위 ESD 후내시경소견 성균관대학교의과대학내과이준행
|
|
|
- Ariel Briggs
- 5 years ago
- Views:
Transcription
1 위 ESD 후내시경소견 성균관대학교의과대학내과이준행
2 문제의식 위궤양, 조기위암, 진행위암의내시경소견은배운다. 위암수술후소견은가끔배운다. 위암내시경시술후소견은배운적이없다. 관찰과조직검사에대한가이드라인이없다.
3 ESD 후정상내시경소견 성균관대학교의과대학내과이준행
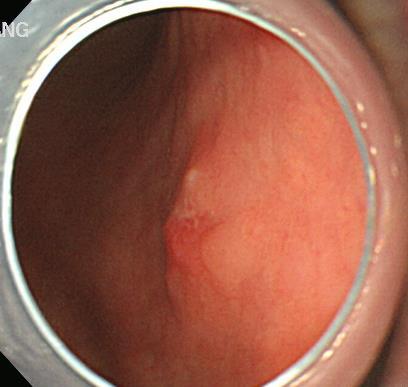
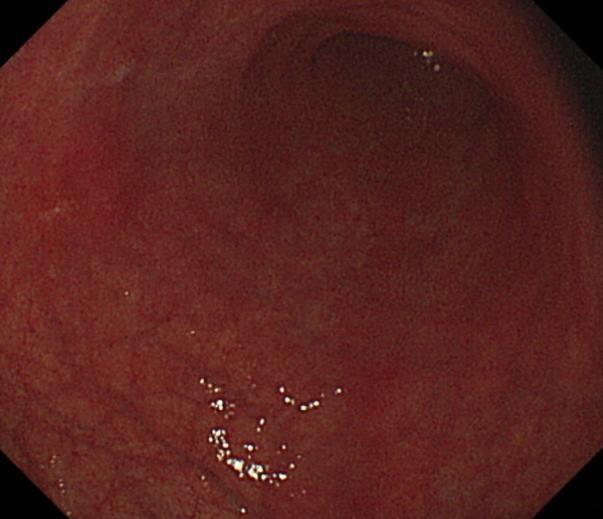
4 처음의뢰되었을때의사진

")
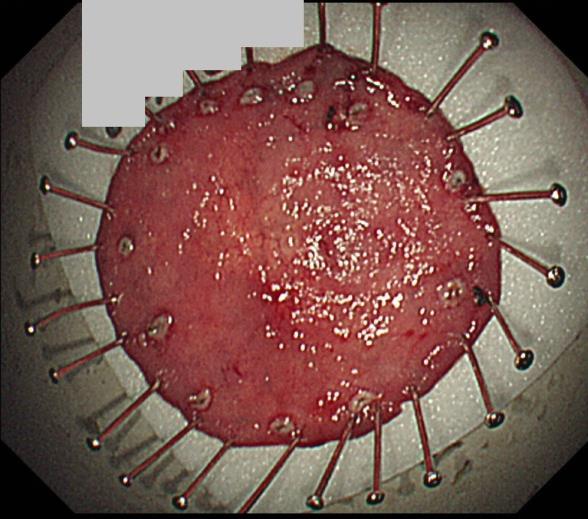
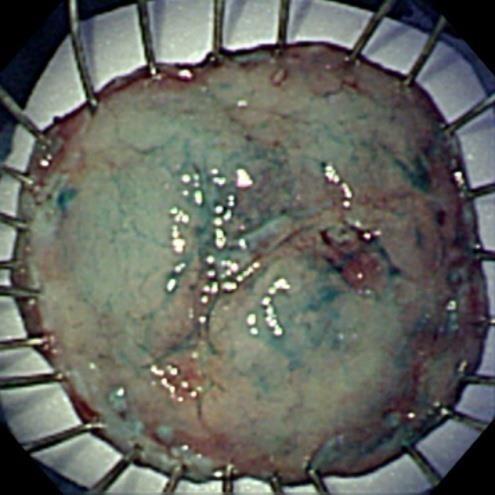
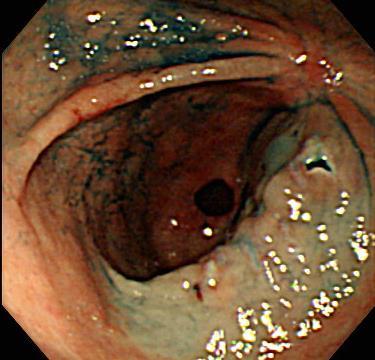
5 ESD M/D, 18mm, LP, RM (-), L/V (-)

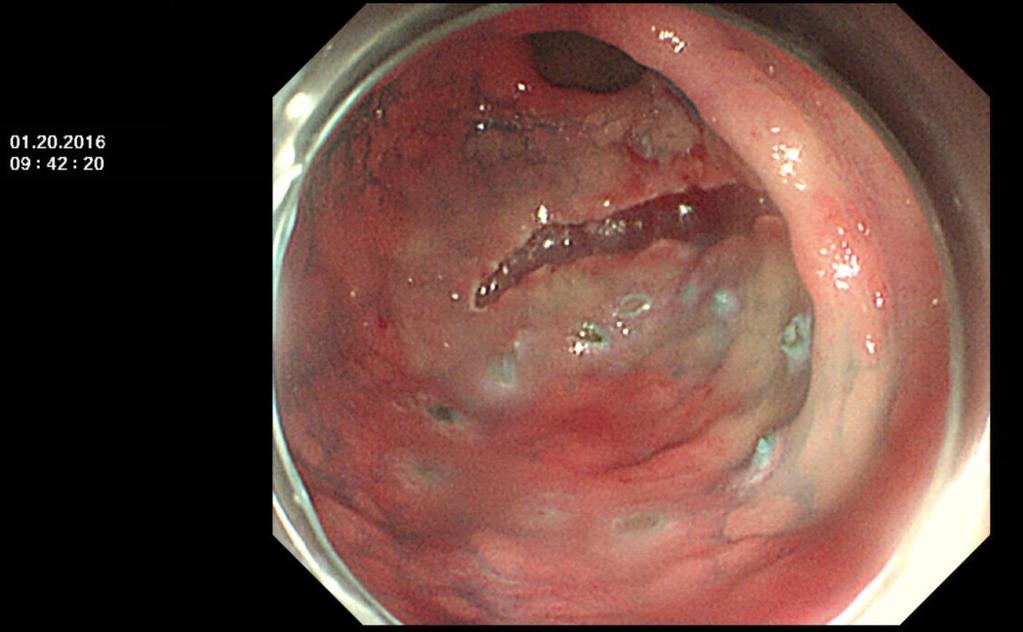
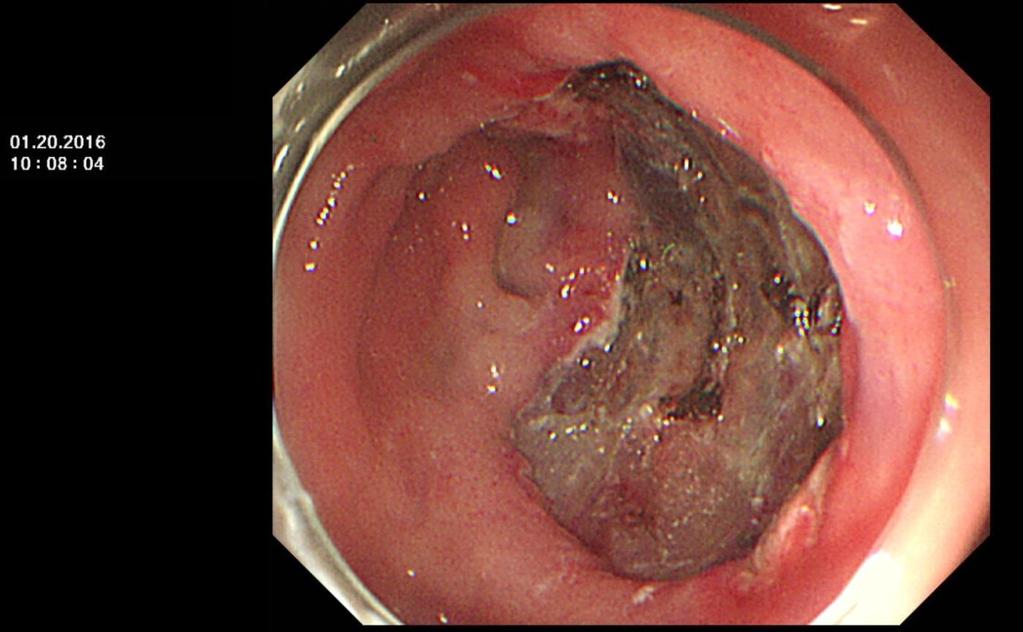
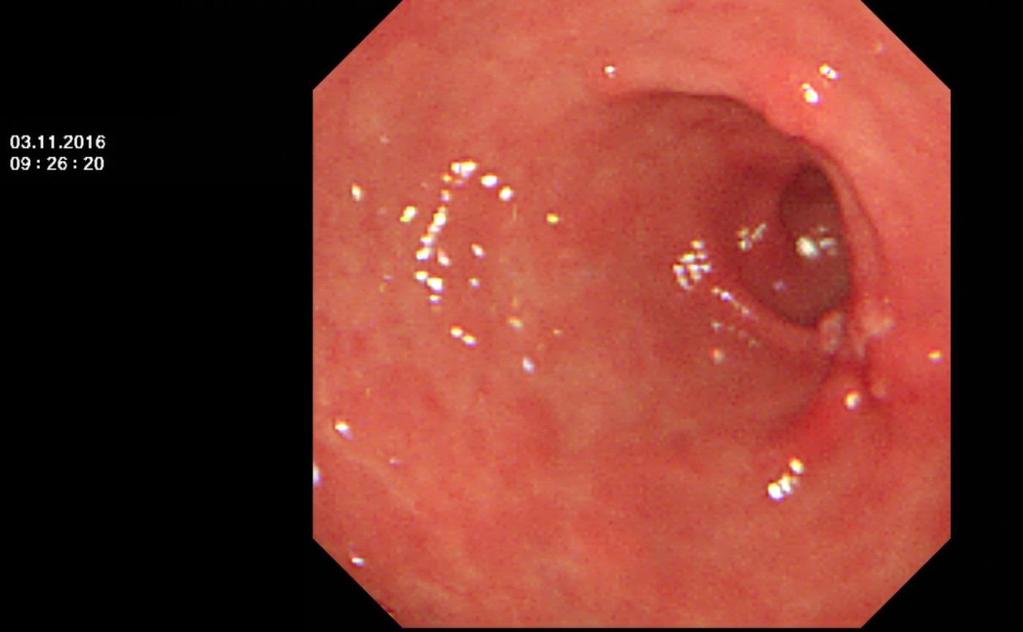
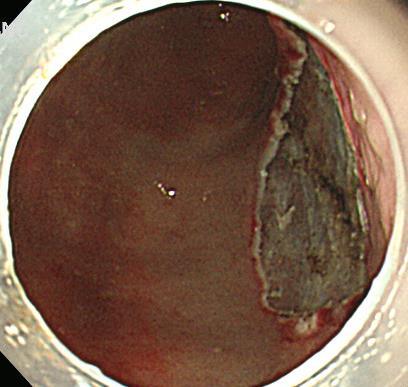
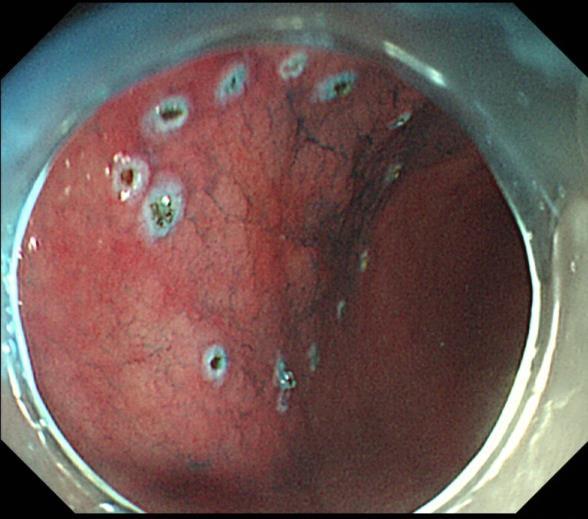
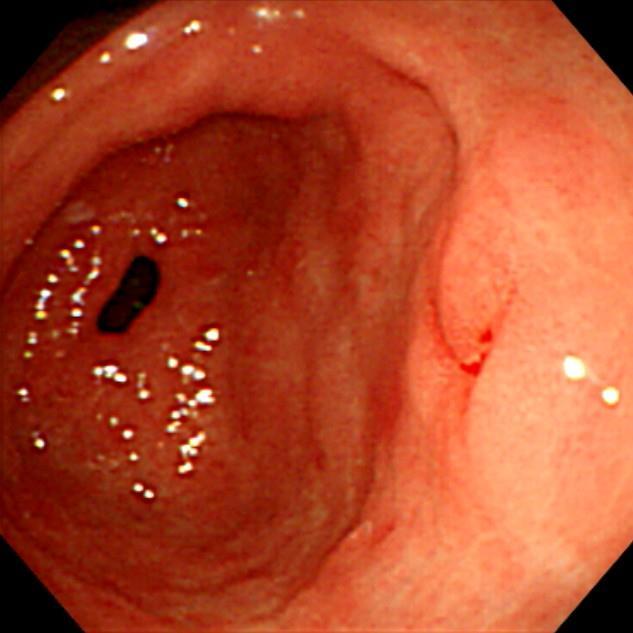
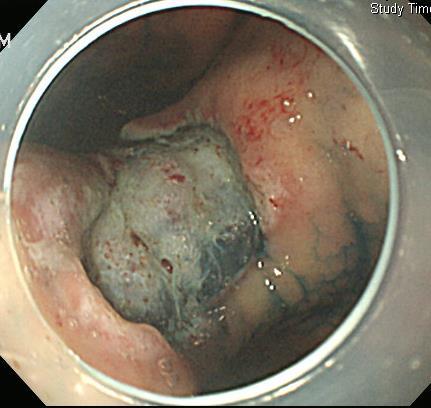
6 추적내시경소견 2 달후 6 달후 3 년후


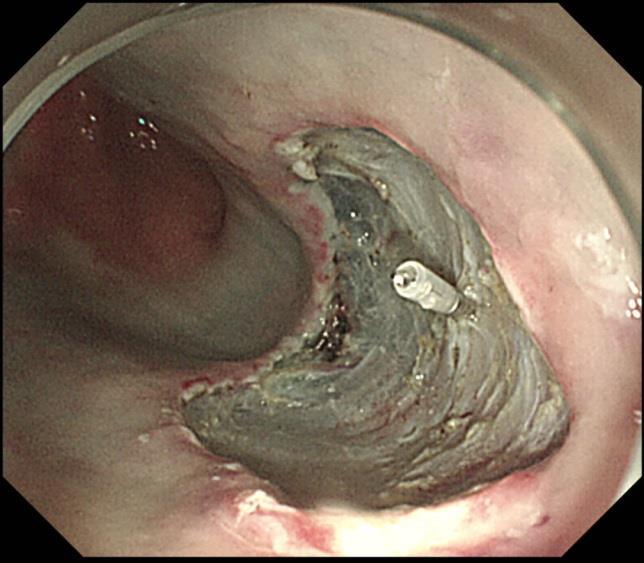
7 ESD (x2) for EGCs 두달후관찰 2 달후


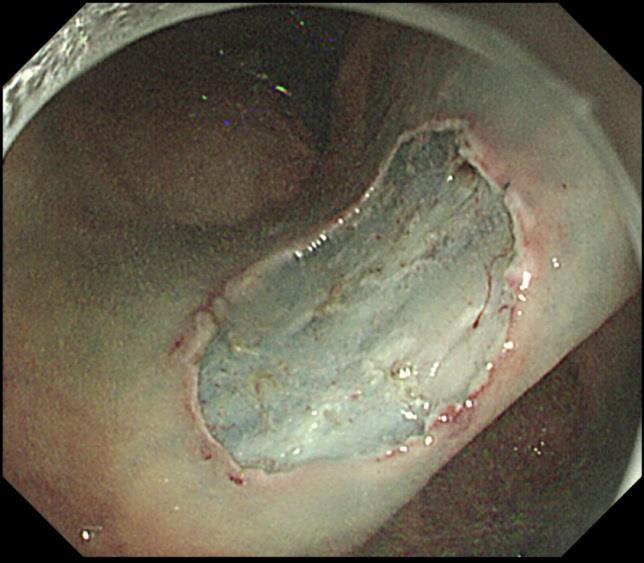
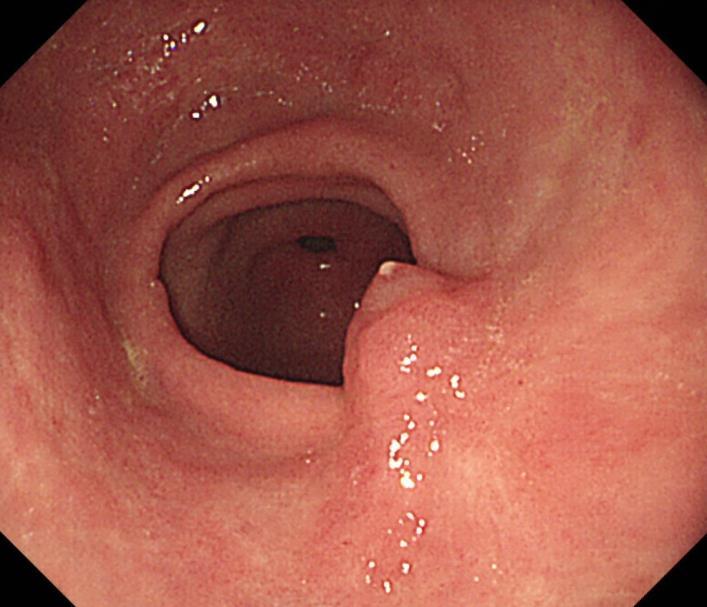
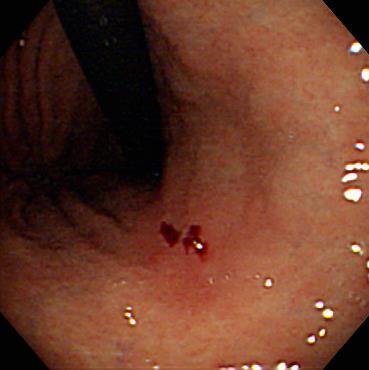
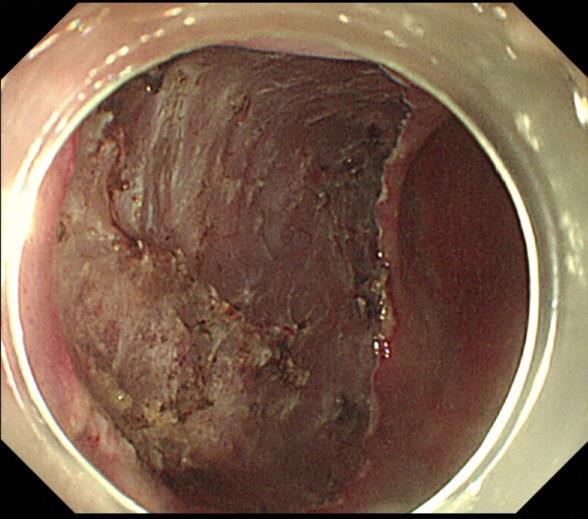
8 8 주후인공궤양이덜아물기도합니다. - M/74, DM, angina, H/O CVA - M/D, 12mm, MM, 8 주후
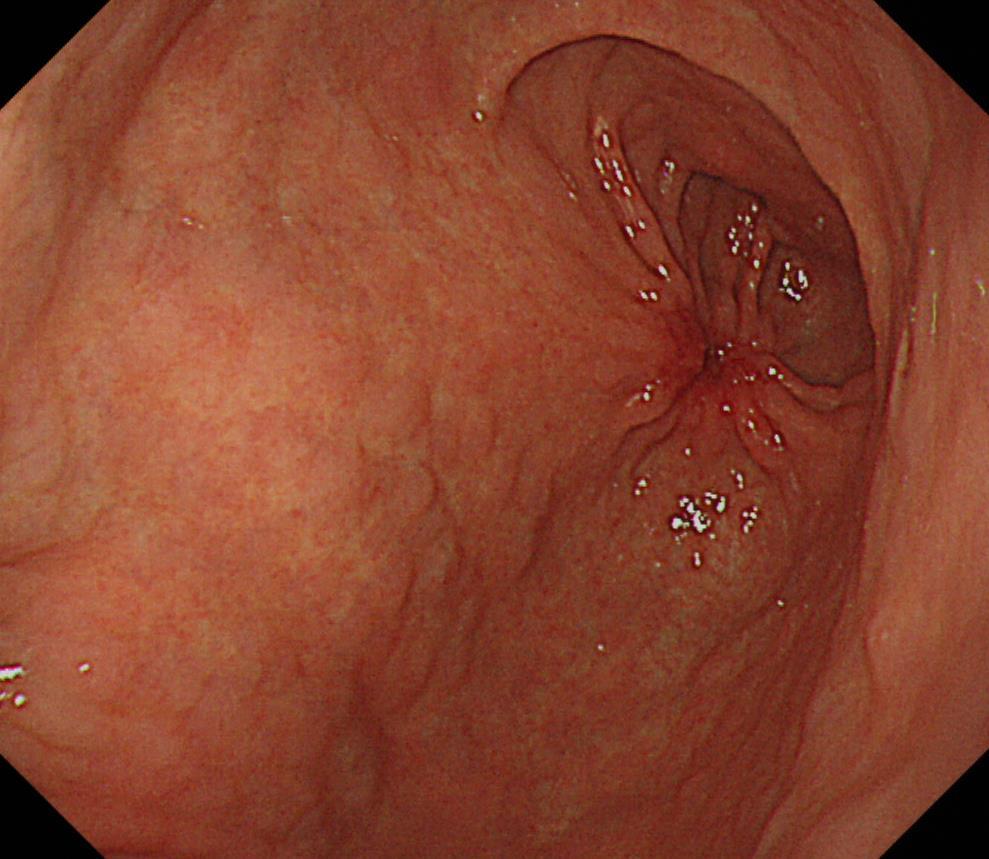
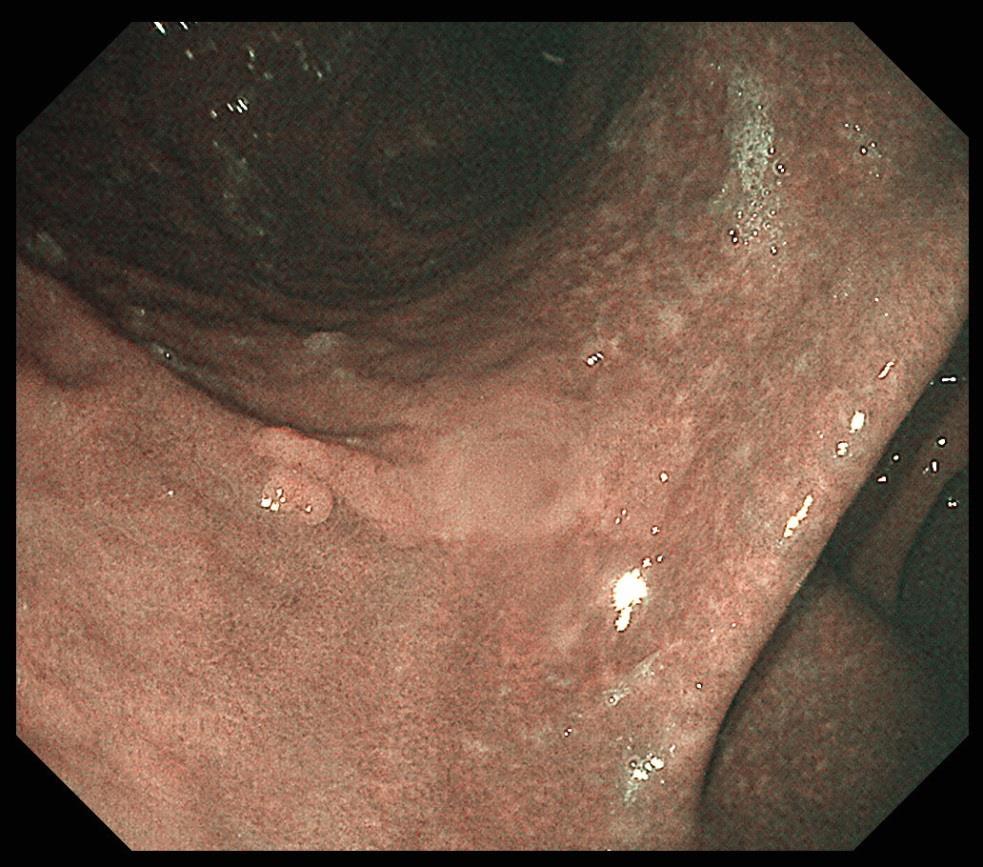
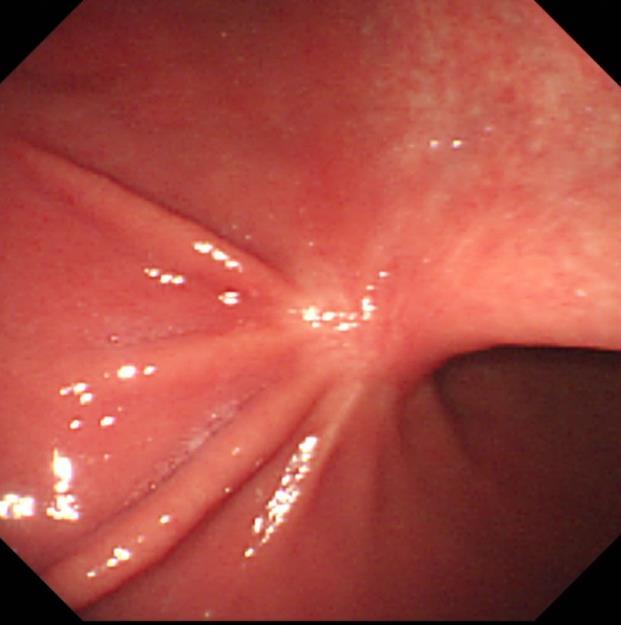
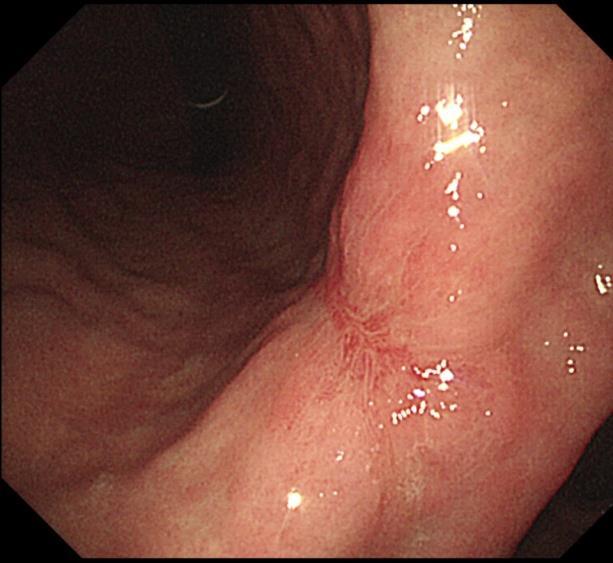
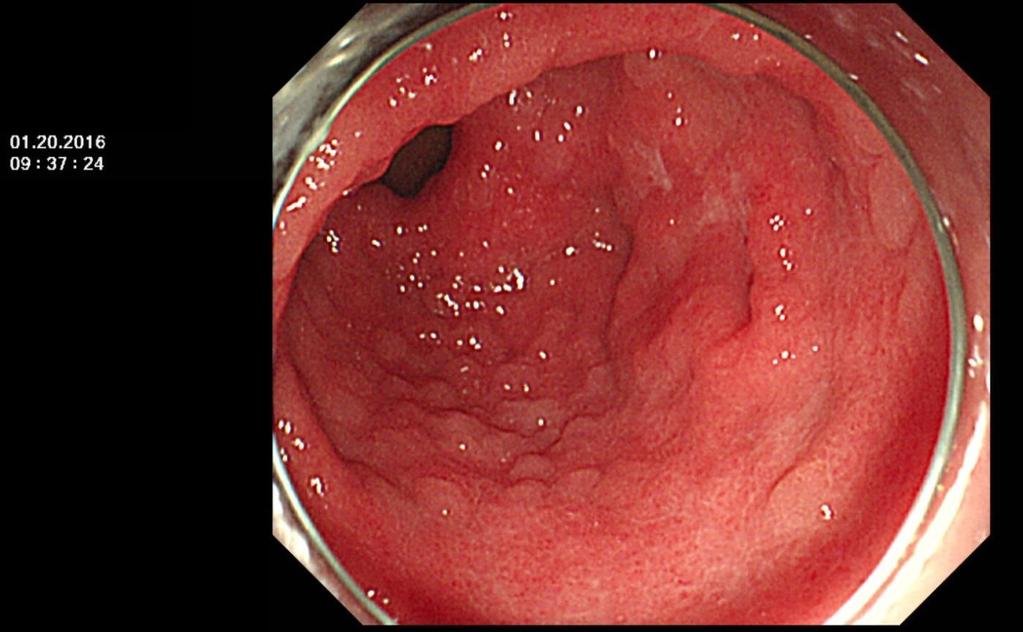
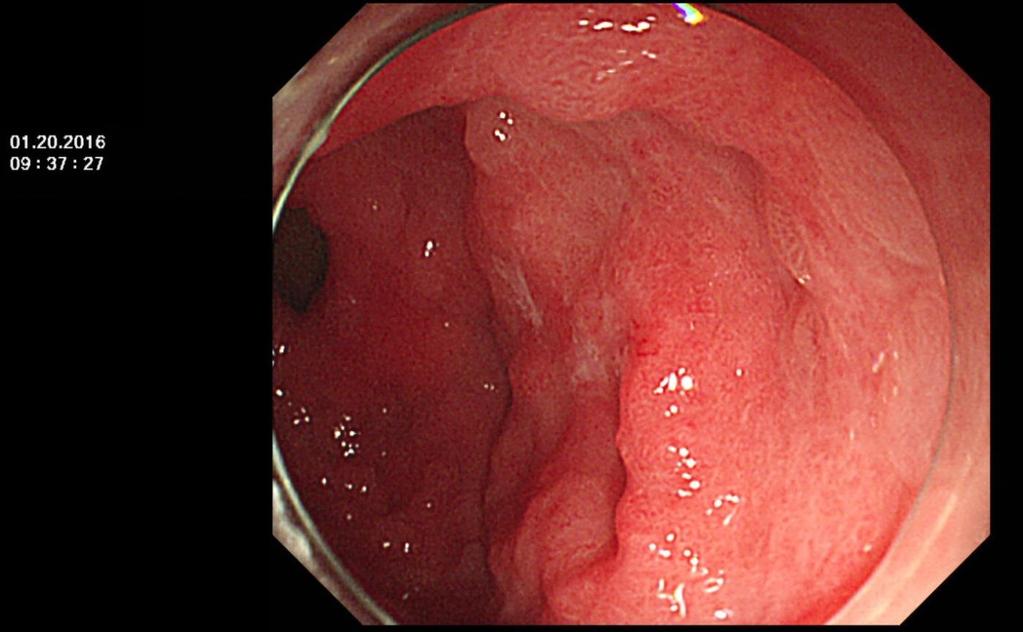
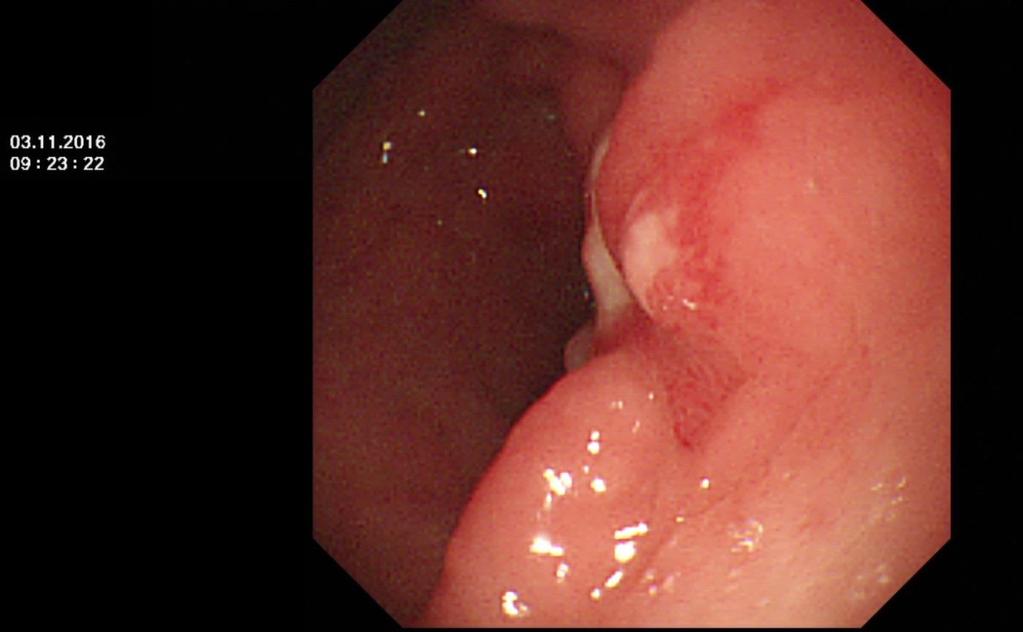
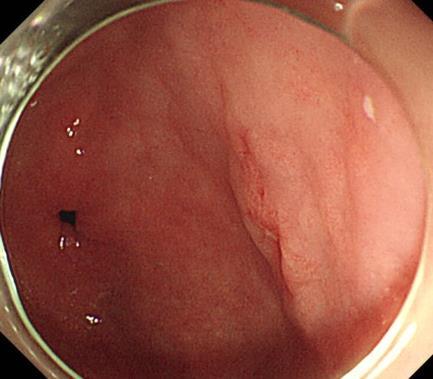
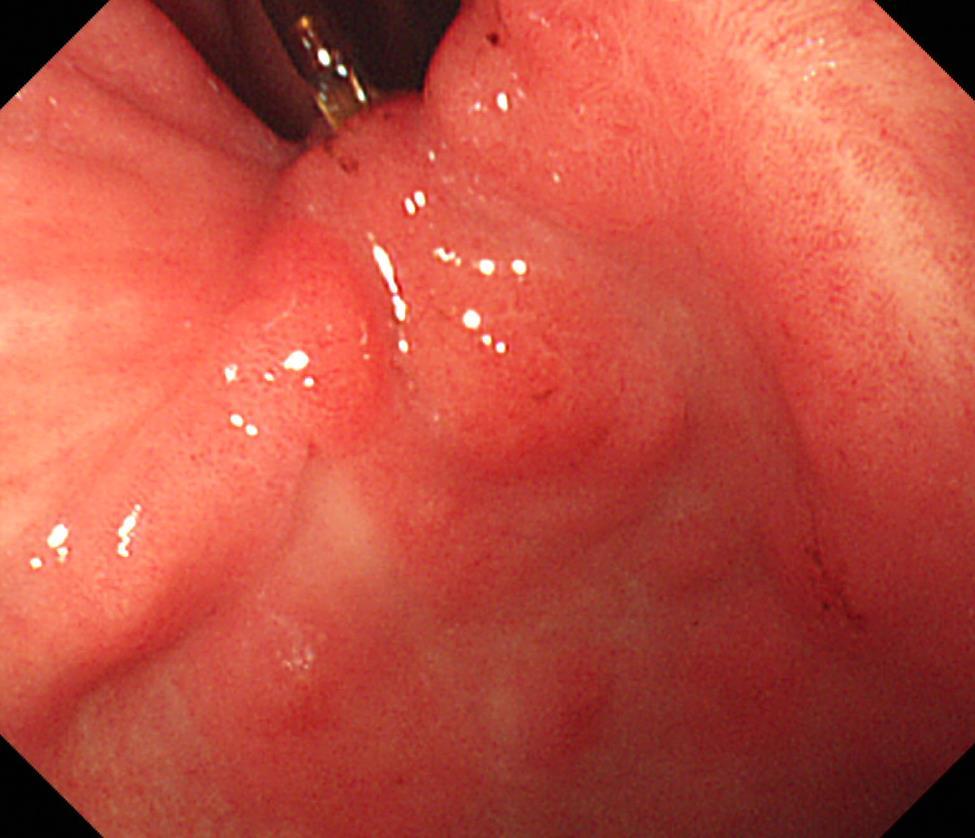
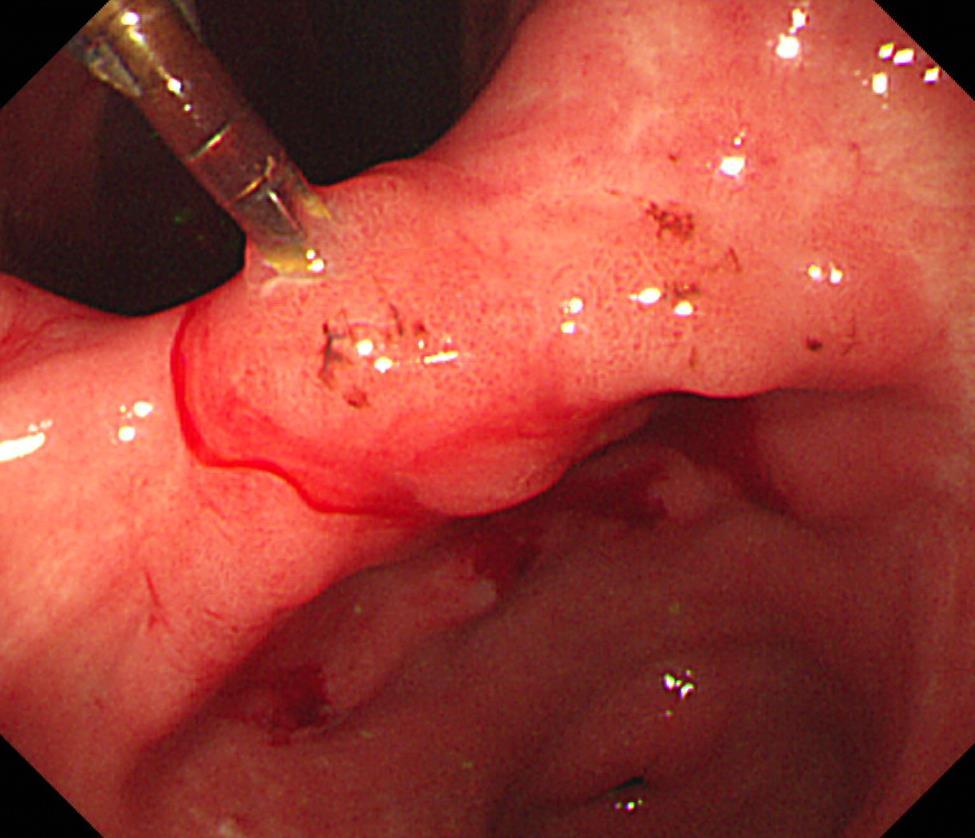
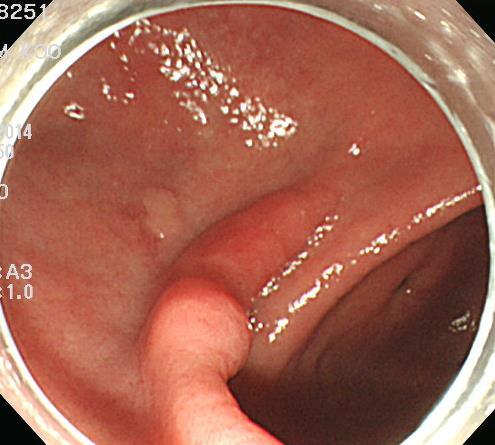
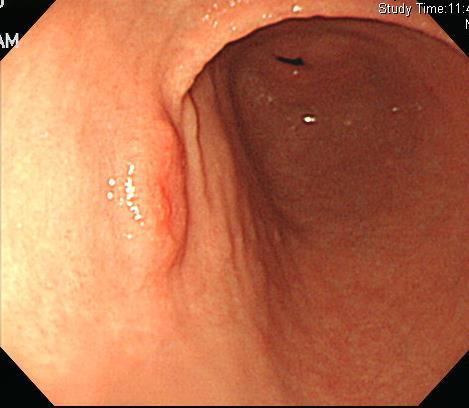
9 Converging fold 를만들기도함


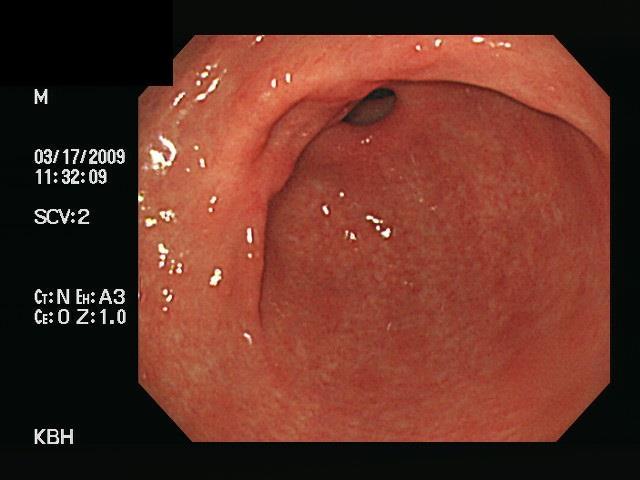

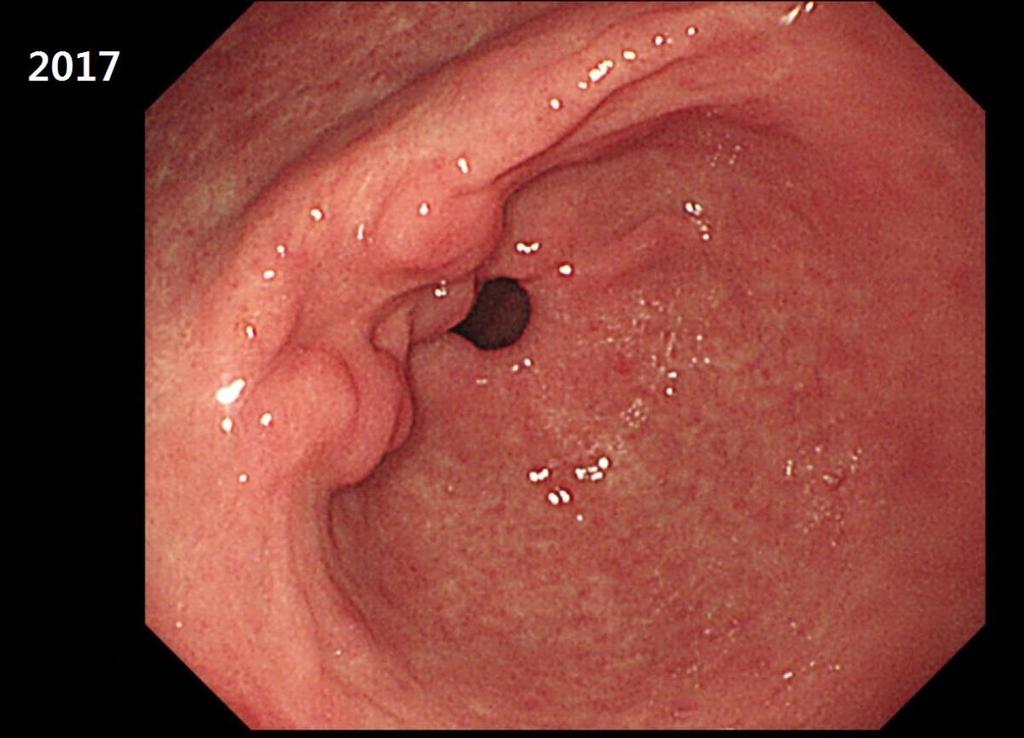
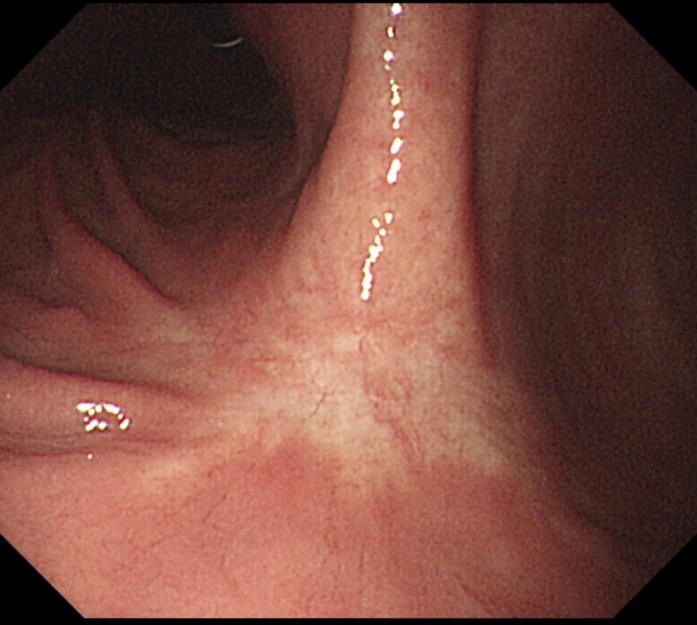
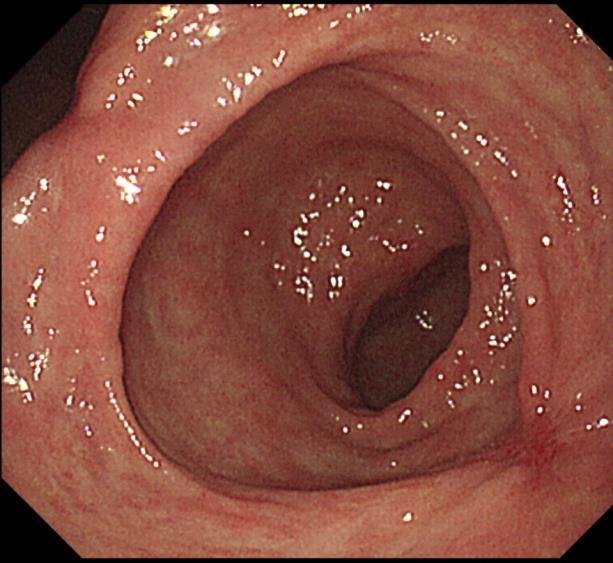
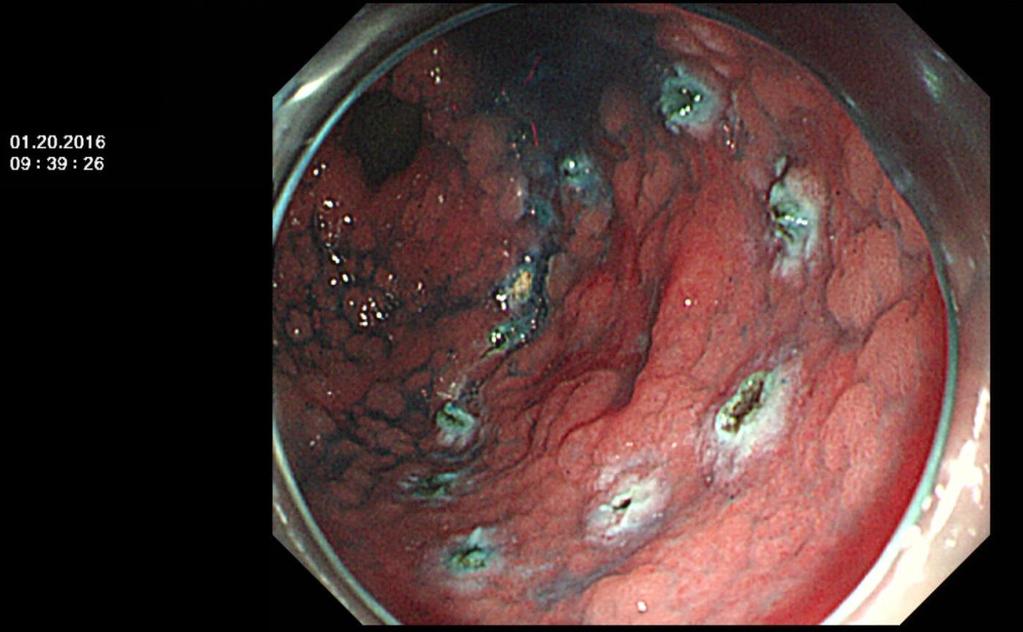
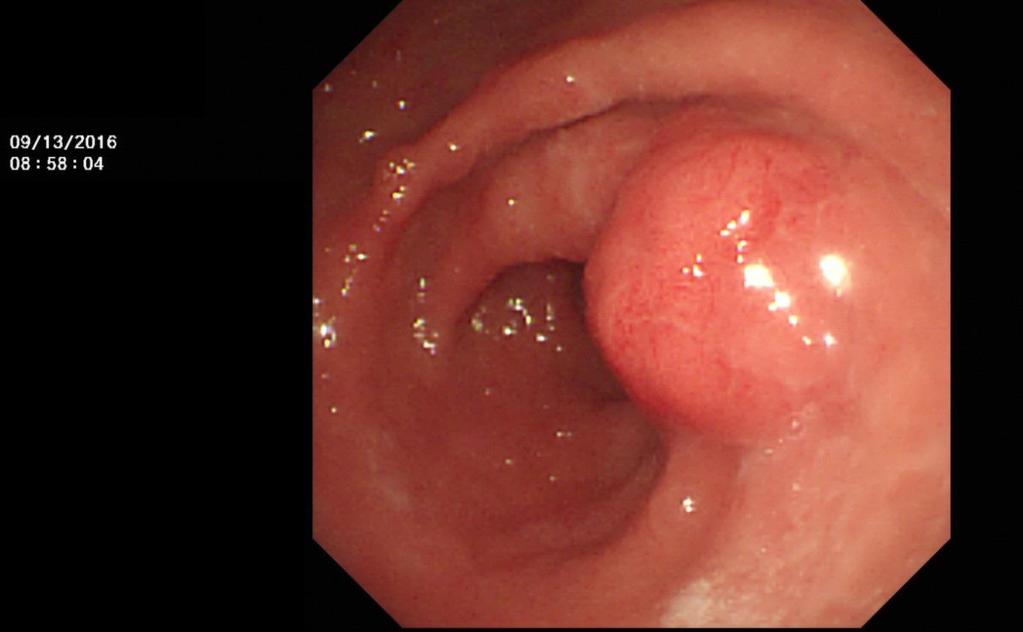
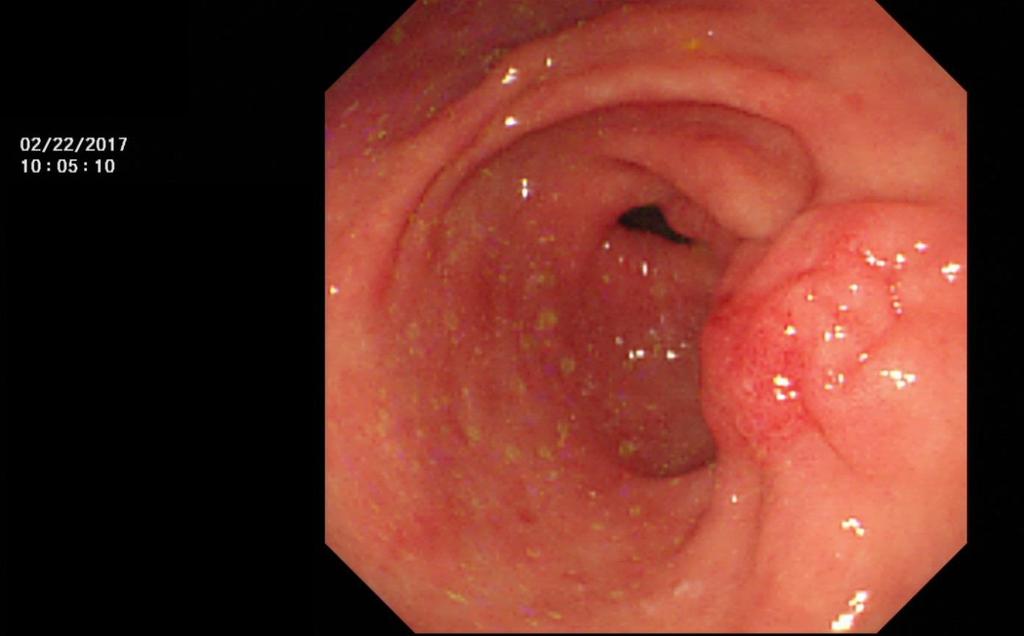
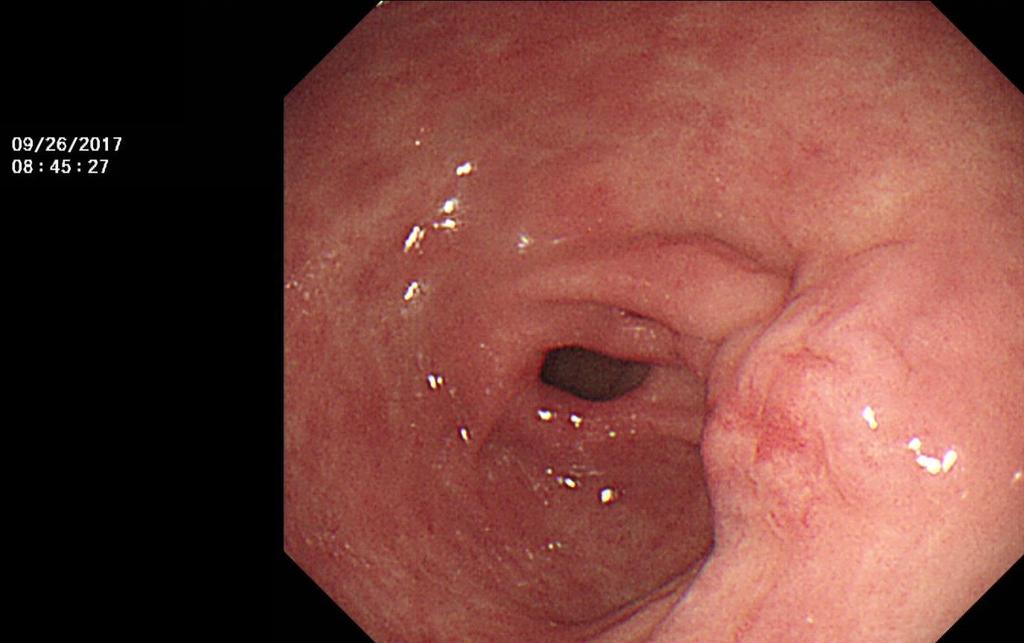
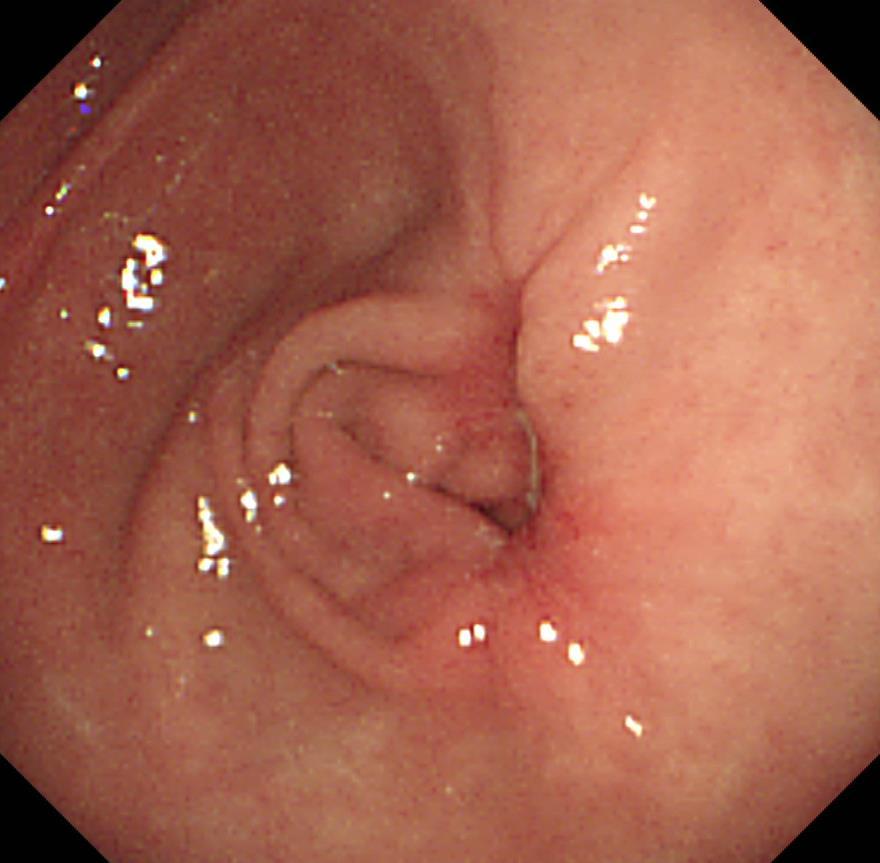
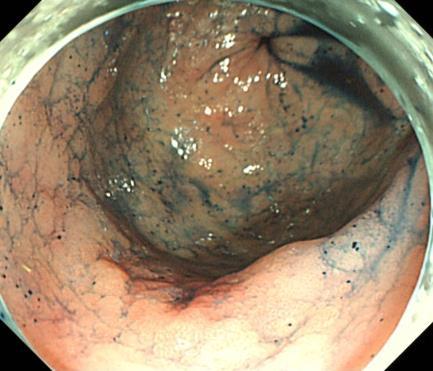
10 2017 묘한모양의 scar 도있습니다.

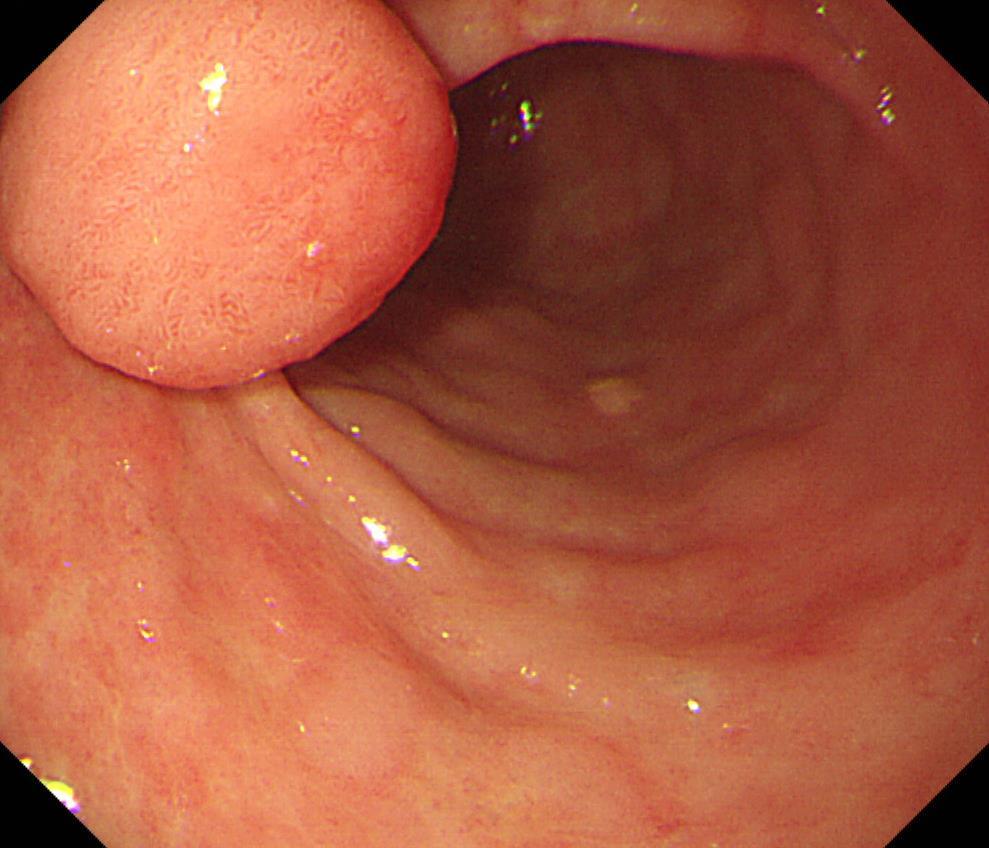
11 ESD 후융기형반흔 11 년간관찰
")
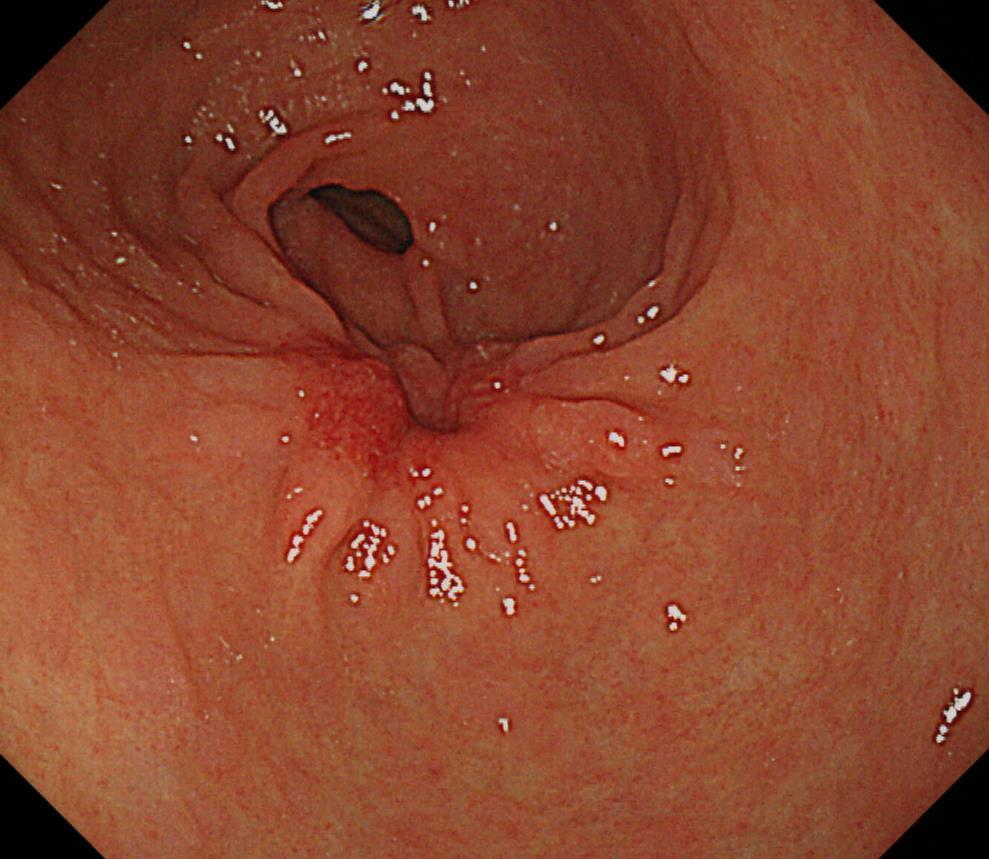
12 다양한융기형반흔 (15%) 대한위암학회지 2001;1:55-59
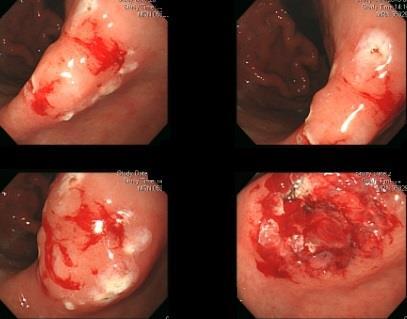
13 ESD scar 의모양은계속변해갑니다. ESD: W/D, 24mm, LP, RM (-), L/V (-/-)



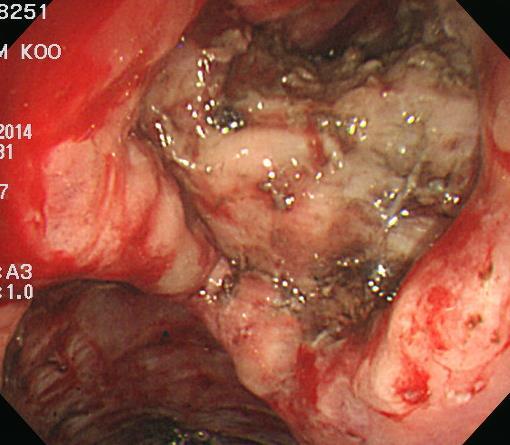
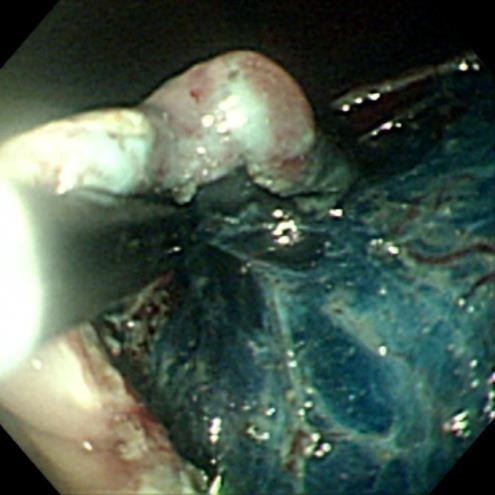
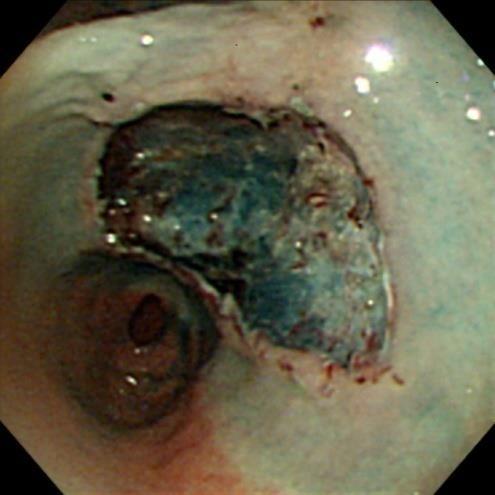
14 Stricture after a very large ESD - 14 x 10 cm resection for 7 x 6 cm EGC 6 weeks after ESD for EGC
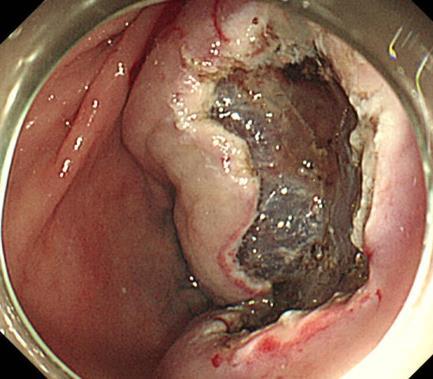

15 세번 ESD 후상당히좁아졌으나증상은없음 첫번째 ESD: 9 년전 두번째 ESD: 3 년전 세번째 ESD: 2 달전
16 협착예방을위한경구 steroid 치료 8 주코스 ESD 2일째 Pd 투약시작 1주 : 매일 30mg (5mg 6알 ) 2주 : 매일 30mg (5mg 6알 ) 3주 : 매일 25mg (5mg 5알 ) 4주 : 매일 25mg (5mg 5알 ) 5주 : 매일 20mg (5mg 4알 ) 4 주코스 ESD 2일째 Pd 투약시작 1주 : 매일 30mg (5mg 6알 ) 2주 : 매일 20mg (5mg 4알 ) 3주 : 매일 10mg (5mg 2알 ) 4주 : 매일 5mg (5mg 1알 ) 5주 : 중단 6주 : 매일 15mg (5mg 3알 ) 7주 : 매일 10mg (5mg 2알 ) 8주 : 매일 5mg (5mg 1알 ) 9주 : 중단




17 ESD 후병소가커서 steroid 를 PPI 와함께사용함 8 weeks later 6 months later
18 SMC policy EGD after ESD - 조기위암 / 위선종내시경치료후추적검사 조기위암 EMR/ESD: 5 년까지추적내시경마다 scar 에서 조직검사 (1-2 점 ) 5 년후부터는재발의심소견이있 을때만조직검사 ( 단, 조기위암 EMR/ESD 후첫추적내 시경에서는 H. pylori 조직검사도함께시행한다.) 선종 EMR/ESD: 1 년까지추적내시경마다 scar 에서조직 검사 (1-2 점 ) 1 년후부터는재발의심소견이있을때 만조직검사 선종 APC: 재발의심소견이있을때만조직검사


19 1.2cm, M/D, LP 암. 7 년후. 조직검사?
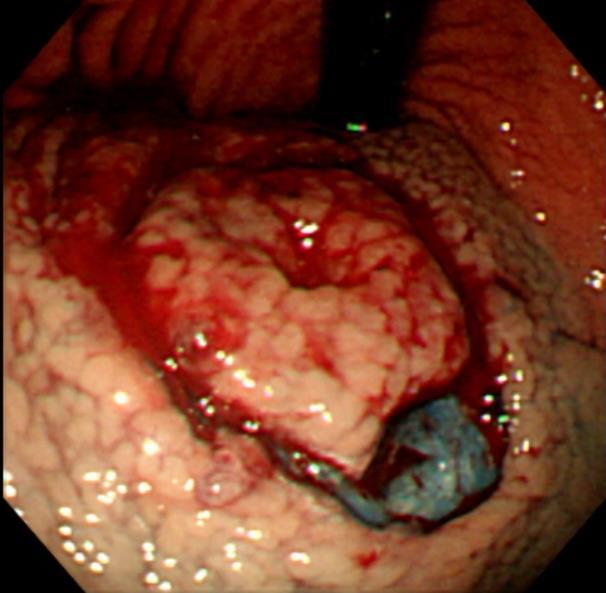
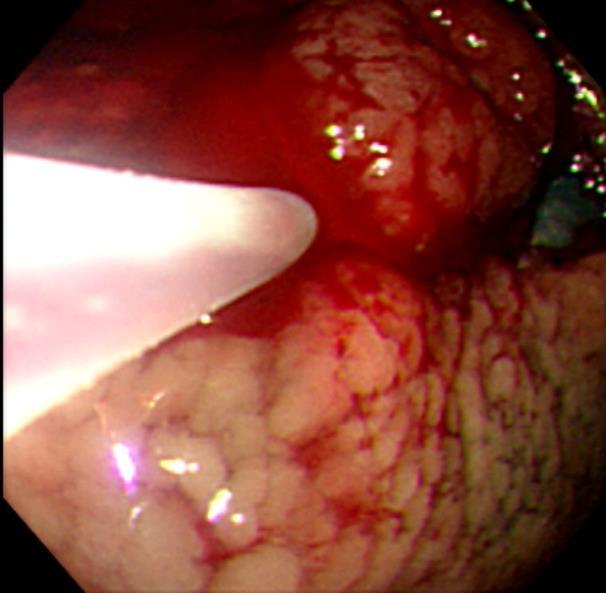
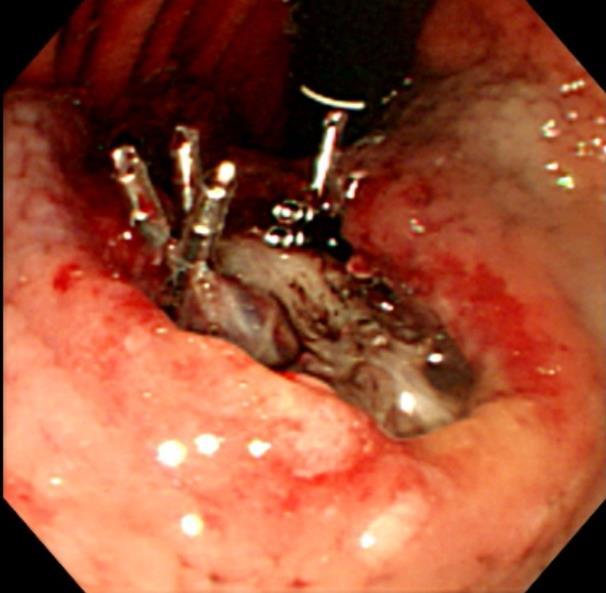
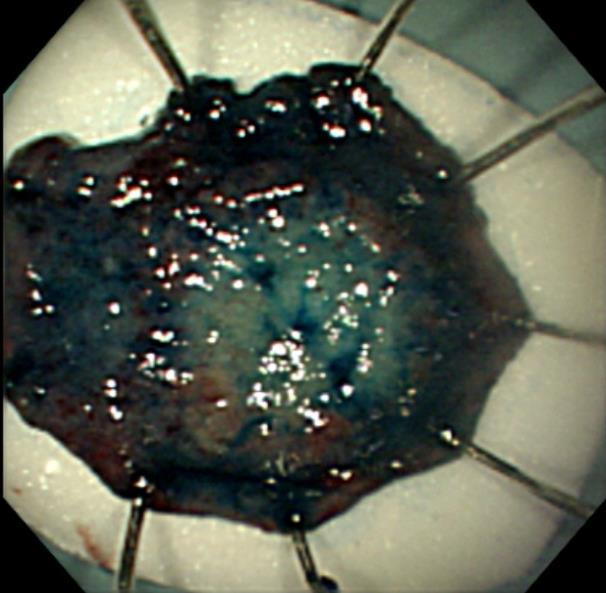
20 Local recurrence 성균관대학교의과대학내과이준행
21 위각 ESD 후재발로의뢰되었으나 수술할수밖에없음 조직검사에서모두암으로나옴
22 Stomach, subtotal gastrectomy: Early gastric carcinoma 1. Location : middle third, Center at antrum, angle and lesser curvature 2. Gross type : EGC type IIb 3. Histologic type : tubular adenocarcinoma, moderately differentiated 4. Histologic type by Lauren : intestinal 5. Size : 2.7x2.3 cm 6. Depth of invasion : invades mucosa (lamina propria) (pt1a) 7. Resection margin: free from carcinoma, safety margin: proximal 3.3 cm, distal 3.4 cm 8. Lymph node metastasis : no metastasis in 17 regional lymph nodes (pn0) (0/17 : "3", 0/2; "4", 0/2; "5", 0/0; "6", 0/5; "7", 0/1; "9", 0/2; "8a", 0/0; "11p", 0/2; "12a", 0/2; "4sb", 0/1; "1", 0/0) 9. Lymphatic invasion : not identified 10. Venous invasion : not identified 11. Perineural invasion : not identified 12. AJCC stage by 7th edition: pt1a N0

 - safety margin:")


23 2006 국소재발 - M/D, 3.2x2.5 cm - Depth of invasion: pt1a - RM (-) - safety margin: 0.1, 0.2, 0.9, and 2cm Subtotal gastrectomy: M/D, 0.8x0.4cm, pt1a, RM (-), LN (-)
 >= 10")

24 Initial biopsy: M/D ESD: P/D, 14mm, LP, RM (-) >= 10 mm Biopsy: M/D Subtotal gastrectomy: W/, 0.7cm, lamina propria

25 EMR-C at a low-volume center (2010) 국소재발로의뢰되어재검하여또다른암발견 수술 사망
 ESD for EGC - Gross type")


 - Resection margin :")

26 ESD 후첫내시경에서암 (locally residual cancer) ESD for EGC - Gross type : EGC type IIb - Tubular adenocarcinoma, moderately differentiated - Size of carcinoma: 48 x 28mm - Depth of invasion : mucosa (lamina propria) - Resection margin : free from carcinoma(n) - safety margin : D 3 mm, P 1.5 mm, A 10 mm, P 4 mm - L/V/N (-) Ablation 후수년간재발 (-)




27 경계가불분명한위암 ESD 후 lateral margin 양성으로 ablation 치료를했으나국소재발 수술하여 1.5 cm residual 확인 경계가불분명한위암 ESD 소작술국소재발 W/D adenocarcinoma, 1.5 cm, lamina propria, LN (-)






28 Local recurrence ESD - tumor 와 scar 를포함하여 en bloc resection 하였음 ESD for adenoma with HGD Review: EGC in MM EGC at 6 month
 4. Histologic type by Lauren : intestinal 5.")
29 Stomach, LC of mid antrum, endoscopic submucosal dissection: Status post endoscopic submucosal dissection (O ) Early gastric carcinoma 1. Location : antrum, lesser curvature 2. Gross type : EGC type IIa+IIc 3. Histologic type : tubular adenocarcinoma, well differentiated (foveolar type) 4. Histologic type by Lauren : intestinal 5. Size of carcinoma : (1) longest diameter, 26 mm (2) vertical diameter, 23 mm 6. Depth of invasion : invades mucosa (muscularis mucosa) (pt1a) 7. Resection margin : free from carcinoma(n), safety margin : distal 8 mm, proximal 8 mm, anterior 14 mm, posterior 12 mm 8. Lymphatic invasion : not identified(n) 9. Venous invasion : not identified(n) 10. Perineural invasion : not identified(n) 11. Microscopic ulcer : absent 12. Histologic heterogeneity: absent
 4. Histologic type by Lauren : intestinal 5.")
: safety margin : distal 5 mm, proximal 2 mm, anterior 14 mm, posterior 4 mm, deep 150 μm 8. Lymphatic invasion : not identified(n) 9.")
30 ESD 후국소재발 (1 년반 ) Local recurrence 1. Location : body, lesser curvature 2. Gross type : EGC type IIa+IIc 3. Histologic type : tubular adenocarcinoma, moderately differentiated >> tubular adenocarcinoma, poorly differentiated (about 10%) 4. Histologic type by Lauren : intestinal 5. Size of carcinoma : (1) longest diameter, 38 mm (2) vertical diameter, 24 mm 6. Depth of invasion : invades submucosa, (depth of sm invasion : 250 μm ) (pt1b) 7. Resection margin : free from carcinoma(n): safety margin : distal 5 mm, proximal 2 mm, anterior 14 mm, posterior 4 mm, deep 150 μm 8. Lymphatic invasion : not identified(n) 9. Venous invasion : not identified(n) 10. Perineural invasion : not identified(n) 11. Microscopic ulcer : absent 12. Histologic heterogeneity: present Stomach, subtotal gastrectomy: Early gastric carcinoma - Histologic type : tubular adenocarcinoma, moderately differentiated - Size : 2.8x2.4 cm - Depth of invasion : invades mucosa (muscularis mucosae) (pt1a) - Lymph node metastasis : no metastasis in 33 regional lymph nodes (pn0) - LVN (-)




31 ESD 후국소재발 (1 년반 ) 환자의과거사진은어떠하였을까? Local recurrence Stomach, subtotal gastrectomy: Early gastric carcinoma - Histologic type : tubular adenocarcinoma, moderately differentiated - Size : 2.8x2.4 cm - Depth of invasion : invades mucosa (muscularis mucosae) (pt1a) - Lymph node metastasis : no metastasis in 33 regional lymph nodes (pn0) - LVN (-) 2M 12M 6M 18M
")
32 ESD 후수술거부 ( 증례 1)
33
34

35 ESD 후수술거부 28 개월후재발

36 28 months after EMR

37 재발 6 개월전
 > tubular adenocarcinoma, P/D (about 10%) 4. Histologic type by Lauren : intestinal 5. Size : 2.8x1.8 cm 6.")
38 ESD 후수술거부증례 (2) 1. Location : antrum, anterior wall 2. Gross type : EGC type IIc 3. Histologic type : tubular adenocarcinoma, M/D >> papillary adenocarcinoma, M/D (about 20%) > tubular adenocarcinoma, P/D (about 10%) 4. Histologic type by Lauren : intestinal 5. Size : 2.8x1.8 cm 6. Depth of invasion : invades submucosa, (depth of sm invasion: 1500 μm ) (pt1b) 7. Resection margin: free from carcinoma 8. Lymphatic invasion : present 9. Venous invasion : present 10. Perineural invasion : not identified 11. Microscopic ulcer : absent 12. Histologic heterogeneity: present
39 ESD 후수술거부 38 개월후재발 Advanced gastric carcinoma Histologic type : tubular adenoca (M/D) Size : 2.8x2.4 cm Penetrates subserosal connective tissue Lymph node metastasis : positive (1/34) Lymphatic invasion : present Venous invasion : not identified Perineural invasion : not identified Recurrent mass at 38 months Peritoneal cytology : negative



40 Limited role of follow-up EGD ESD 7 months 13 months 20 months 26 months 38 months
41 어떤경우에 local recur 를의심? Unclear tumor border before ESD Not sufficient resection margin Larger tumor SM invasion Mixed histology / undifferentiated type Delayed healing Asymmetry, focal hyperemia, SMT-like buldging
42 Other site recurrences - synchronous / metachronous 성균관대학교의과대학내과이준행
43 EMR/ESD data analysis at SMC Endoscopic resection Differentiated Undiffererentiated Curative resection Poorly differentiated Noncurative resection Signet ring cell carcinoma
44 Study population EGCs treated by ESD at Samsung Medical Center 1,838 patients with 1,889 differentiated-type EGCs November 2003 May 2011 Censoring date: May 2014 Differentiated-type EGC Well or moderately differentiated or papillary EGC According to the quantitatively predominant histologic type Differentiated-type EGC > 50% Min BH (SMC). Endoscopy 2015
45 Immediate outcome measures - 1,838 cases with 1,889 EGCs treated by ESD - Patients enrollment: November May 2011 En bloc resection rate: 96.9% R0 resection rate: 94.0% En bloc and R0 resection rate: 92.2% Curative resection: 81.5% (1,539 EGCs in 1,497 patients / 1,838 EGCs in 1,889 patients) Bleeding: 4.1%, perforation: 3.2% Min BH (SMC). Endoscopy 2015
46 1,838 patients with 1,889 differentiated-type EGCs 1151 patients with 1171 EGCs-absolute - Single lesion: Two lesions: patients with 331 EGCs-expanded - Single lesion: 325 -Two lesions: 3 18 patients with 37 EGCs including both EGC-absolute and EGC-expanded - Two lesions: 17 -Three lesions: patients with at least one lesion treated with non-curative resection - Single lesion: Two lesions: 7 - Three lesions: 1 - Op: 1 - Residual lesion: 2 - Synchronous lesion: 9 - Follow up < 1 year: Op: 21 - Residual lesion: 0 - Synchronous lesion: 4 - Follow up < 1 year: 44 - Op: 0 - Residual lesion: 0 - Synchronous lesion: 0 - Follow up < 1 year: 3 *1032 patients with 1049 EGCs-absolute *259 patients with 261 EGCs-expanded *15 patients with 31 EGCs including both EGC-absolute and EGC-expanded 1 LR - EGC: 1 38 MR - EGC: 36 - pt2 AGC: 2 1 EGR 0 LR 8 MR - EGC: 7 - pt2 AGC: 1 1 EGR 0 LR 1 MR - EGC: 1 0 EGR Op: 1 Op: 16 ER: 22 Op: 1 Op: 3 ER: 5 Palliative Op: 1 ER: 1 * A total of 1,306 patients with 1,341 EGCs were included in the outcome analysis.
 - Among 1,306 curative ESDs from December 2003 to")
: 1 - pt2, LN (+): 2")
47 Metachronous recurrence (n=47, 3.6%) - Among 1,306 curative ESDs from December 2003 to May 2011 EGC: 44 cases - ESD alone: 28 - Surgery +/- ESD: 16 AGC: 3 cases - pt2, LN (-): 1 - pt2, LN (+): 2 Min BH (SMC). Endoscopy 2015
.")

48 Min BH (SMC). Endoscopy 2015

49 전정부위암 2 개 ESD

 -")
50 전정부위암 2 개 ESD 3 년후 fundus cancer 발견 - Histologic type : TA M/D with focal P/D - Size : 2.7x2.0 cm - Proper muscle invasion (pt2) - LN (-) 11 months ago



51 Second gastric cancer 10 months after ESD ESD First follow up Second follow up

52 ESD for EGC
53 Stomach, ESD. Early gastric carcinoma 1. Location : proximal antrum, anterior wall 2. Gross type : EGC type IIa 3. Histologic type : tubular adenocarcinoma, moderately differentiated 4. Histologic type by Lauren : intestinal 5. Size of carcinoma : (1) longest diameter, 28 mm (2) vertical diameter, 16 mm 6. Depth of invasion : invades mucosa (muscularis mucosa) (pt1a) 7. Resection margin : free from carcinoma(n). safety margin : distal 9 mm, proximal 8 mm, anterior 12 mm, posterior 14 mm 8. Lymphatic invasion : not identified(n) 9. Venous invasion : not identified(n) 10. Perineural invasion : not identified(n) 11. Microscopic ulcer : absent 12. Histologic heterogeneity: absent




54 ER for EGC EGC detected during surveillance in patient with UIP (M/73) EMR (submucosal dissection method using IT knife) W/D, 16mm, MM
55 Fold effect - 첫추적검사에서인근부위에서두번째암발견

56 처음사진을다시열어보겠습니다. Fold effect 를알수있겠습니까? Initial endoscopy before ER

57 첫추적검사에서두번째암발견 M/D, 6mm, MM

58 위선종 EMR 1 년후위암발견

 (pt1a)")

59 ESD using needle knife (2009) ESD: Early gastric carcinoma : - Histologic type : tubular adenocarcinoma, well differentiated - Size : 1x0.6x0.1 cm - Depth of invasion : invades mucosa (lamina propria) (pt1a) - Resection margin: free from carcinoma, safety margin: distal 0.8 cm, proximal 1 cm, anterior 1.2 cm, posterior 1.2 cm - Lymphatic invasion : not identified - Venous invasion : not identified


60 이소성위암을모두 ESD 할수있지않다. - Biopsy: P/D adenocarcinoma
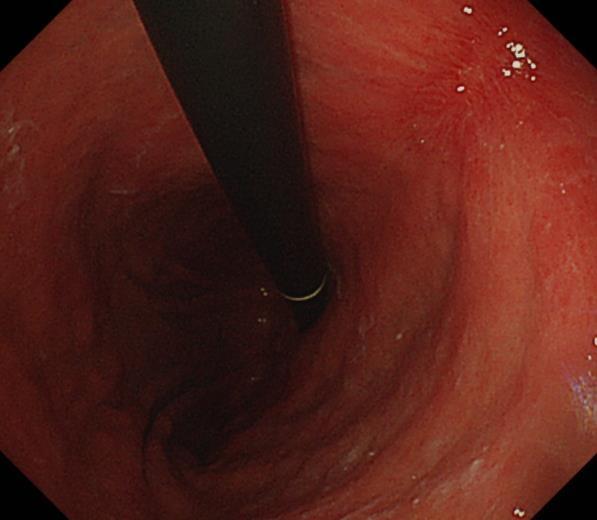
61 집으로가져가는메세지 Field cancerization. 위암혹은위선종환자에서다른부위의병소는언제나발생할수있습니다. ESD 후 local recurrence에유의합시다. 특히고위험환자에서. ESD 후첫추적검사에서는인근부위위암에유의합시다. Fold effect. 식도와십이지장도주의합시다.
62 SMC policy EGD after ESD - 조기위암 / 위선종내시경치료후추적검사 조기위암 EMR/ESD: 5 년까지추적내시경마다 scar 에서 조직검사 (1-2 점 ) 5 년후부터는재발의심소견이있 을때만조직검사 ( 단, 조기위암 EMR/ESD 후첫추적내 시경에서는 H. pylori 조직검사도함께시행한다.) 선종 EMR/ESD: 1 년까지추적내시경마다 scar 에서조직 검사 (1-2 점 ) 1 년후부터는재발의심소견이있을때 만조직검사 선종 APC: 재발의심소견이있을때만조직검사
Treatment Strategy for Non-curative Resection of Early Gastric Cancer. Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea
 Treatment Strategy for Non-curative Resection of Early Gastric Cancer Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea Classic EMR/ESD data analysis style Endoscopic resection
Treatment Strategy for Non-curative Resection of Early Gastric Cancer Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea Classic EMR/ESD data analysis style Endoscopic resection
위암내시경진단 (2019) - 융기형위암을중심으로 성균관대학교의과대학내과이준행
 - 융기형위암을중심으로 성균관대학교의과대학내과이준행") 위암내시경진단 (2019) - 융기형위암을중심으로 성균관대학교의과대학내과이준행 위암내시경진단 (2019) 위암검진에대한짧지않은 comment 융기형암은융기되어있는가? 함몰형암은함몰되어있는가? Semi-pedunculated polyp Sentinel polyp or EGJ cancer? IIa + IIc 위암검진에대한짧지않은 comment 성균관대학교의과대학내과이준행
위암내시경진단 (2019) - 융기형위암을중심으로 성균관대학교의과대학내과이준행 위암내시경진단 (2019) 위암검진에대한짧지않은 comment 융기형암은융기되어있는가? 함몰형암은함몰되어있는가? Semi-pedunculated polyp Sentinel polyp or EGJ cancer? IIa + IIc 위암검진에대한짧지않은 comment 성균관대학교의과대학내과이준행
ESD for EGC with undifferentiated histology
 ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Current status of gastric ESD in Korea. Jun Haeng Lee. Department of Medicine Sungkyunkwanuniversity School of Medicie, Seoul, Korea
 Current status of gastric ESD in Korea Jun Haeng Lee. Department of Medicine Sungkyunkwanuniversity School of Medicie, Seoul, Korea Contents Brief history of gastric ESD in Korea ESD/EMR for gastric adenoma
Current status of gastric ESD in Korea Jun Haeng Lee. Department of Medicine Sungkyunkwanuniversity School of Medicie, Seoul, Korea Contents Brief history of gastric ESD in Korea ESD/EMR for gastric adenoma
How to treat early gastric cancer? Endoscopy
 How to treat early gastric cancer? Endoscopy Presented by Pierre H. Deprez Institution Cliniques universitaires Saint-Luc, Brussels Université catholique de Louvain 2 3 4 5 6 Background Diagnostic or therapeutic
How to treat early gastric cancer? Endoscopy Presented by Pierre H. Deprez Institution Cliniques universitaires Saint-Luc, Brussels Université catholique de Louvain 2 3 4 5 6 Background Diagnostic or therapeutic
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS
 COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 Final Pathology:
 Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Imaging in gastric cancer
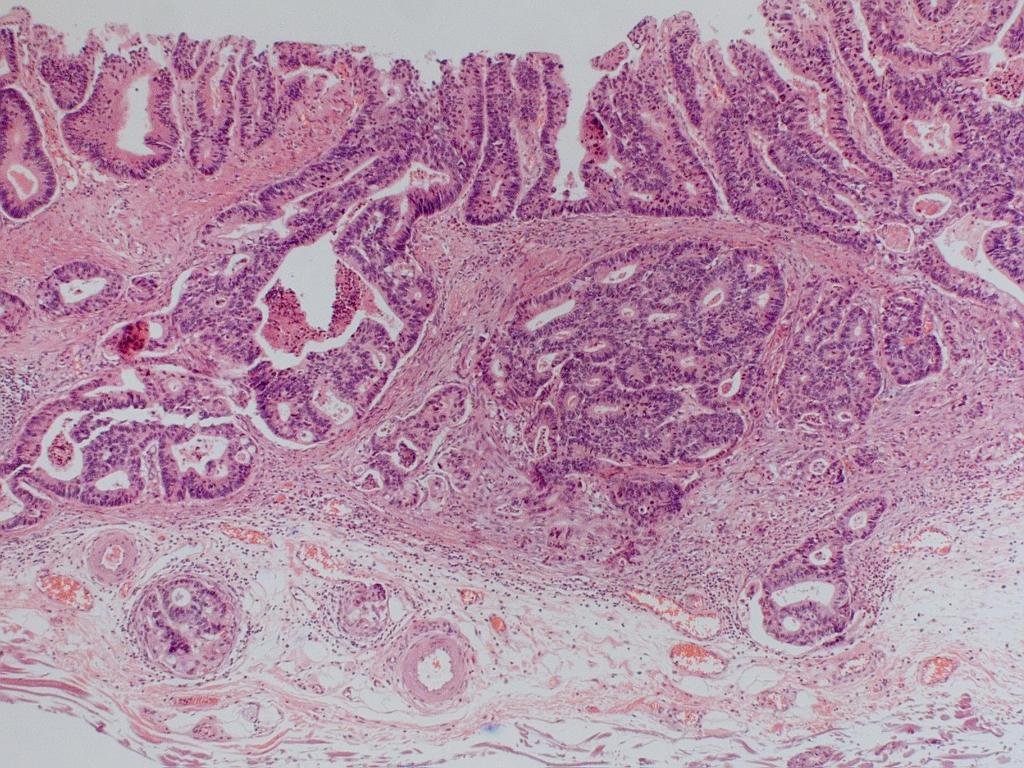
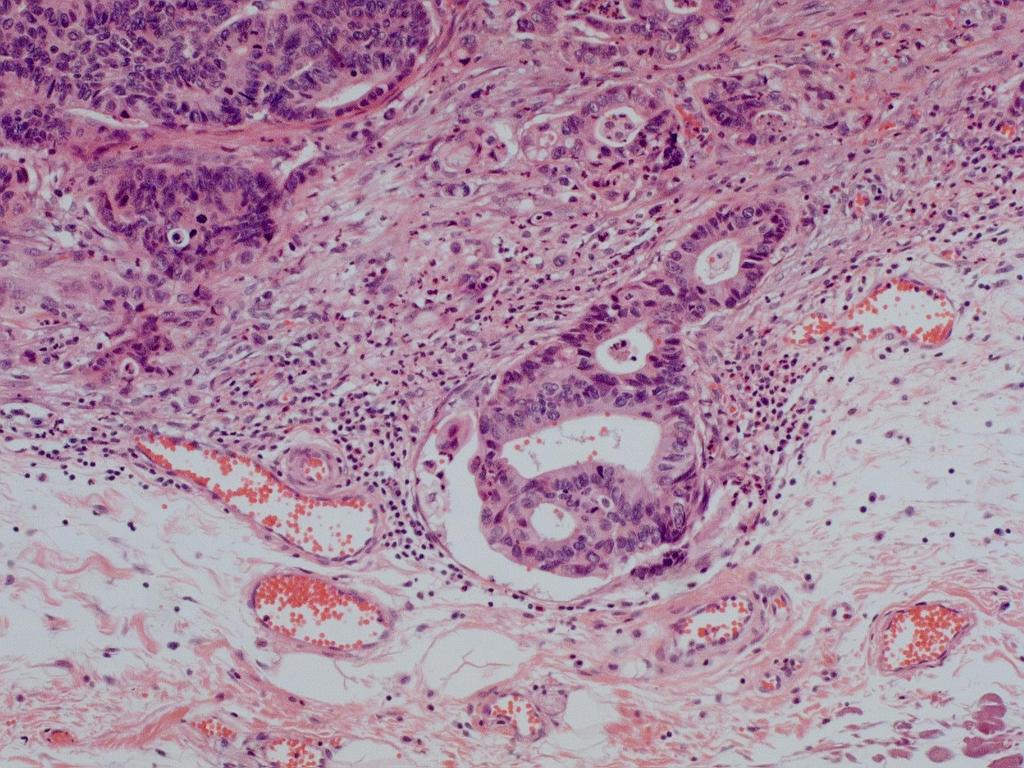
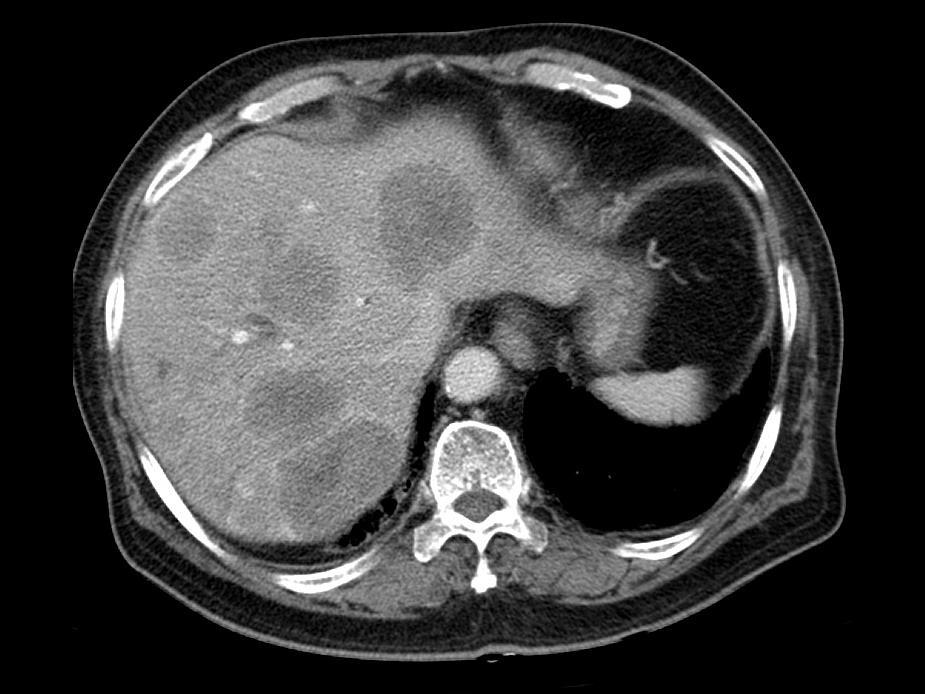
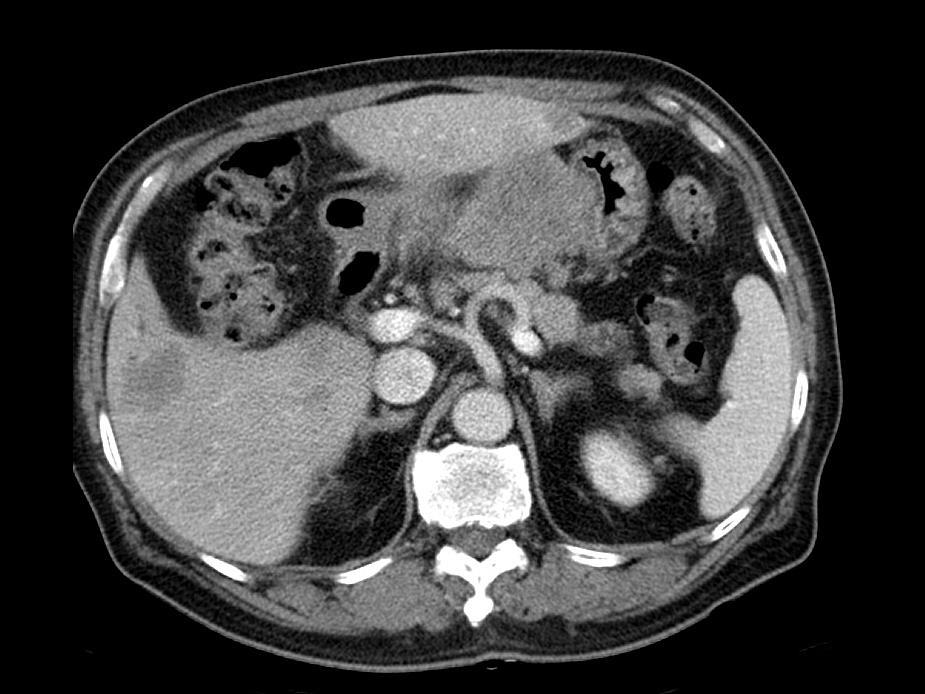
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Departmental and institutional affiliation: Departments of Medicine, Samsung Medical
 Endoscopic Submucosal Dissection for Early Gastric Neoplasia Occurring in the Remnant Stomach after Distal Gastrectomy Short running title: ESD for tumors in the remnant stomach Authors: Ji Young Lee,
Endoscopic Submucosal Dissection for Early Gastric Neoplasia Occurring in the Remnant Stomach after Distal Gastrectomy Short running title: ESD for tumors in the remnant stomach Authors: Ji Young Lee,
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Quiz Adenocarcinoma of the distal stomach has been increasing in the last 20 years. a. True b. False
 Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Delayed Perforation Occurring after Endoscopic Submucosal Dissection for Early Gastric Cancer
 CASE REPORT Clin Endosc 2015;48:251-255 Print ISSN 2234-2400 / On-line ISSN 2234-2443 http://dx.doi.org/10.5946/ce.2015.48.3.251 Open Access Delayed Perforation Occurring after Endoscopic Submucosal Dissection
CASE REPORT Clin Endosc 2015;48:251-255 Print ISSN 2234-2400 / On-line ISSN 2234-2443 http://dx.doi.org/10.5946/ce.2015.48.3.251 Open Access Delayed Perforation Occurring after Endoscopic Submucosal Dissection
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Gastric Cancer in a Young Postpartum Female. Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012
 Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma
 Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
How to remove BE cancer: EMR or ESD? Expected outcome
 How to remove BE cancer: EMR or ESD? Expected outcome Presented by Horst Neuhaus Institution Dpt. of Gastroenterology Evangelisches Krankenhaus Düsseldorf, Germany Indications for endoscopic resection
How to remove BE cancer: EMR or ESD? Expected outcome Presented by Horst Neuhaus Institution Dpt. of Gastroenterology Evangelisches Krankenhaus Düsseldorf, Germany Indications for endoscopic resection
A218 : Esophagus cancer tissues. (formalin fixed)
") (formalin fixed) For research use only Specifications: No. of cases: 40 Tissue type: Esophagus cancer tissues No. of spots: 2 spots from each cancer case (80 spots) 4 non-neoplastic spots (4 spots) Total
(formalin fixed) For research use only Specifications: No. of cases: 40 Tissue type: Esophagus cancer tissues No. of spots: 2 spots from each cancer case (80 spots) 4 non-neoplastic spots (4 spots) Total
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
A916: rectum: adenocarcinoma
 General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
Endoscopic Submucosal Dissection of an Inverted Early Gastric Cancer-Forming False Gastric Diverticulum
 CSE REPORT Clin Endosc 2016;49:86-90 http://dx.doi.org/10.5946/ce.2016.49.1.86 Print ISSN 2234-2400 / On-line ISSN 2234-2443 Open ccess Endoscopic Submucosal Dissection of an Inverted Early Gastric Cancer-Forming
CSE REPORT Clin Endosc 2016;49:86-90 http://dx.doi.org/10.5946/ce.2016.49.1.86 Print ISSN 2234-2400 / On-line ISSN 2234-2443 Open ccess Endoscopic Submucosal Dissection of an Inverted Early Gastric Cancer-Forming
Oesophagus and Stomach update dysplasia and early cancer
 Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
Oesophagus and Stomach update dysplasia and early cancer Dr Tim Bracey STR teaching 13/4/16 Please check pathkids.com for previous talks One of the biggest units in the country (100 major resections per
University Mainz. Early Gastric Cancer. Ralf Kiesslich. Johannes Gutenberg University Mainz, Germany. Early Gastric Cancer 15.6.
 Ralf Kiesslich Johannes Gutenberg University Mainz, Germany DIAGNOSIS Unmask lesions - Chromoendoscopy -NBI Red flag technology - Autofluorescence Surface and detail analysis - Magnifying endoscopy - High
Ralf Kiesslich Johannes Gutenberg University Mainz, Germany DIAGNOSIS Unmask lesions - Chromoendoscopy -NBI Red flag technology - Autofluorescence Surface and detail analysis - Magnifying endoscopy - High
Gastric Cancer: Surgery and Regional Therapy. Epidemiology. Risk factors
 Gastric Cancer: Surgery and Regional Therapy Timothy J. Kennedy, MD Montefiore Medical Center Assistant Professor of Surgery Upper Gastrointestinal and Pancreas Surgery December 15, 2012 1 Epidemiology
Gastric Cancer: Surgery and Regional Therapy Timothy J. Kennedy, MD Montefiore Medical Center Assistant Professor of Surgery Upper Gastrointestinal and Pancreas Surgery December 15, 2012 1 Epidemiology
Clinical Outcomes of Endoscopic Submucosal Dissection in Patients under 40 Years Old with Early Gastric Cancer
 ORIGINAL ARTICLE ISSN 1738-3331, http://dx.doi.org/10.7704/kjhugr.2016.16.3.139 The Korean Journal of Helicobacter and Upper Gastrointestinal Research, 2016;16(3):139-146 Clinical Outcomes of Endoscopic
ORIGINAL ARTICLE ISSN 1738-3331, http://dx.doi.org/10.7704/kjhugr.2016.16.3.139 The Korean Journal of Helicobacter and Upper Gastrointestinal Research, 2016;16(3):139-146 Clinical Outcomes of Endoscopic
A case of local recurrence and distant metastasis following curative endoscopic submucosal dissection of early gastric cancer
 Gastric Cancer (2015) 18:188 192 DOI 10.1007/s10120-014-0341-7 CASE REPORT A case of local recurrence and distant metastasis following curative endoscopic submucosal dissection of early gastric cancer
Gastric Cancer (2015) 18:188 192 DOI 10.1007/s10120-014-0341-7 CASE REPORT A case of local recurrence and distant metastasis following curative endoscopic submucosal dissection of early gastric cancer
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ
 - Project manual + FAQ") Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
Barrett Esophagus - RadioFrequency Ablation (BE-RFA) - Project manual + FAQ Table of contents 1 General project information...3 1.1 Inclusion criteria...3 1.2 Registration time points...3 1.3 Project variable
Staging Challenges in Lower GI Cancers. Disclosure of Relevant Financial Relationships. AJCC 8 th edition and CAP protocol updates
 Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Patient. Male 76 year old C.C: abdominal pain
 Patient Male 76 year old C.C: abdominal pain Bowel stool retention Suspected pulmonary TB at right upper lung Infiltration in right lower lung Pleural thickening at the Right chest Localized dilated small
Patient Male 76 year old C.C: abdominal pain Bowel stool retention Suspected pulmonary TB at right upper lung Infiltration in right lower lung Pleural thickening at the Right chest Localized dilated small
AGA SECTION. Gastroenterology 2016;150:
 Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Gastroenterology 2016;150:1026 1030 April 2016 AGA Section 1027 Procedural intervention (3) Upper endoscopy indications 3 6 Non-response of symptoms to a 4 8 week empiric trial of twice-daily PPI Troublesome
Risk factors for lymph node metastasis in histologically poorly differentiated type early gastric cancer
 498 Original article Risk factors for lymph node metastasis in histologically poorly differentiated type early gastric cancer Authors C. Kunisaki 1, M. Takahashi 2, Y. Nagahori 3, T. Fukushima 3, H. Makino
498 Original article Risk factors for lymph node metastasis in histologically poorly differentiated type early gastric cancer Authors C. Kunisaki 1, M. Takahashi 2, Y. Nagahori 3, T. Fukushima 3, H. Makino
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of endoscopic submucosal dissection of gastric lesions This procedure can be
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of endoscopic submucosal dissection of gastric lesions This procedure can be
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
We are IntechOpen, the first native scientific publisher of Open Access books. International authors and editors. Our authors are among the TOP 1%
 We are IntechOpen, the first native scientific publisher of Open Access books 3,350 108,000 1.7 M Open access books available International authors and editors Downloads Our authors are among the 151 Countries
We are IntechOpen, the first native scientific publisher of Open Access books 3,350 108,000 1.7 M Open access books available International authors and editors Downloads Our authors are among the 151 Countries
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Principles of diagnosis, work-up and therapy The Gastroenterologist s role
 Principles of diagnosis, work-up and therapy The Gastroenterologist s role Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University
Principles of diagnosis, work-up and therapy The Gastroenterologist s role Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University
Update on staging colorectal carcinoma, the 8 th edition AJCC. General overview of staging. When is staging required? 11/1/2017
 Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Mucinous Adenocarcinoma of the Stomach Clinicopathological
 THE KURUME MEDICAL JOURNAL Vo1. 43, p. 289-294, 1996 ORIGINAL ARTICLE Mucinous Adenocarcinoma of the Stomach Clinicopathological Studies KIKUO KOUFUJI, JINRYO TAKEDA, ATSUSHI TOYONAGA, ISSEI KODAMA, KEISHIRO
THE KURUME MEDICAL JOURNAL Vo1. 43, p. 289-294, 1996 ORIGINAL ARTICLE Mucinous Adenocarcinoma of the Stomach Clinicopathological Studies KIKUO KOUFUJI, JINRYO TAKEDA, ATSUSHI TOYONAGA, ISSEI KODAMA, KEISHIRO
Gastric Cancer Staging AJCC eighth edition. Duncan McLeod Westmead Hospital, NSW
 Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Prognostic analysis of gastric mucosal dysplasia after endoscopic resection: A single-center retrospective study
 JBUON 2019; 24(2): 679-685 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Prognostic analysis of gastric mucosal dysplasia after endoscopic resection:
JBUON 2019; 24(2): 679-685 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Prognostic analysis of gastric mucosal dysplasia after endoscopic resection:
A215- Urinary bladder cancer tissues
 A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
Early and long term outcomes of endoscopic submucosal dissection for early gastric cancer in a large patient series
 594 Early and long term outcomes of endoscopic submucosal dissection for early gastric cancer in a large patient series KEN OHNITA 1, HAJIME ISOMOTO 1, SABURO SHIKUWA 2, HIROYUKI YAJIMA 1, HITOMI MINAMI
594 Early and long term outcomes of endoscopic submucosal dissection for early gastric cancer in a large patient series KEN OHNITA 1, HAJIME ISOMOTO 1, SABURO SHIKUWA 2, HIROYUKI YAJIMA 1, HITOMI MINAMI
GASTRIC CANCER. Joyce Au SUNY Downstate Grand Rounds July 11, 2013
 GASTRIC CANCER Joyce Au SUNY Downstate Grand Rounds July 11, 2013 xxm with gastric adenocarcinoma on biopsy of antral lesion on EGD at outside hospital PMH: residual schizophrenia, HTN PSH: exploratory
GASTRIC CANCER Joyce Au SUNY Downstate Grand Rounds July 11, 2013 xxm with gastric adenocarcinoma on biopsy of antral lesion on EGD at outside hospital PMH: residual schizophrenia, HTN PSH: exploratory
Earlyoesophagealcancer. dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia
 Earlyoesophagealcancer dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia Early carcinoma of oesophagus = tumor limited to mucosa or submucosa, not extending into
Earlyoesophagealcancer dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia Early carcinoma of oesophagus = tumor limited to mucosa or submucosa, not extending into
Barrett s Esophagus: Old Dog, New Tricks
 Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Histopathology: gastritis and peptic ulceration
 Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
Endoscopic UltraSound (EUS) Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C.
 Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C.") Endoscopic UltraSound (EUS) Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Research Grants: Disclosures
Endoscopic UltraSound (EUS) Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Research Grants: Disclosures
Management of pt1 polyps. Maria Pellise
 Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE
 COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia
 National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
Upper GIT IV Gastric cancer
 Upper GIT IV Gastric cancer Luigi Tornillo PathoBasic 23.10.2014 Pathology Introduction Classification Morphogenesis Problems Intraepithelial neoplasia Surveillance EGJ Predictive factors Gastric cancer
Upper GIT IV Gastric cancer Luigi Tornillo PathoBasic 23.10.2014 Pathology Introduction Classification Morphogenesis Problems Intraepithelial neoplasia Surveillance EGJ Predictive factors Gastric cancer
Endoscopic submucosal dissection: European Society of Gastrointestinal Endoscopy (ESGE) Guideline
 Guideline") Guideline 829 Endoscopic submucosal dissection: European Society of Gastrointestinal Endoscopy (ESGE) Guideline Authors Institutions Bibliography DOI http://dx.doi.org/ 10.1055/s-0034-1392882 Endoscopy
Guideline 829 Endoscopic submucosal dissection: European Society of Gastrointestinal Endoscopy (ESGE) Guideline Authors Institutions Bibliography DOI http://dx.doi.org/ 10.1055/s-0034-1392882 Endoscopy
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
recurrence (range: 2 35%) in such cases, especially when resections are not accomplished en bloc or the margins are not clear [8].
![recurrence (range: 2 35%) in such cases, especially when resections are not accomplished en bloc or the margins are not clear [8].](/thumbs/90/103291995.jpg "recurrence (range: 2 35%) in such cases, especially when resections are not accomplished en bloc or the margins are not clear [8].") Original article 311 Clinical outcomes of endoscopic submucosal dissection in elderly patients with early gastric cancer Hajime Isomoto a,b, Ken Ohnita a,b, Naoyuki Yamaguchi a,b, Eiichiro Fukuda a, Kohki
Original article 311 Clinical outcomes of endoscopic submucosal dissection in elderly patients with early gastric cancer Hajime Isomoto a,b, Ken Ohnita a,b, Naoyuki Yamaguchi a,b, Eiichiro Fukuda a, Kohki
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Gastric Extremely Well-Diferentiated Intestinal-Type Adenocarcinoma: A Challenging Lesion to Achieve Complete Endoscopic Resection
 Gastric Extremely Well-Diferentiated Intestinal-Type Adenocarcinoma: A Challenging Lesion to Achieve Complete Endoscopic Resection The Harvard community has made this article openly available. Please share
Gastric Extremely Well-Diferentiated Intestinal-Type Adenocarcinoma: A Challenging Lesion to Achieve Complete Endoscopic Resection The Harvard community has made this article openly available. Please share
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Gastrointestinal Tract Cancer
 Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Endoscopic Submucosal Dissection ESD
 Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Protocol for the Examination of Specimens From Patients With Carcinoma of the Stomach
 Protocol for the Examination of Specimens From Patients With Carcinoma of the Stomach Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For
Protocol for the Examination of Specimens From Patients With Carcinoma of the Stomach Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual For
Approaches to Surgical Treatment of Gastric Cancer. Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service
 Approaches to Surgical Treatment of Gastric Cancer Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service Disclosures I do not have anything to disclose Outline Background Diagnosis Histology Staging Surgery
Approaches to Surgical Treatment of Gastric Cancer Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service Disclosures I do not have anything to disclose Outline Background Diagnosis Histology Staging Surgery
Large polyps: EMR, ESD, TEM and segmental resection. Terry Phang 2017 SON fall update
 Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
Esophageal cancer: Biology, natural history, staging and therapeutic options
 EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
Is Hepatic Resection Needed in the Patients with Peritoneal Side T2 Gallbladder Cancer?
 Is Hepatic Resection Needed in the Patients with Peritoneal Side T2 Gallbladder Cancer? Lee H, Park JY, Youn S, Kwon W, Heo JS, Choi SH, Choi DW Department of Surgery, Samsung Medical Center Sungkyunkwan
Is Hepatic Resection Needed in the Patients with Peritoneal Side T2 Gallbladder Cancer? Lee H, Park JY, Youn S, Kwon W, Heo JS, Choi SH, Choi DW Department of Surgery, Samsung Medical Center Sungkyunkwan
Key words: gastric cancer, lymphovascular invasion, recurrence
 Key words: gastric cancer, lymphovascular invasion, recurrence 139 (2177) Table I Relationship between clinicopathologic factors and lymphatic invasion in 2146 patients with gastric cancer Factors P-value
Key words: gastric cancer, lymphovascular invasion, recurrence 139 (2177) Table I Relationship between clinicopathologic factors and lymphatic invasion in 2146 patients with gastric cancer Factors P-value
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Clinicopathologic Characteristics and Prognosis of Gastric Cancer in Young Patients
 Yonago Acta medica 2012;55:57 61 Clinicopathologic Characteristics and Prognosis of Gastric Cancer in Young Patients Hiroaki Saito, Seigo Takaya, Yoji Fukumoto, Tomohiro Osaki, Shigeru Tatebe and Masahide
Yonago Acta medica 2012;55:57 61 Clinicopathologic Characteristics and Prognosis of Gastric Cancer in Young Patients Hiroaki Saito, Seigo Takaya, Yoji Fukumoto, Tomohiro Osaki, Shigeru Tatebe and Masahide
Case 1- B.N. 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids.
 Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
CASE REPORT. Introduction. Case Report. Kimitoshi Kubo 1, Noriko Kimura 2, Katsuhiro Mabe 1, Yusuke Nishimura 1 and Mototsugu Kato 1
 doi: 10.2169/internalmedicine.0842-18 Intern Med 57: 2951-2955, 2018 http://internmed.jp CASE REPORT Synchronous Triple Gastric Cancer Incorporating Mixed Adenocarcinoma and Neuroendocrine Tumor Completely
doi: 10.2169/internalmedicine.0842-18 Intern Med 57: 2951-2955, 2018 http://internmed.jp CASE REPORT Synchronous Triple Gastric Cancer Incorporating Mixed Adenocarcinoma and Neuroendocrine Tumor Completely
Carcinoma of the Renal Pelvis and Ureter Histopathology
 Carcinoma of the Renal Pelvis and Ureter Histopathology Reporting Proforma (NEPHROURETERECTOMY AND URETERECTOMY) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Renal Pelvis and Ureter Histopathology Reporting Proforma (NEPHROURETERECTOMY AND URETERECTOMY) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Risk Factors and Tumor Recurrence in pt1n0m0 Gastric Cancer after Surgical Treatment
 pissn : 293-582X, eissn : 293-5641 J Gastric Cancer 216;16(4):215-22 https://doi.org/1.523/jgc.216.16.4.215 Original Article Risk Factors and Tumor Recurrence in pt1nm Gastric Cancer after Surgical Treatment
pissn : 293-582X, eissn : 293-5641 J Gastric Cancer 216;16(4):215-22 https://doi.org/1.523/jgc.216.16.4.215 Original Article Risk Factors and Tumor Recurrence in pt1nm Gastric Cancer after Surgical Treatment
THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD
 SNARE THE CASE FOR EMR AND ESD") THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD Surgical Oncology Network meeting Dr. Eric Lam MD FRCPC October 14, 2017 DISCLOSURES None OBJECTIVES Appreciate
THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD Surgical Oncology Network meeting Dr. Eric Lam MD FRCPC October 14, 2017 DISCLOSURES None OBJECTIVES Appreciate
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
References. GI Biopsies. What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD
 What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
GASTRIC CANCER DR AMIR ASHRAFI
 GASTRIC CANCER DR AMIR ASHRAFI Epidemiology Aetiologic factors Classification Clinical features Investigations Staging Treatment EPIDEMIOLOGY AND FACTS ü Worldwide, gastric cancer is the fourth most common
GASTRIC CANCER DR AMIR ASHRAFI Epidemiology Aetiologic factors Classification Clinical features Investigations Staging Treatment EPIDEMIOLOGY AND FACTS ü Worldwide, gastric cancer is the fourth most common
Gastric Polyps. Bible class
 Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Management of Barrett s: From Imaging to Resection
 Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
AUSTRALIAN PATHOLOGY UNITS AND TERMINOLOGY (APUTS) Reporting Terminology and Codes Anatomical Pathology. (v2.1)
 Reporting Terminology and Codes Anatomical Pathology. (v2.1)") AUSTRALIAN PATHOLOGY UNITS AND TERMINOLOGY (APUTS) Reporting Terminology and Codes Anatomical Pathology (v2.1) ISBN: Pending 1 State Health Publication Number (SHPN): Pending Online copyright RCPA 2014
AUSTRALIAN PATHOLOGY UNITS AND TERMINOLOGY (APUTS) Reporting Terminology and Codes Anatomical Pathology (v2.1) ISBN: Pending 1 State Health Publication Number (SHPN): Pending Online copyright RCPA 2014
EMR, ESD and Beyond. Peter Draganov MD. Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida
 EMR, ESD and Beyond Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated by Endoscopy
EMR, ESD and Beyond Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated by Endoscopy
Rectal EMR: Techniques and Tips
 Rectal EMR: Techniques and Tips Dr Paul Urquhart Epworth Eastern Eastern Health (Head of Endoscopy) The context of EMR Basic Technique Recurrence Perforation Bleeding Introduction 1 I don t treat rectal
Rectal EMR: Techniques and Tips Dr Paul Urquhart Epworth Eastern Eastern Health (Head of Endoscopy) The context of EMR Basic Technique Recurrence Perforation Bleeding Introduction 1 I don t treat rectal
Local Excision for early rectal cancer
 Local Excision for early rectal cancer M. Trompetto, E. Ganio, G. Clerico, A. Realis Luc, RJ Nicholls Colorectal Eporediensis Centre Clinica S. Rita Vercelli Gruppo Policlinico di Monza Mortality Morbidity
Local Excision for early rectal cancer M. Trompetto, E. Ganio, G. Clerico, A. Realis Luc, RJ Nicholls Colorectal Eporediensis Centre Clinica S. Rita Vercelli Gruppo Policlinico di Monza Mortality Morbidity
Long-term survival after endoscopic resection versus surgery in early gastric cancers
 Original article 293 Long-term survival after endoscopic versus surgery in early gastric cancers Authors Institution submitted 21. April 214 accepted after revision 27. October 214 Bibliography DOI http://dx.doi.org/
Original article 293 Long-term survival after endoscopic versus surgery in early gastric cancers Authors Institution submitted 21. April 214 accepted after revision 27. October 214 Bibliography DOI http://dx.doi.org/
Advanced techniques for resection of large polyps. John G. Lee, MD February 2, 2018
 Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
The surface mucous cells and the cardiac and pyloric glands secrete mucus which protects the stomach from self-digestion.
 PATHOLOGY OF THE STOMACH Stomach mucosa Gastric mucosa is covered by a layer of mucus. The mucosal glands comprise the cardiac glands, the fundic glands in the fundus and body of the stomach, and the pyloric
PATHOLOGY OF THE STOMACH Stomach mucosa Gastric mucosa is covered by a layer of mucus. The mucosal glands comprise the cardiac glands, the fundic glands in the fundus and body of the stomach, and the pyloric
Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD
 Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD Surgical Therapy of Gastric Cancer CLINICAL QUESTIONS 1. How much of the stomach should be removed? 2. How many lymph
Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD Surgical Therapy of Gastric Cancer CLINICAL QUESTIONS 1. How much of the stomach should be removed? 2. How many lymph
The Royal Marsden. Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum
 The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum The Royal Marsden William Allum Conflict of Interest None Any surgeon can cure Surgeon - dependent
The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum The Royal Marsden William Allum Conflict of Interest None Any surgeon can cure Surgeon - dependent
Case Report Intramucosal Signet Ring Cell Gastric Cancer Diagnosed 15 Months after the Initial Endoscopic Examination
 Hindawi Publishing Corporation Case Reports in Medicine Volume 2015, Article ID 479625, 5 pages http://dx.doi.org/10.1155/2015/479625 Case Report Intramucosal Signet Ring Cell Gastric Cancer Diagnosed
Hindawi Publishing Corporation Case Reports in Medicine Volume 2015, Article ID 479625, 5 pages http://dx.doi.org/10.1155/2015/479625 Case Report Intramucosal Signet Ring Cell Gastric Cancer Diagnosed
Japanese gastric cancer treatment guidelines 2014 (ver. 4)
") Gastric Cancer (2017) 20:1 19 DOI 10.1007/s10120-016-0622-4 SPECIAL ARTICLE Japanese gastric cancer treatment guidelines 2014 (ver. 4) Japanese Gastric Cancer Association 1 Received: 13 May 2016 / Accepted:
Gastric Cancer (2017) 20:1 19 DOI 10.1007/s10120-016-0622-4 SPECIAL ARTICLE Japanese gastric cancer treatment guidelines 2014 (ver. 4) Japanese Gastric Cancer Association 1 Received: 13 May 2016 / Accepted:
Ritu Nayar, MD Professor and Vice Chair of Pathology Northwestern University, Feinberg School of Medicine Chicago, IL
 Ritu Nayar, MD Professor and Vice Chair of Pathology Northwestern University, Feinberg School of Medicine Chicago, IL email: r-nayar@northwestern.edu Nothing to disclose College of American Pathologists
Ritu Nayar, MD Professor and Vice Chair of Pathology Northwestern University, Feinberg School of Medicine Chicago, IL email: r-nayar@northwestern.edu Nothing to disclose College of American Pathologists
Disclosures. Gastric Intestinal Metaplasia and Early Gastric Cancer: Screening, Surveillance, and Endoscopic Therapy. ASGE Guidelines.
 Gastric Intestinal Metaplasia and Early Gastric Cancer: Screening, Surveillance, and Endoscopic Therapy Consultant for: Olympus Medtronic US Endoscopy Disclosures Joo Ha Hwang, MD, PhD Associate Professor
Gastric Intestinal Metaplasia and Early Gastric Cancer: Screening, Surveillance, and Endoscopic Therapy Consultant for: Olympus Medtronic US Endoscopy Disclosures Joo Ha Hwang, MD, PhD Associate Professor
Construction and external validation of a nomogram that predicts lymph node metastasis in early gastric cancer patients using preoperative parameters
 Original Article Construction and external validation of a nomogram that predicts lymph node metastasis in early gastric cancer patients using preoperative parameters Yinan Zhang 1*, Yiqiang Liu 2*, Ji
Original Article Construction and external validation of a nomogram that predicts lymph node metastasis in early gastric cancer patients using preoperative parameters Yinan Zhang 1*, Yiqiang Liu 2*, Ji