David P. Ryan, M.D. Clinical Director, MGH Cancer Center Chief, Hematology-Oncology, MGH
|
|
|
- Branden McCarthy
- 6 years ago
- Views:
Transcription


1 Colon Cancer 2015 David P. Ryan, M.D. Clinical Director, MGH Cancer Center Chief, Hematology-Oncology, MGH

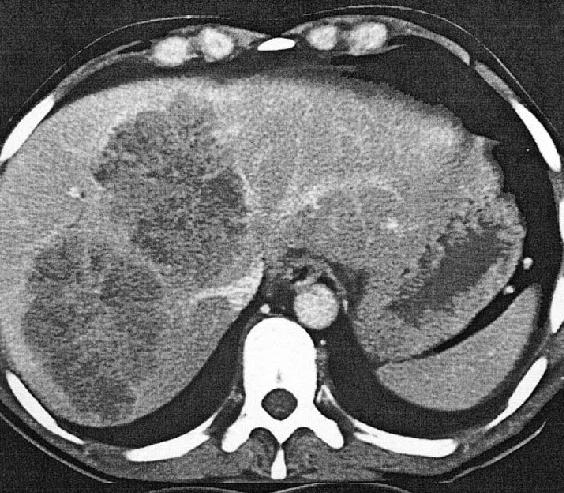
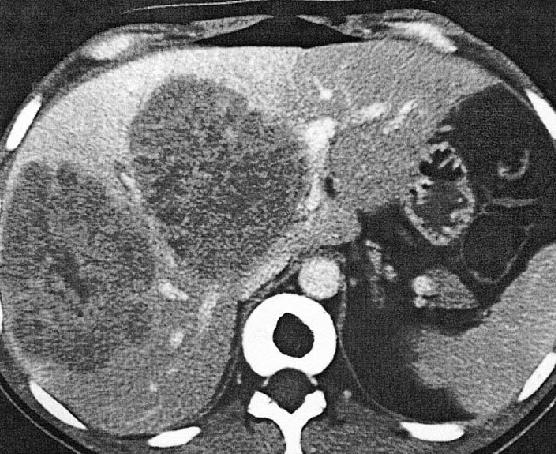
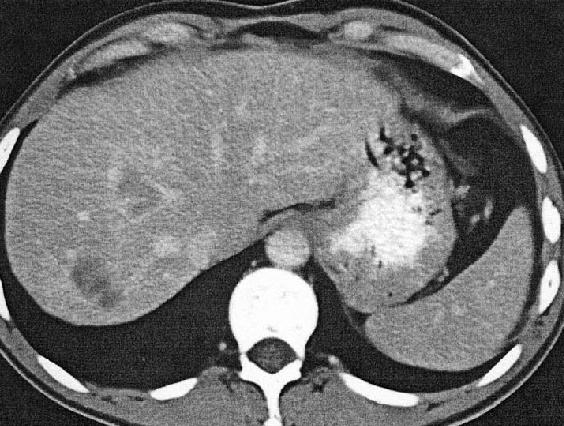
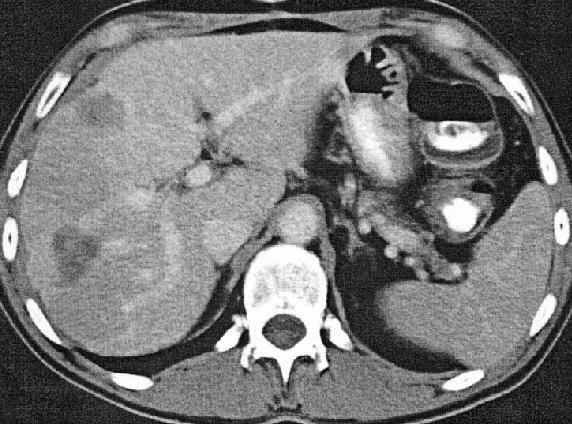
2 Colon Cancer Case presentation 72yo woman presented 1/03 abd discomfort and nausea Found to have Hct 30 MCV 71 Alk Ph 150 USG of pelvis to f/u fibroids demonstrated liver mass Colonoscopy: splenic flexure mass = adenocarcinoma
3 Agenda Statistics and Epidemiology Inherited Syndromes Approach to Screening Treatment
4 Statistics
5 Statistics
6 Cancer Trends

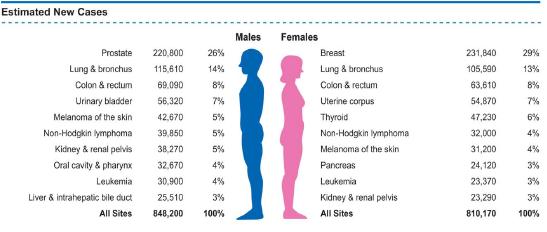
7 7 Probability of Developing Cancer
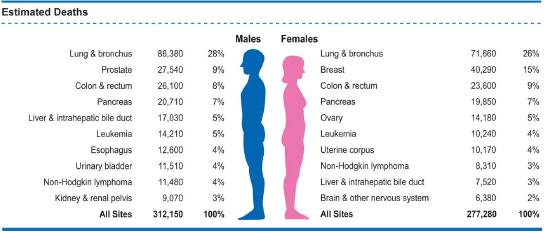
8 5 Leading Cancer Deaths
9 Colon Cancer Epidemiologic Associations Western/urbanized societies High meat High saturated fat and cholesterol Increased bowel anaerobic flora Deconjugated fecal bile acid excretion Diabetes Mellitus Tobacco use Obesity Alcohol
10 Colon Cancer Epidemiologic Associations Western/urbanized societies High meat High saturated fat and cholesterol Increased bowel anaerobic flora Deconjugated fecal bile acid excretion Diabetes Mellitus Tobacco use Obesity Alcohol

11 11 Obesity and Cancer in Men

12 12 Obesity and Cancer in Women
13 Colon Cancer Epidemiologic Associations IBD Risk in UC correlates with extent, duration and severity of disease Risk of cancer in UC 9% at 10 yrs, 20% at 20yrs, and >35% at 30 years Total colectomy eliminates the risk Cholecystectomy Ureterocolic anastamoses Pelvic Radiation Low Vit D
14 Colon Cancer Protective Factors NSAIDs, folate, calcium, estrogens prevent development of polyps No clear benefit for prevention of cancer What is the role in patients getting adequately screened? Physical activity Diets high in fish and low in red meat associated with reduced incidence of colorectal cancer Out of favor: anti-oxidants and fiber
15 Colon Cancer Chemoprevention with Aspirin Multiple retrospective studies: reduced risk of colorectal adenomas and cancer in regular aspirin users The Nurses' Health Study: regular use of aspirin ( 2 standard aspirin tables per day) was associated with a 25 percent reduction in the risk of an adenoma (RR 0.75, 95 percent CI 0.66 to 0.84) Randomized studies of aspirin after a diagnosis of colorectal adenoma/carcinoma demonstrate reduced rate of adenomas
16 Colon Cancer Chemoprevention with Aspirin BUT, the Physician s Health Study (prospective) failed to demonstrate a significant effect of aspirin use on the incidence of colorectal cancer SUMMARY: The overall risk/benefit of prolonged daily aspirin for the primary prevention of colorectal cancer is unknown

17 But
18 Colon Cancer Polyps: hamartoma, hyperplastic, adenoma Adenomas are pre-malignant Occur in 30-50% of adults <1% polyps become cancer Adenomatous polyps more likely to become cancer if sessile, villous, and > 1.5cm Takes at least 5 yrs for polyp to become cancer Some hyperplastic polyps may be pre-malignant Serrated polyps associated with right sided colon cancers that are braf mutant

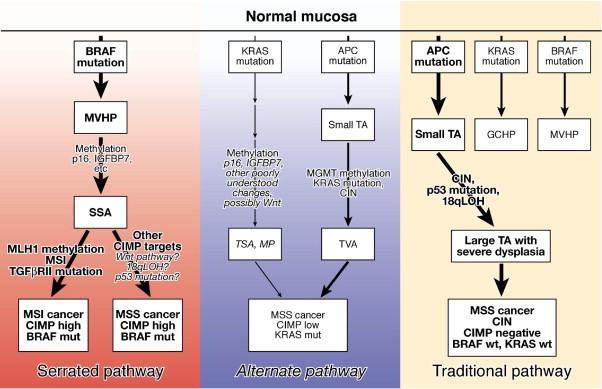
19 Colon Cancer: Vogelgram
20 Carcinogenesis
21 Causes of colorectal cancer Sporadic (65% 85%) Familial (10% 30%) Rare CRC syndromes (<0.1%) Familial adenomatous polyposis (FAP) (1%) Hereditary nonpolyposis colorectal cancer (HNPCC) (5%) Adapted from Burt RW et al. Prevention and Early Detection of CRC, 1996
22 Familial Risk for Colorectal Cancer Approximate lifetime CRC risk (%) % None One 1 Aarnio M et al. Int J Cancer 64:430, 1995 Houlston RS et al. Br Med J 301:366, 1990 St John DJ et al. Ann Intern Med 118:785, % 8% 10% One 1 and two 2 One 1 <45 yo 17% Two 1 Affected family members 70% HNPCC mutation
23 Colon Cancer Epidemiology Inherited Syndromes Hereditary Non-Polyposis Colon Cancer Familial Adenomatous Polyposis MYH
24 Colon Cancer Epidemiology Hereditary Non-Polyposis Colon Cancer (Lynch Syndrome) Autosomal dominant Germline mutations in Mismatch Repair (MMR) genes leads to Microsatellite Instability (MSI) Median age for tumors < 50 Proximal colon >> distal colon May account for 5% of colon cancers
25 Cancer Risks in HNPCC 100 % with cancer Colorectal 78% Aarnio M et al. Int J Cancer 64:430, 1995 Age (years) Endometrial 43% Stomach 19% Biliary tract 18% Urinary tract 10% Ovarian 9%
26 HNPCC Diagnosis Amsterdam criteria Bethesda criteria

27 Amsterdam Criteria Failure to meet these criteria does not exclude HNPCC

28 HNPCC: Bethesda Criteria
29 Laboratory Testing for HNPCC Tests on the Tumor Immunohistochemistry testing of the tumor MSI testing Tests on the Blood Sequence analysis
30 Surveillance Options for Carriers of HNPCC- Associated Mutations Malignancy Colorectal cancer Endometrial cancer Intervention Colonoscopy l l Transvaginal ultrasound Endometrial aspirate Recommendation Begin at age 20 25, repeat every 1 2 years Annually, starting at age 25 35
31 Other Surveillance in HNPCC Annual EGD Annual urinalysis with cytology Annual abdominal ultrasound

32 Clinical Features of FAP Estimated penetrance for adenomas >90% Untreated polyposis leads to 100% risk of cancer
33 Colon Cancer Epidemiology Familial Adenomatous Polyposis Associated with Congenital hypertophy of the retinal pigment epithelium Desmoid tumors (Gardner s Syndrome) Brain tumors (Turcot s Syndrome) Screening of first degree relatives by age 10 Thousands of adenomatous polyps develop by age 20 and lead to cancer Total colectomy with ileoanal anastomosis is treatment of choice
34 Lifetime Risk of Extra-Colonic Cancer in FAP Site Type of Cancer Risk of Cancer Small bowel: duodenum or periampulla Small bowel: distal to the duodenum Carcinoma 4-12% Rare Stomach Adenocarcinoma 0.5% Pancreas ~2% Thyroid CNS Liver Bile ducts Adrenal gland Papillary thyroid carcinoma Usually medulloblastoma Hepatoblastoma Adenocarcinoma ~2% <1% 1.6% (children <age 5 years) Low, but increased

35 Many adenomas but no germline mutation in APC Consider germline mutations in MYH: Base-excision repair gene. Bi-allelic germline mutations predispose to APC mutations that lead to colon adenomas, tumors. Family history of colon cancer shows recessive inheritance. Tens-to-hundreds of colorectal adenomas.
36 MGH Center for Cancer Risk Analysis Genetic Counselors: Programs:»6 counselors Breast and Ovarian: Leif Ellisen, MD, PhD Gastrointestinal: Daniel Chung, MD; Andy Chan, MD; Von Hippel Lindau: Othon Iliopoulos, MD Melanoma: Hensin Tsao, MD, PhD Psychiatry: William Pirl, MD
37 Colorectal Cancer Screening How should I approach it?

38 US MultiSociety Task Force 2008 CA A Cancer J for Clin 2008; 58:
39 39 US Multisociety Task Force, 2012 Update
40 Colon Cancer Screening Hemoccult: gfobt or FIT 2-4% of adults with test positive and 60% will have no mucosal abnormality in their large bowel 50% of pts with CRC will have a false negative study Minnesota study demonstrated that screening reduces deaths from CRC BUT 36% of pts assigned to annual screening underwent endoscopy and there were 20% less cancers in this subgroup
41 Colon Cancer Screening sdna Sensitivity 52-91% Specificity 93-97%?interval?need for endoscopy

42 FIT vs sdna Imperiale TF et al. N Engl J Med 2014;370: Imperiale T et al. N Engl J Med 2004;351:
43 Colon Cancer Screening Barium Enema DON T DO IT
44 Colon Cancer Screening Endoscopy Flexible sigmoidoscopy vs Colonscopy Approximately 2% of asymptomatic adults will have proximal precancerous or cancerous lesions and have TOTALLY NORMAL sigmoidoscopies Fecal occult blood testing plus sigmoidoscopy has a sensitivity of 75%, ie will miss 25% of lesions Colonoscopy may miss lesions as much as 4% of time
45 Colonoscopy vs Flex Sig Source Lieberman NEJM 2000 Imperiale NEJM 2000 % % pts adequate advanced exam neoplasm* *advanced neoplasm=carcinoma, dysplasia, or villous adenoma
46 Colonoscopy vs Flex Sig % pts with proximal neoplasm if distal bowel showed Source Advanced neoplasm Tubular adenoma No polyp Lieberman NEJM 2000 Imperiale NEJM

47 Colonoscopy and CRC Death Baxter, N. N. et. al. Ann Intern Med 2009;150:1-8

48 Colonoscopy and CRC Death Baxter, N. N. et. al. Ann Intern Med 2009;150:1-8
49 US Preventive Services Task Force March 2008 When to stop? U.S. Preventive Services Task Force, Ann Intern Med 2008;0: E-243
50 Colon Cancer Screening Average Risk Colonoscopy beginning at age 50 every 10 years If pathology found, follow the recommendation of the gastroenterologist For low risk adenoma, they will recommend repeat screening at 5 years For high risk adenoma, they will recommend repeat screening at 3 years
51 Colon Cancer Increased Risk Screening Made Easy Have you ever had colorectal cancer or an adenomatous polyp? Have you had inflammatory bowel disease (ulcerative colitis or Crohn's disease)? Has a family member had colorectal cancer or an adenomatous polyp? If so, how many, was it a first-degree relative (parent, sibling, or child), and at what age was the cancer or polyp first diagnosed?
52 Colon Cancer Screening Made Easy Have you ever had colorectal cancer or an adenomatous polyp? Colonoscopy q 3-5years Have you had inflammatory bowel disease (ulcerative colitis or Crohn's disease)? Has a family member had colorectal cancer or an adenomatous polyp? If so, how many, was it a first-degree relative (parent, sibling, or child), and at what age was the cancer or polyp first diagnosed?
53 Colon Cancer Screening Made Easy Have you ever had colorectal cancer or an adenomatous polyp? Colonoscopy q 3-5years Have you had inflammatory bowel disease (ulcerative colitis or Crohn's disease)? refer to Gastroenterology Has a family member had colorectal cancer or an adenomatous polyp? If so, how many, was it a first-degree relative (parent, sibling, or child), and at what age was the cancer or polyp first diagnosed?
54 Colon Cancer Screening Made Easy Has a family member had colorectal cancer or an adenomatous polyp? If so, how many, was it a first-degree relative (parent, sibling, or child), and at what age was the cancer or polyp first diagnosed? Begin screening at least 10 years younger than the youngest member in the family with colon cancer Begin screening at age 40 if first degree relative had colon cancer <60 Refer to High Risk Genetics if HNPCC suspected
55 Colon Cancer: Screening CT Colonography Appears to be just as good for lesions that are 1cm in size Very good for patients who have incomplete colonoscopies Still have to give GI prep Novel preps under investigation Not able to biopsy
56 Colon Cancer Clinical Presentation Nearly half of colon cancers are found in the right side of the colon Trend is for unknown reasons Different biology (e.g. braf mutation) Presenting symptoms (ie bleeding, change in bowel habits, anemia, obstuction) depend on location Clinical pearls
57 Colon Cancer Clinical Presentation Clinical pearls If you feel something on rectal exam, never assume that it is an internal hemorrhoid
58 Colon Cancer Clinical Presentation Clinical pearls If you feel something on rectal exam, never assume that it is an internal hemorrhoid A walled off perforation from a colon cancer can masquerade as diverticulitis
59 Colon Cancer Clinical Presentation Clinical pearls If you feel something on rectal exam, never assume that it is an internal hemorrhoid A walled off perforation from a colon cancer can masquerade as diverticulitis If an Fe def anemia workup has been done and nothing found, repeat the colonoscopy right sided lesions could have been missed

60 Staging of Colorectal Cancer Stage Extent of tumor 5-year survival I (T1) No deeper than submucosa >90% I (T2) Not through bowel wall >90% II Through bowel wall 80% IIIa Not through bowel wall: lymph node metastases 70-90% IIIb/c Through bowel wall: lymph node metastases 40-80% IV Distant metastases 20% Lung Mucosa Muscularis mucosa Submucosa Liver Lung Bone Skin Brain Muscularis propria Serosa Fat Lymph nodes Adapted from Skarin AT, ed. Atlas of Diagnostic Oncology. 3rd ed. St. Louis, Mo: Mosby Inc; 2003:155.
61 Colon Cancer Treatment Stage I: surgery Laparoscopic or open colectomy Stage II: surgery +?chemotherapy Stage III: surgery + chemotherapy Stage IV: chemotherapy +?surgery Patients with isolated liver or lung metastases can be cured with surgical resection

62 Rectal Cancer: Total Mesorectal Excision
63 Rectal Cancer Treatment Stage I: surgery Stage II: surgery + chemotherapy + radiation Stage III: surgery + chemotherapy + radiation Stage IV: chemotherapy +?surgery
64 Colorectal Cancer Surveillance Colonoscopy 1 year after diagnosis and then every 3-5 years For stage 2 and 3, every 3 month CEA/LFTs/physical exam and annual CT for 3 years. Then follow annually with cea and LFTs until year 5 Lifestyle/Dietary Changes: Very good retrospective or observational evidence Exercise, ASA, Vit D?Red meat
65 Colorectal Cancer: Chemotherapy for Metastatic Disease or By little and little 3 reasons for seeing an oncologist Be Cured Live Longer Feel Better
66 How to Explain to Patients Stage 3c
67 How to Explain to Patients Stage 3c
68 How to Explain to Patients Stage 3c
69 How to Explain to Patients Stage 3a
70 How to Explain to Patients Stage 3a
71 Advances in the Treatment of Colorectal Cancer FU Irinotecan Capecitabine Oxaliplatin Cetuximab Bevacizumab Panitumumab Regorafenib TAS 102 Adjuvant chemotherapy Neoadjuvant chemotherapy

72 Stage 4 Colon Cancer: Improved Survival Kopetz et al JCO 2012
73 Overall Survival for Liver Resection Adam R, et al., Ann Surgery Oct;240(4):

 30.")
 26.")
74 CALGB/SWOG 80405: Overall Survival FOLFOX Treated Arm N (Events) OS (m) Median 95% CI FOLFOX + Cetux 426 (277) FOLFOX + Bev 409 (290) P=0.09 HR 0.9 ( )
75 75
76 76

77 Colon Cancer Case presentation Left hemicolectomy for T4, N1, M1 colon cancer Treated with chemotherapy

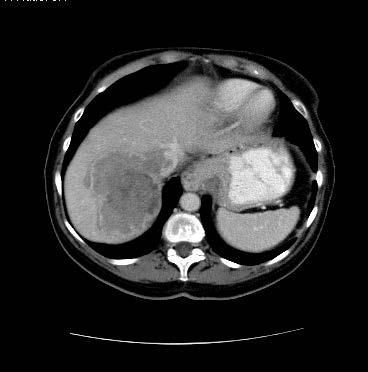
78 Colon Cancer Case presentation
79 Colorectal Cancer Summary Obesity and Exercise Colonoscopy: Left >>Right Identification of high risk patients is key in offering appropriate screening All stage III and some stage II patients will get 6 months of adjuvant therapy Treatment of metastatic disease has changed dramatically in last 10 years
Colorectal Neoplasia. Dr. Smita Devani MBChB, MRCP. Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi
 Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
Colon Cancer Screening & Surveillance. Amit Patel, MD PGY-4 GI Fellow
 Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Risk of Colorectal Cancer (CRC) Hereditary Syndromes in GI Cancer GENETIC MALPRACTICE
 Hereditary Syndromes in GI Cancer GENETIC MALPRACTICE") Identifying the Patient at Risk for an Inherited Syndrome Sapna Syngal, MD, MPH, FACG Director, Gastroenterology Director, Familial GI Program Dana-Farber/Brigham and Women s Cancer Center Associate Professor
Identifying the Patient at Risk for an Inherited Syndrome Sapna Syngal, MD, MPH, FACG Director, Gastroenterology Director, Familial GI Program Dana-Farber/Brigham and Women s Cancer Center Associate Professor
EARLY DETECTION OF COLORECTAL CANCER. Epidemiology of CRC
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Clinical Colon Cancer Abby Siegel MD COLON CANCER. 1. Epidemiology 2. Risk factors 3. Manifestations 4. Treatment
 Clinical Colon Cancer 2008 Abby Siegel MD COLON CANCER 1. Epidemiology 2. Risk factors 3. Manifestations 4. Treatment 1 1. EPIDEMIOLOGY - Colorectal cancer is the third most common cancer in the United
Clinical Colon Cancer 2008 Abby Siegel MD COLON CANCER 1. Epidemiology 2. Risk factors 3. Manifestations 4. Treatment 1 1. EPIDEMIOLOGY - Colorectal cancer is the third most common cancer in the United
Colon, or Colorectal, Cancer Information
 Colon, or Colorectal, Cancer Information Definition Colon, or colorectal, cancer is cancer that starts in the large intestine (colon) or the rectum (end of the colon). Other types of cancer can affect
Colon, or Colorectal, Cancer Information Definition Colon, or colorectal, cancer is cancer that starts in the large intestine (colon) or the rectum (end of the colon). Other types of cancer can affect
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
Familial Adenomatous Polyposis
 Familial Adenomatous Polyposis 1 in 10,000 incidence 100 s to 1000 s of colonic adenomas by teens Cancer risk: colon, gastric, duodenum (periampulla), small bowel, pancreas, papillary thyroid, childhood
Familial Adenomatous Polyposis 1 in 10,000 incidence 100 s to 1000 s of colonic adenomas by teens Cancer risk: colon, gastric, duodenum (periampulla), small bowel, pancreas, papillary thyroid, childhood
COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University
 Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University") COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University 1. I am a surgeon; of course I have nothing to disclose.
COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University 1. I am a surgeon; of course I have nothing to disclose.
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
For identification, support and follow up related to Familial Gastrointestinal Cancer conditions. South Island Cancer Nurses Network September 2013
 For identification, support and follow up related to Familial Gastrointestinal Cancer conditions South Island Cancer Nurses Network September 2013 Who are we? Specialist multidisciplinary team: Nurse coordinators,
For identification, support and follow up related to Familial Gastrointestinal Cancer conditions South Island Cancer Nurses Network September 2013 Who are we? Specialist multidisciplinary team: Nurse coordinators,
Screening & Surveillance Guidelines
 Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Primary Care Approach to Genetic Cancer Syndromes
 Primary Care Approach to Genetic Cancer Syndromes Jason M. Goldman, MD, FACP FAU School of Medicine Syndromes Hereditary Breast and Ovarian Cancer (HBOC) Hereditary Nonpolyposis Colorectal Cancer (HNPCC)
Primary Care Approach to Genetic Cancer Syndromes Jason M. Goldman, MD, FACP FAU School of Medicine Syndromes Hereditary Breast and Ovarian Cancer (HBOC) Hereditary Nonpolyposis Colorectal Cancer (HNPCC)
By: Tania Cortas, MD Arizona Oncology 03/10/2015
 By: Tania Cortas, MD Arizona Oncology 03/10/2015 Epidemiology In the United States, CRC incidence rates have declined about 2 to 3 percent per year over the last 15 years Death rates from CRC have declined
By: Tania Cortas, MD Arizona Oncology 03/10/2015 Epidemiology In the United States, CRC incidence rates have declined about 2 to 3 percent per year over the last 15 years Death rates from CRC have declined
Caring for a Patient with Colorectal Cancer. Objectives. Poll question. UNC Cancer Network Presented on 10/15/18. For Educational Use Only 1
 Caring for a Patient with Colorectal Cancer Tammy Triglianos RN, APRN-BC, AOCNP Nurse Practitioner, GI Oncology 10/15/2018 Objectives Describe common signs and symptoms of colorectal cancer Understand
Caring for a Patient with Colorectal Cancer Tammy Triglianos RN, APRN-BC, AOCNP Nurse Practitioner, GI Oncology 10/15/2018 Objectives Describe common signs and symptoms of colorectal cancer Understand
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Objectives. Definitions. Colorectal Cancer Screening 5/8/2018. Payam Afshar, MS, MD Kaiser Permanente, San Diego. Colorectal cancer background
 Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Gastric and Colon Cancer. Dr. Andres Wiernik 2017
 Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
This is the portion of the intestine which lies between the small intestine and the outlet (Anus).
.") THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
removal of adenomatous polyps detects important effectively as follow-up colonoscopy after both constitute a low-risk Patients with 1 or 2
 Supplementary Table 1. Study Characteristics Author, yr Design Winawer et al., 6 1993 National Polyp Study Jorgensen et al., 9 1995 Funen Adenoma Follow-up Study USA Multi-center, RCT for timing of surveillance
Supplementary Table 1. Study Characteristics Author, yr Design Winawer et al., 6 1993 National Polyp Study Jorgensen et al., 9 1995 Funen Adenoma Follow-up Study USA Multi-center, RCT for timing of surveillance
Colonic polyps and colon cancer. Andrew Macpherson Director of Gastroentology University of Bern
 Colonic polyps and colon cancer Andrew Macpherson Director of Gastroentology University of Bern Improtance of the problem of colon cancers - Epidemiology Lifetime risk 5% Incidence/10 5 /annum (US Detroit
Colonic polyps and colon cancer Andrew Macpherson Director of Gastroentology University of Bern Improtance of the problem of colon cancers - Epidemiology Lifetime risk 5% Incidence/10 5 /annum (US Detroit
Cancer Genomics 101. BCCCP 2015 Annual Meeting
 Cancer Genomics 101 BCCCP 2015 Annual Meeting Objectives Identify red flags in a person s personal and family medical history that indicate a potential inherited susceptibility to cancer Develop a systematic
Cancer Genomics 101 BCCCP 2015 Annual Meeting Objectives Identify red flags in a person s personal and family medical history that indicate a potential inherited susceptibility to cancer Develop a systematic
CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING
 CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING This guideline is designed to assist practitioners by providing the framework for colorectal cancer (CRC) screening, and is not intended to replace
CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING This guideline is designed to assist practitioners by providing the framework for colorectal cancer (CRC) screening, and is not intended to replace
COLON CANCER PROFILE 2012} Cancer Outcomes Analysis Report. The Institute for. Cancer Care
 COLON CANCER PROFILE 2012} Cancer Outcomes Analysis Report The Institute for Cancer Care FACT} People with a first-degree relative (parent, sibling, or children) who has colon cancer are between two and
COLON CANCER PROFILE 2012} Cancer Outcomes Analysis Report The Institute for Cancer Care FACT} People with a first-degree relative (parent, sibling, or children) who has colon cancer are between two and
Content. Diagnostic approach and clinical management of Lynch Syndrome: guidelines. Terminology. Identification of Lynch Syndrome
 of Lynch Syndrome: guidelines 17/03/2009 Content Terminology Lynch Syndrome Presumed Lynch Syndrome Familial Colorectal Cancer Identification of Lynch Syndrome Amsterdam II criteria Revised Bethesda Guidelines
of Lynch Syndrome: guidelines 17/03/2009 Content Terminology Lynch Syndrome Presumed Lynch Syndrome Familial Colorectal Cancer Identification of Lynch Syndrome Amsterdam II criteria Revised Bethesda Guidelines
Colorectal adenocarcinoma leading cancer in developed countries In US, annual deaths due to colorectal adenocarcinoma 57,000.
 Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Guidelines for Breast, Cervical and Colorectal Cancer Screening
 Guidelines for Breast, Cervical and Colorectal Cancer Screening Your recommendation counts. Talk to your patients about screening for cancer. CancerCare Manitoba provides organized, population-based screening
Guidelines for Breast, Cervical and Colorectal Cancer Screening Your recommendation counts. Talk to your patients about screening for cancer. CancerCare Manitoba provides organized, population-based screening
General Surgery Grand Grounds
 General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
COME HOME Innovative Oncology Business Solutions, Inc.
 COME HOME Rectal Cancer Pathway V8, April 2015 Diagnostic Workup: Bethesda Criteria: Pathology Review All patients H&P All patients Biopsy All patients Colonoscopy All patients CEA All Patients Chest/Abdominal/Pelvic
COME HOME Rectal Cancer Pathway V8, April 2015 Diagnostic Workup: Bethesda Criteria: Pathology Review All patients H&P All patients Biopsy All patients Colonoscopy All patients CEA All Patients Chest/Abdominal/Pelvic
GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS. Family Health Clinical Genetics. Clinical Genetics department
 GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS Full Title of Guideline: Author (include email and role): Division & Speciality: GUIDELINES FOR THE GENETIC MANAGEMENT OF A FAMILY
GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS Full Title of Guideline: Author (include email and role): Division & Speciality: GUIDELINES FOR THE GENETIC MANAGEMENT OF A FAMILY
UPDATE IN THE MANAGEMENT AND TREATMENT OF COLORECTAL CANCER. Edwin A. Empaynado, MD Advocare Colon and Rectal Surgical Specialists
 UPDATE IN THE MANAGEMENT AND TREATMENT OF COLORECTAL CANCER Edwin A. Empaynado, MD Advocare Colon and Rectal Surgical Specialists WHAT IS COLON CANCER? WHAT CAUSES COLORECTAL CANCER? WHAT ARE THE RISK
UPDATE IN THE MANAGEMENT AND TREATMENT OF COLORECTAL CANCER Edwin A. Empaynado, MD Advocare Colon and Rectal Surgical Specialists WHAT IS COLON CANCER? WHAT CAUSES COLORECTAL CANCER? WHAT ARE THE RISK
Colon Cancer Screening and Surveillance. Louis V. Antignano, M.D. Wilson Gastroenterology October 11, 2011
 Colon Cancer Screening and Surveillance Louis V. Antignano, M.D. Wilson Gastroenterology October 11, 2011 Colorectal Cancer Preventable cancer Number 2 cancer killer in the USA Often curable if detected
Colon Cancer Screening and Surveillance Louis V. Antignano, M.D. Wilson Gastroenterology October 11, 2011 Colorectal Cancer Preventable cancer Number 2 cancer killer in the USA Often curable if detected
Pathology reports, related operative reports and consult letters must be provided with a request for assessment.
 Page 1 of 6 Polyposis Syndromes Inherited risk for colorectal cancer is associated with a number of polyposis syndromes (genes), some of which are well-defined and others are less common. Identification
Page 1 of 6 Polyposis Syndromes Inherited risk for colorectal cancer is associated with a number of polyposis syndromes (genes), some of which are well-defined and others are less common. Identification
2. Describe pros/cons of screening interventions (including colonoscopy, CT colography, fecal tests)
") Learning Objectives 1. Review principles of colon adenoma/cancer biology that permit successful prevention regimes 2. Describe pros/cons of screening interventions (including colonoscopy, CT colography,
Learning Objectives 1. Review principles of colon adenoma/cancer biology that permit successful prevention regimes 2. Describe pros/cons of screening interventions (including colonoscopy, CT colography,
Colorectal Cancer Prevention Quantity and Quality Count
 Colorectal Cancer Prevention Quantity and Quality Count Ernesto Drelichman, MD Gastrointestinal Surgery & Endoscopy Providence Hospital Key Messages Colorectal cancer can be prevented Screening reduces
Colorectal Cancer Prevention Quantity and Quality Count Ernesto Drelichman, MD Gastrointestinal Surgery & Endoscopy Providence Hospital Key Messages Colorectal cancer can be prevented Screening reduces
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
Mr Chris Wakeman. General Surgeon University of Otago, Christchurch. 12:15-12:40 Management of Colorectal Cancer
 Mr Chris Wakeman General Surgeon University of Otago, Christchurch 12:15-12:40 Management of Colorectal Cancer Bowel cancer Chris Wakeman Colorectal Surgeon Christchurch Sam Simon (Simpsons) Elizabeth
Mr Chris Wakeman General Surgeon University of Otago, Christchurch 12:15-12:40 Management of Colorectal Cancer Bowel cancer Chris Wakeman Colorectal Surgeon Christchurch Sam Simon (Simpsons) Elizabeth
ADVANCES IN COLORECTAL CANCERS IS THERE HOPE? Dr Lim Hwee Yong Medical Oncologist
 ADVANCES IN COLORECTAL CANCERS IS THERE HOPE? Dr Lim Hwee Yong Medical Oncologist limhweeyong@live.com CRC: Epidemiology in 2012 Third most common cancer diagnosis in US [1] Estimated 143,460 new cases
ADVANCES IN COLORECTAL CANCERS IS THERE HOPE? Dr Lim Hwee Yong Medical Oncologist limhweeyong@live.com CRC: Epidemiology in 2012 Third most common cancer diagnosis in US [1] Estimated 143,460 new cases
Colorectal Cancer in 2006: New Developments
 James J. Stark, MD Colorectal Cancer in 2006: New Developments Melissa Bennett, MS, CGC Myriad Genetic Laboratories Thomas Duntemann,, MD Ray Ramirez, Jr., MD Hereditary Colon Cancer and Genetic Testing
James J. Stark, MD Colorectal Cancer in 2006: New Developments Melissa Bennett, MS, CGC Myriad Genetic Laboratories Thomas Duntemann,, MD Ray Ramirez, Jr., MD Hereditary Colon Cancer and Genetic Testing
GI EMERGENCIES Acute Abdominal Pain
 GI EMERGENCIES Acute Abdominal Pain Marcia Cruz-Correa, MD, PhD, AGAF. FASGE Associate Professor of Medicine, Biochemistry, Surgery Director Translational Research University of Puerto Rico Comprehensive
GI EMERGENCIES Acute Abdominal Pain Marcia Cruz-Correa, MD, PhD, AGAF. FASGE Associate Professor of Medicine, Biochemistry, Surgery Director Translational Research University of Puerto Rico Comprehensive
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE
 COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
Colon Screening in 2014 Offering Patients a Choice. Clark A Harrison MD The Nevada Colon Cancer Partnership
 Colon Screening in 2014 Offering Patients a Choice Clark A Harrison MD The Nevada Colon Cancer Partnership Objectives 1. Understand the incidence and mortality rates for CRC in the US. 2. Understand risk
Colon Screening in 2014 Offering Patients a Choice Clark A Harrison MD The Nevada Colon Cancer Partnership Objectives 1. Understand the incidence and mortality rates for CRC in the US. 2. Understand risk
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci. Colon polyps. Colorectal cancer
 Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Resident Seminar Aug 19 th, 2015 Colon: Neoplastic. Scott Rieder Dr. Colquhoun
 Resident Seminar Aug 19 th, 2015 Colon: Neoplastic Scott Rieder Dr. Colquhoun Objectives Medical Expert: 1. The biologic basis of colon neoplasia 2. Colon cancer screening (guidelines and evidence) 3.
Resident Seminar Aug 19 th, 2015 Colon: Neoplastic Scott Rieder Dr. Colquhoun Objectives Medical Expert: 1. The biologic basis of colon neoplasia 2. Colon cancer screening (guidelines and evidence) 3.
Colorectal Cancer Screening: Cost-Effectiveness and Adverse events October, 2005
 Colorectal Cancer Screening: Cost-Effectiveness and Adverse events October, 2005 David Lieberman MD Chief, Division of Gastroenterology Oregon Health and Science University Portland VAMC Portland, Oregon
Colorectal Cancer Screening: Cost-Effectiveness and Adverse events October, 2005 David Lieberman MD Chief, Division of Gastroenterology Oregon Health and Science University Portland VAMC Portland, Oregon
Navigators Lead the Way
 RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
Colon Cancer Screening. Layth Al-Jashaami, MD GI Fellow, PGY 4
 Colon Cancer Screening Layth Al-Jashaami, MD GI Fellow, PGY 4 -Colorectal cancer (CRC) is a common and lethal cancer. -It has the highest incidence among GI cancers in the US, estimated to be newly diagnosed
Colon Cancer Screening Layth Al-Jashaami, MD GI Fellow, PGY 4 -Colorectal cancer (CRC) is a common and lethal cancer. -It has the highest incidence among GI cancers in the US, estimated to be newly diagnosed
Colorectal Cancer. Mark Chapman. MA MS FRCS EBSQ(coloproct) 21 st March 2018 Consultant Coloproctologist
 21 st March 2018 Consultant Coloproctologist") Colorectal Cancer Mark Chapman MA MS FRCS EBSQ(coloproct) 21 st March 2018 Consultant Coloproctologist Overview Epidemiology of colorectal cancer Adenoma carcinoma sequence Tumour diagnosis & staging Treatment
Colorectal Cancer Mark Chapman MA MS FRCS EBSQ(coloproct) 21 st March 2018 Consultant Coloproctologist Overview Epidemiology of colorectal cancer Adenoma carcinoma sequence Tumour diagnosis & staging Treatment
COLORECTAL CANCER CASES
 COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
ACG Clinical Guideline: Colorectal Cancer Screening
 ACG Clinical Guideline: Colorectal Cancer Screening Douglas K. Rex, MD, FACG 1, David A. Johnson, MD, FACG 2, Joseph C. Anderson, MD 3, Phillip S. Schoenfeld, MD, MSEd, MSc (Epi), FACG 4, Carol A. Burke,
ACG Clinical Guideline: Colorectal Cancer Screening Douglas K. Rex, MD, FACG 1, David A. Johnson, MD, FACG 2, Joseph C. Anderson, MD 3, Phillip S. Schoenfeld, MD, MSEd, MSc (Epi), FACG 4, Carol A. Burke,
Colorectal Cancer Screening. Daniel C. Chung, MD GI Unit and GI Cancer Genetics Service Massachusetts General Hospital
 Colorectal Cancer Screening Daniel C. Chung, MD GI Unit and GI Cancer Genetics Service Massachusetts General Hospital March, 2018 CRC Epidemiology 4th most common malignancy in US (136,000 cases/yr) 2nd
Colorectal Cancer Screening Daniel C. Chung, MD GI Unit and GI Cancer Genetics Service Massachusetts General Hospital March, 2018 CRC Epidemiology 4th most common malignancy in US (136,000 cases/yr) 2nd
CRC Risk Factors. U.S. Adherence Rates Cancer Screening. Genetic Model of Colorectal Cancer. Epidemiology and Clinical Consequences of CRC
 10:45 11:45 am Guide to Colorectal Cancer Screening SPEAKER Howard Manten M.D. Presenter Disclosure Information The following relationships exist related to this presentation: Howard Manten MD: No financial
10:45 11:45 am Guide to Colorectal Cancer Screening SPEAKER Howard Manten M.D. Presenter Disclosure Information The following relationships exist related to this presentation: Howard Manten MD: No financial
Joint Session with ACOFP and Cancer Treatment Centers of America (CTCA): Cancer Screening: Consensus & Controversies. Ashish Sangal, M.D.
: Cancer Screening: Consensus & Controversies. Ashish Sangal, M.D.") Joint Session with ACOFP and Cancer Treatment Centers of America (CTCA): Cancer Screening: Consensus & Controversies Ashish Sangal, M.D. Cancer Screening: Consensus & Controversies Ashish Sangal, MD Director,
Joint Session with ACOFP and Cancer Treatment Centers of America (CTCA): Cancer Screening: Consensus & Controversies Ashish Sangal, M.D. Cancer Screening: Consensus & Controversies Ashish Sangal, MD Director,
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Disclosures. Colorectal Cancer Update GAFP November Risk Assessment. Colon and Rectal Cancer The Challenge. Issues in Colon and Rectal Cancer
 Disclosures Colorectal Cancer Update GAFP November 2006 Robert C. Hermann, MD Georgia Center for Oncology Research and Education Northwest Georgia Oncology Centers, PC WellStar Health System Marietta,
Disclosures Colorectal Cancer Update GAFP November 2006 Robert C. Hermann, MD Georgia Center for Oncology Research and Education Northwest Georgia Oncology Centers, PC WellStar Health System Marietta,
FAMILIAL COLORECTAL CANCER. Lyn Schofield Manager Familial Cancer Registry
 FAMILIAL COLORECTAL CANCER Lyn Schofield Manager Familial Cancer Registry Cancer in WA 2004 4000 3500 ASPR, rate per 100,000 3000 2500 2000 1500 1000 Male incidence Female incidence Male mortality Female
FAMILIAL COLORECTAL CANCER Lyn Schofield Manager Familial Cancer Registry Cancer in WA 2004 4000 3500 ASPR, rate per 100,000 3000 2500 2000 1500 1000 Male incidence Female incidence Male mortality Female
Bowel obstruction and tumors
 Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE
 COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
LIST OF ABBREVIATIONS
 Gastroenter oenterology 2005 Royal College of Physicians of Edinburgh Screening and surveillance for upper and lower gastrointestinal cancer JN Plevris Consultant Gastroenterologist and Honorary Senior
Gastroenter oenterology 2005 Royal College of Physicians of Edinburgh Screening and surveillance for upper and lower gastrointestinal cancer JN Plevris Consultant Gastroenterologist and Honorary Senior
Cancer Screenings and Early Diagnostics
 Cancer Screenings and Early Diagnostics Ankur R. Parikh, D.O. Medical Director, Center for Advanced Individual Medicine Hematologist/Medical Oncologist Atlantic Regional Osteopathic Convention April 6
Cancer Screenings and Early Diagnostics Ankur R. Parikh, D.O. Medical Director, Center for Advanced Individual Medicine Hematologist/Medical Oncologist Atlantic Regional Osteopathic Convention April 6
COLON CANCER & GENETICS VERMONT COLORECTAL CANCER SUMMIT NOVEMBER 15, 2014
 COLON CANCER & GENETICS VERMONT COLORECTAL CANCER SUMMIT NOVEMBER 15, 2014 WENDY MCKINNON, MS, CGC CERTIFIED GENETIC COUNSELOR FAMILIAL CANCER PROGRAM UNIVERSIT Y OF VERMONT MEDICAL CENTER 1 CHARACTERISTICS
COLON CANCER & GENETICS VERMONT COLORECTAL CANCER SUMMIT NOVEMBER 15, 2014 WENDY MCKINNON, MS, CGC CERTIFIED GENETIC COUNSELOR FAMILIAL CANCER PROGRAM UNIVERSIT Y OF VERMONT MEDICAL CENTER 1 CHARACTERISTICS
Colorectal cancer Chapelle, J Clin Oncol, 2010
 Colorectal cancer Chapelle, J Clin Oncol, 2010 Early-Stage Colorectal cancer: Microsatellite instability, multigene assay & emerging molecular strategy Asit Paul, MD, PhD 11/24/15 Mr. X: A 50 yo asymptomatic
Colorectal cancer Chapelle, J Clin Oncol, 2010 Early-Stage Colorectal cancer: Microsatellite instability, multigene assay & emerging molecular strategy Asit Paul, MD, PhD 11/24/15 Mr. X: A 50 yo asymptomatic
Wellness Along the Cancer Journey: Healthy Habits and Cancer Screening Revised October 2015 Chapter 7: Cancer Screening and Early Detection of Cancer
 Wellness Along the Cancer Journey: Healthy Habits and Cancer Screening Revised October 2015 Chapter 7: Cancer Screening and Early Detection of Cancer Healthy Habits and Cancer Screening Rev 10.20.15 Page
Wellness Along the Cancer Journey: Healthy Habits and Cancer Screening Revised October 2015 Chapter 7: Cancer Screening and Early Detection of Cancer Healthy Habits and Cancer Screening Rev 10.20.15 Page
Colorectal Cancer Screening and Surveillance
 1 Colorectal Cancer Screening and Surveillance Jeffrey Lee MD, MAS Assistant Clinical Professor of Medicine University of California, San Francisco jeff.lee@ucsf.edu Objectives Review the various colorectal
1 Colorectal Cancer Screening and Surveillance Jeffrey Lee MD, MAS Assistant Clinical Professor of Medicine University of California, San Francisco jeff.lee@ucsf.edu Objectives Review the various colorectal
CENTERS FOR DISEASE CONTROL AND PREVENTION CENTERS FOR DISEASE CONTROL AND PREVENTION. Incidence Male. Incidence Female.
 A Call to Action: Prevention and Early Detection of Colorectal Cancer (CRC) 5 Key Messages Screening reduces mortality from CRC All persons aged 50 years and older should begin regular screening High-risk
A Call to Action: Prevention and Early Detection of Colorectal Cancer (CRC) 5 Key Messages Screening reduces mortality from CRC All persons aged 50 years and older should begin regular screening High-risk
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population
 Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
Latest Endoscopic Guidelines for FAP, HNPCC, IBD, and the General Population David T. Rubin, M.D. Assistant Professor of Medicine Inflammatory Bowel Disease Center MacLean Center for Clinical Medical Ethics
Prevention of Bowel Cancer: which patients do I send for colonoscopy?
 Prevention of Bowel Cancer: which patients do I send for colonoscopy? Dr Chris Groves Consultant Gastroenterologist and Honorary Senior Lecturer St George s Hospital and Medical School Director, SW London
Prevention of Bowel Cancer: which patients do I send for colonoscopy? Dr Chris Groves Consultant Gastroenterologist and Honorary Senior Lecturer St George s Hospital and Medical School Director, SW London
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
B Base excision repair, in MUTYH-associated polyposis and colorectal cancer, BRAF testing, for hereditary colorectal cancer, 696
 Index Note: Page numbers of article titles are in boldface type. A Adenomatous polyposis, familial. See Familial adenomatous polyposis. Anal anastomosis, ileal-pouch, proctocolectomy with, in FAP, 591
Index Note: Page numbers of article titles are in boldface type. A Adenomatous polyposis, familial. See Familial adenomatous polyposis. Anal anastomosis, ileal-pouch, proctocolectomy with, in FAP, 591
A Brief Overview of Screening and Management of Colorectal Cancer
 A Brief Overview of Screening and Management of Colorectal Cancer Gentry King MD Assistant Professor Hematology and Medical Oncology University of Colorado Disclosures Nothing to disclose Objectives Review
A Brief Overview of Screening and Management of Colorectal Cancer Gentry King MD Assistant Professor Hematology and Medical Oncology University of Colorado Disclosures Nothing to disclose Objectives Review
Hereditary Colorectal Cancer Syndromes Miguel A. Rodriguez-Bigas, MD
 Hereditary Colorectal Cancer Syndromes Miguel A. Rodriguez-Bigas, MD Living Beyond Cancer A-Z January 12,2019 Hereditary CRC Syndromes Objectives are to discuss the : Most common Hereditary CRC syndromes
Hereditary Colorectal Cancer Syndromes Miguel A. Rodriguez-Bigas, MD Living Beyond Cancer A-Z January 12,2019 Hereditary CRC Syndromes Objectives are to discuss the : Most common Hereditary CRC syndromes
Hereditary Non Polyposis Colorectal Cancer(HNPCC) From clinic to genetics
 From clinic to genetics") From clinic to genetics Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Autosomal dominant Question 2) Incidence of
From clinic to genetics Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Autosomal dominant Question 2) Incidence of
Third Line and Beyond: Management of Refractory Colorectal Cancer
 Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
GENERAL COLORECTAL CANCER INFORMATION. What is colorectal cancer?
 GENERAL COLORECTAL CANCER INFORMATION What is colorectal cancer? Colorectal cancer is cancer that develops in the colon or the rectum. The colon and rectum are parts of the digestive system, which is also
GENERAL COLORECTAL CANCER INFORMATION What is colorectal cancer? Colorectal cancer is cancer that develops in the colon or the rectum. The colon and rectum are parts of the digestive system, which is also
Colorectal Cancer Screening: A Clinical Update
 11:05 11:45am Colorectal Cancer Screening: A Clinical Update SPEAKER Kevin A. Ghassemi, MD Presenter Disclosure Information The following relationships exist related to this presentation: Kevin A. Ghassemi,
11:05 11:45am Colorectal Cancer Screening: A Clinical Update SPEAKER Kevin A. Ghassemi, MD Presenter Disclosure Information The following relationships exist related to this presentation: Kevin A. Ghassemi,
THE CROSSROADS: Drug Development, Biomarkers, and Colorectal Cancer
 THE CROSSROADS: Drug Development, Biomarkers, and Colorectal Cancer SANJAY GOEL, M.D., M.S. PROFESSOR OF MEDICINE ALBERT EINSTEIN COLLEGE OF MEDICINE MONTEFIORE MEDICAL CENTER DEPT. OF ONCOLOGY JUN 22,
THE CROSSROADS: Drug Development, Biomarkers, and Colorectal Cancer SANJAY GOEL, M.D., M.S. PROFESSOR OF MEDICINE ALBERT EINSTEIN COLLEGE OF MEDICINE MONTEFIORE MEDICAL CENTER DEPT. OF ONCOLOGY JUN 22,
A Trip Through the GI Tract: Common GI Diseases and Complaints. Jennifer Curtis, MD
 A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
A Trip Through the GI Tract: Common GI Diseases and Complaints Jennifer Curtis, MD Colon Cancer How does it develop? Most cancers arise from polyps Over time these can turn into cancer Combination of genetic
What All of Us Should Know About Cancer and Genetics
 What All of Us Should Know About Cancer and Genetics Beth A. Pletcher, MD, FAAP, FACMG Associate Professor of Pediatrics UMDNJ- New Jersey Medical School Disclosures I have no relevant financial relationships
What All of Us Should Know About Cancer and Genetics Beth A. Pletcher, MD, FAAP, FACMG Associate Professor of Pediatrics UMDNJ- New Jersey Medical School Disclosures I have no relevant financial relationships
FACT SHEET 49. What is meant by a family history of bowel cancer? What is bowel cancer? What causes bowel cancer?
 Important points The most important factors that can influence an individual s chance of developing bowel cancer are getting older and having a family history of bowel cancer A family history of bowel
Important points The most important factors that can influence an individual s chance of developing bowel cancer are getting older and having a family history of bowel cancer A family history of bowel
Carol A. Burke, MD, FACG
 Updated Guidelines for CRC C Screening and Surveillance Carol A. Burke MD, FACG, FASGE, FACP Cleveland Clinic, Cleveland, OH Gastroenterology t 2012;143:844 143 Gut 2010;59:666 1 Caveat for all Recommendations
Updated Guidelines for CRC C Screening and Surveillance Carol A. Burke MD, FACG, FASGE, FACP Cleveland Clinic, Cleveland, OH Gastroenterology t 2012;143:844 143 Gut 2010;59:666 1 Caveat for all Recommendations
Guidelines on Genetic Evaluation and Management of Lynch Syndrome: A Consensus Statement by the US Multi-Society Task Force on Colorectal Cancer
 s on Genetic Evaluation and Management of Lynch Syndrome: A Consensus Statement by the US Multi-Society Task Force on Colorectal Cancer Francis M. Giardiello, MD, 1 John I. Allen, 2 Jennifer E. Axilbund,
s on Genetic Evaluation and Management of Lynch Syndrome: A Consensus Statement by the US Multi-Society Task Force on Colorectal Cancer Francis M. Giardiello, MD, 1 John I. Allen, 2 Jennifer E. Axilbund,
Personalized Aspirin Therapy
 Personalized Aspirin Therapy Nadir Arber, MD, MSc, MHA Head - Integrated Cancer Prevention Center Tel Aviv Medical Centre and Tel Aviv University Heidelberg 2014 CRC is Preventable Early detection Chemoprevention
Personalized Aspirin Therapy Nadir Arber, MD, MSc, MHA Head - Integrated Cancer Prevention Center Tel Aviv Medical Centre and Tel Aviv University Heidelberg 2014 CRC is Preventable Early detection Chemoprevention
Historical. Note: The parenthetical numbers in the Clinical Indications section refer to the source documents cited in the References Section below.
 Clinical UM Guideline Subject: Colonoscopy Guideline #: CG-SURG-01 Current Effective Date: 01/21/2015 Status: Revised Last Review Date: 05/15/2014 Description Colonoscopy describes the direct visual inspection
Clinical UM Guideline Subject: Colonoscopy Guideline #: CG-SURG-01 Current Effective Date: 01/21/2015 Status: Revised Last Review Date: 05/15/2014 Description Colonoscopy describes the direct visual inspection
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Management of higher risk of colorectal cancer. Huw Thomas
 Management of higher risk of colorectal cancer Huw Thomas Colorectal Cancer 41,000 new cases pa in UK 16,000 deaths pa 60% 5 year survival Adenoma-carcinoma sequence (Morson) Survival vs stage (Dukes)
Management of higher risk of colorectal cancer Huw Thomas Colorectal Cancer 41,000 new cases pa in UK 16,000 deaths pa 60% 5 year survival Adenoma-carcinoma sequence (Morson) Survival vs stage (Dukes)
CRC and Endoscopy. Objectives. Background
 CRC and Endoscopy Darren Ballard, MD Assistant Professor Gastroenterology/Hepatology Medical College of Wisconsin Objectives Review background demographics and pathways for colon cancer Review colorectal
CRC and Endoscopy Darren Ballard, MD Assistant Professor Gastroenterology/Hepatology Medical College of Wisconsin Objectives Review background demographics and pathways for colon cancer Review colorectal
Hereditary GI tumor syndromes ACG guidelines of genetic testing and management. Dr. med. Henrik Csaba Horváth PhD
 Hereditary GI tumor syndromes ACG guidelines of genetic testing and management Dr. med. Henrik Csaba Horváth PhD Genetic testing and management of hereditary GI tumor syndromes June 29, 2016 2 Clinical
Hereditary GI tumor syndromes ACG guidelines of genetic testing and management Dr. med. Henrik Csaba Horváth PhD Genetic testing and management of hereditary GI tumor syndromes June 29, 2016 2 Clinical
Structured Follow-Up after Colorectal Cancer Resection: Overrated. R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007
 Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
Colorectal Cancer: Screening & Surveillance
 Objectives Colorectal Cancer: Screening & Surveillance Chanda K. Ho, MD MPH Advances in Internal Medicine Brief overview epidemiology and pathogenesis of colorectal cancer (CRC) To review screening modalities
Objectives Colorectal Cancer: Screening & Surveillance Chanda K. Ho, MD MPH Advances in Internal Medicine Brief overview epidemiology and pathogenesis of colorectal cancer (CRC) To review screening modalities
CHEMOTHERAPY FOR COLON CANCER OUTLINE OF TODAY S TALK. Colon Cancer Epidemiology 11/6/2012 GATRA/GCCR FALL CONFERENCE NOVEMBER 14 16, 2012
 CHEMOTHERAPY FOR COLON CANCER JONATHAN C. BENDER,MD MEDICAL DIRECTOR OF PIEDMONT FAYETTE CANCER CENTER OUTLINE OF TODAY S TALK 1. Overview of Colon Cancer in the US 2. Colon Cancer staging and risks of
CHEMOTHERAPY FOR COLON CANCER JONATHAN C. BENDER,MD MEDICAL DIRECTOR OF PIEDMONT FAYETTE CANCER CENTER OUTLINE OF TODAY S TALK 1. Overview of Colon Cancer in the US 2. Colon Cancer staging and risks of
Universal Screening for Lynch Syndrome
 Universal Screening for Lynch Syndrome St. Vincent/Ameripath protocol proposal Lynch syndrome (HNPCC) 1/35 individuals with colorectal cancer has Lynch syndrome Over half individuals are >50 at time of
Universal Screening for Lynch Syndrome St. Vincent/Ameripath protocol proposal Lynch syndrome (HNPCC) 1/35 individuals with colorectal cancer has Lynch syndrome Over half individuals are >50 at time of
Classification of polyposis syndromes two major groups. Adenomatous polyposis syndromes. Hamartomatous polyposis syndromes
 Hereditary polyposis syndromes Classification of polyposis syndromes two major groups adenomatous and non-adenomatous polyposis syndromes Adenomatous polyposis syndromes Familial adenomatous polyposis(fap)
Hereditary polyposis syndromes Classification of polyposis syndromes two major groups adenomatous and non-adenomatous polyposis syndromes Adenomatous polyposis syndromes Familial adenomatous polyposis(fap)
Colon Cancer Update Christie J. Hilton, DO
 POMA Winter Conference Christie Hilton DO Medical Oncology January 2018 None Colon Cancer Numbers Screening (brief update) Practice changing updates in colon cancer MSI Testing Immunotherapy in Colon Cancer
POMA Winter Conference Christie Hilton DO Medical Oncology January 2018 None Colon Cancer Numbers Screening (brief update) Practice changing updates in colon cancer MSI Testing Immunotherapy in Colon Cancer
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
LET S TALK ABOUT CANCER
 LET S TALK ABOUT CANCER COLORECTAL CANCER AND CROHN S DISEASE & ULCERATIVE COLITIS crohnsandcolitis.ca BACKGROUND Colorectal cancer is the second-leading cause of cancer death in this country. In 2013,
LET S TALK ABOUT CANCER COLORECTAL CANCER AND CROHN S DISEASE & ULCERATIVE COLITIS crohnsandcolitis.ca BACKGROUND Colorectal cancer is the second-leading cause of cancer death in this country. In 2013,