Colorectal Cancer Prevention Quantity and Quality Count
|
|
|
- Marcia White
- 5 years ago
- Views:
Transcription
1 Colorectal Cancer Prevention Quantity and Quality Count Ernesto Drelichman, MD Gastrointestinal Surgery & Endoscopy Providence Hospital
2 Key Messages Colorectal cancer can be prevented Screening reduces mortality from CRC All persons aged 50 years or older should be screened High-risk individuals should begin screening earlier Several effective screening options are available; not screening is no longer an option
3 Key Messages Quality Risk Assessment Consent Screening Study with quality indicators Pathology Communication Computerized Registry Follow up
4 Colon & Rectal Cancer 2 nd leading cause of cancer death 3rd most common cancer overall 147,500 new cases annually 57,100 deaths annually
5 Why Screen?...the primary strategy for preventing colorectal cancer deaths is to detect and remove precancerous polyps or to detect and treat cancer in its earliest stages CDC 2/99
")
6 Colorectal Carcinogenesis Normal Mucosa Aberrant Crypt Foci Adenoma Cancer T(0) T(10)
7 Staging and Prognosis Stage TNM Grouping 5-Yr. Survival 0 Tis; N0; M0 100% I T1-2; N0; M % II T3-4; N0 M % III Any T; N1-3; M0 40% IV Any T; Any N; M1 5%


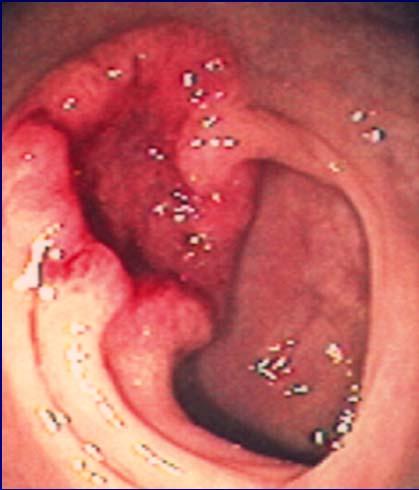
8 Colorectal Adenocarcinoma Flat Raised Ulcerated Infiltrating

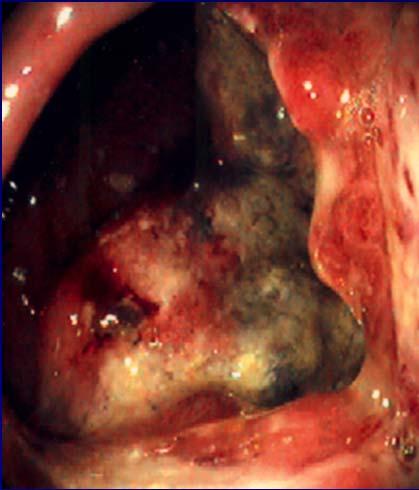
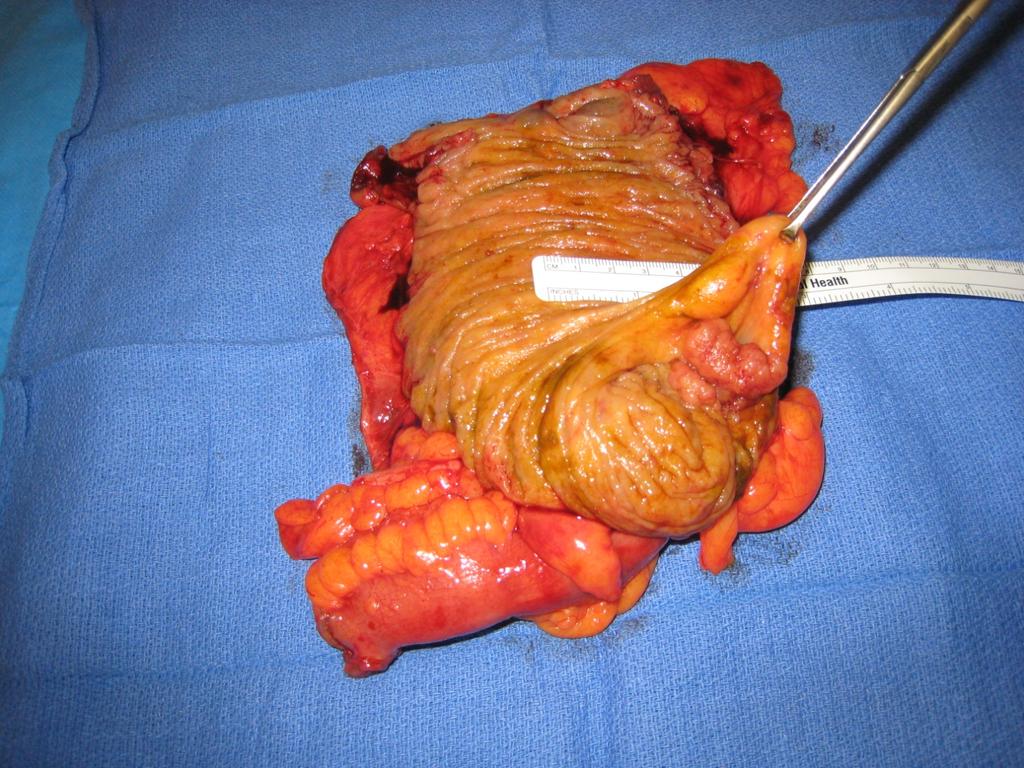
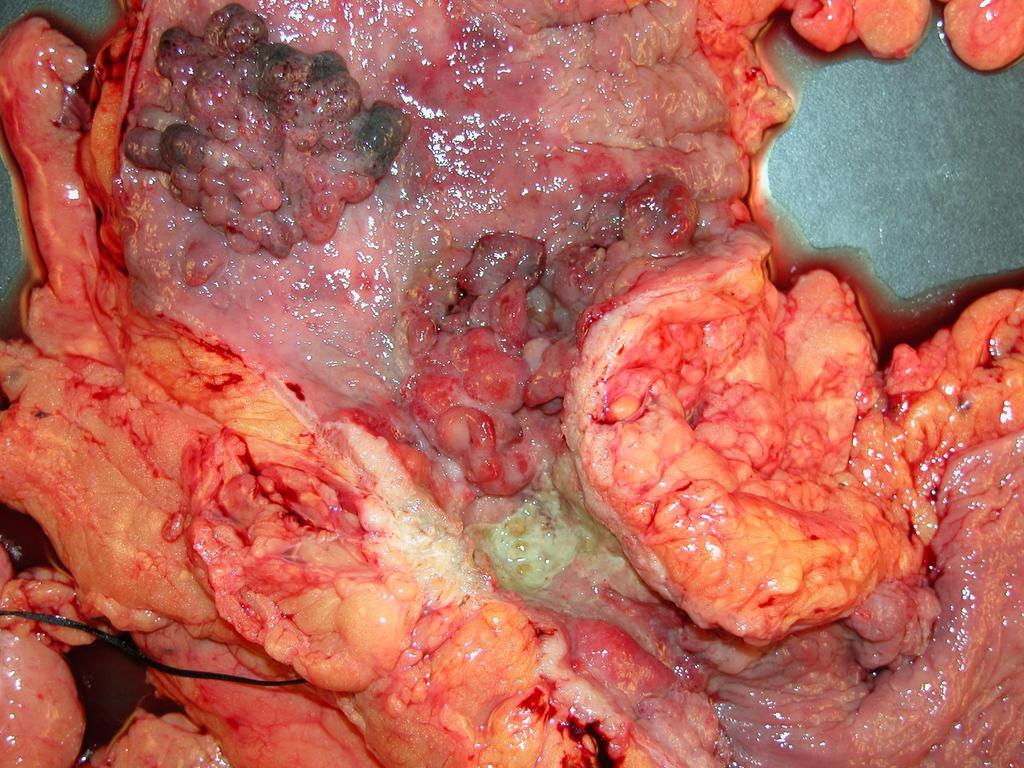
9 Stage IV Colon Cancer
10 Diagnosis vs Screening People with symptoms or signs that suggest the presence of colorectal cancer or polyps fall outside the domain of screening and should be offered an appropriate diagnostic evaluation.
11 Presentation Proximal (R-side) Ill-defined abd. pain Weight loss Occult bleeding Distal (L-side) Altered bowel habits Dec. stool caliber BRBPR
12 Screening vs Surveillance Screening = Detection of asymptomatic disease in healthy individuals at average risk (e.g. no identifiable risk factors other than age) Surveillance = Search for asymptomatic disease among higher risk individuals (e.g. personal history of polyps or cancer, etc.)

13 Screening Compliance CRC Overall 53% Breast Cancer 77% Behavioral Risk Factor Surveillance System, 2001
14 Barriers to Screening Patient Lack of information Low perceived risk Inconvenience Discomfort Expense Provider Lack of information Competing priorities Too many options Access concerns Petersen GM - Gastroenterol Clin North Am 2002;31: Vernon SW - J Natl Cancer Inst 1997;89:
15

16 Katie s first colonoscopy "It really didn't hurt"
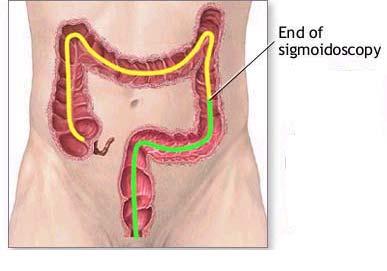
17 Screening Options Interval Fecal occult blood test (FOBT) 1 year Flexible sigmoidoscopy 5 years FOBT/Flex. Sig. 1 year/5 years Barium enema (DCBE) 5 years Colonoscopy 10 years Choice of screening tests should be suited to the situation.
18 IDEAL SCREENING TEST Detect all curable cancers Detect and allows excision adenomas Available, acceptable, safe Affordable and cost effective Providers must tailor to patients
19 FOBT Detect the pseudoperoxidase activity of heme Sensitivity neoplasms = 15% to 30% Poor specificity and high false positives
20 A better FIT Noninvasiveness No prep No diet restrictions Sensitivities of 66% for detecting cancer and 27% for detecting advanced polyps and a specificity of 95% Cost $18 and $30 Medicare reimbursed Morikawa T et al Gastroenterology. 2005;129:422-8

21 DNA Detect gene mutations in tumor cells sloughed into stool Noninvasiveness No prep No diet restrictions
22 DNA The DNA panel Sensitivity for invasive cancers = 40.8% Hemoccult P<0.001 = 14.1 percent Expensive Imeriale et al. N Engl J Med. 2004;351:

23 Barium Enema Screening No sedation required Reasonable sensitivity for cancer (83%) 1 1 Rex, et al. - Gastroenterology 1997;112:17-23; 2 Winawer, et al. - N Engl J Med 2000 Jun 15;342(24):
24 Barium Enema Screening Low Specificity - frequent need for repeat bowel prep and colonoscopy Lipoma Large fold Residual stool Poor sensitivity for polyps > 10 mm (48%) 2 1 Rex, et al. - Gastroenterology 1997;112:17-23; 2 Winawer, et al. - N Engl J Med 2000 Jun 15;342(24):
25 Virtual Colonoscopy Lack of consensus about its role in screening. Sensitivity 60% for cancer detection
26 SCREENING COLONOSCOPY If the result of a screening test is abnormal, physicians should recommend a complete colonic Evaluation: Colonoscopy Ko, Hyman Dis Colon Rectum 2006; 49: 1 3
27 COLONOSCOPY SCREENING IN THE U.S. Recommended as an option in 1997 Proposed as the preferred method of screening by ACG in 2000 Reimbursement by Medicare in 2001
28 Advantages Colonoscopy Gold Standard for Quality Highest sensitivity and specificity Entire colorectum assessed Neoplasms can be biopsied and/or removed during the screening exam (no follow-up testing required)
29
30
31
32

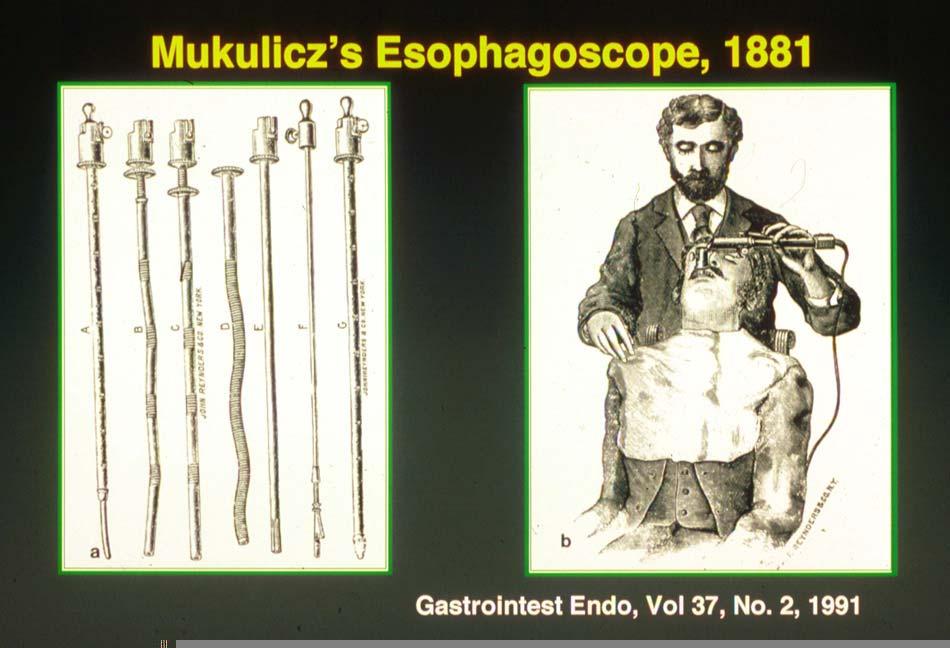
33 How to bend light?

34
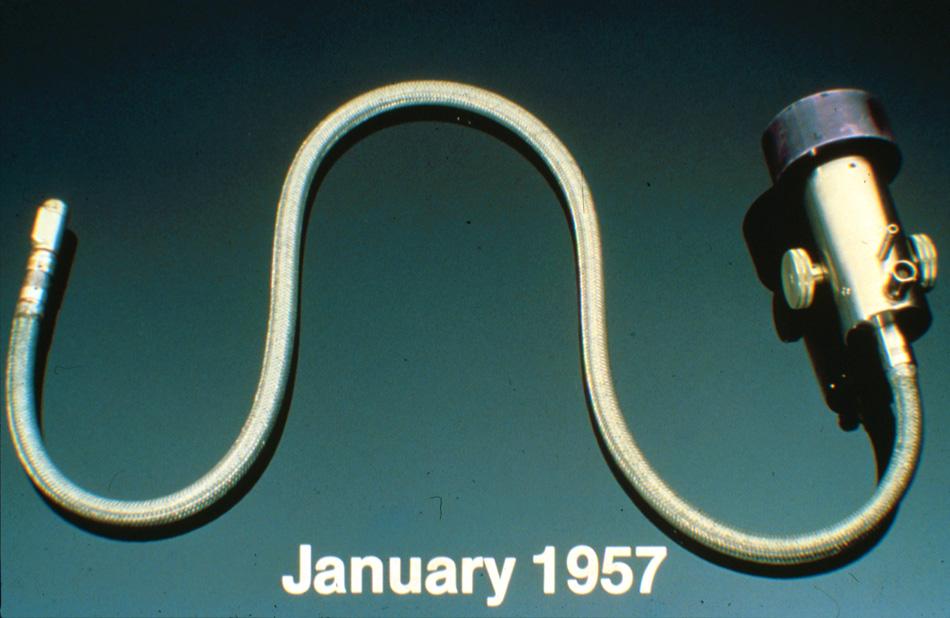
35 Prototype Fiberscope
36 Basil Hirschowitz, MD Emeritus Professor UAB

37 Basil Hirschowitz, M.D

38


39

40
41 Quality Screening Study Risk Assessment Uses and documents quality indicators in report Avoids potential complications of exam Makes correct recommendations in report Communicates to patients and referring physicians Registry to assure follow up

42 Perianal and DRE Photograph IC Valve appendiceal orifice Describe Prep Extraction time >6min Recommendations/risk Letter to referral Communicate to patient Computerized Registry Quality Indicators for Colonoscopy

43 A Quality exam starts here Perianal Exam and DRE
44

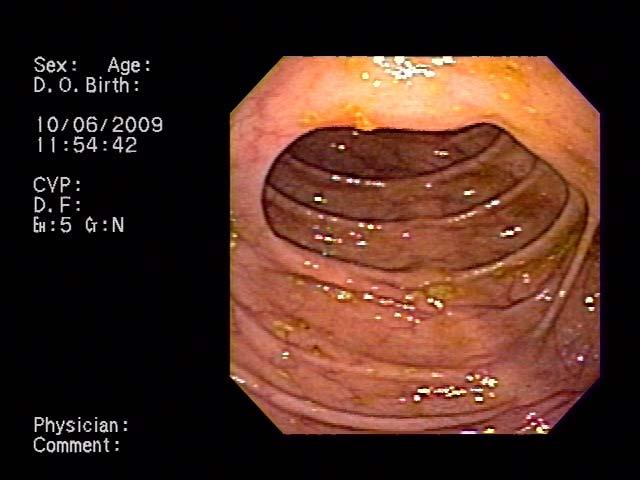
45 Terminal Ileum
46
47
48 Complete Study No cecal intubation Why and how was study completed what were the results Ileocolonic anastomosis Landmarks Appendiceal orifice Ileocecal valve Terminal ileum Transabdominal illumination*

49 Transillumination The Light at the End of the Tunnel

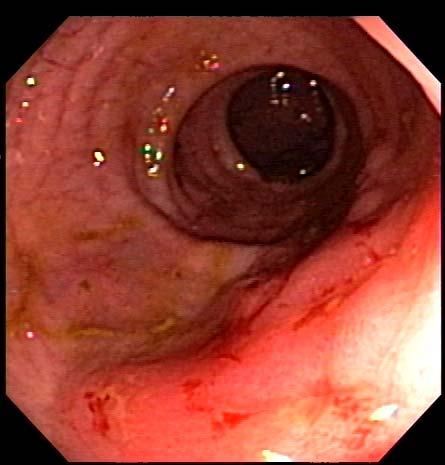
50 Diverticulosis Tics

51

52 Pedunculated Polyp Excision
53 Identification and removal of polyps prevents colorectal cancer

54 Piece-meal Polypectomy
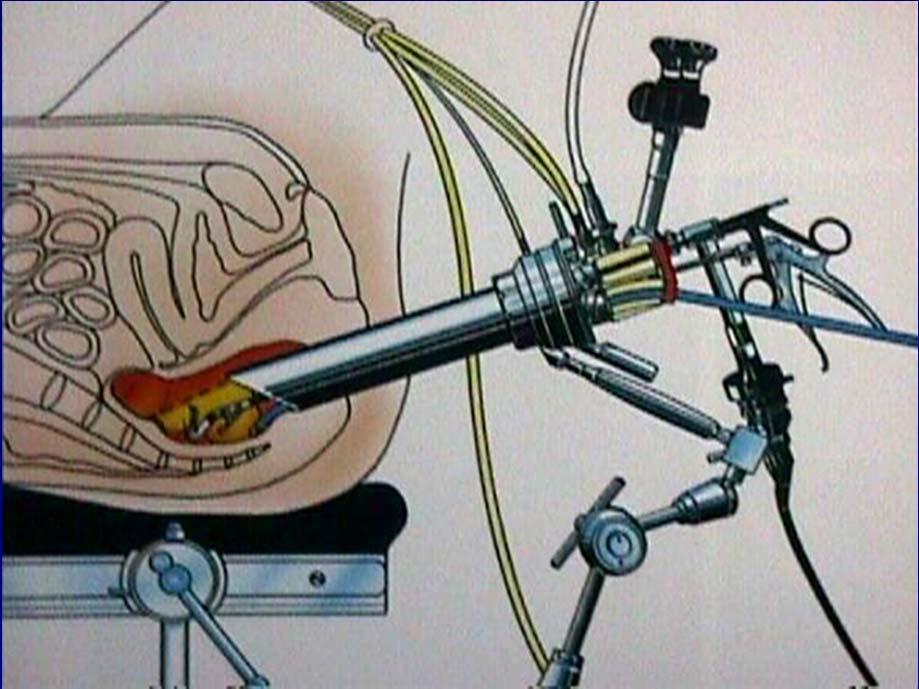
55 Transanal Endoscopic Microsurgery

56 Direct Drive Endoscopy

57

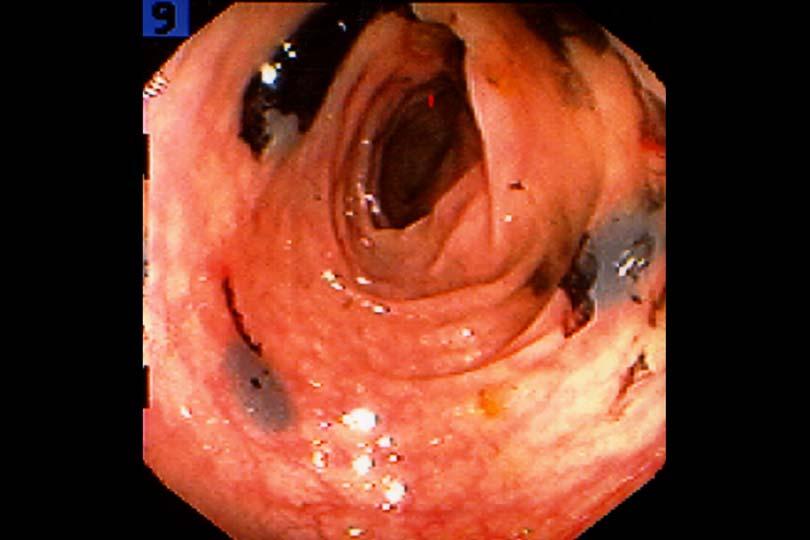
58 Location, Location, Location Ink
59 Laparoscopic Colectomy
60 Informed Consent Perforation 1 of 1000 Major hemorrhage 3 of 1000 Respiratory depression 5 of 1000 Death from complication 3 of 10,000 Multiple series of prospective studies
61 Quality Perform a Safe Exam Good Risk Assessment Preop Appropriate study Cardiac and pulmonary monitors Complete hemostasis Avoid excessive looping Be aware of depth during polepectomy Admit high risk patient and obtain labs and dx studies
62 Know when to say Uncle Order BE to complete study


63 Know how to identify a complication

64 Know how to correct a complication Perforation

65 Know how to identify a Complication

66 Splenic injury
67 Key Messages Risk Assessment FAMILIAL RISK OF CRC Familial Setting Lifetime Risk General population in U.S. 6% 1 First degree relative CRC 2-3 x 2 first degree relative 3-4 x First degree CRC < x AGA. Gastroent 2003; 124:544
68 High Risk Individuals Amsterdam Criteria (AC I,II) 3 relatives with CRC w 1 being a 1st degree relative of other 2 successive generations 1 CRC onset < 50 yrs of age AC II: substitute other HNPCC related CRC

69 Familial Colorectal Cancers HNPCC lifetime risk CRC 80-85% proximal to splenic flexure Extracolonic Cancers endometrial Ca- 60% ovarian Ca, UGI tumors GU cancers biliary and pancreatic tumors Risk of 2nd malignancy 50% in 15 years
70 Screening Recommendations Site Procedure Lower age limit Interval (years) (years) Colon Colonoscopy Endometrium/ovaries GYN exam, CA Transvaginal U/S Stomach Gastroscopy Urinary tract U/S, urine cytology Thorson AG Dis Colon Rectum 1999;42:1-9
71 Colon Cancer in HNPCC Surgeons Approach Surgical Options (+ Malignancy): 1. Total Colectomy with Ileorectal Anastomosis 2. Segmental Colectomy 3. Proctocolectomy +/- IPAA (+/- Prophylactic TAH, BSO) Cancer Prevention and Quality of Life
72 Polyposis Syndromes of the Colon Neoplastic Syndromes Familial Adenomatous Polyposis Attenuated Adenomatous Polyposis
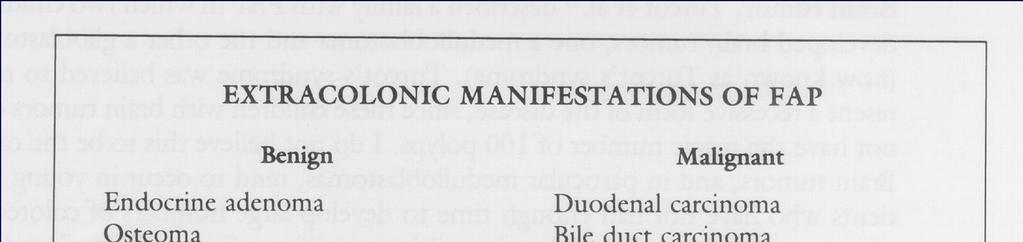
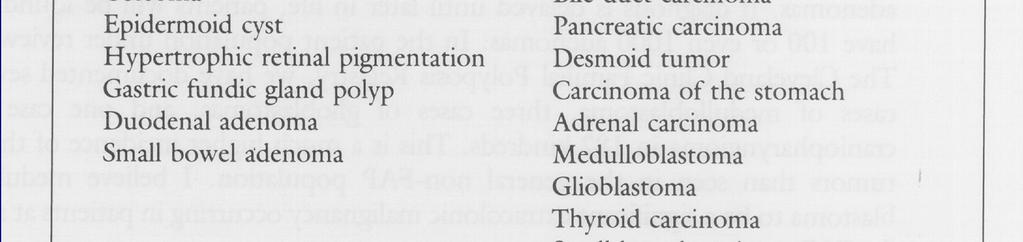
73 FAP APC (5q21) 1 in 5,000 persons > 100 CR adenomas UGI polyps, osteomas, extra teeth Extracolonic cancers: - periampullary
74 FAP-Clinical Presentation

75 FAP - Colon

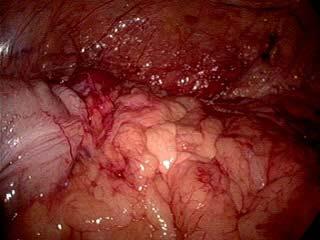
76 Gardner s Syndrome AD - subtype of FAP Additional features: - CHRPEs - desmoids, epidermoid cysts, fibromas, lipomas Extracolonic cancers: - thyroid, adrenal, HB Multifocal CHRPE Image courtesy of Dr. N. Lindor, Mayo Clinic Rochester

77 CT Scan Abdomen and Pelvis

78 Ulcerative Colitis and Crohn s Colitis

79 RISK OF COLORECTAL CANCER
80 Surveillance Colonoscopy should begin at 8-10 years duration of disease Then at 1-2 year intervals Exam full colonoscopy and 2-4 random biopsy samples at 10cm intervals along entire length of colon Eaden J et al. Gastrointestinal Endoscopy 2000

81 SURVEILLANCE BIOPSY PROTOCOL

82 PSEUDOPOLYPS

83 DALMS IN ULCERATIVE COLITIS
84 Risk of Cancer associated with Dysplasia Review of ten prospective studies Probability of cancer DALM 43% HGD 42% LGD 19% Bernstein et al. Lancet 1994
85 Surveillance Problems Questionnaire sent to GI (UK) Only 35% maintain a registry and only 49% of these were computerized Only 53% advised colectomy with HGD Only 4% for LGD Eaden J et al. Gastrointestinal Endoscopy 2000

86 Vosser
87 Vosser

88 SURGICAL OPTIONS IN ULCERATIVE COLITIS
89
90

91 Pathology Endo Path 24 hours What to do with results
92 Key Messages Communication recommendations Computerized Registry Follow up
93 nccn.org
94 Current Guidelines High Risk Average Risk Family Hx Personal Hx Age < 50 Age > 50 Heritable No Defined Syndrome Syndrome CRN IBD Screen Later Screen Now* Screen Early Screen Early Surveillance Colonoscopy Colonoscopy if Positive * Multiple options
95 Report Quality Indicators
96 Key Messages Colorectal cancer can be prevented Screening reduces mortality from CRC All persons aged 50 years or older should be screened High-risk individuals should begin screening earlier Several effective screening options are available; not screening is no longer an option
97 Key Messages Quality Study Risk Assessment Consent Safe Screening Study, dictated and photodocument Pathology and localization Communication Computerized Registry Follow up know what to do with results
98 GI Surgery and Endoscopy MISSION To Prevent colorectal cancer and its impact through education, risk assessment, screening and surveillance ENDO (3636)
Colon Cancer Screening & Surveillance. Amit Patel, MD PGY-4 GI Fellow
 Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Colon Screening in 2014 Offering Patients a Choice. Clark A Harrison MD The Nevada Colon Cancer Partnership
 Colon Screening in 2014 Offering Patients a Choice Clark A Harrison MD The Nevada Colon Cancer Partnership Objectives 1. Understand the incidence and mortality rates for CRC in the US. 2. Understand risk
Colon Screening in 2014 Offering Patients a Choice Clark A Harrison MD The Nevada Colon Cancer Partnership Objectives 1. Understand the incidence and mortality rates for CRC in the US. 2. Understand risk
2. Describe pros/cons of screening interventions (including colonoscopy, CT colography, fecal tests)
") Learning Objectives 1. Review principles of colon adenoma/cancer biology that permit successful prevention regimes 2. Describe pros/cons of screening interventions (including colonoscopy, CT colography,
Learning Objectives 1. Review principles of colon adenoma/cancer biology that permit successful prevention regimes 2. Describe pros/cons of screening interventions (including colonoscopy, CT colography,
Colorectal Neoplasia. Dr. Smita Devani MBChB, MRCP. Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi
 Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
EARLY DETECTION OF COLORECTAL CANCER. Epidemiology of CRC
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Screening & Surveillance Guidelines
 Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING
 CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING This guideline is designed to assist practitioners by providing the framework for colorectal cancer (CRC) screening, and is not intended to replace
CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING This guideline is designed to assist practitioners by providing the framework for colorectal cancer (CRC) screening, and is not intended to replace
Quality Measures In Colonoscopy: Why Should I Care?
 Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
Colorectal Cancer Screening: A Clinical Update
 11:05 11:45am Colorectal Cancer Screening: A Clinical Update SPEAKER Kevin A. Ghassemi, MD Presenter Disclosure Information The following relationships exist related to this presentation: Kevin A. Ghassemi,
11:05 11:45am Colorectal Cancer Screening: A Clinical Update SPEAKER Kevin A. Ghassemi, MD Presenter Disclosure Information The following relationships exist related to this presentation: Kevin A. Ghassemi,
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population
 Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
CRC Risk Factors. U.S. Adherence Rates Cancer Screening. Genetic Model of Colorectal Cancer. Epidemiology and Clinical Consequences of CRC
 10:45 11:45 am Guide to Colorectal Cancer Screening SPEAKER Howard Manten M.D. Presenter Disclosure Information The following relationships exist related to this presentation: Howard Manten MD: No financial
10:45 11:45 am Guide to Colorectal Cancer Screening SPEAKER Howard Manten M.D. Presenter Disclosure Information The following relationships exist related to this presentation: Howard Manten MD: No financial
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Colon Cancer Screening and Surveillance. Louis V. Antignano, M.D. Wilson Gastroenterology October 11, 2011
 Colon Cancer Screening and Surveillance Louis V. Antignano, M.D. Wilson Gastroenterology October 11, 2011 Colorectal Cancer Preventable cancer Number 2 cancer killer in the USA Often curable if detected
Colon Cancer Screening and Surveillance Louis V. Antignano, M.D. Wilson Gastroenterology October 11, 2011 Colorectal Cancer Preventable cancer Number 2 cancer killer in the USA Often curable if detected
Familial Adenomatous Polyposis
 Familial Adenomatous Polyposis 1 in 10,000 incidence 100 s to 1000 s of colonic adenomas by teens Cancer risk: colon, gastric, duodenum (periampulla), small bowel, pancreas, papillary thyroid, childhood
Familial Adenomatous Polyposis 1 in 10,000 incidence 100 s to 1000 s of colonic adenomas by teens Cancer risk: colon, gastric, duodenum (periampulla), small bowel, pancreas, papillary thyroid, childhood
GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS. Family Health Clinical Genetics. Clinical Genetics department
 GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS Full Title of Guideline: Author (include email and role): Division & Speciality: GUIDELINES FOR THE GENETIC MANAGEMENT OF A FAMILY
GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS Full Title of Guideline: Author (include email and role): Division & Speciality: GUIDELINES FOR THE GENETIC MANAGEMENT OF A FAMILY
CENTERS FOR DISEASE CONTROL AND PREVENTION CENTERS FOR DISEASE CONTROL AND PREVENTION. Incidence Male. Incidence Female.
 A Call to Action: Prevention and Early Detection of Colorectal Cancer (CRC) 5 Key Messages Screening reduces mortality from CRC All persons aged 50 years and older should begin regular screening High-risk
A Call to Action: Prevention and Early Detection of Colorectal Cancer (CRC) 5 Key Messages Screening reduces mortality from CRC All persons aged 50 years and older should begin regular screening High-risk
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Colorectal Cancer: Screening & Surveillance
 Objectives Colorectal Cancer: Screening & Surveillance Chanda K. Ho, MD MPH Advances in Internal Medicine Brief overview epidemiology and pathogenesis of colorectal cancer (CRC) To review screening modalities
Objectives Colorectal Cancer: Screening & Surveillance Chanda K. Ho, MD MPH Advances in Internal Medicine Brief overview epidemiology and pathogenesis of colorectal cancer (CRC) To review screening modalities
Measure #425: Photodocumentation of Cecal Intubation National Quality Strategy Domain: Effective Clinical Care
 Measure #425: Photodocumentation of Cecal Intubation National Quality Strategy Domain: Effective Clinical Care 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: The
Measure #425: Photodocumentation of Cecal Intubation National Quality Strategy Domain: Effective Clinical Care 2017 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process DESCRIPTION: The
11/9/2015 OUTLINE. Quality Indicators for the Doctor Performing Screening Colonoscopy: What you should expect from your Endoscopist
 Quality Indicators for the Doctor Performing Screening Colonoscopy: What you should expect from your Endoscopist Anil K Sharma MD FACP Professor of Clinical Medicine, University of Rochester Chief of Gastroenterology,
Quality Indicators for the Doctor Performing Screening Colonoscopy: What you should expect from your Endoscopist Anil K Sharma MD FACP Professor of Clinical Medicine, University of Rochester Chief of Gastroenterology,
Colorectal Cancer Screening: Cost-Effectiveness and Adverse events October, 2005
 Colorectal Cancer Screening: Cost-Effectiveness and Adverse events October, 2005 David Lieberman MD Chief, Division of Gastroenterology Oregon Health and Science University Portland VAMC Portland, Oregon
Colorectal Cancer Screening: Cost-Effectiveness and Adverse events October, 2005 David Lieberman MD Chief, Division of Gastroenterology Oregon Health and Science University Portland VAMC Portland, Oregon
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Pathology reports, related operative reports and consult letters must be provided with a request for assessment.
 Page 1 of 6 Polyposis Syndromes Inherited risk for colorectal cancer is associated with a number of polyposis syndromes (genes), some of which are well-defined and others are less common. Identification
Page 1 of 6 Polyposis Syndromes Inherited risk for colorectal cancer is associated with a number of polyposis syndromes (genes), some of which are well-defined and others are less common. Identification
Objectives. Definitions. Colorectal Cancer Screening 5/8/2018. Payam Afshar, MS, MD Kaiser Permanente, San Diego. Colorectal cancer background
 Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Updates in Colorectal Cancer Screening & Prevention
 Updates in Colorectal Cancer Screening & Prevention Swati G. Patel, MD MS Assistant Professor of Medicine Division of Gastroenterology & Hepatology Gastrointestinal Cancer Risk and Prevention Clinic University
Updates in Colorectal Cancer Screening & Prevention Swati G. Patel, MD MS Assistant Professor of Medicine Division of Gastroenterology & Hepatology Gastrointestinal Cancer Risk and Prevention Clinic University
PENETRANCE ACTIONABILITY SIGNIFICANCE/BURDEN OF DISEASE NEXT STEPS. YES ( 1 of above) YES (Proceed to Stage II)
 YES (Proceed to Stage II)") Stage I: Binning Dashboard GENE/GENE PANEL: APC ACTIONABILITY 1. Is there a qualifying resource, such as a practice guideline or systematic review, for the genetic condition? 2. Does the practice guideline
Stage I: Binning Dashboard GENE/GENE PANEL: APC ACTIONABILITY 1. Is there a qualifying resource, such as a practice guideline or systematic review, for the genetic condition? 2. Does the practice guideline
Colorectal adenocarcinoma leading cancer in developed countries In US, annual deaths due to colorectal adenocarcinoma 57,000.
 Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Financial Disclosers
 Slide 1 Colorectal Cancer Screening Jason Hemming, MD NESGNA November 15, 2014 Slide 2 Bio Slide 3 Financial Disclosers I have no actual or potential conflict of interest relation to this presentation
Slide 1 Colorectal Cancer Screening Jason Hemming, MD NESGNA November 15, 2014 Slide 2 Bio Slide 3 Financial Disclosers I have no actual or potential conflict of interest relation to this presentation
General and Colonoscopy Data Collection Form
 Identifier: Sociodemographic Information Type: Zip Code: Inpatient Outpatient Birth Date: m m d d y y y y Gender: Height: (inches) Male Female Ethnicity: Weight: (pounds) African American White, Non-Hispanic
Identifier: Sociodemographic Information Type: Zip Code: Inpatient Outpatient Birth Date: m m d d y y y y Gender: Height: (inches) Male Female Ethnicity: Weight: (pounds) African American White, Non-Hispanic
Wellness Along the Cancer Journey: Healthy Habits and Cancer Screening Revised October 2015 Chapter 7: Cancer Screening and Early Detection of Cancer
 Wellness Along the Cancer Journey: Healthy Habits and Cancer Screening Revised October 2015 Chapter 7: Cancer Screening and Early Detection of Cancer Healthy Habits and Cancer Screening Rev 10.20.15 Page
Wellness Along the Cancer Journey: Healthy Habits and Cancer Screening Revised October 2015 Chapter 7: Cancer Screening and Early Detection of Cancer Healthy Habits and Cancer Screening Rev 10.20.15 Page
David P. Ryan, M.D. Clinical Director, MGH Cancer Center Chief, Hematology-Oncology, MGH
 Colon Cancer 2015 David P. Ryan, M.D. Clinical Director, MGH Cancer Center Chief, Hematology-Oncology, MGH Colon Cancer Case presentation 72yo woman presented 1/03 abd discomfort and nausea Found to have
Colon Cancer 2015 David P. Ryan, M.D. Clinical Director, MGH Cancer Center Chief, Hematology-Oncology, MGH Colon Cancer Case presentation 72yo woman presented 1/03 abd discomfort and nausea Found to have
Measure #425: Photodocumentation of Cecal Intubation National Quality Strategy Domain: Effective Clinical Care
 Measure #425: Photodocumentation of Cecal Intubation National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION: The rate of screening
Measure #425: Photodocumentation of Cecal Intubation National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION: The rate of screening
Colorectal cancer screening: Is total prevention possible?
 Just the facts colorectal cancer Colorectal cancer screening: Is total prevention possible? Jeffrey Fox, MD, MPH Concepts and Controversies 2011 2010 NCI estimates for US: 142, 570 new CRC diagnoses 51,370
Just the facts colorectal cancer Colorectal cancer screening: Is total prevention possible? Jeffrey Fox, MD, MPH Concepts and Controversies 2011 2010 NCI estimates for US: 142, 570 new CRC diagnoses 51,370
CANCER SCREENING. Er Chaozer Department of General Medicine, Tan Tock Seng Hospital
 CANCER SCREENING Er Chaozer Department of General Medicine, Tan Tock Seng Hospital Introduction Screening average risk patients Benefits and harms from screening Early cancer detection early treatment
CANCER SCREENING Er Chaozer Department of General Medicine, Tan Tock Seng Hospital Introduction Screening average risk patients Benefits and harms from screening Early cancer detection early treatment
Classification of polyposis syndromes two major groups. Adenomatous polyposis syndromes. Hamartomatous polyposis syndromes
 Hereditary polyposis syndromes Classification of polyposis syndromes two major groups adenomatous and non-adenomatous polyposis syndromes Adenomatous polyposis syndromes Familial adenomatous polyposis(fap)
Hereditary polyposis syndromes Classification of polyposis syndromes two major groups adenomatous and non-adenomatous polyposis syndromes Adenomatous polyposis syndromes Familial adenomatous polyposis(fap)
Clinical UM Guideline
 Subject: Guideline #: Current Effective Date: 06/28/2016 Status: Revised Last Review Date: 05/05/2016 Description This document addresses colonoscopy, an endoscopic procedure which allows direct visual
Subject: Guideline #: Current Effective Date: 06/28/2016 Status: Revised Last Review Date: 05/05/2016 Description This document addresses colonoscopy, an endoscopic procedure which allows direct visual
COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University
 Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University") COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University 1. I am a surgeon; of course I have nothing to disclose.
COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University 1. I am a surgeon; of course I have nothing to disclose.
FREQUENTLY ASKED QUESTIONS
 FREQUENTLY ASKED QUESTIONS What is CRC? CRC (CRC) is cancer of the large intestine (colon), the lower part of the digestive system. Rectal cancer is cancer of the last several inches of the colon. Together,
FREQUENTLY ASKED QUESTIONS What is CRC? CRC (CRC) is cancer of the large intestine (colon), the lower part of the digestive system. Rectal cancer is cancer of the last several inches of the colon. Together,
LIST OF ABBREVIATIONS
 Gastroenter oenterology 2005 Royal College of Physicians of Edinburgh Screening and surveillance for upper and lower gastrointestinal cancer JN Plevris Consultant Gastroenterologist and Honorary Senior
Gastroenter oenterology 2005 Royal College of Physicians of Edinburgh Screening and surveillance for upper and lower gastrointestinal cancer JN Plevris Consultant Gastroenterologist and Honorary Senior
Quality ID #439: Age Appropriate Screening Colonoscopy National Quality Strategy Domain: Efficiency and Cost Reduction
 Quality ID #439: Age Appropriate Screening Colonoscopy National Quality Strategy Domain: Efficiency and Cost Reduction 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Efficiency DESCRIPTION:
Quality ID #439: Age Appropriate Screening Colonoscopy National Quality Strategy Domain: Efficiency and Cost Reduction 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Efficiency DESCRIPTION:
A Trip Through the GI Tract: Common GI Diseases and Complaints. Jennifer Curtis, MD
 A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
Historical. Note: The parenthetical numbers in the Clinical Indications section refer to the source documents cited in the References Section below.
 Clinical UM Guideline Subject: Colonoscopy Guideline #: CG-SURG-01 Current Effective Date: 01/21/2015 Status: Revised Last Review Date: 05/15/2014 Description Colonoscopy describes the direct visual inspection
Clinical UM Guideline Subject: Colonoscopy Guideline #: CG-SURG-01 Current Effective Date: 01/21/2015 Status: Revised Last Review Date: 05/15/2014 Description Colonoscopy describes the direct visual inspection
Guidelines for Breast, Cervical and Colorectal Cancer Screening
 Guidelines for Breast, Cervical and Colorectal Cancer Screening Your recommendation counts. Talk to your patients about screening for cancer. CancerCare Manitoba provides organized, population-based screening
Guidelines for Breast, Cervical and Colorectal Cancer Screening Your recommendation counts. Talk to your patients about screening for cancer. CancerCare Manitoba provides organized, population-based screening
Colorectal Cancer Screening. Daniel C. Chung, MD GI Unit and GI Cancer Genetics Service Massachusetts General Hospital
 Colorectal Cancer Screening Daniel C. Chung, MD GI Unit and GI Cancer Genetics Service Massachusetts General Hospital March, 2018 CRC Epidemiology 4th most common malignancy in US (136,000 cases/yr) 2nd
Colorectal Cancer Screening Daniel C. Chung, MD GI Unit and GI Cancer Genetics Service Massachusetts General Hospital March, 2018 CRC Epidemiology 4th most common malignancy in US (136,000 cases/yr) 2nd
Colorectal Cancer Screening
 Recommendations from the U.S. Multi-Society Task Force on Colorectal Cancer Colorectal Cancer Screening Rex DK, Boland CR, Dominitz JA, Giardiello FM, Johnson DA, Kaltenbach T, Levin TR, Lieberman D, Robertson
Recommendations from the U.S. Multi-Society Task Force on Colorectal Cancer Colorectal Cancer Screening Rex DK, Boland CR, Dominitz JA, Giardiello FM, Johnson DA, Kaltenbach T, Levin TR, Lieberman D, Robertson
The New Grade A: USPSTF Updated Colorectal Cancer Screening Guidelines, What does it all mean?
 The New Grade A: USPSTF Updated Colorectal Cancer Screening Guidelines, What does it all mean? Robert A. Smith, PhD Cancer Control, Department of Prevention and Early Detection American Cancer Society
The New Grade A: USPSTF Updated Colorectal Cancer Screening Guidelines, What does it all mean? Robert A. Smith, PhD Cancer Control, Department of Prevention and Early Detection American Cancer Society
Risk of Colorectal Cancer (CRC) Hereditary Syndromes in GI Cancer GENETIC MALPRACTICE
 Hereditary Syndromes in GI Cancer GENETIC MALPRACTICE") Identifying the Patient at Risk for an Inherited Syndrome Sapna Syngal, MD, MPH, FACG Director, Gastroenterology Director, Familial GI Program Dana-Farber/Brigham and Women s Cancer Center Associate Professor
Identifying the Patient at Risk for an Inherited Syndrome Sapna Syngal, MD, MPH, FACG Director, Gastroenterology Director, Familial GI Program Dana-Farber/Brigham and Women s Cancer Center Associate Professor
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Colorectal cancer: colonoscopic surveillance for prevention of colorectal cancer in patients with ulcerative colitis, Crohn
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Colorectal cancer: colonoscopic surveillance for prevention of colorectal cancer in patients with ulcerative colitis, Crohn
Colorectal Cancer Screening. Paul Berg MD
 Colorectal Cancer Screening Paul Berg MD What is clinical integration? AMA Definition The means to facilitate the coordination of patient care across conditions, providers, settings, and time in order
Colorectal Cancer Screening Paul Berg MD What is clinical integration? AMA Definition The means to facilitate the coordination of patient care across conditions, providers, settings, and time in order
Colorectal Cancer Screening What are my options?
 069-Colorectal cancer (Rosen) 1/23/04 12:59 PM Page 69 What are my options? Wayne Rosen, MD, FRCSC As presented at the 37th Annual Mackid Symposium: Cancer Care in the Community (May 22, 2003) There are
069-Colorectal cancer (Rosen) 1/23/04 12:59 PM Page 69 What are my options? Wayne Rosen, MD, FRCSC As presented at the 37th Annual Mackid Symposium: Cancer Care in the Community (May 22, 2003) There are
Colon Cancer Screening. Layth Al-Jashaami, MD GI Fellow, PGY 4
 Colon Cancer Screening Layth Al-Jashaami, MD GI Fellow, PGY 4 -Colorectal cancer (CRC) is a common and lethal cancer. -It has the highest incidence among GI cancers in the US, estimated to be newly diagnosed
Colon Cancer Screening Layth Al-Jashaami, MD GI Fellow, PGY 4 -Colorectal cancer (CRC) is a common and lethal cancer. -It has the highest incidence among GI cancers in the US, estimated to be newly diagnosed
This is the portion of the intestine which lies between the small intestine and the outlet (Anus).
.") THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
Dysplasia 4/19/2017. How do I practice Chromoendoscopy for Surveillance of Colitis? SCENIC: Polypoid Dysplasia in UC. Background
 SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
ACG Clinical Guideline: Colorectal Cancer Screening
 ACG Clinical Guideline: Colorectal Cancer Screening Douglas K. Rex, MD, FACG 1, David A. Johnson, MD, FACG 2, Joseph C. Anderson, MD 3, Phillip S. Schoenfeld, MD, MSEd, MSc (Epi), FACG 4, Carol A. Burke,
ACG Clinical Guideline: Colorectal Cancer Screening Douglas K. Rex, MD, FACG 1, David A. Johnson, MD, FACG 2, Joseph C. Anderson, MD 3, Phillip S. Schoenfeld, MD, MSEd, MSc (Epi), FACG 4, Carol A. Burke,
GI CANCER SCREENING- Is It Worth It? Sylvia M. Oats, MSN, APRN, ANP-BC Susan H. Miedecke, MSN, APRN, FNP-BC Gastroenterology Clinic of Acadiana
 GI CANCER SCREENING- Is It Worth It? Sylvia M. Oats, MSN, APRN, ANP-BC Susan H. Miedecke, MSN, APRN, FNP-BC Gastroenterology Clinic of Acadiana Life is a sexually transmitted disease, and the mortality
GI CANCER SCREENING- Is It Worth It? Sylvia M. Oats, MSN, APRN, ANP-BC Susan H. Miedecke, MSN, APRN, FNP-BC Gastroenterology Clinic of Acadiana Life is a sexually transmitted disease, and the mortality
What Questions Should You Ask?
 ? Your Doctor Has Ordered a Colonoscopy. What Questions Should You sk? From the merican College of Gastroenterology www.acg.gi.org Normal colon Is the doctor performing your colonoscopy a Gastroenterologist?
? Your Doctor Has Ordered a Colonoscopy. What Questions Should You sk? From the merican College of Gastroenterology www.acg.gi.org Normal colon Is the doctor performing your colonoscopy a Gastroenterologist?
Colorectal Cancer Screening and Risk Assessment Workflow. Documentation Guide for Health Center NextGen Users
 Colorectal Cancer Screening and Risk Assessment Workflow Documentation Guide for Health Center NextGen Users Colorectal Cancer Screening and Risk Assessment Workflow and Documentation Guide for Health
Colorectal Cancer Screening and Risk Assessment Workflow Documentation Guide for Health Center NextGen Users Colorectal Cancer Screening and Risk Assessment Workflow and Documentation Guide for Health
Prevention of Bowel Cancer: which patients do I send for colonoscopy?
 Prevention of Bowel Cancer: which patients do I send for colonoscopy? Dr Chris Groves Consultant Gastroenterologist and Honorary Senior Lecturer St George s Hospital and Medical School Director, SW London
Prevention of Bowel Cancer: which patients do I send for colonoscopy? Dr Chris Groves Consultant Gastroenterologist and Honorary Senior Lecturer St George s Hospital and Medical School Director, SW London
Summary. Cezary ŁozińskiABDF, Witold KyclerABCDEF. Rep Pract Oncol Radiother, 2007; 12(4):
:") Rep Pract Oncol Radiother, 2007; 12(4): 201-206 Original Paper Received: 2006.12.19 Accepted: 2007.04.02 Published: 2007.08.31 Authors Contribution: A Study Design B Data Collection C Statistical Analysis
Rep Pract Oncol Radiother, 2007; 12(4): 201-206 Original Paper Received: 2006.12.19 Accepted: 2007.04.02 Published: 2007.08.31 Authors Contribution: A Study Design B Data Collection C Statistical Analysis
Colorectal Cancer Screening
 Scan for mobile link. Colorectal Cancer Screening What is colorectal cancer screening? Screening examinations are tests performed to identify disease in individuals who lack any signs or symptoms. The
Scan for mobile link. Colorectal Cancer Screening What is colorectal cancer screening? Screening examinations are tests performed to identify disease in individuals who lack any signs or symptoms. The
Navigators Lead the Way
 RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
Content. Diagnostic approach and clinical management of Lynch Syndrome: guidelines. Terminology. Identification of Lynch Syndrome
 of Lynch Syndrome: guidelines 17/03/2009 Content Terminology Lynch Syndrome Presumed Lynch Syndrome Familial Colorectal Cancer Identification of Lynch Syndrome Amsterdam II criteria Revised Bethesda Guidelines
of Lynch Syndrome: guidelines 17/03/2009 Content Terminology Lynch Syndrome Presumed Lynch Syndrome Familial Colorectal Cancer Identification of Lynch Syndrome Amsterdam II criteria Revised Bethesda Guidelines
Colorectal Cancer Screening in Ohio CHCs. Ohio Association of Community Health Centers
 Colorectal Cancer Screening in Ohio CHCs Ohio Association of Community Health Centers 2 1/29/2015 Your Speakers Dr. Ted Wymyslo Ashley Ballard Randy Runyon 3 1/29/2015 Facts 3 rd most common cancer in
Colorectal Cancer Screening in Ohio CHCs Ohio Association of Community Health Centers 2 1/29/2015 Your Speakers Dr. Ted Wymyslo Ashley Ballard Randy Runyon 3 1/29/2015 Facts 3 rd most common cancer in
Joint Session with ACOFP and Cancer Treatment Centers of America (CTCA): Cancer Screening: Consensus & Controversies. Ashish Sangal, M.D.
: Cancer Screening: Consensus & Controversies. Ashish Sangal, M.D.") Joint Session with ACOFP and Cancer Treatment Centers of America (CTCA): Cancer Screening: Consensus & Controversies Ashish Sangal, M.D. Cancer Screening: Consensus & Controversies Ashish Sangal, MD Director,
Joint Session with ACOFP and Cancer Treatment Centers of America (CTCA): Cancer Screening: Consensus & Controversies Ashish Sangal, M.D. Cancer Screening: Consensus & Controversies Ashish Sangal, MD Director,
Colorectal Cancer in 2006: New Developments
 James J. Stark, MD Colorectal Cancer in 2006: New Developments Melissa Bennett, MS, CGC Myriad Genetic Laboratories Thomas Duntemann,, MD Ray Ramirez, Jr., MD Hereditary Colon Cancer and Genetic Testing
James J. Stark, MD Colorectal Cancer in 2006: New Developments Melissa Bennett, MS, CGC Myriad Genetic Laboratories Thomas Duntemann,, MD Ray Ramirez, Jr., MD Hereditary Colon Cancer and Genetic Testing
For identification, support and follow up related to Familial Gastrointestinal Cancer conditions. South Island Cancer Nurses Network September 2013
 For identification, support and follow up related to Familial Gastrointestinal Cancer conditions South Island Cancer Nurses Network September 2013 Who are we? Specialist multidisciplinary team: Nurse coordinators,
For identification, support and follow up related to Familial Gastrointestinal Cancer conditions South Island Cancer Nurses Network September 2013 Who are we? Specialist multidisciplinary team: Nurse coordinators,
GENERAL COLORECTAL CANCER INFORMATION. What is colorectal cancer?
 GENERAL COLORECTAL CANCER INFORMATION What is colorectal cancer? Colorectal cancer is cancer that develops in the colon or the rectum. The colon and rectum are parts of the digestive system, which is also
GENERAL COLORECTAL CANCER INFORMATION What is colorectal cancer? Colorectal cancer is cancer that develops in the colon or the rectum. The colon and rectum are parts of the digestive system, which is also
Cancer Genomics 101. BCCCP 2015 Annual Meeting
 Cancer Genomics 101 BCCCP 2015 Annual Meeting Objectives Identify red flags in a person s personal and family medical history that indicate a potential inherited susceptibility to cancer Develop a systematic
Cancer Genomics 101 BCCCP 2015 Annual Meeting Objectives Identify red flags in a person s personal and family medical history that indicate a potential inherited susceptibility to cancer Develop a systematic
10/25/2011 OBJECTIVES Cancer Screening in the United States, 2011 A Review of Current American Cancer Society Guidelines and Issues in Cancer Screenin
 OBJECTIVES Cancer Screening in the United States, 2011 A Review of Current American Cancer Society Guidelines and Issues in Cancer Screening Kathy Gray, DNP, CRNP, FNP-BC Cancer Screenings and Guidelines
OBJECTIVES Cancer Screening in the United States, 2011 A Review of Current American Cancer Society Guidelines and Issues in Cancer Screening Kathy Gray, DNP, CRNP, FNP-BC Cancer Screenings and Guidelines
Bowel cancer screening and prevention
 Bowel cancer screening and prevention Cancer Incidence and Mortality Victoria 2012 Number 6000 5000 4000 3000 2000 Incidences = 29,387 Mortality = 10,780 Incidence Mortality 1000 0 Prostate Breast Bowel
Bowel cancer screening and prevention Cancer Incidence and Mortality Victoria 2012 Number 6000 5000 4000 3000 2000 Incidences = 29,387 Mortality = 10,780 Incidence Mortality 1000 0 Prostate Breast Bowel
Colonoscopy MM /01/2010. PPO; HMO; QUEST Integration 10/01/2017 Section: Surgery Place(s) of Service: Outpatient
 of Service: Outpatient") Colonoscopy Policy Number: Original Effective Date: MM.12.003 12/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration 10/01/2017 Section: Surgery Place(s) of Service: Outpatient
Colonoscopy Policy Number: Original Effective Date: MM.12.003 12/01/2010 Line(s) of Business: Current Effective Date: PPO; HMO; QUEST Integration 10/01/2017 Section: Surgery Place(s) of Service: Outpatient
Colon, or Colorectal, Cancer Information
 Colon, or Colorectal, Cancer Information Definition Colon, or colorectal, cancer is cancer that starts in the large intestine (colon) or the rectum (end of the colon). Other types of cancer can affect
Colon, or Colorectal, Cancer Information Definition Colon, or colorectal, cancer is cancer that starts in the large intestine (colon) or the rectum (end of the colon). Other types of cancer can affect
Colorectal Cancer Screening and Surveillance
 Medical Coverage Policy Effective Date...10/15/2017 Next Review Date...10/15/2018 Coverage Policy Number... 0148 Colorectal Cancer Screening and Surveillance Table of Contents Related Coverage Resources
Medical Coverage Policy Effective Date...10/15/2017 Next Review Date...10/15/2018 Coverage Policy Number... 0148 Colorectal Cancer Screening and Surveillance Table of Contents Related Coverage Resources
Early detection and screening for colorectal neoplasia
 Early detection and screening for colorectal neoplasia Robert S. Bresalier Department of Gastroenterology, Hepatology and Nutrition. The University of Texas. MD Anderson Cancer Center. Houston, Texas U.S.A.
Early detection and screening for colorectal neoplasia Robert S. Bresalier Department of Gastroenterology, Hepatology and Nutrition. The University of Texas. MD Anderson Cancer Center. Houston, Texas U.S.A.
How to start a screening Program? WEO Colorectal Cancer Screening Committee Meeting Brasilia Nov R. Sáenz, FACG,FASGE
 How to start a screening Program? WEO Colorectal Cancer Screening Committee Meeting Brasilia Nov 11 2017 R. Sáenz, FACG,FASGE Wheel has been discovered already Policy Planning Thanks to GBD Big Data CRC
How to start a screening Program? WEO Colorectal Cancer Screening Committee Meeting Brasilia Nov 11 2017 R. Sáenz, FACG,FASGE Wheel has been discovered already Policy Planning Thanks to GBD Big Data CRC
Colorectal Cancer Screening and Surveillance
 1 Colorectal Cancer Screening and Surveillance Jeffrey Lee MD, MAS Assistant Clinical Professor of Medicine University of California, San Francisco jeff.lee@ucsf.edu Objectives Review the various colorectal
1 Colorectal Cancer Screening and Surveillance Jeffrey Lee MD, MAS Assistant Clinical Professor of Medicine University of California, San Francisco jeff.lee@ucsf.edu Objectives Review the various colorectal
Endoscopic techniques for surveillance and treatment of FAP
 Endoscopic techniques for surveillance and treatment of FAP Evelien Dekker MD PhD Department of Gastroenterology & Hepatology Academic Medical Center Amsterdam The Netherlands FAP: endoscopic surveillance
Endoscopic techniques for surveillance and treatment of FAP Evelien Dekker MD PhD Department of Gastroenterology & Hepatology Academic Medical Center Amsterdam The Netherlands FAP: endoscopic surveillance
Detection of Colorectal Neoplasms in Asymptomatic Patients
 Detection of Colorectal Neoplasms in Asymptomatic Patients Scope This guideline provides recommendations for the detection of colorectal cancer and adenomas in asymptomatic patients. These recommendations
Detection of Colorectal Neoplasms in Asymptomatic Patients Scope This guideline provides recommendations for the detection of colorectal cancer and adenomas in asymptomatic patients. These recommendations
Improving Outcomes in Colorectal Cancer: The Science of Screening. Colorectal Cancer (CRC)
") Improving Outcomes in Colorectal Cancer: The Science of Screening Tennessee Primary Care Association October 23, 2014 Durado Brooks, MD, MPH Director, Prostate and Colorectal Cancers Colorectal Cancer
Improving Outcomes in Colorectal Cancer: The Science of Screening Tennessee Primary Care Association October 23, 2014 Durado Brooks, MD, MPH Director, Prostate and Colorectal Cancers Colorectal Cancer
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
1101 First Colonial Road, Suite 300, Virginia Beach, VA Phone (757) Fax (757)
 Fax (757)") 1101 First Colonial Road, Suite 300, Virginia Beach, VA 23454 www.vbgastro.com Phone (757) 481-4817 Fax (757) 481-7138 1150 Glen Mitchell Drive, Suite 208 Virginia Beach, VA 23456 www.vbgastro.com Phone
1101 First Colonial Road, Suite 300, Virginia Beach, VA 23454 www.vbgastro.com Phone (757) 481-4817 Fax (757) 481-7138 1150 Glen Mitchell Drive, Suite 208 Virginia Beach, VA 23456 www.vbgastro.com Phone
Page 1. Selected Controversies. Cancer Screening! Selected Controversies. Breast Cancer Screening. ! Using Best Evidence to Guide Practice!
 Cancer Screening!! Using Best Evidence to Guide Practice! Judith M.E. Walsh, MD, MPH! Division of General Internal Medicine! Womenʼs Health Center of Excellence University of California, San Francisco!
Cancer Screening!! Using Best Evidence to Guide Practice! Judith M.E. Walsh, MD, MPH! Division of General Internal Medicine! Womenʼs Health Center of Excellence University of California, San Francisco!
Mr Chris Wakeman. General Surgeon University of Otago, Christchurch. 12:15-12:40 Management of Colorectal Cancer
 Mr Chris Wakeman General Surgeon University of Otago, Christchurch 12:15-12:40 Management of Colorectal Cancer Bowel cancer Chris Wakeman Colorectal Surgeon Christchurch Sam Simon (Simpsons) Elizabeth
Mr Chris Wakeman General Surgeon University of Otago, Christchurch 12:15-12:40 Management of Colorectal Cancer Bowel cancer Chris Wakeman Colorectal Surgeon Christchurch Sam Simon (Simpsons) Elizabeth
DIGESTIVE SYSTEM SURGICAL PROCEDURES May 1, 2015 INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 Asst Surg Anae") ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
Wellness Along the Cancer Journey: Cancer Types Revised October 2015 Chapter 4: Colorectal Cancer Overview
 Wellness Along the Cancer Journey: Cancer Types Revised October 2015 Chapter 4: Colorectal Cancer Overview Cancer Types Rev. 10.20.15 Page 35 Colorectal Cancer Overview Group Discussion True False Not
Wellness Along the Cancer Journey: Cancer Types Revised October 2015 Chapter 4: Colorectal Cancer Overview Cancer Types Rev. 10.20.15 Page 35 Colorectal Cancer Overview Group Discussion True False Not
removal of adenomatous polyps detects important effectively as follow-up colonoscopy after both constitute a low-risk Patients with 1 or 2
 Supplementary Table 1. Study Characteristics Author, yr Design Winawer et al., 6 1993 National Polyp Study Jorgensen et al., 9 1995 Funen Adenoma Follow-up Study USA Multi-center, RCT for timing of surveillance
Supplementary Table 1. Study Characteristics Author, yr Design Winawer et al., 6 1993 National Polyp Study Jorgensen et al., 9 1995 Funen Adenoma Follow-up Study USA Multi-center, RCT for timing of surveillance
2012 update. Bowel Cancer. Information for people at increased risk of bowel cancer. Published by the New Zealand Guidelines Group
 2012 update Bowel Cancer Information for people at increased risk of bowel cancer Published by the New Zealand Guidelines Group i Contents Introduction 1 The bowel 1 Bowel cancer 3 What are the symptoms
2012 update Bowel Cancer Information for people at increased risk of bowel cancer Published by the New Zealand Guidelines Group i Contents Introduction 1 The bowel 1 Bowel cancer 3 What are the symptoms
Hereditary Colorectal Cancer Syndromes Miguel A. Rodriguez-Bigas, MD
 Hereditary Colorectal Cancer Syndromes Miguel A. Rodriguez-Bigas, MD Living Beyond Cancer A-Z January 12,2019 Hereditary CRC Syndromes Objectives are to discuss the : Most common Hereditary CRC syndromes
Hereditary Colorectal Cancer Syndromes Miguel A. Rodriguez-Bigas, MD Living Beyond Cancer A-Z January 12,2019 Hereditary CRC Syndromes Objectives are to discuss the : Most common Hereditary CRC syndromes
FECAL OCCULT BLOOD TEST
 MEDICAL POLICY For use with the UnitedHealthcare Laboratory Benefit Management Program, administered by BeaconLBS FECAL OCCULT BLOOD TEST Policy Number: CMP - 023 Effective Date: January 1, 2018 Table
MEDICAL POLICY For use with the UnitedHealthcare Laboratory Benefit Management Program, administered by BeaconLBS FECAL OCCULT BLOOD TEST Policy Number: CMP - 023 Effective Date: January 1, 2018 Table
CASE DISCUSSION: The Patient with Dysplasia: Surgery or Active Surveillance? Noa Krugliak Cleveland, MD David T. Rubin, MD
 CASE DISCUSSION: The Patient with Dysplasia: Surgery or Active Surveillance? Noa Krugliak Cleveland, MD David T. Rubin, MD Disclosure Statement NKC: No relevant conflicts to disclose. DTR: No relevant
CASE DISCUSSION: The Patient with Dysplasia: Surgery or Active Surveillance? Noa Krugliak Cleveland, MD David T. Rubin, MD Disclosure Statement NKC: No relevant conflicts to disclose. DTR: No relevant
Structured Follow-Up after Colorectal Cancer Resection: Overrated. R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007
 Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci. Colon polyps. Colorectal cancer
 Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
GUIDANCE ON THE INDICATIONS FOR DIAGNOSTIC UPPER GI ENDOSCOPY, FLEXIBLE SIGMOIDOSCOPY AND COLONOSCOPY
 Position Statement produced by BSG, AUGIS and ACPGBI GUIDANCE ON THE INDICATIONS FOR DIAGNOSTIC UPPER GI ENDOSCOPY, FLEXIBLE SIGMOIDOSCOPY AND COLONOSCOPY Introduction In 2011 the Independent Practice
Position Statement produced by BSG, AUGIS and ACPGBI GUIDANCE ON THE INDICATIONS FOR DIAGNOSTIC UPPER GI ENDOSCOPY, FLEXIBLE SIGMOIDOSCOPY AND COLONOSCOPY Introduction In 2011 the Independent Practice