has higher sensitivity than conventional colonoscopy for detection of colorectal carcinoma, including its ability to detect abnormalities proximal to obstructing lesion, accurate segmental localization of lesions and staging. However, some limitations of CT colonography were difficulty in detection of flat lesions and lack of information about hyperemia and superficial mucosal erosion.

54

55

56
.. Larger polyps between 1.5 and 3.")
 or endoscopic submucosal dissection (ESD),")
57 Approximately 80%-90% of adenomas are less than 1 cm (polyps 5 mm have negligible risk of malignancy) therefore amenable to standard endoscopic removal with conventional snare (especially pedunculated polyps).. Larger polyps between 1.5 and 3.5 cm have higher malignant potential (19%-43%) and should be approached with more caution. It is more challenging and require more advanced techniques, such as endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD), which are being used with increasing frequency in specialized centers. (Aarons et al; World J Gastroenterol.2014)






58

59
60 Polypectomy resection margin: The requisite margin is a matter of much debate due to the risk of luminal recurrence. This ranges from 0% to 2% in malignant polyps with a margin of resection greater than 1 mm. However, when the resection margin is involved, or < 1 mm, the percentage of relapse ranges between 21% and 33%. Subsequently, many authors believe that a resection margin of 2 mm is ideal (Butte et al; Dis Colon Rectum 2012)



61




62




63

64



65

66 EMR is a safe and effective treatment for large difficult polyps with an overall complication rate of 7%. It avoided surgery in 93% of cases with substantial cost savings. EMR of large and difficult benign polyps should be the new standard of care.
67 Despite limitations of the study as limited number of patients, single endoscopist, retrospective design, and short term followup, however, we suggest that when faced with a lesion that is nonlifting due to a prior intervention, it may be reasonable to proceed with endoscopic treatment if the patient is adequately informed of the risks, and the endoscopic team is sufficiently experienced

68
69 For smaller lesions, mucosal resection (EMR) is very promising, potentially sparing patients an open or laparoscopic surgery. For larger lesions, submucosal dissection [ESD] may provide a similar opportunity. Neither EMR nor ESD preclude subsequent surgical resection if required. For many polyps the endoscopic approach can be curative, tend to reduce cost, lower the observed adverse event rate and, most importantly, spare patients a significant surgery and partial colectomy,
, surgical resection remains prevalent despite limited outcomes data.")
70 Although endoscopic resection is a safe and effective treatment for benign complex colorectal polyps ('complex polyps'), surgical resection remains prevalent despite limited outcomes data.








71


72
73

74

75
76

77 Lowenfeld et al; Seminar in colon and rectal surgery; 2017
78 Surgical Treatment Colorectal Disease ª (Suppl. 1), 61 66
79 There is general agreement that patients with FAP should undergo prophylactic colectomy. The surgical options include total colectomy with ileo-rectal anastomosis (IRA) and restorative proctocolectomy (RPC) with an ileo-pouch anal anastomosis (IAA). There are no guidelines for the timing of surgery. Considering that the risk of cancer becomes clinically significant after years of age and increases over time [4,5], surgery is usually planned after the legal age, unless large polyps or severe dysplasia are found before that time. Urso et al; Colorectal Disease.2014

80

81

82
83 Laparoscopic approach Advantages of safety, trauma reduction, improved short-term outcome, less intraoperative blood loss, less postoperative pain, a reduced incidence of small bowel obstruction and incisional hernia formation, and shorter hospital stay. In addition, the cosmetic benefits are relevant in this young population. Another question is the development of desmoid tumours after surgery. Moreover, the advantages of minimally invasive surgery is supported by fast-track rehabilitation. Some surgeons advocate a hand-assisted techniques using a hand port with shorter learning curve because some maneuvers are similar to those used in open surgery. The first single-incision laparoscopic restorative proctocolectomy was reported in 2010, and later studies showed that this can be safely performed with short-term results comparable to conventional laparoscopy with a significant reduction in the operation time and blood loss. Urso et al; Colorectal Disease.2014
84 CONCLUSION Laparoscopic colectomy for endoscopic nonresectable colonic polyps is generally a safe procedure associated with a low rate of conversions and complications. The incidence of malignancy documented on final pathology may be high and cannot be ruled out before surgery. Results emphasize the fact that colonic lesions with benign pathology that have an endoscopic benign polypoid appearance may also harbor an invasive cancer. This is a major consideration when operating on these patients, mandating strict adherence to surgical oncological principles with adequate lymph node harvesting and wound precautions. Surgeons experienced with laparoscopy for colorectal cancer should be involved in these procedures.

85

86

87
88 Colonoscopy is a complex task, meticulously done by expert or at least under his supervision. Done with good preparation, high resolution facilities, and the colon is thoroughly inspected during scope retrieval All tactics must be practiced during endoscopy as NBI imaging, cap-assisted colonoscopy (CAC), retroflexion, magnifying techniques, chromoendoscopy, tattooing and marking lesions, and different biopsy techniques Effort must be done for possibility of treatment if feasible But gastroenterologists and endoscopist : please consult GIT surgeons specially in challenging and debatable situations: * Big polyp * Flat non-lifted polyps * Large number, disseminated * recurrent polyps * Complication, or suspected complications


89
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Colon Polyps: Detection, Inspection and Characteristics
 Colon Polyps: Detection, Inspection and Characteristics Stephen Kim, M.D. Assistant Professor of Medicine Interventional Endoscopy Services UCLA Division of Digestive Diseases September 29, 2018 1 Disclosures
Colon Polyps: Detection, Inspection and Characteristics Stephen Kim, M.D. Assistant Professor of Medicine Interventional Endoscopy Services UCLA Division of Digestive Diseases September 29, 2018 1 Disclosures
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
Screening & Surveillance Guidelines
 Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Emerging Interventions in Endoscopy. Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital
 Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
Advanced techniques for resection of large polyps. John G. Lee, MD February 2, 2018
 Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
Endoscopic Corner CASE 1. Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R
 170 Endoscopic Corner Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R CASE 1 A 54-year-old woman underwent a colorectal cancer screening. Her fecal immunochemical test was positive.
170 Endoscopic Corner Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R CASE 1 A 54-year-old woman underwent a colorectal cancer screening. Her fecal immunochemical test was positive.
Gastric Polyps. Bible class
 Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci. Colon polyps. Colorectal cancer
 Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Do any benign polyps require an operation?
 Do any benign polyps require an operation? Kevin Waschke MD.,CM., FRCPC, FASGE McGill University Health Center President Elect Canadian Association of Gastroenterology Colonoscopy Education Day - Tuesday
Do any benign polyps require an operation? Kevin Waschke MD.,CM., FRCPC, FASGE McGill University Health Center President Elect Canadian Association of Gastroenterology Colonoscopy Education Day - Tuesday
THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD
 SNARE THE CASE FOR EMR AND ESD") THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD Surgical Oncology Network meeting Dr. Eric Lam MD FRCPC October 14, 2017 DISCLOSURES None OBJECTIVES Appreciate
THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD Surgical Oncology Network meeting Dr. Eric Lam MD FRCPC October 14, 2017 DISCLOSURES None OBJECTIVES Appreciate
The Paris classification of colonic lesions
 The Paris classification of colonic lesions Training to improve the interobserver agreement among international experts Sascha van Doorn, MD, PhD-student in CRC-reserach group of Evelien Dekker Introduction
The Paris classification of colonic lesions Training to improve the interobserver agreement among international experts Sascha van Doorn, MD, PhD-student in CRC-reserach group of Evelien Dekker Introduction
GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS. Family Health Clinical Genetics. Clinical Genetics department
 GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS Full Title of Guideline: Author (include email and role): Division & Speciality: GUIDELINES FOR THE GENETIC MANAGEMENT OF A FAMILY
GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS Full Title of Guideline: Author (include email and role): Division & Speciality: GUIDELINES FOR THE GENETIC MANAGEMENT OF A FAMILY
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Colorectal cancer: colonoscopic surveillance for prevention of colorectal cancer in patients with ulcerative colitis, Crohn
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Colorectal cancer: colonoscopic surveillance for prevention of colorectal cancer in patients with ulcerative colitis, Crohn
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Management of pt1 polyps. Maria Pellise
 Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Colon Cancer Screening & Surveillance. Amit Patel, MD PGY-4 GI Fellow
 Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
EARLY DETECTION OF COLORECTAL CANCER. Epidemiology of CRC
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Large polyps: EMR, ESD, TEM and segmental resection. Terry Phang 2017 SON fall update
 Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
Colon Screening in 2014 Offering Patients a Choice. Clark A Harrison MD The Nevada Colon Cancer Partnership
 Colon Screening in 2014 Offering Patients a Choice Clark A Harrison MD The Nevada Colon Cancer Partnership Objectives 1. Understand the incidence and mortality rates for CRC in the US. 2. Understand risk
Colon Screening in 2014 Offering Patients a Choice Clark A Harrison MD The Nevada Colon Cancer Partnership Objectives 1. Understand the incidence and mortality rates for CRC in the US. 2. Understand risk
Pathology reports, related operative reports and consult letters must be provided with a request for assessment.
 Page 1 of 6 Polyposis Syndromes Inherited risk for colorectal cancer is associated with a number of polyposis syndromes (genes), some of which are well-defined and others are less common. Identification
Page 1 of 6 Polyposis Syndromes Inherited risk for colorectal cancer is associated with a number of polyposis syndromes (genes), some of which are well-defined and others are less common. Identification
Familial Adenomatous Polyposis
 Familial Adenomatous Polyposis 1 in 10,000 incidence 100 s to 1000 s of colonic adenomas by teens Cancer risk: colon, gastric, duodenum (periampulla), small bowel, pancreas, papillary thyroid, childhood
Familial Adenomatous Polyposis 1 in 10,000 incidence 100 s to 1000 s of colonic adenomas by teens Cancer risk: colon, gastric, duodenum (periampulla), small bowel, pancreas, papillary thyroid, childhood
Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer
 SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer Author : SAGES Webmaster PREAMBLE The following
SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer Author : SAGES Webmaster PREAMBLE The following
DIGESTIVE SYSTEM SURGICAL PROCEDURES May 1, 2015 INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 Asst Surg Anae") ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
This is the portion of the intestine which lies between the small intestine and the outlet (Anus).
.") THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
Paris classification (2003) 삼성의료원내과이준행
 삼성의료원내과이준행") Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis
 Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis Bret A. Lashner, M.D. Professor of Medicine Director,
Chromoendoscopy or Narrow Band Imaging with Targeted biopsies Should be the Cancer Surveillance Endoscopy Procedure of Choice in Ulcerative Colitis Bret A. Lashner, M.D. Professor of Medicine Director,
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia
 Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Predict, Resect and discard : Yes we can! (at least in some hands)
") Diminutive polyps : Real time endoscopic histology Predict, Resect and discard : Yes we can! (at least in some hands) Robert Benamouzig Hôpital Avicenne AP-HP & Paris 13 University France Why it is important?
Diminutive polyps : Real time endoscopic histology Predict, Resect and discard : Yes we can! (at least in some hands) Robert Benamouzig Hôpital Avicenne AP-HP & Paris 13 University France Why it is important?
Colorectal Neoplasia. Dr. Smita Devani MBChB, MRCP. Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi
 Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
EMR, ESD and Beyond. Peter Draganov MD. Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida
 EMR, ESD and Beyond Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated by Endoscopy
EMR, ESD and Beyond Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated by Endoscopy
Endoscopic techniques for surveillance and treatment of FAP
 Endoscopic techniques for surveillance and treatment of FAP Evelien Dekker MD PhD Department of Gastroenterology & Hepatology Academic Medical Center Amsterdam The Netherlands FAP: endoscopic surveillance
Endoscopic techniques for surveillance and treatment of FAP Evelien Dekker MD PhD Department of Gastroenterology & Hepatology Academic Medical Center Amsterdam The Netherlands FAP: endoscopic surveillance
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
Dysplasia 4/19/2017. How do I practice Chromoendoscopy for Surveillance of Colitis? SCENIC: Polypoid Dysplasia in UC. Background
 SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
Citation for published version (APA): Bartels, S. A. L. (2013). Laparoscopic colorectal surgery: beyond the short-term effects
: Bartels, S. A. L. (2013). Laparoscopic colorectal surgery: beyond the short-term effects") UvA-DARE (Digital Academic Repository) Laparoscopic colorectal surgery: beyond the short-term effects Bartels, S.A.L. Link to publication Citation for published version (APA): Bartels, S. A. L. (2013).
UvA-DARE (Digital Academic Repository) Laparoscopic colorectal surgery: beyond the short-term effects Bartels, S.A.L. Link to publication Citation for published version (APA): Bartels, S. A. L. (2013).
COLON: Innovations 3 steps, 3 parts..
 COLON: Innovations 3 steps, 3 parts.. Detection: I see an abnormality (usually a polyp) Characterization: Is this abnormality neoplastic? (for example: an adenoma) Treatment: it is neoplastic. Can I treat
COLON: Innovations 3 steps, 3 parts.. Detection: I see an abnormality (usually a polyp) Characterization: Is this abnormality neoplastic? (for example: an adenoma) Treatment: it is neoplastic. Can I treat
How to characterize dysplastic lesions in IBD?
 How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
Structured Follow-Up after Colorectal Cancer Resection: Overrated. R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007
 Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions
 Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions Digestive Disease Center, Showa University Northern Yokohama Hospital Department of Pathology Yoshiki Wada, Shin-ei Kudo, Hiroshi
Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions Digestive Disease Center, Showa University Northern Yokohama Hospital Department of Pathology Yoshiki Wada, Shin-ei Kudo, Hiroshi
Endoscopic Submucosal Dissection ESD
 Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Difficult Polypectomy 2015 Tool of the Trade
 Difficult Polypectomy 2015 Tool of the Trade Jonathan Cohen, MD FACG FASGE Clinical Professor of Medicine NYU Langone School of Medicine Improving Therapeutics in the Colon Improved detection of polyp
Difficult Polypectomy 2015 Tool of the Trade Jonathan Cohen, MD FACG FASGE Clinical Professor of Medicine NYU Langone School of Medicine Improving Therapeutics in the Colon Improved detection of polyp
CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING
 CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING This guideline is designed to assist practitioners by providing the framework for colorectal cancer (CRC) screening, and is not intended to replace
CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING This guideline is designed to assist practitioners by providing the framework for colorectal cancer (CRC) screening, and is not intended to replace
When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool
 When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool Adenomas/Carcinoma Sequence Providing Time for Screening Normal 5-20 yrs 5-15 yrs
When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool Adenomas/Carcinoma Sequence Providing Time for Screening Normal 5-20 yrs 5-15 yrs
Colorectal Cancer Screening
 Scan for mobile link. Colorectal Cancer Screening What is colorectal cancer screening? Screening examinations are tests performed to identify disease in individuals who lack any signs or symptoms. The
Scan for mobile link. Colorectal Cancer Screening What is colorectal cancer screening? Screening examinations are tests performed to identify disease in individuals who lack any signs or symptoms. The
removal of adenomatous polyps detects important effectively as follow-up colonoscopy after both constitute a low-risk Patients with 1 or 2
 Supplementary Table 1. Study Characteristics Author, yr Design Winawer et al., 6 1993 National Polyp Study Jorgensen et al., 9 1995 Funen Adenoma Follow-up Study USA Multi-center, RCT for timing of surveillance
Supplementary Table 1. Study Characteristics Author, yr Design Winawer et al., 6 1993 National Polyp Study Jorgensen et al., 9 1995 Funen Adenoma Follow-up Study USA Multi-center, RCT for timing of surveillance
Research Article Endoscopic Management of Nonlifting Colon Polyps
 Diagnostic and Therapeutic Endoscopy Volume 2013, Article ID 412936, 5 pages http://dx.doi.org/10.1155/2013/412936 Research Article Endoscopic Management of Nonlifting Colon Polyps Shai Friedland, 1,2
Diagnostic and Therapeutic Endoscopy Volume 2013, Article ID 412936, 5 pages http://dx.doi.org/10.1155/2013/412936 Research Article Endoscopic Management of Nonlifting Colon Polyps Shai Friedland, 1,2
The Usefulness Of Narrow Band Imaging Endoscopy For The Real Time Characterization Of Colonic Lesions
 Acta Medica Marisiensis 2016;62(2):182-186 DOI: 10.1515/amma-2016-0004 RESEARCH ARTICLE The Usefulness Of Narrow Band Imaging Endoscopy For The Real Time Characterization Of Colonic Lesions Boeriu Alina
Acta Medica Marisiensis 2016;62(2):182-186 DOI: 10.1515/amma-2016-0004 RESEARCH ARTICLE The Usefulness Of Narrow Band Imaging Endoscopy For The Real Time Characterization Of Colonic Lesions Boeriu Alina
Resident Seminar Aug 19 th, 2015 Colon: Neoplastic. Scott Rieder Dr. Colquhoun
 Resident Seminar Aug 19 th, 2015 Colon: Neoplastic Scott Rieder Dr. Colquhoun Objectives Medical Expert: 1. The biologic basis of colon neoplasia 2. Colon cancer screening (guidelines and evidence) 3.
Resident Seminar Aug 19 th, 2015 Colon: Neoplastic Scott Rieder Dr. Colquhoun Objectives Medical Expert: 1. The biologic basis of colon neoplasia 2. Colon cancer screening (guidelines and evidence) 3.
Hyperplastische Polyps Innocent bystanders?
 Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Aberrant crypt foci, chromocolonoscopy for, 539 540 Absorptive stains, for chromocolonoscopy, 522 524 Accessories, for colonoscopy, 680 684
Note: Page numbers of article titles are in boldface type. A Aberrant crypt foci, chromocolonoscopy for, 539 540 Absorptive stains, for chromocolonoscopy, 522 524 Accessories, for colonoscopy, 680 684
Classification of polyposis syndromes two major groups. Adenomatous polyposis syndromes. Hamartomatous polyposis syndromes
 Hereditary polyposis syndromes Classification of polyposis syndromes two major groups adenomatous and non-adenomatous polyposis syndromes Adenomatous polyposis syndromes Familial adenomatous polyposis(fap)
Hereditary polyposis syndromes Classification of polyposis syndromes two major groups adenomatous and non-adenomatous polyposis syndromes Adenomatous polyposis syndromes Familial adenomatous polyposis(fap)
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population
 Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
Pathology in Slovenian CRC screening programme:
 Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
Expert panel observations
 Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer
 Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
GI Coding Updates. Rhonda Buckholtz, CPC, CPCI, CPMS, CRC, CDEO, CHPSE, CGSC, COBGC, CENTC, CPEDC
 GI Coding Updates Rhonda Buckholtz, CPC, CPCI, CPMS, CRC, CDEO, CHPSE, CGSC, COBGC, CENTC, CPEDC Copyright/Disclaimer 2014 AAPC text CPT copyright 2016 American Medical Association. All rights reserved.
GI Coding Updates Rhonda Buckholtz, CPC, CPCI, CPMS, CRC, CDEO, CHPSE, CGSC, COBGC, CENTC, CPEDC Copyright/Disclaimer 2014 AAPC text CPT copyright 2016 American Medical Association. All rights reserved.
LIST OF ABBREVIATIONS
 Gastroenter oenterology 2005 Royal College of Physicians of Edinburgh Screening and surveillance for upper and lower gastrointestinal cancer JN Plevris Consultant Gastroenterologist and Honorary Senior
Gastroenter oenterology 2005 Royal College of Physicians of Edinburgh Screening and surveillance for upper and lower gastrointestinal cancer JN Plevris Consultant Gastroenterologist and Honorary Senior
Summary. Cezary ŁozińskiABDF, Witold KyclerABCDEF. Rep Pract Oncol Radiother, 2007; 12(4):
:") Rep Pract Oncol Radiother, 2007; 12(4): 201-206 Original Paper Received: 2006.12.19 Accepted: 2007.04.02 Published: 2007.08.31 Authors Contribution: A Study Design B Data Collection C Statistical Analysis
Rep Pract Oncol Radiother, 2007; 12(4): 201-206 Original Paper Received: 2006.12.19 Accepted: 2007.04.02 Published: 2007.08.31 Authors Contribution: A Study Design B Data Collection C Statistical Analysis
Supporting Information 2. ESGE QIC Lower GI Delphi voting process: Round 1 Working Group chair: Michal F. Kaminski, Poland
 Supporting Information 2. ESGE QIC Lower GI Delphi voting process: Round 1 Working chair: Michal F. Kaminski, Poland Population Interventions Comparator Outcome Additional evidence 1.1 Rate of adequate
Supporting Information 2. ESGE QIC Lower GI Delphi voting process: Round 1 Working chair: Michal F. Kaminski, Poland Population Interventions Comparator Outcome Additional evidence 1.1 Rate of adequate
Large Colorectal Adenomas An Approach to Pathologic Evaluation
 Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Colon Cancer Screening. Layth Al-Jashaami, MD GI Fellow, PGY 4
 Colon Cancer Screening Layth Al-Jashaami, MD GI Fellow, PGY 4 -Colorectal cancer (CRC) is a common and lethal cancer. -It has the highest incidence among GI cancers in the US, estimated to be newly diagnosed
Colon Cancer Screening Layth Al-Jashaami, MD GI Fellow, PGY 4 -Colorectal cancer (CRC) is a common and lethal cancer. -It has the highest incidence among GI cancers in the US, estimated to be newly diagnosed
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE
 COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
Endoscopic Mucosal Resection (EMR) & Endoscopic Submucosal Dissection (ESD)
 & Endoscopic Submucosal Dissection (ESD)") Endoscopic Mucosal Resection (EMR) & Endoscopic Submucosal Dissection (ESD) Minimally Invasive Polyp Removal IE-02700-Understanding EMR and ESD Brochure_R3.indd 1 Occasionally, a polyp that infiltrates
Endoscopic Mucosal Resection (EMR) & Endoscopic Submucosal Dissection (ESD) Minimally Invasive Polyp Removal IE-02700-Understanding EMR and ESD Brochure_R3.indd 1 Occasionally, a polyp that infiltrates
ACG Clinical Guideline: Colorectal Cancer Screening
 ACG Clinical Guideline: Colorectal Cancer Screening Douglas K. Rex, MD, FACG 1, David A. Johnson, MD, FACG 2, Joseph C. Anderson, MD 3, Phillip S. Schoenfeld, MD, MSEd, MSc (Epi), FACG 4, Carol A. Burke,
ACG Clinical Guideline: Colorectal Cancer Screening Douglas K. Rex, MD, FACG 1, David A. Johnson, MD, FACG 2, Joseph C. Anderson, MD 3, Phillip S. Schoenfeld, MD, MSEd, MSc (Epi), FACG 4, Carol A. Burke,
Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN
 Serrated Adenomas: What do they mean and what to do about them? Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN Colorectal Cancer Molecular Basis Pathway Frequency Genes MSI Precursor Speed
Serrated Adenomas: What do they mean and what to do about them? Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN Colorectal Cancer Molecular Basis Pathway Frequency Genes MSI Precursor Speed
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care
 Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
BENEFIT APPLICATION BLUE CARD/NATIONAL ACCOUNT ISSUES
 Medical Policy BCBSA Ref. Policy: 2.01.84 Last Review: 11/15/2018 Effective Date: 11/15/2018 Section: Medicine Related Policies 2.01.87 Confocal Laser Endomicroscopy 6.01.32 Virtual Colonoscopy/Computed
Medical Policy BCBSA Ref. Policy: 2.01.84 Last Review: 11/15/2018 Effective Date: 11/15/2018 Section: Medicine Related Policies 2.01.87 Confocal Laser Endomicroscopy 6.01.32 Virtual Colonoscopy/Computed
Objectives. Definitions. Colorectal Cancer Screening 5/8/2018. Payam Afshar, MS, MD Kaiser Permanente, San Diego. Colorectal cancer background
 Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Extended cold snare polypectomy for small colorectal polyps increases the R0 resection rate
 Extended cold snare polypectomy for small colorectal polyps increases the R0 resection rate Authors Yasuhiro Abe 1,HaruakiNabeta 1, Ryota Koyanagi 1, Taro Nakamichi 1, Hayato Hirashima 1, Alan Kawarai
Extended cold snare polypectomy for small colorectal polyps increases the R0 resection rate Authors Yasuhiro Abe 1,HaruakiNabeta 1, Ryota Koyanagi 1, Taro Nakamichi 1, Hayato Hirashima 1, Alan Kawarai
Bowel obstruction and tumors
 Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Spartan Medical Research Journal
 Spartan Medical Research Journal Research at Michigan State University College of Osteopathic Medicine Volume 2 Number 2 Winter, 2017 Pages 14-21 Title: Endoscopic Combined Snare-Forceps Technique for
Spartan Medical Research Journal Research at Michigan State University College of Osteopathic Medicine Volume 2 Number 2 Winter, 2017 Pages 14-21 Title: Endoscopic Combined Snare-Forceps Technique for
References. GI Biopsies. What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD
 What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
what is the alternative mechanism of histogenesis? Aspects of the morphology of the adenomacarcinoma Morphology of the
 Refer to: Morson B: Polyps and cancer of the large bowel. West J Med 125:93-99, Aug 1976 THE WESTERN Journal of Miedicine Polyps and Cancer of the Large Bowel BASIL MORSON, MD, London MORTALITY STATISTICS
Refer to: Morson B: Polyps and cancer of the large bowel. West J Med 125:93-99, Aug 1976 THE WESTERN Journal of Miedicine Polyps and Cancer of the Large Bowel BASIL MORSON, MD, London MORTALITY STATISTICS
6 semanas de embarazo. Tubulovillous adenoma with dysplasia icd 10. Inicio / Embarazo / 6 semanas de embarazo
 Inicio / Embarazo / 6 semanas de embarazo 6 semanas de embarazo Tubulovillous adenoma with dysplasia icd 10 Free, official coding info for 2018 ICD-10-CM D13.2 - includes detailed rules, notes, synonyms,
Inicio / Embarazo / 6 semanas de embarazo 6 semanas de embarazo Tubulovillous adenoma with dysplasia icd 10 Free, official coding info for 2018 ICD-10-CM D13.2 - includes detailed rules, notes, synonyms,
Polyps Adenomas Lipomas
 30 Chapter 2 CT Colonography Chapter 2 Polyps Adenomas Lipomas Case 8 Case 9 Case 10 Case 11 Case 12 Case 13 Case 14 Case 15 Case 16 Case 17 Case 18 Pseudopolyp Polyp after intravenous administration of
30 Chapter 2 CT Colonography Chapter 2 Polyps Adenomas Lipomas Case 8 Case 9 Case 10 Case 11 Case 12 Case 13 Case 14 Case 15 Case 16 Case 17 Case 18 Pseudopolyp Polyp after intravenous administration of
ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease
 ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease DOWNERS GROVE, Ill., (March 5, 2015) The American Society for Gastrointestinal
ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease DOWNERS GROVE, Ill., (March 5, 2015) The American Society for Gastrointestinal
Diagnostics guidance Published: 10 May 2017 nice.org.uk/guidance/dg28
 Virtual chromoendoscopy to assess colorectal polyps during colonoscopy Diagnostics guidance Published: 10 May 2017 nice.org.uk/guidance/dg28 NICE 2017. All rights reserved. Subject to Notice of rights
Virtual chromoendoscopy to assess colorectal polyps during colonoscopy Diagnostics guidance Published: 10 May 2017 nice.org.uk/guidance/dg28 NICE 2017. All rights reserved. Subject to Notice of rights
Colorectal adenocarcinoma leading cancer in developed countries In US, annual deaths due to colorectal adenocarcinoma 57,000.
 Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
B Base excision repair, in MUTYH-associated polyposis and colorectal cancer, BRAF testing, for hereditary colorectal cancer, 696
 Index Note: Page numbers of article titles are in boldface type. A Adenomatous polyposis, familial. See Familial adenomatous polyposis. Anal anastomosis, ileal-pouch, proctocolectomy with, in FAP, 591
Index Note: Page numbers of article titles are in boldface type. A Adenomatous polyposis, familial. See Familial adenomatous polyposis. Anal anastomosis, ileal-pouch, proctocolectomy with, in FAP, 591
Joint Session with ACOFP and Cancer Treatment Centers of America (CTCA): Cancer Screening: Consensus & Controversies. Ashish Sangal, M.D.
: Cancer Screening: Consensus & Controversies. Ashish Sangal, M.D.") Joint Session with ACOFP and Cancer Treatment Centers of America (CTCA): Cancer Screening: Consensus & Controversies Ashish Sangal, M.D. Cancer Screening: Consensus & Controversies Ashish Sangal, MD Director,
Joint Session with ACOFP and Cancer Treatment Centers of America (CTCA): Cancer Screening: Consensus & Controversies Ashish Sangal, M.D. Cancer Screening: Consensus & Controversies Ashish Sangal, MD Director,
Duodenal adenomas Management. Dr Stratis Alexandridis Consultant Gastroenterologist BRI
 Duodenal adenomas Management Dr Stratis Alexandridis Consultant Gastroenterologist BRI Introduction Ampullary and non ampullary polyps of the duodenum are diagnosed within and outside genetic syndromes.
Duodenal adenomas Management Dr Stratis Alexandridis Consultant Gastroenterologist BRI Introduction Ampullary and non ampullary polyps of the duodenum are diagnosed within and outside genetic syndromes.
BOWEL CANCER. Causes of bowel cancer
 A cancer is an abnormality in an organ that grows without control. The growth is often quite slow, but will continue unabated until it is detected. It can cause symptoms by its presence in the organ or
A cancer is an abnormality in an organ that grows without control. The growth is often quite slow, but will continue unabated until it is detected. It can cause symptoms by its presence in the organ or
GI Polyp syndromes in children. Screening and surveillance, surgery.
 Dr Warren Hyer Consultant Paediatric Gastroenterologist St Mark s Hospital, UK GI Polyp syndromes in children Screening and surveillance, surgery. No conflict of interests to declare Objectives Understand
Dr Warren Hyer Consultant Paediatric Gastroenterologist St Mark s Hospital, UK GI Polyp syndromes in children Screening and surveillance, surgery. No conflict of interests to declare Objectives Understand
Historical. Note: The parenthetical numbers in the Clinical Indications section refer to the source documents cited in the References Section below.
 Clinical UM Guideline Subject: Colonoscopy Guideline #: CG-SURG-01 Current Effective Date: 01/21/2015 Status: Revised Last Review Date: 05/15/2014 Description Colonoscopy describes the direct visual inspection
Clinical UM Guideline Subject: Colonoscopy Guideline #: CG-SURG-01 Current Effective Date: 01/21/2015 Status: Revised Last Review Date: 05/15/2014 Description Colonoscopy describes the direct visual inspection
General Surgery Grand Grounds
 General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
Bowel Screening Colonoscopy in Glasgow How well are we doing? How well should we be doing? How can we evidence and improve performance?
 Bowel Screening Colonoscopy in Glasgow 2017 How well are we doing? How well should we be doing? How can we evidence and improve performance? Bowel Screening Standards - Scotland Definitions Completion
Bowel Screening Colonoscopy in Glasgow 2017 How well are we doing? How well should we be doing? How can we evidence and improve performance? Bowel Screening Standards - Scotland Definitions Completion
A superficial radiotherapy B single pass curettage C excision with 2 mm margins D excision with 5 mm margins E Mohs micrographic surgery.
 1- A 63-year-old woman presents with a non-healing lesion on her right temple that has been present for over two years. On examination there is a 6 mm well defined lesion with central ulceration, telangiectasia
1- A 63-year-old woman presents with a non-healing lesion on her right temple that has been present for over two years. On examination there is a 6 mm well defined lesion with central ulceration, telangiectasia
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma
 Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
2. Describe pros/cons of screening interventions (including colonoscopy, CT colography, fecal tests)
") Learning Objectives 1. Review principles of colon adenoma/cancer biology that permit successful prevention regimes 2. Describe pros/cons of screening interventions (including colonoscopy, CT colography,
Learning Objectives 1. Review principles of colon adenoma/cancer biology that permit successful prevention regimes 2. Describe pros/cons of screening interventions (including colonoscopy, CT colography,
Colorectal Cancer Prevention Quantity and Quality Count
 Colorectal Cancer Prevention Quantity and Quality Count Ernesto Drelichman, MD Gastrointestinal Surgery & Endoscopy Providence Hospital Key Messages Colorectal cancer can be prevented Screening reduces
Colorectal Cancer Prevention Quantity and Quality Count Ernesto Drelichman, MD Gastrointestinal Surgery & Endoscopy Providence Hospital Key Messages Colorectal cancer can be prevented Screening reduces
Title Description Type / Priority
 Merit-based Incentive Payment system (MIPS) 2019 Qualified Clinical Data Registry (QCDR) Measure Specifications Summary Listing of QCDR measures supported by the NHCR Measure # NHCR4 NHCR5 GIQIC12 GIQIC15
Merit-based Incentive Payment system (MIPS) 2019 Qualified Clinical Data Registry (QCDR) Measure Specifications Summary Listing of QCDR measures supported by the NHCR Measure # NHCR4 NHCR5 GIQIC12 GIQIC15
Update on Colonic Serrated (and Conventional) Adenomatous Polyps
 Adenomatous Polyps") Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical