Crossroads Congress in Cardiothoracic Surgery Athens 2018 Malignant Pleural Mesothelioma in the UK: Current Research and Experience
|
|
|
- Sheena Greer
- 5 years ago
- Views:
Transcription
1 Crossroads Congress in Cardiothoracic Surgery Athens 2018 Malignant Pleural Mesothelioma in the UK: Current Research and Experience Mr Apostolos Nakas Consultant Thoracic Surgeon Head of Department of Thoracic Surgery Glenfield Hospital University Hospitals of Leicester NHS Trust United Kingdom
2 Declarations of Interest Investigator in MARS 2, MesoTRAP, MiST, MEDUSA studies Member of BTS Mesothelioma Guidelines Development Group Lead Clinician for East Midlands Cancer Network Mesothelioma Expert Clinical Advisory Group and Regional Mesothelioma MDT Received training related sponsorship from Medtronics, Ethicon, Synthes Received Honoraria related to educational and proctorship activities from Johnson and Johnson, KLS Martin Gmbh and Lynton Lasers Ltd I am a Surgeon and openly support Surgery for MPM


3 Sir William Osler, Medicine is a science of uncertainty and an art of probability The greater the ignorance, the greater the dogmatism
4 Epidemiology and pathogenesis

5 Epidemiology and Incidence Relationship of pleural malignancy with Asbestos Exposure was first recognized in 1906 ( textile workers) 1920: DuBray, first use of term Mesothelioma to describe pleural malignancy In 1986 Wagner et al demonstrated the epidemiologic relationship between exposure and MPM Klerk and Armstrong in 1992 reported the significance of the type of asbestos fibre in the development of the disease.

6 563 new cases in the UK in 2002 The annual number of mesothelioma deaths has increased from 153 in 1968 to 1874 in 2003 and to 2,500 in 2014 The latest projections suggest that the annual total number of mesothelioma deaths in Great Britain is estimated to peak at around 2,500 deaths some time after new cases per year in US Epidemiology and Incidence Estimated DEATHS in Western Europe over the next 30 years
7 MPM IN GB 2014: HSE
8 Epidemiology and Incidence Amphibole Fibres: Small Fibres MPM Crocidolite (Blue Asbestos) Amosite Tremolite Anthophyllite Actinolite Serpentine Fibres Large fibres Lung Chrysotile Cancer
9 Epidemiology and Incidence Less common causes of MPM Radiation exposure years before MPM occurs Beryllium Liquid Paraffin TB Pleuritis Recurrent Lung Infections Shoe Industry, Petrochemical workers, Stone Cutters Genetic Predisposition
10 Peak Age 7 th Decade of Life Male:Female ratio 5: years latency period It can occur in childhood Epidemiology and Incidence
11 Histopathology

12 Pathology Epithelioid (50%) Sarcomatoid (16%) Biphasic (34%) The histologic appearance of MPM is easily confused with that of other neoplasms. Immunohistochemistry is very often essential for diagnosis.





13 Molecular Biology Relatively little is understood Asbestos is thought to cause DNA damage partly through the production of free radicals from the iron contained in asbestos fibres. Multiple chromosomal changes can occur in combination suggesting a genetic cascade involvement Overexpression of PDGF? SV 40 virus synergistic role (contaminated polio vaccines 1950s)

14 Diagnosis and staging

15 Clinical Presentation Insidious Onset Pleural effusion and dyspnea Chest Discomfort Severe Chest Pain Mediastinal Shift and compression of contralateral lung Weight Loss Cough Weakness Dysphagia Haemoptysis Hoarseness


16 Radiological Features Pleural Effusion Localised Tumour


17 Radiological Features Mediastinal Pleural Thickening


18 Radiological Features Pleural Effusion Pleural Thickening Pleural based mass Mediastinal Thickening/ Infiltration Mediastinal Adenopathy Pericardial Effusion Diaphragmatic Infiltration
 Total Glycolytic Volume might be useful for")
19 CT PET Scanning for MPM Useful in detecting distant disease (10% undetected on CT) Not useful in assessing locoregional disease ( local tumor extension and mediastinal nodal involvement) Total Glycolytic Volume might be useful for prognosis

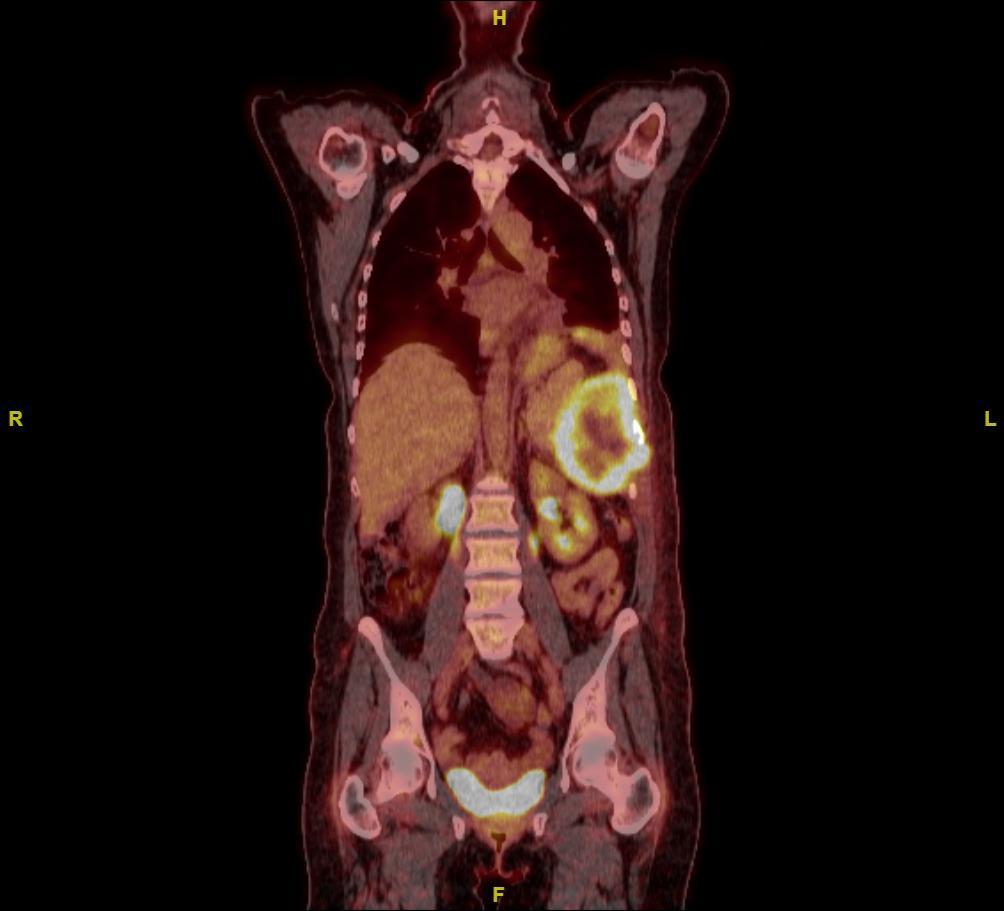
20 PET in Localized MPM
 essential for: Treatment")
21 Diagnosis Thoracentesis is usually the first diagnostic attempt 30-50% cytology is positive for malignancy though rarely diagnostic for MPM and cannot diagnose subtype Thoracoscopy is diagnostic in 80% of cases Open biopsy when pleural space is obliterated Tissue subtyping (Epithelioid/ Biphasic/ Sarcomatoid) essential for: Treatment Prognosis Survival

22 T: Tx T0 T1 ipsilateral parietal pleura +/- visceral (a,b) T2 T1 + at least 1 of: fissure, diaphragm, lung parenchyma T3 T1 + at least 1 of: endothoracic fascia, mediastinal fat, chest wall, non trans pericardium T4 chest wall, rib, peritoneum, mediastinum, contralateral pleura, positive pericardial effusion, brachial plexus N:Nx N1 Ipsilateral bronchopulmonary and/ or hilar N2 Subcarinal and or IMA LN N3 contralateralmediastinal, ipsilateral SC M:Mx M0 M1 Staging AJCC / UICC/ IMIG (1995)
23 Primary tumor T0 No evidence of primary tumor T1 Tumor involves ipsilateral parietal pleura AJCC-UICC MPM Staging System 8 th Revision T1a T1b T2 T3 T4 Tumor involves ipsilateral parietal (mediastinal, diaphragmatic) pleura with no involvement of the visceral pleura Tumor involves ipsilateral parietal (mediastinal, diaphragmatic) pleura with focal involvement of visceral pleura Tumor involves any of the ipsilateral pleural surfaces with at least one of the following: invasion of diaphragmatic muscle extension into the lung parenchyma Describes locally advanced but potentially resectable tumor (i.e., it might be possible to remove it) Tumor involves any of the ipsilateral pleural surfaces with at least one of the following: invasion of the endothoracic fascia invasion into mediastinal fat solitary, completely resectable focus of tumor invading the soft tissues of the chest wall non-transmural involvement of the pericardium Describes locally advanced technically unresectable tumor (i.e., it cannot be removed) Tumor involves any of the ipsilateral pleural surfaces with at least one of the following: diffuse or multifocal masses in the chest wall (with or without rib destruction) invasion through the diaphragm to the peritoneum direct extension to the contralateral pleura extension to mediastinal organs invasion into the spine extension through the internal surface of the pericardium (with or without a pericardial effusion or involvement of the myocardium)
24 Regional lymph nodes (N) N0 N1 N1 N2 No regional lymph node metastasis Metastasis in the ipsilateral bronchopulmonary and/or hilar lymph nodes Metastasis in the subcarinal lymph nodes, ipsilateral internal mammary, mediastinal lymph nodes, or the peridiaphragmatic lymph nodes Metastases in the contralateral mediastinal, contralateral internal mammary, or hilar lymph nodes and/or the ipsilateral supraclavicular or scalene lymph nodes AJCC- UICC MPM Staging System 8 th Revision
25 AJCC-UICC MPM Staging System 8 th Revision Distant metastases (M) M0 M1 No distant metastases Distant metastases present
26 Group Stage AJCC-UICC MPM Staging System 8 th Revision IA IB II IIIA IIIB T1, N0 T2,T3, N0 T1, T2, N1 T3, N1 T1, T2, T3, N2 IV Any T, Any N, M1
27 National Lung Cancer audit Mesothelioma Report 2018
28 2018 NLCA Mesothelioma Audit ( data) No of UK cases:7,192 (3 years) Pleural: 6,932 (96%) Peritoneal: 260 (4%) 84% male 46 % Disease Stage not recorded 31% PS not recorded 51% PS % PS2 11% PS3-4 46% of cases NOT subtyped MDT :81% LCNS input: 28-93% (Avg for England 54%) Chemo: 40% Anticancer Treatment:51% Radical Surgery: 4% 1 year Survival: 38% 3 year Survival: 7%
29 2018 NLCA Mesothelioma Audit ( data) Pathology 1 year survival 3 year survival Median survival (days) Epithelioid 51% 3% 400( ) Biphasic 28% 1% 243( ) Sarcomatoid 14% 1% 133(69-249) Unspecified 29% 2% 195(69-447)
30 Treatment options

31 Treatment Options Surgery Radiation Therapy Chemotherapy Immunotherapy Supportive Care Combinations

32 Surgery Part 1: Radical Aims to extend survival Aims to remove all disease achieving Macroscopic Complete Resection (R1)
33 Surgery Part 2: Non Radical Diagnosis Staging Effusion control Dyspnoea Control Pain Control Survival Benefit

34 Procedures on offer VATS Biopsy and Pleurodesis VATS Decortication Open Decortication Extended Pleurectomy Decortication Extrapleural Pneumonectomy + Cervical Mediastinoscopy Staging Thoracoscopy Staging Laparoscopy Airway Stenting Oesophageal Stenting IC Chemotherapy PDT
35 1. Vats Biopsy and talc
 Drainage of Effusion Targeted Biopsies (4-5, deep layer) <5 grs")
36 1. VATS Pleural Biopsy +/- Talc Pleurodesis Single 2 cm port access (in line of thoracotomy) Drainage of Effusion Targeted Biopsies (4-5, deep layer) <5 grs talc
37 1. VATS Bx + Talc Advantages 1. Minimal Surgical Insult, Can be tolerated by most of the patients 2. Targeted biopsies, high diagnostic yield 3. Biopsy and effusion control achieved in one procedure 4. Radical surgery can still be performed at a latter stage Disadvantages 1. Palliative procedure, median survival similar to natural progress of disease 2. General Anaesthetic 3. If lung is trapped pleurodesis will fail: 1. IPC 2. VATS PD
38 1. VATS Bx + Talc Evidence 1. Phase III intergroup study of talc poudrage vs talc slurry sclerosis for malignant pleural effusion. Dresler et al, Chest RCT, Insufflation vs slurry, 480 pts 2. Similar efficacy, insufflation might be better in lung cancer or breast Not much Evidence 1. We need the biopsies 1. Guide Treatment 2. Inform prognosis 2. We might need to have a look (+/- feel) 3. Collapsed Lung makes assessment easier 4. We choose where to do the incision
39 2. Vats Pleurectomy Decortication

40 2. VATS Pleurectomy Decortication Three 2 cm ports Parietal Pleurectomy Visceral Decortication Debulking Lung re expansion
41 2. VATS P/D Advantages 1. Elderly patients 2. Lung re expansion might (?) achieve better effusion control 3. Could (?) be superior to VATS talc pleurodesis in effusion/ pain/ dyspnoea control 1. Significant mortality 2. Prolonged Air Leak Disadvantages 3. Difficulty in debulking mediastinum/ diaphragm 4. Not suitable for bulky disease 5. Unlikely to prolong survival If lung does not expand conversion to Open P/D might be necessary
42 2. VATS P/D Evidence 1. Efficacy and cost of video-assisted thoracoscopic partial pleurectomy versus talc pleurodesis in patients with malignant pleural mesothelioma (MesoVATS): an open-label, randomised, controlled trial, RC Rintoul et al, Lancet 2014: RCT, 175 pts, no benefit in survival and worse complications and LOS in VATS PD group Not much Evidence 1. Operation Relevant in the EPP era, not relevant now 2.? Group of patients? Radical Surgery offered to octogenarians
43 196 patients recruited as planned, 98 each arm, 9 years 11% in VATS PP and 10% in Pleurodesis arm did not have MPM leaving 87 and 88 pts respectively. 12/12/ deaths: 48% VATS PP, 43% Talc, 12/12 survival: 52% vs 57%, median 13.1 vs 13.5, HR 1.04, 95% CI , p=0.81. MesoVATS: Results 16% and 17% respectively withdrew from study or did not attend final appointment Secondary outcomes at 12 months were available for 34 (39%) of patients in VATS PP and 37 (42%) in Talc group. VAT PP group had better effusion control at 1 and 6 months but not at 3 and 12! QoL similar Higher FEV1 and greater distance on SWT but only 36 patients had SWT. Longer Hospital stay (7 vs 3 days) and more complications on VAT PP Mean cost of VAT PP was 3,800 higher per case on average. VAT PP offered the equivalent of 12.5 days of full health (0.035 QALYs)
44 3. Simple Pleurectomy Decortication
45 3. Simple Pleurectomy Decortication Thoracotomy and full (?) pleurectomy/ decortication Spares diaphragm and pericardium: likely to leave>r2 disease Aims to debulk disease and re expand the lung
46 3. Simple P/D Advantages 1. Easier to achieve lung expansion than VATS P/D 2. Avoids complications associated with diaphragmatic/ pericardial resection 3. Spares the lung compared to EPP 4. Might (?) achieve macroscopic clearance in very few early cases Disadvantages 1. Adds thoracotomy to surgical insult 2. Pericardium and diaphragm are usually heavily involved in MPM 3. If we accept that macroscopic clearance is important we need to consider Extended Pleurectomy Decortication
47 3. Simple P/D Evidence 1. Systematic review of pleurectomy in the treatment of malignant pleural mesothelioma, Cao et al, Lung Cancer 2013: Evidence from the existing literature suggests that selected patients who undergo extended P/D may achieve a longer overall and disease-free survival compared to patients who undergo less aggressive procedures such as P/D or partial pleurectomy. However, this may be associated with higher morbidity and longer hospitalization. Not much Evidence 1. Acceptable (?) Compromise if EPD not feasible intraoperatively 2. Patients suitable for Simple PD will be suitable for EPD 3. Macroscopic Complete Resection makes more sense than leaving disease behind
48 4. Extended Pleurectomy Decortication

49 4. Extended PD (EPD) P/D that removes ALL macroscopic disease Full parietal pleurectomy Visceral decortication extending into fissures Removal of pericardium and diaphragm and reconstruction with synthetic/ biological patches
50 4. EPD Advantages 1. Spares the lung 2. Achieves macroscopic clearance 3. Suitable for patients who would not tolerate pneumonectomy 4. Probably more suitable for elderly patients 5. Significantly less morbidity, complications and impact on QoL than EPP Disadvantages 1. Prolonged air leak and pleural sepsis secondary to prolonged drainage 2. Significant blood loss and perioperative mortality (2-7%) 3. Patients need to be fit for surgery 4. Technically demanding, better results in high volume centres 5. Presence of lung does not allow hemithorax radiotherapy 6. If disease involves the lung parenchyma extensively EPP might be necessary (?).
51 4. EPD Evidence 1. A systematic review and meta-analysis of surgical treatments for malignant pleural mesothelioma, Cao et al, Lung Cancer 2014: results of the present meta-analysis suggested that extended P/D can be performed with lower morbidity and mortality outcomes, as well as comparable long-term survival outcomes to EPP. However, it is important to emphasize that EPP and extended P/D are not interchangeable procedures for all patients, and that individualized treatment plans should be based on the extent of disease, patient comorbidities and surgeon's experience. Not much Evidence 1. MPM is not Lung Cancer: the lung can be spared 2. Pneumonectomy is (?) a disease in itself 3. If volume of disease is associated with outcome (TGV, response to chemo, RECIST criteria), surely removing all disease makes sense(?) 4. Cytoreduction works in other diffuse malignancies (ovarian, pseudomyxoma)
52 2 stage (registration followed by randomization) unblinded two-arm parallel design randomized trial EPD+ Chemotherapy versus Chemotherapy (2+4 Cisplatin Pemetrexed) Feasibility: 50 patients in 2 years or recruit 25 patients in any 6 month period: Completed Full Study 285 within 5 years (Total 335 including the 50 from pilot study) MARS 2 Trial 4 Surgical Centres: Leicester Sheffield London Glasgow Methodology: Assessment, consent, Chemotherapy 2 cycles CT week 5, MDT week 6,if patient randomized to non surgical arm 4 more cycles of chemo starting week7-8

53 MARS2 Recruitment Aug 2018 Centre Jun 18 Jul 18 Aug 18 Number randomised Clatterbridge Leicester Derby Barts Wythenshawe Papworth Royal Marsden Colchester Sheffield Glasgow Beatson South Tees South Tyneside Wolverhampton Royal Gwent Leeds Peterborough Bristol Cardiff Norwich Barking Plymouth Overall
54 MARS 2 Inclusion / Exclusion Criteria Inclusion 1. Histological confirmation of Mesothelioma 2. Disease confined to one hemithorax Exclusion 1. Unable to give informed consent 2. Unwillingness to randomization 3. Unresectable disease 4. ECOG>=2 5. ppofev1/ TLCO<20% 6. Severe Heart Failure (EF<30%) 7. End Stage CKD requiring dialysis 8. Liver Failure 9. Participants in other interventional clinical trial
 Progression on chemotherapy Age>80 Absolute Contraindications: EPD Selection Criteria True T4/ N3/ M1")
55 T3N2M0 T3/4 not clearly defined PS<=1 Normal Cardiac Function Sterile Pleural Space Relative Contraindications: Sarcomatoid (include in MARS 2) Progression on chemotherapy Age>80 Absolute Contraindications: EPD Selection Criteria True T4/ N3/ M1 Infected Space

56 Resectability: Factors Thickness Hardness Subclavian Vessels SVC IVC Chest Wall Lung Pericardium Heart Spine

57 Operability: Factors PFTs Cardiac Reserve Previous Thoracic Operations CABG Pulmonary Procedures Presence of Infection Cell Type Time from Pleurodesis/ chemotherapy Progression on chemotherapy Age
58 EPP n=112 EPD n=140 Overall n=252 Median Survival months SE 95% CI 1 year % (pts at risk) % (82) 60% (73) 2 years % (pts at risk) 40% (45) 31% (33) 3 years % (pts at risk) 20% (23) 21% (19) 4 years % (pts at risk) 15% (15) 12% (10) 5 years % (pts at risk) 11% (10) 5% (3) Predictors of long-term survival following radical surgery for malignant pleural mesothelioma. Nakas A. et al, Eur J Cardiothorac Surg Sep;46(3):380-5 Survival following Radical Surgery: EPP no different to EPD, p=0.92
59 Predictors of long-term survival following radical surgery for malignant pleural mesothelioma. Nakas A. et al, Eur J Cardiothorac Surg Sep;46(3):380-5 Chemotherapy (n = 230) No chemo (n = 102) Chemo (n = 128) Median survival SE 95% CI Total Significance, P year survival (patients at risk) 51% 47 81% 99 2 years survival (patients at risk) 26% 23 43% 47 3 years survival (patients at risk) 12% 10 28% 29 4 years survival (patients at risk) 7% 4 20% 19 5 years survival (patients at risk) 3% 2 12% 10 Multimodality treatment?
60 5. Pleuropneumonectomy

61 5. Pleuropneumonectomy, aka Extra Pleural Pneumonectomy (EPP) En bloc removal of pleura, lung pericardium and diaphragm. Reconstruction of pericardium and diaphragm with synthetic patches
62 5. EPP Advantages 1. Maximum cytoreduction (but not necessarily better than Extended P/D) 2. Empty Hemithorax can be treated with High Dose Radiotherapy (albeit with risk of complications) 3. Not complicated by air leak Disadvantages 1. Not suitable for N2 disease (debatable) 2. Adds pneumonectomy to an already major operation 3. Space problems 4. High morbidity (40-60%) and mortality (6-7%) rates 5. Removal of lung compromises QoL 6. Patient should be able to tolerate pneumonectomy 7. High morbidity will result in less patients completing trimodality treatment.
63 5. EPP Evidence 1. Extra-pleural pneumonectomy versus no extra-pleural pneumonectomy for patients with malignant pleural mesothelioma: clinical outcomes of the Mesothelioma and Radical Surgery (MARS) randomised feasibility study. T. Treasure et al, Lancet Oncol 2011: In view of the high morbidity associated with EPP in this trial and in other nonrandomised studies a larger study is not feasible. These data, although limited, suggest that radical surgery in the form of EPP within trimodal therapy offers no benefit and possibly harms patients. Not much Evidence 1. MPM is not Lung Cancer: the lung can be spared 2. Pneumonectomy is (?) a disease in itself 3. EPP is technically easier than EPD 4. EPP can be part of 3modality, EPD not. 5. EPP is dead?
64 MARS Feasibility Trial: Lancet Oncology 2011 Feasibility study: objective was to recruit 50 patients in one year to EPP or no EPP and to measure clinical outcomes It was estimated that the power required for the main trial to show difference between EPP and no EPP would be 670 patients. 12 UK hospitals 3 cycles of platinum based chemotherapy after randomization followed by EPP and hemithorax irradiation or no EPP
65 112 patients registered Oct 2005-Nov randomized to EPP (n=24) or no EPP (n=26) 24 assigned to EPP: 5 EPP not started MARS Trial: Results 3 patient refusal 2 clinical decision 3 EPP abandoned 1 perioperative death 2 unexpected disease progression 16 had EPP 11 postoperative complications 8 received Radical Radiotherapy 8 did not receive Radical Radiotherapy 1 clinical decision 2 toxicity 2 disease progression 3 died
66 MARS Trial: Results EPP median survival 14.4 months vs 19.5 months for no EPP HR for EPP 2.75 ( , p=0.016) 30 day mortality 10.5% (2/19 patients that EPP was started) 1 more patient died 6/52 post op from pneumonia Conclusion was that EPP within trimodality therapy offers no benefit and potentially harms patients
67 And the reaction was: The MARS study did not show the feasibility of doing a trial comparing chemotherapy with EPP and radiotherapy. We believe the interpretation of the study These data, although limited, suggest that radical surgery in the form of EPP within trimodal therapy offers no benefit and possibly harms patients is inappropriate, could move clinical research for mesothelioma in the wrong direction, and might be harmful to patients seeking advice. Walter Weder, Rolf A Stahel, Paul Baas, Urania Dafni, Marc de Perrot, Brian C McCaughan, Takashi Nakano, Harvey I Pass, Bruce W S Robinson, Valerie W Rusch, David J Sugarbaker, Nico van Zandwijk


68 Accelerated hemithoracic radiation followed by extrapleural pneumonectomy for malignant pleural mesothelioma, deperrot et al, JTCVS /256 patients with MPM 25 Gy over 5 days+5 Gy to volumes at high risk EPP within 6+/-2 days Operative Mortality 1.6% 94% Stage III-IV, 52% ypn2 Median survival 36 months (66% 3y with ypn0 Epithelioid disease)
69 Which operation?
70 Therapeutic Procedures for MPM: From 5 to 2 1. VATS Pleural Biopsy +/- Talc Pleurodesis 2. VATS Pleurectomy/ Decortication 3. Open Non Radical Pleurectomy/ Decortication 4. Extended Pleurectomy Decortication 5. Pleuropneumonectomy
71 Trials MARS 2 Pilot (n=50) completed N=161 Recruited Aug 2018 Target: 335 Should report in 3 years (2021) MesoTRAP A pilot clinical trial and feasibility study comparing video-assisted thoracoscopic partial pleurectomy/decortication with indwelling pleural catheter in patients with trapped lung due to malignant pleural mesothelioma designed to address recruitment and randomisation uncertainties and sample size requirements for a phase III trial. (n=38 pts) i) What are the standard deviations of Visual Analogue Scale scores for dyspnoea in each treatment group following randomisation? ii) Will patients accept randomisation to IPC or VAT-PD in a real life trial situation? iii) How prevalent is trapped lung in MPM?
72 The future
73 1. VATS P/D has a very limited role to play in the elderly and unfit for radical surgery patients.. 2. If we have to perform a thoracotomy Radical P/D (EPD) is preferable to Non Radical P/D 3. Radical P/D is not inferior to EPP in survival and is a sensible option even in the presence of pn2 disease 4. Radical P/D can be offered to an older age group than EPP 5. Macroscopic (R1) resection is the key target of Radical Surgery Conclusions 6. Clinical Nodal Staging is not accurate therefore patients should not be denied radical surgery on the basis of this. 7. Pathological staging descriptors need modifications to improve accuracy 8. Surgical Centre experience is important: Surgical expertise and aggressive perioperative management of complications can drastically decrease mortality and increase percentage of patients undergoing radical surgery. 9. Beneficial effect of Radical Surgery will be tested in MARS 2 trial.
 Develop Regional MPM MDTs to improve access to treatment")
74 Training Be open and honest with ourselves: avoid surgical hubris Quality Control The (bright) future of Surgery for MPM Ensure equal access to treatment Engage with MPM patients and support groups Audited Results Trials with new regimes of multimodality treatment Remember that the whole team will need development, not just the surgeon(s) Develop Regional MPM MDTs to improve access to treatment and share expertise

75 Hippocrates, BC Life is short, and art long, opportunity fleeting, experimentations perilous, and judgement difficult.
76 Thank You
North of Scotland Cancer Network Clinical Management Guideline for Mesothelioma
 THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Mesothelioma [Based on WOSCAN SCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED WHEN PRINTED Document
THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Mesothelioma [Based on WOSCAN SCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED WHEN PRINTED Document
The surgeon: new surgical aproaches
 The surgeon: new surgical aproaches Paul Van Schil, MD Department of Thoracic and Vascular Surgery Antwerp University, Belgium no disclosures, no conflict of interest Malignant pleural mesothelioma: clinical,
The surgeon: new surgical aproaches Paul Van Schil, MD Department of Thoracic and Vascular Surgery Antwerp University, Belgium no disclosures, no conflict of interest Malignant pleural mesothelioma: clinical,
The Imaging Journey of Patients with Malignant Pleural Mesothelioma: Experience of a Tertiary Mesothelioma MDT
 The Imaging Journey of Patients with Malignant Pleural Mesothelioma: Experience of a Tertiary Mesothelioma MDT V. Lam, J. Brozik, A. J. Sharkey, A. Bajaj, D. T. Barnes Glenfield Hospital, Leicester, United
The Imaging Journey of Patients with Malignant Pleural Mesothelioma: Experience of a Tertiary Mesothelioma MDT V. Lam, J. Brozik, A. J. Sharkey, A. Bajaj, D. T. Barnes Glenfield Hospital, Leicester, United
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES LUNG SITE MESOTHELIOMA Lung Site Group Mesothelioma Authors: Dr. Meredith Giuliani, Dr. Andrea Bezjak 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES LUNG SITE MESOTHELIOMA Lung Site Group Mesothelioma Authors: Dr. Meredith Giuliani, Dr. Andrea Bezjak 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
Slide 1. Slide 2. Slide 3. Investigation and management of lung cancer Robert Rintoul. Epidemiology. Risk factors/aetiology
 Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
An Update: Lung Cancer
 An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
Malignant Effusions. Anantham Devanand Respiratory and Critical Care Medicine Singapore General Hospital
 Malignant Effusions Anantham Devanand Respiratory and Critical Care Medicine Singapore General Hospital Malignant Effusions Definition: Presence of malignant cells in the pleural space 75% are caused by
Malignant Effusions Anantham Devanand Respiratory and Critical Care Medicine Singapore General Hospital Malignant Effusions Definition: Presence of malignant cells in the pleural space 75% are caused by
Pleurectomy/decortication versus extrapleural pneumonectomy: a critical choice
 Editorial Pleurectomy/decortication versus extrapleural pneumonectomy: a critical choice Pier Luigi Filosso, Francesco Guerrera, Paolo Olivo Lausi, Roberto Giobbe, Paraskevas Lyberis, Enrico Ruffini, Alberto
Editorial Pleurectomy/decortication versus extrapleural pneumonectomy: a critical choice Pier Luigi Filosso, Francesco Guerrera, Paolo Olivo Lausi, Roberto Giobbe, Paraskevas Lyberis, Enrico Ruffini, Alberto
Video assisted thoracoscopic and open chest surgery in diagnosis and treatment of malignant pleural diseases
 Review Article on Thoracic Surgery Video assisted thoracoscopic and open chest surgery in diagnosis and treatment of malignant pleural diseases Periklis Perikleous, David A. Waller Department of thoracic
Review Article on Thoracic Surgery Video assisted thoracoscopic and open chest surgery in diagnosis and treatment of malignant pleural diseases Periklis Perikleous, David A. Waller Department of thoracic
Extrapleural Pneumonectomy: A Blessing or a Curse in the Management of Pleural Malignant Mesothelioma?
 Original Research Extrapleural Pneumonectomy: A Blessing or a Curse in the Management of Pleural Malignant Mesothelioma? PLEURA January-December 2015: 1-7 ª The Author(s) 2015 DOI: 10.1177/2373997515595219
Original Research Extrapleural Pneumonectomy: A Blessing or a Curse in the Management of Pleural Malignant Mesothelioma? PLEURA January-December 2015: 1-7 ª The Author(s) 2015 DOI: 10.1177/2373997515595219
Malignant Pleural Mesothelioma COMBINED TREATMENT
 Malignant Pleural Mesothelioma COMBINED TREATMENT Federica Grosso incidence Italy
Malignant Pleural Mesothelioma COMBINED TREATMENT Federica Grosso incidence Italy
Standardizing surgical treatment in malignant pleural mesothelioma
 Perspective Standardizing surgical treatment in malignant pleural mesothelioma David Rice University of Texas M.D. Anderson Cancer Center, Houston, TX, USA Corresponding to: David Rice. University of Texas
Perspective Standardizing surgical treatment in malignant pleural mesothelioma David Rice University of Texas M.D. Anderson Cancer Center, Houston, TX, USA Corresponding to: David Rice. University of Texas
Thoracic Surgery; An Overview
 Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer
 THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
Lung Cancer Clinical Guidelines: Surgery
 Lung Cancer Clinical Guidelines: Surgery 1 Scope of guidelines All Trusts within Manchester Cancer are expected to follow this guideline. This guideline is relevant to: Adults (18 years and older) with
Lung Cancer Clinical Guidelines: Surgery 1 Scope of guidelines All Trusts within Manchester Cancer are expected to follow this guideline. This guideline is relevant to: Adults (18 years and older) with
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
Role of Surgery in Management of Non Small Cell Lung Cancer. Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City
 Role of Surgery in Management of Non Small Cell Lung Cancer Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City Introduction Surgical approach Principle and type of surgery
Role of Surgery in Management of Non Small Cell Lung Cancer Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City Introduction Surgical approach Principle and type of surgery
Therapeutic Surgery for Nonepithelioid Malignant Pleural Mesothelioma: Is it Really Worthwhile?
 Therapeutic Surgery for Nonepithelioid Malignant Pleural Mesothelioma: Is it Really Worthwhile? Bram Balduyck, MD, Delphine Trousse, MD, Apostolos Nakas, MD, Antonio E. Martin-Ucar, MD, John Edwards, MD,
Therapeutic Surgery for Nonepithelioid Malignant Pleural Mesothelioma: Is it Really Worthwhile? Bram Balduyck, MD, Delphine Trousse, MD, Apostolos Nakas, MD, Antonio E. Martin-Ucar, MD, John Edwards, MD,
Surgical management of lung cancer
 Surgical management of lung cancer Nick Roubos FRACS Cardiothoracic Surgeon Box Hill Hospital, Epworth Eastern Thoracic Oncology Non Small Cell Lung Cancer (NSCLC) Small Cell Lung Cancer Mesothelioma Pulmonary
Surgical management of lung cancer Nick Roubos FRACS Cardiothoracic Surgeon Box Hill Hospital, Epworth Eastern Thoracic Oncology Non Small Cell Lung Cancer (NSCLC) Small Cell Lung Cancer Mesothelioma Pulmonary
Extended pleurectomy decortication for malignant pleural mesothelioma in the elderly: the need for an inclusive yet selective approach
 Interactive CardioVascular and Thoracic Surgery 25 (2017) 696 702 doi:10.1093/icvts/ivx221 Advance Access publication 21 July 2017 ORIGINAL ARTICLE Cite this article as: Sharkey AJ, Bilancia R, Tenconi
Interactive CardioVascular and Thoracic Surgery 25 (2017) 696 702 doi:10.1093/icvts/ivx221 Advance Access publication 21 July 2017 ORIGINAL ARTICLE Cite this article as: Sharkey AJ, Bilancia R, Tenconi
The Itracacies of Staging Patients with Suspected Lung Cancer
 The Itracacies of Staging Patients with Suspected Lung Cancer Gerard A. Silvestri, MD,MS, FCCP Professor of Medicine Medical University of South Carolina Charleston, SC silvestri@musc.edu Staging Lung
The Itracacies of Staging Patients with Suspected Lung Cancer Gerard A. Silvestri, MD,MS, FCCP Professor of Medicine Medical University of South Carolina Charleston, SC silvestri@musc.edu Staging Lung
GUIDELINES FOR CANCER IMAGING Lung Cancer
 GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
Video-assisted thoracoscopic PlasmaJet ablation for malignant pleural mesothelioma
 Case Report on Thoracic Surgery Page 1 of 5 Video-assisted thoracoscopic PlasmaJet ablation for malignant pleural mesothelioma Periklis Perikleous, Nizar Asadi, Vladimir Anikin Department of Thoracic Surgery,
Case Report on Thoracic Surgery Page 1 of 5 Video-assisted thoracoscopic PlasmaJet ablation for malignant pleural mesothelioma Periklis Perikleous, Nizar Asadi, Vladimir Anikin Department of Thoracic Surgery,
Malignant pleural mesothelioma (MPM) has a poor prognosis,
 has a poor prognosis,") ORIGINAL ARTICLE Outcome for Patients with Malignant Pleural Mesothelioma Referred for Trimodality Therapy in Western Australia Arman Hasani, MBBS, FRACP,* John M. Alvarez, MBBS, FRACS, Jenny Ma Wyatt,
ORIGINAL ARTICLE Outcome for Patients with Malignant Pleural Mesothelioma Referred for Trimodality Therapy in Western Australia Arman Hasani, MBBS, FRACP,* John M. Alvarez, MBBS, FRACS, Jenny Ma Wyatt,
Mediastinal Staging. Samer Kanaan, M.D.
 Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Protocol for the Examination of Specimens From Patients With Malignant Pleural Mesothelioma
 Protocol for the Examination of Specimens From Patients With Malignant Pleural Mesothelioma Based on AJCC/UICC TNM, 7th edition Protocol web posting date: February 1, 2011 Procedures Resection Authors
Protocol for the Examination of Specimens From Patients With Malignant Pleural Mesothelioma Based on AJCC/UICC TNM, 7th edition Protocol web posting date: February 1, 2011 Procedures Resection Authors
Thoracoscopic Lobectomy for Locally Advanced Lung Cancer. Masters of Minimally Invasive Thoracic Surgery Orlando September 19, 2014
 for Locally Advanced Lung Cancer Masters of Minimally Invasive Thoracic Surgery Orlando September 19, 2014 Thomas A. D Amico MD Gary Hock Endowed Professor and Vice Chair of Surgery Chief Thoracic Surgery
for Locally Advanced Lung Cancer Masters of Minimally Invasive Thoracic Surgery Orlando September 19, 2014 Thomas A. D Amico MD Gary Hock Endowed Professor and Vice Chair of Surgery Chief Thoracic Surgery
The Journal of Thoracic and Cardiovascular Surgery
 Accepted Manuscript Mesothelioma: Live to Fight Another Day Andrea S. Wolf, MD, Raja M. Flores, MD PII: S0022-5223(17)32747-2 DOI: 10.1016/j.jtcvs.2017.11.060 Reference: YMTC 12301 To appear in: The Journal
Accepted Manuscript Mesothelioma: Live to Fight Another Day Andrea S. Wolf, MD, Raja M. Flores, MD PII: S0022-5223(17)32747-2 DOI: 10.1016/j.jtcvs.2017.11.060 Reference: YMTC 12301 To appear in: The Journal
THORACIC MALIGNANCIES
 THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010
 LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
The 8th Edition Lung Cancer Stage Classification
 The 8th Edition Lung Cancer Stage Classification Elwyn Cabebe, M.D. Medical Oncology, Hematology, and Hospice and Palliative Care Valley Medical Oncology Consultants Director of Quality, Medical Oncology
The 8th Edition Lung Cancer Stage Classification Elwyn Cabebe, M.D. Medical Oncology, Hematology, and Hospice and Palliative Care Valley Medical Oncology Consultants Director of Quality, Medical Oncology
T3 NSCLC: Chest Wall, Diaphragm, Mediastinum
 for T3 NSCLC: Chest Wall, Diaphragm, Mediastinum AATS Postgraduate Course April 29, 2012 Thomas A. D Amico MD Professor of Surgery, Chief of Thoracic Surgery Duke University Health System Disclosure No
for T3 NSCLC: Chest Wall, Diaphragm, Mediastinum AATS Postgraduate Course April 29, 2012 Thomas A. D Amico MD Professor of Surgery, Chief of Thoracic Surgery Duke University Health System Disclosure No
Systemic Management of Malignant Pleural Mesothelioma
 ESO-ESMO EASTERN EUROPE AND BALKAN REGION MASTERCLASS IN MEDICAL ONCOLOGY 15.June-19.June 2018 Belgrade, Serbia Systemic Management of Malignant Pleural Mesothelioma Dragana Jovanovic University Hospital
ESO-ESMO EASTERN EUROPE AND BALKAN REGION MASTERCLASS IN MEDICAL ONCOLOGY 15.June-19.June 2018 Belgrade, Serbia Systemic Management of Malignant Pleural Mesothelioma Dragana Jovanovic University Hospital
Lung Cancer: Determining Resectability
 Lung Cancer: Determining Resectability Leslie E. Quint lequint@umich.edu No disclosures Lung Cancer: Determining Resectability AIM: Review imaging features that suggest resectability / unresectability
Lung Cancer: Determining Resectability Leslie E. Quint lequint@umich.edu No disclosures Lung Cancer: Determining Resectability AIM: Review imaging features that suggest resectability / unresectability
Surgery for early stage NSCLC
 1-3 March 2017, Manchester, UK Surgery for early stage NSCLC Dominique H. Grunenwald, MD, PhD Professor Emeritus in Thoracic and Cardiovascular surgery Pierre & Marie Curie University. Paris. France what
1-3 March 2017, Manchester, UK Surgery for early stage NSCLC Dominique H. Grunenwald, MD, PhD Professor Emeritus in Thoracic and Cardiovascular surgery Pierre & Marie Curie University. Paris. France what
Accepted Manuscript. Surgery for mesothelioma: less is more, more or less. Steven Milman, MD, Thomas Ng, MD
 Accepted Manuscript Surgery for mesothelioma: less is more, more or less Steven Milman, MD, Thomas Ng, MD PII: S0022-5223(17)32706-X DOI: 10.1016/j.jtcvs.2017.11.029 Reference: YMTC 12266 To appear in:
Accepted Manuscript Surgery for mesothelioma: less is more, more or less Steven Milman, MD, Thomas Ng, MD PII: S0022-5223(17)32706-X DOI: 10.1016/j.jtcvs.2017.11.029 Reference: YMTC 12266 To appear in:
Original Article. Keywords: Mesothelioma; surgery; platelet
 Original Article Clinical role of a new prognostic score using platelet-tolymphocyte ratio in patients with malignant pleural mesothelioma undergoing extrapleural pneumonectomy Tetsuzo Tagawa 1,2, Masaki
Original Article Clinical role of a new prognostic score using platelet-tolymphocyte ratio in patients with malignant pleural mesothelioma undergoing extrapleural pneumonectomy Tetsuzo Tagawa 1,2, Masaki
Malignant pleural mesothelioma: key determinants in tailoring the right treatment for the right patient
 Editorial Malignant pleural mesothelioma: key determinants in tailoring the right treatment for the right patient Ori Wald, David J. Sugarbaker Division of General Thoracic Surgery, Michael E. DeBakey
Editorial Malignant pleural mesothelioma: key determinants in tailoring the right treatment for the right patient Ori Wald, David J. Sugarbaker Division of General Thoracic Surgery, Michael E. DeBakey
Understanding Pleural Mesothelioma
 Understanding Pleural Mesothelioma UHN Information for patients and families Read this booklet to learn about: What is pleural mesothelioma? What causes it? What are the symptoms? What tests are done to
Understanding Pleural Mesothelioma UHN Information for patients and families Read this booklet to learn about: What is pleural mesothelioma? What causes it? What are the symptoms? What tests are done to
Malignant pleural mesothelioma: Role of MDCT in early diagnosis and prediction of resectability for radical surgery
 Malignant pleural mesothelioma: Role of MDCT in early diagnosis and prediction of resectability for radical surgery Poster No.: C-0890 Congress: ECR 2010 Type: Educational Exhibit Topic: Chest Authors:
Malignant pleural mesothelioma: Role of MDCT in early diagnosis and prediction of resectability for radical surgery Poster No.: C-0890 Congress: ECR 2010 Type: Educational Exhibit Topic: Chest Authors:
Collaborative Stage. Site-Specific Instructions - LUNG
 Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
The role of surgical resection in the management of malignant
 ORIGINAL ARTICLE Frequency of Use and Predictors of Cancer-Directed Surgery in the Management of Malignant Pleural Mesothelioma in a Community-Based (Surveillance, Epidemiology, and End Results [SEER])
ORIGINAL ARTICLE Frequency of Use and Predictors of Cancer-Directed Surgery in the Management of Malignant Pleural Mesothelioma in a Community-Based (Surveillance, Epidemiology, and End Results [SEER])
Chemotherapy Induced Pathologic Complete Response in Malignant Pleural Mesothelioma. A Review and Case Report
 STATE OF THE ART: CONCISE REVIEW Chemotherapy Induced Pathologic Complete Response in Malignant Pleural Mesothelioma A Review and Case Report Cecilia Bech, MD, and Jens Benn Sørensen, MD, DMSc, MPA Introduction:
STATE OF THE ART: CONCISE REVIEW Chemotherapy Induced Pathologic Complete Response in Malignant Pleural Mesothelioma A Review and Case Report Cecilia Bech, MD, and Jens Benn Sørensen, MD, DMSc, MPA Introduction:
Prevalence and Pattern of Lymph Node Metastasis in Malignant Pleural Mesothelioma
 Prevalence and Pattern of Lymph Node Metastasis in Malignant Pleural Mesothelioma Abdel Rahman M. Abdel Rahman, MD, Rabab M. Gaafar, MD, Hoda A. Baki, MD, Hesham M. El Hosieny, MD, Fatma Aboulkasem, MD,
Prevalence and Pattern of Lymph Node Metastasis in Malignant Pleural Mesothelioma Abdel Rahman M. Abdel Rahman, MD, Rabab M. Gaafar, MD, Hoda A. Baki, MD, Hesham M. El Hosieny, MD, Fatma Aboulkasem, MD,
Lung Cancer Imaging. Terence Z. Wong, MD,PhD. Department of Radiology Duke University Medical Center Durham, NC 9/9/09
 Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
MEDIASTINAL STAGING surgical pro
 MEDIASTINAL STAGING surgical pro Paul E. Van Schil, MD, PhD Department of Thoracic and Vascular Surgery University of Antwerp, Belgium Mediastinal staging Invasive techniques lymph node mapping cervical
MEDIASTINAL STAGING surgical pro Paul E. Van Schil, MD, PhD Department of Thoracic and Vascular Surgery University of Antwerp, Belgium Mediastinal staging Invasive techniques lymph node mapping cervical
Pleurectomy-decortication (P/D) was first popularized in
 was first popularized in") Technique of Pleurectomy and Decortication Andrew J. Kaufman, MD, and Raja M. Flores, MD Pleurectomy-decortication (P/D) was first popularized in the mid 1950s as a surgical method for treating entrapped
Technique of Pleurectomy and Decortication Andrew J. Kaufman, MD, and Raja M. Flores, MD Pleurectomy-decortication (P/D) was first popularized in the mid 1950s as a surgical method for treating entrapped
Lung cancer LUNG CANCER. Box 1 Clinical signs
 22 LUNG CANCER Lung cancer Bronchial carcinoma refers to two distinct clinical entities small cell and non-small cell carcinoma. Although these conditions have much in common, with broadly similar presenting
22 LUNG CANCER Lung cancer Bronchial carcinoma refers to two distinct clinical entities small cell and non-small cell carcinoma. Although these conditions have much in common, with broadly similar presenting
Lung Cancer 83 (2014) Contents lists available at ScienceDirect. Lung Cancer. journal homepage:
 Contents lists available at ScienceDirect. Lung Cancer. journal homepage:") Lung Cancer 83 (2014) 78 82 Contents lists available at ScienceDirect Lung Cancer journal homepage: www.elsevier.com/locate/lungcan Radical pleurectomy/decortication followed by high dose of radiation
Lung Cancer 83 (2014) 78 82 Contents lists available at ScienceDirect Lung Cancer journal homepage: www.elsevier.com/locate/lungcan Radical pleurectomy/decortication followed by high dose of radiation
Complex Thoracoscopic Resections for Locally Advanced Lung Cancer
 Complex Thoracoscopic Resections for Locally Advanced Lung Cancer Duke Thoracoscopic Lobectomy Workshop March 21, 2018 Thomas A. D Amico MD Gary Hock Professor of Surgery Section Chief, Thoracic Surgery,
Complex Thoracoscopic Resections for Locally Advanced Lung Cancer Duke Thoracoscopic Lobectomy Workshop March 21, 2018 Thomas A. D Amico MD Gary Hock Professor of Surgery Section Chief, Thoracic Surgery,
Video-Mediastinoscopy Thoracoscopy (VATS)
") Surgical techniques Video-Mediastinoscopy Thoracoscopy (VATS) Gunda Leschber Department of Thoracic Surgery ELK Berlin Chest Hospital, Berlin, Germany Teaching Hospital of Charité Universitätsmedizin Berlin
Surgical techniques Video-Mediastinoscopy Thoracoscopy (VATS) Gunda Leschber Department of Thoracic Surgery ELK Berlin Chest Hospital, Berlin, Germany Teaching Hospital of Charité Universitätsmedizin Berlin
Well-differentiated Papillary Mesothelioma of the Pleura Diagnosed by Video-Assisted Thoracic Surgical Pleural Biopsy : A Case Report
 Showa Univ J Med Sci 25 1, 67 72, March 2013 Case Report Well-differentiated Papillary Mesothelioma of the Pleura Diagnosed by Video-Assisted Thoracic Surgical Pleural Biopsy : A Case Report Yuri TOMITA
Showa Univ J Med Sci 25 1, 67 72, March 2013 Case Report Well-differentiated Papillary Mesothelioma of the Pleura Diagnosed by Video-Assisted Thoracic Surgical Pleural Biopsy : A Case Report Yuri TOMITA
The 7th Edition of TNM in Lung Cancer.
 10th European Conference Perspectives in Lung Cancer. Brussels, March 2009. The 7th Edition of TNM in Lung Cancer. Peter Goldstraw, Consultant Thoracic Surgeon, Royal Brompton Hospital, Professor of Thoracic
10th European Conference Perspectives in Lung Cancer. Brussels, March 2009. The 7th Edition of TNM in Lung Cancer. Peter Goldstraw, Consultant Thoracic Surgeon, Royal Brompton Hospital, Professor of Thoracic
APPROACH TO PLEURAL EFFUSIONS. Raed Alalawi, MD, FCCP
 APPROACH TO PLEURAL EFFUSIONS Raed Alalawi, MD, FCCP CASE 65-year-old woman with H/O breast cancer presented with a 1 week H/O progressively worsening exersional dyspnea. Physical exam: Diminished breath
APPROACH TO PLEURAL EFFUSIONS Raed Alalawi, MD, FCCP CASE 65-year-old woman with H/O breast cancer presented with a 1 week H/O progressively worsening exersional dyspnea. Physical exam: Diminished breath
Treatment of oligometastatic NSCLC
 Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón
 Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
HISTORY SURGERY FOR TUMORS WITH INVASION OF THE APEX 15/11/2018
 30 EACTS Annual Meeting Barcelona, Spain 1-5 October 2016 SURGERY FOR TUMORS WITH INVASION OF THE APEX lung cancer of the apex of the chest involving any structure of the apical chest wall irrespective
30 EACTS Annual Meeting Barcelona, Spain 1-5 October 2016 SURGERY FOR TUMORS WITH INVASION OF THE APEX lung cancer of the apex of the chest involving any structure of the apical chest wall irrespective
Lung Cancer Epidemiology. AJCC Staging 6 th edition
 Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Malignant pleural mesothelioma (MPM) is an aggressive
 is an aggressive") ORIGINAL ARTICLE Tomotherapy after Pleurectomy/Decortication or Biopsy for Malignant Pleural Mesothelioma Allows the Delivery of High Dose of Radiation in Patients with Intact Lung Emilio Minatel, MD,*
ORIGINAL ARTICLE Tomotherapy after Pleurectomy/Decortication or Biopsy for Malignant Pleural Mesothelioma Allows the Delivery of High Dose of Radiation in Patients with Intact Lung Emilio Minatel, MD,*
Malignant pleural mesothelioma (MPM) remains a major
 remains a major") Original Article Pleurectomy/Decortication is Superior to Extrapleural Pneumonectomy in the Multimodality Management of Patients with Malignant Pleural Mesothelioma Loïc Lang-Lazdunski, MD*, Andrea Bille,
Original Article Pleurectomy/Decortication is Superior to Extrapleural Pneumonectomy in the Multimodality Management of Patients with Malignant Pleural Mesothelioma Loïc Lang-Lazdunski, MD*, Andrea Bille,
General. for Thoracic Surgery GTS
 General Thoracic Surgery Radical pleurectomy/decortication and intraoperative radiotherapy followed by conformal radiation with or without chemotherapy for malignant pleural mesothelioma Terry T. Lee,
General Thoracic Surgery Radical pleurectomy/decortication and intraoperative radiotherapy followed by conformal radiation with or without chemotherapy for malignant pleural mesothelioma Terry T. Lee,
VATS after induction therapy: Effective and Beneficial Tips on Strategy
 VATS after induction therapy: Effective and Beneficial Tips on Strategy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J. Swanson, M.D. Professor of
VATS after induction therapy: Effective and Beneficial Tips on Strategy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J. Swanson, M.D. Professor of
Treatment of Clinical Stage I Lung Cancer: Thoracoscopic Lobectomy is the Standard
 Treatment of Clinical Stage I Lung Cancer: Thoracoscopic Lobectomy is the Standard AATS General Thoracic Surgery Symposium May 5, 2010 Thomas A. D Amico MD Professor of Surgery, Duke University Medical
Treatment of Clinical Stage I Lung Cancer: Thoracoscopic Lobectomy is the Standard AATS General Thoracic Surgery Symposium May 5, 2010 Thomas A. D Amico MD Professor of Surgery, Duke University Medical
Larry Tan, MD Thoracic Surgery, HSC. Community Cancer Care Educational Conference October 27, 2017
 Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Radiation Therapy in SCLC. What is New? Prof. Dr. Hoda Abdel Baky El Bakry Cairo Cancer Institute Radiation Oncology Department
 Radiation Therapy in SCLC What is New? Prof. Dr. Hoda Abdel Baky El Bakry Cairo Cancer Institute Radiation Oncology Department Background Overview Small Cell Lung cancer constitute about 15 % of all newly
Radiation Therapy in SCLC What is New? Prof. Dr. Hoda Abdel Baky El Bakry Cairo Cancer Institute Radiation Oncology Department Background Overview Small Cell Lung cancer constitute about 15 % of all newly
The incidence of malignant pleural mesothelioma
 Operation and Photodynamic Therapy for Pleural Mesothelioma: 6-Year Follow-up Thomas L. Moskal, MD, Thomas J. Dougherty, PhD, John D. Urschel, MD, Joseph G. Antkowiak, MD, Anne-Marie Regal, MD, Deborah
Operation and Photodynamic Therapy for Pleural Mesothelioma: 6-Year Follow-up Thomas L. Moskal, MD, Thomas J. Dougherty, PhD, John D. Urschel, MD, Joseph G. Antkowiak, MD, Anne-Marie Regal, MD, Deborah
Determining the Optimal Surgical Approach to Esophageal Cancer
 Determining the Optimal Surgical Approach to Esophageal Cancer Amit Bhargava, MD Attending Thoracic Surgeon Department of Cardiovascular and Thoracic Surgery Open Esophagectomy versus Minimally Invasive
Determining the Optimal Surgical Approach to Esophageal Cancer Amit Bhargava, MD Attending Thoracic Surgeon Department of Cardiovascular and Thoracic Surgery Open Esophagectomy versus Minimally Invasive
FDG PET/CT in Lung Cancer Read with the experts. Homer A. Macapinlac, M.D.
 FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
MALIGNANT PLEURAL MESOTHELIOMA: SPOTLIGHT ON RECENT ADVANCES IN DIAGNOSIS AND TREATMENT
 MALIGNANT PLEURAL MESOTHELIOMA: SPOTLIGHT ON RECENT ADVANCES IN DIAGNOSIS AND TREATMENT Aline N. Zouk, *Hitesh Batra Division of Pulmonary, Allergy, and Critical Care Medicine, University of Alabama at
MALIGNANT PLEURAL MESOTHELIOMA: SPOTLIGHT ON RECENT ADVANCES IN DIAGNOSIS AND TREATMENT Aline N. Zouk, *Hitesh Batra Division of Pulmonary, Allergy, and Critical Care Medicine, University of Alabama at
Lung Cancer. Current Therapy JEREMIAH MARTIN MBBCh FRCSI MSCRD
 Lung Cancer Current Therapy JEREMIAH MARTIN MBBCh FRCSI MSCRD Objectives Describe risk factors, early detection & work-up of lung cancer. Define the role of modern treatment options, minimally invasive
Lung Cancer Current Therapy JEREMIAH MARTIN MBBCh FRCSI MSCRD Objectives Describe risk factors, early detection & work-up of lung cancer. Define the role of modern treatment options, minimally invasive
Staging Issues: Lung Cancer & Mesothelioma. Mick Peake Clinical Lead, NCIN Chair, Lung SSCRG
 Staging Issues: Lung Cancer & Mesothelioma Mick Peake Clinical Lead, NCIN Chair, Lung SSCRG Staging systems Non-Small Cell Lung Cancer (>85%): UICC TNM v6 used until 1.1.10 transition since then to v7
Staging Issues: Lung Cancer & Mesothelioma Mick Peake Clinical Lead, NCIN Chair, Lung SSCRG Staging systems Non-Small Cell Lung Cancer (>85%): UICC TNM v6 used until 1.1.10 transition since then to v7
British Thoracic Society Guideline for the investigation and management of malignant pleural mesothelioma
 Additional material is published online only. To view, please visit the journal online (http:// dx. doi. org/ 10. 1136/ thoraxjnl- 2017-211321). For numbered affiliations see end of article. Correspondence
Additional material is published online only. To view, please visit the journal online (http:// dx. doi. org/ 10. 1136/ thoraxjnl- 2017-211321). For numbered affiliations see end of article. Correspondence
surgical approach for resectable NSCLC
 surgical approach for resectable NSCLC Dominique H. Grunenwald, MD, PhD Professor Emeritus in Thoracic and Cardiovascular surgery Pierre & Marie Curie University. Paris. France 1933 Graham EA, Singer JJ.
surgical approach for resectable NSCLC Dominique H. Grunenwald, MD, PhD Professor Emeritus in Thoracic and Cardiovascular surgery Pierre & Marie Curie University. Paris. France 1933 Graham EA, Singer JJ.
Combined modality treatment for N2 disease
 Combined modality treatment for N2 disease Dr Clara Chan Consultant in Clinical Oncology 3 rd March 2017 Overview Background The evidence base Systemic treatment Radiotherapy Future directions/clinical
Combined modality treatment for N2 disease Dr Clara Chan Consultant in Clinical Oncology 3 rd March 2017 Overview Background The evidence base Systemic treatment Radiotherapy Future directions/clinical
Radiological staging of lung cancer. Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh
 Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Charles Mulligan, MD, FACS, FCCP 26 March 2015
 Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Controversies in management of squamous esophageal cancer
 2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
REVIEW. The role of imaging in the management of primary pleural malignancies
 Cancer Imaging (2003) 3, 139 145 DOI: 10.1102/1470-7330.2003.0020 CI REVIEW The role of imaging in the management of primary pleural malignancies C S Ng Department of Radiology, MD Anderson Cancer Center,
Cancer Imaging (2003) 3, 139 145 DOI: 10.1102/1470-7330.2003.0020 CI REVIEW The role of imaging in the management of primary pleural malignancies C S Ng Department of Radiology, MD Anderson Cancer Center,
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease
 Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
National Mesothelioma Audit. National Mesothelioma Audit report 2018 (for the audit period )
") National Mesothelioma Audit National Mesothelioma Audit report 2018 (for the audit period 2014 16) The Royal College of Physicians (RCP) plays a leading role in the delivery of high-quality patient care
National Mesothelioma Audit National Mesothelioma Audit report 2018 (for the audit period 2014 16) The Royal College of Physicians (RCP) plays a leading role in the delivery of high-quality patient care
Enterprise Interest None
 Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
Enterprise Interest None Cervical Cancer -Management of late stages ESP meeting Bilbao Spain 2018 Dr Mary McCormack PhD FRCR Consultant Clinical Oncologist University College Hospital London On behalf
Pneumonectomy After Induction Rx: Is it Safe?
 Pneumonectomy After Induction Rx: Is it Safe? David J. Sugarbaker, M.D. Director, Chief, Division of Thoracic Surgery The Olga Keith Weiss Chair of Surgery of Medicine at, Pneumonectomy after induction
Pneumonectomy After Induction Rx: Is it Safe? David J. Sugarbaker, M.D. Director, Chief, Division of Thoracic Surgery The Olga Keith Weiss Chair of Surgery of Medicine at, Pneumonectomy after induction
PET CT for Staging Lung Cancer
 PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
PET CT for Staging Lung Cancer Rohit Kochhar Consultant Radiologist Disclosures Neither I nor my immediate family members have financial relationships with commercial organizations that may have a direct
The epidemiology of mesothelioma first came to light in
 Treatment of Malignant Pleural Mesothelioma: Pleurectomy with Adjuvant Therapy Raja M. Flores, MD,* and Naveed Alam, MD The epidemiology of mesothelioma first came to light in 1960 with the report by Wagner
Treatment of Malignant Pleural Mesothelioma: Pleurectomy with Adjuvant Therapy Raja M. Flores, MD,* and Naveed Alam, MD The epidemiology of mesothelioma first came to light in 1960 with the report by Wagner
Positron emission tomography predicts survival in malignant pleural mesothelioma
 Flores et al General Thoracic Surgery Positron emission tomography predicts survival in malignant pleural mesothelioma Raja M. Flores, MD, a Timothy Akhurst, MD, b Mithat Gonen, PhD, c Maureen Zakowski,
Flores et al General Thoracic Surgery Positron emission tomography predicts survival in malignant pleural mesothelioma Raja M. Flores, MD, a Timothy Akhurst, MD, b Mithat Gonen, PhD, c Maureen Zakowski,
Sponsored document from The Lancet Oncology
 Sponsored document from The Lancet Oncology Extra-pleural pneumonectomy versus no extra-pleural pneumonectomy for patients with malignant pleural mesothelioma: clinical outcomes of the Mesothelioma and
Sponsored document from The Lancet Oncology Extra-pleural pneumonectomy versus no extra-pleural pneumonectomy for patients with malignant pleural mesothelioma: clinical outcomes of the Mesothelioma and
Leah Taylor Mesothelioma UK CNS Team Leader
 Leah Taylor Mesothelioma UK CNS Team Leader Mesothelioma Update EAG Audit Event Thursday 27 th September 2018 2 National Mesothelioma Audit report 2018 3 4 Performance National Pathological subtype 64%
Leah Taylor Mesothelioma UK CNS Team Leader Mesothelioma Update EAG Audit Event Thursday 27 th September 2018 2 National Mesothelioma Audit report 2018 3 4 Performance National Pathological subtype 64%
Understanding surgery
 What does surgery for lung cancer involve? Surgery for lung cancer involves an operation, which aims to remove all the cancer from the lung. Who will carry out my operation? In the UK, we have cardio-thoracic
What does surgery for lung cancer involve? Surgery for lung cancer involves an operation, which aims to remove all the cancer from the lung. Who will carry out my operation? In the UK, we have cardio-thoracic
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer
 Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Case presentation. Paul De Leyn, MD, PhD Thoracic Surgery University Hospitals Leuven Belgium
 Case presentation Paul De Leyn, MD, PhD Thoracic Surgery University Hospitals Leuven Belgium Perspectives in Lung Cancer Brussels 6-7 march 2009 LEUVEN LUNG CANCER GROUP Department of Thoracic Surgery
Case presentation Paul De Leyn, MD, PhD Thoracic Surgery University Hospitals Leuven Belgium Perspectives in Lung Cancer Brussels 6-7 march 2009 LEUVEN LUNG CANCER GROUP Department of Thoracic Surgery
The International Association for the Study of Lung Cancer (IASLC) Lung Cancer Staging Project, Data Elements
 Lung Cancer Staging Project, Data Elements") Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
AJCC-NCRA Education Needs Assessment Results
 AJCC-NCRA Education Needs Assessment Results Donna M. Gress, RHIT, CTR Survey Tool 1 Survey Development, Delivery, Analysis THANKS to NCRA for the following work Developed survey with input from partners
AJCC-NCRA Education Needs Assessment Results Donna M. Gress, RHIT, CTR Survey Tool 1 Survey Development, Delivery, Analysis THANKS to NCRA for the following work Developed survey with input from partners
Malignant pleural mesothelioma (MPM) affects nearly
 affects nearly") ORIGINAL ARTICLE Patterns of Local and Nodal Failure in Malignant Pleural Mesothelioma After Extrapleural Pneumonectomy and Photon-Electron Radiotherapy Vishal Gupta, MD,* Lee M. Krug, MD, Benjamin Laser,
ORIGINAL ARTICLE Patterns of Local and Nodal Failure in Malignant Pleural Mesothelioma After Extrapleural Pneumonectomy and Photon-Electron Radiotherapy Vishal Gupta, MD,* Lee M. Krug, MD, Benjamin Laser,
Lung cancer Surgery. 17 TH ESO-ESMO MASTERCLASS IN CLINICAL ONCOLOGY March, 2017 Berlin, Germany
 17 TH ESO-ESMO MASTERCLASS IN CLINICAL ONCOLOGY 24-29 March, 2017 Berlin, Germany Lung cancer Surgery Sven Hillinger MD, Thoracic Surgery, University Hospital Zurich Case 1 59 y, female, 40 py, incidental
17 TH ESO-ESMO MASTERCLASS IN CLINICAL ONCOLOGY 24-29 March, 2017 Berlin, Germany Lung cancer Surgery Sven Hillinger MD, Thoracic Surgery, University Hospital Zurich Case 1 59 y, female, 40 py, incidental
Case Conference: Post-Operative Radiotherapy for Non-Small Cell Lung Cancer. Doug Rahn 6/1/12
 Case Conference: Post-Operative Radiotherapy for Non-Small Cell Lung Cancer Doug Rahn 6/1/12 Outline I. Presentation of Case II. Epidemiology III. Staging IV. Review of Literature V. Recommendations VI.
Case Conference: Post-Operative Radiotherapy for Non-Small Cell Lung Cancer Doug Rahn 6/1/12 Outline I. Presentation of Case II. Epidemiology III. Staging IV. Review of Literature V. Recommendations VI.
Radical Pleurectomy and Intraoperative Photodynamic Therapy for Malignant Pleural Mesothelioma
 Radical Pleurectomy and Intraoperative Photodynamic Therapy for Malignant Pleural Mesothelioma Joseph S. Friedberg, MD, Melissa J. Culligan, BSN, Rosemarie Mick, MS, James Stevenson, MD, Stephen M. Hahn,
Radical Pleurectomy and Intraoperative Photodynamic Therapy for Malignant Pleural Mesothelioma Joseph S. Friedberg, MD, Melissa J. Culligan, BSN, Rosemarie Mick, MS, James Stevenson, MD, Stephen M. Hahn,
Malignant pleural mesothelioma (MPM) remains a major
 remains a major") ORIGINAL ARTICLE Pleurectomy/Decortication, Hyperthermic Pleural Lavage with Povidone-Iodine Followed by Adjuvant Chemotherapy in Patients with Malignant Pleural Mesothelioma Loïc Lang-Lazdunski, MD, PhD,
ORIGINAL ARTICLE Pleurectomy/Decortication, Hyperthermic Pleural Lavage with Povidone-Iodine Followed by Adjuvant Chemotherapy in Patients with Malignant Pleural Mesothelioma Loïc Lang-Lazdunski, MD, PhD,
Thoracic Surgery. Treating a wide range of chest disorders
 Thoracic Surgery Treating a wide range of chest disorders Thoracic Surgery at UCLA The UCLA Division of Cardiothoracic Surgery is among the nation s leaders in providing care for a wide range of chest
Thoracic Surgery Treating a wide range of chest disorders Thoracic Surgery at UCLA The UCLA Division of Cardiothoracic Surgery is among the nation s leaders in providing care for a wide range of chest
EVIDENCE BASED MANAGEMENT OF STAGE III NSCLC MILIND BALDI
 EVIDENCE BASED MANAGEMENT OF STAGE III NSCLC MILIND BALDI Overview Introduction Diagnostic work up Treatment Group 1 Group 2 Group 3 Stage III lung cancer Historically was defined as locoregionally advanced
EVIDENCE BASED MANAGEMENT OF STAGE III NSCLC MILIND BALDI Overview Introduction Diagnostic work up Treatment Group 1 Group 2 Group 3 Stage III lung cancer Historically was defined as locoregionally advanced