Do any benign polyps require an operation?
|
|
|
- Tracey Cunningham
- 5 years ago
- Views:
Transcription




1 Do any benign polyps require an operation? Kevin Waschke MD.,CM., FRCPC, FASGE McGill University Health Center President Elect Canadian Association of Gastroenterology Colonoscopy Education Day - Tuesday October 2 nd 2018 ( )
2 X X X X X CanMEDS Roles Covered Medical Expert (as Medical Experts, physicians integrate all of the CanMEDS Roles, applying medical knowledge, clinical skills, and professional values in their provision of highquality and safe patient-centered care. Medical Expert is the central physician Role in the CanMEDS Framework and defines the physician s clinical scope of practice.) Communicator (as Communicators, physicians form relationships with patients and their families that facilitate the gathering and sharing of essential information for effective health care.) Collaborator (as Collaborators, physicians work effectively with other health care professionals to provide safe, high-quality, patient-centred care.) Leader (as Leaders, physicians engage with others to contribute to a vision of a high-quality health care system and take responsibility for the delivery of excellent patient care through their activities as clinicians, administrators, scholars, or teachers.) Health Advocate (as Health Advocates, physicians contribute their expertise and influence as they work with communities or patient populations to improve health. They work with those they serve to determine and understand needs, speak on behalf of others when required, and support the mobilization of resources to effect change.) Scholar (as Scholars, physicians demonstrate a lifelong commitment to excellence in practice through continuous learning and by teaching others, evaluating evidence, and contributing to scholarship.) Professional (as Professionals, physicians are committed to the health and well-being of individual patients and society through ethical practice, high personal standards of behaviour, accountability to the profession and society, physician-led regulation, and maintenance of personal health.)
3 Disclosure Pendopharm - Advisory Board (2018/9)
4 Learning Objectives After attending this session, the learner should be able to 1. Understand what techniques can be used to characterize polyps 2. Understand which polyps should be referred for surgical resection 3. Understand which polyps are potentially amenable to advanced polypectomy techniques
5 Polypectomy and surgery Most polyps can and should be removed endoscopically Surgery is indicated for polyps that are: Malignant with a high risk of lymph node metastases Not removable endoscopically* (depends on expertise) Polypectomy skills vary among endoscopists A standardized approach to polyps can avoid unnecessary surgeries
6 Polypectomy techniques 1. Cold biopsy polypectomy (CBP) 2. Cold snare polypectomy (CSP) Routine care 3. Hot snare polypectomy (HSP) 4. Endoscopic mucosal resection (EMR) Specialized care 5. Endoscopic submucosal dissection (ESD)


7 Approach to advanced polyps 1. Identify the polyp (careful withdrawal technique many flat polyps can be difficult to detect without careful inspection) 2. Determine the size, morphology of the polyp Paris classification 1 routine EMR + surgery 1. Gastro Endo Vol. 58, No. 6, (Suppl), 2003, S23.

8 3. Inspect the polyp Use white light and NBI technique Take photographs while inspecting Define the pit pattern / NICE classification o Identify high risk features Type V pit pattern Type 3 NICE
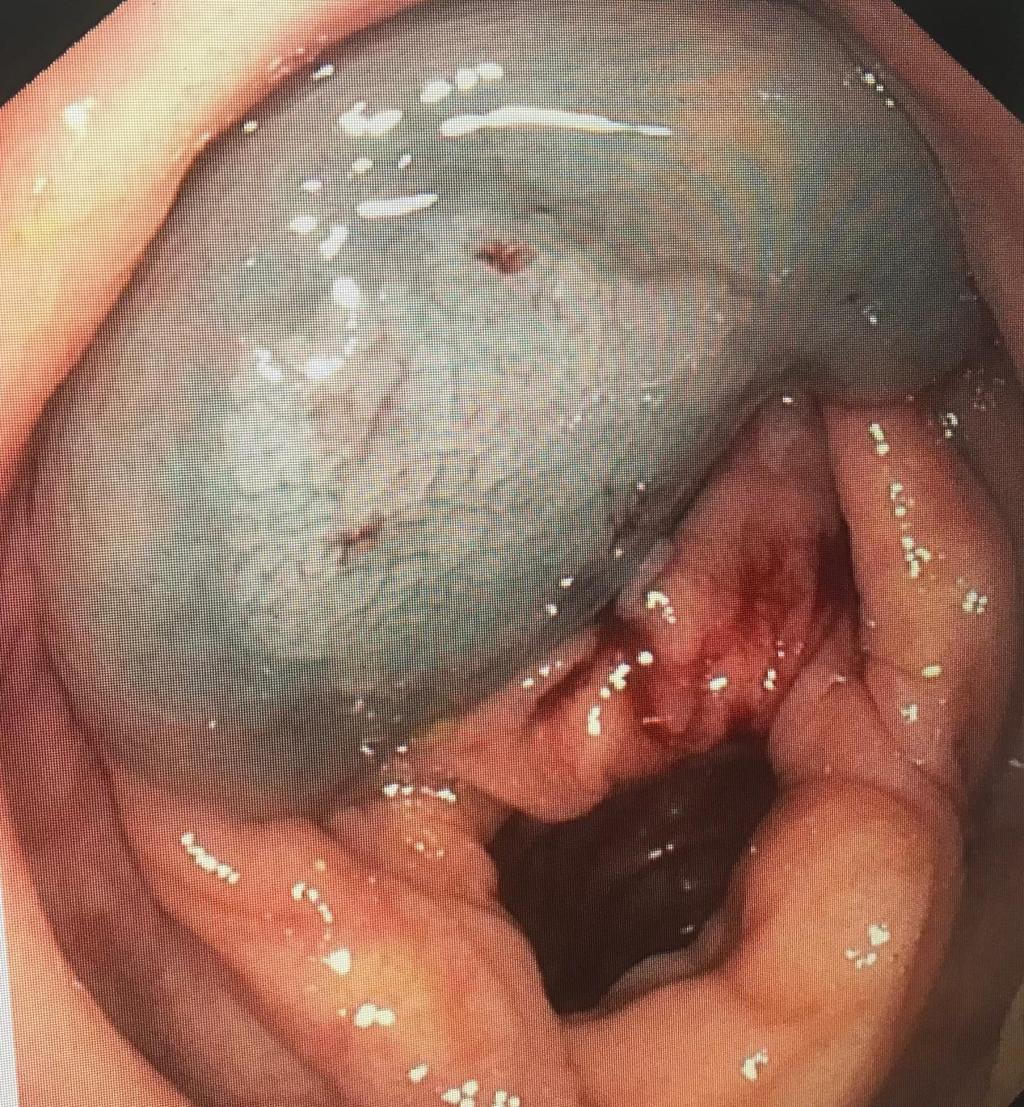
9 Should these polyps be removed endoscopically?
 18 (Suppl.")
10 Kudo Pit pattern Digestive Endoscopy (2006) 18 (Suppl. 1), S52 S56
11 11
12


13 Should these polyps be removed endoscopically?
14 Approach to advanced polyps 4. Assess the ideal position of the polyp / endoscope stability prior to any attempted resection This is easier using a scope imager and is important for referral. o Polyps in the appendiceal orifice, diverticular edge, flexures, difficult loops (unstable position) or near the dentate line are all potentially more difficult. Book cases based on expected procedure time


15 Consider lifting polyps o Minimize complications of electrical current o Improve resection completeness o Identify margins (SSA/Ps) o Identify suspicious lesions via non lifting sign o Improves your tattoo technique 15
16 16
17 17




18 Non-Lifting Sign is a sign of fibrosis / scarring or submucosal involvement Submucosal involvement Fibrosis and scarring Incomplete (partial) polypectomy Biopsies Prior tattoo 18
19 Additional considerations for referral If a polyp has any features that are not routine, consider referral Difficult location (appendix, ileocecal valve, flexures, dentate line, unstable position) Lifting is not working well Indistinct borders (risk of incomplete resection) Near a tattoo or has been biopsied or partially removed
20 If the polyp cannot be removed by you but someone else might be able to 1. Consider referral to a specialist in polypectomy 2. DO NOT BIOPSY (It is OK to inject / use lifting solution as part of inspection) 3. DO NOT PARTIALLY PERFORM POLYPECTOMY 4. Tattoo > 3 cm from the polyp margins 5. Send high resolution pictures with the referral. ( or text if possible)





21 Target Target your biopsy to the high risk features PHOTOGRAPH DO NOT PARTIALLY PERFORM POLYPECTOMY If the polyp cannot be removed by you and you are convinced there are high risk features for a polyp with submucosal involvement Tattoo Tattoo > 3 cm from the polyp margins
22 When to tattoo 1. Suspected cancer 2. Any polyp > 1 cm (suggested by ESGE guideline) RATIONALE: 1. Higher rate of malignant polyps in polyps > 1 cm. 2. Higher rate of recurrence in piecemeal polypectomy Any polyp requiring EMR should have surveillance including biopsy of polypectomy site not all scars are easy to find post Enter footer here 22


23 Tattoo technique Discuss with local surgeon re their preference - 5 cm proximal to the lesion (1-2 folds). - SALINE then BLACK then SALINE (Avoid staining the peritoneal cavity!) Enter footer here 23
 tent the needle")


24 Keys to injection technique 45 degree angle to the mucosa 1) tent the needle tip slightly upwards OR 2) start injecting fluid before the needle pierces the mucosa it is always easier to inject into areas that have already been lifted 24
25 When to refer mega polyps (pedunculated) surgery or specialized polypectomy referral There are no standardized criteria for this indication Cancer risk with polyps > 20 mm Mega polyps can be difficult to remove due to technical factors (putting the snare over the head piecemeal resection, trimming of head) and higher risk of postpolypectomy bleeding Polyps > 30 mm in size are generally more difficult to treat than those < 30 mm Some authors have used ESD to dissect the base 25
26 Polyps that should undergo endoscopic resection Pedunculated polyps Non-pedunculated polyps that are amenable to endoscopic resection Stable endoscope position with good prep No high risk morphology No high risk pit pattern / NBI features Good response to lifting Local expertise Malignant polyps with a low risk histology features for lymph node metastases < 1000 um SM involvement well to mod differentiated no lymphovascular involvement NOTE THAT EMR PATIENTS NEED CLOSE SURVEILLANCE
27 Polyps that should undergo surgery Abnormal morphology (central ulceration, fold convergence) Abnormal pit pattern Type V Kudo pit pattern 2 Type 3 NICE Classification 3 Polyps that are not amenable to endoscopic resection Non-lifting sign* Some locations may be difficult Histologic features that suggest an increased risk of lymph node metastases Deep submucosal involvement (1000 um) Poorly differentiated 1 (G3) Lymphovascular involvement 1. Am J Surg Pathol Feb;36(2): doi: /PAS.0b013e318235edee. 2. Digestive Endoscopy (2006) 18 (Suppl. 1), S52 S56 3. Volume 78, No. 4 : 2013 GASTROINTESTINAL ENDOSCOPY 625
28 Final message Too many polyps are sent to surgery that can be removed endoscopically size is not the issue. Many large / complex polyps can be removed using EMR/ ESD. Photograph, tattoo and refer for EMR.
(Hot Snare) Polypectomy : Best Practice
 Polypectomy : Best Practice") (Hot Snare) Polypectomy : Best Practice Kevin Waschke MD.,CM., FRCPC, FASGE McGill University Health Center President Elect Canadian Association of Gastroenterology Tuesday October 2 nd 1440-1515 X X X
(Hot Snare) Polypectomy : Best Practice Kevin Waschke MD.,CM., FRCPC, FASGE McGill University Health Center President Elect Canadian Association of Gastroenterology Tuesday October 2 nd 1440-1515 X X X
THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD
 SNARE THE CASE FOR EMR AND ESD") THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD Surgical Oncology Network meeting Dr. Eric Lam MD FRCPC October 14, 2017 DISCLOSURES None OBJECTIVES Appreciate
THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD Surgical Oncology Network meeting Dr. Eric Lam MD FRCPC October 14, 2017 DISCLOSURES None OBJECTIVES Appreciate
Advanced techniques for resection of large polyps. John G. Lee, MD February 2, 2018
 Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
Pre and Post Liver Transplantation Issues in NAFLD
 Pre and Post Liver Transplantation Issues in NAFLD Karim Qumosani MD, PCME, ABIM, FRCPC Multiorgan Transplant Unit University Hospital London Ontario, Canada Financial Disclosures Research Grants Merck,
Pre and Post Liver Transplantation Issues in NAFLD Karim Qumosani MD, PCME, ABIM, FRCPC Multiorgan Transplant Unit University Hospital London Ontario, Canada Financial Disclosures Research Grants Merck,
Rectal EMR: Techniques and Tips
 Rectal EMR: Techniques and Tips Dr Paul Urquhart Epworth Eastern Eastern Health (Head of Endoscopy) The context of EMR Basic Technique Recurrence Perforation Bleeding Introduction 1 I don t treat rectal
Rectal EMR: Techniques and Tips Dr Paul Urquhart Epworth Eastern Eastern Health (Head of Endoscopy) The context of EMR Basic Technique Recurrence Perforation Bleeding Introduction 1 I don t treat rectal
Colon Polyps: Detection, Inspection and Characteristics
 Colon Polyps: Detection, Inspection and Characteristics Stephen Kim, M.D. Assistant Professor of Medicine Interventional Endoscopy Services UCLA Division of Digestive Diseases September 29, 2018 1 Disclosures
Colon Polyps: Detection, Inspection and Characteristics Stephen Kim, M.D. Assistant Professor of Medicine Interventional Endoscopy Services UCLA Division of Digestive Diseases September 29, 2018 1 Disclosures
Emerging Interventions in Endoscopy. Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital
 Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
Large polyps: EMR, ESD, TEM and segmental resection. Terry Phang 2017 SON fall update
 Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
Improving Your Adenoma Detection Rate
 Improving Your Adenoma Detection Rate JILL TINMOUTH, ASSOCIATE PROFESSOR, UNIVERSITY OF TORONTO JERRY MCGRATH, ASSOCIATE PROFESSOR, MEMORIAL UNIVERSITY OF NEWFOUNDLAND FEB. 11 2017 X CanMEDS Roles Covered
Improving Your Adenoma Detection Rate JILL TINMOUTH, ASSOCIATE PROFESSOR, UNIVERSITY OF TORONTO JERRY MCGRATH, ASSOCIATE PROFESSOR, MEMORIAL UNIVERSITY OF NEWFOUNDLAND FEB. 11 2017 X CanMEDS Roles Covered
Is there justification for levels of polyp competency? Dr Roland Valori Gloucestershire Hospitals United Kingdom
 Is there justification for levels of polyp competency? Dr Roland Valori Gloucestershire Hospitals United Kingdom What exactly will be required? Defining levels of polypectomy competency in terms of complexity/time/risk
Is there justification for levels of polyp competency? Dr Roland Valori Gloucestershire Hospitals United Kingdom What exactly will be required? Defining levels of polypectomy competency in terms of complexity/time/risk
Difficult Polypectomy 2015 Tool of the Trade
 Difficult Polypectomy 2015 Tool of the Trade Jonathan Cohen, MD FACG FASGE Clinical Professor of Medicine NYU Langone School of Medicine Improving Therapeutics in the Colon Improved detection of polyp
Difficult Polypectomy 2015 Tool of the Trade Jonathan Cohen, MD FACG FASGE Clinical Professor of Medicine NYU Langone School of Medicine Improving Therapeutics in the Colon Improved detection of polyp
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Endoscopic Submucosal Dissection ESD
 Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Benchmarking For Colonoscopy. Technology and Technique to Improve Adenoma Detection
 Benchmarking For Colonoscopy Technology and Technique to Improve Adenoma Detection Objectives 1. Review the latest data on performance characteristics and efficacy for colon cancer prevention 2. Highlight
Benchmarking For Colonoscopy Technology and Technique to Improve Adenoma Detection Objectives 1. Review the latest data on performance characteristics and efficacy for colon cancer prevention 2. Highlight
FUNCTIONAL DISORDERS TREATMENT ADVANCES. Dr. Adriana Lazarescu MD FRCPC Director GI Motility Lab, Edmonton Associate Professor University of Alberta
 FUNCTIONAL DISORDERS TREATMENT ADVANCES Dr. Adriana Lazarescu MD FRCPC Director GI Motility Lab, Edmonton Associate Professor University of Alberta Name: Dr. Adriana Lazarescu Conflict of Interest Disclosure
FUNCTIONAL DISORDERS TREATMENT ADVANCES Dr. Adriana Lazarescu MD FRCPC Director GI Motility Lab, Edmonton Associate Professor University of Alberta Name: Dr. Adriana Lazarescu Conflict of Interest Disclosure
Quality Measures In Colonoscopy: Why Should I Care?
 Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
Short and longterm outcomes after endoscopic resection of malignant polyps.
 Short and longterm outcomes after endoscopic resection of malignant polyps. Short and longterm outcomes High risk features Lymph node metastasis Lymph node metastases sm1 sm2 sm3 Son 2008 3.1 % 14.9% 25.0
Short and longterm outcomes after endoscopic resection of malignant polyps. Short and longterm outcomes High risk features Lymph node metastasis Lymph node metastases sm1 sm2 sm3 Son 2008 3.1 % 14.9% 25.0
Management of pt1 polyps. Maria Pellise
 Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Supporting Information 2. ESGE QIC Lower GI Delphi voting process: Round 1 Working Group chair: Michal F. Kaminski, Poland
 Supporting Information 2. ESGE QIC Lower GI Delphi voting process: Round 1 Working chair: Michal F. Kaminski, Poland Population Interventions Comparator Outcome Additional evidence 1.1 Rate of adequate
Supporting Information 2. ESGE QIC Lower GI Delphi voting process: Round 1 Working chair: Michal F. Kaminski, Poland Population Interventions Comparator Outcome Additional evidence 1.1 Rate of adequate
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Aberrant crypt foci, chromocolonoscopy for, 539 540 Absorptive stains, for chromocolonoscopy, 522 524 Accessories, for colonoscopy, 680 684
Note: Page numbers of article titles are in boldface type. A Aberrant crypt foci, chromocolonoscopy for, 539 540 Absorptive stains, for chromocolonoscopy, 522 524 Accessories, for colonoscopy, 680 684
Gastric Polyps. Bible class
 Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Accepted Manuscript. En bloc resection for mm polyps to reduce post-colonoscopy cancer and surveillance. C. Hassan, M. Rutter, A.
 Accepted Manuscript En bloc resection for 10-20 mm polyps to reduce post-colonoscopy cancer and surveillance C. Hassan, M. Rutter, A. Repici PII: S1542-3565(19)30412-4 DOI: https://doi.org/10.1016/j.cgh.2019.04.022
Accepted Manuscript En bloc resection for 10-20 mm polyps to reduce post-colonoscopy cancer and surveillance C. Hassan, M. Rutter, A. Repici PII: S1542-3565(19)30412-4 DOI: https://doi.org/10.1016/j.cgh.2019.04.022
Bowel Screening Colonoscopy in Glasgow How well are we doing? How well should we be doing? How can we evidence and improve performance?
 Bowel Screening Colonoscopy in Glasgow 2017 How well are we doing? How well should we be doing? How can we evidence and improve performance? Bowel Screening Standards - Scotland Definitions Completion
Bowel Screening Colonoscopy in Glasgow 2017 How well are we doing? How well should we be doing? How can we evidence and improve performance? Bowel Screening Standards - Scotland Definitions Completion
EMR, ESD and Beyond. Peter Draganov MD. Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida
 EMR, ESD and Beyond Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated by Endoscopy
EMR, ESD and Beyond Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated by Endoscopy
Endoscopic Mucosal Resection (EMR) & Endoscopic Submucosal Dissection (ESD)
 & Endoscopic Submucosal Dissection (ESD)") Endoscopic Mucosal Resection (EMR) & Endoscopic Submucosal Dissection (ESD) Minimally Invasive Polyp Removal IE-02700-Understanding EMR and ESD Brochure_R3.indd 1 Occasionally, a polyp that infiltrates
Endoscopic Mucosal Resection (EMR) & Endoscopic Submucosal Dissection (ESD) Minimally Invasive Polyp Removal IE-02700-Understanding EMR and ESD Brochure_R3.indd 1 Occasionally, a polyp that infiltrates
Research Article Endoscopic Management of Nonlifting Colon Polyps
 Diagnostic and Therapeutic Endoscopy Volume 2013, Article ID 412936, 5 pages http://dx.doi.org/10.1155/2013/412936 Research Article Endoscopic Management of Nonlifting Colon Polyps Shai Friedland, 1,2
Diagnostic and Therapeutic Endoscopy Volume 2013, Article ID 412936, 5 pages http://dx.doi.org/10.1155/2013/412936 Research Article Endoscopic Management of Nonlifting Colon Polyps Shai Friedland, 1,2
The Paris classification of colonic lesions
 The Paris classification of colonic lesions Training to improve the interobserver agreement among international experts Sascha van Doorn, MD, PhD-student in CRC-reserach group of Evelien Dekker Introduction
The Paris classification of colonic lesions Training to improve the interobserver agreement among international experts Sascha van Doorn, MD, PhD-student in CRC-reserach group of Evelien Dekker Introduction
Dysplasia 4/19/2017. How do I practice Chromoendoscopy for Surveillance of Colitis? SCENIC: Polypoid Dysplasia in UC. Background
 SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
How to treat early gastric cancer? Endoscopy
 How to treat early gastric cancer? Endoscopy Presented by Pierre H. Deprez Institution Cliniques universitaires Saint-Luc, Brussels Université catholique de Louvain 2 3 4 5 6 Background Diagnostic or therapeutic
How to treat early gastric cancer? Endoscopy Presented by Pierre H. Deprez Institution Cliniques universitaires Saint-Luc, Brussels Université catholique de Louvain 2 3 4 5 6 Background Diagnostic or therapeutic
Spartan Medical Research Journal
 Spartan Medical Research Journal Research at Michigan State University College of Osteopathic Medicine Volume 2 Number 2 Winter, 2017 Pages 14-21 Title: Endoscopic Combined Snare-Forceps Technique for
Spartan Medical Research Journal Research at Michigan State University College of Osteopathic Medicine Volume 2 Number 2 Winter, 2017 Pages 14-21 Title: Endoscopic Combined Snare-Forceps Technique for
Endoscopic Corner CASE 1. Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R
 170 Endoscopic Corner Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R CASE 1 A 54-year-old woman underwent a colorectal cancer screening. Her fecal immunochemical test was positive.
170 Endoscopic Corner Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R CASE 1 A 54-year-old woman underwent a colorectal cancer screening. Her fecal immunochemical test was positive.
SE140. guidelines. Background! Methods!
 SE140 European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition Management of lesions detected in colorectal cancer screening Co-Funded by the Health Programme
SE140 European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition Management of lesions detected in colorectal cancer screening Co-Funded by the Health Programme
Measure #425: Photodocumentation of Cecal Intubation National Quality Strategy Domain: Effective Clinical Care
 Measure #425: Photodocumentation of Cecal Intubation National Quality Strategy Domain: Effective Clinical Care 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: The
Measure #425: Photodocumentation of Cecal Intubation National Quality Strategy Domain: Effective Clinical Care 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: The
EXPERT WORKING GROUP Surveillance after neoplasia removal. Meeting Chicago, May 5th 2017 Chair: Rodrigo Jover Uri Ladabaum
 EXPERT WORKING GROUP Surveillance after neoplasia removal Meeting Chicago, May 5th 2017 Chair: Rodrigo Jover Uri Ladabaum AIM To improve the quality of the evidences we have regarding post- polypectomy
EXPERT WORKING GROUP Surveillance after neoplasia removal Meeting Chicago, May 5th 2017 Chair: Rodrigo Jover Uri Ladabaum AIM To improve the quality of the evidences we have regarding post- polypectomy
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
How to characterize dysplastic lesions in IBD?
 How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
Principles of diagnosis, work-up and therapy The Gastroenterologist s role
 Principles of diagnosis, work-up and therapy The Gastroenterologist s role Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University
Principles of diagnosis, work-up and therapy The Gastroenterologist s role Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University
High Resolution Esophageal Manometry
 High Resolution Esophageal Manometry Dr. Geoffrey Turnbull MD, FRCPC Dalhousie University Dr. Yvonne Tse MD, FRCPC University of Toronto Name: Dr. Geoffrey Turnbull Conflict of Interest Disclosure (over
High Resolution Esophageal Manometry Dr. Geoffrey Turnbull MD, FRCPC Dalhousie University Dr. Yvonne Tse MD, FRCPC University of Toronto Name: Dr. Geoffrey Turnbull Conflict of Interest Disclosure (over
Treatment Strategy for Non-curative Resection of Early Gastric Cancer. Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea
 Treatment Strategy for Non-curative Resection of Early Gastric Cancer Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea Classic EMR/ESD data analysis style Endoscopic resection
Treatment Strategy for Non-curative Resection of Early Gastric Cancer Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea Classic EMR/ESD data analysis style Endoscopic resection
Finding and Removing Difficult Polyps (safely)
") Finding and Removing Difficult Polyps (safely) David Lieberman MD Chief, Division of Gastroenterology and Hepatology Oregon Health and Science University Colonoscopy Clouds Interval Cancers Interval Cancer:
Finding and Removing Difficult Polyps (safely) David Lieberman MD Chief, Division of Gastroenterology and Hepatology Oregon Health and Science University Colonoscopy Clouds Interval Cancers Interval Cancer:
Retroflexion and prevention of right-sided colon cancer following colonoscopy: How I approach it
 Retroflexion and prevention of right-sided colon cancer following colonoscopy: How I approach it Douglas K Rex 1 MD, MACG 1. Indiana University School of Medicine Division of Gastroenterology/Hepatology
Retroflexion and prevention of right-sided colon cancer following colonoscopy: How I approach it Douglas K Rex 1 MD, MACG 1. Indiana University School of Medicine Division of Gastroenterology/Hepatology
3/8/2017. Why is endoscopic marking important? Goals of program
 DISCLOSURES Successful completion: Participants must attend the entire program, including any resulting Q & A, and submit required documentation. "Keep Calm and Get the GI Tract Tattooed: Proper Techniques
DISCLOSURES Successful completion: Participants must attend the entire program, including any resulting Q & A, and submit required documentation. "Keep Calm and Get the GI Tract Tattooed: Proper Techniques
Adenoma to Carcinoma Pathway
 It is widely accepted that more than 95% of colorectal cancers arise from adenomatous polyps, which are generally defined as benign lesions with dysplastic epithelium that have variable potential for malignancy.
It is widely accepted that more than 95% of colorectal cancers arise from adenomatous polyps, which are generally defined as benign lesions with dysplastic epithelium that have variable potential for malignancy.
With CRC Screening Rates on the Rise, Quality Control Becomes Center of Attention
 print this article In the News ISSUE: OCTOBER 2009 VOLUME: 60:10 With CRC Screening Rates on the Rise, Quality Control Becomes Center of Attention by Monica J. Smith New York In just the past year, New
print this article In the News ISSUE: OCTOBER 2009 VOLUME: 60:10 With CRC Screening Rates on the Rise, Quality Control Becomes Center of Attention by Monica J. Smith New York In just the past year, New
Measure #425: Photodocumentation of Cecal Intubation National Quality Strategy Domain: Effective Clinical Care
 Measure #425: Photodocumentation of Cecal Intubation National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION: The rate of screening
Measure #425: Photodocumentation of Cecal Intubation National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION: The rate of screening
Factors for Endoscopic Submucosal Dissection in Early Colorectal Neoplasms: A Single Center Clinical Experience in China
 ORIGINAL ARTICLE Clin Endosc 2015;48:405-410 http://dx.doi.org/10.5946/ce.2015.48.5.405 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Factors for Endoscopic Submucosal Dissection in Early Colorectal
ORIGINAL ARTICLE Clin Endosc 2015;48:405-410 http://dx.doi.org/10.5946/ce.2015.48.5.405 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Factors for Endoscopic Submucosal Dissection in Early Colorectal
GI Coding Updates. Rhonda Buckholtz, CPC, CPCI, CPMS, CRC, CDEO, CHPSE, CGSC, COBGC, CENTC, CPEDC
 GI Coding Updates Rhonda Buckholtz, CPC, CPCI, CPMS, CRC, CDEO, CHPSE, CGSC, COBGC, CENTC, CPEDC Copyright/Disclaimer 2014 AAPC text CPT copyright 2016 American Medical Association. All rights reserved.
GI Coding Updates Rhonda Buckholtz, CPC, CPCI, CPMS, CRC, CDEO, CHPSE, CGSC, COBGC, CENTC, CPEDC Copyright/Disclaimer 2014 AAPC text CPT copyright 2016 American Medical Association. All rights reserved.
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Introduction. Piecemeal EMR (EPMR) Symposium
 Symposium") Symposium Symposium II - Lower GI : Colonoscopy Issues in 2015 Resection of Large Polyps Using Techniques other than Endoscopic Submucosal Dissection: Piecemeal Resection, Underwater Endoscopic Mucosal
Symposium Symposium II - Lower GI : Colonoscopy Issues in 2015 Resection of Large Polyps Using Techniques other than Endoscopic Submucosal Dissection: Piecemeal Resection, Underwater Endoscopic Mucosal
Endoscopic UltraSound (EUS) Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C.
 Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C.") Endoscopic UltraSound (EUS) Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Research Grants: Disclosures
Endoscopic UltraSound (EUS) Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Research Grants: Disclosures
ADENOMA SURVEILLANCE BCSP Guidance Note No 1 Version 1 September 2009
 ADENOMA SURVEILLANCE BCSP Guidance Note No 1 Version 1 September 2009 Published by: NHS Cancer Screening Programmes Fulwood House Old Fulwood Road Sheffield S10 3TH Tel: 0114 271 1060 Fax: 0114 271 1089
ADENOMA SURVEILLANCE BCSP Guidance Note No 1 Version 1 September 2009 Published by: NHS Cancer Screening Programmes Fulwood House Old Fulwood Road Sheffield S10 3TH Tel: 0114 271 1060 Fax: 0114 271 1089
Quality indicators for colonoscopy and colonoscopist. Mirjana Kalauz Clinical Hospital Center Zagreb
 Quality indicators for colonoscopy and colonoscopist Mirjana Kalauz Clinical Hospital Center Zagreb Why is quality monitoring important in CRC screening programme? Quality adjustment in all endoscopic
Quality indicators for colonoscopy and colonoscopist Mirjana Kalauz Clinical Hospital Center Zagreb Why is quality monitoring important in CRC screening programme? Quality adjustment in all endoscopic
Advice Leaflet Medical Division. Having an Endoscopic Mucosal Resection (Lower) East Lancashire Hospitals NHS Trust
 East Lancashire Hospitals NHS Trust") East Lancashire Hospitals NHS Trust Providing the very best care for our patients in every way Having an Endoscopic Mucosal Resection (Lower) Patient Information Advice Leaflet Medical Division www.elht.nhs.uk
East Lancashire Hospitals NHS Trust Providing the very best care for our patients in every way Having an Endoscopic Mucosal Resection (Lower) Patient Information Advice Leaflet Medical Division www.elht.nhs.uk
Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions
 Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions Digestive Disease Center, Showa University Northern Yokohama Hospital Department of Pathology Yoshiki Wada, Shin-ei Kudo, Hiroshi
Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions Digestive Disease Center, Showa University Northern Yokohama Hospital Department of Pathology Yoshiki Wada, Shin-ei Kudo, Hiroshi
i-scan Mini-Atlas Case studies from clinical practice with HD + and i-scan.
 i-scan Mini-Atlas Case studies from clinical practice with and i-scan. Visible excellence. Gastrointestinal endoscopy with and i-scan. Index Introduction 3 and i-scan at a glance 4 5 PENTAX i-scan in characterization
i-scan Mini-Atlas Case studies from clinical practice with and i-scan. Visible excellence. Gastrointestinal endoscopy with and i-scan. Index Introduction 3 and i-scan at a glance 4 5 PENTAX i-scan in characterization
Size of colorectal polyps determines time taken to remove them endoscopically
 Original article Size of colorectal polyps determines time taken to remove them endoscopically Authors Heechan Kang 1, Mo Hameed Thoufeeq 2 Institutions 1 Department of Medicine, Peterborough Hospitals
Original article Size of colorectal polyps determines time taken to remove them endoscopically Authors Heechan Kang 1, Mo Hameed Thoufeeq 2 Institutions 1 Department of Medicine, Peterborough Hospitals
References. GI Biopsies. What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD
 What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
Screening & Surveillance Guidelines
 Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID
 ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN
 Serrated Adenomas: What do they mean and what to do about them? Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN Colorectal Cancer Molecular Basis Pathway Frequency Genes MSI Precursor Speed
Serrated Adenomas: What do they mean and what to do about them? Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN Colorectal Cancer Molecular Basis Pathway Frequency Genes MSI Precursor Speed
How to remove BE cancer: EMR or ESD? Expected outcome
 How to remove BE cancer: EMR or ESD? Expected outcome Presented by Horst Neuhaus Institution Dpt. of Gastroenterology Evangelisches Krankenhaus Düsseldorf, Germany Indications for endoscopic resection
How to remove BE cancer: EMR or ESD? Expected outcome Presented by Horst Neuhaus Institution Dpt. of Gastroenterology Evangelisches Krankenhaus Düsseldorf, Germany Indications for endoscopic resection
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Interval Cancers: What is Next?
 Interval Cancers: What is Next? Douglas Corley, MD, PhD Kaiser Permanente, Northern California Gastroenterologist, TPMG Director of Delivery Science & Applied Research Defining the mission Mercury project:
Interval Cancers: What is Next? Douglas Corley, MD, PhD Kaiser Permanente, Northern California Gastroenterologist, TPMG Director of Delivery Science & Applied Research Defining the mission Mercury project:
2015 Winter School 대장종양성병변의진단과치료. Dong Kyung Chang. Sungkyunkwan University, School of Medicine Samsung Medical Center
 2017 gastroenterology Winter School 77 2015 Winter School 대장종양성병변의진단과치료 Dong Kyung Chang Sungkyunkwan University, School of Medicine Samsung Medical Center Colon Polyps (Epithelial origin) Neoplastic Premalignant
2017 gastroenterology Winter School 77 2015 Winter School 대장종양성병변의진단과치료 Dong Kyung Chang Sungkyunkwan University, School of Medicine Samsung Medical Center Colon Polyps (Epithelial origin) Neoplastic Premalignant
Clinical Roundtable Monograph
 Clinical Roundtable Monograph Gastroenterology & Hepatology August 2018 Incomplete Resection Rates in Polyps Smaller Than 2 Centimeters Proceedings From a Live Clinical Roundtable Held During Digestive
Clinical Roundtable Monograph Gastroenterology & Hepatology August 2018 Incomplete Resection Rates in Polyps Smaller Than 2 Centimeters Proceedings From a Live Clinical Roundtable Held During Digestive
Commonly Encountered Neuro-Endocrine Tumors of the Gut
 Commonly Encountered Neuro-Endocrine Tumors of the Gut Moderators: Giuseppe Aliperti, MD Steven Edmundowicz, MD Panelists Douglas O. Faigel, MD Professor of Medicine Department of Gastroenterology Oregon
Commonly Encountered Neuro-Endocrine Tumors of the Gut Moderators: Giuseppe Aliperti, MD Steven Edmundowicz, MD Panelists Douglas O. Faigel, MD Professor of Medicine Department of Gastroenterology Oregon
Clinical Study Endoscopic Submucosal Dissection for Early Colorectal Neoplasms: Clinical Experience in a Tertiary Medical Center in Taiwan
 Gastroenterology Research and Practice Volume 2013, Article ID 891565, 7 pages http://dx.doi.org/10.1155/2013/891565 Clinical Study Endoscopic Submucosal Dissection for Early Colorectal Neoplasms: Clinical
Gastroenterology Research and Practice Volume 2013, Article ID 891565, 7 pages http://dx.doi.org/10.1155/2013/891565 Clinical Study Endoscopic Submucosal Dissection for Early Colorectal Neoplasms: Clinical
Paris classification (2003) 삼성의료원내과이준행
 삼성의료원내과이준행") Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Local recurrence after endoscopic resection of colorectal tumors
 Int J Colorectal Dis (2009) 24:225 230 DOI 10.1007/s00384-008-0596-8 ORIGINAL ARTICLE Local recurrence after endoscopic resection of colorectal tumors Kinichi Hotta & Takahiro Fujii & Yutaka Saito & Takahisa
Int J Colorectal Dis (2009) 24:225 230 DOI 10.1007/s00384-008-0596-8 ORIGINAL ARTICLE Local recurrence after endoscopic resection of colorectal tumors Kinichi Hotta & Takahiro Fujii & Yutaka Saito & Takahisa
SAGES 2019 Flexible Endoscopy Course for Fellows
 Goals and Objectives: At the end of the course, the MIS fellow will be familiar with GI endoscopes, towers, and the instruments used for endoscopy and endoscopic surgery. The fellow will also be able to
Goals and Objectives: At the end of the course, the MIS fellow will be familiar with GI endoscopes, towers, and the instruments used for endoscopy and endoscopic surgery. The fellow will also be able to
ESD for EGC with undifferentiated histology
 ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease
 ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease DOWNERS GROVE, Ill., (March 5, 2015) The American Society for Gastrointestinal
ASGE and AGA Issue Consensus Statement on Surveillance and Management of Dysplasia in Patients With Inflammatory Bowel Disease DOWNERS GROVE, Ill., (March 5, 2015) The American Society for Gastrointestinal
05/07/2018. Organisation. The English screening programme what is happening? Organisation. Bowel cancer screening in the UK is:
 Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
Feasibility of endoscopic mucosa-submucosa clip closure method (with video)
") Feasibility of endoscopic mucosa-submucosa clip closure method (with video) Authors Toshihiro Nishizawa 1, Shigeo Banno 2, Satoshi Kinoshita 1,HidekiMori 2, Yoshihiro Nakazato 3,YuichiroHirai 2,Yoko Kubosawa
Feasibility of endoscopic mucosa-submucosa clip closure method (with video) Authors Toshihiro Nishizawa 1, Shigeo Banno 2, Satoshi Kinoshita 1,HidekiMori 2, Yoshihiro Nakazato 3,YuichiroHirai 2,Yoko Kubosawa
Extended cold snare polypectomy for small colorectal polyps increases the R0 resection rate
 Extended cold snare polypectomy for small colorectal polyps increases the R0 resection rate Authors Yasuhiro Abe 1,HaruakiNabeta 1, Ryota Koyanagi 1, Taro Nakamichi 1, Hayato Hirashima 1, Alan Kawarai
Extended cold snare polypectomy for small colorectal polyps increases the R0 resection rate Authors Yasuhiro Abe 1,HaruakiNabeta 1, Ryota Koyanagi 1, Taro Nakamichi 1, Hayato Hirashima 1, Alan Kawarai
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY
 Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
Lower GI bleeding Management DR EHSANI PROFESSOR IN GASTROENTEROLOGY AND HEPATOLOGY 15 FEB 2018 Sources Sources Sources Initial evaluation History Physical examination Laboratory evaluation Obtained at
Duodenal adenomas Management. Dr Stratis Alexandridis Consultant Gastroenterologist BRI
 Duodenal adenomas Management Dr Stratis Alexandridis Consultant Gastroenterologist BRI Introduction Ampullary and non ampullary polyps of the duodenum are diagnosed within and outside genetic syndromes.
Duodenal adenomas Management Dr Stratis Alexandridis Consultant Gastroenterologist BRI Introduction Ampullary and non ampullary polyps of the duodenum are diagnosed within and outside genetic syndromes.
COLON: Innovations 3 steps, 3 parts..
 COLON: Innovations 3 steps, 3 parts.. Detection: I see an abnormality (usually a polyp) Characterization: Is this abnormality neoplastic? (for example: an adenoma) Treatment: it is neoplastic. Can I treat
COLON: Innovations 3 steps, 3 parts.. Detection: I see an abnormality (usually a polyp) Characterization: Is this abnormality neoplastic? (for example: an adenoma) Treatment: it is neoplastic. Can I treat
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 3,900 116,000 120M Open access books available International authors and editors Downloads Our
Role Description: Regional Colon Cancer Screening/GI Endoscopy Clinical Lead
 South West Regional Cancer Program London Health Sciences Centre E4-100 Wing 800 Commissioners Road East London, Ontario N6A 5W9 Role Description: Regional Colon Cancer Screening/GI Endoscopy Clinical
South West Regional Cancer Program London Health Sciences Centre E4-100 Wing 800 Commissioners Road East London, Ontario N6A 5W9 Role Description: Regional Colon Cancer Screening/GI Endoscopy Clinical
ColonCancerCheck Recommendations for Post-Polypectomy Surveillance
 ColonCancerCheck Recommendations for Post-Polypectomy Surveillance C. Dubé, B.R. McCurdy, T. Bronstein, A. Pollett, N.N. Baxter, D. Morgan, J. Tinmouth Table of Contents Background... 5 Methodology...
ColonCancerCheck Recommendations for Post-Polypectomy Surveillance C. Dubé, B.R. McCurdy, T. Bronstein, A. Pollett, N.N. Baxter, D. Morgan, J. Tinmouth Table of Contents Background... 5 Methodology...
Barrett s Esophagus: Ablate Everyone?
 Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
GI Coding Updates. Rhonda Buckholtz, CPC, CPCI, CPMS, CRC, CDEO, CHPSE, CGSC, COBGC, CENTC, CPEDC
 GI Coding Updates Rhonda Buckholtz, CPC, CPCI, CPMS, CRC, CDEO, CHPSE, CGSC, COBGC, CENTC, CPEDC Copyright/Disclaimer 2014 AAPC text CPT copyright 2016 American Medical Association. All rights reserved.
GI Coding Updates Rhonda Buckholtz, CPC, CPCI, CPMS, CRC, CDEO, CHPSE, CGSC, COBGC, CENTC, CPEDC Copyright/Disclaimer 2014 AAPC text CPT copyright 2016 American Medical Association. All rights reserved.
Clinical Outcome of Endoscopic Resection for Nonampullary Duodenal Tumors
 2016.10.20 The 9 th Nottingham Endoscopy Masterclass 9:50-10:10 Clinical Outcome of Endoscopic Resection for Nonampullary Duodenal Tumors Satoru Nonaka, MD, PhD Endoscopy Division National Cancer Center
2016.10.20 The 9 th Nottingham Endoscopy Masterclass 9:50-10:10 Clinical Outcome of Endoscopic Resection for Nonampullary Duodenal Tumors Satoru Nonaka, MD, PhD Endoscopy Division National Cancer Center
Risk Factors for Incomplete Polyp Resection during Colonoscopic Polypectomy
 Gut and Liver, Vol. 9, No. 1, January 2015, pp. 66-72 ORiginal Article Risk Factors for Incomplete Polyp Resection during Colonoscopic Polypectomy Sang Pyo Lee, In-Kyung Sung, Jeong Hwan Kim, Sun-Young
Gut and Liver, Vol. 9, No. 1, January 2015, pp. 66-72 ORiginal Article Risk Factors for Incomplete Polyp Resection during Colonoscopic Polypectomy Sang Pyo Lee, In-Kyung Sung, Jeong Hwan Kim, Sun-Young
위 ESD 후내시경소견 성균관대학교의과대학내과이준행
 위 ESD 후내시경소견 성균관대학교의과대학내과이준행 문제의식 위궤양, 조기위암, 진행위암의내시경소견은배운다. 위암수술후소견은가끔배운다. 위암내시경시술후소견은배운적이없다. 관찰과조직검사에대한가이드라인이없다. ESD 후정상내시경소견 성균관대학교의과대학내과이준행 처음의뢰되었을때의사진 ESD M/D, 18mm, LP, RM (-), L/V (-) 추적내시경소견 2
위 ESD 후내시경소견 성균관대학교의과대학내과이준행 문제의식 위궤양, 조기위암, 진행위암의내시경소견은배운다. 위암수술후소견은가끔배운다. 위암내시경시술후소견은배운적이없다. 관찰과조직검사에대한가이드라인이없다. ESD 후정상내시경소견 성균관대학교의과대학내과이준행 처음의뢰되었을때의사진 ESD M/D, 18mm, LP, RM (-), L/V (-) 추적내시경소견 2
Clinical Policy Title: Mucosal and submucosal endoscopic resection of colorectal polyps
 Clinical Policy Title: Mucosal and submucosal endoscopic resection of colorectal polyps Clinical Policy Number: CCP.1328 Effective Date: October 1, 2017 Initial Review Date: August 17, 2017 Most Recent
Clinical Policy Title: Mucosal and submucosal endoscopic resection of colorectal polyps Clinical Policy Number: CCP.1328 Effective Date: October 1, 2017 Initial Review Date: August 17, 2017 Most Recent
Esophageal submucosal mass icd 10
 Esophageal submucosal mass icd 10 Search 6-6-2011 ICD-10; Risk Adjustment / HCC; Evaluation & Management (E/M). I'm hoping someone can help me with this DX, "soft tissue mass in. Upper gastrointestinal
Esophageal submucosal mass icd 10 Search 6-6-2011 ICD-10; Risk Adjustment / HCC; Evaluation & Management (E/M). I'm hoping someone can help me with this DX, "soft tissue mass in. Upper gastrointestinal
The focus of Chapter 9 is on anoscopy, proctosigmoidoscopy, flexible sigmoidoscopy, and colonoscopy procedures and all
 9 Anoscopy, 45380 45380 45385 Proctosigmoidoscopy, Flexible Sigmoidoscopy, and Colonoscopy 45378 The focus of Chapter 9 is on anoscopy, proctosigmoidoscopy, flexible sigmoidoscopy, and colonoscopy procedures
9 Anoscopy, 45380 45380 45385 Proctosigmoidoscopy, Flexible Sigmoidoscopy, and Colonoscopy 45378 The focus of Chapter 9 is on anoscopy, proctosigmoidoscopy, flexible sigmoidoscopy, and colonoscopy procedures
Endoscopic Submucosal Dissection of an Inverted Early Gastric Cancer-Forming False Gastric Diverticulum
 CSE REPORT Clin Endosc 2016;49:86-90 http://dx.doi.org/10.5946/ce.2016.49.1.86 Print ISSN 2234-2400 / On-line ISSN 2234-2443 Open ccess Endoscopic Submucosal Dissection of an Inverted Early Gastric Cancer-Forming
CSE REPORT Clin Endosc 2016;49:86-90 http://dx.doi.org/10.5946/ce.2016.49.1.86 Print ISSN 2234-2400 / On-line ISSN 2234-2443 Open ccess Endoscopic Submucosal Dissection of an Inverted Early Gastric Cancer-Forming
General Surgery PURPLE SERVICE MUHC-RVH Site
 Preamble HPB is a clinical teaching unit with several different vocations: It regroups all solid organ Transplantation as well as most advanced Hepatobiliary and Pancreatic clinical activities performed
Preamble HPB is a clinical teaching unit with several different vocations: It regroups all solid organ Transplantation as well as most advanced Hepatobiliary and Pancreatic clinical activities performed
BC CRC Update Malignant Polyp Who Needs Surgery
 BC CRC Update Malignant Polyp Who Needs Surgery Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary
BC CRC Update Malignant Polyp Who Needs Surgery Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset