Anaesthetic considerations and peri-operative risks in patients with liver disease
|
|
|
- Andrea Paulina Boone
- 5 years ago
- Views:
Transcription
1 Anaesthetic considerations and peri-operative risks in patients with liver disease Dr. C. K. Pandey Professor & Head Department of Anaesthesiology & Critical Care Medicine Institute of Liver and Biliary Sciences, New Delhi
2 Objectives Recognize which coexisting disease processes are associated with increased morbidity Understand which features of the patient s condition can be improved Realize that a simple operation does not always mean an equally simple or risk-free anaesthetic
3 Natural progression of chronic liver disease Chronic liver disease Compensated cirrhosis Decompensated cirrhosis Death
4
5
6 Risk scoring systems The risks are assessed in all surgical patients with liver disease: Child-Turcotte-Pugh Model for End-Stage Liver Disease (MELD) Scoring system Na + MELD
7 The Child-Turcotte-Pugh scoring system The risk of postoperative mortality and morbidity correlate well with the categorization of the patient as per the Child-Turcotte-Pugh (CTP) class of cirrhosis Scoring System assigns 1 to 3 points on the basis of five simple factors Sr. bilirubin Sr. albumin prothrombin time Ascites grade of encephalopathy
8 Risk scoring systems Variables Points Encephalopathy None 1 & 2 3 & 4 grade Ascites Absent Controlled Refractory Bilirubin mg/dl >2.0 Albumin gm/dl < 2.0 PT >6 Points Class One year survival Two year survival 5-6 A 100% 85% 7-9 B 81% 57% C 45% 35%
9 Model for end-stage liver disease (MELD) Scoring system The MELD scoring system was developed to prioritize eligibility for liver transplantation The MELD score is considered more objective and reliable because it is based on objective criteria i.e. serum bilirubin, serum creatinine and international normalized ratio (INR)
10 Model for end-stage liver disease MELD = 3.78 log e (bilirubin in mg/dl) log e (INR) log e (creatinine in mg/dl) (a bilirubin or creatinine value of less than 1.0 mg/dl is rounded to 1.0 mg/dl and the maximum creatinine value allowed is 4.0 mg/dl )
11 Strengths of the MELD score An objective metric using a continuous scale that lends itself to ranking patients based on disease severity It incorporates laboratory parameters that are easily available and reproducible Its validity as a robust mathematical model to assess mortality risk in patients with end-stage liver disease Superior to clinical judgment in identifying patients at risk of mortality
12 Evaluation MELD uses the patient's values for serum Bilirubin, serum Creatinine and the INR to predict survival. In interpreting the MELD Score in hospitalized patients, the 3 month mortality is: 40 or > <9 71.3% mortality 52.6% mortality 19.6% mortality 6.0% mortality 1.9% mortality
13 Open abdominal surgery MELD<10 :Survival rate 99% at 7 days 96% at 30 days 92% at 90 days CTP 5-6 :10% Mortality CTP 7-9 :30% Mortality MELD> 10 :Survival rates significantly lower CTP>9 :70 % Mortality Suman A.CleveJ Med 2006;73:
14 The relation between risk of 90-day mortality and individual MELD variables after adjustment for the other components. Gish RG. Liver Transpl 2007.
15 Na + MELD Serum sodium concentration - an important prognostic factor in patients with cirrhosis Addition of serum sodium into the MELD score predicts waiting list mortality better than MELD alone Serum sodium predicts mortality in patients listed for liver transplantation Hyponatremia is associated with neurologic dysfunction, refractory ascites, hepatorenal syndrome, and death from liver disease
16
17
18
19 Peri-operative risks Surgery in acute liver disease Nature of Surgery Type of surgery Anaesthetic factors
20 Surgery in acute liver disease
21 Surgery in acute liver disease Acute liver diseases have higher operative risk Acute viral and alcoholic hepatitis has poor outcomes in surgical patients Major elective surgery for a patient with suspected acute hepatitis should be deferred until the patient has recovered Patients with acute hepatitis of any cause are regarded as having increased risk
22 Surgery in alcoholic hepatitis Alcoholic hepatitis is a contraindication to elective surgery and increases perioperative mortality Laparotomy in patient with alcoholic hepatitis may have serious consequences The mortality rate was 58% among the 12 patients who underwent open liver biopsy, compared with 10% among the 39 patients who underwent percutaneous liver biopsy Abstinence from alcohol for 12 weeks resulted in dramatic improvement in hepatic inflammation and hyperbilirubinemia Greenwood SM, Leffler CT, Minkowitz S. The increased mortality rate of open liver biopsy in alcoholic hepatitis. Surg Gynecol Obstet 1972;134:600-4
23 Patients with acute liver are critically ill and all surgery other than liver transplantation is contraindicated
24 Nature of surgery
25 Emergency surgery 138 patients with cirrhosis undergoing non hepatic general surgical procedure 120% 100% 80% 51% 60% 40% 20% 8.70% 49% 47% Elective Emergency 0% Patients Mortality Neeff H et al J Gastrointest Surg 2011 High risk :Emergency surgery
26
27 TYPE OF SURGERY
28 Only MELD score, American Society of Anesthesiologists class, and age predicted mortality at 30 and 90 days, 1 year, and long-term independent of type of surgery
29 Type of surgery
30 Open abdominal surgery Fifty-three adult patients with cirrhosis undergoing abdominal surgery Patients undergoing hepatic surgery (resection or transplantation) or closed abdominal surgery (hernia repair) were excluded Total 13 patients (25%) had poor outcomes including 9 deaths (17%) Befeler AS, Palmer DE, Hoffman M, Longo W, Solomon H, Di Bisceglie AM. The safety of intra-abdominal surgery in patients with cirrhosis. Arch Surg 2005;140:
31 Open abdominal surgery Model for end-stage liver disease score and plasma hemoglobin levels lower than10 g/dl found to be independent predictors of poor outcomes A MELD score of 14 or greater was a better clinical predictor of poor outcome than CTP C Befeler AS, Palmer DE, Hoffman M, Longo W, Solomon H, Di Bisceglie AM. The safety of intra-abdominal surgery in patients with cirrhosis. Arch Surg 2005;140:
32 Open abdominal surgery The mortality rate was higher in patients with one or more of the followings: elevated bilirubin prolonged prothrombin time ascites decreased albumin encephalopathy portal hypertension emergent surgery Befeler AS, Palmer DE, Hoffman M, Longo W, Solomon H, Di Bisceglie AM. The safety of intra-abdominal surgery in patients with cirrhosis. Arch Surg 2005;140:
33 Obstructive jaundice Retrospective analysis 373 patients - risk factors for perioperative death were Hematocrit< 30% Sr Bilirubin >11 mg/dl Malignant cause of biliary obstruction Mortality 60 % if all 3 present 5% if none present If Benign Condition, preoperative optimization with ERCP Stenting External PTBD with radiology guidance Madical M/M - Ursodeoxycholic acid, lactulose
34 Cardiac surgery Safe in CTP A and selected CTP B Best cut of values for predicting mortality and hepatic decompensation CTP >7 & MELD >13 Clin Gastroenterol Hepatol 2004;2:
35 Laparoscopic cholecystectomy Laparoscopic cholecystectomy carries a low mortality rate. In a retrospective analysis of 226 patients with cirrhosis (Child-Pugh class A or B) who underwent laparoscopic cholecystectomy, only two died (0.88%) The reported mortality is low, but this figure is still significantly higher than in non-cirrhotic controls (0.01%) Yeh CN, Chen MF, Jan YY. Laparoscopic cholecystectomy in 226 cirrhotic patients. Experience of a single center in Taiwan. Surg Endosc 2002;16:
36 Laparoscopic cholecystectomy This suggest cutoff mark of MELD 8 for clearing patients with cirrhosis for laparoscopic cholecystectomy
37 Laparoscopic cholecystectomy Patients with cirrhosis undergone laparoscopic cholecystectomy, 2 out of the 33 (6%) patients with cirrhosis died at 90 days, compared with no mortality in 31 matched controls The rate of morbidity was 33% vs. 17% in the study Perkins L, Jeffries M, Patel T. Utility of preoperative scores for predicting morbidity after cholecystectomy in patients with cirrhosis. Clin Gastroenterol Hepatol 2004;2:
38 Asymptomatic gallstone disease? Patients with cirrhosis who have incidental GSD on ultrasonography should not undergo cholecystectomy unless the gallstones are symptomatic Because chances of liver function to deteriorate after surgery
39 Cholecystectomy: open or laparoscopic Retrospectively analysis 50 patients who had undergone cholecystectomy for symptomatic gallstone disease The procedure was open in half of the patients and laparoscopic in the other half All patients had Child-Pugh class A or B cirrhosis. Poggio JL, Rowland CM, Gores GJ, Nagorney DM, Donohue JH. A comparison of laparoscopic and open cholecystectomy in patients with compensated cirrhosis and asymptomatic gallstone disease. Surgery 2000;127:
40 Cholecystectomy: open or laparoscopic The study concluded that laparoscopic cholecystectomy is associated with statistically significant reductions in operating room time, blood loss, and length of hospital stay There was no deaths in either group Laparoscopic cholecystectomy should be recommended for patients with liver disease without decompensation
41 Mortality rates in patients undergone cholecystectomy with or without cirrhosis Variables Patients with normal liver function Patients with cirrhosis (P T < 2.5 second than control) Patient with cirrhosis PT > 2.5 seconds than control Mortality 1% 9% 83% Aranha GV, Sontag SJ, Greenlee HB. Cholecystectomy in cirrhotic patients: a formidable operation. Am J Surg 1982;143:55-60.
42 Preoperative variables and mortality rates of survivors and non-survivors of abdominal surgery Preoperative variables % of mortality if factors present % of mortality if factors absent Child Class A 10 B 31 C 76 Ascites Emergency Surgery Bilirubin > 3 mg/dl Albumin < 3gm/dl Prothrombin time > 1.5second above control WBC count > P < 0.01 for all variables
43 Preoperative variable associated with mortality Preoperative variable Mortality % if present Pulmonary failure 100 Cardiac failure 92 Requirement of > 2 antibiotics 82 Renal failure 73 Hepatic failure 66 Gastrointestinal bleeding 86 Required 2 nd operation 81 Positive cultures 61 Blood requirement > 2 units 69 Blood requirement < 2 units 22 Garrison RN, Cryer HM, Howard DA, Polk HC Jr. Clarification of risk factors for abdominal operations in patients with hepatic cirrhosis. Ann Surg 1984;199:
44 Anesthetic considerations
45 Anesthetic considerations The risk of surgery cannot be separated from the risk of anesthesia Anesthesia can affect the liver by reducing its blood flow.
46 Anesthetic considerations animals studies have shown that under the conditions of stress, hepatic blood flow increases to compensate for the reduced portal blood flow but patients with liver disease, especially cirrhosis, cannot compensate for the reduced portal blood flow, which may cause hepatic dysfunction
47 Anesthetic considerations In healthy volunteers, hepatic blood flow decreased by 35% to 42% in the first 30 minutes of induction of anesthesia
48 Anesthetic considerations The anesthetic agents Halothane and Enflurane reduce hepatic arterial blood flow These effects are minimal with Isoflurane Inhalational agents Isoflurane, Desflurane, and Sevoflurane undergo hepatic metabolism, extent of which is 0.2% for isoflurane, 2-4% for Enflurane, and 20% for Halothane Isoflurane has become the inhalation agent of choice in patients with liver disease
49 Anesthetic considerations Anesthetic agents, sedatives, and skeletal muscle relaxants can all have adverse effects The actions of neuromuscular blocking agents may be prolonged in patients with liver disease because of reduced pseudocholinesterase activity, decreased biliary excretion, and larger volume of distribution Metabolism of Atracurium is by Hoffman reaction and does not depend on liver Use of Atracurium is safe and is recommended in liver disease
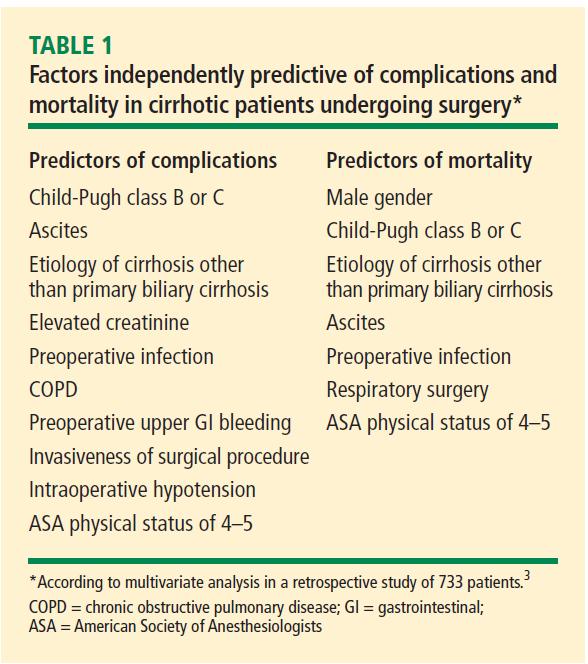
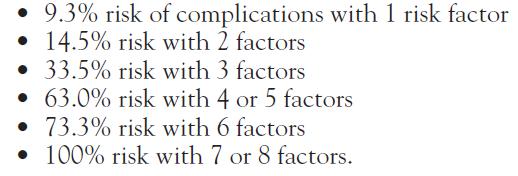
50 Anesthetic considerations The use of various narcotics like fentanyl, sufentanil and sedatives like Oxazepam, Lorazepam, is recommended No correlation could however be established in patients with cirrhosis undergoing cardiac surgery and hepatic decompensation or mortality between the use of Enflurane, Isoflurane, Fentanyl, Sufentanil, Midazolam, or Morphine The type of anesthetic management either general anesthesia, regional anesthesia, or monitored anesthesia care did not affect the mortality in one of the largest reported series of 733 patients. Ziser A, Plevak DJ, Wiesner RH, Rakela J, Offord KP, Brown DL. Morbidity and mortality in cirrhotic patients undergoing anesthesia and surgery. Anesthesiology 1999;90:42-53
51 Conclusion Various type of surgeries can be safely performed in CTP score 7 CTP & MELD scores predict morbidity and mortality in cirrhotics In acute liver diseases surgery should be avoided Emergency surgery carries high mortality in cirrhotics
52 Conclusion Abdominal wall surgery may be safely performed in Child-Pugh in A & B Laparoscopic surgery should be preferred over open surgeries Asymptomatic GSD should not be operated


53


54 WELCOME TO TRANCRIT 2012 AT ILBS
Predicting Outcome After Cardiac Surgery in Patients With Cirrhosis: A Comparison of Child Pugh and MELD Scores
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2004;2:719 723 Predicting Outcome After Cardiac Surgery in Patients With Cirrhosis: A Comparison of Child Pugh and MELD Scores AMITABH SUMAN,* DAVID S. BARNES,*
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2004;2:719 723 Predicting Outcome After Cardiac Surgery in Patients With Cirrhosis: A Comparison of Child Pugh and MELD Scores AMITABH SUMAN,* DAVID S. BARNES,*
Update in abdominal Surgery in cirrhotic patients
 Update in abdominal Surgery in cirrhotic patients Safi Dokmak HBP department and liver transplantation Beaujon Hospital, Clichy, France Cairo, 5 April 2016 Cirrhosis Prevalence in France (1%)* Patients
Update in abdominal Surgery in cirrhotic patients Safi Dokmak HBP department and liver transplantation Beaujon Hospital, Clichy, France Cairo, 5 April 2016 Cirrhosis Prevalence in France (1%)* Patients
Peri-operative Abnormal Liver Function Test
 Peri-operative Abnormal Liver Function Test Naichaya Chamroonkul. MD. Division of Gastroenterology and Hepatology,Department of Internal Medicine Faculty of Medicine, Prince of Songkla University Liver
Peri-operative Abnormal Liver Function Test Naichaya Chamroonkul. MD. Division of Gastroenterology and Hepatology,Department of Internal Medicine Faculty of Medicine, Prince of Songkla University Liver
An assessment of different scoring systems in cirrhotic patients undergoing nontransplant surgery
 The American Journal of Surgery (2012) 203, 589 593 North Pacific Surgical Association An assessment of different scoring systems in cirrhotic patients undergoing nontransplant surgery Marlin Wayne Causey,
The American Journal of Surgery (2012) 203, 589 593 North Pacific Surgical Association An assessment of different scoring systems in cirrhotic patients undergoing nontransplant surgery Marlin Wayne Causey,
Chronic liver failure affects multiple organ systems and
 ORIGINAL ARTICLES Model for End-Stage Liver Disease (MELD) Predicts Nontransplant Surgical Mortality in Patients With Cirrhosis Patrick G. Northup, MD,* Ryan C. Wanamaker, MD, Vanessa D. Lee, MD, Reid
ORIGINAL ARTICLES Model for End-Stage Liver Disease (MELD) Predicts Nontransplant Surgical Mortality in Patients With Cirrhosis Patrick G. Northup, MD,* Ryan C. Wanamaker, MD, Vanessa D. Lee, MD, Reid
Home Intravenous Antibiotic Treatment for Intractable Cholangitis in Biliary Atresia
 Home Intravenous Antibiotic Treatment for Intractable Cholangitis in Biliary Atresia Hye Kyung Chang, Jung-Tak Oh, Seung Hoon Choi, Seok Joo Han Division of Pediatric Surgery, Department of Surgery, Yonsei
Home Intravenous Antibiotic Treatment for Intractable Cholangitis in Biliary Atresia Hye Kyung Chang, Jung-Tak Oh, Seung Hoon Choi, Seok Joo Han Division of Pediatric Surgery, Department of Surgery, Yonsei
For patients with cirrhosis, increased operative risk relative
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:451 457 ORIGINAL ARTICLES LIVER, PANCREAS, AND BILIARY TRACT Factors That Predict Outcome of Abdominal Operations in Patients With Advanced Cirrhosis DANA
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:451 457 ORIGINAL ARTICLES LIVER, PANCREAS, AND BILIARY TRACT Factors That Predict Outcome of Abdominal Operations in Patients With Advanced Cirrhosis DANA
Patterns of abnormal LFTs and their differential diagnosis
 Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function / liver function
Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function / liver function
The burden of chronic liver disease continues to grow dramatically
 Session 2B: Liver Disease THE RISKS OF SURGERY IN PATIENTS WITH LIVER DISEASE Joseph K. Lim, MD, FACG The burden of chronic liver disease continues to grow dramatically in the United States, driven primarily
Session 2B: Liver Disease THE RISKS OF SURGERY IN PATIENTS WITH LIVER DISEASE Joseph K. Lim, MD, FACG The burden of chronic liver disease continues to grow dramatically in the United States, driven primarily
Liver Transplantation Evaluation: Objectives
 Liver Transplantation Evaluation: Essential Work-Up Curtis K. Argo, MD, MS VGS/ACG Regional Postgraduate Course Williamsburg, VA September 13, 2015 Objectives Discuss determining readiness for transplantation
Liver Transplantation Evaluation: Essential Work-Up Curtis K. Argo, MD, MS VGS/ACG Regional Postgraduate Course Williamsburg, VA September 13, 2015 Objectives Discuss determining readiness for transplantation
Total Joint Arthroplasty In Patients With Liver Cirrhosis: A Systematic Review
 Total Joint Arthroplasty In Patients With Liver Cirrhosis: A Systematic Review Fofiu Alexandru, Msc, PhD Student Bataga Simona, MD, PhD Fofiu Crina, Msc, PhD Student Bataga Tiberiu, MD, PhD University
Total Joint Arthroplasty In Patients With Liver Cirrhosis: A Systematic Review Fofiu Alexandru, Msc, PhD Student Bataga Simona, MD, PhD Fofiu Crina, Msc, PhD Student Bataga Tiberiu, MD, PhD University
Patterns of abnormal LFTs and their differential diagnosis
 Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function tests / tests of
Patterns of abnormal LFTs and their differential diagnosis Professor Matthew Cramp South West Liver Unit and Peninsula Schools of Medicine and Dentistry, Plymouth Outline liver function tests / tests of
Chronic Hepatic Disease
 Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
Chronic Hepatic Disease 10 th Leading Cause of Death Liver Functions Energy Metabolism Protein Synthesis Solubilization, Transport, and Storage Protects and Clears drugs, damaged cells Causes of Liver
LIVER. Question 1 ~ Anatomy. Answer 1 ~ Anatomy 1/5/2018. SEMCME Board Review January 11-12, 2017
 SEMCME Board Review January 11-12, 2017 Surgical Treatment of Hepatobiliary and Splenic Disorders Michael J. Jacobs, MD, FACS, FICS Clinical Professor of Surgery- MSU CHM Associate Chair of Surgery Director
SEMCME Board Review January 11-12, 2017 Surgical Treatment of Hepatobiliary and Splenic Disorders Michael J. Jacobs, MD, FACS, FICS Clinical Professor of Surgery- MSU CHM Associate Chair of Surgery Director
Surgical Treatment of Hepatobiliary and Splenic Disorders
 SEMCME Board Review January 10-11, 2019 Surgical Treatment of Hepatobiliary and Splenic Disorders Michael J. Jacobs, MD, FACS, FICS Clinical Professor of Surgery- MSU CHM Associate Chair of Surgery Director
SEMCME Board Review January 10-11, 2019 Surgical Treatment of Hepatobiliary and Splenic Disorders Michael J. Jacobs, MD, FACS, FICS Clinical Professor of Surgery- MSU CHM Associate Chair of Surgery Director
Preoperative Risk Assessment for Patients with Liver Disease
 Preoperative Risk Assessment for Patients with Liver Disease Shahid M. Malik, MD, Jawad Ahmad, MD, MRCP* KEYWORDS Operative risk Liver disease Cirrhosis CTP score MELD Underlying liver disease has effects
Preoperative Risk Assessment for Patients with Liver Disease Shahid M. Malik, MD, Jawad Ahmad, MD, MRCP* KEYWORDS Operative risk Liver disease Cirrhosis CTP score MELD Underlying liver disease has effects
Liver failure &portal hypertension
 Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Liver failure &portal hypertension Objectives: by the end of this lecture each student should be able to : Diagnose liver failure (acute or chronic) List the causes of acute liver failure Diagnose and
Contraindications. Indications. Complications. Currently TIPS is considered second or third line therapy for:
 Contraindications Absolute Relative Primary prevention variceal bleeding HCC if centrally located Active congestive heart failure Obstruction all hepatic veins Thomas D. Boyer, M.D. University of Arizona
Contraindications Absolute Relative Primary prevention variceal bleeding HCC if centrally located Active congestive heart failure Obstruction all hepatic veins Thomas D. Boyer, M.D. University of Arizona
Workup of a Solid Liver Lesion
 Workup of a Solid Liver Lesion Joseph B. Cofer MD FACS Chief Quality Officer Erlanger Health System Affiliate Professor of Surgery UTHSC-Chattanooga I have no financial or other relationships with any
Workup of a Solid Liver Lesion Joseph B. Cofer MD FACS Chief Quality Officer Erlanger Health System Affiliate Professor of Surgery UTHSC-Chattanooga I have no financial or other relationships with any
Learning Objectives. After attending this presentation, participants will be able to:
 Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
Learning Objectives After attending this presentation, participants will be able to: Describe HCV in 2015 Describe how to diagnose advanced liver disease and cirrhosis Identify the clinical presentation
Management of Cirrhotic Complications Uncontrolled Ascites. Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University
 Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
Management of Cirrhotic Complications Uncontrolled Ascites Siwaporn Chainuvati, MD Siriraj Hospital Mahidol University Topic Definition, pathogenesis Current therapeutic options Experimental treatments
The Yellow Patient. Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust
 The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
The Yellow Patient Dr Chiradeep Raychaudhuri, Consultant Hepatologist, Hull University Teaching Hospitals NHS Trust there s a yellow patient in bed 40. It s one of yours. Liver Cirrhosis Why.When.What.etc.
Posthepatectomy Liver Failure. C. Jeske
 Posthepatectomy Liver Failure C. Jeske Introduction Major source of morbidity and mortality after liver resection Devastating complication Little treatment Incidence: 4-19% Recently < 10% Mortality following
Posthepatectomy Liver Failure C. Jeske Introduction Major source of morbidity and mortality after liver resection Devastating complication Little treatment Incidence: 4-19% Recently < 10% Mortality following
How to Address an Inappropriately high Mortality Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion
 How to Address an Inappropriately high Mortality Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion Disclosure Slide No COI and no disclosures. Hospital Mortality rate : is it
How to Address an Inappropriately high Mortality Rate? Joe Sharma, MD Associate Professor of Surgery NSQIP Surgical Champion Disclosure Slide No COI and no disclosures. Hospital Mortality rate : is it
Module 1 Introduction of hepatitis
 Module 1 Introduction of hepatitis 1 Training Objectives At the end of the module, trainees will be able to ; Demonstrate improved knowledge of the global epidemiology of the viral hepatitis Understand
Module 1 Introduction of hepatitis 1 Training Objectives At the end of the module, trainees will be able to ; Demonstrate improved knowledge of the global epidemiology of the viral hepatitis Understand
Information for patients (and their families) waiting for liver transplantation
 waiting for liver transplantation") Information for patients (and their families) waiting for liver transplantation Waiting list? What is liver transplant? Postoperative conditions? Ver.: 5/2017 1 What is a liver transplant? Liver transplantation
Information for patients (and their families) waiting for liver transplantation Waiting list? What is liver transplant? Postoperative conditions? Ver.: 5/2017 1 What is a liver transplant? Liver transplantation
Severity and Mortality Prediction in Chronic Liver Disease using Child PUGH and MELD scales
 International Journal of Advanced Biotechnology and Research (IJABR) ISSN 0976-2612, Online ISSN 2278 599X, Vol-10, Issue-1, 2019, pp519-524 http://www.bipublication.com Research Article Severity and Mortality
International Journal of Advanced Biotechnology and Research (IJABR) ISSN 0976-2612, Online ISSN 2278 599X, Vol-10, Issue-1, 2019, pp519-524 http://www.bipublication.com Research Article Severity and Mortality
Chronic liver failure Assessment for liver transplantation
 Chronic liver failure Assessment for liver transplantation Liver Transplantation Dealing with the organ shortage Timing of listing must reflect length on waiting list Ethical issues Justice, equity, utility
Chronic liver failure Assessment for liver transplantation Liver Transplantation Dealing with the organ shortage Timing of listing must reflect length on waiting list Ethical issues Justice, equity, utility
Laparoscopic Cholecystectomy in Child-Pugh Class C Cirrhotic Patients
 SCIENTIFIC PAPER Laparoscopic Cholecystectomy in Child-Pugh Class C Cirrhotic Patients Giuseppe Currò, MD, Giuliano Iapichino, MD, Giuseppinella Melita, MD, Cesare Lorenzini, MD, Eugenio Cucinotta, MD
SCIENTIFIC PAPER Laparoscopic Cholecystectomy in Child-Pugh Class C Cirrhotic Patients Giuseppe Currò, MD, Giuliano Iapichino, MD, Giuseppinella Melita, MD, Cesare Lorenzini, MD, Eugenio Cucinotta, MD
Ammonia level at admission predicts in-hospital mortality for patients with alcoholic hepatitis
 Gastroenterology Report, 5(3), 2017, 232 236 doi: 10.1093/gastro/gow010 Advance Access Publication Date: 1 May 2016 Original article ORIGINAL ARTICLE Ammonia level at admission predicts in-hospital mortality
Gastroenterology Report, 5(3), 2017, 232 236 doi: 10.1093/gastro/gow010 Advance Access Publication Date: 1 May 2016 Original article ORIGINAL ARTICLE Ammonia level at admission predicts in-hospital mortality
Protocol for daclatasvir (Daklinza ) Approved October 2015 (updated February 2018)
 Approved October 2015 (updated February 2018)") PREFERRED AGENTS: (See drug specific NOTES for exceptions.) Protocol for daclatasvir (Daklinza ) Approved October 2015 (updated February 2018) https://providers.amerigroup.com For genotype 1, Mavyret and
PREFERRED AGENTS: (See drug specific NOTES for exceptions.) Protocol for daclatasvir (Daklinza ) Approved October 2015 (updated February 2018) https://providers.amerigroup.com For genotype 1, Mavyret and
PAPER. Umbilical Hernia Repair in Patients With Signs
 PAPER Umbilical Hernia Repair in Patients With Signs of Portal Hypertension Surgical Outcome and Predictors of Mortality Sung W. Cho, MB, BS, MSc; Neil Bhayani, MD; Pippa Newell, MD; Maria A. Cassera,
PAPER Umbilical Hernia Repair in Patients With Signs of Portal Hypertension Surgical Outcome and Predictors of Mortality Sung W. Cho, MB, BS, MSc; Neil Bhayani, MD; Pippa Newell, MD; Maria A. Cassera,
Preoperative elective transjugular intrahepatic portosystemic shunt for cirrhotic patients undergoing abdominal surgery
 REVIEW ARTICLE Annals of Gastroenterology (2017) 31, 330-337 Preoperative elective transjugular intrahepatic portosystemic shunt for cirrhotic patients undergoing abdominal Deepanshu Jain a, Ejaz Mahmood
REVIEW ARTICLE Annals of Gastroenterology (2017) 31, 330-337 Preoperative elective transjugular intrahepatic portosystemic shunt for cirrhotic patients undergoing abdominal Deepanshu Jain a, Ejaz Mahmood
DISCLOSURES. This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea
 DISCLOSURES This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea Cardea Services is approved as a provider of continuing nursing education by Montana Nurses Association,
DISCLOSURES This activity is jointly provided by Northwest Portland Area Indian Health Board and Cardea Cardea Services is approved as a provider of continuing nursing education by Montana Nurses Association,
ESLD a Guide for HIV Physicians. Marion Peters University of California San Francisco June 2015
 ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche Natural
ESLD a Guide for HIV Physicians Marion Peters University of California San Francisco June 2015 Disclosures Honararia from Johnson and Johnson Roche Merck Gilead Spouse employee of Hoffman La Roche Natural
Hepatocellular Carcinoma: Diagnosis and Management
 Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Bariatric Surgery For Patients With End-Organ Failure
 Bariatric Surgery For Patients With End-Organ Failure Arnold D. Salzberg, M.D. Andrew M. Posselt, M.D., PhD Divisions of Transplant and Minimally Invasive Surgery University of California, San Francisco
Bariatric Surgery For Patients With End-Organ Failure Arnold D. Salzberg, M.D. Andrew M. Posselt, M.D., PhD Divisions of Transplant and Minimally Invasive Surgery University of California, San Francisco
Denver Shunts vs TIPS for Ascites
 Denver Shunts vs TIPS for Ascites Hooman Yarmohammadi MD Assistant Professor of Radiology Interventional Radiology & Image Guided Therapies Memorial Sloan-Kettering Cancer Center, New York, USA Hooman
Denver Shunts vs TIPS for Ascites Hooman Yarmohammadi MD Assistant Professor of Radiology Interventional Radiology & Image Guided Therapies Memorial Sloan-Kettering Cancer Center, New York, USA Hooman
Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association
 CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
CIRRHOSIS AND PORTAL HYPERTENSION Cirrhosis and Portal Hypertension Gastroenterology Teaching Project American Gastroenterological Association WHAT IS CIRRHOSIS? What is Cirrhosis? DEFINITION OF CIRRHOSIS
Suspected Isoflurane Induced Hepatitis from Cross Sensitivity in a Post Transplant for Fulminant Hepatitis from Halothane.
 ISPUB.COM The Internet Journal of Anesthesiology Volume 25 Number 1 Suspected Isoflurane Induced Hepatitis from Cross Sensitivity in a Post Transplant for Fulminant Hepatitis from Halothane. V Sampathi,
ISPUB.COM The Internet Journal of Anesthesiology Volume 25 Number 1 Suspected Isoflurane Induced Hepatitis from Cross Sensitivity in a Post Transplant for Fulminant Hepatitis from Halothane. V Sampathi,
Abdominal wall hernia in cirrhotic patients: emergency surgery results in higher morbidity and mortality
 Andraus et al. BMC Surgery (2015) 15:65 DOI 10.1186/s12893-015-0052-y RESEARCH ARTICLE Open Access Abdominal wall hernia in cirrhotic patients: emergency surgery results in higher morbidity and mortality
Andraus et al. BMC Surgery (2015) 15:65 DOI 10.1186/s12893-015-0052-y RESEARCH ARTICLE Open Access Abdominal wall hernia in cirrhotic patients: emergency surgery results in higher morbidity and mortality
Steps in Assessing Fibrosis 4/30/2015. Overview of Liver Disease Associated With HCV
 Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
Overview of Liver Disease Associated With HCV Marion G. Peters, MD John V. Carbone, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco San Francisco,
Surgery in the Patient With Liver Disease
 TUSHAR PATEL, MBCHB easesare poorly understood but are greater with increased impairment of hepatic function. dentifying preexisting problems that could be optimally and appropriately managed before surgery
TUSHAR PATEL, MBCHB easesare poorly understood but are greater with increased impairment of hepatic function. dentifying preexisting problems that could be optimally and appropriately managed before surgery
EDUCATION PRACTICE. Management of Refractory Ascites. Clinical Scenario. The Problem
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2005;3:1187 1191 EDUCATION PRACTICE Management of Refractory Ascites ANDRÉS CÁRDENAS and PERE GINÈS Liver Unit, Institute of Digestive Diseases, Hospital Clínic,
End-Stage Liver Disease (ESLD): A Guide for HIV Physicians
: A Guide for HIV Physicians") Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
Slide 1 of 32 End-Stage Liver Disease (ESLD): A Guide for HIV Physicians Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California
Assessment of Liver Function: Implications for HCC Treatment
 Assessment of Liver Function: Implications for HCC Treatment A/P Dan Yock Young MBBS, PhD, MRCP, MMed. FAMS Chair, University Medicine Cluster. NUHS Head, Department of Medicine, National University of
Assessment of Liver Function: Implications for HCC Treatment A/P Dan Yock Young MBBS, PhD, MRCP, MMed. FAMS Chair, University Medicine Cluster. NUHS Head, Department of Medicine, National University of
Management of Cirrhosis Related Complications
 Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Management of Cirrhosis Related Complications Ke-Qin Hu, MD, FAASLD Professor of Clinical Medicine Director of Hepatology University of California, Irvine Disclosure I have no disclosure related to this
Management of Decompensated Chronic Hepatitis B
 Management of Decompensated Chronic Hepatitis B Dr James YY Fung, FRACP, MD Department of Medicine The University of Hong Kong Liver Transplant Center Queen Mary Hospital State Key Laboratory for Liver
Management of Decompensated Chronic Hepatitis B Dr James YY Fung, FRACP, MD Department of Medicine The University of Hong Kong Liver Transplant Center Queen Mary Hospital State Key Laboratory for Liver
Hepatitis C: How sick can we treat? Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of
 Hepatitis C: How sick can we treat? Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology www.livermd.org HCV in advanced disease In principle
Hepatitis C: How sick can we treat? Robert S. Brown, Jr., MD, MPH Vice Chair, Transitions of Care Interim Chief, Division of Gastroenterology & Hepatology www.livermd.org HCV in advanced disease In principle
Causes of Liver Disease in US
 Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
Learning Objectives Updates in Outpatient Cirrhosis Management Jennifer Guy, MD MAS Director, Liver Cancer Program California Pacific Medical Center guyj@sutterhealth.org Review cirrhosis epidemiology,
B C Outlines. Child-Pugh scores
 B C 2016-12-09 Outlines Child-Pugh scores CT MRI Fibroscan / ARFI Histologic Scoring Systems for Fibrosis Fibrosis METAVIR Ishak None 0 0 Portal fibrosis (some) 1 1 Portal fibrosis (most) 1 2 Bridging
B C 2016-12-09 Outlines Child-Pugh scores CT MRI Fibroscan / ARFI Histologic Scoring Systems for Fibrosis Fibrosis METAVIR Ishak None 0 0 Portal fibrosis (some) 1 1 Portal fibrosis (most) 1 2 Bridging
This survey aims to look at individual practice and can be completed by any healthcare professional.
 This survey aims to look at individual practice and can be completed by any healthcare professional. If you have any questions about how this form should be completed please contact Dr Grace Ting (ghlting@doctors.net.uk)
This survey aims to look at individual practice and can be completed by any healthcare professional. If you have any questions about how this form should be completed please contact Dr Grace Ting (ghlting@doctors.net.uk)
Ascites Management. Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology
 Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
Ascites Management Atif Zaman, MD MPH Oregon Health & Science University Professor of Medicine Division of Gastroenterology and Hepatology Disclosure 1. The speaker Atif Zaman, MD MPH have no relevant
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist. K V Speeg, MD, PhD UT Health San Antonio
 The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
The Continuum of Care for Advanced Liver Disease: Partnering with the Liver Specialist K V Speeg, MD, PhD UT Health San Antonio Objectives Review staging of liver disease Review consequences of end-stage
ORIGINAL ARTICLE. Jun Zheng 1, Rong-chun Xing 1, Wei-hong Zheng 2, Wei Liu 1, Ru-cheng Yao 1, Xiao-song Li 1, Jian-ping Du 1, Lin Li 1.
 JBUON 2017; 22(3): 709-713 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE A comparative study on postoperative mortality prediction of SFLI scoring
JBUON 2017; 22(3): 709-713 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE A comparative study on postoperative mortality prediction of SFLI scoring
Hepatitis C: New Antivirals in the Liver Transplant Setting. Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona
 Hepatitis C: New Antivirals in the Liver Transplant Setting Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Patient survival Hepatitis C and Liver Transplantation Years after transplantation
Hepatitis C: New Antivirals in the Liver Transplant Setting Maria Carlota Londoño Liver Unit Hospital Clínic Barcelona Patient survival Hepatitis C and Liver Transplantation Years after transplantation
GI bleeding in chronic liver disease
 GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
GI bleeding in chronic liver disease Stuart McPherson Consultant Hepatologist Liver Unit, Freeman Hospital, Newcastle upon Tyne and Institute of Cellular Medicine, Newcastle University. Case 54 year old
Evaluating HIV Patient for Liver Transplantation. Marion G. Peters, MD Professor of Medicine University of California San Francisco USA
 Evaluating HIV Patient for Liver Transplantation Marion G. Peters, MD Professor of Medicine University of California San Francisco USA Slide 2 ESLD and HIV Liver disease has become a major cause of death
Evaluating HIV Patient for Liver Transplantation Marion G. Peters, MD Professor of Medicine University of California San Francisco USA Slide 2 ESLD and HIV Liver disease has become a major cause of death
In patients undergoing cardiovascular operations, advanced
 Risk Factor Analysis in Patients With Liver Cirrhosis Undergoing Cardiovascular Operations Akimasa Morisaki, MD, Mitsuharu Hosono, MD, Yasuyuki Sasaki, MD, Shoji Kubo, MD, Hidekazu Hirai, MD, Shigefumi
Risk Factor Analysis in Patients With Liver Cirrhosis Undergoing Cardiovascular Operations Akimasa Morisaki, MD, Mitsuharu Hosono, MD, Yasuyuki Sasaki, MD, Shoji Kubo, MD, Hidekazu Hirai, MD, Shigefumi
Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL
 Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL Terminology Acute decompensation of cirrhosis - stable patient with sudden deterioration Acute-on-chronic liver failure
Management of Acute Decompensation of Cirrhosis JOHN O GRADY KING S COLLEGE HOSPITAL Terminology Acute decompensation of cirrhosis - stable patient with sudden deterioration Acute-on-chronic liver failure
JMSCR Vol 05 Issue 11 Page November 2017
 www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 71.58 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i11.33 Prevalence of Hyponatremia among patients
www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 71.58 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i11.33 Prevalence of Hyponatremia among patients
The Management of Ascites & Hepatorenal Syndrome. Florence Wong University of Toronto. Falk Symposium March 14, 2008
 The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
The Management of Ascites & Hepatorenal Syndrome Florence Wong University of Toronto Falk Symposium March 14, 2008 Management of Ascites Sodium Restriction Mandatory at all stages of ascites in order to
Hepatocytes produce. Proteins Clotting factors Hormones. Bile Flow
 R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
R.J.Bailey MD Hepatocytes produce Proteins Clotting factors Hormones Bile Flow Trouble.. for the liver! Trouble for the Liver Liver Gall Bladder Common Alcohol Hep C Fatty Liver Cancer Drugs Viruses Uncommon
SOLAR-1 (Cohorts A and B)
") Phase 2 Treatment Naïve and Treatment Experienced Ledipasvir-Sofosbuvir + RBV in HCV GT 1,4 and Advanced Liver Disease SOLAR-1 (Cohorts A and B) Charlton M, al. Gastroenterology. 2015; 149:649-59. Ledipasvir-Sofosbuvir
Phase 2 Treatment Naïve and Treatment Experienced Ledipasvir-Sofosbuvir + RBV in HCV GT 1,4 and Advanced Liver Disease SOLAR-1 (Cohorts A and B) Charlton M, al. Gastroenterology. 2015; 149:649-59. Ledipasvir-Sofosbuvir
SOLAR-1 (Cohorts A and B)
") Phase 2 Treatment Naïve and Treatment Experienced Ledipasvir-Sofosbuvir + RBV in HCV GT 1,4 and Advanced Liver Disease SOLAR-1 (Cohorts A and B) Charlton M, al. Gastroenterology. 2015; [Epub ahead of print]
Phase 2 Treatment Naïve and Treatment Experienced Ledipasvir-Sofosbuvir + RBV in HCV GT 1,4 and Advanced Liver Disease SOLAR-1 (Cohorts A and B) Charlton M, al. Gastroenterology. 2015; [Epub ahead of print]
Clinical Controversies in Perioperative Medicine
 Update on Perioperative Medicine Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Medications & Perioperative
Update on Perioperative Medicine Clinical Controversies in Perioperative Medicine Hugo Quinny Cheng, MD Division of Hospital Medicine University of California, San Francisco Cardiac Medications & Perioperative
Indian Journal of Basic and Applied Medical Research; June 2017: Vol.-6, Issue- 3, P
 Original article: Study of usefulness of Discriminant Function (DF) and Glasgow Alcoholic Hepatitis Score (GAHS) in treatment of patients of Alcoholic Hepatitis in Indian Population Dr Mugdha Thakur, Dr
Original article: Study of usefulness of Discriminant Function (DF) and Glasgow Alcoholic Hepatitis Score (GAHS) in treatment of patients of Alcoholic Hepatitis in Indian Population Dr Mugdha Thakur, Dr
During the course of the 12 month fellowship, candidates will attend at least one international liver meeting (generally AASLD).
.") Hepatology and Liver Transplantation fellowship Length: 1 year Number of positions: 2 Type of fellowship: Clinical and Research Fellowship Director: Dr. Deschenes McGill University Health Centre Fellowship
Hepatology and Liver Transplantation fellowship Length: 1 year Number of positions: 2 Type of fellowship: Clinical and Research Fellowship Director: Dr. Deschenes McGill University Health Centre Fellowship
Effects of Liver Disease on Pharmacokinetics
 Effects of Liver Disease on Pharmacokinetics Juan J.L. Lertora, M.D., Ph.D. Director Clinical Pharmacology Program October 31, 2013 National Institutes of Health Clinical Center 1 GOALS of Effects of Liver
Effects of Liver Disease on Pharmacokinetics Juan J.L. Lertora, M.D., Ph.D. Director Clinical Pharmacology Program October 31, 2013 National Institutes of Health Clinical Center 1 GOALS of Effects of Liver
SERUM CYSTATIN C CONCENTRATION IS A POWERFUL PROGNOSTIC INDICATOR IN PATIENTS WITH CIRRHOTIC ASCITES
 SERUM CYSTATIN C CONCENTRATION IS A POWERFUL PROGNOSTIC INDICATOR IN PATIENTS WITH CIRRHOTIC ASCITES YEON SEOK SEO, 1 SOO YOUNG PARK, 2 MOON YOUNG KIM, 3 SANG GYUNE KIM, 4 JUN YONG PARK, 5 HYUNG JOON YIM,
SERUM CYSTATIN C CONCENTRATION IS A POWERFUL PROGNOSTIC INDICATOR IN PATIENTS WITH CIRRHOTIC ASCITES YEON SEOK SEO, 1 SOO YOUNG PARK, 2 MOON YOUNG KIM, 3 SANG GYUNE KIM, 4 JUN YONG PARK, 5 HYUNG JOON YIM,
Management of the Cirrhotic Patient in the ICU
 Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Management of the Cirrhotic Patient in the ICU Peter E. Morris, MD Professor & Chief, Pulmonary, Critical Care and Sleep Medicine University of Kentucky Conflict of Interest Funding US National Institutes
Organ allocation for liver transplantation: Is MELD the answer? North American experience
 Organ allocation for liver transplantation: Is MELD the answer? North American experience Douglas M. Heuman, MD Virginia Commonwealth University Richmond, VA, USA March 1998: US Department of Health and
Organ allocation for liver transplantation: Is MELD the answer? North American experience Douglas M. Heuman, MD Virginia Commonwealth University Richmond, VA, USA March 1998: US Department of Health and
Preoperative hepatic dysfunction could predict postoperative mortality and morbidity in patients
 Murata and Kato et al. Liver dysfunction and open heart surgery, page 1 Preoperative hepatic dysfunction could predict postoperative mortality and morbidity in patients undergoing cardiac surgery: Utilization
Murata and Kato et al. Liver dysfunction and open heart surgery, page 1 Preoperative hepatic dysfunction could predict postoperative mortality and morbidity in patients undergoing cardiac surgery: Utilization
Ontario s Adult Referral and Listing Criteria for Liver Transplantation
 Ontario s Adult Referral and Listing Criteria for Liver Transplantation Version 3.0 Trillium Gift of Life Network Ontario s Adult Referral & Listing Criteria for Liver Transplantation PATIENT REFERRAL
Ontario s Adult Referral and Listing Criteria for Liver Transplantation Version 3.0 Trillium Gift of Life Network Ontario s Adult Referral & Listing Criteria for Liver Transplantation PATIENT REFERRAL
Hepatology for the Nonhepatologist
 Hepatology for the Nonhepatologist Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Cincinnati, Ohio Learning
Hepatology for the Nonhepatologist Kenneth E. Sherman, MD, PhD Gould Professor of Medicine Director, Division of Digestive Diseases University of Cincinnati College of Medicine Cincinnati, Ohio Learning
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis
 ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
ACG & AASLD Joint Clinical Guideline: Prevention and Management of Gastroesophageal Varices and Variceal Hemorrhage in Cirrhosis Guadalupe Garcia-Tsao, M.D., 1 Arun J. Sanyal, M.D., 2 Norman D. Grace,
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer
 What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
Laparoscopic Cholecystectomy and Cirrhosis: A Case-Control Study of Outcomes
 Laparoscopic Cholecystectomy and Cirrhosis: A Case-Control Study of Outcomes Neville F. Fernandes, * Wayne H. Schwesinger, Susan G. Hilsenbeck, * Glenn W.W. Gross, * Michael K. Bay, * Kenneth R. Sirinek,
Laparoscopic Cholecystectomy and Cirrhosis: A Case-Control Study of Outcomes Neville F. Fernandes, * Wayne H. Schwesinger, Susan G. Hilsenbeck, * Glenn W.W. Gross, * Michael K. Bay, * Kenneth R. Sirinek,
Management of HepatoCellular Carcinoma
 9th Symposium GIC St Louis - 2010 Management of HepatoCellular Carcinoma Overview Pierre A. Clavien, MD, PhD Department of Surgery University Hospital Zurich Zurich, Switzerland Hepatocellular carcinoma
9th Symposium GIC St Louis - 2010 Management of HepatoCellular Carcinoma Overview Pierre A. Clavien, MD, PhD Department of Surgery University Hospital Zurich Zurich, Switzerland Hepatocellular carcinoma
Editorial Process: Submission:07/25/2018 Acceptance:10/19/2018
 RESEARCH ARTICLE Editorial Process: Submission:07/25/2018 Acceptance:10/19/2018 Clinical Outcome and Predictive Factors of Variceal Bleeding in Patients with Hepatocellular Carcinoma in Thailand Jitrapa
RESEARCH ARTICLE Editorial Process: Submission:07/25/2018 Acceptance:10/19/2018 Clinical Outcome and Predictive Factors of Variceal Bleeding in Patients with Hepatocellular Carcinoma in Thailand Jitrapa
Surgical Management of CBD Injury Jin Seok Heo
 Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
Surgical Management of CBD Injury Jin Seok Heo Department of Surgery, Samsung Medical Center Sungkyunkwan University School of Medicine, Seoul, Republic of Korea Bile duct injury (BDI) Introduction Incidence
General anesthetics. Dr. Shamil AL-Noaimy Lecturer of Pharmacology Dept. of Pharmacology College of Medicine
 General anesthetics Dr. Shamil AL-Noaimy Lecturer of Pharmacology Dept. of Pharmacology College of Medicine Rationale General anesthesia is essential to surgical practice, because it renders patients analgesic,
General anesthetics Dr. Shamil AL-Noaimy Lecturer of Pharmacology Dept. of Pharmacology College of Medicine Rationale General anesthesia is essential to surgical practice, because it renders patients analgesic,
Alcoholic Hepatitis: Management Options
 Alcoholic Hepatitis: Management Options Paul J. Thuluvath, MD. FRCP Institute of Digestive Health & Liver Diseases, Mercy Medical Center, Baltimore Professor of Surgery & Medicine, Georgetown University,
Alcoholic Hepatitis: Management Options Paul J. Thuluvath, MD. FRCP Institute of Digestive Health & Liver Diseases, Mercy Medical Center, Baltimore Professor of Surgery & Medicine, Georgetown University,
Clear for Surgery. What are the components of a good preoperative evaluation? What are not? Preoperative Risk Assessment: an evidence based approach
 Preoperative Risk Assessment: an evidence based approach Daniel M. Swangard, M.D. UCSF Department of Anesthesia & Perioperative Care AIM - May/June 2007 What are the components of a good preoperative evaluation?
Preoperative Risk Assessment: an evidence based approach Daniel M. Swangard, M.D. UCSF Department of Anesthesia & Perioperative Care AIM - May/June 2007 What are the components of a good preoperative evaluation?
ASSESSMENT AND MANAGEMENT OF POTENTIAL LIVER TRANSPLANT CANDIDATES
 ASSESSMENT AND MANAGEMENT OF POTENTIAL LIVER TRANSPLANT CANDIDATES James YY Fung MBChB, MD, FRACP, FHKCP, FHKAM Consultant & Hon. Assoc. Professor Liver Transplant Center Department of Surgery, Queen Mary
ASSESSMENT AND MANAGEMENT OF POTENTIAL LIVER TRANSPLANT CANDIDATES James YY Fung MBChB, MD, FRACP, FHKCP, FHKAM Consultant & Hon. Assoc. Professor Liver Transplant Center Department of Surgery, Queen Mary
Faculty Disclosure. Objectives. Cirrhosis Management for the Family Physician 18/11/2014
 Cirrhosis Management for the Family Physician Mang Ma, MD, FRCP Professor University of Alberta Faculty: Mang Ma Faculty Disclosure Relationships with commercial interests: Advisory Board: Merck, Gilead
Cirrhosis Management for the Family Physician Mang Ma, MD, FRCP Professor University of Alberta Faculty: Mang Ma Faculty Disclosure Relationships with commercial interests: Advisory Board: Merck, Gilead
Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate
 Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate Patrick Northup, MD, FAASLD, FACG Medical Director, Liver Transplantation University of Virginia
Controversies in Management of Portal Hypertension and Cirrhosis Complications in the Transplant Candidate Patrick Northup, MD, FAASLD, FACG Medical Director, Liver Transplantation University of Virginia
Clinical Controversies in Perioperative Medicine!
 Clinical Controversies in Perioperative Medicine! Hugo Quinny Cheng, MD! Division of Hospital Medicine! University of California, San Francisco! Disclosures! Perioperative beta-blockade & statin therapy
Clinical Controversies in Perioperative Medicine! Hugo Quinny Cheng, MD! Division of Hospital Medicine! University of California, San Francisco! Disclosures! Perioperative beta-blockade & statin therapy
Management of Ascites and Hepatorenal Syndrome. Florence Wong University of Toronto. June 4, /16/ Gore & Associates: Consultancy
 Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Management of Ascites and Hepatorenal Syndrome Florence Wong University of Toronto June 4, 2016 6/16/2016 1 Disclosures Gore & Associates: Consultancy Sequana Medical: Research Funding Mallinckrodt Pharmaceutical:
Stick or twist management options in hepatitis C
 Stick or twist management options in hepatitis C Dr. Chris Durojaiye & Dr. Matthijs Backx SpR Microbiology and Infectious Diseases University Hospital of Wales, Cardiff Patient history 63 year old female
Stick or twist management options in hepatitis C Dr. Chris Durojaiye & Dr. Matthijs Backx SpR Microbiology and Infectious Diseases University Hospital of Wales, Cardiff Patient history 63 year old female
RISK STRATIFICATION IN CIRRHOSIS: FOCUS ON UMBILICAL HERNIA Sam Hawkins MD PGY5
 RISK STRATIFICATION IN CIRRHOSIS: FOCUS ON UMBILICAL HERNIA Sam Hawkins MD PGY5 PATIENT PRESENTATION 73M w/ Hep B Cirrhosis, HTN, DM II Liver disease followed at OSH x2 years (when moved from China), on
RISK STRATIFICATION IN CIRRHOSIS: FOCUS ON UMBILICAL HERNIA Sam Hawkins MD PGY5 PATIENT PRESENTATION 73M w/ Hep B Cirrhosis, HTN, DM II Liver disease followed at OSH x2 years (when moved from China), on
Intron A Hepatitis C. Intron A (interferon alfa-2b) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.05 Subject: Intron A Hepatitis C Page: 1 of 5 Last Review Date: November 30, 2018 Intron A Hepatitis
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.01.05 Subject: Intron A Hepatitis C Page: 1 of 5 Last Review Date: November 30, 2018 Intron A Hepatitis
Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC
 Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC mino.mitri@ubc.ca No Conflict of Interest 157 patients 157 patients 6 transplanted Criteria Liver
Treating patients with end-stage liver disease: Are we ready? Dr. Mino R. Mitri, M.D., C.M., M.Ed., FRCPC mino.mitri@ubc.ca No Conflict of Interest 157 patients 157 patients 6 transplanted Criteria Liver
CIRROSI E IPERTENSIONE PORTALE NELLA DONNA
 Cagliari, 16 settembre 2017 CIRROSI E IPERTENSIONE PORTALE NELLA DONNA Vincenza Calvaruso, MD, PhD Ricercatore di Gastroenterologia Gastroenterologia & Epatologia, Di.Bi.M.I.S. Università degli Studi di
Cagliari, 16 settembre 2017 CIRROSI E IPERTENSIONE PORTALE NELLA DONNA Vincenza Calvaruso, MD, PhD Ricercatore di Gastroenterologia Gastroenterologia & Epatologia, Di.Bi.M.I.S. Università degli Studi di
Prognosis of untreated Primary Sclerosing Cholangitis (PSC) Erik Christensen Copenhagen, Denmark
 Erik Christensen Copenhagen, Denmark") Prognosis of untreated Primary Sclerosing Cholangitis (PSC) Erik Christensen Copenhagen, Denmark Study of Prognosis of PSC Difficulties: Disease is rare The duration of the course of disease may be very
Prognosis of untreated Primary Sclerosing Cholangitis (PSC) Erik Christensen Copenhagen, Denmark Study of Prognosis of PSC Difficulties: Disease is rare The duration of the course of disease may be very
Staging & Current treatment of HCC
 Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
4/26/2017. Liver Transplant and Palliative Care: Teaming up to improve care
 Liver Transplant and Palliative Care: Teaming up to improve care Jody C. Olson, M.D., FACP Assistant Professor of Medicine and Surgery Hepatology and Critical Care Medicine All patients with end-stage
Liver Transplant and Palliative Care: Teaming up to improve care Jody C. Olson, M.D., FACP Assistant Professor of Medicine and Surgery Hepatology and Critical Care Medicine All patients with end-stage
Peri-operative challenges and long-term outcomes in liver transplantation for polycystic liver disease
 DOI:10.1111/j.1477-2574.2012.00579.x HPB ORIGINAL ARTICLE Peri-operative challenges and long-term outcomes in liver transplantation for polycystic liver disease Roberto Gedaly, Paige Guidry, Daniel Davenport,
DOI:10.1111/j.1477-2574.2012.00579.x HPB ORIGINAL ARTICLE Peri-operative challenges and long-term outcomes in liver transplantation for polycystic liver disease Roberto Gedaly, Paige Guidry, Daniel Davenport,
Course Handouts & Post Test
 End Stage Liver Disease (ESLD) End Stage Renal Disease (ESRD) Disease Trajectory and Hospice Eligibility Terri Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Inc. & Hospice Education
End Stage Liver Disease (ESLD) End Stage Renal Disease (ESRD) Disease Trajectory and Hospice Eligibility Terri Maxwell PhD, APRN VP, Strategic Initiatives Weatherbee Resources Inc. & Hospice Education