LIVER. Question 1 ~ Anatomy. Answer 1 ~ Anatomy 1/5/2018. SEMCME Board Review January 11-12, 2017
|
|
|
- Beverly Lynch
- 5 years ago
- Views:
Transcription


 Arantius Ligament B) Ligamentum Venosum C) Hepatogastric D) Coronary E) LienoRenal LIVER Answer 1 ~ Anatomy Which of")
1 SEMCME Board Review January 11-12, 2017 Surgical Treatment of Hepatobiliary and Splenic Disorders Michael J. Jacobs, MD, FACS, FICS Clinical Professor of Surgery- MSU CHM Associate Chair of Surgery Director of Hepatobiliary Pancreas Program OBJECTIVES Anatomical considerations Indications Contraindications Operative treatment options Imaging studies Advanced techniques Survival, Recurrence, Surveillance Question 1 ~ Anatomy Which of the following are not ligaments of the liver? A) Arantius Ligament B) Ligamentum Venosum C) Hepatogastric D) Coronary E) LienoRenal LIVER Answer 1 ~ Anatomy Which of the following are not ligaments of the liver? A) Arantius Ligament B) Ligamentum Venosum C) Hepatogastric D) Coronary E) LienoRenal 1
 Reaspiration and catheter drainage B) Observation C) Enucleation/excision D) Left trisectionectomy E) Marsupialization Post-resection Imaging BENIGN LESIONS CYSTIC LESIONS SIMPLE CYSTS POLYCYSTIC")

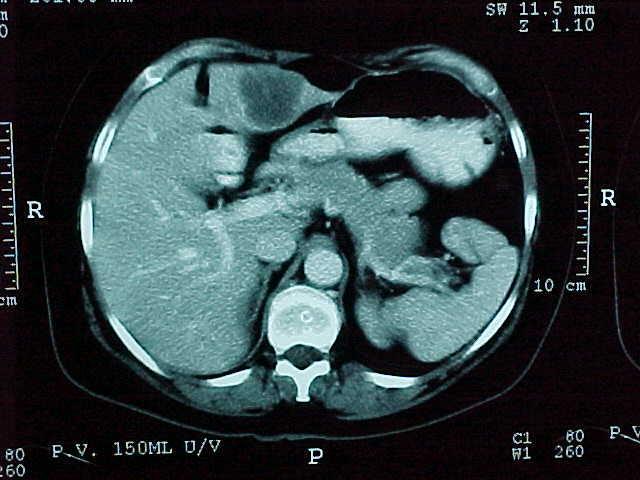
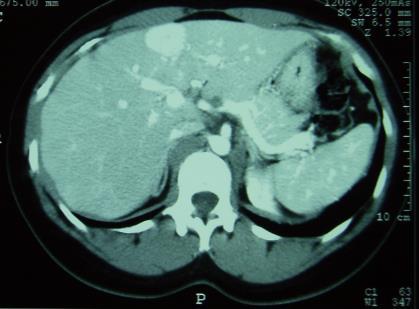
2 Question 2 A 40-year old female presents with dull left upper quadrant pain and presents with the following imaging after attempted aspiration. Which of the following is the best treatment? A) Reaspiration and catheter drainage B) Observation C) Enucleation/excision D) Left trisectionectomy E) Marsupialization Post-resection Imaging BENIGN LESIONS CYSTIC LESIONS SIMPLE CYSTS POLYCYSTIC LIVER BILIARY CYSTADENOMA Question 2 ~ Answer A 40-year old female presents with dull left upper quadrant pain and presents with the following imaging after attempted aspiration. Which of the following is the best treatment? A) Reaspiration and catheter drainage B) Observation C) Enucleation/excision D) Left trisectionectomy E) Marsupialization Question 3 A 32-year old female complains of progressive left upper abdominal pain and early satiety with solid meals. She presents with the following imaging. Which of the following is the best treatment? A) Cessation of birth control pills B) Radiofrequency ablation C) Left partial liver resection D) Observation E) Referral for liver transplantation evaluation 2






3 Imaging Intraoperative Images BENIGN LESIONS SOLID LESIONS HEMANGIOMA HEPATIC ADENOMA FOCAL NODULAR HYPERPLASIA BILIARY HAMARTOMA Von Meyenberg complex Giant Hemangioma Focal Nodular Hyperplasia HEPATIC ADENOMA 3


 Observation E) Referral for liver")

 Bilobar metachronous breast cancer")


4 Question 3~ Answer A 32-year old female complains of progressive left upper abdominal pain and early satiety with solid meals. She presents with the following imaging. Which of the following is the best treatment? A) Cessation of birth control pills B) Radiofrequency ablation C) Left partial liver resection D) Observation E) Referral for liver transplantation evaluation Question 4 Which of the following are indications for resection? A) 3-cm asymptomatic hemangioma left liver B) 10-cm simple symptomatic cyst- left liver C) Bilobar metachronous breast cancer mets D) 5-cm left liver colorectal met into antrum E) Left CholangioCa with right PV thrombus MALIGNANT LESIONS METASTATIC LESIONS COLORECTAL CANCER NEUROENDOCRINE GIST BREAST / OVARIAN PRIMARY LIVER CANCERS HEPATOCELLULAR CANCER CHOLANGIOCELLULAR CYSTADENOCARCINOMA COLORECTAL METASTASES Hepatocellular Carcinoma Milan Criteria <5-cm, 3<3-cm MELD Score Child Pugh METASTASECTOMY 4
 procedure Predict: Short-term survival in")
] + 11.2[Ln INR] + 9.57[Ln serum creatinine (mg/dl)] + 6.")

5 MELD Score The Model for End-Stage Liver Disease Scoring system for assessing the severity of chronic liver disease. MELD was developed to predict death within three months of surgery in patients who had undergone a transjugular intrahepatic portosystemic shunt (TIPS) procedure Predict: Short-term survival in patients on wait list for liver transplantation Risk of postoperative mortality MELD United Network for Organ Sharing (UNOS) use MELD score to prioritize organ allocation MELD = 3.78[Ln serum bilirubin (mg/dl)] [Ln INR] [Ln serum creatinine (mg/dl)] If the patient has been dialyzed twice within the last 7 days, then serum creatinine should be assigned a value of 4.0 Any value less than one should be converted to 1.0 Patients with MELD scores 17 or greater are considered candidates for liver transplantation MELD Score 3 Month Mortality Child-Pugh-Turcotte Score Measure 1 point 2 points 3 points MELD Score 3 Month Mortality Total bilirubin, μmol/l (mg/dl) <34 (<2) (2 3) >50 (>3) 40 or more 71.3% mortality % mortality % mortality % mortality <9 1.9% mortality Serum albumin, g/dl Prothrombin time, prolongation (s) OR INR Ascites Hepatic encephalopathy > <2.8 <4.0 < > 6.0 >2.3 None Mild (or suppressed with medication) Moderate to severe (or refractory) None Grade I II Grade III IV CPT Score SEGMENTAL RESECTION Points Class One year survival Two year survival 5 6 A 100% 85% 7 9 B 81% 57% C 45% 35% -Child CG, Turcotte JG. Surgery and portal hypertension. In: The liver and portal hypertension. Edited by CG Child. Philadelphia: Saunders 1964: Pugh RNH, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R. Transection of the esophagus in bleeding oesophageal varices. Br J Surg 1973;60:


 80 100")





6 COLORECTAL METASTASES ACTUARIAL SURVIVAL CYSTIC MALIGNANT NEOPLASMS Cum Survival FOLLOWUP (Months) CYSTADENOCARCINOMA n=161 survival 48% at 7 years (Lodge-Leeds) HEPATIC RESECTION IMPROVING RESULTS Adjuvant therapies Careful follow up Tumor markers Complex radiology Further surgery Redo hepatic surgery Recurrent colorectal cancer excision Lung surgery Further chemotherapy / radiotherapy 6



7 CUMULATIVE SURVIVAL 1/5/2018 REDO RESECTION ALTERNATIVES FOLLOWUP (MONTHS) 100 Radiofrequency ablation Cryotherapy Microwave therapy Radioactive microspheres Hepatic artery infusion pump Laparoscopic hepatectomy Question 4 ~ Answer Which of the following are indications for resection? A) 3-cm asymptomatic hemangioma left liver B) 10-cm simple symptomatic cyst- left liver C) Bilobar metachronous breast cancer mets D) 5-cm left liver colorectal met into antrum E) Left CholangioCa with right PV thrombus Bile Duct Exploration-Steps Cholangiogram via cystic duct (repeated) Kocher maneuver and palpation Flush with Saline Open Duct longitudinally just above duodenum Flush again, cholangiogram +/- endoscopy T tube to dependent drainage May need bypass- Avoid side to side Duodenotomy, sphincterotomy Cholangiogram timing post op and management Bile Duct Injury < 1% of cholecystectomy procedures Use Critical View Approach Early cholangiogram to verify and clarify anatomy Convert to Open Technique Roux en y Hepaticojejunostomy Leave drains and transfer to HPB unit Question 5 An otherwise healthy 65-year old man presents with progressive jaundice and itching. The Total Bili is 30 and Ultrasound of the liver shows intrahepatic biliary ductal dilation and cholelithiasis. Which of the following is the next step? A) Stop lipitor and rescan in 1 month B) Laparoscopic cholecystectomy C) Staging CT imaging D) Laparotomy and cholecystectomy/cholangiogram E) ERCP 7






 Stop lipitor and rescan in 1 month B)")
8 CHOLANGIOCARCINOMA Evaluation and Management Diagnostic Studies -Imaging Spiral CT +/- Angiography MRI/MRCP Eovist ERCP/PTC Stent Brushings Laparoscopy PET Benign or Malignant Ask IBD/UC PSC Cholangiocarcinoma CT scan MRI/MRCP ERCP/PTC/Brushings Grade Level CA 19-9 Stent STRICTURE Question 5 ~ Answer An otherwise healthy 65-year old man presents with progressive jaundice and itching. The Total Bili is 30 and Ultrasound of the liver shows intrahepatic biliary ductal dilation and cholelithiasis. Which of the following is the next step? A) Stop lipitor and rescan in 1 month B) Laparoscopic cholecystectomy C) Staging CT imaging D) Laparotomy and cholecystectomy/cholangiogram E) ERCP 8
 Observation B) Surgery C) Percutaneous biopsy D) Ursodeoxycholic Acid (URSO) E) ERCP and biopsy GALLBLADDER CANCER RISK FACTORS DIAGNOSIS-TREATMENT Gallstones Porcelain gallbladder Female gender")

9 Question 6 A 50-year old female is found to have an asymptomatic 2-cm hypoechoic polypoid mass in the gallbladder on an ultrasound. She has normal liver function tests. What is the best treatment? A) Observation B) Surgery C) Percutaneous biopsy D) Ursodeoxycholic Acid (URSO) E) ERCP and biopsy GALLBLADDER CANCER RISK FACTORS DIAGNOSIS-TREATMENT Gallstones Porcelain gallbladder Female gender Obesity Older age Ethnicity Choledochal cysts Abnormalities of the bile ducts Gallbladder polyps Industrial and environmental chemicals Typhoid Timing Preoperative Intraoperative Postoperative Extent of Resection T1a- Cholecystectomy Radical Cholecystectomy +/- CBD resection Survival Statistics by Stage Stage 5-Year Survival Rate 0 81% IA 50% IB 29% IIA 7% IIB 9% III 3% IV 2% Question 6 ~ Answer A 50-year old female is found to have an asymptomatic 2-cm hypoechoic polypoid mass in the gallbladder on an ultrasound. She has normal liver function tests. What is the best treatment? A) Observation B) Surgery C) Percutaneous biopsy D) Ursodeoxycholic Acid (URSO) E) ERCP and biopsy 9

10 Spleen-Resection Failure to respond to conservative Tx Advanced splenic trauma En bloc for Cancers of stomach, pancreas, and colon Blood dyscrasias ITP, Thal Major, HS, Primary lymphoma Beware of the patient sent for low platelets sent for splenectomy who has liver disease Vaccinate-Pneumovax Expect transient leukocytosis/thrombocytosis QUESTIONS / COMMENTS? 10
Surgical Treatment of Hepatobiliary and Splenic Disorders
 SEMCME Board Review January 10-11, 2019 Surgical Treatment of Hepatobiliary and Splenic Disorders Michael J. Jacobs, MD, FACS, FICS Clinical Professor of Surgery- MSU CHM Associate Chair of Surgery Director
SEMCME Board Review January 10-11, 2019 Surgical Treatment of Hepatobiliary and Splenic Disorders Michael J. Jacobs, MD, FACS, FICS Clinical Professor of Surgery- MSU CHM Associate Chair of Surgery Director
Resident Teaching Conference:
 Resident Teaching Conference: Evaluation of the Dreaded Liver Mass May 6, 2011 Sunil Geevarghese, MD, HS 00 Matt Landman, MD Anatomy Overview Couinaud anatomy Resection nomenclature Functional Assessment
Resident Teaching Conference: Evaluation of the Dreaded Liver Mass May 6, 2011 Sunil Geevarghese, MD, HS 00 Matt Landman, MD Anatomy Overview Couinaud anatomy Resection nomenclature Functional Assessment
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons
 General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
General Surgery Curriculum Royal Australasian College of Surgeons, General Surgeons Australia & New Zealand Association of General Surgeons MODULE TITLE: UPPER GI & HPB - HEPATIC, PANCREATIC & BILIARY
LiverGroup.org. Case Report Form (CRF) for STAGED procedures
 for STAGED procedures") Case Report Form (CRF) for STAGED procedures Patient Characteristics Case number * Age * ( 18)y Gender * Male Female Race * Caucasian Asian African Other If other race, please specify Height * cm Weight
Case Report Form (CRF) for STAGED procedures Patient Characteristics Case number * Age * ( 18)y Gender * Male Female Race * Caucasian Asian African Other If other race, please specify Height * cm Weight
Hepatobiliary and Pancreatic Malignancies
 Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
6 th August 2018 Day 1 - Gallbladder & Bile duct Topic
 Venue: Sterling Hospital Auditorium, Sterling Hospitals, Gurukul Road Ahmedabad, Gujarat 6 th August 2018 Day 1 - Gallbladder & Bile duct Registration(8:00am-8:15am) Inauguration(8:15am-8:30am) Welcome
Venue: Sterling Hospital Auditorium, Sterling Hospitals, Gurukul Road Ahmedabad, Gujarat 6 th August 2018 Day 1 - Gallbladder & Bile duct Registration(8:00am-8:15am) Inauguration(8:15am-8:30am) Welcome
BILIARY TRACT & PANCREAS, PART II
 CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
CME Pretest BILIARY TRACT & PANCREAS, PART II VOLUME 41 1 2015 A pretest is mandatory to earn CME credit on the posttest. The pretest should be completed BEFORE reading the overview. Both tests must be
Workup of a Solid Liver Lesion
 Workup of a Solid Liver Lesion Joseph B. Cofer MD FACS Chief Quality Officer Erlanger Health System Affiliate Professor of Surgery UTHSC-Chattanooga I have no financial or other relationships with any
Workup of a Solid Liver Lesion Joseph B. Cofer MD FACS Chief Quality Officer Erlanger Health System Affiliate Professor of Surgery UTHSC-Chattanooga I have no financial or other relationships with any
Cholangiocellular carcinoma. Dr. med. Henrik Csaba Horváth PhD
 Cholangiocellular carcinoma Dr. med. Henrik Csaba Horváth PhD Acalculous biliary diseases April 12, 2017 2 Cholangiocarcinoma A slow growing malignancy of the biliary tract which tend - to infiltrate locally
Cholangiocellular carcinoma Dr. med. Henrik Csaba Horváth PhD Acalculous biliary diseases April 12, 2017 2 Cholangiocarcinoma A slow growing malignancy of the biliary tract which tend - to infiltrate locally
Liver Cancer (Hepatocellular Carcinoma or HCC) Overview
 Overview") Liver Cancer (Hepatocellular Carcinoma or HCC) Overview Recent advances in liver cancer care seek to address the rising incidence of liver cancer, which has steadily increased over the past three decades.
Liver Cancer (Hepatocellular Carcinoma or HCC) Overview Recent advances in liver cancer care seek to address the rising incidence of liver cancer, which has steadily increased over the past three decades.
Newcastle HPB MDM updated radiology imaging protocol recommendations. Author Dr John Scott. Consultant Radiologist Freeman Hospital
 Newcastle HPB MDM updated radiology imaging protocol recommendations Author Dr John Scott. Consultant Radiologist Freeman Hospital This document is intended as a guide to aid radiologists and clinicians
Newcastle HPB MDM updated radiology imaging protocol recommendations Author Dr John Scott. Consultant Radiologist Freeman Hospital This document is intended as a guide to aid radiologists and clinicians
Cholangiocarcinoma (Bile Duct Cancer)
") Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Cholangiocarcinoma (Bile Duct Cancer) The Bile Duct System (Biliary Tract) A network of bile ducts (tubes) connects the liver and the gallbladder to the small intestine. This network begins in the liver
Imaging of liver and pancreas
 Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Imaging of liver and pancreas.. Disease of the liver Focal liver disease Diffusion liver disease Focal liver disease Benign Cyst Abscess Hemangioma FNH Hepatic adenoma HCC Malignant Fibrolamellar carcinoma
Liver Tumors. Prof. Dr. Ahmed El - Samongy
 Liver Tumors Prof. Dr. Ahmed El - Samongy Objective 1. Identify the most important features of common benign liver tumors 2. Know the risk factors, diagnosis, and management of hepatocellular carcinoma
Liver Tumors Prof. Dr. Ahmed El - Samongy Objective 1. Identify the most important features of common benign liver tumors 2. Know the risk factors, diagnosis, and management of hepatocellular carcinoma
Surgical Management of CBD Injury Jin Seok Heo
 Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
Liver Tumors. Patient Education. Treatment options 8 4A. About the Liver. Surgical Specialties
 Patient Education Treatment options This handout describes different kinds of tumors that form in the liver and how they are treated. About the Liver Your liver is the largest organ in your abdomen. It
Patient Education Treatment options This handout describes different kinds of tumors that form in the liver and how they are treated. About the Liver Your liver is the largest organ in your abdomen. It
GALLBLADDER CANCER. Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011
 GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction
 Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction Ann S. Fulcher, MD Medical College of Virginia Virginia Commonwealth University Richmond, Virginia Objectives To
Navigating the Biliary Tract with CT & MR: An Imaging Approach to Bile Duct Obstruction Ann S. Fulcher, MD Medical College of Virginia Virginia Commonwealth University Richmond, Virginia Objectives To
INTERNATIONAL HEPATO-PANCREATO-BILIARY ASSOCIATION (IHPBA), INDIAN CHAPTER 6TH CERTIFICATE COURSE IN HEPATO-PANCREATO-BILIARY SURGERY
, INDIAN CHAPTER 6TH CERTIFICATE COURSE IN HEPATO-PANCREATO-BILIARY SURGERY") Day 1-28 th August 2013 Liver TS Ravikumar, Goro Honda, R Surendran, V Sitaram, George Kurien Swatee Halbe, Biju Pottakkat, Vibha Naik, Deepak Barathi 1 Surgical quality and safety Inaugural lecture 2
Day 1-28 th August 2013 Liver TS Ravikumar, Goro Honda, R Surendran, V Sitaram, George Kurien Swatee Halbe, Biju Pottakkat, Vibha Naik, Deepak Barathi 1 Surgical quality and safety Inaugural lecture 2
General Surgery PURPLE SERVICE MUHC-RVH Site
 Preamble HPB is a clinical teaching unit with several different vocations: It regroups all solid organ Transplantation as well as most advanced Hepatobiliary and Pancreatic clinical activities performed
Preamble HPB is a clinical teaching unit with several different vocations: It regroups all solid organ Transplantation as well as most advanced Hepatobiliary and Pancreatic clinical activities performed
Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options
 Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options Poster No.: C-1501 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Hadjivassiliou,
Post-operative complications following hepatobiliary surgery: imaging findings and current radiological treatment options Poster No.: C-1501 Congress: ECR 2015 Type: Educational Exhibit Authors: A. Hadjivassiliou,
Surgical Hepatobiliary Diseases
 Case 1 Surgical Hepatobiliary Diseases M. Sinanan MD, PhD 48 yo WF with RUQ, postprandial pain, fever, nausea, vomiting, and tenderness. US and HIDA done Issues 1. 2. Interpretation Adequate WU? 2 Normal
Case 1 Surgical Hepatobiliary Diseases M. Sinanan MD, PhD 48 yo WF with RUQ, postprandial pain, fever, nausea, vomiting, and tenderness. US and HIDA done Issues 1. 2. Interpretation Adequate WU? 2 Normal
Intraoperative staging of GIT cancer using Intraoperative Ultrasound
 Intraoperative staging of GIT cancer using Intraoperative Ultrasound Thesis For Fulfillment of MSc Degree In Surgical Oncology By Abdelhalim Salah Abdelhalim Moursi M.B.B.Ch (Cairo University ) Supervisors
Intraoperative staging of GIT cancer using Intraoperative Ultrasound Thesis For Fulfillment of MSc Degree In Surgical Oncology By Abdelhalim Salah Abdelhalim Moursi M.B.B.Ch (Cairo University ) Supervisors
The Fellowship Council And The American Hepato-Pancreatico Biliary Association
 The Fellowship Council And The American Hepato-Pancreatico Biliary Association Advanced GI Surgery Curriculum for Hepato-Pancreatic & Biliary Surgery Fellowship 1. Introduction The purpose of Fellowship
The Fellowship Council And The American Hepato-Pancreatico Biliary Association Advanced GI Surgery Curriculum for Hepato-Pancreatic & Biliary Surgery Fellowship 1. Introduction The purpose of Fellowship
CHOLANGIOCARCINOMA (CCA)
") CHOLANGIOCARCINOMA (CCA) Deepak Hariharan MD (Research), FRCS, Locum Consultant HPB Surgeon AIM Outline essential facts & principles Present 4 cases Discuss Challenges /Controversies INTRODUCTION Most
CHOLANGIOCARCINOMA (CCA) Deepak Hariharan MD (Research), FRCS, Locum Consultant HPB Surgeon AIM Outline essential facts & principles Present 4 cases Discuss Challenges /Controversies INTRODUCTION Most
Update in abdominal Surgery in cirrhotic patients
 Update in abdominal Surgery in cirrhotic patients Safi Dokmak HBP department and liver transplantation Beaujon Hospital, Clichy, France Cairo, 5 April 2016 Cirrhosis Prevalence in France (1%)* Patients
Update in abdominal Surgery in cirrhotic patients Safi Dokmak HBP department and liver transplantation Beaujon Hospital, Clichy, France Cairo, 5 April 2016 Cirrhosis Prevalence in France (1%)* Patients
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Cystic Disease of the Liver Work Up and Management. Louis Ferrari MD, PGY 3 6/9/16 SUNY Downstate Medical Center
 Cystic Disease of the Liver Work Up and Management Louis Ferrari MD, PGY 3 6/9/16 SUNY Downstate Medical Center The Case 73F presents to clinic after diagnostic laparoscopy at OSH. Known liver mass for
Cystic Disease of the Liver Work Up and Management Louis Ferrari MD, PGY 3 6/9/16 SUNY Downstate Medical Center The Case 73F presents to clinic after diagnostic laparoscopy at OSH. Known liver mass for
GASTROINTESTINAL IMAGING STUDY GUIDE
 GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
GASTROINTESTINAL IMAGING STUDY GUIDE Pharynx Diverticula Foreign bodies Trauma o Motility Disorders Esophagus Diverticula Trauma Esophagitis Barrett esophagus Rings, webs, and strictures Varices Benign
Personal Profile. Name: 劉 XX Gender: Female Age: 53-y/o Past history. Hepatitis B carrier
 Personal Profile Name: 劉 XX Gender: Female Age: 53-y/o Past history Hepatitis B carrier Chief complaint Fever on and off for 2 days Present illness 94.10.14 Sudden onset of epigastric pain 94.10.15 Fever
Personal Profile Name: 劉 XX Gender: Female Age: 53-y/o Past history Hepatitis B carrier Chief complaint Fever on and off for 2 days Present illness 94.10.14 Sudden onset of epigastric pain 94.10.15 Fever
Liver Cancer And Tumours
 Liver Cancer And Tumours What causes liver cancer? Many factors may play a role in the development of cancer. Because the liver filters blood from all parts of the body, cancer cells from elsewhere can
Liver Cancer And Tumours What causes liver cancer? Many factors may play a role in the development of cancer. Because the liver filters blood from all parts of the body, cancer cells from elsewhere can
Appendix 5. EFSUMB Newsletter. Gastroenterological Ultrasound
 EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
EFSUMB Newsletter 87 Examinations should encompass the full range of pathological conditions listed below A log book listing the types of examinations undertaken should be kept Training should usually
Jaundice. Agnieszka Dobrowolska- Zachwieja, MD, PhD
 Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Jaundice Agnieszka Dobrowolska- Zachwieja, MD, PhD Jaundice definition Jaundice, as in the French jaune, refers to the yellow discoloration of the skin. It arises from the abnormal accumulation of bilirubin
Multiple Primary Quiz
 Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Multiple Primary Quiz Case 1 A 72 year old man was found to have a 12 mm solid lesion in the pancreatic tail by computed tomography carried out during a routine follow up study of this patient with adult
Hepato-Pancreatico-Biliary Surgery. Dr. Ankur J. Shah. MS, DNB, MNAMS, MRCSEd (UK), FRCS (UK)
, FRCS (UK)") Hepato-Pancreatico-Biliary Surgery Dr. Ankur J. Shah MS, DNB, MNAMS, MRCSEd (UK), FRCS (UK) Consultant Hepato-Pancreatico-Biliary and Liver Transplant Surgeon Ansh Liver Clinic Prevention to Cure Address
Hepato-Pancreatico-Biliary Surgery Dr. Ankur J. Shah MS, DNB, MNAMS, MRCSEd (UK), FRCS (UK) Consultant Hepato-Pancreatico-Biliary and Liver Transplant Surgeon Ansh Liver Clinic Prevention to Cure Address
Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology
 Physiology") Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology 95% of bile acids reabsorbed; colic and chenodeoxycolic primary bile acids cholecystokinin (CCK) major stimulus of gallbladder
Vesalius SCALpel : Biliary (see also: biliary/pancreatic folios) Physiology 95% of bile acids reabsorbed; colic and chenodeoxycolic primary bile acids cholecystokinin (CCK) major stimulus of gallbladder
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer
 What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
PANCREATIC CANCER GUIDELINES
 PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
PANCREATIC CANCER GUIDELINES North-East London Cancer Network & Barts and the London HPB Centre PROTOCOL FOR MANAGEMENT OF PANCREATIC CANCER (SEPTEMBER 2010) I. PRE-REFERRAL GUIDELINES Screening 1. Offer
Revised Annual Program Volumes for ASTS Accreditation Approved May 2013 Revised June 2016
 Overview This document outlines new requirements and processes for ASTS accreditation of transplant surgery fellowships including volume requirements for ASTS accreditation, as well as the individual training
Overview This document outlines new requirements and processes for ASTS accreditation of transplant surgery fellowships including volume requirements for ASTS accreditation, as well as the individual training
Cholangiocarcinoma. GI Practice Guideline. Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist)
 Barbara Fisher, MD, FRCPC (Radiation Oncologist)") Cholangiocarcinoma GI Practice Guideline Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist) Approval Date: October 2006 This guideline is a statement of consensus
Cholangiocarcinoma GI Practice Guideline Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist) Approval Date: October 2006 This guideline is a statement of consensus
Anaesthetic considerations and peri-operative risks in patients with liver disease
 Anaesthetic considerations and peri-operative risks in patients with liver disease Dr. C. K. Pandey Professor & Head Department of Anaesthesiology & Critical Care Medicine Institute of Liver and Biliary
Anaesthetic considerations and peri-operative risks in patients with liver disease Dr. C. K. Pandey Professor & Head Department of Anaesthesiology & Critical Care Medicine Institute of Liver and Biliary
Approach to Liver Lesions. Anjana A. Pillai, MD Associate Professor of Medicine Director, Liver Tumor Clinic The University of Chicago Medical Center
 Approach to Liver Lesions Anjana A. Pillai, MD Associate Professor of Medicine Director, Liver Tumor Clinic The University of Chicago Medical Center Objectives Identify common clinical features and imaging
Approach to Liver Lesions Anjana A. Pillai, MD Associate Professor of Medicine Director, Liver Tumor Clinic The University of Chicago Medical Center Objectives Identify common clinical features and imaging
Case Reports. Intraductal Papillary Cholangiocarcinoma: Case Report and Review of the Literature INTRODUCTION CASE REPORT
 Case Reports Kongkam K, Rerknimitr R 45 Case Report and Review of the Literature Pradermchai Kongkam, M.D. Rungsun Rerknimitr, M.D. ABSTRACT A case of papillary cholangiocarcinoma is presented. A 64-year-old
Case Reports Kongkam K, Rerknimitr R 45 Case Report and Review of the Literature Pradermchai Kongkam, M.D. Rungsun Rerknimitr, M.D. ABSTRACT A case of papillary cholangiocarcinoma is presented. A 64-year-old
CBD stones & strictures (Obstructive jaundice)
") 1 CBD stones & strictures (Obstructive jaundice) Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA), MHPE (Nl & Eg) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz
1 CBD stones & strictures (Obstructive jaundice) Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA), MHPE (Nl & Eg) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz
Primary Sclerosing Cholangitis and Cholestatic liver diseases. Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants
 Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Primary Sclerosing Cholangitis and Cholestatic liver diseases Ahsan M Bhatti MD, FACP Bhatti Gastroenterology Consultants I have nothing to disclose Educational Objectives What is PSC? Understand the cholestatic
Liver surgery, acute GI tract bleeding
 Semmelweis University, Faculty of Medicine, 1 st Department of Surgery Liver surgery, acute GI tract bleeding Oszkár HAHN M.D. LIVER CYST US, CT, MRI Parasite (ELISA, eosinophil, anaphylaxy) Echinococcus
Semmelweis University, Faculty of Medicine, 1 st Department of Surgery Liver surgery, acute GI tract bleeding Oszkár HAHN M.D. LIVER CYST US, CT, MRI Parasite (ELISA, eosinophil, anaphylaxy) Echinococcus
Radiology of hepatobiliary diseases
 GI cycle - Lecture 14 436 Teams Radiology of hepatobiliary diseases Objectives 1. To Interpret plan x-ray radiograph of abdomen with common pathologies. 2. To know the common pathologies presentation.
GI cycle - Lecture 14 436 Teams Radiology of hepatobiliary diseases Objectives 1. To Interpret plan x-ray radiograph of abdomen with common pathologies. 2. To know the common pathologies presentation.
Malignant Focal Liver Lesions
 Malignant Focal Liver Lesions Other Than HCC Pablo R. Ros, MD, MPH, PhD Departments of Radiology and Pathology University Hospitals Cleveland Medical Center Case Western Reserve University Pablo.Ros@UHhospitals.org
Malignant Focal Liver Lesions Other Than HCC Pablo R. Ros, MD, MPH, PhD Departments of Radiology and Pathology University Hospitals Cleveland Medical Center Case Western Reserve University Pablo.Ros@UHhospitals.org
Management of Cholangiocarcinoma. Roseanna Lee, MD PGY-5 Kings County Hospital
 Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
REFERRAL GUIDELINES: GALLSTONES
 REFERRAL GUIDELINES: GALLSTONES Document Purpose To ensure patients with gallstones disease are managed appropriately in primary/ secondary care Oxford Radcliffe Hospital Surgical Department Surgical Registrar
REFERRAL GUIDELINES: GALLSTONES Document Purpose To ensure patients with gallstones disease are managed appropriately in primary/ secondary care Oxford Radcliffe Hospital Surgical Department Surgical Registrar
Surgical conditions of liver Somkit Mingphruedhi, M.D.
 Surgical conditions of liver Somkit Mingphruedhi, M.D. Division of HPB Surgery, Department of Surgery Ramathibodi Hospital Anatomy IVC Portal Vein Hepatic Artery Splenic Vein Gallbladder CBD SMV Anatomy
Surgical conditions of liver Somkit Mingphruedhi, M.D. Division of HPB Surgery, Department of Surgery Ramathibodi Hospital Anatomy IVC Portal Vein Hepatic Artery Splenic Vein Gallbladder CBD SMV Anatomy
Management of Colorectal Liver Metastases
 Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
Endoscopic Management of Biliary Strictures. Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center
 Endoscopic Management of Biliary Strictures Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Malignant Biliary Strictures Etiologies: Pancreatic
Endoscopic Management of Biliary Strictures Sammy Ho, MD Director of Pancreaticobiliary Services and Endoscopic Ultrasound Montefiore Medical Center Malignant Biliary Strictures Etiologies: Pancreatic
Hilar cholangiocarcinoma. Frank Wessels, Maarten van Leeuwen, UMCU utrecht
 Hilar cholangiocarcinoma Frank Wessels, Maarten van Leeuwen, UMCU utrecht Content Anatomy Biliary strictures (Hilar) Cholangiocarcinoom Staging Biliary tract 1 st order Ductus hepatica dextra Ductus hepaticus
Hilar cholangiocarcinoma Frank Wessels, Maarten van Leeuwen, UMCU utrecht Content Anatomy Biliary strictures (Hilar) Cholangiocarcinoom Staging Biliary tract 1 st order Ductus hepatica dextra Ductus hepaticus
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
Index Note: Page numbers of article titles are in boldface type. A Acute variceal bleeding management of, 251 262 balloon tamponade of esophagus in, 257 258 endoscopic therapies in, 255 257. See also Endoscopy,
MAKING CONNECTIONS. Los Angeles Medical Center
 MAKING CONNECTIONS Los Angeles Medical Center Resident: Chris Molloy, MD Fellow: Christian Coroian, MD, MBA Attending: Tina Hardley, MD Program/Dept(s): Los Angeles Medical Center CHIEF COMPLAINT & HPI
MAKING CONNECTIONS Los Angeles Medical Center Resident: Chris Molloy, MD Fellow: Christian Coroian, MD, MBA Attending: Tina Hardley, MD Program/Dept(s): Los Angeles Medical Center CHIEF COMPLAINT & HPI
Hepatocellular Carcinoma: Diagnosis and Management
 Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A ACLF. See Acute-on-chronic liver failure (ACLF) Acute kidney injury (AKI) in ACLF patients, 967 Acute liver failure (ALF), 957 964 causes
Index Note: Page numbers of article titles are in boldface type. A ACLF. See Acute-on-chronic liver failure (ACLF) Acute kidney injury (AKI) in ACLF patients, 967 Acute liver failure (ALF), 957 964 causes
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Hepatobiliary Malignancies Retrospective Study at Truman Medical Center
 Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
PORTAL HYPERTENSION. Tianjin Medical University LIU JIAN
 PORTAL HYPERTENSION Tianjin Medical University LIU JIAN DEFINITION Portal hypertension is present if portal venous pressure exceeds 10mmHg (1.3kPa). Normal portal venous pressure is 5 10mmHg (0.7 1.3kPa),
PORTAL HYPERTENSION Tianjin Medical University LIU JIAN DEFINITION Portal hypertension is present if portal venous pressure exceeds 10mmHg (1.3kPa). Normal portal venous pressure is 5 10mmHg (0.7 1.3kPa),
HEPATO-BILIARY IMAGING
 HEPATO-BILIARY IMAGING BY MAMDOUH MAHFOUZ MD PROF.OF RADIOLOGY CAIRO UNIVERSITY mamdouh.m5@gmail.com www.ssregypt.com CT ABDOMEN Indications Patient preparation Patient position Scanogram Fasting 4-6 hours
HEPATO-BILIARY IMAGING BY MAMDOUH MAHFOUZ MD PROF.OF RADIOLOGY CAIRO UNIVERSITY mamdouh.m5@gmail.com www.ssregypt.com CT ABDOMEN Indications Patient preparation Patient position Scanogram Fasting 4-6 hours
Evaluation of Liver Mass Lesions. American College of Gastroenterology 2013 Regional Postgraduate Course
 Evaluation of Liver Mass Lesions American College of Gastroenterology 2013 Regional Postgraduate Course Lewis R. Roberts, MB ChB, PhD Division of Gastroenterology and Hepatology Mayo Clinic College of
Evaluation of Liver Mass Lesions American College of Gastroenterology 2013 Regional Postgraduate Course Lewis R. Roberts, MB ChB, PhD Division of Gastroenterology and Hepatology Mayo Clinic College of
Surgical Workload, Outcome and Research Database: V1.1
 Technical Guidance for Surgical Workload, Outcome and Research Database: V1.1 Contents 1. Standard Indicators... 5 1.1. Activity Volume... 5 1.2. Average Length of Stay (Days)... 5 1.3. 2/7/30 day Re-admission
Technical Guidance for Surgical Workload, Outcome and Research Database: V1.1 Contents 1. Standard Indicators... 5 1.1. Activity Volume... 5 1.2. Average Length of Stay (Days)... 5 1.3. 2/7/30 day Re-admission
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Rokitansky-Aschoff sinuses are epithelial invaginations in the gallbladder wall that from as a result of increased gallbladder pressures.
 Anatomy The complexity of the biliary tree can be broken down into much simpler segments. The intrahepatic ducts converge to form the right and left hepatic ducts which exit the liver and join to become
Anatomy The complexity of the biliary tree can be broken down into much simpler segments. The intrahepatic ducts converge to form the right and left hepatic ducts which exit the liver and join to become
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
CASE 1 11/1/2016 HEPATOBILIARY IMAGING CASE PRESENTATIONS DECLARATION. Dr. Chirag Patel ORGAN IMAGING yr old lady
 HEPATOBILIARY IMAGING CASE PRESENTATIONS DECLARATION No financial disclosures or affiliations with commercial organisations No discussion of investigational or off-label use of medical devices, products
HEPATOBILIARY IMAGING CASE PRESENTATIONS DECLARATION No financial disclosures or affiliations with commercial organisations No discussion of investigational or off-label use of medical devices, products
Tata Memorial Centre s opinion is summarized as follows: 1. Given the type 1 stricture (as mentioned in the structured summary), assessment
, assessment") March 5 th 2016 Dear Ms. Malti Sinha, Thank you for reaching out to Tata Memorial Centre for an expert opinion in regard to assessing your treatment options. Navya Network is pleased to offer this online
March 5 th 2016 Dear Ms. Malti Sinha, Thank you for reaching out to Tata Memorial Centre for an expert opinion in regard to assessing your treatment options. Navya Network is pleased to offer this online
Jesse Civan, M.D. Medical Director, Jefferson Liver Tumor Center
 Liver Tumors Jesse Civan, M.D. Medical Director, Jefferson Liver Tumor Center Differential Diagnosis Malignant Metastatic from non-hepatic primary Hepatocellular carcinoma Cholangiocarcinoma Biliary cystcarcinoma
Liver Tumors Jesse Civan, M.D. Medical Director, Jefferson Liver Tumor Center Differential Diagnosis Malignant Metastatic from non-hepatic primary Hepatocellular carcinoma Cholangiocarcinoma Biliary cystcarcinoma
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases
 Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
LIVER SURGERY 2. Case 1. Med 5 Refresher Course (Surgery) 2013/14. Dr Sunny Cheung
 2013/14. Dr Sunny Cheung") LIVER SURGERY 2 Med 5 Refresher Course (Surgery) 2013/14 24 Jun 2013 Dr Sunny Cheung Case 1 50/M Sudden onset of epigastric pain Abdominal distension Confused HR 120 BP 80/50 Haemocue = 8 What should you
LIVER SURGERY 2 Med 5 Refresher Course (Surgery) 2013/14 24 Jun 2013 Dr Sunny Cheung Case 1 50/M Sudden onset of epigastric pain Abdominal distension Confused HR 120 BP 80/50 Haemocue = 8 What should you
Biliary tree dilation - and now what?
 Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
PANCREAS DUCTAL ADENOCARCINOMA PDAC
 CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
CONTENTS PANCREAS DUCTAL ADENOCARCINOMA PDAC I. What is the pancreas? II. III. IV. What is pancreas cancer? What is the epidemiology of Pancreatic Ductal Adenocarcinoma (PDAC)? What are the risk factors
Endoscopic management of postoperative bile duct injuries: a single center experience.
 1- Endoscopic management of postoperative bile duct injuries: a single center experience. BACKGROUND/AIM: Biliary endoscopic procedures may be less invasive than surgery for management of postoperative
1- Endoscopic management of postoperative bile duct injuries: a single center experience. BACKGROUND/AIM: Biliary endoscopic procedures may be less invasive than surgery for management of postoperative
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010
 Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Management of biliary injury after laparoscopic cholecystectomy N. Dayes Kings County Hospital Center & Long Island College Hospital 8/19/2010 Case Presentation 30 y.o. woman with 2 weeks of RUQ abdominal
Afternoon Session Cases
 Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Case Report Uncommon Mixed Type I and II Choledochal Cyst: An Indonesian Experience
 Case Reports in Surgery Volume 2013, Article ID 821032, 4 pages http://dx.doi.org/10.1155/2013/821032 Case Report Uncommon Mixed Type I and II Choledochal Cyst: An Indonesian Experience Fransisca J. Siahaya,
Case Reports in Surgery Volume 2013, Article ID 821032, 4 pages http://dx.doi.org/10.1155/2013/821032 Case Report Uncommon Mixed Type I and II Choledochal Cyst: An Indonesian Experience Fransisca J. Siahaya,
ACG Clinical Guideline: Diagnosis and Management of Focal Liver Lesions
 ACG Clinical Guideline: Diagnosis and Management of Focal Liver Lesions Jorge A. Marrero, MD, 1 Joseph Ahn, MD, FACG, 2 K. Rajender Reddy, MD, FACG 3 1 University of Texas at Southwestern, Dallas, Texas,
ACG Clinical Guideline: Diagnosis and Management of Focal Liver Lesions Jorge A. Marrero, MD, 1 Joseph Ahn, MD, FACG, 2 K. Rajender Reddy, MD, FACG 3 1 University of Texas at Southwestern, Dallas, Texas,
HEPATIC METASTASES. We can state 3 types of metastases depending on their treatment options:
 HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
5/17/2013. Pancreatic Cancer. Postgraduate Course in General Surgery CASE 1: CASE 1: Overview. Case presentation. Differential diagnosis
 Overview Case presentation Postgraduate Course in General Surgery Differential diagnosis Diagnosis and therapy Eric K. Nakakura Koloa, HI March 26, 2013 Outcomes CASE 1: CASE 1: A 78-year-old man developed
Overview Case presentation Postgraduate Course in General Surgery Differential diagnosis Diagnosis and therapy Eric K. Nakakura Koloa, HI March 26, 2013 Outcomes CASE 1: CASE 1: A 78-year-old man developed
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY
 A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
A LEADER IN ADVANCED ENDOSCOPY AND HEPATOBILIARY SURGERY St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center Welcome The St. Peter s Hospital Advanced Endoscopy & Hepatobiliary Center is a leader
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: van der Gaag NA, Rauws EAJ, van Eijck CHJ, et al. Preoperative
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: van der Gaag NA, Rauws EAJ, van Eijck CHJ, et al. Preoperative
Biliary MRI w Eovist
 Biliary MRI w Eovist Is there any added value? Elmar M. Merkle, MD Director of MR Imaging Duke University Medical Center elmar.merkle@duke.edu Declaration of Conflict of Interest or Relationship Research
Biliary MRI w Eovist Is there any added value? Elmar M. Merkle, MD Director of MR Imaging Duke University Medical Center elmar.merkle@duke.edu Declaration of Conflict of Interest or Relationship Research
Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association
 CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
Primary Hepatic Neoplasms. estimated 560,000 new cases per year. There is tremendous regional variation in incidence of
 Primary Hepatic Neoplasms Hepatocellular Carcinoma Incidence and Epidemiology Worldwide, hepatocellular carcinoma is the 3 rd most common causes of cancer death with an estimated 560,000 new cases per
Primary Hepatic Neoplasms Hepatocellular Carcinoma Incidence and Epidemiology Worldwide, hepatocellular carcinoma is the 3 rd most common causes of cancer death with an estimated 560,000 new cases per
Approach to the Patient with Liver Disease
 Approach to the Patient with Liver Disease Diagnosis of liver disease Careful history taking Physical examination Laboratory tests Radiologic examination and imaging studies Liver biopsy Liver diseases
Approach to the Patient with Liver Disease Diagnosis of liver disease Careful history taking Physical examination Laboratory tests Radiologic examination and imaging studies Liver biopsy Liver diseases
3/28/2012. Periampullary Tumors. Postgraduate Course in General Surgery CASE 1: CASE 1: Overview. Eric K. Nakakura Ko Olina, HI
 Overview Postgraduate Course in General Surgery Case presentation Differential diagnosis Diagnosis and therapy Outcomes Principles of palliative care Eric K. Nakakura Ko Olina, HI March 27, 2012 CASE 1:
Overview Postgraduate Course in General Surgery Case presentation Differential diagnosis Diagnosis and therapy Outcomes Principles of palliative care Eric K. Nakakura Ko Olina, HI March 27, 2012 CASE 1:
Biliary Tract Disease. Emmet Andrews Cork University Hospital 6 th September 2010
 Biliary Tract Disease Emmet Andrews Cork University Hospital 6 th September 2010 Overview Gallstones Biliary tract tumours Other conditions Acute acalculous cholecystitis Mirizzi s syndrome Primary Biliary
Biliary Tract Disease Emmet Andrews Cork University Hospital 6 th September 2010 Overview Gallstones Biliary tract tumours Other conditions Acute acalculous cholecystitis Mirizzi s syndrome Primary Biliary
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES
 JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
JOHN M UECKER, MD, FACS COMPLEX PANCREATICODUODENAL INJURIES THE PROBLEM DUODENAL / PANCREATIC INJURIES Difficult to diagnose Not very common Anatomic and physiologic challenges 90% rate of associated
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers
 Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Proximal Bile Duct Cancer: Contemporary Management. William R. Jarnagin, MD, FACS
 Proximal Bile Duct Cancer: Contemporary Management William R. Jarnagin, MD, FACS Biliary Tract Adenocarcinoma Spectrum of disease Intrahepatic (IHC) Hilar EH Gallbladder GB CBD Distal D PD Biliary Tract
Proximal Bile Duct Cancer: Contemporary Management William R. Jarnagin, MD, FACS Biliary Tract Adenocarcinoma Spectrum of disease Intrahepatic (IHC) Hilar EH Gallbladder GB CBD Distal D PD Biliary Tract
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
NAACCR Webinar Series 1
 Collecting Cancer Data: Liver 2013 2014 NAACCR Webinar Series June 5, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Liver 2013 2014 NAACCR Webinar Series June 5, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Bile Duct Injury during Lap Chole. Bile Duct Injury during cholecystectomy TOPICS. 1. Prevalence, mechanisms, prevention and diagnosis
 Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation
Bile Duct Injury during cholecystectomy Catherine HUBERT Jean-Fran François GIGOT Benoît t NAVEZ Division of Hepato-Biliary Biliary-Pancreatic Surgery Department of Abdominal Surgery and Transplantation
Radiofrequency Ablation of Liver Tumors
 Radiofrequency Ablation of Liver Tumors Michael M. Awad, Michael A. Choti Indications and Contraindications Indications Unresectable malignant tumors of the liver (e.g., hepatocellular carcinoma, colorectal
Radiofrequency Ablation of Liver Tumors Michael M. Awad, Michael A. Choti Indications and Contraindications Indications Unresectable malignant tumors of the liver (e.g., hepatocellular carcinoma, colorectal
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM
 A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
A CASE REPORT OF SPONTANEOUS BILOMA - AN ENIGMATIC SURGICAL PROBLEM *Sumanta Kumar Ghosh and Biswajit Mukherjee ESIC Medical College, Joka, Kolkata, India *Author for Correspondence ABSTRACT Occurrence
Original article: new surgical approaches to the Klatskin tumour
 Alimentary Pharmacology & Therapeutics Original article: new surgical approaches to the Klatskin tumour T. M. VAN GULIK*, S. DINANT*, O. R. C. BUSCH*, E. A. J. RAUWS, H. OBERTOP* & D. J. GOUMA Departments
Alimentary Pharmacology & Therapeutics Original article: new surgical approaches to the Klatskin tumour T. M. VAN GULIK*, S. DINANT*, O. R. C. BUSCH*, E. A. J. RAUWS, H. OBERTOP* & D. J. GOUMA Departments