NEVENWERKINGEN ONDER IMMUNOTHERAPIE
|
|
|
- Felix Brown
- 5 years ago
- Views:
Transcription


1
2 NEVENWERKINGEN ONDER IMMUNOTHERAPIE AANPAK EN DIAGNOSTIEK 14 OKTOBER 2017 Ximena Elzo Kraemer Medisch Oncoloog geintegreerd Kankercentrum Gent Klinische Studiedienst Oncologie
3 Immunotherapy Immunotherapy with monoclonal antibodies (MoAbs)targeting: cytotoxic T lymphocyte-associated antigen 4 (CTLA4) Ipilimumab the programmed death-1 receptor (PD-1) and its ligand PD-L1 Nivolumab (PD-1) Pembrolizumab (PD-1) Atezolizumab (PD-L1)
4 Nevenwerkingen Aanvallen eigen orgaansystemen Anders dan chemotherapie nevenwerkingen Vaak mild en zelflimiterend, maar kunnen ernstig of levensbedreigend zijn en soms blijvend (endocrinopathies) Meestal binnen de eerste weken na opstart
5 Nevenwerkingen Toxicities from immune checkpoint inhibitors (ICPis)can be divided into: infusion reactions and immune-related adverse events (iraes)
6 Immune related adverse events can affect any organ system
7 Ipilimumab-associated immune-related toxicities Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up Ann Oncol. 2017;28(suppl_4):iv119-iv142. doi: /annonc/mdx225 Ann Oncol The Author Published by Oxford University Press on behalf of the European Society for Medical Oncology. All rights reserved. For Permissions, please

8 antipd1 IKG-symposium
9 Combination of CTLA4 and PD-1/PD-L1 blockade immune-related toxicities Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up Ann Oncol. 2017;28(suppl_4):iv119-iv142. doi: /annonc/mdx225 Ann Oncol The Author Published by Oxford University Press on behalf of the European Society for Medical Oncology. All rights reserved. For Permissions, please
10 Algemene richtlijnen IKG-symposium

11 Principes van behandeling IKG-symposium
12 Welke? Graad 1-2: check voor elke volgende kuur Pruritis Rash Leverfunctiestoornissen Diarree Endocrinopathies Hypophysitis Thyroiditis Antralgieën
13 Levels of evidence I Evidence from at least one large randomised, controlled trial of good methodological quality (low potential for bias) or meta-analyses of well-conducted randomised trials without heterogeneity II Small randomised trials or large randomised trials with a suspicion of bias (lower methodological quality) or meta-analyses of such trials or of trials demonstrated heterogeneity III IV V Prospective cohort studies Retrospective cohort studies or case control studies Studies without control group, case reports, expert opinions Levels of evidence and grades of recommendation (adapted from the Infectious Diseases Society of America-United States Public Health Service Grading System)
14 a Grades of recommendation A Strong evidence for efficacy with a substantial clinical benefit, strongly recommended B Strong or moderate evidence for efficacy but with a limited clinical benefit, generally recommended C Insufficient evidence for efficacy or benefit does not outweigh the risk or the disadvantages (adverse events, costs,...). optional D Moderate evidence against efficacy or for adverse outcome, generally not recommended E Strong evidence against efficacy or for adverse outcome, never recommended By permission of the Infectious Diseases Society of America [88].

15 Huidtoxiciteit

16 Huidtoxiciteit

17 Huidtoxiciteit
18 Table 1. Grading of rash, pruritus and hypopigmentation according to Common Terminology Criteria of Adverse Events, version Grade Rash Pruritus Hypopigmentation 1 Macular or papular eruption covering <10% BSA with or without symptoms (e.g., pruritus, burning, tightness) Mild or localized; topical intervention indicated Hypopigmentation or depigmentation covering <10% BSA; no psychosocial impact 2 Macular or popular eruption covering 10 30% BSA with or without symptoms (e.g., pruritus, burning, tightness); limiting instrumental ADL 3 Macules/papules covering >30% BSA with or without associated symptoms; limiting self-care ADL Intense or widespread; intermittent; skin changes from scratching (e.g., edema, population, excoriations, lichenification, oozing/ crusts); oral intervention indicated; limiting instrumental ADL Intense or widespread; constant; limiting self care ADL or sleep; oral corticosteroid or oral immunosuppressive therapy indicated 4 Generalized exfoliative, ulcerative, or bullous dermatitis 5 Death Hypopigmentation or depigmentation covering >10% BSA; associated psychosocial impact
19 Huidtoxiciteit
20 Immune-related skin toxicity (ESMO-guidelines) For grade 1 2 skin AEs, continue (at least 1 week) with ICPis. Start topical emollients, antihistamines in the case of pruritus and/or topical (mild strength) corticosteroid creams. Reinitiate ICPi when grade 1. For grade 3 skin AEs, interrupt ICPi and start immediate treatment with topical emollients, antihistamines and high strength corticosteroid creams [II, B]. For grade 4 skin AEs, discontinue ICPi (permanently), consider admitting patient and always consult dermatologist immediately. Start i.v. corticosteroids [1 2 mg/kg (methyl)prednisone] and taper based on response of AE [II, B].

21 Gastro-intestinale toxiciteit
22 Gastrointestinaltoxicity (ESMO-guidelines) In patients with non-severe diarrhea (grade 1), ICPi can be continued. Treatment with antidiarrheal medication (e.g. loperamide) should be prescribed [IV V, B]. In grade 2 diarrhea, ICPi should be interrupted and the patient should start with corticosteroids depending on the severity and other symptoms (either budesonide or oral corticosteroids 1 mg/kg). In the case of no improvement within 3 5 days, colonoscopy should be carried out and, in the case of colitis, infliximab 5 mg/kg should be administered [IV V, B]. In patients with severe diarrhea (grade 3 to 4), permanently discontinue ICPi. Admit patient to the hospital and initiate (methyl)prednisone 2 mg/kg i.v. Add MMF if improvement is observed within 2 3 days. Consult a hepatologist if no improvement under double immunosuppression. Other immunosuppressive drugs to consider are ATG and tacrolimus. Consult or refer patient to an experienced center. Taper over 6 weeks under close monitoring of liver tests [IV V, B].
23 Immune-related endocrinopathies (ESMO-guidelines) In symptomatic hyperthyroism patients, usually grade 1 or 2, interrupt ICPi, start beta-blocker therapy (propranolol or atenolol/metoprolol). Restart ICPi when asymptomatic [IV V, B]. In the case of hypothyroidism, rarely > grade 2, start HRT depending on the severity ( μg/day). Increase the dose until TSH is normal. In the case of inflammation of the thyroid gland, start prednisone orally 1 mg/kg. Taper based on recovery of clinical symptoms. Consider interruption of ICPi treatment when symptomatic [IV V, B]. In the case of hypophysitis (rarely > grade 2), when headache, diplopia or other neurological symptoms are present, start (methyl)prednisone 1 mg/kg orally and taper over 2 4 weeks. Start HRT depending on the affected hormonal axis (levothyroxine, hydrocortisol, testosterone) [V, B]. In patients with type I DM grade 3 to 4 [ketoacidotic (sub)coma], admit to hospital immediately and start treatment of newly onset type I DM [I, A]. Role of corticosteroids in preventing complete loss of insulin producing cells is unknown and not recommended
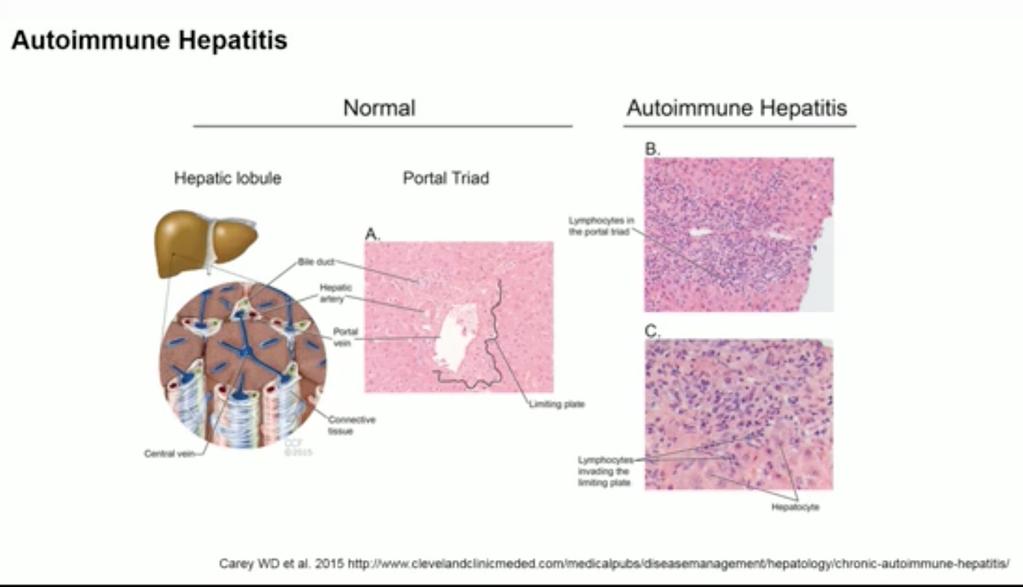
24 Hepatitis
25 Immune-related hepatotoxicity (ESMO-guidelines) For grade 2 hepatitis, withhold ICPi and monitor AST/ALT levels closely (1 2 times/week). When no improvement over 1 week, start (methyl)prednisone (0.5 1 mg/kg). Taper over several weeks under close monitoring of AST/ALT and bilirubin [IV V, B]. For grade 3 hepatitis, discontinue ICPi and immediately start with (methyl)prednisone 1 2 mg/kg. When no improvement in 2 3 days, add MMF (1000 mg 3 daily). Taper immunosuppression over 4 6 weeks under close monitoring of AST/ALT and bilirubin [IV V, B]. For grade 4 hepatitis, permanently discontinue ICPi, admit patient to the hospital and initiate (methyl)prednisone 2 mg/kg i.v. Add MMF if no improvement is observed within 2 3 days. Consult hepatologist if no improvement under double immunosuppression. Other immunosuppressive drugs to consider are ATG and tacrolimus. Consult or refer patient to an experienced centre. Taper over 6 weeks under close monitoring of liver tests [IV V, B].

26 Pneumonitis
27 Immune-related pneumonitis (ESMO-guidelines) In grade 1 and 2 pneumonitis, interrupt ICPi therapy, try to rule out infection and start with prednisone 1 2 mg/kg orally. Taper over 4 6 weeks [IV V, B]. In grade 3 and 4 pneumonitis, discontinue ICPi permanently, admit the patient to the hospital, even ICU if necessary and immediately start highdose (methyl)prednisone 2 4 mg/kg i.v. Add infliximab, MMF or cyclophosphamide in the case of deterioration under steroids. Taper over a period of 4 6 weeks [IV V, B].

28 Duurzame responsen als nevenwerkingen IKG-symposium
29 Impact of immunosuppression on efficacy The need for immunosuppressive therapy to manage iraes does not appear to affect the response to checkpoint inhibition with either anti-pd-1 antibodies or ipilimumab. Anti-PD-1 antibodies IrAEs are significantly less frequent with the anti-pd-1 antibodies compared with ipilimumab. In an analysis of 576 patients with advanced melanoma treated in four clinical trials, 24 percent received immunosuppressive therapy for the management of treatment-related adverse events [3]. There was no significant difference in the objective response rate between those who received immunosuppressive treatment and those who did not (29.8 versus 31.8 percent). The median duration of response was not reached in those with immunosuppressive therapy, compared with 22 months in those not requiring immunosuppressive therapy. Ipilimumab The most extensive data with ipilimumab come from a single-institution experience that analyzed the incidence of iraes and treatment outcomes in 298 melanoma patients treated with ipilimumab (3 mg/kg) outside of a clinical trial setting [4]. IrAEs were seen in 254 patients (85 percent), and 103 patients (35 percent) required corticosteroids. Anti-tumor necrosis factor-alpha therapy was used in 29 cases (10 percent) who did not respond promptly to corticosteroids. The median overall survival was 16.5 months, and the estimated two-year survival rate was 39 percent for the entire cohort. Overall survival was the same in patients who had an irae compared with those without an irae, and there was no difference between those requiring corticosteroids and those not requiring immunosuppressive therapy. The time to treatment failure, defined as the need for alternative therapy or death, was 5.7 months for the entire cohort. As with overall survival, there were no significant differences between those with and without an irae or between those treated with corticosteroids and those not receiving corticosteroids.
30 Weinig voorkomende toxiciteit
31 Cardiac toxicity (ESMO-guidelines) When a myocarditis is suspected, admit the patient and immediately start high-dose (methyl)prednisone (1 2 mg/kg). In the case of deterioration, consider adding another immunosuppressive drug (MMF or tacrolimus) [V, B].
32 Neurological toxicity (ESMO-guidelines) In the case of mild neurological AEs, withhold ICPi and perform work-up (MRI scan, lumbar puncture) to define nature of neurotoxicity. In the case of deterioration or severe neurological symptoms, admit the patient and start (methyl)prednisone 1 2 mg/kg orally or i.v. In the case of Guillain- Barré or myasthenia-like symptoms, consider adding plasmapheresis or i.v. Ig [V, B].
33 Hematologic Auto-immuun anaemia neutropenia thrombocytopenia
34 Rheumatological toxicity (ESMO-guidelines) For mild arthralgia, start NSAIDs, and in the case of no improvement, consider low dose steroids (10 20 mg prednisone). In the case of severe polyarthritis, refer patient to or consult a rheumatologist and start prednisone 1 mg/kg. Sometimes infliximab or another anti-tnfα drug is required for improvement of arthritis [V, B].
35 Renal toxicity (ESMO-guidelines) In case of nephritis, rule out other causes of renal failure first. Interrupt or permanently discontinue ICPi depending on the severity of the renal insufficiency. Stop other nephrotoxic drugs. Start (methyl)prednisone 1 2 mg/kg. Consider renal biopsy to confirm diagnosis [V, B].
36 Vaccinaties
37 Vaccinaties Geen vaccinaties met levende verzwakte organismen: bv: rubella, mazelen, gele koorts, enz. Opletten bij contact met personen, die een levend verzwakt organisme, oraal gegeven: rotavirus bij kinderen. Griepvaccin: vooralsnog wordt het aangeraden, niet de nasale vorm, echter
38 Griepvaccin Immune response and adverse events to influenza vaccine in cancer patients undergoing PD-1 blockade: Metastatic cancer pts treated with at least one dose of either nivolumab or pembrolizumab were vaccinated with a trivalent inactive influenza vaccination between October and November We included 23 pts and 7 age-matched healthy controls. 16 pts had a diagnosis of non-small cell lung cancer, 3 pts had renal cell carcinoma and 3 pts a malignant melanoma. 12 pts (52.2%) experienced an irae. 6 pts (26.1%) had grade 3 or 4 (G3/4) iraes. Conclusion: The seasonal influence vaccination reaches a protective range in these pts. Unexpectedly, however, an increased rate of clinically relevant iraes was observed. Confirmation in a larger population and mechanistic understanding is required.

39 Take Home Message

40 DANK!
OPTIMAL MANAGEMENT OF IMMUNE- RELATED ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT INHIBITORS
 OPTIMAL MANAGEMENT OF IMMUNE- RELATED ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT INHIBITORS Alberto Fusi Charité Comprehensive Cancer Centre Berlin, Germany 1 Immune check point blockade with CTLA-4, anti-pd-1
OPTIMAL MANAGEMENT OF IMMUNE- RELATED ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT INHIBITORS Alberto Fusi Charité Comprehensive Cancer Centre Berlin, Germany 1 Immune check point blockade with CTLA-4, anti-pd-1
Adverse effects of Immunotherapy. Asha Nayak M.D
 Adverse effects of Immunotherapy Asha Nayak M.D None Financial Disclosures Objectives Understand intensity of the AEs. Understanding unique side-effects. Develop effective monitoring and management guidelines.
Adverse effects of Immunotherapy Asha Nayak M.D None Financial Disclosures Objectives Understand intensity of the AEs. Understanding unique side-effects. Develop effective monitoring and management guidelines.
Nursing Perspective on iraes: Patient Education, Monitoring and Management
 Nursing Perspective on iraes: Patient Education, Monitoring and Management Rebecca Lewis, CRNP Nurse Practitioner University of Pittsburgh-HCC Shadyside Disclosures No relevant financial relationships
Nursing Perspective on iraes: Patient Education, Monitoring and Management Rebecca Lewis, CRNP Nurse Practitioner University of Pittsburgh-HCC Shadyside Disclosures No relevant financial relationships
CANCER IMMUNOTHERAPY. Pocket Guide
 CANCER IMMUNOTHERAPY Pocket Guide Unique Clinical Features Tumor Response Kinetics Response patterns associated with immune checkpoint blockade may differ from those associated with conventional therapies,
CANCER IMMUNOTHERAPY Pocket Guide Unique Clinical Features Tumor Response Kinetics Response patterns associated with immune checkpoint blockade may differ from those associated with conventional therapies,
PEMBROLIZUMAB (KEYTRUDA ) for the treatment of advanced melanoma or previously treated NSCLC
 for the treatment of advanced melanoma or previously treated NSCLC") DRUG ADMINISTRATION SCHEDULE Day Drug Dose Route Diluent Rate Day 1 Pembrolizumab 2mg/kg IV Infusion 100mL 0.9% Sodium Chloride* Or 100mL 5% Glucose* *Final concentration must be between 1 to 10mg/mL Over
DRUG ADMINISTRATION SCHEDULE Day Drug Dose Route Diluent Rate Day 1 Pembrolizumab 2mg/kg IV Infusion 100mL 0.9% Sodium Chloride* Or 100mL 5% Glucose* *Final concentration must be between 1 to 10mg/mL Over
Melanoma Immunotherapy. Nursing Perspective on Immune-Related Adverse Events: Patient education, Monitoring & Management
 Melanoma Immunotherapy Nursing Perspective on Immune-Related Adverse Events: Patient education, Monitoring & Management Mike Buljan, NP UCSF Medical Center Melanoma Oncology Disclosures None Only FDA-approved
Melanoma Immunotherapy Nursing Perspective on Immune-Related Adverse Events: Patient education, Monitoring & Management Mike Buljan, NP UCSF Medical Center Melanoma Oncology Disclosures None Only FDA-approved
MANAGEMENT OF IMMUNE-RELATED SIDE EFFECTS OF IMMUNE CHECKPOINT INHIBITORS
 MANAGEMENT OF IMMUNE-RELATED SIDE EFFECTS OF IMMUNE CHECKPOINT INHIBITORS John B.A.G. Haanen MD PhD CONTENT OF THIS PRESENTATION General aspects of immune related adverse events related to immune checkpoint
MANAGEMENT OF IMMUNE-RELATED SIDE EFFECTS OF IMMUNE CHECKPOINT INHIBITORS John B.A.G. Haanen MD PhD CONTENT OF THIS PRESENTATION General aspects of immune related adverse events related to immune checkpoint
ENDOCRINE ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT IMMUNOTHERAPY
 ENDOCRINE ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT IMMUNOTHERAPY Lauren Clarine DO, Renil Rodriguez Martinez MD, Matthew Levine MD, Amy Chang MD, and Megan McGarvey MD May 6, 2017 Immune checkpoint inhibitors
ENDOCRINE ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT IMMUNOTHERAPY Lauren Clarine DO, Renil Rodriguez Martinez MD, Matthew Levine MD, Amy Chang MD, and Megan McGarvey MD May 6, 2017 Immune checkpoint inhibitors
Immunotherapy: Toxicity Management. Dr. Megan Lyle Medical Oncologist Liz Plummer Cancer Care Centre Cairns Hospital
 Immunotherapy: Toxicity Management Dr. Megan Lyle Medical Oncologist Liz Plummer Cancer Care Centre Cairns Hospital Disclosures Honoraria and travel support from BMS, MSD, Novartis Advisory board for MSD
Immunotherapy: Toxicity Management Dr. Megan Lyle Medical Oncologist Liz Plummer Cancer Care Centre Cairns Hospital Disclosures Honoraria and travel support from BMS, MSD, Novartis Advisory board for MSD
ATEZOLIZUMAB (TECENTRIQ ) in urothelial carcinoma
 in urothelial carcinoma") DRUG ADMINISTRATION SCHEDULE Day Drug Daily Dose Route Diluent Rate Day 1 Atezolizumab 1200 mg IV Infusion 250mL 0.9% Sodium Chloride Over 60 minutes* *The initial dose of atezolizumab must be administered
DRUG ADMINISTRATION SCHEDULE Day Drug Daily Dose Route Diluent Rate Day 1 Atezolizumab 1200 mg IV Infusion 250mL 0.9% Sodium Chloride Over 60 minutes* *The initial dose of atezolizumab must be administered
ATEZOLIZUMAB (TECENTRIQ )
") DRUG ADMINISTRATION SCHEDULE Day Drug Daily Dose Route Diluent Rate Day 1 Atezolizumab 1200 mg IV Infusion 250mL 0.9% Sodium Chloride Over 60 minutes* *The initial dose of atezolizumab must be administered
DRUG ADMINISTRATION SCHEDULE Day Drug Daily Dose Route Diluent Rate Day 1 Atezolizumab 1200 mg IV Infusion 250mL 0.9% Sodium Chloride Over 60 minutes* *The initial dose of atezolizumab must be administered
Managing immune related toxicity. Karijn Suijkerbuijk May 27 th 2017
 Managing immune related toxicity Karijn Suijkerbuijk May 27 th 2017 Disclosures Advisory role: BMS, Merck Travel support: Amgen, Novartis, Roche Whybother? Patients are dying from toxicity Eggermont ipilimumab
Managing immune related toxicity Karijn Suijkerbuijk May 27 th 2017 Disclosures Advisory role: BMS, Merck Travel support: Amgen, Novartis, Roche Whybother? Patients are dying from toxicity Eggermont ipilimumab
Checkpoint inhibitors: Strategies to checkmate T-cell mediated toxicity. Disclosure Statement. Learning Objectives
 Checkpoint inhibitors: Strategies to checkmate T-cell mediated toxicity Adam J. DiPippo, PharmD Clinical Pharmacy Specialist Leukemia Texas Society of Health-System Pharmacists 2017 Annual Seminar April
Checkpoint inhibitors: Strategies to checkmate T-cell mediated toxicity Adam J. DiPippo, PharmD Clinical Pharmacy Specialist Leukemia Texas Society of Health-System Pharmacists 2017 Annual Seminar April
Immunotherapy in Lung Cancer
 Immunotherapy in Lung Cancer Jamie Poust Pharm. D., BCOP Oncology Pharmacist University of Colorado Hospital Objectives Describe the recent advances in immunotherapy for patients with lung cancer Outline
Immunotherapy in Lung Cancer Jamie Poust Pharm. D., BCOP Oncology Pharmacist University of Colorado Hospital Objectives Describe the recent advances in immunotherapy for patients with lung cancer Outline
Immune checkpoint inhibitors in clinical practice: update on management of immune-related toxicities
 Review Article on Lung Cancer Diagnostics and Treatments 2015: A Renaissance of Patient Care Immune checkpoint inhibitors in clinical practice: update on management of immune-related toxicities Jeryl Villadolid
Review Article on Lung Cancer Diagnostics and Treatments 2015: A Renaissance of Patient Care Immune checkpoint inhibitors in clinical practice: update on management of immune-related toxicities Jeryl Villadolid
Management of Immune Checkpoint Inhibitor Related Toxicities
 Management of Immune Checkpoint Inhibitor Related Toxicities Katie Wolfram, PharmD Clinical Pharmacist, Oncology Memorial Hospital of South Bend A Webinar for HealthTrust Members November 12, 2018 Disclosures
Management of Immune Checkpoint Inhibitor Related Toxicities Katie Wolfram, PharmD Clinical Pharmacist, Oncology Memorial Hospital of South Bend A Webinar for HealthTrust Members November 12, 2018 Disclosures
Toxicity of Systemic Melanoma Therapies. Alex Guminski Melanoma Institute Australia Royal North Shore Hospital University of Sydney
 Toxicity of Systemic Melanoma Therapies Alex Guminski Melanoma Institute Australia Royal North Shore Hospital University of Sydney Disclosures Advisory Board Novartis, BMS, Sanofi, Pfizer Travel support
Toxicity of Systemic Melanoma Therapies Alex Guminski Melanoma Institute Australia Royal North Shore Hospital University of Sydney Disclosures Advisory Board Novartis, BMS, Sanofi, Pfizer Travel support
Immune-Related Adverse Reaction (irar) Management Guide
 Management Guide") REGIMEN Immune-Related Adverse Reaction (irar) Management Guide OPDIVO as monotherapy is indicated for the treatment of locally advanced or metastatic squamous non-small cell lung cancer (NSCLC) with progression
REGIMEN Immune-Related Adverse Reaction (irar) Management Guide OPDIVO as monotherapy is indicated for the treatment of locally advanced or metastatic squamous non-small cell lung cancer (NSCLC) with progression
HEY Guidelines for the management of Toxicities associated with immune checkpoint inhibitors.
 Hull and East Yorkshire Hospital NHS Trust Queen s centre for Oncology and Haematology Castle Hill Hospital HEY Guidelines for the management of Toxicities associated with immune checkpoint inhibitors.
Hull and East Yorkshire Hospital NHS Trust Queen s centre for Oncology and Haematology Castle Hill Hospital HEY Guidelines for the management of Toxicities associated with immune checkpoint inhibitors.
Ipilimumab in Melanoma
 Ipilimumab in Melanoma Indication: Advanced (unresectable or metastatic) melanoma in adults who have received prior therapy LCNDG criteria to be met: Histologically confirmed unresectable stage III or
Ipilimumab in Melanoma Indication: Advanced (unresectable or metastatic) melanoma in adults who have received prior therapy LCNDG criteria to be met: Histologically confirmed unresectable stage III or
Safety Immune Related Adverse Events (irae) Focus on NSCLC Aaron Hansen, BSc, MBBS, FRACP
 Focus on NSCLC Aaron Hansen, BSc, MBBS, FRACP") Safety Immune Related Adverse Events (irae) Focus on NSCLC Aaron Hansen, BSc, MBBS, FRACP Division of Medical Oncology and Hematology Bras Drug Development Program Princess Margaret Cancer Centre, Toronto,
Safety Immune Related Adverse Events (irae) Focus on NSCLC Aaron Hansen, BSc, MBBS, FRACP Division of Medical Oncology and Hematology Bras Drug Development Program Princess Margaret Cancer Centre, Toronto,
NCCP Chemotherapy Regimen
 INDICATIONS FOR USE: Pembrolizumab 2mg/kg INDICATION ICD10 Regimen Code *Reimbursement Status First line monotherapy for the treatment of advanced (unresectable or C43 00347a ODMS metastatic) melanoma
INDICATIONS FOR USE: Pembrolizumab 2mg/kg INDICATION ICD10 Regimen Code *Reimbursement Status First line monotherapy for the treatment of advanced (unresectable or C43 00347a ODMS metastatic) melanoma
Atezolizumab Non-small cell lung cancer
 Systemic Anti Cancer Treatment Protocol Atezolizumab Non-small cell lung cancer PROTOCOL REF: MPHAATNSCLC (Version No: 1.0) Approved for use in: Locally advanced/metastatic non squamous or squamous non-small
Systemic Anti Cancer Treatment Protocol Atezolizumab Non-small cell lung cancer PROTOCOL REF: MPHAATNSCLC (Version No: 1.0) Approved for use in: Locally advanced/metastatic non squamous or squamous non-small
Managing Checkpoint Inhibitor Toxicities. Megan L. Menon, Pharm.D., BCOP Roswell Park Cancer Institute
 Managing Checkpoint Inhibitor Toxicities Megan L. Menon, Pharm.D., BCOP Roswell Park Cancer Institute Approved Indications Ipilimumab Nivolumab Pembrolizumab* Atezolizumab Avelumab Durvalumab Ipi + Nivol
Managing Checkpoint Inhibitor Toxicities Megan L. Menon, Pharm.D., BCOP Roswell Park Cancer Institute Approved Indications Ipilimumab Nivolumab Pembrolizumab* Atezolizumab Avelumab Durvalumab Ipi + Nivol
Pembrolizumab 200mg Monotherapy
 Pembrolizumab 200mg This regimen supercedes NCCP Regimen 00347 Pembrolizumab 2mg/kg as of September 2018 due to a change in the licensed dosing posology. INDICATIONS FOR USE: INDICATION ICD10 Regimen Code
Pembrolizumab 200mg This regimen supercedes NCCP Regimen 00347 Pembrolizumab 2mg/kg as of September 2018 due to a change in the licensed dosing posology. INDICATIONS FOR USE: INDICATION ICD10 Regimen Code
Complications of Immunotherapy
 Complications of Immunotherapy Sarah Norskog, PharmD, BCOP Oncology Pharmacy Specialist University of Colorado Hospital Disclosures I have no relevant financial relationships with commercial interests
Complications of Immunotherapy Sarah Norskog, PharmD, BCOP Oncology Pharmacy Specialist University of Colorado Hospital Disclosures I have no relevant financial relationships with commercial interests
TOXICITY RELATED TO IO IN LUNG CANCER
 TOXICITY RELATED TO IO IN LUNG CANCER Dr. Jorge A. Alatorre Alexander Head of the Thoracic Oncology Clinic at Instituto Nacional de Enfermedades Respiratorias American British Cowdray Medical Center Mexico
TOXICITY RELATED TO IO IN LUNG CANCER Dr. Jorge A. Alatorre Alexander Head of the Thoracic Oncology Clinic at Instituto Nacional de Enfermedades Respiratorias American British Cowdray Medical Center Mexico
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes. Disclosures
 Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
Immunotherapy Treatment Developments in Medical Oncology
 Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Immune-Related Adverse Events (IRAEs) due to Cancer Immunotherapy
 due to Cancer Immunotherapy") Immune-Related Adverse Events (IRAEs) due to Cancer Immunotherapy Philip Mease MD Director, Rheumatology Clinical Research, Swedish- Providence St. Joseph Health Clinical Professor, University of Washington
Immune-Related Adverse Events (IRAEs) due to Cancer Immunotherapy Philip Mease MD Director, Rheumatology Clinical Research, Swedish- Providence St. Joseph Health Clinical Professor, University of Washington
KEYTRUDA is also indicated in combination with pemetrexed and platinum chemotherapy for the
 FDA-Approved Indication for KEYTRUDA (pembrolizumab) in Combination With Carboplatin and Either Paclitaxel or Nab-paclitaxel for the Firstline Treatment of Patients With Metastatic Squamous Non Small Cell
FDA-Approved Indication for KEYTRUDA (pembrolizumab) in Combination With Carboplatin and Either Paclitaxel or Nab-paclitaxel for the Firstline Treatment of Patients With Metastatic Squamous Non Small Cell
BC Cancer Protocol Summary for Treatment of Advanced Non- Small Cell Lung Cancer Using Pembrolizumab
 BC Cancer Protocol Summary for Treatment of Advanced Non- Small Cell Lung Cancer Using Pembrolizumab Protocol Code Tumour Group Contact Physician ULUAVPMB Lung Dr. Christopher Lee ELIGIBILITY: Advanced
BC Cancer Protocol Summary for Treatment of Advanced Non- Small Cell Lung Cancer Using Pembrolizumab Protocol Code Tumour Group Contact Physician ULUAVPMB Lung Dr. Christopher Lee ELIGIBILITY: Advanced
CANCER IMMUNOTHERAPY Presented by John A Keech Jr DO MultiCare Regional Cancer Center
 CANCER IMMUNOTHERAPY 2018 Presented by John A Keech Jr DO MultiCare Regional Cancer Center Successful anti-cancer immunity is autoimmunity Green, The Scientist, 2014 Immunotherapy strategies Cancer vaccines
CANCER IMMUNOTHERAPY 2018 Presented by John A Keech Jr DO MultiCare Regional Cancer Center Successful anti-cancer immunity is autoimmunity Green, The Scientist, 2014 Immunotherapy strategies Cancer vaccines
Immune-Mediated Adverse Events Management Handbook
 Immune-Mediated Adverse Events Management Handbook Your guide to addressing the immune-mediated adverse events (imaes) associated with patients taking PD-L1 inhibition therapy Indications and Usage IMFINZI
Immune-Mediated Adverse Events Management Handbook Your guide to addressing the immune-mediated adverse events (imaes) associated with patients taking PD-L1 inhibition therapy Indications and Usage IMFINZI
Overview of Immunotherapy Related Adverse Event (irae) Management
 Management") Overview of Immunotherapy Related Adverse Event (irae) Management DR. ROLAND LEUNG MEDICAL ONCOLOGY DEPARTMENT OF MEDICINE THE UNIVERSITY OF HONG KONG QUEEN MARY HOSPITAL Outline Immune system overview
Overview of Immunotherapy Related Adverse Event (irae) Management DR. ROLAND LEUNG MEDICAL ONCOLOGY DEPARTMENT OF MEDICINE THE UNIVERSITY OF HONG KONG QUEEN MARY HOSPITAL Outline Immune system overview
New Era of Cancer Therapy Immuno-Oncology: PD1/PD-L1 inhibitors
 New Era of Cancer Therapy Immuno-Oncology: PD1/PD-L1 inhibitors Farah Brasfield, MD Chair, Regional Chiefs of Oncology Kaiser Permanente Jennifer Chang, PharmD, MPH Supervisor, Drug Information Services
New Era of Cancer Therapy Immuno-Oncology: PD1/PD-L1 inhibitors Farah Brasfield, MD Chair, Regional Chiefs of Oncology Kaiser Permanente Jennifer Chang, PharmD, MPH Supervisor, Drug Information Services
Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy. Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016
 Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016 Overcoming toxicity A new context for evaluating toxicity
Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016 Overcoming toxicity A new context for evaluating toxicity
MANAGEMENT OF IMMUNE-RELATED GI AND LIVER TOXICITY
 MANAGEMENT OF IMMUNE-RELATED GI AND LIVER TOXICITY Alberto Fusi Charité Comprehensive Cancer Centre - Berlin St. George s University - London TAO Meeting - Cancer Toxicity Management Paris - 8th-9th December
MANAGEMENT OF IMMUNE-RELATED GI AND LIVER TOXICITY Alberto Fusi Charité Comprehensive Cancer Centre - Berlin St. George s University - London TAO Meeting - Cancer Toxicity Management Paris - 8th-9th December
Cancer Immunotherapy: Promises and Challenges. Disclosures
 Cancer Immunotherapy: Promises and Challenges David B. Page, MD Medical Oncology PMG East Hematology & Oncology Earle A. Chiles Research Institute Portland, Oregon Disclosures Consulting: Celldex, Nektar,
Cancer Immunotherapy: Promises and Challenges David B. Page, MD Medical Oncology PMG East Hematology & Oncology Earle A. Chiles Research Institute Portland, Oregon Disclosures Consulting: Celldex, Nektar,
Nivolumab and Ipilimumab
 Nivolumab and Ipilimumab Indication Advanced (unresectable or metastatic) melanoma. (NICE TA400) ICD-10 codes Codes prefixed with C43 Regimen details Cycles 1-4 Nivolumab and Ipilimumab every 3 weeks Day
Nivolumab and Ipilimumab Indication Advanced (unresectable or metastatic) melanoma. (NICE TA400) ICD-10 codes Codes prefixed with C43 Regimen details Cycles 1-4 Nivolumab and Ipilimumab every 3 weeks Day
NECN CHEMOTHERAPY HANDBOOK PROTOCOL
 Nivolumab (Opdivo ) for treatment of advanced melanoma and Renal Cell Cancer (Also advanced/ metastatic NSCLC EMAS patients only -Nov 2016) DRUG ADMINISTRATION SCHEDULE (SINGLE AGENT Day Drug Daily dose
Nivolumab (Opdivo ) for treatment of advanced melanoma and Renal Cell Cancer (Also advanced/ metastatic NSCLC EMAS patients only -Nov 2016) DRUG ADMINISTRATION SCHEDULE (SINGLE AGENT Day Drug Daily dose
Ipilimumab Monotherapy
 INDICATIONS FOR USE: Ipilimumab INDICATION ICD10 Regimen Code *Reimbursement Indicator Treatment of advanced (unresectable or metastatic) melanoma in adults C43 00105a ODMS *If a reimbursement indicator
INDICATIONS FOR USE: Ipilimumab INDICATION ICD10 Regimen Code *Reimbursement Indicator Treatment of advanced (unresectable or metastatic) melanoma in adults C43 00105a ODMS *If a reimbursement indicator
MANAGEMENT OF IMMUNOTHERAPY RELATED GI AND HEPATIC ADVERSE EVENTS
 MANAGEMENT OF IMMUNOTHERAPY RELATED GI AND HEPATIC ADVERSE EVENTS Wai K. Leung Li Shu Fan Medical Foundation Professor in Gastroenterology Associate Dean (Human Capital), LKS Faculty of Medicine, University
MANAGEMENT OF IMMUNOTHERAPY RELATED GI AND HEPATIC ADVERSE EVENTS Wai K. Leung Li Shu Fan Medical Foundation Professor in Gastroenterology Associate Dean (Human Capital), LKS Faculty of Medicine, University
DOSING GUIDE. Indications. Important Safety Information. Enable the immune system. RECOGNIZE. RESPOND.
 DOSING GUIDE For patients with unresectable Stage III NSCLC following concurrent CRT For patients with locally advanced or metastatic UC previously treated with platinum-based therapy Enable the immune
DOSING GUIDE For patients with unresectable Stage III NSCLC following concurrent CRT For patients with locally advanced or metastatic UC previously treated with platinum-based therapy Enable the immune
BCCA Protocol Summary for the Treatment of Unresectable or Metastatic Melanoma Using Ipilimumab
 BCCA Protocol Summary for the Treatment of Unresectable or Metastatic Melanoma Using Ipilimumab Protocol Code Tumour Group Contact Physician USMAVIPI Skin and Melanoma Dr. Kerry Savage ELIGIBILITY: Unresectable
BCCA Protocol Summary for the Treatment of Unresectable or Metastatic Melanoma Using Ipilimumab Protocol Code Tumour Group Contact Physician USMAVIPI Skin and Melanoma Dr. Kerry Savage ELIGIBILITY: Unresectable
Summary of the risk management plan (RMP) for Opdivo (nivolumab)
 for Opdivo (nivolumab)") EMA/285771/2015 Summary of the risk management plan (RMP) for Opdivo (nivolumab) This is a summary of the risk management plan (RMP) for Opdivo, which details the measures to be taken in order to ensure
EMA/285771/2015 Summary of the risk management plan (RMP) for Opdivo (nivolumab) This is a summary of the risk management plan (RMP) for Opdivo, which details the measures to be taken in order to ensure
HIGHLIGHTS OF PRESCRIBING INFORMATION
 HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use OPDIVO safely and effectively. See full prescribing information for OPDIVO. OPDIVO (nivolumab) injection,
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use OPDIVO safely and effectively. See full prescribing information for OPDIVO. OPDIVO (nivolumab) injection,
BCCA Protocol Summary for the Treatment of Unresectable or Metastatic Melanoma Using Nivolumab
 BCCA Protocol Summary for the Treatment of Unresectable or Metastatic Melanoma Using Nivolumab Protocol Code Tumour Group Contact Physician USMAVNIV Skin and Melanoma Dr. Kerry Savage ELIGIBILITY: Unresectable
BCCA Protocol Summary for the Treatment of Unresectable or Metastatic Melanoma Using Nivolumab Protocol Code Tumour Group Contact Physician USMAVNIV Skin and Melanoma Dr. Kerry Savage ELIGIBILITY: Unresectable
Healthcare Professional. Frequently Asked. Questions. Brochure
 YERVOY (ipilimumab) Healthcare Professional Frequently Asked Questions Brochure YERVOY is indicated for the treatment of advanced (unresectable or metastatic) melanoma in adults. 1 This medicinal product
YERVOY (ipilimumab) Healthcare Professional Frequently Asked Questions Brochure YERVOY is indicated for the treatment of advanced (unresectable or metastatic) melanoma in adults. 1 This medicinal product
Rheumatology winter clinical symposium 9 th annual meeting Maui, Hawaii February
 New onset polyarthritis secondary to pembrolizumab [anti-pd1 antibody] in a patient with metastatic melanoma successfully treated with IL-6 receptor [IL-6R] inhibitor. Salvador R. Garcia1, MD; Adi Diab2,
New onset polyarthritis secondary to pembrolizumab [anti-pd1 antibody] in a patient with metastatic melanoma successfully treated with IL-6 receptor [IL-6R] inhibitor. Salvador R. Garcia1, MD; Adi Diab2,
Toxicity from Checkpoint Inhibitors. James Larkin FRCP PhD
 Toxicity from Checkpoint Inhibitors James Larkin FRCP PhD Disclosures Research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): BMS, Eisai, GSK, MSD, Novartis, Pfizer, Roche/Genentech
Toxicity from Checkpoint Inhibitors James Larkin FRCP PhD Disclosures Research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): BMS, Eisai, GSK, MSD, Novartis, Pfizer, Roche/Genentech
Toxicities of the anti-pd-1 and anti-pd-l1 immune checkpoint antibodies
 26: 2375 2391, 2015 doi:10.1093/annonc/mdv383 Published online 14 September 2015 Toxicities of the anti-pd-1 and anti-pd-l1 immune checkpoint antibodies J. Naidoo 1 *, D. B. Page 2,B.T.Li 3, L. C. Connell
26: 2375 2391, 2015 doi:10.1093/annonc/mdv383 Published online 14 September 2015 Toxicities of the anti-pd-1 and anti-pd-l1 immune checkpoint antibodies J. Naidoo 1 *, D. B. Page 2,B.T.Li 3, L. C. Connell
Special pediatric considerations are noted when applicable, otherwise adult provisions apply.
 DRUG NAME: Avelumab SYNONYM(S): MSB0010718C 1 COMMON TRADE NAME(S): BAVENCIO CLASSIFICATION: monoclonal antibody Special pediatric considerations are noted when applicable, otherwise adult provisions apply.
DRUG NAME: Avelumab SYNONYM(S): MSB0010718C 1 COMMON TRADE NAME(S): BAVENCIO CLASSIFICATION: monoclonal antibody Special pediatric considerations are noted when applicable, otherwise adult provisions apply.
7.3 Suggested Evaluation and Treatment for Immunerelated Adverse Events Gastrointestinal Tract
 7.3 Suggested Evaluation and Treatment for Immunerelated Adverse Events Early diagnosis and treatment intervention for high-grade iraes can help prevent the occurrence of complications, such as GI perforation.
7.3 Suggested Evaluation and Treatment for Immunerelated Adverse Events Early diagnosis and treatment intervention for high-grade iraes can help prevent the occurrence of complications, such as GI perforation.
University of Texas Southwestern Medical Center Department of Internal Medicine Grand Rounds October 26, 2018
 University of Texas Southwestern Medical Center Department of Internal Medicine Grand Rounds October 26, 2018 Title: Immune Checkpoint Inhibitor related Endocrinopathies Speaker: Sadia Ali, M.D. This is
University of Texas Southwestern Medical Center Department of Internal Medicine Grand Rounds October 26, 2018 Title: Immune Checkpoint Inhibitor related Endocrinopathies Speaker: Sadia Ali, M.D. This is
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS
 ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 1. NAME OF THE MEDICINAL PRODUCT YERVOY 5 mg/ml concentrate for solution for infusion 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each ml of concentrate contains
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 1. NAME OF THE MEDICINAL PRODUCT YERVOY 5 mg/ml concentrate for solution for infusion 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each ml of concentrate contains
KEYTRUDA Pembrolizumab
 PRODUCT MONOGRAPH INCLUDING PATIENT MEDICATION INFORMATION KEYTRUDA Pembrolizumab powder for solution for infusion 50 mg solution for infusion 100 mg/4ml vial Antineoplastic agent, monoclonal antibody
PRODUCT MONOGRAPH INCLUDING PATIENT MEDICATION INFORMATION KEYTRUDA Pembrolizumab powder for solution for infusion 50 mg solution for infusion 100 mg/4ml vial Antineoplastic agent, monoclonal antibody
Immunotherapy for NSCLC: Current State of the Art and Future Directions. H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States
 Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Pembrozulimab Induced Collagenous Colitis. Mokshya Sharma 1, MD, Santhosh Ambika 2, MD University of Nevada, Reno SOM
 Pembrozulimab Induced Collagenous Colitis Mokshya Sharma 1, MD, Santhosh Ambika 2, MD University of Nevada, Reno SOM Background Immune modulating therapy that targets PD1 pathway such as pembrozulimab
Pembrozulimab Induced Collagenous Colitis Mokshya Sharma 1, MD, Santhosh Ambika 2, MD University of Nevada, Reno SOM Background Immune modulating therapy that targets PD1 pathway such as pembrozulimab
Nivolumab Ipilimumab Combination Therapy
 INDICATIONS FOR USE: Nivolumab Ipilimumab Combination INDICATION ICD10 Regimen Code *Reimbursement Status Nivolumab in combination with ipilimumab is indicated for the treatment of advanced (unresectable
INDICATIONS FOR USE: Nivolumab Ipilimumab Combination INDICATION ICD10 Regimen Code *Reimbursement Status Nivolumab in combination with ipilimumab is indicated for the treatment of advanced (unresectable
Immune-Mediated Adverse Reactions Management Guide
 Immune-Mediated Adverse Reactions Management Guide Please see Important Safety Information for OPDIVO on pages 35 39 and US Full Prescribing Information for OPDIVO. Please refer to the end of the Important
Immune-Mediated Adverse Reactions Management Guide Please see Important Safety Information for OPDIVO on pages 35 39 and US Full Prescribing Information for OPDIVO. Please refer to the end of the Important
Immunotherapy toxicities. Dr Fiona Taylor
 Immunotherapy toxicities Dr Fiona Taylor Outline Understand toxicities Anticipate toxicities Key steps to safely using and achieving the most benefits from immunotherapies for patients Manage toxicities
Immunotherapy toxicities Dr Fiona Taylor Outline Understand toxicities Anticipate toxicities Key steps to safely using and achieving the most benefits from immunotherapies for patients Manage toxicities
Supplementary Online Content
 Supplementary Online Content Powles T, O Donnell PH, Massard C, et al. Efficacy and safety of durvalumab in locally advanced or metastatic urothelial carcinoma: updated results from a phase 1/2 openlabel
Supplementary Online Content Powles T, O Donnell PH, Massard C, et al. Efficacy and safety of durvalumab in locally advanced or metastatic urothelial carcinoma: updated results from a phase 1/2 openlabel
KEYTRUDA Pembrolizumab
 PRODUCT MONOGRAPH INCLUDING PATIENT MEDICATION INFORMATION KEYTRUDA Pembrolizumab powder for solution for infusion 50 mg solution for infusion 100 mg/4ml vial Antineoplastic agent, monoclonal antibody
PRODUCT MONOGRAPH INCLUDING PATIENT MEDICATION INFORMATION KEYTRUDA Pembrolizumab powder for solution for infusion 50 mg solution for infusion 100 mg/4ml vial Antineoplastic agent, monoclonal antibody
Tumor Immunity and Immunotherapy. Andrew Lichtman M.D., Ph.D. Brigham and Women s Hospital Harvard Medical School
 Tumor Immunity and Immunotherapy Andrew Lichtman M.D., Ph.D. Brigham and Women s Hospital Harvard Medical School Lecture Outline Evidence for tumor immunity Types of tumor antigens Generation of anti-tumor
Tumor Immunity and Immunotherapy Andrew Lichtman M.D., Ph.D. Brigham and Women s Hospital Harvard Medical School Lecture Outline Evidence for tumor immunity Types of tumor antigens Generation of anti-tumor
Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management
 Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management Stacey Jassey Megan Brafford David Kwasny This CE activity was originally presented live at the 2015 NASP Annual Meeting
Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management Stacey Jassey Megan Brafford David Kwasny This CE activity was originally presented live at the 2015 NASP Annual Meeting
Managing Adverse Events Associated with Immuno-oncologic Agents
 Managing Adverse Events Associated with Immuno-oncologic Agents Jennifer Diehl RN, BSN, OCN Cutaneous Oncology Program Moffitt Cancer Center Tampa, FL September 10, 2015 12-1 p.m. EST ICLIO ecourse 05
Managing Adverse Events Associated with Immuno-oncologic Agents Jennifer Diehl RN, BSN, OCN Cutaneous Oncology Program Moffitt Cancer Center Tampa, FL September 10, 2015 12-1 p.m. EST ICLIO ecourse 05
Immuno-Oncology: Essentials for Nurses in Cancer Care
 Immuno-Oncology: Essentials for Nurses in Cancer Care BERNADINE O LEARY RN, MN, CON (C) CLINICAL EDUCATOR, EASTERN HEALTH CANCER CARE PROGRAM COURSE FACILITATOR- EASTERN HEALTH ADULT CHEMOTHERAPY COURSE
Immuno-Oncology: Essentials for Nurses in Cancer Care BERNADINE O LEARY RN, MN, CON (C) CLINICAL EDUCATOR, EASTERN HEALTH CANCER CARE PROGRAM COURSE FACILITATOR- EASTERN HEALTH ADULT CHEMOTHERAPY COURSE
KEYTRUDA (pembrolizumab) for injection, for intravenous use KEYTRUDA (pembrolizumab) injection, for intravenous use Initial U.S.
 for injection, for intravenous use KEYTRUDA (pembrolizumab) injection, for intravenous use Initial U.S.") HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use KEYTRUDA safely and effectively. See full prescribing information for KEYTRUDA. KEYTRUDA (pembrolizumab)
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use KEYTRUDA safely and effectively. See full prescribing information for KEYTRUDA. KEYTRUDA (pembrolizumab)
KEYTRUDA (pembrolizumab) for injection, for intravenous use KEYTRUDA (pembrolizumab) injection, for intravenous use Initial U.S.
 for injection, for intravenous use KEYTRUDA (pembrolizumab) injection, for intravenous use Initial U.S.") HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use safely and effectively. See full prescribing information for. (pembrolizumab) for injection, for
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use safely and effectively. See full prescribing information for. (pembrolizumab) for injection, for
RAVE DATA ENTRY GUIDELINES S1400 & SUB-STUDIES. Protocol Ver. 1/8/18
 RAVE DATA ENTRY GUIDELINES S1400 & SUB-STUDIES Protocol Ver. 1/8/18 S1400 Forms Case Report Forms Onstudy: Patient & Disease Description Form 3 Onstudy: Prior Treatment Form 4 Source Documentation: Baseline
RAVE DATA ENTRY GUIDELINES S1400 & SUB-STUDIES Protocol Ver. 1/8/18 S1400 Forms Case Report Forms Onstudy: Patient & Disease Description Form 3 Onstudy: Prior Treatment Form 4 Source Documentation: Baseline
KEYTRUDA (pembrolizumab) for injection, for intravenous use KEYTRUDA (pembrolizumab) injection, for intravenous use Initial U.S.
 for injection, for intravenous use KEYTRUDA (pembrolizumab) injection, for intravenous use Initial U.S.") HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use safely and effectively. See full prescribing information for. (pembrolizumab) for injection, for
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use safely and effectively. See full prescribing information for. (pembrolizumab) for injection, for
Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment
 Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment Patrick Medina, Pharm.D., BCOP Professor The University of Oklahoma College of Medicine Stephenson Cancer Center Faculty Disclosure
Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment Patrick Medina, Pharm.D., BCOP Professor The University of Oklahoma College of Medicine Stephenson Cancer Center Faculty Disclosure
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS
 ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked
9/22/2016. Introduction / Goals. What is Cancer? Pharmacologic Strategies to Treat Cancer. Immune System Modulation
 Immunomodulatory Therapies in Cancer Treatment Bill O Hara, PharmD, BCPS, BCOP Advanced Practice Pharmacist, Oncology/BMT Thomas Jefferson University Hospital Introduction / Goals What is Cancer? How can
Immunomodulatory Therapies in Cancer Treatment Bill O Hara, PharmD, BCPS, BCOP Advanced Practice Pharmacist, Oncology/BMT Thomas Jefferson University Hospital Introduction / Goals What is Cancer? How can
KEYTRUDA Pembrolizumab
 PRODUCT MONOGRAPH INCLUDING PATIENT MEDICATION INFORMATION KEYTRUDA Pembrolizumab powder for solution for infusion 50 mg solution for infusion 100 mg/4ml vial Antineoplastic agent, monoclonal antibody
PRODUCT MONOGRAPH INCLUDING PATIENT MEDICATION INFORMATION KEYTRUDA Pembrolizumab powder for solution for infusion 50 mg solution for infusion 100 mg/4ml vial Antineoplastic agent, monoclonal antibody
BAVENCIO is supplied in a single-dose vial of 200 mg/10 ml (20 mg/ml) individually packed
 individually packed") Coding for BAVENCIO (avelumab) Injection 20 mg/ml in the Hospital Outpatient Department BAVENCIO is indicated for the treatment of: Adults and pediatric patients 12 years and older with metastatic Merkel
Coding for BAVENCIO (avelumab) Injection 20 mg/ml in the Hospital Outpatient Department BAVENCIO is indicated for the treatment of: Adults and pediatric patients 12 years and older with metastatic Merkel
New Oncology Drugs: Nadeem Ikhlaque, M.D Subtitle Would Go Here
 New Oncology Drugs: A PowerPoint Brief Primer Cover Title Nadeem Ikhlaque, M.D 05.19.2017 Subtitle Would Go Here Learning Objectives List novel chemotherapies and the indications of these newer agents
New Oncology Drugs: A PowerPoint Brief Primer Cover Title Nadeem Ikhlaque, M.D 05.19.2017 Subtitle Would Go Here Learning Objectives List novel chemotherapies and the indications of these newer agents
First and only FDA-approved combination of two Immuno-Oncology agents 1
 Bristol-Myers Squibb Receives Approval from the U.S. Food and Drug Administration for the Opdivo (nivolumab) + Yervoy (ipilimumab) Regimen in BRAF V600 Wild-Type Unresectable or Metastatic Melanoma First
Bristol-Myers Squibb Receives Approval from the U.S. Food and Drug Administration for the Opdivo (nivolumab) + Yervoy (ipilimumab) Regimen in BRAF V600 Wild-Type Unresectable or Metastatic Melanoma First
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS
 ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked
NEW ZEALAND DATA SHEET
 NEW ZEALAND DATA SHEET 1 PRODUCT NAME KEYTRUDA 50 mg powder for solution for infusion. 2 QUALITATIVE AND QUANTITATIVE COMPOSITION CAS No.: 1374853-91-4 One vial contains 50 mg of pembrolizumab. After reconstitution,
NEW ZEALAND DATA SHEET 1 PRODUCT NAME KEYTRUDA 50 mg powder for solution for infusion. 2 QUALITATIVE AND QUANTITATIVE COMPOSITION CAS No.: 1374853-91-4 One vial contains 50 mg of pembrolizumab. After reconstitution,
Immunotherapy Overview, Rationale, and Role in Clinical Practice
 Immunotherapy Overview, Rationale, and Role in Clinical Practice Financial Disclosure Bradi L. Frei, PharmD, BCOP, BCPS has no relevant financial relationships with commercial interests to disclose. OBJECTIVES
Immunotherapy Overview, Rationale, and Role in Clinical Practice Financial Disclosure Bradi L. Frei, PharmD, BCOP, BCPS has no relevant financial relationships with commercial interests to disclose. OBJECTIVES
ICLIO Webinar: Immuno-Oncology: From a Community Radiologist Perspective Michael J. DeLeo III, MD
 ICLIO Webinar: Immuno-Oncology: From a Community Radiologist Perspective Michael J. DeLeo III, MD Foundation Medical Partners Southern New Hampshire Health System December 1, 2016 accc-iclio.org Overview
ICLIO Webinar: Immuno-Oncology: From a Community Radiologist Perspective Michael J. DeLeo III, MD Foundation Medical Partners Southern New Hampshire Health System December 1, 2016 accc-iclio.org Overview
Case report: AVELUMAB INDUCING HYPOTHYROIDISM AND HYPOADRENALISM: A CASE REPORT AND REVIEW OF LITERATURE
 Case report: AVELUMAB INDUCING HYPOTHYROIDISM AND HYPOADRENALISM: A CASE REPORT AND REVIEW OF LITERATURE Kashif Aziz*, Amir Shahbaz, Muhammad Umair, Isaac Sachmechi Department of Medicine, Icahn School
Case report: AVELUMAB INDUCING HYPOTHYROIDISM AND HYPOADRENALISM: A CASE REPORT AND REVIEW OF LITERATURE Kashif Aziz*, Amir Shahbaz, Muhammad Umair, Isaac Sachmechi Department of Medicine, Icahn School
Dra. Omayra Reyes, MD. Hematologist- Oncologist. Introduction to Immuno Oncology
 Dra. Omayra Reyes, MD. Hematologist- Oncologist Introduction to Immuno Oncology Disclosure I have no conflicts of interest Objectives Review Basic concepts of onco- immunology. Recognize different mechanisms
Dra. Omayra Reyes, MD. Hematologist- Oncologist Introduction to Immuno Oncology Disclosure I have no conflicts of interest Objectives Review Basic concepts of onco- immunology. Recognize different mechanisms
BCCA Protocol Summary for Treatment of Metastatic or Advanced Renal Cell Carcinoma Using Nivolumab
 BCCA Protocol Summary for Treatment of Metastatic or Advanced Renal Cell Carcinoma Using Nivolumab Protocol Code Tumour Group Contact Physician UGUAVNIV Genitourinary Dr. C. Kollmannsberger ELIGIBILITY:
BCCA Protocol Summary for Treatment of Metastatic or Advanced Renal Cell Carcinoma Using Nivolumab Protocol Code Tumour Group Contact Physician UGUAVNIV Genitourinary Dr. C. Kollmannsberger ELIGIBILITY:
Durvalumab (previously known as MEDI 4736) Maintenance (Arm A3) PLATFORM study
 Maintenance (Arm A3) PLATFORM study") Durvalumab (previously known as MEDI 4736) Maintenance (Arm A3) PLATFORM study PLAnning Treatment For Oesophago-gastric cancer: a Randomised Maintenance therapy trial. ***See Protocol for further details***
Durvalumab (previously known as MEDI 4736) Maintenance (Arm A3) PLATFORM study PLAnning Treatment For Oesophago-gastric cancer: a Randomised Maintenance therapy trial. ***See Protocol for further details***
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Risk Minimisation Information for Healthcare Professionals. Guide for Prescribing
 Risk Minimisation Information for Healthcare Professionals Guide for Prescribing YERVOY (ipilimumab), as monotherapy, is indicated for the treatment of patients with unresectable or metastatic melanoma
Risk Minimisation Information for Healthcare Professionals Guide for Prescribing YERVOY (ipilimumab), as monotherapy, is indicated for the treatment of patients with unresectable or metastatic melanoma
U.S. Food and Drug Administration Accepts Supplemental Biologics License Application for Opdivo
 U.S. Food and Drug Administration Accepts Supplemental Biologics License Application for Opdivo (nivolumab) in Patients with Previously Untreated Advanced Melanoma Application includes CheckMate -066,
U.S. Food and Drug Administration Accepts Supplemental Biologics License Application for Opdivo (nivolumab) in Patients with Previously Untreated Advanced Melanoma Application includes CheckMate -066,
Guidelines for Management of Immunotherapy-Related Adverse Events
 Guidelines f Management of Immunotherapy-Related Adverse Events These guidelines apply to all patients who are receiving, have received, treatment with any of the immune checkpoint inhibits; ipilimumab,
Guidelines f Management of Immunotherapy-Related Adverse Events These guidelines apply to all patients who are receiving, have received, treatment with any of the immune checkpoint inhibits; ipilimumab,
Nivolumab Monotherapy 240mg -14 days
 Nivolumab Monotherapy 240mg -14 days This regimen supercedes NCCP Regimen 00349 Nivolumab Monotherapy as of May 2018 due to a change in the licensed dosing posology. INDICATIONS FOR USE: INDICATION ICD10
Nivolumab Monotherapy 240mg -14 days This regimen supercedes NCCP Regimen 00349 Nivolumab Monotherapy as of May 2018 due to a change in the licensed dosing posology. INDICATIONS FOR USE: INDICATION ICD10
KEYTRUDA (pembrolizumab) for injection, for intravenous use KEYTRUDA (pembrolizumab) injection, for intravenous use Initial U.S.
 for injection, for intravenous use KEYTRUDA (pembrolizumab) injection, for intravenous use Initial U.S.") HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use safely and effectively. See full prescribing information for. (pembrolizumab) for injection, for
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use safely and effectively. See full prescribing information for. (pembrolizumab) for injection, for
Summary of the risk management plan (RMP) for Nivolumab BMS (nivolumab)
 for Nivolumab BMS (nivolumab)") EMA/359171/2015 Summary of the risk management plan (RMP) for Nivolumab BMS (nivolumab) This is a summary of the risk management plan (RMP) for Nivolumab BMS, which details the measures to be taken in
EMA/359171/2015 Summary of the risk management plan (RMP) for Nivolumab BMS (nivolumab) This is a summary of the risk management plan (RMP) for Nivolumab BMS, which details the measures to be taken in
IMMUNOTHERAPY OVERVIEW. Gloria Roldan Urgoiti MD, MSc, FRCPC Tom Baker Cancer Centre April 22, 2017
 IMMUNOTHERAPY OVERVIEW Gloria Roldan Urgoiti MD, MSc, FRCPC Tom Baker Cancer Centre April 22, 2017 Faculty/Presenter Disclosure Speaker: Dr. Gloria Roldan Urgoiti Relationships with commercial interests:
IMMUNOTHERAPY OVERVIEW Gloria Roldan Urgoiti MD, MSc, FRCPC Tom Baker Cancer Centre April 22, 2017 Faculty/Presenter Disclosure Speaker: Dr. Gloria Roldan Urgoiti Relationships with commercial interests:
Bristol-Myers Squibb Announces Regulatory Update for Opdivo (nivolumab) in Advanced Melanoma
 in Advanced Melanoma") December 2, 2015 Bristol-Myers Squibb Announces Regulatory Update for Opdivo (nivolumab) in Advanced Melanoma (PRINCETON, NJ, November 27, 2015) Bristol-Myers Squibb Company (NYSE:BMY) announced that the
December 2, 2015 Bristol-Myers Squibb Announces Regulatory Update for Opdivo (nivolumab) in Advanced Melanoma (PRINCETON, NJ, November 27, 2015) Bristol-Myers Squibb Company (NYSE:BMY) announced that the
Nivolumab/Ipilimumab Combination Therapy for Renal Cell Carcinoma (RCC)
") Nivolumab/Ipilimumab Combination Therapy for Renal Cell Carcinoma (RCC) An HCP Tool From the Immuno-Oncology Essentials Initiative The combination of nivolumab (Opdivo ) and ipilimumab (Yervoy ) is approved
Nivolumab/Ipilimumab Combination Therapy for Renal Cell Carcinoma (RCC) An HCP Tool From the Immuno-Oncology Essentials Initiative The combination of nivolumab (Opdivo ) and ipilimumab (Yervoy ) is approved
Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016
 Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016
Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016
Merck and DNAtrix Announce Phase 2 Immuno-Oncology Collaboration in Patients with Aggressive Form of Brain Cancer
 Merck and DNAtrix Announce Phase 2 Immuno-Oncology Collaboration in Patients with Aggressive Form of Brain Cancer KENILWORTH, N.J. & HOUSTON--(BUSINESS WIRE)--Merck (NYSE:MRK), known as MSD outside the
Merck and DNAtrix Announce Phase 2 Immuno-Oncology Collaboration in Patients with Aggressive Form of Brain Cancer KENILWORTH, N.J. & HOUSTON--(BUSINESS WIRE)--Merck (NYSE:MRK), known as MSD outside the
Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up
 Annals of Oncology 28 (Supplement 4): iv119 iv142, 2017 doi:10.1093/annonc/mdx225 CLINICAL PRACTICE GUIDELINES Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis,
Annals of Oncology 28 (Supplement 4): iv119 iv142, 2017 doi:10.1093/annonc/mdx225 CLINICAL PRACTICE GUIDELINES Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis,